
Improving Soft Tissue Form Around Implants via Forced Eruption
17
Improving Soft Tissue Form Around Implants via Forced Eruption Tal Morr, OM 0, MSO I . O ntegration of a single-tooth implant in the esthetic zone can be one of the most diffi- cult treatment options because of the nu- merous biologic and esthetic requirements. Of critical importance is the soft tissue integration of the implant-supported restoration relative to the rest of the anterior teeth. Failure to mimic the nat- ural gingival form from both the cervical contour and the papillary form can create an esthetic dilemma. The need to preserve the gingival form has led to the trend of immediate implant place- ment. After anterior tooth loss, the normal course of wound healing will cause the facial bone and soft tissue to recede both facially and palatally.'-4 Without support, this recession may be com- pounded by the loss of the interdental papilla. s This creates a narrower residual ridge that may im- pede placement of an implant in an ideal, restora- Private practice, Aventura, Florida, USA. Correspondence to: Dr Tal Morr, 20760 West Dixie Hwy, Aventura, FL33180, USA. Fax: +305 935 6753. E-mail: [email protected] _QDT2005 tively driven position without additional surgical procedures, even if the soft tissue form looks ac- ceptable. 6 Although surgical procedures to rebuild the residual ridge can be performed with gener- ally good results, rebuilding the papilla to its proper form can be much more of a challenge. Forced eruption via orthodontics can be a critical adjunct to regenerating papillae adjacent to an implant, especially when papillary regeneration via a surgical procedure may not achieve the de- sired result. CASE 1 A 40-year-old woman was referred to the office by an orthodontist who questioned the integrity of an existing anterior restoration made 18 years earlier. At age 18, the patient had had an accident in which she lost tooth 6(13) and fractured the re- maining incisors, with a resultant need for en- dodontic treatment. The patient was rehabilitated with a fixed partial denture from teeth 3(16) through 8(11) (tooth 5[14] was extracted for or-
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Improving Soft Tissue Form Around Implants via Forced Eruption

Improving Soft Tissue Form Around Implantsvia Forced Eruption
Tal Morr, OM 0, MSO
I.
O ntegration of a single-tooth implant in theesthetic zone can be one of the most diffi-cult treatment options because of the nu-
merous biologic and esthetic requirements. Ofcritical importance is the soft tissue integration ofthe implant-supported restoration relative to therest of the anterior teeth. Failure to mimic the nat-ural gingival form from both the cervical contourand the papillary form can create an estheticdilemma. The need to preserve the gingival formhas led to the trend of immediate implant place-ment. After anterior tooth loss, the normal courseof wound healing will cause the facial bone andsoft tissue to recede both facially and palatally.'-4Without support, this recession may be com-pounded by the loss of the interdental papilla.s
This creates a narrower residual ridge that may im-pede placement of an implant in an ideal, restora-
Private practice, Aventura, Florida, USA.Correspondence to: Dr Tal Morr, 20760 West Dixie Hwy,Aventura, FL33180, USA. Fax: +305 935 6753.E-mail: [email protected]
_QDT2005
tively driven position without additional surgicalprocedures, even if the soft tissue form looks ac-ceptable.6 Although surgical procedures to rebuildthe residual ridge can be performed with gener-ally good results, rebuilding the papilla to itsproper form can be much more of a challenge.Forced eruption via orthodontics can be a criticaladjunct to regenerating papillae adjacent to animplant, especially when papillary regenerationvia a surgical procedure may not achieve the de-sired result.
CASE 1
A 40-year-old woman was referred to the office byan orthodontist who questioned the integrity of anexisting anterior restoration made 18 years earlier.
At age 18, the patient had had an accident inwhich she lost tooth 6(13) and fractured the re-maining incisors, with a resultant need for en-dodontic treatment. The patient was rehabilitatedwith a fixed partial denture from teeth 3(16)through 8(11) (tooth 5[14] was extracted for or-

