vietnam intervention project to assist persons with disabilities

181
Thoughts and ProgressIt is the goal of this section to publish material that provides information regarding specific issues, aspects of artificial organapplication, approach, philosophy, suggestions, and/or thoughts for the future.
Artificial Organs27(2):181–198, Blackwell Publishing, Inc.© 2003 International Society for Artificial Organs
Received November 2001; revised June 2002.Address correspondence and reprint requests to Dr. Yasuhiko
Tabata, Institute for Frontier Medical Sciences, Kyoto University,53 Kawara-cho Shogoin, Sakyo-ku, Kyoto 606-8507 Japan. E-mail:[email protected]
Improved Therapeutic Efficacy inCardiomyocyte Transplantation for
Myocardial Infarction with Release Systemof Basic Fibroblast Growth Factor
*Masaya Yamamoto, †Yutaka Sakakibara,†Kazunobu Nishimura, †Masashi Komeda,
and *Yasuhiko Tabata, *Department ofBiomaterials, Institute for Frontier Medical Sciences,
Kyoto University, Japan; and †Department ofCardiovascular Surgery, Graduate School of
Medicine, Kyoto University, Japan
Abstract: Several studies have demonstrated that celltransplantation was effective for the therapy of myocardialinfarction. However, little care has been taken for theblood supply indispensable to cell transplantation. Thisstudy is an investigation to evaluate the feasibility of inadvance angiogenesis by gelatin microspheres incorporat-ing basic fibroblast growth factor (bFGF) for the trans-plantation therapy of cardiomyocytes with an ischemiccardiomyopathy model. Rats with myocardial infarctionreceived the intramuscular injection of culture medium(Control), or that containing fetal cardiomyocytes (TX) or gelatin microspheres incorporating bFGF (FGF), andgelatin microspheres incorporating bFGF plus fetal car-diomyocytes 1 week later (FGF-TX). The left ventricle(LV) function of rat hearts was assessed by echocardiogra-phy and cardiac catheterization 4 weeks later. The LVmaximum time-varying elastance was significantly higherin the FGF-TX group than in other groups. The combina-tion of bFGF-induced angiogenesis and cardiomyocytetransplantation is a promising procedure to improve the LV function in rats with myocardial infarction. KeyWords: Cardiomyocyte transplantation—Prevasculariza-tion—Biodegradable gelatin microspheres—Basic fibrob-last growth factor—Controlled release—Cardiac infarctiontherapy.
Recently, cardiomyocyte transplantation hasattracted much attention in the research field of car-diovascular surgery as a next-generation therapy forthe majority of patients with end-stage heart failure
because of the shortage of donor hearts for cardiactransplantation. In North America, for instance,fewer than 20% of transplantation candidatesreceive donor hearts. Several research groups havereported that the transplantation of cardiomyocyteor non-cardiomyocyte cells, such as skeletal myo-blasts, on mesenchymal stem cells, was effective toimprove the left ventricular (LV) function in ratmyocardial infarction models (1,2). However, thereare several problems for cell transplantation, such aspoor supply of oxygen and nutrients to the cell trans-planted and the source of donor cells. The trans-planted cells are exposed to ischemia, inflammation,and oxidative stress when they are transplanted tothe ischemic regions. To improve the in vivo envi-ronment of transplanted cells, it is promising toinduce in advance angiogenesis around the trans-planted site by any means. This blood supply willenable the transplanted cells to prolong survival andmaintain cell functions.
It is well known that growth factors, such as basic fibroblast growth factor (bFGF) and vascularendothelial growth factor (VEGF), fundamentallycontribute to angiogenesis in the body (3). However,one cannot always expect any biological activities ofgrowth factors in vivo when they are injected in thesolution form, because of their short half-life. Thus,one of the possible technologies to enhance the invivo efficacy of growth factors is to achieve their controlled release over an extended time period byuse of a release carrier (4). We have succeeded ininducing angiogenesis through the controlled releaseof bFGF from gelatin hydrogels based on hydrogelbiodegradation (4,5). In this study, we investigate fea-sibility of prevascularization by the bFGF release inimproving efficacy of cardiomyocyte transplantationin a rat ischemic cardiomyopathy model.
MATERIALS AND METHODS
Ventricular cardiomyocytes were isolated from the heart of 20-day-old fetal Lewis rats syngeneic to the recipient rats (1). The bFGF-incorporatedmicrospheres were prepared by dropping 20 mL ofbFGF solution (100 mg bFGF, Kaken PharmaceuticalCo., Tokyo, Japan) onto 2 mg of the freeze-driedmicrospheres, followed by incubation at 4°C for 12 hr

182 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
to obtain bFGF-incorporated gelatin microspheres(5).
Rats (male Lewis, 250–290 g) with myocardialinfarction were prepared by the proximal left ante-rior descending coronary artery (LAD) ligation witha 5-0 polypropylene suture (6). Rats were randomlyclassified into 4 groups (11 rats/group) four weeksafter LAD ligation; intramyocardial injection of the culture medium (Control group), fetal cardio-myocytes (TX group), bFGF-incorporated gelatinmicrospheres (FGF group), and bFGF-incorporatedgelatin microspheres followed by cardiomyocytestransplantation 1 week later (FGF-TX group). In theTX, FGF, and FGF-TX groups, 6 ¥ 106 cultured fetalcardiomyocytes and/or bFGF-incorporated gelatinmicrospheres suspended in 50 mL of the serum-freeculture medium were injected with a fine syringe intothe central portion of scar tissue of the left ventricu-lar (LV) free wall.
Various LV functions were assessed by echocar-diography (SONOS 5500 imaging system, AgilentTechnologies, Andover, MA, U.S.A.) and a microm-anometer-tipped catheter (Millar Instruments Inc.,Houston, TX, U.S.A.). The parameters of LV end-diastolic dimension (LVDd: mm), LV end-systolicdimension (LVDs: mm), and fractional shortening(FS: %) were obtained from the M-mode tracing (7).The LV maximum time-varying elastance (LV Emax:mm Hg/mL) and LV end diastolic pressure (LVEDP:mm Hg) as an index of global systolic and diastolicfunction were examined. For statistical analysis, allthe values were shown as the mean value ± the stan-dard deviation of the mean. The pairwise compar-
isons of individual group means were conducted bymeans of Tukey test. Values of p < 0.05 were con-sidered statistically significant.
The explanted hearts were processed for histolog-ical study. Every specimen was cut in half by theshort-axis section including the injection point; onepart was fixed with 10% formalin for hematoxylinand eosin staining, and the other part was sectionedby cryomicrotome for fluorescent microscopic obser-vation of PKH26 dye-labeled cells.
RESULTS
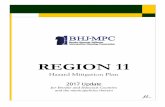
Table 1 summarizes the cardiac functions ofinfarcted hearts treated by bFGF-incorporatedgelatin microspheres and cardiomyocytes. There wasno significant difference in cardiac function or infarc-tion size before treatment among all the experi-mental groups. Four weeks after each treatment,LVDd in the FGF and FGF-TX groups was smallerthan in the Control group. The TX, FGF, and FGF-TX groups had significantly smaller LV systolicdimension (LVDs) than the Control group did. Thesethree groups had better FS than the Control group.LVEmax in the FGF-TX group was 430% (p < 0.01)higher than that in the Control group, and 172% (p < 0.05) higher than in the TX group (Fig. 1).LVEDP in the FGF-TX group was the lowest, and55% lower than that in the FGF-TX group (Fig. 1).
Four weeks after transplantation of fluorescent-labeled cardiomyocytes, many fluorescently positivecells were detected in the scar area. Whereas most ofthe transplanted cells were found around peri-infarc-
TABLE 1. Cardiac function data by echocardiography among Control, TX, FGF,FGF-TX groups
Pre-treatment
Control group TX group FGF group FGF-TX group
LVDd (mm) 10.3 ± 0.8 10.1 ± 0.7 9.7 ± 0.9 9.7 ± 0.9LVDs (mm) 7.9 ± 2.2 7.8 ± 0.9 7.9 ± 1.1 7.8 ± 1.0FS (%) 18.8 ± 5.4 22.4 ± 5.4 19.1 ± 6.7 19.8 ± 4.1HR (bpm) 373 ± 32 364 ± 31 359 ± 47 372 ± 43Infarction size (%) 27.4 ± 2.9 27.0 ± 4.1 30.8 ± 5.3 29.3 ± 4.0
Post-treatment
Control group TX group FGF group FGF-TX group
LVDd (mm) 10.7 ± 0.6 10.0 ± 1.1 9.5 ± 0.7** 9.6 ± 0.6*LVDs (mm) 8.8 ± 0.7 7.2 ± 0.9** 7.2 ± 1.1** 7.0 ± 1.0**FS (%) 17.3 ± 4.6 28.4 ± 4.4** 24.5 ± 8.6 27.4 ± 7.3**HR (bpm) 357 ± 31 374 ± 36 363 ± 40 376 ± 56Infarction size (%) 27.5 ± 3.5 27.0 ± 4.6 28.1 ± 5.2 24.9 ± 5.0
LVDd, left ventricular end-diastolic dimension; LVDs, end-systolic dimension; FS, fractionalshortening; HR, heart rate; Infarction size, the percentage of akinetic endocardial length to thewhole left ventricular endocardial circumference. All values are shown as the means ± SD (* P < .05 vs. Control group; ** P < .01 vs. Control group).
THOUGHTS AND PROGRESS 183
Artif Organs, Vol. 27, No. 2, 2003
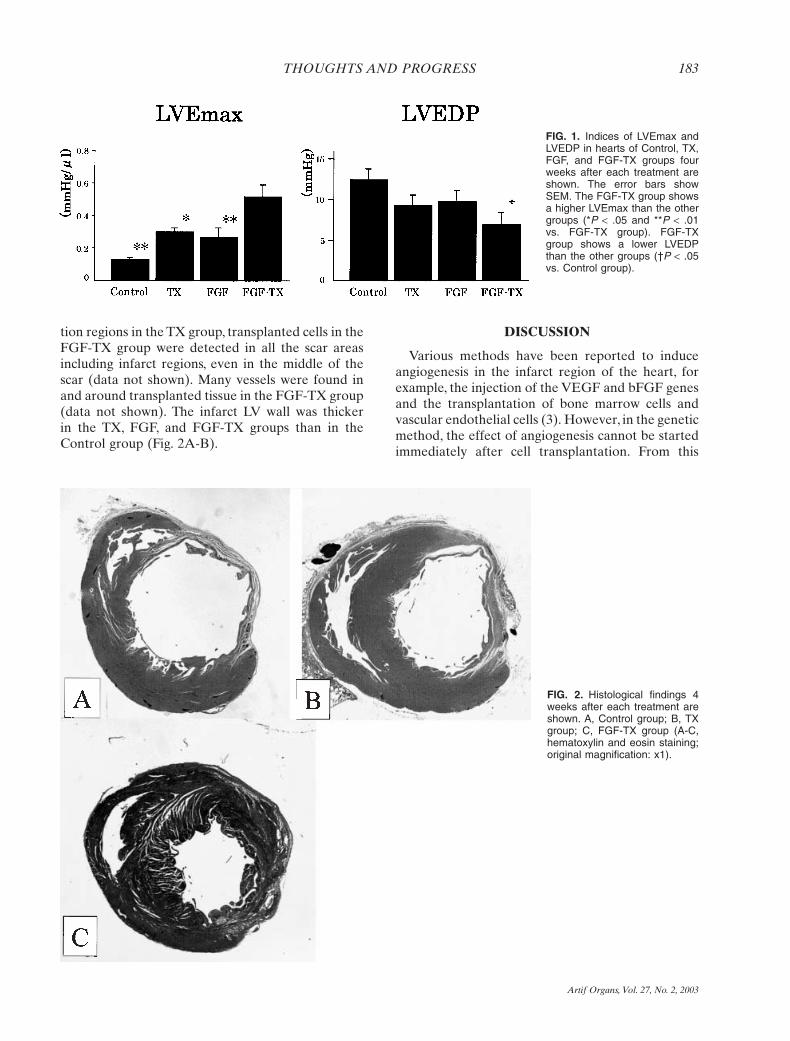
tion regions in the TX group, transplanted cells in theFGF-TX group were detected in all the scar areasincluding infarct regions, even in the middle of thescar (data not shown). Many vessels were found inand around transplanted tissue in the FGF-TX group(data not shown). The infarct LV wall was thicker in the TX, FGF, and FGF-TX groups than in theControl group (Fig. 2A-B).
DISCUSSION
Various methods have been reported to induceangiogenesis in the infarct region of the heart, forexample, the injection of the VEGF and bFGF genesand the transplantation of bone marrow cells andvascular endothelial cells (3). However, in the geneticmethod, the effect of angiogenesis cannot be startedimmediately after cell transplantation. From this
FIG. 1. Indices of LVEmax andLVEDP in hearts of Control, TX,FGF, and FGF-TX groups fourweeks after each treatment areshown. The error bars showSEM. The FGF-TX group showsa higher LVEmax than the othergroups (*P < .05 and **P < .01vs. FGF-TX group). FGF-TXgroup shows a lower LVEDPthan the other groups (†P < .05vs. Control group).
FIG. 2. Histological findings 4weeks after each treatment areshown. A, Control group; B, TXgroup; C, FGF-TX group (A-C,hematoxylin and eosin staining;original magnification: x1).

