
Food Surface Texture Measurement Using Reflective Confocal Laser Scanning Microscopy

In vivo oral biofilm analysis by confocal laser scanning microscopy:
methodological approaches
Tomás I1, Henderson B
2, Diz P
1, Donos N
3
1-Special Needs Unit. School of Medicine and Dentistry. Santiago de Compostela University. Spain. 2-Department of Microbial Diseases. UCL Eastman Dental Institute. London. United Kingdom. 3-Periodontology Unit. UCL Eastman Dental Institute. London. United Kingdom.
The scientific community is showing an increasing interest in exploring the in vivo formation of the undisturbed human oral biofilm, because understanding the processes involved may open new avenues for interfering with the pathogenic properties of biofilms. The present chapter is focused on in vivo human models of undisturbed oral biofilm analysed by confocal laser scanning microscopy (CLSM). The different types of oral appliances and substrates used, the several microbiological and microscopic methods applied in combination with CLSM, as well as CLSM technical aspects are discussed. Finally, a new microscopic technique is described, the so called, confocal endomicroscopy, which will offer numerous exciting opportunities for the in vivo microscopic investigation in the field of Dentistry.
Keywords: dental plaque; dental biofilm; in vivo models; Confocal Laser Scanning Microscopy; Confocal Endomicroscopy.
1. Introduction
In nature, the immense majority of micro-organisms are adherent to the surfaces on which they grow, forming biofilms [1]. Of the various definitions of the concept of biofilm to be found in the literature, we would like to draw particular attention to the one proposed by Donlan and Costerton in 2002 [2]: a biofilm is “a microbially-derived sessile community characterized by cells that are irreversible attached to a substratum or interface or to each other, are embedded in a matrix of extracellular polymeric substances that they have produced, and exhibit an altered phenotype with respect to growth rate and gene transcription”. The oral biofilm and, specifically, dental plaque, is considered to be an example of a specialized microbial biofilm [3,4]. More than 6000 species-level phylotypes have been identified in dental plaque -determined by pyrosequencing analysis- [5]. The adherent biofilm that forms on the hard and soft tissues of the mouth constitutes the principal aetiological agent in the origin of caries, gingivitis and periodontal disease [6-8]; these can therefore be considered as biofilm-mediated diseases. Confocal laser scanning microscopy (CLSM) has been used in the biological sciences since 1961, when the concept of “optical sectioning” of a biological specimen was introduced. CLSM is a variation of white light microscopy in which specimens are visualized by stimulating light emission by a low power laser beam after application of fluorescent contrast agents. CLSM provides the capacity for direct, non-invasive, serial optical sectioning of intact, thick, live specimens with a minimum of sample preparation; in addition, it shows a marginal improvement in lateral resolution [9]. To date, more than 150 papers on oral biofilm analysis by CLSM have been published. There is now a specific interest in exploring the early stages of the in vivo formation of the oral biofilm on undisturbed samples as an understanding of the processes involved may open new avenues for acting on the pathogenic properties of biofilms [10-13]. This chapter provides a detailed description of the methodological characteristics of CLSM analysis of in vivo models of undisturbed human oral biofilm.
2. Limitations of the in vitro and destructured in vivo human oral biofilm models
The in vitro development of biofilm models led to significant advances in the study of oral biofilms [14-18]. However, in vitro oral biofilm models tend to involve limited numbers of species and, in addition, they are created under conditions that still cannot adequately reflect the physiological situation in the mouth [19-22]. Factors related to the oral cavity, such as the turnover rate of saliva, the ability of antibacterial substances to adhere to the pellicle of the tooth or the surface of soft tissues in order to achieve their effects, and the interaction with unculturable bacteria, cannot be modelled in in vitro experiments [12]. At the present time, the scientific community recognizes that in vitro models cannot guarantee the creation of oral biofilms whose composition and structure is comparable with those that form in vivo [20-22]. For this reason, some authors consider that the results obtained in in vitro studies should be interpreted with caution [12, 20, 23], and that there is a need to develop in vivo biofilm models that can subsequently be analysed intact ex vivo [20, 23-25].
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 597
______________________________________________

Many authors have used microbiological plate culture techniques to study the composition of the in vivo dental plaque (DP) biofilm and the antimicrobial activity of different agents, such as chlorhexidine (CHX) [26-29]. However, the numerous disadvantages associated with the use of culture-dependent methods are well known [12, 30]. Fluorescence methods have also been used to analyse the oral composition and antibacterial effect of some antiseptics on the in vivo DP-biofilm [31-34]. A common methodological characteristic of all these papers is that evaluation of the supragingival bacterial plaque was performed on material previously removed from the surface of the tooth [31-34], whereas the subgingival bacterial plaque was obtained by paper point sampling or by mechanical debridement [28, 35], which is likely to disturb the delicate three-dimensional architecture and organization of the DP-biofilm [10, 13, 19, 36]. Another disadvantage of this type of studies is that the level of penetration of an antimicrobial agent into the plaque samples cannot be evaluated as the samples are dispersed for analysis [33]. This methodology therefore does not provide an optimal analysis of the architecture and organization of in vivo DP-biofilms, as well as of the action of antimicrobial agents on its structure [11, 21].
3. Undisturbed in vivo oral biofilm analysis by confocal laser scanning microscopy
In the early 1990s, Watson et al [37, 38] suggested the possible application of CLSM in in vivo clinical dental research, and Netuschil et al, in 1998, [39] were the first investigators to use this non-invasive method to analyse the thickness and bacterial viability of undisturbed human DP-biofilm. Later, some authors designed special removable oral appliances that held a number of discs on which growth of the DP-biofilm took place [11, 22, 40]. This undisturbed DP-biofilm was then analysed using CLSM [11, 22, 40]. At present, the scientific community considers that this methodological design is the most suitable approach for studying the in vivo architecture and physiology of DP-biofilm formation on dental materials, as well as the antibacterial effect of antimicrobials on this microbial structure.
3.1. Removable appliances and substrates to collect dental plaque biofilm
It has been demonstrated that oral biofilms on mucosal surfaces are different from those on hard tissues, and that the composition of supragingival dental plaque differs from that of subgingival plaque [25]. As a result, these factors need to be taken into consideration when designing models of in vivo DP-biofilm. Probably due to the marked inter-individual variability detected in the characteristics of DP-biofilm [10, 11, 20, 41, 42], in the majority of the studies the number of volunteers who had worn the removable appliances ranged from 3 to 10 [11, 42-46]. With regard to the type of removable appliance used to collect the supragingival dental plaque, Wood et al [10, 47], Watson et al [21], and Robinson et al [48] used the “Leeds in situ device”, composed of a nylon ring holding an enamel substrate, as previously described by Robinson et al [49], on which the DP-biofilm grew. These devices were bonded to free buccal surfaces of the first or second upper molars by means of a composite resin, providing a stagnation site for the formation of DP-biofilm [49]. The research group led by Kolenbrander [42, 50-52] designed two bilateral mandibular stents (spanning the posterior buccal surfaces from the first premolar to first molar), each of which contained several discs. A number of other authors have used different types of individualised acrylic splints for growing DP-biofilm [11, 12, 20, 22, 40, 53]. Recently the authors of the present chapter designed individualised splints of the lower arch for each volunteer in the study being performed. Figure 1 shows this splint formed of two vinyl sheets, an internal sheet with a thickness of 1 mm to which 6 discs were attached, and an external sheet with a thickness of 0.5 mm that was fenestrated to permit contact of the vestibular surface of the discs with the saliva whilst protecting them from the action of the cheeks and tongue; similar to previous designs [11, 20, 22], several discs were positioned on each hemiarch and inserted towards the interdental area between two adjacent teeth in order to imitate an approximal DP-biofilm which is only minimally influenced by the shear forces of the oral soft tissues. This particular design ensured that the biofilm was not touched or disturbed during removal or repositioning of the appliance.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
598 ©FORMATEX 2010
______________________________________________

Figure 1. A) Individualised splint of the lower arch: 1. internal vinyl sheet; 2. polished glass discs; 3. fenestrated external vinyl sheet. B) Clinical view of the individualised splint with the glass discs inserted (arrows).
