
in first aid Evidence-based practice - Lirias
180
Katholieke Universiteit Leuven Group Biomedical Sciences Faculty of Medicine Academic Department of General Practice Doctoral thesis in Medical Sciences Leuven, 2011 in first aid Stijn Van de Velde Evidence-based practice
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of in first aid Evidence-based practice - Lirias

Katholieke Universiteit LeuvenGroup Biomedical SciencesFaculty of MedicineAcademic Department of General Practice
Doctoral thesis in Medical SciencesLeuven, 2011
in first aid
Stijn Van de Velde
Evidence-based practice

Copyright cover photo: Rode Kruis-Vlaanderen |Carl Vandervoort

Katholieke Universiteit Leuven
Group Biomedical Sciences
Faculty of Medicine
Academic Department of General Practice
Belgian Centre for Evidence-Based Medicine
Belgian Branch of the Dutch Cochrane Centre
EVIDENCE-BASED PRACTICE IN FIRST AID
Stijn Van de Velde
Jury: F. Buntinx, D. Knockaert, B. Nemery de Bellevaux, K. Vandewoude, J. Volmink
Promoter: B. Aertgeerts
Co-promoter: D. Ramaekers
Co-promoter: P. Vandekerckhove
Leuven, 30 June 2011
Doctoral Thesis in Medical Sciences


TABLE OF CONTENTS
1

CHAPTER 1 Introduction 5
The importance of first aid training 6
The role of evidence-based practice 7
Evidence-based practice and first aid 9
Specific objectives and outline of the thesis 10
CHAPTER 2 European first aid guidelines 13
CHAPTER 3 Effectiveness of nonresuscitative first aid training in
laypersons: a systematic review
27
CHAPTER 4 Does training on barriers to helping facilitate
emergency helping behaviour among laypersons
trained in first aid? A randomised deception trial
45
CHAPTER 5 Rapid reviews 67
BestBET 1: optimal body position in oral poisoning
cases
68
BET 2: Potato peel dressings for burn wounds 72
Medicinal use of potato-derived products:
conclusions of a rapid versus full systematic
review
76
CHAPTER 6 Rigour of development does not AGREE with
recommendations in practice guidelines on the use
of ice for acute ankle sprains
81
2

CHAPTER 7 Discussion 91
Contributions of this thesis 92
Current methodological perspectives on evidence-
based guidelines in general and on the European
first aid guidelines in particular
94
Potential solutions for drawing the line between
evidence-based and ‘evidence-biased’ guidelines
99
Suggestions for future research 100
Conclusions 103
REFERENCES 105
SUMMARY 113
SAMENVATTING 119
PROFESSIONAL CAREER 125
LIST OF PUBLICATIONS 129
ACKNOWLEDGEMENTS 133
APPENDICES
European first aid guidelines: search strategy 137
RCT: Questionnaires 157
RCT: Didactical plan experimental and control
intervention
167
3

4

INTRODUCTION
CHAPTER 1
5

1.1 The importance of first aid training
Injuries account for 8% of mortality and 13% of disability-adjusted life years
(DALY) in the European region.1 Incidence estimates for trauma from accidents
and violence equate to 1 death and 18 persons needing first aid treatment per
minute in Europe.1 The burden of injuries to health globally is considerable.
Many of these deaths are inevitable and occur before pre-hospital medical care
is available.2-4 However, post-mortem examinations of pre-hospital deaths
indicated that at least one third could have been prevented by means of simple
actions.4;5 Observational studies reported that in more than half of the cases
bystanders were at the accident site before the arrival of medical care.6;7 If
these bystanders are able and willing to provide aid, they have the potential to
save lives. The provision of such immediate help by laypeople to suddenly ill or
injured persons before the arrival of professional medical care is commonly
defined as first aid.8 From the above it has been advocated that as many people
as possible should be trained in first aid.
The concept of first aid training for laypeople exists since the 19th century. Henri
Dunant, the founder of the Red Cross, developed the idea after the bloody
battle of Solferino in 1859. He noticed that the wounded lacked medical
attention and organised local volunteers to provide care. Since its start, the
curricula have constantly been revised.9 In the past, first aid handbooks were
primarily based on experience and specialist knowledge. By the end of the 20th
century more importance was given to evidence-based curricula and to the
demonstration of educational efficacy.10 Since 2000 there have been
international guidelines for resuscitation which are evidence-based.11 The
guidelines are updated every five years12 and now form an important basis for
European first aid handbooks.
6

1.2 The role of evidence-based practice
While first aid aims to bridge the gap between an emergency and initiation of
medical care,8 the evidence-based movement seeks to bridge the gap between
scientific evidence and practice. In 1991 the term evidence-based medicine was
coined for the first time in published literature.13 In a key article, published in
1992, the evidence-based concept was presented as a new approach to
teaching and practising medicine.14 A common definition of evidence-based
medicine is “the conscientious, explicit, and judicious use of current best
evidence in making decisions about the care of individual patients”.15 The
evidence-based principles can be applied to diverse topics from astronomy over
psychology to zoology.16 As the evidence-based movement rapidly expanded to
areas outside medicine, this gave rise to the term evidence-based practice.
The evidence-based principle found its origin in the realisation that intuition,
experience and pathophysiological reasoning were insufficient grounds to
decide on medical care.14 New skills to acquire and appraise available evidence
were propagated. Evidence-based guidelines and systematic reviews evolved
from the explosion of clinical research as an instrument to translate evidence
into practice. A systematic review is “a review of a clearly formulated question
that uses systematic and explicit methods to identify, select, and critically
appraise relevant research, and to collect and analyse data from the studies
that are included in the review. Statistical methods (meta-analysis) may or may
not be used to analyse and summarise the results of the included studies.”17;18 A
difference with traditional or narrative reviews is that the latter lack systematic
strategies to reduce bias.19 Since 1980 the number of systematic reviews has
grown tremendously. An important milestone was the launch of the Cochrane
Collaboration in 1993 which develops and disseminates systematic reviews on
the effects of health care interventions. Today there are 4,500 Cochrane
7

reviews and 14,000 other systematic reviews in the Cochrane library. Eleven
new systematic reviews of trials are being published every day.20
The Institute of Medicine defined clinical practice guidelines as “systematically
developed statements to assist practitioner and patient decisions about
appropriate health care for specific clinical circumstances”.21 Regarding its
development three main types of guidelines can be distinguished: a) informal
consensus-based guidelines which are developed by a group of experts based
on their opinion and practical experience; b) formal consensus-based guidelines
which use systematic methods to translate expert opinion in recommendations;
and c) evidence-based practice guidelines which represent the best judgment of
a team of clinical and methodological experts taking into account findings from
a systematic literature review, practical experience, values, preferences and
circumstances for a specific topic.22 Evidence-based guidelines are generally
considered to produce more valid recommendations because they
systematically integrate the scientific evidence.23;24 Two important databases of
guidelines worldwide are the G-I-N Guideline Library (http://www.g-i-n.net/)
and the National Guideline Clearinghouse (http://www.guideline.gov/
The main objective of evidence-based guidelines is to improve the quality of
care. For those receiving care, this can imply improved health outcomes, and
consistency of care. For care providers, guidelines can address the risk of
performing interventions that are outdated, ineffective or even harmful. From
the policy perspective, guidelines have the potential to get the best value for
money. The gaps in literature identified in guidelines can also benefit
researchers in defining the future research agenda.23
). While
the latter database contained 700 guidelines in 2000, it now holds 2400
guidelines. Because many guidelines exist outside this database, it is not the
precise number which is important but rather the illustration of the growth
which has occurred.
8

1.3 Evidence-based practice and first aid
The case of first aid for burns provides an early example of how evidence-based
practice can contribute to first aid. In contrast to current first aid manuals, the
use of water for burns was not a standard procedure in initial first aid manuals.
Since 1928, experiments with boiled eggs and animals, and evidence from
humans have provided support for the use of water for burns.25 Thirty years
later this principle gradually diffused into first aid manuals.26
At the start of this thesis, the evidence regarding the effectiveness of first aid
procedures and training remained to be systematically assessed. Several areas
of controversy existed among experts on which first aid procedures were most
appropriate. This was reflected in unpublished surveys among Red Cross
National Societies in Europe and in scientific literature.5;27;28 While
cardiopulmonary resuscitation by laypeople was extensively studied29 and
evidence-based guidelines were published in 2000 and updated in 2005,11;12 the
field of non-resuscitative first aid lagged behind in applying evidence-based
practice.
Taking into account a) the considerable burden of injury, b) the life-saving
potential of first aid, c) the potential benefits of evidence-based practice, d)
areas of controversy in first aid, and e) the gaps in systematic analysis of first aid
evidence, it was the purpose of this thesis to introduce evidence-based practice
in the first aid training activities of the Belgian Red Cross-Flanders and to add
new empirical data to the research base.
9

1.4 Specific objectives and outline of the thesis
The scope of the research is non-resuscitative first aid training for laypeople
with no formal medical education. We focussed on the development of
evidence-based training curricula and on the evaluation of educational efficacy.
To realise this objective we performed multiple studies, which we describe in
chapters 2 to 6. Chapter 7 discusses the contributions, strengths and limitations
and implications of the studies in this thesis.
Chapter 2. European First Aid Guidelines
First aid training courses for the public in European countries often vary in
terms of the first aid procedures which they recommend.
We developed evidence-based guidelines to determine the most effective, safe,
and feasible first aid techniques and procedures, and to formulate
recommendations for training.
Chapter 3. Systematic review
The effectiveness of non-resuscitative first aid training remained to be critically
assessed. We systematically reviewed studies on the effects of non-resuscitative
first aid training with regard to acquisition and retention of competence or
modification of helping behaviour.
Chapter 4. Randomised controlled trial
The evidence on the effect of first aid training on helping behaviour is
incomplete and of low quality. Therefore, we measured the effects of a newly
developed training programme on first aid self-efficacy beliefs and helping
behaviour by means of a randomised controlled trial (RCT).
Chapter 5. Rapid reviews
10

Practitioners, especially in emergency care settings, often have a pressing need
for information. While evidence-based practice is an important goal, it can be
challenging to find a compromise between scientific rigour, transparency and
timeliness. This situation has given rise to the methodology of rapid reviews in
which methods for the search, appraisal, synthesis and analysis are determined
by time constraints.19 BestBETs is a database of such reviews with a main focus
on emergency medicine (www.bestbets.org). The Best Evidence Topic reports
(BETs) provide brief and structured summaries of the best available evidence for
very specific clinical questions. They are not systematic reviews, but rapid
reviews that can be performed by busy emergency physicians30. We conducted
a review of the best available evidence on 1) optimal body position in oral
poisoning cases and on 2) potato peel dressings for burn wounds, within a
limited timeframe and containing the essential elements of an evidence-based
literature review.
Although the concept of rapid review is rising, there is limited evidence
regarding its validity. Therefore, we compared the results of this rapid review
with a systematic review focusing on the same topic and produced
independently of each other within the same timeframe.
Chapter 6. Comparison of guidelines on ankle sprains
While the number of published evidence-based guidelines has grown rapidly in
many areas of medicine, conflicting and poorly constructed guidelines
sometimes lead to confusion. We tried to add to the research in the quality of
evidence-based guidelines by evaluating the content and rigour of development
of recommendations on the use of ice in guidelines for acute ankle sprains.
11

12

European first aid guidelines
CHAPTER 2
Van de Velde S, Broos P, Van Bouwelen M, De Win R, Sermon A, Verduyckt J,
Van Tichelen A, Lauwaert D, Vantroyen B, Tobback C, Van den Steene P, Villere
S, Mieres CU, Gobl G, Schunder S, Monsieurs K, Bierens J, Cassan P, Davoli E,
Sabbe M, Lo G, De Vries M, Aertgeerts B. European first aid guidelines.
Resuscitation. 2007;72(2):240-251.
13

Resuscitation (2007) 72, 240—251
TRAINING AND EDUCATIONAL PAPER
European first aid guidelinesq,qq
Stijn Van de Velde ∗, Paul Broos, Marc Van Bouwelen, Rudy De Win,An Sermon, Johann Verduyckt, Andre Van Tichelen, Door Lauwaert,Barbara Vantroyen, Christina Tobback, Patrick Van den Steene,Sarmite Villere, Carlos Urkia Mieres, Gabor Gobl, Susanne Schunder,Koenraad Monsieurs, Joost Bierens, Pascal Cassan, Enrico Davoli,Marc Sabbe, Grace Lo, Maaike De Vries, Bert Aertgeerts,
on behalf of the European First Aid Manual project by the Belgian RedCrossFlanders
Training Department, Belgian Red CrossFlanders, Motstraat 40, 2800 Mechelen, Belgium
Received 26 August 2006; received in revised form 20 October 2006; accepted 20 October 2006
KEYWORDS
Emergency treatment;
Evidencebased
medicine;
First aid;
Guidelines;
Training
Summary
Aim: Our objectives were to determine the most effective, safe, and feasible firstaid (FA) techniques and procedures, and to formulate valid recommendations fortraining. We focussed on emergencies involving few casualties, where emergencymedical services or healthcare professionals are not immediately present at thescene, but are available within a short space of time. Due to time and resourceconstraints, we limited ourselves to safety, emergency removal, psychosocial FA,traumatology, and poisoning. Cardiopulmonary resuscitation (CPR) was not includedbecause guidelines are already available from the European Resuscitation Council(ERC). The FA guidelines are intended to provide guidance to authors of FA handbooksand those responsible for FA programmes. These guidelines, together with the ERCresuscitation guidelines, will be integrated into a European FA Reference Guide anda European FA Manual.
q A Spanish translated version of the summary of this article appears as Appendix in the final online version atdoi:10.1016/j.resuscitation.2006.10.023
qq Guidelines are not a substitute for the caregiver’s own judgment of a specific medical or health condition. Casualties shouldconsult a qualified healthcare professional for advice about a specific condition. The authors disclaim any liability to any party forany damages arising out of the use or nonuse of this material and any information contained therein, and all warranties, expressedor implied.∗ Corresponding author. Tel.: +32 15 44 34 76.
Email address: [email protected] (S. Van de Velde).
03009572/$ — see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2006.10.023
14

European first aid guidelines 241
Methods: To create these guidelines we used an evidencebased guideline development process, based on the methodology of the Scottish Intercollegiate GuidelinesNetwork (SIGN).Results: The recommendations cover FA for bleeding, wounds, burns, spinal and headtrauma, musculoskeletal trauma, and poisoning, as well as safety and psychosocial FA.Conclusions: Where good evidence was available, we were able to turn science intopractice. Where evidence was lacking, the recommendations were consensusbased.These guidelines provide systematically developed recommendations and justifications for the procedures and techniques that should be included in FA manuals andtraining programmes.© 2006 Elsevier Ireland Ltd. All rights reserved.
Introduction
Every year, thousands of people experience orwitness medical emergencies. When emergenciesoccur, family members, friends, colleagues, orbystanders often provide spontaneous help.1—3
Citizens can take safety precautions and helpothers until professional help arrives. First aid(FA) training is essential in preparing the general public for an initial response to suchsituations.
To improve the outcome of the casualty, firstaiders must be taught correctly; they must be giventraining in the right things. Incorrect training canresult in inadequate, even harmful, interventions.The procedures and techniques taught to the publicvary between European countries, but these differences cannot always be justified. Recently, theAmerican Heart Association published guidelinesfor resuscitation and FA,4 the European guidelines that were published at the same time onlycovered resuscitation.5 European FA guidelines,which incorporate research and expert opinion systematically and transparently, therefore are muchneeded.
Belgian Red CrossFlanders initiated a project todetermine the most effective, safe, and feasibleFA techniques and procedures, and to formulatevalid recommendations. This project received support from the European Commission. The guidelinescover emergencies involving few casualties, whereemergency medical services (EMS) or healthcareprofessionals are not present at the scene immediately, but are available within a short space oftime. Due to time and resource constraints, welimited ourselves to safety, emergency removal,psychosocial FA, traumatology, and poisoning. Cardiopulmonary resuscitation (CPR) is not included,because guidelines5 are already available from theEuropean Resuscitation Council (ERC).
We define FA as ‘immediate help provided to asick or injured person’. FA consists of proceduresand techniques, requiring minimal or no equip
ment, that can be taught to the general public inbasic FA courses. FA is not only concerned with thetreatment of physical injury but also with providingother initial care to the individual, including psychosocial FA—–assistance given to people sufferingemotional distress caused by experiencing or witnessing a stressful event. A first aider is defined asa layperson trained in FA.
These guidelines have been designed to provideguidance to authors of FA handbooks and thoseresponsible for FA programmes. They are intendedto be a blueprint for local training programmes andto increase the usefulness, quality, impact, andharmonisation of training. This will improve boththe quality of FA provided and the outcome for thecasualty.
Together with the resuscitation guidelines ofthe ERC, these guidelines will be bundled intothe European Reference Guide for FA Instruction.This Reference Guide should be a helpful toolfor the dissemination of the guidelines throughoutEurope. To implement the new guidelines simplyand efficiently across Europe, we produced EFAMor European FA Manual. EFAM collates all the newguidelines for first aid and resuscitation into oneunique tool to update teaching material. It offersreadytouse digital texts and high quality photos ofall the latest techniques. The Reference Guide andEFAM can be requested from the European First AidManual website http://www.efam.be.
Methodology
The guideline development process was based onthe methodology of the Scottish IntercollegiateGuidelines Network (SIGN).6 This is a recognisedreference for the development of guidelines.7
Guideline Development Group
When composing the Guideline DevelopmentGroup, we ensured participation from all relevant
15
svelde
Rechthoek

242 S. Van de Velde et al.
key groups and disciplines. The group consisted ofEuropean specialists in anaesthesiology, cardiology,traumatology, emergency medicine, disaster management, psychosocial care, medical education,and FA training. The director of the Belgian branchof the Cochrane Collaboration, i.e. the BelgianCentre for EvidenceBased Medicine (CEBAM), gaveadvice on methodology. The experts who conductedthe systematic literature review participated intraining in evidencebased medicine.
Literature search and data sources
The objective of the search was to find all relevant studies using sensitive search strategies. Aninitial search was performed for guidelines and systematic reviews (SR) in the Cochrane Database ofSystematic Reviews, the Guidelines InternationalNetwork database, the Health Evidence Network,the National Guideline Clearinghouse, the NationalElectronic Library for Health Guidelines Finder, andPubmed. A subsequent search for other studies wascarried out using Pubmed, Embase, and the Webof Science. Where eligible guidelines or SRs werefound, the subsequent search focussed on studies published thereafter, up to December 2005.Hand searching and checking the reference listsof selected studies enabled the inclusion of studies that were not retrieved in the initial search.The detailed search strategy is available uponrequest.
Selection of studies
Inclusion and exclusion criteria were defined beforethe selection procedure. There were no languagerestrictions or limits on study design. Studies wereselected from the titles and abstracts of all theretrieved references. Full texts were then screenedand irrelevant studies were excluded.
Quality assessment
All the selected studies were evaluated for methodological quality using checklists. We used theAGREE instrument8 from the AGREE Collaborationfor assessing guidelines, and the SIGN checklist forreviewing SRs, randomised controlled trials (RCT),and cohort and case—control studies. We developedadditional checklists for other study designs.
Data extraction
The data from valid studies were tabulated in evidence tables and summarized by level of evidence.Evidence statements and recommendations were
formulated at a conference held in Riga, Latvia,in February 2006. If no relevant research evidencewas found, recommendations were based on a consensus of what was considered good practice. Foreach recommended FA technique or procedure, weassessed the effectiveness, safety, and feasibility. In accordance with the SIGN grading system6
(Figure 1), our recommendations are graded fromA to D. These grades match the strength of thesupporting evidence, ranging from LOE 1 to 4.Where evidence was unavailable, the recommendation is based on a consensus of the GuidelineDevelopment Group as to what constitutes goodpractice.
Validation
External reviewers, including medical specialists,experts in psychosocial care, training managers,and trainers, made an initial assessment of eachguideline statement. They gave feedback on scope,quality, clarity, and usefulness. The GuidelineDevelopment Group then considered the responses.An independent expert committee, following theCEBAM external validation procedure, officially validated the final guidelines.
Evidence
Table 1 shows the number of studies identified,included, and excluded. In total we selected88 studies to support our recommendations. TheAmerican FA guidelines4 were included under multiple topics, thus explaining why ‘total included’ inTable 1 amounts to 93 rather than 88.
We included 23 guidelines, 5 SRs, 2 RCTs,1 cohort study, 14 case reports or series, 2crosssectional surveys, and 41 miscellaneousmanuscripts (narrative reviews, letters, comments,etc.). Five guidelines contained specific recommendations for FA.4,9—12 The other guidelines werefor use by healthcare professionals, but extrapolation to FA recommendations was possible. Twelveguidelines4,10,12—21 used systematic and transparent methods for integrating research evidence,two guidelines9,11 were based on expert consensus, and for nine guidelines22—30 we couldnot retrace what method was used. Eight guidelines included grades of recommendation. Whenappropriate guidelines or SRs were found, wefocussed the subsequent search on later publications, up to December 2005. This was thecase for psychosocial FA, wounds, burns, spinaland head trauma, musculoskeletal trauma, andpoisoning.
16
svelde
Rechthoek

European first aid guidelines 243
Figure 1 SIGN grading system.6
Safety measures
Findings
We included eight studies on road accidents,31—38
two on fire,39,40 and seven on electricalaccidents.40—46 Except for one crosssectionalsurvey on fire safety (LOE 339), all the selectedstudies on safety measures are expert opiniondocuments (LOE 4). As to road accidents, there isdebate among specialists whether parking the carbefore or after the accident is important.
Recommendations (Grade D)
General principlesAlways make personal safety your first priority.Check the situation and identify any potential dan
ger. Only approach the scene if it is safe foryou to do so. If possible, try to ensure safetyfor the casualty and bystanders. If it is unsafefor you to approach the casualty, alert the emergency services and wait at a safe distance for theirarrival.
Road accidentAlways act according to local laws.
When approaching a road accident, reduce speedand avoid sudden braking. Park your car in asafe place, off the road or at the side of theroad. Wear high visibility clothing. Use warning signs (e.g. warning triangle) to alert passingtraffic. Do not run across busy travel lanes onmotorways.
Identify any downed electrical cables and ensurethat nobody touches or approaches them.
17
svelde
Rechthoek

244 S. Van de Velde et al.
Tab
le1
Resu
lts
of
identi
fica
tion
and
sele
ctio
nof
studie
s
Safe
tyPsy
choso
cial
FAW
ounds
Ble
edin
gB
urn
sSp
inal,
head
traum
aM
usc
ulo
skele
tal
traum
aPois
onin
g
Incl
uded
guid
eli
nes
23
61
61
45
Incl
uded
SRs
01
12
00
10
Oth
er
pote
nti
all
yre
leva
nt
studie
s657
59
a463
a397
155
a40
a144
a28
a
Exc
luded
on
conte
nt/
quali
ty−
635
−51
−457
−358
−134
−35
−143
−26
Unlo
cata
ble
studie
s−
5−
1−
6−
12
−16
−3
−1
0O
ther
incl
uded
studie
s17
70
27
52
02
Tota
lno.
of
studie
sin
cluded
19
11
730
11
35
7
aIf
eli
gible
guid
eli
nes
or
SRs
were
found,
ati
me
lim
itw
as
use
dfo
roth
er
studie
s.
Prevent fire by switching off the ignition of vehicles involved in the accident, and ensuring thatnobody smokes. Be aware of the danger of airbags.If possible, apply the handbrake to stabilise thevehicles involved.
Fire at homeTry to warn everybody at risk without putting yourself at risk. Do not enter a burning house. Moveaway from the area to a safe distance. If you arein a burning building, leave the area immediatelyand help other people to leave, provided you cando this safely.
Electrical accident at homeConsider electrical devices and cables as ‘live’until proven to be disconnected. Do not touch acasualty connected to a power source. Remember that liquids or objects in contact with thecasualty can potentially conduct electricity. Switchoff the current. If it is not possible to disconnect the power, stand on insulating materialand push the power source away using nonconductive material. If this is not feasible, waitfor the fire brigade or specialised personnel toarrive.
Emergency removal of the casualty
Findings
Three expert opinion manuscripts are included onemergency removal of the casualty (LOE 44,23,47).There is no evidence on which technique of movinga casualty is best.
Recommendations (Grade D)
As a general rule, do not move a casualty fromthe scene of the accident. Only move a casualtyif he or she is in uncontrollable danger, and ifit is safe for you to do so. In that case movethe casualty to the nearest place of safety. Tryto shield the casualty from cold or heat, but onlymove a casualty if he or she has been exposedto cold for a long time. Explain to a consciouscasualty what you are going to do and ask forhis or her cooperation. Use a technique thatis safe for you and the casualty, is easily andquickly applied, without the need for special equipment. If possible, support the neck and avoidtwisting the head, neck, and body during the procedure.
18
svelde
Rechthoek

European first aid guidelines 245
Initial evaluation and calling for help
Findings
The recommendations below are based on a consensus of the Guideline Development Group as towhat constitutes good practice.
Recommendations (Grade D)
Introduce yourself and explain what you are goingto do. This will increase the casualty’s confidencein you. Evaluate the casualty’s condition. If help isneeded, alert the EMS or local emergency responsesystem, the Poison Control Centre (PCC) or otherhealthcare professionals as appropriate. Remember that 112 is the recognised emergency telephonenumber in all countries of the European Union.Always refer to healthcare professionals or socialservices if you have any suspicion of nonaccidentalinjury.
Psychosocial first aid
Findings
The focus of the literature tends to be onthe first weeks after an incident has occurred.Three guidelines on acute and post traumaticstress disorder,13,14,22 one systematic review ondebriefing,48 and seven expert opinion scripts49—55
were selected. Single session debriefing or activelyexploring emotions should not be done (LOE1+,14,48 LOE 413,22,49,53); this has proven tobe ineffective and potentially harmful. Singlesession debriefing is a psychological techniquefor a structured conversation about emotionaland cognitive experiences. Laypersons providing initial psychosocial support need continuoustraining and assistance (LOE 451,54). Taking careof basic needs is part of psychosocial FA, butfood or drink should not be given because thiscomplicates professional care if anaesthesia isrequired.
Recommendations (Grade D)
Approach the casualty in a nonjudgmental way. Listen empathetically to the casualty, be supportive,and offer practical assistance. Do not give food ordrink to a sick or injured casualty, unless advisedotherwise by professional healthcare providers.Explain carefully to the casualty what has happenedand what is going to happen.
Infection control
Findings
We included three guidelines related to infectioncontrol.11,15,30 Crossinfection between first aiderand casualty must be avoided. Hand hygiene, byusing liquid soap and water, is an effective methodof preventing crossinfection (LOE 1+,15 LOE 430).The risk of crossinfection can be reduced by using abarrier (e.g. gloves) between the first aider and theblood or body fluids of the casualty (LOE 411,15,30).Careful handling and disposal of glass, needles, orother sharp objects that might cut, graze, or prickis essential in preventing infection (LOE 415,30).
Recommendations (Grades B and D)
Whenever possible, wash your hands with liquidsoap and water before and after giving FA (B). Usedisposable gloves if they are available (D); if not,a plastic bag may be used instead (D). Handle anddispose of sharp objects safely (D). If needles arepresent as a result of recreational drug use, thenthey should be identified and left to professionalsto handle (D).
Bleeding
Findings
One guideline,4 2 SRs on control of arterial puncture56 and on femoral vessel injuriesin warfare,57 2 RCTs on control of arterialpuncture,58,59 11 case reports or series,60—70 and14 expert opinion scripts71—84 were selected.The effectiveness of controlling external bleedingthrough applying direct pressure or a compression bandage to the site of bleeding is provenby high level of evidence (LOE 1+,4,56,58,59
LOE 3,61,62,65,67,68 LOE 44,71—78,80—83). There isinsufficient evidence about the effectiveness ofindirect pressure on pressure points and elevation (LOE 44,72,74—76,80—82). Because of the possiblecomplications, the use of a tourniquet is contraindicated for laypersons (LOE 360,63—66,68—70,LOE 44,57,72,75,76,79,80,82,84).
Recommendations (Grades B and D)
To control external bleeding, apply direct pressureor a compression bandage to the site of bleeding(B). If bleeding continues, apply more pressure oran additional bandage without removing the original dressing (D). Maintain pressure on the site of the
19
svelde
Rechthoek

246 S. Van de Velde et al.
wound until the EMS arrives (D). Do not use indirectpressure on pressure points and elevation, and donot use a tourniquet to control bleeding (D).
Wounds
Findings
Three guidelines on wound management4,12,20 andone SR on water for wound cleansing85 wereselected. Irrigating wounds with water reducesinfection rates and improves healing rate (LOE1+85). Irrigation should be continued until thereappears to be no foreign matter left in the wound(LOE 44). Swabbing the wound can damage thewound tissue (LOE 420). There is debate amongstresearchers as to whether the potential toxiceffects of antiseptics and antibacterials on tissue may delay the healing of wounds; therefore,at present, use of antiseptics and antibacterialsshould be undertaken with caution (LOE 412,20).Wound dressings are necessary to protect thewound (LOE 420). Tetanus immunisation is neededfor all wounds.12 Many people do not know theirexact immunisation status. One guideline includedcriteria for referral to healthcare professionals.12
Recommendations (Grades B and D)
After controlling bleeding, irrigate wounds withclean, running, cold, tap water if available (B); ifnot, use any source of drinkable water (B). Irrigate directly on the wound and continue until thereappears to be no foreign matter left in the wound(D). Do not swab a wound (D). After cleaning awound, cover it with sterile gauze if available (B);if not, use a clean dry cloth (D). Advise the casualty to seek medical advice to determine his/hertetanus immunisation status (D).
Do not remove an object that is embedded in awound (D). Instead, try to immobilise it (D), thencover the wound with sterile gauze if available, ora clean dry cloth (D).
Referral to healthcare professionals is indicatedif (D):
• an object is embedded in the wound;• there is uncontrollable bleeding;• an abrasion is larger than half the width of the
palm of the casualty;• bone, muscle, or other subcutaneous tissue is
exposed;• a wound involves the face, eyes, or genital area;• a wound cannot be cleaned properly;• a wound is caused by a bite.
Try to control bleeding until professional help is athand.
Burns
Findings
We included six guidelines,4,9,10,16,17,24 two casereports or series,86,87 one crosssectional survey,88
and two expert opinion scripts89,90 on burns management. Burns should be cooled as soon aspossible with tapwater (LOE 2++,4 LOE 3,86—88 LOE49,16,24,90). For some types of chemical burns, rinsing with water is potentially harmful (LOE 49).The incidence of such burns, in a nonoccupationalsetting, is low. This recommendation should, therefore, apply to both types of burn to allow uniformand simple guidelines for first aiders. The evidencefor the optimum length of time a burn should becooled is inconclusive (LOE 387,88, LOE 44,9,16,89).When cooling, hypothermia in the casualty mustbe prevented (LOE 3,86—88 LOE 44,9,89). Clothingand jewellery can be removed, if they are notadhering to the skin (LOE 3,86,88 LOE 49,24,89,90).Intact burn blisters should not be opened (LOE 3,4
LOE 490). Antibiotic creams should not be used asFA.10 Wet wound dressings can protect the burn(LOE 3,88 LOE 49,10,24,89,90). Tetanus immunisationis needed for burns.10,16 Many people do not knowtheir exact immunisation status. Four guidelines(LOE 410,16,17,24) included criteria for referral tohealthcare professionals. The extent of a burncan be assessed with the Rule of Nines, the Lundand Browder chart, or with the palm of the casualty’s hand (LOE 410,16). The palm and fingers ofthe casualty’s hand is approximately 1% of theirtotal body surface area. There is no consensusin the research on the best method. The Rule ofNines should not be used for children under 16years old. Using the casualty’s hand is a feasiblemethod for estimating the size of a burn at thescene.
Recommendations (Grades B and D)
Cool burns as soon as possible with tapwater (B).Continue cooling for 15—20 min or until pain relief isachieved or until professional help arrives (D). Prevent hypothermia in the casualty by avoiding useof very cold water for cooling, protecting casualties from the wind, and using blankets to keep thecasualty warm (D). Remove clothing and jewelleryif they are not adhering to the skin (D). After cooling, apply wet wound dressings (D). Do not openintact burn blisters (D). Advise the casualty to seek
20
svelde
Rechthoek

European first aid guidelines 247
medical advice to determine his/her tetanus immunisation status (D).
Referral to healthcare professionals is indicatedif (D):
• the casualty is a child under 5 years or an adultover 60 years;
• a burn involves face, ears, hands, feet, the genital area, or joints;
• there is a circumferential burn of the limbs,torso, or neck;
• there are burns covering more than 5% of totalbody surface area in children under 16 years,or more than 10% in adults over 16 years. Thepalm and fingers of the casualty’s hand is approximately 1% of the total body surface area;
• there is a thirddegree burn. If the deepest layerof the skin is burned, there is usually no painin the wound itself, because the nerves in thisarea have also been destroyed. The burn can lookblack, parchmentlike or white and is dry. However the skin around the wound, which is oftenless deeply burned, is painful;
• burns are electrical or chemical, or due to ionizing radiation, or high pressure steam;
• there is an inhalation burn.
Spinal and head trauma
Findings
One guideline on head trauma,21 one cohort study91
and one case series92 on spinal trauma wereselected. Assessment of spinal or head trauma isdifficult; in children this is even more difficult. Allthree studies provide criteria for referral to healthcare professionals (LOE 2++,21,91 LOE 392). Thereis no good evidence about when first aiders shouldexpect head injury in children. There is no evidencethat manual immobilisation in a nonmoving victimis effective.
Recommendations (Grades B and D)
Initial evaluation of casualties who have an alteredmental state, or who are intoxicated or in greatpain is not very reliable. Alert the EMS if there isuncertainty about the nature of any injury (B).
Suspect head injury and alert the EMS if the casualty (B):
• is a victim of highimpact trauma such as from atraffic accident or a fall from higher than standingheight;
• is or becomes drowsy, sleepy, agitated, or unconscious;
• does not remember precisely what has happened;• has severe and persistent headache, nausea
and vomiting, irritability, or altered behaviour,seizure;
• has major lesions to the head.
Suspect spinal injury and alert the EMS if thecasualty (B):
• is a victim of high impact trauma such as from atraffic accident, or a fall from higher than standing height;
• is or becomes drowsy, sleepy, agitated, or unconscious;
• does not remember precisely what has happened;• complains about numbness or tingling;• is not complaining about serious injuries of the
lower body or legs that would normally beexpected to be painful;
• has pain or tenderness in the neck or back.
Calm a casualty with spinal or head trauma andtry to convince him/her not to move (D). Onlyimmobilise the casualty if he or she is cooperative(D). If the casualty is agitated, do not immobilisethe head and neck against his/her will (D).
Musculoskeletal trauma
Findings
Four guidelines4,18,25,26 on musculoskeletal traumaand one SR93 about the use of ice in acute softtissue injury were selected. Initial evaluation oflimb injuries is difficult. Evidence is inconclusiveon the effectiveness of immediate postinjury cooling (LOE 1+4,18,93), and on the optimum duration ofcooling (LOE 1+93). No evidence was found aboutthe effectiveness of elevation and compression.Avoiding standing on an injured lower limb (LOE 44),or self immobilisation of an injured upper limb (LOE425,26), are often adequate and less painful thanputting the limb in a bandage or a sling.
Recommendations (Grade D)
In case of doubt about the severity, assume thata fracture has occurred and refer to healthcareprofessionals. Do not try to reduce angulated ordislocated limbs. Cool the injury with ice. Whencooling, use a barrier such as a towel between theice and the skin and do not use for a prolongedtime. Limit each period of cold application to amaximum of 20 min. Do not immobilise the injuredlimb if medical help is available within a short timespan. Advise the casualty not to stand on an injured
21
svelde
Rechthoek

