
Impetigo: An Overview
12
CLINICAL AND LABORATORY INVESTIGATIONS Pediatric Dermatology Vol. 11 No. 4 293-303 Impetigo; An O¥erview Gary L. Darmstadt, M.D., and Alfred T. Lane, M.D. Department of Dermatology, Stanford University School of Medicine, Stanford, California Abstract: This article reviews in detail tiie pathogenesis, ciinical char- acteristics and management of impetigo in children. Impetigo is the most common bacterial skin infection of children. Most cases of nonbullous impetigo and al! cases of bulious impetigo are caused by Stapfiy/ococcus aureus. The remainder of cases of nonbullous impetigo are due to group A beta bemoiytic streptococci (GABHS). GABHS colonize tbe skin directly by binding to sites on fibronectin tbat are exposed by trauma. In contrast, S. aureus colonizes the nasal epithelium first; from this reservoir, coloni- zation of the skin occurs. Patients with recurrent impetigo shouid be eval- uated for carriage of S. aureus. Superficial, localized impetigo may be treated successfully in more than 90% of cases with topicai application of mupirocin ointment. Impetigo that is widespread or involves deeper tis- sues should be treated with a beta-lactamase-resistant oral antibiotic. The choice of antibiotics is affected by the local prevalence of resistance to erythromycin among strains of S. aureus, antibiotic cost and availability, and issues of compliance. Skin complaints or findings are noted in 20% to 30% of children who attend general pediatric clinics (Table 1) (1,2). Bacterial skin infection is the single most common diagnosis among those with skin problems, accounting for 17% of all clinic visits. The most common bacterial skin infection of chil- dren is impetigo, which makes up approximately 10% of all skin problems (1,2). PATHOGENESIS In order to understand the pathogenesis of im- petigo, it is essential to appreciate the factors which alter the normal flora of the skin and which promote colonization and infection of the skin with patho- genic bacteria. This subject has recently been re- viewed extensively by Roth and James (3). Resident and Transient Cutaneous Flora Normal skin microflora falls into two broad catego- ries: 1) resident flora which are attached to the skin and are present in relatively stable numbers, and 2) transient flora, which are introduced from the envi- ronment onto exposed skin and lie free on the skin surface, without attachment in the absence of a dis- turbance in the integrity of the skin (3). The most important of the transient bacteria are the group A beta-hemolytic streptococci {Streptococcus pyo- genes; GABHS) and Staphylococcus aureus. Coagulase-negative staphylococci are the most numerous of the resident flora, whereas coagulase- positive S. aureus encounters a high degree of nat- ural resistance to colonization of the skin. Most body sites are free from colonization with S. aureus (4). However, persistent nasal carriage is detected in 20% to 40% of normal adults (5,6), and up to 20% of people may be colonized on the perineum (7). In contrast, patients with atopic dermatitis will yield S. aureus from upwards of 90% of skin lesions and 70% of cultures from nonlesional skin (8,9). Coryneform organisms are lipophilic, pleomor- Address correspondence to Gary L. Darmstadt, M.D., De- partment of Dermatology, Stanford University School of Medi- cine, 900 Blake Wilbur Drive, Palo Alto, CA 94304. 293
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Impetigo: An Overview
CLINICAL AND LABORATORY INVESTIGATIONS
Pediatric Dermatology Vol. 11 No. 4 293-303
Impetigo; An O¥erview
Gary L. Darmstadt, M.D., and Alfred T. Lane, M.D.
Department of Dermatology, Stanford University School of Medicine, Stanford, California
Abstract: This article reviews in detail tiie pathogenesis, ciinical char-acteristics and management of impetigo in children. Impetigo is the mostcommon bacterial skin infection of children. Most cases of nonbullousimpetigo and al! cases of bulious impetigo are caused by Stapfiy/ococcusaureus. The remainder of cases of nonbullous impetigo are due to groupA beta bemoiytic streptococci (GABHS). GABHS colonize tbe skin directlyby binding to sites on fibronectin tbat are exposed by trauma. In contrast,S. aureus colonizes the nasal epithelium first; from this reservoir, coloni-zation of the skin occurs. Patients with recurrent impetigo shouid be eval-uated for carriage of S. aureus. Superficial, localized impetigo may betreated successfully in more than 90% of cases with topicai application ofmupirocin ointment. Impetigo that is widespread or involves deeper tis-sues should be treated with a beta-lactamase-resistant oral antibiotic. Thechoice of antibiotics is affected by the local prevalence of resistance toerythromycin among strains of S. aureus, antibiotic cost and availability,and issues of compliance.
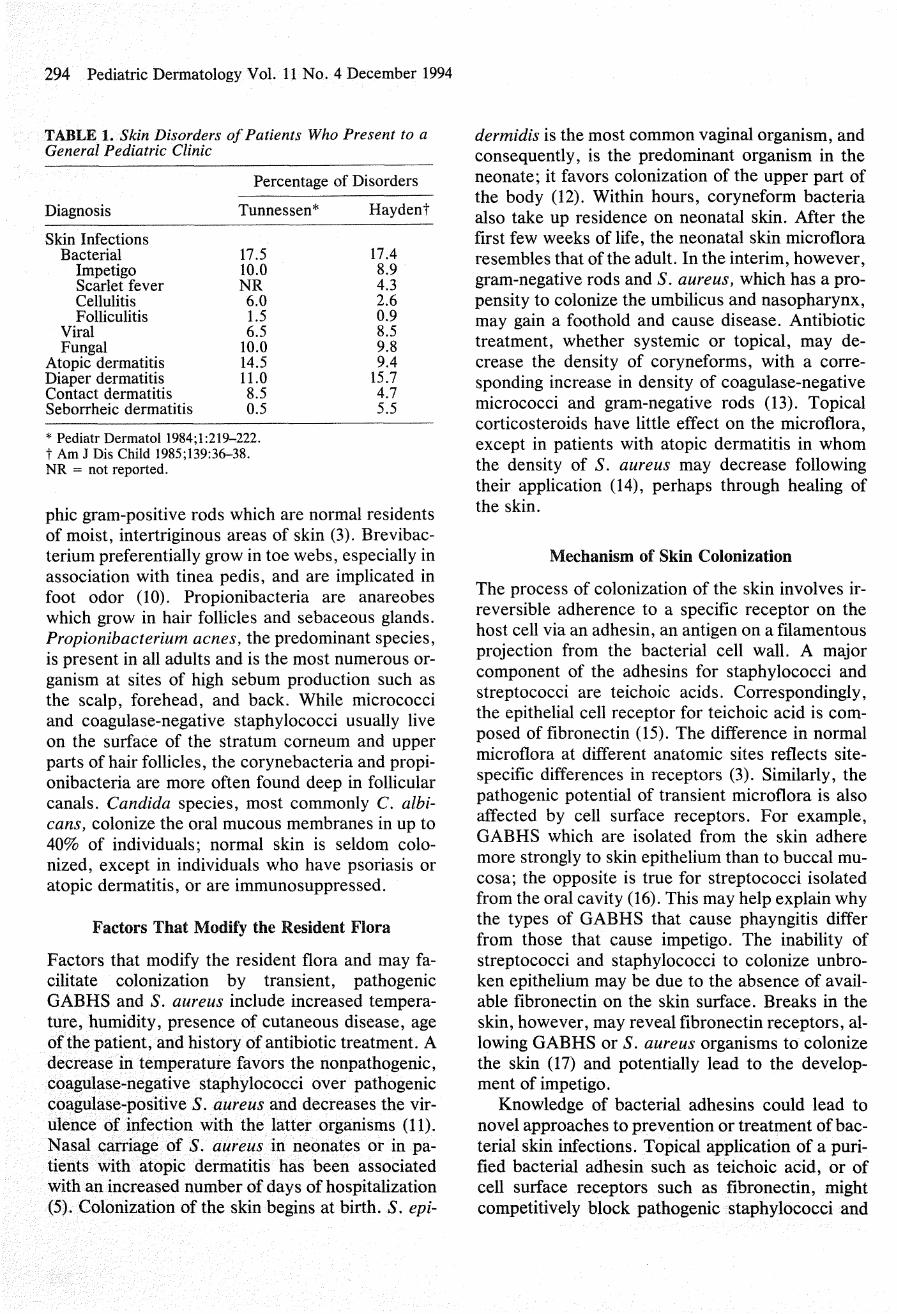
Skin complaints or findings are noted in 20% to30% of children who attend general pediatric clinics(Table 1) (1,2). Bacterial skin infection is the singlemost common diagnosis among those with skinproblems, accounting for 17% of all clinic visits.The most common bacterial skin infection of chil-dren is impetigo, which makes up approximately10% of all skin problems (1,2).
