
Multidimensional tomographic imaging using volume holography
Upload
independentCategory
view
1download
0
Cognitive Therapy and Research, Vol. 10, No. 2, 1986, pp. 187-200
Imagery Assessment By Self Report: A Multidimensional Analysis of Clinical Imagery
Kirk D. Strosahl 2 University of Washington
James Ascough Wabash Valley Mental Health Center
Arleen Rojas Purdue University
Two studies examined the theory that emotive-abstract, sensory modality, and control imagery are functionally distinct abilities and that emotive- abstract imagery and image control are directly related to the quality o f in- therapy imagery. In Study One, 199 subjects completed self-report measures o f sensory modality, molar imagery, and image control and completed an analogue clinical visualization task. In Study Two, 53 test-anxious covert behavior therapy participants completed the self-report battery and provid- ed ratings o fin-therapy image clarity. Results indicated that emotive~abstract imagery, sensory modality imagery, and image control are factorially distinguishable abilities; a cross-sample factor analysis revealed some instabili- ty but a theoretically consistent pattern o f results. Regression analyses demonstrated that emotive-abstract imagery abilities were the best predic-
11 wish to thank the two anonymous reviewers of an earlier version of this paper, whose comments were exceedingly helpful in preparing the present version. My thanks also to Philip C. Kendall for his valuable suggestions.
2Address all correspondence to Kirk Strosahl, Department o f Psychology, NI-25, University of Washington, Seattle, Washington 98195.
187
0147-5916/86/0400-0187505.00/0 © 1986 Plenum Publishing Corporation
188 Strosahl, Ascough, and Rojas
tors o f performance on the analogue task, whereas both image control and emotive imagery were related to the clarity o f in-therapy imagery. Results illustrate the qualitative difference between low- and high-order image pro- cesses and the possible interaction between emotive imagery and image con- trol. Implications for imagery assessment and individual differences research are discussed.
KEY WORDS: clinical imagery; imagery measures; factor analysis of emotive imagery; imagery control in psychotherapy.
A variety of cognitive behavior therapies use mental imagery as a means to achieve therapeutic objectives (cf. Cautela, 1971; Meichenbaum, 1977; Singer, 1974; Stampfl & Levis, 1967; Wolpe, 1958), although many issues remain regarding the role of imagery in the acquisition and maintenance of behavior change (Strosahl & Ascough, 1981a; Tower & Singer, 1981). An intuitively appealing and frequently discussed notion is that individual differences in certain imagery abilities moderate the effects of imagery-based therapies. Unfortunately, pertinent research has produced equivocal results (Beere, 1972; Davis, McLemore, & London, 1970; Dyckman & Cowan, 1978; McLemore, 1972; McSweeney, 1976), and investigations of imagery self-report measures further suggest that they are marginally adequate as research instruments (Danaher & Thoresen, 1972; McLemore, 1976; Rehm, 1973; Rimm & Bot- trell, 1969). This problem is compounded by the fact that alternative methods for assessing imagery (behavioral or physiological) lack the capacity to discriminate between good and poor imagers and do not correlate highly with self-report inventories of imagery ability (Strosahl & Ascough, 1981a).
Imagery assessment clearly is a major obstacle to meaningful individual differences research. In part, this is due to confusion regarding the struc- tural and functional properties of therapeutic imagery. Some covert therapies assume that images are "mental photographs," which act as "functional equivalents" to their real-life referents (cf. Cautela & Barron, 1977). Generally, this model emphasizes that vivid pictorial representations of threatening situa- tions are required for effective therapy. An alternative view emphasizes that images are multidimensional arrays of spatial, abstract, and emotional in- formation that, strictly speaking, cannot be rendered in pictorial form (Strosahl & Ascough, 1981a). A related concept is that imagery can be evaluated from both a structural (format of representation) and a functional (processing of formatted information) viewpoint. A long tradition of information-processing research supports the utility of this distinction (Kosslyn & Pomerantz, 1977; Paivio, 1978), and a series of clinical fear im- agery studies demonstrates the functional relationship between imagery and emotional behavior (Lang, 1977, Lang, Levin, Miller, & Kozak, 1983). As

Imagery Assessment 189
a first step in addressing the imagery assessment issue, one needs to specify and test those processes that are hypothesized in different models to under- pin the quality of in-therapy imagery, apart from any presumed functional impact upon level of therapeutic success. This research examined three im- agery processes that are commonly believed to be clinically relevant: sensory modality imagery, emotive-abstract imagery, and imagery control.
