Impact of previous antimicrobial therapy on the etiology and outcome of ventilator-associated...
8
1993;104;1230-1235 Chest J Rello, V Ausina, M Ricart, J Castella and G Prats pneumonia. etiology and outcome of ventilator-associated Impact of previous antimicrobial therapy on the http://chestjournal.chestpubs.org/content/104/4/1230 can be found online on the World Wide Web at: The online version of this article, along with updated information and services ) ISSN:0012-3692 http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( without the prior written permission of the copyright holder. reserved. No part of this article or PDF may be reproduced or distributed Chest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights of been published monthly since 1935. Copyright1993by the American College is the official journal of the American College of Chest Physicians. It has Chest © 1993 American College of Chest Physicians by guest on July 13, 2011 chestjournal.chestpubs.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Impact of previous antimicrobial therapy on the etiology and outcome of ventilator-associated...
1993;104;1230-1235Chest J Rello, V Ausina, M Ricart, J Castella and G Prats pneumonia.etiology and outcome of ventilator-associated Impact of previous antimicrobial therapy on the
http://chestjournal.chestpubs.org/content/104/4/1230
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright1993by the American College is the official journal of the American College of Chest Physicians. It hasChest
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from

*Fr�,1) the Intensive Care, Microbiolog)� and Respiratory Depart-
ments, hospital (Ic Ia S. Creu i S. Pan, Universitat Autonomna deBarcelona, Barcelona, Spain.
Manuscript received October 13. 1992; revision accepted February23, 1993
1230 Impact of Previous Antimicrobial Therapy in Ventilator-associated Pneumonia (Reio at a!)
Impact of Previous Antimicrobial Therapyon the Etiology and Outcome of Ventilator-associated Pneumonia*Jordi Rello, M. D. , Ph . D. ; Vicen#{231}Ai�sina, Al. D. , Ph . D. ; Maite Ricart, RN.;
Joan Ca.s’tella, M.D. , Ph .D.; and Guilleni &ats, M.D. , Ph.D.
Objective: To define the influence of prior antibiotic use on
the etiology and mortality of ventilator-associated pneu-
monia (YAP).
Setting: A university hospital medical-surgical ICU.
Design: Prospective clinical study.
Methods: Over a 35-month period, we prospectively studied
129 consecutive episodes of YAP. Etiologic diagnosis was
established using a protected specimen brush and quanti-
tative culture techniques. We examined prognostic factors
by univariate and multivariate analyses using a statistical
software package (SPSS).
Results: The rate of YAP caused by Gram-positive cocci or
Haemophilus influenzae was statistically lower (p<O.OS) in
the patients who had received antibiotics previously, while
the rate of YAP caused by Pseudomonas aeruginosa wasstatistically higher (p<O.Ol). Patients died ofcauses directlyrelated to the infection in 18 (14.0 percent) episodes, P
aeruginosa being isolated in 9 of these fatal cases. Indeed,
we found that 27.7 percent (15/54) of patients who had
received prior antimicrobial therapy before the onset of
pneumonia died, compared with only 4.0 percent (3/75) of
those who did not. In the univariate analysis, the variables
significantly associated with attributable mortality were age
older than 45 years, use of corticosteroids, presence of
shock, hospital day of VAP over 9, antecedent COPD, and
a prior antibiotic use. A step-forward logistic regression
analysis defined only prior antibiotic use (p<O.0001,
OR = 9.2) as significantly influencing the risk of death from
YAP. The same result was obtained when severity was
included in the model. However, prior antibiotic use
entirely dropped out as a significant risk factor when the
etiologic agent was included in the regression equation.
Conclusions: Distribution of infecting microorganisms re-
sponsible for YAP differs in patients who received prior
antimicrobial therapy, and this factor determines a higher
mortality rate. We suggest a restrictive antibiotic policy in
mechanically ventilated patients with the purpose of reduc-
ing the risk of death from YAP. (Chest 1993� 104:1230-35)
MV = mechanical ventilation; VAP ventilator-associated pneu-monia
N osoconual pneumonia occurs in 0.5 to 2 percent
ofpatients hospitalized’2 and is the leading cause
of death from nosocomial infection. � Moreover,
intubated patients receiving mechanical ventilation
(MV) have an important increase in risk for pneumno-
nia,5 with the incidence of ventilator-associated pneu-
moma (VAP) ranging between 9 and 68 percent,
depending on the poptiIat�Ion studied. I,69
The impact on mortality is the most important
aspect ofany clinical problem. Identification of factors
For editorial comment see page 993
influencing mortality offers the possibility of improv-
ing prognosis through the identification of patients
with “high risk ofdeath” and the modification of so�ne
of these factors by medical intervention. The use of
multiple regression analysis helps to identify inde-
pendent prognostic factors for a disease as complex
and multifactorial as nosocomial pneumonia.
A high percentage of intubated patients have con-
comitant infections, which often leads to broad-spec-
trum antimicrobial therapy. Moreover, some atm-
thors’��’2 have recommended the use of prophylactic
antibiotics in intubated patients, because of the high
morbidity and niortality associated with VAP. In con-
trast, Fagon et al� have recently reported that previous
antimicrobial therapy 1)rior to the onset of VAP may
be associated with higher mnortality� However, to our
knowledge, the influence ofthis factor in the prognosis
of YAP has itot been studied previously using a
multivariate analysis.
