Hydroxyurea and growth in young children with sickle cell disease
10
DOI: 10.1542/peds.2014-0917 ; originally published online August 25, 2014; Pediatrics and Bruce Thompson Waclawiw Goldsmith, James F. Casella, Caroline K. Reed, Zora R. Rogers, Myron A. Sohail Rana, Patricia E. Houston, Winfred C. Wang, Rathi V. Iyer, Jonathan Hydroxyurea and Growth in Young Children With Sickle Cell Disease http://pediatrics.aappublications.org/content/early/2014/08/19/peds.2014-0917 located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly by Lorelle Bradley on September 11, 2014 pediatrics.aappublications.org Downloaded from by Lorelle Bradley on September 11, 2014 pediatrics.aappublications.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Hydroxyurea and growth in young children with sickle cell disease

DOI: 10.1542/peds.2014-0917; originally published online August 25, 2014;Pediatrics
and Bruce ThompsonWaclawiwGoldsmith, James F. Casella, Caroline K. Reed, Zora R. Rogers, Myron A.
Sohail Rana, Patricia E. Houston, Winfred C. Wang, Rathi V. Iyer, JonathanHydroxyurea and Growth in Young Children With Sickle Cell Disease
http://pediatrics.aappublications.org/content/early/2014/08/19/peds.2014-0917
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

Hydroxyurea and Growth in Young Children WithSickle Cell Disease
WHAT’S KNOWN ON THIS SUBJECT: Growth impairment in sickledisease has been a consistent finding in published reports.Hydroxyurea (HU) decreases vasoocclusive events and increaseshemoglobin levels, which may improve growth. However, HU mayadversely affect growth in young children by its effect on DNAsynthesis.
WHAT THIS STUDY ADDS: Height, weight, and head circumferencewere normal in HU-treated children in the study as comparedwith the World Health Organization standards. Height, weight, andBMI z scores were similar in placebo and treatment groups. Therewere no harmful effects of HU on growth.
abstractBACKGROUND: Growth impairment is a known complication of sicklecell disease. Effects of hydroxyurea (HU) on growth in very young chil-dren are not known.
METHODS: Height, weight, BMI, and head circumference (HC) werecompared with World Health Organization (WHO) standards in BABYHUG, a multicenter, randomized, double-blinded, placebo-controlled2-year clinical trial of HU in 193 children 9 to 18 months of age. An-thropometric data were closely monitored and converted to z scoresby using WHO standardized algorithms for descriptive analyses. Thetreatment and placebo groups were compared longitudinally by usinga mixed model analysis.
RESULTS: At entry, the z scores of BABY HUG children were higher thanWHO norms. After 2 years of HU or placebo treatment, there were nosignificant differences between the groups, except for the mean HCz scores at study exit (HU: +0.8 versus placebo: +1.0, P = .05). Baselinez scores were the best predictors of z scores at study exit. Theabsolute neutrophil count, absolute reticulocyte count, and total whiteblood cell count had significant negative correlations with growthmeasures.
CONCLUSIONS: Both groups had normal or near normal anthropomet-ric measures during the study. The HC z scores at study entry and exitwere slightly greater than WHO norms. Higher baseline white bloodcell count, absolute reticulocyte count, and absolute neutrophil countwere associated with poorer growth. The significance of the slightlylower HC in the treatment group at study exit is not clear. Trendstoward normalization of weight and height and effects on HC willbe monitored in ongoing BABY HUG follow-up studies. Pediatrics2014;134:465–472
AUTHORS: Sohail Rana, MD,a Patricia E. Houston, MS,a
Winfred C. Wang, MD,b Rathi V. Iyer, MD,c JonathanGoldsmith, MD,d James F. Casella, MD,e Caroline K. Reed,MSN, FNP-BC,a Zora R. Rogers, MD,f Myron A. Waclawiw,PhD,d and Bruce Thompson, PhD,g for the BABY HUGInvestigatorsaDepartment of Pediatrics and Child Health, Howard University,Washington, District of Columbia; bSt. Jude Children’s ResearchHospital, Memphis, Tennessee; cUniversity of Mississippi MedicalCenter, Jackson, Mississippi; dNational Heart, Lung, and BloodInstitute, Bethesda, Maryland; eDivision of Hematology,Department of Pediatrics, Johns Hopkins University, Baltimore,Maryland; fUT Southwestern Medical Center, Dallas, Texas; andgClinical Trials & Surveys Corporation, Owings Mills, Maryland
KEY WORDSsickle cell disease, growth, hydroxyurea, children, height, weight,head circumference, BMI
ABBREVIATIONSANC—absolute neutrophil countARC—absolute reticulocyte countCSSCD—Cooperative Study of Sickle Cell DiseaseHb—hemoglobinHC—head circumferenceHU—hydroxyureaSCD—sickle cell diseaseWBC—white blood cellWHO—World Health Organization
(Continued on last page)
PEDIATRICS Volume 134, Number 3, September 2014 465
ARTICLE
by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

