
Phylogeny and evolutionary history of the blister beetles (Coleoptera, Meloidae)
Br J clin Pharmac 1994; 38: 221-227
The stereoselective disposition of the enantiomers ofibuprofen in blood, blister and synovial fluid
P. SEIDEMAN', F. LOHRER2, G.G. GRAHAM2, M.W. DUNCAN3, K.M. WILLIAMS2 & R.O. DAY2'Department of Internal Medicine, Division of Rheumatologi, Karolinska Institutet, S-18288 Danderyd, Sweden,2Department of Clinical Pharmacology and Toxicology, St Vincent's Hospital, and School of Physiology andPharmacology, University of New South Wales, Sydney, 2033 and 3Biomedical Mass Spectrometry Unit, Universityof New South Wales, Sydney, 2033, Australia
1 A sensitive, stereospecific assay using gas chromatography-mass spectrometry(GC/MS) was established to measure the concentrations of the enantiomers ofibuprofen in small volumes (50 gl) of blister fluid.
2 The concentrations of the enantiomers in blister fluid, assessed in eight patients,were similar to those in synovial fluid, both fluids behaving as peripheral compart-ments with respect to plasma.
3 The mean rate constants of transfer of R-ibuprofen into (0.14 ± 0.06 h-1) and outof (0.20 ± 0.04 h-1) blister fluid were not significantly different from those forsynovial fluid (0.19 ± 0.12 h-1, 0.34 ± 0.11 h-1, respectively). Similarly, the meanrate constants of transfer of S-ibuprofen into (0.22 ± 0.07 h-1) and out of (0.27 +0.08 h-1) blister fluid were not significantly different from those for synovial fluid(0.29 ± 0.10, 0.36 ± 0.11 h-1). However, the correlations were poor between thetransfer constants for each of the enantiomers between plasma, and both blisterand synovial fluid (P > 0.2).
4 The complex rate constant of transfer of S-ibuprofen into blister fluid (0.22 +0.07 h-1) was greater than that of R-ibuprofen (0.14 ± 0.07 h-1), which may beexplained by the lesser protein binding of the S-enantiomer.
5 The mean AUC of the S-enantiomer was greater than of the R-enantiomer in bothblister (116 ± 43 mg 1-' h, 73 ± 32 mg 1-l h, respectively; P < 0.05) and insynovial fluid (110 ± 28 mg 1-' h, 56 ± 8 mg 1-F h, respectively; P < 0.01). Thedifference between the mean AUC values of the enantiomers in synovial fluid vsblister fluid was not significant.
6 Despite similar concentration-time profiles, and mean pharmacokinetic par-ameters, blister fluid was not a good model for predicting the kinetics of theenantiomers of ibuprofen in synovial fluid in individual patients. However, theblister as a peripheral compartment, better simulates the time course of concen-trations in synovial fluid than does plasma, and consequently drug concentrationstherein might better relate to clinical efficacy than do those in plasma.
Keywords stereoselectivity ibuprofen enantiomers
Introduction
The major site of action of the non-steroidal anti- pharmacodynamic studies. Drug concentrations ininflammatory drugs (NSAIDs) in the treatment of synovial fluid may better reflect those in the syn-rheumatic diseases is probably the synovium but this ovium than plasma concentrations. However, thetissue is not easily sampled for pharmacokinetic and collection of synovial fluid is not always possible and
Correspondence: Dr Kenneth Williams, Department of Clinical Pharmacology and Toxicology, St Vincent's Hospital, VictoriaStreet, Darlinghurst, NSW, 2010, Australia
221

222 P. Seideman et al.
a suggested alternative is to measure drug in blisterfluid. Suction-induced blisters have been used toassess the pharmacokinetics of antimicrobials inextravascular fluid [1-4] and a recent study demon-strated that the time courses of the concentations ofthe enantiomers of ibuprofen in blister fluid resemblethose in synovial fluid [5]. However, in this study thekinetics of ibuprofen were evaluated only in blisterfluid and the findings compared with the kinetics insynovial fluid from other subjects in a separate study.By contrast, in the present study, the pharmaco-kinetics of ibuprofen were examined in both synovialand blister fluids in the sample patients to determinewhether blister fluid is a sutiable alternative tosynovial fluid in investigations of the extravascularpharmacokinetics of this NSAID. Additionally,ibuprofen has a rather complex metabolic disposition,being racemic with the interesting feature that thereis chiral inversion of the R-enantiomer to the S-enantiomer in vivo [6,7]. The latter is a much morepotent inhibitor of prostanoid synthesis [8]. For thesereasons, it was also important that concentrations ofthe individual enantiomers be monitored.