Therefore, we performed a prospective study of 129
consecutive episodes of VAP to determine the influ-
ence ofa variety ofepidemiologic and clinical variables
on the outcome , by means of univariate and multivar-
iate analyses. Our specific goal was to provide current
inforniation oil the influence of antinucrobial therapy
before the onset of pneumonia on the frequency of
nncrobial etiologies and subsequent mortality.
NI ETIIOI)S
Population Study
Our intensive care unit (ICLT) is a 16-lied medical-surgical unit,
�vith an average of6()0 admissions per year, in a 1 ,0()0-1)ed university
hospital that serves as both a referral center and a first-line hospital.
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from

CHEST I 104 I 4 I OCTOBER, 1993 1231
Table 1 -Summary ofindicationsfor Antibiotic Therapy
Indication Cases, No.
Previous nosocomial infection 19
Community-acquired pneumonia 10
Open fractures 8
Postoperative prophylaxis* 5
Septic shock 4
Pancreatitis 3
NFIt in transplant recipient 2
Miscellaneoust 3
*Prolonged for more than 48 h.
tNFI = nosocomial febrile illness.
�Tetarn,s, peritonitis, and fever ofunknown origin.
It is located in an urban area with a population of over 3 million.
During a 35-month period, all patients who developed pneumonia
in our ICU were considered eligible and were prospectively
evaluated by one of the investigators (JR.). We did not use any
selective decontamination regimen.
A diagnosis of pneumonia was considered when new and persist-
ent pulmonary infiltrates not otherwise explained appeared on chest
radiographs. Moreover, at least two of the following criteria were
also required: (1) fever �38#{176}C; (2) leukocytosis � 10,000/mm3; and
(3) purulent respiratory secretions. Pneumonia was considered
ventilator associated when its onset occurred after 48 h of MV and
was thus judged not to have been incubated before starting MV. To
analyze factors that might influence outcome, the following variables
were recorded: age, sex, severity prior trauma or surgery, under-
lying disease, the presence of COPD, diabetes, renal failure
requiring dialysis, cardiopathy, persistence of coma during MV, the
duration of MV prior to the development ofVAP, corticosteroid use,
and presence of shock (either prior as subsequent to the diagnosis
of yAP). All antimicrobials received for more than 48 h during the
10 days preceding the episode of VAP were recorded. Antibiotics
administered forless than 48 h, mainly for perioperative prophylaxis,
were not considered and the corresponding epis(xles of VAP were
classified as “free of exposition.’
Antecedent COPD was diagnosed using the standard criteria
recommended by the American Thoracic oc’3 Coma was
diagnosed when a Glasgow Coma Score lower than 9 was obtained’�
for more than 24 h. Criteria for corticosteroid use have been defined
previously.” Surgery or trauma was considered to be present if
recorded within 2 weeks prior to the episode. Presence of cardi-
opathy was considered if the patient had undergone surgery or if
an episode of angina or cardiac failure was previously diagnosed.
Diabetes was diagnosed if the patient received insulin previously
to hospital admission. Shock was defined as a systolic blood pressure
below 90 mm Hg accompanied by clinical signs of hypoperfusion,
such as oliguria and peripheral vasoconstriction. Severity of under-
lying medical conditions was stratified in three categories according
to the criteria proposed by McCabe and Jackson6 and in five
categories according to NNIS ICU severity-of-illness clinical clas-
sification codes. � Crude mortality included all deaths that occurred
in the ICU among patients with VA? Mortality was considered as
attributable to the pulmonary infection if death ensued before any
objective response to antimicrobial therapy or if the pulmonary
infection was considered a contributing factor to death in patients
with additional conditions.�
Microbiology
Fiberoptic bronchoscopic examination using a protected sped-
men brush” was performed on each of these patients within the
first 12 h after the development of a new pulmonary infiltrate,
except on weekends. A telescoping canula brush with a distal
polyethylene glycol occlusion (model BWF/10/70/90; Meditech Inc.
Watertown, Mass) was inserted through the inner suction channel
ofthe bronchoscope (model BF 10; Olympus Corp ofAmerica, New
Hyde Park, NY). This protected brush was advanced and aseptically
cut into a sterile tul)e containing 1 ml of sterile saline solution.
Specimens were taken to the microbiology laboratory immediately
after collection. The vial was then vortexed vigorously for at least
60 s to suspend all material from the brush. Two serial 100-fold
dilutions were carried out, and 0. 1-ml aliquots of the original
suspension and each dilution were inoculated on agar plates for
aerobic and anaerobic culture; one agar plate with selective buffered
charcoal-yeast extract medium for isolation of Legionella species
was included!� Bacterial count �1000 cfu/ml was the cutoff point
to diagnose pulmonary infections, according to the standards
adopted in previous studies.21 Bacterial identification and suscepti-
bility testing were performed by standard methods.�
Statistical Analysis
Contingency tal)les were analyzed using the two-tailed x2 test.
Multivariate analysis was performed using the stepwise logistic
regression model ofa software package (SPSS). using 0.05 as a limit
for entering new terms. The cutoff point for those variables with
more than two categories was chosen depending on the univariate
analysis results. Odds ratios (OR) were calculated using standard
methods.�’
RESULTS
During the period of the study, 150 episodes of
nosocomial pneumonia were identified in our ICU.