184 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
viewpoint, we chose to make use of angiogenicgrowth factor in the protein form, aiming at creationof an environment that is favorable for transplanta-tion of various cells to therapeutically treat the heartfailure with myocardial infarction.
Although bFGF is one of the angiogenic proteins,its biological activities cannot always be expectedwhen the bFGF solution is only injected into thebody because of the in vivo instability. One possiblestrategy to tackle the problem is to apply a controlledrelease technology to the growth factor. Our previ-ous study clearly indicates that the controlled releaseof bFGF could be achieved by use of the biodegrad-able gelatin hydrogel, and this release system waseffective in enhancing bFGF-induced angiogenesis(4,5).
Cardiomyocyte transplantation was therapeu-tically effective for the ischemic failing heart whencombined with in advance angiogenesis induced bythe controlled release of bFGF. Many cardiomy-ocytes were found in the scar tissue in the FGF-TXgroup in comparison with the other control groups(data not shown), and the cardiac function of thegroup was improved to a significantly greater extentthan that of the TX group (Table 1 and Fig. 1). Fur-thermore, there are many blood vessels newly formedin the infarct and peri-infarct area for both the FGFand FGF-TX groups (data not shown). These resultsstrongly suggest that the angiogenesis in advanceinduced by the controlled release of bFGF frombFGF-incorporated gelatin microspheres played animportant role in creating an environment suitablefor the survival and activity of transplanted cells. Theangiogenesis would be useful for sufficient supply ofnutrients and oxygen to the cells transplanted.
It is possible that there is the effect of gelatinmicrosphere on the stiffening of an infarctedsegment, resulting in improved cardiac function.However, based on our previous study, the micros-phere used in this study was completely degraded invivo within 2 weeks. Therefore, we think it is difficultfor the gelatin microspheres to play a role in theimprovement of cardiac function.
In conclusion, prevascularization induced by thecontrolled release of bFGF enabled the cardiomy-ocytes transplanted to improve the LV function inrats with myocardial infarction.
REFERENCES
1. Sakai T, Li RK, Weisel RD, Mickle DA, Jia ZQ, Tomita S, KimEJ, Yau TM. Fetal cell transplantation: a comparison of threecell types. J Thorac Cardiovasc Surg 1999;118:715–25.
2. Taylor DA, Atkins BZ, Hungspreugs P, Jones TR, Reedy MC,Hutcheson KA, Glower DD, Kraus WE. Regenerating func-
tional myocardium: improved performance after skeletalmyoblast transplantation. Nat Med 1998;4:929–33.
3. Simons M, Bonow RO, Chronos NA, Cohen DJ, Giordano FJ,Hammond HK, Laham RJ, Li W, Pike M, Sellke FW, StegmannTJ, Udelson JE, Rosengart TK. Clinical trials in coronary angio-genesis: issues, problems, consensus. An expert panel summary.Circulation 2000;102:E73–86.
4. Tabata Y, Ikada Y. Protein release from gelatin matrices. AdvDrug Deliv Rev 1998;31:287–301.
5. Tabata Y, Hijikata S, Muniruzzaman MD, Ikada Y. Neovascu-larization effect of biodegradable gelatin microspheres incor-porating basic fibroblast growth factor. J Biomater Sci PolymEd 1999;10:79–94.
6. Isgaard J, Kujacic V, Jennische E, Holmang A, Sun XY, HednerT, Hjalmarson A, Bengtsson BA. Growth hormone improvescardiac function in rats with experimental myocardial infarc-tion. Eur J Clin Invest 1997;27:517–25.
7. Burrell LM, Chan R, Phillips PA, Calafiore P, Tonkin AM,Johnston CI. Validation of an echocardiographic assessment ofcardiac function following moderate size myocardial infarctionin the rat. Clin Exp Pharmacol Physiol 1996;23:570–2.
Development of an Implantable High-Energy and Compact Battery
System for Artificial Heart
*E. Okamoto, †T. Inoue, *K. Watanabe,*T. Hashimoto, *E. Iwazawa, §Y. Abe, #T. Chinzei,
#T. Isoyama, ¶S. Kobayashi, §I. Saito, ||F. Sato,||H. Matsuki, §K. Imachi, and ‡Y. Mitamura,
*Department of Electric and InformationEngineering, Graduate School of Science andEngineering; †Department of Bioscience and
Technology, School of Engineering, Hokkaido TokaiUniversity, Sapporo; ‡Course of System Information
Engineering, Graduate School of Engineering,Hokkaido University, Sapporo; §Department of
Biomedical Engineering, Graduate School ofMedicine; #Research Center for Advanced Science
and Technology, University of Tokyo, Tokyo;¶Institute of Development, Aging and Cancer,
Tohoku University, Sendai; and Department ofElectrical and Communication Engineering,
Graduate School of Engineering, Tohoku University,Sendai, Japan
Abstract: The purpose of this study was to demonstratethe feasibility of the use of an implantable, high-energy, andcompact battery system for an undulation pump total
||
Received November 2001; revised May 2002.Presented in part at the 13th World Congress of International
Society for Artificial Organs, held November 5–8, 2001, in Osaka,Japan.
Address correspondence and reprint requests to Dr. EijiOkamoto, Department of Electric and Information Engineering,Graduate School of Science and Engineering, Hokkaido TokaiUniversity, Minami-sawa 5-1-1-1, Minami-ku, Sapporo 005-8601,Japan. E-mail: [email protected]