A number of solid substrates of different characteristics have been used in the published studies on DP-biofilm, including human enamel [10, 39, 40, 50, 51], bovine enamel [12, 46, 53], bovine dentine [41, 46], hydroxyapatite [54], and polished glass [11, 13, 20, 22, 39]. Zaura-Arite et al [41] used bovine dentine discs, where three parallel grooves were cut perpendicular to the surface (each 200 µm wide and approximately 500 µm deep) in order to imitate fissured dental plaque. Other authors have described DP-biofilm formation on dental restorative materials, using various substrates: amalgam, gold, ceramic, resin composite, compomer, glass-ionomer cement, and polymethyl methacrylate [43, 55, 56].
With the aim of collecting subgingival dental plaque as predominantly undisturbed biofilm, Wecke et al [19] designed carriers consisting of gold foil or polytetrafluoroethylene membranes that were inserted into the periodontal pockets of patients suffering rapidly progressive periodontitis whereas, Schaudinn et al [57] studied in vivo bacterial biofilm in the endodontic root canals of teeth extracted after failed endodontic treatment. In the majority of the studies on DP-biofilm, the time the appliance remained in the oral cavity varied between 4 hours [42, 51, 52, 55] and 7 days [12, 21, 48], depending on the type of DP-biofilm to be analysed. Auchill et al [20] demonstrated that the mean thickness of 48-hour biofilm -with a range from 14 to 150 µm- was not affected by the position of the removable device within the oral cavity (maxillary buccal region vs mandibular buccal region) or by the position of the disc (distal vs mesial; right vs left). In addition, Arweiler et al [11] observed that disc location in the oral cavity affected neither the mean bacterial viability values -with a range from 64% to 77%- nor the bacterial viability pattern in the 48-hour biofilm. Although the roughness of the surface of the substrate and its free energy are considered to be important factors for in vivo growth of the DP-biofilm [20], Netuschil et al [39] found no major differences in the thickness of 48-hour biofilm on using enamel or glass discs; some authors recommend using glass to avoid any optical disturbance due to the known autofluorescence of enamel [39, 44]. Jung et al [46] detected a significantly higher number of bacteria adherent to bovine dentine discs than to bovine enamel discs, and that the number of bacteria on the dentine increased with increasing oral exposure time (at 2 hours and 6 hours), whereas it remained relatively constant on the enamel. Interestingly, Wood et al [10] observed that the DP-biofilm generated over a 4-day period varied within each disc: the biofilm was thicker at the enamel disc/ring junction (depth of 75 to 220 µm) and thinner towards the centre (depth of 35 to 215 µm).
3.2. Microbiological techniques in combination with confocal laser scanning microscopy
It has been shown that the use of a combination of different microbiological techniques is the only means to achieve a realistic representation of the bacterial spatial distribution and dynamics of DP-biofilm and to be able to examine the role of distinct species as coadhesive microbial agents in dental plaque [12, 46].
•Fluorescence-labelled antibodies
In some studies of the undisturbed in vivo DP-biofilm of healthy subjects, fluorescence-labelled polyclonal antibodies have been used in combination with CLSM to look at the initial stages of biofilm development (at 4, 6, and 8 hours), and at the specific interactions between early colonizers of the tooth surface (such as Streptococcus spp., Actinomyces spp., and Veillonella spp.) [50-52]. Gu et al [54] explored the possibility of using 3 well-characterized monoclonal antibodies against Streptococcus mutans, Actinomyces naeslundii, and Lactobacillus casei, to identify these important members of the oral microbial community in the DP-biofilm, while Chalmers et al [50] used antibodies
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 599
______________________________________________
against Streptococcus mutans. It has been observed that this methodological approach does not disturb the biofilm structure and allows simultaneous assessment of the relative proportions and the spatial arrangement of several pathogenic genera (or species) within DP-biofilm grown in vivo, together with real-time monitoring of the dynamic changes involved in biofilm formation [54]. However, it has been recognized that the characteristics of the in vivo DP-biofilm can potentially influence the specificity of the antibodies, as well as the conjugation of the respective fluorescent labels to the antibodies could block the antigen recognition sites of the antibodies [54]. In consequence, Gu et al [54] stated that each newly raised fluorescently labelled antibody should be analyzed regarding their detection abilities and behaviour under various biofilm conditions.
•Fluorescence in situ hybridization
It has recently been shown that fluorescence in situ hybridization (FISH), a technique that employs fluorescence-labelled species-specific DNA probes, is an useful method for the detection of bacteria without disruption of their natural environment [12, 13, 42, 44, 45, 57]. Several authors have used the combination of FISH with CLSM to obtain images of three-dimensional reconstructions of the natural microbiological environments of in vivo DP-biofilm, evaluating the levels of up to 4 different micro-organisms in the biofilm formation after different periods of time [12, 13, 19, 42, 44-46]. The most important oral micro-organisms studied using the FISH/CLSM techniques have been the genera Streptococcus (the most widely studied), Actinomyces, Veillonella, Prevotella, and Treponema, as well as species such as Actinomyces naeslundii and Fusobacterium nucleatum [12, 13, 19, 42, 44-46]. Al-Almad et al [12] considered that the advantages of using FISH to identify micro-organisms in DP-biofilm include the possibility of detecting unculturable bacteria and the faster development of new probes compared to the production and characterization of antibodies. Besides, a good correlation between FISH and the results after staining with 4’ 6-diamino-2-phenylindole dihydrochloride (DAPI) has been detected [58]. On the other hand, one of the limitations of FISH is that it uses ribosomal (r) RNA-targeted probes, and its sensitivity is therefore limited by the metabolic state of the bacteria within the DP-biofilm, as metabolically inactive micro-organisms are generally considered to have a lower cellular ribosomal content (relative “inaccessibility” to FISH probes) [59]. Dongari-Bagtzoglou [59] stated that to detect metabolically active cells more specifically, it is possible to synthesise FISH oligonucleotide probes that bind to intergenic spacer regions in rRNA genes, which are quickly degraded during ribosome maturation in bacteria. These probes would therefore only detect bacteria that are producing new rRNA at the time of sampling [60]. Also, FISH requires specimen fixation including dehydration, potentially leading to similar problems to those observed with transmission electron microscopy (TEM) and scanning electron microscopy (SEM), and it cannot be utilized to study the dynamic changes occurring in live biofilms [54, 59].