248 S. Van de Velde et al.
lower limb. In case of upper limb injury, ask thecasualty to immobilise the arm against the trunkhimself/herself. If there is major bleeding at thefracture site, apply direct pressure or a compression bandage.
Poisoning through oral ingestion
Findings
Five guidelines4,19,27—29 and two expert opinionscripts94,95 were selected. Activated charcoal (LOE44,27,29,94), water, or milk (LOE 44,94) should onlybe used if this is advised by a PCC or a professional healthcare provider. Ipecac syrup should notbe used (LOE 1+,4 LOE 3,19 LOE 427,28,28,94,95). Wedid not investigate whether body position has aneffect on poison absorption. Future investigationis needed to test the hypothesis that left lateraldecubitus decreases absorption.
Recommendations (Grade D)
Contact the PCC or professional healthcareproviders and follow their instructions.
Discussion
There was limited evidence addressing FA. It wassometimes possible to extrapolate research findingson professional healthcare to FA; the 21 guidelines retrieved were very useful for this purpose.When evidence was available, we were able toturn science into practice. When evidence wasnot available, our recommendations are consensusbased. Effective and appropriate FA proceduresand techniques have been described, and interventions that are contraindicated have been identified.Even though the evidence base was limited, theseguidelines provide systematically developed recommendations and justifications for the proceduresand techniques that should be included in FA manuals and training programmes.
Customary practices are not always correct. Ifresearch shows that first aid can become better,one should not be blind to that fact. It is stronglyadvised that FA manuals and programmes bereviewed in the light of these guidelines and revisedwhere appropriate. The European Reference Guidefor FA Instruction and EFAM are handy tools toupdate or develop teaching material and can berequested at the website http://www.efam.be.
Until now, there has been no explicit description of the status of research on FA. This studyillustrates the need for more research which isnecessary to ensure the quality of FA provision.Specifically, research is required on how well firstaiders can perform immobilisation techniques, andon the optimum duration of irrigation for burns andcooling after musculoskeletal trauma.
We hope these guidelines will encourage the scientific community to start new research effortsin FA. As new evidence becomes available, theseguidelines will need to be revised. A strategy mustbe developed to bring in wider European representation and to include additional basic and advancedFA topics when these guidelines are updated.
Contributors
The Belgian Red CrossFlanders is very grateful forthe work that has been done by the participatingexperts. S. Van de Velde, (Belgian Red CrossFlanders) planned, coordinated, facilitated anddrafted the study report. P. Broos (University Hospital Gasthuisberg Leuven, Belgium) supervised thestudy and chaired the expert group. B. Aertgeerts(Belgian Centre for EvidenceBased Medicine) gavemethodological advice. The systematic literaturereview was done by: R. De Win (Belgian Red CrossFlanders), D. Lauwaert (Academic Hospital FreeUniversity Brussels, Belgium), A. Sermon (University Hospital Gasthuisberg Leuven, Belgium), C.Tobback (Poison Control Centre Belgium), M. VanBouwelen (Belgian Red CrossFlanders), P. Van denSteene (Stressteam Federal Police Belgium), A. vanTichelen (SaintMarie Hospital Halle, Belgium), B.Vantroyen (University Hospital Gasthuisberg Leuven, Belgium), J. Verduyckt (University HospitalGasthuisberg Leuven, Belgium). Advisors on specialist topics were: J. Bierens (VU University MedicalCentre Amsterdam, Netherlands), P. Broos, P. Cassan (European Reference Centre for First AidEducation, France), E. Davoli (World Health Organisation), M. De Vries (Impact Foundation, DutchKnowledge Centre for PostDisaster PsychosocialCare), G. Gobl (Hungarian Red Cross), G. Lo (International Federation of the Red Cross and RedCrescent Societies, IFRC), C. Urkia Mieres (SpanishRed Cross), K. Monsieurs (European ResuscitationCouncil), M. Sabbe (University Hospital Gasthuisberg Leuven, Belgium), S. Schunder (Austrian RedCross), and S. Villere (Latvian Red Cross). Externalvalidators were D. Ramaekers (Belgian Health CareKnowledge Centre), H. Van Brabant (Belgian HealthCare Knowledge Centre) and P. Vranckx (Virga JesseHospital Hasselt, Belgium).
22
svelde
Rechthoek

European first aid guidelines 249
Conflict of interest statement
The Red Cross provides training in first aid.
Acknowledgements
We are grateful to the IFRC for their permission tocite from the First recommendations on lifesavingtechniques report.11 We thank A. Handley (Colchester, UK) for reviewing and editing the manuscript.
Funding: The European Commission funded thisstudy. The Commission did not participate in theguideline development process and is not responsible for any use that may be made of the informationin this publication.
References
1. Mauritz W, Pelinka LE, Kaff A, Segall B, Fridrich P. Firstaid measures by bystanders at the place of accident. Aprospective, epidemiologic study in the Vienna area. WienKlin Wochenschr 2003;115:698—704.
2. Larsson EM, Martensson NL, Alexanderson KA. Firstaid training and bystander actions at traffic crashes—–a populationstudy. Prehospital Disaster Med 2002;17:134—41.
3. Abernethy L, MacAuley D, McNally O, McCann S. Immediatecare of school sport injury. Inj Prev 2003;9:270—3.
4. American Heart Association Guidelines for CardiopulmonaryResuscitation and Emergency Cardiovascular Care. Circulation 2005;112:IV1—IV203.
5. Handley AJ, Koster R, Monsieurs K, Perkins GD, DaviesS, Bossaert L. European Resuscitation Council guidelinesfor resuscitation 2005. Section 2. Adult basic life supportand use of automated external defibrillators. Resuscitation2005;67:S7—S23.
6. Scottish Intercollegiate Guidelines Network. SIGN 50: Aguideline developer’s handbook. Edinburgh: SIGN; 2004.Available from: http://www.sign.ac.uk/guidelines.
7. Atkins D, et al. Systems for grading the quality of evidenceand the strength of recommendations. I. Critical appraisalof existing approaches. BMC Health Serv Res 2004;4:38.
8. The AGREE Collaboration. Appraisal of Guidelines forResearch & Evaluation (AGREE) Instrument. The AGREE Collaboration; 2001. Available from: http://www.agreecollaboration.org.
9. Allison K, Porter K. Consensus on the prehospital approach toburns patient management. Emerg Med J 2004;21(1):112—4.
10. Sowerby Centre for Health Informatics at Newcastle (SCHIN).Prodigy Guidance: burns and scalds. Prodigy Guidance; 2004.Available from: http://www.prodigy.nhs.uk.
11. International harmonization of First Aid. First recommendations on lifesaving techniques. International Federation ofRed Cross and Red Crescent Societies; 2004.
12. Sowerby Centre for Health Informatics at Newcastle (SCHIN).Prodigy Guidance: lacerations. Prodigy Guidance; 2004.Available from: http://www.prodigy.nhs.uk.
13. Ursano RJ, Bell C, Eth S, et al. Practice guideline for thetreatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161:3—31.
14. National Collaborating Centre for Mental Health. Post traumatic stress disorder: the management of PTSD in adults
and children in primary and secondary care. London (UK):National Institute for Clinical Excellence (NICE); 2005. Available from: http://www.guideline.gov.
15. National Collaborating Centre for Nursing, Supportive Care.Infection control. Prevention of healthcareassociated infection in primary and community care. London (UK): NationalInstitute for Clinical Excellence (NICE); 2003. Available from:http://www.nice.org.uk.
16. American Burn Association. Practice guidelines for burn care.J Burn Care Rehabil 2001;22:19s—26s.
17. National Burn Care Review Committee. National burn carereview. British Association of Plastic Surgeons; 2001. Available from: http://www.baps.co.uk.
18. van Dijk CN. CBOguideline for diagnosis and treatment of the acute ankle injury. National organizationfor quality assurance in hospitals. Ned Tijdschr Geneeskd1999;143:2097—101.
19. Manoguerra AS, Cobaugh DJ. Guideline on the use of ipecacsyrup in the outofhospital management of ingested poisons. Clin Toxicol 2005;43:1—10.
20. Crest. Guidelines on the general principles of caringfor patients with wounds. Belfast: Clinical Resource Efficiency Support Team; 1998. Available from: http://www.crestni.org.uk.
21. Scottish Intercollegiate Guidelines Network. SIGN 46: Earlymanagement of patients with a head injury. Edinburgh: SIGN;2000. Available from: http://www.sign.ac.uk/guidelines.
22. Gray MJ, Litz BT. Behavioral interventions for recenttrauma: empirically informed practice guidelines. BehavModif 2005;29:189—215.
23. Joint Royal Colleges Ambulance Liaison Committee(JRCALC). Street safety. Emergency Care Specialist Library,Joint Royal Colleges Ambulance Liaison Committee; 2004.Available from: http://www.library.nhs.uk/emergency.
24. Joint Royal Colleges Ambulance Liaison Committee(JRCALC). Burns. Emergency Care Specialist Library, JointRoyal Colleges Ambulance Liaison Committee; 2004.Available from: http://www.library.nhs.uk/emergency.
25. Joint Royal Colleges Ambulance Liaison Committee(JRCALC). Limb trauma. Emergency Care Specialist Library,Joint Royal Colleges Ambulance Liaison Committee; 2004.Available from: http://www.library.nhs.uk/emergency.
26. Joint Royal Colleges Ambulance Liaison Committee(JRCALC). Splintage. Emergency Care Specialist Library,Joint Royal Colleges Ambulance Liaison Committee; 2004.Available from: http://www.library.nhs.uk/emergency.
27. American Academy of Pediatrics Committee on Injury, Violence, Poison Prevention. Poison treatment in the home.Pediatrics 2003;112:1182—5.
28. American Academy of Clinical Toxicology, European Association of Poisons Centres and Clinical Toxicologists. Positionpaper: Ipecac syrup. J Toxicol Clin Toxicol 2004;42:133—43.
29. Chyka PA, Seger D, Krenzelok EP, Vale JA. Position paper:singledose activated charcoal. Clin Toxicol 2005;43:61—87.
30. Joint Royal Colleges Ambulance Liaison Committee(JRCALC). Infection control. Emergency Care SpecialistLibrary, Joint Royal Colleges Ambulance Liaison Committee; 2004. Available from: http://www.library.nhs.uk/emergency.
31. Coats TJ, Davies G. Prehospital care for road traffic casualties. Br Med J 2002;324:1135—8.
32. Meade DM, Dernocoeur K. Principles of emergency vehicleplacement. Emerg Med Serv 1998;27:34—5.
33. Czajkowski J, Kidd S. Extrication challenges. 10 tips for EMScrews working at extrication scenes. EMS on scene. JEMS2001;26:50—61.
23
svelde
Rechthoek

250 S. Van de Velde et al.
34. Meola JJ. Fresh ideas for keeping crews safe. Occup HealthSaf 2000;69(38—42):44.
35. Methner P. Extrication scene tips for EMS personnel: EMS considerations to enhance scene operations and personal safety.JEMS 2004;29:28—35.
36. Moore JE, Giuliano G, Cho S. Secondary accident rates on LosAngeles freeways. J Transport Eng ASCE 2004;130:280—5.
37. Platt WD. Behaviour at the scene of an accident. Br J Nurs1992;1:678—80.
38. Stack JK. Immediate measures at site of accident. J Trauma1966;6:285—98.
39. Jaslow D, Ufberg J, Yoon R, McQueen C, Zecher D,Jakubowski G. Fire safety knowledge and practices of theelderly. Emerg Med Serv 2004;33:111—5.
40. Chamberlain A. First aid in chemical environments. Chem Br1983;19:318—23.
41. First aid series. Electrocution. Nurs Times 1999;95:49.42. Clave M. Accidents due to electricity. Rev Infirm
1980;30:33—9.43. Erskine JF. Electrical accidents. Practitioner 1979;222:
777—81.44. Lederer W, Wiedermann FJ, Cerchiari E, Baubin MA.
Electricityassociated injuries. I. Outdoor management ofcurrentinduced casualties. Resuscitation 1999;43:69—77.
45. Pedersen EB. Safety at disaster sites. Aust Fam Physician1978;7, 25—7, 29.
46. Zorn H. First aid in electric injuries. Zentralbl ArbeitsmedArbeitsschutz Prophyl 1976;26:180—8.
47. Doering JJ. Emergency lift for the immobile elderly. CanNurse 2002;98:31—5.
48. Rose S, Bisson J, Churchill R, Wessely S. Psychologicaldebriefing for preventing post traumatic stress disorder(PTSD). Cochrane Database Syst Rev 2005.
49. Bryant RA. Psychosocial approaches of acute stress reactions. CNS Spectr 2005;10:116—22.
50. Kutz I, Bleich A. Mental health interventions in a generalhospital following terrorist attacks: the Israeli experience. JAggr Maltreat Trauma 2005;10:425—37.
51. Pardess E. Training and mobilizing volunteers for emergencyresponse and longterm support. J Aggr Maltreat Trauma2005;10:609—20.
52. Resnick H, Acierno R, Kilpatrick DG, Holmes M. Description of an early intervention to prevent substance abuseand psychopathology in recent rape victims. Behav Modif2005;29:156—88.
53. Schnyder U. Psychotherapies for PTSD—–an overview. Psychotherapies 2005;25:39—52.
54. Van Ommeren M, Saxena S, Saraceno B. Mental and socialhealth during and after acute emergencies: emerging consensus? Bull World Health Org 2005;83:71—5.
55. Watson PJ, Shalev AY. Assessment and treatment of adultacute responses to traumatic stress following mass traumaticevents. CNS Spectr 2005;10:123—31.
56. Koreny M, Riedmuller E, Nikfardjam M, Siostrzonek P, MullnerM. Arterial puncture closing devices compared with standardmanual compression after cardiac catheterization: systematic review and metaanalysis. JAMA 2004;291:350—7.
57. Pearl JP, McNally MP, Perdue PW. Femoral vesselinjuries in modern warfare since Vietnam. MilitaryMed 2003;168:733—5.
58. Lehmann KG, HeathLange SJ, Ferris ST. Randomizedcomparison of hemostasis techniques after invasive cardiovascular procedures. Am Heart J 1999;138:1118—25.
59. Walker SB, Cleary S, Higgins M. Comparison of the FemoStopdevice and manual pressure in reducing groin puncture sitecomplications following coronary angioplasty and coronarystent placement. Int J Nurs Pract 2001;7:366—75.
60. Lakstein D, Blumenfeld A, Sokolov T, et al. Tourniquetsfor hemorrhage control on the battlefield: a 4year accumulated experience. J Trauma Injury Infect Crit Care2003;54:S221—5.
61. Naimer SA, Nash M, Niv A, Lapid O. Control of massive bleeding from facial gunshot wound with a compactelastic adhesive compression dressing. Am J Emerg Med2004;22:586—8.
62. Gadzhiev NA, Kosenkov AN. Organization of treating patientswith major vessel injuries at stages of evacuation. Khirurgiia2003;6:22—7.
63. Pilcher DB, Gettinger Jr CE, Seligson D. Recurrent themesin ambulance critique review sessions over eight years. JTrauma 1979;195:324—8.
64. Bouma S. First aid in hemorrhages, the use of tourniquets.Ned Tijdschr Geneeskd 1966;110:1255—7.
65. Dorlac WC, DeBakey ME, Holcomb JB, et al. Mortality fromisolated civilian penetrating extremity injury. J TraumaInjury Infect Crit Care 2005;59:217—22.
66. Calkins D, Snow C, Costello M, Bentley TB. Evaluation ofpossible battlefield tourniquet systems for the farforwardsetting. Military Med 2000;165:379—84.
67. Pohlemann T, Paul C, Gansslen A, Regel G, Tscherne H.Traumatic hemipelvectomy. Experiences with 11 cases.Unfallchirurg 1996;99:304—12.
68. Fasol R, Irvine S, Zilla P. Vascular injuries caused by antipersonnel mines. J Cardiovasc Surg 1989;30:467—72.
69. Kornbluth ID, Freedman MK, Sher L, Frederick RW. Femoral,saphenous nerve palsy after tourniquet use: a case report.Arch Phys Med Rehabil 2003;84:909—11.
70. Savvidis E, Parsch K. Prolonged transitory paralysis afterpneumatic tourniquet use on the upper arm. Unfallchirurg1999;102:141—4.
71. Beck A, Gebhard F, Kinzl L, Strecker W. Principles and techniques of accident surgery primary care at the accident site.Unfallchirurg 2001;104:1082—99.
72. Boericke PH, Boericke CH. Emergency! Part 2. First aid foropen wounds, severe bleeding, shock, and closed wounds.Nursing 1975;5:40—6.
73. Broos PL, Willaert WI. Notorious pitfalls in the care of multitrauma patients. Acta Chir Belg 2003;103:346—54.
74. Clifford CC. Treating traumatic bleeding in a combat setting.Mil Med 2004;169(8—10):4.
75. Donelan S. Teaching wound care and bandaging: an historicalperspective. Wilderness Environ Med 2003;14:47—56.
76. Dunant JH. Emergency treatment of hemorrhage. TherUmsch 1979;36:1059—61.
77. Garner JP, Brown RFR. Recent advances in topical agents forprehospital haemostasis. Trauma 2002;4:203—9.
78. Holcomb JB. Methods for improved hemorrhage control. CritCare 2004;8:S57—60.
79. Husum H, Gilbert M, Wisborg T, PillgramLarsen J. Prehospital tourniquets: there should be no controversy. J TraumaInjury Infect Crit Care 2004;56:214—5.
80. Jacobs LM. Initial management and evaluation of themultisystem injured patient, Part 1. J Natl Med Assoc1987;79:361—70.
81. Kunin IJ. Principles of first aid. Dent Clin North Am1965:789—801.
82. London PS. Treatment of soft tissue injuries at the roadside.Br Med J 1969;4:284—6.
83. Muhr G, Tscherne H. Rescue and first aid for the severelytraumatized. Chirurg 1978;49:593—600.
84. Navein J, Coupland R, Dunn R. The tourniquet controversy.J Trauma 2003;54:S219—20.
85. Fernandez R, Griffiths R, Ussia C. Water for wound cleansing.Cochrane Database Syst Rev 2005.
24
svelde
Rechthoek

European first aid guidelines 251
86. Jester I, Jester A, Demirakca S, Waag KL. Prehospital emergency management in pediatric burns. Intensivmedizin undNotfallmedizin 2005;42:60—5.
87. O’Neill AC, Purcell E, Jones D, Pasha N, McCann J, Regan P.Inadequacies in the first aid management of burns presentingto plastic surgery services. Ir Med J 2005;98:15—6.
88. Walker A, Baumber R, Robson B. Prehospital managementof burns by the UK fire service. Emerg Med J 2005;22:205—8.
89. Hudspith J, Rayatt S. ABC of burns: first aid and treatmentof minor burns. Br Med J 2004;328:1487—9.
90. Morgan ED, Bledsoe SC, Barker J. Ambulatory managementof burns. Am Fam Physician 2000;62:2015—26.
91. Dunn TM, Dalton A, Dorfman T, Dunn WW. Are emergencymedical technicianbasics able to use a selective immobi
lization of the cervical spine protocol? A preliminary report.Prehosp Emerg Care 2004;8:207—11.
92. Domeier RM, Frederiksen SM, Welch K. Prospective performance assessment of an outofhospital protocol forselective spine immobilization using clinical spine clearancecriteria. Ann Emerg Med 2005;46:123—31.
93. Bleakley C, McDonough S, MacAuley D. The use of icein the treatment of acute softtissue injury: a systematicreview of randomized controlled trials. Am J Sports Med2004;32:251—61.
94. Bailey B. Gastrointestinal decontamination triangle [2]. JToxicol Clin Toxicol 2005;43:59—60.
95. Krenzelok EP. Ipecac syrupinduced emesis . . . no evidenceof benefit. Clin Toxicol 2005;43:11—2.
25
svelde
Rechthoek

26

Effectiveness of nonresuscitative first aid training in
laypersons: a systematic review
CHAPTER 3
Van de Velde S, Heselmans A, Roex A, Vandekerckhove P, Ramaekers D,
Aertgeerts B. Effectiveness of nonresuscitative first aid training in laypersons: a
systematic review. Ann Emerg Med. 2009;54(3):447-457.
27

EVIDENCE-BASED EMERGENCY MEDICINE/CRITICALLY APPRAISED TOPIC
Effectiveness of Nonresuscitative First Aid Training in Laypersons:A Systematic Review
Stijn Van de Velde, MPH
Annemie Heselmans, MSc
Ann Roex, MD
Philippe Vandekerckhove, MD,
PhD
Dirk Ramaekers, MD, PhD
Bert Aertgeerts, MD, PhD
From the Belgian Red Cross–Flanders, Mechelen, Belgium (Van de Velde, Vandekerckhove); the
Centre for Evidence-Based Medicine, Katholieke Universiteit Leuven, Leuven, Belgium (Heselmans,
Ramaekers, Aertgeerts); and the Department of General Practice, Katholieke Universiteit Leuven,
3000 Leuven, Belgium (Roex).
Study objective: This study reviewed evidence on the effects of nonresuscitative first aid training on
competence and helping behavior in laypersons.
Methods: We identified randomized and nonrandomized controlled trials and interrupted time series on
nonresuscitative first aid training for laypersons by using 12 databases (including MEDLINE, EMBASE, and
PsycINFO), hand searching, reference checking, and author communication. Two reviewers independently
evaluated selected studies with the Cochrane Effective Practice and Organisation of Care Review Group quality
criteria. One reviewer extracted data with a standard form and another checked them. In anticipation of
substantial heterogeneity across studies, we elected a descriptive summary of the included studies.
Results: We included 4 studies, 3 of which were randomized trials. We excluded 11 studies on quality
issues. Two studies revealed that participants trained in first aid demonstrated higher written test scores
than controls (poisoning first aid: relative risk 2.11, 95% confidence interval [CI] 1.64 to 2.72; various first
aid cases: mean difference 4.75, 95% CI 3.02 to 6.48). Two studies evaluated helping responses during
unannounced simulations. First aid training improved the quality of help for a bleeding emergency (relative
risk 25.94; 95% CI 3.60 to 186.93), not the rate of helping (relative risk 1.13; 95% CI 0.88 to 1.45).
Training in first aid and helping behavior increased the helping rates in a chest pain emergency compared
with training in first aid only (relative risk 2.80; 95% CI 1.05 to 7.50) or controls (relative risk 3.81; 95% CI
0.98 to 14.89). Participants trained in first aid only did not help more than controls (relative risk 1.36; 95%
CI 0.28 to 6.61).
Conclusion: First aid programs that also train participants to overcome inhibitors of emergency helping behavior
could lead to better help and higher helping rates. [Ann Emerg Med. 2009;54:447-457.]
0196-0644/$-see front matter
Copyright © 2008 by the American College of Emergency Physicians.
doi:10.1016/j.annemergmed.2008.11.005
INTRODUCTION
In case of an accident, injury, or sudden illness, first aid
delivered by bystanders can save lives and limit damage until
professional help has arrived.1,2 Laypersons trained in first
aid can also potentially reduce delays in seeking medical
assistance. The latter is also potentially lifesaving because in
emergencies time may constitute a critical determinant of
victims’ outcomes. Recently, the potential value of first aid
training for laypersons has assumed a heightened importance
in the context of both manmade and natural mass casualty
incidents and disasters. When a sudden disaster strikes,
survivors often constitute the sole source of initial help to
others because professional help takes time to mobilize or isinsufficient.3,4
Reports from the recent bombings in New York and Londonstate that first aid by bystanders might have saved lives.5,6 In theMadrid bombings, 67% of the injured persons arrived at thehospital in nonambulance vehicles.7 Victim transport bybystanders occurs in many mass casualty disasters if ambulancetransport is lacking.3 First aid training can reduce the risks ofprivate victim transport and provide laypersons with guidanceabout when not to move a victim.3 After the Armenia and Kobeearthquakes, bystanders provided only minimal first aidefforts.5,8 Officials interviewed after the disaster strongly agreedthat first aid training for laypersons would likely decrease death
Volume , . : September Annals of Emergency Medicine 447
28
svelde
Rechthoek

rates in similar events.8 Conversely, in disaster preparednessefforts, emergency personnel and authorities often disregard thepotential role of individual laypersons.3,4
Although laypersons rarely panic or develop psychologicalshock in disasters, the emotional stress of the situation cantemporarily limit their reasoning ability.9 Experts widelyadvocate layperson first aid training as a way of improving theinitial response in such situations. Recommendations rangefrom voluntary or mandatory first aid courses to be offered tothe community at large, to courses limited to target groups suchas workers, professional drivers, family members of high riskindividuals, or citizens living in disaster-prone areas.3,4,6,9-12
Given the increased premium on layperson first aid skillsunder conditions of disaster and the consequent likelihood ofsubstantial increase in resources devoted to training efforts, theevaluation of effectiveness of such training assumes paramountimportance. Such evaluations need to assess whether courseparticipants acquire appropriate attitudes, competences, andbehavior for first aid provision. This implies that courseparticipants demonstrate a positive attitude and helping reactiontoward emergencies, and furthermore that they can assess thesituation, ensure safety, assess the condition of the victim, gethelp if required, and administer first aid and provide emotionalsupport to victims.Published reports of effectiveness of first aid training are
scattered across a large array of biomedical journals published indifferent languages and in journals associated with differentpractice specialties, making it difficult to derive a validassessment of current knowledge in this area. The objective ofthis study was to systematically review primary studies on theeffects of nonresuscitative first aid training with regard toacquisition and retention of competence or modification ofhelping behavior.
MATERIALS AND METHODSWe reported this study in accordance with the QUOROM
statement for meta-analyses.13
Search StrategyWe developed the search strategy in consultation with an
information specialist and conducted a literature search ofMEDLINE (PubMed), EMBASE (EMBASE.com), theCochrane Central Register of Controlled Trials (Wiley), C2-SPECTR (Campbell Collaboration), Cinahl (EBSCOhost),British Nursing Index and Archive (OVID), SPORTDiscus(EBSCOhost), PsycINFO (WebSPIRS), and EducationResources Information Center database (EBSCOhost). A searchof the abovementioned databases took place from inceptionuntil May 2007. Appendix E1 (available online athttp://www.annemergmed.com) contains the description of theactual search strategies.We searched for grey literature reports14 about first aid
training in the Open Archives Initiative (OAIster) database andthe British Library Integrated Catalogue and consulted the
database of the Netherlands Institute for Health ServicesResearch (NIVEL) for Dutch-language reports on June 19,2007. We further searched for studies by communicating withthe authors of included studies, checking reference lists ofselected studies and of related systematic reviews,15-21 and handsearching. We hand searched conference proceedings andsupplement issues of the journals Resuscitation and Prehospitaland Disaster Medicine from January 1997 to April 2007.
Study SelectionIn anticipation of finding only a few studies with useful data,
we deliberately defined broad inclusion criteria. Systematicreviews with broad questions are valid on the condition thatthey do not generalize findings across differing conditions.22Weincluded randomized controlled trials, nonrandomizedcontrolled trials, controlled before-and-after trials, andinterrupted time series in our review.We defined a layperson as somebody who has never received
a formal health care education, and we included studiescovering first aid training for laypersons of all education levels.We included studies including participants with previousknowledge of first aid but excluded studies on patient educationand studies involving training for health care students andprofessionals. There were no restrictions on participants’ age,sex, ethnicity, motivation, learning potential, learning behavior,or education level. We defined first aid as immediate helpprovided to a suddenly ill or injured person, until that personhas recovered or medical care is available.We defined first aid training as a formal learning activity,
with learning goals defined in terms of skills and attitudespertaining to immediate help in case of accidents, injuries, orsudden illness. We did not include studies about the effect ofinformal learning activities, such as mass media awarenesscampaigns.We included studies that reported learning and behavior
outcomes relating to first aid training for bleeding, shock,wounds, injuries, poisoning, stroke, chest pain, asthmaticattacks, epileptic seizures, or diabetic crisis. We excluded studiesfocusing only on basic life support or the use of automatedexternal defibrillators. If studies covered both first aid andresuscitation training, we included only results of theeffectiveness of first aid training. We placed no restrictionsabout training methods, materials, duration, or delivery format.Primary outcomes of interest included measures of helping
behavior in real situations, including deception experiments. Indeception experiments, the study participants are unaware thatan emergency is being simulated and do not know that theirhelping behavior is being evaluated. This concept originatesfrom social psychology research and differs from customarysimulations in which participants know that it is an imitation ofan emergency. Secondary outcomes included measures oflearning gains in knowledge and skills. We did not includecourse participant views on the training or self-assessmentmeasures as outcome measures. There was no restriction on theoutcome assessment method or timing. Our interest focused
Effectiveness of Layperson First Aid Training Van de Velde et al
448 Annals of Emergency Medicine Volume , . : September
29
svelde
Rechthoek

both on the outcomes directly after completing the first aidtraining and outcomes in the weeks or months afterward.Because of time and resource constraints, we considered onlystudies reported in English, German, French, or Dutch.Two reviewers (S.V.D.V., A.H.) independently selected
studies from titles and abstracts. Interrater agreement wasevaluated with a Cohen’s k. The reviewers resolveddisagreements on the selection of studies by discussion and thenscreened full texts and excluded irrelevant studies.
Assessment of Risk of Bias in Selected StudiesTwo reviewers (S.V.D.V., A.H.) independently evaluated all
the selected studies for methodological quality. We used thequality criteria of the Cochrane Effective Practice andOrganisation of Care Review Group23 because they providevalidated checklists for every type of study design that wasincluded in our review. The quality criteria for randomizedcontrolled trials included concealment of allocation, participantfollow-up, blinded assessment, measurement of baseline data,reliability of outcome measures, and protection againstcontamination among study groups. Appendix E2 (availableonline at http://www.annemergmed.com) contains the actualchecklist for randomized controlled trials.We rated studies as having low risk of bias if all the quality
criteria were met and as having moderate risk of bias if 2 criteriawere not met, partially met, or not clear. Studies received a highrisk of bias rate when 3 or more criteria were not met, partiallymet, or not clear. Some quality issues about eligibility aroseduring the assessment process in studies in which bias wasexplicitly clear. The group of reviewers decided in agreement toset a cut point for inclusion between studies with a risk of biasand undoubtedly biased studies. This is one of the possibleapproaches to limit bias in a systematic review.22We consideredwhether to include studies with fewer than 10 participants anddecided not to do so because the allocation could not lead tobalanced groups. We decided to exclude studies if thecomparison groups had substantial differences at baselinebecause this made groups noncomparable. We excluded studieswith clear indications of exposure to the intervention in thecontrol group because this creates contamination bias anddilutes the effect of the intervention. We also discussed whetherto include studies with limited compliance with the interventionand decided not to do so because this raises serious concernsabout the representativeness of the data and might bemisleading. We contacted authors of selected studies if certaindata were not reported in the article, and if essential informationwas not forthcoming, we excluded the study from furtheranalysis. In cases of disagreement on the quality, a third reviewer(B.A.) resolved differences.
Data Extraction and SynthesisBecause there is no single data extraction form that fits all
uses, we adapted the Best Evidence Medical EducationCollaboration (BEME) coding sheet24 to the needs of ourreview. The extracted data related to methodology, participants,
setting, educational descriptors, assessment features, outcomes,and the study’s conclusions. We classified education levelsaccording to the International Standard Classification ofEducation (ISCED) levels.25
For the outcome measures, we entered indications of face,content, construct, concurrent, or predictive validity andreliability measures such as internal consistency, interraterreliability, or test-retest reliability in the data extraction form.One reviewer (S.V.D.V.) extracted data and another (A.H.)checked them. Disagreements were resolved by discussion.The group of reviewers (S.V.D.V., A.H., B.A.) assessed
clinical heterogeneity by evaluating the type of participants,intervention, and outcome for each study. In anticipation offinding only a few and very heterogeneous studies, there was noplan to conduct subgroup or sensitivity analysis, or meta-analysis methods. Instead, we conducted a descriptive review ofthe included studies. To present the outcomes uniformly acrossstudies, we used the Review Manager software version 4.2.10(The Nordic Cochrane Centre, The Cochrane Collaboration,Copenhagen, Denmark) to calculate mean differences forstudies with continuous data and relative risks for studies withdichotomous data.
RESULTSTrial FlowFigure 1 provides a flowchart of the identification and
selection of studies. The reviewers screened 7,644 citations,including 1,540 duplicates. Evaluation of titles and abstractsresulted in 146 citations. Agreement between the 2 reviewerswas high (Cohen’s k of 0.89). After full text evaluation, 15studies matched every selection criteria. The reviewers agreed
Figure 1. Flowchart of identification and selection ofstudies.
Van de Velde et al Effectiveness of Layperson First Aid Training
Volume , . : September Annals of Emergency Medicine 449
30
svelde
Rechthoek

unanimously to exclude 10 studies26-35 after the assessment ofprobable bias. One poorly reported study was excluded becauseit did not provide sufficient information to evaluate itsquality.36 Table 1 presents the results of the quality assessmentper included study; Table 2, per excluded study.
Study CharacteristicsTable 3 summarizes the characteristics of 4 included studies.
Three studies37-39 were randomized controlled trials, and one40
was a nonrandomized controlled trial.Kelly et al37 tested a 9-minute video clip about first aid for
poisoning, combined with the distribution of pamphlets andstickers. Participants were parents of young children who visiteda women, infant, and children clinic. Outcome measuresincluded knowledge about first aid for poisoning. The authorscarried out the assessment by means of written and oralinterviews.Moore38 evaluated the effects of assertion training and first
aid instruction for primary school children. This program wasintended to increase the children’s autonomy and ability to takecare of their own health. The training consisted of anoncompulsory course within the school setting, with randomallocation of participants to one of 4 comparison groups. Thegroups received either 6 hours of assertion training, 6 hours offirst aid training, 3 hours of assertion training, and 3 hours offirst aid training or received no training but watched 6 hours ofscience films without health education content. The first aidtraining covered bleeding, injuries, burns, shock, poisoning, andother topics outside the review. Assertiveness training focusedon developing assertive behavior so that participants couldbecome more autonomous health care consumers. Thisconsisted of learning how to express feelings, ask forinformation, and make requests or refusals. The authors used awritten test to assess first aid knowledge and skills.Shotland and Heinold39 evaluated the change in first aid
practice among university students after first aid training. Thefirst aid training was part of a program organized by the healtheducation department. The duration of the training course isunclear. Passing the final examination would lead to anAmerican Red Cross certificate in advanced first aid andemergency care. This study evaluated the helping responses of
participants during unannounced simulations. The participantswere deceived and the simulations carefully staged so that theyactually believed it was a real accident.The simulated accident was that of a fallen worker who was
bleeding severely. The influence of training was tested againstthe presence of bystanders and level of ambiguity. The numberof bystanders was either none or 2. In ambiguous conditions,there was only the sound of the falling worker; in unambiguousconditions, there was also a moan for help. Participant responseswere categorized as providing no help, calling for help, orproviding direct help.Hawks and Egan40 evaluated the effect of training at a
university during a health and wellness education course open toall university students. The majority of students were from thefaculty of education. Students took part in the course forreasons of personal interest or because it was a compulsorylesson or an elective. The trainers randomly allocatedparticipants to one of 4 comparison groups: first aid trainingcomplemented with training in overcoming the inhibitors ofemergency helping behavior, training that mentioned theinhibitors, training without focus on inhibitors, or no training.The training in the inhibitors of emergency helping behaviorstressed during the lectures that bystanders often are held backfrom helping when there are other bystanders or when there isambiguity about the gravity of the emergency. The participantsdiscussed how to deal with these barriers to providing help andexercised this in simulations with situational ambiguity andpresence of bystanders. The only difference between the 3training programs was the amount of time spent on theinhibitors of emergency helping behavior. The exact duration ofthe training courses is unclear.As in the previously described study, the participants were
deceived and unexpectedly confronted with a simulatedemergency. The simulation was chest pain in a middle-agedand overweight worker. Four actors played bystanders in theroom with the casualty who was urgently in need of help.The study recorded whether the participants provided help.No data were available on the type of help provided. Thisstudy also carried out a preliminary test in the interventiongroups of first aid knowledge and skills by means of a writtenand a practical test.
Table 1. Assessment of quality criteria about risk of bias among the 4 included studies meeting quality and nonquality eligibility
criteria for inclusion.
Included Study by
First Author
Concealment of
Allocation
Participant
Follow-up
Blinded or Objective
Assessment
Baseline
Measurement
Reliable
Outcome(s)
Protection Against
Contamination Global Assessment
Kelly, 200337 Partially done Done Done Partially done Unclear Done Included study with
a high risk of bias
Moore, 198738 Not done Done Not done Done Partially done Done Included study with
a high risk of bias
Shotland, 198539 Partially done Partially done Unclear Not done Done Unclear Included study with
a high risk of bias
Hawks, 199840 Not done Done Done Done Partially done Done Included study with
a moderate risk of
bias
Effectiveness of Layperson First Aid Training Van de Velde et al
450 Annals of Emergency Medicine Volume , . : September
31
svelde
Rechthoek