Sensory modality imagery is a critical ability in the mental photograph model and has been the object of study in most previous individual differences studies. The disappointing results of those studies may be due to the fact that sensory modality imagery ability is not a particularly significant predic- tor of in-therapy imagery. For example, the ability to imagine the smell of burnt toast (a representative sensory modality imagery item) hardly seems comparable to imagining oneself in an anxiety-producing situation. This ex- ample suggests that emotive and abstract processes may be required to im- bue any memory image with a clinically significant "valence." The ability to imagine complex conceptual relationships and emotional reactions may therefore be a central determinant of in-therapy image quality. At present, however, there is insufficient empirical evidence to conclude that emotive- abstract imagery is a qualitatively distinct form of imagery. Image control is an intriguing ability because it may act to "harness" images that have a strong negative valence. Further, image control has consistently been shown to be factorially distinguishable from sensory modality imagery (Hiscock, 1978; McLemore, 1976). On the basis of the preceding assumptions, we predicted that emotive-abstract imagery and image control would be more strongly related to in-therapy image quality than sensory modality imagery. This prediction was tested in two separate studies, one involving performance on an analogue visualization task and the other an examination of in-therapy imagery.
Imagery abilities may differ not only in their functional contribution to imagery in therapy but in their structural properties as well. McLemore (1976) suggested that there may be both state and trait components to im- agery. The well-documented inverse relationship between emotional arousal and image clarity suggests that emotive-abstract imagery is likely to be state- determined (Haney & Euse, 1976; Strosahl & Ascough, 1981b). Our hypothesis was that self-report measures of emotive-abstract imagery will exhibit low temporal stability but high internal consistency. Since different cognitive or affective processes may underpin emotive-abstract imagery, we predicted that these abilities will be factorially distinguishable from both sen- sory modality imagery and image control. These hypotheses were examined in a psychometric analysis of imagery self-report measures, a second major objective of Study One.
190 Strosahl, Ascough, and Rojas
STUDY ONE
Method
Subjects. Subjects were 199 introductory psychology students (92 male, 107 female) who received course credit for participation. No other screening criteria were used. Each subject attended a minimum of two and a maximum of three testing sessions. Sessions 1 and 2 were conducted 1 day apart; ses- sion 3 occurred 1 week after session 2. All subjects participated in the first two sessions; 132 subjects (59 male, 73 female) attended session 3 for addi- tional credit: Six of these subjects did not complete tasks properly and were excluded from data analyses.
Instruments and Procedure. During session 1, subjects completed the visual and auditory scales of the Betts Questionnaire (Sheehan, 1967), the Gordon Scale of Image Control (GOR; Gordon, 1949), and the imagery (IDQ- VIS) and verbal (IDQ-VERB) scales of the Individual Differences Question- naire (Hiscock, 1978). The latter measure assesses tendency to use a visual or verbal "cognitive style" and was included to evaluate its relationship to therapeutic imagery. The Betts and Gordon scales are widely used measures of sensory modality memory imagery and image control, respectively. Dur- ing session 2, subjects completed three emotive-abstract imagery question- naires and a revised measure of image control, developed for this study. The Emotive Imagery Inventory (EI) is a 14-item scale assessing ability to im- agine mild emotional responses (e.g., nostalgia) experienced by another per- son. The Abstract Image Inventory (AI) is a 12-item measure of capacity to form conceptual relationships between imagined objects (e.g., a man and a flag, imagine loyalty). The Positive-Negative Image Scale is a 16-item scale composed of highly negative (a person close to you dies) and positive (you are deeply in love) scenes. Image clarity ratings are summed to form separate positive (VP) and negative (VN) scales. Each experimental questionnaire is scaled on a 1 (image, concept, or emotion perfect) to 7 (no image, concept, or emotion present) scale. The Image Control Inventory is a 20-item measure, using a 1 (no control at all) to 5 (complete control) scale. Ten items are neutral valence scenes (ICNEU), adapted from the original Gordon scale and designed to eliminate the psychometric problems associated with the original scale's Yes-No-Uncertain scaling format (cf. Strosahl & Ascough, 1981a). Ten items involve negative valence scenes (ICNEG). Individual item ratings are summed to form image control scores. During session 3, subjects completed the experimental questionnaires again and participated in an analogue visualiza- tion task. The task required subjects to imagine personally relevant, emo- tionally arousing scenes, such as being trapped in an elevator or giving a talk in front of a large audience. Twenty scenes were imagined in succession, each for a period of 30 seconds, followed by a 1-minute rest period. During the
Imagery Assessment 191
II
<
O
<
e~. i , ~ i
O
>
,..¢
¢ '4
¢'4
~ t t -
~o~
,.Q c~
A
..=
?