One hundred twenty-nine of them met criteria of YAP
and were prospectively followed. The mean ± SD age
of these patients was 49.5 ± 20.3 years; 91 were men
and 38 were women. Patients had received antimicro-
bial therapy for more than 48 h, in the 10 days
preceding the onset of YAP, in 54 of these episodes.
Indications for these antimicrobials are listed in Table
1 . Table 2 shows which type of antibiotics were used
prior to development of VAP, separated by etiologies,
for episodes with etiologic diagnosis.
Crude mortality was 34.1 percent. Patients died of
causes directly related to the pulmonary infection in
18 (14.0 percent) episodes. All patients with VAP
caused by Gram-positive cocci or Haemophilus influen-
zae recovered. Pseudomonas aeruginosa was the mi-
Table 2-Class ofAntibiotics Used Prior to DevelopmentofPneumonia in 89 Episodes With Established
Etiologk Diagnosis*
Microorganism C I A V Cl Other
Staphylococcus aureus 3 2 1 1 2
CNS I 1
Haemophilus influenzae 2 1 1
Pseudoinonas aeruginosa 6 9 5 6 1 7
Alcaligenesfaecalis 1 1 2
Serratia marcescens 2 1 3 2 1
Proteus mirabili,s 2 1 1 1 1
Acinetobacter calcoaceticus 2 1 2 1
Anaerobic flora 2 2 1
Fungi 2 1 1 1
*CNS = coagulase-negative staphylococci; C cephalosporins;
I = imipenem; A aminoglycosides; V vancomycin;
Cl = cloxacillin.
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from
1232 Impact of Previous Antimicrobial Therapy in Ventilator-associated Pneumonia (Re!!o at a!)
Table 3-Characteristics ofPatients Who Died From VAP*
Case/
Age, yr/Sex Diagnosis pATB Microorganisms
1/43/NI Heart transplant Yes Aspergillus species
Candida species
2/59/M COPD ‘m�s P.seudonwnas a(’ruginosa
3/33/M Heart transplant Yes P aerUgiflosa
Serratia inarcescens
4176/NI CET Yes P acruginosa
5,�75/M Cardiogenic shock Yes Aspergilltms species
6/62/NI CAP Yes P aeruginosa
S mnarcescens
7170/NI COPD Yes Ac! netobacter
calcoaceticus
8174/M COPD Yes P aeruginosa
9/71fF COPD Yes A calcoaceticus
10/46/M Asthma Yes P aeruginosa
1 1/65/NI Cardiac surgery Yes P aeruginosa
12/72/F Pancreatitis Yes P aeruginosa
13/54/M Septic shock Yes Proteus mirabilis
14J21/M Multiple trauma Yes Uncertain
15/48/F Neurosurgery Yes Uncertain
16/68/M Cardiac surgery No Uncertain
17/51/NI Multiple trauma No S marcescens
18/71/M Thoracic surgery No P aeruginosa
*VAP = ventilator-associated pneumonia; CET cranioencephalic
trauma; CAP = commumty-ac(�uired pneumonia; COPD chronic
obstructive pulmonary disease; pATB = previous antibiotic therap);
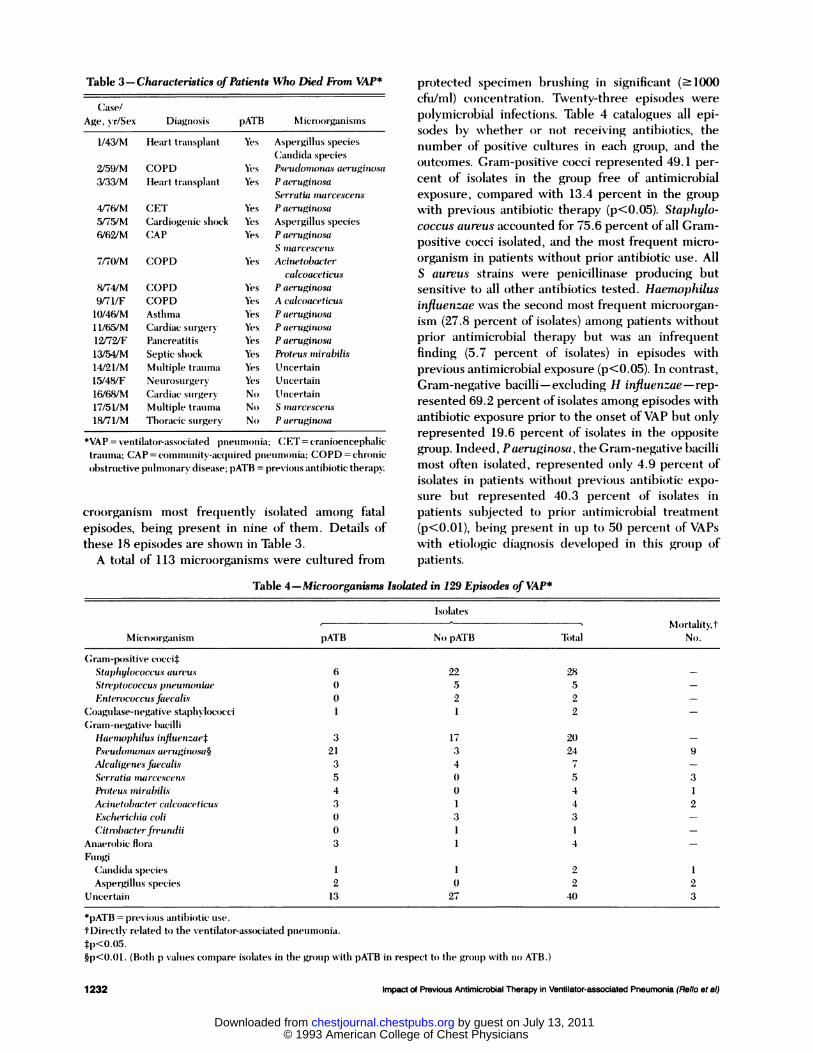
croorganism most frequently isolated among fatal
episodes, being present in nine of them. Details of
these 18 episodes are shown in Table 3.