artificial heart (UPTAH). The implantable battery systemtested consists of six lithium-ion batteries in series, a chargeunit, and a charge/discharge control unit. A lithium-ionbattery is currently the best energy-storage device becauseit has more energy density, a better life cycle, and a smallertemperature rise than those of other secondary batteries.The performance of the implantable battery system wasevaluated in an in vitro experiment using an electric loadthat simulated the UPTAH. Also, sufficiently reliable operation of a system for supplying energy to a UPTAHconsisting of a transcutaneous energy transmission system(TETS) and an implantable battery system was confirmedin three experiments using goats. The results of the in vitroand in vivo experiments showed that the implantablebattery system supplied sufficient current to the UPTAHfor maintenance of physiological conditions in the goatwith maximum rise in temperature to less than 43°C. KeyWords: Artificial heart—Total artificial heart—Undula-tion pump total artificial heart—Lithium-ion battery—Transcutaneous energy transmission system.
An implantable secondary battery system is one ofthe key components of an implantable artificialheart. It serves as a power source for the artificial
heart in the case of interruption of power supplyfrom a transcutaneous energy transmission system(TETS). The performance of secondary batteries has improved dramatically in recent years due toresearch and development of new battery technol-ogy. Lithium-ion secondary batteries are currentlythe best energy-storage devices for an artificial heartbecause lithium-ion batteries have greater energydensity and less temperature rise than do other secondary batteries, because a lithium-ion batteryhas a long life of about 2 years (1).
The purpose of this study was to determine the feasibility of utilization of an implantable, high-energy, and compact battery system using a lithium-ion battery for an undulation pump total artificialheart (UPTAH) (2).
METHOD
An implantable battery system must supply amean motor current of 1.1 A with a terminal voltage
THOUGHTS AND PROGRESS 185
Artif Organs, Vol. 27, No. 2, 2003
FIG. 1. In vitro experimental results of the implantable battery system are shown.

of 24 V for 1 hour to drive a UPTAH. The batterysystem used in this study consists of six hermeticallysealed Li-ion batteries (Sony, US18650G, Tokyo,Japan) in series, a charge unit, and a charge/discharge control unit. Each lithium-ion battery hasa terminal voltage of 3.7 V and an energy capacity of1.5 Ah.
The battery is charged by a constant current andconstant voltage method (3) using electric energyderived from the TETS (4). A charge/discharge con-troller automatically switches between discharge andcharge phases, depending on the presence of trans-mitted energy from outside the body and on thevalue of battery terminal voltage.
The case holding the implantable battery systemwas designed, using CAD/CAM technology, so thatit could be implanted easily under the skin, andwould prevent biological fluid ingress. The case, withdimension of 124 mm ¥ 101 mm ¥ 23 mm, and avolume of 288 ml, was made from epoxy resin.
Experimental methodsIn the in vitro experiment, the battery system was
charged by a DC power supply instead of a TETS.The load for discharge was simulated, as the UPTAHrequired a pulsatile current waveform, using an elec-tronic load (Kikusui, PLZ153W, Yokohama, Japan).The temperature around the battery case was kept at37°C. The temperature of each Li-ion battery and ofthe battery case were continuously monitored bytemperature sensors (NS, LM35Z, USA) during boththe charge and the discharge phases.
In animal experiments, the implantable batterysystem and an energy-receiving unit were implantedunder the skin of the left thoracic region in healthyyoung male goats (body weight of 45 kg) afterimplantation of a UPTAH in the chest cavity of thegoats. The flat shape of the case of the implantablebattery system was suitable for the chest wall of theleft thoracic region in the goat. The current andvoltage in each component, left and right pumpoutputs, left arterial pressure (LAP), and aortic pres-sure (AoP) were measured at 3-minute intervals,and data were stored in a personal computer. Whenbattery terminal voltage during the discharge phasehad decreased to 23 V, the battery system wasswitched to charge to prevent malfunction of thepump controller. An autopsy was performed afterthe experiments.
RESULTS
Figure 1 shows the results of the in vitro experi-ment. The battery system was able to supply 1.7 A/0.3
A pulsatile currents (at a frequency of 2 Hz) for 60min with only a small rise in temperature (less than43°C) during the charge and discharge phases.
We carried out experiments using three goats. Thedata obtained from the animal that survived for thelongest period are shown in Fig. 2. The experimenton the animal was terminated on the 3rd day becauseof edema of the lung. The implanted batteries werefully charged by a constant current phase in 210 min,and the condition of the batteries was maintained bya constant voltage charge. When the TETS wasturned off, the implanted battery system automati-cally switched to the discharge phase, in which elec-tric energy was supplied to the UPTAH. When theTETS was turned on during the discharge phase ofthe implanted battery system, electric energy wassupplied from both the implanted battery system andthe TETS. When the battery voltage had decreasedto 23 V, the implanted battery system was switched tothe charge phase.
DISCUSSION
An implantable secondary battery system is one ofthe key components of a total artificial heart system.Lithium-ion secondary batteries are currently thebest energy-storage devices for portable computerelectronics because of their high energy density (1).
Safety and prevention of large temperature riseare important factors in design of an implantablebattery system. The lithium-ion batteries used in thisstudy were hermetically sealed to prevent electrolyteleakage. The case holding the implantable batterysystem was also hermetically sealed to prevent bio-logical fluid ingress. The maximum rise in tempera-ture of the surfaces of the lithium-ion batteriesduring the charge and discharge phases in the in vitroexperiment was less than 43°C, an acceptable degreeof temperature rise for use of the batteries in aUPTAH.
The performance of the implantable batterysystem was examined in three animal experiments.The energy source for the UPTAH was automaticallyswitched between the TETS and the implantablebattery system. The implantable battery system wasable to supply sufficient electric current for theUPTAH pumping in order to maintain cardiac cir-culation in the goat. However, impedance matchingbetween the implantable battery system and theUPTAH’s controller was a problem to be solvedbecause excessive current was applied to the con-troller during a period of cessation of energy trans-mission from outside the body. Further study isneeded to resolve this problem.
186 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003

CONCLUSION
We have developed an implantable battery systemusing Li-ion batteries to drive a UPTAH. In an invitro experiment, the battery system showed noproblems in terms of electric energy and temperaturerise during the charge and discharge phases. Theanimal experiments also showed that the perfor-mance of the implantable battery system was suffi-cient for maintenance of the physiological conditionsof the animals by operation of the UPTAH. As thenext step, we are planning to develop a battery man-agement and alarm system to ensure safety of thesystem for patients.
Acknowledgments: This study was supported bythe Program of Promotion of Fundamental Studiesin Health Sciences of the Organization for DrugADR Relief, R&D Promotion and Products Reviewof Japan.
REFERENCES
1. Okamoto E, Watanabe K, Hashiba K, Inoue T, Iwazawa E,Momoi M, Hashimoto T, Mitamura Y. Optimum selection of animplantable secondary battery for artificial heart by examina-tion of cycle life test. ASAIO J 2002;48(5):495–502.
2. Abe Y, Isoyama T, Ono T, Mochizuki S, Saito I, Iwasaki K,Ishimaru M, Baba A, Kouno A, Ozeki T, Tohyama T, Baba K,Imachi K. A step forward for the undulation pump total artificial heart. Int J Artif Organs 2000;3(2):70–4.
THOUGHTS AND PROGRESS 187
Artif Organs, Vol. 27, No. 2, 2003
FIG. 2. The results of the animalexperiment for evaluation of theimplantable battery system areshown.

