
Increased Expression of Cytoskeletal, Linkage, and Extracellular Proteins in Failing Human...
11
Erwin Bauer, Wolf-Peter Klövekorn, Martin Schlepper, Wolfgang Schaper and Jutta Schaper Annette Heling, René Zimmermann, Sawa Kostin, Yoshi Maeno, Stefan Hein, Bruno Devaux, Human Myocardium Increased Expression of Cytoskeletal, Linkage, and Extracellular Proteins in Failing Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 2000 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation Research doi: 10.1161/01.RES.86.8.846 2000;86:846-853 Circ Res. http://circres.ahajournals.org/content/86/8/846 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circres.ahajournals.org/content/suppl/2000/07/19/86.8.846.DC1.html Data Supplement (unedited) at: http://circres.ahajournals.org//subscriptions/ is online at: Circulation Research Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer about this process is available in the located, click Request Permissions in the middle column of the Web page under Services. Further information Editorial Office. Once the online version of the published article for which permission is being requested is can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Circulation Research in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on July 7, 2014 http://circres.ahajournals.org/ Downloaded from by guest on July 7, 2014 http://circres.ahajournals.org/ Downloaded from by guest on July 7, 2014 http://circres.ahajournals.org/ Downloaded from by guest on July 7, 2014 http://circres.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Increased Expression of Cytoskeletal, Linkage, and Extracellular Proteins in Failing Human...

Erwin Bauer, Wolf-Peter Klövekorn, Martin Schlepper, Wolfgang Schaper and Jutta SchaperAnnette Heling, René Zimmermann, Sawa Kostin, Yoshi Maeno, Stefan Hein, Bruno Devaux,
Human MyocardiumIncreased Expression of Cytoskeletal, Linkage, and Extracellular Proteins in Failing
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 2000 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.86.8.8462000;86:846-853Circ Res.
http://circres.ahajournals.org/content/86/8/846World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org/content/suppl/2000/07/19/86.8.846.DC1.htmlData Supplement (unedited) at:
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Researchin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from

Increased Expression of Cytoskeletal, Linkage, andExtracellular Proteins in Failing Human Myocardium
Annette Heling, Rene Zimmermann, Sawa Kostin, Yoshi Maeno, Stefan Hein, Bruno Devaux,Erwin Bauer, Wolf-Peter Klovekorn, Martin Schlepper, Wolfgang Schaper, Jutta Schaper
Abstract—Experimental studies have shown that in hypertrophy and heart failure, accumulation of microtubules occurs thatimpedes sarcomere motion and contributes to decreased ventricular compliance. We tested the hypothesis that thesechanges are present in the failing human heart and that an entire complex of structural components, includingcytoskeletal, linkage, and extracellular proteins, are involved in causing functional deterioration. In explanted humanhearts failing because of dilated cardiomyopathy (ejection fraction#20%), expression ofa- and b-tubulin, desmin,vinculin, fibronectin, and vimentin was determined by Northern and Western blot analysis and compared with normalmyocardium from explants not used for transplantation. The mRNA fora- and b-tubulin was increased to 2.4-fold(P,0.01) and 1.25-fold (NS), respectively; for desmin, 1.2-fold (P,0.05); for fibronectin, 5-fold (P,0.001); and forvimentin, 1.7-fold (P,0.05). Protein levels fora-tubulin increased 2.6-fold (P,0.02); for b-tubulin, 1.2-fold(P,0.005); for desmin, 2.1-fold (P,0.001); for vinculin, 1.2-fold (P,0.005); for fibronectin, 2.9-fold (P,0.001); andfor vimentin, 1.5-fold (P,0.005). Confocal microscopy showed augmentation and disorganization of all proteinsstudied. In combination with the loss of myofilaments and sarcomeric skeleton previously reported, these changessuggest cardiomyocyte remodeling. Increased fibronectin and elevated interstitial cellularity (vimentin labeling) indicateprogressive fibrosis. The present results suggest a causative role of cytoskeletal abnormalities and myofilament loss forintrinsic contractile and diastolic dysfunction in failing hearts.(Circ Res. 2000;86:846-853.)
Key Words: heart failuren cardiomyopathyn cytoskeletonn fibrosisn structure
End-stage human chronic heart failure is the common finalmanifestation of a group of different diseases (such as
ischemic heart disease, hypertension, valve defects, dilatedcardiomyopathy, and others), and it is usually accompaniedby myocardial hypertrophy.1 Only a few animal models existto study this pathophysiologic situation, and these usually arenot able to mimic the slowly developing human situation.Therefore, most studies concerning the mechanism of re-duced function are carried out in tissue samples from humanhearts obtained at the time of cardiac transplantation, eitherfrom ischemic hearts or from those with dilated cardiomyop-athy (DCM). In this study, we present data obtained in failinghuman hearts with DCM. In the late stages of this disease,numerous degenerative structural alterations of the cardio-myocytes, as well as areas of focal fibrosis, are scatteredthroughout the ventricular walls.2–4
Decompensated hypertrophy occurs when increased cardiacmass fails to normalize wall stress,5 and it has been postulatedthat in the transition of compensated hypertrophy to a decom-pensated state, the cardiomyocyte cytoskeleton plays a key rolein causing contractile and diastolic dysfunction.6–8
Alterations of the cytoskeleton have been described in manyexcellent studies, by Tsutsui et al6,7 and Tagawa et al,8–11 in
hypertrophied and failing right ventricles of feline6,7,9–11 andcanine8 myocardium. It was shown that the increase in tubulinoccurs at the mRNA as well as at the protein level and that anincreased viscosity and stiffness of the cardiomyocytes is theconsequence of increased amounts and abnormal polymerizationof microtubules.11 Evidence was presented that increased micro-tubular density imposes an intracellular load on the cardiacmyocyte that will result in impediment of sarcomere motion andcontribute to decreased compliance of the hypertrophied myo-cardium. In another study, microtubule stabilization and theelevated expression of microtubule-associated protein-4 havebeen associated with contractile dysfunction.12 It was further-more shown that accumulation ofb-tubulin and contractiledysfunction may be related to the mechanical forces imposed onthe myocardium during the onset and progression of pressureoverload.13
The view that increased microtubular stabilization may be animportant factor in causing cellular stiffness and contractiledysfunction in pressure-overload hypertrophy is shared by Wanget al.14 On the other hand, Collins et al,15 investigating cytoskel-etal gene expression in a similar experimental model, found theopposite. The authors concluded that neither the level of
Received October 12, 1999; accepted February 25, 2000.From the Department of Experimental Cardiology (A.H., S.K., Y.M., M.S., W.S., J.S.), Max Planck Institute, and Department of Cardiac Surgery (R.Z., S.H.,
E.B., W.-P.K.), Kerckhoff-Clinic, Bad Nauheim, Germany, and Centre Hospitalier (B.D.), Universite de Rouen, France.Correspondence to Jutta Schaper, MD, Department of Experimental Cardiology, Max-Planck-Institute, Benekestrasse D-61231, Bad Nauheim, Germany.