Growth involvescomplex interactionsofnutrients, hormones, and genetic fac-tors. Numerous genetic and epigeneticfactors interact with influences frominternal and external environments toregulate growth and account for a ma-jor portion of variation in growthwithinpopulations. The effects of sickle celldisease (SCD) on weight and height inchildrenwerefirstdescribedmore thanhalf a century ago.1,2 Previous studieshave revealed a consistent pattern ofdiminished growth among individualswith SCD from all regions of the world,with evidence linking growth failure toendocrine dysfunction, metabolic de-rangement, and nutrient deficiencies.3
The Cooperative Study of Sickle CellDisease (CSSCD) data on growth andsexual maturation of more than 2000children and young adults with varioussickle genotypes revealed that individ-uals with HbSS and HbSb0 thalassemiawere smaller compared with those withHbSC and HbSb+ thalassemia. All 4genotypes were below norms for Afri-can Americans.4 Growth differenceswere evident even in the youngest groupof children (2–4 years old). Numerousother studies have confirmed theseobservations.1,2,5–16 Al-Saqladi et al3
reviewed 46 studies of anthropometricparameters, body composition, energymetabolism, micronutrient deficiency,and endocrine dysfunction in individu-als with SCD. There was a consistentpattern of growth failure among af-fected individuals from all geographicareas. In a recent prospective longitu-dinal study of 148 childrenwith SCDwhowere evaluated for 4 years, height,weight, or BMI declined in 84% of sub-jects; 38% fell below the fifth percentileon Centers for Disease Control andPrevention growth curves in 1 or moremeasures.17
In the Stroke Prevention Clinical Trial forSickle Cell Anemia, individuals receivingchronic transfusion therapy for 2 yearshad improved growth velocities thatwere
close to normal for age compared withstandardized US growth charts from theNational Center for Health Statistics.18
Hydroxyurea (HU) decreases the fre-quency of acute vasoocclusive events andimproves hematologic parameters inSCD; however, it is not clear if it alsoimproves growth. A phase I-II safety studyof HU (HUG KIDS) compared 68 childrenages 5 to 16 years at baseline withhistorical controls from the CSSCD andrevealed improvement in weight, butno significant improvement in heightpercentiles.19 In a comparison betweenhealthy controls and 41 childrenwith SCDwho had received HU for at least 2 years,there was significant improvement inaerobic exercise tolerance, but the meanvalues for weight, height, and lean bodymass were all lower in the children withSCD.20 Most studies have either usedcontrols from the local population orNHANES data. Only 1 recent study usedWorld Health Organization (WHO) growthdata as a comparison group.9
BABY HUG was a clinical trial of treat-ment with HU in young children withSCD. Careful serial growth measure-ments were included as a safety out-come because of concerns regardingpotential adverse effects of HU ongrowth in very young children. Theseconcerns stemmed from unpublishedbut widely disseminated animal datasuggesting that HU may have a delete-rious effect on the growth and de-velopment of the brain.
METHODS
In 2003, the BABY HUG study, a double-blind, multicenter, placebo-controlledclinical trial of HU, was initiated, and193eligible infants9 to18monthsof agewith HbSS or HbSb0 thalassemia (en-rolled from 2003 to 2007) were ran-domly assigned to 24 months oftreatment with HU or placebo. Theprimary end points of the study werepreservation of spleen and renal func-tion. Evaluation of growth parameters
was among the secondary end points.The methodology, challenges of de-signing this trial, and main results ofthe study have been reported in de-tail.21,22 This article summarizes theanalyses of the anthropometric datacollected from the children enrolled inBABY HUG.
All measurements were obtained induplicate by trained study coordinatorsusing standardized techniques. Mea-surements were obtained at screening,treatment initiation, 2weeks, 4weeks, 6weeks, and 8 weeks, and then every 4weeks thereafter. If predefined tox-icities occurred, study visits wereconducted every 2 weeks.
Weight, without clothing, was measuredin study participants up to 12 months ofage by using a pan-type balance scale,with a beam balance or electronic re-cording. Subjects older than 12 monthswho could stand were weighed on a lev-eledplatformscale,without clothingor inlight clothing. Two measurements weremade, with a third being obtained if thefirst 2 differed by more than 100 g.
Recumbent length was obtained inchildren up to 18 months of age, withstanding height measured after 18months. Recumbent length was mea-sured by using a measuring board witha fixed headboard and moveable foot-board, with centimeter markings. Twomeasurementsweremade, with a thirdbeing obtained, if the first 2 differed bymore than 0.5 cm.