•Molecular biology techniques
When studying clinical isolates of Veillonella spp. obtained from undisturbed in vivo DP-biofilm, Palmer et al [52] not only used fluorescence-labelled antibodies/CLSM but also simultaneously applied molecular techniques including phylogenetic characterization of clinical isolates by 16S rRNA gene sequencing. Those authors then analyzed the relationship between the isolates at strain level using enterobacterial repetitive intergenic consensus (ERIC) PCR fingerprinting, a technique that provides an assessment of diversity within a species (microdiversity) [52].
•Conventional culture-dependent techniques
In some studies on in vivo DP-biofilm by CLSM, the number of colony forming units obtained from the biofilm samples was quantified using conventional microbiological techniques [46, 52, 61]. In the series by Jung et al [46] and von Ohle et al [61], the cultural viability was examined by plating the serially diluted biofilm samples on different types of non-selective media for aerobic and anaerobic bacteria. On the contrary, in the series by Palmer et al [52] a selective-medium such as Veillonella enrichment agar plates was used.
•Other techniques
Von Ohle et al [61] demonstrated the utility of microelectrodes to provide a non-destructive, real-time measurement of the effects of sucrose and CHX on the physiology of DP-biofilm. The microelectrode data were correlated with microscopic examination by CLSM of the biofilm structure, thus allowing a relationship to be made between biofilm physiology and structure [61].
3.3. Fluorescence techniques in combination with confocal laser scanning microscopy
Since Netuschil first used fluorescence techniques to investigate the DP-biofilm in 1983 [62], many authors have employed a variety of fluorochromes, including acridine orange [63], fluorescein [10], DAPI [46], fluorescein diacetate plus ethidium bromide [22, 39, 40, 41, 53], and SYTO 9 plus propidium iodide (PI) [33]. Both fluorescein plus ethidium
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
600 ©FORMATEX 2010
______________________________________________
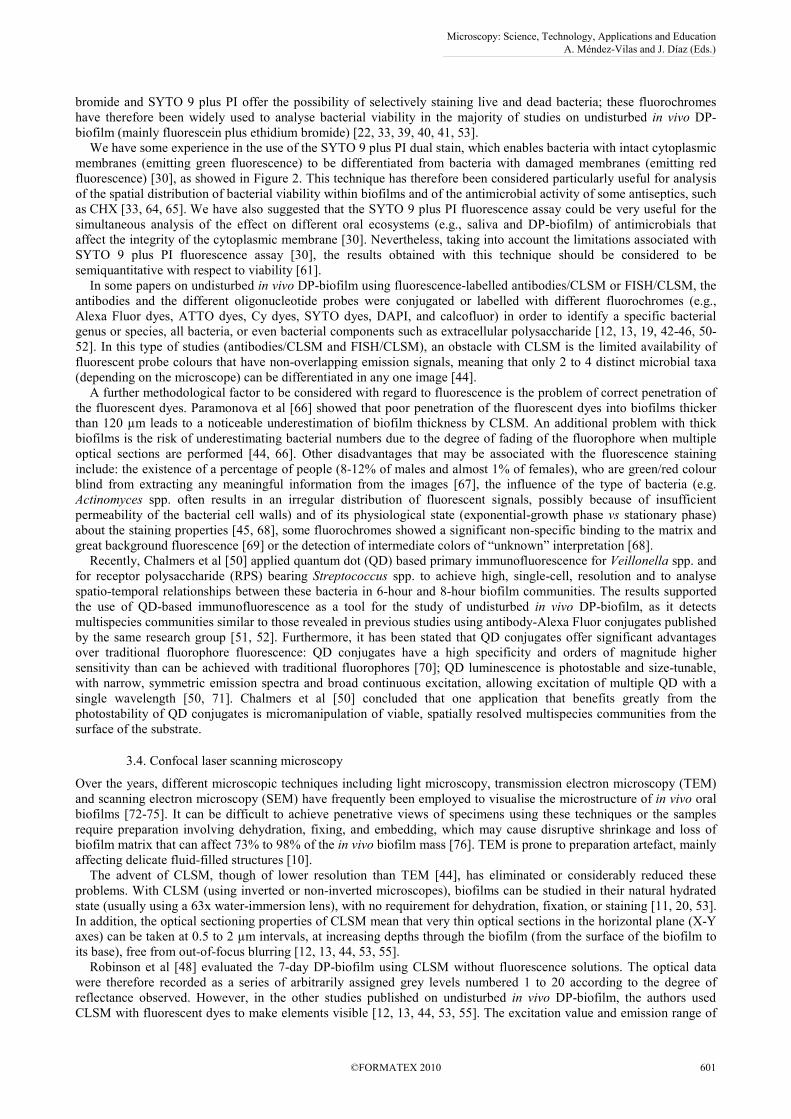
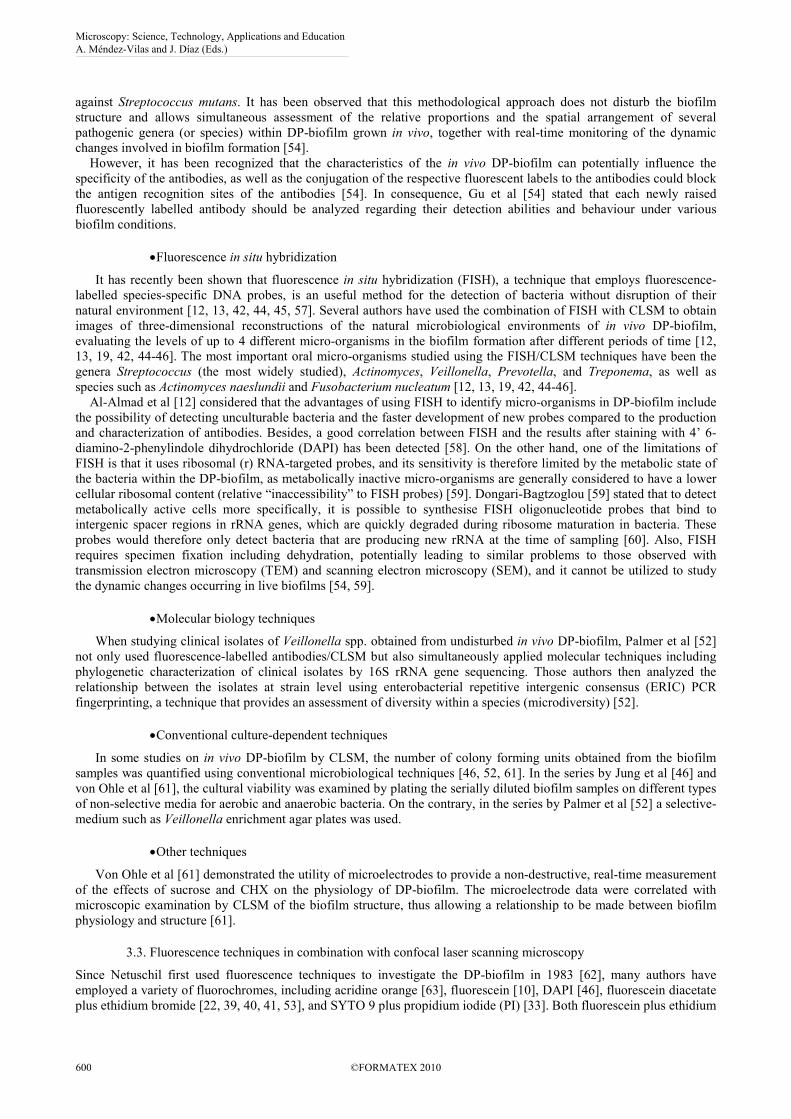
bromide and SYTO 9 plus PI offer the possibility of selectively staining live and dead bacteria; these fluorochromes have therefore been widely used to analyse bacterial viability in the majority of studies on undisturbed in vivo DP-biofilm (mainly fluorescein plus ethidium bromide) [22, 33, 39, 40, 41, 53]. We have some experience in the use of the SYTO 9 plus PI dual stain, which enables bacteria with intact cytoplasmic membranes (emitting green fluorescence) to be differentiated from bacteria with damaged membranes (emitting red fluorescence) [30], as showed in Figure 2. This technique has therefore been considered particularly useful for analysis of the spatial distribution of bacterial viability within biofilms and of the antimicrobial activity of some antiseptics, such as CHX [33, 64, 65]. We have also suggested that the SYTO 9 plus PI fluorescence assay could be very useful for the simultaneous analysis of the effect on different oral ecosystems (e.g., saliva and DP-biofilm) of antimicrobials that affect the integrity of the cytoplasmic membrane [30]. Nevertheless, taking into account the limitations associated with SYTO 9 plus PI fluorescence assay [30], the results obtained with this technique should be considered to be semiquantitative with respect to viability [61]. In some papers on undisturbed in vivo DP-biofilm using fluorescence-labelled antibodies/CLSM or FISH/CLSM, the antibodies and the different oligonucleotide probes were conjugated or labelled with different fluorochromes (e.g., Alexa Fluor dyes, ATTO dyes, Cy dyes, SYTO dyes, DAPI, and calcofluor) in order to identify a specific bacterial genus or species, all bacteria, or even bacterial components such as extracellular polysaccharide [12, 13, 19, 42-46, 50-52]. In this type of studies (antibodies/CLSM and FISH/CLSM), an obstacle with CLSM is the limited availability of fluorescent probe colours that have non-overlapping emission signals, meaning that only 2 to 4 distinct microbial taxa (depending on the microscope) can be differentiated in any one image [44]. A further methodological factor to be considered with regard to fluorescence is the problem of correct penetration of the fluorescent dyes. Paramonova et al [66] showed that poor penetration of the fluorescent dyes into biofilms thicker than 120 µm leads to a noticeable underestimation of biofilm thickness by CLSM. An additional problem with thick biofilms is the risk of underestimating bacterial numbers due to the degree of fading of the fluorophore when multiple optical sections are performed [44, 66]. Other disadvantages that may be associated with the fluorescence staining include: the existence of a percentage of people (8-12% of males and almost 1% of females), who are green/red colour blind from extracting any meaningful information from the images [67], the influence of the type of bacteria (e.g. Actinomyces spp. often results in an irregular distribution of fluorescent signals, possibly because of insufficient permeability of the bacterial cell walls) and of its physiological state (exponential-growth phase vs stationary phase) about the staining properties [45, 68], some fluorochromes showed a significant non-specific binding to the matrix and great background fluorescence [69] or the detection of intermediate colors of “unknown” interpretation [68]. Recently, Chalmers et al [50] applied quantum dot (QD) based primary immunofluorescence for Veillonella spp. and for receptor polysaccharide (RPS) bearing Streptococcus spp. to achieve high, single-cell, resolution and to analyse spatio-temporal relationships between these bacteria in 6-hour and 8-hour biofilm communities. The results supported the use of QD-based immunofluorescence as a tool for the study of undisturbed in vivo DP-biofilm, as it detects multispecies communities similar to those revealed in previous studies using antibody-Alexa Fluor conjugates published by the same research group [51, 52]. Furthermore, it has been stated that QD conjugates offer significant advantages over traditional fluorophore fluorescence: QD conjugates have a high specificity and orders of magnitude higher sensitivity than can be achieved with traditional fluorophores [70]; QD luminescence is photostable and size-tunable, with narrow, symmetric emission spectra and broad continuous excitation, allowing excitation of multiple QD with a single wavelength [50, 71]. Chalmers et al [50] concluded that one application that benefits greatly from the photostability of QD conjugates is micromanipulation of viable, spatially resolved multispecies communities from the surface of the substrate.
3.4. Confocal laser scanning microscopy
Over the years, different microscopic techniques including light microscopy, transmission electron microscopy (TEM) and scanning electron microscopy (SEM) have frequently been employed to visualise the microstructure of in vivo oral biofilms [72-75]. It can be difficult to achieve penetrative views of specimens using these techniques or the samples require preparation involving dehydration, fixing, and embedding, which may cause disruptive shrinkage and loss of biofilm matrix that can affect 73% to 98% of the in vivo biofilm mass [76]. TEM is prone to preparation artefact, mainly affecting delicate fluid-filled structures [10]. The advent of CLSM, though of lower resolution than TEM [44], has eliminated or considerably reduced these problems. With CLSM (using inverted or non-inverted microscopes), biofilms can be studied in their natural hydrated state (usually using a 63x water-immersion lens), with no requirement for dehydration, fixation, or staining [11, 20, 53]. In addition, the optical sectioning properties of CLSM mean that very thin optical sections in the horizontal plane (X-Y axes) can be taken at 0.5 to 2 µm intervals, at increasing depths through the biofilm (from the surface of the biofilm to its base), free from out-of-focus blurring [12, 13, 44, 53, 55]. Robinson et al [48] evaluated the 7-day DP-biofilm using CLSM without fluorescence solutions. The optical data were therefore recorded as a series of arbitrarily assigned grey levels numbered 1 to 20 according to the degree of reflectance observed. However, in the other studies published on undisturbed in vivo DP-biofilm, the authors used CLSM with fluorescent dyes to make elements visible [12, 13, 44, 53, 55]. The excitation value and emission range of
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 601
______________________________________________

the fluorescence imaging were measured at different wavelengths depending on the fluorochrome used –e.g. the SYTO 9 and PI excitation values and emission range wavelengths are 488 nm (492–550 nm) and 561 nm (588–655 nm), respectively [30]. Fluorescence emission was analyzed in series of X-Y images in which each image corresponded to a single Z position (depth) [12, 13, 44, 53, 55], as showed in Figure 2. DP-biofilm thickness is usually used as an initial quantitative measurement of biomass [10, 12, 22, 45]. DP-biofilm thickness has been defined as the distance between the substrate and the peaks of the highest cell clusters [77]. However, some authors observed that the substrate surface was never exactly horizontal with respect to the microscope stage, and the number of optical sections per specimen was not directly translatable to DP-biofilm thickness [44, 45, 51]. Bacterial quantification can be performed by manual counting, which requires high-magnification images to allow differentiation between single cells. Furthermore, to obtain representative estimates, a large number of consecutive images need to be recorded and counted, which is time-consuming [13]. Also it has been recognized that counting of cells in aggregates is complicated because densely packed cells cannot easily be separated during image segmentation [13, 75]. It is probably for these reasons that the majority of authors have employed automated (digital) image analysis tools that have been developed for the quantification of fluorescence signals [10-12, 20, 22, 39-42, 46, 53]. Figure 2 shows as in automated image analysis, the images of each fluorochrome are defined as channels (e.g., for the quantification of viability, SYTO 9 occupies the green channel and PI the red channel) and are subsequently converted to quantitative data. However, Dige et al [13] stated that the generation of quantitative data from images based on fluorescence signals is a complex process. A number of researchers therefore performed quantitative analyses based on the ratios of the area occupied by each micro-organism to the whole area (mainly in studies on biofilm viability) [10, 11, 20, 22, 39-41, 53]; others quantified the biomass of different targets (probes) in the DP-biofilm by setting the EUB338-corresponding fluorescence volume at 100%; they then calculated other targets as a percentage of the EUB338-fluorescing biomass (mainly in studies on biofilm topography) [12, 42, 46].