192 Strosahl, Ascough, and Rojas
rest period, subjects rated scene clarity on a 1 (perfect clarity) to 7 (no image present), scale. After all scenes had been imagined, subjects rated their most negative scene, and the associated clarity rating was used as the criterion score.
RESULTS
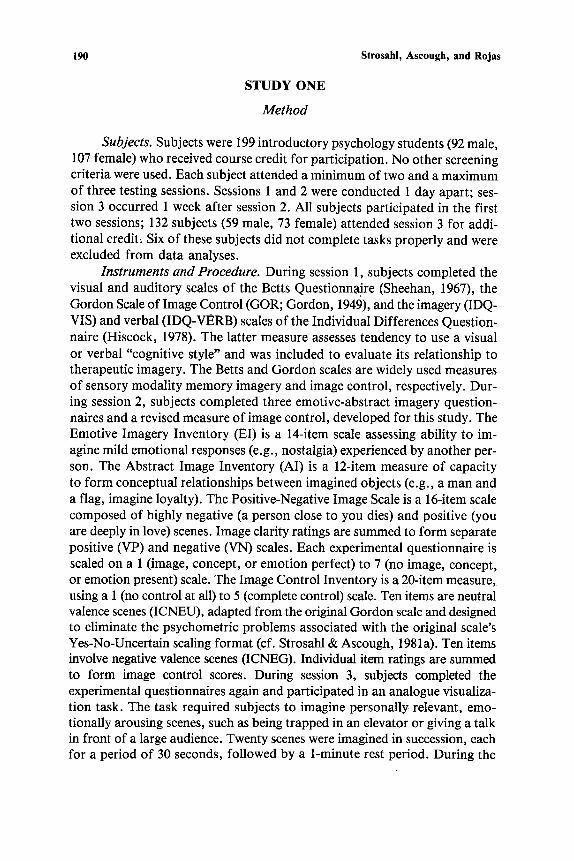
Principal Components Analysis. The correlation matrix for all imagery questionnaires was analyzed using principal components analysis without iteration and using varimax rotation (SPSS; Nie, Hull, Jenkins, Steinbren- ner& Bent, 1975). Components were ratained if their corresponding eigen- values exceeded 1. As Table I demonstrates, four components exist, each defining a theoretically consistent dimension of imagery ability. In accord with predictions, emotive-abstract imagery defines the first component, ac- counting for 22% of variation. The second and third factors define the separate dimensions of image control and sensory modality memory imagery. Interestingly, ICNEG and ICNEU define the image control factor, whereas the GOR fails to load significantly on any factor, supporting previous reports of its factor instability (Hiscock, 1978; McLemore, 1976). The IDQ-VIS and IDQ-VERB scales occupy the same factor, failing to replicate an earlier report of their factor separation (Hiscock, 1978). 3 Although these questionnaires share substantial common method variance, each component accounts for a significant amount of unique variance. This factor separation is more im- pressive when one considers the inherent bias of principal axis factoring to produce a disproportionately large first component (Mulaik, 1972). 4
Reliability Analyses. Test-retest reliability coefficients for the EI, AI, VP, and VN were .46, .44, .35, and .34. For the ICNEU and ICNEG, these figures were .55 and .43. Internal consistency was computed using the split- half method. The resulting coefficients for the EI, AI, VP, and VN were .85, .82, .79, and .77, while similar analyses of the ICNEU and ICNEG pro- duced values of .89 and .85. As predicted, emotive-abstract imagery ability conforms closely to a state performance model.