PATHOGENESIS
In order to understand the pathogenesis of im-petigo, it is essential to appreciate the factors whichalter the normal flora of the skin and which promotecolonization and infection of the skin with patho-genic bacteria. This subject has recently been re-viewed extensively by Roth and James (3).
Resident and Transient Cutaneous Flora
Normal skin microflora falls into two broad catego-ries: 1) resident flora which are attached to the skin
and are present in relatively stable numbers, and 2)transient flora, which are introduced from the envi-ronment onto exposed skin and lie free on the skinsurface, without attachment in the absence of a dis-turbance in the integrity of the skin (3). The mostimportant of the transient bacteria are the group Abeta-hemolytic streptococci {Streptococcus pyo-genes; GABHS) and Staphylococcus aureus.
Coagulase-negative staphylococci are the mostnumerous of the resident flora, whereas coagulase-positive S. aureus encounters a high degree of nat-ural resistance to colonization of the skin. Mostbody sites are free from colonization with S. aureus(4). However, persistent nasal carriage is detectedin 20% to 40% of normal adults (5,6), and up to 20%of people may be colonized on the perineum (7). Incontrast, patients with atopic dermatitis will yieldS. aureus from upwards of 90% of skin lesions and70% of cultures from nonlesional skin (8,9).
Coryneform organisms are lipophilic, pleomor-
Address correspondence to Gary L. Darmstadt, M.D., De-partment of Dermatology, Stanford University School of Medi-cine, 900 Blake Wilbur Drive, Palo Alto, CA 94304.
293
294 Pediatric Dermatology Vol. 11 No. 4 December 1994
TABLE 1. Skin Disorders of Patients Who Present to aGeneral Pediatric Clinic
Percentage of Disorders
Diagnosis
Skin InfectionsBacterial
ImpetigoScarlet feverCellulitisFolliculitis
ViralFungal
Atopic dermatitisDiaper dermatitisContact dermatitisSeborrheic dermatitis
Tunnessen*
17.510.0NR6.01.56.5
10.014.511.08.50.5
Hay dent
17.48.94.32.60.98.59.89.4
15.74.75.5
* Pediatr Dermatol 1984;l:219-.222.t Am J Dis Child 1985;139:36-38.NR = not reported.
phic gram-positive rods which are normal residentsof moist, intertriginous areas of skin (3). Brevibac-terium preferentially grow in toe webs, especially inassociatioti with tinea pedis, atid are implicated infoot odor (10). Propionibacteria are anareobeswhich grow in hair follicles and sebaceous glands.Propionibacterium acnes, the predominant species,is present iti all adults and is the most numerous or-ganism at sites of high sebum production such asthe scalp, forehead, and back. While micrococciand coagulase-negative staphylococci usually liveon the surface of the stratum corneum and upperparts of hair follicles, the corynebacteria and propi-otiibacteria are more often found deep in follicularcanals. Candida species, most commonly C. albi-cans, colonize the oral mucous membranes in up to40% of individuals; normal skin is seldom colo-nized, except in individuals who have psoriasis oratopic dermatitis, or are immunosuppressed.
Factors That Modify the Resident Flora
Factors that modify the resident flora and may fa-cilitate colonization by transient, pathogenicGABHS and S. aureus include increased tempera-ture, humidity, presence of cutaneous disease, ageof the patient, and history of antibiotic treatment. Adecrease in temperature favors the nonpathogenic,coagulase-negative staphylococci over pathogeniccoagulase-positive S. aureus and decreases the vir-ulence of infection with the latter organisms (11).Nasal carriage of S. aureus in neonates or in pa-tients with atopic dermatitis has been associatedwith an increased number of days of hospitalization(5). Colonization of the skin begins at birth. S. epi-
dermidis is the most common vaginal organism, andconsequently, is the predominant organism in theneonate; it favors colonization of the upper part ofthe body (12). Within hours, coryneform bacteriaalso take up residence on neonatal skin. After thefirst few weeks of life, the neonatal skin microfloraresembles that of the adult. In the interim, however,gram-negative rods and S. aureus, which has a pro-pensity to colonize the umbilicus and nasopharynx,may gain a foothold and cause disease. Antibiotictreatment, whether systemic or topical, may de-crease the density of coryneforms, with a corre-sponding increase in density of coagulase-negativemicrococci and gram-negative rods (13). Topicalcorticosteroids have little effect on the microflora,except in patients with atopic dermatitis in whomthe density of S. aureus may decrease followingtheir application (14), perhaps through healing ofthe skin.
Mechanism of Skin Colonization
The process of colonization of the skin involves ir-reversible adherence to a specific receptor on thehost cell via an adhesin, an antigen on a filamentousprojection from the bacterial cell wall. A majorcomponent of the adhesins for staphylococci andstreptococci are teichoic acids. Correspondingly,the epithelial cell receptor for teichoic acid is com-posed of fibronectin (15). The difference in normalmicrofiora at different anatomic sites reflects site-specific differences in receptors (3). Similarly, thepathogenic potential of transient microflora is alsoaffected by cell surface receptors. For example,GABHS which are isolated from the skin adheremore strongly to skin epithelium than to buccal mu-cosa; the opposite is true for streptococci isolatedfrom the oral cavity (16). This may help explain whythe types of GABHS that cause phayngitis differfrom those that cause impetigo. The inability ofstreptococci and staphylococci to colonize unbro-ken epithelium may be due to the absence of avail-able fibronectin on the skin surface. Breaks in theskin, however, may reveal fibronectin receptors, al-lowing GABHS or S. aureus organisms to colonizethe skin (17) and potentially lead to the develop-ment of impetigo.
Knowledge of bacterial adhesins could lead tonovel approaches to prevention or treatment of bac-terial skin infections. Topical application of a puri-fied bacterial adhesin such as teichoic acid, or ofcell surface receptors such as fibronectin, mightcompetitively block pathogenic staphylococci and

Darmstadt and Lane: Impetigo 295
streptococci from adhering to the skin (18,19).Competitive binding to cell surface receptors byresident flora or transient flora of low virulence mayalso prevent pathogenic bacteria from colonizingthe skin. A nonvirulent strain of 5. aureus has beenuseful in neonates during nursery epidemics to pre-vent colonization of the nasal mucosa with a patho-genic strain of S. aureus (20), and in adults to pre-vent spread of recurrent staphylococcal abscesseswithin families (21).
Defenses Against Colonization byPathogenic Bacteria
Once a pathogenic bacteria has adhered to the skin,it must overcome several avenues of host defensebefore itifection can develop. Intact stratum cor-neum provides the first and foremost mechanism ofdefense. Cells of the stratum corneum overlap, andare tightly adherent, providing a mechanical bar-rier. In addition, the stratum corneum turns over anaverage of every 14 days, favoring the readherenceof resident flora over the relatively weakly adherentpathogenic microflora. To overcome this barrier,staphylococci have been observed to advance be-tween corneocytes, through intercellular spaces(22). Likewise, S. aureus has a predilection for en-tering the skin at appendageal structures (3).