A plastic measuring tape that was notsubject to stretching was used in thestudy to measure head circumference(HC). Two measurements were made,with a third being obtained if the first 2differed by more than 0.4 cm. Everyeffort was made to circumvent theproblems associated with braiding orother hair styles.
WechoseWHOnormativedata, basedonrecommendations by the Centers forDisease Control and Prevention and the
466 RANA et al by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

American Academy of Pediatrics forchildren younger than 2 years of age.23
The WHO data are intended to reflectoptimal growth and are based ona high quality study from selectedethnically diverse communities world-wide. Growth charts such as thosebased on NHANES are actually refer-ences and not standards, and describehow certain children grew in a partic-ular place and time, whereas WHOnormative data are intended to provideuniversal standards.
Z scores for height, weight, BMI, and HCwere calculated by using SAS (SAS In-stitute, Inc, Cary, NC) macros down-loaded from the WHO Web site.24 EachZ score calculation was controlled forgender and age (in days) when makingthe calculation from the WHO standardpopulation. BABY HUG growth datawere averaged within each 3-monthinterval after treatment assignment(eg, 0–3 months, 3–6 months, etc), withthe baseline measurement being usedas the time 0 measurement.
Baseline z scores were compared withthe WHO norms by testing whether themean z score was equal to zero, versusthe alternative that it was not equal tozero, using student’s t test. All longitu-dinal data were analyzed by using ProcMIXED, with an autoregressive co-variance structure used to account forthe covariance between each serialmeasurement. Covariables includedin each analysis were the baselinemeasurements of the following: theoutcome being reviewed, time inmonths since enrollment, hemoglobin(Hb) level, absolute reticulocyte count(ARC), total white blood cell (WBC)count, and absolute neutrophil count(ANC). Backward elimination (using0.05 as the significance level) for theHb, ARC, WBC count, and ANC covari-ables was used to arrive at the finalmodel for each outcome measure.
Simple Pearson correlations betweeneach outcome measure (at each time
point) and the corresponding baselinemeasurement of Hb, ARC, WBC count,andANCweremadebyusingProcCORR.All analyses used SAS version 9.2.
RESULTS
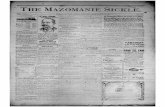
All 193 randomized children were in-cluded in the analysis. See Table 1 fordemographic information. Unadjustedmean Z scores and SEs for height atbaseline and for each 3-month intervalare presented by randomized study as-signment in Fig 1. There was no signifi-cant difference in growth trajectoriesbetween the 2 treatment groups (P = .7).The baseline height z scoreswere slightly,but significantly greater than the WHOnorm andwere positively correlated withall subsequently measured height zscores. The baseline ANC in both groupswas negatively correlated with heightover the course of the study (P = .004).
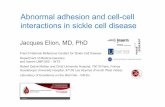
Baseline weight z scores in both treat-ment groups were also higher than theWHO norms and were positively corre-
lated with all subsequent measure-ments. Unadjusted mean z scores andSEs for weight at baseline and for each3-month interval are presented by studygroup in Fig 2. There were no significantdifferences in the HU and placebo tra-jectories over time (P = .43). HigherWBCcount and ARC were negatively corre-lated with weight z scores.
The mean baseline BMI z score washigher in the HU treatment groupcompared with the placebo group, andboth measurements were greater thanthe WHO norm (HU: +0.220 and placebo:+0.086). Unadjusted mean z scores andSEs for BMI at baseline and for each3-month interval are presented bystudy group in Fig 3. In both groups, thebaseline BMI was positively and theWBC count and ARC were negativelycorrelated to the BMI z scores duringand at the end of treatment. A generalquadratic trend (with a single concav-ity as compared with linear) was ap-parent for the BMI z scores. Once
FIGURE 1Longitudinal comparison of WHO standardized height z scores between children treated with HU andplacebo. Z scores for height, weight, BMI, and HC were calculated by using SAS macros downloadedfrom the WHO Web site and controlled for gender and age. Data were averaged within each 3-monthinterval after treatment assignments with the baseline measurement used as the time 0. Student’st test was used for comparison with the WHO normal population. Proc MIXED was used to analyzelongitudinal data. BABY HUG children were larger than the WHO population on all parameters at thebeginning of the study, and there was no difference between the treatment groups except for the BMIthat was larger at each observation point in the HU group (trend not significant). There were nosignificant differences between the treatment groups for height, weight, and BMI at exit. The HC in thetreatment group was slightly smaller but still within normal limit at the end of the study. Baselinez scores were the best predictors of z scores for all growth parameters.
ARTICLE
PEDIATRICS Volume 134, Number 3, September 2014 467 by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

adjusted for the difference in thebaseline measurements, there was nostatistically significant difference inthe 2 trajectories (P = .7).