As a possible alternative, Dige et al [13, 45] recently suggested that the combined use of FISH/CLSM and stereological methods is an attractive tool for quantification of bacterial populations in undisturbed in vivo DP-biofilm. This technique provides an unbiased and reliable determination of the numerical contribution of specific species in mixed bacterial communities. Importantly, stereological methods avoid the inherent problems associated with varying intensity of the fluorophore, which gives rise to a possible bias in automated image analysis. However, the stereological methods have their own disadvantages: they are relatively time-consuming compared to automated digital image analysis, and they require prior knowledge of bacterial morphology [13].
Irrespective of the quantification strategy, the dense packing of bacteria in DP-biofilms sometimes makes analysis difficult because of interference by fluorescence signals from adjacent, out-of-focus planes [44]. Other problems have also been detected: fading of the fluorophore following optical sectioning; differences in fluorescence intensities depending on the dyes used for probe labelling and in cell-specific uptakes of fluorescence stains; and varying thresholds [13, 45]. Sekar et al [78] therefore recommended that CLSM of the biofilm area/volume should include size standards such as microbeads during image acquisition in order to minimize the inherent error in quantitative measurements. Among the possible drawbacks of CLSM, is the use of microscopy as the basis of the technique which makes the selection of regions of dental plaque for analysis highly observer-dependent [33]. The high density of DP-biofilms grown in vivo can limit the laser penetration depth of CLSM (conventional one-photon excitation) to the outer 40 to 100 µm of the biofilm cell clusters; this could mean that deeper areas are not reliably visualised [33, 61]. Kawaguchi and Decho [79] demonstrated that two-photon excitation CLSM could achieve deeper penetration of tissue biofilms and enhance resolution.
Schaudinn et al [57] proposed a combined method using more than one microscopic technique to provide unique information about a structure that is difficult or even impossible to obtain with a single imaging regimen. However, the application of combined microscopy techniques for the characterisation of undisturbed in vivo DP-biofilm has been underexploited [80], as few authors have used CLSM in combination with other methods of microscopy, such as SEM, TEM, or epifluorescence microscopy [10, 46, 56, 57].
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
602 ©FORMATEX 2010
______________________________________________
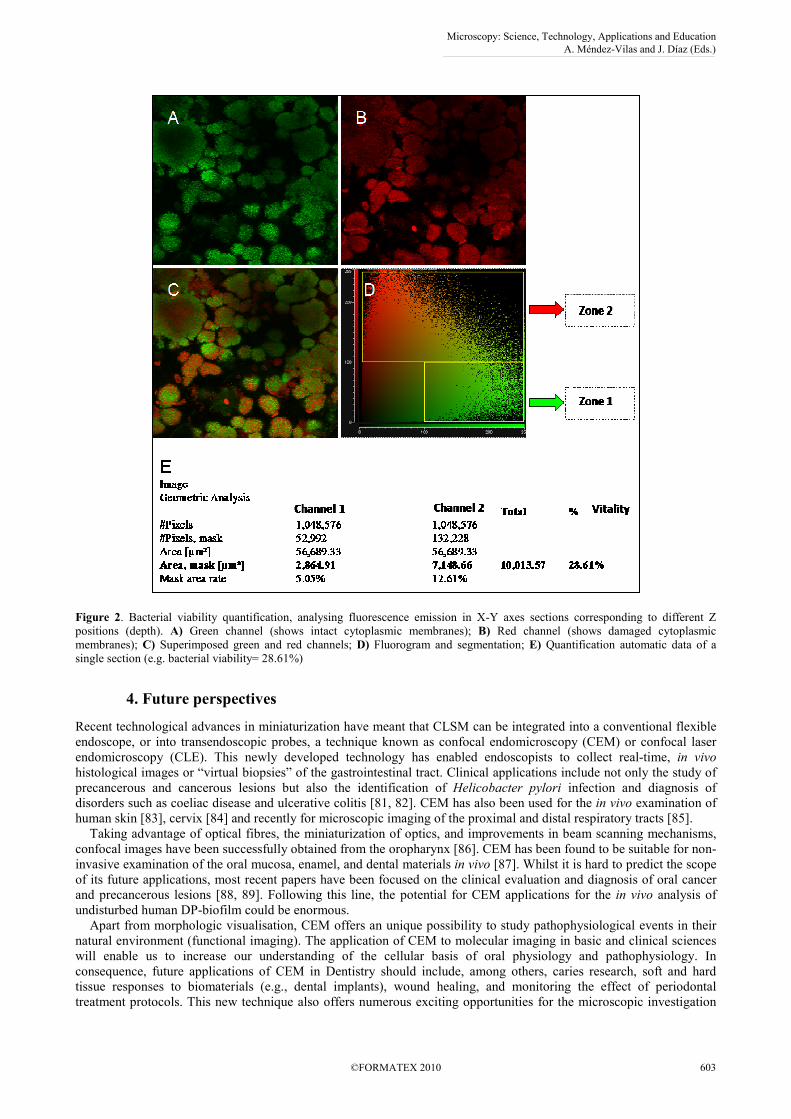
Figure 2. Bacterial viability quantification, analysing fluorescence emission in X-Y axes sections corresponding to different Z positions (depth). A) Green channel (shows intact cytoplasmic membranes); B) Red channel (shows damaged cytoplasmic membranes); C) Superimposed green and red channels; D) Fluorogram and segmentation; E) Quantification automatic data of a single section (e.g. bacterial viability= 28.61%)
4. Future perspectives
Recent technological advances in miniaturization have meant that CLSM can be integrated into a conventional flexible endoscope, or into transendoscopic probes, a technique known as confocal endomicroscopy (CEM) or confocal laser endomicroscopy (CLE). This newly developed technology has enabled endoscopists to collect real-time, in vivo histological images or “virtual biopsies” of the gastrointestinal tract. Clinical applications include not only the study of precancerous and cancerous lesions but also the identification of Helicobacter pylori infection and diagnosis of disorders such as coeliac disease and ulcerative colitis [81, 82]. CEM has also been used for the in vivo examination of human skin [83], cervix [84] and recently for microscopic imaging of the proximal and distal respiratory tracts [85]. Taking advantage of optical fibres, the miniaturization of optics, and improvements in beam scanning mechanisms, confocal images have been successfully obtained from the oropharynx [86]. CEM has been found to be suitable for non-invasive examination of the oral mucosa, enamel, and dental materials in vivo [87]. Whilst it is hard to predict the scope of its future applications, most recent papers have been focused on the clinical evaluation and diagnosis of oral cancer and precancerous lesions [88, 89]. Following this line, the potential for CEM applications for the in vivo analysis of undisturbed human DP-biofilm could be enormous. Apart from morphologic visualisation, CEM offers an unique possibility to study pathophysiological events in their natural environment (functional imaging). The application of CEM to molecular imaging in basic and clinical sciences will enable us to increase our understanding of the cellular basis of oral physiology and pathophysiology. In consequence, future applications of CEM in Dentistry should include, among others, caries research, soft and hard tissue responses to biomaterials (e.g., dental implants), wound healing, and monitoring the effect of periodontal treatment protocols. This new technique also offers numerous exciting opportunities for the microscopic investigation
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 603
______________________________________________
of many clinical operative procedures in vivo, allowing the response of the oral tissues to be non-destructively monitored over time at high resolution.
