
Improved survival in patients with ventricular assist device therapy: the University of Wisconsin...
8
Improved survival in patients with ventricular assist device therapy: the University of Wisconsin experience Satoru Osaki a, * , Niloo M. Edwards a , Mauricio Velez b , Maryl R. Johnson b , Margaret A. Murray a , Jennifer A. Hoffmann b , Takushi Kohmoto a a Cardiothoracic Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States b Heart Failure and Transplant Cardiology, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States Received 5 October 2007; received in revised form 17 April 2008; accepted 21 April 2008; Available online 2 June 2008 Abstract Objective: Ventricular assist devices (VADs) have been implanted since 1990 in our institution, becoming an increasingly common treatment for end-stage heart failure. Beginning in 1997, VAD patients were discharged home when feasible. In August 2003, a dedicated multidisciplinary VAD team (cardiac surgeons, cardiologists, VAD coordinators, nurses, rehabilitation specialists, nutrition experts, psychologists, pharmacists, social workers, and administrators) was created to optimize the management of VAD patients. The purpose of this study is to analyze the impact of these changes in care at our center over the last 17 years. Methods: We retrospectively studied 107 consecutive VAD recipients between June 1990 and August 2006. VADs were implanted as bridge to recovery, bridge to transplant and destination therapy. The cohort was divided by care plans into early (n = 37, June 1990—1996), mid (n = 32, 1997—July 2003), and late groups (n = 38, August 2003—August 2006). Demographic profile, survival and complications were assessed. Results: Patient demographics tended to show an increased severity of illness over time. Post-VAD survival rate significantly improved in the late group (post-VAD 1- and 3-year survival rates; early: 54.1% and 40.5%; mid: 51.6% and 41.9%; late: 86.8% and 82.5%, p < 0.001, respectively). The incidence of complications including re-operation, major bleeding and major infection, significantly decreased in the late group ( p < 0.05). Conclusions: Outcomes have improved dramatically in recent VAD patients, despite an increasingly high- risk patient population. These data suggest that advances in device technology and medical therapies, as well as a multidisciplinary approach, have improved survival on VAD therapy. # 2008 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved. Keywords: Mechanical circulatory support; Ventricular assist device; Congestive heart failure 1. Introduction Mechanical circulatory support has become an important therapeutic option for patients with end-stage heart failure refractory to medical and other surgical therapies [1,2]. Over the last 20 years, significant clinical and engineering advances have been achieved in the field of mechanical circulatory support, which led to the first successful cardiac transplant, following bridging with a left ventricular assist device (LVAD), reported in 1984 [3]. In 1994, the United States Food and Drug Administration approved LVADs as a bridge to cardiac transplantation and the first wearable LVADs were used clinically in the same year [4]. Due to technological advances and the increasing need to treat different types of patients, indications for VAD implantation have been broadened to include patients who were once thought to be unsuitable for device insertion. Recently, the REMATCH trial has shown that LVAD therapy for selected patients, who are not candidates for cardiac transplantation, is superior to medical therapy in alleviating symptoms and improving survival rates and quality of life [5]. The care of patients with refractory heart failure who are VAD candidates is also changing as technology advances [6]. Implantable VAD therapy started at our institution in 1990, and has become increasingly common for the treatment of severe decompensated heart failure. Since 1997, our institution allowed VAD patients to be discharged home. In August 2003, a dedicated multidisciplinary VAD team including cardiac surgeons, cardiologists, VAD coordinators, nurses, rehabilitation specialists, nutrition experts, psychol- ogists, pharmacists, social workers, and administrators, was created to optimize the management of VAD patients. The purpose of this study is to evaluate the changing demographic profile of VAD recipients and to analyze the impact of changes in the care approach at our center on survival and VAD- related complications over the last 17 years. www.elsevier.com/locate/ejcts European Journal of Cardio-thoracic Surgery 34 (2008) 281—288 * Corresponding author. Address: Department of Surgery, Division of Cardi- ovascular Surgery, University of Wisconsin School of Medicine and Public Health, H4/337 Clinical Science Center 600 Highland Avenue, Madison, WI 53792-3236, United States. Tel.: +1 608 263 4071; fax: +1 608 263 0547. E-mail address: [email protected] (S. Osaki). 1010-7940/$ — see front matter. # 2008 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejcts.2008.04.023
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Improved survival in patients with ventricular assist device therapy: the University of Wisconsin...

Improved survival in patients with ventricular assist device therapy:the University of Wisconsin experience
Satoru Osaki a,*, Niloo M. Edwards a, Mauricio Velez b, Maryl R. Johnson b,Margaret A. Murray a, Jennifer A. Hoffmann b, Takushi Kohmoto a
aCardiothoracic Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, United StatesbHeart Failure and Transplant Cardiology, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States
Received 5 October 2007; received in revised form 17 April 2008; accepted 21 April 2008; Available online 2 June 2008
Abstract
Objective: Ventricular assist devices (VADs) have been implanted since 1990 in our institution, becoming an increasingly common treatment forend-stage heart failure. Beginning in 1997, VAD patients were discharged home when feasible. In August 2003, a dedicated multidisciplinary VADteam (cardiac surgeons, cardiologists, VAD coordinators, nurses, rehabilitation specialists, nutrition experts, psychologists, pharmacists, socialworkers, and administrators) was created to optimize themanagement of VAD patients. The purpose of this study is to analyze the impact of thesechanges in care at our center over the last 17 years.Methods: We retrospectively studied 107 consecutive VAD recipients between June 1990 andAugust 2006. VADs were implanted as bridge to recovery, bridge to transplant and destination therapy. The cohort was divided by care plans intoearly (n = 37, June 1990—1996), mid (n = 32, 1997—July 2003), and late groups (n = 38, August 2003—August 2006). Demographic profile, survivaland complications were assessed. Results: Patient demographics tended to show an increased severity of illness over time. Post-VAD survival ratesignificantly improved in the late group (post-VAD 1- and 3-year survival rates; early: 54.1% and 40.5%; mid: 51.6% and 41.9%; late: 86.8% and82.5%, p < 0.001, respectively). The incidence of complications including re-operation, major bleeding and major infection, significantlydecreased in the late group ( p < 0.05). Conclusions: Outcomes have improved dramatically in recent VAD patients, despite an increasingly high-risk patient population. These data suggest that advances in device technology and medical therapies, as well as a multidisciplinary approach,have improved survival on VAD therapy.# 2008 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved.
Keywords: Mechanical circulatory support; Ventricular assist device; Congestive heart failure
www.elsevier.com/locate/ejctsEuropean Journal of Cardio-thoracic Surgery 34 (2008) 281—288
1. Introduction
Mechanical circulatory support has become an importanttherapeutic option for patients with end-stage heart failurerefractory to medical and other surgical therapies [1,2]. Overthe last 20 years, significant clinical and engineeringadvances have been achieved in the field of mechanicalcirculatory support, which led to the first successful cardiactransplant, following bridging with a left ventricular assistdevice (LVAD), reported in 1984 [3]. In 1994, the UnitedStates Food and Drug Administration approved LVADs as abridge to cardiac transplantation and the first wearable LVADswere used clinically in the same year [4]. Due totechnological advances and the increasing need to treatdifferent types of patients, indications for VAD implantation
* Corresponding author. Address: Department of Surgery, Division of Cardi-ovascular Surgery, University of Wisconsin School of Medicine and PublicHealth, H4/337 Clinical Science Center 600 Highland Avenue, Madison, WI53792-3236, United States. Tel.: +1 608 263 4071; fax: +1 608 263 0547.