Table 2. Assessment of quality criteria about risk of bias among 11 excluded studies meeting nonquality eligibility criteria for
inclusion.
Excluded Study by
First Author
Concealment
of Allocation
Participant
Follow-up
Blinded or
Objective
Assessment
Baseline
Measurement
Reliable
Outcome(s)
Protection
Against
Contamination Global Assessment
Marchand-Martella,
199226
Not done Done Not done Unclear Done Unclear Study excluded because the
sample size was less than
10 and the allocation could
not lead to balanced groups
Peterson, 198427 Not done Done Unclear Done Done Unclear Study excluded because the
sample size was less than
10 and the allocation could
not lead to balanced groups
Timko, 199928 Not
applicable
Done Unclear Not done Done Not done Study excluded because the
sample size was less than
10 and the allocation could
not lead to balanced
groups, and the controls
were exposed to the
intervention
McKenna, 198229 Not done Partially
done
Unclear Not done Unclear Unclear Study excluded because the
comparison groups had
substantial differences at
baseline, which made
groups noncomparable
Stern, 199930 Not done Unclear Unclear Not done Unclear Done Study excluded because the
comparison groups had
substantial differences at
baseline, which made
groups noncomparable
Frederick, 200031 Partially done Done Partially done Not done Partially
done
Unclear Study excluded because the
comparison groups had
substantial differences at
baseline, which made
groups noncomparable
Campbell, 200132 Partially done Partially
done
Done Done Partially
done
Not done Study excluded because there
was insufficient compliance
with the intervention
(overall 57% attendance at
the sessions), and the
controls were exposed to
the intervention
Engeland, 200233 Partially done Not done Not done Done Partially
done
Done Study excluded because only
26% of the participating
schools complied with the
intervention, which raises
serious concerns about the
representativeness of the
data
Capone, 200034 Partially done Done Done Done Partially
done
Not done Study excluded because the
controls were exposed to
the intervention
Raynal, 199135 Not done Done Done Done Unclear Not done Study excluded because the
controls were exposed to
the intervention
Breivik, 198036 Unclear Unclear Unclear Unclear Unclear Unclear Study excluded because of
insufficient information to
evaluate the quality
Van de Velde et al Effectiveness of Layperson First Aid Training
Volume , . : September Annals of Emergency Medicine 451
32
svelde
Rechthoek

All studies measured the final outcomes within 1 month ofthe intervention.37-40
Risk of BiasTable 1 summarizes the methodological quality of the 4
included studies.
Kelly et al37 allocated the participants at random to thecomparison groups but did not report on procedures forconcealment. Eighty-nine percent of the enrolledparticipants completed the study. Researchers, blind to groupstatus, recorded the outcomes. The study obtained baselinemeasurements of first aid knowledge. There was no reporting
Table 3. Characteristics of included studies.
Study by
First Author Education Level Setting Participants Intervention Outcome
Kelly, 200337 Higher
(nonuniversity)
Training at 2
women, infant,
and children
clinics.
Parents of young
children who visited
the clinic.
N: 323
Age: u
I5video (9 min),
pamphlets, and stickers
about first aid for
poisoning
C5educational class on
immunizations and
healthy snacks
Assessment of knowledge about
first aid for poisoning with
written and oral interviews
Moore,
198738
Primary Training in primary
school as a
noncompulsory
course.
Pupils from 2 primary
schools.
N: 92
A: 10–11 y
I(1)5training to develop
assertive behavior to
become a more
autonomous health care
consumer (6 h)
I(2)5first aid training on
bleeding, injuries, burns,
shock, poisoning, and
other topics outside the
review (6 h)
I(3)5assertion training (3
h) and first aid training
on abovementioned
topics (3 h)
C5viewing science films
without health education
content (6 h)
Assessment of first aid
knowledge and skills on first
aid for bleeding, broken
bones, burns, head injuries,
poisoning, and heat stroke
with a written test
Shotland,
198539
Higher (university) Training at university
during a first aid
program organized
by the health
education
department.
Participants from the
usual enrollments for
the training program.
Passing the
examination led to an
American Red Cross
certificate.
N: 209
A: u
I5first aid training on
bleeding, wounds, and
other undefined topics
(duration5u)
C5receiving same training
as I but took tests
before lesson on
bleeding control
(duration5u)
Assessment of helping behavior
during a deception experiment
with a simulated arterial
bleeding emergency
Hawks,
199840
Higher (university) Training at university
during a health
and wellness
education course
open to all
university
students.
Recruitment through the
normal university
registration process.
Reasons for
participation in the
training included
personal interest, as
a compulsory lesson,
or as an elective.
N: 98
A: 18-53 y
I(1)5first aid training that
also addressed 2
inhibitors of emergency
helping behavior, ie,
situational ambiguity
and bystander effect
(duration5u)
I(2)5first aid training that
mentioned inhibitors of
helping behavior
(duration5u)
I(3)5first aid training
without focus on
inhibitors of helping
behavior (duration5u)
C5no first aid training
Assessment of first aid
knowledge and skills with a
written and a practical test
(no data reported in study)
Assessment of helping rates
during a deception experiment
with a simulated chest pain
emergency
u, Unclear; I, intervention group; C, control group.
Effectiveness of Layperson First Aid Training Van de Velde et al
452 Annals of Emergency Medicine Volume , . : September
33
svelde
Rechthoek

of reliability data. Protection against contamination wasadequate. The study did not provide indications of facevalidity and did not report whether content experts hadreviewed the test instrument before the trial. However, wecould derive content validity indications from the providedtest descriptions. We assessed the study to have a high risk ofbias.Moore38 did not use concealment of randomization. All the
enrolled participants completed the study. The study failed toblind the researchers. Baseline measurements recorded first aidknowledge and skills with a written test. The test instrumenthad a satisfactory internal consistency (Crohnbach’s a of 0.67).Protection against contamination was adequate. Face validitywas evaluated by asking the children for feedback on the testinstruments in a pilot study with another primary school.Content experts had reviewed the test instrument before thetrial, and the provided test descriptions showed content validity.Participants who received more training also performed betteron the test, which indicates construct validity. We assessed thestudy to have a high risk of bias.Shotland and Heinold39 allocated the participants at random
to the comparison groups but did not describe procedures forconcealment. Seventy-eight percent of the enrolled participantscompleted the study. The study failed to report on blinding andprotection against contamination. The study did not recordbaseline measurements of outcomes. Video recordings allowedverifying the helping behavior data of participants obtained bythe researcher’s observations. No data collection errors weredetected. Demonstrating a high credibility with suspicion scoresabout the induced deception provided an indirect indication offace validity. It was unclear whether content experts hadreviewed the test instrument before the trial, but the providedtest descriptions showed content validity. We assessed the studyto have a high risk of bias.Hawks and Egan40 allocated the participants to the
comparison groups through the normal universityregistration process. All the enrolled participants completedthe study. Researchers, blind to group status, recorded theoutcomes. Baseline measurements recorded first aidknowledge and skills. Video recordings allowed verifying thehelping behavior data of participants obtained by theresearcher’s observations. No data collection errors weredetected. Protection against contamination was adequate.The study did not report whether content experts hadreviewed the test instrument before the trial, but the testdescriptions provided in the article showed content validity.It was unclear whether the study obtained suspicion scores,but this study did report high credibility of the test in apreceding experiment. Participants who received moretraining also performed better on the test, which indicatesconstruct validity. In relation to concurrent and predictivevalidity, the study compared scores on a written and practicaltest with scores during the helping behavior test. The 3groups trained in first aid had comparable scores on the
written knowledge test and practical skills test. The controlgroup did not take the written and practical test. Therefore,no actual comparison between scores on both tests waspossible. We assessed the study to have a moderate risk ofbias.
Effect of InterventionTable 4 gives a summary of the most important study results.
Without statistical pooling, forest plots graphically represent the
Table 4. Summary of main findings.
Study by
First Author Outcome Measure Main Results
Kelly, 200337 Written and oral test
on first aid
knowledge for
poisoning
Trained persons have a
significantly better
knowledge of Poison
Control Center telephone
number (RR 3.35; 95% CI
2.33 to 4.81) and of first
aid in case of household
bleach ingestion (RR 2.11;
95% CI 1.64 to 2.72)
Moore,
198738
Written test on first aid
knowledge and skills
for multiple cases
Significantly better
knowledge and skills
among those with 6 h first
aid training vs controls
(MD 4.75; 95% CI 3.02 to
6.48) and among those
with 3 h first aid training
vs controls (MD 2.56;
95% CI 0.99 to 4.13)
Shotland,
198539
Deception experiment
on helping behavior
Trained participants provided
significantly better first aid
for an arterial bleeding
emergency (RR 25.94;
95% CI 3.60 to 186.93).
Helping response for an
arterial bleeding
emergency did not occur
significantly more in
trained participants (RR
1.13; 95% CI 0.88 to
1.45)
Hawks,
199840
Deception experiment
on helping behavior
Helping response for a chest
pain emergency did not
significantly differ between
people trained in first aid
only and controls (RR
1.36; 95% CI 0.28 to
6.61). Helping response
occurred significantly more
among those trained in
first aid and helping
behavior than among
those trained in first aid
only (RR 2.80; 95% CI
1.05 to 7.50) or than in
controls (RR 3.81; 95% CI
0.98 to 14.89)
RR, relative risk; MD, mean difference.
Van de Velde et al Effectiveness of Layperson First Aid Training
Volume , . : September Annals of Emergency Medicine 453
34
svelde
Rechthoek

main findings of the 2 deception experiments (Figure 2).Appendix E3 contains the data used to calculate relative risk andmean difference for each comparison (available athttp://www.annemergmed.com).The study by Kelly et al37 on first aid for poisoning revealed
significantly better knowledge of the Poison Control Centerwork and its telephone number in trained participants (relativerisk 3.35; 95% confidence interval [CI] 2.33 to 4.81). In thecase of household bleach ingestion, participants receiving theintervention responded twice more that they would call thePoison Control Center (relative risk 2.11; 95% CI 1.64 to2.72).The study by Moore38 with first aid training for primary
education children revealed significantly greater knowledge andskills in the groups receiving first aid instruction. The highestdifference in scores occurred between the group receiving 6hours of first aid training and the control group (meandifference 4.75; 95% CI 3.02 to 6.48; range of scores possible 0to 20).The study by Shotland and Heinold39 that unexpectedly
confronted university students with an arterial bleedingemergency revealed that some type of help was provided by64% of participants in the intervention group and by 57% ofthe controls. The chances of helping were not significantlydifferent when comparing the 2 groups (relative risk 1.13; 95%CI 0.88 to 1.45). The number of respondents was significantlyhigher in unambiguous situations (relative risk 1.86; 95% CI1.40 to 2.46) and when individuals were alone with the casualty
(relative risk 1.29; 95% CI 0.99 to 1.66). Untrainedparticipants limit their helping response significantly more to acall for help only. Trained participants applied significantlymore direct pressure to control the bleeding than untrained andperformed much better in the combination of calling for helpand applying direct pressure (relative risk 25.94; 95% CI 3.60to 186.93).The study by Hawks and Egan40 about university students’
helping response to a chest pain emergency found a 45%helping rate in the group trained in first aid and helpingbehavior. Some type of help was provided by 26% of theparticipants in the group addressing helping behavior in smallmeasure, 16% in the group receiving first aid training withouthelping behavior, and 12% among controls. Levels ofsignificance were reached when helping behavior in the groupbeing trained in first aid and helping behavior with thosetrained in first aid only were compared (relative risk 2.80; 95%CI 1.05 to 7.50) or with controls (relative risk 3.81; 95% CI0.98 to 14.89). The group addressing helping behavior in smallmeasure did not help significantly more than controls (relativerisk 2.20; 95% CI 0.52 to 9.39), nor did the group receivingfirst aid training without focus on helping behavior (relative risk1.36; 95% CI 0.28 to 6.61).
LIMITATIONSAnalyzing the references obtained per source shows that the
search strategy can be improved. Searching MEDLINE(PubMed), EMBASE (EMBASE.com), PsycINFO
Figure 2. Forest plots without statistical pooling for the main findings of the 2 deception experiments first sorted bycomparison and then by outcome. The squares display the effect sizes and the horizontal lines represent the CIs. If the CIcrosses the vertical line, it means there is no statistically significant difference.
Effectiveness of Layperson First Aid Training Van de Velde et al
454 Annals of Emergency Medicine Volume , . : September
35
svelde
Rechthoek

(WebSPIRS), and Education Resources Information Centerdatabase (EBSCOhost) would have been sufficient to retrieve allrelevant studies. Dropping key words such as “emergencymedicine” and “emergency nursing” that did not add anyrelevant studies for laypersons can increase the specificity of thesearch formula. Inserting a set of terms describing the criteriafor study designs is recommended. Adding search terms onspecific first aid topics to the intervention terms and adding thekey words “helping behavior” with OR to the outcome termscould be meaningful. As a result of checking the reference listsof all relevant studies and related systematic reviews andcommunication with authors of included studies, it is highlyunlikely that any studies were missed. As a safeguard, weperformed the search again after completion of the review,adding the key words “helping behavior,” but this did not revealany new relevant studies.A limitation in our study is that we excluded studies from
our review if they were not reported in English, German,French, or Dutch. Because emergency and disaster preparednessis a topic of major interest in Europe and elsewhere, it ispossible that important studies were not included in our reviewbecause of their choice of language.Another potential source of bias is incomplete reporting of
results in the published reports of the studies included in thereview. We contacted the authors of the 4 included studies witha request for more information, and 2 replied with more details.The research question in this systematic review was broadly
defined and included 4 studies that vary by either participants oroutcomes, making it difficult to make generalizations.
DISCUSSIONWe know of 3 previous reviews on the effectiveness of
cardiopulmonary resuscitation training for cardiac arrest.15-17
We believe that ours is the first systematic review of effectivenessof nonresuscitative first aid training in laypersons.All 4 of the studies we included found statistically significant
effects of first aid training on either competence or helpingbehavior of laypersons.37-40 The identification of 2 studies thatmeasured the change in practice39,40 is an important finding ofthis review.Although first aid training appeared to improve the quality
of first aid procedures for a bleeding emergency, it did not leadto an increased helping rate.39 The presence of bystanders andambiguity of situations emerged as barriers to providing help.39
A training program that focused both on first aid proceduresand on inhibitors of emergency helping behavior was closelyassociated with higher helping rates in a chest pain emergency.40
Although it is difficult to generalize from the 4 included studies,it nonetheless appears likely that traditional first aid trainingimproves objectively measured skill competences more than itdevelops a positive attitude and a likely helping reaction towardemergencies on the part of trainees.The evidence available to answer our question about the
effects of first aid training is of low quality and incomplete. The
studies provided little evidence to demonstrate validity andreliability of the outcome measures. Data are available only forsingle-victim emergencies. The findings are also limited totraining at a few educational levels and to observation ofeffectiveness of training within 1 month of the intervention.Furthermore, the evidence is too limited to take into accounteither the variability across cases or across components ofcompetence.New rigorous randomized controlled trials on the acquisition
and retention of competence and the modification of helpingbehavior are needed to explore the provisional findings of oursystematic review. The key challenge is to gain a betterunderstanding of actual helping behavior. The study by Hawksand Egan40 found that 45% of the participants trained in firstaid and helping behavior demonstrated helping behavior.Participants in this group helped almost 3 times more thanthose trained in first aid only. Nevertheless, 55% of trainees didnot provide any type of help. Many social psychologyexperiments have studied the influence of different contextual,personal, group, and victim factors in medical emergencies. Asystematic review of these studies might help to determinewhich factors are likely to be important for enhancement of theeffectiveness of first aid training.Deception experiments seem potentially useful means of
testing behavioral effectiveness. However, there are some ethicalconsiderations. Researchers may only use deception as part of astudy if the research question is important and deception is theonly way to obtain valid data. Participants should be informedabout the risks involved in the research and should not beexposed to harmful stress levels. At the end of the study,participants should be fully debriefed.41 Caution is alsorecommended to prevent harm to simulation participants.First aid covers assistance for a variety of situations. It is
important for the validity of the outcome measures to gather abroad sample of performance when possible. When newrandomized controlled trials are designed, it is essential tocarefully consider the reliability and validity of the outcomesthat will be measured. Apart from the recommendation above,we refer readers to the International Handbook of Research inMedical Education, by Norman et al,42 for an elaboratediscussion on obtaining valid and reliable outcomemeasurements.In conclusion, on the basis of 2 studies with university
students, programs for first aid that also train participants toovercome inhibitors of emergency helping behavior could leadto better help and higher helping rates for single-victimemergencies. Because the overall completeness and quality of theevidence is low, full confidence in this conclusion should beconsidered to be contingent on further research.
The authors are grateful to J. Collins, P. Donceel, M. VanNuland, for their critical reflections on this review. They thank J.Vlayen for his advice on composing the search strategy. The authorswould also like to thank the following authors for providing
Van de Velde et al Effectiveness of Layperson First Aid Training
Volume , . : September Annals of Emergency Medicine 455
36
svelde
Rechthoek

additional information: K. Frederick, J. Moore, G. Smedslund,J.C. Lane, H. Breivik, S. Hawks, and D. Kendrick.
Author contributions: This review was made on behalf of
Belgian Red Cross-Flanders. SVDV, BA, and DR conceived and
designed the study. SVDV implemented and wrote the review.
AH was the second reviewer and screened retrieved papers
against inclusion criteria, appraised the methodological quality
of studies, and checked if data extraction was accurate. BA
and DR gave methodological advice. AR provided a medical
education perspective. PV provided general advice on the
review. B Aertgeerts was the guarantor of the study.
Funding and support: By Annals policy, all authors are required
to disclose any and all commercial, financial, and other
relationships in any way related to the subject of this article
that might create any potential conflict of interest. See the
Manuscript Submission Agreement in this issue for examples
of specific conflicts covered by this statement. This study was
funded by the Belgian Red Cross–Flanders. Belgian Red
Cross–Flanders is one of the 186 National Societies of the
International Red Cross and Red Crescent Movement. First aid
training is an important activity of the organization. To further
improve the quality and effectiveness of the first aid
programs, the Belgian Red Cross–Flanders aims at the
establishment of evidence-based practice in first aid. S Van de
Velde and P Vandekerckhove are in employment at the Belgian
Red Cross-Flanders, which provides training in first aid.
Publication date: Available online January 21, 2009.
Reprints not available from the authors.
Address for correspondence: Stijn Van de Velde, Belgian Red
Cross-Flanders, Motstraat 40, 2800 Mechelen, Belgium; 32-0-
15-44-34-76, fax 32-0-15-44-33-08; E-mail
REFERENCES1. Van de Velde S, Broos P, Van Bouwelen M, et al. European first
aid guidelines. Resuscitation. 2007;72:240-251.
2. Handley AJ, Koster R, Monsieurs K, et al. European Resuscitation
Council guidelines for resuscitation 2005. Section 2. Adult basic
life support and use of automated external defibrillators.
Resuscitation. 2005;67(suppl 1):S7-23.
3. Auf der Heide E. The importance of evidence-based disaster
planning. Ann Emerg Med. 2006;47:34-49.
4. Helsloot I, Ruitenberg A. Citizen response to disasters: a survey
of literature and some practical implications. J Contingencies
Crisis Manage. 2004;12:98-111.
5. Crippen D. The World Trade Center attack. Similarities to the
1988 earthquake in Armenia: time to teach the public life-
supporting first aid? Crit Care. 2001;5:312-314.
6. Wessely S. The London attacks—aftermath: victimhood and
resilience. N Engl J Med. 2005;353:548-550.
7. Carresi AL. The 2004 Madrid train bombings: an analysis of pre-
hospital management. Disasters. 2008;32:41-65.
8. Adamson S. First aid response to the Kobe earthquake, January
17, 1995. Natural Hazards Center (1997). Available at: http://
www.colorado.edu/hazards/research/qr/qr102.html. Accessed
October 21, 2008.
9. Perry RW, Lindell MK. Understanding citizen response to disasters
with implications for terrorism. J Contingencies Crisis Manage.
2003;11:49-60.
10. World Health Organization. Prehospital trauma care systems (2005).
Available at: http://www.who.int/violence_injury_prevention/
publications/services/39162_oms_new.pdf. Accessed October 21,
2008.
11. Abrams JI, Pretto EA, Angus D, et al. Guidelines for rescue training
of the lay public. Prehosp Disaster Med. 1993;8:151-156.
12. Kano M, Siegel JM, Bourque LB. First-aid training and capabilities of
the lay public: a potential alternative source of emergency medical
assistance following a natural disaster. Disasters. 2005;29:58-74.
13. Moher D, Cook DJ, Eastwood S, et al. Improving the quality of
reports of meta-analyses of randomised controlled trials: the
QUOROM statement. Lancet. 1999;354:1896-1900.
14. Auger CP. Information Sources in Grey Literature (Guides to
Information Sources). 4th ed. London, England: Bowker Saur; 1998.
15. International Liaison Committee on Resuscitation. 2005
International consensus on cardiopulmonary resuscitation and
emergency cardiovascular care science with treatment
recommendations. Part 8: Interdisciplinary topics. Resuscitation.
2005;67:305-314.
16. Jabbour M, Osmond MH, Klassen TP. Life support courses: are
they effective? Ann Emerg Med. 1996;28:690-698.
17. Makinen M, Niemi-Murola L, Makela M, et al. Methods of
assessing cardiopulmonary resuscitation skills: a systematic
review. Eur J Emerg Med. 2007;14:108-114.
18. Kendrick D, Coupland C, Mulvaney C, et al. Home safety
education and provision of safety equipment for injury prevention.
Cochrane Database Syst Rev. 2007;(1):CD005014.
19. Spinks A, Turner C, McClure R, et al. Community based
prevention programs targeting all injuries for children. Inj Prev.
2004;10:180-185.
20. Turner C, Spinks A, McClure R, et al. Community-based
interventions for the prevention of burns and scalds in children.
Cochrane Database Syst Rev. 2004;(3):CD004335.
21. Harborview Injury Prevention and Research Center. Best
practices: poisoning. Available at: http://depts.washington.edu/
hiprc/practices/topic/poisoning/index.html. Accessed September
25, 2007.
22. Higgins JPT, Green S, eds. Cochrane handbook for systematic
reviews of interventions 4.2.5 [updated May 2005]. Available at:
http://www.cochrane.org/resources/handbook. Accessed June
11, 2007.
23. Cochrane Effective Practice and Organisation of Care Group. The
data collection checklist. Available at: http://www.epoc.cochrane.
org/files/website%20files/Documents/Reviewer%20Resources/
datacollectionchecklist.pdf. Accessed June 11, 2007.
24. Best Evidence Medical Education Collaboration. Appendix IIIA
prototype BEME coding sheet. Available at:
http://www.bemecollaboration.org/beme/pages/start.html.
Accessed June 11, 2007.
25. UNESCO. International standard classification of education
(ISCED 1997). Available at: http://www.unesco.org/education/
information/nfsunesco/doc/isced_1997.htm. Accessed
November 5, 2007.
26. Marchand-Martella NE, Martella RC. Teaching a first aid skill to
students with disabilities using two training programs. Educ Treat
Child. 1992;15:15-31.
27. Peterson L. Teaching home safety and survival skills to latch-key
children: a comparison of two manuals and methods. J Appl
Behav Anal. 1984;17:279-293.
28. Timko TC, Sainato DM. Effects of first aid training using small
group instruction with young children with disabilities. J Early
Intervent. 1999;22:323-336.
29. McKenna SP, Hale AR. Changing behavior towards danger: the
effect of first aid training. J Occup Accidents. 1982;4:47-59.
Effectiveness of Layperson First Aid Training Van de Velde et al
456 Annals of Emergency Medicine Volume , . : September
37
svelde
Rechthoek

30. Stern EB, Berman M, Thomas JJ, et al. Community education for
stroke awareness: an efficacy study. Stroke. 1999;30:720-723.
31. Frederick K, Bixby E, Orzel MN, et al. An evaluation of the
effectiveness of the Injury Minimization Programme for Schools
(IMPS). Inj Prev. 2000;6:92-95.
32. Campbell NR, Ayala GX, Litrownik AJ, et al. Evaluation of a first
aid and home safety program for Hispanic migrant adolescents.
Am J Prev Med. 2001;20:258-265.
33. Engeland A, Roysamb E, Smedslund G, et al. Effects of first-aid training
in junior high schools. Inj Control Saf Promot. 2002;9:99-106.
34. Capone PL, Lane JC, Kerr CS, et al. Life supporting first aid
(LSFA) teaching to Brazilians by television spots. Resuscitation.
2000;47:259-265.
35. Raynal A, Gear JS, de Beer M. Child health and childminding. S
Afr Med J. 1991;80:28-31.
36. Breivik H, Ulvik NM, Blikra G, et al. Life-supporting first aid self-
training. Crit Care Med. 1980;8:654-658.
37. Kelly NR, Huffman LC, Mendoza FS, et al. Effects of a videotape
to increase use of poison control centers by low-income and
Spanish-speaking families: a randomized, controlled trial.
Pediatrics. 2003;111:21-26.
38. Moore JB. Effects of assertion training and first aid instruction on
children’s autonomy and self-care agency. Res Nurs Health.
1987;10:101-109.
39. Shotland RL, Heinold WD. Bystander response to arterial bleeding:
helping skills, the decision-making process, and differentiating the
helping response. J Pers Soc Psychol. 1985;49:347-356.
40. Hawks SR, Egan M. The impact of three different first aid
curricula on emergency helping among college students. J Health
Educ. 1998;29:289-293.
41. American Psychological Association. Ethical principles of
psychologists and code of conduct (2002). Available at:
http://www.apa.org/ethics/code2002.html. Accessed June
25, 2008.
42. Norman GR, van der Vleuten CPM, Newble DI, eds. International
Handbook of Research in Medical Education. Dordrecht, The
Netherlands: Kluwer Academic Publishers; 2002.
Van de Velde et al Effectiveness of Layperson First Aid Training
Volume , . : September Annals of Emergency Medicine 457
38
svelde
Rechthoek

APPENDIX E1. Search formulas.This file contains further details of methods to accompany
the paper Effectiveness of non-resuscitative first aid training forincreasing competence and helping behaviour in laypersons: Asystematic review by Stijn Van de Velde, Annemie Heselmans,Ann Roex, Philippe Vandekerckhove, Dirk Ramaekers and BertAertgeerts.Below we describe the search formula per consulted database.
We consulted the databases on 4 June 2007.MEDLINE (Pubmed)1. “First Aid”[mh] OR “Emergency
Treatment”[mh:NoExp] OR “EmergencyMedicine”[mh] OR “Emergency Nursing”[mh] OR“first aid”[tw] OR “first response”[tw] OR “prehospitalcare”[tw] OR “prehospital management”[tw] ORlifesupport*[tw] OR “life support*”[tw] ORlifesaving[tw] OR “life saving”[tw] OR “wildernessmedicine”[tw] OR “mountain rescue*”[tw]
2. ”Education”[mh] OR “Learning”[mh] OR educat*[tw]OR train*[tw] OR teach*[tw] OR instruct*[tw] ORlearn*[tw]
3. 1 AND 24. “Educational Measurement”[mh] OR “Health
Knowledge, Attitudes, Practice”[mh] OR“Knowledge”[mh] OR “Psychomotor Performance”[mh]OR “Competency-Based Education”[mh] ORknowledge[tw] OR attitude*[tw] OR skill*[tw] ORcompetenc*[tw] OR perform*[tw] OR abilit*[tw]
5. ”Retention (psychology)”[mh] OR retention[tw] ORretain*[tw] OR recall*[tw] OR maintenance[tw] ORmaintain*[tw] OR remember*[tw]
6. 4 OR 57. 3 AND 6EMBASE (EMBASE.com)1. (‘first aid’/de OR ‘emergency treatment’/de OR
‘emergency medicine’/de OR ‘emergency nursing’/deOR ‘first aid’:ab,ti OR ‘first response’:ab,ti OR‘prehospital care’:ab,ti OR ‘prehospital management’:ab,ti OR lifesupport*:ab,ti OR ‘life support*’:ab,ti ORlifesaving:ab,ti OR ‘life saving’:ab,ti OR ‘wildernessmedicine’:ab,ti OR ‘mountain rescue*’:ab,ti)
2. (‘Education’/exp OR ‘Learning’/exp OR educat*:ab,tiOR train*:ab,ti OR teach*:ab,ti OR instruct*:ab,ti ORlearn*:ab,ti)
3. 1 AND 24. (‘attitude to health’/de OR ‘knowledge’/exp OR
‘psychomotor performance’/exp OR knowledge:ab,ti ORattitude*:ab,ti OR skill*:ab,ti OR competenc*:ab,ti ORperform*:ab,ti OR abilit*:ab,ti)
5. long term memory’de OR retention:ab,ti OR retain*:ab,ti OR recall*:ab,ti OR maintenance:ab,ti ORmaintain*:ab,ti OR remember*:ab,ti
6. 4 OR 57. 3 AND 6
COCHRANE CENTRAL (Wiley)1. MeSH descriptor Emergency Treatment, this term
only2. MeSH descriptor First Aid, this term only3. MeSH descriptor Emergency Medicine explode all
trees4. MeSH descriptor Emergency Nursing explode all trees5. first aid OR “first response” OR “prehospital care” OR
“prehospital management” OR lifesupport* OR “lifesupport*” OR lifesaving OR “life saving” OR“wilderness medicine” OR “mountain rescue*”
6. OR 1-57. MeSH descriptor Education explode all trees8. MeSH descriptor Learning explode all trees9. educat* OR train* OR teach* OR instruct* OR
learn*10. OR 7-911. 6 AND 1012. MeSH descriptor Educational Measurement explode all
trees13. MeSH descriptor Health Knowledge, Attitudes,
Practice explode all trees14. MeSH descriptor Knowledge explode all trees15. MeSH descriptor Psychomotor Performance explode all
trees16. MeSH descriptor Competency-Based Education
explode all trees17. MeSH descriptor Retention (Psychology) explode all
trees18. knowledge OR attitude* OR skill* OR competenc* OR
perform* OR abilit* OR retention OR retain* ORrecall* OR maintenance OR maintain* OR remember*
19. OR 12-1820. 11 AND 19C2-SPECTR (Campbell Collaboration)1. {first aid} OR {first response} OR {prehospital care}
OR {prehospital management} OR {lifesupport} OR{life support} OR {lifesaving} OR {life saving} OR{wilderness medicine} OR {mountain rescue} OR{Emergency Treatment} OR {Emergency Medicine}OR {Emergency Nursing} [SEARCH ALL INDEXEDFIELDS]
2. {first aid} OR {first response} OR {prehospital care} OR{prehospital management} OR {lifesupport} OR {lifesupport} OR {lifesaving} OR {life saving} OR {wildernessmedicine} OR {mountain rescue} OR {EmergencyTreatment} OR {Emergency Medicine} OR {EmergencyNursing} [SEARCH ALL NON-INDEXED FIELDS]
3. 1 OR 2CINAHL (EBSCOhost)1. (MH “First Aid”) or (MH “First Aid (Iowa NIC)”) or
“first aid” or “first response” or lifesupport* or “lifesupport*” or lifesaving or “life saving” or “wildernessmedicine” or “mountain rescue*”
457.e1 Annals of Emergency Medicine Volume , . : September
39
svelde
Rechthoek

