In adults with atrial switch operation for transposition of the great arteries low physical activity...
9
49 Address for correspondence: Prof. Luc Vanhees; Department of Rehabilitation Sciences, Tervuursevest 101 - bus 01501, B-3001 Heverlee, Belgium. E-mail: [email protected] Received 7 October 2011; accepted for publication 11 October 2011. INTRODUCTION A few decades ago, atrial switch repair was generally performed in patients with dextro-transposition of the great arteries (d-TGA). Nowadays, these atrial switch techniques are replaced by the arterial switch operation. However, 75% to 80% of the d-TGA patients have sur- vived into adulthood and are still visiting the outpatient clinics for grown-up congenital heart disease 1,2 . It has been well documented that patients with d-TGA have a substantially impaired exercise capacity, In adults with atrial switch operation for transposition of the great arteries low physical activity relates to reduced exercise capacity and decreased perceived physical functioning Roselien BUYS 1 , MS; Alexander VAN DE BRUAENE 2 , MD; Werner BUDTS 2 , PhD; Christophe DELECLUSE 3 , PhD; Luc VANHEES 1 , PhD 1 Research Centre for Cardiovascular and Respiratory Rehabilitation, Department of Rehabilitation Sciences, Catholic University of Leuven, Heverlee, Belgium; 2 Internal Medicine, Division of Cardiovascular Medicine, University Hospitals Leuven, Leuven, Belgium; 3 Research Centre for Exercise and Health, Department of Biomedical Kinesiology, Catholic University of Leuven, Heverlee, Belgium. Objective Patients with Mustard/Senning repair for transposition of the great arteries (d-TGA) have an impaired exercise capacity, but information about physical activity levels is scarce. The aim of the study was to come to a better understanding of the interrelationships between determinants of exercise capacity, physical activity and self-perceived health status. Methods and results We studied 39 d-TGA patients who underwent echocardiography and exercise testing, and who completed questionnaires about physical activity and perceived health status. All results were compared with normal values. Stepwise multiple regression analysis was used to assess the determinants of peak VO 2 % and exercise duration. Peak VO 2 averaged 64 ± 14.1% of the predicted normal values, which is significantly lower than expected (P < 0.0001). Physical activity measures as well as perceived general health were significantly lower compared to a reference population (P < 0.05). Peak heart rate and peak oxygen pulse explained together 90% of the variability in exercise duration (model F = 162.72; P < 0.0001). Type of surgery, total energy expenditure and right ventricular contractility were independent predictors of peak VO 2 % explaining 43% of the variability (model F = 8.75; P = 0.0002). Conclusions Impaired peak exercise performance in d-TGA patients results mainly from the inability to increase stroke volume and heart rate at higher exercise intensities. Senning repair and a well-preserved right ventricular function are related to a better peak VO 2 %. Furthermore, an active lifestyle has a positive effect on exercise capacity and perceived physical functioning. Therefore it might be indicated to encourage d-TGA patients to adopt a more physically active lifestyle. Keywords Transposition of the great arteries – Mustard repair – Senning repair – exercise performance – physical activity – SF 36. which probably lowers faster with age compared to healthy controls 1,3-5 . This reduced peak VO 2 has been related to impaired chronotropic response, impaired systemic ventricular function, impaired function of the intra-atrial conduit, the inability to increase stroke vol- ume, impaired lung function and peripheral decon- ditioning 1,4-8 . Moreover, poor exercise capacity identifies d-TGA patients at risk for hospitalization and death 10 . Recently published guidelines recommend low to moderate dynamic and low static exercise in this patient population 10 . However, most studies do not report on physical activity, although physical activity is well known to improve the aerobic capacity in the general popula- tion 10 . Despite a few recent studies, there still is a lack of information on physical activity levels or attitudes towards exercise in this population 11-13 . Furthermore, although patients with congenital heart disease generally experience a good health status, poorer Acta Cardiol 2012; 67(1): 49-57 doi: 10.2143/AC.67.1.2146565
Transcript of In adults with atrial switch operation for transposition of the great arteries low physical activity...

49
Address for correspondence:
Prof. Luc Vanhees; Department of Rehabilitation Sciences, Tervuursevest 101 - bus 01501, B-3001 Heverlee, Belgium. E-mail: [email protected]
Received 7 October 2011; accepted for publication 11 October 2011.
INTRODUCTION
A few decades ago, atrial switch repair was generally performed in patients with dextro-transposition of the great arteries (d-TGA). Nowadays, these atrial switch techniques are replaced by the arterial switch operation. However, 75% to 80% of the d-TGA patients have sur-vived into adulthood and are still visiting the outpatient clinics for grown-up congenital heart disease1,2.