E-mail address: [email protected] (S. Osaki).
1010-7940/$ — see front matter. # 2008 European Association for Cardio-Thoracicdoi:10.1016/j.ejcts.2008.04.023
have been broadened to include patients who were oncethought to be unsuitable for device insertion. Recently, theREMATCH trial has shown that LVAD therapy for selectedpatients, who are not candidates for cardiac transplantation,is superior to medical therapy in alleviating symptoms andimproving survival rates and quality of life [5].
The care of patients with refractory heart failure who areVAD candidates is also changing as technology advances [6].Implantable VAD therapy started at our institution in 1990,and has become increasingly common for the treatment ofsevere decompensated heart failure. Since 1997, ourinstitution allowed VAD patients to be discharged home. InAugust 2003, a dedicated multidisciplinary VAD teamincluding cardiac surgeons, cardiologists, VAD coordinators,nurses, rehabilitation specialists, nutrition experts, psychol-ogists, pharmacists, social workers, and administrators, wascreated to optimize the management of VAD patients. Thepurpose of this study is to evaluate the changing demographicprofile of VAD recipients and to analyze the impact of changesin the care approach at our center on survival and VAD-related complications over the last 17 years.
Surgery. Published by Elsevier B.V. All rights reserved.

S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288282
2. Materials and methods
Between June 1990 and August 2006, 107 patientsreceived a VAD as bridge to recovery (BTR), bridge totransplant (BTT) and destination therapy (DT) at ourinstitution (Table 1). The patients were divided, accordingto the changes in our institutional VAD program, into early(n = 37, 1990—1996), mid (n = 32, 1997—July 2003), and lategroups (n = 38, August 2003—August 2006), respectively. Datawas collected prospectively and analyzed retrospectively.The institutional review board committee approved thisretrospective study.
Preoperative patient demographics, cardiac function,hemodynamics, serum laboratory values, intra-aortic bal-loon pump (IABP) insertion, ventilatory dependence, andneed for continuous veno-venous hemodialysis (CVVH) orintermittent hemodialysis (HD) were recorded for eachpatient. In addition, in order to evaluate relative pre-operative risk factors, we used the existing VAD scoringsystem published by Rao et al. [7]. This scoring system isderived from five clinical variables, including ventilatorydependence, postcardiotomy shock, previous LVAD, centralvenous pressure >16 mmHg, and prothrombin time >16 s.The survival during VAD support was assessed and patientswere censored at the time of transplant or device explant.Also, post-VAD survival rate was calculated includingtransplant and device explant due to recovery. Clinicaloutcomes included survival to hospital discharge and lengthof hospital stay. Postoperative complications included re-operation within 7 days from VAD insertion, major bleeding,
Table 1Intention to treat, device selection, support length and type
Early
Intention to treatBridge to transplant 35 (95%)Bridge to recovery 2 (5%)Destination therapy —
DevicesHeartMateW IP 24 (65%)HeartMateW VE 2 (5%)HeartMateW XVE —HeartMateW II —ThoratecW 9 (25%)ThoratecW IVAD —DeBakeyW —AbiomedW BVS 5000 —Medtronic Bio-MedicusW 2 (5%)
Device support length (days) (range) 45 (0—331)Bridge to transplant 52 (0—331)Bridge to recovery 1 (1)Destination therapy —
Device assist typeBiVAD 7 (19%)LVAD 30 (81%)RVAD 0 (0%)
HeartMateW and ThoratecW, Thoratec Corp, Pleasanton, Calif, USA; DeBakeyW, MicDanvers, Mass, USA; Medtronic Bio-MedicusW, Medtronic Bio-Medicus, Inc., Eden Praidevice; RVAD, right ventricular assist device. HeartMateW IP, implantable and pneumelectric pulsatile; HeartMateW II, implantable and nonpulsatile; ThoratecW, paracoDeBakeyW, implantable and nonpulsatile; AbiomedW BVS 5000, extracorporeal andnonpulsatile.
a Including three replacements.
major infection, neurological and renal dysfunction,respiratory failure, right heart failure (RHF), and devicemalfunction. These definitions, except for re-operation,were based on the Interagency Registry for MechanicallyAssisted Circulatory Support (INTERMACS) (http://www.uab.edu/ctsresearch/intermacs/manuals.htm).
2.1. Patient selection
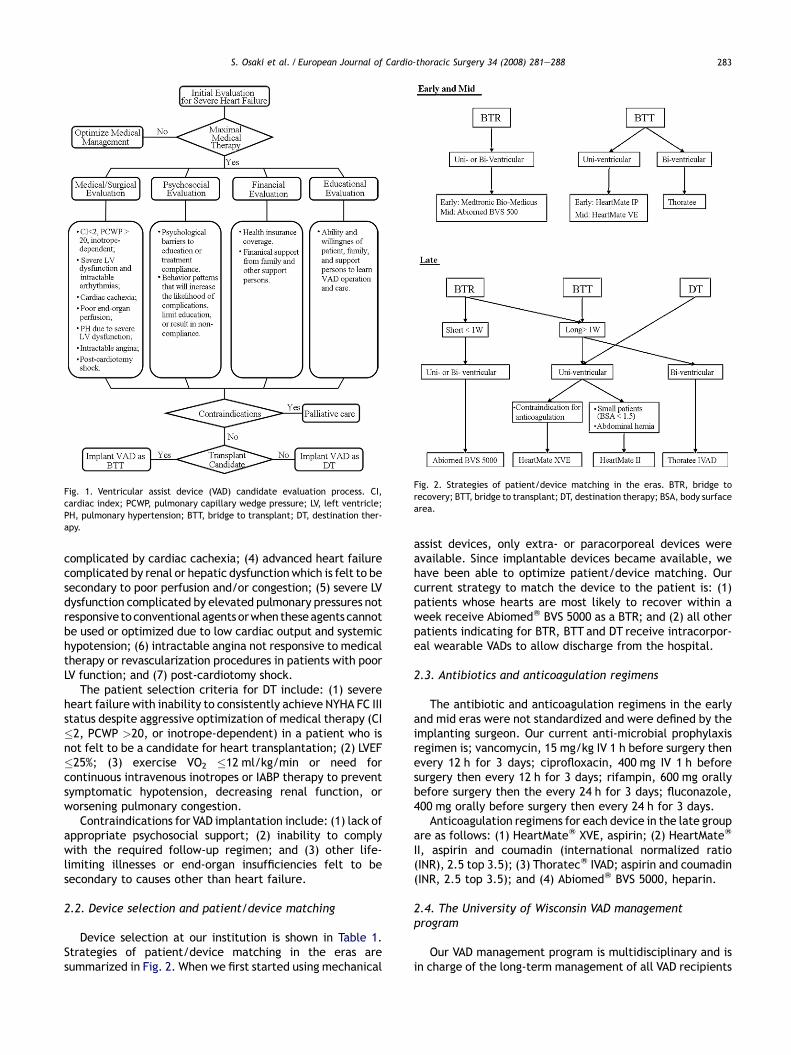
Patient selection criteria have varied slightly over time,reflecting general implantation practices in the United Statesduring each era [2,5,8]. Prior to the availability of evidence-based implantation criteria, patient selection was based onexpert opinion. The patient selection criteria in the early andmid groups generally included patients with severe heartfailure despite IABP or inotrope support, with unstablehemodynamics, and with early signs of end-organ dysfunc-tion. Fig. 1 shows a typical patient selection process. Clinicaljudgment is applied to each individual case to evaluatecandidacy for VAD implantation. However, patient selectioncriteria are followed as a guide for decision-making.
