Assessment of methyl thiophanate–Cu (II) induced DNA damage in human lymphocytes

IL-23 Inhibits Osteoclastogenesis Indirectly throughLymphocytes and Is Required for the Maintenance of BoneMass in Mice1
Julian M. W. Quinn,2*† Natalie A. Sims,*† Hasnawati Saleh,*† Danijela Mirosa,*Keith Thompson,*‡ Stelios Bouralexis,* Emma C. Walker,* T. John Martin,*†
and Matthew T. Gillespie*†
IL-23 stimulates the differentiation and function of the Th17 subset of CD4� T cells and plays a critical role in chronic inflam-mation. The IL-23 receptor-encoding gene is also an inflammatory disease susceptibility gene. IL-23 shares a common subunit withIL-12, a T cell-dependent osteoclast formation inhibitor, and we found that IL-23 also dose-dependently inhibited osteoclasto-genesis in a CD4� T lymphocyte-dependent manner. When sufficiently enriched, �� T cells also mediated IL-23 inhibition. LikeIL-12, IL-23 acted synergistically with IL-18 to block osteoclastogenesis but, unlike IL-12, IL-23 action depended on T cellGM-CSF production. IL-23 did not mediate IL-12 action although IL-12 induced its expression. Male mice lacking IL-23 (IL-23p19�/�) had �30% lower bone mineral density and tibial trabecular bone mass (bone volume (BV)/total volume (TV)) thanwild-type littermates at 12 wk and 40% lower BV/TV at 26 wk of age; male heterozygotes also had lower bone mass. FemaleIL-23p19�/� mice also had reduced BV/TV. IL-23p19�/� mice had no detectable osteoclast defect in trabecular bone but IL-23p19�/� had thinner growth plate hypertrophic and primary spongiosa zones (and, in females, less cartilage remnants) comparedwith wild type. This suggests increased osteoclast action at and below the growth plate, leading to reduced amounts of maturetrabecular bone. Thus, IL-23 inhibits osteoclast formation indirectly via T cells in vitro. Under nonpathological conditions (unlikeinflammatory conditions), IL-23 favors higher bone mass in long bones by limiting resorption of immature bone forming belowthe growth plate. The Journal of Immunology, 2008, 181: 5720–5729.
T he formation of osteoclasts from myelomonocytic pro-genitors, a critical point of control of osteolysis, is pow-erfully influenced by factors released by T cells (1, 2).
Osteoclast formation requires two essential factors, namely, M-CSF and receptor activator of NF-�B ligand (RANKL),3 a TNF-related ligand (3, 4). RANKL also plays important roles in cell-mediated immunity and is essential for lymph node organogenesis(5–7). Hormonally regulated expression of membrane-boundRANKL by osteoblasts constitutes the major physiological controlof osteoclastogenesis (8), but activated T lymphocytes also pro-duce significant amounts of membrane-bound and soluble RANKL(9, 10). Activated T cells can thus stimulate osteoclast formationand osteolysis and contribute to pathological osteolysis in peri-odontal disease and rheumatoid arthritis (9, 11). Sato et al. (12)
found that the major source of T cell-derived RANKL derivesfrom activated Th17 cells, a population recently defined as IL-17-secreting Th cells distinct from Th1 or Th2 subsets and whichrequires IL-23 for maturation and cytokine secretion. Th17 cells,IL-17, and IL-23 are emerging as critical agents in chronic auto-immune disease models (13, 14), and the common association ofchronic inflammation with osteolysis may be explained by acti-vated Th17 cell production of RANKL and the pro-osteolytic cy-tokine IL-17.
In contrast to activated T cell stimulation of osteolysis, naiveor nonactivated T cells mediate inhibitory actions of severalcytokines on osteoclasts, including IL-4, IL-18, and IL-12 (15–17). Some immunosuppressants also cause clinical and experi-mental bone loss (18). Such observations raise the possibilitythat under normal physiological conditions T cells mediate sig-nificant antiosteolytic effects, but contribute to bone loss underlocal inflammatory conditions that result in high levels of T cellactivation.
IL-23 is a heterodimeric cytokine structurally related to IL-12.IL-12 is a p35/p40 heterodimer which promotes Th1 developmentand suppresses Th2. IL-12 induces IFN-� secretion by Th1 andNK cells (19) and synergizes with IL-18 via reciprocal enhance-ment of specific receptor subunits, which can greatly amplifyIL-12 actions (19, 20). IL-23 consists of an IL-12p40 subunit com-plexed with IL-23 specific p19 subunit (13, 19); receptors forIL-23 and IL-12 are also heterodimers sharing the IL-12R�1 sub-unit and activate many of the same signaling molecules (13, 21).IL-23 strongly stimulates IL-17 production by Th17 cells and stim-ulates IFN-� production though less potently than IL-12 (13).IL-23 also induces IL-17 production in �� T cells (22), a CD4� Tcell population with innate immune functions.
*St Vincent’s Institute, Fitzroy, Victoria, Australia; †Department of Medicine, Uni-versity of Melbourne, St. Vincent’s Hospital, Fitzroy, Victoria, Australia; and ‡Insti-tute of Medical Sciences, University of Aberdeen, Aberdeen, United Kingdom
Received for publication April 1, 2008. Accepted for publication August 17, 2008.
The costs of publication of this article were defrayed in part by the payment of pagecharges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.1 This work was supported by Program Grant 345401 from the National Health andMedical Research Council of Australia.2 Address correspondence and reprint requests to Dr. Julian Quinn, St. Vincent’sInstitute of Medical Research, 9 Princes Street, Fitzroy, Victoria 3065, Australia.E-mail address: [email protected] Abbreviations used in this paper: RANKL, receptor activator of NF-�B ligand;1,25(OH)2 D3, 1�,25-dihydroxyvitamin D3; BMM, bone marrow macrophage;pQCT, peripheral quantitative computer-aided tomography; Ct, cortical; Tb, trabec-ular; WT, wild type; BMD, bone mineral density; TRAP, tartrate-resistant acid phos-phatase; MNC, multinucleated cell; BV, bone volume; TV, Tb volume.
Copyright © 2008 by The American Association of Immunologists, Inc. 0022-1767/08/$2.00
The Journal of Immunology
www.jimmunol.org

The similarities of IL-12 and IL-23 structure and their elicitedsignaling pathways suggest that IL-23 may also affect osteoclastdifferentiation. We therefore studied the influence of IL-23 on os-teoclast formation and its dependence on T cells. In addition, todetermine whether IL-23 influences bone mass and structure, weexamined mice lacking the IL-23 p19 subunit. These mice havepreviously been characterized as resistant to induced autoinflam-matory challenge and as lacking Th17 responses. Our results sug-gest not only that IL-23 does indeed reduce osteoclast formation inthe presence of T cells but also that lack of IL-23 leads to signif-icantly lower levels of trabecular (Tb) bone mass in otherwiseunchallenged, healthy mice. Although several mechanisms of ac-tion of IL-23 could explain this effect, we have identified novel andunusual features of IL-23 null mice that point to a previously un-suspected way in which such a cytokine could affect bone massand structure.
Materials and MethodsC57BL/6J mice were obtained from the Animal Resource Centre (Perth,Australia). IL-23p19�/� (C57BL6/J background) mice were provided byDr N. Ghilardi (Genentech, San Francisco, CA) and have previously beencharacterized as having an abnormal hypersensitivity response (23–25).Mice were maintained at St. Vincent’s Hospital Campus (Fitzroy, Austra-lia) and procedures approved by the Animal Ethics Committee at St. Vin-cent’s Health (Fitzroy, Australia). Littermate controls from heterozygouscrosses were used. Cells were cultured in �-MEM (Life Technologies) with10% FBS (CSL Biosciences). Recombinant GST-RANKL158–316
(RANKL) was produced using a bacterial construct provided by Dr. F.Patrick Ross (Washington University School of Medicine, St. Louis, MO).Other recombinant proteins were obtained from R&D Systems. 1�,25-di-hydroxyvitamin D3 (1,25(OH)2 D3) was obtained from Wako Pure Chem-ical. Other reagents were analytical grade obtained from Sigma-Aldrichunless noted.
Cells and assays
Spleen cells were obtained by spleen disaggregation through a fine wiresieve (16). Lymphocytes were extracted from spleen cells (16) by immu-nomagnetic Dynabeads (Dynal) coated with Abs to B220 (B cells), Thy1.2(pan-T cells), L3T4 (CD4� cells), or Lyt2 (CD8� cells). �� T cells wereisolated using a Miltenyi Biotec kit according to the manufacturer’s in-structions. Bone marrow cells were flushed from long bones with sterilesaline (26) and bone marrow macrophages (BMM) prepared as previouslydescribed (26). Osteoblasts were prepared from newborn mice calvariae bysequential digestion with 0.1% collagenase/0.2% dispase (Godo Shusei).Osteoclasts were generated in 10-mm diameter culture wells (Greiner Bio-One) seeded with 5 � 105 spleen cells/well or 105 bone marrow or BMMper well and stimulated with RANKL (100 ng/ml) and M-CSF (30 ng/ml)(26); cells were fixed and histochemically stained to identify tartrate-re-sistant acid phosphatase (TRAP)-positive multinucleated cells (MNCs),previously validated as osteoclasts (26). Alternatively, spleen cells orBMM were cocultured with 2 � 104 osteoblasts or Kusa O cells (27) and
10�8 M 1,25(OH)2 D3. To investigate osteoblast mineralization, cells wereseeded (5 � 104/well) in 16-mm diameter culture wells (Greiner Bio-One)in MEM/FBS with 50 �g/ml ascorbate, 10 mM �-glycerophosphate, and10 nM dexamethasone and incubated for 21 days, with medium and me-diators changed every 3 days. Cells were ethanol fixed, immersed in 0.5%alizarin red (pH 4.2) for 30 min, rinsed in PBS, and incubated in 10%cetylpyridinium chloride, and eluted alizarin red was measured by spec-trophotometer (28).