A total of 1 13 microorganisms �vere cultured from
protected specimen brushing in significant (� 1000
cfu/ml) concentration. Twenty-three episodes were
polymicrobial infections. Table 4 catalogues all epi-
sodes l)y whether or not receiving antibiotics, the
number of positive cultures in each group, and the
outcomes. Gram-positive cocci represented 49. 1 per-
cent of isolates in the group fi-ee of antimicrobial
exposure, compared with 13.4 percent in the group
with previous antibiotic therapy (p<O.OS). Staph yb-
coccus aureus accounted for 75.6 percent ofall Gram-
positive cocci isolated, and the most frequent micro-
organism in patients without prior antibiotic use. All
S aureus strains were penicillinase producing but
sensitive to all other antibiotics tested. Haernophibus
influenzae was the second most frequent microorgan-
i5IT1 (27.8 percent of isolates) among patients without
prior antimicrobial therapy but was an infrequent
finding (5.7 percent of isolates) in episodes with
previous antimicrobial exposure (p<O.O5). In contrast,
Gram-negative bacilli - excluding H influenzae - rep-
resented 69.2 percent ofisolates among episodes with
antibiotic exposure prior to the onset of YAP but only
represented 19.6 percent of isolates in the opposite
group. Indeed, Paeruginosa, the Gram-negative bacilli
most often isolated, represented only 4.9 percent of
isolates in patients without previous antibiotic expo-
sure but represented 40.3 percent of isolates in
patients subjected to prior antimicrobial treatluent
(p<O.Ol), l)eing present in up to 50 percent of VAPs
with etiologic diagnosis developed in this group of
patients.
Table 4-Microorganisms Isolated in 129 Episodes of VAP*
Microrganism
Isolates
- Mortality,t
No.
,�pATB No pATB Total
c;ram-f�Ositi%’e cocci�
Staphylococcus aureus 6 22 28 -
Streptococcus pneunumiae 0 5 5 -
bnt(’rococcusfaecalis 0 2 2 -
Coagulase-negative staplwlococci 1 1 2 -
c;ramii-mmegative l)acilli
Hacinophilus influenzaet 3 17 20 -
P.seudonmonas aeruginosa* 21 3 24 9
Alcaligenesfaecalis 3 4 7 -
Serratia mnarcescen.s 5 0 5 3
&Ot(’U.S mniralnli.s 4 0 4 1
Acinetol�u:ter calco(zceticu.s 3 1 4 2
bscho’riclmia coli 0 3 3 -
Citrohacterfrcundii 0 1 1 -
Anaerobic flora 3 1 4 -
Fungi
Candida species 1 1 2 1Aspergillus species 2 0 2 2
Uncertain 13 27 40 3
*pATB = pre\i�tIs antibiotic use.
tDirectly related tO) the ventilator-associated pneun)onia.
�I)<0.05.§p<O.Ol. (Both p values c�fl)l)are isolates in the group with pATB in respect to the group with no ATB.)
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from
48 (37.2) 3 (6.2) 1
81 (62.7) 15 (18.5) 3.6
91 (70.5� 15 (16.5� 2.3
38 (29.4) 3 (7.9) 1
22 (17.0) 1 (4.5) 1
107 (82.9� 17 (15.9) 3.9
64 (49.6) 7 (10.9� 1
65 (50:3) ii (16.9) 1.4
44 (:34.1) 3 (6.8) 1 NS
85 (aSS) 15 (17.6� 2.9
61 (47.2) 7 (11.5) 1
68 (52.7) 1! (16.2) 1.4
Age, yr
<45
>45
(;em)der
NIale
Fenlale
I.Jm�lerlving condition
NF
1JF/RFSeveritvll
Codes A, B. C
Codes I). ETrammm��i
Yes
No
Surgery
Yes
No
Prior antil)iotic
therapy
Yes
No
Corticosteroid use
Yes
No
hospital day of VAP
5;9 d>9d
I)iala-tes
Yes
No
Renal fail,mre
Yes
No
Shock
Yes
No
(�)nbl
Yes
No
c;�mrdi )pathv
Yes
No
c;()PI) antece(lent
Yes
No
54 (41.8)
75 (58.1)
26 (20.1)
103 (79.8�
15 (27.8)
3 (4.0)
7 (26.9)
11 (10.7)
14 (10.8) 4 (28.6) 2.8
115 (84.1) 14 (12.2) 1
15 (ll.(i� 5 (:3:3:3) 3.8114 (S8.;3� 13 (12.8) 1
NS
0.02
19 (14.7) :3 (15.8) 1.1
110 (85.2) 15 (l3.6� 1
24 (18(i) 8 (;33.:3) 3.0 0.0()2
105 (81.3) 10 (9.5) 1
*(�)PD = chronic obstructive l)mIln1�m1ar\ (liseas \AP - ventilator-
assx.’iated I)neIIIla)Ilia; NF = Iu)nlatal: iT J” mmltimnotelv fatal; RF
rapidl� fatal; NS = not significant.