2. (MH “Education1”) or (MH “Learning1”) or educat*OR train* OR teach* OR instruct* OR learn*
3. 1 AND 24. (MH “Educational Measurement1”) or (MH“Knowledge1”) or (MH “Health Knowledge andBehavior (Iowa NOC) (Non-Cinahl)1”) or (MH“Education, Competency-Based”) or (MH “PsychomotorPerformance1”) or (MH “Student PerformanceAppraisal1”) OR knowledge OR attitude* OR skill* ORcompetenc* OR perform* OR abilit*
5. (MH “Skill Retention”) OR retention OR retain* ORrecall* OR maintenance OR maintain* OR remember*
6. 4 0R 57. 3 AND 6
BRITISH NURSING INDEX AND ARCHIVE (OVID)1. first aid/ or “accident and emergency nursing”/ or (”firstaid” or “first response” or “prehospital care” or“prehospital management” or lifesupport$ or lifesupport$ or lifesaving or life saving or wildernessmedicine or mountain rescue$).mp. [mp5title, abstract,heading words]
2. (educat$ or train$ or teach$ or instruct$ or learn$).mp.[mp5title, abstract, heading words]
3. 1 AND 24. knowledge OR attitude$ OR skill$ OR competenc$ OR
perform$ OR abilit$5. retention OR retain$ OR recall$ OR maintenance OR
maintain$ OR remember$6. 4 OR 57. 3 AND 6
SPORTSDISCUS (EBSCOhost)1. (DE “FIRST aid in illness & injury”) or (DE
“EMERGENCY medicine”) or “first aid” OR “firstresponse” OR “prehospital care” OR “prehospitalmanagement” OR lifesupport* OR “life support*” ORlifesaving OR “life saving” OR “wilderness medicine”OR “mountain rescue*”
2. DE “EDUCATION” OR DE “HEALTH education”OR DE “OUTDOOR education” OR DE “PHYSICALeducation & training” OR DE “SPECIAL education” orDE “TRAINING” or DE “TEACHING” OR educat*OR train* OR teach* OR instruct* OR learn*
3. 1 AND 24. DE “PERFORMANCE” OR DE “JOB performance”
OR knowledge OR attitude* OR skill* OR competenc*OR perform* OR abilit*
5. retention OR retain* OR recall* OR maintenance ORmaintain* OR remember*
6. 4 OR 57. 3 AND 6PsycINFO (WebSPIRS)1. ”first aid” or “first response” or “prehospital care” or
“prehospital management” or lifesupport* or “life
support*” or lifesaving or “life saving” or “wildernessmedicine” or “mountain rescue*”
2. (explode “Teaching-” in MJ,MN) or (explode “Training-” in MJ,MN) or (explode “Learning-” in MJ,MN) or(explode “Education-” in MJ,MN) or (educat* or train*or teach* or instruct* or learn*)
3. 1 AND 24. (knowledge or attitude* or skill* or competenc* orperform* or abilit*) or ((explode “Ability-1” in MJ,MN)or (explode “Competence-” in MJ,MN) or (explode“Performance-1” in MJ,MN)) or (explode “Knowledge-Level” in MJ,MN) or ((”Health-Attitudes” in MJ,MN)or (”Health-Behavior” in MJ,MN) or (”Health-Knowledge” in MJ,MN)) or (explode “Educational-Measurement” in MJ,MN)
5. ”Retention (psychology)”[mh] OR retention[tw] ORretain*[tw] OR recall*[tw] OR maintenance[tw] ORmaintain[tw] OR remember*[tw]
6. 4 OR 57. 3 AND 6ERIC (EBSCOhost)1. DE “First Aid” OR “first aid” OR “first response” ORlifesupport* OR “life support*” OR lifesaving OR “lifesaving” OR “wilderness medicine” OR “mountainrescue*”
2. (DE “Education” OR DE “Academic Education” ORDE “Adult Education” OR DE “After SchoolEducation” OR DE “Aging Education” OR DE “AlliedHealth Occupations Education” OR DE “CitizenshipEducation” OR DE “Coeducation” OR DE“Community Education” OR DE “ComparativeEducation” OR DE “Compensatory Education” ORDE “Competency Based Education” OR DE“Compulsory Education” OR DE “CorporateEducation” OR DE “Correctional Education” OR DE“Distance Education” OR DE “Driver Education” ORDE “Early Childhood Education” OR DE “ElementarySecondary Education” OR DE “Family LifeEducation” OR DE “Health Education” OR DE“Industrial Education” OR DE “Informal Education”OR DE “Inservice Education” OR DE “IntergroupEducation” OR DE “Leisure Education” OR DE“Migrant Education” OR DE “NoncategoricalEducation” OR DE “Nondiscriminatory Education”OR DE “Nonformal Education” OR DE“Nontraditional Education” OR DE “OpenEducation” OR DE “Outcome Based Education” ORDE “Outdoor Education” OR DE “Patient Education”OR DE “Physical Education” OR DE “PoliceEducation” OR DE “Popular Education” OR DE“Population Education” OR DE “PostsecondaryEducation” OR DE “Process Education” OR DE“Professional Education” OR DE “ProgressiveEducation” OR DE “Public Education” OR DE “Rural
Volume , . : September Annals of Emergency Medicine 457.e2
40
svelde
Rechthoek

Education” OR DE “Safety Education” OR DE“Special Education” OR DE “SupplementaryEducation” OR DE “Urban Education” OR DE“Values Education” OR DE “Vocational Education”OR DE “Womens Education”)
3. (DE “Learning” OR DE “Active Learning” OR DE“Adult Learning” OR DE “Associative Learning” ORDE “Aural Learning” OR DE “Cooperative Learning”OR DE “Discovery Learning” OR DE “DiscriminationLearning” OR DE “Experiential Learning” OR DE“Incidental Learning” OR DE “Intentional Learning”OR DE “Lifelong Learning” OR DE “MasteryLearning” OR DE “Multisensory Learning” OR DE“Nonverbal Learning” OR DE “ObservationalLearning” OR DE “Prior Learning” OR DE “ProblemBased Learning” OR DE “Rote Learning” OR DE“Sequential Learning” OR DE “Serial Learning” ORDE “Transfer of Training” OR DE “TransformativeLearning” OR DE “Verbal Learning” OR DE “VisualLearning”)
4. (DE “Instruction” or DE “Assignments” OR DE“College Instruction” OR DE “Concept Teaching” ORDE “Group Instruction” OR DE “Home Instruction”OR DE “Individual Instruction” OR DE “MassInstruction”)
5. (DE “Training” OR DE “Caregiver Training” OR DE“Industrial Training” OR DE “Job Training” OR DE“Laboratory Training” OR DE “Military Training” ORDE “Professional Training” OR DE “Retraining” ORDE “Volunteer Training”)
6. OR 2-57. 1 AND 68. DE “Knowledge Level” or DE “Ability” OR DE
“Cognitive Ability” OR DE “Competence” OR DE“Skills” or DE “Performance” OR DE “JobPerformance” OR DE “Attitudes” OR knowledge ORattitude* OR skill* OR competenc* OR perform* ORabilit*
9. DE “Recall (Psychology)” or DE “Retention(Psychology)” OR retention OR retain* OR recall* ORmaintenance OR maintain* OR remember*
10. 8 OR 911. 7 AND 10
APPENDIX E2. EPOC quality criteria for randomizedcontrolled trials.This file contains further details of methods to accompany
the paper Effectiveness of non-resuscitative first aid training forincreasing competence and helping behaviour in laypersons: Asystematic review by Stijn Van de Velde, Annemie Heselmans,Ann Roex, Philippe Vandekerckhove, Dirk Ramaekers and BertAertgeerts.Below we list the EPOC Quality criteria for randomised
controlled trials. (Extract from the following reference :
Cochrane Effective Practice and Organisation of Care Group.The data collection checklist. Available at:http://www.epoc.uottawa.ca/checklist2002.doc.)Seven standard criteria are used for randomised controlled
trials and controlled clinical trials included in EPOC reviews:a) Concealment of allocation (protection against selection bias)Score DONE if the unit of allocation was by institution,
team or professional and any random process is describedexplicitly, e.g. the use of random number tables or coin flips; theunit of allocation was by patient or episode of care and therewas some form of centralised randomisation scheme, an on-sitecomputer system or sealed opaque envelopes were used.Score NOT CLEAR if the unit of allocation is not described
explicitly; the unit of allocation was by patient or episode of careand the authors report using a ‘list’ or ‘table’, ‘envelopes’ or‘sealed envelopes’ for allocation.Score NOT DONE if the authors report using alternation
such as reference to case record numbers, dates of birth, day ofthe week or any other such approach (as in CCTs);the unit of allocation was by patient or episode of care and
the authors report using any allocation process that is entirelytransparent before assignment such as an open list of randomnumbers or assignments; allocation was altered (by investigators,professionals or patients).b) Follow-up of professionals (protection against exclusion bias)Score DONE if outcome measures obtained for 80-100% of
subjects randomised. (Do not assume 100% follow up unless statedexplicitly.); Score NOT CLEAR if not specified in the paper; ScoreNOTDONE if outcome measures obtained for less than 80% ofsubjects randomised.c) Follow-up of patients or episodes of careScore DONE if outcome measures obtained for 80-100% of
subjects randomised or for patients who entered the trial. (Do notassume 100% follow up unless stated explicitly.) Score DONE ifthere is an objective data collection system; Score NOT CLEAR ifnot specified in the paper; Score NOTDONE if outcomemeasures obtained for less than 80% of subjects randomised or forless than 80% of patients who entered the trial.d) Blinded assessment of primary outcome(s)* (protection
against detection bias)Score DONE if the authors state explicitly that the primary
outcome variables were assessed blindly OR the outcomevariables are objective, e.g. length of hospital stay, drug levels asassessed by a standardised test; Score NOT CLEAR if notspecified in the paper; Score NOT DONE if the outcome(s)were not assessed blindly.* Primary outcome(s) are those variables that correspond to
the primary hypothesis or question as defined by the authors. Inthe event that some of the primary outcome variables wereassessed in a blind fashion and others were not, score eachseparately and label each outcome variable clearly.e) Baseline measurementScore DONE if performance or patient outcomes were
measured prior to the intervention, and no substantial differences
457.e3 Annals of Emergency Medicine Volume , . : September
41
svelde
Rechthoek

were present across study groups; Score NOT CLEAR if baseline
measures are not reported, or if it is unclear whether baseline
measures are substantially different across study groups; Score
NOTDONE if there are differences at baseline in main outcome
measures likely to undermine the post intervention differences (e.g.
are differences between the groups before the intervention similar
to those found post intervention).
f) Reliable primary outcome measure(s)*
Score DONE if two or more raters with at least 90% agreement
or kappa greater than or equal to 0.8 OR the outcome is obtained
from some automated system e.g. length of hospital stay, drug
levels as assessed by a standardised test; Score NOT CLEAR if
reliability is not reported for outcome measures that are obtained
by chart extraction or collected by an individual; Score NOT
DONE if agreement is less than 90% or kappa is less than 0.8.
* In the event that some outcome variables were assessed in a
reliable fashion and others were not, score each separately on the
back of the form and label each outcome variable clearly.
g) Protection against contamination
Score DONE if allocation was by community, institution or
practice and it is unlikely that the control received the intervention;
Score NOT CLEAR if professionals were allocated within a clinic
or practice and it is possible that communication between
experimental and group professionals could have occurred;
Score NOT DONE if it is likely that the control group
received the intervention (e.g. cross-over trials or if patients
rather than professionals were randomised).
APPENDIX E3. Data and comparisons.This file contains further details of methods to accompany
the paper Effectiveness of non-resuscitative first aid training for
increasing competence and helping behaviour in laypersons: A
systematic review by Stijn Van de Velde, Annemie Heselmans,
Ann Roex, Philippe Vandekerckhove, Dirk Ramaekers and Bert
Aertgeerts.
Below we describe the comparisons and data used to calculate
RR or MD.
Kelly 2003
Knowledge of the Poison Control Center telephone number
(First aid training versus Controls)
Intervention
n
Intervention
N
Control
n
Control
N
91 145 27 144
Knowledge of first aid for ingestion of household bleach
(First aid training versus Controls)
Intervention
n
Intervention
N
Control
n
Control
N
102 145 48 144
Moore 1987
Knowledge of first aid for multiple cases (First aid training
versus Controls)
Intervention
N
Intervention
Mean
Intervention
SD
Control
N
Control
Mean
Control
SD
22 11.92 3.43 23 7.17 2.35
Shotland 1985
Helping rates for bleeding (First aid training versus Controls)
Intervention
n
Intervention
N
Control
n
Control
N
51 80 47 83
Helping rates for bleeding (Unambiguous versus Ambiguous
situation)
Unambiguous
n
Unambiguous
N
Ambiguous
n
Ambiguous
N
64 82 34 81
Helping rates for bleeding (Alone versus Group situation)
Alone n
Alone
N
Group
n
Group
N
56 83 42 80
Adequate first aid for bleeding (First aid training versus
Controls)
Intervention
n
Intervention
N
Control
n
Control
N
25 80 1 83
Hawks 1998
Helping rates for chest pain (Training in first aid and helping
behaviour versus Controls)
Intervention
n
Intervention
N
Control
n
Control
N
13 29 2 17
Helping rates for chest pain (Training in first aid and helping
behaviour (small measure) versus Controls)
Intervention
n
Intervention
N
Control
n
Control
N
7 27 2 17
Volume , . : September Annals of Emergency Medicine 457.e4
42
svelde
Rechthoek

Helping rates for chest pain (First aid training only versusControls)
Intervention
n
Intervention
N
Control
n
Control
N
4 25 2 17
Helping rates for chest pain (Training in first aid and helpingbehaviour versus First aid training only)
Intervention
n
Intervention
N
Intervention
(3) n
Intervention
(3) N
13 29 4 25
457.e5 Annals of Emergency Medicine Volume , . : September
43
svelde
Rechthoek

44

CHAPTER 4
Does training on barriers to helping facilitate emergency
helping behaviour among laypersons trained in first aid?
A randomised deception trial
Stijn Van de Velde, Ann Roex, Karoline Vangronsveld, Lidewij Niezink, Koen Van
Praet, Annemie Heselmans, Peter Donceel, Philippe Vandekerckhove, Dirk
Ramaekers, Bert Aertgeerts. Does training on barriers to helping facilitate
emergency helping behaviour among laypersons trained in first aid? A
randomised deception trial. Article submitted.
45

Abstract
Objective To investigate the effect of conventional first aid training versus
conventional training plus a supplementary training module to decrease
barriers to helping.
Design A randomised controlled trial with deception where the participants
were unaware that an acute myocardial infarction was simulated and did not
know that their helping behaviour was being evaluated.
Setting Ten training courses organised by six local Red Cross branches.
Participants 144 participants, from 18 years onwards, without formal medical
education or profession.
Interventions All participants first received 24 hours conventional first aid
training. According to random number lists, participants then either attended
an experimental lesson with a training module to reduce barriers to helping or
followed an active control lesson. Both the experimental and control training
lasted two hours.
Main outcome measures During the deception test we assessed how much
time elapsed between the start of the simulation and seeking help (primary
outcome). Other main outcomes measured were the rate of helping actions,
and first aid self-efficacy beliefs. Two persons, blinded towards group status,
independently extracted data from the video recordings of the deception test.
Results We randomised 72 participants to both the experimental and control
group. 22 participants were included in the analysis for the experimental group
and 36 in the control group. We found no statistically or clinically significant
differences between the experimental and control group for any of the
measures. The time until seeking help (geometrical mean and 95% confidence
46

interval) was 55.5 seconds (42.9 to 72.0) in the experimental group and 56.5
(43.0 to 74.3) in the control group. All participants showed some kind of helping
reaction. About 57% (n=33) of the participants asked a bystander to seek help,
40% (n=23) left the victim to seek help themselves, and 3% (n=2) did not seek
any help within the allocated 3 minutes. Participants indicated a mean self-
efficacy score of 25.2 (23.9 to 26.6) in the experimental group and 24.4 (23.0 to
25.8) in the control group. The self-efficacy score did not correlate with the
time-related outcomes.
Conclusion Supplementary training on dealing with barriers to helping did not
alter the time or rate of helping in an acute myocardial infarction emergency.
Despite the very high helping rates, there is still a need to increase the
timeliness and appropriateness of the aid provided. First aid self-efficacy beliefs
did not appear to be a useful predictor of performance.
Trial registration Clinical Trials NCT00954161
Introduction
Training laypersons in first aid is widely advocated to save lives. To achieve this
goal the training must improve knowledge, attitudes, and skills, and the trainees
must use these abilities appropriately in case of emergency. Despite the general
belief in the potential of first aid training, a systematic review of the
effectiveness of non-resuscitative first aid training showed that it does not
always translate into helping behaviour.1 Three trials used deception
experiments to evaluate the helping behaviour for bleeding and heart attack
emergencies after first aid training.2-4 The deception implied that the
participants were unaware of any simulation and did not know that their
helping behaviour was being evaluated. These trials showed that laypersons
trained in first aid provided better help,2 but did not help more often than
47

untrained laypersons.2;4 These trials also found that conventional first aid
training was less effective than training supplemented by a training module that
concentrated on the obstacles to action.3;4 The systematic review concluded
that conventional first aid training improved competences but not performance,
and that supplementary training on dealing with barriers to helping might
enhance helping behaviour.1 The conclusions are only tentative because the
evidence was of low quality and are limited to university student populations in
the U.S.1
Social-psychological research has extensively documented the role of different
factors such as individual differences, victim characteristics, presence of other
bystanders, and situational ambiguity on bystander helping behaviour.5-7
Barriers to helping identified in surveys among laypersons include fear of
causing further harm, legal consequences, disease transmission, and increasing
the burden on the emergency medical services without good reason.8-10
We integrated the information on bystander helping behaviour in a training
module to decrease barriers to helping. This module can be given in addition to
conventional first aid training. This study aimed to investigate the effect of
conventional first aid training versus conventional training plus this
supplementary training module in a community-based randomised controlled
trial. Our primary hypothesis was that the time until seeking help is shorter
among people trained with the supplementary intervention.
Having the confidence to provide first aid may influence helping barriers. We
therefore also measured the participants’ self-efficacy beliefs11;12 and related
these to the performance demonstrated in the deception. While deception is a
useful instrument to test first aid performance, this technique runs the potential
risk of creating mistrust or harm from high stress levels.13 For that reason this
study also evaluated the impact of the deception on the participants.
48

Methods
Participants
Belgian Red Cross-Flanders provides first aid training at almost 300 local
branches which are supported and coordinated by its central services. Red Cross
staff recruited study participants from September 2009 until October 2010
during the first lesson of 10 first aid training courses organised by six branches
(Mechelen, Muizen, Duffel, Kampenhout-Herent, Sint-Katelijne-Waver, Lier).
The selection of branches was based on proximity to the headquarters of the
Belgian Red Cross-Flanders. Participants had a minimum age of 18 years and
were not allowed to follow additional first aid training outside the study. We
excluded health care students and professionals from the study. Participants
that completed the full study protocol received a gift coupon to the value of
€40. The follow-up ended in January 2011.
Informed consent
At the start of the study, we obtained informed consent for a study to test first
aid self-efficacy after attending one of two new training lessons and for an
apparently separate study on driving proficiency. Immediately after the
deception test we provided a third informed consent form in which we notified
participants about the deception.
Design
An investigator, who was not involved in the enrollment of study participants,
used random number lists obtained from www.randomisation.com to allocate
participants. The randomisation was done per branch, assuring an equal
number of enrolled participants per group (if the number of participants was
even). All participants first received conventional first aid training. Participants
then either attended an experimental lesson with a training module to reduce
barriers to helping or followed an active control lesson. We informed
participants that both lessons were newly developed and had to be evaluated.
49

They received no information about the scope of these lessons until they
started.
The conventional first aid training programme was a 24-hour course which
covered first aid procedures for the most important emergencies including
acute myocardial infarction. Teaching methods included lectures, skills practice
on manikins or other participants, and exercises with simulated patients. No
more than 20 participants were allowed per course. The participants were able
to take a written and practical exam to assess competence, but this was not
obligatory. Volunteer trainers gave the programme over two to three month
periods. All trainers were trained in facilitation learning and assessment.
Intervention
The experimental training module aimed to sensitise participants towards a
helping reaction and to reduce barriers to helping. Instructional methods
included: a) Group work and discussion on the likelihood of witnessing an emergency
situation; personal experiences with emergencies; moral aspects of helping;
feelings and perspectives of the victim and bystanders; barriers to helping
behaviour, and how to deal with them.
b) Role play for specific situations where barriers to helping are present.
c) Formulation and writing down of personal helping goals.
In addition, the participants received a booklet containing information on
barriers to helping and how to deal with them.
The active control training focussed on first aid for alcohol and drug incidents
and was an extension of the conventional first aid training.
Both the experimental and control training lasted two hours and took place one
week after completion of the conventional training programme. The maximum
number of participants per group was ten. One professional first aid trainer
gave all the experimental and control lessons.
50

Deception test
Within one month of the experimental or control training, we assessed each
study participant individually during a deception test at the headquarters
(Mechelen) of the Belgian Red Cross-Flanders. We deceived participants by
making them believe that they were participating in a driving proficiency test.
Upon arrival, participants placed their mobile phones in a locker and went to
the test room. This room contained four chairs placed side by side in front of a
games computer with a steering wheel, and accelerator and brake pedals. The
study participant took a seat in the middle next to the imminent ‘victim’. Two
actors in the role of passive bystanders sat at the sides. The actors were blinded
towards group status. The test supervisor left the room while the participants
practised on the computer game. Shortly after this the victim started the
simulation by grabbing his chest and imitating shortness of breath. The victim
also had a pale and sweaty appearance. The other actors reacted as if they were
concerned but did not know what to do. When a help-seeking reaction
occurred, or after 3 minutes without a help-seeking reaction, the test supervisor
informed the participant about the deception and the reasons for the test. A
hidden camera filmed the assessment. A counsellor specialised in supporting
people involved in distressing situations facilitated a defusing immediately after
the test.13 Content experts and researchers in medical education, experimental
psychology and social psychology evaluated the test scenario before the trial.
Outcomes
At baseline, we collected data on socio-demographic factors and scores on a
multiple choice test measuring the knowledge about procedures for various first
aid situations.
Outcomes measured directly after the experimental or control training
comprised first aid self-efficacy beliefs and satisfaction. The satisfaction
questionnaire consisted of seven statements relating to novelty,
comprehensibility, clarity, applicability of the information, teaching quality,
group dynamics, and overall satisfaction.
51

During the deception test we assessed the primary outcome, i.e. the time until
seeking help. The time was measured between the start of the simulation and a
person leaving the room to get help. This person could either be the study
participant or an actor who had been instructed by the participant to get help.
When no help-seeking action occurred after three minutes, the test was
aborted. Post hoc, we decided to explore how much time elapsed between a)
the start of the simulation and visual notice of the emergency by the
participant: detection delay, b) notice and any helping response: response
delay, and c) notice and seeking help: help-seeking delay. A helping response
was defined as either assessing the victim, seeking help, or providing direct help
to the victim. Two persons, blinded towards group status, independently
extracted data from the video recordings. Any differences were discussed and
verified on the recordings.
Other outcomes measured during the deception test were the rate of helping
actions, credibility and impact of the deception, and state of positive and
negative mood after being told about the deception. For the state of mood
participants indicated how they felt in relation to five positive and five negative
mood items: nervous, enthusiastic, confused, strong, ashamed, determined,
anxious, proud, angry, and inspired. The latter scale was based on the Positive
And Negative Affect Schedule.14
The participants rated self-efficacy, satisfaction, credibility, impact of deception,
and state of positive and negative mood on a Likert scale.
Sample size and statistical analysis
We estimated that we would need 25 participants in both the experimental and
control group to detect a difference in mean delay time for seeking help of 30
seconds for a power of 80 % at a 5% level of significance, a standard deviation
of 37 seconds and a control/experimental patient ratio of 1. We based the
52

estimated data required for the sample size calculation on the raw data from a
study published by Hawks3. We periodically monitored whether the target
number of participants for the analysis had been reached and then decided if
new participants had to be enrolled.
Responses to items regarding self-efficacy, satisfaction, and positive and
negative mood were summed up per scale to yield composite scores. When a
specific item was not answered, we imputed the mean individual score for the
other completed items in the scale. For the time-related variables we applied a
logarithmic transformation (natural logarithm) to obtain a symmetric
distribution of the model residuals. We reported the geometric mean values
and 95% confidence intervals in both groups after back-transforming
(exponential function) to the original scale.
We used descriptive statistics for the baseline variables, rate of helping, various
types of helping actions, credibility scores, the impact of event, the state of
mood, and satisfaction. We used Cronbach's alpha to evaluate the reliability of
the self-efficacy and training satisfaction scale. To evaluate the time-related
variables and the self-efficacy scores, we used a two-way ANOVA. The first
factor was the training branch; the second factor was the comparison group.
Since the training branch was not an effect modifier, we reported the effect for
all the training branches together. By calculating the Spearman’s correlation
coefficient we evaluated the relationship between scores on the self-efficacy
beliefs and the time-related variables. We initially planned to compare the rate
of helping in both groups and to evaluate the relationship between scores on
the self-efficacy beliefs and the rate of helping. Since all participants showed
some type of helping reaction this was no longer relevant.
We analysed the data per protocol. This means that we analysed the
participants according to the group they actually attended. Because suspicion
about the deception test might influence helping behaviour, we excluded
participants that reported credibility scores below four. An intention-to-treat
analysis was not considered, since participants only switched groups when the
timeslot was not convenient for them.
53

P-values are two-sided and considered significant if smaller than 0.05. We used
PASW Statistics 18 (SPSS) for the statistical analysis.
Results
The median (IQR) number of days between the experimental or control training
and the deception test was 7 (5.5 to 11.5) days. Figure 1 illustrates the
participant flow in the trial. We randomised 72 participants to both the
experimental and control group. Fifteen participants switched from group
because the timeslot of the allocated group was inconvenient for them. The
most important reason for dropping out before the interventions was lack of
time. More participants dropped out in the experimental arm versus the
controls. Time-related factors and bad weather with heavy snowfall were the
main cause of this imbalance. We excluded two participants because they had
prior knowledge of the deception. Nine participants were not included in the
analysis because they did not find the deception sufficiently credible. One
person who did not notice the emergency was also excluded.
54

Figure 1: Flow of participants in the trial.
55

Table 1 presents the baseline data for the randomised participants per allocated
group, and for the participants included in the analysis per attended group.
Baseline data are similar per allocated and per analysed group. Participants that
switched groups were mainly female, in a relationship, and older.
Experimental group (n=72)
Active control group (n=72)
Analysed in experimental group (n=22)
Analysed in active control group (n=36)
Sex (female) 48 (66.7%) 48 (66.7%) 17 (77.3%) 25 (69.4%)
Age (years) 32.9 (24.4 – 41.6)
31.8 (23.3 – 42.9)
27.0 (22.5 - 40.8)
26.7 (21.9 - 38.7)
Nationality
(Belgian)
69 (95.8%) 69 (100%) 21 (95.5%) 36 (100%)
Education
Primary
Secondary
Higher
2 (2.8%)
35 (48.6%)
35 (48.6%)
0 (0%)
38 (52.8%)
34 (47.2%)
0 (0%)
9 (40.9%)
13 (59.1%)
1 (2.8%)
19 (52.8%)
16 (44.4%)
Profession
Employed
Retired/disabled
Housewife
Unemployed
Student
51 (70.8%)
4 (5.6%)
1 (1.4%)
3 (4.2%)
13 (18.1%)
44 (61.1%)
2 (2.8%)
3 (4.2%)
7 (9.7%)
16 (22.2%)
12 (54.5%)
2 (9.1%)
1 (4.5%)
0 (0%)
7 (31.8%)
24 (66.7%)
0 (0%)
1 (2.8%)
4 (11.1%)
7 (19.4%)
Table 1: Summary statistics in allocated and attended groups. Medians (Q1-Q3) or frequencies are reported.
56

Experimental group (n=72)
Active control group (n=72)
Analysed in experimental group (n=22)
Analysed in active control group (n=36)
Relationship status (no partner)
38 (52.8%) 33 (45.8%) 12 (54.5%) 20 (55.6%)
Red Cross volunteer (no)
66 (91.7%) 63 (87.5%) 18 (81.8%) 34 (94.4%)
Previous first aid training (no)
49 (68.1%) 44 (61.1%) 13 (59.1%) 24 (66.7%)
Experienced a life-threatening emergency (no)
56 (77.8%) 49 (68.1%) 18 (81.8%) 27 (75.0%)
Multiple choice test score (max. possible score=18)
9 (7 – 10) 8 (7 – 10) 10 (7 – 12) 8 (7 – 11)
Table 1: Continued.
We found no statistically or clinically significant differences between the
experimental and control group for any of the measures. Table 2 shows the
results for the time-related outcomes per analysed group. The ratio of the time
until seeking help in the control group versus the experimental group was 1.02
(95% CI 0.71 to 1.35).
Experimental group (n=22)
Active control group (n=36)
Time between start of simulation and seeking help
55.5 (42.9 – 72.0) 56.5 (43.0-74.3)
Detection delay 15.0 (10.2-22.3) 18.3 (12.1-27.8)
Response delay 4.0 (2.2 – 7.3) 4.8 (2.6 – 9.1)
Help-seeking delay 37.5 (27.7-50.8) 31.7 (23.0 – 43.7)
Table 2: Geometrical means and 95% confidence intervals for time-related
57

variables (seconds).
All participants showed some kind of helping reaction. Nearly all participants
asked the victim what was wrong and took measures to obtain help. About 57%
(n=33) asked a bystander to seek help, 40% (n=23) left the victim to seek help
themselves, and 3% (n=2) did not seek any help within the allocated 3 minutes.
Table 3 reports the results per analysed group.
Experimental group
(n=22)
Active control group (n=36)
Any helping reaction (yes) 22 (100%) 36 (100%)
Asking victim what is wrong (yes) 21 (95.5%) 34 (94.4%)
Seeking help
By study participant
By bystander (at request of study
participant)
By nobody
9 (40.9%)
12 (54.5%)
1 (4.5%)
14 (38.9%)
21 (58.3%)
1 (2.8%)
Asking about medication use (yes) 1 (4.5%) 2 (5.6%)
Attention to body position of victim (yes)
10 (45.5%) 12 (33.3%)
Telling the victim to stay calm (yes) 8 (36.4%) 10 (27.8%)
Table 3: Frequencies of types of helping reactions
Most participants found the deception test rather impactful with an overall
median (IQR) score of 4 (3 to 5). We found substantially higher median (IQR)
scores for the positive mood affect, 18.5 (15 to 20), than for the negative mood
affect, 8 (6 to 10) (possible range= 5 to 25). The positive and negative mood
items with the highest score were feeling proud with median (IQR) score of 4 (3
to 5), and feeling nervous, 2 (2 to 3). Five participants indicated being either
very nervous (n=3), confused (n=2), ashamed (n=1), anxious (n=1), or angry
(n=1). One person indicated the maximum score on every negative mood
58

question.
Participants indicated a mean (95% CI) self-efficacy score of 25.2 (23.9 to 26.6)
in the experimental group and 24.4 (23.0 to 25.8) in the control group (Possible
range= 6 to 30; Cronbach’s alpha = 0.68). The self-efficacy score did not
correlate with the time-related outcomes. The experimental training group
scored a median (IQR) of 21.5 (12 to 24) on the satisfaction scale (Possible
range= 7 to 28 ; Cronbach’s alpha = 0.94) versus a median (IQR) of 18.5 (12 to
26) in the control group.
Discussion
The experimental training on dealing with barriers to helping did not alter the
time or rate of helping. The good news is that all the participants demonstrated
some type of helping reaction and nearly all the participants sought help within
three minutes after the start of the simulation. Ten percent remained passive
for more than one minute, which was an awfully long time in the context of this
study. Although the first aid training curriculum teaches participants to stay
with the victim if bystanders are available to seek help, almost 40% left the
victim to seek help themselves. This might be a flight reaction in response to the
acutely stressful situation.
While our results regarding the time to helping response were similar to the
findings of Hawks et al,3 we made some divergent observations regarding the
rate of helping behaviour. It is remarkable that we found a 100% helping rate in
our study versus 16% and 45% in the trials by Hawks.3;4 However, the trials
differed in several ways. Participants in our community-based study were older
and included more women than the student-based studies by Hawks. The
studies by Hawks took place in the United States, while ours was conducted in
Europe. The diffusion of responsibility to help might have played a greater role
in the studies by Hawks, with four to five passive bystanders versus two in our
59

study. The emergency might have been more ambiguous in the Hawks studies,
where the victim periodically grabbed for his heart and tried to catch his breath.
In our study, the victim simulated the same signs but on a continuous basis,
which might have made the emergency more explicit. In the studies by Hawks,
participants had two minutes to respond to the emergency, versus three
minutes in our trial. Even after two minutes we found a 93% helping rate.
Almost half of the participants in Hawks 1992 were moderately to extremely
suspicious about the deception test.3 This proportion was considerably higher
than in our study (13%). Moreover, Hawks did not exclude these participants
from the analysis. The study by Hawks 1998 did not measure credibility but
used the same scenario for the deception test.4 In our study most participants
were assessed within two weeks after the intervention versus within one4 or
two months3. The level of prior first aid training might also have differed, but
this was not clear from the manuscripts.
The first aid self-efficacy beliefs were on average high, but did not predict the
performance during the deception test. This corresponds with other studies
which found that self-assessment of performance is often substantively
flawed.15
The satisfactory positive and negative mood scores, collected after the
participants were told about the deception, provide support for their use in new
trials on the helping behaviour of first aid trainees.
Strengths and limitations of the study
To get the required sample size, we had to oversample substantially. Forty
percent of the enrolled participants dropped out before taking part in the
experimental or control training. This high number is consistent with the drop-
out rates in general for this training. Considering the community-based setting,
the non-obligatory character of the training and the option to follow only part
of it, the resulting adequately powered study can be seen as a strength.
60

Although we found no difference in baseline data between those analysed and
those who dropped out (results not reported), it is possible that unmeasured
factors such as personality traits might have been important. Those participants
for whom the experimental training may have been most beneficial, might have
dropped out. We lost more participants in the experimental group than the
control group. This difference can be explained by the sign-up procedure for the
deception experiment. In the first year of the trial we asked the participants to
sign up at the end of the control or experimental training. Since the active
control training always preceded the experimental training, the control
participants were able to select the most convenient timeslots on the timetable.
In the last part of the trial, we presented the timetable before the participants
attended the experimental or control training. After this correction the loss to
follow-up became similar in both groups. Despite the high number of drop-outs
the comparability of the two groups remained intact. The experimental training
may have been weakened by the high drop-out rates, since it relied on the
contribution of participants in group discussions and role plays. It was not
always possible to give this training according to the didactical plan because of
the very small training groups. Another element which might have diluted the
effect of the intervention was that trainers were not restricted to talking about
helping behaviour during the preceding 24 hours of first aid training. Although
the didactical plan for this course did not fully address helping behaviour,
trainers may have incorporated it. Contamination between the study groups
may also have diluted any effect.
A strength of this study is the evaluation of the effects of the deception test on
the participants. Although deception is common in social-psychological
research, this aspect is not typically evaluated.13
Meaning of the study
This trial found no difference in time or rate of helping between conventional
61

first aid training and conventional training plus a supplementary training to
reduce barriers to helping. The high loss to follow-up was an important
limitation of this study making it difficult to derive conclusions. Despite the very
high rates of seeking help or providing help in general, there is still a need to
increase the timeliness and appropriateness of the aid provided. Help-seeking
represented both actions to obtain professional medical care or help from the
test supervisor. From the findings it is not clear how many participants would
actually have called for professional medical help. Since the participants were
focusing on the driving test, the detection delay might have been longer than in
more normal conditions. With regard to first aid self-efficacy beliefs, we
conclude that these were not useful to predict performance during an
emergency.
Deception in future research
The deception test did not have a negative impact on the study participants and
can be used in new trials on emergency helping behaviour of first aid trainees.
In this trial we used deception as a tool to evaluate the effectiveness of a
training intervention. Some study participants informed us that the deception
test was a learning experience for them. An RCT with medical students found
that feedback from unannounced simulation patients was a highly effective
educational method in itself.16 When conducting other trials about first aid
training, it might also be interesting to evaluate the potential of the deception
test as a teaching tool. The main first aid training course in the RCT offered
formal assessment leading to a certificate of first aid competence. To our
knowledge, the predictive validity of such a formal assessment for actual
helping behaviour still needs to be assessed. A deception test could be used as a
reference standard for this purpose.
62