Regression Analyses. Hierarchical stepwise regression analyses were used to identify, among the imagery self-report measures, the most efficient predic- tors of performance on the analogue visualization task (cf. Cohen & Cohen, 1975). Grouping of variables and order of entrance were based upon the prin- cipal components analysis. A conservative test of prediction was made possi- ble by having subjects complete the prediction battery 1 week prior to the
3PCA analysis of these data separately for males and females revealed similar composition and ordering of components.
4A common factor analysis (CFA) was conducted to identify the stability of resuts using different factoring methods. The factor pattern was extremely similar to that obtained using PCA.
Imagery Assessment 193
criterion task. Results indicated that emotive-abstract imagery was a signifi- cant predictor of performance (F(4, 121) = 3.83, p < .01, r 2 = . 15); no other variable sets added significantly to the prediction equation. Protected F tests, designed to test each individffal member of this prediction group (cf. Cohen & Cohen, 1975), revealed that the ability to imagine abstract relationships (AI) and highly negative events (VN) were significant contributors to the observed prediction effect. To assess the incremental validity of the emotive-abstract imagery measures relative to sensory modality imagery, order of hierarchical entrance was changed so that the visual (VI) and auditory (AU) imagery scales were entered first, followed by the emotive-abstract imagery group. Results indicated that sensory modality imagery did not predict performance on the analogue visualization task (F(2, 123) = 1.25, p < . 15). However, a signifi- cant prediction effect again emerged when emotive-abstract imagery entered the equation at the next step (F(6, 119) = 2.95, p < .05, r 2 = .18).
STUDY TWO
Method
Subjects. Subjects were 55 test-anxious Purdue University students (22 males, 33 females), with a mean age of 20.7, who participated in a test-anxiety treatment program using covert behavior therapy. Each participant completed the Suinn Test Anxiety Behavior Scale (Suinn, 1969), the Test Anxiety Scale (Sarason, 1972), and the Debilitating Anxiety Scale of the Alpert-Haber Achievement Anxiety Test (Alpert & Haber, 1963) and scored above 130, 20, and 30 on these measures. Two subjects did not complete questionnaires properly and were excluded.
Instruments. Self-report imagery measures were identical to those used in Study One and were completed prior to the first treatment session. A state imagery assessment procedure was used to allow subjects to rate the quality of their in-therapy imagery. State ratings were obtained after the first and last time a test-anxiety scene was imagined. With the image in mind, subjects provided an image clarity rating using a 1 (image perfect) to 5 (no image at all) finger signal system; ratings were recorded by therapists on a standard protocol. The treatments used 15 standard test-anxiety scenes, and therefore a total of 30 image clarity ratings were obtained across the course of therapy. These ratings were used as the criteria in the regression analyses.
Treatments. Treatments were systematic desensitization (n = 23), covert modeling (n = 20), and prolonged controlled exposure (n = 10). (Detailed descriptions of each treatment procedure and method of subject assignment are available from the first author.) Briefly, five treatment sessions involved the structured use of in-therapy imagery. On average, three test-anxiety- relevant situations were imagined during each therapy session. Scene descrip-
194 Strosahl, Ascough, and Rojas
tions varied in the amount of detail provided by therapists. Covert modeling scenes described an initial anxiety response, adaptive responses, and positive consequences following modeled responses. Desensitization and prolonged exposure scenes simply described the anxiety-provoking situation.