Flow cytometry determination of �� T cell numbers
Spleen cells (106) from four mice were incubated in PBS with 2% FBS andanti-mouse FcR Ab (2.4G2 hybridoma supernatant), rinsed, incubated in 1�g/ml PE-labeled GL3 anti-mouse �� TCR Ab (BD Bisociences), rinsed,and paraformaldehyde fixed. Forty thousand viable cells per sample (usingforward/side scatter gating) were analyzed by single-color flow cytometry(FACSCalibur; BD Biosciences). Negative controls were incubated in anti-FcR Ab alone.
Analysis of mRNA expression
RNA was isolated using TRIzol reagent (Invitrogen) according to the man-ufacturer’s instructions. RNA was then treated with RNase-free DNase(Roche Diagnostics) for 30 min at 37°C. RNA concentration was deter-mined by spectrophotometer (Nanodrop ND1000). cDNA was synthesized(random hexamers, 10 mM dNTP, 5� First Strand Buffer, 0.1 M DTT,RNaseOUT, and Superscript III RT (200 U/�l)) using 2 �g of startingmaterial under the following conditions: 5 min at 65°C, 5 min at 4°C, 60min at 50°C, 15 min at 70°C, and 8 min at 4°C (Bio-Rad iCycler). Real-time PCR analysis (Stratagene Mx3000P) of cDNA was performed usingPlatinum SYBR Green qPCR supermix UDG (Invitrogen) according to themanufacturer’s instructions and the following conditions: 1 cycle for 10min at 95°C; 40 cycles for 30 s at 95°C, 1 min at 60°C, 30 s at 72°C and1 cycle for 1 min at 95°C, 30 s at 55°C, 0 s at 95°C normalized to hypo-xanthine phosphoribosyltransferase (HPRT). IL-23p19 and IL-23R mRNAwere analyzed by semiquantitative RT-PCR as previously described (29).Oligonucleotide primer sequences (Table I) were obtained from Primer-bank (30).
Peripheral quantitative computer-aided tomography (pQCT)analysis of murine femora
Femoral cortical (Ct) and Tb bone mineral density (BMD), femoral cir-cumference, and femoral Ct thickness were measured by pQCT (StratecX-CT Research SA�, version 5.5) by methods adapted from Sims et al.(31). Metaphyseal scans of the distal femur were taken at a resolution of 70�m; Tb and Ct measurements (including circumference) were taken at adistance proximal to the distal growth plate of 5 and 25% of the length ofthe femur, respectively; Tb BMD was determined as the inner 45% of thetotal area (peel mode 20).
Bone histomorphometric analysis of murine tibia and femora
Tibiae were collected at 4, 12, or 26 wk of age, fixed in 4% paraformal-dehyde in PBS, and embedded in methylmethacrylate (32). Double fluo-rochrome labeling was performed with calcein injections 10 and 3 days
Table I. Sequences of oligonucleotide primers used for RT-PCR analysis
Gene GenBank No. Description Sequence
GM-CSF NM_009969 Forward TCGTCTCTAACGAGTTCTCCTTReverse GCAGTATGTCTGGTAGTAGCTGG
IL-17A NM_010552 Forward TGTCTCTGATGCTGTTGCTGReverse CTTTCCCTCCGCATTGACAC
IL-17A NM_010552 Forward TGTCTCTGATGCTGTTGCTGReverse CTTTCCCTCCGCATTGACAC
IFNg NM_008337 Forward AGCTCTTCCTCATGGCTGTTReverse TGTGGGTTGTTGACCTCAAAC
IL-23R NM_144548 Forward (1) TTCAGATGGGCATGAATGTTTCTReverse TTCAGATGGGCATGAATGTTTCTForward (2) CAGCTCGGATTTGGTATAAAGGC
IL-12Rb1 NM_008353 Forward ATGGCTGCTGCGTTGAGAAReverse CGGTGTGGGTATGGTTCGG
HPRT J00423 Forward TGATTAGCGATGATGAACCAGReverse AGAGGGCCACAATGTGATG
5721The Journal of Immunology
before tissue collection (32). Five-micrometer sections were stained withtoluidine blue or stained with xylenol orange for fluorochrome labels ac-cording to standard procedures using the Osteomeasure System (Osteo-
Metrics). Bone and growth plate histomorphometric parameters were mea-sured as previously described (32); safranin O-stained cartilage remnantswere measured as described elsewhere (33). Femoral length and width
****
**
Spleen CellsA
0
50
100
150
200
Neg. 0 0.01 0.1 1 10 20
BMCells
BMM precursors
0
100
200
300
RAW264.7 cells
IL-23 (ng/ml)0 20 0 20 0 20
TRA
P+
MN
C/w
ell
TRA
P+
MN
C/w
ell
Control IL-23 (ng/ml)IL-23, Day 0-3: 0 20 0IL-23, Day 3-7: 0 0 20
**TRA
P+
MN
C/w
ell
0
100
200
B C
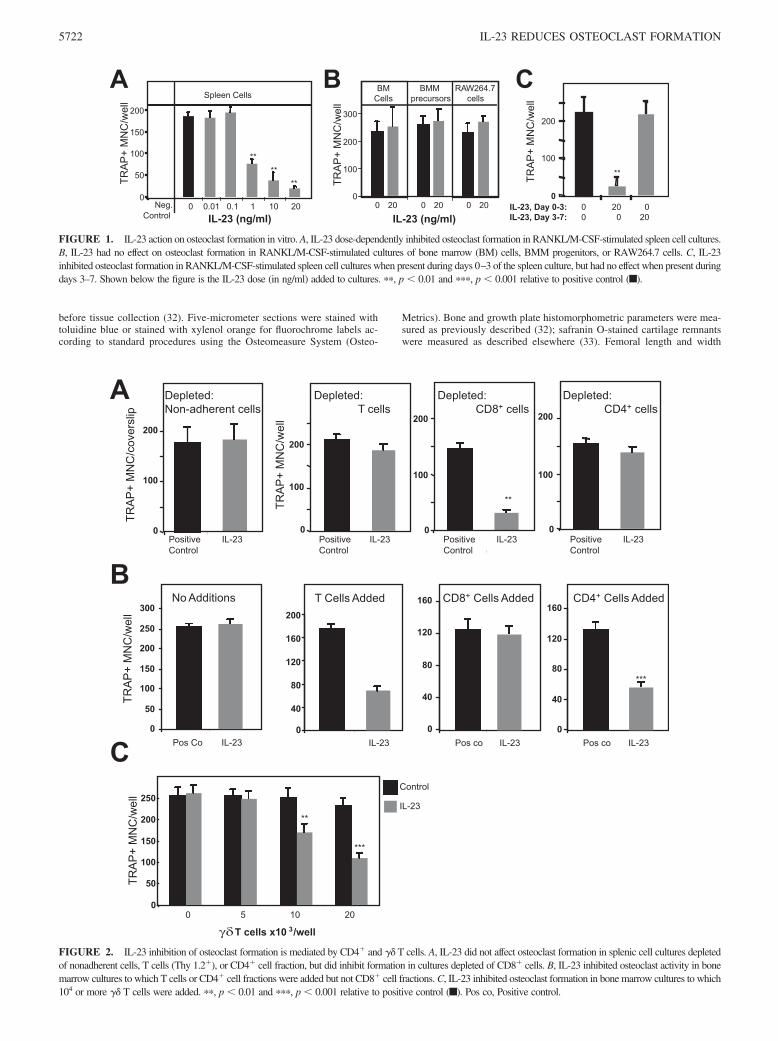
FIGURE 1. IL-23 action on osteoclast formation in vitro. A, IL-23 dose-dependently inhibited osteoclast formation in RANKL/M-CSF-stimulated spleen cell cultures.B, IL-23 had no effect on osteoclast formation in RANKL/M-CSF-stimulated cultures of bone marrow (BM) cells, BMM progenitors, or RAW264.7 cells. C, IL-23inhibited osteoclast formation in RANKL/M-CSF-stimulated spleen cell cultures when present during days 0–3 of the spleen culture, but had no effect when present duringdays 3–7. Shown below the figure is the IL-23 dose (in ng/ml) added to cultures. ��, p � 0.01 and ���, p � 0.001 relative to positive control (f).