Unadjusted mean z scores and SEs forHC at baseline and for each 3-monthinterval are presented by study groupin Fig 4. The mean HC z scores werehigher than the WHO standards in bothgroups at baseline (HU: 1.031 and pla-cebo: 0.989). The baseline HC z scorewas the most significant predictor ofHC during and at the end of treatment.The trajectory of HC z scores was lowerin the HU treatment group comparedwith placebo (HU: 0.852 versus placebo:0.968, P = .05) after adjusting for thebaseline difference in HC z scores be-tween the HU and placebo groups. TheANC was negatively correlated with HCz scores during and after treatment.
On average, children enrolled in BABYHUG were larger than the WHO refer-ence population with respect to height,
weight, BMI, and HC at the beginning ofthe study. HU treatment was associatedwith a slightly lower HC over the timecourse of treatment. The analysis ofvariance for each of the above analysesis presented in Supplemental Tables 5–8 for this article. During the trial, eachchild was evaluated to determine if heor she ever crossed downward over 2major percentiles of the WHO growthcurves (defined as the 95, 75, 50, 25, 10,5, and 1.5th percentiles) or crossedbelow the 1.5th percentile. In all, one-quarter to one-fifth of the childrenwere observed to have one of theseevents (height: 27%; weight: 19%; andHC: 21%), with most occurrences at-tributable to crossing 2 major percen-tiles of the growth curves. There wasno statistically significant differencebetween HU and placebo-treated chil-dren in the number of times a majorpercentile was crossed.
In addition, “normal” growth curves forheight, weight, BMI, andHC of 1- to 3-year-
old children with HbSS were generatedby using data from the BABY HUG pla-cebo group and are presented in theSupplemental Materials.25 These growthcurves may be useful as historical con-trols for future comparisons of thera-peutic interventions.
DISCUSSION
Growth impairment is a known compli-cation of SCD. The CSSCD growth curvesfor individuals with sickle hemoglobin-opathiesweresignificantlydifferent fromthe published norms for African Ameri-cans, and HbSS and HbSb0 thalassemiaindividuals were smaller than those withHbSC and HbSb+ thalassemia. Sincepublication of the CSSCD data, severalother studies have revealed that childrenand adolescents with SCD had signifi-cantly lower height, weight, and BMI com-pared with reference growth curves.9–16
In general the adverse influence of SCDhas been more pronounced for weightthan height. Endocrine dysfunction, poornutrient intake, micronutrient deficien-cies, hypermetabolism, and high proteinturnover have been described in individ-uals with SCD and growth failure.26–31
Growth hormone deficiency may ac-count for a small percentage of chil-dren with SCD who have severe growthdelay.32 Hemolysis, chronic anemia,and a high metabolic rate appear to bethe most significant adverse factorsfor growth in SCD. Resting energy ex-penditure was increased in severalstudies of children with SCD and isprobably related to anemia, chronicinflammation, high cardiac output, andhigh protein turnover.33–35 Interventionsthat decrease anemia and inflammationmay have a beneficial effect on growthas well. HU has modest effects onthe severity of hemolysis and anemiaand may also decrease inflammation.Therefore, it is reasonable to hypothe-size that HU could have a positive in-fluence on growth.36
FIGURE 2Longitudinal comparison of WHO standardized weight z scores between children treated with HU andplacebo. Z scores for height, weight, BMI, and HC were calculated by using SAS macros downloadedfrom the WHO Web site and controlled for gender and age. Data were averaged within each 3-monthinterval after treatment assignments with the baseline measurement used as the time 0. Student’st test was used for comparison with the WHO normal population. Proc MIXED was used to analyzelongitudinal data. BABY HUG children were larger than the WHO population on all parameters at thebeginning of the study, and there was no difference between the treatment groups except for the BMIthat was larger at each observation point in the HU group (trend not significant). There were nosignificant differences between the treatment groups for height, weight, and BMI at exit. The HC in thetreatment group was slightly smaller but still within normal limit at the end of the study. Baselinez scores were the best predictors of z scores for all growth parameters.
468 RANA et al by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

Although spleen and kidney functionwere theprimary endpoints of theBABYHUG trial, assessments of growth wereimportant secondary end points anda safety measure due to concerns thatHU might have an adverse effect ongrowth.22 At study entry, BABY HUGchildren were generally similar butslightly larger than the WHO standardpopulation for height, weight, and BMI,while having significantly larger HC.During the study, therewas a downwardpercentile trend for weight in bothtreatment and placebo groups; none-theless, the mean z scores remainedclose to the WHO norms, suggesting thatthere was no significant impairment ofoverall growth in either group by studyend. In addition, there were no signifi-cant differences for height, weight, andBMI based on study treatment.