It has been well documented that patients with d-TGA have a substantially impaired exercise capacity,
In adults with atrial switch operation for transposition of the great arteries low physical activity relates to reduced exercise capacity and decreased perceived physical functioning
Roselien BUYS1, MS; Alexander VAN DE BRUAENE2, MD; Werner BUDTS2, PhD;
Christophe DELECLUSE3, PhD; Luc VANHEES1, PhD1Research Centre for Cardiovascular and Respiratory Rehabilitation, Department of Rehabilitation Sciences, Catholic University of Leuven, Heverlee, Belgium; 2Internal Medicine, Division of Cardiovascular Medicine, University Hospitals Leuven, Leuven, Belgium; 3Research Centre for Exercise and Health, Department of Biomedical Kinesiology, Catholic University of Leuven, Heverlee, Belgium.
Objective Patients with Mustard/Senning repair for transposition of the great arteries (d-TGA) have an impaired exercise capacity, but information about physical activity levels is scarce. The aim of the study was to come to a better understanding of the interrelationships between determinants of exercise capacity, physical activity and self-perceived health status.
Methods and results We studied 39 d-TGA patients who underwent echocardiography and exercise testing, and who completed questionnaires about physical activity and perceived health status. All results were compared with normal values. Stepwise multiple regression analysis was used to assess the determinants of peak VO
2% and exercise duration. Peak VO
2 averaged 64 ± 14.1% of the predicted normal values, which is signifi cantly lower than expected
(P < 0.0001). Physical activity measures as well as perceived general health were signifi cantly lower compared to a reference population (P < 0.05). Peak heart rate and peak oxygen pulse explained together 90% of the variability in exercise duration (model F = 162.72; P < 0.0001). Type of surgery, total energy expenditure and right ventricular contractility were independent predictors of peak VO
2% explaining 43% of the variability (model F = 8.75; P = 0.0002).
Conclusions Impaired peak exercise performance in d-TGA patients results mainly from the inability to increase stroke volume and heart rate at higher exercise intensities. Senning repair and a well-preserved right ventricular function are related to a better peak VO
2%. Furthermore, an active lifestyle has a positive
eff ect on exercise capacity and perceived physical functioning. Therefore it might be indicated to encourage d-TGA patients to adopt a more physically active lifestyle.
Keywords Transposition of the great arteries – Mustard repair – Senning repair – exercise performance – physical activity – SF 36.
which probably lowers faster with age compared to healthy controls1,3-5. This reduced peak VO2 has been related to impaired chronotropic response, impaired systemic ventricular function, impaired function of the intra-atrial conduit, the inability to increase stroke vol-ume, impaired lung function and peripheral decon-ditioning1,4-8. Moreover, poor exercise capacity identifies d-TGA patients at risk for hospitalization and death10.
Recently published guidelines recommend low to moderate dynamic and low static exercise in this patient population10. However, most studies do not report on physical activity, although physical activity is well known to improve the aerobic capacity in the general popula-tion10. Despite a few recent studies, there still is a lack of information on physical activity levels or attitudes towards exercise in this population11-13.
Furthermore, although patients with congenital heart disease generally experience a good health status, poorer
Acta Cardiol 2012; 67(1): 49-57 doi: 10.2143/AC.67.1.2146565
95259_ActaCardio_67/1__07_11-5199.indd 4995259_ActaCardio_67/1__07_11-5199.indd 49 2/02/12 14:302/02/12 14:30

R. Buys et al.50
uptake (VO2) and carbon dioxide production (VCO2) were determined from the continuous measurement of oxygen and carbon dioxide concentration in the inspired and expired air. Peak VO2 was defined as the highest 30-second average of VO2 at the end of the test. The per-cent of predicted peak VO2 (peak VO2%) was calculated as peak VO2 divided by the maximal predicted VO2, using the equations reported by Wasserman and col-leagues17.
A standard pulmonary function test was performed prior to the exercise test, using the same equipment for breath-by-breath analysis. The best values out of three satisfactory executions were taken into account. Meas-ures were expressed as percentages of predicted values18.
Transthoracic echocardiography
Routine transthoracic echocardiography was per-formed with standard gray-scale, and Doppler imaging examinations using a Vivid 7 or 9 ultrasound system (General Electric Vingmed Ultrasound, Horten, Nor-way) equipped with a 3-MHz transducer. All echocar-diographic studies were performed with the participant in a supine position. Qualitative evaluations were used for the evaluation of right ventricular hypertrophy (0 = no hypertrophy, 1 = hypertrophy), right ventricular dilatation (no, slight, moderate and severe dilatation, scaling from 1 to 4) and right ventricular contractility (normal, mild, moderate, and severe dysfunction, scal-ing from 1 to 4).
Questionnaires
A postal survey was used to collect information regarding physical activity and perceived health status. Patients who did not return their questionnaires, were asked to complete them during the next follow-up visit at the outpatient clinic (at most 1 year later).
Self-reported physical activity was assessed by the Flemish Physical Activity Computerized Questionnaire (FPACQ). This questionnaire indicates how much time and at which intensity the subjects are involved in dif-ferent physical activities during a usual week in a usual year. The FPACQ is a reliable and valid questionnaire about regular physical activity19. Reference values from the Flemish Policy Research Centre Sport, Physical Activity and Health were used for comparative pur-poses20. Health-related sports participation was based on all sports of which the associated MET value was at least 4.5 for subjects younger than 35 years old, or at least 4.0 for subjects between 35 and 40 years old20.