tPercentage within (‘�lch categor��
:1:Percentage of de’aths Iron) pn(’lIIIIiOIiia svitliin o’pisodes in each
group.
§\Vithin each category au odds ratiO) of 1 svas arl)itrarllv assigmied to
the variable sulxlivision with the lowest risk rate.
INNIS ICU severitv-ofillness clinical classific.,tion.
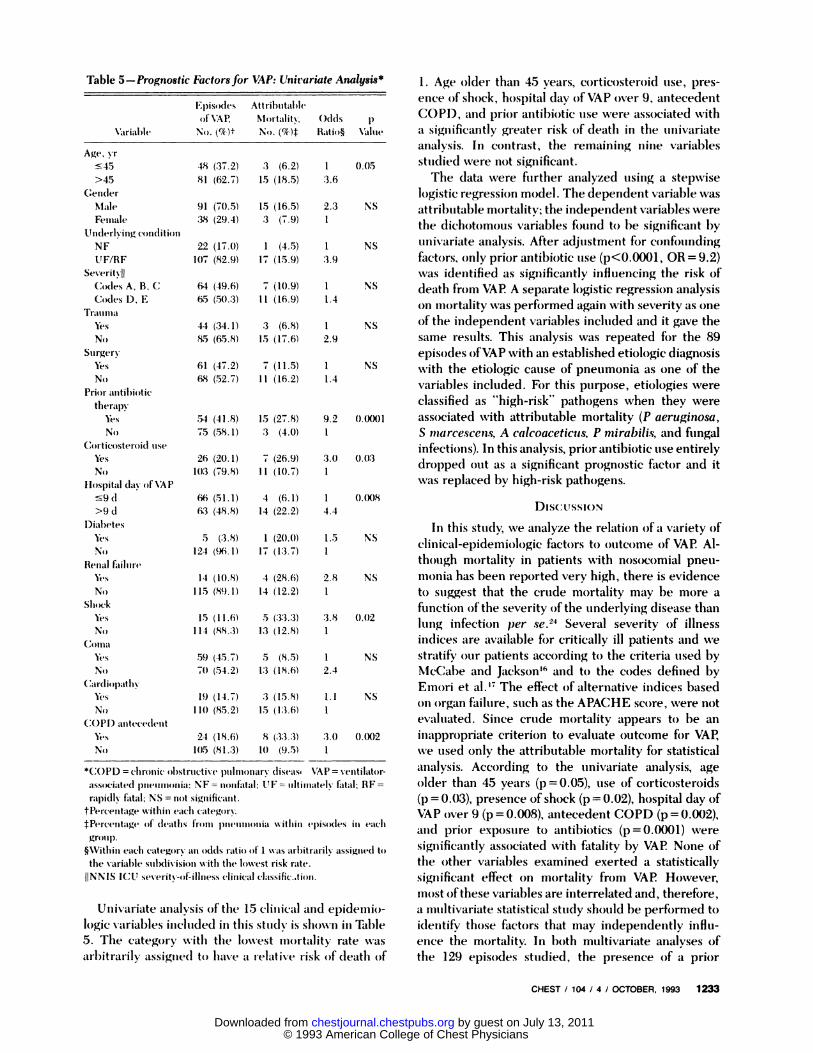
Univariate analysis of the 15 climmical and epidemio-
logic variables included in this stud� is shown in Table
5. The category With the lo�vest mortality rate ��‘as
arl)itrarily assigned to ha�’e a relative risk of death of
CHEST I 104 I 4 I OCTOBER, 1993 1233
Table 5-Prognostic Factorsfor VAP: Univariate Analysis* 1 . Age older than 45 years, corticosteroid use, pres-
ence of shock, hospital day of YAP over 9, antecedent
COPI), and prior antibiotic use were associated with
a significantly greater risk of death in the univariate
analysis. In contrast, the remaining nine variables
0.05 studied were iiot significant.The data were further analyzed using a stepwise
logistic regression model. The dependent variable was
NS attributable mortality; the independent variables were
the dichotomous variables found to he significant by
NS univariate analysis. After adjustment for confoundingfactors, only prior antibiotic use (p<0.000l , OR = 9.2)
was identified as significantly influencing the risk of
NS death from VAP A separate logistic regression analysis
on mortality was performed again with severity as o�e
of the independent variables included and it gave the
same results. This analysis was repeated for the 89
episodes ofVAP with an established etiologic diagnosis
NS with the etiologic cause of pneumonia as one of the
variables included. For this I)t1�P�se, etiologies were
classified as “high-risk” pathogens when they were
9.2 0.0(X)l associated with attributable mortality (P aeruginosa,S inarcescens, A calcoaceticus, P mirabilis, and fungalinfections). In this analysis, prior antibiotic use entirely
3.0 0.03 . �. .
urop�e�i out as a signmcant prognostic tactor anu itwas replaced by high-risk pathogens.