Breakdown products of the stratum corneum, in-cluding free fatty acids, polar lipids, and gly-cosphingolipids, have antistaphylococcal and an-tistreptococcal activity (22). Many of the residentflora, particularly the lipophilic corynebacteria,have Upases, and thus contribute to defense againstGABHS and S. aureus by liberating fatty acids fromthe triglycerides of sebum (23). The acid mantlethus created favors growth of propionibacteria,which in turn produce propionic acid; this com-pound has relatively more antimicrobial activityagainst organisms than against resident flora.
Humoral immunity may aid in defense against in-fection through secretion of IgA in sweat. The cel-lular immune system, including antigen presenta-tion by epidermal Langerhans cells, plays animportant role in defending from infection, as evi-denced by patients with defects in cellular immunitysuch as mucocutaneous candidiasis and chronicgranulomatous disease who have increased suscep-tibility to cutaneous infection.
A mechanism whereby a given organism can gainan advantage over others is through the productionof antibiotics which harm other organisms but notthe producer of the substance. Gram-negative bac-
teria tend to produce substances with a wide-spectrum of activity, whereas the substances se-creted by gram-positive organisms tend to affectonly the same or closely related species of bacteria.These narrow-spectrum substances are called bac-teriocins (24). Bacteriocin producers, including S.aureus, tend to increase in number and become thepredominant species when the skin is damaged (25).
As expected, based on the above review of fac-tors which modify the balance of skin flora, condi-tions that favor development of impetigo includewarm ambient temperature, humidity, preexistingdermatitis such as atopic dermatitis or tinea capitis,crowded living conditions, and poor hygiene.
CLINICAL CHARACTERISTICS
Nonbullous Impetigo
There are two classic forms of impetigo: nonbullousand bullous. Nonbullous impetigo accounts formore than 70% of cases of impetigo (26-31). Le-sions of nonbullous impetigo typically begin on skinof the face or extremities which has been trauma-tized; intact skin is resistent to impetiginization oreven colonization (32), perhaps due to unavailabil-ity of fibronectin receptors for teichoic acid moitieson GABHS and S. aureus organisms. The mostcommon lesions which precede nonbullous im-petigo include chickenpox, insect bites, abrasions,lacerations, and burns. A tiny vesicle or pustuleforms initially and rapidly develops a honey-colored, crusted plaque which is generally less than2 cm in diameter. Lesions are associated with littleto no pain or surrounding erythema, and constitu-tional symptoms are generally absent. Pruritis oc-curs occasionally, regional adenopathy is found inup to 90% of cases (29,33), and leukocytosis ispresent in approximately 50% of patients (34).Without treatment, lesions may progress slowly forseveral weeks and occasionally may form a chroniculcer, but in most cases will resolve spontaneouslywithout scarring within approximately two weeks(35). The differential diagnosis of nonbullous im-petigo includes viral (herpes simplex, varicellazoster), fungal (tinea corporis, kerion), and para-sitic infections (scabies, pediculosis capitis), all ofwhich may become impetiginized secondarily (36).
From the 1940s to the mid 1960s, nonbullous im-petigo in the United States was primarily of staphy-lococcal origin (27,36). During the later 1960s andthe 1970s, GABHS became the predominant patho-genic organism. Prospective studies of impetigo inan endemic area, the Red Lake Indian reservation

296 Pediatric Dermatology Vol. 11 No. 4 December 1994
of Minnesota, during 1969 demonstrated that earlylesions of nonbullous impetigo more commonlygrew pure cultures of GABHS (36%) than S. aureus(9%); GABHS more commonly outlasted staphylo-cocci in mixed lesions which were cultured sequen-tially; and while the same strain of GABHS per-sisted in 85% of sequentially cultured lesions duringan average time of 12.6 days to spontaneous heal-ing, the strain of staphylococcus changed in 57% oflesions (35). Unlike today, the clinical response ofnonbullous impetigo to penicillin was found to bethe same, regardless of whether culture of the lesiongrew pure GABHS as opposed to either mixedGABHS and penicillin-resistant staphylococci (37),or pure penicillin-resistant staphylococci (38). Apossible explanation for this finding was that S. au-reus produced a bacteriocin, which interfered withgrowth of GABHS in culture (39).
Studies during the 1960s also clarified the differ-ing natural history of GABHS and staphylococci inlesions of nonbullous impetigo. In 21 of 31 (70%)cases of impetigo in Red Lake Native Americanchildren, the skin became colonized with GABHSan average of 10 days before development of im-petigo; in approximately 74% of episodes, the sameserotype was recovered from normal skin and thesubsequent lesion of impetigo (40). After gaining afoothold in the skin, GABHS then colonized the na-sopharynx; in 74% of episodes of impetigo, thesame strain of GABHS was recovered from thenose and throat an average of 15 and 20 days, re-spectively, after the appearance of lesions of im-petigo. Among family contacts, streptococcal skininfection developed without going through interme-diate respiratory colonization or infection. Routinecultures of normal skin of the wrist, ankle, and backwere three times more likely to be positive forGABHS (31% of 4021 cultures) than cultures fromthe nose (11% positive) or throat (10% positive)(40). These data suggest that the upper respiratorytract does not serve as t;he reservoir for infection ofthe skin with GABHS, but vice versa (40,41).
In contrast to streptococci, staphylococci gener-ally spread from the nose to normal skin, andthence are able to infect the skin (29,35). Among 31patients with bullous impetigo, 19 (61%) had con-current impetigo and a positive staphylococcal cul-ture from the nose or throat; 79% of cultures grewthe same strain from both sites (29). At the RedLake Indian Reservation, a single strain of Staphy-lococcus, phage type 75, accounted for the majorityof staphylococcal isolates from the respiratory tract
(56%), normal skin (68%), and skin lesions (58%) of37 children (35).
During the early 1980s S. aureus again becamethe predominant organism of nonbullous impetigoin the United States (42). Staphylococci can now becultured from approximately 80% or more of lesionsof impetigo of most populations, and is the solepathogen in approximately 50% to 60% of cases (3,27,30,31,43,44). Furthermore, several recent stud-ies have demonstrated that treatment regimenswhich utilize antistaphylococcal agents now pro-duce cure rates superior to those regimens whichemploy beta-lactamase sensitive antibiotics.
Lesions of nonbullous impetigo which growstaphylococci in culture cannot be distinguishedclinically from those which grow pure cultures ofGABHS (26,29,30,42). Whereas S. aureus can becultured from lesions of impetigo on children of allages, GABHS is most common in children of pre-school age and is unusual before 2 years of age ex-cept in highly endemic areas (36,45).
The staphylococcal types which cause nonbul-lous impetigo are variable and are from phage group2, which is associated with scalded skin and toxicshock syndromes, in the minority of cases (29).Several serotypes of GABHS, termed "impetigostrains," are found most frequently in lesions ofnonbullous impetigo (41) and are different fromthose that cause pharyngitis. The risk of developingimpetigo following colonization with GABHS var-ies with the specific serotype (40).
Bullous Impetigo
Bullous impetigo is always caused by coagulase-positive S. aureus; approximately 80% are fromphage group 2, 60% are type 71, and most of theremainder are types 3A, 3B, 3C, and 55 (29,46).Flaccid, transparent buUae develop most commonlyon skin of the face, buttocks, trunk, perineum, andextremities (27,29). Rupture of bullae occurs easily,leaving a narrow rim of scale at the edge of a shal-low, moist erosion (29). Surrounding erythema andregional adenopathy are generally absent.
Unlike nonbullous impetigo, lesions of bullousimpetigo are a manifestation of localized staphylo-coccal scalded skin syndrome (SSSS) and thereforedevelop on intact skin. When S. aureus of phagegroup 2 were injected into newborn mice, a gener-alized exfoliative erythroderma developed, regard-less of whether the 5. aureus organisms had beenisolated from lesions of patients with buUous im-petigo or SSSS (47).