B
C
A Depleted: CD4+ cells
PositiveControl
IL-23PositiveControl
IL-23
Depleted:Non-adherent cells
PositiveControl
IL-23
Depleted: T cells
PositiveControl
IL-23
Depleted: CD8+ cells
**
0
100
200
0
100
200
0
100
200
0
100
200
0
50
100
150
200
250
300
Pos Co IL-23
No Additions
Pos co IL-23
***
CD4+ Cells Added
Pos co IL-23
CD8+ Cells Added
0
40
80
120
160
200
IL-23
T Cells Added
0
40
80
120
160
0
40
80
120
160
TRA
P+
MN
C/c
over
slip
TRA
P+
MN
C/w
ell
TRA
P+
MN
C/w
ell
γδ 3
Control
IL-23
0
50
100
150
200
250
0 5 10 20
***
**
T cells x10 /well
TRA
P+
MN
C/w
ell
FIGURE 2. IL-23 inhibition of osteoclast formation is mediated by CD4� and �� T cells. A, IL-23 did not affect osteoclast formation in splenic cell cultures depletedof nonadherent cells, T cells (Thy 1.2�), or CD4� cell fraction, but did inhibit formation in cultures depleted of CD8� cells. B, IL-23 inhibited osteoclast activity in bonemarrow cultures to which T cells or CD4� cell fractions were added but not CD8� cell fractions. C, IL-23 inhibited osteoclast formation in bone marrow cultures to which104 or more �� T cells were added. ��, p � 0.01 and ���, p � 0.001 relative to positive control (f). Pos co, Positive control.
5722 IL-23 REDUCES OSTEOCLAST FORMATION
were determined from contact X-rays measured using NIH Image 1.62(32).
Statistical analysis
Data are shown as mean � SE. Cell culture data are pooled from more thanthree independent experiments. For mRNA expression, triplicate analysesof two independent experiments were performed and statistical significancewas determined by Student’s t test. Bone histomorphometric analyses usedeight mice per category that were analyzed by one-way ANOVA withFisher’s post hoc test.
ResultsIL-23 inhibits osteoclast formation in the presence of T cellsin vitro
When spleen cells were stimulated with RANKL and M-CSF, nu-merous osteoclasts were formed; this was dose-dependently inhib-ited by IL-23 (Fig. 1A). Maximal effects were seen at 20 ng/ml,which reduced osteoclast formation by �80% relative to positivecontrols; even 50 ng/ml IL-23 did not abolish osteoclast formation(data not shown). In contrast, IL-23 (20 ng/ml) did not affect os-teoclast formation in RANKL- and M-CSF-stimulated cultures ofbone marrow cells, BMM precursors, or of RAW264.7 cells (Fig.1A). Similar to previous observations with IL-12 and IL-18 (16,17), IL-23 inhibited osteoclast formation in spleen cell cultureswhen present from days 0 to 3, having no effects when addedthereafter (Fig. 1B). In all experiments described below, IL-23 waspresent only during days 0 to 3 of culture. IL-23 did not influencesurvival of mature osteoclasts (data not shown).
To determine whether IL-23 may act via osteoblasts to influenceosteoclast formation, we performed cocultures of primary osteo-blasts (or the preosteoblastic Kusa O cell line) with bone marrowcells stimulated with 10�8 M 1,25(OH)2 D3 and PGE2; osteoclastformation was not affected by IL-23 treatment (data not shown).Real-time RT-PCR analysis (see Table I for oligonucleotideprimer details) of three independent samples of osteoblast and
Kusa O cell mRNA was unable to detect expression of IL-23RmRNA (i.e., Ct � 39) although this was easily detected in spleencell mRNA (Ct � 31.7). This was repeated with a different forwardoligonucleotide primer with a similar result. In contrast, the secondsubunit of the IL-23 receptor, IL-12R�1, was detectable (osteo-blast Ct � 28.8, Kusa O Ct � 28.2, spleen cell Ct � 21.2).
To determine the mechanism of action of IL-23 inhibition ofosteoclast formation in spleen cells, we depleted spleen cell sub-populations. When the nonadherent spleen cell fraction had beenremoved (leaving predominantly adherent macrophages) or T cellswere depleted using Thy1.2-labeled magnetic beads, IL-23 had noeffect on osteoclast formation (Fig. 2A). Removal of B cells fromthe spleen had no effect on IL-23 inhibitory action (data notshown). IL-23 strongly inhibited osteoclast formation in spleencell cultures in CD8� depleted cultures, but had no effect in CD4�
depleted cultures (Fig. 2A). This dependency on CD4� cells wasnot seen in the action of IL-12 in similar cultures (data not shown),as previously reported (17). To confirm the mediation of IL-23effects by CD4� cells, we added T cell subsets into RANKL/M-CSF stimulated cultures of bone marrow cells, a population inwhich IL-23 did not affect osteoclast formation (Fig. 1A). Consis-tent with the action of IL-23 through Th17 cells, when either Tcells or CD4� cells (Fig. 2B) were added to cultures of bone mar-row cells, IL-23 inhibited osteoclast formation. This was not ob-served when CD8� cells were added (Fig. 2B).
A second population of T cells, �� T cells, has also been re-ported to respond to IL-23 (22). We found that when isolatedsplenic �� T cells were added to bone marrow cells IL-23 signif-icantly inhibited osteoclast formation, but this was only observedwhen a minimum of 104 �� T cells/well was added (Fig. 2C).However, osteoclast formation was detected in CD4� strippedspleen cell populations that contained �� T cells when treated withIL-23 (Fig. 2A). By FACS analysis, we determined that in ourC57BL/6 mouse spleen cell populations the mean proportion of ��
A B
FD
C
E0
200
400
600
800
Control IL-23
**
TRA
P+
MN
C/w
ell
******
No Antibody***
Anti-GM-CSF
*** ***Anti-IFNγ
0
50
100
150
200 ControlIL-23IL-12
TRA
P+
MN
C/w
ell
0
2
4
6
8***
*****
IL-23 treatment (Hours)0 Co
1 2 4 8 12 24 24Co
rela
tive
GM
-CS
F
Control
IL-23
0
50
100
150
200
No Antibody Anti-GM-CSF
**
0
1000
2000
3000
Control IL-23
***
0
2
4
6
8
10
12 Spleen cells T cells
Co IL-23
** **
Co IL-23
rela
tive
IL-1
7m
RN
A le
vels
mR
NA
leve
ls
mR
NA
leve
ls
rela
tive
GM
-CS
F
TRA
P+
MN
C/w
ell
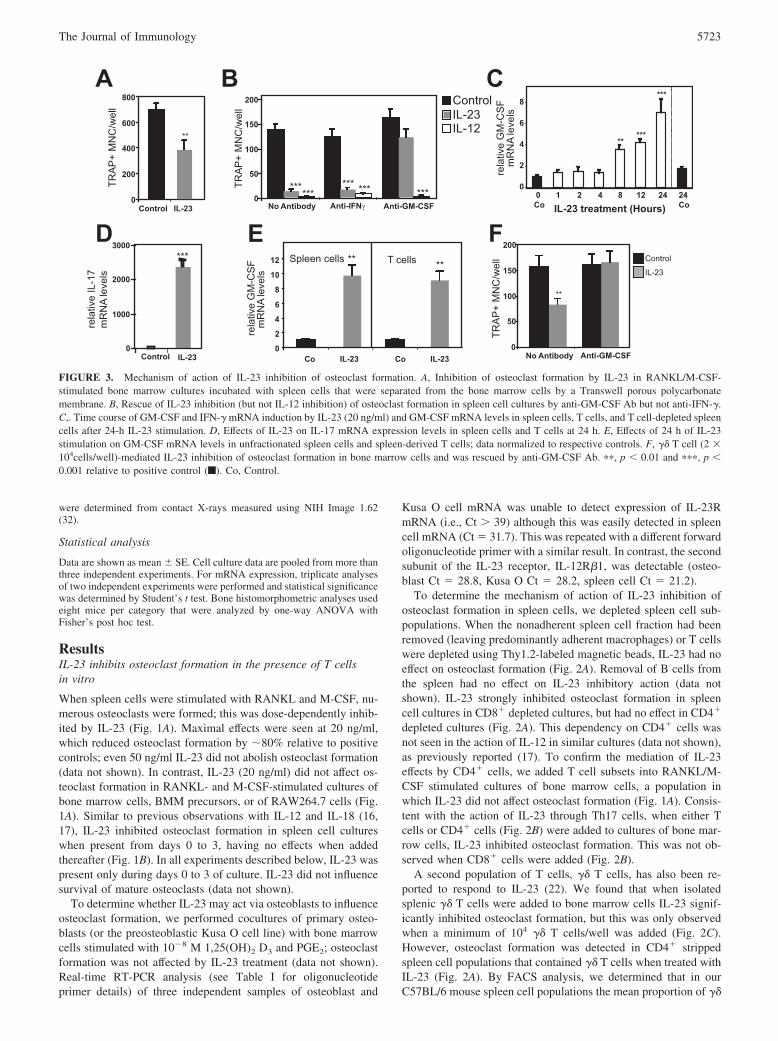
FIGURE 3. Mechanism of action of IL-23 inhibition of osteoclast formation. A, Inhibition of osteoclast formation by IL-23 in RANKL/M-CSF-stimulated bone marrow cultures incubated with spleen cells that were separated from the bone marrow cells by a Transwell porous polycarbonatemembrane. B, Rescue of IL-23 inhibition (but not IL-12 inhibition) of osteoclast formation in spleen cell cultures by anti-GM-CSF Ab but not anti-IFN-�.C,. Time course of GM-CSF and IFN-� mRNA induction by IL-23 (20 ng/ml) and GM-CSF mRNA levels in spleen cells, T cells, and T cell-depleted spleencells after 24-h IL-23 stimulation. D, Effects of IL-23 on IL-17 mRNA expression levels in spleen cells and T cells at 24 h. E, Effects of 24 h of IL-23stimulation on GM-CSF mRNA levels in unfractionated spleen cells and spleen-derived T cells; data normalized to respective controls. F, �� T cell (2 �104cells/well)-mediated IL-23 inhibition of osteoclast formation in bone marrow cells and was rescued by anti-GM-CSF Ab. ��, p � 0.01 and ���, p �0.001 relative to positive control (f). Co, Control.