Improving Soft Tissue Form Around Implants via Forced Eruption ••
Fig 1 Initial radiographs at presenta-tion.
Fig 2 Lips at rest during initial evalua-tion.
Fig 3 Smile during initial evaluation.Note the papillary levels from right toleft; the papillae on the right side areshorter.
Fig 4 Intraoral frontal at presentation.Note the discrepancy in the level ofthe gingiva, which is higher on theright side.
Fig 5 Initial preparations. Note theshort preparations and form of thepontic area.
thodontic purposes, 6[13] because of trauma),with single units (full-coverage crowns) on teeth9(21) and 10(22).
Implants were not readily available at the timeof the injury, so the patient opted for a fixed partialdenture to replace the missing canine. Radio-graphic evaluation revealed fairly short roots onthe anterior teeth, with good residual height ofbone in the area of tooth 6(13),although there hadbeen both vertical and horizontal bone loss (Fig 1).
Clinical evaluation of the incisal edge at rest po-sition revealed approximately 5 mm of tooth expo-
sure (Fig 2). Assessment during smiling showedmore papilla on the left side than the right (Fig 3).
At the time of examination the patient was al-ready in mandibular orthodontic appliances for thecorrection of crowding (Figs 4 and 5). After intra-oral evaluation, it was determined that the marginalintegrity of the restorations was compromised bywashout of the cement and the resultant decay.
Evaluation of the pontic area 6(13) revealed fairto good remaining soft tissue form, although defi-cient in the horizontal aspect and the papillae(Figs 4 and 5). The soft tissue margin was posi-
QDT200Sa.
iiiMORR
tioned more cervically around tooth 7(12) andmore coronally around tooth 11(23) than aroundthe other remaining anterior teeth. The marginaltissue contours on the central incisors were notsymmetrical or level. The papillary heights werenot level; the papillae on the left side were morecoronal than on the right (see Figs 3 and 4).
Treatment Plan
The patient wanted to have single-tooth prosthesesrather than bridgework. To determine if this waspossible, the teeth would be evaluated periodon-tally at the time of provisionalization to determinewhether they could be maintained as single units.Once the determination was made that the teethcould be made into single units from the stand-points of function, mechanics, and biology, themarginal heights of the soft tissue would be cor-rected with crown lengthening along with an im-plant placed in the area of tooth 6(13). The softtissue around tooth 7(12) would be coronally posi-tioned to cover the exposed root and help to levelthe soft tissue. Shortening of the incisal edges andcervical positioning of the soft tissue would main-tain the proportions of the teeth.
The final restorations would be fabricated withProcera crowns (Nobel Biocare, Goteborg, Swe-den) to replace teeth 3(16), 5(14), 7(12), 8(11),9(21), and 10(22), with a porcelain-fused-to-metalcrown and a gold custom abutment replacingtooth 6(13) and a feldspathic veneer tooth replac-ing tooth 11(23).
The patient began treatment as described. Atthe time of provisionalization, it became evidentthat the patient needed crown lengthening, notonly for esthetic reasons but also for form retentionand resistance of the preparations because of theinadequate height (see Fig 5). The mobility of theteeth was negligible; therefore, an implant wasdeemed appropriate for replacement of tooth6(13). Once the functional and esthetic require-ments were fulfilled in the provisional phase (Fig 6),the patient was sent to a periodontist for estheticcrown lengthening and an implant to replace the
IIIIIODT 2005
missing maxillary right canine. The patient wasanesthetized with Xylocaine (AstraZeneca, London,United Kingdom) 1:100,000 epinephrine. A sulcularincision was made around tooth 7(12) and contin-ued into an inverse bevel incision at the newmarginal levels of the remaining maxillary anteriorteeth, sparing the papilla from the mesial of tooth7(12) to the distal of tooth 12(24). In the area ofteeth 3(16) through 5(14), facial and palatal flapswere reflected to enable circumferential ostectomyfor resistance and retention form of the prepara-tions. Vertical incisions were made on the mesial oftooth 5(14) and the distal of tooth 7(12) internal tothe papilla on either side to enable coronal posi-tioning of the soft tissue over the implant site 6(13).In the area of the residual ridge, the flap was ex-tended slightly palatal of the center of the ridge toobtain extra tissue. Upon reflection of the flap, thebone was reshaped on all teeth slightly coronal tothe bony level of tooth 7(12), as it was the limitingfactor because of its bony dehiscence, short root,and minimal bony support. No bone was removedaround tooth 7(12) at all. A narrow-diameter stan-dard neck dental implant (Straumann,Waldenburg,Switzerland) was placed in the area of tooth 6(13)with the head of the implant 3.0 mm cervical to thedesired gingival margin of the future implant crownas dictated by the surgical stent (Figs 7 and 8). Thesoft tissue was sutured in place with the flap overthe implant coronally positioned to gain verticalheight (Fig 9). The soft tissue around tooth 7(12)was also coronally positioned to level the gingivalmargins (Fig 10).
At 5.5 months, the biologic width had re-estab-lished itself, and the patient was ready to begin re-lining of the provisionals and soft tissue manipula-tion in the area of the implant. Verification ofmaturation was made by sounding to bone andcomparing the biologic width in the implant area toareas that were not surgically modified. The massof the papilla on the mesial of the implant (distal of7[12]) was almost negligible, with only the palatalaspect remaining (Figs 11 and 12). The marginalridge remained very flat, with an angular transitionfrom the marginal ridge to the papilla rather than anice scallop (Fig 12). The gingival margin around

Improving Soft Tissue Form Around Implants via Forced Eruption ••
Fig 6 First set of provisionals.
Fig 7 Implant placement from an occlusal view. Notethe reflection of the papilla on the distal of tooth 7(12).
Fig 8 Implant placement from a facial perspectivewith the provisional in place.
Fig 9 Coronal positioning of the flap over the implantand healing abutment.
Fig 10 Facial view of suturing after implant placementin the area of tooth 6(13), crown lengthening of theanteriors (except tooth 7[12]), and coronal positioning'of the soft tissue over tooth 7(12).
tooth 7(12) ended up in a more cervical positionthan the remaining anterior teeth (Fig 11). Theteeth were prepared again to the gingival level, ex-cept for tooth 7(12),which was left slightly coronalto the margin (Fig 11). An octa-abutment wastorqued into the implant, followed by modificationof a titanium temporary abutment with addition ofacrylic resin to create a root form to support and
mold the soft tissue (Figs 13 and 14).The provision-als were relined, and the patient was told to returnin 3 months.After 3 months, the soft tissue form around the
implant was still unacceptable. Not only was the fa-cial half of the papilla almost nonexistent, with onlythe palatal aspect remaining, but the marginalridge form around the implant was too flat and an-
ODT 2005II1II

• MORR
gular, creating a defect on the mesial of the canine(Fig 15). The marginal ridge height of tooth 7(12)remained more cervical than the remaining teeth.
At the time of the initial evaluation it seemedthat there was adequate soft tissue and bony to-
• QDT 2005
Fig 11 Soft tissue form after full healing and refor-mation of the biologic width. Note the defect aroundthe implant at site 6(13).
Fig 12 Lateral view of the soft tissue around the im-plant at site 6(13).
Fig 13 Placement of an acta-abutment prior to fabri-cation of a temporary abutment.
Fig 14 Temporary abutment in place after beingmodified with a bur and acrylic resin. Note the flatgingival form and deficient papilla on the mesial ofthe implant.
Fig 15 Provisional relined over the temporary abut-ment. Note the short papilla on the mesial of the ca-nine compared to the other teeth.
pography to adequately restore tooth 6(13)with animplant without bone augmentation prior to place-ment. In hindsight, it may have been appropriate inthis caseto augment at least the soft tissue compo-nent in this area. The patient had fairly thin soft tis-