E-mail [email protected]© 2000 American Heart Association, Inc.
Circulation Researchis available at http://www.circresaha.org
846 by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from

b-tubulin nor its polymerization state affected the contractileperformance of the overloaded left ventricle. The role of tubulinaccumulation and polymerization was also questioned by Baileyet al,16 who failed to find an effect of colchicine on contractiondynamics in isolated feline myocytes from hypertrophied hearts,and by de Tombe,17 who studied the effects of colchicine andtaxol on rat trabecula contractility.
In 1991, our group described accumulation and disorganiza-tion of microtubules and desmin filaments in human tissue withchronic heart failure.3 In continuation of this work, we tested thehypothesis and present here quantitative protein and mRNA datathat show that an entire system of structural proteins, includingthe cytoskeleton and proteins linking the intracellular milieu tothe extracellular matrix such as vinculin and fibronectin, areinvolved in causing the functional and structural deteriorationcharacteristic of heart failure.
Materials and MethodsNineteen patients with end-stage heart failure (ejection fraction#20%) due to DCM without any evidence of myocardial infarctionundergoing heart transplantation were studied. Hearts from donorswith normal left ventricular function not used for transplantationserved as controls. The study was approved by the institutionalethical committee. All clinical data are presented in Table 1.
Tissue SamplingAt the time of transplantation, tissue was removed from the leftventricular free wall excluding papillary muscles. Up to 3 sampleswere used for either Western or Northern blot and 5 to 8 samples forconfocal microscopy. Samples for Western blot were also examinedby microscopy. Samples were immediately frozen in liquid nitrogenand stored at –80°C until further use.
Western BlotAll antibodies used for Western blot and immunofluorescence arelisted in Table 2.
SDS-PAGE (separating gels 12%) and immunoblotting were carriedout following routine protocols. At least 2 different gels were preparedfrom each heart. For each lane, 30mg of protein was loaded. Tissuesamples from 3 donors served as control.
Quantification was done by densitometry either by using the gel-analyzing program Quantity One (Protein Imageware System) or byscanning the immunoblots on a STORM 860 imager (AmershamPharmacia Biotech) using ImageQuant software. All data were ex-pressed as mean6SEM. Statistical analysis by unpairedt test wasconsidered significant whenP,0.05.
StandardizationTo exclude the possibility that the tubulin measured originated froman increased number of fibroblasts in fibrotic tissue, myocardiumwas first evaluated by light microscopy, and samples showingabsence of fibrosis were selected. However, the contribution of an
Figure 1. Illustration of the localization of the proteins investi-gated. a, Isolated rat myocyte shows network-like longitudinallyoriented localization of b-tubulin. b, Schematic representation oflocalization of desmin around the Z-disks of the sarcomeres. c,Localization of vinculin (Vc) as a link between the intracellularmilieu and extracellular fibronectin via the integrins of the sarco-lemma. Tubulin is present also in fibroblasts. Vimentin present infibroblasts and endothelial cells is not shown here.
TABLE 1. Clinical Characteristics of the Patient Population
No. ofPatients Sex Age, Years LVEDP, mm Hg EF, % PAP Mean, mm Hg LVEDD, mm
DCM (n519) 17 male/2 female 50.868.3 29.169.1 1663.9 30.168.5 69.965.6
Control (n54) 4 male 48610 8–12 65–70 15–18 35–56
All patients with DCM were treated with digitalis, angiotensin-converting enzyme inhibitors, b-blockers, and diuretics at individualdosages. Depending on the individual situation of the patients, treatment with antiarrhythmic drugs was added.
EF indicates ejection fraction; PAP, pulmonary arterial pressure; and LVEDD, left ventricular end-diastolic diameter.
TABLE 2. Antibodies Used for Western Blotting (WB) andImmunofluorescence (IF)
Antigen Clone Host Dilution:WB/IF Company
Desmin DE-U-10 Mouse 1:100/20 Sigma
Vinculin hVIN-1 Mouse 1:100/40 Sigma
a-Tubulin DM 1A Mouse 1:100/100 Sigma
b-Tubulin 2-28-33 Mouse 1:100/100 Sigma
Fibronectin Polyclonal Rabbit 1:100/100 ICN
Vimentin Vg Mouse 1:100/10 Immunotech
Pan-actin HHF35 Mouse 1:100 DAKO
Heling et al Cytoskeleton in Heart Failure 847
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from
increased number of fibroblasts cannot be entirely excluded. Immu-noblotting for pan-actin was performed, and only samples showing asimilar density of the actin band at 42 kDa were used in this study.The total protein applied to the gel was kept constant.