What is already known on this topic
A systematic review tentatively concluded that conventional first aid training
improved competences but not performance. Supplementary training on
dealing with barriers to helping might increase helping rates.
The available evidence is of low quality and limited to university student
populations in the U.S.
What this study adds
This community-based trial found that supplementary training on dealing with
barriers to helping did not alter the time or rate of helping in an acute
myocardial infarction emergency.
Despite the very high helping rates, there is still a need to increase the
timeliness and appropriateness of the aid provided.
First aid self-efficacy beliefs were not useful to predict performance.
Competing interest: All authors have completed the Unified Competing Interest
form at www.icmje.org/coi_disclosure.pdf (available on request from the
corresponding author) and declare that (1) PV, SVDV, KVP are employed and KV
volunteers in the Belgian Red Cross-Flanders which provides training in first aid
and which received funding for this study from the Laerdal Foundation for Acute
Medicine; (2) AH, AR, BA, DR, LN, and PD have no relationships with companies
that might have an interest in the submitted work in the previous 3 years; (3)
their spouses, partners, or children have no financial relationships that may be
relevant to the submitted work; and (4) AH, AR, BA, DR, LN, PD have no non-
financial interests that may be relevant to the submitted work.
Contributions: SVDV, BA, and DR conceived and designed the study. SVDV
wrote the protocol. BA and DR gave methodological advice. AR provided a
medical education perspective. KV provided an experimental clinical and health
63

psychology perspective. LN provided a social psychology perspective. KVP
provided a psycho-social support perspective. PV, PD, AH provided general
advice on the study. BA was the guarantor of the study.
Ethical approval: Ethics committee approval for this study was obtained from
the University Hospitals Leuven Medical Ethics Committee. Participants
provided informed consent before and after the study.
Funding: This study was co-funded by the Belgian Red Cross-Flanders and the
Laerdal Foundation for Acute Medicine. The Laerdal Foundation was not
involved in any part of the study.
Trial registration: We registered this trial at ClinicalTrials.gov as NCT00954161.
References
(1) Van de Velde S, Heselmans A, Roex A, Vandekerckhove P, Ramaekers
D, Aertgeerts B. Effectiveness of Nonresuscitative First Aid Training in
Laypersons: A Systematic Review. Ann Emerg Med 2009; 54(3):447-
457.
(2) Shotland RL, Heinold WD. Bystander response to arterial bleeding:
helping skills, the decision-making process, and differentiating the
helping response. J Pers Soc Psychol 1985; 49(2):347-356.
(3) Hawks SR, Peck SL, Vail-Smith K. An educational test of health behavior
models in relation to emergency helping. Health Psychol 1992;
11(6):396-402.
(4) Hawks SR, Egan M. The impact of three different first aid curricula on
emergency helping among college students. J Health Educ 1998;
29(5):289-293.
64

(5) Darley JM, Latane B. Bystander intervention in emergencies: diffusion
of responsibility. J Pers Soc Psychol 1968; 8(4):377-383.
(6) Latane B, Rodin J. A Lady in Distress - Inhibiting Effects of Friends and
Strangers on Bystander Intervention. J Exp Soc Psychol 1969; 5(2):189-
202.
(7) Penner LA, Dovidio JF, Piliavin JA, Schroeder DA. Prosocial behavior:
multilevel perspectives. Annu Rev Psychol 2005; 56:365-392.
(8) Rowe BH, Shuster M, Zambon S, Wilson E, Stewart D, Nolan RP et al.
Preparation, attitudes and behaviour in nonhospital cardiac
emergencies: evaluating a community's readiness to act. Can J Cardiol
1998; 14(3):371-377.
(9) Mogielnicki RP, Stevenson KA, Willemain TR. Patient and bystander
response to medical emergencies. Med Care 1975; 13(9):753-762.
(10) Smith KL, Cameron PA, Meyer AD, McNeil JJ. Is the public equipped to
act in out of hospital cardiac emergencies? Emerg Med J 2003;
20(1):85-87.
(11) van der Bijl JJ, Shortridge-Baggett LM. The theory and measurement of
the self-efficacy construct. Sch Inq Nurs Pract 2001; 15(3):189-207.
(12) Luszczynska A, Gutiérrez-Dona B, Schwarzer R. General self-efficacy in
various domains of human functioning: Evidence from five countries.
Int J Psychol 2005; 40(2):80-89.
(13) Pittenger DJ. Deception in research: Distinctions and solutions from the
perspective of utilitarianism. Ethics Behav 2002; 12(2):117-142.
65

(14) Watson D, Clark LA, Tellegen A. Development and validation of brief
measures of positive and negative affect: the PANAS scales. J Pers Soc
Psychol 1988; 54(6):1063-1070.
(15) Dunning D, Heath C, Suls JM. Flawed self-assessment: Implications for
Health, Education, and the Workplace. Psychol Sci Publ Interest 2004;
5(3):69-106.
(16) Elman D, Hooks R, Tabak D, Regehr G, Freeman R. The effectiveness of
unannounced standardised patients in the clinical setting as a teaching
intervention. Med Educ 2004; 38(9):969-973.
66

CHAPTER 5
Rapid reviews
De Buck E, Van de Velde S. Towards evidence based emergency medicine: best
BETs from the Manchester Royal Infirmary. BET 1. Optimal body position in oral
poisoning cases. Emerg Med J. 2010; 27(12):952-3.
De Buck E, Van de Velde S. Towards evidence based emergency medicine: best
BETs from the Manchester Royal Infirmary. BET 2: potato peel dressings for
burn wounds. Emerg Med J. 2010;27(1):55-56.
Van de Velde S, De Buck E, Dieltjens T, Aertgeerts B. Medicinal use of potato-
derived products: conclusions of a rapid versus full systematic review. Phytother
Res. 2010 (Epublication ahead of print).
67

Systematic reviews are considered to be the most reliable summaries of primary
studies. However, their production is a time-consuming process. Time
constraints have led to the development of rapid reviews in which
methodological shortcuts are applied to accelerate the production process.
Rapid reviews provide concise summaries of the best available evidence for very
specific clinical questions. BestBETs is a database of such rapid reviews relating
to emergency medicine (www.bestbets.org). In this chapter we present two
rapid reviews that were published as Best Evidence Topic reports
Although the number of published rapid reviews is rising, limited research has
been done to evaluate its validity. Therefore this chapter also compares the
results of one of these rapid reviews with a systematic review focusing on the
same topic.
5.1. BestBET 1: optimal body position in oral poisoning cases
Three-part question
In [orally poisoned patients] does [a specific body position] result in [a better
outcome for the patient]?
Clinical scenario
A 30-year-old woman had swallowed an overdose of pills. Her husband asks you
what he could have done to help his wife while waiting for the emergency
medical services te arrive. You wonder whether he could have laid her in a
particular position to ensure that the poisoning would have less detrimental
effects.
68

Search strategy
Ovid MEDLINE(R) 1950 to August Week 3 2010: Exp poisoning/0R exp
Acetaminophen/po (Poisoning) AND exp posture/. 144 records.
Embase 1947 to 1 February 2010 via the http://www.Embase.com interface:
‘intoxication'/exp OR poison* AND 'body posture'/exp AND (english)/Iim. 118
records.
The Cochrane Library August 2010: (MeSH descriptor Poisoning explode all trees
OR MeSH descriptor Acetaminophen explode all trees) AND MeSH descriptor
Posture explode all trees. 9 records 0 relevant.
Search outcome
Two hundred and fifty nine papers were found of which 257 were irrelevant or
of insufficient quality. The remaining two papers are shown in the table 1.
Comments
Thc evidence suggests that drug absorption is lowest in patients Iying on their
left side. However, the left side position is relatively poor at reducing the risk of
aspiration pneumonia in patients with a reduced level of consciousness.
International basic lifc support guidelines for laypersons reccommend that
patients who are unconscious but breathing should be placed in the recovery
position.
69

Table 1 Optimal body position in oral poisoning cases
Author, date and country
Patient group Study type Outcomes Key results
Study weaknesses
Vance et al, 1992, USA
12 healthy volunteers that ingested an overdose of acetaminophen (80 mg/kg) following an 8 h fasting period. Placed in left side, right side, supine, prone and sitting positions.
Experimental Group mean drug absorption
Differences between different body positions could be exaggerated because volunteers fasted for 8 h. Small sample size. Co-ingestants such as ethanol were absent and this may affect the findings.
(AUC 0-2 h, mg/l/min)
6.0
Left side 9.0 Right side 6.7 Supine 7.4 Prone 8.6
(p <0.05)
Adnet et al, 1999, France
205 acutely poisoned comatose patients < 65 years with a Glasgow Coma Scale less than or equal to 12. Placed in left side, right side, supine, prone, or semi-recumbent position.
Observational study
Frequency of suspected aspiration pneumonia
There are baseline differences between comparison groups. Blinded outcome measurement was not reported. Risk of contamination bias.
Left side 36.7%
Right side 45%
Supine 39.3%
Prone 8%
Semi-recumbent
11.1% (p=0.006)
AUC. area under the curve.
Clinical bottom line
Placing awake patients who have ingested oral poisons on to their left side may
reduce absorption of the poison. If the patient has reduced conscious level,
then the risk of aspiration pneumonia must be considered and the prone or
semi-recumbent positions are safer.
70

Contributions EDB and SVDV conceived the review question and search
strategy. They independently screened the literature to identify and select
retrieved studies against inclusion criteria. ED extracted the data and SVDV
checked if the synthesis was accurate. ED submitted the report to BestBETs.
References
Vance MV, Selden BS, Clark RF. Optimal patient position for transport and initial
management of toxic ingestions. Ann Emerg Med 1992; 21: 243-6.
Adnet F, Borron SW, Finot MA, et al. Relation of body position at the time of
discovery with suspected aspiration pneumonia in poisoned comatose patients.
Crit Care Med 1999; 27:745-8.
71
5.2. BET 2: Potato peel dressings for burn wounds
A short-cut review was carried out to establish whether potato peel dressings
are better than gauze alone in the acute management of burns. Nineteen
papers were found using the reported searches, of which three presented the
best evidence to answer the clinical question. The author, date and country of
publication, patient group studied, study type, relevant outcomes, results and
study weaknesses of these best papers are shown in table 1. It is concluded that
there is no evidence to show that potato peel is of benefit in the acute phase,
but that sterile potato peel dressings are better than gauze alone in the healing
phase.
Three-part question
In [patients with acute burns] is [potato peel dressing better than gauze or cloth
alone] at [promoting healing and preventing infection]?
Clinical scenario
During a camp trip in a remote area, a 32-year-old man has burned his hand and
arm in the camp fire. As he had neither a first aid kit nor bandages or dressings
to cover the wounds, he used cooked potato peels for this purpose. When you
see him some time later in the emergency department you are very impressed
by his innovative use of vegetables, though somewhat less sure of their efficacy
and safety in burns. Before you dismiss the idea completely, however, you
wonder if there is any published evidence.
Search strategy
Medline 1966–2008/09 using the Pubmed interface: (‘‘Burns’’ [Mesh] OR
Burn*[TW]) AND (‘‘Bandages’’ [Mesh] OR ‘‘dressing’’ [TW]) AND ‘‘potato’’ [TW]
72

LIMITS to English. Ovid MEDLINE(R) 1950 to September week 4 2009: Exp
Burns/AND exp Solanum tuberosum/OR potato.mp.
Embase via the NLH interface 1980–30 September 2009: exp BURN/OR exp
potato/OR potato.mp.
The Cochrane Library, Issue 3, 2009: MeSH descriptor Burns explode all trees
AND MeSH descriptor Solanum tuberosum explode all trees OR potato, ti, ab,
kw.
Search outcome
Nineteen papers were found of which 16 were irrelevant or of insufficient
quality. Details of the three remaining papers are shown in table 2.
Comments
The evidence presented is all from burns units in areas of the world where skin
homographs and xenographs are rarely available and is therefore not directly
applicable to settings in which such grafts are common. Furthermore, all the
studies use sterile potato peel dressings, not rough cut potato peel as set out in
the clinical scenario. The value of potato peel seems to be in reducing
desiccation and thereby promoting healing during the burns unit phase; there is
little evidence of independent antibacterial effect.
Clinical bottom line
There is no evidence to suggest that potato peel is effective as a burns dressing
in the acute phase. Sterile potato peel dressings are better than gauze alone
during the healing phase.
73

Table 2 Potato peel dressings for burn wounds
Author, date and country
Patient group Study type Outcomes Key results Study weaknesses
Keswani et al, 1990, India
17 hospital patients aged 1.5–45 years with burns between 5% and 42% of body surface area (mean 18.6%). Gauze with potato peel vs gauze alone in similar burns on each patient. All patients had silver sulfadia-zine applied below the dressing.
Clinical trial Bacterial growth
No difference in bacterial growth
Much of the data here is histological; there are no patient outcomes. No statistics performed. Blinding and follow-up are not clear.
Epidermal regeneration
Faster epithelial regeneration in potato peel dressings
Formation of exudates
Prevention of dessication in potato peel dressings
Survival of superficial skin cells
Increased survival of superficial skin cells in potato peel dressings
Subrah-manyam, 1996, India
100 patients with partial thickness burns over ,40% of body surface area treated within 6 h. Potato peel vs honey.
Randomised controlled trial
Days for complete healing
16.2 vs 10.2 days (p<0.001)
Randomisa-tion not clear; blinding not reported. Persistent
infection at day 7
10% vs 100% (p<0.001)
Adverse effects There were no adverse effects in either of the groups
Subjective relief of pain
No significant difference
Gore and Akolekar, 2003, India
30 patients aged 40 years with a burn size 50% of body surface area. Gauze with potato peel vs gauze with banana leaf. Potato peel applied to the left side and banana leaf dressing to the right.
Clinical trial Days until complete epithelialisation.
No clinical difference No statistics performed; blinding is not clear; no control group (crossover trial)
Eschar formation
No clinical difference
Number of areas requiring skin grafting
No clinical difference
Pain No clinical difference
Patient comfort
No clinical difference
Dressing handling
No clinical difference
74

Contributions EDB and SVDV conceived the review question and search
strategy. They independently screened the literature to identify and select
retrieved studies against inclusion criteria. ED extracted the data and SVDV
checked if the synthesis was accurate. ED submitted the report to BestBETs.
References
Keswani MH, Vartak AM, Patil A, et al. Histological and bacteriological studies of
burn wounds treated with boiled potato peel dressings. Burns 1990;16: 137–43.
Subrahmanyam M. Honey dressing versus boiled potato peel in the treatment
of burns: a prospective randomized study. Burns 1996;22:491–3.
Gore MA, Akolekar D. Evaluation of banana leaf dressing for partial thickness
burn wounds. Burns 2003;29:487–92.
75

5.3. Medicinal use of potato-derived products: conclusions of a rapid versus full systematic review
Abstract
Vlachojannis et al reported a systematic review on the medicinal use of potato-
derived products. The authors identified five trials for inclusion in the review,
including one study on the treatment of burns.Based on this RCT the review
authors concluded that potato peel is not recommended for burns.
As the authors of a rapid review on the use of potato peels for burns, we read
this systematic review with great interest. Although the concept of rapid review
is rising, accelerating the review process might introduce bias and its
conclusions may be subject to change once a systematic review is available.
Since this rapid and systematic review were done at similar times, we explored
if the results were consistent.
We identified three trials on the use of potato peels. Two of these trials were
not mentioned in the systematic review. The evidence indicates that sterile
potato peel dressings are better than gauze alone during the healing
phase.While there is no evidence of an antibacterial effect, we concluded that
potato peels promote healing.
Potato peel dressings might be the best available dressing in resource poor
countries. Because systematic reviews have a major impact it is crucial that
systematic reviews meet specified quality criteria. Therefore we draw attention
to adherance to the PRISMA statement.
76

Letter to the editor
Vlachojannis et al. reported the results of a systematic review on the medicinal
use of potato-derived products (Vlachojannis et al., 2010). Searching MEDLINE
and CENTRAL (based on the terms potato or Solanum tuberosum) plus hand
searching yielded 132 potentially relevant citations. From these, the authors
identified five clinical trials for inclusion in the review, including one study on
the treatment of burn wounds (Subrahmanyam, 1996).This RCT demonstrated
that burns covered with honey dressings healed better than burns covered with
potato peels. Based on this unique RCT the authors of the systematic review
concluded that topical potato peel is not recommended for the treatment of
burns.
As the authors of a rapid review on the efficacy and safety of potato peel
dressings for burns, we read this systematic review with great interest (De Buck
and Van de Velde, 2010). Rapid review means that we accelerated the
systematic research process by restricting the number of electronic databases
searched, building a specific search strategy, not searching for grey literature,
using focused selection criteria, and not performing a meta-analysis. These
shortcuts are a compromise between scientific rigour, transparency and
timeliness. Our rapid review was not meant to be a full systematic review and
this is also mentioned in the publication.
The need to provide quick but accurate evidence-based information is
increasing in the healthcare sector and the concept of rapid reviews is rising
(Watt et al., 2008). However, accelerating the review process might introduce
bias and therefore it may be subject to change once a systematic review is
available (Ganann et al., 2010). Since these rapid and regular systematic reviews
were done at similar times, we considered it an opportunity to explore if the
findings and conclusions were consistent.
77

Our rapid review was produced in approximately 1 month. We searched
MEDLINE, EMBASE and CENTRAL using strategies based on the terms potato,
Solanum tuberosum, burns, bandages. From 19 references screened, we
identified three trials on the use of potato peel dressings (Subrahmanyam,
1996; Gore and Akolekar, 2003; Keswani et al., 1990). To our surprise, two of
these clinical trials were not mentioned in the full systematic review (Gore and
Akolekar, 2003; Keswani et al., 1990). These studies compared potato peel
dressings with either gauze alone, or banana leaf dressing. The evidence
indicates that sterile potato peel dressings are better than gauze alone during
the healing phase. While there is no evidence of an independent antibacterial
effect, we concluded that potato peels promote healing, which could be
possibly due to a reduction in desiccation.
It is important that our conclusion was different from that of Vlachojannis.
Systematic reviews tend to be the most read and cited type of article and have a
major impact (Dijkers, 2009).While potato peel dressings are not directly
applicable to Western settings, it might be the best available dressing in
resource poor countries. This is illustrated by the fact that all the trials included
in our rapid review were all conducted in burn centres in India where they had
an acute need for cheap and easily available dressings (Gore and Akolekar,
2003). One explanation for the evidence gap in the review of Vlachojannis and
ours might be the lack of awareness of relevant evidence: the study by Gore
might have been missed during the screening of citation titles, because the title
only mentions banana leaf dressings and not potato peels.Another explanation
might be exclusion of evidence that did not match the eligibility criteria: in the
study by Keswani the data are histological and there are no patient outcomes
which could have been a reason to exclude the study. However, based on the
manuscript it is not possible to evaluate this.
78

The difference in conclusions between these two reviews shows the
implications this can have for practice. Therefore it is crucial that systematic
reviews meet specified quality criteria. In order to be able to evaluate the
strengths and weaknesses of systematic reviews,we draw attention to
adherence to the Preferred Reporting Items for Systematic Reviews and Meta-
Analyses, i.e. the PRISMA statement (Liberati et al., 2009). Amongst other items,
the PRISMA statement asks authors of systematic reviews to describe eligibility
criteria and the results of the study selection process.
Contributions: SVDV wrote the letter to the editor. EDB, TD, and BA provided
feedback on the letter.
Conflicts of Interest SVDV and EDB are authors of the rapid review on potato
peel dressings for burn wounds. TD and BA have no conflicts of interests.
Ethical approval Not applicable
References
De Buck E, Van de Velde S. 2010. Towards evidence based emergency medicine:
best BETs from the Manchester Royal Infirmary. BET 2: potato peel dressings for
burn wounds. Emerg Med J 27: 55–56.
Dijkers MP. 2009. The value of traditional reviews in the era of systematic
reviewing. Am J Phys Med Rehabil 88: 423–430.
Ganann R, Ciliska D, Thomas H. 2010. Expediting systematic reviews: methods
and implications of rapid reviews. Implement Sci 5: 56.
Gore MA, Akolekar D. 2003. Evaluation of banana leaf dressing for partial
thickness burn wounds. Burns 29: 487–492.
79

Keswani MH, Vartak AM, Patil A, Davies JW. 1990. Histological and
bacteriological studies of burn wounds treated with boiled potato peel
dressings. Burns 16: 137–143.
Liberati A, Altman DG, Tetzlaff J et al. 2009. The PRISMA statement for reporting
systematic reviews and meta-analyses of studies that evaluate healthcare
interventions: explanation and elaboration. Br Med J 339: b2700.
Subrahmanyam M. 1996. Honey dressing versus boiled potato peel in the
treatment of burns: a prospective randomized study. Burns 22: 491–493.
Vlachojannis JE, Cameron M, Chrubasik S. 2010. Medicinal use of potato-derived
products: a systematic review. Phytother Res 24: 159–162.
Watt A, Cameron A, Sturm L et al. 2008. Rapid reviews versus full systematic
reviews: an inventory of current methods and practice in health technology
assessment. Int J Technol Assess Health Care 24: 133–139
80

Rigour of development does not AGREE with
recommendations in practice guidelines on the use of
ice for acute ankle sprains
CHAPTER 6
Van de Velde S, Heselmans A, Donceel P, Vandekerckhove P, Ramaekers D,
Aertgeerts B. Rigour of development does not AGREE with recommendations in
practice guidelines on the use of ice for acute ankle sprains. BMJ Qual Saf. 2011
(Epublication ahead of print).
81

Rigour of development does notAGREE with recommendations inpractice guidelines on the use of ice foracute ankle sprains
S Van de Velde,1,2 A Heselmans,2 P Donceel,3 P Vandekerckhove,1
D Ramaekers,2 B Aertgeerts2
ABSTRACTObjective: This study evaluated whether the Appraisal
of Guidelines Research and Evaluation (AGREE) rigour
of development score of practice guidelines on ice for
acute ankle sprains is related to the convergence
between recommendations.
Design: The authors systematically reviewed guidelines
on ice for acute ankle sprains. Four appraisers
independently used the AGREE instrument to evaluate
the rigour of development of selected guidelines. For
each guideline, one reviewer listed the cited evidence on
ice and calculated a cited evidence score. The authors
plotted the recommended durations and numbers of ice
applications over the standardised rigour of
development score to explore the relationships.
Data sources: Three reviewers searched for
guidelines in Medline, Embase, Sportdiscus, PEDro,
G-I-N Guideline Library, Trip Database, SumSearch,
National Guideline Clearinghouse and the Health
Technology Assessment database, and conducted
a web-based search for guideline development
organisations.
Eligibility criteria: Eligible guidelines had
a development methodology that included a process to
search or use results from scientific studies and the
participation of an expert group to formulate
recommendations.
Results: The authors identified 21 guidelines,
containing clinically significant variations in
recommended durations and numbers of ice
applications. The median standardised rigour of
development score was 57% (IQR 18 to 77). Variations
occurred evenly among guidelines with low moderate
or high rigour scores. The median evidence citation
score in the guidelines was 7% (IQR 0 to 61).
Conclusions: There is no relationship between the
rigour of development score and the
recommendations in guidelines on ice for acute ankle
sprains. The guidelines suffered from methodological
problems which were not captured by the AGREE
instrument.
INTRODUCTION
Evidence-based guidelines form a typical
approach to bridging the gap between
evidence and practice.1 Although practice
guidelines aim to reduce inappropriate
treatment variations, guidelines on the same
topic often make conflicting recom-
mendations.2e4 The reasons behind these
conflicting recommendations include insuf-
ficient evidence, lack of awareness of relevant
evidence or ignoring such evidence, failure
to appraise the evidence critically, the
composition and interactions of a guideline
panel, differences in context, values and
preferences, and the applicability of the
evidence.5 6 Only differences in context,
values and preferences can be considered
as valid reasons for disagreement between
recommendations. In other cases, guideline
divergence is the result of suboptimal deci-
sions. This may confuse guideline users and
raises concerns about the use of biased
practice guidelines.7 8
Critical appraisal instruments for practice
guidelines exist to give healthcare providers
an idea of the quality of guidelines before
adopting the recommendations. One limita-
tion of these instruments is that they do not
evaluate the guideline content.9 The
Appraisal of Guidelines Research and Evalu-
ation (AGREE) instrument is a validated
instrument that is widely used to evaluate
guidelines.10 11 Studies that evaluated the
link between the methodological quality of
a guideline and its content found no rela-
tionship.12 13 This is troubling if a high-
quality score does not necessarily imply
clinically appropriate recommendations.12 13
One limitation of the existing studies on
1Belgian Red Cross-Flanders,
Mechelen, Belgium2Belgian Branch of the
Cochrane Collaboration,
Belgian Centre for
Evidence-Based Medicine,
Katholieke Universiteit
Leuven, Leuven, Belgium3School of Public Health,
Katholieke Universiteit
Leuven, Leuven, Belgium
Correspondence to
S Van de Velde, Belgian Red
Cross-Flanders, Motstraat
40, 2800 Mechelen, Belgium;
stijn.vandevelde@rodekruis.
be
Accepted 13 October 2010
Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435 1
82
svelde
Rechthoek

conflicting recommendations is that variations could be
attributed to reasonable differences in context. This
study evaluates whether the AGREE domain for rigour of
development is related to the convergence between
recommendations for a common disorder and a cheap
and available treatment: acute ankle sprain and ice.
Rest, ice, compression and elevation is the usual
treatment for ankle sprains.14 15 However, textbook
information on the use of ice for acute sprains varies
greatly as regards the time and frequency of its applica-
tion.16 MacAuley propagated evidence-based guidelines
to reach consensus on the appropriate management.
METHODOLOGY
Selection of guidelines
Three authors (BA, DR, SVDV) searched for practice
guidelines in Medline, Embase, Sportdiscus, PEDro, G-I-
N Guideline Library, Trip Database, SumSearch,
National Guideline Clearinghouse and the Health
Technology Assessment database, and conducted a web-
based search for guideline development organisations.
Because soft-tissue injury is a very broad domain, this
study focused on guidelines with recommendations on
ice for ankle sprains and strains. This criterion excluded
guidelines on other joints than ankles. Guidelines
focusing on soft-tissue injuries in general were included
if they encompassed ankle sprains or strains. We
excluded guidelines that focused only on bruises, dislo-
cations, subluxations, fractures or chronic injuries, as
well as those for paediatric patients only.
We used the Institute of Medicine definition of clinical
guidelines, namely systematically developed statements
to assist practitioner and patient decisions about appro-
priate healthcare for specific circumstances. This study
only considered practice guidelines if their development
methodology included a process to search or use results
from scientific studies and the participation of an
expert group to formulate recommendations. Consensus
statements, systematic reviews, narrative reviews, text-
books and patient information leaflets belong to the
exclusion criteria. If two or more guidelines by the same
group were available, we selected only the most recent
one.
Rigour of development
To evaluate the quality of the selected guidelines, we
used the AGREE instrument,10 but limited ourselves to
the domain for rigour of development. Because ice
application is a cheap and available treatment, in our
opinion this domain was the most relevant
AGREE category to explain divergence between practice
guidelines on this topic. Four appraisers (AH, BA, DR,
SVDV) independently used the corresponding domain
questions in the AGREE instrument to evaluate each
selected guideline.10
We calculated the standardised domain score as
instructed in the AGREE checklist (obtained scoree
minimum possible score)/(maximum possible scoree
minimum possible score).
If the guideline did not report certain information, we
either tried to collect information from background
documents on the guideline or contacted the authors. If
the information for a certain item was still unclear, this
item was scored as ‘strongly disagree.’ The intraclass
correlation coefficient two-way mixed model for single
measurements was calculated using an agreement defi-
nition,17 18 to measure the appraiser agreement for the
rigour of development domain.10 During a panel
meeting, the appraisers discussed any deviations in
scores and resolved disagreements.
Data extraction
For each guideline, one reviewer (SVDV) tabulated
those recommendations on the duration per ice appli-
cation, the number of applications per 12 h, and the
number of days of ice applications. If guidelines
recommended a minimum and maximum duration and
frequency, both were extracted. For each guideline, we
calculated the overall ice application duration
(¼minutes per ice application3times per day3number
of days).
For each guideline, one reviewer (SVDV) checked the
references cited in the sections on the application of ice.
From the cited references, he extracted all the inter-
vention studies that tested the effect of cryotherapy. The
group of authors decided to include studies of patients
with sprains or strains to the ankle, which compared
any type of cryotherapy with a control condition,
another type of cryotherapy or another type of treatment
for any type of outcome. We also included intervention
studies cited in secondary sources, if these sources
provided sufficient details about the characteristics and
results of the presented intervention study. Next, we
calculated the cited evidence score as follows: (number
of cited intervention studies in a single guideline)/
(maximum possible number of unique intervention
studies cited according to the publication date of the
guideline). In this study we did not perform an inde-
pendent systematic review on the role of ice for ankle
sprains. So, the maximum possible number of unique
intervention studies is the sum of studies retrieved by
screening the selected guidelines, existing systematic
reviews19 20 and the ‘Related citations’ in Pubmed.
Data synthesis
One reviewer (SVDV) tabulated the rigour of develop-
ment score, cited evidence score and overall ice
2 Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
83
svelde
Rechthoek

application duration to explore the relationships. To
visualise this, we made highelow plots. Since the
number of guidelines was too few to perform statistical
tests, we conducted a descriptive analysis of the
quantitative data.
RESULTS
Identification of guidelines
Figure 1 provides a flow chart of the identification and
selection of practice guidelines. We screened 56 publi-
cations and included 21 guidelines for the analysis.
Target users of the selected guidelines included general
practitioners, specialists, physiotherapists, nurses and
first-aiders.
Table 1 describes the key data of the selected practice
guidelines.
Description of recommendations
While 19 guidelines recommended the use of ice, two
guidelines found that the benefit was too uncertain to
give any recommendation for or against.26 30 The
guidelines recommended durations of each ice applica-
tion ranging from 12 to 30 min, with 20 min recom-
mended most frequently. The recommended frequency
of ice applications varied from one to eight times a day,
with six times a day recommended most frequently. The
recommended number of days of ice application varied
from 1 to 7 days. Data from two guidelines mentioning
that ice applications might be prolonged in the reha-
bilitation phase were not included in the analysis. The
maximum recommended overall duration of ice appli-
cation was 14 h,27 while the minimum recommended
overall duration was 45 min.21 Five guidelines recom-
mended ice,29 31 35 38 39 without any further details about
the time or frequency.
Rigour of development
The median standardised rigour of development score
was 57% (IQR: 18e77). For guidelines published within
the last 5 years (n¼15) this was 54% (IQR: 19e77) versus
59% (IQR: 56e77) for older guidelines (n¼6). The
initial intraclass correlation coefficient was 73%, and
after discussion of deviations among the panel members
the score evolved to 93%.
Comparison of cited intervention studies
From the selected guidelines and its secondary sources,
we identified a total of seven relevant intervention
studies.42e48 None of the recent guidelines captured the
study published by Bleakley in 2006.49 While it was not
the intent of this study to do a systematic review on the
role of ice for ankle sprains, we provide an informative
summary with the relevant evidence in table 2.
A guideline published in 2009 which captured six
relevant intervention studies obtained the highest
evidence citation score (six cited intervention studies/
eight unique intervention studies available by
2009¼75%).23 Nine guidelines did not refer to any
intervention study on cryotherapy.25 27 31 33 35 36 38 39 41
In three guidelines, we could not assess the number of
cited intervention studies because there were no in-text
citations, or because the secondary sources could not be
obtained.34 37 40 The median evidence citation score in
the guidelines was 7% (IQR 0 to 61). The guidelines
cited positive or negative results equally (RR 0.8; 95% CI
0.5 to 1.2).
Relationship between rigour of development and guideline
recommendations
Figures 2e5 plot the guideline recommendations over
the standardised rigour of development score. Clinically
significant variations in recommended durations,
frequencies and number of days occur evenly among
guidelines with low, moderate or high rigour scores.
DISCUSSION
The AGREE rigour of development score of practice
guidelines on ice for acute ankle sprains is not related to
the convergence between recommendations. The diver-
sity of the recommended durations and frequencies of
ice application is remarkable and comparable with the
reported variety in textbooks.16 The evidence-based
guidelines did not lead to a consensus on the use of ice
Figure 1 Flow chart of identification and selection of
guidelines. G-I-N, G-I-N Guideline Library; NGC, National
Guideline Clearinghouse.
Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435 3
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
84
svelde
Rechthoek