66 (51.1) 4 (6.1) 16:3 (48.8) 14 (22.2) 4.4 DIS(:USSION
In this Stu(IV, we analyze the relation of a variety of5 (:3.8) 1 (20.0) 1.5 NS . . � . ‘ . .
124 (96 1) 17 (13 7) 1 clmIcal-epiuemioioglc tactors to outcome or VAP A -
though nR)rtahty in patients with nos()comial pneu-monia has been reported very high, there is evidence
to suggest that the crude mortality may be more a
function ofthe severity ofthe underlying disease than
lung infection p� se.24 Several severity of illness
indices are available for critically ill patients and we
59 (45.7) 5 (8.5) 1 NS stratify Ofl� patients according to the criteria used by
70 (54.2) 13 (18.6) 2.4 McCabe and Jacksonm6 and to the codes defined by
, . Emnori et al.’7 The effect of alternative indices basedNS OH organ failure, such as the APACHE score, were not
evaluated. Since crude mortality appears to be an
inappropriate criterion to evaluate outcome for YAP,
we used only the attributable mortality for statistical
analysis. According to the univariate analysis, age
older than 45 years (p = 0.05), use of corticosteroids
(p = 0.03), presence of shock (p = 0.02), hospital day of
VAP O’Ver 9 (p = 0.008), antecedent COPD (p 0.002),
and prior exposure to antibiotics (p = 0.()()01) were
significantly associated with fatality by YAP None of
the other variables examined exerted a statistically
significant effect on mortality from VAP However,
IflOst ofthese variables are interrelated and, therefore,
a multivariate statistical study should he performed to
identify those factors that may independently info-
ence the mortality. In 1)0th multivariate analyses of
the 129 episodes studied, the presence of a prior
Episodes Attributable
of \‘A� NIortalit�� Odds p
\�oriable’ No. (��i)1� No. (%)� I1atio� \�mlmie
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from

1234 Impact of Previous Antimicrobial Therapy in Ventilator-associated Pneumonia (Re!!o et a!)
antimicrobial treatment (p<O.000l) was the only factor
that independently influenced mortality. Previously,
Fagon et al,� in a prospective study of 52 episodes of
YAP, reported that the overall mortality in a group of
31 patients who had received antimicrobial therapy
before the onset of pneumonia was 83 percent, corn-
pared with a mortality of 48 percent in the group of
21 patients who had not received prior antibiotics
(p<O.Ol). Our data agree with their suggestion that
antimicrobial therapy before onset of VAP may be
associated with a negative impact on outcome.
Furthermore, a strong relationship between the use
ofantibiotics prior to the onset ofVAP and the etiologic
agent is clearly observed in our study Our finding that
prior antibiotic use entirely dropped out as a significant
risk factor when the etiologic agent was included in
the logistic regression analysis demonstrated that the
increased mortality associated with prior antibiotic
use is due to the selection of more lethal organisms.
Indeed, Gram-positive cocci and H influenzae repre-
sented more than three quarters of isolates among
episodes free of antimicrobial exposure . However,
these agents were an infrequent etiology among pa-
tients subjected to prior antimicrobial therapy, and a
high proportion of episodes in this group were due to
P aerugino.s’a or multiresistant Gram-negative bacilli.
Suppression ofthe normal bacterial flora by antibiotics,
with the subsequent emergence of a resistant Gram-
negative flora, may explain this observation. Fagon et
al� also reported that pneumonia with P aerugino.ca or
Acinetobacter species was higher in the 31 patients
who had received prior antibiotics (65 vs 19 percent,
p<O.Ol). Other studies have reported the influence of
antibiotics in the selection of microbial flora and in
determining etiologic patterns of nosocomial I)11e11
monia . �27
A close relationship between the agent responsible
for nosocornial pneumonia and mortality has also been
previously observed by other investigators.58� In our
study, this observation cannot be related to made-
quate antibiotic treatment for selected etiologies,
except for the two patients with fungal pneumonia,
since all patients received a broad-spectrum empiri-
cal treatment , including antipseudomonadal coverage.
Several previous studies have reported the relation-
ship between mortality and patients with Gram-
negative hacillary pneumonia.329”#{176} In our study, the
risk of mortality was very high in those patients with
YAP caused by P aeruginosa, multiresistant Gram-
negative bacilli, or fungi. Indeed, P aeruginosa was
isolated in 60 percent of fatal episodes with etiologic
diagnosis. Conversely, when YAP was caused by Gram-
positive cocci or by H influenzae, the prognosis was
benign. The large increase of high-risk pathogens in
patients who received prior antimicrobial therapy may
explain the relationship between mortality and prior
antil)iOtiC use.
Antibiotic therapy has a great ecologic impact.