3. http://www.sony.co.jp/en/Products/BAT/ION/Catalog-e.pdf4. Matsuki H, Yamakawa Y, Chubachi N. Transcutaneous
DC-DC converter for totally implantable artificial heart usingsynchronous rectifier. IEEE Trans Magn 1996;32(5):118–20.
In Vivo Evaluation of a MPC PolymerCoated Continuous Flow Left Ventricular
Assist System
*Shin’ichiro Kihara, †‡Kenji Yamazaki,*Kenneth N. Litwak, *Philip Litwak,
*Marina V. Kameneva, †Hiroyuki Ushiyama,†Toshimasa Tokuno, *†David C. Borzelleca,
§Mitsuo Umezu, §Jun Tomioka, ‡Osamu Tagusari,‡Takehide Akimoto, ‡Hitoshi Koyanagi,
‡Hiromi Kurosawa, *Robert L. Kormos, and#Bartley P. Griffith, *Department of Surgery,
University of Pittsburgh, Pittsburgh, PA, U.S.A.;†Sun Medical Technology Research Corporation,Nagano; ‡Department of Cardiovascular Surgery,
Tokyo Women’s Medical University, Tokyo;§Department of Mechanical Engineering, WasedaUniversity, Tokyo, Japan; #Department of Surgery,
University of Maryland, Baltimore, MD, U.S.A.
Abstract: The aim of this study was the evaluation of thethrombogenicity and the biocompatibility of the SunMed-ical EVAHEART left ventricular assist system (LVAS)coated with 2-methacryloyloxyethyl phosphorylcholine(MPC) polymer compared to a diamond-like carbon(DLC) coating. Four calves were implanted with the MPCpolymer-coated LVAS. Eight calves were implanted withDLC coated LVAS. The thrombogenicity and biocompati-bility of the pumps were evaluated. At explant, 60.0 ±37.2% (5–85%) of the pump surface area was still coatedwith MPC polymer after the duration of 45.0 ± 32.0 days.In 1 out of 4 MPC and 2 out of 8 DLC coated pumps, therewas a very small amount of thrombus around the seal ring;otherwise the blood contacting surfaces were free ofthrombus. Major organs were normal except for a fewlesions in kidneys from both groups. The MPC poly-mer coated EVAHEART LVAS seems to have low thrombogenicity and high biocompatibility similar to theDLC coated system. The current study demonstrated thatthe MPC polymer coating shows great promise for beingused as an antithrombogenic substrate for the LVAS dueto its ease of application, significant cost benefit, and reduc-tion in anticoagulation therapy in acute postoperativeperiod. Key Words: Left ventricular assist device—2-methacryloyloxyethyl phosphorylcholine—Diamond-likecarbon—Biocompatibility—Thrombogenicity—Rotaryblood pump.
Systemic thromboembolism is one of the majorcomplications accompanying mechanical circulatorysupport (1–3). Minimization of thromboembolismrequires significant systemic anticoagulation. Exces-sive anticoagulation can increase the incidence ofhemorrhagic complications, especially in the acutepostoperative period, potentially resulting in re-operation and excessive blood transfusion (1–3).Although continuous flow left ventricular assistsystems (LVAS) have less stagnation areas thanvolume displacement pumps, thromboembolism isstill a major complication (4–6). The aim of this studywas the in vivo evaluation of SunMedical EVA-HEART LVAS (SunMedical Technology ResearchCorporation, Nagano, Japan), a continuous flowpump, coated with 2-methacryloyloxyethyl phospho-rylcholine (MPC) polymer, poly MPC-co-butylmethacrylate (7) (NOF Corporation, Tokyo, Japan).Thrombogenicity and biocompatibility of the MPCcoated LVAS were compared to previously im-planted LVAS with a diamond-like carbon coating(DLC).
MATERIALS AND METHOD
Animals used and device descriptionFour Jersey breed calves (81–87 kg) were
implanted with the MPC polymer coated Sun-Medical EVAHEART LVAS. This centrifugal bloodpump is made of pure titanium, with the bearingaround the seal-shaft being continuously flushed andlubricated by a purge system (8). The blood contact-ing surfaces of the pump were first polished to aplane mirror finish and then coated with the MPCpolymer by immersing all blood contacting pumpparts in an alcohol solution containing MPC. Thealcohol was then allowed to evaporate, leaving theMPC adhered to the surface by surface tension. Eightcalves previously implanted with the same type ofpumps with DLC coating, using 2-phase ion beamdeposition, were used for coating comparison (8).Both systems had either a gelatin sealed knitted poly-ester graft (3 of 4 MPC pumps and 3 of 8 DLCpumps, Gelseal; Sulzer Vascutek Ltd, Scotland, UK)or expanded polytetrafluoroethylene graft (1 of 4MPC pumps and 5 of 8 DLC pumps, Gore-Tex; W. L.Gore & Associates, Inc., Flagstaff, AZ, U.S.A.) forinflow and outflow conduits.
Implant procedureThe calves were intubated endotracheally after
anesthesia induction and maintained with isofluraneand oxygen. A left thoracotomy through the 5th inter-costal space was used for implant. The device was
188 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
Received April 2002; revised July 2002.Address correspondence and reprint requests to Dr. Shin’ichiro
Kihara, McGowan Institute for Regenerative Medicine, Univer-sity of Pittsburgh, 300 Technology Drive, Pittsburgh, PA 15219,U.S.A. E-mail:[email protected]

implanted in a left ventricle-descending thoracicaorta bypass configuration without cardiopulmonarybypass. An outflow graft was first sewn onto thedescending thoracic aorta and then an inflow cannulawas inserted into a left ventricle and secured. Twoultrasonic flow probes (T206 series, TransonicSystems, Inc., Ithaca, NY, U.S.A.) were set on the pulmonary artery and the pump outflow graft.
Anticoagulation protocolOne MPC polymer coated pump was operated
without any anticoagulation after surgery. For allother calves (3 MPC polymer and 8 DLC coatedpumps), heparin was used as a bolus injection duringthe surgery, followed by continuous intravenousadministration to keep activated coagulation timewithin 200 to 250 seconds. Intravenous anticoagula-tion was then converted to oral warfarin sodium tokeep a prothrombin time international normalizedratio (INR) of 2.5–3.5 for the study duration.
Operation mode and data collectionThe pumps were operated at a fixed rotational
pump speed to keep pump assist rate at a goal of 50to 70% of total cardiac output. Arterial pressure,pump flow, and pulmonary artery flow were continu-ously monitored. Hemorheological studies, includingblood cell counts, chemistries, plasma free hemoglo-bin, blood hemoglobin, hematocrit, blood viscosity,plasma viscosity, plasma osmolality, erythrocytedeformability, and oxygen delivery index were mea-sured weekly to assess major organ function and biocompatibility of the pump. Each study was termi-nated at the end of the planned study protocol toevaluate the pump and major organ pathology.Blood-contacting surfaces of the pump wereinspected to check for thrombus formation. Theblood-contacting surfaces within the pump volutewere photographed. By following the margin of theMPC polymer, the percent area of residual MPCpolymer coating (Area of residual MPC coating/Total blood-contacting surface area) was quantifiedby planimetry software (Scion Image Beta 4.02, ScionCorporation, Frederick, MD, U.S.A.). Repeated blindmeasures of MPC surface area were ±10%.
At macroscopic inspection, renal lesions werequantified by percentage of the renal cortical surfacecovered by lesions, and were graded into four levels(Grade 1, 0–5%; Grade 2, 5–10%; Grade 3, 10–15%;Grade 4, >15%). The tissue samples were then fixedwith 10% buffered formalin for light microscopy andevaluated. The Mann-Whitney U test was applied totest statistical significance of difference between
groups (StatView 4.5, SAS Institute Inc., Cary, NC,U.S.A.).
All animals received humane care in accordancewith the Principles of Laboratory Animal Care formulated by the National Society for MedicalResearch as well as with the Guide for the Care andUse of Laboratory Animals, prepared by the Instituteof Laboratory Animal Resources, Natural ResearchCouncil, and published by the National AcademyPress (Revised in 1996) and the guidelines deter-mined by the Institutional Animal Care and UseCommittee of the University of Pittsburgh.
RESULTS
Perioperative characteristicsExperimental characteristics are shown in Table 1.
There was no difference between the DLC and theMPC group in study duration, pump, or hemody-namic parameters.
Evaluation of major organ functionThe hepatorenal markers (blood urea nitrogen,
serum creatinine, total bilirubin, alanine aminotrans-ferase, and aspartate aminotransferase) were stableand within the normal range throughout the study inboth groups. No clinically evident thromboembolicor hemorrhagic events occurred throughout thestudy. There was no sign of thromboembolism inmajor organs except a few minor renal lesions. Thesemacroscopically pale lesions on kidney surfaces didnot appear as infarctions, microscopically (Fig. 1). Nodifference in grade of renal lesions was observedbetween groups (MPC vs. DLC, 1.20 vs. 1.33, p =0.75). The liver, spleen, and gastrointestinal tracts hadno visible or histopathological infarctions.
Biocompatibility of the pumpOther hemorheologic parameters to evaluate the
biocompatibility, including plasma free hemoglobin,blood viscosity, plasma viscosity, erythrocyte defor-
THOUGHTS AND PROGRESS 189
Artif Organs, Vol. 27, No. 2, 2003
TABLE 1. Experimental characteristics
MPC group DLC group P value
Number of animals 4 8Duration (days) 45.0 ± 32.0 84.0 ± 64.0 0.18Pump flow rate (L/min) 4.51 ± 1.17 5.68 ± 1.61 0.07Assist flow ratio
(Pump/PA flow) 0.47 ± 0.15 0.46 ± 0.14 0.21Arterial pressure (mm Hg)
Systole 113.3 ± 8.0 112.0 ± 6.2 0.66Diastole 79.1 ± 7.8 81.7 ± 6.7 0.38Mean 91.7 ± 7.2 95.3 ± 5.9 0.20
Pulsatility Index 0.38 ± 0.10 0.32 ± 0.06 0.11