Darmstadt and Lane: Impetigo 297
fflSTOPATHOLOGY
On histopathologic examination, lesions of bullousimpetigo show vesicle formation in the subcornealor granular region, occasional acantholytic cellswithin the bhster, spongiosis, edema of the papil-lary dermis, and a mixed infiltrate of lymphocytesand neutrophils around blood vessels of the super-ficial plexus. Neutrophils are generally visiblewithin the blister cavity. Unless staphylococci canbe cultured from the bullae or, less commonly, canbe seen on gram stain, it may be impossible to dif-ferentiate bullous impetigo from pemphigus folia-ceus histopathologically. Pemphigus foliaceus tendsto have more acantholysis and fewer neutrophilswithin the subcorneal blister and may have dyskera-totic changes in cells of the granular layer (48). Clin-ically, pemphigus folliaceus differs from impetigo inits presentation with multiple small fiaccid blisterswhich easily rupture, leaving erythematous, crustederosions. Subcorneal pustular dermatosis may alsobe indistinguishable, histopathologically, from im-petigo, but its clinical presentation is that of cropsof grouped pustules in a serpiginous outline, gener-ally on the abdomen or in the axillary and inguinalfolds, sparing the face. Nonbullous impetigo hashistopathologic findings similar to the bullous vari-ant, except that blister formation is slight.
The differential diagnosis of bullous impetigoalso includes allergic contact dermatitis, bullouspemphigoid, burns, dermatitis herpetiformis, anderythema multiforme. Although these conditionsare histopathologically distinct from impetigo, eachmay become impetiginized secondarily.
COMPLICATIONS
Potential complications of either nonbullous or bul-lous impetigo include osteomyelitis, septic arthritis,pneumonia, and septicemia (29). Positive blood cul-tures are rare, but are more common with skin thanrespiratory infection with GABHS (46). Cellulitishas been reported in approximately 10% of patientswith nonbullous impetigo, but rarely follows thebullous form (29). Lymphangitis, suppurative lym-phadenitis, guttate psoriasis, and scarlet fever mayfollow streptococcal disease occasionally. There isno correlation between number of lesions and clini-cal involvement of the lymphatics or developmentof cellulitis in association with streptococcal im-petigo (29).
Infection with nephritogenic strains of GABHSmay result in acute poststreptococcal glomerolone-
phritis (APSGN). The clinical character of impetigolesions is not different between those that lead toAPSGN and those that do not (29,33). Fewer than5% of patients with APSGN are less than 2 years ofage; it most commonly affects those 3 to 7 yearsold. The latent period from onset of impetigo to de-velopment of APSGN averages 18 to 21 days, whichis longer than the 10-day latency period followingpharyngitis (41,49).
APSGN occurs sporadically, due primarily to Mtype 12 infection of the pharynx, and epidemicallyfollowing either pharyngeal or skin infection.Impetigo-associated epidemics are caused by Mgroups 2, 49, 53, 55, 56, 57, and 60 (41,49), whereasM groups 1 and 12 are most often associated withAPSGN following pharyngitis. M types 1 and 12 arerarely isolated from lesions of impetigo.
The most common site of GABHS infectionwhich results in APSGN varies according to geo-graphic location. While 76% of symptomaticAPSGN in children in Chicago was associated withupper respiratory tract infection (50), 40% to 80% ofepisodes of APSGN in children in the southeast fol-lowed impetigo (41,51,52). In general, since the1960s APSGN in the United States has appearedmore frequently following pharyngitis than impetigo(53).
The true incidence of APSGN is difficult to de-termine, as many mild or subclinical cases go unde-tected. A prospective study of 248 children withstreptococcal infection demonstrated that 22% de-veloped asymptomatic urinary abnormalities, a lowserum C3 concentration, or both (54). The risk ofnephritis after impetigo varies widely with the strainof GABHS. During an epidemic of acute nephritisdue to M group 49 GABHS, 24% of children withstreptococcal impetigo developed acute nephritis orunexplained hematuria; the risk was highest in chil-dren less than 6V2 years of age (43%) (55). Multiplesubclinical and clinical cases of nephritis often oc-cur within a family (41). Strains of GABHS whichare associated with endemic impetigo in the UnitedStates have little or no nephritogenic potential (55).There have been no cases of glomerulonephritisamong the more than 500 patients from trials whichcompared the efficacy of erythromycin and mupiro-cin treatments (28,30,31,43,44,56,57).
IMMUNE RESPONSE TOSTREPTOCOCCAL IMPETIGO
Anti-DNAase B is the test of choice for detectingpreceding streptococcal impetigo. Of patients with
298 Pediatric Dermatology Vol. 11 No. 4 December 1994
uncomplicated impetigo and impetigo-associatedAPSGN, 67% and 92%, respectively, had elevatedantideoxyribonuclease B (anti-DNAase B) titers(33). After an episode of nonbullous impetigocaused by GABHS, the antistreptolysin O responseis slight or absent, perhaps due to binding of strep-tolysin O by lipids, including cholesterol, in the skin(58). In one study, 43% and 51% of patients withuncomplicated impetigo and impetigo-associatedAPSGN, respectively, developed an elevated ASOtiter. The anti-DNAase B response is greater afterimpetigo than after pharyngitis, whereas the ASOtiter is more highly elevated following pharyngitis(49). The antihyaluronidase test is also thought tobe superior to the ASO test in documenting a pre-ceding streptococcal skin infection (59). The strep-tozyme test measures more than five antibodies tostreptococcal antigens, including ASO, anti-DNAase B, and antihyaluronidase. When only oneof the antibodies is minimally elevated, however,false negative results may be obtained (60). In addi-tion, the combination of individual ASO and anti-DNAase B tests is more effective than the strep-tozyme test in detecting preceding GABHSinfection (61). Treatment, whether systemic or top-ical, in cases of APSGN following impetigo, doesnot prevent the development of APSGN in the in-dex case (36,62), but may prevent spread of im-petigo to others and thus reduce the incidence ofAPSGN in the community. Acute rheumatic feverdoes not occur as a result of impetigo.
TREATMENT
Several studies have demonstrated that topical(neomycin, bacitracin, polysporin, gentamicin, ormixtures of these) or systemic antibiotic treatmentis superior to placebo or cleansing with 3% hexa-chlorophene soap (63). Furthermore, cleansing with3% hexachlorophene soap adds little to no benefitover systemic antibiotics alone (36). Until the intro-duction of mupirocin (Bactroban), topical antibiot-ics were inferior to systemic antibiotics (64,65).
Factors to consider when selecting the optimalantibiotic for treatment of impetigo include ease ofuse, low potential for adverse reactions, delivery ofa high concentration of drug to the site of infection,low risk for development of bacterial resistance orcross resistance to other agents, chemical structureand mechanism of action which is unrelated to otherantibiotics, activity against common bacterial skinpathogens (i.e., GABHS, 5. aureus, includingmethicillin resistant and beta-lactamase producing
strains), utility as a single agent, lack of alteration ofresident skin and gut fiora, and competitive price.
Topical Antibiotics
Mupirocin is produced during fermentation byPseudomonas fluorescens. It was first introduced inthe United Kingdom in 1985. Its chemical structureis unique among antibiotics, and it is highly unlikelyto cause photoreactions because the wavelength ofultraviolet light which it is capable of absorbing tothe greatest degree (222 nm) never reaches theearth's surface, but rather is filtered out by theozone layer (66). Mupirocin is bactericidal at theconcentration achieved following topical applica-tion and is not absorbed systemically. Even whenadministered systemically, however, mupirocin isconverted rapidly to an inactive metabolite (67).Therefore, side effects from mupirocin, especiallycontact hypersensitivity, appear to be due to thepolyethylene glycol vehicle rather than the activeingredient (67). Mupirocin's mode of action is thereversible inhibition of bacterial isoleucyl-tRNAsynthetase; it has a relatively low affinity for mam-malian isoleucyl-tRNA synthetase. Micrococcusspp., coryneforms, and propionibacteria are lesssensitive than GABHS or S. aureus to mupirocin(68); thus, the natural skin flora is left relatively un-disturbed. Rare instances of bacterial resistance tomupirocin have been reported (68,69). Coagulase-negative staphylococci, 5. aureus, and GABHS arethought to share a common antibiotic resistancegene pool, which theoretically could be transferredfrom the resident fiora, particularly 5. epidermidis,to pathogens during infections (68,69). Most pa-tients who have demonstrated resistance to mupiro-cin have been treated irregularly and/or prophylac-tically for prolonged periods of time (more than twoweeks).