5723The Journal of Immunology
TCR-positive cells was 1.07% (range, 0.90–1.25%) of live cells.Thus, RANKL/M-CSF-stimulated spleen cell cultures describedabove (which contained 5 � 105 cells in total) contained �5 � 103
cells, insufficient to mediate IL-23 inhibition.
Mechanism of action of T cell-dependent IL-23 inhibition ofosteoclast formation
When spleen cells and bone marrow cells were cultured togetherbut separated by a porous Transwell membrane well, RANKL/M-CSF stimulation caused formation of numerous osteoclasts fromthe bone marrow cells; this was reduced significantly in the pres-ence of IL-23 (20 ng/ml; Fig. 3A). This suggested that IL-23 elicitsthe release of a soluble diffusible osteoclast formation inhibitor.IL-23 is known to induce secretion of TNF, IL-17, GM-CSF, andIFN-� by Th cells (13). TNF and IL-17 are not known to directlyinhibit osteoclast formation and in recombinant form (both 10 ng/ml) neither affected osteoclast formation in RANKL/M-CSF-stim-ulated bone marrow cells (data not shown). IFN-� action wasblocked using an anti-IFN-�-neutralizing Ab as previously de-scribed (17), but no effect on IL-23 inhibition was seen (Fig. 3B).In contrast, a neutralizing Ab to GM-CSF ablated IL-23 action(Fig. 3B). Treatment with both Abs had the same effect as anti-GM-CSF alone (data not shown); as a further control, neither theanti-IFN-�-neutralizing Ab nor the neutralizing Ab to GM-CSFblocked IL-12 action (Fig. 3B).
Since GM-CSF mediated IL-23 action, we investigated GM-CSF mRNA regulation in spleen cells. IL-23 treatment of spleencells increased GM-CSF mRNA levels �5-fold relative to controlat 24 h by IL-23 (Fig. 3C). A somewhat weaker and transient
induction of IFN-� mRNA levels (�2-fold, peaking at 2 h) wasalso noted (data not shown). IL-23 treatment enhanced IL-17mRNA levels very robustly (2500-fold) after 24 h, from a barelydetectable level in untreated cells (Fig. 3D). At 24 h, IL-23 induc-tion of GM-CSF mRNA was also observed in magnetic bead-pu-rified T cells (Fig. 3E), with a response magnitude similar to thatobserved in unfractionated splenic cells.
Because we found that �� T cells mediated an inhibitory effectof IL-23, we examined the role of GM-CSF in this action. As withCD4� cell action above, the inhibitory effect mediated by �� T cellaction was ablated by addition of GM-CSF Ab (Fig. 3F).
IL-12 inhibition of osteoclast formation does not dependon IL-23
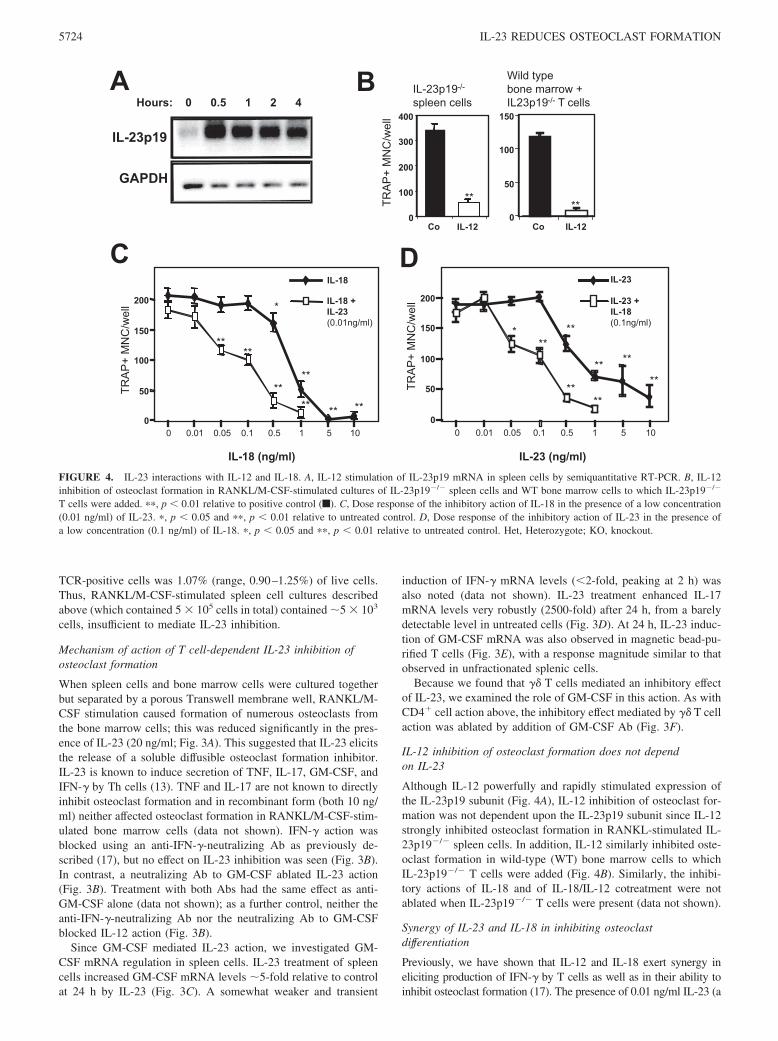
Although IL-12 powerfully and rapidly stimulated expression ofthe IL-23p19 subunit (Fig. 4A), IL-12 inhibition of osteoclast for-mation was not dependent upon the IL-23p19 subunit since IL-12strongly inhibited osteoclast formation in RANKL-stimulated IL-23p19�/� spleen cells. In addition, IL-12 similarly inhibited oste-oclast formation in wild-type (WT) bone marrow cells to whichIL-23p19�/� T cells were added (Fig. 4B). Similarly, the inhibi-tory actions of IL-18 and of IL-18/IL-12 cotreatment were notablated when IL-23p19�/� T cells were present (data not shown).
Synergy of IL-23 and IL-18 in inhibiting osteoclastdifferentiation
Previously, we have shown that IL-12 and IL-18 exert synergy ineliciting production of IFN-� by T cells as well as in their ability toinhibit osteoclast formation (17). The presence of 0.01 ng/ml IL-23 (a
BHours: 0 0.5 1 2 4
IL-23p19
GAPDH
A Wild typebone marrow +IL23p19-/- T cells
0
50
100
150
Co IL-12
**
IL-23p19-/-
spleen cells
0
100
200
300
400
Co IL-12
**
0
50
100
150
200
IL-18
IL-18 + IL-23 (0.01ng/ml)
*
**
** **
****
****
0.01 0.05 0.1 0.5 1 01500
50
100
150
200
D
0.01 0.05 0.1 0.5 1 0150
**
** **
**
***
****
IL-23 (ng/ml)
IL-23
IL-23 +IL-18(0.1ng/ml)
IL-18 (ng/ml)
TRA
P+
MN
C/w
ell
TRA
P+
MN
C/w
ell
TRA
P+
MN
C/w
ell
C
FIGURE 4. IL-23 interactions with IL-12 and IL-18. A, IL-12 stimulation of IL-23p19 mRNA in spleen cells by semiquantitative RT-PCR. B, IL-12inhibition of osteoclast formation in RANKL/M-CSF-stimulated cultures of IL-23p19�/� spleen cells and WT bone marrow cells to which IL-23p19�/�
T cells were added. ��, p � 0.01 relative to positive control (f). C, Dose response of the inhibitory action of IL-18 in the presence of a low concentration(0.01 ng/ml) of IL-23. �, p � 0.05 and ��, p � 0.01 relative to untreated control. D, Dose response of the inhibitory action of IL-23 in the presence ofa low concentration (0.1 ng/ml) of IL-18. �, p � 0.05 and ��, p � 0.01 relative to untreated control. Het, Heterozygote; KO, knockout.
5724 IL-23 REDUCES OSTEOCLAST FORMATION
concentration at least an order of magnitude below that required toshow a measurable effect on osteoclast formation) increased the po-tency of IL-18 in these assays, shifting the dose-response curve ofIL-18 to the left (Fig. 4C). A similar effect on the IL-23 dose-responsecurve was seen in the presence of 0.1 ng/ml IL-18 (Fig. 4D), a con-centration also without effect on osteoclast formation.