The short form 36 health survey questionnaire (SF-36) was used to evaluate the self-perceived health status. The SF-36 is an eight-scale profile, which provides a score
perceived physical functioning and perceived general health as measured by a self-reported health questionnaire has been reported, and is related to exercise capacity14-16. Better understanding of the interrelationship between determinants of exercise capacity, physical activity and self-perceived health status may be useful to guide these patients towards a healthier and more active lifestyle.
Therefore the aim of our study was: (1) to investigate the determinants of exercise capacity in adults with Mustard/Senning repair for dextro-transposition of the great arteries, (2) to investigate physical activity behav-iour and perceived health, and (3) to investigate the relationships among exercise capacity, physical activity and health status.
METHODS
Patients
Thirty-nine consecutive patients with d-TGA (mean age 26.2 ± 6.6 years; range 16-40 years; 69% male) who underwent exercise testing and cardiac ultrasound during their routine control at the outpatient clinic, were included in the study and were asked to complete two question-naires. Patients with concomitant pathology, who did not perform a maximal exercise test or who were mentally not able to fill in the questionnaires, were excluded.
Furthermore, 149 healthy adults (mean age 27.0 ± 6.1 years; range 16-40 years; 61% male) who are representative of the general Flemish population under-went the same exercise testing protocol and formed the control group. Baseline demographic and clinical data were obtained from the patients’ medical records.
The study was approved by the Institutional Review board of the University Hospitals Leuven.
Cardiopulmonary exercise test
The exercise tests on the bicycle ergometer (Ergo-metrics 800S, Ergometrics, Bitz, Germany) were per-formed in a laboratory where the temperature was sta-bilized at 18-22°C. The initial workload of 20 W was increased by 20 W every minute until exhaustion, as defined by shortness of breath and/or fatigue of the legs. Systolic and diastolic blood pressures were measured at rest and every two minutes during the exercise test. Heart rate was calculated from the continuously regis-tered 12-lead electrocardiogram (Max Personal Exercise TestingR, Marquette, Wisconsin) and respiratory data were continuously measured through breath-by-breath analysis (Oxygen AlphaR, Jaeger, Mijnhardt, Bunnik, The Netherlands). Before each test, the gas analysers and the flow meter were calibrated according to the manu-facturer’s instructions. During the exercise test, oxygen
95259_ActaCardio_67/1__07_11-5199.indd 5095259_ActaCardio_67/1__07_11-5199.indd 50 2/02/12 14:302/02/12 14:30

Exercise and health in Mustard/Senning-patients 51
6 patients were treated with beta blockers, 9 patients with ACE-inhibitors, 2 patients with both digoxin/digi-toxin and diuretics, and 6 patients with vitamin K antag-onists. Four patients were smokers. Surprisingly, no patients in our study sample were pacemaker-dependent; this is probably due to the fact that we consecutively recruited our patients only on 2 days of the week.
Exercise data
Peak VO2% in the patient group was significantly lower than expected in healthy controls. Also forced vital capacity and forced expiratory volume in one second, expressed as a percentage of the expected value, were significantly reduced, but still within acceptable ranges. Moreover, all exercise measures in the patient group were significantly lower compared to the control group.
Questionnaires
Data concerning physical activity and its correlation with peak VO2% are summarized in table 2. Nineteen patients were not involved in health-related sports. On the other hand, 3 patients participated in the following competitive sports: football (4 hours/week), badminton (5 hours/week) and horse riding (20 hours/week). Based on the classification of physical activity levels of the World Health Organization, 62% of all patients were sedentary, 27% had an active or moderately active life-style and 11% of the group had a vigorously active life-style. Time, intensity and volume of leisure time physi-cal activity as well as energy expenditure at work and total energy expenditure were significantly correlated with peak VO2%. Health-related sports participation, time spent in active leisure time and total energy expen-diture were significantly lower compared to the reference population (figure 1).
between 0 and 100 for the following eight subscales: physical and social functioning, role limitations attrib-uted to physical and emotional problems, mental health, vitality (energy/fatigue), pain, and general health per-ception. Higher scores indicate a better health percep-tion. Results were compared with reference values pub-lished by Aaronson and colleagues21.
STATISTICAL ANALYSIS
SAS statistical software version 9.2 was used for data analysis (SAS Institute Inc, Cary, NC, USA). Data are reported as means ± SD, as median (range) or as num-bers for dichotomous variables. The Shapiro-Wilk test was used to check normality.