5000 h.p.l.c., a Waters Wisp 710B autosampler anda Hitachi F 1000 fluorescence detector (excitation225 nm, emission 290 nm). A Beckman UltrasphereC-18 reversed phase column (5 p, 4.6 mm x 25 cm)was used. The mobile phase was acetonitrile (58%v/v), water (42% v/v), triethylamine (0.0002%v/v), and acetic acid (0.001% v/v) at a flow rate of1.6 ml min-'.
Study protocol
The study was conducted in patients with rheumatoidarthritis and chronic effusions of the knee. Writteninformed consent from the patients and approval fromthe ethics committee of the Karolinska Hospital wereobtained. Blisters were made by suction [9] immedi-ately prior to the study. Ibuprofen tablets (Boots, 2 x600 mg) were taken after the patients had fastedovernight. Blood, blister (5) and synovial (10) fluidswere collected aseptically at 1, 2, 4, 6, 8, 12 and 24 hafter dosage. The blood was collected into Venoject®tubes and the plasma separated and stored at -20° Cuntil assay.
Analytical method-assay of ibuprofen enantiomers
Methods
Materials
The enantiomers and racemate of ibuprofen were sup-plied by the Boots Company PLC, U.K. who alsosupplied the internal standard, (R)-flurbiprofen, forthe h.p.l.c. assay. The internal standard for GC/MSanalysis, S-[2H3]-ibuprofen, was synthesised in-houseand was shown to be 94% isotopically pure (6%undeuterated, 94% trideuterated). Data were correctedfor the isotopic impurity.
The Sigma Chemical Company (St Louis, MO,USA) supplied 1,1-carbonyldiimidazole (CDI) andAldrich Chemical Co. (Milwaukee, Wis, USA) (S)-ax-methylbenzylamine (S-MBA; >98% optically pure).A Hewlett-Packard 5890 Series II gas chromato-
graph directly interfaced with a Hewlett-Packard5971A mass selective detector was used for all quan-titative GC/MS analyses. Gas chromatography wasperformed using a fused silica capillary column(12 m x 0.22 mm i.d., cross-linked methylsiliconestationary phase BPI, 0.33 ,um film thickness; SGEScientific, Australia). Helium was the carrier gas(inlet pressure 34 kPa). The oven temperature washeld at 800 C for 1 min and then raised to 280° C at300 C/min. A split/splitless injector operated in thesplitless mode was used (split flow 50 ml min-',septum purge approx. 1.0 ml min'-). A Hewlett-Packard 7673A autoinjector was used to deliversamples (1 1l) to the column. The injection portand GC/MS interface were maintained at 2500 Cand 280°C, respectively. For quantitation, masses ofm/z 309 and m/z 312 were scanned (dwell-time50 ms).
H.p.l.c. analyses were performed using a Varian
The enantiomers of ibuprofen were assayed byh.p.l.c. (plasma) and by GC/MS (blister fluid andsynovial fluid). The stereospecific assay was based onthe preparation of the diastereomeric amides pro-duced by reaction with S-a-methylbenzylaminedescribed previously for GC/MS analyses by Baillieet al. [11], but was further developed to allow thesensitivity required to assay the small samplevolumes of blister fluid (30-50 gl).
Plasma Plasma (0.8 ml) was extracted with hexane-ether (70:30; 10 ml) after addition of internalstandard (5 pg) and acidification with HCI solution(0.5 ml, 3 N). The organic layer was evaporated undernitrogen and to the residue was added a freshlyprepared solution of CDI in toluene (0.5 ml, 5.0 mgml-'). After 10 min at room temperature, glacialacetic acid (10 p.l) was added followed by S-MBA(50 p.l). Samples were allowed to stand for 1 hand, after acidification (5 ml, 0.2 N HCI), theywere extracted into toluene (0.5 ml). The toluenewas evaporated under nitrogen and the residueresuspended in mobile phase (100 gl).
Blister and synovial fluid
Extraction and derivatisation were as for plasmasamples but only 50 ,l of sample was taken, and25 ng internal standard was added. Derivatisation wasaccomplished with 250 pl CDI and 25 pl S-MBA.Samples were resuspended in toluene (20 p1) forGC/MS analysis.
GCMS analysis Peak area ratios were used to estab-lish standard curves and for sample analysis. Day-to-day variability in the GC/MS assay was assessed at

Ster-eoselective disposition of ibuprofen 223
drug concentrations of 0.25, 1.0, 5.0, 10.0 and 20.0gg ml-1. A full set of standards and a quality controlspecimen were analysed with each batch of samples.Standard curves were generated by unweighted least-squares linear regression analysis using the ratio ofthe 309/312 ion pair.