Improving Soft Tissue Form Around Implants via Forced Eruption II
sue, especially in the papillary area distal to tooth7(12) (see Fig 5). Evaluation of the preoperativephotographs reveals that the papillary heights onthe right side of the maxilla were at least 1.5 mmshorter than those on the left side (see Figs 4 and5). Without augmentation, the two sides wouldnever be at the same levels.
At the time of surgery, a vertical incision wasmade through the distal papilla of tooth 7(12) toallow coronal repositioning of the flap over thehealing abutment so that the soft tissue could gainvertical height. Close observation of the surgicalprocedure shows that the incision was placed veryclose to tooth 7(12), leaving very little bulk or massof papilla (see Figs 8 and 9). As a result, the bloodflow to the area was compromised, and the facialaspect of the papilla sloughed over time, leavingonly the palatal aspect. Both a loss in vertical andhorizontal massof the papilla was evident (see Figs11 and 12). A better approach may have been to in-clude the papilla in the flap by making the verticalincision at the distal line angle of the central incisorrather than through the papilla. This would have al-lowed even greater freedom to coronally positionthe flap and possibly get root coverage over thelateral incisor.
Options for Redevelopment of the Papillaand Marginal Tissue
One option for regeneration of the papilla andmesial marginal ridge of the implant was to wait forthe biologic width to regenerate. The dentogingivalcomplex was described in 1961 by Garguilo et all ina study in which they measured the distance fromthe free gingival margin to the underlying bone.This complex comprises the connective tissue at-tachment, the epithelial attachment Qunctionalep-ithelium), and the gingival sulcus. They reportedmeasurements of 2.04 mm for the depth of theconnective tissue and epithelial attachments and0.69 mm for the depth of the sulcus. KoisB de-scribed a similar biologic width of 3 to 4 mm on thefacial aspect of central incisors,with 85%of the sub-jects within the 3-mm range. Interproximally,a mea-
surement of 4.5 mm was observed. This coincideswith the study done by Tarnow and associates inwhich they measured the distance from the cervicalcontact to the underlying bone and evaluated thepresence or absence of a papilla.9 There was com-plete presence of a papilla when the distance waslessthan 5 mm. Both of these studies evaluated thepapilla between two adjacent intact teeth. Betweentwo teeth, the papillary height is actually controlledby the shape and volume of the gingival embra-sure, which is determined by the contours of theadjacent roots and teeth and the level of interseptalbone. When one of the contacts is eliminated viatooth loss, aswas the casewith the missing canine,the papilla will generally collapse to a normal bio-logic dimension of 3 mm. The connective tissue at-tachment and junctional epithelium in the papillaryarea still compose only 2 mm of the total length ofthe papilla, as they do at the free gingival margin.Between a tooth and an implant, bony support ofthe soft tissue papilla comes from the attachmentlevel at the tooth side, not the bone level of the im-plant.lO Waiting for the regeneration of the papillacould take up to 1 year,and there would still remaina vertical and horizontal deficiency in comparisonwith the adjacent papilla. This would also not ad-dress the marginal discrepancy of tooth 7(12). Thesecond option for redeveloping the papilla was tosurgically rebuild the papilla. Several techniqueshave been proposed for rebuilding the papillaaround single-tooth implants,11.12although they aredifficult to perform, predictability hasnot been doc-umented, and there are no data regarding long-term stability. These surgical techniques also relysolely on thickening of the overlying soft tissuewithout augmentation of the underlying supportingbone. The most biologically sound and predictablemethod for altering gingival/eve/s and papillary lev-elswas to forcibly erupt tooth 7(12).
Forced Eruption
Forced eruption is defined as an orthodontic pro-cess whereby a tooth is intentionally moved in acoronal direction through the application of gen-
ODT 2005