The HC was significantly larger inchildren enrolled in BABY HUG andremained so throughout the study pe-riod. Measurement of HC in AfricanAmerican children is challenging, be-cause of hair styles that may includebraids, dreadlocks, beads, etc. It ispossible that the overall larger HCthroughout the studymayhave resultedfrom these hair styles, although ex-aminers were specifically trained tominimize the effect of hair style on HC.Oro-facial and cranio-skeletal abnor-malities that may contribute to HC havebeen described in individuals with SCDand are frequently the result ofmarrowhyperplasia.37–39 Even though the dif-ference was small, the HC percentilewas lower in the HU treatment groupby the end of the study, possibly asa result of suppression of bone mar-row hyperplasia. Nonetheless, the HCremained well above the WHO 50thpercentile standard. Further evalua-tion of children in the ongoing BABYHUG follow-up studies will be neces-sary to determine if this effect persistsand assess its significance.
FIGURE 3Longitudinal comparison of WHO standardized BMI z scores between children treated with HU andplacebo. Z scores for height, weight, BMI, and HC were calculated by using SAS macros downloadedfrom the WHO Web site and controlled for gender and age. Data were averaged within each 3-monthinterval after treatment assignments with the baseline measurement used as the time 0. Student’st test was used for comparison with the WHO normal population. Proc MIXED was used to analyzelongitudinal data. BABY HUG children were larger than the WHO population on all parameters at thebeginning of the study, and there was no difference between the treatment groups except for the BMIthat was larger at each observation point in the HU group (trend not significant). There were nosignificant differences between the treatment groups for height, weight, and BMI at exit. The HC in thetreatment group was slightly smaller but still within normal limit at the end of the study. Baselinez scores were the best predictors of z scores for all growth parameters.
FIGURE 4Longitudinal comparison of WHO standardized HC z scores between children treated with HU andplacebo. Z scores for height, weight, BMI, and HC were calculated by using SAS macros downloadedfrom the WHO Web site and controlled for gender and age. Data were averaged within each 3-monthinterval after treatment assignments with the baseline measurement used as the time 0. Student’st test was used for comparison with the WHO normal population. Proc MIXED was used to analyzelongitudinal data. BABY HUG children were larger than the WHO population on all parameters at thebeginning of the study, and there was no difference between the treatment groups except for the BMIthat was larger at each observation point in the HU group (trend not significant). There were nosignificant differences between the treatment groups for height, weight, and BMI at exit. The HC in thetreatment group was slightly smaller but still within normal limit at the end of the study. Baselinez scores were the best predictors of z scores for all growth parameters.
ARTICLE
PEDIATRICS Volume 134, Number 3, September 2014 469 by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

These data provide evidence that ininfants and toddlers enrolled in BABYHUG, HU did not adversely affect theweight or linear growth of infants. Theirgrowth parameters were normal andcomparable to the WHO standards. Al-though our preliminary analysis dem-onstrated higher weight z scores in thetreatment group compared with theplacebo group, this difference lostsignificance after accounting for dif-ferences in weight at baseline.
In the BABY HUG trial, HU treatment wasassociated with a decreased rate ofclinical events and improved hemato-logic profile.21 Clinical events and dis-ease severity have been considered animportant reason for poor growth inchildren with SCD; however, in thisstudy, the decrease in clinical eventswith HU treatment did not producea significant difference in growthparameters between the 2 treatmentarms.17 The association of high ANC andWBC counts with lower height andweight in this study potentially supportsan important role of inflammation asboth increased WBC count and ANC areassociated with inflammation anda higher rate of complications in per-sons with SCD. Alternatively, theseparameters may simply be markers ofmore severe disease.40
This study has several limitations. Astandard dose of HU of 20 mg/kg wasused throughout the BABY HUG study.This dose was chosen because of itsdemonstrated safety in this age group inpreliminary studies and because a rel-atively low fixed dose was expected toreduce the likelihood of toxicity.41 Manypediatric hematologists in the UnitedStates treat children with SCD withhigher doses of HU, up to 35 mg/kg. Ahigher dose is more likely to increaseHbF, decrease chronic hemolysis, andpossibly reduce inflammation as well;therefore, it is possible that a higherdose of HU may have greater impact ongrowth parameters. Also, the better
height andweight z scores of children atbaseline and on placebo, as well as onHUwhen comparedwithWHO standardsare puzzling. BABY HUG children wereseen frequently, and there was intensemonitoring of growth parameters at thecentral study coordinating site, becauseof concerns regarding safety. Theserepeated measurements could haveraised awareness of parents and care-takers regarding the potential of earlygrowth failure and thus produced anincreased focus on nutrition. Perhapsthis dampened any growth differencesbetween those in the 2 arms of the trial.We are not aware of any studies thathave looked at the effects of frequentclinic visits and close central monitor-ing of growth parameters in individualswith chronic illness; however, frequentvisits have been shown to have favor-able effects on other health outcomes,such as improved HbA1c levels in indi-viduals with type 2 diabetes and hy-pertension.42–44 More frequent studyvisits (required for dosage titration insome subjects) were associated withbetter adherence to medications inBABY HUG.45
CONCLUSIONS
We saw no clinically significant differ-ences in height, weight, or BMI betweenthe HU and placebo treated groupsdemonstrating the lack of harmfuleffectsongrowthdue toHUtreatmentof2 years starting at a young age. It isimportant to note that the height,weight, BMI, and HC were all eithernormal or close to normal in bothtreatment groups compared with theWHO standards, possibly impeding anydemonstration of additional benefitfrom HU. There were no significantdifferences between treatment groupsfor any of the growth measures, exceptfor HC. Increased WBC count, ARC, andANC that have been associated withmore severe disease in other studieswere associated with significantly de-
creased growth in our subjects. Thestudy was limited by an observationperiod of only 2 years. However, follow-up of these children is continuing, and itremains to be seen if normal growthpatterns will persist in these ongoingstudies,whicharecharacterizedby lessfrequent visits, but generally highermilligram per kilogram doses of HU.