In order to avoid any bias by age, gender and anthro-pometry, exercise capacity was expressed by peak VO2% for regression statistics. Exercise capacity was compared with average (mean percent predicted value = 100%) using a 1-sample t-test. The Student’s unpaired t-test and analysis of variance were used to compare two means or more between groups. Possible determinants of exer-cise tolerance were investigated by regression analysis. Factors included in the regression models are patient characteristics, type of surgery, age at surgery, resting variables, exercise testing variables and leisure time activities. Stepwise multiple regression analysis was per-formed with all significant variables from single regres-sion analysis. The Spearman correlation coefficient was used to estimate correlations between physical activity data and exercise capacity and with SF-36-scores. Results from the questionnaires were compared with reference values by calculation of the mean standardized differ-ences. For each patient, the score of the reference group was subtracted from the patient’s score and this was divided by the standard deviation of the reference group, generating a standardized difference for that patient. The average of the patients’ values resulted in a mean standardized difference. The one-sample t-test was used to evaluate whether the mean standardized differences significantly differed from zero. All statistical tests were two-sided at a significance level of 0.05. Correction for multiple testing was applied according to the false dis-covery rate method of Benjamini22.
RESULTS
Patient characteristics
Eleven patients underwent Mustard repair and 28 Senning repair. Baseline and exercise variables are summarized in table 1. Mean age at surgery was 0.89 years (range 0.04-4.25 years). At the time of the follow-up visit,
Fig. 1 Physical activity measures.Mean standardized differences of health-related sports, active leisure time and total energy expenditure in comparison with a reference population. *P < 0.0001.
95259_ActaCardio_67/1__07_11-5199.indd 5195259_ActaCardio_67/1__07_11-5199.indd 51 2/02/12 14:302/02/12 14:30

R. Buys et al.52
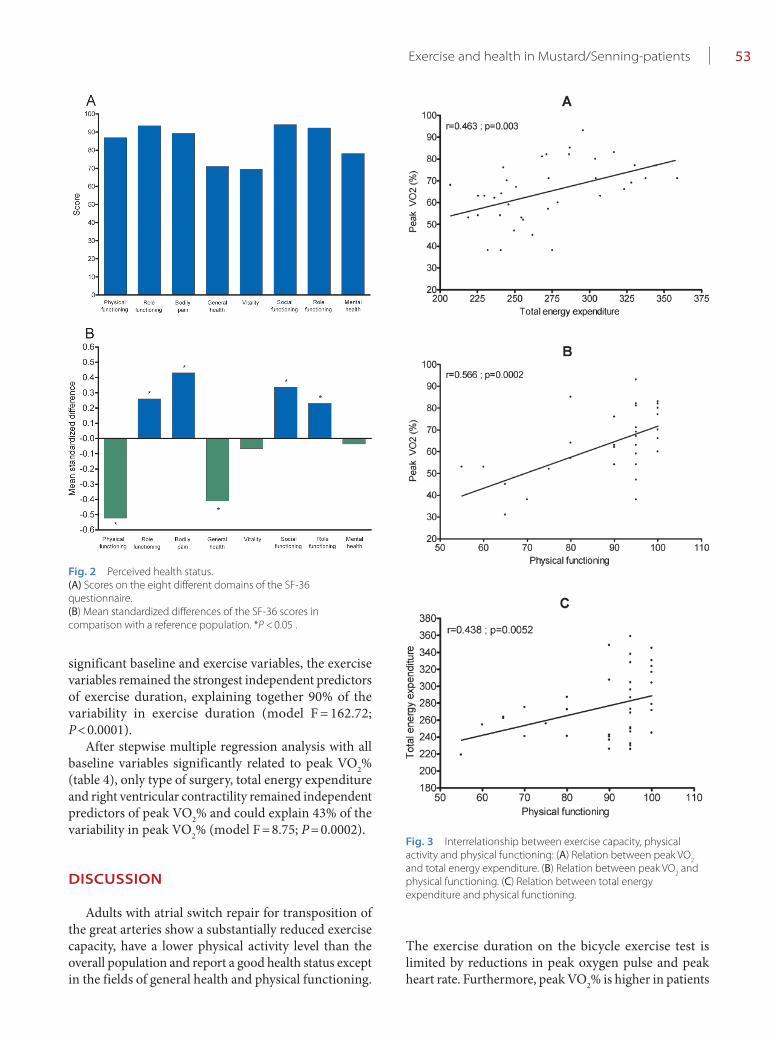
was significantly correlated with peak VO2% (r = 0.566, P = 0.0002) and with total energy expenditure (r = 0.438, P = 0.0052).