IIMORR
tie, continuous force in order to effect changes inthe soft tissue and bone.13.14Because forced erup-tion modifies the gingival and alveolar crest, it hasbeen used to alter gingival discrepancies and os-seous defects of periodontally involved teeth.15-19The fibers of the periodontal ligament are at-tached to the bone by fibers, with formation ofnew bone around the ends of the fibers.20.21Boneis dynamic in nature and hence is constantly beingresorbed and rebuilt. When tension is applied tothe periodontal ligament, periodontal fibers areelongated, and osteoblasts are induced to de-posit new bone in the alveolus, where the attach-ment is.22.23When a tooth is erupted, the bonecomes with it and the height of the fiber attach-ment remains constant.24 If a tooth is forciblyerupted and, following the movement, held in itsnew position for 4 to 6 months, the bone and softtissue should re-establish themselves in this new3-dimensional position.
Technique
The provisional restorations were sectioned, leav-ing the restoration at 7(12)as a single unit. This unitwas cemented with a final cement (RelyXARC, 3MESPE,St Paul, MN) to prevent loosening during theforced eruption. Only three brackets were used forthe eruptive process (Fig 16): one on the maxillaryright canine, one on the maxillary right lateral in-cisor, and one on the maxillary right central incisor.Because the canine was an implant and the rightcentral incisor was splinted to the other central in-cisor and the left lateral incisor medially, there wasno mobility and hence no reason to add morebrackets posteriorly. The bracket on the lateral in-cisor was placed more cervical in relation to thebrackets on the canine and central incisor to createa coronal force on the lateral incisor for eruptivepurposes (Fig 16). Once the brackets were placedand the acrylic resin was set, nickel titanium wirewas placed in the brackets and held with ties. Asmall-diameter 0.016-mm wire was used to create aslow force during eruption to bring down the boneand soft tissue with the maxillary right lateral in-
: GDT 2005
cisor.The forced eruption process in this case tookonly 2 weeks (Fig 17).This was most likely becauseof the limited bony support around the root of thelateral incisor (Fig 19). Once the lateral incisor waserupted to its correct position, it was luted back to-gether with the remaining provisionals and thebrackets were removed. The incisal edge wasshortened to compensate for the eruption. Gener-ally, a 4- to 6-month stabilization period is advo-cated to allow for proper reorganization of the softtissue and bone and for prevention of relapse (in-trusion).25In this case, a 4-month stabilization pe-riod was chosen to allow redevelopment of thepapilla and the gingival margin around the implant.Not only was the gingival margin around the lateralincisor brought more coronal, but the papillaryheight was increased by approximately 1.5 mm(Figs 18 and 20). Although there was good im-provement in the papillary form and the gingivalmargin of both the canine and lateral incisor, thethickness and bulk of the papilla preventedachievement of an ideal form on the mesial aspectof the marginal ridge of the canine (Figs 20 and21). Once the tissue was healthy, final impressionswere taken (Fig 22).
All of the restorations other than the implantcrown and the veneer were fabricated from all-ceramic Procera crowns (Nobel Biocare). For theimplant crown, a castable custom gold abutmentwas fabricated (Fig 23). It was decided to use goldrather than a ceramic abutment because thecrown for the implant was going to be made ofporcelain fused to metal, allowing the same typeof porcelain to be used for the porcelain veneersfor the purpose of color matching. If a Proceracrown had been made for the implant, the porce-lain used for the veneer would have to have beenmade of a different type of porcelain than theoverlay porcelain for the Procera. This in turnwould have been difficult to match.
The final results were good considering theoriginal soft tissue defect following surgery (Figs24 through 26). Radiographs showed that theimplant was well integrated, and the new boneapical to the root of tooth 7(12) filled in nicely(Figs 19 and 27).
Improving Soft Tissue Form Around Implants via Forced Eruption.
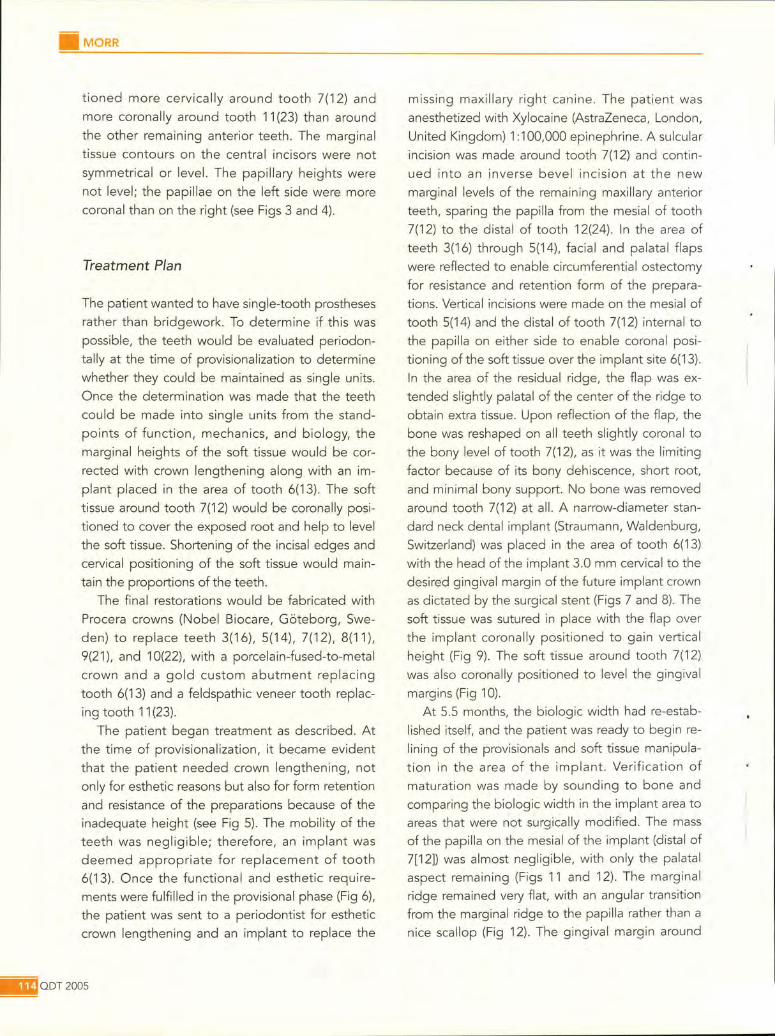
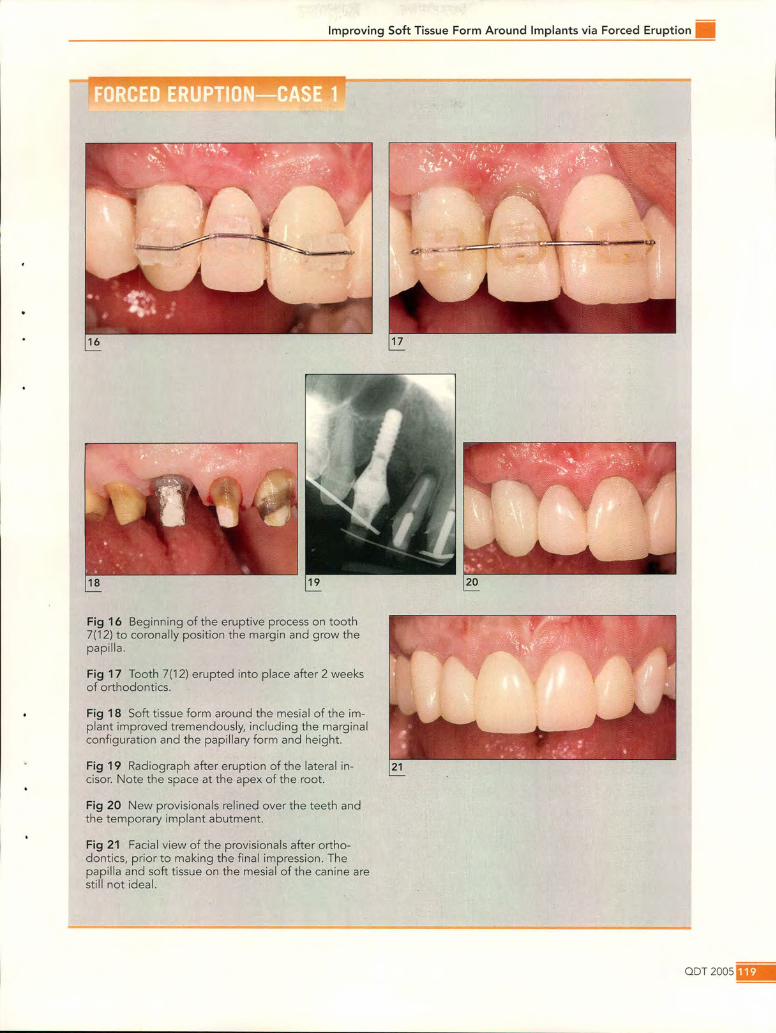
Fig 16 Beginning of the eruptive process on tooth7(12) to coronally position the margin and grow thepapilla.
Fig 17 Tooth 7(12) erupted into place after 2 weeksof orthodontics.
Fig 18 Soft tissue form around the mesial of the im-plant improved tremendously, including the marginalconfiguration and the papillary form and height.
Fig 19 Radiograph after eruption of the lateral in- 21cisar. Note the space at the apex of the root.
Fig 20 New provisionals relined over the teeth andthe temporary implant abutment.
Fig 21 Facial view of the provisionals after ortho-dontics, prior to making the final impression. Thepapilla and soft tissue on the mesial of the canine arestill not ideal.
QDT200S_