ACKNOWLEDGMENTSWe thank the following BABY HUG per-sonnel at the participating clinical cen-ters and the Medical CoordinatingCenter: Children’s National Medical Cen-ter: Catherine Driscoll, MD, CaterinaMinniti, MD, Brenda Martin, MSN, CPNP,Barbara Speller-Brown, MSN, andRomuladus Azuine, MPH; Duke Univer-sityMedical Center: Courtney Thornburg,MD, Sherri Zimmerman, MD, RussellWare, MD, William Schultz, MHS, PA-C,and Tracy Kelly, MSN, CPNP; HowardUniversity College of Medicine: ErinYeagley, FNP, and Connie Nguyen, RPh;Johns Hopkins University School ofMedicine: Catherine Freer, PNP, PhillipSeaman, PA-C, Jeffrey Keefer, MD, PhD,Sue Dixon, and Patrice Sharp; MedicalUniversity of South Carolina: RamKalpatthi, MD, Sherron Jackson, MD,Betsy Rackoff, RN, Lisa Kuisel, andDeborah Disco, RNP; St. Jude Children’sResearch Hospital: Lane Faughnan,BSN, and Lynn Wynn, MSN, PNP; SUNYDownstate Medical Center/Kings CountyHospital Center: Scott Miller, MD, KathyRey, PA-C, Sreedhar P. Rao, MD, andSandraGraham,PA-C; University ofMiami:Stuart Toledano, MD, Julie Barredo, MD,Tally Hustace, ARNP, Noeline Lewis,ARNP, and Ofelia Alvarez, MD; Universityof Mississippi Medical Center: GlendaThomas, RN; University of Texas South-westernMedical Center at Dallas: CindyCochran, MSN, CPNP, Leah Adix, CCRP,Nicole Corrigan, MD, Jennifer Marshall,RN, and Claudette Vicks, RN; Universityof Alabama at Birmingham: ThomasHoward, MD, Jennifer McDuffie, CRNP,
470 RANA et al by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

KimberlyWhelan,MD, and RoyMcDonald,MPH; Drexel University: Carlton Dampier,MD, Lori Luck,MD,Mary LouMacDermott,CRNP, Maureen Meier, RN, and MicheleCahill; Emory University School of Medi-cine: R. Clark Brown, MD, PhD, IfeyinwaOsunkwo, MD, MPH, Ellen Debenham, RN,
Leann Hassen, MPH, and Terrell Faircloth;Children’s Hospital of Michigan: SharadaSarniak, MD, Wanda Whitten-Shurney,MD, Mary Murphy, MSN, CNP, MadhviPajpurkar, MD, and Kristin Storie-Kennedy,RN; and Clinical Trials & Surveys Corp:ZhibaoMi, PhD, Zhaoyu Luo, PhD, Xiangke
Huang, MS, Billie Fish, CCRP, and AnneMartien, MBA, CCRP, CRCP.
We acknowledge the efforts of the BABYHUG subjects and their families and thecontributions of all who participated inBABYHUG(http://www.c-tasc.com/cms/StudySites/babyhug.htm).