References
[1] Marsh PD. Dental plaque: Biological significance of a biofilm and community life-style. Journal of Clinical Periodontology. 2005;32:7-15.
[2] Donlan RM, Costerton JW. Biofilms: Survival mechanisms of clinically relevant microorganisms. Clinical Microbiology Reviews. 2002;15:167-193.
[3] Socransky SS, Haffajee AD. Dental biofilms: Difficult therapeutic targets. Periodontology 2000. 2002;28:12-55. [4] Marsh PD. Dental plaque as a microbial biofilm. Caries Research. 2004;38:204-211. [5] Keijser BJ, Zaura E, Huse SM, van der Vossen JM, Schuren FH, Montijn RC, ten Cate JM, Crielaard W. Pyrosequencing analysis
of the oral microflora of healthy adults. Journal Dental Research. 2008;87:1016-1020. [6] Madianos PN, Bobetsis YA, Kinane DF. Generation of inflammatory stimuli: How bacteria set up inflammatory responses in the
gingiva. Journal of Clinical Periodontology. 2005;32:57-71. [7] Takahashi N, Nyvad B. Caries ecology revisited: Microbial dynamics and the caries process. Caries Research. 2008;42:409-418. [8] Schaudinn C, Gorur A, Keller D, Sedghizadeh PP, Costerton JW. Periodontitis: An archetypical biofilm disease. Journal of
American Dental Association. 2009;140:978-986. [9] Wright SJ, Wright DJ. Introduction to confocal microscopy. Methods in Cell Biology. 2002;70:1-85. [10] Wood SR, Kirkham J, Marsh PD, Shore RC, Nattress B, Robinson C. Architecture of intact natural human plaque biofilms
studied by confocal laser scanning microscopy. Journal of Dental Research. 2000;79:21-27. [11] Arweiler NB, Hellwig E, Sculean A, Hein N, Auschill TM. Individual vitality pattern of in situ dental biofilms at different
locations in the oral cavity. Caries Research. 2004;38:442-447. [12] Al-Ahmad A, Wunder A, Auschill TM, Follo M, Braun G, Hellwig E, Arweiler NB. The in vivo dynamics of Streptococcus
spp., Actinomyces naeslundii, Fusobacterium nucleatum and Veillonella spp. in dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. Journal of Medical Microbiology. 2007;56:681-687.
[13] Dige I, Nyengaard JR, Kilian M, Nyvad B. Application of stereological principles for quantification of bacteria in intact dental biofilms. Oral Microbiology and Immunology. 2009;24:69-75.
[14] Kolenbrander PE, Palmer RJ Jr, Rickard AH, Jakubovics NS, Chalmers NI, Diaz PI. Bacterial interactions and successions during plaque development. Periodontology 2000. 2006;42:47-79.
[15] Jefferson KK, Cerca N. Bacterial-bacterial cell interactions in biofilms: Detection of polysaccharide intercellular adhesins by blotting and confocal microscopy. Methods in Molecular Biology. 2006;341:119-126.
[16] McBain AJ. Chapter 4: In vitro biofilm models: An overview. Advances in Applied Microbiology. 2009;69:99-132. [17] Nobbs AH, Lamont RJ, Jenkinson HF. Streptococcus adherence and colonization. Microbiology and Molecular Biology
Reviews. 2009;73:407-450. [18] Palmer RJ Jr. Supragingival and subgingival plaque: Paradigm of biofilms. The Compendium of Continuing Education in
Dentistry. 2010;31:104-138. [19] Wecke J, Kersten T, Madela K, Moter A, Göbel UB, Friedmann A, Bernimoulin J. A novel technique for monitoring the
development of bacterial biofilms in human periodontal pockets. FEMS Microbiology Letters. 2000;191:95-101. [20] Auschill TM, Hellwig E, Sculean A, Hein N, Arweiller NB. Impact of the intraoral location on the rate of biofilm growth.
Clinical Oral Investigations. 2004;8:97-101. [21] Watson PS, Pontefract HA, Devine DA, Shore RC, Nattres BR, Kirkham J, Robinson C. Penetration of fluoride into natural
plaque biofilms. Journal of Dental Research. 2005;84:451-455. [22] Auschill TM, Hein N, Hellwig E, Follo M, Sculean A, Arweiler NB. Effect of two antimicrobial agents on early in situ biofilm
formation. Journal of Clinical Periodontology. 2005;32:147-152. [23] Hannig C, Hannig M. The oral cavity--a key system to understand substratum-dependent bioadhesion on solid surfaces in man.
Clinical Oral Investigations. 2009;13:123-139. [24] Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: A common cause of persistent infections. Science. 1999;284:1318-
1322. [25] Palmer RJ Jr, Wu R, Gordon S, Bloomquist CG, Liljemark WF, Kilian M, Kolenbrander PE. Retrieval of biofilms from the oral
cavity. Methods in Enzymology. 2001;337:393-403. [26] Rosin M, Welk A, Bernhardt O, Ruhnau M, Pitten FA, Kocher T, Kramer A. Effect of a polyhexamethylene biguanide
mouthrinse on bacterial counts and plaque. Journal of Clinical Periodontology. 2001;28:1121-1126. [27] Rosin M, Welk A, Kocher T, Majic-Todt A, Kramer A, Pitten FA. The effect of a polyhexamethylene biguanide mouthrinse
compared to an essential oil rinse and a chlorhexidine rinse on bacterial counts and 4-day plaque regrowth. Journal of Clinical Periodontology. 2002;29:392-399.
[28] Daneshmand N, Jorgensen MG, Nowzari H, Morrison JL, Slots J. Initial effect of controlled release chlorhexidine on subgingival microorganisms. Journal of Periodontal Research. 2002;37:375-379.
[29] Sreenivasan PK, Mattai J, Nabi N, Xu T, Gaffar A. A simple approach to examine early oral microbial biofilm formation and the effects of treatments. Oral Microbiology and Inmunology. 2004;19:297-302.
[30] Tomás I, García-Caballero L, Cousido M, Limeres J, Álvarez M, Diz P. Evaluation of chlorhexidine substantivity on salivary flora by epifluorescence microscopy. Oral Diseases. 2009;15:428-433.