The selection criteria in the late group for a BTT intentincludes patients listed/deemed candidates for hearttransplantation, and having one or more of the following:(1) severe heart failure despite optimal medical therapy(cardiac index (CI) �2, pulmonary capillary wedge pressure(PCWP) >20, or inotrope-dependent), especially if thepatient’s body size and blood type suggest that the waitfor a donor organ will be prolonged; (2) severe LV dysfunctionand intractable arrhythmias; (3) advanced heart failure
Mid Latea p-Value
27 (84%) 28 (74%)5 (16%) 3 (8%)— 7 (18%)
9 (28%) —6 (19%) —3 (9%) 31 (75%)— 2 (5%)10 (31%) 4 (10%)— 2 (5%)— 2 (5%)4 (13%) —— —
90 (0—524) 167 (34—860) <0.001129 (0—524) 163 (34—503)
3 (0—14) 123 (81—185)— 451 (253—860)
0.0248 (25%) 3 (7%)
20 (63%) 34 (91%)4 (12%) 1 (2%)
roMed Technology, Inc., Houston, Tex, USA; AbiomedW BVS 5000, Abiomed,rie, Minn, USA; BiVAD, biventricular assist device; LVAD, left ventricular assistatic pulsatile; HeartMateW VE and HeartMateW XVE, implantable and vented
rporeal and pneumatic pulsatile; ThoratecW IVAD, implantable and pulsatile;pneumatic pulsatile; Medtronic Bio-MedicusW, extracorporeal and centrifugal
S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288 283
Fig. 1. Ventricular assist device (VAD) candidate evaluation process. CI,cardiac index; PCWP, pulmonary capillary wedge pressure; LV, left ventricle;PH, pulmonary hypertension; BTT, bridge to transplant; DT, destination ther-apy.
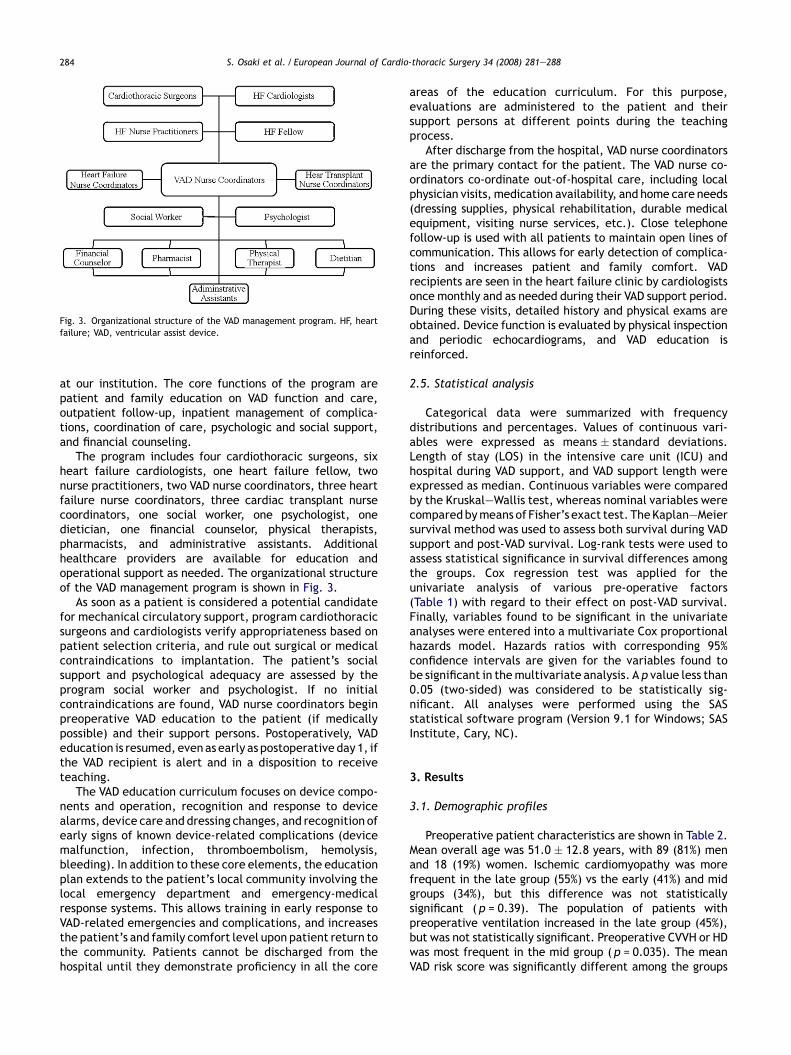
Fig. 2. Strategies of patient/device matching in the eras. BTR, bridge torecovery; BTT, bridge to transplant; DT, destination therapy; BSA, body surfacearea.
complicated by cardiac cachexia; (4) advanced heart failurecomplicated by renal or hepatic dysfunctionwhich is felt to besecondary to poor perfusion and/or congestion; (5) severe LVdysfunction complicated by elevated pulmonary pressures notresponsive toconventional agents orwhen theseagents cannotbe used or optimized due to low cardiac output and systemichypotension; (6) intractable angina not responsive to medicaltherapy or revascularization procedures in patients with poorLV function; and (7) post-cardiotomy shock.
The patient selection criteria for DT include: (1) severeheart failure with inability to consistently achieve NYHA FC IIIstatus despite aggressive optimization of medical therapy (CI�2, PCWP >20, or inotrope-dependent) in a patient who isnot felt to be a candidate for heart transplantation; (2) LVEF�25%; (3) exercise VO2 �12 ml/kg/min or need forcontinuous intravenous inotropes or IABP therapy to preventsymptomatic hypotension, decreasing renal function, orworsening pulmonary congestion.
Contraindications for VAD implantation include: (1) lack ofappropriate psychosocial support; (2) inability to complywith the required follow-up regimen; and (3) other life-limiting illnesses or end-organ insufficiencies felt to besecondary to causes other than heart failure.