IIMORR
_ODT2005
Fig 22 Final preparations with chord and implant transfer coping on implant 6(13).Note the improved clinical crown length on the teeth.
Fig 23 Final gold abutment on implant 6(13).
Fig 24 Intraoral frontal view of the final case.
Fig 25 Final smile.
Fig 26 Lateral view of final crowns.
Fig 27 Final radiograph of implant 6(13).

Improving Soft Tissue Form Around Implants via Forced Eruption II
CASE 2
A 55-year-old man presented with a porcelain-fused-to-metal crown on tooth 7(12) in his hand.The crown had come loose the previous day (Fig28); the post had remained within the crown. Thisis a classicexample of the failure associated with alack of ferrule in which the cement seal breaks, thecement washes out, and the post comes out withthe crown, leaving decay in the canal and a bro-ken-down tooth.26 There was approximately 0.5mm of remaining tooth structure above the gingi-val line with decay into the canal space (Fig 28).For long-term predictability, there needs to be atleast 1.5 mm of tooth structure beyond the coreto create a "ferrule effect."26
Evaluation of the gingival levels revealed anideal gingival margin location, and the patient de-sired an ideal esthetic result. The patient wasgiven three options, although there were only twooptions (options 1 and 2) for treatment that wouldmaintain the same gingival levels:
• Option 1: Forced eruption of tooth 7(12) alongwith supracrestal fiberotomy
• Option 2: Extraction of the tooth and immediateimplant placement
• Option 3: Crown lengthening, which would cre-ate a "long tooth" relative to the adjacent teethand disturb the esthetic balance
The patient refused to wear braces due to van-ity reasonsand therefore chose option 2. Alginateswere taken, and a removable provisional was fabri-cated to replace tooth 7(12). The patient was re-ferred to an oral surgeon for extraction of thetooth and immediate implant placement. Peri-otomes were used to extract tooth 7(12) with notrauma to the surrounding bone and soft tissue. A4.1 X 3.8-mm implant (Straumann)was placed inthe extraction socket with the head of the implantplaced 3 mm apical to the desired marginal ridge(Fig 29). An implant design that decreases in diam-eter apically (ie, a tapered implant) is ideal to pre-vent perforation or stress to the thin labial plate.The surgeon modified a plastic healing abutment
to create the proper anatomical emergence form(Figs 30 and 31). The healing abutment was leftabove the gingival margin to allow full support forthe papilla. The removable provisional was in-serted as a temporary prosthesis (Fig 31).
After 6 months of healing, the patient was readyfor restoration. A titanium temporary abutment wasmodified with acrylic resin to create the properemergence profile (Fig 32). The acrylic resin wasapplied with a salt-and-pepper technique directlyinto the sulcus form created by the healing abut-ment. Once set, the temporary abutment was pre-pared directly in the mouth. The provisional was re-lined over the abutment, and the tissue wasallowed to heal for 1 month prior to the final im-pression (Fig 33). Even with meticulous surgicaltechnique, there was slight recession on the distalaspect of the central incisor papilla.
At the time of the final impression, acrylic resinwas added to the transfer coping to register theemergence profile to the final model. A polyvinylsiloxane impressionwas taken and poured in stone.
A custom abutment was fabricated using acastable abutment. Porcelain was baked on theabutment to create the emergence form and tocover the metal of the abutment so that an all-ceramic crown could be used (Fig 34). An Inceramcrown (Vita, Bad Sackingen, Germany) was fabri-cated to match the existing porcelain Dicor crowns(Dentsply, York, PAl (Fig 35). After torquing theabutment and cementing the final crown, the pa-tient was told to return in 1 week for photographs.
Emergency Visit
Six days after delivery of the implant crown, tooth8(11) had fractured down to the gingival line. Thepatient again presented to the office with a crownin his hand, although this time, the preparationwas broken within the crown (Fig 36).
Intraoral evaluation revealed that the gingivalmargin of tooth 8(11)was in the ideal position. Thetooth had fractured to the gum line with no remain-ing ferrule effect, but radiographically, there wasenough root length to restore the tooth if the
aDT 2005

iiiMORR
mQDT200S
Fig 28 Tooth fracture down to thegum line.
Fig 29 Implant placed immedi-ately at the site of tooth 7(12).
Fig 30 Healing abutment support-ing the soft tissue around the im-p/ant.
Fig 31 Flipper in place with softtissue, supported by the healingabutm\"nt.,
Fig 32 Temporary abutmentprepped and modified with acrylicresin to create the proper emer-gence form.
Fig 33 Placement of the provi-sional.
Fig 34 Final porcelain-fused-to-metal abutment. Porcelain wasbaked on the abutment to coverthe metal and create a tooth-colored margin and post.
Fig 35 Final crown at try-in.