REFERENCES
1. Jimenez CT, Scott RB, Henry HL, SampsonCC, Ferguson AD. Studies in sickle cellanemia. XXVI. The effects of homozygoussickle cell disease on the onset of menarche,pregnancy, fertility, pubescent changes, andbody growth in Negro subjects. Am J DisChild. 1966;111:497–504
2. Scott RB, Ferguson AD, Jenkins ME, ClarkHM. Studies in sickle-cell anemia. VIII. Fur-ther observations on the clinical manifes-tations of sickle-cell anemia in children.AMA Am J Dis Child. 1955;90(6):682–691
3. Al-Saqladi AW, Cipolotti R, Fijnvandraat K,Brabin BJ. Growth and nutritional status ofchildren with homozygous sickle cell dis-ease. Ann Trop Paediatr. 2008;28(3):165–189
4. Platt OS, Rosenstock W, Espeland MA. In-fluence of sickle hemoglobinopathies ongrowth and development. N Engl J Med.1984;311(1):7–12
5. Whitten CF. Growth status of children withsickle-cell anemia. Am J Dis Child. 1961;102:355–364
6. McCormack MK, Dicker L, Katz SH, et al.Growth patterns of children with sickle-celldisease. Hum Biol. 1976;48(3):429–437
7. Lowry MF, Desai P, Ashcroft MT, Serjeant BF,Serjeant GR. Heights and weights ofJamaican children with homozygous sicklecell disease. Hum Biol. 1977;49(3):429–436
8. Luban NLC, Leikin SL, August GA. Growthand development in sickle cell anemia.Preliminary report. Am J Pediatr HematolOncol. 1982;4(1):61–65
9. Al-Saqladi AW, Bin-Gadeen HA, Brabin BJ.Growth in children and adolescents withsickle cell disease in Yemen. Ann TropPaediatr. 2010;30(4):287–298
10. Mukherjee MB, Gangnkhedkar RR. Physicalgrowth of children with sickle cell disease.Indian J Hum Genet. 2004;10:70–72
11. Osei-Yeboah C, Rodrigues O, Enweronu-Laryea C. Nutritional status of children withsickle cell disease at Korle Bu TeachingHospital, Accra, Ghana. West Afr J Med.2011;30(4):262–267
12. Thomas PW, Singhal A, Hemmings-Kelly M,Serjeant GR. Height and weight reference
curves for homozygous sickle cell disease.Arch Dis Child. 2000;82(3):204–208
13. Silva CM, Viana MB. Growth deficits inchildren with sickle cell disease. Arch MedRes. 2002;33(3):308–312
14. Singhal A, Thomas P, Cook R, Wierenga K,Serjeant G. Delayed adolescent growth inhomozygous sickle cell disease. Arch DisChild. 1994;71(5):404–408
15. Rhodes M, Akohoue SA, Shankar SM, et al.Growth patterns in children with sickle cellanemia during puberty. Pediatr Blood Can-cer. 2009;53(4):635–641
16. Isah HO, Oche MO, Ibrahim KO, Gande-Isa S.Anthropomorphic profiles of homozygoussickle cell children in north-westernNigeria: findings from Usmanu DanfoiyoUniversity Teaching Hospital, Sokoto, Nigeria.Sahel Med Journal. 2008;11(2):45–48
17. Zemel BS, Kawchak DA, Ohene-Frempong K,Schall JI, Stallings VA. Effects of delayedpubertal development, nutritional status,and disease severity on longitudinal pat-terns of growth failure in children withsickle cell disease. Pediatr Res. 2007;61(5pt 1):607–613
18. Wang WC, Morales KH, Scher CD, et al; STOPInvestigators. Effect of long-term trans-fusion on growth in children with sicklecell anemia: results of the STOP trial. JPediatr. 2005;147(2):244–247
19. Wang WC, Helms RW, Lynn HS, et al. Effect ofhydroxyurea on growth in children withsickle cell anemia: results of the HUG-KIDSStudy. J Pediatr. 2002;140(2):225–229
20. Wali YA, Moheeb H. Effect of hydroxyurea onphysical fitness indices in children withsickle cell anemia. Pediatr Hematol Oncol.2011;28(1):43–50
21. Wang WC, Ware RE, Miller ST, et al; BABYHUG investigators. Hydroxycarbamide invery young children with sickle-cell anae-mia: a multicentre, randomised, controlledtrial (BABY HUG). Lancet. 2011;377(9778):1663–1672
22. Thompson BW, Miller ST, Rogers ZR, et al.The pediatric hydroxyurea phase III clinicaltrial (BABY HUG): challenges of study de-
sign. Pediatr Blood Cancer. 2010;54(2):250–255
23. Grummer-Strawn LM, Reinold C, Krebs NF;Centers for Disease Control and Prevention(CDC). Use of World Health Organizationand CDC growth charts for children aged 0-59 months in the United States. MMWRRecomm Rep. 2010;59(RR-9):1–15
24. World Health Organization. SAS macros. Avail-able at: www.who.int/childgrowth/softward/en/. Accessed July 7, 2014