Results
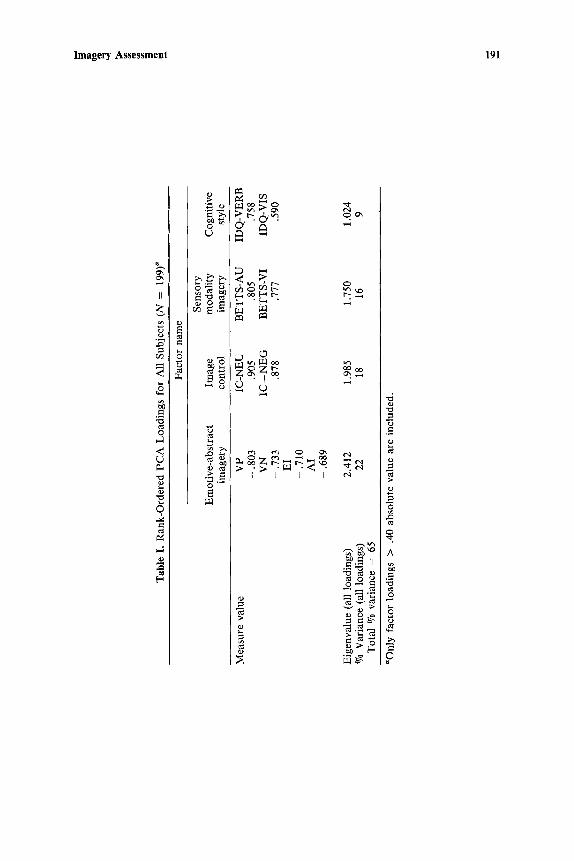
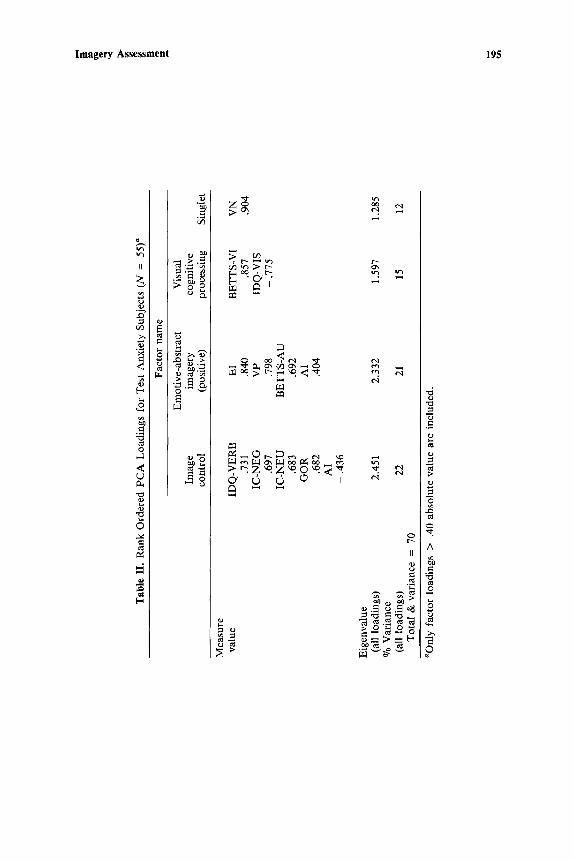
Replication Principal Components Analysis. Correlations among the pretreatment imagery self-report measures were analyzed using the principal components method; results are presented in Table II. As can be seen, the ordering and composition of factors is somewhat different from that observed in Study One. The first component clearly defines an image control dimen- sion, with an unexpectedly strong contribution from verbal cognitive style. The second component is largely defined by the emotive-abstract imagery measures but is not as well identified as the emotive imagery component noted in Study One. In addition, capacity for highly negative imagery (VN) does not load on the emotive-abstract imagery factor but instead appears as an uninterpretable singlet factor. The third factor represents a general visual/representational dimension and is consistent with research relating visual cognitive style to visual sensory modality imagery ability (Hiscock, 1978).