2.2. Device selection and patient/device matching
Device selection at our institution is shown in Table 1.Strategies of patient/device matching in the eras aresummarized in Fig. 2. When we first started using mechanical
assist devices, only extra- or paracorporeal devices wereavailable. Since implantable devices became available, wehave been able to optimize patient/device matching. Ourcurrent strategy to match the device to the patient is: (1)patients whose hearts are most likely to recover within aweek receive AbiomedW BVS 5000 as a BTR; and (2) all otherpatients indicating for BTR, BTT and DT receive intracorpor-eal wearable VADs to allow discharge from the hospital.
2.3. Antibiotics and anticoagulation regimens
The antibiotic and anticoagulation regimens in the earlyand mid eras were not standardized and were defined by theimplanting surgeon. Our current anti-microbial prophylaxisregimen is; vancomycin, 15 mg/kg IV 1 h before surgery thenevery 12 h for 3 days; ciprofloxacin, 400 mg IV 1 h beforesurgery then every 12 h for 3 days; rifampin, 600 mg orallybefore surgery then the every 24 h for 3 days; fluconazole,400 mg orally before surgery then every 24 h for 3 days.
Anticoagulation regimens for each device in the late groupare as follows: (1) HeartMateW XVE, aspirin; (2) HeartMateW
II, aspirin and coumadin (international normalized ratio(INR), 2.5 top 3.5); (3) ThoratecW IVAD; aspirin and coumadin(INR, 2.5 top 3.5); and (4) AbiomedW BVS 5000, heparin.
2.4. The University of Wisconsin VAD managementprogram
Our VAD management program is multidisciplinary and isin charge of the long-term management of all VAD recipients
S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288284
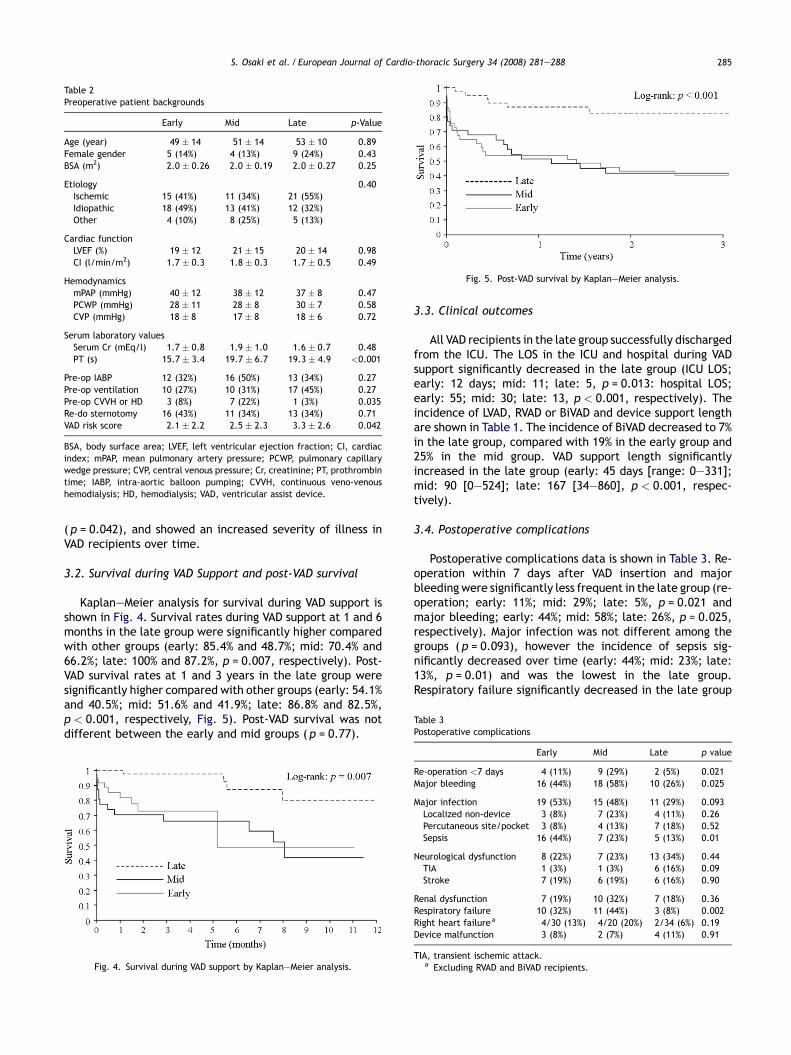
Fig. 3. Organizational structure of the VAD management program. HF, heartfailure; VAD, ventricular assist device.
at our institution. The core functions of the program arepatient and family education on VAD function and care,outpatient follow-up, inpatient management of complica-tions, coordination of care, psychologic and social support,and financial counseling.
The program includes four cardiothoracic surgeons, sixheart failure cardiologists, one heart failure fellow, twonurse practitioners, two VAD nurse coordinators, three heartfailure nurse coordinators, three cardiac transplant nursecoordinators, one social worker, one psychologist, onedietician, one financial counselor, physical therapists,pharmacists, and administrative assistants. Additionalhealthcare providers are available for education andoperational support as needed. The organizational structureof the VAD management program is shown in Fig. 3.
As soon as a patient is considered a potential candidatefor mechanical circulatory support, program cardiothoracicsurgeons and cardiologists verify appropriateness based onpatient selection criteria, and rule out surgical or medicalcontraindications to implantation. The patient’s socialsupport and psychological adequacy are assessed by theprogram social worker and psychologist. If no initialcontraindications are found, VAD nurse coordinators beginpreoperative VAD education to the patient (if medicallypossible) and their support persons. Postoperatively, VADeducation is resumed, even as early as postoperative day 1, ifthe VAD recipient is alert and in a disposition to receiveteaching.
The VAD education curriculum focuses on device compo-nents and operation, recognition and response to devicealarms, device care and dressing changes, and recognition ofearly signs of known device-related complications (devicemalfunction, infection, thromboembolism, hemolysis,bleeding). In addition to these core elements, the educationplan extends to the patient’s local community involving thelocal emergency department and emergency-medicalresponse systems. This allows training in early response toVAD-related emergencies and complications, and increasesthe patient’s and family comfort level upon patient return tothe community. Patients cannot be discharged from thehospital until they demonstrate proficiency in all the core
areas of the education curriculum. For this purpose,evaluations are administered to the patient and theirsupport persons at different points during the teachingprocess.
After discharge from the hospital, VAD nurse coordinatorsare the primary contact for the patient. The VAD nurse co-ordinators co-ordinate out-of-hospital care, including localphysician visits, medication availability, and home care needs(dressing supplies, physical rehabilitation, durable medicalequipment, visiting nurse services, etc.). Close telephonefollow-up is used with all patients to maintain open lines ofcommunication. This allows for early detection of complica-tions and increases patient and family comfort. VADrecipients are seen in the heart failure clinic by cardiologistsonce monthly and as needed during their VAD support period.During these visits, detailed history and physical exams areobtained. Device function is evaluated by physical inspectionand periodic echocardiograms, and VAD education isreinforced.