Pharmacokinetic modelling
Plasma concentrations of the ibuprofen enantiomers(C) were fitted by two or three exponential functionsof the general form:
C = C.e-Xit (1)
where C. and Xi are constants. If it is assumed that theibuprofen enantiomers are transferred between thecentral compartment of distribution and synovial or
blister fluids by first order processes and that theamounts so transfered do not alter the concentrationsin the central compartment significantly [12,13], thenthe concentrations in these fluids are defined byequations 2 and 3.
c k -VC/V [X;C.-(e-Xite ksPt)/(k (2)
Cb =kpb Vc/Vb[Ci.(eit-e kbPt)/(kbp_ki)] (3)
where k and kpb are the first order rate constants oftransfer from the central compartment to synovial andblister fluids, while Vc, Vs and Vb are the volumes ofthe central compartment, synovial fluid and blisterfluid, respectively. The rate constants of loss fromsynovial and blister fluids are ksp and kbp' respect-ively. The constants C1, kX, ks kbp and the complexconstants k 1//VK and kbp V/_ were determined bysimultaneous logarithmic least squares analysis usingthe Minim program (R.D. Purves, University ofOtago, New Zealand). The ratios of these kinetic andvolume constants were also determined. These were
k Vc/ks V andkspbV Ikbp Vb. These ratios representthe ratios of the clearances of the drugs into andout of synovial and blister fluids, respectively[14,15]. The areas under the time-course of drug con-
centrations in plasma, synovial and blister fluids(AUC, AUCS and AUCb) were determined by trap-ezoidal integration.
Statistical analysis
Data were analysed using the paired Student's t-test.
Results
Assay validation
Day-to-day variability in the GC/MS assay (n = 7) ofthe enantiomers of ibuprofen in synovial fluid was
less than 8.6% at all concentrations. Similarly, forblister fluid, the coefficients of variation were lessthan 7.2% for all concentrations for each enantiomer,except for R-ibuprofen at 0.25 gg ml-' (12.0%). Themean measured value of each standard for eachenantiomer was within 5% of the spiked value.
H.p.l.c. retention times were: 12.0 min and 13.5min for S-ibuprofen and R-ibuprofen, respectively,and 8.5 min for S-flurbiprofen. The coefficients ofvariation were less than 5.0% for each enantiomer at2.0 ,ug ml-' and 5.0 ,ug ml-' for analysis of plasmasamples (n = 4).
Pharmacokinetics of enantiomers in blood, blisterand synovial fluid
The concentrations of the enantiomers in both fluidswere initially lower than those in plasma butexceeded the plasma concentrations after about 4 to8 h. In two patients, the concentrations of bothenantiomers were initially higher in blister fluid thansynovial fluid, while in two other patients the concen-
trations were higher in synovial fluid than in blisterfluid for about 2 h after dosage. As shown by thegreater values of AUCS and AUCb (Table 1), the con-
centrations of the S-enantiomer were, on average,greater than those of the R-enantiomer in bothsynovial and blister fluids. There was no correspond-ing difference between the enantiomers with respectto the plasma AUC values of the R- and S-enantiomers, although plasma AUC was considerablygreater for the S-enantiomer in four of the seven
patients.The main aim of the study was to compare the
kinetics of the enantiomers in blister fluid with those
Table 1 Mean (± 95% confidence limits) constants describing the transferof R-ibuprofen and S-ibuprofen into and out of synovial and blister fluids
S-ibupr-ofen R-ibuprofen P Difference S vs R
kps-Vc/Vs (h-') 0.29 ± 0.10 0.19 ± 0.12 < 0.01 0.10 ± 0.06
ksp (h-1) 0.36±0.11 0.34±0.11 NS 0.03 ±0.09
kpb VVb (h 1) 0.22 ± 0.07 0.14 ± 0.06 < 0.01 0.08 ± 0.05
kbp (h-') 0.27 ± 0.08 0.20 ± 0.04 < 0.05 0.07 ± 0.05
AUC(mgl- h) 134±47 94±21 NS 40±47
AUCS (mg 1-1 h) 116 ± 29 58 ± 8 < 0.01 58 ± 34
AUCb (mg 1-1 h) 120 ± 48 78 ± 34 < 0.05 42 ± 38
224 P. Seideman et al.
in synovial fluid with the greater interest in thepharmacokinetics of S-ibuprofen because of its moremarked pharmacological activity. There was nodifference between AUCS and AUCb for either enan-tiomer in synovial fluid and blister fluid. There was asignificant, although weak correlation between thevalues of AUCS and AUCb for S-ibuprofen (r2 = 0.62,P < 0.05). No such correlation was observed for theR-enantiomer.