Northern BlotThe following molecular probes were used for Northern blot analy-sis: humana- and b-tubulin and human vimentin (American TypeCulture Collection), human desmin (R. Zimmermann, unpublished),rat fibronectin clone pRCabFN1 (K. Boheler, National Heart andLung Institute, London, UK), and a murine 18S ribosomal RNAcDNA probe (a gift of I. Oberbaumer, Max-Planck-Institut, Mar-tinsried, Germany).
Standard methods for Northern blots were used.18 Each gel was doneat least in duplicate to control for variability within and between gels.For each well, 15mg of total RNA was loaded. Tissue samples from 3donors served as control.
Quantification of mRNA levels was performed using a Phosphor-Imager and ImageQuant software (Molecular Dynamics). For normal-ization, the data of each hybridization signal were divided by thematching 18S signal. All data are presented as mean6SEM. Expressionwas assessed by an unpairedt test. Statistical significance was acceptedasP,0.05.
Immunolabeling and Confocal MicroscopyFrom each left ventricle, 5 to 8 randomly chosen samples wereprepared as previously described.19 Omission of primary antibodiesserved as negative controls. Preparations were viewed in a confocallaser microscope (Leica) equipped with appropriate filter blocks. Theoptical confocal sections taken through the depth of tissue samples at0.5- to 1-mm intervals were viewed and photographed individually or
were superimposed for reconstruction in a 3-dimensional mode usinga Silicon Graphics Indy workstation and 3-dimensional multichannelimage processing software (Bitplane).
ResultsAll proteins studied, with the exception of vimentin, areschematically represented in Figure 1. Vimentin is present infibroblasts and in endothelial cells.
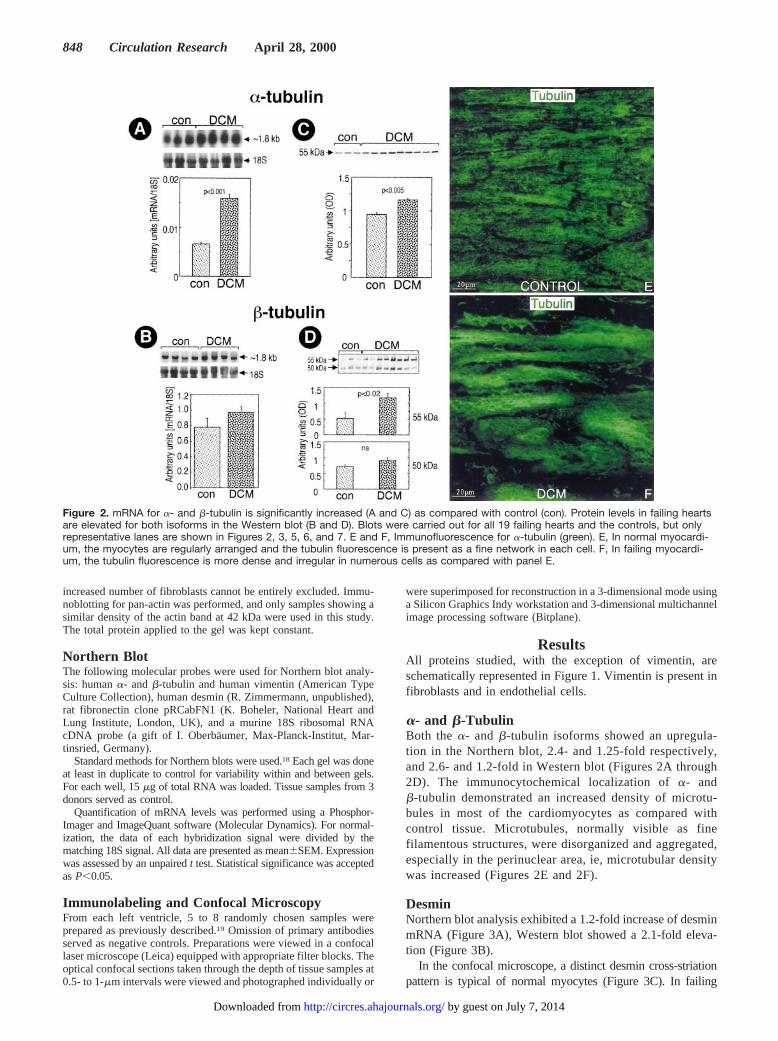
a- and b-TubulinBoth thea- and b-tubulin isoforms showed an upregula-tion in the Northern blot, 2.4- and 1.25-fold respectively,and 2.6- and 1.2-fold in Western blot (Figures 2A through2D). The immunocytochemical localization ofa- andb-tubulin demonstrated an increased density of microtu-bules in most of the cardiomyocytes as compared withcontrol tissue. Microtubules, normally visible as finefilamentous structures, were disorganized and aggregated,especially in the perinuclear area, ie, microtubular densitywas increased (Figures 2E and 2F).
DesminNorthern blot analysis exhibited a 1.2-fold increase of desminmRNA (Figure 3A), Western blot showed a 2.1-fold eleva-tion (Figure 3B).