Analysis of long bones of WT, IL-23p19�/�, and IL-23p19�/�
mice
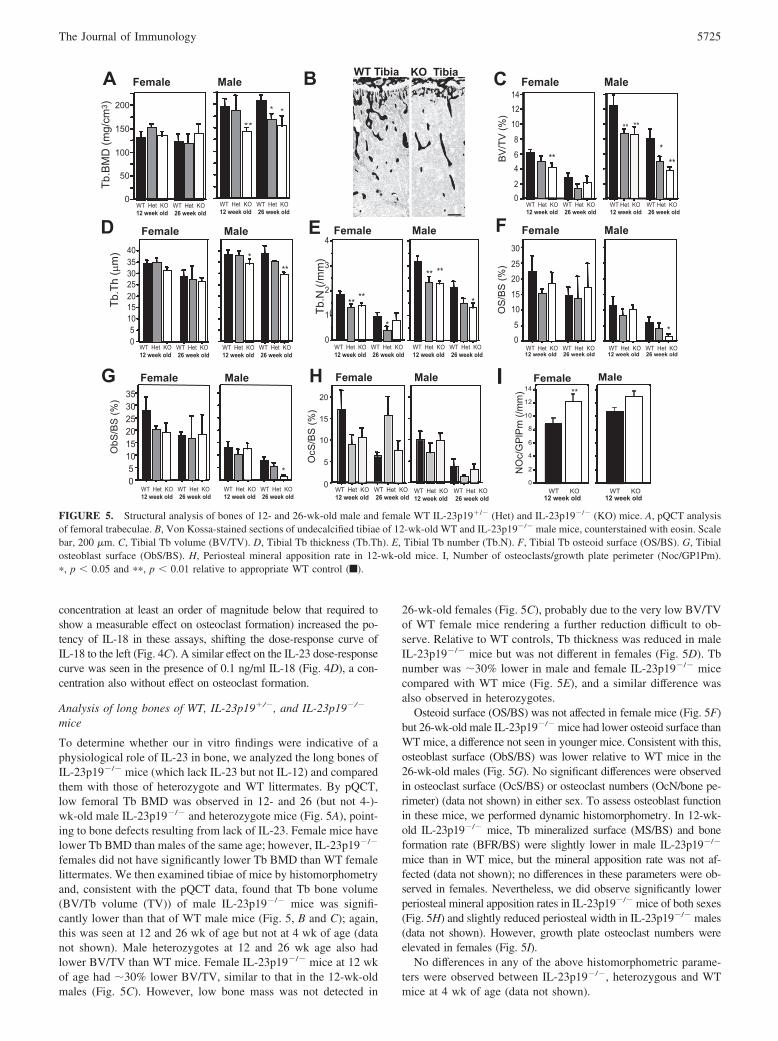
To determine whether our in vitro findings were indicative of aphysiological role of IL-23 in bone, we analyzed the long bones ofIL-23p19�/� mice (which lack IL-23 but not IL-12) and comparedthem with those of heterozygote and WT littermates. By pQCT,low femoral Tb BMD was observed in 12- and 26 (but not 4-)-wk-old male IL-23p19�/� and heterozygote mice (Fig. 5A), point-ing to bone defects resulting from lack of IL-23. Female mice havelower Tb BMD than males of the same age; however, IL-23p19�/�
females did not have significantly lower Tb BMD than WT femalelittermates. We then examined tibiae of mice by histomorphometryand, consistent with the pQCT data, found that Tb bone volume(BV/Tb volume (TV)) of male IL-23p19�/� mice was signifi-cantly lower than that of WT male mice (Fig. 5, B and C); again,this was seen at 12 and 26 wk of age but not at 4 wk of age (datanot shown). Male heterozygotes at 12 and 26 wk age also hadlower BV/TV than WT mice. Female IL-23p19�/� mice at 12 wkof age had �30% lower BV/TV, similar to that in the 12-wk-oldmales (Fig. 5C). However, low bone mass was not detected in
26-wk-old females (Fig. 5C), probably due to the very low BV/TVof WT female mice rendering a further reduction difficult to ob-serve. Relative to WT controls, Tb thickness was reduced in maleIL-23p19�/� mice but was not different in females (Fig. 5D). Tbnumber was �30% lower in male and female IL-23p19�/� micecompared with WT mice (Fig. 5E), and a similar difference wasalso observed in heterozygotes.
Osteoid surface (OS/BS) was not affected in female mice (Fig. 5F)but 26-wk-old male IL-23p19�/� mice had lower osteoid surface thanWT mice, a difference not seen in younger mice. Consistent with this,osteoblast surface (ObS/BS) was lower relative to WT mice in the26-wk-old males (Fig. 5G). No significant differences were observedin osteoclast surface (OcS/BS) or osteoclast numbers (OcN/bone pe-rimeter) (data not shown) in either sex. To assess osteoblast functionin these mice, we performed dynamic histomorphometry. In 12-wk-old IL-23p19�/� mice, Tb mineralized surface (MS/BS) and boneformation rate (BFR/BS) were slightly lower in male IL-23p19�/�
mice than in WT mice, but the mineral apposition rate was not af-fected (data not shown); no differences in these parameters were ob-served in females. Nevertheless, we did observe significantly lowerperiosteal mineral apposition rates in IL-23p19�/� mice of both sexes(Fig. 5H) and slightly reduced periosteal width in IL-23p19�/� males(data not shown). However, growth plate osteoclast numbers wereelevated in females (Fig. 5I).
No differences in any of the above histomorphometric parame-ters were observed between IL-23p19�/�, heterozygous and WTmice at 4 wk of age (data not shown).
A C
F
Female Male
WT Het KO12 week old
WT Het KO 26 week old
WT Het KO12 week old
WT Het KO 26 week old
02
46
8
10
1214
**
****
***
0
5
10
15
20
25
30
*
Female Male
WT Het KO12 week old
WT Het KO 26 week old
WT Het KO12 week old
WT Het KO 26 week old
Female Male
WT Het KO12 week old
WT Het KO 26 week old
50
100
150
200
0
**
* *
WT Het KO12 week old
WT Het KO 26 week old
WT Tibia KO TibiaB
D
05
10152025303540
***
WT Het KO12 week old
WT Het KO 26 week old
WT Het KO12 week old
WT Het KO 26 week old
Female Male
WT Het KO12 week old
WT Het KO 26 week old
WT Het KO12 week old
WT Het KO 26 week old
05
101520253035
*
Female MaleG
E
WT Het KO12 week old
WT Het KO 26 week old
WT Het KO12 week old
WT Het KO 26 week old
(
0
1
2
3
4
****
*** **
Female Male
*
H Female Male
WT Het KO12 week old
WT Het KO 26 week old
WT Het KO12 week old
WT Het KO 26 week old
0
5
10
15
20
OcS
/BS
(%)
Female MaleI
0
2
4
6
8
10
12
14
WT KO 12 week old
WT KO 12 week old
NO
c/G
PlP
m (/
mm
)
Tb.B
MD
(mg/
cm3 )
Tb.T
h (µ
m)
Tb.N
(/m
m)
BV
/TV
(%)
OS
/BS
(%)
ObS
/BS
(%)
**
FIGURE 5. Structural analysis of bones of 12- and 26-wk-old male and female WT IL-23p19�/� (Het) and IL-23p19�/� (KO) mice. A, pQCT analysisof femoral trabeculae. B, Von Kossa-stained sections of undecalcified tibiae of 12-wk-old WT and IL-23p19�/� male mice, counterstained with eosin. Scalebar, 200 �m. C, Tibial Tb volume (BV/TV). D, Tibial Tb thickness (Tb.Th). E, Tibial Tb number (Tb.N). F, Tibial Tb osteoid surface (OS/BS). G, Tibialosteoblast surface (ObS/BS). H, Periosteal mineral apposition rate in 12-wk-old mice. I, Number of osteoclasts/growth plate perimeter (Noc/GP1Pm).�, p � 0.05 and ��, p � 0.01 relative to appropriate WT control (f).
5725The Journal of Immunology

Analysis of bone length, growth plate, and cartilage remnants
Slightly shorter (Fig. 6A) and narrower (data not shown) femorawere noted in 26-wk-old IL-23p19�/� male mice compared withWT, but this difference was not detected earlier. The difference inlength was small (8.6%) but significant and suggested that IL-23p19�/� mice could have an abnormality in bone growth at orafter 12 wk of age. Indeed, we found that at 12 wk of age (but not4 wk), the IL-23p19�/� and heterozygote tibial growth plate wassignificantly narrower in both sexes than in WT controls (Fig. 6, Band C), with a greater extent of growth plate closure (data notshown). The narrower growth plates were characterized by asmaller hypertrophic zone but not proliferating zone (Fig. 6C),suggesting that chondrocyte proliferation was not affected byIL-23 deletion. The smaller hypertrophic zone may be explainedby increased resorption of the hypertrophic cartilage as it miner-alizes. Consistent with this, the length of the primary spongiosawas strikingly truncated in IL-23p19�/� males (Fig. 6D) suggest-ing that this layer of primitive, woven bone is removed more rap-idly than in WT. This also suggests a local increase in bone re-sorption. Osteoclasts are abundant in this region in both WT andIL-23p19�/� mice, but differences in osteoclast numbers provedimpossible to interpret due to grossly different surface areas ofprimary spongiosa and growth plate between the two genotypes.Female IL-23p19�/� and heterozygote mice also had truncatedgrowth plate hypertrophic zones, but did not display significantlyshorter primary spongiosa. Nevertheless, female IL-23p19�/� andheterozygotes had reduced cartilage remnants within TB bone(Fig. 6E), consistent with increased bone resorption; this was notobserved in males, suggesting that their elevated bone resorptionwas confined to the growth plate region.