The data were well described by the model equa-tions (Figure 1) and both the synovial and blisterfluids behaved pharmacokinetically as peripheralcompartments of distribution of the ibuprofen enan-tiomers. In four of the seven patients, the absorptionphase was not well defined and the rate constant ofabsorption was set at 2.1 h-', corresponding to a halflife of absorption of 20 min. However, changing thehalf-life of absorption to 10 or to 30 min changed thehalf-lives of transfer into or out of the synovial orblister fluids by less than 20% and did not alter thegeneral conclusions of the study. In most patients, alag time had to be introduced to the time variable
35
30 R-ibuprofenP
25
20-
15
10 SF
I 5
E B
0 5 10 15 20 25 3c0
C 35 -0) I.
o03
in equation 3 to provide a satisfactory fit to theexperimental data.
There was a trend for the rate constants describingthe kinetics of transfer into and out of blister fluid tobe smaller than the corresponding kinetic constantsfor synovial fluid (Table 1, Figure 2) but most con-trasts were not significant. The rate constant fordiffusion of R-ibuprofen from blister fluid wassmaller than that from synovial fluid (P = 0.05). Themean rate constants of loss of S-ibuprofen fromsynovial and blister fluids were 0.36 and 0.27 h-1,corresponding to half-lives of 1.9 and 2.6 h. Thesehalf-lives are of the order of the values of theinitial half-lives of the equations. The delayedtimes at which peaks were produced is due to therelatively slow loss of the enantiomers from thesecompartments.The correlations between the kinetic constants of
transfer of the enantiomers into or out of synovialfluid and the corresponding constants in blister fluidwere poor and not statistically significant (r2 < 0.3,P > 0.20). In most patients, the rate constants of
1F
p
B
5 0
Time (h)
S-ibuprofen
p
lop kt SF
p
B
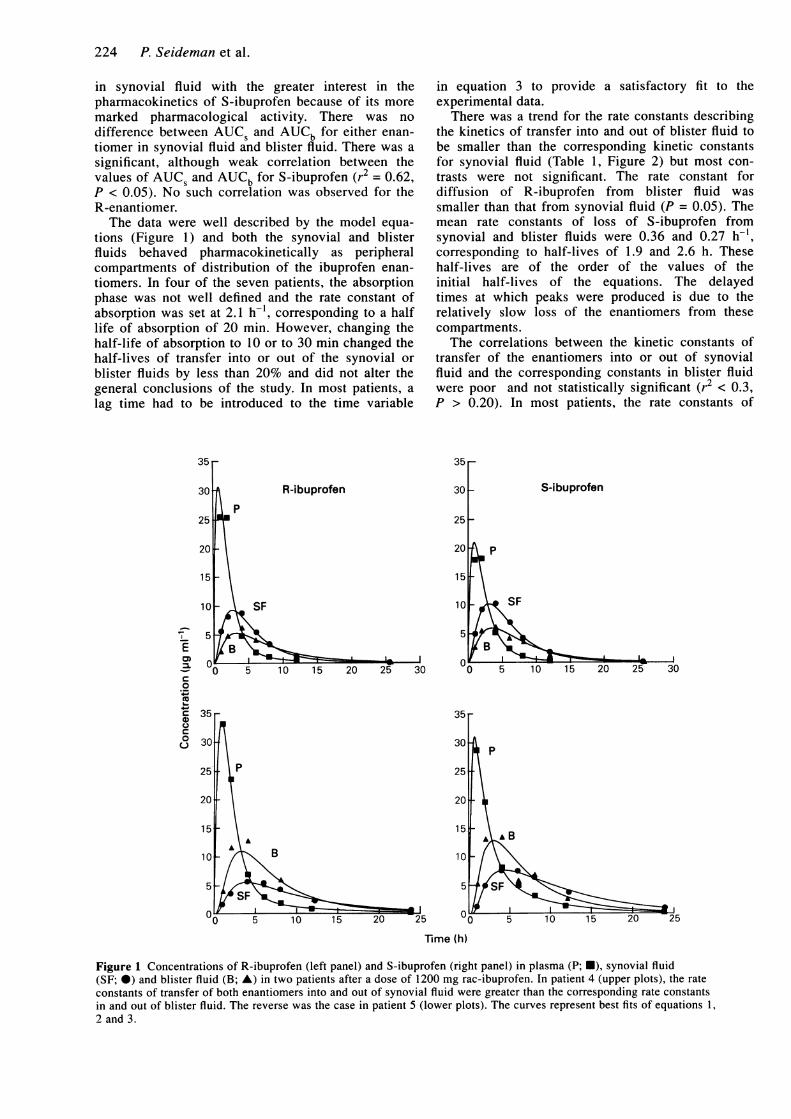
Figure 1 Concentrations of R-ibuprofen (left panel) and S-ibuprofen (right panel) in plasma (P; U), synovial fluid(SF; 0) and blister fluid (B; A) in two patients after a dose of 1200 mg rac-ibuprofen. In patient 4 (upper plots), the rateconstants of transfer of both enantiomers into and out of synovial fluid were greater than the corresponding rate constantsin and out of blister fluid. The reverse was the case in patient 5 (lower plots). The curves represent best fits of equations 1,2 and 3.