2.5. Statistical analysis
Categorical data were summarized with frequencydistributions and percentages. Values of continuous vari-ables were expressed as means � standard deviations.Length of stay (LOS) in the intensive care unit (ICU) andhospital during VAD support, and VAD support length wereexpressed as median. Continuous variables were comparedby the Kruskal—Wallis test, whereas nominal variables werecomparedbymeans of Fisher’s exact test. TheKaplan—Meiersurvival method was used to assess both survival during VADsupport and post-VAD survival. Log-rank tests were used toassess statistical significance in survival differences amongthe groups. Cox regression test was applied for theunivariate analysis of various pre-operative factors(Table 1) with regard to their effect on post-VAD survival.Finally, variables found to be significant in the univariateanalyses were entered into a multivariate Cox proportionalhazards model. Hazards ratios with corresponding 95%confidence intervals are given for the variables found tobe significant in themultivariate analysis. A p value less than0.05 (two-sided) was considered to be statistically sig-nificant. All analyses were performed using the SASstatistical software program (Version 9.1 for Windows; SASInstitute, Cary, NC).
3. Results
3.1. Demographic profiles
Preoperative patient characteristics are shown in Table 2.Mean overall age was 51.0 � 12.8 years, with 89 (81%) menand 18 (19%) women. Ischemic cardiomyopathy was morefrequent in the late group (55%) vs the early (41%) and midgroups (34%), but this difference was not statisticallysignificant ( p = 0.39). The population of patients withpreoperative ventilation increased in the late group (45%),but was not statistically significant. Preoperative CVVH or HDwas most frequent in the mid group ( p = 0.035). The meanVAD risk score was significantly different among the groups
S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288 285
Table 2Preoperative patient backgrounds
Early Mid Late p-Value
Age (year) 49 � 14 51 � 14 53 � 10 0.89Female gender 5 (14%) 4 (13%) 9 (24%) 0.43BSA (m2) 2.0 � 0.26 2.0 � 0.19 2.0 � 0.27 0.25
Etiology 0.40Ischemic 15 (41%) 11 (34%) 21 (55%)Idiopathic 18 (49%) 13 (41%) 12 (32%)Other 4 (10%) 8 (25%) 5 (13%)
Cardiac functionLVEF (%) 19 � 12 21 � 15 20 � 14 0.98CI (l/min/m2) 1.7 � 0.3 1.8 � 0.3 1.7 � 0.5 0.49
HemodynamicsmPAP (mmHg) 40 � 12 38 � 12 37 � 8 0.47PCWP (mmHg) 28 � 11 28 � 8 30 � 7 0.58CVP (mmHg) 18 � 8 17 � 8 18 � 6 0.72
Serum laboratory valuesSerum Cr (mEq/l) 1.7 � 0.8 1.9 � 1.0 1.6 � 0.7 0.48PT (s) 15.7 � 3.4 19.7 � 6.7 19.3 � 4.9 <0.001
Pre-op IABP 12 (32%) 16 (50%) 13 (34%) 0.27Pre-op ventilation 10 (27%) 10 (31%) 17 (45%) 0.27Pre-op CVVH or HD 3 (8%) 7 (22%) 1 (3%) 0.035Re-do sternotomy 16 (43%) 11 (34%) 13 (34%) 0.71VAD risk score 2.1 � 2.2 2.5 � 2.3 3.3 � 2.6 0.042
BSA, body surface area; LVEF, left ventricular ejection fraction; CI, cardiacindex; mPAP, mean pulmonary artery pressure; PCWP, pulmonary capillarywedge pressure; CVP, central venous pressure; Cr, creatinine; PT, prothrombintime; IABP, intra-aortic balloon pumping; CVVH, continuous veno-venoushemodialysis; HD, hemodialysis; VAD, ventricular assist device.
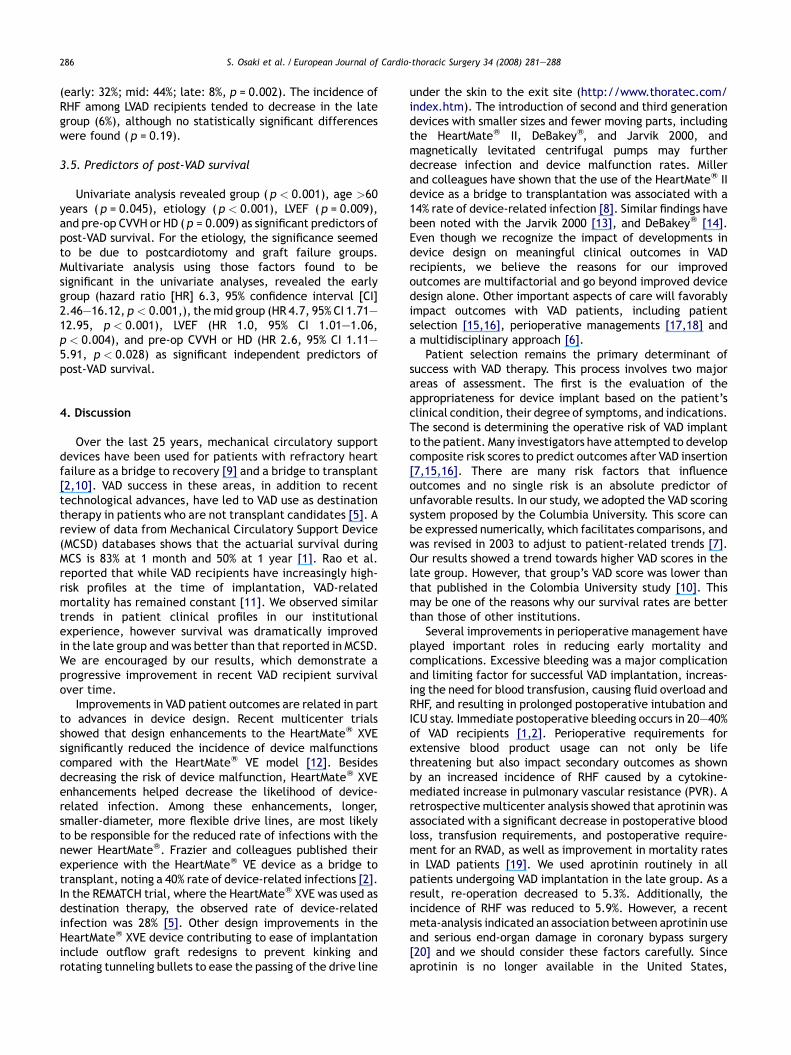
Fig. 5. Post-VAD survival by Kaplan—Meier analysis.
Table 3Postoperative complications
( p = 0.042), and showed an increased severity of illness inVAD recipients over time.
3.2. Survival during VAD Support and post-VAD survival
Kaplan—Meier analysis for survival during VAD support isshown in Fig. 4. Survival rates during VAD support at 1 and 6months in the late group were significantly higher comparedwith other groups (early: 85.4% and 48.7%; mid: 70.4% and66.2%; late: 100% and 87.2%, p = 0.007, respectively). Post-VAD survival rates at 1 and 3 years in the late group weresignificantly higher compared with other groups (early: 54.1%and 40.5%; mid: 51.6% and 41.9%; late: 86.8% and 82.5%,p < 0.001, respectively, Fig. 5). Post-VAD survival was notdifferent between the early and mid groups ( p = 0.77).