Determinants of exercise capacity
Data from univariate and multivariate regression analysis for exercise duration are summarized in table 3. After stepwise multiple regression analysis with all
Correlation between questionnaires and exercise capacity
Mean perceived health scores and mean standardized differences are shown in figure 2. Patients reported a similar or better health status in all domains, except for physical functioning and general health that were both decreased, however, significance was only reached for general health (P = 0.0539 and P = 0.0227, respectively). As shown in figure 3, perceived physical functioning
Table 1 Baseline and exercise variables
AS-TGA Control group P
Number (male/female) 39 (27/12) 149 (91/58)
Age at exercise test (years) 26.2 ± 6.6 27.0 ± 6.1 NS
Body mass index (kg/m²) 23.8 ± 4.6 22.6 ± 2.8 NS
Systolic blood pressure at rest (mmHg) 117 ± 20 123 ± 17 NS
HR rest (beats/min) 80.1 ± 16.0 74.6 ± 13.5 NS
Exercise test results
Exercise duration 7.5 ± 2.28 11.4 ± 3.47 < 0.0001
Peak VO2 (ml/min/kg) 24.9 ± 7.3 38.9 ± 8.4 < 0.0001
Peak VO2 (% of predicted) 63.8 ± 14.6*** 99.0 ± 16.9 < 0.0001
Peak HR (beats/min) 166 ± 25.7 184 ± 18.9 0.0002
Peak oxygen pulse (ml/min*kg*beat) 10.7 ± 3.7 15.5 ± 7.7 < 0.0001
Peak RER 1.16 ± 0.07 1.22 ± 0.11 0.0002
Peak ventilation (l/min) 69.0 ± 21.3 102 ± 30.8 < 0.0001
VE/VCO2-slope 32.7 ± 10.2 24.9 ± 4.14 < 0.0001
Lung function
Forced vital capacity (% of predicted) 92.9 ± 22.2***
Forced expiratory volume in one second (% of predicted) 91.4 ± 16.9***
Right ventricular function
RV contractility (normal/slightly/moderately/severely reduced) 7/9/22/1
RV hypertrophy (no hypertrophy/hypertrophy) 3/36
RV dilatation (no/slight/moderate/severe dilatation) 3/2/29/5
Measures are expressed as mean ± standard deviation or as numbers. NS = not significant. *** Significantly different from the reference population (p > 0.0001).
Table 2 Daily physical activity measures and Spearman correlation coeffi cients with peak VO2%
Median (range) r P
Volume of active leisure time (MET *hours/week) 33 (2-132) 0.347 0.0138
Intensity of active leisure time (METS) 3.2 (1.5-6.3) 0.390 0.0031
Time spent in active leisure time (hours/week) 10 (0.5-39.5) NS
Volume of health-related sports/week (MET *hours/week) 0.5 (0-50) NS
Intensity of health-related sports/week (METS) 4.0 (1-10) NS
Time spent in health-related sports/week (hours/week) 0.12 (0-5) NS
Housekeeping and gardening (MET *hours/week) 15.3 (0-78) NS
Profession (MET*hours/week) 87 (0-160) 0.357 0.0087
Total energy expenditure (MET *hours/week) 269 (207-359) 0.463 0.0003
Physical activity level (METS) 1.60 (1.23-2.14) 0.463 0.0003
Measures are expressed as median (range). NS = not significant.
95259_ActaCardio_67/1__07_11-5199.indd 5295259_ActaCardio_67/1__07_11-5199.indd 52 2/02/12 14:302/02/12 14:30
Exercise and health in Mustard/Senning-patients 53
The exercise duration on the bicycle exercise test is limited by reductions in peak oxygen pulse and peak heart rate. Furthermore, peak VO2% is higher in patients
significant baseline and exercise variables, the exercise variables remained the strongest independent predictors of exercise duration, explaining together 90% of the variability in exercise duration (model F = 162.72; P < 0.0001).
After stepwise multiple regression analysis with all baseline variables significantly related to peak VO2% (table 4), only type of surgery, total energy expenditure and right ventricular contractility remained independent predictors of peak VO2% and could explain 43% of the variability in peak VO2% (model F = 8.75; P = 0.0002).
DISCUSSION
Adults with atrial switch repair for transposition of the great arteries show a substantially reduced exercise capacity, have a lower physical activity level than the overall population and report a good health status except in the fields of general health and physical functioning.
Fig. 2 Perceived health status.(A) Scores on the eight different domains of the SF-36 questionnaire.(B) Mean standardized differences of the SF-36 scores in comparison with a reference population. *P < 0.05 .
Fig. 3 Interrelationship between exercise capacity, physical activity and physical functioning: (A) Relation between peak VO
2
and total energy expenditure. (B) Relation between peak VO2 and
physical functioning. (C) Relation between total energy expenditure and physical functioning.
95259_ActaCardio_67/1__07_11-5199.indd 5395259_ActaCardio_67/1__07_11-5199.indd 53 2/02/12 14:302/02/12 14:30

R. Buys et al.54
of stroke volume and heart rate. However, peak oxygen pulse and peak heart rate seem to be important limiting factors of exercise performance in d-TGA patients. When we consider the peripheral oxygen extraction to be stable, the oxygen pulse can be interpreted as an indirect meas-ure of stroke volume. Apparently, d-TGA patients have difficulties in increasing stroke volume with increasing workloads. Budts et al. previously suggested that the inability to increase stroke volume is probably one of the most important contributing factors for the decreased exercise capacity1. When the stroke volume plateaus
with Senning repair, with a well-preserved right ven-tricular function and a more active lifestyle. Generally, the more physically active d-TGA patients show a better exercise capacity and report a better physical health status than patients who are less active.