Improving Soft Tissue Form Around Implants via Forced Eruption.
Fig 36 Tooth8(11) fractlJredto the gumline 1 weekafter deliveryof an implant-supportedcrownat site 7(12).
Fig 37 Radiographof the fracturedtooth. Note the angularpeaksof bone aroundthe root.
crown was lengthened or the tooth erupted (Fig37). The root taper was fairly significant, so a nar-rower marginal diameter would be created if thetooth was crown lengthened or erupted. The inter-proximal bone surrounding the root of tooth 8(11)
was angular, not horizontal, with the peaks morecoronal than the adjacent bone. The root was actu-ally supporting the two peaks of interseptal bone.Taking the aforementioned into consideration,
the patient was given two options for treatment.Only option 1 would ensure an ideal gingivalmarginal relationship; however, option 2 was moresound biomechanically:
• Option 1: Forced eruption with supracrestalfiberotomy and restoration with a crown
• Option 2: Implant placement immediately post-extraction and restoration with a single crown
Even though it would take much longer toforcibly erupt tooth 8(11}, and even with thebiomechanical compromise of maintaining thetooth versus placing an implant, the patient chose
to maintain his tooth for esthetic reasons and felthe could always have an implant placed if thetooth failed over time.There were many reasonswhy forcibly erupting
the central would create a more esthetic result. Ra-diographically, it was evident that the root of tooth8(11) was supporting the angular interproximalpeaksof bone surrounding the root (Fig 36). Extrac-tion of the root, even with immediate implantplacement, would inevitably have resulted in theloss of the interseptal bony peaks. After extractionand immediate implant placement, there is gener-ally up to 1 mm of apical migration of the free gin-gival margin.27.28Interproximally, the ideal bonewidth is approximately 1.5 mm at the crest to mini-mize lateral resorption of the osseouscrest and bio-logic width violation after implant placement withresultant bone loss.29The bone on the distal of theroot of tooth 8(11) adjacent to the implant was thin(lessthan 1.5 mm), especially in the coronal portion(Fig 37). Becausethe interproximal bone was angu-lar, in order to maintain the peaks of bone, the im-plant would need to have been placed more coro-
ODT 20051&11

• MORR
nal than the adjacent implant and tooth 9(21).Thiswould have created a very short distance from theimplant head to the free gingival margin, whichwould have made creating a smooth emergenceprofile very difficult. Placementof the implant in thecorrect depth for creation of a smooth emergenceprofile would have necessitated obliteration of theangular peaks of interseptal bone. The last disad-vantage of placing an implant adjacent to anotherimplant is that when 2 adjacent implants areplaced, the biologic width around flat implantsdoes not support the papilla interproximally.30Infact, only 3 to 4 mm of interproximal soft tissueheight is routinely possible, even with a 3-mm dis-tance between implants, as advocated by Tarnowet al.29Becausethe biologic width is apical to thecrest of interproximal bone between implants, theconnective tissue attachment and the epithelial at-tachment will not support the papilla. Findings byTarnow et al31indicated that the height of the softtissue covering the inter-implant bony crest is 2 to4 mm as compared to the 5 mm found aroundteeth. Kois and Kan32also found comparable mea-surements of 3 to 4 mm of peri-implant mucosaforanterior single implants.
Taking the aforementioned into consideration,placement of an implant in the area of tooth 8(11)would most likely have created an esthetic night-mare due to loss of papilla, especially betweenthe two implants, as compared to forced eruptionwith a supracrestal fiberotomy of the remainingroot of tooth 8(11). Again, the patient chose tomaintain his natural root.
Forced Eruption with SupracrestalFiberotomy
It is advantageous to erupt a tooth for the purposeof crown lengthening when there is need forsound tooth structure and the gingival height andcontour is ideal. Given that surgery would createan imbalance in the marginal levels and increasethe crown-to-root ratio, orthodontic eruption witha fiberotomy is the treatment of choice. Kozlovskyet al33used forced eruption combined with an inci-
. QDT 2005
sion of the supracrestal gingival attachment. Theintrasulcular incisions were performed in conjunc-tion with root-surface curettage at 2-week inter-vals. This technique prevented coronal displace-ment of the attachment apparatus, eliminating theneed for surgery. Pontoriero et al34indicated thatthe fiberotomy eliminated tensile stress on thealveolar bone and allowed more rapid toothmovement. Bone and soft tissue were left behind,although they recommended weekly fiberotomies.
Technique
The patient was sent to an endodontist for rootcanal treatment of the maxillary right central in-cisor. Once week later, a GC post pattern (GCDental, Tokyo, Japan) was fabricated and cast intype III gold alloy. After cementation with zincphosphate cement, the preparation was refinedwith a diamond bur, and an acrylic resin provi-sional was fabricated. The provisional was ce-mented with RelyXARC cement to ensure reten-tion during the eruption process.
Five brackets were placed; one on the implantcrown at site 7(12), one on the provisional, andthree on the contralateral central incisor, lateral in-cisor,and canine for anchorage (Fig 38).
The bracket on tooth 8(11) was placed 2.5 mmcervical to the remaining brackets to create acoronal force after wire placement. Prior to plac-ing the wire, the patient was anesthetized on boththe facial and palatal aspects of the soft tissue sur-rounding tooth 8(11).A no. 15C blade was placeddirectly into the sulcus until contact with bone oc-curred. The blade was pulled against the root sur-face and moved around the full circumference ofthe root to ensure severing of the supracrestalgingival fibers. The root was planed to the level ofthe bony crest as described by Kozlovsky et al.33
A 0.018 nickel titanium round wire was used torapidly extrude the right central incisor. Eventhough the tooth reached its final position afteronly 2 weeks, the patient returned for a fibero-tomy every week for 5 weeks to ensure that thefibers would not reattach. The brackets remained