Ex vivo cultures of cells from WT and IL-23p19�/� mice
Both bone marrow cells and spleen cells from 10-wk-old maleIL-23p19�/� mice formed a greater number of osteoclasts whenstimulated with RANKL and M-CSF in vitro compared with age-matched male WT mice (Fig. 6F). We found no difference betweencalvarial osteoblasts derived from WT and IL-23p19�/� mice intheir ability to mineralize in vitro (data not shown).
IL-23 treatment does not affect osteoblasts directly or indirectlyvia lymphocytes
Consistent with the lack of IL-23R mRNA expression (see above),IL-23 did not affect the ability of WT or IL-23p19�/� osteoblastsor Kusa O cells to mineralize matrix in vitro or induce osteocalcinexpression in ascorbate-treated cultures (data not shown). IL-23also had no effect on osteocalcin mRNA expression in ascorbate-treated Kusa O osteoblastic cells grown in the presence or absenceof T cells (or unfractionated spleen cells) in direct coculture orseparated by Transwell membrane (data not shown).
DiscussionIL-23 is emerging as a cytokine of critical importance in chronicinflammation. Elevated incidence of ankylosing spondylitis, in-flammatory bowel disease, psoriasis, and myocardial infarctionalso associate with variants of the gene encoding IL-23R (34–37).Bone destruction notably occurs at or near sites affected by chronicinflammation, and IL-23 may influence this by participating inprocesses that maintain inflammation. However, examining boneloss secondary to inflammation does not shed light on the role ofIL-23 in normal bone homeostasis. To clarify this, we investigated
AWT
KOHet
11
12
13
14
15
16
4 12 26
17
0
Males
*
4 12 260
Females
Weeks of ageWeeks of age
B
C E F******
******HypertrophicZone Width
ProliferatingZone Width
0
20
40
60
80
WT Het KO
FemaleWT Het KO
Male
100
Bone marrow cells Spleen cells
***
0
100
200
300
400
WT IL-23p19-/-
***
WT IL-23p19-/-
ProlHypPrim
1
2
3
4
0
***
0
40
80
120
160
******
WT Het KO
FemaleWT Het KO
MaleWT Het KO
FemaleWT Het KO
Male
DWT KO
Prol
Hyp
Prim
b
b
mm
c
c
FIGURE 6. IL-23p19�/� male mice develop shorter limb bones than WT: analysis of femoral length, growth plate, primary spongiosa, and cartilageremnants. A, Femoral length and width. �, p � 0.05 relative to WT control. B, Growth plate region of tibia showing reduced hypertrophic zones inIL-23p19�/� mice at 12 wk. Prol, Chondrocyte proliferation zone; Hyp, hypotrophic zone; Prim, primary spongiosa; b, mature Tb bone; m, bone marrow.C, Relative widths of proliferating zone (f) and hypertrophic zone (�) of growth plates of 12-wk-old mice. �, p � 0.05 and ��, p � 0.01 relative tohypertrophic zone of WT control. D, Length of primary spongiosa. E, Cartilage remnants in Tb bone (proportion of area). F, Ex vivo cultures of hemopoieticcells from WT and IL-23p19�/� mice: osteoclast formation in RANKL/M-CSF- stimulated cultures of spleen and bone marrow cells. �, p � 0.05 and��, p � 0.01 relative to appropriate WT control. Het, Heterozygote IL-23p19�/�; KO, knockout IL-23p19�/�.
5726 IL-23 REDUCES OSTEOCLAST FORMATION

actions of rIL-23 on osteoclasts in vitro and the bone phenotype ofIL-23p19�/� mice which lacks functional IL-23.
IL-23p19�/� mice displayed a progressively developing os-teopenia, evident at 12 wk of age. The progressive nature of thisosteopenia may explain a report of normal bone mass in 10-wk-oldIL-23p19 null mice (12). Tb BMD and bone volume were reducedin male IL-23p19�/� mice, the latter due mainly to low Tb num-ber, although Tb thickness was reduced in older males. Surpris-ingly, bone mass was also reduced in heterozygotes, suggestingthat low IL-23 levels (assuming it occurs in heterozygotes) signif-icantly affect bone, and is consistent with data on IL-23R variants.In contrast to males, female IL-23p19�/� mice had low Tb bonemass at 12 wk but had otherwise a less pronounced bone pheno-type. As commonly observed, female WT mice had less bone massthan males, which possibly makes further reduced bone massharder to observe. Indeed, this is likely in 26-wk-old females withtheir extremely low bone mass; Tb BMD was also normal in fe-male IL-23p19�/� mice. As well as lower bone mass, female micehave a higher bone remodeling rate than males (and consequentlya shorter primary spongiosa) as well as different patterns of boneapposition and longitudinal bone growth. Such differences be-tween the sexes may result in differing patterns of response tocytokine ablation that influence bone turnover rate, even where sexhormone responsiveness is not targeted.
The bone abnormalities in IL-23p19�/� mice could not be ex-plained by high osteoclast or decreased osteoblast numbers, al-though osteoblast numbers and osteoid were mildly reduced in26-wk-old males. We were alerted to another explanation by find-
ing that IL-23p19�/� femora are slightly shorter than those of WT,suggesting bone growth defects. Indeed, IL-23p19�/� mice ofboth sexes had abnormally narrow growth plates, but this was re-stricted to the hypertrophic zone, indicating that the shortenedbone length was not a result of impaired chondrocyte proliferation.Bone growth occurs due to growth plate expansion; as well asexpansion due to chondrocyte proliferation, mineralized cartilageat the hypertrophic zone is resorbed by osteoclasts and replaced bylow-density primary spongiosa (Fig. 7A). This woven bone is alsoresorbed, forming a template for denser (lamellar) Tb bone for-mation (secondary spongiosa) that we routinely examine by pQCTand histomorphometry. Unresorbed cartilage remnants are detect-able in Tb bone and excessive persistence of such remnants occurswhen bone resorption is impaired (33).
The thin growth plate hypertrophic zones in IL-23p19�/� tibiacould be due to abnormal chondrocyte differentiation or excessiveosteoclast action. The latter was strongly suggested by the trun-cated primary spongiosa in male IL-23p19�/� mice. This featureis rarely reported but is apparent in 13-wk-old male osteoprote-gerin null (OPG�/�) and OPG�/� mice (38). The primary spon-giosa region is abundant in osteoclasts, but due to its complexmorphology and gross differences in bone surfaces (BS) (on whichosteoclasts form) between genotypes, it was impossible to deter-mine whether osteoclast numbers were elevated in IL-23p19�/�
mice. Nevertheless, since Tb bone is built on primary spongiosawhich in turn is built on calcified cartilage, it is likely that a re-duction in primary spongiosa results in less Tb bone (summarizedin Fig. 7A) and/or reduced initiation of new trabeculae. In females,
OB
WildType
IL-23p19-/-
Resorption of CalcifiedCartilage
PrimarySpongiosaFormation
PrimarySpongiosaResorption
Secondary Spongiosa(Trabecula)Formation
OB
OCOC OC
OBOB
Hyp
A
IL-23
Th17 cellexpansionT cells
IL-23
GM-CSF
IL-17
Osteoblasts
RANKL
Antigen presentation
RANKL
IL-17
Osteoblasts
RANKL
B
OB OBOBOB
OCOCOCOC
Hyp
FIGURE 7. A, Tb formation by bone model-ing and remodeling below the growth plate, leftto right. In the hypertrophic zone (Hyp) of thegrowth plate, calcified cartilage (light gray) isresorbed by osteoclasts (OC). Resulting smallprocesses form scaffolds for woven bone forma-tion (primary spongiosa, darker gray) by osteo-blasts (OB). This is later remodeled by oste-oclasts and osteoblasts to form mature Tb(darkest gray). Remnants of the original carti-lage are left embedded in trabeculae. In IL-23p19�/� mice, the width of the calcified carti-lage layer (both sexes) and primary spongiosa(in males) is reduced. This suggests greater os-teoclast activity in these regions resulting in for-mation of smaller Tb structures. B, Model ofIL-23 indirect actions on bone cells. IL-23 hasactions upon T cells, resulting in expansion ofTh17 subsets. Upon Ag presentation, Th17 cellsexpress RANKL as well as IL-17, which elicitsosteoblast-derived RANKL. Both sources ofRANKL would stimulate osteoclast differentia-tion. In contrast, IL-23 acts upon Th17 cells (and�� T cells), which results in increased GM-CSFproduction, reducing osteoclast differentiation.
5727The Journal of Immunology

the primary spongiosa was not shorter but cartilage remnants werereduced, which also points to elevated osteolysis and may alsosuggest that increased resorption is less localized than in males. Itshould also be noted that the primary spongiosa is shorter in WTfemales than in matched males due to higher bone remodelingrates in females and the elevation in osteolysis due to IL-23 abla-tion may not have as pronounced effects on female primary spon-giosa width. Collectively, these observations indicate that IL-23particularly influences resorption near the growth plate and that inother models displaying osteopenia (particularly involving lym-phocyte-mediated cytokines) defects at this location should beexamined.