Table
1Descriptionofselectedguidelines
Guideline,yearandcountrycode
Standardised
rigour
score
(%)
Cited
evidence
score
(%)
Duration(m
in)
perice
application
Noof
times
perday
Noof
days
Overall
duration(h)
oficeapplication
RoyalDutchSociety
forPhysicalTherapyd2006dNL21
87
57
15e20
1e3
30.75e3
AssociationofCharteredPhysiotherapists
inSports
Medicined1998dUK22
85
71
20e30
63
6e9
Work
LossData
Instituted2009dUS23
83
75
uu
1e2
u
BelgianRedCrossd2007dBE24
80
57
20
uu
u
AmericanCollegeofOccupationalandEnvironmental
Medicined2008dUS25
77
0u
u1.5e2
u
DutchInstitute
forHealthcare
Improvementd
1998dNL26
77
57
uu
uu
Institute
forClinicalSystemsIm
provementd
2006dUS27
75
015e20
4e6
77e14
NationalFirstAid
ScienceAdvisory
Boardd2005dUS28
68
29
20
uu
u
FrenchNationalAgencyforAccreditationandEvaluation
InHealthd2000dFR29
60
71
uu
uu
DutchCollegeofGeneralPractitionersd2000dNL30
58
71
uu
uu
Duodecim
d2009dFI31
57
0u
uu
u
FlemishCollegeofGeneralPractitionersd2001dBE32
56
14
15e25
4e8
33e10
SowerbyCentreforHealthInform
aticsatNewcastled2008dUK33
54
015e20
4e6
2e3
2e6
MexicanInstitute
ofSocialSecurityd2004dMX34
29
u12e20
2e3
3e7
1.2e7
BrazilianSociety
ofOrthopaedicsandTraumatologyd2008dBR35
20
0u
uu
u
Emedecined2008dUS36
20
015e20
31e3
0.75e3
MadiganArm
yMedicalCentere
2007dUS37
19
u20
63eu
6eu
ColoradoDivisionofLabourandEmploymentd
2009dUS38
14
0u
uu
u
GovernmentofWestern
Australia,Carepointd
2009dAU39
70
uu
uu
Junta
DeExtremadurad2004dSP40
5u
20
62e3
4e6
HealthCanadad2000dCA41
50
12e14
62eu
2.4eu
u,unclear.
4 Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
85
svelde
Rechthoek
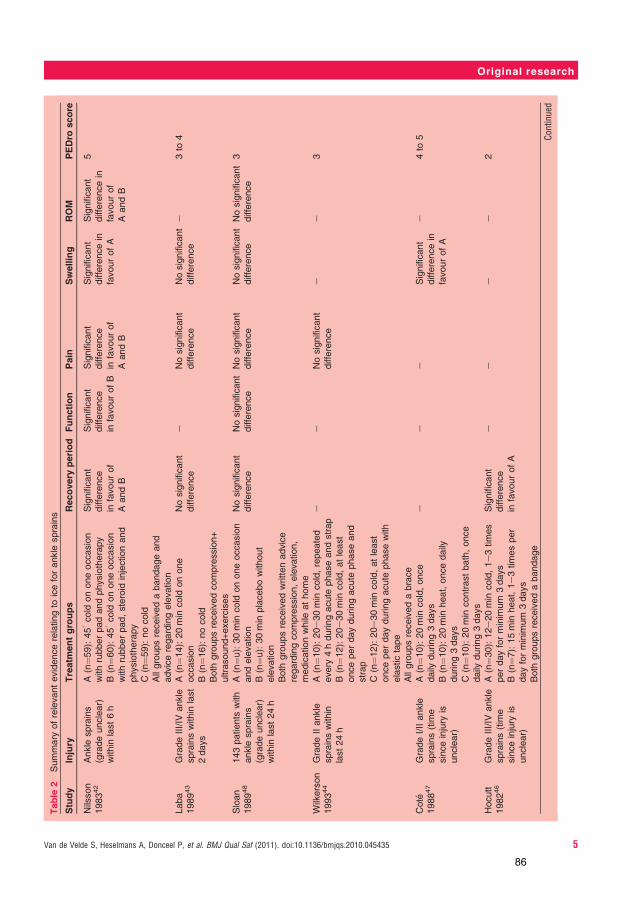
Table
2Summary
ofrelevantevidencerelatingto
iceforankle
sprains
Study
Injury
Treatm
entgroups
Recovery
period
Function
Pain
Swelling
ROM
PEDro
score
Nilsson
198342
Ankle
sprains
(gradeunclear)
within
last6h
A(n¼59):459cold
ononeoccasion
withrubberpadandphysiotherapy
B(n¼60):459cold
ononeoccasion
withrubberpad,steroid
injectionand
physiotherapy
C(n¼59):nocold
Allgroupsreceivedabandageand
adviceregardingelevation
Significant
difference
infavourof
AandB
Significant
difference
infavourofB
Significant
difference
infavourof
AandB
Significant
differencein
favourofA
Significant
differencein
favourof
AandB
5
Laba
198943
GradeIII/IV
ankle
sprainswithin
last
2days
A(n¼14):20min
cold
onone
occasion
B(n¼16):nocold
Both
groupsreceivedcompression+
ultrasound+exercises
Nosignificant
difference
eNosignificant
difference
Nosignificant
difference
e3to
4
Sloan
198948
143patients
with
ankle
sprains
(gradeunclear)
within
last24h
A(n¼u):30min
cold
ononeoccasion
andelevation
B(n¼u):30min
placebowithout
elevation
Both
groupsreceivedwrittenadvice
regardingcompression,elevation,
medicationwhile
athome
Nosignificant
difference
Nosignificant
difference
Nosignificant
difference
Nosignificant
difference
Nosignificant
difference
3
Wilkerson
199344
GradeIIankle
sprainswithin
last24h
A(n¼10):20e30min
cold,repeated
every
4hduringacute
phaseandstrap
B(n¼12):20e30min
cold,atleast
onceperdayduringacute
phaseand
strap
C(n¼12):20e30min
cold,atleast
onceperdayduringacute
phasewith
elastictape
Allgroupsreceivedabrace
ee
Nosignificant
difference
ee
3
Cote
198847
GradeI/IIankle
sprains(tim
e
sinceinjury
is
unclear)
A(n¼10):20min
cold,once
daily
during3days
B(n¼10):20min
heat,oncedaily
during3days
C(n¼10):20min
contrastbath,once
daily
during3days
ee
eSignificant
differencein
favourofA
e4to
5
Hocutt
198246
GradeIII/IV
ankle
sprains(tim
e
sinceinjury
is
unclear)
A(n¼30):12e20min
cold,1e3times
perdayforminim
um
3days
B(n¼7):15min
heat,1e3timesper
dayforminim
um
3days
Both
groupsreceivedabandage
Significant
difference
infavourofA
ee
ee
2
Continued
Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435 5
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
86
svelde
Rechthoek

for ankle injuries. Since it was not the objective of this
study to evaluate the validity of the recommendations,
we take no position on which recommendations on ice
are most appropriate.
This study identified a number of methodological
problems of guidelines and shortcomings in the AGREE
instrument to capture these. Only six guidelines
discussed half or more of the available evidence on ice
for ankle sprains. One potential explanation is that
guideline developers compromised on the literature
review to save time or resources. Making use of existing
systematic reviews19 20 or adaptation of other guidelines
with a well-conducted systematic review may substantially
reduce the time and resources required.50 51 As the
PEDro quality score was low for most of the trials, it is
Table
2Continued
Study
Injury
Treatm
entgroups
Recovery
period
Function
Pain
Swelling
ROM
PEDro
score
Basur
197645
Ankle
sprains
(gradeunclear,
timesinceinjury
isunclear)
A(n¼30):cold
every
4hduring
2daysandbandage
B(n¼30):bandageonly
Significant
difference
infavourofA
ee
ee
3
Bleakley
200649
GradeI/IIankle
sprainswithin
last48h
A(n¼46):20min
cold,every
2h
until72hpostinjury
B(n¼43):10min
coldd10min
restd
10min
cold,every
2huntil
72hpostinjury
Both
groupsreceivedhome
exercises
eNosignificant
difference
Nosignificant
differencefor
pain
atrest
Significant
differencewithin
firstweekforpain
duringactivityin
favourofB
Nosignificant
differencewithin
weeks2to
6for
pain
duringactivity
Nosignificant
difference
e7
Significantdifferencerefers
tostatisticaltests
ofsignificanceandnotto
clinicalsignificance.Data
onthePhysiotherapyEvidenceDatabase(PEDro)ScoringScale
were
collectedfrom
two
systematicreviews1920andthePEDro
databaseitself(http://www.pedro.org.au/).
Figure 2 Highelow plot of maximum and minimum duration
per individual ice application expressed in minutes over the
standardised rigour of development score.
Figure 3 Highelow plot of maximum and minimum number of
applications per 12 h over the standardised rigour of
development score.
6 Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
87
svelde
Rechthoek

possible that guideline authors decided to exclude
studies with a risk of bias. This might also explain the low
evidence citation score.
A number of guidelines succeed in getting good or
high AGREE rigour of development scores, while their
cited evidence score is suboptimal.21 24e28 These find-
ings illustrate that an evaluation of the validity of the
literature search is an important component of guide-
line appraisal. This problem was previously described as
an important limitation of AGREE,9 and is unfortunately
not solved with the publication of AGREE II. We fully
support the plan of the AGREE Trust to address the
clinical validity or appropriateness in the AGREE A3
initiative.52
Guideline grading systems are proposed to help users
in the interpretation of guidelines. GRADE is such
a system and asks those making the recommendations to
categorise recommendations as strong or weak.53 The
strength of recommendations is determined in GRADE
by the balance between benefits and harms, quality of
evidence, values and preferences, and costs. Guideline
authors are instructed to be transparant on their
judgements. Only half of the guidelines used a grading
system to indicate the degree of confidence one can
have in the evidence or recommendations. Given the
elusive evidence, incorporating a grading system could
better indicate the current uncertainty associated with
ice applications. The new item in AGREE II that requires
a clear description of the strengths and limitations of the
body of evidence is pertinent in this regard.54
Only occasionally did guidelines describe how consid-
erations about the uncertain benefit of prolonged/
minimal/no ice application versus the discomfort/risks
for the patient influenced the final recommendation.
Information about the role of opinion versus the
evidence is only mentioned as an additional consider-
ation in item 12 of AGREE II. This is an improvement
compared with the original AGREE instrument, but we
believe that this item should explicitly request trans-
parency on the influence of opinion per final decision.
This study has several limitations. Because identifying
guidelines requires a laborious search of multiple data-
bases, we might have missed relevant guidelines.55 The
National Guideline Clearinghouse (http://www.guide-
line.gov/) contained only two of the selected guidelines
in our study. The G-I-N Guideline Library (http://www.
g-i-n.net/) was the most comprehensive guideline data-
base, containing half of the selected guidelines.
While we evaluated the rigour of development for the
guideline document as a whole, we further focused on
the individual recommendations on ice for ankle
sprains. Because the quality of the evidence review may
vary per recommendation in a guideline, the conclu-
sions on the gathering of evidence may not be applicable
for the whole guideline.
Another limitation of this study is that guidelines
authors poorly reported their methodology. We emailed
the authors of 18 included guidelines with a request for
more information. Only five replied with more details.
This might under- or overvalue the actual rigour of
development score. Many guidelines referred to
a general manual endorsed by their organisation
describing the various steps that should be followed.
Because ‘should’ does not always mean that it has been
done, the rigour score might be overvalued for certain
guidelines. Poor reporting is a common problem with
guidelines and has been identified in previous studies.56
In contrast with publication guidelines such as Quorum
Figure 4 Highelow plot of maximum and minimum number of
days of ice application over the standardised rigour of
development score.
Figure 5 Highelow plot of maximum and minimum overall ice
application duration expressed in hours over the standardised
rigour of development score.
Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435 7
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
88
svelde
Rechthoek

for the reporting of systematic reviews, there are no
recommendations for the transparent reporting of
guidelines.57 Because many guidelines are not published
in scientific journals, it might be more challenging to
enforce such criteria. A related problem was that we
could not identify the last date of the literature search.
To calculate the evidence citation score, we therefore
used the publication date of the guideline as denomi-
nator rather than the last date of the literature search.
Given the time between initiation and publication of
guidelines, the evidence score might be underestimated.
However, we do not think that this influenced the
conclusions for the following reasons. The two oldest
guidelines published in 1998, mentioned that they
searched until 199822 or cited studies published in 1998
for related topics.26 This shows that they were in the
ability of retrieving the seven trials published before
1994. For the guidelines published between 2007 and
2009, it is possible that the trial49 published in August
2006 fell outside the literature search date range.
However, eight of these guidelines did not refer to any
intervention study. The other guideline cited studies
published in 2009 for related topics, which indicates
that they were in the ability of retrieving this trial
from 2006.
The evidence citation score is an indicator of the
quality of the literature review, but it does not address
correspondence between the evidence description and
the recommendations. Therefore, we cannot judge if the
lack of agreement between guidelines is explained by
differences in evidence. Additionally, the total body of
evidence is wider than the best available evidence which
we screened. Some guidelines also referred to indirect
evidence from surgery patients or healthy subjects, case
studies and animal studies, which may explain the
differences in recommendations.
A final limitation is the difficulty of scoring items with
AGREE that only partially fulfil the criteria. While it is
clear when to use a score of ‘strongly agree’ or ‘strongly
disagree,’ it is less obvious for an ‘agree’ or ‘disagree’
score. The more explicit scoring system of AGREE II
might improve this.54 58
In conclusion, we identified 21 guidelines on ankle
sprains and ice. The recommended durations and
number of ice applications varied significantly. The role
of evidence versus expert opinion was obscure in many
guidelines. As the differences occurred evenly among
guidelines with low, moderate or high rigour scores, we
conclude that the guidelines suffered from methodo-
logical shortcomings which the AGREE instrument did
not capture. We believe that a verification of the validity
of the literature search and an item assessing the
description of the role of expert opinion should be
added to the AGREE instrument.
Funding This study was funded by the Belgian Red CrossdFlanders.
Competing interests PVDK and SVDV are employed in the Belgian Red
Cross-Flanders from which a guideline was included; BA, DR and SVDV
regularly review practice guidelines for the Flemish College of General
Practitioners from which a guideline was included. AH, PD and PVDK have no
relationships with companies that might have an interest in the submitted work
in the previous 3 years; AH, BA, DR, PD, PVDK and SVDV, their spouses,
partners and children have no financial relationships that may be relevant to
the submitted work; BA and SVDV are authors of a guideline which is included
in the analysis and have non-financial interests that may be relevant to the
submitted work.
Contributors SVDV, BA and DR conceived and designed the study. SVDV, BA
and DR searched for eligible guidelines. SVDV, AH, BA and DR evaluated the
retrieved guidelines on rigour of development. PVDK and PD provided general
advice on the study. SVDV wrote the research paper. BA was the guarantor of
the study.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1. Woolf SH, Grol R, Hutchinson A, et al. Clinical guidelines: potential
benefits, limitations, and harms of clinical guidelines. BMJ1999;318:527e30.
2. Burgers JS, Bailey JV, Klazinga NS, et al. Inside guidelines:comparative analysis of recommendations and evidence in diabetesguidelines from 13 countries. Diabetes Care 2002;25:1933e9.
3. Matthys J, De MM, van Driel ML, et al. Differences amonginternational pharyngitis guidelines: not just academic. Ann Fam Med2007;5:436e43.
4. Georg G, Colombet I, Durieux P, et al. A comparative analysis of fourclinical guidelines for hypertension management. J Hum Hypertens2008;22:829e37.
5. Oxman AD, Glasziou P, Williams JW Jr. What should cliniciansdo when faced with conflicting recommendations? BMJ2008;337:a2530.
6. Gardner B, Davidson R, McAteer J, et al. A method for studyingdecision-making by guideline development groups. Implement Sci2009;4:48.
7. Hitchen L. Conflicting guidelines on same topics cause doctorsconfusion, say MPs. BMJ 2007;335:1012.
8. Shaneyfelt TM, Centor RM. Reassessment of clinical practiceguidelines: go gently into that good night. JAMA 2009;301:868e9.
9. Vlayen J, Aertgeerts B, Hannes K, et al. A systematic review ofappraisal tools for clinical practice guidelines: multiple similarities andone common deficit. Int J Qual Health Care 2005;17:235e42.
10. AGREE Collaboration. Development and validation of an internationalappraisal instrument for assessing the quality of clinical practiceguidelines: the AGREE project. Qual Saf Health Care2003;12:18e23.
11. Cluzeau F. Conflicting recommendations. Let’s not forget AGREE.BMJ 2009;338:b407.
12. Watine J, Friedberg B, Nagy E, et al. Conflict between guidelinemethodologic quality and recommendation validity: a potentialproblem for practitioners. Clin Chem 2006;52:65e72.
13. McIntosh HM, Neal RD, Rose P, et al. Follow-up care for menwith prostate cancer and the role of primary care: a systematicreview of international guidelines. Br J Cancer 2009;100:1852e60.
14. MacAuley D. Musculoskeletal medicine/sports medicine. Emerg MedJ 2003;20:500.
15. Hubbard TJ, Hicks-Little CA. Ankle ligament healing after an acuteankle sprain: an evidence-based approach. J Athl Train2008;43:523e9.
16. MacAuley D. Do textbooks agree on their advice on ice? Clin J SportMed 2001;11:67e72.
17. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing raterreliability. Psychol Bull 1979;86:420e8.
18. McGraw KO, Wong SP. Forming inferences about some intraclasscorrelation coefficients. Psychol Methods 1996;1:30e46.
19. Bleakley C, McDonough S, MacAuley D. The use of ice in thetreatment of acute soft-tissue injury: a systematic review ofrandomized controlled trials. Am J Sports Med 2004;32:251e61.
20. Hubbard TJ, Aronson SL, Denegar CR. Does cryotherapy hastenreturn to participation? A systematic review. J Athl Train2004;39:88e94.
21. van der Wees J, Lenssen AF, Feijts YAEJ, et al. Practice GuidelineAnkle Sprain. Royal Dutch Society for Physical Therapy. 2006.
8 Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
89
svelde
Rechthoek

http://nhg.artsennet.nl/kenniscentrum/k_richtlijnen/k_nhgstandaarden/NHGStandaard/M04_std.htm#Richtlijnenbeleid.
22. Kerr K, Daley L, Booth L, et al. Guidelines for the PhysiotherapyManagement of Soft Tissue Injury with Protection, Rest, Ice,Compression and Elevation (PRICE) During the first 72 Hours.Chartered Society for Physiotherapy and Association ofChartered Physiotherapists in Sports Medicine. 1998.http://www.csp.org.uk/.
23. Ankle & Foot (Acute & Chronic). Work Loss Data Institute. 2008.http://www.odg-twc.com/odgtwc/ankle.htm.
24. Van de Velde S, Broos P, Van Bouwelen M, et al. European first aidguidelines. Resuscitation 2007;72:240e51.
25. Ankle and Foot Complaints. American College of Occupational andEnvironmental Medicine. 2004. http://apg-i.acoem.org/.
26. Consensus on diagnostics and treatment of the acutely injured ankle.Dutch Institue for health care improvement (CBO). 1998. http://www.cbo.nl.
27. Health care guideline: ankle sprain. Institute for Clinical SystemsImprovement. 2006. http://www.icsi.org/.
28. Part 14: first aid. Circulation 2005;112(22 Suppl):III115e25.29. Reeducation After Lateral Ankle Distorsion. Recommendations for
Clinical Practice. French National Agency for Accreditation andEvaluation in Health. 2000. http://www.has-sante.fr/portail/display.jsp?id¼c_272059.
30. Goudswaard A, Thomas S, Van den Bosch WJHM, et al. AnkleSprains. Dutch College of General Practitioners, 2000. http://nhg.artsennet.nl/upload/104/standaarden/M04/start.htm.
31. Ristiniemi J. Evidence Based Medicine Guidelines: Ankle Sprain.Duodecim Medical Publications. 2009. http://ebmg.wiley.com/ebmg/ltk.koti.
32. Wyffels P, De Naeyer P, Van Royen P. Ankle Distorsion:Recommendations for Good Medical Practice. Flemish College ofGeneral Practitioners, 2001. http://www.domusmedica.be/kwaliteit/aanbevelingen/overzicht/enkeldistorsie-horizontaalmenu-379.html.
33. Sprains and Strains. Sowerby Centre for Health Informatics atNewcastle. 2008. http://cks.library.nhs.uk/sprains_and_strains.
34. Perez Rojas JEA, Hernandez Elizarraras E, Mazadiego GonzalezME, et al. Mexican Institute of Social Security. Clinical guidelines forthe Attention of Patients with Ankle Distorsion. Revista Medica delIMSS 2004;42:437e44.
35. Rodrigues FL, Waisberg G. Ankle Distorsion. Brazilian Society ofOrthopaedics and Traumatology. 2008. http://www.projetodiretrizes.org.br/7_volume/03-Entorce_Tornozelo.pdf.
36. Rimando P. Ankle Sprain. eMedicine. 2008. http://emedicine.medscape.com/.
37. Physical Therapy Referral Guidelines: Ankle Sprain. Madigan ArmyMedical Center. 2007. http://www.mamc.amedd.army.mil/referral/guidelines/pt_ankle.htm.
38. Lower Extremity Injury Medical Treatment Guidelines. ColoradoDivision of Labour and Employment. 2009. http://www.coworkforce.com/dwc/notices/adopted_rules/lower_extremity.pdf.
39. Occupational Health Nurse Practitioner Clinical Practice Guideline:Ankle/Foot Injury. Carepoint Industrial Health Services, 2010. http://www.nursing.health.wa.gov.au/docs/career/np/carepoint/CPG_ankle_Foot_Injury.pdf.
40. Clinical Guidelines for the Treatment of Ankle Distorsions. Junta deExtremadura. 2004. http://www.areasaludplasencia.es/3/35/protocolos.php.
41. First Nations and Inuit Health Branch Clinical Practice Guidelines forNurses in Primary Care. Health Canada. 2000. http://www.hc-sc.gc.ca/fniah-spnia/pubs/services/_nursing-infirm/2000_clin-guide/index-eng.php.
42. Nilsson S. Sprains of the lateral ankle ligaments. J Oslo City Hosp1983;33:13e36.
43. Laba E, Roestenburg M. Clinical evaluation of ice therapy for acuteankle sprain injuries. New Zealand Journal of Physiotherapy1989;17:7e9.
44. Wilkerson GB, Horn-Kingery HM. Treatment of the inversion anklesprain: comparison of different modes of compression andcryotherapy. J Orthop Sports Phys Ther 1993;17:240e6.
45. Basur RL, Shephard E, Mouzas GL. A cooling method in thetreatment of ankle sprains. Practitioner 1976;216:708e11.
46. Hocutt JE Jr, Jaffe R, Rylander CR, et al. Cryotherapy in anklesprains. Am J Sports Med 1982;10:316e19.
47. Cote DJ, Prentice WE Jr, Hooker DN, et al. Comparison of threetreatment procedures for minimizing ankle sprain swelling. Phys Ther1988;68:1072e6.
48. Sloan JP, Hain R, Pownall R. Clinical benefits of early cold therapy inaccident and emergency following ankle sprain. Arch Emerg Med1989;6:1e6.
49. Bleakley CM, McDonough SM, MacAuley DC, et al. Cryotherapy foracute ankle sprains: a randomised controlled study of two differenticing protocols. Br J Sports Med 2006;40:700e5.
50. Harrison MB, Legare F, Graham ID, et al. Adapting clinical practiceguidelines to local context and assessing barriers to their use. CMAJ2010;182:E78e84.
51. Pavlidis N. Evidence-based medicine: development andimplementation of guidelines in oncology. Eur J Cancer 2009;45(Suppl 1):468e70.
52. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: Advancingguideline development, reporting, and evaluation in health care.Prev Med 2010;51:421e4.
53. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emergingconsensus on rating quality of evidence and strength ofrecommendations. BMJ 2008;336:924e6.
54. Brouwers MC, Kho ME, Browman GP, et al. Development of theAGREE II, part 1: performance, usefulness and areas forimprovement. CMAJ 2010;182:1045e52.
55. Feder G, Eccles M, Grol R, et al. Clinical guidelines: using clinicalguidelines. BMJ 1999;318:728e30.
56. Shaneyfelt TM, Mayo-Smith MF, Rothwangl J. Are guidelinesfollowing guidelines? The methodological quality of clinical practiceguidelines in the peer-reviewed medical literature. JAMA1999;281:1900e5.
57. Moher D, Cook DJ, Eastwood S, et al. Improving the Quality ofReports of Meta-Analyses of Randomised Controlled Trials: TheQUOROM Statement. Onkologie 2000;23:597e602.
58. Ann S, Carmen M, Christa H. Making the AGREE tool more user-friendly: the feasibility of a user guide based on Boolean operators.J Eval Clin Pract 2009;15:1061e73.
Van de Velde S, Heselmans A, Donceel P, et al. BMJ Qual Saf (2011). doi:10.1136/bmjqs.2010.045435 9
Original research
group.bmj.com on February 25, 2011 - Published by qualitysafety.bmj.comDownloaded from
90
svelde
Rechthoek

DISCUSSION
CHAPTER 7
91

7.1 Contributions of this thesis
The main achievement of this thesis is that we introduced evidence-based
practice to the practice-oriented domain of first aid training and to the Belgian
Red Cross-Flanders. Following the European first aid guidelines project,
evidence-based practice became an integral part of the Belgian Red Cross-
Flanders. The Expertise Centre was founded in 2009 to review evidence in all
the areas where the organisation is active: from blood supply to international
humanitarian aid and social care. In the strategic plan “Pledge 2015” of the
Belgian Red Cross-Flanders, the evidence-based principle is the central thread.
After a project to help develop evidence-based first aid guidelines and materials
specifically directed at the African context, we have now taken the initiative to
introduce evidence-based practice within the network of 186 National Red
Cross and Red Crescent societies.
Although the development of evidence-based guidelines (chapter 2) was new
for the Belgian Red Cross-Flanders, we were able to complete this task within a
strict two-year timeline through an intense collaboration. This was a particular
challenge because the formal development of evidence-based guidelines is
cumbersome and often takes two years or more.31;32 To implement the
guidelines efficiently and effectively, we developed the European First Aid
Manual (EFAM). EFAM combines the guidelines for first aid and guidelines for
resuscitation from the European Resuscitation Council in a format ready for
training the lay public. Authors of first aid manuals can use the EFAM digital
texts and photos to develop or update their first aid courses along the current
European guidelines. By 2011, 32 organisations were already making use of
EFAM for their first aid programmes. An updated version of EFAM is now being
developed taking into account the recommendations of the more recent 2010
guidelines.33-35
92

In a systematic review on the effectiveness of first aid training (chapter 3), we
identified 15 relevant studies. It was regrettable that 10 studies were excluded
because of probable bias. Another study was excluded because of poor
reporting. This finding was an illustration of the amount of waste in research.
However, this review did find two studies that measured the change in practice
with unannounced simulations. From this review we tentatively concluded that
conventional first aid training improved competences but not performance.
Supplementary training on dealing with barriers to helping might increase
helping rates. A limitation of our process for assessing the risk of bias is that we
did not take into account the potential impact of the different quality criteria on
the results of the selected studies. While allocation concealment is one of the
most important quality criteria for RCTs it received equal weight as the other
quality criteria.
The systematic review was paramount to the choice of research question for
the RCT (chapter 4) in this thesis. Designing the RCT with reference to this
systematic review was important because it not only identified, but also
justified the research question and informed us when deciding on the study
design.36;37
In the community-based RCT we found that supplementary training on dealing
with barriers to helping did not alter the time or rate of helping in an acute
myocardial infarction emergency. This finding is different from previous trials
which did find an increase. The good news was that all the participants
demonstrated some type of helping reaction and nearly all the participants
sought help. Despite the very high helping rates, there is still a need to increase
the timeliness and appropriateness of the aid provided. First aid self-efficacy
beliefs were not useful to predict performance.
Since the development of a systematic review is time-consuming and typically
takes 6 to 12 months,38 the Expertise Centre of the Belgian Red Cross-Flanders
93

also uses rapid reviews to realise its goals within the given time and resource
constraints. Two examples of such a rapid review are given in chapter 5.
Although the rapid review on pototo peel dressings for burns presents three
studies, it should be mentioned that only one study provided direct evidence to
the specific question asked. The other two studies provided indirect evidence as
a summary of the best available evidence.
Because evidence regarding the implications of rapid reviews is limited, we
compared the results of this rapid review with a systematic review on the same
topic. We found differences in the selected evidence and conclusions.
Unfortunately the manuscript of the systematic review did not contain the
information required to evaluate why these differences occurred. This
observation illustrated the importance of the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses, i.e. the PRISMA statement.39 It is a
limitation of this thesis that we were not able to compare a broader sample of
rapid and systematic reviews.
An evaluation of guidelines on ice for ankle sprains (chapter 6) illustrated
methodological problems among the included guidelines and shortcomings of
the AGREE instrument to identify them. Later in this chapter we make the link
between the methods used for the European first aid guidelines, the
conclusions from this methodological research, and conclusions from key
commentaries.
7.2 Current methodological perspectives on evidence-based
guidelines in general and on the European first aid guidelines in
particular
Evidence-based guidelines are promoted as an important tool to bridge the gap
between evidence and practice. To be a reliable source of information, it is
94

widely accepted that guideline development methods need to be rigorous and
transparent. Such formal methods must prevent invalid guidelines from
replacing normal clinician variation with consistently inappropriate practice.40
However, a systematic review of guideline appraisal studies, including a total of
627 guidelines published since 1980, demonstrated that many guidelines are of
low quality. Only half of the guidelines (55%, 168 on a subsample of 270
guidelines) could be recommended or recommended with provisos after an
evaluation with the AGREE instrument. The most worrying was the low mean
score for the AGREE rigour of development domain (43%; 95% CI 41.0 to 45.2),
since this domain is considered as the most important indicator of guideline
quality.41
In our methodological research on the rigour of development of practice
guidelines on ice for acute ankle sprains, we illustrated a recurrent problem
associated with evidence-based guidelines: different panels coming to different
conclusions based on a review for the same topic.42 The reasons for this are
many and vary between valid and invalid. From key commentaries on the
quality of guidelines in general we identified five main problems in the
development of evidence-based guidelines relating to: 1) incomplete
identification of evidence, 2) composition of guideline panels, 3) conflicts of
interest, 4) consensus development methods, 5) independent review before
dissemination.32;42;43
Below we discuss the strengths and weaknesses of the European first aid
guideline from this perspective. We also incorporate relevant conclusions from
our methodological research on ice for ankle sprains, since the European first
aid guidelines were among the 21 guidelines analysed.
95

Incomplete identification of evidence
On the one hand, most guidelines cannot be based on evidence alone because
of inevitable gaps in the research for many questions.32;42 On the other hand
they often rely too much on expert opinion because the authors do not cite the
available evidence.43 Reasons for this can be lack of awareness of relevant
evidence or ignoring such evidence.44 Giannakakis et al found that among 40
guidelines published in 1999 in six influential medical journals, only 12.5% did a
systematic review and pertinent RCTs were often not included.45 Now a decade
later, our study on ankle sprain guidelines provides another illustration of this
problem.
Despite the fact that the development process for the European first aid
guidelines included a systematic literature review, we relied heavily on existing
guidelines as a source of information. Although we appraised these guidelines
with the AGREE instrument, our methodological research shows that this was
not a guarantee for identifying the relevant evidence. The ADAPTE procedure
provides a framework on how to use existing guidelines as a source of
information.46
Composition of guideline panels
Studies have shown that the characteristics of experts in panels might influence
the recommendations.47 Sniderman defines this problem as follows: “ what is to
be decided is often already decided with the selection of the deciders”.42 For
example, there is evidence that current performers of a specific procedure
judge it as more appropriate versus non-performing clinicians.47 The
composition of an expert panel is therefore a vital step and advice is given on
this matter in all guideline development handbooks.48 To compose the expert
panel for the European first aid guidelines, we focussed on obtaining a
multidisciplinary panel as it was described in the SIGN guideline developers’
handbook. We selected panellists from a variety of backgrounds with either
96

clinical, training or evidence-based expertise. Taking into account the
importance of this step, we believe that it would be useful if the SIGN handbook
could provide more rigorous procedures for the selection of experts.
Conflict of interest
In guideline panels, a conflict of interest is a situation in which an expert’s
judgement of a recommendation is improperly influenced by financial,
professional, or other personal interest. A typical example is involvement with
drug companies. Such conflicts can make guidelines marketing tools for the
industry.42 Since layperson first aid assumes that minimal or no equipment is
required, the potential for commercial conflicts is limited. More relevant are
intellectual conflicts, which may arise when an expert holds personal strong
views on a guideline topic. In the European first aid guidelines panel members
were asked to declare any possible conflict of interest with respect to the topics
being included. Although the input of experts in the formulation of the
recommendations was important, it was a strength that unconflicted
methodological experts had the main responsibility for the guidelines.
Consensus development methods
The assumed principle behind consensus is that a group has a more valid and
reliable view than an individual.32 However, the presence and actions of a panel
member also affects the actions of others.47;49 To safeguard the validity of
consensus-based recommendations, rigorous procedures on how the experts
interact when formulating recommendations have been recommended.32
Formal consensus methods explicitly define the procedures and output in the
guideline development plan.49 Typical formal approaches include the Delphi
method, the Nominal group technique and the RAND method. While the Delphi
method assembles the viewpoints with mailed questionnaires, the Nominal
Group Technique involves a face-to-face meeting. The RAND method combines
both approaches, by first using mailed questionnaires and then following up
97

with a face-to-face meeting. All approaches include the recording of personal
views, formal group feedback on these views using a structured interaction, and
explicit methods to aggregate the personal views.49
In the European first aid guidelines, the role of expert opinion was significant
since the body of evidence with relevance to layperson first aid is incomplete.
At the start of the meeting we explained the consensus procedures. According
to the SIGN methods we used the considered judgement procedure to move
from the evidence synthesis to formulating recommendations. This considered
judgement took the following factors into account: quantity and quality of the
evidence, the clinical impact and the implementability. During the meeting, the
panel members first considered the available evidence and then discussed the
recommendations until a consensus was reached. While we made extensive use
of consensus to agree on the recommendations, it is a weakness that we did not
use a more formal consensus method. This would have allowed us to structure
the interaction between panel members and to represent the extent of
agreement in the panel per recommendation.
Independent review before dissemination
Many guidelines are not published in scientific journals and the decision to
undertake an external review often depends on the authors. Even if guidelines
are published in a scientific journal, they often bypass the peer-review system.42
As a consequence, many guidelines are disseminated without independent
review or external validation. Among the 21 guidelines on ice for ankle sprains,
only half included an external review before its publication. It was definitely a
strength that the European first aid guidelines were formally validated before
dissemination. This means that an independent committee of three experts
appraised the guidelines using the AGREE instrument.
98

7.3 Potential solutions for drawing the line between evidence-
based and ‘evidence-biased’50 guidelines
The last word on the development of guidelines has clearly not been said. Below
we propose various solutions to improve the quality of guidelines.
Balanced guideline development panels
The selection of panel members usually takes the form of purposive sampling by
the guideline organising committee. This type of sampling opens the door to
bias since the panel is selected subjectively. Formalising the identification and
selection process through public vacancies and criteria listed in expert profile
descriptions might already be an improvement. Below we present two
approaches which are not mentioned in general guideline development
handbooks48 but which might be useful when composing guideline panels.
Maximum heterogeneity sampling, also called maximum variation sampling,
could reduce the risk of selecting a sample with little variation in viewpoints
when a wide variation or controversy is present among experts.51 This selection
procedure involves the identification of extremes in the relevant area of
expertise.
Nominations by practitioners in the field is another approach which might
increase the perceived credibility of the panel among stakeholders and the
chances of implementation.52
Addressing conflict of interest
While evidence-based guidelines usually report on any financial conflicts, this is
much less the case for intellectual conflicts. Disclosure of both financial and
intellectual conflicts would be an improvement. However, disclosing conflicts of
interest is not enough to prevent biased recommendations. If conflicts occur,
these also have to be managed. Several approaches have been suggested.
99

One approach is to ensure that in guideline panels conflicted experts are
balanced by unconflicted ones.43 A more stringent approach is to allow
conflicted experts to provide input in a panel, but to exclude them from
decision-making for the related recommendations.53 One step further is to
exclude conflicted experts from participation in guideline panels.42 Since
participation in a guideline panels is also a type of intellectual conflict, it has
been suggested that the members of the guideline panel are changed each time
a new edition of a guideline is being developed.42;54
Validation framework for guidelines
Reforming the guideline development process is difficult because guideline
development is not centralised and because many guidelines are not published
in peer-reviewed journals.43 In Belgium, the Belgian Centre for Evidence-Based
Medicine (CEBAM) validates guidelines with the AGREE instrument in
combination with a limited analysis of the content. The validation procedure
results in a decision to recommend or not to recommend use of the guideline by
the targeted caregivers. This validation procedure is quite unique. Embedding
such a procedure in other countries or at international level might improve the
quality of guidelines and support the users of guidelines. Further research
comparing the quality of validated with non-validated guidelines is warranted.
7.4 Suggestions for future research
Keeping up-to-date
The number of new trials being published per day is impressive and still
growing. Keeping up-to-date with current evidence is therefore a major
challenge.20 Systematic reviews have an important role to play in keeping track.
Taking into account the findings of our RCT, an update of our systematic review
is recommended.
100