Several studies have demonstrated that mupiro-cin applied three times daily for 7 to 10 days is equalto or greater in effectiveness than oral erythromycinethylsuccinate 30 to 50 mg/kg/day for 7 to 10 daysfor treatment of impetigo in children (30,31,43,44,56,57). Treatment success rate with mupirocin wasgreater than 90%, regardless of whether the lengthof treatment was 7, 8, or 10 days. There were fewerside effects of treatment (30,31,43,56), in somecases lesions cleared more rapidly, and the rate oferradication of pyogenic bacteria was equivalent(28) or greater (30,57) in those treated with topicalmupirocin compared with systemic erythromycin.A cost-effectiveness analysis evaluated the total
Darmstadt and Lane: Impetigo 299
cost, including physician fees, transportation ex-penses, and cost of the medication for a 10-daycourse of treatment with mupirocin compared witherythromycin ethylsuccinate. Although the cost oftreatment was significantly greater for mupirocin($62.30) than for erythromycin ($56.85), this extracost was offset by increased side effects (43% vs22%) and number of schooldays (3.0 vs 1.2) andworkdays (0.5 vs 0.2) missed in the group treatedwith erythromycin (28).
Studies which have compared the effectivenessof mupirocin with erythromycin have generally re-stricted their patient population to those with super-ficial, localized primary pyoderma. Low-grade fe-ver (31,56) and regional adenopathy (31), however,are not absolute contraindications to treatment withmupirocin. Lesions around the mouth should prob-ably not be treated with mupirocin, as the medica-tion may be licked off (30).
A patient with recurrent impetigo should be eval-uated for S. aureus carriage. Colonization of thenares, via teichoic acid adhesins (70), correlateswith carriage at other sites such as the perineum(71) and the axillae, but screening for nasal carriagealone may miss approximately one-fourth of carri-ers (72). The first clinical trial of mupirocin for elim-ination of nasal carriage of 5. aureus demonstratedthat application of mupirocin four times daily forfive days to the anterior nares eliminated nasal car-riage within two days in all 32 patients (73).Coagulase-negative staphylococci and coryneformsbecame the dominant nasal flora, and may havecontributed to prevention of reaquisition of S. au-reus by the mechanism of bacterial interference(74); there was no overgrowth of gram-negative or-ganisms (73). Twenty-two weeks after therapy,however, half of the patients were recolonized withS. aureus; 29% reacquired the same phage type(73). Several studies have reproduced these results,showing elimination of nasal carriage of methicillin-sensitive and methicillin-resistant S. aureus(MRSA) from greater than 90% of patients withintwo to four days (75,76). In time, however, mea-sured in weeks to months, the nares become recol-onized. Mupirocin is better tolerated intranasallywhen formulated as a calcium ointment than as Bac-troban, which utilizes polyethylene glycol as the ve-hicle (75,77). Calcium mupirocin ointment, how-ever, is not currently available in the United States.Although rates of staphylococcal infection havebeen reduced in patients with atopic dermatitis (78)and those on hemodialysis (79) following elimina-tion of nasal carriage, it is recommended that use of
mupirocin for elimination of nasal carriage be re-served for outbreaks, primarily when MRSA is in-volved (76,80), to minimize the emergence of resis-tant strains of S. aureus. Consideration should alsobe given to using mupirocin intranasally for thosewith recurrent impetigo, particularly if the phagetypes which are cultured from the nares and lesionsof impetigo are identical repeatedly.
Systemic Oral Antibiotics
PenicillinsThe majority of strains of S. aureus isolated fromlesions of impetigo in various areas of the UnitedStates are resistant to penicillin or amoxicillin (26,27,31,57), resulting in treatment failure rates of one-fourth or more (26,27,42). Given that lesions of non-bullous impetigo due to GABHS or S. aureuscannot be distinguished clinically (26,29,30,42),treatment with penicillin or amoxicillin is no longerappropriate (81). Adding clavulanic acid, a beta-lactamase inhibitor, to amoxicillin significantly im-proved the efficacy of amoxicillin from a 20% fail-ure rate to no failures (82). In two studies,amoxicillin (20 [83] or 25 [84] mg/kg/day given TIDfor 10 days) plus clavulanic acid (Augmentin) wascompared with cefaclor (20 mg/kg/day given TIDfor 10 days) for treatment of impetigo in children.Augmentin produced an equivalent rate of clinicalcure (89% [83] or 86% [84] for Augmentin versus81% [83] or 90% [84] for cefaclor) but a superior rateof bacteriologic cure (86% [83] or 100% [84] forAugmentin versus 33% [83] or 90% [84] for ce-faclor). Treatment with cloxacillin resulted in a100% cure rate among 33 children with impetigo(85).
CephalosporinsThe first generation cephalosporin, cephalexin (40to 50 mg/kg/day for 10 days) produced more rapid(21 to 23 patients cured within three to five days)clearing of lesions of impetigo than did erythromy-cin estolate (30 to 40 mg^g/day for 10 days; 16 of 25patients cured within three to five days), but thecure rate at the end of 10 days of treatment wasequivalent (100% for cephalexin versus 94% forerythromycin) (26).
Cefprozil (Cefzil) is a second generation cephalo-sporin which has greater in vitro activity thancefaclor or cephalexin against GABHS andmethicillin-susceptible 5. aureus (86). Cefprozil (20mg/kg once daily), cefaclor (20 mg/kg divided threetimes daily), or erythromycin ethylsuccinate (30mg/kg/d divided four times daily), each given for 5
300 Pediatric Dermatology Vol. 11 No. 4 December 1994