These results confirm severely reduced peak exercise performance in d-TGA patients. The exercise perfor-mance depends on the cardiovascular system that deliv-ers oxygen to the working muscles of the body, and the cardiac output needs to increase with increasing exercise intensity. Cardiac output is determined by the product
Table 3 Univariate and multivariate predictors of exercise duration
r-square P-value
Univariate predictors
Gender 0.19 0.0065
Volume of health-related sports/week 0.23 0.0025
Time spent in health-related sports/week 0.24 0.0021
Total energy expenditure 0.20 0.0059
Forced vital capacity 0.14 0.0206
Intensity of active leisure time 0.24 0.0019
Type of repair (Mustard = 0, Senning = 1) 0.11 0.0430
Peak heart rate 0.13 0.0048
Peak oxygen pulse 0.32 0.0003
Multivariate predictors after inclusion of baseline variables
Intensity of active leisure time 0.24 0.0019
Forced vital capacity 0.14 0.0048
Gender 0.13 0.0134
Type of repair (Mustard = 0, Senning = 1) 0.06 0.0300
Total energy expenditure 0.06 0.0407
Multivariate predictors after inclusion of baseline and exercise variables
Peak heart rate 0.53 <0.0001
Peak oxygen pulse 0.37 0.0003
Table 4 Univariate and multivariate baseline predictors of peak VO2%
r-square P-value
Univariate predictors
Volume of health-related sports/week 0.11 0.0366
Time spent in health-related sports/week 0.10 0.0462
Total energy expenditure 0.16 0.0116
Forced vital capacity 0.20 0.0041
Forced expiratory volume in 1 second 0.15 0.0140
Type of repair (Mustard = 0, Senning = 1) 0.15 0.0123
Right ventricular contractility 0.13 0.0234
Multivariate predictors
Type of repair (Mustard = 0, Senning = 1) 0.0043
Right ventricular contractility 0.0262
Total energy expenditure 0.0037
95259_ActaCardio_67/1__07_11-5199.indd 5495259_ActaCardio_67/1__07_11-5199.indd 54 2/02/12 14:302/02/12 14:30

Exercise and health in Mustard/Senning-patients 55
in general. Some ventilatory limitation during exercise is present in the patient group, which might explain a low sports participation level. Other investigators pre-viously reported low levels of physical activity in d-TGA patients and stated that this is partly caused by lower exercise intensities compared to healthy controls12,13. Our results suggest that exercising at greater intensities is important in order to improve exercise capacity. Indeed, the volume and intensity of active leisure time, but not the time spent in active leisure time, were sig-nificantly correlated with peak VO2%. This indicates that, when patients receive optimal medical care, active encouragement to participate in physical activities of moderate intensity will probably result in an improve-ment of the patient’s physical condition. Recent guide-lines published by Hirth et al. state that d-TGA patients benefit from regular low to moderate intense physical activity, but are not eligible for competitive sport10. The current lack of knowledge about the effects and safety of physical activity programmes in this patient group, warrants further research in order to be able to accu-rately and safely guide the patients towards a more active lifestyle27.
Generally, d-TGA patients report a good health status with higher scores in the fields of role, social and emo-tional functioning and bodily pain. We only recorded significant reductions in the field of physical functioning and general health perception, which is in line with other investigators14-16,28. Since perceived physical functioning is related to peak VO2%, a more active lifestyle will prob-ably also have a positive impact on the patients’ per-ceived health status even though an important part of the participants who report normal physical functioning still has a severely reduced exercise capacity. This mis-conception of their physical abilities might be due to the fact that these patients have always been living with their heart condition and that they consider their situation as normal.
Study limitations
First, the low patient number makes it impossible to generalize our results and underpowers the study for separate analysis between Mustard and Senning patients.
Second, our results indicate that Senning repair is related to a better exercise capacity, compared to the Mustard procedure. Since we used the percentage of predicted peak VO2 as dependent variable in our regres-sion analysis, this finding cannot entirely be explained by the fact that Mustard patients are generally older than Senning patients. However, as the exercise capacity might decrease more rapidly with age in d-TGA patients compared to healthy adults, a small effect of the age difference cannot be excluded.
during exercise, a further increase in heart rate enables a further increase in cardiac output. However, our results, in concordance with other studies, show that d-TGA patients present with chronotropic incompetence2,3,5,8.
For clinical purposes, it would be interesting to know which baseline parameters can be influenced in order to improve exercise capacity in this population. First, our results indicate that exercise capacity in d-TGA patients is more impaired in Mustard patients compared to Senning patients. It has previously been reported that Senning patients report a better functional status, are more engaged in sports, and show fewer baffle obstruc-tions, which might explain the better exercise capacity in comparison with Mustard patients2.
Second, the impaired exercise capacity can also partly be explained by right ventricular function. Information from previous investigations of the relation between right ventricular function and exercise capacity is con-flicting and more research is certainly needed1,4,5,13,25,26. Difficulties and differences in the evaluation of right ventricular function, as well as differences in the size and composition of the investigated groups, might be at the origin of this conflicting information.