Stereoselective disposition of ibuprofen 225
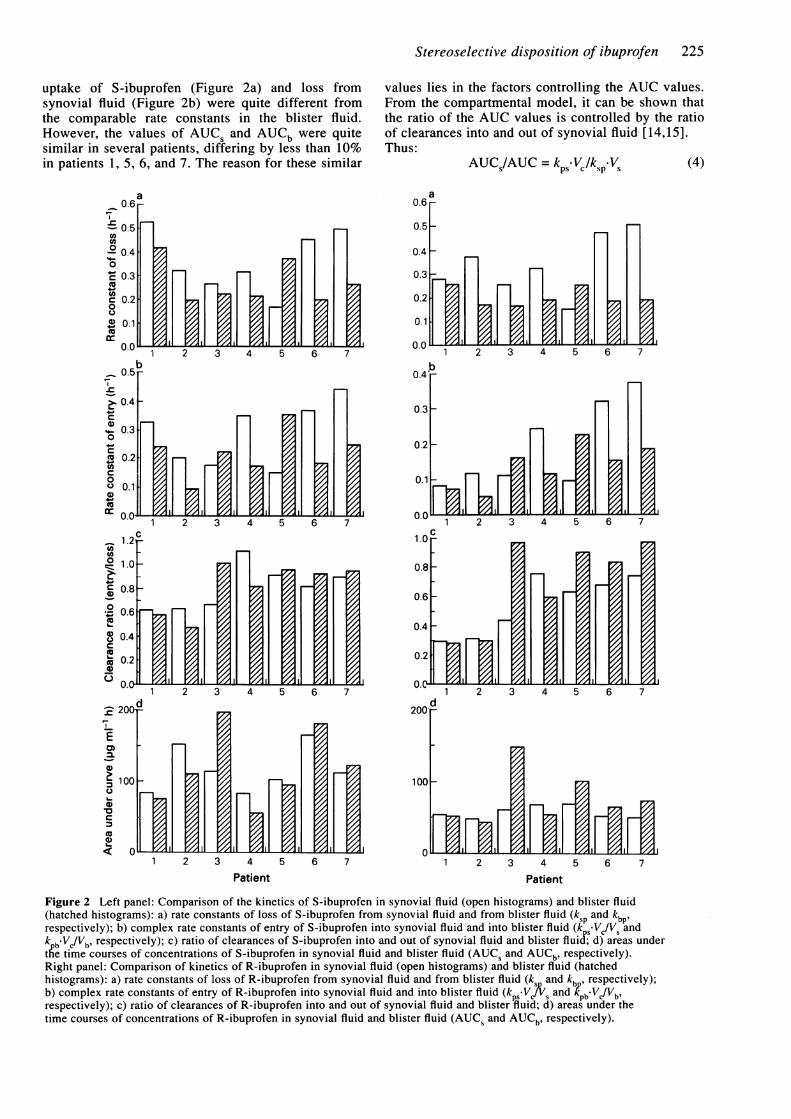
uptake of S-ibuprofen (Figure 2a) and loss fromsynovial fluid (Figure 2b) were quite different fromthe comparable rate constants in the blister fluid.However, the values of AUCS and AUCb were quitesimilar in several patients, differing by less than 10%in patients 1, 5, 6, and 7. The reason for these similar
values lies in the factors controlling the AUC values.From the compartmental model, it can be shown thatthe ratio of the AUC values is controlled by the ratioof clearances into and out of synovial fluid [14,15].Thus:
AUC /AUC = kp5 .1/JksVs Ps
- Vc /k~~~~s. (4)
ao.6 r
0.5H
0.4
0.31.3O37
1 2 3 4 5 6 7
b0.4_
0.3
0.2
I, I Ir
1 2 3 4 5
2 3 4 5
,
1 2 3 4 5 6 7Patient
Figure 2 Left panel: Comparison of the kinetics of S-ibuprofen in synovial fluid (open histograms) and blister fluid(hatched histograms): a) rate constants of loss of S-ibuprofen from synovial fluid and from blister fluid (ksp and kbPlrespectively); b) complex rate constants of entry of S-ibuprofen into synovial fluid and into blister fluid (k s-V/V andk -V /Vb, respectively); c) ratio of clearances of S-ibuprofen into and out of synovial fluid and blister fluiJ; d) areas underthe time courses of concentrations of S-ibuprofen in synovial fluid and blister fluid (AUCS and AUCb, respectively).Right panel: Comparison of kinetics of R-ibuprofen in synovial fluid (open histograms) and blister fluid (hatchedhistograms): a) rate constants of loss of R-ibuprofen from synovial fluid and from blister fluid (ks and kb, respectively);b) complex rate constants of entry of R-ibuprofen into synovial fluid and into blister fluid (kpS.VSj and k'pbVc/Vb,respectively); c) ratio of clearances of R-ibuprofen into and out of synovial fluid and blister fluid; d) areas under thetime courses of concentrations of R-ibuprofen in synovial fluid and blister fluid (AUCS and AUCb, respectively).