mability, oxygen delivery index, fibrinogen, andplasma osmolality were stable and there was no dif-ference during the full course of study in both groups(Table 2).
Inspection of the blood-contacting surface of the pump
In the DLC group, the blood-contacting surfaceswere free of thrombus in 6 out of 8 pumps at explant.A very small amount of thrombus around the seal
ring was observed in 2 of the DLC coated pumps. Inthe MPC polymer group, the one pump, which wasoperated without anticoagulation for 34 days, had avery small amount of thrombus formation around theseal ring (Fig. 2). The other 3 MPC polymer coatedpumps did not have any thrombus on blood contact-ing surfaces. In MPC polymer coated pumps, 60.0 ±37.2% (5–85%) of the blood contacting surface wasstill coated with MPC polymer after an assist dura-tion of 45.0 ± 32.0 days. Three out of 4 MPC pumps,with short-term (mean study duration; 30.0 days),had at least 70% of mean residual MPC coating at explant, while the remaining pump (implant duration; 91 days) had only 5%.
DISCUSSION
LVAS support generally requires significant anti-coagulation to avoid systemic thromboembolism.Excessive anticoagulation can increase the incidenceof bleeding complications, especially within the acutepostoperative period with a reported complicationrate of 37%–64% (1–3). Several surface modificationtechnologies have been established to minimizethrombus formation (9,10), but thromboembolismremains one of the major complications after LVASimplantation. The MPC polymer is a phospholipidpolymer, which was designed to resemble the surfacestructure of the biomembrane (11). This polymer hasexcellent blood compatibility and is now widely usedin blood contacting devices (12–14), but there is noknown report of these polymers being applied to animplantable LVAS. In our study, all of the hemorhe-ological parameters were stable within the normalrange, regardless of coating type, suggesting goodbiocompatibility of the MPC polymer-coated LVAS
190 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
FIG. 1. Shown are explanted kidneys from the calf with MPCpolymer-coated EVAHEART LVAS at explant after 34-day oper-ation without anticoagulation. Only a few, small pale lesions werenoted.
TABLE 2. Rheological study after implant
MPC group DLC group P value
Plasma free hemoglobin(mg/dl) 7.2 ± 2.4 8.1 ± 4.4 0.49
Hematocrit (%) 29.2 ± 4.2 30.1 ± 3.0 0.42Hemoglobin (g/dl) 10.2 ± 1.5 10.2 ± 1.1 0.94Fibrinogen (mg/dl) 522 ± 130 506 ± 127 0.76Total protein (g/dl) 5.7 ± 0.7 6.4 ± 0.6 <0.01Osmolality (mOsm/kg
H2O) 285 ± 1 275 ± 21 0.43Blood viscosity (cPs) 4.03 ± 0.58 3.75 ± 0.21 0.53Plasma viscosity (cPs) 1.80 ± 0.12 1.90 ± 0.14 0.33Deformability index 2.95 ± 0.11 2.90 ± 0.14 0.55Oxygen delivery index 7.21 ± 0.41 6.95 ± 0.78 0.47
FIG. 2. Shown is the inspection of MPC polymer-coated EVAHEART LVAS at explant after 34-day operation without anticoagulation.

(15). Function of the major organs was also main-tained within normal range in all calves throughoutthe study.
Surfaces modified with the MPC polymer havebeen shown to reduce platelet adhesion, complementactivation, and protein absorption, suggesting thatthis coating is effective against thrombus formation(11,14,16). The method to modify the pump surfacewith this coating is very simple, such that the assem-bled pump only needs to be immersed into an alco-holic solution containing the MPC polymer. There isno need for complicated technologies and expensiveequipment as with DLC coating (9) or texturedsurface (10). For example, with the DLC coatedsystem, it is difficult to deposit DLC film to the partswith complicated figures, like the pump rotor. Thiscan result in pump design limitations (17). As a result of using the MPC polymer coated system,we have been able to make significant pump designimprovements.
The major limitation of this coating appears to bethe loss of 20%–30% of the coating within a month,primarily in those areas facing a high bloodstreamvelocity. We also noted that the pump operated for91 days had only 5% of the MPC polymer remain-ing. This suggests that long-term anticoagulation willstill be needed. However, this limitation is likely nota critical issue for the EVAHEART LVAS becausein addition to the current report, low thromboem-bolism of this system without MPC polymer coatinghas already been reported (18), in fact the one MPCpolymer coated pump with only 5% MPC polymerremaining had no thrombus present. This study didsuggest that pump surfaces modified with the MPCpolymer have low thrombogenicity for approxi-mately 1 month of operation without anticoagulationtherapy, even in a thrombus prone model such as thecalf. While the long-term effectiveness of this coatingis unclear, the advantage of this coating is that theincidence of bleeding complications in the acutepostoperative period might be reduced, as anticoag-ulation results in most of the bleeding complicationwithin the 2 weeks after surgery. This may decreasethe risk of infection due to re-operation, as well asexcessive blood transfusions. While any thrombusdevelopment is potentially significant, the MPCpolymer-coating shows great promise for being usedas an antithrombogenic substrate for the LVAS dueto its ease of application, cost benefit, and reductionin anticoagulation therapy in acute postoperativeperiod.
Acknowledgments: This study was supported bySunMedical Technology Research Corporation and
the McGowan Institute for Regenerative Medicineat the University of Pittsburgh. We express gratitudeto NOF Corporation for supplying MPC, to Dr.Kazuhiko Ishihara (University of Tokyo) for hisadvice, and to Mary J. Watach and Lisa Gordon (University of Pittsburgh) for their excellent tech-nical assistance. This paper was presented in part at the 9th Congress of the International Society forRotary Blood Pumps, on August 20th, 2001 in Seattle,U.S.A.
REFERENCES
1. Frazier OH, Rose EA, Macmanus Q, Burton NA, Lefrak EA,Poirier VL, Dasse KA. Multicenter clinical evaluation of theHeartMate 1000 IP left ventricular assist device. Ann ThoracSurg 1992:53;1080–90.
2. Wasler A, Springer WE, Radovancevic B, Myers TJ, Stutts LA,Frazier OH. A comparison between intraperitoneal andextraperitoneal left ventricular assist system placement.ASAIO J 1996:42;M573–6.
3. Schmid C, Deng M, Hammel D, Weyand M, Loick HM, ScheldHH. Emergency versus elective/urgent left ventricular assist device implantation. J Heart Lung Transplant 1998:17;1024–8.
4. Wieselthaler GM, Schima H, Lassnigg AM, Dworschak M,Pacher R, Grimm M, Wolner E. Lessons learned from the firstclinical implants of the DeBakey ventricular assist device axialpump: a single center report. Ann Thorac Surg 2001:71;S139–43; discussion S44–6.
5. Frazier OH, Myers TJ, Jarvik RK, Westaby S, Pigott DW,Gregoric ID, Khan T, Tamez DW, Conger JL, Macris MP.Research and development of an implantable, axial-flow leftventricular assist device: the Jarvik 2000 Heart. Ann ThoracSurg 2001:71;S125–32; discussion S44–6.
6. Burke DJ, Burke E, Parsaie F, Poirier V, Butler K, Thomas D,Taylor L, Maher T. The HeartMate II: design and developmentof a fully sealed axial flow left ventricular assist system. ArtifOrgans 2001:25;380–5.
7. Ishihara K, Ueda T, Nakabayashi N. Preparation of phospho-lipid polymers and their properties as hydrogel membrane.Polym J 1990:22;355–60.
8. Yamazaki K, Litwak P,Tagusari O, Mori T, Kono K, KamenevaM, Watach M, Gordon L, Miyagishima M, Tomioka J, UmezuM, Outa E, Antaki JF, Kormos RL, Koyanagi H, Griffith BP.An implantable centrifugal blood pump with a recirculatingpurge system (Cool-Seal system). Artif Organs 1998:22;466–74.
9. Monties JR, Dion I, Havlik P, Rouais F, Trinkl J, Baquey C.Cora rotary pump for implantable left ventricular assistdevice: biomaterial aspects. Artif Organs 1997:21;730–4.
10. Spanier TB, Chen JM, Oz MC, Stern DM, Rose EA, SchmidtAM. Time-dependent cellular population of textured-surfaceleft ventricular assist devices contributes to the developmentof a biphasic systemic procoagulant response. J Thorac Cardiovasc Surg 1999:118;404–13.
11. Ishihara K, Aragaki R, Ueda T, Watenabe A, Nakabayashi N.Reduced thrombogenicity of polymers having phospholipidpolar groups. J Biomed Mater Res 1990:24;1069–77.
12. Ishihara K, Nakabayashi N. Hemocompatible cellulose dialy-sis membranes modified with phospholipid polymers. ArtifOrgans 1995:19;1215–21.
13. Furuzono T, Ishihara K, Nakabayashi N, Tamada Y. Chemicalmodification of silk fibroin with 2-methacryloyloxyethyl phos-phorylcholine. II. Graft-polymerization onto fabric through 2-methacryloyloxyethyl isocyanate and interaction betweenfabric and platelets. Biomaterials 2000:21;327–33.
14. Ishihara K. New polymeric biomaterials-phospholipid poly-
THOUGHTS AND PROGRESS 191
Artif Organs, Vol. 27, No. 2, 2003