In the confocal microscope, a distinct desmin cross-striationpattern is typical of normal myocytes (Figure 3C). In failing
Figure 2. mRNA for a- and b-tubulin is significantly increased (A and C) as compared with control (con). Protein levels in failing heartsare elevated for both isoforms in the Western blot (B and D). Blots were carried out for all 19 failing hearts and the controls, but onlyrepresentative lanes are shown in Figures 2, 3, 5, 6, and 7. E and F, Immunofluorescence for a-tubulin (green). E, In normal myocardi-um, the myocytes are regularly arranged and the tubulin fluorescence is present as a fine network in each cell. F, In failing myocardi-um, the tubulin fluorescence is more dense and irregular in numerous cells as compared with panel E.
848 Circulation Research April 28, 2000
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from

myocardium, desmin was disorganized and accumulated inmany cardiomyocytes (Figure 3D).
A good correlation was found between the amount of cy-toskeletal proteins (desmin and tubulin) and the left ventricularend-diastolic pressure (LVEDP) in controls and DCM patients(Figure 4).
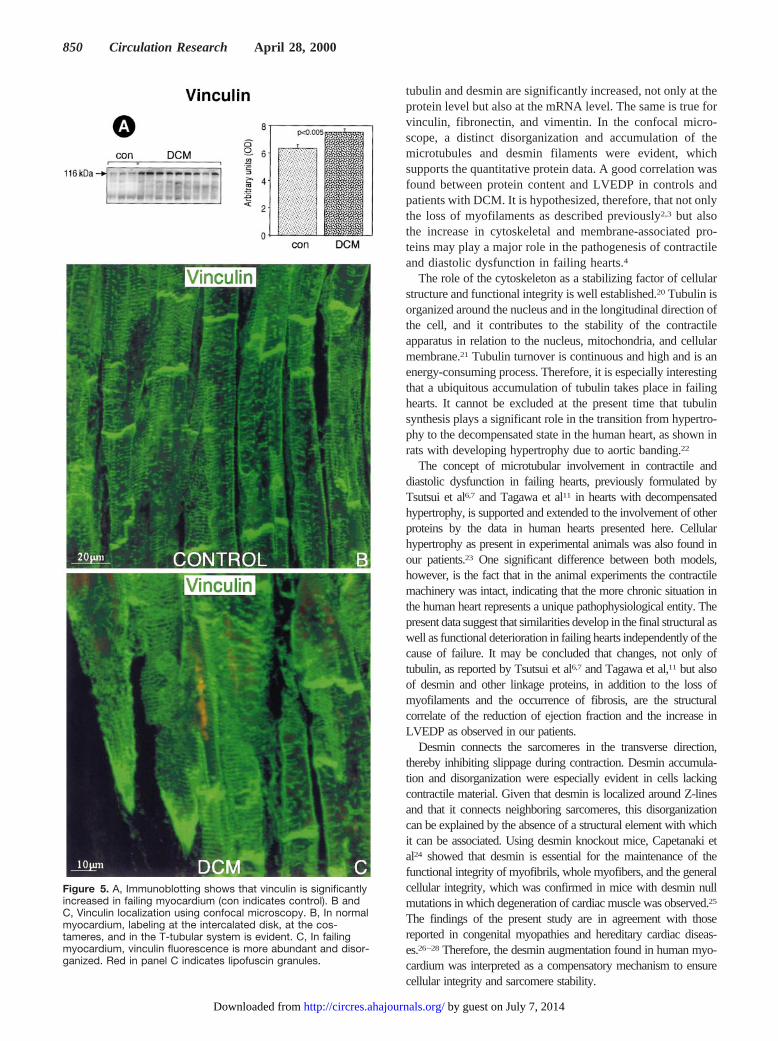
VinculinAs compared with normal myocardium, vinculin was 1.2-foldincreased in patients with failing hearts in Western blot(Figure 5A).
In the confocal microscope, vinculin showed a distinct local-ization at the intercalated disks and at the lateral sarcolemma innormal myocardium. This localization was more intense infailing hearts, corresponding to the results from Western blotting(Figure 5B).
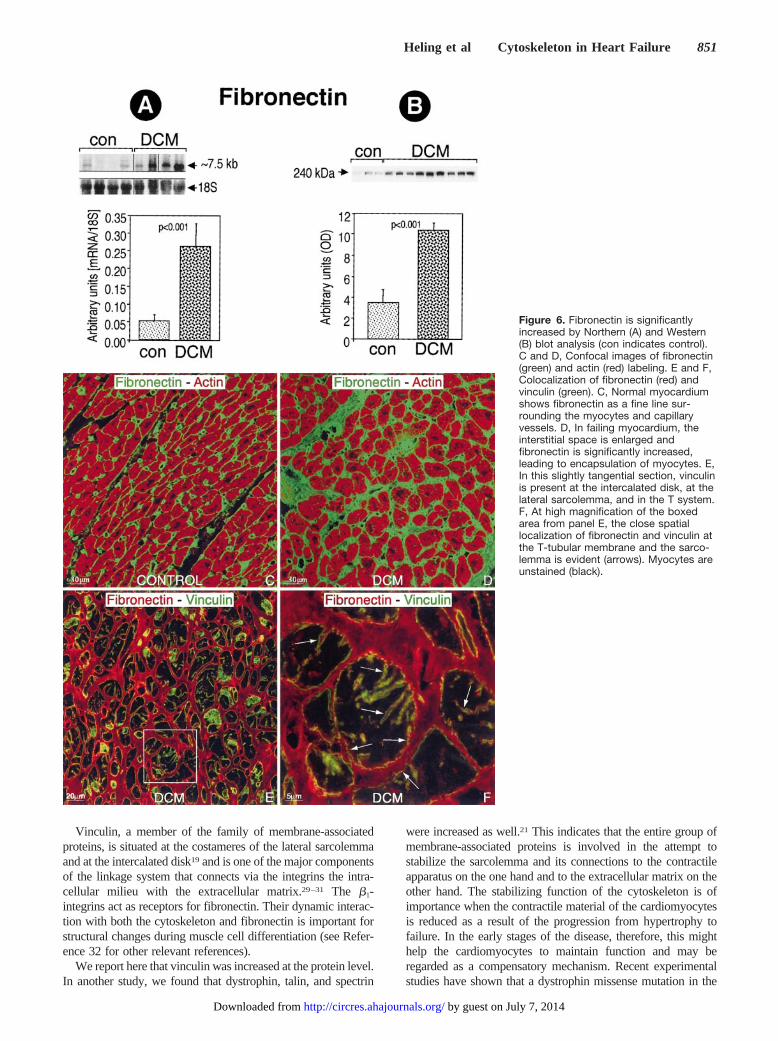
FibronectinThe mRNA for fibronectin was 5-fold increased as comparedwith controls (Figure 6A); the protein was increased 2.9-fold(Figure 6B).