This will also allow the inclusion of an additional study that we missed, and the
identification of any new relevant studies published since the completion of our
search in May 2007.
Can rapid reviews be quick without being dirty 19?
The success of evidence-based practice has led to a rise in review studies.20
Grant and Booth identified 14 commonly published types of reviews, including
rapid reviews. For the reader of such reviews, the value of the different types of
reviews is not always clear. Therefore, it is recommended to explicitly report the
methods and its limitations.19 This is particularly important for rapid reviews,
because of the methodological shortcuts which increase the risk of bias.
Our rapid review was published as a BestBet. In the general introduction of the
BestBet journal section the reader is informed about the standard methods
used and it is reported that BestBets are not meant to be full systematic
reviews. The first sentence of our specific BestBet even mentions that it is a
“short-cut review”.
Informing the reader about the likely effect of this approach would have been
of added value. However, from current research it is not possible to evaluate
how robust they are in comparison to systematic reviews. We believe this forms
an opportunity for further research and we suggest the following plan. When
planning a new systematic review, a preliminary assessment of the available
evidence is also required. If rapid review procedures are consistently used
during this scoping phase, it would be possible to compare the results of the
rapid and fully systematic process afterwards.
Further primary research in non-resuscitative first aid
All the research that we have done illustrates the lack of evidence in the field of
non-resuscitative first aid. The considerable burden of injuries highlights the
need for further primary research. Unfortunately there is a poor correlation
101

between the burden of disease or injury and funding for health and research.55
This is illustrated by the budget allocation of the WHO. In 2006 the WHO
allocated less than 1% of its total budget to injuries, although injuries account
for one tenth of the global burden of disease and injury.1;56
We give as an example ankle sprains, for which the incidence has been
estimated at 1/10000 people per day.57 Common sense and practical experience
have led to the widespread use of bandages as first aid management for
sprained ankle. If you need 1 meter of bandage per ankle sprain, this amounts
to 32,000 km (by way of reference, the length of the equator is about 40,000
km) of bandage per year in Europe alone.28 However, there is weak evidence
that in the case of mild or moderate ankle sprains, elastic bandages do not have
significantly better outcomes than no bandages, and might even lead to worse
outcomes.58-61 New robust evidence would be relevant to reassure users about
which procedures are most appropriate.
Evidence-based practice for laypeople
Typically, the evidence-based discourse is held among professionals. However,
the concept of evidence-based practice is diffusing gradually towards the
general lay public. The layperson can come into contact with evidence-based
practice through shared decision-making during medical visits, information on
the internet or in the general media. In the setting of first aid training, lay first
aid trainers and those attending the training are the end users of the guidelines.
Every five years, these stakeholders are expected to learn the procedures from
the newly published guidelines for basic life-support and now also the
guidelines for non-resuscitative first aid. Encouraging them to do so is especially
difficult when the guidelines contain procedures that conflict with customary
practice or with information in previous versions. This has led to situations in
which laypeople are frustrated with evidence-based practice.
102

A main problem is that many laypeople are unfamiliar with terms related to
medical evidence and may misunderstand the concept of evidence-based
practice.62 While training in evidence-based medicine is now well established
for professional care providers, it is hard to find such training for non-medical
laypeople.63 Effective communication about evidence-based practice is essential
to engage the lay public in evidence-based practice. Since the research on such
training for laypeople is still in its infancy, we believe the first aid setting
provides an opportunity to contribute to this research.
7.5 Conclusions
The number of recommendations in the European first aid guidelines for which
no strong evidence was available, the amount of relevant but biased studies in
the systematic review, and the findings from the methodological research on
guidelines for ice and ankle sprains illustrated that the evidence in first aid was
sometimes disastrous. However, when available we turned evidence into
practice.
Although an editorial about the European first aid guidelines reported that the
European first aid guidelines were “highly appropriate” and an “excellent
start”,64 we are also aware of its shortcomings. A particular strength of the
guidelines was the positive evaluation by a formal external validation
committee. Since the use of external validation procedures for guidelines is
quite unique, this approach might be an important strategy for improving the
quality of guidelines.
Despite the general belief in the potential of first aid training, our systematic
review on the effectiveness of non-resuscitative first aid training showed that it
does not always translate into helping behaviour. The use of deception tests
was identified as a way of measuring emergency helping behaviour.
103

In our community-based trial on conventional first aid training only versus
conventional first aid training with a supplementary intervention to decrease
barriers, we made diverging observations regarding the rate of helping
behaviour versus previous trials. We found that supplementary training did not
alter the helping behaviour. The high loss to follow-up was an important
limitation of this study, making it difficult to derive conclusions. Further
research is necessary to gather information on the helping behaviour of
laypeople trained in first aid.
Unfortunately we were not able to address the question about the validity of
rapid reviews. We believe this provides an opportunity for further research and
have proposed a plan by which it might be evaluated.
The low quality of clinical practice guidelines in general is an important
problem.41 Our methodological study on the quality of guidelines showed that
there is only a thin line between evidence-based practice for accidents and
accidents in evidence-based practice. The AGREE instrument did not highlight
essential methodological shortcomings. We suggest an additional analysis of the
content of the recommendations to evaluate the validity of guidelines. As the
rigour of development and overall quality of many guidelines is low,41 we
recommend caution in viewing guidelines themselves as a form of evidence.
The different studies included in this thesis illustrate that first aid is not merely a
medical topic; it also touches the fields of social psychology, and education.
Using the evidence-based methodology in collaboration with experts in the
range of included topics, we made considered judgements on these matters.
We believe that this thesis made a significant contribution to the field of
evidence-based first aid and has created the enthusiasm to start new evidence-
based projects in first aid and beyond in the area of humanitarian aid.
104

References
105

1 World Health Organisation. The global burden of disease: 2004 update.
Available at:
www.who.int/healthinfo/global_burden_disease/2004_report_update
/en/index.html.
2 Baker CC, Oppenheimer L, Stephens B et al. Epidemiology of trauma
deaths. Am J Surg. 1980;140(1):144-150.
3 Trunkey DD. Trauma. Accidental and intentional injuries account for
more years of life lost in the U.S. than cancer and heart disease. Among
the prescribed remedies are improved preventive efforts, speedier
surgery and further research. Sci Am. 1983;249(2):28-35.
4 Hussain LM, Redmond AD. Are pre-hospital deaths from accidental
injury preventable? BMJ. 1994;308(6936):1077-1080.
5 Coats TJ, Davies G. Prehospital care for road traffic casualties. BMJ.
2002;324(7346):1135-1138.
6 Pelinka LE, Thierbach AR, Reuter S et al. Bystander trauma care--effect
of the level of training. Resuscitation. 2004;61(3):289-296.
7 Donner-Banzhoff N, Schuster C, Hofmann S et al. [Community
emergency medical service. Epidemiology and quality of treatment in a
rural district]. Anasthesiol Intensivmed Notfallmed Schmerzther.
1999;34(3):140-145.
8 Miles S. First-aid training. BMJ. 1969;4(5681):485-487.
9 Pearn J. The earliest days of first aid. BMJ. 1994;309(6970):1718-1720.
10 Chamberlain DA, Hazinski MF. Education in resuscitation. Resuscitation.
2003;59(1):11-43.
11 Part 3: adult basic life support. European Resuscitation Council.
Resuscitation. 2000;46(1-3):29-71.
12 2005 International Consensus on Cardiopulmonary Resuscitation and
Emergency Cardiovascular Care Science with Treatment
106

Recommendations. Part 2: Adult basic life support. Resuscitation.
2005;67(2-3):187-201.
13 Guyatt G. Evidence-based Medicine. ACP J Club. 1991;114(suppl 2):A16.
14 Evidence-based medicine. A new approach to teaching the practice of
medicine. JAMA. 1992;268(17):2420-2425.
15 Sackett DL, Rosenberg WM, Gray JA et al. Evidence based medicine:
what it is and what it isn't. BMJ. 1996;312(7023):71-72.
16 Petticrew M. Systematic reviews from astronomy to zoology: myths
and misconceptions. BMJ. 2001;322(7278):98-101.
17 Cochrane Handbook for Systematic Reviews of Interventions Version
5.0.2. Available at: www.cochrane-handbook.org.
18 Moher D, Liberati A, Tetzlaff J et al. Preferred reporting items for
systematic reviews and meta-analyses: the PRISMA statement. Ann
Intern Med. 2009;151(4):264-9, W64.
19 Grant MJ, Booth A. A typology of reviews: an analysis of 14 review
types and associated methodologies. Health Info Libr J. 2009;26(2):91-
108.
20 Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven
systematic reviews a day: how will we ever keep up? PLoS Med.
2010;7(9):e1000326.
21 Clinical Practice Guidelines: Directions for a New Program. Institute of
Medicine. Washington DC: National Academy Press; 1990.
22 Rosenfeld RM. Commentary: guidelines and otolaryngology.
Otolaryngol Head Neck Surg. 2006;134(4 Suppl):S1-S3.
23 Woolf SH, Grol R, Hutchinson A et al. Clinical guidelines: potential
benefits, limitations, and harms of clinical guidelines. BMJ.
1999;318(7182):527-530.
24 Cruse H, Winiarek M, Marshburn J et al. Quality and methods of
developing practice guidelines. BMC Health Serv Res. 2002;2(1):1.
107

25 Ofeigsson OJ. Observations and experiments on the immediate cold-
water treatment for burns and scalds. Br J Plast Surg. 1959;12:104-119.
26 Cuttle L, Pearn J, McMillan JR et al. A review of first aid treatments for
burn injuries. Burns. 2009;35(6):768-775.
27 Apostoli A, Caula C. Treatment of minor burns: treatment of burns is
controversial. BMJ. 2004;329(7460):292.
28 Wilson S, Cooke M. Double bandaging of sprained ankles. BMJ.
1998;317(7174):1722-1723.
29 Thierbach AR, Pelinka LE, Reuter S et al. Comparison of bystander
trauma care for moderate versus severe injury. Resuscitation.
2004;60(3):271-277.
30 Mackway-Jones K, Carley S. bestbets.org: odds on favourite for
evidence in emergency medicine reaches the world wide web. J Accid
Emerg Med. 2000;17(4):235-236.
31 Schunemann HJ, Hill SR, Kakad M et al. Transparent development of
the WHO rapid advice guidelines. PLoS Med. 2007;4(5):e119.
32 Raine R, Sanderson C, Black N. Developing clinical guidelines: a
challenge to current methods. BMJ. 2005;331(7517):631-633.
33 Markenson D, Ferguson JD, Chameides L et al. Part 13: First aid: 2010
American Heart Association and American Red Cross International
Consensus on First Aid Science With Treatment Recommendations.
Circulation. 2010;122(16 Suppl 2):S582-S605.
34 Markenson D, Ferguson JD, Chameides L et al. Part 17: first aid: 2010
American Heart Association and American Red Cross Guidelines for
First Aid. Circulation. 2010;122(18 Suppl 3):S934-S946.
35 Sayre MR, Koster RW, Botha M et al. Part 5: Adult basic life support:
2010 International Consensus on Cardiopulmonary Resuscitation and
Emergency Cardiovascular Care Science With Treatment
Recommendations. Circulation. 2010;122(16 Suppl 2):S298-S324.
108

36 Chalmers I, Glasziou P. Avoidable waste in the production and
reporting of research evidence. Lancet. 2009;374(9683):86-89.
37 Clarke M, Hopewell S, Chalmers I. Clinical trials should begin and end
with systematic reviews of relevant evidence: 12 years and waiting.
Lancet. 2010;376(9734):20-21.
38 Allen IE, Olkin I. Estimating time to conduct a meta-analysis from
number of citations retrieved. JAMA. 1999;282(7):634-635.
39 Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for
reporting systematic reviews and meta-analyses of studies that
evaluate health care interventions: explanation and elaboration. J Clin
Epidemiol. 2009;62(10):e1-34.
40 Thomson R, McElroy H, Sudlow M. Guidelines on anticoagulant
treatment in atrial fibrillation in Great Britain: variation in content and
implications for treatment. BMJ. 1998;316(7130):509-513.
41 Alonso-Coello P, Irfan A, Sola I et al. The quality of clinical practice
guidelines over the last two decades: a systematic review of guideline
appraisal studies. Qual Saf Health Care. 2010;19(6):e58.
42 Sniderman AD, Furberg CD. Why guideline-making requires reform.
JAMA. 2009;301(4):429-431.
43 Shaneyfelt TM, Centor RM. Reassessment of clinical practice
guidelines: go gently into that good night. JAMA. 2009;301(8):868-869.
44 Oxman AD, Glasziou P, Williams JW, Jr. What should clinicians do when
faced with conflicting recommendations? BMJ. 2008;337:a2530.
45 Giannakakis IA, Haidich AB, Contopoulos-Ioannidis DG et al. Citation of
randomized evidence in support of guidelines of therapeutic and
preventive interventions. J Clin Epidemiol. 2002;55(6):545-555.
46 Fervers B, Burgers JS, Haugh MC et al. Adaptation of clinical guidelines:
literature review and proposition for a framework and procedure. Int J
Qual Health Care. 2006;18(3):167-176.
109

47 Hutchings A, Raine R. A systematic review of factors affecting the
judgments produced by formal consensus development methods in
health care. J Health Serv Res Policy. 2006;11(3):172-179.
48 Turner T, Misso M, Harris C et al. Development of evidence-based
clinical practice guidelines (CPGs): comparing approaches. Implement
Sci. 2008;3:45.
49 Murphy MK, Black NA, Lamping DL et al. Consensus development
methods, and their use in clinical guideline development. Health
Technol Assess. 1998;2(3):i-88.
50 Evidence b(i)ased medicine. BMJ. 2003;326(7389):602.
51 Bruce JC, Langley GC, Tjale AA. The use of experts and their judgments
in nursing research: an overview. Curationis. 2008;31(4):57-61.
52 Johnston SC, Nguyen-Huynh MN, Schwarz ME et al. National Stroke
Association guidelines for the management of transient ischemic
attacks. Ann Neurol. 2006;60(3):301-313.
53 Hirsh J, Guyatt G. Clinical experts or methodologists to write clinical
guidelines? Lancet. 2009;374(9686):273-275.
54 Guyatt G, Akl EA, Hirsh J et al. The vexing problem of guidelines and
conflict of interest: a potential solution. Ann Intern Med.
2010;152(11):738-741.
55 Chalmers I, Glasziou P. Avoidable waste in the production and
reporting of research evidence. Lancet. 2009;374(9683):86-89.
56 Stuckler D, King L, Robinson H et al. WHO's budgetary allocations and
burden of disease: a comparative analysis. Lancet.
2008;372(9649):1563-1569.
57 Kannus P, Renstrom P. Treatment for acute tears of the lateral
ligaments of the ankle. Operation, cast, or early controlled
mobilization. J Bone Joint Surg Am. 1991;73(2):305-312.
110

58 Rucinkski TJ, Hooker DN, Prentice WE et al. The effects of intermittent
compression on edema in postacute ankle sprains. J Orthop Sports Phys
Ther. 1991;14(2):65-69.
59 Brooks SC, Potter BT, Rainey JB. Treatment for partial tears of the
lateral ligament of the ankle: a prospective trial. Br Med J (Clin Res Ed).
1981;282(6264):606-607.
60 Watts BL, Armstrong B. A randomised controlled trial to determine the
effectiveness of double Tubigrip in grade 1 and 2 (mild to moderate)
ankle sprains. Emerg Med J. 2001;18(1):46-50.
61 Linde F, Hvass I, Jurgensen U et al. Compression bandage in the
treatment of ankle sprains. A comparative prospective study. Scand J
Rehabil Med. 1984;16(4):177-179.
62 Carman KL, Maurer M, Yegian JM et al. Evidence that consumers are
skeptical about evidence-based health care. Health Aff (Millwood ).
2010;29(7):1400-1406.
63 Berger B, Steckelberg A, Meyer G et al. Training of patient and
consumer representatives in the basic competencies of evidence-based
medicine: a feasibility study. BMC Med Educ. 2010;10:16.
64 Handley AJ. European first aid guidelines. Resuscitation.
2007;72(2):178-179.
111

112

Summary
113

Introduction
In order to improve the quality of care, evidence-based practice seeks to bridge
the gap between evidence and practice.While cardiopulmonary resuscitation by
laypeople was extensively studied and evidence-based guidelines were
published, the field of non-resuscitative first aid lagged behind in applying
evidence-based practice. Taking into account the considerable burden of injury,
the life-saving potential of first aid, the potential benefits of evidence-based
practice, areas of controversy in first aid, and the gaps in systematic analysis of
first aid evidence, it was the purpose of this thesis to introduce evidence-based
practice in the first aid training activities of the Belgian Red Cross-Flanders and
to add new empirical data to the research base.
Methods
To realise this objective we first produced an evidence-based guideline to
determine the most effective, safe, and feasible first aid techniques and
procedures, and to formulate recommendations for training.
Next we performed a systematic review to evaluate the effectiveness of first aid
training. This systematic review also led us to the design of a randomised
controlled trial (RCT) to evaluate if training on barriers to helping facilitates
emergency helping behaviour among laypersons trained in first aid. We
evaluated this by means of a deception test in which the participants were
unaware that an emergency was simulated and did not know that their helping
behaviour was being evaluated. Having the confidence to provide first aid may
influence helping barriers. Therefore this RCT also measured the participants’
self-efficacy beliefs and related these to the performance demonstrated in the
deception.
114

The pressing need for information, especially in emergency care settings, has
given rise to the methodology of rapid reviews in which methods for the search,
appraisal, synthesis and analysis are determined by time constraints. We
conducted two such rapid reviews for very specific clinical questions. Because
there is limited evidence regarding the validity of rapid reviews, we compared
the results of one of our rapid reviews with a systematic review on the same
topic. Finally, we tried to add to the research in the quality of evidence-based
guidelines by evaluating the content and rigour of development of
recommendations on the use of ice in guidelines for acute ankle sprains.
Results
With a multidisciplinary panel of European experts that considered the findings
from the available evidence, we produced European guidelines on safety
measures, emergency removal of victims, psychosocial first aid and first aid for
trauma and oral poisoning. Our systematic review found two studies that
succeeded in measuring the change in helping behaviour after first aid training.
Based on these studies we tentatively concluded that conventional first aid
training improved competences but not performance. Supplementary training
on dealing with barriers to helping might increase helping rates. In our RCT we
found that such supplementary training did not alter the time or rate of helping
in an acute myocardial infarction emergency. The good news was that all the
participants demonstrated some type of helping reaction and nearly all the
participants sought help. Despite the very high helping rates, there is still a need
to increase the timeliness and appropriateness of the aid provided. First aid self-
efficacy beliefs were not correlated with performance.
The comparison between a rapid review and a systematic review on the same
topic demonstrated differences in the selected evidence and conclusions. From
the manuscript of the systematic review it was not possible to evaluate the
reasons for these differences. In a published letter to the editor we drew
attention to adherence to the Preferred Reporting Items for Systematic Reviews
and Meta-Analyses, i.e. the PRISMA statement.
115

The evaluation of guidelines on ice for ankle sprains found methodological
problems among the included guidelines and shortcomings of the AGREE
instrument to identify them. The 21 guidelines included in the analysis,
contained clinically significant variations in their recommendations. The
variation was not related to the quality of the guideline.
Discussion
The main achievement of this thesis is that we introduced evidence-based
practice to the practice-oriented domain of first aid training and to the Belgian
Red Cross-Flanders. In 2009, the Belgian Red Cross-Flanders founded the
Expertise Centre which reviews evidence in all the areas where the organisation
is active. Furthermore, the evidence-based principle became the central
principle in the strategic plan “Pledge 2015” of the Belgian Red Cross-Flanders.
The number of recommendations in the European first aid guidelines for which
no strong evidence was available, the amount of relevant but biased studies in
the systematic review, and the findings from the methodological research on
guidelines for ice and ankle sprains illustrated that the evidence in first aid was
sometimes disastrous. However, when available we turned evidence into
practice.
In our community-based trial we made diverging observations versus previous
trials regarding the effect of supplementary training on dealing with barriers to
helping and regarding the rate of helping behaviour. The high loss to follow-up
was an important limitation of this study, making it difficult to derive
conclusions. First aid self-efficacy beliefs did not appear to be a good predictor
of performance. Deception tests showed to be a useful way to gather
information on the helping behaviour of laypeople trained in first aid.
Our comparison of guidelines on ankle sprains illustrated that many guidelines
suffer from methodological shortcomings. To evaluate the validity of guidelines,
we suggest an analysis of the content of the recommendations in addition to an
116

AGREE evaluation. We recommend caution in viewing guidelines themselves as
a form of evidence and we made suggestions to improve the quality of
evidence-based guidelines. Further research is needed to address the question
about the validity of rapid reviews and a concept to evaluate this has been
presented.
We believe that this thesis made a significant contribution to the field of
evidence-based first aid and has created the enthusiasm to start new evidence-
based projects in first aid and beyond in the area of humanitarian aid.
117

118

Samenvatting
119

Inleiding
Evidence-based practice tracht de kwaliteit van zorg te verhogen door de kloof
tussen onderzoek en praktijk te overbruggen. Er is uitgebreid onderzoek gedaan
naar cardiopulmonaire reanimatie door leken en de bevindingen werden
vertaald naar evidence-based richtlijnen. Op het vlak van eerste hulp naast
reanimatie stond evidence-based practice nog in de kinderschoenen.
Rekening houdend met de aanzienlijke impact van traumatische letsels, het
levensreddende potentieel van eerste hulp, de potentiële voordelen van
evidence-based practice, gebieden van tegenstrijdigheid in eerste hulp, en de
nood aan een systematische analyse van evidence aangaande eerste hulp, was
het doel van deze thesis om evidence-based practice te introduceren in het
eerstehulponderwijs van Rode Kruis-Vlaanderen en om nieuwe empirische
gegevens te verzamelen.
Methodes
Om deze doelstelling te realiseren, ontwikkelden we eerst een evidence-based
richtlijn. Deze richtlijn bepaalde de meest effectieve, veilige en toepasbare
eerstehulptechnieken en formuleerde aanbevelingen voor training.
Vervolgens voerden we een systematische review uit om de effectiviteit van
eerstehulponderwijs te evalueren. Deze review bepaalde ook het
onderzoeksplan voor een randomised controlled trial (RCT). Deze RCT
onderzocht of training aangaande drempels tot het bieden van hulp een
positieve invloed heeft op het helpend gedrag in noodsituaties van leken
getraind in eerste hulp. We maakten gebruik van een misleidingstest om het
helpend gedrag te evalueren. In deze misleidingstest wisten de deelnemers niet
dat een noodsituatie gesimuleerd werd, noch dat hun helpend gedrag
geobserveerd werd. Vertrouwen hebben in het bieden van eerste hulp, zou de
drempels tot het bieden van hulp kunnen beïnvloeden. Daarom hebben we in
120

deze RCT ook gekeken of er een verband was tussen de
zelfeffectiviteitsverwachting van de deelnemers en hun helpend gedrag tijdens
de misleidingstest.
De nood aan snel beschikbare informatie, in het bijzonder in de context van
spoedeisende hulp, heeft geleid tot de methodologie van rapid reviews. In deze
rapid reviews worden de methodes voor het zoeken, beoordelen en
samenvatten van evidence bepaald door de tijdsbeperkingen. Wij hebben rapid
reviews uitgevoerd voor twee specifieke praktijkvragen. Omdat het onderzoek
naar de validiteit van rapid reviews erg beperkt is, hebben we de conclusies van
een van onze rapid reviews vergeleken met die van een systematische review
over hetzelfde onderwerp. Tenslotte, probeerden we een bijdrage te leveren
aan het onderzoek naar de kwaliteit van evidence-based richtlijnen door de
inhoud en methodologische kwaliteit van richtlijnen over het gebruik van ijs
voor acute enkelverstuikingen te vergelijken.
Resultaten
Een multidisciplinair panel van Europese experten nam de beschikbare evidence
in overweging en produceerde aanbevelingen aangaande
veiligheidsmaatregelen, noodevacuatie van slachtoffers, psychosociale eerste
hulp en eerste hulp voor trauma en orale vergiftiging.
De systematische review vond twee studies die erin geslaagd waren om het
effect van eerstehulptraining op het helpend gedrag te meten. Gebaseerd op
deze studies concludeerden we, onder voorbehoud van verdere studies, dat
conventioneel eerstehulponderwijs wel de competenties verhoogde maar geen
invloed had op het helpend gedrag. Bijkomende training aangaande drempels
tot het bieden van hulp zou het aantal mensen die hulp bieden in noodsituaties
kunnen verhogen.
In onze RCT vonden we dat deze bijkomende training geen invloed had op het
121

helpend gedrag voor een acute hartaanval. Het goede nieuws was dat bijna alle
deelnemers enige vorm van hulp boden. Desondanks bleek er ook een nood om
de snelheid en juistheid van de geboden hulp te verbeteren. De
zelfeffectiviteitsverwachting was niet gecorreleerd met het helpend gedrag.
De vergelijking tussen een rapid review en een systematische review over
hetzelfde onderwerp stelde verschillen vast met betrekking tot de
geselecteerde evidence en de conclusies. Het manuscript van deze
systematische review stond niet toe om de redenen voor deze verschillen te
achterhalen. In een gepubliceerde brief aan de redactie beklemtoonden we het
belang van een goede rapportering van het systematische review proces aan de
hand van de Preferred Reporting Items for Systematic Reviews and Meta-
Analyses, met name de PRISMA statements.
De evaluatie van aanbevelingen over ijs voor enkelverstuikingen vond
methodologische problemen in de richtlijnen die het AGREE instrument niet kon
identificeren. De 21 geïdentificeerde richtlijnen waren beduidend verschillend
in hun aanbevelingen. Deze variatie was niet gerelateerd aan de kwaliteit van
de richtlijn.
Discussie
De belangrijkste verwezenlijking van deze thesis is dat we evidence-based
practice hebben geïntroduceerd in het praktijkgerichte eerstehulponderwijs en
in de werking van Rode Kruis-Vlaanderen in het algemeen. In 2009 richtte Rode
Kruis-Vlaanderen het Expertisecentrum op dat evidence samenvat voor alle
activiteiten van de organisatie. Bovendien werd de evidence-based aanpak de
rode draad in het strategische plan, “Afspraak 2015”, van Rode Kruis-
Vlaanderen.
Het aantal aanbevelingen in de Europese eerstehulprichtlijnen waarvoor geen
sterke evidence beschikbaar was, het aantal relevante maar gebiaste studies in
122

de systematische review, en de bevindingen van het methodologisch onderzoek
over richtlijnen voor ijs bij enkelverstuikingen illustreerden dat de evidence over
eerste hulp soms rampzalig was. Wanneer er echter evidence beschikbaar was,
hebben we deze wetenschappelijke resultaten kunnen vertalen naar de praktijk.
In onze RCT maakten we, in vergelijking met vorige studies, afwijkende
vaststellingen aangaande het effect van bijkomende training over drempels tot
het bieden van hulp en aangaande het helpend gedrag in het algemeen. Het
hoge aantal uitvallers in de studie was een belangrijke beperking die het
moeilijk maakte om besluiten te trekken. De zelfeffectiviteitsverwachting
aangaande eerste hulp bleek geen goede predictor te zijn van het helpend
gedrag. Misleidingstesten bleken een nuttige manier om informatie te
verzamelen over het helpend gedrag van leken getraind in eerste hulp.
Onze vergelijking van richtlijnen over enkelverstuikingen illustreerde dat vele
richtlijnen methodologische problemen hebben. Om de geldigheid van
richtlijnen te evalueren, stellen we aanvullend bij de AGREE evaluatie ook een
analyse van de inhoud van de aanbevelingen voor. We manen aan tot
voorzichtigheid wanneer richtlijnen als een vorm van evidence worden gezien
en maakten suggesties om de kwaliteit van evidence-based guidelines te
verhogen. Verder onderzoek is nodig om de vraag over de validiteit van rapid
reviews te beantwoorden. Een concept om dit te evalueren werd voorgesteld in
de thesis.
We denken dat deze thesis een belangrijke bijdrage heeft geleverd in het
domein van evidence-based eerste hulp. Tevens hebben we het nodige
enthousiasme gecreëerd om nieuwe evidence-based projecten te starten in het
domein van eerste hulp en ook ruimer in het gebied van humanitaire hulp.
123

124

Professional career
125

In 2000, Stijn Van de Velde completed his Licence in Physical Therapy at the
University of Ghent. He commenced his career as a physical therapist working
with children suffering from asthma, mucoviscidosis or obesity and served the
Belgian national rowing teams in training camps and international competitions.
As a result of his strong interest in humanitarian aid, Stijn studied in a
Postgraduate program on Development Cooperation.
After that, he joined the Belgian Red Cross-Flanders in 2002 as project manager
on sports injury prevention. During his work at the Belgian Red Cross, he started
a part-time Masters degree in Public Health Methodology and graduated with
great distinction in 2005. In this study he was intrigued by the evidence-based
methodology and, as project manager of the European first aid guidelines and
manual project, Stijn took up the challenge to implement this within the Red
Cross.
Evidence-based practice has since become an integral part of the Belgian Red
Cross-Flanders. To implement evidence-based practice in the Belgian Red Cross-
Flanders, Stijn was closely involved in the establishment of the Expertise Centre.
This centre systematically revises all the programmes that are run so that they
can carry the label ‘evidence-based’. Following the European first aid project, he
also used the evidence-based methodology to create African first aid guidelines
and training material.
Within the international Red Cross movement, Stijn has been elected by the
First Aid Education European Network as member of the steering committee.
This network brings together those responsible for first aid from Red Cross
National Societies in the Pan-European region. He also co-authored the
International first aid guidelines published in 2010 by the International
Federation of the Red Cross and Red Crescent.
126

In parallel with his work at the Red Cross, Stijn started working for the Belgian
Centre for Evidence-based Medicine (CEBAM) in 2007. In this Centre he gives
methodological advice to guideline authors, participates in the validation of
Belgian clinical practice guidelines, and gives training on evidence-based
medicine.
Stijn Van de Velde (32 years) is married to Kriki and they have 3 daughters.
127

128

List of publications
129

International peer reviewed journals
Van de Velde S, Heselmans A, Donceel P, Vandekerckhove P, Ramaekers D,
Aertgeerts B. Rigour of development does not AGREE with recommendations in
practice guidelines on the use of ice for acute ankle sprains. BMJ Qual Saf. 2011
(Epublication ahead of print).
Van de Velde S, De Buck E, Dieltjens T, Aertgeerts B. Medicinal use of potato-
derived products: conclusions of a rapid versus full systematic review. Phytother
Res. 2010 (Epublication ahead of print).
De Buck E, Van de Velde S. Towards evidence based emergency medicine: best
BETs from the Manchester Royal Infirmary. BET 1. Optimal body position in oral
poisoning cases. Emerg Med J. 2010; 27(12):952-3.
De Buck E, Van de Velde S. Towards evidence based emergency medicine: best
BETs from the Manchester Royal Infirmary. BET 2: potato peel dressings for
burn wounds. Emerg Med J. 2010;27(1):55-56.
Heselmans A, Donceel P, Aertgeerts B, Van de Velde S, Ramaekers D. The
attitude of Flemish occupational health physicians toward evidence-based
occupational health and clinical practice guidelines. Int Arch Occup Environ
Health . 2010;83(2):201-208.
Van de Velde S, Heselmans A, Roex A, Vandekerckhove P, Ramaekers D,
Aertgeerts B. Effectiveness of nonresuscitative first aid training in laypersons: a
systematic review. Ann Emerg Med. 2009;54(3):447-457.
Heselmans A, Van de Velde S, Donceel P, Aertgeerts B, Ramaekers D.
Effectiveness of electronic guideline-based implementation systems in
ambulatory care settings - a systematic review. Implement Sci. 2009;4:82.
130

Heselmans A, Donceel P, Aertgeerts B, Van de Velde S, Ramaekers D. The
attitude of Belgian social insurance physicians towards evidence-based practice
and clinical practice guidelines. BMC Fam Pract. 2009;10:64.
Van de Velde S, Broos P, Van Bouwelen M, De Win R, Sermon A, Verduyckt J,
Van Tichelen A, Lauwaert D, Vantroyen B, Tobback C, Van den Steene P, Villere
S, Mieres CU, Gobl G, Schunder S, Monsieurs K, Bierens J, Cassan P, Davoli E,
Sabbe M, Lo G, De Vries M, Aertgeerts B. European first aid guidelines.
Resuscitation. 2007;72(2):240-251.
Other journals
Van de Velde S, Broos P, Van Bouwelen M, De Win R, Sermon A, Verduyckt J,
Van Tichelen A, Lauwaert D, Vantroyen B, Tobback C, Van den Steene P, Villere
S, Mieres CU, Göbl G, Schunder S, Monsieurs K, Bierens J, Cassan P, Davoli E,
Sabbe M, Lo G, De Vries M, Aertgeerts B; Europese richtlijnen voor eerste hulp.
Huisarts Nu. 2009;38(4):159-166.
Training manuals
AFAM project Group. African first aid materials. Published by the Belgian Red
Cross-Flanders, 2010.
EFAM project Group. European First Aid Manual. Published by the Belgian Red
Cross-Flanders, 2007.
131

Translations
Van de Velde S, Verbeke H, Rosenbrand K, Burgers J. (2010). Translation from
English to Dutch of the Appraisal of Guidelines for Research and Evaluation
(AGREE) II Instrument. Available at www.agreetrust.org.
Presentations on symposia
Van de Velde S, Heselmans A, Roex A, Vandekerckhove P, Ramaekers D,
Aertgeerts B. (2008). How effective is first aid training? Association for Medical
Education in Europe (AMEE) Conference, Prague, Czech Republic.
Van de Velde S. (2007).First aid guidelines and evidence-based medicine.
European first aid guidelines. European congress on CPR, Prehospital Care and
Prevention, Ostend, Belgium.
Van de Velde S. (2007). Evidence based practice in first aid. Expert meeting
Science and Practice in Disaster Management, Arnhem, Netherlands.
Van de Velde S. (2007). Evidence based practice in first aid. First aid symposium,
Tampere, Finland.
132

Acknowledgements
133

Now that my PhD project is coming to an end, I want to express my sincere
gratitude to many people for their support, interest and enthusiasm.
First of all I would like to thank my promoters Bert Aertgeerts, Dirk Ramaekers
and Philippe Vandekerckhove. It was a great honour to learn from you and I
hope that my respect came across. Thanks to you, I have reached a professional
milestone in my career. Bert, you wisely guided me along the way and patiently
answered my many questions. Your ‘people first’ approach made the work a
pleasure and strongly encouraged me to continue when the going got tough.
Dirk, your commitment to excellence always challenged and motivated me.
Many thanks for being such a valuable sparring partner. Philippe, thank you for
the opportunities to achieve this goal and for your enthusiasm in setting up the
Expertise Centre.
My sincere thanks also goes to the members of the jury for their efforts in
evaluating my work. I also want to thank the co-authors in my research and the
Medical Commission of the Belgian Red Cross-Flanders for the productive
collaboration.
To the members of the RESCUI research group. Apart from the advice and
guidance that you offered, I very much enjoyed all the good laughs during our
monthly meetings. Annemie, my fellow PhD student, thank you for your help
with the research. You definitely have my respect for your achievements, keep
going. Olivier, good luck with your project.
I am grateful to my colleagues and volunteers from the Red Cross for helping
me to implement the research. I was lucky to work with you. To my manager
Katja, thank you for the confidence and I especially remember the great times
we had during the Nairobi and Cape Town meetings. Special thanks to Emmy,
Tessa and Nele for being such a motivated colleagues. It’s a pleasure to walk
the evidence-based path with you (and I am not referring to the memorable
134

walks after the colloquia in Colorado and London). For those that were involved
in the deception tests, I hope it has been memorable for you as well. A special
word of thanks to Firmin, Frans and Jacques for simulating the many heart
attacks and to Bea for giving the training sessions for the RCT.
To my colleagues from CEBAM, I admire you for your talent to explain
something difficult in an easy way and thanks for the friendly and supportive
work environment.
Marina and Katrien, I very much appreciated your practical assistance during
and at the end of my thesis.
On a personal level I also want to thank my friends for the nice moments
throughout these years which have helped me think of something other than
evidence.
Maarten, many thanks for the good times that we always have together and for
being my brother and dearest friend.
Of course I cannot thank my parents enough for all they have given me. Thank
you for being such a great example and for your support in making my dreams
come true. I recall some time ago how you always wanted me to get a bit more
organised. You would be surprised to see how I have my ‘stuff’ managed now.
However, evidence-based searches still can’t solve the problem of where I left
my keys this time.
Finally, my gratitude goes to my dear Kriki. Thank you for helping me see things
in perspective and for reminding me of what is important in life. I’m fortunate
that you are my personal coach.
Eleni, Stiene en Nienke, ook jullie hebben een hele bijdrage geleverd (ondanks
dat ik even werkonbekwaam was toen Stiene vakkundig de toetsen van mijn
135

klavier had gepeuterd). Met jullie zelf bereide ‘goestingsiroop’ zijn jullie mijn
drie kleine feeën.
136