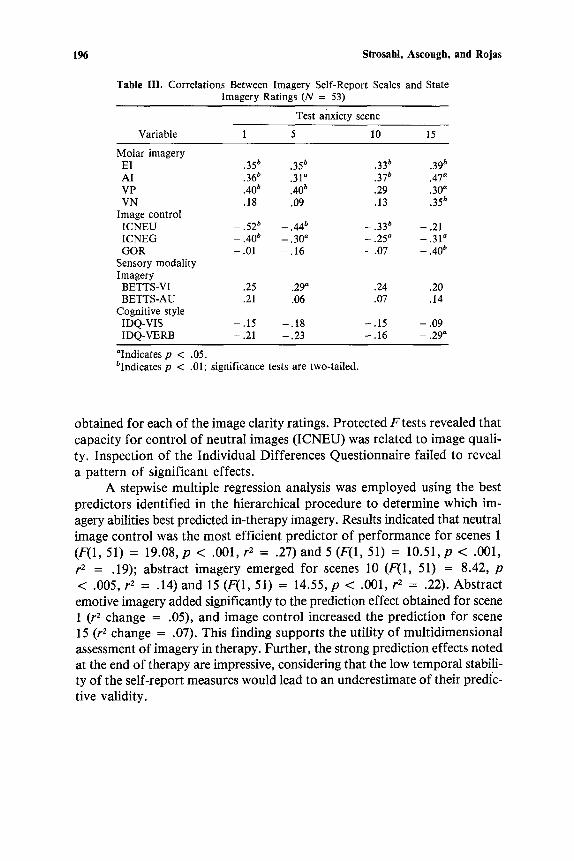
Regression Analyses. Correlations between the imagery self-report measures and in-therapy imagery ratings were first computed separately by treatment and were analyzed using z-score comparisons. No pattern of signifi- cant differences was found to exist as a function of treatment condition. Hierarchical regression analysis was used to determine which imagery self- report measures best predicted in-therapy image clarity ratings. Variable sets were grouped and entered as in Study One. The criteria were in-therapy im- age clarity ratings obtained after the first visualization of test-anxiety scenes 1, 5, 10, and 15. The use of multiple image clarity criteria allowed any changes in the predictive capacity of the self-report measures over the course of therapy to be identified. Table III presents correlations between the self-report measures and the image clarity criteria. Results indicated that emotive-abstract imagery ability did not consistently predict in-therapy image clarity, although a significant prediction effect was obtained for test-anxiety scenes 1 and 15. Protected F tests did not reveal a significant predictor for the scene 1 predic- tion effect but did show that capacity for abstract imagery was significantly related to image clarity during scene 15. Visual and auditory sensory modality imagery failed to produce a significant prediction effect for any of the criteria, suggesting that this type of imagery may not be a prominent factor in deter- mining the quality of in-therapy imagery. Inspection of image control revealed a strong association with image clarity, as significant prediction effects were
Imagery Assessment 195
II
<
0 ,.a < u
©
~ ~ ' ~ > o
~aO~
~g ~ U
z~
u~
¢'4
II
..=
c~
A
o
?
1 9 6 S t r o s a h l , A s c o u g h , a n d R o j a s
Table I I I . Correlat ions Between Imagery Self-Report Scales and State Imagery Ratings (N = 53)
Test anxiety scene
Variable 1 5 10 15
Molar imagery EI .354 .35 b AI .364 .31" VP .404 .404 VN .18 .09
Image control I C N E U - .52 b - .444 I C N E G - .404 - . 3 0 " G O R - .01 - . 16
Sensory modali ty Imagery
BETTS-VI .25 .29" BETTS-AU .21 .06
Cognitive style IDQ-VIS - . 15 - . 18 IDQ-VERB - .21 - .23
.334 .394
.374 .47"
.29 .30"
.13 .354
- .334 - .25 a - .07
- . 21
- . 31 ~ - .404
.24 .20
.07 .14
- .15 - .16
- . 0 9
- . 2 9 "
"Indicates p < .05. blndicates p < .01; significance tests are two-tailed.
obtained for each of the image clarity ratings. Protected F tests revealed that capacity for control of neutral images (ICNEU) was related to image quali- ty. Inspection of the Individual Differences Questionnaire failed to reveal a pattern of significant effects.
A stepwise multiple regression analysis was employed using the best predictors identified in the hierarchical procedure to determine which im- agery abilities best predicted in-therapy imagery. Results indicated that neutral image control was the most efficient predictor of performance for scenes 1 (F(1, 51) = 19.08, p < .001, r z = .27) and 5 (F(1, 51) = 10.51, p < .001, r 2 = .19); abstract imagery emerged for scenes 10 (F(1, 51) = 8.42, p < .005, r 2 = .14) and 15 (F(1, 51) = 14.55, p < .001, r 2 = .22). Abstract emotive imagery added significantly to the prediction effect obtained for scene 1 (r 2 change = .05), and image control increased the prediction for scene 15 (r z change = .07). This finding supports the utility of multidimensional assessment of imagery in therapy. Further, the strong prediction effects noted at the end of therapy are impressive, considering that the low temporal stabili- ty of the self-report measures would lead to an underestimate of their predic- tive validity.