In immunolabeling, it was evident that fibronectin was presentin the extracellular space and in the basement membrane ofmyocytes, smooth muscle cells, and endothelial cells (Figure6C). The expression was more intense in the widened interstitialspace of failing hearts (Figure 6D). A close colocalization offibronectin and vinculin was shown by double labeling (Figures6E and 6F)
VimentinThe mRNA for vimentin was upregulated 1.7-fold as com-pared with controls (Figure 7A), and the protein was in-creased 1.5-fold in patients with heart failure (Figure 7B).
Immunostaining of normal myocardium showed that vimen-tin was present in fibroblasts and endothelial cells (Figure 7C).In failing hearts, fibroblasts were more numerous, correspondingto the values from Western blot (Figure 7D).
DiscussionThis study demonstrates for the first time significant changesof cytoskeletal and membrane-associated proteins in humanhearts failing because of longstanding DCM. We show that
Figure 3. Desmin is significantly increased on the mRNA andprotein levels as shown by Northern (A) and Western (B) blotanalysis (con indicates control). C and D, Confocal microscopyfor desmin. C, Normal human myocardium shows a regularcross-striation at the Z-level and distinct intercalated disk label-ing. D, In failing myocardium, the cross-striation pattern is dis-turbed and desmin is accumulated in many irregularly shapedcells. Nuclei are red.
Figure 4. A good correlation exists between LVEDP andcytoskeletal protein content (tubulin and desmin).
Heling et al Cytoskeleton in Heart Failure 849
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from
tubulin and desmin are significantly increased, not only at theprotein level but also at the mRNA level. The same is true forvinculin, fibronectin, and vimentin. In the confocal micro-scope, a distinct disorganization and accumulation of themicrotubules and desmin filaments were evident, whichsupports the quantitative protein data. A good correlation wasfound between protein content and LVEDP in controls andpatients with DCM. It is hypothesized, therefore, that not onlythe loss of myofilaments as described previously2,3 but alsothe increase in cytoskeletal and membrane-associated pro-teins may play a major role in the pathogenesis of contractileand diastolic dysfunction in failing hearts.4
The role of the cytoskeleton as a stabilizing factor of cellularstructure and functional integrity is well established.20 Tubulin isorganized around the nucleus and in the longitudinal direction ofthe cell, and it contributes to the stability of the contractileapparatus in relation to the nucleus, mitochondria, and cellularmembrane.21 Tubulin turnover is continuous and high and is anenergy-consuming process. Therefore, it is especially interestingthat a ubiquitous accumulation of tubulin takes place in failinghearts. It cannot be excluded at the present time that tubulinsynthesis plays a significant role in the transition from hypertro-phy to the decompensated state in the human heart, as shown inrats with developing hypertrophy due to aortic banding.22
The concept of microtubular involvement in contractile anddiastolic dysfunction in failing hearts, previously formulated byTsutsui et al6,7 and Tagawa et al11 in hearts with decompensatedhypertrophy, is supported and extended to the involvement of otherproteins by the data in human hearts presented here. Cellularhypertrophy as present in experimental animals was also found inour patients.23 One significant difference between both models,however, is the fact that in the animal experiments the contractilemachinery was intact, indicating that the more chronic situation inthe human heart represents a unique pathophysiological entity. Thepresent data suggest that similarities develop in the final structural aswell as functional deterioration in failing hearts independently of thecause of failure. It may be concluded that changes, not only oftubulin, as reported by Tsutsui et al6,7 and Tagawa et al,11 but alsoof desmin and other linkage proteins, in addition to the loss ofmyofilaments and the occurrence of fibrosis, are the structuralcorrelate of the reduction of ejection fraction and the increase inLVEDP as observed in our patients.
Desmin connects the sarcomeres in the transverse direction,thereby inhibiting slippage during contraction. Desmin accumula-tion and disorganization were especially evident in cells lackingcontractile material. Given that desmin is localized around Z-linesand that it connects neighboring sarcomeres, this disorganizationcan be explained by the absence of a structural element with whichit can be associated. Using desmin knockout mice, Capetanaki etal24 showed that desmin is essential for the maintenance of thefunctional integrity of myofibrils, whole myofibers, and the generalcellular integrity, which was confirmed in mice with desmin nullmutations in which degeneration of cardiac muscle was observed.25
The findings of the present study are in agreement with thosereported in congenital myopathies and hereditary cardiac diseas-es.26–28Therefore, the desmin augmentation found in human myo-cardium was interpreted as a compensatory mechanism to ensurecellular integrity and sarcomere stability.