Broad-spectruml3 antibu)tic tlwrapy; used in most ICUs,
i�i-iay alter patients’ niicroflora, leading to airway cob-
nization and tilti niatelv i nfection with miiethicillin-
resistant staphylococci , multiple resistant E nterobac-
teriaceae , psetidomonads, and ye;tsts.23’ u Most
nosocornial outbreaks caused liv resistant pathogens
l)egan in the small fraction of I)atientS hospitalized in
the ICU and afltii)iotiC Iresstire was usually found to
be one of the niost important factors preclisposing
these patients to infection with resistant organisrns.�Iu
Antibiotics tiot OIIIV alter colonization in the orophar-
ynx and gastrointestinal tract, but they mna�’ also have
deleterious effects 013 the host irnniimne response to
infection.�5 Some clinicians have opted f�r the liberal
LIS(’ of l)roacl-spectrunl aI�tin�icrol)iab agents in ole-
chanicall’v ventilated I)atiellts when the� developed a
febribe nosoconlial episode, or even f�r 1)roPhyl�Lxis of
nosocoiiiial 1)�eu iiionia . \Ve agree �vith Johan SOfl3() that
such practices are expensive, niav cause avoidal)le
side effects, an(l compromise efforts to document
causative agents precisely in future infections. Fur-
thermore, Our current results suggest that this strategy
may be ass()ciated with a higher mortality, directly
related to infection if such patients developed a YAP
Consequentl�; we suggest the development of specific
guidelines for antimicrobial therapy of infections in
the ICU and an ai’ltiI)iOtiC control policy based on the
restriction of broad-spectrum agents. We support the
proposition of Flaherty and \Veinstein2 that the use of
l)road-spectrunl antibiotics in critically ill patients
should be surveyed and approved by a designated
antibiotic expert who should l)e an infectious (liSease
I)hvsiCial1 or a critical care physician with expertise inantimicrobial therapy and infection control . I n our
opinion, avoidance of unnecessary administration of
antibiotics should form part of the reconlrnended
procedim res in tile treatment of mechanically ventilated
patients.
ACKNOWLED(;MENT: \Ve thank W c;. JOh�sm�sOm), NI . D. , NI PH.,and ;. Verger, M.D. , for helpful simg�estions concerning themanuscript. \Ve also thank meml)ers of the ICU for their coopera-tion.
RE FE RE N( :ES
1 Craven DE, Kunches LM, Kilinsky � Lichtenherg DA, NIake
BJ, NlcCabe \VR. Risk factors for pm1e1In�)m)ia and fatality in
patiel)ts receiving continuous niechanical ventilation. An RevRespir Dis 1986; 13.3:792-96
2 Flaliertv JP, \Veinstein HA. Infection control am�l pneumonia
prophylaxis strategies in the intensive care unit. Semain Respir
Infect 1990; 5:191-203
3 Pennington JE. Nosoconiial resI)irator\ infection. Iii: Nlandell
(;L, Douglas Rc; Jr. Bennett JE, eds. Principles an�1 l)r�Ictice of
infectious diseases. Ness’ ‘turk: John \Vile� & Sons, 1985; 1620-
25
4 Garibaldi BA, Britt NIR. Coleman NIL, Reading JC. Pace NL.
Risk factors for postoperative pneumnonia. Am J NIed 1981;
70:677-80
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from
CHEST I 104 I 4 I OCTOBER, 1993 1235
5 Cehis R, fo)rres A, Gatell JNI, Almela NI, Rodrigmmez-Roisin R,
Agusti-Vidal A. Nosx�mial pnetmmonia: a mtmltivariate analysis
of risk and prognosis. Chest 1988; 93:318-24
6 Seidenfeld JJ, Pohl DF, Bell RC, Harrys GD. Incidence, site
and O)IltcO)me O)f infections in patiemits with the adult respirato)r\
distress syndrome. Am Rev Respir Dis 1986; 134: 12-6
7 Torres A, Azmiar R, Gatell JM, Jinienez P. Gonzalez J, Ferrer A,
et al. Incidence, risk and prognosis factors of no)so)co)mial
pmieunlo)nia in mechanically ventilated patients. Am Rev Respir
Dis 199(); 142:523-28
8 Fagon JY, Chastre J, Domnart Y, Trouillet JL, Pierre J, Dame
Cli, et al. Nosox.omial pneunio)nia in patients receiving co)ntin-
IlOtis mnechamiical ventilatiomi: pro)spective analysis of52 episoxies
�5�itl� use O)f a pro)tected specimen brush and quantitative culture
techniques. Am Rev Respir Dis 1989; 139:877-84
9 Meduri CU. Ventilator asso)ciatecl � in patients with
respirato)ry failure: a diagnostic approach. Chest 1990; 97:1208-
19
10 \Veinstein RA. Selective intestinal decontamination: an infection
control mneasure whose time has come? Ann Intern Med 1989;