In spleen cell cultures, we characterized antiosteoclastogenicand potentially antiosteolytic actions of IL-23 that resemble thoseof IL-12 and IL-18 (16, 17). A number of cell types respond toIL-23, including subpopulations of macrophages, CD4� andCD8� T cells (39), and �� T cells. BMM cultures (devoid of Tcells) and T cell depletion and addition experiments demonstratedthat CD4� T cells mediated these inhibitory actions of IL-23. Thissuggests that the mediating cells are Th17 cells, which are char-acterized by IL-23-elicited secretion of IL-17 and IL-6 (13). How-ever, CD4� �� T cells also secrete IL-17 in response to IL-23 (22).�� T cells are a poorly understood T cell subpopulation partici-pating in innate immune functions and compose only a small frac-tion of T cells in spleen (22). Addition of 104 or more �� T cellsto bone marrow cell cultures resulted in sensitivity to IL-23 inhi-bition. �� T cells were present in our splenic cell cultures, includ-ing CD4� cell-depleted splenic cultures; these were insensitive toIL-23 due to insufficient �� T cells (5 � 103 per culture) to mediatesignificant inhibition. �� T cells can accumulate in pathologicalconditions and exert both positive and negative effects on jointinflammation progression. Our data point to an unsuspected influ-ence of these cells on bone.
We determined that IL-23 effects on osteoclast formation viaCD4�/�� T cells were dependent on GM-CSF production; IL-23induction of GM-CSF protein in IL-2-treated CD4� cells has beennoted by Aggarwal et al. (25). No mediation by IFN-� Abs wasnoted, although IFN-� is better characterized as a target of IL-23action (13). The effect of IL-23 resembles that of IL-18 (16), whichalso exerts actions on osteoclasts via T cell-derived GM-CSF; con-sistent with this, we found synergy between IL-23 and IL-18.Thus, IL-23 effects may be strongly influenced by other local cy-tokines. In addition, production of IL-23 by dendritic cells (13)(which form in the presence of GM-CSF) and GM-CSF-stimulatedmacrophages (40) suggest that IL-23 and GM-CSF may cause lo-cal positive feedback enhancement of each other’s production.
The T cell populations we used were not activated and in theabsence of IL-23 did not affect osteoclasts. However, we previ-ously found that T cell activation results in RANKL productionand osteoclast formation (9), and in an important extension tothose observations Sato et al. (12) showed anti-CD3/anti-CD28-activated Th17 cells are the RANKL-producing T cell subset. Thisimplies that IL-23 treatment of activated T cells has a net osteo-lytic effect. GM-CSF powerfully inhibits osteoclast formation, butonly in progenitors exposed to both GM-CSF with RANKL (16).When GM-CSF treatment is withdrawn before RANKL exposure,no inhibition occurs (41); indeed, osteoclast progenitors expand(42). IL-23 elicits T cell IL-17 and IL-6 production, both stimu-lators of osteoblast RANKL expression (43). IL-23 stimulus thusresults in exposure to both RANKL and GM-CSF, the latter po-tentially blocking action of the former (Fig. 7B). In contrast, ininflammatory lesions with high levels of T cell activation, IL-23expansion of Th17 cells may result in levels of T cell-derivedRANKL high enough to overcome GM-CSF effects.
We found no evidence that IL-23 influenced osteoblasts in vitroand could not detect their expression of IL-23R mRNA. IL-23 mayindirectly affect osteoblasts, which is suggested by low periostealmineral apposition in IL-23p19�/� mice; notably, these cells areof a different origin than the osteoblasts on Tb bone. It is unclearhow this effect on periosteal osteoblasts may occur, although IL-23acts on cell types that may influence stromal cells (21, 24, 44).
In contrast, IL-23-elicited GM-CSF powerfully affects the oste-oclast lineage; however, as no GM-CSF null bone phenotype hasbeen reported and GM-CSF-transgenic mice have a complex in-flammatory syndrome (45) (rendering its influence on bone hard tointerpret), the contribution of GM-CSF to the IL-23p19�/� phe-notype mice is difficult to assess. Indeed, although our in vitroobservations suggest that IL-23-elicited GM-CSF is a plausiblemechanism to explain the lower bone mass in IL-23p19�/� mice,IL-23 ablation may also result in a lack of Th17 cells (and perhapsother subpopulations yet to be defined) that may reduce bone massdue to lack of some other osteoclast inhibitory influence. IL-23may also elicit other T cell-derived osteoclast inhibitors in vivothat it does not under our in vitro culture conditions.
Thus, with these considerations in mind and since the localiza-tion of IL-23 responsive or IL-23-dependent T cells in long bonesare unknown, we cannot fully explain the localization of the IL-23p19�/� bone defect. However, the abundance of osteoclasts atthe growth plate may render this site particularly sensitive to in-hibitors such as GM-CSF. Alternatively, differences in osteoclastprogenitors found at different sites or in proximity of Th17 cellsmay account for our observations, but further work is needed toclarify this.
In summary, we have identified that lack of IL-23 has significantnegative consequences for bone mass and found powerful T cell-mediated effects of IL-23 on osteoclast formation. This providesnew evidence regarding lymphocyte influence on physiologicalbone homeostasis and suggests this influence differs from that ex-erted when activated lymphocytes are present under inflammatorycircumstances.
AcknowledgmentsWe thank Nico Ghilardi of Genentech Inc. (South San Francisco, CA) forsupplying us with IL-23p19�/� mice. We thank Dr. David Izon (St. Vin-cent’s Institute, Fitzroy, Australia) for advice with flow cytometry.
DisclosuresThe authors have no financial conflict of interest.
References1. Gillespie, M. T. 2007. Impact of cytokines and T lymphocytes upon osteoclast
differentiation and function. Arthritis Res. Ther. 9: 103–106.2. Walsh, M. C., N. Kim, Y. Kadono, J. Rho, S. Y. Lee, J. Lorenzo, and Y. Choi.
2006. Osteoimmunology: interplay between the immune system and bone me-tabolism. Annu. Rev. Immunol. 24: 33–63.
3. Yoshida, H., S. Hayashi, T. Kunisada, M. Ogawa, S. Nishikawa, H. Okamura,T. Sudo, and L. D. Shultz. 1990. The murine mutation osteopetrosis is in thecoding region of the macrophage colony stimulating factor gene. Nature 345:442–444.
4. Yasuda, H., N. Shima, N. Nakagawa, K. Yamaguchi, M. Kinosaki, S. Mochizuki,A. Tomoyasu, K. Yano, M. Goto, A. Murakami, et al. 1998. Osteoclast differ-entiation factor is a ligand for osteoprotegerin/osteoclastogenesis-inhibitory fac-tor and is identical to TRANCE/RANKL. Proc. Natl. Acad. Sci. USA 95:3597–3602.
5. Kong, Y. Y., H. Yoshida, I. Sarosi, H. L. Tan, E. Timms, C. Capparelli,S. Morony, A. J. Oliveira-dos-Santos, G. Van, A. Itie, et al. 1999. OPGL is a keyregulator of osteoclastogenesis, lymphocyte development and lymph-node orga-nogenesis. Nature 397: 315–323.
6. Wong, B. R., R. Josien, S. Y. Lee, B. Sauter, H. L. Li, R. M. Steinman, andY. Choi. 1997. TRANCE (tumor necrosis factor [TNF]-related activation-in-duced cytokine), a new TNF family member predominantly expressed in T cells,is a dendritic cell-specific survival factor. J. Exp. Med. 186: 2075–2080.
7. Maruyama, K., Y. Takada, N. Ray, Y. Kishimoto, J. M. Penninger, H. Yasuda,and K. Matsuo. 2006. Receptor activator of NF-�B ligand and osteoprotegerin
5728 IL-23 REDUCES OSTEOCLAST FORMATION

regulate proinflammatory cytokine production in mice. J. Immunol. 177:3799–3805.
8. Martin, T. J. 2004. Paracrine regulation of osteoclast formation and activity:milestones in discovery. J. Musculoskelet. Neuronal Interact. 4: 243–253.
9. Horwood, N. J., V. Kartsogiannis, J. M. Quinn, E. Romas, T. J. Martin, andM. T. Gillespie. 1999. Activated T lymphocytes support osteoclast formation invitro. Biochem. Biophys. Res. Commun. 265: 144–150.
10. Kong, Y. Y., W. J. Boyle, and J. M. Penninger. 1999. Osteoprotegerin ligand: acommon link between osteoclastogenesis, lymph node formation and lymphocytedevelopment. Immunol. Cell Biol. 77: 188–193.
11. Kawai, T., T. Matsuyama, Y. Hosokawa, S. Makihira, M. Seki, N. Y. Karimbux,R. B. Goncalves, P. Valverde, S. Dibart, Y. P. Li, et al. 2006. B and T lympho-cytes are the primary sources of RANKL in the bone resorptive lesion of peri-odontal disease. Am. J. Pathol. 169: 987–998.
12. Sato, K., A. Suematsu, K. Okamoto, A. Yamaguchi, Y. Morishita, Y. Kadono,S. Tanaka, T. Kodama, S. Akira, Y. Iwakura, et al. 2006. Th17 functions as anosteoclastogenic helper T cell subset that links T cell activation and bone de-struction. J. Exp. Med. 203: 2673–2682.
13. Iwakura, Y., and H. Ishigame. 2006. The IL-23/IL-17 axis in inflammation.J. Clin. Invest. 116: 1218–1222.
14. Cua, D. J., J. Sherlock, Y. Chen, C. A. Murphy, B. Joyce, B. Seymour, L. Lucian,W. To, S. Kwan, T. Churakova, et al. 2003. Interleukin-23 rather than interleu-kin-12 is the critical cytokine for autoimmune inflammation of the brain. Nature421: 744–748.