[31] König J, Storcks V, Kocher T, Bössmann K, Plagmann HC. Anti-plaque effect of tempered 0.2% chlorhexidine rinse: An in vivo study. Journal of Clinical Periodontology. 2002;29:207-210.
[32] Arweiler NB, Boehnke N, Sculean A, Hellwig E, Auschill TM. Differences in efficacy of two commercial 0.2% chlorhexidine mouthrinse solutions: A 4-day plaque regrowth study. Journal of Clinical Periodontology. 2006;33:334-339.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
604 ©FORMATEX 2010
______________________________________________
[33] van der Mei HC, White D.J, Atema-Smit J, van de Belt-Gritter E, Busscher HJ. A method to study sustained antimicrobial activity of rinse and dentifrice components on biofilm viability in vivo. Journal of Clinical Periodontology. 2006;33:14-20.
[34] Al-Ahmad A, Roth D, Wolkewitz M, Wiedmann-Al-Ahmad M, Follo M, Ratka-Krüger P, Deimling D, Hellwig E, Hannig C. Change in diet and oral hygiene over an 8-week period: Effects on oral health and oral biofilm. Clinical Oral Investigations. 2010;14:391-396.
[35] Loivukene K, Pahkla ER, Koppel T, Saag M, Naaber P. The microbiological status of patients with periodontitis in southern Estonia after non-surgical periodontal therapy. Stomatologija. 2005;7:45-47.
[36] Sculean A, Auschill TM, Donos N, Brecx M, Arweiler NB. Effect of an enamel matrix protein derivative (Emdogain) on ex vivo dental plaque vitality. Journal Clinical Periodontology. 2001;28:1074-1078.
[37] Watson TF. Applications of confocal scanning optical microscopy to dentistry. British Dental Journal. 1991;171:287-291. [38] Watson TF, Petroll WM, Cavanagh HD, Jester JV. In vivo confocal microscopy in clinical dental research: An initial appraisal.
Journal of Dentistry. 1992;20:352-358. [39] Netuschil L, Reich E, Unteregger G, Sculean A, Brecx M. A pilot study of confocal laser scanning microscopy for the
assessment of undisturbed dental plaque vitality and topography. Archives of Oral Biology. 1998;43:277-285. [40] Auschill TM, Arweiler NB, Netuschil L, Brecx M, Reich E, Sculean A. Spatial distribution of vital and dead microorganisms in
dental biofilms. Archives of Oral Biology. 2001;46:471-476. [41] Zaura-Arite E, van Marle J, ten Cate JM. Confocal microscopy study of undisturbed and chlorhexidine-treated dental biofilm.
Journal of Dental Research. 2001;80:1436-1440. [42] Diaz PI, Chalmers NI, Rickard AH, Kong C, Milburn CL, Palmer RJ Jr, Kolenbrander PE. Molecular characterization of
subject-specific oral microflora during initial colonization of enamel. Applied and Environmental Microbiology. 2006;72:2837-2848.
[43] Auschill TM, Arweiler NB, Brecx M, Reich E, Sculean A, Netuschil L. The effect of dental restorative materials on dental biofilm. European Journal of Oral Sciences. 2002;110:48-53.
[44] Dige I, Nilsson H, Kilian M, Nyvad B. In situ identification of streptococci and other bacteria in initial dental biofilm by confocal laser scanning microscopy and fluorescence in situ hybridization. European Journal of Oral Sciences. 2007;115:459-467.
[45] Dige I, Raarup MK, Nyengaard JR, Kilian M, Nyvad B. Actinomyces naeslundii in initial dental biofilm formation. Microbiology. 2009;155:2116-2126.
[46] Jung DJ, Al-Ahmad A, Follo M, Spitzmüller B, Hoth-Hannig W, Hannig M, Hannig C. Visualization of initial bacterial colonization on dentine and enamel in situ. Journal of Microbiological Methods. 2010;81:166-174.
[47] Wood S, Nattress B, Kirkham J, Shore R, Brookes S, Griffiths J, Robinson C. An in vitro study of the use of photodynamic therapy for the treatment of natural oral plaque biofilms formed in vivo. Journal of Photochemistry and Photobiology B, Biology. 1999;50:1-7.
[48] Robinson C, Strafford S, Rees G, Brookes SJ, Kirkham J, Shore RC, Watson PS, Wood S. Plaque biofilms: The effect of chemical environment on natural human plaque biofilm architecture. Archives of Oral Biology. 2006;51:1006-1014.
[49] Robinson C, Kirkham J, Percival R, Shore RC, Bonass WA, Brookes SJ, Kusa L, Nakagaki H, Kato K, Nattress B. A method for the quantitative site-specific study of the biochemistry within dental plaque biofilms formed in vivo. Caries Research. 1997;31:194-200.
[50] Chalmers NI, Palmer RJ Jr, Du-Thumm L, Sullivan R, Shi W, Kolenbrander PE. Use of quantum dot luminescent probes to achieve single-cell resolution of human oral bacteria in biofilms. Applied and Environmental Microbiology. 2007;73:630-636.
[51] Palmer RJ Jr, Gordon SM, Cisar JO, Kolenbrander PE. Coaggregation-mediated interactions of streptococci and actinomyces detected in initial human dental plaque. Journal of Bacteriology. 2003;185:3400-3409.
[52] Palmer RJ Jr, Diaz PI, Kolenbrander PE. Rapid succession within the Veillonella population of a developing human oral biofilm in situ. Journal of Bacteriology. 2006;188:4117-4124.
[53] Arweiler NB, Lenz R, Sculean A, Al-Ahmad A, Hellwig E, Auschill TM. Effect of food preservatives on in situ biofilm formation. Clinical Oral Investigations. 2008;12:203-208.
[54] Gu F, Lux R, Du-Thumm L, Stokes I, Kreth J, Anderson MH, Wong DT, Wolinsky L, Sullivan R, Shi W. In situ and non-invasive detection of specific bacterial species in oral biofilms using fluorescently labeled monoclonal antibodies. Journal of Microbiological Methods. 2005;62:145-160.
[55] Konishi N, Torii Y, Kurosaki A, Takatsuka T, Itota T, Yoshiyama M. Confocal laser scanning microscopic analysis of early plaque formed on resin composite and human enamel. Journal of Oral Rehabilitation. 2003;30:790-795.
[56] Perez Davidi M, Beyth M, Sterer N, Feuerstein O, Weiss EI. Effect of liquid-polish coating on in vivo biofilm accumulation on provisional restorations: part 1. Quintessence International. 2007;38:591-596.
[57] Schaudinn C, Carr G, Gorur A, Jaramillo D, Costerton JW, Webster P. Imaging of endodontic biofilms by combined microscopy (FISH/CLSM-SEM). Journal of Microscopy. 2009;235:124-127.
[58] Foster JS, Palmer RJ Jr, Kolenbrander PE. Human oral cavity as a model for the study of genome-genome interactions. The Biological Bulletin. 2003;204:200-204.
[59] Dongari-Bagtzoglou A. Pathogenesis of mucosal biofilm infections: Challenges and progress. Expert Review Anti-Infective Therapy. 2008;6:201-208.