Figure 5. A, Immunoblotting shows that vinculin is significantlyincreased in failing myocardium (con indicates control). B andC, Vinculin localization using confocal microscopy. B, In normalmyocardium, labeling at the intercalated disk, at the cos-tameres, and in the T-tubular system is evident. C, In failingmyocardium, vinculin fluorescence is more abundant and disor-ganized. Red in panel C indicates lipofuscin granules.
850 Circulation Research April 28, 2000
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from
Vinculin, a member of the family of membrane-associatedproteins, is situated at the costameres of the lateral sarcolemmaand at the intercalated disk19 and is one of the major componentsof the linkage system that connects via the integrins the intra-cellular milieu with the extracellular matrix.29–31 The b1-integrins act as receptors for fibronectin. Their dynamic interac-tion with both the cytoskeleton and fibronectin is important forstructural changes during muscle cell differentiation (see Refer-ence 32 for other relevant references).
We report here that vinculin was increased at the protein level.In another study, we found that dystrophin, talin, and spectrin
were increased as well.21 This indicates that the entire group ofmembrane-associated proteins is involved in the attempt tostabilize the sarcolemma and its connections to the contractileapparatus on the one hand and to the extracellular matrix on theother hand. The stabilizing function of the cytoskeleton is ofimportance when the contractile material of the cardiomyocytesis reduced as a result of the progression from hypertrophy tofailure. In the early stages of the disease, therefore, this mighthelp the cardiomyocytes to maintain function and may beregarded as a compensatory mechanism. Recent experimentalstudies have shown that a dystrophin missense mutation in the
Figure 6. Fibronectin is significantlyincreased by Northern (A) and Western(B) blot analysis (con indicates control).C and D, Confocal images of fibronectin(green) and actin (red) labeling. E and F,Colocalization of fibronectin (red) andvinculin (green). C, Normal myocardiumshows fibronectin as a fine line sur-rounding the myocytes and capillaryvessels. D, In failing myocardium, theinterstitial space is enlarged andfibronectin is significantly increased,leading to encapsulation of myocytes. E,In this slightly tangential section, vinculinis present at the intercalated disk, at thelateral sarcolemma, and in the T system.F, At high magnification of the boxedarea from panel E, the close spatiallocalization of fibronectin and vinculin atthe T-tubular membrane and the sarco-lemma is evident (arrows). Myocytes areunstained (black).
Heling et al Cytoskeleton in Heart Failure 851
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from

mouse,33 muscle LIM protein (MLP) deficiency in mice,34 orcleavage of dystrophin by enteroviral proteases35 result in theclinical picture of DCM. On the basis of these data, thehypothesis was put forward that DCM is a disease of cytoskel-etal damage.36,37 This view, however, is in contradistinction tothe increased density of the major cytoskeletal components inhuman hearts with DCM as reported here.
Fibronectin is the major extracellular matrix protein and is animportant component of the cellular basement membrane.38 It isincreased in hearts with DCM, resulting, together with anincrease of other extracellular proteins, in a significant degree offibrosis.4,39 Vimentin, the intermediate filament of fibroblastsand endothelial cells, was studied because it represents anindicator of the cellularity of the interstitium.40 It was signifi-cantly elevated because the number of fibroblasts was higherthan in control. Taken together, these findings indicate that thesynthesis of connective tissue components is continuous and willresult in progressive fibrosis despite pretransplantation treatmentof all patients with angiotensin-converting enzyme inhibitors. Inan experimental study, we have recently shown that fibrosisdevelopment cannot be prevented indefinitely by this treat-ment,41 which would confirm the data presented here. Fibrosiswill contribute to an increased stiffness and loss of ventricularcompliance.42
The cytoskeleton also plays an important role in mechano-transduction across the cell surface, where integrins act asmechanoreceptors.43 Transfer of force from integrins to thecytoskeleton is thought to represent a proximal step in intracel-lular mechanical signaling that leads to global cytoskeletalrearrangements.43 Furthermore, it has been shown that theextracellular matrix controls cytoskeletal mechanics and struc-ture, particularly by binding of fibronectin to integrins.44,45
Interestingly, increasing extracellular matrix contacts by bindingthrough an elevated number of integrins increases cytoskeletalstiffness and apparent viscosity.44 Transferring these data to ourown findings, it may be assumed that the increased content offibronectin found in failing hearts is the inducer of changes ofcytoskeletal structure and function.
The question remains open whether the changes describedhere are effects rather than causes of heart failure. The presentdata, however, are more in support of the hypothesis that thesestructural changes are contributory to the transition to heartfailure. This hypothesis will be tested in human hearts withcompensatory hypertrophy. Another question is whether thecytoskeletal proteins either have a structural role only or partic-ipate in cellular signaling. As discussed recently, “chronicincreases in wall stress mediated by cytoskeletal pathways”(page 558) as is the case in failing hearts with DCM, may playa decisive role in cellular hypertrophy and cell survival.46 Recentevidence concerninga- or d-sarcoglycan47 or LIM domainprotein34 –deficient mice strongly suggests that the cytoskeletonmight be involved in cellular signaling.
In conclusion, in myocytes from failing human hearts, themajor components of the cytoskeleton tubulin and desmin, aswell as the membrane-associated protein vinculin, are increased,most probably as a mechanism compensatory for the loss ofcontractile filaments, thereby contributing to an increased stiff-ness of individual cardiomyocytes. Furthermore, the linkageprotein vinculin and the extracellular matrix protein fibronectin
Figure 7. Vimentin is significantly increased on the mRNA (A)and protein (B) levels (con indicates control). C and D, Confocalimages of immunofluorescence for vimentin (red), with myocytescounterstained with phalloidin (green). C, Normal myocardiumwith few fibroblasts and capillaries. D, In failing myocardium, themyocytes are separated by fibrotic material containing manyfibroblasts. Only few capillaries are visible. Red in myocytesindicates lipofuscin granules.