Improving Soft Tissue Form Around Implants via Forced Eruption •
Fig 38 Orthodontic forcederuptionof tooth 8(11)after a supracrestalfiberotomy.
Fig 39 Finalpositioningof tooth 8(11) after forcederuption.
Fig 40 Radiographicviewof tooth 8(11) in its finalpositionfollowing forcederuption.
•
in place for 4 months to allow reformation of thebiologic width and for bone deposition apical tothe root (Figs 39 and 40). At this point, there wasno movement of the gingival margin.
Choosing Orthodontic Brackets
There are two main types of orthodontic tech-niques, the standard edgewise technique and thestraight-wire technique. The standard edgewiseincorporates a brace with no torque and noangulation. The clinician must introduce torque
and angulation by means of bending a stainlesssteel wire. For the general practitioner who doesnot understand angulation and torque, this can beconfusing. A more popular technique is the easier-to-use straight wire system. This involves using abrace that has a predetermined angulation andtorque. The brace itself controls the root torqueand angulation of the tooth. The torque and an-gulation are determined by a prescription, de-pending on which method is used. The mostpopular prescription is the Roth technique. Thiswas the technique used by the author.

iiiMORR
Choosing a Wire
There are round and rectangular wires. When around wire is used, only angulation can be al-tered; the torque of the brace is not expressed.The torque and angulation of the root can only becontrolled using a rectangular wire. Torque controlbecomes very important when the premaxilla isthin, and it is imperative to avoid moving the rootfacially and possibly creating a dehiscence. Mostof the time, a round wire is appropriate. The typeof wire used by the author was a round, heat-sen-sitive, superelastic nickel titanium wire. For a slow,controlled eruption aimed at bringing the boneand soft tissue down with the tooth, a 0.014- or0.016-size wire can be used. For fast eruption,one can use 0.018-size wire or a rectangular wire.
Provisional and Final Restoration
During the healing process, redoing the res-toration on tooth 9(21) was discussed with the pa-tient. The objective was to modify the papillaryform between the centrals to close the cervicalembrasure. The only way to do this was to restoreboth of the centrals and change the interproximalshape of the crowns. Redoing the maxillary leftcentral crown would make matching to the maxil-lary right central much more predictable. Oncethe bone filled in apical to the root, as verified bya periapical radiograph (see Fig 40), the provi-sional was removed along with the old crown onthe maxillary left central incisor (Fig 41). There wasvery little remaining tooth structure on the prepa-ration (Fig 41); this may be why tooth 8(11) frac-tured. Care was taken not to touch the existingpreparation. Provisionals were fabricated from awaxup of the proposed new restorations (Fig 42).Because the preparations were narrow at themargin, especially the right central incisor, a morehorizontal emergence form on the interproximalhad to be developed to mold and shape thepapilla as well as to close the cervical embrasure(Fig 43). After 2 weeks, the papillary form wasdeveloped and final impressions were taken
EQDT2005
(Fig 44). Individual porcelain-fused-to-metalcrowns were fabricated to help mask the color ofthe gold post of the maxillary right central incisor(Fig 45). The final crowns were cemented withRelyX ARC cement. A harmonious gingival bal-ance and a healthy soft tissue response wasachieved via forced eruption (Figs 45 and 46).
DISCUSSION
Soft tissue integration of a single-tooth implant isthe most difficult and the most important estheticaspect in creating an implant prosthesis that ap-pears natural. Not only is the marginal level im-portant, but the papillary form and height are criti-cal. When the soft tissue outcome followingimplant placement is not as desired, a proceduresuch as orthodontic eruption can be a tremen-dous tool in your armamentarium to assistthe ma-nipulation of the soft tissue form around an im-plant or on a tooth adjacent to an implant.Surgically rebuilding the soft tissue can be quiteunpredictable and very technique-sensitive, andno long-term data are available on the stability ofrebuilt soft tissue. With orthodontics, not only canthe marginal tissue of an adjacent tooth be coro-nally moved, but the papilla can be brought downas well. What makes this even more valuable as aprocedure is the long-term predictability of mov-ing the biologic complex 3-dimensionally to anew position rather than rebuilding one aspect ofthe biologic component (the soft tissue) withoutsupport by the other (the bone). Orthodonticsmay make it possible to save and restore teeththat previously may have been deemed hopelessbecause of lack of tooth structure, especiallyadjacent to an implant restoration. This can becritical when the soft tissue form is ideal and asoft tissue defect will be assured following extrac-tion and placement of one implant adjacent toanother.

l
Improving Soft Tissue Form Around Implants via Forced Eruption ••
•
Fig 41 Preparations after removingold crown 9(21) and temporarycrown 8(11). Note the excess softtissue on the mesial of tooth 8(11)from the orthodontic procedure.Also note the previous overprepa-ration of tooth 9(21).
Fig 42 Provisionals 8(11) and9(21)-manipulating the papillaryform to close the embrasure.
Fig 43 Cervical view of provision-als. Note the cervical contour ofthe provisional compared to themargin of the preparation. Amesial cantilever was made to ma-nipulate the soft tissue.
Fig 44 Soft tissue after manipula-tion of the soft tissue with provi-sionals.
Fig 45 Final crowns 7(12) through9(21).
Fig 46 Lateral view of final crowns7(12) through 9(21).
aDT 20051&1