a
r 12
b2 3 4 E
.
6
r
H
0.6e-
- 0.50
° 0.4'4.-
0
C 0.3
c 0.20
@ 0.1incs
0.5
0.4
0.30
X 0.2
0.10.
01.2
0 1.0
0.8a)
0o 06
@ 0.4
, 0.2
0.0
M 200
E
100
O
1,71 2 3 i
I. I
d
PIr IF IF
Patient
U. ( l l ZA--- --
n nl -L
Il .,A1 z~ 1r
E1-
i If
P.oo000000
I
6
vv 1
L
u.u 1--K"- II VA
226 P. Seideman et al.
A similar relationship exists for the ratio AUCb/AUC.The influence of these factors on the AUC values canbe seen, for example, in patient 5. Both the complexrate constant of uptake into and the rate constant ofloss from synovial fluid are smaller than the compar-able rate constants of blister fluid (Figure 2a,b).However, the ratios of the constants, the clearanceratios, are similar and the values of AUCS and AUCbare, therefore, nearly identical (Figure 2c,d). Becauseof the faster transfer of S-ibuprofen both into and outof blister fluid, the concentration of S-ibuprofenpeaks earlier in blister fluid but is less sustained thanin synovial fluid (Figure 1, Patient 5). The values ofAUCS and AUCb of R-ibuprofen were not as close aswas the case with the S-enantiomer. In only twopatients was AUCb of R-ibuprofen within 15% of thevalue of AUCS.
Discussion
The pharmacokinetics of antiinflammatory drugs havebeen investigated in synovial fluid because the con-centrations at this site might reflect those in the pre-sumed site of action of the drug, the synovium, betterthan concentrations in plasma. Multiple, sequentialsampling of the synovial cavity can be carried outsafely, but does pose a potential, although very small,risk of infection and may not be acceptable to allpatients. Consequently, there has been an interest insuction blisters as a model to simulate extravascularcompartments such as the synovial cavity and toassess the kinetics and dynamics of drugs. Suctionblisters allow sequential sampling with virtually nomorbidity and greater acceptability, but limit samplesto very small volumes, typically 30-50 gl from eachblister. This presents analytical problems but thesewere overcome in the present study by developing asensitive, stereospecific assay based on preparation ofthe diastereomers of ibuprofen after reaction ofthe enantiomers with a well known, chiral reagent,S-a-methylbenzylamine and the subsequent use ofGC/MS for resolution and detection. These drugs aregenerally administered as their racemates butantiinflammatory activity is believed to resideentirely in the S-enantiomers [16]. Additionally, thereis stereospecific chiral inversion of R-ibuprofen to S-ibuprofen in humans [17]. Consequently, stereoselec-tive analysis is important for a proper understandingof the disposition of the 2-arylpropionates. However,surprisingly, while S-ibuprofen is an effectiveantiinflammatory agent [18], correlations betweenplasma concentrations and measures of clinicalefficacy were not improved when the concentrationdata were expressed in terms of the S-ibuprofen ascompared with R,S-ibuprofen [19].