mers with a biocompatible surface. Front Med Biol Eng2000:10;83–95.
15. Kameneva MV, Watach MJ, Litwak P, Antaki JF, Butler KC,Thomas DC, Taylor LP, Borovetz HS, Kormos RL, Griffith BP.Chronic animal health assessment during axial ventricularassistance: importance of hemorheologic parameters. ASAIOJ 1999:45;183–8.
16. Ishihara K, Ishikawa E, Iwasaki Y, Nakabayashi N. Inhibitionof fibroblast cell adhesion on substrate by coating with 2-methacryloyloxyethyl phosphorylcholine polymers. J Biomater Sci Polym Ed 1999:10;1047–61.
17. Alanazi A, Nojiri C, Kido T, Noguchi T, Ohgoe Y, Matsuda T,Hirakuri K, Funakubo A, Sakai K, Fukui Y. Engineeringanalysis of diamond-like carbon coated polymeric materialsfor biomedical applications. Artif Organs 2000:24;624–7.
18. Yamazaki K, Kormos RL, Litwak P,Tagusari O, Mori T,AntakiJF, Kameneva M, Watach M, Gordon L, Mukuo H, Umezu M,Tomioka J, Outa E, Griffith BP, Koyanagai H. Long-termanimal experiments with an intraventricular axial flow bloodpump. ASAIO J 1997:43;M696–700.
Development of Disposable Self-Regulating Blood Pumps and
Automatically-Controlled PortableExtracorporeal Membrane Oxygenation
Systems for Neonatal ExtracorporealMembrane Oxygenation
*Takahiko Seo, *Hisami Ando, *Takahiro Ito,*Hiroyuki Takagi, †Yoshitaka Inagaki, and
†Akira Suzuki, *Department of Pediatric Surgery,Nagoya University Graduate School of Medicine, Nagoya;
and †Aisin Human Systems, Kariya, Japan.
Abstract: For safer and simpler neonatal ECMO man-agement, the authors have been developing an innovative,automatically-controlled ECMO machine using self-regulating blood pumps. The newest model is an air-driven,tube-type blood pump. A pair of blood pumps are placedin parallel and actuated alternately with compressed air.The pump flow is automatically regulated in accordancewith hemodynamic changes of the body. The need for avenous reservoir is eliminated because the circuit does notgenerate excessive negative pressure when there are short-ages of draining blood. Therefore, the priming volume ofthe circuit is only 85 ml. This ECMO apparatus has threedriving modes, one of which is a “delay” mode. This enablesthe pump flow to easily be varied from 10 to 500 ml/minunder automatic control, and it can be used when the pumpflow is decreased for weaning. This newest ECMO appa-ratus was clinically used in 3 neonates with severe lunghypoplasia and persistent fetal circulation. The ECMOduration was 139 h to 168 h, and the maximum ECMO flow71.3 to 109.0 ml/min/kg. Thanks to the self-regulation,intensive observation of the circuit was not necessary
during ECMO. Damage to blood cells was less significant,and the use of blood products was only minimal (15.7 ml/kg/day) because a large volume of blood to stabi-lize the pump performance was not necessary. In conclu-sion, the automatically-controlled ECMO apparatusworked well without complications by changing theECMO flow automatically in accordance with hemody-namic changes. This automatic ECMO system requiredfewer personnel expenditures and was also favorable interms of hematological findings. Key Words: Extracor-poreal membrane oxygenation—Self-regulating bloodpumps—Automatic control system—Neonatal respiratoryfailure—Blood transfusion.
Neonatal extracorporeal membrane oxygenation(ECMO) has been widely accepted as the ultimatetreatment for acute respiratory failure. However, theconventional neonatal ECMO circuit has not basi-cally changed, using a roller pump since its introduc-tion for neonatal diseases in the early 1970s (1). Themechanism of the roller pump is simple and its oper-ation is reliable; however, the roller pump keepsrunning even when draining blood to the pumpdecreases or an afferent circuit is occluded. This situation causes serious complications such as airembolism and raceway breakdown. Some deviceshave been added to the circuit (2,3), but one mustalways pay close attention to the pump to preventsuch complications (4). In America and Europe, well-trained perfusionists have an important role in themanagement of ECMO (5). In contrast, in Japan,pediatric surgeons, pediatricians, and intensive carephysicians handle the ECMO machine while treatingthe patients as well. ECMO management is verytroublesome and labor-intensive, with the result that the entire staff is exhausted by the time ECMO is terminated. Thus, the development of anautomatically-controlled ECMO machine and lesslaborious ECMO management are needed.
For safer and simpler neonatal ECMO manage-ment, we have been developing and modifying an innovative self-regulating ECMO machine usingTakagi blood pumps since 1987 (6–11). In the Takagipump, two sac-type blood pumps are placed in parallel and actuated alternately with compressed air(12,13). While one pump expands with drainingblood, the other ejects blood at the same time as a pulsatile flow. The degree and frequency of expansions of the blood chambers are detected withsensors and transmitted to the control unit, whichcomputes and promptly commands the pump tochange the air pressure and pumping rates. TheTakagi pump acts as a natural heart under Starling’slaw (13). The pump flow is automatically regulated inorder to fix the ratio of the expansion and compres-
192 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
Received September 2001; revised July 2002.Address correspondence and reprint requests to Dr. Takahiko
Seo, Department of Pediatric Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku,Nagoya 466-8550, Japan. E-mail: [email protected]

sion of the blood chambers at 1 to 1. When drainingblood to the chamber decreases and the expansiontime is prolonged at the time of the decrease invenous pressure, the pump acts to prolong the com-pression time by decreasing the air pressure andpumping rates. As a result, the pump flow decreases.If the venous return increases, the pump flow con-versely increases. When arterial pressure increases,the pump keeps the same pump flow level by in-creasing air pressure. Our ECMO circuit has severaladvantages over the roller pump: self-regulated pumpflow in accordance with hemodynamic changes;no venous reservoir is needed because the circuit does not generate excessive negative pressure on the inflow side even in cases of a shortage of draining blood small priming volume of the circuitand automatic stop during excessive positive pres-sure on the arterial side due to circuit occlusion.
For simpler ECMO management with a moredurable ECMO machine, we have changed the mate-rials and shapes of the blood pumps. Also, the driveand control unit has been modified using the controlcomponent of an adult artificial heart device. Wedescribe herein the characteristics and performanceof our newest ECMO machine, and the outcome ofits clinical use.
MATERIALS AND METHODS
Before developing our latest type of blood pump and driving and control unit, we devised two
prototypes. Both prototypes were sac-type double-chambered pneumatic pumps. In the second generation blood pumps, a saline chamber was posi-tioned between the blood chamber and air housing,because blood chambers made of silicone rubbermay cause small lacerations during a long ECMOoperation, and contamination of the blood by air. Thedrive and control unit consists of an air compressor,a pressure regulator, and solenoid valves. The firstprototype unit had a stepping motor, which drove thepressure regulator. For more rapid pressure changes,the second prototype had an electropneumatic airpressure regulator that reacted promptly to hemody-namic changes but tended to overreact to noisebecause of its high sensitivity. The details of theseprototype pumps and drive and control units aredescribed elsewhere (6,7,10,12,13).
To make our ECMO apparatus safer, more reliable, and easier to handle, we created an entirelynew pump, and also modified the drive and controlunit.
Latest modification of self-regulating blood pumpsThe newest model is an air-driven, tube-type self-
regulating blood pump (Fig. 1). The blood chamberand ball valves are made of polyurethane and Teflon,respectively, for longer use. The blood chambervolume is about 6 ml, approximating the strokevolume of the neonatal heart. In the previous sac-type blood pumps, it was rather difficult to make thetwo blood chambers completely the same shape.
THOUGHTS AND PROGRESS 193
Artif Organs, Vol. 27, No. 2, 2003
FIG. 1. This is a schematicdrawing of the newest air-driven,tube-type self-regulating bloodpumps.