Imagery Assessment 197
DISCUSSION
These results suggest that emotive-abstract imagery is a factorially distinct ability and is an important determinant of in-therapy image quality. In ad- dition, the ability to control images emerged as a surprisingly important predictor of in-therapy imagery, whereas sensory modality imagery failed to emerge as a clinically relevant ability. The latter finding is disappointing because previous individual differences studies have assumed that sensory modality imagery ability is in fact related to the quality of in-therapy imagery.
This pattern of results suggests that clinical imagery is not a static, quasi- visual process, as is implied in the mental photograph model. Rather, therapeutic imagery may be a multidimensional process requiring "input" from a number of different cognitive and affective processes. These diverse abilities may combine to determine the "integrity" of clinical imagery (Strosahl & Ascough, 1981b). One can speculate that the imagery processing system is organized along a continuum of complexity, ranging from molar imagery to more concrete representational/memory imagery. As imagery becomes more complex and emotively charged (as is true in therapy), performance is increasingly state-determined, and trait level assessments may lose preci- sion and relevance. Thus, state imagery assessment may be a particularly ef- fective strategy in individual differences studies, where proximity to the events that presumably underpin behavior change is critical. Theoretically, individual differences could exist in either the structural or functional realms. There may also be abilities that help "bridge" structural integrity and functional processing of information (i.e., image control).
Variations were noted in the imagery abilities that predicted performance on the analogue versus in-therapy imagery tasks. In general, emotive-abstract imagery ability was strongly related to the quality of imagery on the analogue task, whereas image control was not significant. During therapy, both abilities emerged as important. What factor(s) may explain this different pattern of results? Subjects in the behavior therapy study sought help for debilitating test anxiety and were asked to imagine personally relevant, anxiety-producing situations. Image control was an important ability for these individuals, perhaps because image control not only allows one to sustain a negatively charged image but is necessary for one to reappraise negative cognitions and manipulate the imagined target situation in ways that reduce its negative valence (Strosahl & Ascough, 1981a). The revised image control scale used in this study emerged as factorially stable and exhibited significant predic- tive validity. It is hoped that this measure can overcome the undesirable
198 Strosahl, Aseough, and Rojas
characteristics of the original Gordon scale (cf. White & Ashton, 1977) and permit a better examination of image control as an individual differences variable.
What can be said about the individual differences hypothesis in light of present results? One conclusion is that current knowledge about the struc- tural properties of therapeutic imagery is limited, and this precludes sophisticated research into the functional impact of individual differences. For example, the structural properties of the internal imagery field during therapy are virtually unknown, although a series of innovative information- processing studies demonstrates the potential for extending this kind of research to the clinical setting (cf. Kosslyn, 1975, 1976, 1978). In addition, current theories do not adequately specify the nature of individual differences that are argued to moderate level of therapeutic success. Without a clear con- ception of how therapeutic imagery is organized and the conditions under which the content, format, or processing of imagery is altered, one cannot empirically isolate functionally significant individual differences. Results sug- gest a need for revisions in current theories of psychotherapeutic imagery to permit sound research designs and meaningful, consistent results.
REFERENCES
Alpert, R., & Haber, R. (1963). Anxiety in academic achievement situations. Journal o f Ab- normal and Social Psychology, 61, 207-215.
Beere, D. (1972). Systematic desensitization and imagination: A test of London's cognitive in- tegration of behavior therapies. Dissertation Abstracts International, 32, 5432B-5432B.
Cautela, J. (1971). Covert modeling. Paper presented at the annual convention of the Associa- tion for the Advancement of Behavior Therapy, Washington D.C.
Cautela, J., & Baron, M. (1977). Covert: conditioning: A theoretical analysis. Behavior Modifica- tion, 1, 351-368.
Cohen, A., & Cohen, R. (1975). Applied multiple regression analysis for the social sciences. New York: Wiley.
Danaher, B., & Thoresen, L. (1972). Imagery assessment by self report and behavior measures. Behaviour Research and Therapy, 10, 132-138.
Davis, D., McLemore, C., & London, P. (1970). The role of visual imagery in desensitization. Behaviour Research and Therapy, 8, 11-13.
Dyckman, J., & Cowan, P. (1978). Imaging vividness and the outcome of in vivo and imagined scene desensitization. Journal of Consulting and Clinical Psychology, 46, 1155-1156.
Gordon, R. (1949). An investigation into some of the factors that favour the formation of stereotyped images. British Journal o f Psychology, 39, 156-157.