Fig. 4. Survival during VAD support by Kaplan—Meier analysis.
3.3. Clinical outcomes
All VAD recipients in the late group successfully dischargedfrom the ICU. The LOS in the ICU and hospital during VADsupport significantly decreased in the late group (ICU LOS;early: 12 days; mid: 11; late: 5, p = 0.013: hospital LOS;early: 55; mid: 30; late: 13, p < 0.001, respectively). Theincidence of LVAD, RVAD or BiVAD and device support lengthare shown in Table 1. The incidence of BiVAD decreased to 7%in the late group, compared with 19% in the early group and25% in the mid group. VAD support length significantlyincreased in the late group (early: 45 days [range: 0—331];mid: 90 [0—524]; late: 167 [34—860], p < 0.001, respec-tively).
3.4. Postoperative complications
Postoperative complications data is shown in Table 3. Re-operation within 7 days after VAD insertion and majorbleeding were significantly less frequent in the late group (re-operation; early: 11%; mid: 29%; late: 5%, p = 0.021 andmajor bleeding; early: 44%; mid: 58%; late: 26%, p = 0.025,respectively). Major infection was not different among thegroups ( p = 0.093), however the incidence of sepsis sig-nificantly decreased over time (early: 44%; mid: 23%; late:13%, p = 0.01) and was the lowest in the late group.Respiratory failure significantly decreased in the late group
Early Mid Late p value
Re-operation <7 days 4 (11%) 9 (29%) 2 (5%) 0.021Major bleeding 16 (44%) 18 (58%) 10 (26%) 0.025
Major infection 19 (53%) 15 (48%) 11 (29%) 0.093Localized non-device 3 (8%) 7 (23%) 4 (11%) 0.26Percutaneous site/pocket 3 (8%) 4 (13%) 7 (18%) 0.52Sepsis 16 (44%) 7 (23%) 5 (13%) 0.01
Neurological dysfunction 8 (22%) 7 (23%) 13 (34%) 0.44TIA 1 (3%) 1 (3%) 6 (16%) 0.09Stroke 7 (19%) 6 (19%) 6 (16%) 0.90
Renal dysfunction 7 (19%) 10 (32%) 7 (18%) 0.36Respiratory failure 10 (32%) 11 (44%) 3 (8%) 0.002Right heart failurea 4/30 (13%) 4/20 (20%) 2/34 (6%) 0.19Device malfunction 3 (8%) 2 (7%) 4 (11%) 0.91
TIA, transient ischemic attack.a Excluding RVAD and BiVAD recipients.
S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288286
(early: 32%; mid: 44%; late: 8%, p = 0.002). The incidence ofRHF among LVAD recipients tended to decrease in the lategroup (6%), although no statistically significant differenceswere found ( p = 0.19).
3.5. Predictors of post-VAD survival
Univariate analysis revealed group ( p < 0.001), age >60years ( p = 0.045), etiology ( p < 0.001), LVEF ( p = 0.009),and pre-op CVVH or HD ( p = 0.009) as significant predictors ofpost-VAD survival. For the etiology, the significance seemedto be due to postcardiotomy and graft failure groups.Multivariate analysis using those factors found to besignificant in the univariate analyses, revealed the earlygroup (hazard ratio [HR] 6.3, 95% confidence interval [CI]2.46—16.12, p < 0.001,), themid group (HR 4.7, 95% CI 1.71—12.95, p < 0.001), LVEF (HR 1.0, 95% CI 1.01—1.06,p < 0.004), and pre-op CVVH or HD (HR 2.6, 95% CI 1.11—5.91, p < 0.028) as significant independent predictors ofpost-VAD survival.
4. Discussion
Over the last 25 years, mechanical circulatory supportdevices have been used for patients with refractory heartfailure as a bridge to recovery [9] and a bridge to transplant[2,10]. VAD success in these areas, in addition to recenttechnological advances, have led to VAD use as destinationtherapy in patients who are not transplant candidates [5]. Areview of data from Mechanical Circulatory Support Device(MCSD) databases shows that the actuarial survival duringMCS is 83% at 1 month and 50% at 1 year [1]. Rao et al.reported that while VAD recipients have increasingly high-risk profiles at the time of implantation, VAD-relatedmortality has remained constant [11]. We observed similartrends in patient clinical profiles in our institutionalexperience, however survival was dramatically improvedin the late group and was better than that reported in MCSD.We are encouraged by our results, which demonstrate aprogressive improvement in recent VAD recipient survivalover time.
Improvements in VAD patient outcomes are related in partto advances in device design. Recent multicenter trialsshowed that design enhancements to the HeartMateW XVEsignificantly reduced the incidence of device malfunctionscompared with the HeartMateW VE model [12]. Besidesdecreasing the risk of device malfunction, HeartMateW XVEenhancements helped decrease the likelihood of device-related infection. Among these enhancements, longer,smaller-diameter, more flexible drive lines, are most likelyto be responsible for the reduced rate of infections with thenewer HeartMateW. Frazier and colleagues published theirexperience with the HeartMateW VE device as a bridge totransplant, noting a 40% rate of device-related infections [2].In the REMATCH trial, where the HeartMateW XVE was used asdestination therapy, the observed rate of device-relatedinfection was 28% [5]. Other design improvements in theHeartMateW XVE device contributing to ease of implantationinclude outflow graft redesigns to prevent kinking androtating tunneling bullets to ease the passing of the drive line
under the skin to the exit site (http://www.thoratec.com/index.htm). The introduction of second and third generationdevices with smaller sizes and fewer moving parts, includingthe HeartMateW II, DeBakeyW, and Jarvik 2000, andmagnetically levitated centrifugal pumps may furtherdecrease infection and device malfunction rates. Millerand colleagues have shown that the use of the HeartMateW IIdevice as a bridge to transplantation was associated with a14% rate of device-related infection [8]. Similar findings havebeen noted with the Jarvik 2000 [13], and DeBakeyW [14].Even though we recognize the impact of developments indevice design on meaningful clinical outcomes in VADrecipients, we believe the reasons for our improvedoutcomes are multifactorial and go beyond improved devicedesign alone. Other important aspects of care will favorablyimpact outcomes with VAD patients, including patientselection [15,16], perioperative managements [17,18] anda multidisciplinary approach [6].
Patient selection remains the primary determinant ofsuccess with VAD therapy. This process involves two majorareas of assessment. The first is the evaluation of theappropriateness for device implant based on the patient’sclinical condition, their degree of symptoms, and indications.The second is determining the operative risk of VAD implantto the patient. Many investigators have attempted to developcomposite risk scores to predict outcomes after VAD insertion[7,15,16]. There are many risk factors that influenceoutcomes and no single risk is an absolute predictor ofunfavorable results. In our study, we adopted the VAD scoringsystem proposed by the Columbia University. This score canbe expressed numerically, which facilitates comparisons, andwas revised in 2003 to adjust to patient-related trends [7].Our results showed a trend towards higher VAD scores in thelate group. However, that group’s VAD score was lower thanthat published in the Colombia University study [10]. Thismay be one of the reasons why our survival rates are betterthan those of other institutions.