852 Circulation Research April 28, 2000
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from

are augmented, which will, by interaction with the integrins,further increase cellular stiffness. Fibronectin and vimentinindicate a progressive development of fibrosis. The present datasupport experimental reports showing the important role ofmicrotubule accumulation in failing hearts. They furthermoreshow that changes of a whole complex of proteins, in addition tothe loss of contractile filaments and proteins of the sarcomericskeleton described previously,3 represent the structural basis forthe reduction of contractile function and compliance in failinghuman hearts.21
AcknowledgmentWe thank Gunther Schuster for computer assistance.
References1. Braunwald E. Pathophysiology of heart failure. In: Braunwald E, ed.
Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia, Pa:WB Saunders Co Inc; 1980:453–483.
2. Hein S, Scholz D, Fujitani N, Rennollet H, Brand T, Friedl A, Schaper J.Altered expression of titin and contractile proteins in failing human myocar-dium. J Mol Cell Cardiol. 1994;26:1291–1306.
3. Schaper J, Froede R, Hein S, Buck A, Hashizume H, Speiser B, Friedl A,Bleese N. Impairment of the myocardial ultrastructure and changes of thecytoskeleton in dilated cardiomyopathy.Circulation. 1991;83:504–514.
4. Schaper J, Speiser B, Brand T. The cytoskeleton and extracellular matrix inhuman hearts with dilated cardiomyopathy. In: Figulla HR, Kandolf R,McManus B, eds.Idiopathic Dilated Cardiomyopathy. Berlin, Germany:Springer-Verlag; 1993:75–80.
5. Grossman W, Jones D, McLaurin MP. Wall stress and patterns of hypertro-phy in the human left ventricle.J Clin Invest. 1975;56:56–64.
6. Tsutsui H, Ishihara K, Cooper G. Cytoskeletal role for contractile dysfunctionof hypertrophied myocardium.Science. 1993;260:682–687.
7. Tsutsui H, Tagawa H, Kent RL, McCollam PL, Ishihara K, Nagatsu M,Cooper G. Role of microtubules in contractile dysfunction of hypertrophiedcardiocytes.Circulation. 1994;90:533–555.
8. Tagawa H, Koide M, Sato H, Zile MR, Carabello BA, Cooper G.Cytoskeletal role in the transition from compensated to decompensated hy-pertrophy during adult canine left ventricular pressure overloading.Circ Res.1998;82:751–761.
9. Tagawa H, Koide M, Sato I, Cooper G. Cytoskeletal role in the contractiledysfunction of cardiocytes from hypertrophied and failing right ventricularmyocardium.Proc Assoc Am Physicians. 1996;108:218–229.
10. Tagawa H, Rozich JD, Tsutsui H, Narishige T, Kuppuswamy D, Sato H,McDermott PJ, Koide M, Cooper G. Basis for increased microtubules inpressure-hypertrophied cardiocytes.Circulation. 1996;93:1230–1243.
11. Tagawa H, Wang N, Narishige T, Ingber DE, Zile MR, Cooper G.Cytoskeletal mechanics in pressure-overload cardiac hypertrophy.Circ Res.1997;80:281–289.
12. Sato II, Nagai T, Kuppuswamy D, Narishige T, Koide M, Menick DR,Cooper G. Microtubule stabilization in pressure overload cardiac hypertro-phy. J Cell Biol. 1997;139:963–973.
13. Watson PA, Hannan R, Carl LL, Giger KE. Contractile activity and passivestrength regulate tubulin mRNA and protein content in cardiac myocytes.Am J Physiol. 1996;271(2 pt 1):C684–C689.
14. Wang X, Li F, Campbell SE, Gerdes M. Chronic pressure overload hyper-trophy and failure in guinea pigs, II: cytoskeletal remodeling.J Mol CellCardiol. 1999;31:319–331.
15. Collins JF, Pawloski-Dahm C, Davies MG, Ball N, Dorn GW, Walsh RA.The role of the cytoskeleton in left ventricular pressure overload hypertrophyand failure.J Mol Cell Cardiol. 1996;28:1435–1443.
16. Bailey BA, Dipla K, Li S, Houser SR. Cellular basis of contractilederangements of hypertrophied ventricular myocytes.J Mol Cell Cardiol.1997;29:1823–1835.
17. de Tombe PP. Altered contractile function in heart failure.Cardiovasc Res.1998;37:367–380.
18. Chomczynski P, Sacchi N. Single step method of RNA isolation by acidguanidinium thiocyanate-phenol-chloroform extraction.Anal Biochem. 1987;162:156–159.
19. Kostin S, Scholz D, Shimada T, Maeno Y, Mollnau H, Hein S, Schaper J.The internal and external protein scaffold of the T-tubular system in cardio-myocytes.Cell Tissue Res. 1998;294:449–460.
20. Stromer MH. The cytoskeleton in skeletal, cardiac and smooth muscle cells.Histol Histopathol. 1998;13:283–291.
21. Kostin S, Heling A, Hein S, Scholz D, Klovekorn W-P, Schaper J. Theprotein composition of the normal and diseased cardiac myocyte.Heart FailRev. 1998;2:245–260.