In the latest version, the shape and elasticity arealmost the same between the two blood chambers,thus pump performance and reliability are greatlyimproving. Blood flows in a straight line in the pumpand clot formation is much less likely after a longECMO operation than in the earlier prototypes. Thesaline chamber used in the previous pump was eliminated because the new blood chamber is muchmore durable. A photosensor and light source areused for automatic regulation. The photosensors,light sources, and air housings, which do not contactblood directly, are reusable, thereby reducing the costof the blood pumps.
Latest modification of drive and control unitsThe newest drive and control unit consists of air
compressors, tanks, and valves (Fig. 2). Aisin HumanSystems, a Toyota affiliate, manufactured it using arti-ficial heart and motor technologies. Compressed airsupplied by the air compressor is directed alternatelyto one of the two air housings of the pump by sole-noid valve opening between the air tank and the airhousings. The solenoid valves and air tanks regulatethe air pressure, and the large tank enables moresmooth and accurate changes in pressure with highcompliance. The control unit regulates the pump flow automatically with a microcomputer. We noticechanges in the decreased flow as changes in thesound of pumping of the pump. An alarm warning issounded and the pump stopped automatically if airpressure and pumping rate exceed the predeter-mined range.
There are three drive modes in the newest drivingand control unit: “automatic mode,” “delay mode,”and “constant mode.” The automatic mode is usedwhen ECMO runs at a maximum flow rate. In thismode, all blood draining from the body is returnedat a full rate. The delay mechanism enables the pumpflow to change easily like a roller pump. The delaymode is used when the ECMO flow is graduallydecreased for weaning. On the constant mode, the airpressure and the pumping rates are fixed, thus the pump flow is not influenced by hemodynamicchanges of the body and is kept constant.
The drive unit uses alternating (AC) current, andcan also run on portable batteries for about 150minutes. The pump operates reliably even underjolting, so it can be used during ambulance transport.
After confirming the safety and durability of thenewest pump system and its performance in mockcirculation and animal experiments, we used thissystem for actual neonatal cases. Its clinical use wasapproved by the Ethics Committee of the NagoyaUniversity School of Medicine, and informed consentwas obtained from the parents.
RESULTS
Pump performance in mock circulation and animal experiments
In mock circulation, the maximum flow of 940 ml/min could be available without an oxygenator,and 555 ml/min with an oxygenator of 0.5 mm2
(MERASILOX-S 0.5; Senko Ika Kogyo Inc., Tokyo,
194 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
FIG. 2. The schematic drawingshows the driving and controlunit.

Japan), under the condition of 100 cm H2O of preloadand 100 mm Hg of afterload. That flow is sufficientfor neonates weighing about 3 kg. At the maximumflow with the oxygenator, the air pressure was 465mm Hg and the pumping rate was 330/min. Pressurewave is damped 1/4–5 through the oxygenator, so themaximum pressure in the blood circuit is about 100 to 120 mm Hg. The pump flow was automatically regulated in response to changes in preload andafterload under automatic control, as mentionedabove. No mechanical problems were encounteredduring continuous drive for 550 h in mock circula-tion. Plasma-free hemoglobin after 48 h of circulationat a flow rate of 420 to 430 ml/min without the oxy-genator was 495 mg/dl for our pump and 1,495 mg/dl for the roller pump. Thus, hemolysis in the circuitwith our pump was less than one third that using theroller pump.
Pump performance under the delay mode wasinvestigated in mock circulation. As mentionedbefore, the ratio of expansion and compression isfixed at 1 to 1. In the delay mode, the delay time isadded to the expansion time. The compression timeequals the expansion time along with the delay time.
Hence, the air pressure and pumping rates decreasein order to increase compression time, resulting in adecrease in pump flow (Fig. 3). The pump flow can be regulated automatically in accordance withchanges in hemodynamics even in the delay mode.As the delay time increases, which is done by simplyturning the switch around, the pump flow decreasesalmost linearly (Fig. 4). The delay mode enables theECMO flow to change easily from 10 to 500 ml/minunder automatic control.
Then we confirmed the pump performance forECMO and isolated liver perfusion in 30 dogs and 45 pigs, with a total driving time of more than 600 husing one pump system (14,15).
Clinical useThis newest ECMO apparatus was clinically used
in three neonates: two neonates with congenitaldiaphragmatic hernia (CDH) and one with congeni-tal cystic adenomatoid malformation (CCAM) of the left lung. The two CDH patients needed venoar-terial ECMO immediately after birth, at 23 h and 15 h after birth, respectively. In the CCAM case,venovenous ECMO (VV-ECMO) was started at the
THOUGHTS AND PROGRESS 195
Artif Organs, Vol. 27, No. 2, 2003
(limited)
FIG. 3. The figure shows representative changes in driving air pressure and bypass flow rate in response to changes in time constantfor the “delay” in the mock circulation. (Output: Bypass flow, Up: Up-regulation signal for air pressure, Down: Down-regulation signal forair pressure, Air-Pr.: Air pressure, Normal: Automatic mode, Limited: Delay mode to increase the time constant)

age of 8 days using a 12 F double-lumen catheterthrough the right internal jugular vein (11). TheECMO durations were 139 h, 149 h, and 168 h,respectively. All three patients were successfullyweaned from ECMO, and two patients (one withCDH and one with CCAM) have been doing wellwithout any sequelae.
Our ECMO circuit is composed of only the pump,membrane oxygenator (MERASILOX-S 0.8), heatexchanger, and the probe of the electromagneticflowmeter (MFV-3100; Nihon Koden Inc., Tokyo,Japan), connected with polyvinylchloride tubing 4.0 mm in inner diameter. The priming volume of ourECMO circuit is only 85 ml in spite of the largermembrane oxygenator with a surface area of 0.8 m2.Systemic heparinization was achieved, and the activated clotting time was maintained at 180–200 s.
During ECMO, patient conditions were stable andoxygenation was improved in all cases. Systolic arte-rial pressure was stable, with a range of 50–70 mmHg, and pulse pressure of about 20 mm Hg. The auto-matic control in response to changes in hemody-namics worked well, and the maximum ECMO flowwas 71.3, 109.0, and 108.5 ml/min/kg, respectively.Under automatic control, ECMO flow was stable but
gradually fluctuated several times to 10 ml/min.When weaning from ECMO, the flow could bechanged conveniently using a delay mode as little as 10 ml/min. When the circulating blood of the bodydecreased, the flow decreased as well. Therefore, wecould estimate the volume of blood loss and theproper volume of blood products to be transfused inorder to keep the ECMO flow constant. Thanks tothe self-regulating blood pumps, intensive observa-tion of the circuit was not necessary during the entirecourse of ECMO in all cases.
In the patient with CCAM, the platelet countremained over one hundred thousand during ECMOfor 7 days, and no platelet transfusion was needed. Inother patients, no further platelet transfusion wasnecessary after the pump performance remainedstable. The urine color did not change during thecourse of ECMO, suggesting that hemolysis was notso prominent. In one patient, the plasma-free hemo-globin remained at 10–15 mg/dl after stabilization ofECMO flow. In all neonates, the use of blood prod-ucts was only minimal, 15.7 ml/kg/day, because a con-siderable amount of blood to stabilize the pumpperformance was not necessary once the circulatingblood volume was maintained adequately. Clot for-mation in the oxygenator fibers as well as the pumpwas minimal. Only some tiny clots were found at theinlet and outlet of the pumps after cessation ofECMO.
DISCUSSION
More than 25 years have passed since the first successful use of neonatal ECMO (1), however, theECMO circuit has basically not changed. A rollerpump has been widely used for the blood pump inmost conventional ECMO circuits. Its disadvantagesinclude the possibility of venous collapse and air con-tamination of the blood at the time of inadequatevenous return, raceway rupture at the time of outletocclusion, and blood cell damage (4). A venous reser-voir and electromechanical on-off switch were addedto the ECMO circuit to automatically stop the rollerpump at the time of venous reservoir collapse (2).However, blood products were needed to restart andstabilize the ECMO flow, and meticulous attentionwas necessary to employ the ECMO machine with-out mishap. Zwischenberger et al. (16) reported4,322 mechanical complications in 7,667 ECMOcases submitted to the ELSO Registry, including 406involving air in the circuit, 133 pump malfunctions,and 23 raceway ruptures. Shanley et al. (17) alsodescribed that, among 446 mechanical complicationsin 460 neonatal cases, air in the circuit occurred in 65
196 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
FIG. 4. The graph shows the relationship between the pumpoutput and time constant of the “delay” mode in a mock circulation.