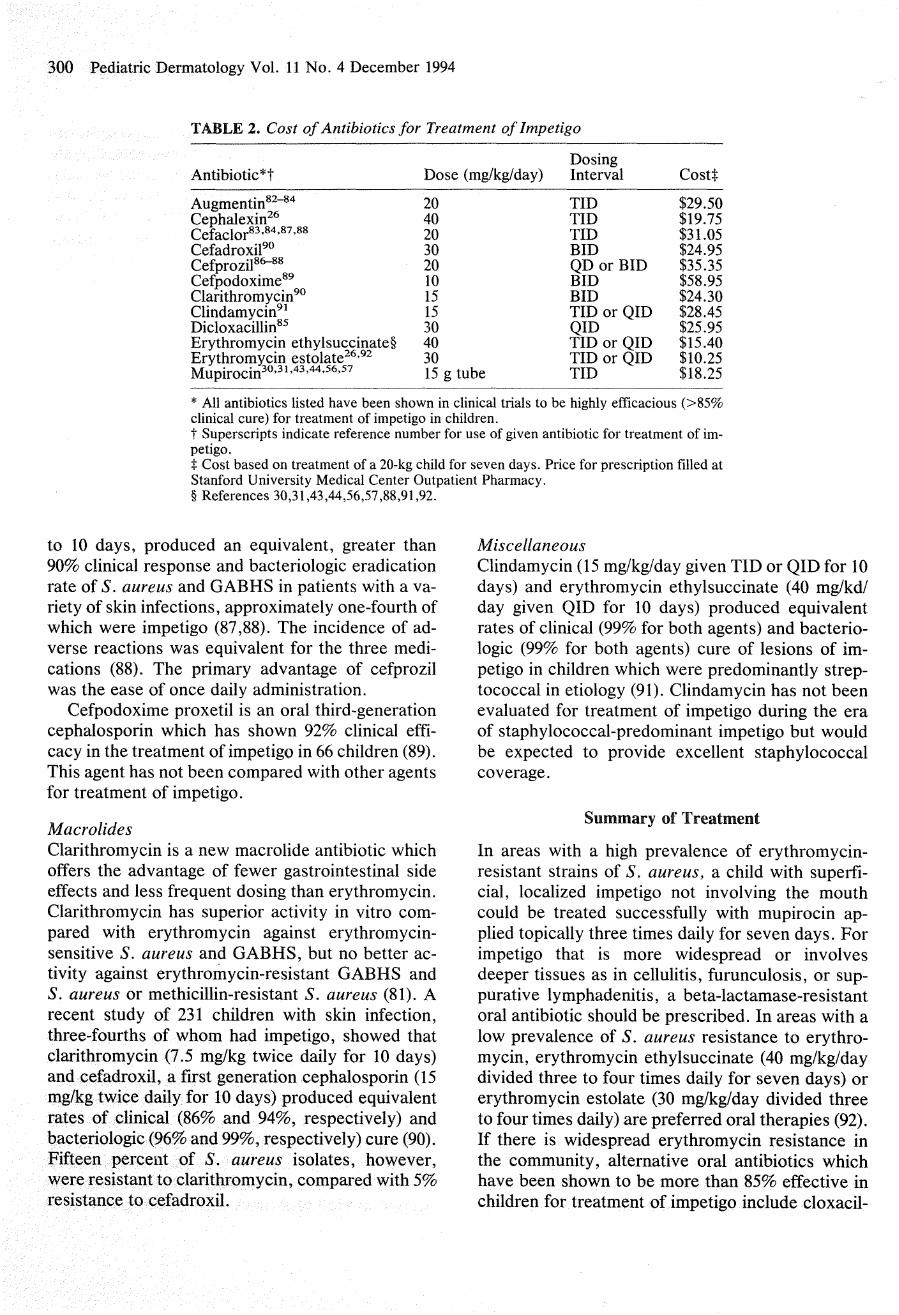
TABLE 2. Cost of Antibiotics for Treatment of Impetigo
Antibiotic*t
Augmentin*^^" '̂*Cephalexin^^Cefador«3-« '̂« '̂««CefadroxiP^Cefprozil«^«Cefpodoxime^^Clarithromycin^^Clindamycin^'Dicloxacillin^^Erythromycin ethylsuccinate§Erythromycin estolate^^-^^Mupirocin^"'^^'^^'^^'^*-"
Dose (mg/kg/day)
204020302010151530403015 g tube
DosingInterval
TIDTIDTIDBIDQD or BIDBIDBIDTID or QIDQIDTID or QIDTID or QIDTID
Costt
$29.50$19.75$31.05$24.95$35.35$58.95$24.30$28.45$25.95$15.40$10.25$18.25
* All antibiotics listed have been shown in clinical trials to be highly efficacious (>85%clinical cure) for treatment of impetigo in children.t Superscripts indicate reference number for use of given antibiotic for treatment of im-petigo.X Cost based on treatment of a 20-kg child for seven days. Price for prescription filled atStanford University Medical Center Outpatient Pharmacy.§ References 30,31,43,44,56,57,88,91,92.
to 10 days, produced an equivalent, greater than90% clinical response and bacteriologic eradicationrate of 5. aureus and GABHS in patients with a va-riety of skin infections, approximately one-fourth ofwhich were impetigo (87,88). The incidence of ad-verse reactions was equivalent for the three medi-cations (88). The primary advantage of cefprozilwas the ease of once daily administration.
Cefpodoxime proxetil is an oral third-generationcephalosporin which has shown 92% clinical effi-cacy in the treatment of impetigo in 66 children (89).This agent has not been compared with other agentsfor treatment of impetigo.
MacrolidesClarithromycin is a new macrolide antibiotic whichoffers the advantage of fewer gastrointestinal sideeffects and less frequent dosing than erythromycin.Clarithromycin has superior activity in vitro com-pared with erythromycin against erythromycin-sensitive S. aureus and GABHS, but no better ac-tivity against erythromycin-resistant GABHS andS. aureus or methicillin-resistant 5. aureus (81). Arecent study of 231 children with skin infection,three-fourths of whom had impetigo, showed thatclarithromycin (7.5 mg/kg twice daily for 10 days)and cefadroxil, a first generation cephalosporin (15mg/kg twice daily for 10 days) produced equivalentrates of clinical (86% and 94%, respectively) andbacteriologic (96% and 99%, respectively) cure (90).Fifteen percent of 5. aureus isolates, however,were resistant to clarithromycin, compared with 5%resistance to cefadroxil.
MiscellaneousClindamycin (15 mg/kg/day given TID or QID for 10days) and erythromycin ethylsuccinate (40 mg/kd/day given QID for 10 days) produced equivalentrates of clinical (99% for both agents) and bacterio-logic (99% for both agents) cure of lesions of im-petigo in children which were predominantly strep-tococcal in etiology (91). Clindamycin has not beenevaluated for treatment of impetigo during the eraof staphylococcal-predominant impetigo but wouldbe expected to provide excellent staphylococcalcoverage.
Summary of Treatment
In areas with a high prevalence of erythromycin-resistant strains of S. aureus, a child with superfi-cial, localized impetigo not involving the mouthcould be treated successfully with mupirocin ap-plied topically three times daily for seven days. Forimpetigo that is more widespread or involvesdeeper tissues as in cellulitis, furunculosis, or sup-purative lymphadenitis, a beta-lactamase-resistantoral antibiotic should be prescribed. In areas with alow prevalence of S. aureus resistance to erythro-mycin, erythromycin ethylsuccinate (40 mg/kg/daydivided three to four times daily for seven days) orerythromycin estolate (30 mg/kg/day divided threeto four times daily) are preferred oral therapies (92).If there is widespread erythromycin resistance inthe community, alternative oral antibiotics whichhave been shown to be more than 85% effective inchildren for treatment of impetigo include cloxacil-
Darmstadt and Lane: Impetigo 301
lin; amoxicillin plus clavulanic acid; clindamycin;or a cephalosporin such as cephalexin, cefaclor, ce-fadroxil, cefprozil, or cefpodoxime. The choiceamong these various agents may be guided primari-ly by issues of cost (Table 2), local availability, andcompliance. Clarithromycin may be advantageousprimarily in instances of intolerance to erythromy-cin, but would not be expected to provide cure ratessuperior to erythromycin in areas with high rates ofS. aureus resistance to erythromycin.
There is little evidence to suggest that a 10-daycourse of therapy is superior to 7-day course. If asatisfactory clinical response is not achieved withinseven days, a culture should be taken by swabbingbeneath the lifted edge of a crusted lesion. If a re-sistant organism is detected, an appropriate antibi-otic should be given for an additional seven days.
REFERENCES
1. Tunnessen WW Jr. A survey of skin disorders seen inpediatric general and dermatology clinics. PediatrDermatol 1984; 1:219-222.
2. Hayden GF. Skin diseases encountered in a pediatricclinic. Am J Dis Child 1985;139:36-38.
3. Roth RR, James WD. Microbiology of the skin: resi-dent flora, ecology, infection. J Am Acad Dermatol1989;20:367-390.
4. Noble WC. Skin carriage of micococcaceae. J ClinPathol 1969;22:249-253.
5. Fekety FR Jr. The epidemiology and prevention ofstaphylococcal infection. Medicine 1964;43:593-613.
6. Martin RR, Buttram V, Besch P, Kirkland JJ, PettyGP. Nasal and vaginal Staphylococcus aureus inyoung women: quantitative studies. Ann Intern Med1982;96:951-953.
7. Barth JH. Nasal carriage of staphylococci and strep-tococci. Int J Dermatol 1987; 26:24-26.
8. Leyden JJ, Marples RR, Kligman AM. Staphyiococ-cus aureus in the lesions of atopic dermatitis. Br JDermatol 1974;90:525-530.