Several improvements in perioperative management haveplayed important roles in reducing early mortality andcomplications. Excessive bleeding was a major complicationand limiting factor for successful VAD implantation, increas-ing the need for blood transfusion, causing fluid overload andRHF, and resulting in prolonged postoperative intubation andICU stay. Immediate postoperative bleeding occurs in 20—40%of VAD recipients [1,2]. Perioperative requirements forextensive blood product usage can not only be lifethreatening but also impact secondary outcomes as shownby an increased incidence of RHF caused by a cytokine-mediated increase in pulmonary vascular resistance (PVR). Aretrospective multicenter analysis showed that aprotinin wasassociated with a significant decrease in postoperative bloodloss, transfusion requirements, and postoperative require-ment for an RVAD, as well as improvement in mortality ratesin LVAD patients [19]. We used aprotinin routinely in allpatients undergoing VAD implantation in the late group. As aresult, re-operation decreased to 5.3%. Additionally, theincidence of RHF was reduced to 5.9%. However, a recentmeta-analysis indicated an association between aprotinin useand serious end-organ damage in coronary bypass surgery[20] and we should consider these factors carefully. Sinceaprotinin is no longer available in the United States,

S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288 287
aminocaproic acid is administrated after induction ofanesthesia in recent cases.
Infection is one of the most serious common complicationsafter VAD implantation, affecting short- and long-termsurvival for patients on mechanical circulatory support, withmost studies documenting a 30—50% occurrence [21]. In theREMATCH trial, although survival was prolonged for the LVADgroup, infection remained a significant cause of morbidityand mortality. Sepsis was the most commonly reported causeof death (31%) and survival of LVAD patients without sepsiswas superior to that of patients who experienced sepsis (60%1-year and 38% 2-year survival in the non-sepsis group vs 39%1-year and 8% 2-year survival in the sepsis group, respec-tively). In our experience, the incidence of sepsis was 44.4%in the early group, however it decreased to 13.2% in the lategroup. It is obvious that the recent increase of implantabledevice usage and advances in antibiotic therapy led to thisimprovement [22]. In terms of perioperative management,we start antibiotic prophylaxis preoperatively and continuedit for at least 3 days post-implant as shown in the Methodssection, compared with the 2 day recommendation of anti-microbial prophylaxis protocol for REMATCH trial [21].Interestingly, the incidence of infection excluding sepsisdid not differ among the groups (localized non-device,p = 0.26; percutaneous site/pocket, p = 0.52). These datasuggest that patient education and self-care teaching in ourrecent VAD program could lead to early recognition ofinfection, preventing the onset of sepsis by early treatment.In addition, our nutrition experts initiate enteral feedingwithin two days of VAD implantation if patients will not beweaned from ventilatory support easily, because enteralnutrition supports gut integrity, can be used to modulate theimmune system, and carries a lower risk of bloodstreaminfection than parenteral nutrition [23].
A major determinant of survival after LVAD implantation isthe ability of the native right ventricle to provide adequateflow across the pulmonary circuit to sufficiently fill the LVAD.Because of this, RHF after LVAD insertion is a dreadedcomplication. RHF refractory to maximal pharmacologicaltherapy occurs in 20—40% of patients supported with LVADs,and the mortality in the RHF group is higher than the non-RHFgroup [24]. In preventing and treating RHF after LVADinsertion, it is particularly important to reduce PVR andvolume overload. As most institutions do, we use inhalednitric oxide (NO) and frequently administrate phosphodies-terase inhibitors (PDE-I) such as milrinone to decrease PVR.Additionally, in order to optimize volume balance, CVVH ispromptly started when aggressive pharmacologic therapyfails to control volume overload. In the late group, we usedperioperatively inhaled NO for nine cases (24%) among 37LVAD implantations, compared with no use in the early andmid groups, and the incidence of RHF after LVAD implant wasreduced to 6% from 22.2% in the mid group. Also, the numberof BiVAD insertions decreased to only three cases (7%) in thelate group, compared with seven (19%) in the early group andnine (25%) in the mid group. The use of NO and PDE-I mayhave contributed to the decreased incidence of RHF andnecessity of BiVAD after LVAD implant.
Neurological dysfunction such as transient ischemic attack(TIA) and stroke have proven problematic with all types ofmechanical circulatory support [25]. The reported incidence
varies widely from 2.7% to 35% and is undoubtedly influencedby patient variables, pump design, and the differentanticoagulant regimens employed. In addition, the degreeof thromboembolic neurological events is dependent on thesensitivity of the observer. In the present study, although theincidence of all neurological dysfunction did not differ amongthe groups, there tended to be a higher incidence of TIA inthe late group (Table 3). This could be related to thesignificantly longer support length in the late group and wealso believe that our recent dedicated multidisciplinaryapproach may have increased the sensitivity of TIA diagnosis.
End-stage heart failure patients in need of a VAD are likelyto be critically ill when compared with typical cardiacsurgical patients. In addition, these patients have becomeincreasingly high-risk [6]. A commitment to provide thehighest quality of care requires a dedicated team focused onthe issues that are unique to this patient population.Especially, ongoing communication and co-operationbetween the cardiac surgeons and heart failure cardiologiststaking care of these patients is vital to this effort. Since ourrecent VAD team was created, cardiologists have askedsurgeons to see potential VAD candidates early and hadongoing discussions regarding timing of VAD placement;surgeons have had cardiologists see high-risk cardiac surgicalpatients (that might need VADs) preoperatively, so the teamwas already on board if indeed a VAD was required. Thecontribution of nurses, LVAD coordinators, rehabilitationspecialists and nutrition experts are also indispensable.Social workers play an important role in supporting thepatient and family. We have found that a weekly meetingattended by the multidisciplinary VAD team facilitates theformulation of a unified treatment plan for patients beingsupported with VADs, as well as patients under considerationfor VAD implantation. By creating a multidisciplinary team,we would argue that we are implanting devices beforepatients develop profound and/or irreversible multiplesystemic organ failure. This institutional multidisciplinaryapproach is thought to have played an important role in therecent improvements in our outcomes.
Limitations of this study include those related to aretrospectively performed analysis. Clinical data wereobtained by chart review, which has inherent limitations,such as access to and accuracy of the recorded data.Additionally, as a retrospective observational study, it issubject to selection bias and incomplete data collection.Finally, extrapolation of the results regarding improvedsuccess in post-VAD survival and the incidence of complica-tions is limited because of inter-institutional variability inclinical practice, especially device selection.
In conclusion, the successful use of VADs and remarkabletechnological advances has led to the increased use of VADsfor patients who were once thought to be unsuitable fordevice insertion. To support and care for these complicatedpatients, a wide range of areas of expertise and supportservices are required. In reviewing our institutional experi-ence, outcomes have improved dramatically in recent VADpatients, despite the increasing high risk of the patientpopulation. Recent improvements in our outcomes likelyoccurred as a result of manymajor advances in device design,patient selection, and perioperative management, as well asthe multidisciplinary approach. Our experience indicates

S. Osaki et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 281—288288
that an institutional comprehensive patient care program isan important approach to successfully supporting patientswith heart failure in need of circulatory support.