22. Watkins SC, Samuel JL, Marotte F, Bertier-Savalle B, Rappaport L. Micro-tubules and desmin filaments during onset of heart hypertrophy in the rat: adouble immunoelectron microscope study.Circ Res. 1987;60:327–336.
23. Scholz D, Diener W, Schaper J. Altered nucleus/cytoplasm relationship anddegenerative structural changes in human dilated cardiomyopathy.Cardio-science. 1994;5:127–138.
24. Capetanaki A, Milner DJ, Weitzer G. Desmin in muscle formation andmaintenance: knockouts and consequences.Cell Struct Funct. 1997;22:103–116.
25. Milner DJ, Weitzer G, Tran D, Bradley A, Capetanaki Y. Disruption ofmuscle architecture and myocardial degeneration in mice lacking desmin.J Cell Biol. 1996;134:1255–1270.
26. Thornell LE, Johanson B, Erikson A, Lehto VP, Virtanen I. Intermediatefilament and associated proteins in the human heart: an immunofluorescencestudy of normal and pathological hearts.Eur Heart J. 1984;5(supplF):231–241.
27. Thornell LE, Price MG. The cytoskeleton in muscle cells in relation tofunction.Biochem Soc Transact. 1991;19:1116–1120.
28. Thornell LE, Carlsson L, Li Z, Mericskay M, Paulin D. Null mutation in thedesmin gene gives rise to a cardiomyopathy.J Mol Cell Cardiol. 1997;29:2107–2124.
29. Geiger B. Vinculin, an intracellular protein localized at specialized siteswhere microfilaments bundles terminate at cell membranes.Proc Natl AcadSci U S A. 1980;77:4127–4131.
30. Craig SW, Pardo JV. Gamma actin, spectrin, and intermediate filamentproteins colocalize with vinculin at costameres, myofibril-to-sarcolemmaattachment sites.Cell Motil. 1983;3:449–462.
31. Pardo JV, Siliciano J, Craig SW. Vinculin is a component of an extensivenetwork of myofibril-sarcolemma attachment regions in cardiac musclefibers.J Cell Biol. 1983;97:1081–1088.
32. Enomoto MI, Boettiger D, Menko AS.a5-Integrin is a critical component ofadhesion plaques in myogenesis.Dev Biol. 1993;155:180–197.
33. Ortiz-Lopez R, Hua L, Su J, Goytia V, Towbin JA. Evidence for a dystrophinmissense mutation as a cause of X-linked dilated cardiomyopathy.Circu-lation. 1997;95:2434–2440.
34. Arber S, Hunter JJ, Ross J Jr, Hongo M, Sansig G, Borg J, Perriard J-C, ChienKR, Caroni P. MLP-deficient mice exhibit a disruption of cardiac cytoarchi-tectural organization, dilated cardiomyopathy, and heart failure.Cell. 1987;88:393–403.
35. Badorff C, Lee GH, Lamphear BL, Martone ME, Campbell KP, Rhoads RE,Knowlton KU. Enteroviral protease 2A cleaves dystrophin: evidence ofcytoskeletal disruption in an acquired cardiomyopathy.Nat Med. 1999;5:320–326.
36. Towbin JA. The role of cytoskeletal proteins in cardiomyopathies.Curr OpinCell Biol. 1998;10:131–139.
37. Towbin JA, Bowles KR, Bowles NE. Etiologies of cardiomyopathy and heartfailure. Nat Med. 1999;5:266–267.
38. Hynes RO.Fibronectins. Berlin, Germany: Springer; 1989.39. Schaper J, Hein S, Scholz D, Mollnau H. Multifaceted morphological alter-
ations are present in the failing human heart.J Mol Cell Cardiol. 1995;27:857–861.
40. Traub P.Intermediate Filaments: A Review. Berlin, Germany: Springer-Verlag; 1985.
41. Zimmermann R, Kastens J, Linz W, Wiemer G, Scholkens BA, Schaper J.Effect of long-term ACE inhibition on myocardial tissue in hypertensivestroke-prone rats.J Mol Cell Cardiol. 1999;31:1447–1456.
42. Weber KT, Brilla CG, Janicki JS. Myocardial fibrosis: functional significanceand regulatory factors.Cardiovasc Res. 1993;27:341–348.
43. Wang N, Butler JP, Ingber DE. Mechanotransduction across the cell surfaceand through the cytoskeleton.Science. 1993;260:1124–1127.
44. Wang N, Ingber DE. Control of cytoskeletal mechanics by extracellularmatrix, cell shape, and mechanical tension.Biophys J. 1994;66:2181–2189.
45. Choquet D, Felsenfeld DP, Sheetz MP. Extracellular-matrix rigidity causesstrengthening of integrin-cytoskeleton linkages.Cell. 1997;88:39–48.
46. Chien KR. Stress pathways and heart failure.Cell. 1999;98:555–558.47. Coral-Vazquez R, Cohn RD, Moore SA, Hill JA, Weiss RM, Davisson RL,
Straub V, Barresi R, Bansal D, Hrstka RF, Williamson R, Campbell K.Disruption of the sarcoglycan-sarcospan complex in vascular smooth muscle:a novel mechanism for cardiomyopathy and muscular dystrophy.Cell. 1999;98:465–474.
Heling et al Cytoskeleton in Heart Failure 853
by guest on July 7, 2014http://circres.ahajournals.org/Downloaded from










![Conservation in tropical Pacific Island countries: why most current approaches are failing [2012]](https://static.fdokumen.com/doc/165x107/63368ffc4e9c1ac02e082302/conservation-in-tropical-pacific-island-countries-why-most-current-approaches-are.jpg)