iiilMORR
ACKNOWLEDGMENTS
Special thanks to Dr Isaac Garazi for his surgical work in case 1and to Dr Stephen Rimer for his surgical work in case 2. Specialthanks also to Mr Harald Heindl for the beautiful porcelain incase 1 and to Emanuele di Piazzera for the beautiful porcelainin case 2.
REFERENCES
1. Abrams H, Kopczyk RA, Kaplan AL. Incidence of anteriorridge deformities in partially edentulous patients. J Pros-thet Dent 1987;57:191-194.
2. Abrams L.Augmentation of the deformed residual eden-tulous ridge for fixed prosthesis. Com pend Contin EducDent 1980;1 :205-213.
3. Tarnow DP, Eskow RN. Considerations for single-unit es-thetic implant restorations. Com pend Contin Educ Dent1995;16:778-788.
4. Jansen CE, Weisgold A. Presurgical treatment planningfor the anterior single-tooth implant restoration. Com-pend Con tin Educ Dent 1995;16:746-761.
5. Weisgold AS, Amoux JP, Lu J. Single-tooth anterior im-plant: A word of caution. Part I. J Esthet Dent 1997;9:225-233.
6. Garber DA. The esthetic dental implant: Letting restora-tion be the guide. J Am Dent Assoc 1995;126:319-325.
7. Garguilo AW,Wentz FM, Orban B. Dimensions and rela-tions of the dentogingival junction in humans. J Periodon-toI1961;32:261-267.
8. Kois Jc. Altering gingival levels: The restorative connec-tion. Part I: Biologic variables. J Esthet Dent 1994;6:3-9.
9. Tarnow DP, Magner AW, Fletcher P.The effect of the dis-tance from the contact point to the crest of bone on thepresence or absence of the interproximal dental papilla.J Periodontol 1992;63:995-996.
10. Salama H, Salama MA, Garber D, Adar P.The interproxi-mal height of bone: A guidepost to predictable aestheticstrategies and soft tissue contours in anterior tooth re-placement. Pract Periodont Aesthet Dent 1998; 10:1131-1141.
11. Jemt 1. Regeneration of gingival papillae after single-implant treatment. Int J Periodontics Restorative Dent1997;17:326-333.
12. Azzi R, Etienne D, Takei H, Fenech P.Surgical thickeningof the existing gingiva and reconstruction of interdentalpapillae around implant-supported restorations. Int JPeriodontics Restorative Dent 2002;22:71-77.
13. Ingber JS. Forced eruption: Part I. A method of treatingone and two wall infrabony osseous defects-Rationaleand case report. J PeriodontoI1974;45:199-206.
14. Ingber JS. Forced eruption: Part II.A method of treatingnonrestorable teeth-Periodontal and restorative consid-erations. J Periodontol 1976;47:203-216.
15. Ingber JS. Forced eruption: Alteration of soft tissuedeformities. lnt J Periodontics Restorative Dent 1989;9:416-425.
: ODT 2005
16. Potash nick SR, Rosenberg ES. Forced eruption: Principlesin periodontics and restorative dentistry. J Prosthet Dent1982;48:141-148.
17. Van Venrooy JR, Yukna RA.Orthodontic extrusion of sin-gle-rooted teeth affected with advanced periodontal dis-ease. Am J Orthod 1985;87:67-74.
18. Brown IS. The effect of orthodontic therapy on certaintypes of periodontal defects. I. Clinical findings. J Peri-odontol 1973;44:742-745.
19. Levine RA. Forced eruption, part 1: Periodontal andorthodontic considerations for treatment of an isolatedperiodontal angular infrabony defect. Compendium1988;9:10-19.
20. Reitan K.Tissue behavior during orthodontic tooth move-ment. Am J Orthod 1960;46:881-900.
21. Reitan K. Clinical and histologic observations on toothmovement during and after orthodontic movement. Am JOrthod 1967;53:721-745.
22. Stern N, Becker A. Forced eruption: Biological and clinicalconsiderations. J Oral Rehabil 1980;7:395-402.
23. Berglundh T, Lindhe J, Ericsson I, Marinello CP, LiljenbergB, Thomsen P.The soft tissue barrier at implants andteeth. Clin Oral Implants Res 1991 ;2:81-90.
24. Wise RJ, Kramer GM. Predetermination of osseouschanges associated with uprighting tipped molars byprobing. Int J Periodontics Restorative Dent 1983;3:68-81.
25. Mantzikos T, Shamus I. Case report: Forced eruption andimplant site development. Angle Orthod 1998:68(2):179-186.
26. Libman WJ, Nicholls JI. Load fatigue of teeth restoredwith cast posts and cores and complete crowns. Int JProsthodont 1995;8:155-161.
27. Kois Jc. Esthetic extraction site development: The bio-logic variables. Contemp Esthet Restorative Pract1998;2:10-18.
28. Sadoun A, LeGall M, Touati B. Selection and ideal tridi-mensional implant position for soft tissue aesthetics. PractPeriodontics Aesthet Dent 1999;11:1063-1072.
29. Tarnow DP,Cho SC, Wallace SS. The effect of inter-im-plant distance on the height of inter-implant bone crest.J Periodontol 2000;71 :546-549.
30. Elian N, Jalbout ZN, Cho S, Froum S, Tarnow DP. Realitiesand limitations in the management of the interdentalpapilla between implants: Three case reports. PractProced Aesthet Dent 2003;15:737-744.
31. Tarnow D, Elian N, Fletcher P, et al. Vertical distance fromthe crest of bone to the height of the interproximalpapilla between adjacent implants. J Periodontol2003;7 4: 1785-1788.
32. Kois JC, Kan JY. Predictable peri-implant gingival aesthet-ics: Surgical and prosthodontic rationales. Pract ProcedAesthet Dent 2001 ;13:691-698.
33. Kozlovsky A, Tal H, Lieberman M. Forced eruption com-bined with gingival fiberotomy. A technique for clinicalcrown lengthening. J Clin Periodontol 1988; 15:534-538.
34. Pontoriero R, Celenza F Jr, Ricci G, Carnevale G. Rapidextrusion with fiber resection: A combined orthodontic-periodontic treatment modality. Int J PeriodonticsRestorative Dent 1987;7(5):30-43.
(i)




