9. Aly R, Maibach HI, Shinefield HR. Microbial flora ofatopic dermatitis. Arch Dermatol 1977;113:780-782.
10. Jackman PJH. Body odor—the role of skin bacteria.Semin Dermatol 1982; 1:143-148.
11. Tuazon CU. Skin and skin infections in the patient atrisk; carrier state of Staphylococcus aureus. Am JMed 1984;76(5A): 166-171.
12. Noble WC. Skin microbiology: coming of age. J MedMicrobiol 1984;17:1-12.
13. Marples RR, Fulton JE, Leyden J, et al. Effect of an-tibiotics on the nasal flora in acne patients. Arch Der-matol 1969;99:647-651.
14. Nilsson EJ, Henning CG, Magnusson J. Topical cor-ticosteroids and Staphylococcus aureus in atopic der-matitis. J Am Acad Dermatol 1992 ;27:29-34.
15. Kuusela P, Vartio T, Vuento M, et al. Binding sitesfor streptococci and staphylococci in fibronectin. In-fect Immun 1984 ;45:43 3-436.
16. Alkan M, Ofek I, Beachey E. Adherence of pharyn-geal and skin strains of group A streptococci to hu-man skin and oral epithelial cells. Infect Immun 1977;18:555-557.
17. Cole GW, Silverberg NL. The adherence of Staphy-lococcus aureus to human corneocytes. Arch Derma-tol 1986;122:166-169.
18. Aly R, Shinefield HR, Maibach HI. Staphylococcusaureus adherence to nasal epithelial cells: studies ofsome parameters. In: Maibach H, Aly R, eds. Skinmicrobiology: relevance to clinical infection. NewYork: Springer-Verlag, 1981:171-179.
19. Feingold DS. Bacterial adherence, colonization andpathogenicity. Arch Dermatol 1986;122:161-163.
20. Shinefield HR, Ribble JC, Boris M, et al. Bacterialinterference: its effect on nursery acquired infectionwith Staphyiococcus aureus I. Preliminary observa-tions on artificial colonization of newboms. Am J DisChild 1963;105:646-654.
21. Steele RW. Recurrent staphylococcal infection infamilies. Arch Dermatol 1980;l 16:189-190.
22. Miller SJ, Aly R, Shinefield HR, Elias PM. In vitroand in vivo antistaphylococcal activity of human stra-tum corneum lipids. Arch Dermatol 1988; 124:209-215.
23. Ushijima T, Takahashi M, Ozaki Y. Acetic, propi-onic, and oleic acid as the possible factors influencingthe predominant residence of some species of Propi-onibacterium and coagulase negative Staphylococcuson normal human skin. Can J Microbiol 1984;30:647-652.
24. Spriggs DR. Bactedocins and antagonism: the killingfields. J Infect Dis 1986;49:31-37.
25. Selwyn S. Natural antibiosis among skin bacteria as aprimary defense against infection. Br J Dermatol1975;93:487-493.
26. Demidovich CW, Wittier RR, Ruff ME, Bass JW,Browning WC. Impetigo. Current etiology and com-parison of penicillin, erythromycin, and cephalexintherapies. Am J Dis Child 1990;144:1313-1315.
27. Schachner L, Taplin D, Scott GB, Morrison M. Atherapeutic update of superficial skin infections. Pe-diatr Clin N Am 1983;30:397-404.
28. Rice TD, Duggan AK, DeAngelis C. Cost effective-ness of erythromycin versus mupirocin for the treat-ment of impetigo in children. Pediatrics 1992;89:210-214.
29. Dillon HC. Impetigo contagiosa: suppurative andnon-suppurative complications. Am J Dis Child 1968;115:530-541.
30. Barton LL, Freidman AD, Sharkey AM, SchnellerDJ, Swierkosz EM. Impetigo contagiosa III. Com-parative efficacy of oral erythromycin, and topicalmupirocin. Pediatr Dermatol 1989;6:134-138.
31. Dagan R, Bar-David Y. Double-blind study compar-ing erythromycin and mupirocin for treatment of im-petigo in children: implications of a high prevalenceof erythromycin-resistant Staphylococcus aureusstrains. Antimicro Agents Chemo 1992;36:287-290.
32. Leyden JJ, Stewart R, Kligman AM. Experimentalinfections with group A streptococci in humans. JClin Invest 1980;75:196-201.
33. Dillon HC, Reeves MSA. Streptococcal immune re-
302 Pediatric Dennatoiogy Vai. 11 No. 4 December 1994
in i^>linti8 after skin infection. Am J Med
34. BuiWt IW. MMsmgement of pyogenic cutaneous in-fections. N En^ J Med 1962;266:164-169.
35. Ik^m AS, Ferried P, Wannmnaker LW. Natural his-tory ctf imi^tigo. II. Etiologic scents and bacterial in-teractions. J Clin Invest 1972;51:2863-2871.
36. Dagan R. Impet^o in childhood: changing epidemiol-ogy Mid new treatments. Pediatr Ann 1993;22:235-240.
37. I>s^m AS, Hill PL, Wannamaker LW. Experimentalinfection of the skin in the hamster simulating humanimpetigo. II. Assessment of various therapeutic regi-mens. Pediatrics 1971;48:83-90.
38. Dillon HC Jr. The treatment of streptococcal skin in-fections. J Pediatr 1970;76:676-684.
39. Dcyani AS, Wannamaker LW. Demonstration of abactericidd substance against beta-hemolytic strep-tococci in supernatant fluids of streptococcal cul-tures. J Bacteriol 1969;97:985-991.
40. Ferrieri P, D^ani AS, Wannamaker LW, ChapmanSS. Natural history of impetigo. I. Site sequence ofeu:quisition and familial patterns of spread of cutane-ous streptococci. J Clin Invest 1972;51:2851-2862.
41. Dillon HC. Streptococcal infections of the skin andits complications: Impetigo and nephritis. In: Wanna-maker LW, Masten P, eds. Streptococci and strepto-coccal diseases. New York: Academic Press, 1972:571-587.
42. Barton LL, Friedman AD. Impetigo: a reassessmentof etiology and therapy. Pediatr Dermatol 1987;4:185-188.
43. Goldfarb J, Crenshaw D, O'Horo J, Lemon E,Blumer JL. Randomized clinical trial of topical mupi-rocin versus oral erythromycin for impetigo. Antimi-cro Agents Chemo 1988;32:1780-1783.
44. Britton JW, Fajardo JE, Krafte-Jacobs B. Compari-son of mupirocin and erythromycin in the treatmentof impetigo. J Pediatr 1990,117:827-829.
45. Blumberg RW, Feldman DB. Observations on acuteglomerulonephritis associated with impetigo. J Pedi-atr 1962;60:677-685.
46. Wannamaker LW. Differences between streptococ-cal infections of the throat and of the skin. N Engl JMed 1970;282:23-30.
47. Melish ME, Glasgow LA. Staphylococcal scaldedskin syndrome: the expanded clinical syndrome. JPediatr 1971;78:958-%7.
48. Lever WF, Schaumburg-Lever G. Bacterial disease.In: Lever WF, Schaumburg-Lever G, eds. Histopa-thology of the skin. 7th ed. Philadelphia: JB Lippin-cott Co., 1990:318-351.
49. Baraff LJ, Fine RN, Knutson DW. Poststreptococcalacute glomeniionephritis: fact and controversy. AnnIntern Med 1979,91:76-86.
50. Lewy JE, Salinas-Madrigal L, Herdson PB, PeraniCL, Metcoff J. Clinico-pathologic correlations inacute poststreptococcal glomerulonephritis. Medi-cine 1971,50:453-501.
51. Travis LB, Dodge WG, Beathard GA, et al. Acuteglomerulonephritis in children. A review of the natu-ral history with emphasis on prognosis. Clin NephrolI973;l: 169^181.
52. Sanjad S, Tolayniat A, Whitworth J, Levin S. Acuteglomerulonephritis in children: a review of 153 cases.South Med J 1977 ;70:1202-1206.