Induction of suction blisters appears to be primar-ily a non-inflammatory event with few inflammatorycells present in the blister fluid at least up to 24 hafter blister induction [20]. Inflammation can beinduced in the blister to give a comparativeinflammatory exudate model. The present study pro-
vided data with respect to a non-inflammatory modeland results may differ when inflammation is present.However, it was felt that study of the non-inflamma-tory model was more appropriate in the first instance.Blister fluid also differs from synovial fluid in that,although hyaluronic acid concentrations are approxi-mately 100 times higher in blister fluid than inplasma [21], they are still orders of magnitude lowerthan in synovial fluid. However, this difference maynot be important because ibuprofen does not bind tohyaluronate.
The concentrations of the ibuprofen enantiomers inblister fluid and synovial fluid followed a qualita-tively similar pattern consistent with data reported ina recent preliminary study [5]. Both the synovial fluidand blister fluid behaved pharmacokinetically asperipheral compartments of distribution of theibuprofen enantiomers, and both required lag times toaccomodate the data. The delay in the appearance ofibuprofen in blister fluid is consistent with datareported for other drugs such as antibiotics [4,22].The mean rate constants for transfer of the ibu-
profen enantiomers into and out of synovial fluid(Table 1) were within 25% of the values found pre-viously during the chronic administration of ibu-profen [7] although the range of values was muchsmaller. Furthermore, as again observed previously[7] the complex rate constant describing transfer ofS-ibuprofen into synovial fluid was greater than thatfor R-ibuprofen. This difference is consistent with alower binding of the S-enantiomer to plasma proteinsas reported previously (percent unbound, 0.419 cf.0.613, R- and S-ibuprofen, respectively, [23], andindicates that the enantiomers diffuse into synovialfluid mainly in the protein free forms. A similar con-trast was seen with blister fluid (Table 1), but thetransfer of S-ibuprofen was, in addition, faster out ofblister fluid. Unfortunately, the limitations of smallblister fluid volumes and analytical sensitivity pre-cluded an assessment of unbound enantiomer concen-trations in this study which may have given a betterunderstanding of the relative distribution of drugbetween the compartments.
Despite the general lack of significance in thedifference in the kinetics of transfer of ibuprofenbetween the compartments, the kinetics of the enan-tiomers in the two fluids cannot be said to be identi-cal, there being a poor correlation between the rateconstants for the compartments. The interpatient dif-ferences in the kinetic constants of transfer into orout of blister fluid were not parallelled by the corre-sponding rate constants for synovial fluid and, inindividual patients, the kinetics in blister fluid werenot predictive of the kinetics in synovial fluid (Figure1, Table 1). The values of AUCS and AUCb weremore closely related than the individual rate constantsfor the individual enantiomers, but there is no guaran-tee that clinical response is related to AUC values.However, even here the correlation was still not pre-cise. Overall, detailed analysis of the kinetics oftransfer confirms that there are interpatient differ-ences in the patterns of concentrations of the ibu-profen enantiomers. Contrary to earlier findings [5],
Stereoselective disposition of ibuprofen 227
the skin blister model did not appear to simulatequantitatively the pharmacokinetics of ibuprofenenantiomers in synovial fluid, at least in individuals,although the blister does more closely simulate thetime course of concentrations of drug in synovialfluid than do plasma concentrations. An inflam-matory blister model might simulate synovial fluidkinetics even better.
The clinical relevance of blister concentrationsof NSAIDs is unclear. One would predict that theconcentrations of NSAIDs in a peripheral locationsuch as blister fluid might relate better to the clinicalefficacy of the drug than plasma concentrations.
Unbound concentrations may provide an even bettercorrelation with effect and the best measure of thesee.g. AUC, peak concentrations etc needs to bestudied. Clinical trials to examine the correlationbetween efficacy of NSAIDs and unbound concentra-tions in blister fluid would be of value.
The skillful assistance of Nurse Agneta Axelson (deceased)is gratefully acknowledged. The assistance of Mr T.Charlton with the GCMS analyses is also gratefullyacknowledged. The study was supported by grants from theKarolinska Institutet, Smedby stiftelse and Riksforbundetmot Reumatism, and the National Health and MedicalResearch Council of Australia.
References
1 Nowak A, Kadykow M, Klimowicz A. Penetration oftrimethoprim and sulfamethoxazole into blister fluid.Eur J clin Pharmac 1983; 25: 825-827.
2 Mouton JW, Horrevorts AA, Mulder PGH, Prens EP,Michel MF. Pharmacokinetics of cephtazidime inserum and suction blisters fluid during continuous andintermittent infusions in healthy volunteers. AntimicrobAgents Chemother 1990; 34: 2307-2311.
3 Schreiner A, Hellum KB, Digranes A, Bergman I.Transfer of penicillin G and ampicillin into human skinblisters induced by suction. Scand J infect Dis 1978;Suppl. 14: 233-237.