cases, tubing rupture in 11, pump malfunction in 9,and raceway rupture in 2 cases.
Some innovative changes have been carried out tochange the ECMO flow successively in proportion tothe expansion of the venous reservoir. Atkinson et al.(3), for example, developed a computer-assisted per-fusion system for the neonatal ECMO circuit, whichenabled slowing or accelerating the roller head andincreasing or decreasing the ECMO flow continu-ously in response to changes in venous return.However, a large venous reservoir also was neededas well as additional priming volume. To eliminatethe venous reservoir from venovenous bypass, a trialwas performed to develop a venous control deviceusing a pneumatic manometer with an adjustablealarm to monitor the blood pressure in the venouslimb of the circuit (18). This mechanism was notapplied widely for clinical use.
To reduce the risk of raceway rupture and person-nel expenditures, Durandy et al. developed a uniquesingle-cannula venovenous bypass system usingalternating clamps and a nonocclusive roller pumpwith a stretchable tubing as the venous reservoir (19).Later, this system was named AREC (assistance res-piratoire extra corporelle) (20), and Trittenwein et al.(21,22) applied this AREC system for rescue ininfants and children. Although promising, its prob-lems were the need for a large priming volume (400 ml for the 1/4 inch tubing) and additionalvolume to maintain central venous pressure of atleast 8 cm of water (21). Also, the raceway needs tobe routinely exchanged every 3 days to preventleakage (22).
Recently, a centrifugal pump has been used todecrease the danger and labor associated withECMO management. The centrifugal pump is pres-sure-limited and unlikely to result in either the aspi-ration of air or disruption of the lines because it stopsautomatically in the case of a shortage of venousdraining blood and circuit occlusion (23). With thecentrifugal pump, when the venous pressure reaches-100 mm Hg, an abrupt decrease in flow occurs (4).Therefore, a venous reservoir is not generallyrequired. However, more negative pressures may beassociated with damage to red cells or right atrialtissue (4). The neonatal ECMO with the centrifugalpump is complicated by significant hemolysis, whichnecessitates a pump head change or a completecircuit change (24). To prevent such negative pres-sure, a servo pressure regulator used on the inlet sideresulted in less hemolysis and better preservation ofrenal function (25). However, there are still problemsof heat generation, thrombus formation, and brokenseals when used for several days (25). Our pump is
unique in providing completely automatic control ofthe ECMO flow against the hemodynamic changes ofthe body with a minimal priming volume.
Nosé (26) mentioned that the design for a clinicallyeffective and safe cardiac prosthesis should includeoptimal size, endurance, efficient operation, antitrau-matic features, antithrombogenicity, and biocompat-ibility. The development of a pump that can satisfyall these requirements is very difficult. However,since a pump for ECMO is used for considerablyshorter time than an implantable artificial heart, ourpump can fulfill these requirements when used forless than 1 month (26). Recently, modern treatmentmodalities other than ECMO such as nitric oxide andhigh frequency oscillation have been developed and will replace the main therapeutic strategies inneonates and children with acute severe respiratoryfailure. ECMO will be indicated in fewer cases andused only for the most severe cases in the near future.Therefore, ECMO management should be less labo-rious, safer, and less invasive, because it may be usedfor much longer durations in seriously ill patients. Incontrast, less dangerous methods, such as VV-ECMO,may become widely used for less severe cases. OurECMO apparatus with a self-regulating blood pumpcan be employed in such situations. Because thisnewest pump correctly detects more subtle changesin hemodynamics, it can be used in a small circula-tion system with low flow pressure. We have beeninvestigating isolated liver perfusion between thehepatic and portal veins in small pigs using thisnewest blood pump (14,15). It can also be used inolder children weighing more only by changing thesize of the blood chamber.
In conclusion, an automatically controlled ECMOsystem was modified for more convenient and saferclinical use. This machine can easily change andcontrol the ECMO flow using the “delay” mode inresponse to hemodynamic changes. Although ourclinical experience is very small, our automaticECMO circuit requires less personnel expendituresand is favorable in terms of the hematological findings.
REFERENCES
1. Bartlett RH, Gazzaniga AB, Jefferies MR, Huxtable RF,Haiduc NJ, Fong SW. Extracorporeal membrane oxygenation(ECMO): cardiopulmonary support in infancy. Trans Am SocArtif Intern Organs 1976;22:80–93.
2. Bartlett RH, Toomasian J, Roloff D, Corwin AG, Rucker R. Extracorporeal membrane oxygenation (ECMO) in neonatal respiratory failure: 100 cases. Ann Surg 1986;204:236–45.
3. Atkinson JB, Emerson P, Wheaton R, Bowman CM. A simplified method for autoregulation of blood flow in the
THOUGHTS AND PROGRESS 197
Artif Organs, Vol. 27, No. 2, 2003

extracorporeal membrane oxygenation circuit. J Pediatr Surg1989;24:251–2.
4. Green TP, Kriesmer P, Steinhorn RH, Payne NR, Irmiter RJ,Meyer CL. Comparison of pressure-volume-flow relationshipsin centrifugal and roller pump extracorporeal membrane oxy-genation systems for neonates. Trans Am Soc Artif InternOrgans 1991;37:572–6.
5. Snyder EJ, Gross L, Weckerly SP, Velez M, Hopkins J, TackelIS. Clinical involvement of biomedical specialists in neonatalextracorporeal membrane oxygenation (ECMO). BiomedInstrum Technol 1991;25:361–72.
6. Ito T, Takagi H, Seo T. New neonatal and pediatric veno-arterial extracorporeal membrane oxygenation circuit usingautomatically driven blood pumps. Artif Organs 1990;14(Suppl 1):186–8.
7. Seo T, Ito T, Ishiguro Y, Takagi H. New neonatal extracorpo-real membrane oxygenation circuit with self-regulating bloodpump. Surgery 1994;115:463–72.
8. Seo T, Ito T, Iio K, Kato J, Takagi H. Experimental study onthe hemodynamic effects of veno-arterial extracorporealmembrane oxygenation with an automatically driven bloodpump on puppies. Artif Organs 1991;15:402–7.
9. Kato J, Seo T, Ando H, Takagi H, Ito T. Coronary arterial perfusion during venoarterial extracorporeal membrane oxy-genation. J Thorac Cardiovasc Surg 1996;111:630–6.
10. Ito T, Seo T, Ishiguro Y, Takagi H. First clinical application ofan automatic VA-ECMO system using artificial hearts as ablood pump. J Pediatr Surg 1993;28:817–8.
11. Seo T, Ando H, Watanabe Y, Harada T, Ito F, Kaneko K, Mimura S. Acute respiratory failure associated with intrathoracic masses in neonates. J Pediatr Surg 1999;34:1633–7.
12. Takagi H, Takahashi T, Ito T, Ohta K, Tamura M. Long-termcontinuous total left heart bypass without synchronization.Trans Am Soc Artif Intern Organs 1977;23:314–7.
13. Takagi H, Okamoto A, Takamatsu M. New artificial heartwhich operates on Starling’s law. Artif Organs 1991;14(Suppl4):49–51.
14. Ito F, Seo T, Ito T, Umeda T, Ando H, Takagi H. Developmentof an isolated perfusion circuit with double bypass using auto-matic blood pumps. Artif Organs 1995;19:866–9.
15. Seo T, Ando H, Watanabe Y, Ito F, Iino S, Takagi H, Ito T.Biochemical and morphological changes in the liver duringisolated liver perfusion with double bypass using automaticblood pumps. J Pediatr Surg 1997;32:75–9.
16. Zwischenberger JB, Nguyen TT, Upp JR Jr, Bush PE, Cox CSJr, Delosh T, Broemling L. Complications of neonatal extra-corporeal membrane oxygenation. Collective experience fromthe Extracorporeal Life Support Organization. J Thorac Cardiovasc Surg 1994;107:838–49.
17. Shanley CJ, Hirschl RB, Schumacher RE, Overbeck MC,Delosh TN, Chapman RA, Coran AG, Bartlett RH. Extracor-poreal life support for neonatal respiratory failure. A 20-yearexperience. Ann Surg 1994;220:269–82.
18. Setz K, Kesser K, Kopotic RJ, Cornish JD. Comparison of anew venous control device with a bladder box system for usein ECMO. ASAIO J 1992;38:835–40.
19. Durandy Y, Chevalier JY, Lecompte Y. Single-cannula ven-ovenous bypass for respiratory membrane lung support. JThorac Cardiovasc Surg 1990;99:404–9.
20. Chevalier JY, Couprie C, Larroquet M, Renolleau S, DurandyY, Costil J. Venovenous single lumen cannula extracorporeallung support in neonates. A five year experience. ASAIO J1993;39:M654–8.
21. Trittenwein G, Fürst G, Golej J, Frenzel C, Burda G, HermonM, Marx M, Wollenek G, Pollak A. Single needle venovenousextracorporeal membrane oxygenation using a nonocclusiveroller pump for rescue in infants and children. Artif Organs1997;21:793–7.
22. Trittenwein G, Golej J, Burda G, Hermon M, Marx M,Wollenek G, Pansi H, Trittenwein H, Pollak A. Neonatal andpediatric extracorporeal membrane oxygenation using nonoc-clusive blood pumps: The Vienna experience. Artif Organs2001;25:994–9.
23. Dembitsky WP, Moreno-Cabral RJ, Adamson RM, Daily PO.Emergency resuscitation using portable extracorporeal mem-brane oxygenation. Ann Thorac Surg 1993;55:304–9.
24. McDonald JV, Green TP, Steinhorn RH. The role of the cen-trifugal pump in hemolysis during neonatal extracorporealsupport. ASAIO J 1997;43:35–8.
25. Pedersen TH, Videm V, Svennevig JL, Karlsen H, OstbakkRW, Jensen O, Mollnes TE. Extracorporeal membrane oxy-genation using a centrifugal pump and a servo regulator to prevent negative inlet pressure. Ann Thorac Surg 1997;63:1333–9.
26. Nosé Y. Design and development strategy for the rotary bloodpump. Artif Organs 1998;22:438–46.
198 THOUGHTS AND PROGRESS
Artif Organs, Vol. 27, No. 2, 2003
Copyright © 2022 FDOKUMEN