Appendix
European first aid guidelines: search strategy
137

Key question
1."What is the efficacy and feasibility of ensuring accident site safety by a lay person after a road accident ?"
Search strategy
N° Type Limits Databases Search terms Date of search
1. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
road accident, traffic accident, site protection, accident spot
july 2005
Individual studies
No limits
Pubmed "Accidents, Traffic"[MeSH] AND ("First Aid" OR "Rescue work" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") AND ("site protection" OR "Accident Prevention"[MeSH] OR "Safety")
sep/05
Embase 'traffic accident'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND ('accident prevention'/exp OR 'site protection' OR 'safety'/exp) AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(road accident OR traffic accident ) AND TS=(first aid OR rescue* OR prehospital OR out of hospital) AND TS=(scene protect* OR site protect* OR scene assess* OR site assess* OR safety)
138

Key question
2. "What is the efficacy and feasibility of ensuring accident site safety by a lay person in case of fire ?"
Search strategy
N° Type Limits Databases Search terms Date of search
2. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
fire july 2005
Individual studies
No limits
Pubmed “Fires”[MeSH] AND ("First Aid" OR "Rescue work" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") AND ("site protection" OR "Accident Prevention"[MeSH] OR "Safety")
sep/05
Embase 'fire'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND ('accident prevention'/exp OR 'site protection' OR 'safety'/exp) AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=fire AND TS=(first aid OR rescue* OR prehospital OR out of hospital) AND TS=(scene protect* OR site protect* OR scene assess* OR site assess* OR safety)
139

Key question
3. "What is the efficacy and feasibility of ensuring accident site safety by a lay person after an electrical accident ?”
Search strategy
N° Type Limits Databases Search terms Date of search
3. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
electric injury, electrocution, electric accident, electric shock
july 2005
Individual studies
No limits
Pubmed "Electric Injuries"[MeSH] AND ("First Aid" OR "Rescue work" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") AND ("site protection" OR "Accident Prevention"[MeSH] OR "Safety")
sep/05
Embase 'electric accident'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND ('accident prevention'/exp OR 'site protection' OR 'safety'/exp) AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(electrocution* OR electric* accident* OR electric* injur* OR electric* shock*) AND TS=(first aid OR rescue* OR prehospital OR out of hospital) AND TS=(scene protect* OR site protect* OR scene assess* OR site assess* OR safety)
140

Key question
4. “Under what conditions should the lay person remove the casualty from the scene of the accident.”
Search strategy
N° Type Limits Databases Search terms Date of search
4 Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
evacuation, emergency removal, casualty removal, casualty transport, casualty movement
july 2005
Individual studies
No limits
Pubmed ("Accidents"[MeSH] OR "Emergencies"[MeSH]) AND (lifting OR evacuation) AND ("First Aid" OR "Rescue work"[MeSH] OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
sep/05
Embase ('accident'/exp OR 'emergency'/exp) AND ('lifting'/exp OR 'evacuation') AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(accident* OR emergenc*) AND TS=(lifting OR evacuation OR) AND TS=(first aid OR rescue OR prehospital OR out of hospital)
141

Key question
5. “What is the safety, efficacy and feasibility of emergency removal from the scene of the accident of a casualty by one or two lay persons.”
Search strategy
N° Type Limits Databases Search terms Date of search
5 Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
evacuation, emergency removal, casualty removal, casualty transport, casualty movement
july 2005
Individual studies
No limits
Pubmed ("Accidents"[MeSH] OR "Emergencies"[MeSH]) AND (lifting OR evacuation) AND ("First Aid" OR "Rescue work"[MeSH] OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
sep/05
Embase ('accident'/exp OR 'emergency'/exp) AND ('lifting'/exp OR 'evacuation') AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(accident* OR emergenc*) AND TS=(lifting OR evacuation OR) AND TS=(first aid OR rescue OR prehospital OR out of hospital)
142

Key question
6. “What is the safety, efficacy and feasibility of using a tourniquet, direct pressure, pressure points and elevation, done in the first aid management by a lay person of a severe external bleeding?”
Search strategy
N° Type Limits Databases Search terms Date of search
6. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
Hemorrhage OR haemorrhage OR bleeding OR hemostasis OR tourniquets
july 2005
Individual studies
No limits
Pubmed ("Hemorrhage"¨[MeSH] OR bleeding*) AND (elevation OR pressure OR "Bandages"[MeSH] OR tourniquet* OR "Hemostasis"[MeSH]) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
sep/05
Embase 'bleeding'/exp AND ('elevation' OR ' pressure'/exp OR 'bandage'/exp OR tourniquet* OR 'hemostasis'/exp) AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(hemorrhage) AND TS=(first aid OR prehospital OR out of hospital) AND TS=(elevation OR pressure OR bandage OR tourniquet OR hemostasis) NOT TS=(surg* OR cerebr* OR stroke OR infarct* OR gastro* OR hepato* OR obstet* OR pulm* OR transfus* OR serum OR fluid* OR neuro*)
143

Key question
7. “Under what conditions should a lay person suspect a spinal injury or head trauma in infants, children and adults?”
Search strategy
N° Type Limits Databases Search terms Date of search
7. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
head injury, cerebral injury, craniocerebral injury, spinal injury
sep/05
7a(infants Individual studies
No limits
Pubmed "Infant"[MeSH] AND ("craniocerebral trauma/diagnosis"[MaJR] OR "spinal injuries/diagnosis*"[MaJR) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT (imaging OR radiography OR "eye"[MeSH] OR dental)
nov/05
Embase infant'/exp AND ('head injury'/exp OR 'spine injury'/exp) AND 'diagnosis'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') NOT ('imaging'/exp OR 'radiography'/exp OR 'eye'/exp OR 'dental') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=infant AND TS=(head injury OR spinal injury) AND TS=(assessment) AND TS=(first aid OR prehospital OR out of hospital) NOT TS=(imag* OR radiograph* OR rehab* OR treatment)
7b(child Individual studies
No limits
Pubmed "Child"[MeSH] AND ("craniocerebral trauma/diagnosis"[MaJR] OR "spinal injuries/diagnosis*"[MaJR) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT (imaging OR radiography OR "eye"[MeSH] OR dental)
nov/05
Embase child'/exp AND ('head injury'/exp OR 'spine injury'/exp) AND 'diagnosis'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') NOT ('imaging'/exp OR 'radiography'/exp OR 'eye'/exp OR 'dental') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=child AND TS=(head injury OR spinal injury) AND TS=(assessment) AND TS=(first aid OR prehospital OR out of hospital) NOT TS=(imag* OR radiograph* OR rehab* OR
144

treatment)
7c(adults Individual studies
No limits
Pubmed "Adult"[MeSH] AND ("craniocerebral trauma/diagnosis"[MaJR] OR "spinal injuries/diagnosis*"[MaJR) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT (imaging OR radiography OR "eye"[MeSH] OR dental)
nov/05
Embase adult'/exp AND ('head injury'/exp OR 'spine injury'/exp) AND 'diagnosis'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') NOT ('imaging'/exp OR 'radiography'/exp OR 'eye'/exp OR 'dental') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=adult AND TS=(head injury OR spinal injury) AND TS=(assessment) AND TS=(first aid OR prehospital OR out of hospital) NOT TS=(imag* OR radiograph* OR rehab* OR treatment)
145

Key question
8. “What is the safety, efficacy and feasibility of immobilization, done by a lay person, in the first aid management of suspected spinal trauma?”
Search strategy
N° Type Limits Databases Search terms Date of search
8. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
spinal injury, immobilization sep/05
Individual studies
No limits
Pubmed “spinal injuries”[MeSH] AND “immobilization”[MeSH] AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
sep/05
Embase 'spine injury'/exp AND 'immobilization'/exp AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=spinal injury AND TS=immobilization AND TS=(first aid OR prehospital OR out of hospital)
146

Key question
9. “What is the safest, most efficacious and feasible first aid management, done by a lay person, for a traumatised extremity with angulation, without angulation, with an open fracture ?”
Search strategy
N° Type Limits Databases Search terms Date of search
9a. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
limb injur* OR limb trauma OR limb fracture* OR luxat* OR dislocat*
dec/05
Individual studies
No limits
Pubmed (limb OR extremit*) AND (injur* OR trauma*) AND (angula* OR displace* OR "abnormal position" OR dislocat*) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT ("Fractures, Open"[MeSH] OR spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR penetrat* OR bite* OR hypotherm* OR imaging OR x-ray* OR operative OR medication OR drug* OR arthroplast* OR osteoporos* OR bone density OR prosthes* OR musculoskeletal disease*)
Embase (limb OR extremit*) AND (injur* OR trauma*) AND (angula* OR displace* OR abnormal position OR dislocat*) AND ('First Aid' OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') NOT ('open fracture'/exp OR spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR penetrat* OR bite* OR hypotherm* OR imaging OR 'x ray*' OR operative OR medication OR drug* OR arthroplast* OR osteoporos* OR 'bone density' OR prosthes* OR musculoskeletal disease*) AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(limb OR extremit*) AND TS=(injur* OR trauma*) AND TS=(angula* OR displace* OR abnormal position OR dislocat*) AND TS=(First Aid OR Emergency Medical Services OR prehospital OR out of hospital) NOT TS=(open fractures OR spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR penetrat* OR bite* OR hypotherm* OR imaging OR x-ray* OR operative OR medication OR drug* OR
147

arthroplast* OR osteoporos* OR bone density OR prosthes* OR musculoskeletal disease*)
9b. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
limb injur* OR limb trauma OR limb fracture* OR luxat* OR dislocat*
dec/05
Individual studies
No limits
Pubmed (limb OR extremit*) AND (injur* OR trauma*) NOT (angula* OR displace* OR abnormal position OR dislocat* OR "Fractures, Open"[MeSH]) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT (spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR penetrat* OR bite* OR hypotherm* OR imaging OR x-ray* OR operat* OR medication OR drug* OR arthroplast* OR osteoporos* OR bone density OR prosthes* OR musculoskeletal disease*)
Embase (limb OR extremit*) AND (injur* OR trauma*) NOT (angula* OR displace* OR abnormal position OR dislocat* OR 'open fracture'/exp) AND ('First Aid' OR 'emergency health service'/exp OR prehospital OR 'out of hospital') NOT (spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR penetrat* OR bite* OR hypotherm* OR imaging OR 'x ray*' OR operat* OR medication OR drug* OR arthroplast* OR osteoporos* OR 'bone density' OR prosthes* OR 'musculoskeletal disease*') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(limb OR extremit*) AND TS=(injur* OR trauma*) NOT TS=(angula* OR displace* OR abnormal position OR dislocat* OR open fracture) AND TS=(first aid OR Emergency Medical Services OR prehospital OR out of hospital) NOT TS=(spin* OR crani* OR abdom* OR chest OR lung OR head OR burn* OR amputat* OR penetrat* OR bite* OR hypotherm* OR imaging OR x-ray* OR operat* OR surg* OR medication OR drug* OR arthroplast* OR osteoporos* OR bone density OR prosthes* OR musculoskeletal disease* OR brain OR stroke OR hemi* OR economic OR prevent*)
148

9c. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
open fracture* dec/05
Individual studies
No limits
Pubmed (limb OR extremit* ) AND (injur* OR trauma*) AND "Fractures, Open"[MeSH] AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT (spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR bite* OR hypotherm* OR imaging OR x-ray* OR operative OR medication OR drug* OR arthroplast* OR osteoporos* OR bone density OR prosthes* OR musculoskeletal disease*)
Embase (limb OR extremit* ) AND (injur* OR trauma*) AND 'open fracture'/exp AND ('First Aid' OR 'emergency health service'/exp OR prehospital OR 'out of hospital') NOT (spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR bite* OR hypotherm* OR imaging OR 'x ray' OR operative OR medication OR drug* OR arthroplast* OR osteoporos* OR 'bone density' OR prosthes* OR 'musculoskeletal disease*') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(limb OR extremit* ) AND TS=(injur* OR trauma*) AND TS= open fractures AND TS=(First Aid OR Emergency Medical Services OR prehospital OR out of hospital) NOT TS=(spinal OR crani* OR abdom* OR chest OR head OR burn* OR amputat* OR bite* OR hypotherm* OR imaging OR x-ray* OR operative OR medication OR drug* OR arthroplast* OR osteoporos* OR bone density OR prosthes* OR musculoskeletal disease*)
149

Key question
10. “What is the safety, efficacy and feasibility of the ICE-principle, done by a lay person, in the first aid management of an minor injured extremity joint?”
Search strategy
N° Type Limits Databases Search terms Date of search
10. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
sprains, strains, joint injury, athletic injury sep/05
Individual studies
2005 Pubmed ("Sprains and strains"[MeSH] OR "Athletic injuries"[MeSH] OR "Joints/injuries"[MeSH]) AND ("cryotherapy"[MeSH] OR "ice"[MeSH] OR "immobilization"[MeSH] OR compression OR elevation)AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital" OR acute)
sep/05
Embase ('sprain'/exp OR 'sport injury'/exp OR 'joint injury'/exp) AND ('cryotherapy'/exp OR 'ice'/exp OR 'immobilization'/exp OR 'compression'/exp OR elevation) AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital' OR 'acute') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(sprain* OR joint injury OR athletic injury) AND TS=(cryotherapy OR ice OR immobilization OR compression OR elevation) AND TS=(first aid OR prehospital OR out of hospital)
150

Key question
11. “What is the safest, most efficacious and feasible first aid management, done by a lay person, for thermal cutaneous burn?”
Search strategy
N° Type Limits Databases Search terms Date of search
11. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
burns july 2005
Individual studies
2004-2005
Pubmed ("Burns/therapy"[MeSH] NOT ("Burns, Inhalation"[MeSH] OR "Burns, Chemical"[MeSH])) AND (cool* OR "Irrigation"[MeSH]) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
sep/05
Embase ('burn'/exp) NOT ('chemical burn'/exp OR 'lung burn'/exp) AND (cool* OR 'lavage'/exp) AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=burns AND TS=(first aid OR prehospital OR out of hospital) AND TS=(cool* OR lavage OR irrigation) NOT TS=(chemical OR inhalation)
151

Key question
12. “What is the safest, most efficacious and feasible first aid, done by a lay person, for the management of a chemical cutaneous burn?”
Search strategy
N° Type Limits Databases Search terms Date of search
12. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
burns july 2005
Individual studies
2004-2005
Pubmed “Burns, Chemical”[MeSH] AND (cool* OR "Irrigation"[MeSH]) AND (“First Aid” OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
sep/05
Embase chemical burn'/exp AND (cool* OR 'lavage'/exp) AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=chemical burns AND TS=(first aid OR prehospital OR out of hospital) AND TS=(cool* OR lavage OR irrigation)
152

Key question
13. “What is the safest, most efficacious and feasible first aid, done by a lay person, for the management of non-penetrating wounds?”
Search strategy
N° Type Limits Databases Search terms Date of search
13. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
wounds, skin, irrigation aug/05
Individual studies
2005 Pubmed Wounds and Injuries/therapy[MeSH] AND skin AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR "out of hospital") NOT "Burns"[MeSH]
sep/05
Embase ('laceration'/exp OR 'skin abrasion'/exp OR 'skin bruising'/exp OR 'bite wound'/exp OR 'knife cut'/exp) AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') NOT 'burn'/exp AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(wound* OR laceration* OR abrasion* OR cut) AND TS=skin AND TS=(first aid OR prehospital OR out of hospital) NOT TS=(burn* OR fracture* OR surg* OR long term OR chronic* OR ulc* OR necro* OR graft* OR nosocomial)
153

Key question
14. “What is the safest, most efficacious and feasible first aid, done by a lay person, for the management of penetrating wounds?”
Search strategy
N° Type Limits Databases Search terms Date of search
14. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
wounds, stab, penetrating aug/05
Individual studies
No limits
Pubmed Wounds, Stab[MeSH] AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital") NOT "Needlestick Injuries"[MeSH]
sep/05
Embase ('stab wound'/exp OR 'penetrating trauma'/exp) AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') NOT 'needlestick injury'/exp AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(penetrating wound* OR stab wound*) AND TS=(first aid OR prehospital OR out of hospital) NOT TS=(laparoscop* OR incidence OR trend*)
154

Key question
15.“What is the safety, efficacy and feasibility of administration of charcoal, ipecac syrup, water or milk or doing nothing in the first aid managament of oral poisoning by a lay person?”
Search strategy
N° Type Limits Databases Search terms Date of search
15. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
poisoning, charcoal, ipecac, dilution july 2005
Individual studies
2004-2005
Pubmed Poisoning[MeSH] AND ("charcoal"[MeSH] OR "ipecac"[MeSH] OR dilut*) AND ("First Aid" OR "Emergency Medical Services"[MeSH] OR prehospital OR "out of hospital")
Embase 'intoxication'/exp AND ('charcoal'/exp OR 'ipecac'/exp OR 'dilution with water' OR 'dilution with milk') AND ('first aid'/exp OR 'emergency health service'/exp OR 'prehospital' OR 'out of hospital') AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(poisoning OR intoxication) AND TS=(charcoal OR ipecac OR dilution) AND TS=(first aid OR prehospital OR out of hospital)
155

Key question
16. “What is the safety, efficacy and feasibility of psychosocial support in the first aid management in the peritraumatic phase by a lay person for postrauma psychopathology after single individual accidents ?”
Search strategy
N° Type Limits Databases Search terms Date of search
16. Guidelines + SR
1995-2005
Cochrane database, Guidelines International Network database (GIN), Health Evidence Network (WHO), National Guideline Clearinghouse (NGC), National Electronic Library for Health Guidelines finder (NHS), Pubmed, Worksheets of the ILCOR process
psychological first aid, psychosocial first aid, psychological care, debrief, early intervention
july 2005
Specific sources : http://www.nimh.nih.gov/publicat/massviolence.pdf Individual
studies 2005 Pubmed ("Life Change Events"[MeSH] OR "Stress Disorders,
Traumatic"[MeSH] OR "Stress Disorders, Post-Traumatic"[MeSH] OR "Stress Disorders, Traumatic, Acute"[MeSH] OR "Adjustment Disorders"[MeSH]) AND ("First aid"[MeSH] OR "Crisis intervention"[MeSH] OR "psychological first aid" OR "psychosocial first aid" OR "early intervention*" OR debrief*)
july 2005
Embase (('first aid'/exp AND [embase]/lim) OR ('psychosocial care'/exp AND [embase]/lim) OR ('crisis intervention'/exp OR 'early intervention' OR debrief* OR 'psychological first aid' OR 'psychosocial first aid' AND [embase]/lim)) AND (('life event'/exp AND [embase]/lim) OR ('acute stress disorder'/exp AND [embase]/lim) OR ('posttraumatic stress disorder'/exp AND [embase]/lim) OR ('adjustment disorder'/exp AND [embase]/lim)) AND [embase]/lim
Social Science Citation Index, Science Citation Index Expanded
TS=(Life Change Event* OR Stress Disorder* OR Adjustment Disorder* OR critical incident*) AND TS=(First aid OR Crisis intervention OR psychological first aid OR psychosocial first aid OR psychological care OR early intervention* OR debrief*)
156

Appendix
RCT: Questionnaires
157

Vragenlijst naar persoonlijke gegevens
Belangrijke informatie vooraf:Voor de kwaliteit van het onderzoek is het van belang dat je alle vragen beantwoordt.
Naam: ................................................................................................
Ben je: Man
Vrouw
Wat is je geboortedatum? / /
Welke nationaliteit heb je? Belg
Andere
Wat is je hoogst behaalde diploma of getuigschrift? geen of lager onderwijs
lager secundair onderwijs (minimum 3 jaar)
hoger secundair onderwijs (minimum 6 jaar)
hoger onderwijs korte type (2-3 jaar)
hoger onderwijs lange type of universiteit
Welk beroep heb je? arbeider
bediende
leidinggevende
zelfstandige
vrij beroep (dokter, advocaat, ...)
werkloos
student
arbeidsongeschikt
gepensioneerde
huisvrouw
Wat is je burgerlijke staat? alleenstaand (geen partner)
getrouwd of geregistreerd partnerschap
samenwonend
gescheiden
weduwe
Ben je ooit al rodekruisvrijwilliger geweest? ja
neen
Heb je ooit al ergens eerstehulptraining gevolgd? ja
neen
Heb je ooit al een levensbedreigende situatie meegemaakt? ja
neen
61109
158

159

160

161

Vragenlijst naar zelf-effectiviteitsverwachting
Naam: ................................................................................................
Deze vragenlijst vraagt hoeveel vertrouwen je er in hebt dat je deze acties zal uitvoeren, indien je aanwezig bent in een noodsituatie met eenvoor jou onbekend slachtoffer. Deze vragenlijst vraagt niet of je deze dingen wel of niet gedaan hebt. Om je antwoord aan te geven moet je ééngetal omcirkelen op de schaal bij elke vraag: 1 betekent 'geheel geen vertrouwen en 5 betekent 'volledig vertrouwen'.
1. Ik zal eerste hulp geven zelfs als er andere omstaandersaanwezig zijn die het slachtoffer kunnen helpen.
2. Ik zal eerste hulp geven zelfs als het slachtoffer ernstig bloedt.
1 2 3 4 5
1 2 3 4 5
geheel geenvertrouwen
volledigvertrouwen
3. Ik zal eerste hulp geven zelfs als ik hartmassages moet geven.
4. Ik zal eerste hulp geven zelfs als ik mond-op-mond beademingmoet geven.
5. Ik zal eerste hulp geven zelfs als het slachtoffer mogelijks eenwervelletsel heeft.
6. Ik zal hulp zoeken zelfs als het slachtoffer zegt dat dit niet nodig is.
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
21133
162

Vragenlijst naar tevredenheid over extra les
Naam: ................................................................................................
Deze vragenlijst peilt je tevredenheid over de extra les. Deze vragenlijst vraagt niet wat je vond van de voorgaande lessen eerste hulp
Om je antwoord aan te geven moet je één getal omcirkelen op de schaal bij elke stelling: 1 betekent 'helemaal juist”, 2 betekent ‘juist’, 3 betekent ‘verkeerd’ en 4 betekent 'helemaal verkeerd'. Ook als het moeilijk is om voor één bepaald vakje te kiezen, willen we je toch vragen om je mening te geven.
Helemaal juist Juist Verkeerd Helemaal verkeerd
1. De dingen die in deze les gezien zijn waren nieuw voor mij 1 2 3 4
2. Ik heb goed begrepen wat mij in de les werd aangeleerd 1 2 3 4
3. De les was duidelijke en overzichtelijk opgebouwd 1 2 3 4
4. Wat ik in de les geleerd heb kan ik nu in de praktijk toepassen 1 2 3 4
5. De les werd op een boeiende en levendige manier gegeven 1 2 3 4
6. De sfeer onder de deelnemers was vriendschappelijk 1 2 3 4
7. Voor mij was deze les echt de moeite waard 1 2 3 4
We willen je ook vragen om op de volgende “open vragen” te antwoorden. Met jouw antwoorden zal zeker rekening gehouden worden als deze les een volgende keer georganiseerd wordt.
8.Wat vind je de sterke punten van deze les? ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
9.Welke punten zijn volgens jou voor verbetering vatbaar ? ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
163

164

.~ 24971
Vragenlijst over stemming
Naam: ............... .................................. , .... .......... ... , ..................... .
Deze vragen gaan over hoe u z;,:h voett nadat we je verteld hebben over de misleid ing. Per vraag staal een antwoord dal emoties of gevoelen! i)nchrijtt . lees "Ik" vraag en gebruik bij de beantwoordiJlg volgende schaal'
1 - helemaal niet 2 • e(!n beetje 3· enigszins 4 · nogal 5 m!leel erg
Beantwoord elke vraag door het best pas,,,,,,,,, cijfer 111 omcir1<elen.
helemaal niet
Hoe nerveus voel ja jeze~ op d~ mQlTl.mt? 1
Hoe enthous iast v~ je jezeW op d~ moment? 1
Hoe verward voel Je jezelf op dit moment? 1
Hoe ster\< voel je jezeH op dit moment? 1
Hoe b<:schaamd voel je jezeN op d~ momen1? 1
Hoe vastberaden voetje jezelf op dit rnGlTlen1? 1
Hoe angstig voel je jezelf op dit moment? 1
Hoe trols voel je jezeH op dit moment? 1
Hoe kwud ~ Je jezeH op dit moment? 1
HQe gelnspl ..... rd voel je jezelf op d~ moment? 1
een bee~ .. enigszins nogal heftl erg
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
2 3 , 5
•
• • 165

166

Appendix
RCT: Didactical plan experimental and control
intervention
167

Lesson preparation extra 2 hours Helping Kim Swyngedouw11/03/2009__________________________________________________________________________
Content
In this extra 2 hours you will learn all about what Red Cross calls ‘helping behaviour’. In the first ...
hours of the course you learned all about how to provide first aid and the important steps involved
in first aid provision. In this part we will look more closely at the barriers that might prevent you
from administering aid, despite all the knowledge and skills that you have.
Objectives� To make course participants aware of the importance of administering first aid
� To let course participants know what it’s like to be a casualty
� To make course participants aware of the existence of different barriers
� To make course participants aware of the relativity of these barriers
� To teach course participants how to deal with barriers so as to be able to demonstrate
helping behaviour
Planning and method
Time allocation
10’ Probability of an emergency situation
15’ Positive and negative experiences of helping
35’ How does it feel to be a casualty
15’ My role as a first aider
45’ The various barriers to helping behaviour
168

Lesson preparation
Probability of an emergency situation
A group discussion will reveal whether there are any course participants who have already witnessed
an accident or a situation in which first aid could have been administered. This can be a life-
threatening as well as a non life-threatening situation (child falls off bike in town, grandpa gets pain
in chest, etc.).
In connection with that a number of questions will be asked:
� Did they take action (e.g. call emergency services, help child with bike to get of road, etc.)?
� How did they feel about it
� How long was it before the emergency services arrived (if nobody called emergency services
you can let them make an estimated guess)
Positive and negative experiences of helping
The course participants are given a case study (see below) and are asked what constitutes an
appropriate or less appropriate reason for bystanders and first aid administrators to help or not. The
course participants should also explain their reasoning for this. Then they should think about
opportunities, steps, …needed to remove the reasons they gave for not helping. Examples are:
Helping Not helping
The casualty urgently needs help I don’t want to catch anything
You get a good feeling from helping others There are other people who can help
You feel guilty if you don’t help I don’t know how to give first aid
You might get a reward later What if this is a trap and they attack me
Everyone should help people in need It is late and dark
It is the right thing to do I have an important meeting to get to, so I haven't
got time
If you help that person, someone might help you
when you’re in need
Helping others creates a better society
Out of sympathy with the casualty
… …
Case study
169

There has been a serious car accident on the motorway. Peter lost control of his car because of a
flat tyre and he smashed into another car before coming to a stop against the central barrier.
Peter is completely distressed when he sees the other car lying upside down, but still goes over
to the casualty. Vera was driving in the first lane and saw what happened. Luckily she was able to
stop in time and walked with her colleague to the casualty. Carl, the driver of the smashed car, is
lying on the road. He is conscious but is bleeding seriously from his left wrist. The blood is pouring
out.
How does it feel to be a casualty
The course participants are divided into four groups and each receive the same case study. The idea
is that they look in detail at the case and then play out the next scene. This is first prepared in
writing: what help can be given, how to approach the casualty,…
Then the different groups act out their case study. One person is the casualty, 1 or 2 people play
the role of first aiders.
A group discussion takes place later in which the casualties reveal how they felt in their role. Which
thoughts, emotions, feelings did they experience. If other people in the group report different
feelings or emotions or thoughts, these are recorded too.
Case study
Andrew is going home on the metro after a hard day’s work. There are lots of people crammed into
the carriage and all the seats are taken. After a few minutes standing, Andrew becomes dizzy and
sees spots before his eyes. A few other commuters notice that Andrew is swaying.
My role as a first aider
The group is split into 3. Each group is given a case study. For this case study they have to imagine
that they witness the situation and ask themselves which first aid skills they would use in this
situation. They start out with the most minimal and most appropriate help. Then the different
groups discuss their plans in a meeting.
Case study
Sarah has overslept and is really late for her class. She cycles like a maniac in the pouring rain
through the morning rush hour. Because it is late and she is in a hurry, she’s not paying attention
to the obstacles on the road. Suddenly her back wheel gets stuck in the tram rails. She loses
control and crashes to the ground. She lies there a little stunned and soon notices that there is
blood trickling over the palm of her hand. You are a pedestrian and you saw what happened.
Case study
You are taking your weekly run in the park. On the way you come across a few boys who are
obviously drunk and who are arguing. Unprovoked, one of the boys is hit in the face. The blood
comes gushing out. Some of the boys run off, a few of them stand looking dazed next to the
casualty.
170

Case study
You are in a checkout queue in a shop. The man in front of you suddenly starts acting strangely. He
is having difficulty breathing, pulls at his tie, …Suddenly he grabs his chest and collapses.
As a conclusion to this part the instructor explains how important it is that first aid isn’t just talk.
Because offering first aid in an emergency or in a situation where help is needed is not easy, we
have designed a format to help every course participant on their way. The instructor briefly outlines
this objectives page.
Different barriers concerning first aid
The course participants are split up into 4 groups and must first of all think about any possible
barriers to them giving first aid and how they could remove these barriers (e.g. remove fear of
infection by wearing gloves). Then they should choose two barriers to look at in more detail.
They prepare a role play in which they show the other group what their barrier is as well as the
solution they have found for it. This can be fun, serious, etc.
When the different groups have played out their barriers, the instructor uses the cartoons in the
brochure (better if they have not already been given this) to go through which barriers might occur
and how they can be removed (with legal stipulations, measures, education, ...).
Material
Work sheets with assignments and case studies
Projector
Brochures for this lesson
Flipchart/blackboard
Paper and pens
171

Lesvoorbereiding extra 2 u Eerste hulp bij alcohol en drugsincidenten (in het kader van veldstudie eerste hulp)Leen Meeremans, Stijn Van de Velde20/10/2009__________________________________________________________________________
Inhoud
In deze extra 2 u leer je wat Rode Kruis-Vlaanderen eerste hulp bij alcohol en drugsincidenten
noemt. In de voorgaande 24u van de cursus leerde je alles over hoe je eerste hulp kan verlenen en
wat belangrijke stappen zijn binnen de eerstehulpverlening.
Ook al ben je in het bezit van een brede eerstehulpkennis, toch zijn er nog een aantal extraaandachtspunten bij de hulpverlening bij alcohol- en drugsincidenten. Bedoeling is om tijdens deze
les dieper in te gaan op deze aandachtspunten en je de eerstehulpverlening te leren in een aantal
specifieke situaties. Hierbij gaan we ook in op theoretische informatie over druggebruik en bij
welke instanties je meer informatie kan krijgen.
Doelstellingen� Cursisten informeren over druggebruik en mogelijke risico’s� Cursisten bewust maken van aandachtspunten bij hulpverlening bij alcohol- en
drugsincidenten
� Cursisten leren eerste hulp verlenen bij een overdosis, oververhitting, bad trip
� Cursisten informeren over instanties waar je extra informatie kan krijgen
Opzet en methodeTijdsindeling
5’ Introductie
10’ Wat zijn drugs en welke risico’s bestaan er ?
10’ Basisprincipes van eerste hulp
15’ Vier stappen in eerste hulp
20’ Overdosis
15’ Oververhitting
20’ Bad Trip
5’ Meer informatie en verdere hulp
20’ Herhalingsoefeningen
172

Lesvoorbereiding
Introductie
Korte uitleg omtrent de opzet van deze les (zie ook inhoud).
Wat zijn drugs ?
Vraag- en antwoordgesprek:
- Vraag aan cursisten wat zij verstaan onder drugs en probeer tot een definitie te komen.
- Vraag aan cursisten om de drugs die zij kennen op te sommen en deel deze in categorieën in.
- Vraag aan cursisten welke acute risico’s druggebruik met zich mee kan brengen en lijst deze
op.
Geef op het einde van de bespreking telkens een samenvattend antwoord adhv de ppt-presentatie
Bij stimulerende middelen zoals speed, cocaïne, en XTC krijgt de gebruiker het gevoel eindeloos te
kunnen presteren of uitgaan, zonder te stoppen. Waarschuwingssignalen voor het lichaam zoals
honger en moeheid vallen weg. Daardoor kan totale uitputting ontstaan, een zogenaamde crash.
Toon het filmpje ter illustratie van een crash.
Basisprincipes
De cursisten krijgen opdracht 1 van het oefenboek voorgelegd.
Aansluitend worden de basisprincipes van eerste hulp herhaald. De bijzonderheden van eerste hulp in situaties met alcohol en drugs worden benadrukt.
Vier stappen
De cursisten krijgen opdracht 2 en 6 voorgelegd.
Per opdracht worden de 4 stappen herhaald en duiden ze de bijzonderheden van eerste hulp in
situaties met alcohol en drugs aan.
Vraag cursisten om de nummers op te sommen die belangrijk zijn voor alarmering bij alcohol- en
drugsincidenten.
Wijs cursisten op het belang van lichaamstemperatuur bij alcohol- en drugsincidenten. Vraag aan de
cursisten wat ze kunnen doen met een slachtoffer dat het te koud/warm heeft en vat samen.
Overdosis
De cursisten krijgen opdracht 7 voorgelegd.Overloop met de cursisten hoe ze een overdosis kunnen vaststellen en wat ze kunnen doen.
OververhittingOverloop met de cursisten hoe ze oververhitting kunnen vaststellen en wat ze kunnen doen.
173

Toon het filmpje ter illustratie van stuipen.
Bad trip
De cursisten krijgen opdracht 8 voorgelegd.
Overloop met de cursisten hoe ze een bad trip kunnen vaststellen en wat ze kunnen doen.
Meer informatie en verdere hulp
Overloop met de cursisten de instanties waar je meer informatie kan verkrijgen over alcohol- en drugsproblemen.
Herhalingsoefeningen
De cursisten krijgen opdrachten 9,10,11,12 voorgelegd.
Materiaal
Ppt-presentatie
Oplossingen opdrachten
Projector
FilmpjesOefenboek bij deze les
Flip over/krijtbord
Papier en stiften
174





