4 Shyu WC, Quintialani R, Nightingale CH. An improvedmethod to determine interstitial fluid pharmacokinetics.J infect Dis 1985; 152: 1328-1331.
5 Walker JS, Knihinicki RD, Seideman P, Day RO. Phar-macokinetics of ibuprofen enantiomers in plasma andsuction blister fluid in healthy volunteers. J pharm Sci1993; 82: 1-4.
6 Kaiser DG, Vangiessen Reischer Wechter WJ. Isomericconversion of ibuprofen (R)-enantiomer in humans. Jpharm Sci 1976; 65: 269-273.
7 Lee, EJD, Williams KM, Graham GG, Day RO, Cham-pion GD. Stereoselective disposition of ibuprofen enan-tiomers in man. Br J clin Pharmac 1985; 19: 669-674.
8 Adams SS, Bresloff P, Mason CG. Pharmacologicaldifferences between the optical isomers of ibuprofen:evidence for metabolic inversion of the (-)-isomer. Jpharm Sci 1976; 28: 256-257.
9 Kiistala U. Suction blister device for the separation ofviable epidermis from dermis. J invest Dermatol 1968;50: 129-137.
10 Day RO, Williams KM, Graham GG, Lee EJ, Cham-pion GD. Stereoselective disposition of ibuprofen enan-tiomers in synovial fluid. Clin Pharmac Ther 1988; 43:480-487.
11 Baillie TA, Adams WJ, Kaiser DG, Olanoff LS, Hal-stead GW, Harpootlian H, van Giessen GJ. Mechanisticstudies of the metabolic chiral inversion of (R)-ibupro-fen in humans. J Pharmac exp Ther 1989; 249:517-523.
12 Coburn WA. Simultaneous pharmacokinetic and phar-macodynamic modeling. J Pharmacokin Biopharm1981; 9: 367-388.
13 Noe DA, Kumor KM. Drug kinetics in low flux (small)anatomic compartments. J phar-m Sci 1983; 72:718-719.
14 Meyer-Carrive I, Graham GG, Ghosh P. Pharmaco-kinetics of tiaprofenic acid in normal rabbits andrabbits subjected to joint immobilisation. AgentsActions 1993; 39: 59-68.
15 Graham GG. Kinetics of non-steroidal anti-inflamma-tory drugs in synovial fluid. Agents Actions Suppl 1988;24: 66-75.
16 Williams KM. Enantiomers in arthritic disorders.Pharmac Ther 1990; 46: 273-295.
17 Lee EJD, Williams KM, Graham GG, Day RO, Cham-pion GD. Stereoselective disposition of ibuprofenenantiomers in man. Br J clin Pharmac 1985; 19:669-674.
18 Stock KP, Geisslinger G, Loew D, Beck WS, Bach GL,Brune K. S-ibuprofen versus ibuprofen-racemate.Rheumatol Int 1991; 11: 199-202.
19 Bradley JD, Rudy AC, Katz BP, Ryan SI, KalasinskiLA, Brater DC, Hall SD, Brandt KD. Correlation ofserum concentrations of ibuprofen stereoisomers withclinical response in the treatment of hip and kneeosteoarthritis. J Rheumatol 1992; 19: 130-134.
20 Kiistala U, Mustakallio KK. Dermo-epidermal separa-tion with suction. J invest Dermatol 1967; 48: 466-467.
21 Juhlin L, Tengblad A, Ortonne JP, Lacour J Ph.Hyaluronate in suction blisters from patients withscleroderma and various skin disorders. Acta Der-mVenereol (Stockh) 1986; 66: 409-413.
22 Fleishaker JC, McNamara PJ. Performance of a diffu-sional clearance model for ,B-lactam antimicrobialagents as influenced by extravascular protein bindingand interstitial fluid kinetics. Antimicr-ob AgentsChemother 1985; 28: 369-374.
23 Evans AM, Nation RL, Sansom LN. Stereoselectiveplasma protein binding of ibuprofen enantiomers. Eur Jclin Pharmac 1989; 36: 283-290.
(Received 2 September 1993,accepted 3 May 1994)
Copyright © 2022 FDOKUMEN









![Condensed bridgehead nitrogen heterocyclic system: Synthesis and pharmacological activities of 1,2,4-triazolo-[3,4- b]-1,3,4-thiadiazole derivatives of ibuprofen and biphenyl-4-yloxy](https://static.fdokumen.com/doc/165x107/632834412089eb31f609dd2b/condensed-bridgehead-nitrogen-heterocyclic-system-synthesis-and-pharmacological.jpg)