Even though our findings are contradictory to some previously published investigations, we do believe that the significant relationship we found between qualita-tively assessed right ventricular function and exercise capacity is no coincidence. Li et al. previously concluded that systemic ventricular function as assessed by quan-titative echocardiographic evaluation is an important determinant of exercise capacity in Mustard patients25. Furthermore, an interrelation between exercise capacity and system ventricular function, assessed by the Tei index, in Mustard patients was shown by Norozi et al.26. In d-TGA patients, right ventricular contractility might be decreased because of a reduced preload related to reduced filling of the baffles. Moreover, the right ven-tricle is not designed to be subjected to systemic pres-sures. Therefore the right ventricle might show a less powerful contraction and generate a smaller stroke vol-ume during exercise at higher intensities.
Third, the depressed exercise capacity can partly be explained by low levels of daily physical activity. This is in agreement with Winter et al. who reported that phys-ical activity is positively associated with exercise capacity and health status in patients with a systemic right ven-tricle13.
Most of the patients have adopted a sedentary life-style and do not reach the recommendations for phys-ical activity of the World Health Organization in order to improve cardiorespiratory and muscular fitness and reduce the risk of non-communicable diseases and depression. Indeed, most of the patients in our study are not involved in sports and show a low active lifestyle
95259_ActaCardio_67/1__07_11-5199.indd 5595259_ActaCardio_67/1__07_11-5199.indd 55 2/02/12 14:302/02/12 14:30

R. Buys et al.56
related to a better exercise capacity. Furthermore, an active lifestyle that includes participation in sports activ-ities of moderate intensity has a positive effect on exer-cise capacity and perceived physical functioning. There-fore it might be indicated to actively encourage d-TGA patients to adopt a more physically active lifestyle.
ACKNOWLEDGEMENTS
We greatly appreciate the work of Jan Meertens and Dirk Schepers in the exercise testing laboratory, as well as the help of Sonia Rens and Sara Van Damme with the collection of the questionnaires.
CONFLICT OF INTEREST: none declared.
Third, even though 20% of the Mustard patients and 5% of the Senning patients treated in our clinic are pacemaker-dependent, no one in our study group had a pacemaker. Consequently, our results cannot be gen-eralized to the entire Mustard/Senning population.
Fourth, information from Holter monitoring was not available, making it impossible to evaluate sinus node dysfunction as an explanation for the suggested chrono-tropic incompetence.
CONCLUSION
d-TGA patients have a severely reduced peak exercise performance that in a large part results from the inabil-ity to increase stroke volume and heart rate at higher exercise intensities. In this patient group, Senning repair and a well-preserved right ventricular function are
1. Budts W, Scheurwegs C, Stevens A, Moons P, Van Deyk K, Vanhees L. The future of adult patients after Mustard or Senning repair for transposition of the great arteries. Int J Cardiol 2006; 113: 209-14.
2. Moons P, Gewillig M, Sluysmans T, Verhaaren H, Viart P, Massin M, Suys B, Budts W, Pasquet A, De Wolf D, Vliers A. Long term outcome up to 30 years after the Mustard or Senning operation: a nationwide multicentre study in Belgium. Heart 2004; 90: 307-13.
3. Buys R, Cornelissen V, Van De Bruaene A, Stevens A, Coeckelberghs E, Onkelinx S, Thomaes T, Delecluse C, Budts W, Vanhees L. Measures of exercise capacity in adults with congenital heart disease. Int J Cardiol 2011; 153: 26-30.
4. Hechter SJ, Webb G, Fredriksen PM, Benson L, Merchant N, Freeman M, Veldtman G, Warsi MA, Siu S, Liu P. Cardiopulmonary exercise performance in adult survivors of the Mustard procedure. Cardiol Young 2001; 11: 407-14.
5. Diller GP, Dimopoulos K, Okonko D, Li W, Babu-Narayan SV, Broberg CS, Johansson B, Mullen MJ, Poole-Wilson PA, Francis DP, Gatzoulis MA. Exercise intolerance in adult congenital heart disease: comparative severity, correlates, and prognostic implication. Circulation 2005; 112: 828-35.
6. Fredriksen PM, Veldtman G, Hechter S, Therrien J, Chen A, Warsi MA, Freeman M,Liu P, Siu S, Thaulow E, Webb G. Aerobic capacity in adults with various congenital heart diseases. Am J Cardiol 2001; 87: 310-4.
7. Warnes CA. Transposition of the great arteries. Circulation 2006; 114: 2699-709.
8. Douard H, Labbe L, Barat JL, Broustet JP, Baudet E, Choussat A. Cardiorespiratory response to exercise
after venous switch operation for transposition of the great arteries. Chest 1997; 111: 23-9.
9. Giardini A, Hager A, Lammers AE, Derrick G, Müller J, Diller GP, Dimopoulos K, Odendaal D, Gargiulo G, Picchio FM, Gatzoulis MA. Ventilatory efficiency and aerobic capacity predict event-free survival in adults with atrial repair for complete transposition of the great arteries. J Am Coll Cardiol 2009; 53: 1548-55.