Acknowledgements
We thank Alejandro Munoz-del-Rio, PhD, for his statisticalanalysis, and Holly Thomas, Sue Ulschmid, and TracySundquist for their assistance in data collection.
References
[1] Deng MC, Edwards LB, Hertz MI, Rowe AW, Keck BM, Kormos R, Naftel DC,Kirklin JK, Taylor DO. Mechanical circulatory support device database ofthe International Society for Heart and Lung Transplantation: ThirdAnnual Report—2005. J Heart Lung Transplant 2005;24:1182—7.
[2] Frazier OH, Rose EA, Oz MC, Dembitsky W, McCarthy P, Radovancevic B,Poirier VL, Dasse KA. Multicenter clinical evaluation of the HeartMatevented electric left ventricular assist system in patients awaiting hearttransplantation. J Thorac Cardiovasc Surg 2001;122:1186—95.
[3] Portner PM, Oyer PE, McGregor CGA. First human use of an electricallypowered implantable ventricular assist system. Artif Organs 1985;9:36.
[4] Goldstein DJ, Oz MC, Rose EA. Implantable left ventricular assist devices.N Engl J Med 1998;339:1522—33.
[5] Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW, DembitskyW, Long JW, Ascheim DD, Tierney AR, Levitan RG, Watson JT, Meier P,Ronan NS, Shapiro PA, Lazar RM, Miller LW, Gupta L, Frazier OH, Svigne-Nickens P, Oz MC, Poirier VL. Long-term mechanical left ventricularassistance for end-stage heart failure. N Engl J Med 2001;345:1435—43.
[6] Helman DN, Oz MC. Developing a comprehensive mechanical supportprogram. J Card Surg 2001;16:203—8.
[7] Rao V, Oz MC, Flannery MA, Catanese KA, Argenziano M, Naka Y. Revisedscreening scale to predict survival after insertion of a left ventricularassist device. J Thorac Cardiovasc Surg 2003;125:855—62.
[8] Miller LW, Pagani FD, Russell SD, John R, Boyle AJ, Aaronson KD, Conte JV,Naka Y, Mancini D, Delgado RM, MacGillivray TE, Farrar DJ, Frazier OH.Use of a continuous-flow device in patients awaiting heart transplanta-tion. N Engl J Med 2007;357:885—96.
[9] Farrar DJ, Holman WR, McBride LR, Kormos RL, Icenogle TB, Hendry PJ,Moore CH, Loisance DY, El-Banayosy A, Frazier H. Long-term follow-up ofThoratec ventricular assist device bridge-to-recovery patients success-fully removed from support after recovery of ventricular function. J HeartLung Transplant 2002;21:516—21.
[10] Morgan JA, John R, Rao V, Weinberg AD, Lee BJ, Mazzeo PA, Flannery MR,Chen JM, Oz MC, Naka Y. Bridging to transplant with the HeartMate leftventricular assist device: The Columbia Presbyterian 12-year experience.J Thorac Cardiovasc Surg 2004;127:1309—16.
[11] Rao V, Oz MC, Flannery MA, Idrissi KA, Argenziano M, Edwards NM, Naka Y.Changing trends in mechanical circulatory assistance. J Card Surg2004;19:361—6.
[12] Pagani FD, Long JW, Dembitsky WP, Joyce LD, Miller LW. Improvedmechanical reliability of the HeartMate XVE left ventricular assist system.Ann Thorac Surg 2006;82:1413—8.
[13] Siegenthaler MP, Martin J, Pernice K, Doenst T, Sorg S, Trummer G,Friesewinkel O, Beyersdorf F. The Jarvik 2000 is associated with lessinfections than the HeartMate left ventricular assist device. Eur J Car-diothorac Surg 2003;23:748—54.
[14] Goldstein DJ. Worldwide experience with the MicroMed DeBakey ventri-cular assist device as a bridge to transplantation. Circulation2003;108:II272—7.
[15] Miller LW, Lietz K. Candidate selection for long-term left ventricularassist device therapy for refractory heart failure. J Heart Lung Transplant2006;25:756—64.
[16] Deng MC, Loebe M, El-Banayosy A, Gronda E, Jansen PG, Vigano M,Wieselthaler GM, Reichart B, Vitali E, Pavie A, Mesana T, Loisance DY,Wheeldon DR, Portner PM. Mechanical circulatory support for advancedheart failure: Effect of patient selection on outcome. Circulation2001;103:231—7.
[17] Wagner FD, Buz S, Knosalla C, Hetzer R, Hocher B. Modulation ofcirculating endothelin-1 and big endothelin by nitric oxide inhalationfollowing left ventricular assist device implantation. Circulation2003;108:II278—84.
[18] Topkara VK, Dang NC, Barili F, Cheema FH, Martens TP, George I, BardakciH, Oz MC, Naka Y. Predictors and outcomes of continuous veno-venoushemodialysis use after implantation of a left ventricular assist device. JHeart Lung Transplant 2006;25:404—8.
[19] Goldstein DJ, Seldomridge JA, Chen JM, Catanese KA, DeRosa CM, Wein-berg AD, Smith CR, Rose EA, Levin HR, Oz MC. Use of aprotinin in LVADrecipients reduces blood loss, blood use, and perioperative mortality. AnnThorac Surg 1995;59:1063—7.
[20] Mangano DT, Tudor IC, Dietzel C. The risk associated with aprotinin incardiac surgery. N Engl J Med 2006;354:353—65.
[21] Holman WL, Park SJ, Long JW, Weinberg A, Gupta L, Tierney AR, AdamsonRM, Watson JD, Raines EP, Couper GS, Pagani FD, Burton NA, Miller LW,Naka Y. Infection in permanent circulatory support: experience from theREMATCH trial. J Heart Lung Transplant 2004;23:1359—65.
[22] Pae WE, Connell JM, Adelowo A, Boehmer JP, Korfer R, El-Banayosy A,Hetzer R, Vigano M, Pavie A. Does total implantability reduce infectionwith the use of a left ventricular assist device? The LionHeart experiencein Europe. J Heart Lung Transplant 2007;26:219—29.
[23] Marik PE, Zaloga GP. Early enteral nutrition in acutely ill patients: asystematic review. Crit Care Med 2001;29:2264—70.
[24] Ochiai Y, McCarthy PM, Smedira NG, Banbury MK, Navia JL, Feng J, Hsu AP,Yeager ML, Buda T, Hoercher KJ, Howard MW, Takagaki M, Doi K, Fuka-machi K. Predictors of severe right ventricular failure after implantableleft ventricular assist device insertion: analysis of 245 patients. Circula-tion 2002;106:I198—202.
[25] Eidelman BH, Obrist WD, Wagner WR, Kormos R, Griffith B. Cerebrovas-cular complications associated with the use of artificial circulatorysupport services. Neurol Clin 1993;11:463—74.




