[60] Daims H, Wagner M. Quantification of uncultured microorganisms by fluorescence microscopy and digital image analysis. Applied Microbiology and Biotechnology. 2007;75:237-248.
[61] von Ohle C, Gieseke A, Nistico L, Decker EM, DeBeer D, Stoodley P. Real-time microsensor measurement of local metabolic activities in ex vivo dental biofilms exposed to sucrose and treated with chlorhexidine. Applied and Environmental Microbiology. 2010 ;76:2326-2334.
[62] Netuschil L. Vitalfärbung von plaque-mikroorganismen mit fluoresceindiacetat und ethidium-bromid. Deutsche Zahnärztliche Zeitschrift. 1983;38:914-917.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 605
______________________________________________

[63] Singh R, Stine OC, Smith DL, Spitznagel JK Jr, Labib ME, Williams HN. Microbial diversity of biofilms in dental unit water systems. Applied and Environmental Microbiology 2003;69:3412-3420.
[64] Hope CK, Wilson M. Analysis of the effects of chlorhexidine on oral biofilm vitality and structure based on viability profiling and an indicator of membrane integrity. Antimicrobial Agents and Chemotherapy. 2004;48:1461-1468.
[65] Filoche SK, Coleman MJ, Angker L, Sissons CH. A fluorescence assay to determine the viable biomass of microcosm dental plaque biofilms. Journal of Microbiological Methods. 2007;69:489-496.
[66] Paramonova E, de Jong ED, Krom BP, van der Mei HC, Busscher HJ. Sharma PK. Low-load compression testing: A novel way of measuring biofilm thickness. Applied and Environmental Microbiology. 2007;73:7023-7028.
[67] Hope CK, Clements D, Wilson M. Determining the spatial distribution of viable and nonviable bacteria in hydrated microcosm dental plaques by viability profiling. Journal of Applied Microbiology. 2002;93:448-455.
[68] Berney M, Hammes F, Bosshard F, Weilenmann HU, Egli T. Assessment and interpretation of bacterial viability by using the LIVE/DEAD Baclight Kit in combination with flow cytometry. Applied and Environmental Microbiology. 2007;73:3283-3290.
[69] Biggerstaff JP, Le Puil M, Weidow BL, Prater J, Glass K, Radosevich M, White DC. New methodology for viability testing in environmental samples. Molecular and Cellular Probes. 2006;20:141-146.
[70] Hahn MA, Tabb JS, Krauss TD. Detection of single bacterial pathogens with semiconductor quantum dots. Analytical Chemistry. 2005;77:4861-4869.
[71] Kloepfer JA, Mielke RE, Wong MS, Nealson KH, Stucky G, Nadeau JL. Quantum dots as strain- and metabolism-specific microbiological labels. Applied and Environmental Microbiology. 2003;69:4205-4213.
[72] Listgarten MA, Mayo HE, Tremblay R. Development of dental plaque on epoxy resin crowns in man. A light and electron microscopic study. Journal of Periodontology. 1975;46:10-26.
[73] Listgarten MA. Structure of the microbial flora associated with periodontal health and disease in man. A light and electron microscopic study. Journal of Periodontology. 1976;47:1-18.
[74] Hannig M. Transmission electron microscopy of early plaque formation on dental materials in vivo. European Journal of Oral Sciences. 1999;107:55-64.
[75] Hannig C, Hannig M, Rehmer O, Braun G, Hellwig E, Al-Ahmad A. Fluorescence microscopic visualization and quantification of initial bacterial colonization on enamel in situ. Archives of Oral Biology. 2007;52:1048-1056.
[76] Handley PS, Sutton NA, Hughes N. Problems associated with electron microscopy of biofilms. In: Wimpenny J, Nichols W, Stickler D, Lappin-Scott H, eds. Bacterial biofilms and their control in medicine and industry. Cardiff: Bio-line; 1993:61-66.
[77] Roberts SK, Bass C, Brading M, Lappin-Scott H, Stoodley P. Biofilm formation and structure; What’s new?. In: Newman HN, Wilson M, eds. Dental plaque revisited-oral biofilms in health and disease. Cardiff: BioLine; 1999:15-36.
[78] Sekar R, Griebe T, Flemming HC. Influence of image acquisition parameters on quantitative measurements of biofilms using confocal laser scanning microscopy. Biofouling. 2002;18:47-56.
[79] Kawaguchi T, Decho AW. In situ microspatial imaging using two-photon and confocal laser scanning microscopy of bacteria and extracellular polymeric secretions (EPS) within marine stromatolites. Marine Biotechnology. 2002;4:127-131.
[80] Wrede C, Heller C, Reitner J, Hoppert M. Correlative light/electron microscopy for the investigation of microbial mats from Black Sea Cold Seeps. Journal of Microbiological Methods 2008;73:85-91.
[81] De Palma GD. Confocal laser endomicroscopy in the in vivo histological diagnosis of the gastrointestinal tract. World Journal of Gastroenterology:WJG. 2009;15:5770-5775.
[82] Goetz M, Kiesslich R. Advances of endomicroscopy for gastrointestinal physiology and diseases. American Journal of Physiology. Gastrointestinal and Liver Physiology. 2010;298:G797-806.
[83] Eichert S, Möhrle M, Breuninger H, Röcken M, Garbe C, Bauer J. Diagnosis of cutaneous tumors with in vivo confocal laser scanning microscopy. Journal der Deutschen Dermatologischen Gessellschaft. 2010;8:400-410.
[84] Tan J, Quinn MA, Pyman JM, Delaney PM, McLaren WJ. Detection of cervical intraepithelial neoplasia in vivo using confocal endomicroscopy. BJOG: An International Journal of Obstetrics and Gynaecology. 2009;116:1663-1670.
[85] Thiberville L, Salaün M, Lachkar S, Dominique S, Moreno-Swirc S, Vever-Bizet C, Bourg-Heckly G. Confocal fluorescence endomicroscopy of the human airways. Proceedings of the American Thoracic Society. 2009;6:444-449.
[86] Haxel BR, Goetz M, Kiesslich R, Gosepath J. Confocal endomicroscopy: A novel application for imaging of oral and oropharyngeal mucosa in human. European Archives of Oto-Rhino-Laryngology. 2010;267:443-448.
[87] Burmeister M, von Schwanewede H, Stave J, Guthoff RF. Intraoral diagnostics using confocal laser scanning microscopy. Biomedizinische Technik. Biomedical Engineering. 2009;54:23-28.
[88] Maitland KC, Gillenwater AM, Williams MD, El-Naggar AK, Descour MR, Richards-Kortum RR. In vivo imaging of oral neoplasia using a miniaturized fiber optic confocal reflectance microscope. Oral Oncology. 2008;44:1059-1066.
[89] Anuthama K, Sherlin HJ, Anuja N, Ramani P, Premkumar P, Chandrasekar T. Characterization of different tissue changes in normal, betel chewers, potentially malignant lesions, conditions and oral squamous cell carcinoma using reflectance confocal microscopy: Correlation with routine histopathology. Oral Oncology. 2010;46:232-248.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
606 ©FORMATEX 2010
______________________________________________
Copyright © 2022 FDOKUMEN




