10. Hirth A, Reybrouck T, Bjarnason-Wehrens B, Lawrenz W, Hoffman A. Recommendations for participation in competitive and leisure sports in patients with congenital heart disease: a consensus document. Eur J Cardiovasc Prev Rehabil 2006; 13: 293-9.
11. Dua JS, Cooper AR, Fox KR, Graham Stuart A. Physical activity levels in adults with congenital heart disease. Eur J Cardiovasc Prev Rehabil 2007; 14: 287-93.
12. De Bleser L, Budts W, Sluysmans T, De Wolf D, Massin M, Gewillig M, Suys B, Moons P. Self-reported physical activities in patients after the Mustard or Senning operation: comparison with healthy control subjects. Eur J Cardiovasc Nurs 2007; 6: 247-51.
13. Winter MM, Bouma BJ, Van Dijk AP, Groenink M, Nieuwkerk PT, Van Der Plas MN, van der Plas MN, Sieswerda GT, Konings TC, Mulder BJ. Relation of physical activity, cardiac function, exercise capacity, and quality of life in patients with a systemic right ventricle. Am J Cardiol 2008; 102: 1258-62.
14. Hager A, Hess J. Comparison of health related quality of life with cardiopulmonary exercise testing in adolescents and adults with congenital heart disease. Heart 2005; 91: 517-20.
15. Lane DA, Lip GY, Millane TA. Quality of life in adults with congenital heart disease. Heart 2002; 88: 71-5.
16. Gratz A, Hess J, Hager A. Self-estimated physical functioning poorly predicts actual exercise capacity in adolescents and adults with congenital heart disease. Eur Heart J 2009; 30: 497-504.
17. Wasserman K, Hansen J, Sue D. Physiology of exercise. Philadelphia: Lea and Febiger; 1999; p. 10-61.
18. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J, ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J 2005; 26: 319-38.
19. Matton L, Wijndaele K, Duvigneaud N, Duquet W, Phillipaerts R, Thomis M, Lefevre J. Reliability and validity of the Flemish Physical Activity Computerized Questionnaire in adults. Res Q Exerc Sport 2007; 78: 293-306.
20. Scheers T, Philippaerts R, Van Langendonck L, Duquet W, Duvigneaud N, Matton L, Thomis M, Wijndaele K, Lefevre J. Lipid profile in men and women with different levels of sports participation and physical activity. Public Health Nutr 2008; 11: 1098-106.
21. Aaronson NK, Muller M, Cohen PD, Essink-Bot ML, Fekkes M, Sanderman R, Sprangers MA, te Velde A, Verrips E. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol 1998; 51: 1055-68.
22. Benjamini Y, Hochberg Y. Controlling for the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society. Series B (Methodological) 1995; 57: 289-300.
23. Roest AA, Lamb HJ, Van Der Wall EE, Vliegen HW, van den Aardweg JG, Kunz P, de Roos A, Helbing WA. Cardiovascular response to physical exercise in adult patients after atrial correction for transposition of the great arteries
REFERENCES
95259_ActaCardio_67/1__07_11-5199.indd 5695259_ActaCardio_67/1__07_11-5199.indd 56 2/02/12 14:302/02/12 14:30

Exercise and health in Mustard/Senning-patients 57
assessed with magnetic resonance imaging. Heart 2004; 90: 678-84.
24. Schaefer A, Tallone EM, Westhoff-Bleck M, Klein G, Drexler H, Röntgen P. Relation of diastolic and systolic function, exercise capacity and brain natriuretic peptide in adults after Mustard procedure for transposition of the great arteries. Cardiology 2010; 117: 112-17.
25. Li W, Hornung TS, Francis DP, O’Sullivan C, Duncan A, Gatzoulis M, Henein M. Relation of
biventricular function quantified by stress echocardiography to cardiopulmonary exercise capacity in adults with Mustard [atrial switch] procedure for transposition of the great arteries. Circulation 2004; 110: 1380-6.
26. Norozi K, Buchhorn R, Alpers V, Arnhold JO, Schoof S, Zoege M, Geyer S, Wessel A. Relation of systemic ventricular function quantified by myocardial performance index [Tei] to cardiopulmonary exercise capacity in adults after Mustard procedure for
transposition of the great arteries. Am J Cardiol 2005; 96: 1721-5.
27. Thaulow E, Fredriksen PM. Exercise and training in adults with congenital heart disease. Int J Cardiol 2004; 97 Suppl 1: 35-8.
28. Kamphuis M, Ottenkamp J, Vliegen HW, Vogels T, Zwinderman KH, Kamphuis RP, Verloove-Vanhorick SP. Health related quality of life and health status in adult survivors with previously operated complex congenital heart disease. Heart 2002; 87: 356-62.
95259_ActaCardio_67/1__07_11-5199.indd 5795259_ActaCardio_67/1__07_11-5199.indd 57 2/02/12 14:302/02/12 14:30