15. Mirosavljevic, D., J. M. Quinn, J. Elliott, N. J. Horwood, T. J. Martin, andM. T. Gillespie. 2003. T-cells mediate an inhibitory effect of interleukin-4 onosteoclastogenesis. J. Bone Miner. Res. 18: 984–993.
16. Horwood, N. J., N. Udagawa, J. Elliott, D. Grail, H. Okamura, M. Kurimoto,A. R. Dunn, T. Martin, and M. T. Gillespie. 1998. Interleukin 18 inhibits oste-oclast formation via T cell production of granulocyte macrophage colony-stim-ulating factor. J. Clin. Invest. 101: 595–603.
17. Horwood, N. J., J. Elliott, T. J. Martin, and M. T. Gillespie. 2001. IL-12 alone andin synergy with IL-18 inhibits osteoclast formation in vitro. J. Immunol. 166:4915–4921.
18. Epstein, S. 1998. Immunosuppressant drugs and bone disease: a clinician’s per-spective. J. Clin. Densitom. 1: 317–321.
19. Watford, W. T., M. Moriguchi, A. Morinobu, and J. J. O’Shea. 2003. The biologyof IL-12: coordinating innate and adaptive immune responses. Cytokine GrowthFactor Rev. 14: 361–368.
20. Chang, J. T., B. M. Segal, K. Nakanishi, H. Okamura, and E. M. Shevach. 2000.The costimulatory effect of IL-18 on the induction of antigen-specific IFN-�production by resting T cells is IL-12 dependent and is mediated by up-regulationof the IL-12 receptor �2 subunit. Eur. J. Immunol. 30: 1113–1119.
21. Parham, C., M. Chirica, J. Timans, E. Vaisberg, M. Travis, J. Cheung, S. Pflanz,R. Zhang, K. P. Singh, F. Vega, et al. 2002. A receptor for the heterodimericcytokine IL-23 is composed of IL-12R�1 and a novel cytokine receptor subunit,IL-23R. J. Immunol. 168: 5699–5708.
22. Lockhart, E., A. M. Green, and J. L. Flynn. 2006. IL-17 production is dominatedby �� T cells rather than CD4 T cells during Mycobacterium tuberculosis infec-tion. J. Immunol. 177: 4662–4669.
23. Ghilardi, N., N. Kljavin, Q. Chen, S. Lucas, A. L. Gurney, and F. J. De Sauvage.2004. Compromised humoral and delayed-type hypersensitivity responses in IL-23-deficient mice. J. Immunol. 172: 2827–2833.
24. Happel, K. I., P. J. Dubin, M. Zheng, N. Ghilardi, C. Lockhart, L. J. Quinton,A. R. Odden, J. E. Shellito, G. J. Bagby, S. Nelson, and J. K. Kolls. 2005.Divergent roles of IL-23 and IL-12 in host defense against Klebsiella pneu-moniae. J. Exp. Med. 202: 761–769.
25. Aggarwal, S., N. Ghilardi, M. H. Xie, F. J. de Sauvage, and A. L. Gurney. 2003.Interleukin-23 promotes a distinct CD4 T cell activation state characterized by theproduction of interleukin-17. J. Biol. Chem. 278: 1910–1914.
26. Quinn, J. M., G. A. Whitty, R. J. Byrne, M. T. Gillespie, and J. A. Hamilton.2002. The generation of highly enriched osteoclast-lineage cell populations. Bone30: 164–170.
27. Allan, E. H., P. W. Ho, A. Umezawa, J. Hata, F. Makishima, M. T. Gillespie, andT. J. Martin. 2003. Differentiation potential of a mouse bone marrow stromal cellline. J. Cell. Biochem. 90: 158–169.
28. Stanford, C. M., P. A. Jacobson, E. D. Eanes, L. A. Lembke, and R. J. Midura.1995. Rapidly forming apatitic mineral in an osteoblastic cell line (UMR 106-01BSP). J. Biol. Chem. 270: 9420–9428.
29. Hausler, K. D., N. J. Horwood, Y. Chuman, J. L. Fisher, J. Ellis, T. J. Martin,J. S. Rubin, and M. T. Gillespie. 2004. Secreted frizzled-related protein-1 inhibitsRANKL-dependent osteoclast formation. J. Bone Miner. Res. 19: 1873–1881.
30. Wang, X., and B. Seed. 2003. A PCR primer bank for quantitative gene expres-sion analysis. Nucleic Acids Res. 31: 1–8.
31. Sims, N. A., K. Brennan, J. Spaliviero, D. J. Handelsman, and M. J. Seibel. 2006.Perinatal testosterone surge is required for normal adult bone size but not fornormal bone remodeling. Am. J. Physiol. 290: E456–E462.
32. Sims, N. A., P. Clement-Lacroix, F. Da Ponte, Y. Bouali, N. Binart, R. Moriggl,V. Goffin, K. Coschigano, M. Gaillard-Kelly, J. Kopchick, et al. 2000. Bonehomeostasis in growth hormone receptor-null mice is restored by IGF-I but in-dependent of Stat5. J. Clin. Invest. 106: 1095–1103.
33. Sims, N. A., B. J. Jenkins, A. Nakamura, J. M. Quinn, R. Li, M. T. Gillespie,M. Ernst, L. Robb, and T. J. Martin. 2005. Interleukin-11 receptor signaling isrequired for normal bone remodeling. J. Bone Miner Res. 20: 1093–1102.
34. Oliver, J., B. Rueda, M. A. Lopez-Nevot, M. Gomez-Garcia, and J. Martin. 2007.Replication of an association between IL23R gene polymorphism with inflam-matory bowel disease. Clin. Gastroenterol. Hepatol. 5: 977–981.
35. Mangino, M., P. Braund, R. Singh, R. Steeds, S. Stevens, K. S. Channer, andN. J. Samani. 2007. Association analysis of IL-12B and IL-23R polymorphismsin myocardial infarction. J. Mol. Med. 86: 99–103.
36. Cargill, M., S. J. Schrodi, M. Chang, V. E. Garcia, R. Brandon, K. P. Callis,N. Matsunami, K. G. Ardlie, D. Civello, J. J. Catanese, et al. 2007. A large-scalegenetic association study confirms IL12B and leads to the identification of IL23Ras psoriasis-risk genes. Am. J. Hum. Genet. 80: 273–290.
37. Brown, M. A. 2008. Breakthroughs in genetic studies of ankylosing spondylitis.Rheumatology 47: 132–137.
38. Mizuno, A., N. Amizuka, K. Irie, A. Murakami, N. Fujise, T. Kanno, Y. Sato,N. Nakagawa, H. Yasuda, S. Mochizuki, et al. 1998. Severe osteoporosis in micelacking osteoclastogenesis inhibitory factor/osteoprotegerin. Biochem. Biophys.Res. Commun. 247: 610–615.
39. He, D., L. Wu, H. K. Kim, H. Li, C. A. Elmets, and H. Xu. 2006. CD8� IL-17-producing T cells are important in effector functions for the elicitation of contacthypersensitivity responses. J. Immunol. 177: 6852–6858.
40. Fleetwood, A. J., T. Lawrence, J. A. Hamilton, and A. D. Cook. 2007. Granu-locyte-macrophage colony-stimulating factor (CSF) and macrophage CSF-depen-dent macrophage phenotypes display differences in cytokine profiles and tran-scription factor activities: implications for CSF blockade in inflammation.J. Immunol. 178: 5245–5252.
41. Takahashi, N., N. Udagawa, T. Akatsu, H. Tanaka, M. Shionome, and T. Suda.1991. Role of colony-stimulating factors in osteoclast development. J. BoneMiner. Res. 6: 977–985.
42. Hodge, J. M., M. A. Kirkland, C. J. Aitken, C. M. Waugh, D. E. Myers,C. M. Lopez, B. E. Adams, and G. C. Nicholson. 2004. Osteoclastic potential ofhuman CFU-GM: biphasic effect of GM-CSF. J. Bone Miner. Res. 19: 190–199.
43. Kotake, S., N. Udagawa, N. Takahashi, K. Matsuzaki, K. Itoh, S. Ishiyama,S. Saito, K. Inoue, N. Kamatani, M. T. Gillespie, et al. 1999. IL-17 in synovialfluids from patients with rheumatoid arthritis is a potent stimulator of osteoclas-togenesis. J. Clin. Invest. 103: 1345–1352.
44. Stark, M. A., Y. Huo, T. L. Burcin, M. A. Morris, T. S. Olson, and K. Ley. 2005.Phagocytosis of apoptotic neutrophils regulates granulopoiesis via IL-23 and IL-17. Immunity 22: 285–294.
45. Lang, R. A., D. Metcalf, R. A. Cuthbertson, I. Lyons, E. Stanley, A. Kelso,G. Kannourakis, D. J. Williamson, G. K. Klintworth, T. J. Gonda, et al. 1987.Transgenic mice expressing a hemopoietic growth factor gene (GM-CSF) de-velop accumulations of macrophages, blindness, and a fatal syndrome of tissuedamage. Cell 51: 675–686.
5729The Journal of Immunology
Copyright © 2022 FDOKUMEN