Haney, J., & Euse, F. (1976). Skin conductance and heart rate responses to neutral positive and negative imagery: Implications for covert behavior therapy procedures. Behavior Therapy, 7, 494-503.
Hiscock, M. (1978). Imagery assessment through self-report: What do imagery questionnaires measure? Journal of Consulting and Clinical Psychology, 46, 223-230.
Kosslyn, S. (1975). Information representation in visual images. Cognitive Psychology, 7, 341-370. Kosslyn, S. (1976). Can imagery be distinguished from other forms of internal representation?
Evidence from studies of information retrieval time. Memory and Cognition, 4, 291-297.
Imagery Assessment 199
Kosslyn, S. (1978). Measuring the visual angle of the mind's eye. Cognitive Psychology, 10, 356-389.
Kosslyn, S., & Pomerantz, J. (1977). Imagery, propositions and the form of internal represen- tation. Cognitive Psychology, 9, 52-76.
Lang, P. (1977). Imagery in therapy: An information processing analysis of fear. Behavior Therapy, 8, 862-886.
Lang, P., Levin, D., Miller, G., & Kozak, M. (1983). Fear behavior, fear imagery, and the psychophysiology of emotion: The problem of affective response integration. Journal of Abnormal Psychology, 92, 276-306.
McLemore, C. (1972). Imagery in desensitization. Behaviour Research and Therapy, 10, 51-57. McLemore, C. (1976). Factorial validity of imagery measures. Behaviour Research and Therapy,
14, 399-408. McSweeney, A. (1976). Imagery as a variable in the efficacy of systematic desensitization. Disser-
tation Abstracts International, 36(10-B), 5271. Meichenbaum, D. (1977). Cognitive behavior modification: An integrative approach. New York:
Plenum Press. Mulaik, S. (1972). The foundations of factor analysis. New York: McGraw-Hill. Nie, N., Hull, C., Jenkins, Jo, Steinbrenner, K., & Bent, D. (1975). Statisticalpackagefor the
social sciences. New York: McGraw-Hill. Paivio, A. (1978). Mental comparisons involving abstract attributes. Memory and Cognition,
6, 199-208. Rehm, L. (1973). Relationships among measures of visual imagery. Behaviour Research and
Therapy, 11, 252-264. Rimm, D., & Bottrell, J. (1969). Four measures of visual imagination. Behaviour Research and
Therapy, 7, 63-69. Sarason, I. (1972). Experimental approaches to test anxiety: Attention and the uses of infor-
mation. In C. Spielberger (Ed.), Anxiety: Current trends in theory and research (Vol. 2). New York: Academic Press.
Sheehan, P. (1967). A shortened form of the Betts Questionnaire upon Mental Imagery. Jour- nal of Clinical Psychology, 23, 386-389.
Singer, J. (1974). Imagery and daydream methods in psychotherapy and behavior modifica- tion. New York: Academic Press.
Stampfl, T., & Levis, D. (1967). Essentials of implosive therapy: A learning theory based psychodynamic therapy. Journal of Abnormal Psychology, 72, 496-503.
Strosahl, K., & Ascough, J. (1981a). Clinical uses of mental imagery: Experimental founda- tions, theoretical misconceptions and research issues. PsychologicalBulletin, 89, 422-438.
Strosahl, K., & Ascough, J. (1981b). A multiple component model of clinical imagery: Theoretical and empirical issues. In E. Klinger (Ed.), Imagery: Concepts, results and applications. New York: Plenum Press.
Suinn, R. (1969). The STABS, a measure of test anxiety for behavior therapy: Normative data. Behaviour Research and Therapy, 7, 335-339.
Tower, R., & Singer, S. (1981). The measurement of imagery: How can it be clinically useful? In P. Kendall & S. Hollon (Eds.), Assessment strategies for cognitive behavioral interven- tions. New York: Academic Press.
White, K., & Ashton, R. (1977). Visual imagery control: One dimension or four? Journal of Mental Imagery, 2, 245-252.
Wolpe, J. (1958). Psychotherapy by reciprocal inhibition. Stanford: Stanford University Press.
Copyright © 2022 FDOKUMEN




