53. Tejani A, Ingulli E. Poststreptococcal glomerulone-phritis. Current clinical and pathologic concepts.Nephron 1990,55:1-5.
54. Sagel I, Treser G, Ty A, Yoshizawa N, et al. Occur-rence and nature of glomenilar lesions after group Astreptococci infections in children. Ann Intern Med1973,79:492-499.
55. Anthony BF, Kaplan EL, Wannamaker LW, BrieseFW, Chapman SS. Attack rates of acute nephritis af-ter type 49 streptococcal infection of the skin and ofthe respiratory tract. J Clin Invest 1%9;48:1697-1704.
56. McLinn S. Topical mupirocin versus systemic eryth-romycin treatment for pybderma. Pediatr Infect Dis J1988;7:785-790.
57. Mertz PM, Marshall DA, Eaglstein WH, PiovanettiY, Montalvo J. Topical mupirocin treatment of im-petigo is equal to oral erythromycin therapy. ArchDermatol 1989; 125:1069-1073.
58. Kaplan EL, Wannamaker LW. Suppression of theantistreptolysin O response by cholesterol and bylipid extracts of rabbit skin. J Exp Med 1976;144:754-767.
59. Ortiz JS, Finklea JF, Potter EV, Poon-King T, Ali D,Earle DP. Endemic nephritis and streptococcal infec-tions in South Trinidad. Surveillance studies duringthe first year following a major epidemic. Arch InternMed 1970;126:640-646.
60. El-Kholy A, Hafez K, Krause RM. Specificity andsensitivity of the streptozyme test for the detection ofstreptococcal antibodies. Appl Microbiol 1974;27:748-752.
61. Klein GC, Jones WL. Comparison of the strep-tozyme test with the antistreptolysin O, antideoxyri-bonuclease B, and antihyaluronidase tests. Appl Mi-crobiol 1971 ;21:257-259.
62. Hall w p , Blumberg RW, Moody MD. Studies in chil-dren with impetigo: bacteriology, serology, and inci-dence of glomerulonephritis. Am J Dis Child 1973;125:800-806.
63. Ruby RJ, Nelson JD. The influence of hexachloro-phene scrubs on the response to placebo or penicillintherapy in impetigo. Pediatrics 1973;52:854-859.
64. Derrick CW, Dillon HC Jr. Further studies on thetreatment of streptococcal skin infection. J Pediatr1970;77:696-700.
65. Tunnessen WW Jr. Practical aspects of bacterial skininfectious in children. Pediatr Dermatol 1985;2:255-265.
66. Leyden JJ. Review of mupirocin ointment in thetreatment of impetigo. Clin Pediatr 1992;31:549-553.
67. Ward A, Campoli-Richards DM. Mupirocin: a reviewof its antibacterial activity, pharmacokinetic proper-ties, and therapeutic use. Drugs 1^6;32:425-444.
68. Cookson BD. Mupirocin resistance in staphylococci.J Antimicro Chemo 1990;25:497-503.
69. Eady EA, Cove JH. Topical antibiotic tiierapy: cur-rent status and future prospects. I h u ^ Exp Oin Res1990;16:423-433.
70. Aly R, Shinefield HR, Litz C, Maibach HI. Role of
Darmstadt and Lane: Impetigo 303
teichoic acid in the binding of Staphylococcus aureusto nasal epithelial cells. J Infect Dis 1980;141:463-465.
71. Guinan ME, Dan BB, Guidotti RJ, et al. Vaginal col-onization with Staphylococcus aureus in healthywomen: a review of four studies. Ann Intem Med1982;%:944-947.
72. Dancer SJ, Noble WC. Nasal, axillary, and perinealcarriage of Staphylococcus aureus among women:identification of strains producing epidermolytictoxin. J CUn Pathol 1991;44:681-684.
73. Casewell MW, Hill RLR. Elimination of nasal car-riage of Staphylococcus aureus with mupirocinCpseudomonic acid')—a controlled trial. J AntimicroChemo 1986; 17:365-372.
74. Martin RR, White A. The reaquisition of staphylo-cocci by treated carriers: a demonstration of bacterialinterference. J Lab Clin Med l%8;71:791-797.
75. poebbeling BN, Breneman DL, Neu HC, et al. Elim-ination of Staphylococcus aureus nasal carriage inhealth care workers: analysis of six clinical trials withcalcium mupirocin ointment. Clin Infect Dis 1993; 17:466-474.
76. Kauffman CA, Terpenning MS, Xiaogong H, et al.Attempts to erradicate methicillin-resistant Staphylo-coccus aureus from a long-term-care facility with theuse of mupirocin ointment. Am J Med 1993;94:371-378.
77. Dacre JE, Emmerson AM, Jenner GA. Nasal car-riage of gentamycin and methicillin-resistant Staphy-lococcus aureus treated with topical pseudomonicacid. Lancet 1983,2:1036.
78. Dhar S, Kanwar AJ, Kaur S, Sharma P, GangulyNK. Role of bacterial flora in the pathogenesis andmanagement of atopic dermatitis. Indian J Med Res1992,95:234-238.
79. Boelaert JR, De Smedt RA, De Baere YA, et al. Theinfluence of calcium mupirocin nasal ointment on theincidence of Staphylococcus aureus infections inhaemodialysis patients. Nephrol Dial Transplant1989;4:278-281.
80. Mulligan ME, Murray-Leisure KA, Ribner BS, et al.Methicillin-resistant Staphylococcus aureus: a con-sensus review of the microbiology, pathogenesis, andepidemiology with implications for prevention andmanagement. Am J Med 1993;94:313-328.
81. Wortman PD. Bacterial infections of the skin. CurrProb Dermatol 1993;5:193-228.
82. Dagan R, Bar-David Y. Comparison of amoxicillinand augmentin for the treatment of non-bullous im-petigo. Am J Dis Child 1989;143:916-918.
83. Jaffe AC, O'Brien CA, Reed MD, Blumer J. Ran-domized comparative evaluation of augmentin andcefaclor in pediatric skin and soft-tissue infections.CurrTherRes 1985 ;38:160-168.
84. Fleisher GR, Wilmott CM, Campos JM. Amoxicillincombined with clavulanic acid for the treatment ofsoft tissue infections in children. Antimicro AgentsChemo 1983;24:679-68l.
85. Schachner L, Taplin D, Scott GB, Morrison M. Atherapeutic update of superficial sidn infections. Pe-diatr CUn N Am 1983;39:397-404.
86. Jones RN, Barry AL, the Collaborative Antimicro-bial Testing Group. BMY-28100, a new oral cephalo-sporin: antimicrobial activity against nearly 7000 re-cent clinical isolates, comparative potency with otheroral agents, and activity against beta-lactamase pro-ducing isolates. Diagn Microbiol Infect Dis 1988;9:11-26.
87. Parish CP, Doyle CA, purham SJ, Wilber RB. Cef-prozil versus cefaclor in the treatment of mild tomoderate skin and skin-structure infections. CUnTher 1992; 14:458-469.
88. Nolen TM. Clinical trials of cefprozil for treatment ofskin and skin-structure infections: review. CUn InfectDis 1992;14(suppl 2):255S-263S.
89. Fujii R. Clinical trials of cefpodoxime proxetil sus-pension in pediatrics. Drugs 1991;42(suppl 3):57-60.
90. Hebert A, Still JG, Reuman PD. Comparative safetyand efficacy of clarithromycin and cefadroxil suspen-sions in the treatment of mild to moderate skin andskin structure infections in children. Pediatr InfectDis 1993;12:112S-117S.
91. DiUon HC, Derrick W. Clinical experience with cUn-damycin hydrochloride: I. Treatment of streptococ-cal and mixed streptococcal-staphylococcal skin in-fections. Pediatrics 1975;55:205-212.
92. Derrick CW, ReiUy KM, Stallworth JR. Erythromy-cin in the treatment of streptococcal infections. PecU-atr Infect Dis 1986;5:172-176.





