110:853-55
11 Van Saemie HKF, Stoutenbeek C� Lawimi P, Ledingham IMcA.
Update in imitemisive care and emergency medicine: infection
contro)l hw selective decontamination. 1st ed. Berlin: Springer-
Verlag, 1989
12 Comit#{233} de Consensus. Seventh Conference de comsensus en
r#{233}animnatio)n et medicine d’imrgence: microbial selective decomi-
taminatio)n in intensive care patients. Paris, December 13-14,
1991
13 American Thoracic Societ�� Standards for the diagnosis and care
of patients with chronic obstructive pulmonary disease (COPD)
and asthma. Ama Rev Respir Dis 1987; 136:225-44
14 Rimel R’iV, lvson G\V. The neumologic examinatio)mi in patients
�ith central miervous system trauma. J Netmrosurg Nurs 1979;
12: 148-52
15 Rello J, Qimintana E, Ausina Y Puzo C, Net A, Prats G. Risk
factors for Staphylococcus aureus mio)so)eomial pneurno)nia in
critically ill patients. Am Rev Respir Dis 1990; 142:1320-24
16 McCabe WR, Jackson GG. Gram-negative l)acteremia: etio)logy
and ecologs: Arch Intern Med 1962; 110:847-55
17 Emori GT, Cmilver DH, human TC, Jarvis \VR, White JW Olson
DR, et al. National noso)co)mial infections surveillance system
( NNIS): description ofsurveillance methods. Am J Infect Comitrol
1991; 19:19-35
18 Fagoii JY, Chastre J, liance AJ, Gimigimet NI , Troimillet JL, Doniart
Y, et al. Detection o)f no)so)eo)mnial lung infection in ventilated
patients: use O)f a I)rotectecl specimen brmmsh and quantitative
culture techniques in 147 patients. Am Rev Respir Dis 1988;
138:110-16
19 Wimberley NW, Bass JB, Boyd BW, Kirkpatrick MB, Serio BA,
Pollock JIM . Use O)f a bronchoscopic protected catheter brush
for the diagnosis of pimimnonary infections. Chest 1982; 82:556-
62
20 Edelstein PH. Improved semiselective medium for isolation of
Legionella pneunwphila from contaminated clinical and enviro)n-
mental specimens. J Clin Microbiol 1981; 14:298-303
21 Chastre J, Viau F, Brun P. Pierre J, Dange MC, Botichaine A.
Prospective evaluation of the protected specimen brush for the
diagnosis ofpulmonary infections in ventilated patients. Am Rev
Respir Dis 1984; 130:924-29
22 Lennette EH, Bullows A, Hausler WJ Jr. Shadomy HJ. ManualO)f clinical microbiology. 4th ed. Washington: American Society
for Microbiologs; 1985
23 Schlesselman JJ. Case-control studies: design, conduct, analysis.
New York: Oxford University Press, 1982
24 A’Court CH, Garrard ChS. Nosocomial pneumomiia in the
intensive care unit: mechanisms and significance. Thorax 1992;
47:465-73
25 Louria DB, Kaminski T The effects of four antimicrobial drug
regimens oti sputum superinfection in hospitalized patients. Am
Rev Respir Dis 1982; 85:649-85
26 Carratala J, Pallares R, Verdaguer R, Santin M , Mascaro J,Manresa F, et al. Risk factors for noso)co)mial pneumococcal
I)netlmo)mlia. Presented at the 31st Interscience Conference onAntimicrobial Agents and Chemotherapy, Chicago, October
1991
27 Rello J, Ricart M, Ausina V, Net A, Prats G. Pneumonia due to
Haenwphilus influenzae among mechanically ventilated patiemits:
incidence, otmtcome and risk factors. Chest 1992; 102: 1562-65
28 Graybill JR, Marshall LW, Charache P. Wallace CK, Melvin VB.
Nosox�omial pneumonia: a continuing major problem. Am Rev
Respir Dis 1973; 108:1130-40
29 Stevemis RM, Teres D, Skillman JJ, Feingold DS. Pneumonia iii
an intensive care unit. Arch Intern Med 1974; 134:106-11
30 Gross PA, Neim HC, Aswapokee P. Van Antwerpen C, Aswapokee
N . Deaths from nosocomial infection: experience in a university
hospital and a community hospital. Am J Med 1980; 68:219-23
31 Sheagren SN . Staphylococcus aureus: the persistent pathogen.
N Engl I Med 1984; 310: 1437-42
32 Peacock JE Jr, Marsik FJ, Wenzel RE Methicillin-resistant
Staphylococcus aureus: introduction and spread withimi a hospi-
tal. Ann Intern Med 1980; 93:526-32
33 Maki DG. Risk factors for nosocomial infection in intensive
care: devices vs nature and goals for the next decade. Arch
Intern Med 1989; 149:30-5
34 \Veinstein BA. Endemic emergence o)f cephalosporin-resistant
Entemobacter: relation to prior therapy. Infect Control 1986;
7(suppl):120-23
35 Hauser \VE JR. Remington JS. Effect on antibiotics on the
immune response. Am J Med 1982; 77:711-16
36 Johanson WIG Jr. Ventilator-associated pneumonia: light at the
end ofthe tunnel. Chest 1990; 97:1026-27
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from
1993;104; 1230-1235ChestJ Rello, V Ausina, M Ricart, J Castella and G Prats
ventilator-associated pneumonia.Impact of previous antimicrobial therapy on the etiology and outcome of
July 13, 2011This information is current as of
http://chestjournal.chestpubs.org/content/104/4/1230Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/104/4/1230#related-urlsThis article has been cited by 51 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
© 1993 American College of Chest Physicians by guest on July 13, 2011chestjournal.chestpubs.orgDownloaded from