25. Cole TJ, Green PJ. Smoothing referencecentile curves: the LMS method and pe-nalized likelihood. Stat Med. 1992;11(10):1305–1319
26. Luporini SM, Bendit I, Manhani R, BraccoOL, Manzella L, Giannella-Neto D. Growthhormone and insulin-like growth factor Iaxis and growth of children with differentsickle cell anemia haplotypes. J PediatrHematol Oncol. 2001;23(6):357–363
27. Kawchak DA, Schall JI, Zemel BS, Ohene-Frempong K, Stallings VA. Adequacy of di-etary intake declines with age in childrenwith sickle cell disease. J Am Diet Assoc.2007;107(5):843–848
28. Barden EM, Kawchak DA, Ohene-FrempongK, Stallings VA, Zemel BS. Body compositionin children with sickle cell disease. Am JClin Nutr. 2002;76(1):218–225
29. Dekker LH, Fijnvandraat K, Brabin BJ, vanHensbroek MB. Micronutrients and sicklecell disease, effects on growth, infection andvaso-occlusive crisis: a systematic review.Pediatr Blood Cancer. 2012;59(2):211–215
30. Prasad AS. Discovery of human zinc de-ficiency: 50 years later. J Trace Elem MedBiol. 2012;26(2–3):66–69
31. Cox SE, Makani J, Fulford AJ, et al. Nutritionalstatus, hospitalization and mortality amongpatients with sickle cell anemia in Tanzania.Haematologica. 2011;96(7):948–953
32. Nunlee-Bland G, Rana SR, Houston-Yu PE,Odonkor W. Growth hormone deficiency inpatients with sickle cell disease andgrowth failure. J Pediatr Endocrinol Metab.2004;17(4):601–606
ARTICLE
PEDIATRICS Volume 134, Number 3, September 2014 471 by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

33. Borel MJ, Buchowski MS, Turner EA, PeelerBB, Goldstein RE, Flakoll PJ. Alterations inbasal nutrient metabolism increase restingenergy expenditure in sickle cell disease.Am J Physiol. 1998;274(2 pt 1):E357–E364
34. Akohoue SA, Shankar S, Milne GL, et al. Energyexpenditure, inflammation, and oxidativestress in steady-state adolescents with sicklecell anemia. Pediatr Res. 2007;61(2):233–238
35. Hibbert JM, Creary MS, Gee BE, BuchananID, Quarshie A, Hsu LL. Erythropoiesis andmyocardial energy requirements contrib-ute to the hypermetabolism of childhoodsickle cell anemia. J Pediatr GastroenterolNutr. 2006;43(5):680–687
36. Fung EB, Barden EM, Kawchak DA, Zemel BS,Ohene-Frempong K, Stallings VA. Effect ofhydroxyurea therapy on resting energy ex-penditure in children with sickle cell disease.J Pediatr Hematol Oncol. 2001;23(9):604–608
37. Ganguly A, Boswell W, Aniq H. Musculo-skeletal manifestations of sickle cell anae-mia: a pictorial review. Anemia. 2011;2011:794283
38. Javed F, Correa FO, Nooh N, Almas K,Romanos GE, Al-Hezaimi K. Orofacial mani-festations in patients with sickle cell dis-ease. Am J Med Sci. 2013;345(3):234–237
39. Martinoli C, Bacigalupo L, Forni GL, BaloccoM, Garlaschi G, Tagliafico A. Musculoskele-tal manifestations of chronic anemias.Semin Musculoskelet Radiol. 2011;15(3):269–280
40. Miller ST, Sleeper LA, Pegelow CH, et al.Prediction of adverse outcomes in childrenwith sickle cell disease. N Engl J Med. 2000;342(2):83–89
41. Wang WC, Wynn LW, Rogers ZR, Scott JP,Lane PA, Ware RE. A two-year pilot trial ofhydroxyurea in very young children with
sickle-cell anemia. J Pediatr. 2001;139(6):790–796
42. Morrison F, Shubina M, Turchin A. Encoun-ter frequency and serum glucose level,blood pressure, and cholesterol level con-trol in patients with diabetes mellitus. ArchIntern Med. 2011;171(17):1542–1550
43. Turchin A, Goldberg SI, Shubina M, EinbinderJS, Conlin PR. Encounter frequency andblood pressure in hypertensive patientswith diabetes mellitus. Hypertension. 2010;56(1):68–74
44. Guthmann R, Davis N, Brown M, Elizondo J.Visit frequency and hypertension. J ClinHypertens (Greenwich). 2005;7(6):327–332
45. Thornburg CD, Rogers ZR, Jeng MR, et al;BABY HUG Investigators. Adherence to studymedication and visits: data from the BABYHUG trial. Pediatr Blood Cancer. 2010;54(2):260–264
(Continued from first page)
Dr Rana contributed to the design of the BABY HUG study, acquisition of data, analysis and interpretation of data, drafting and revising the manuscript, and approvaland accountability for the work; Ms Houston contributed to the study design, data acquisition, regulatory matters, drafting and revising the manuscript, andaccountability for the work; Dr Wang and Dr Iyer contributed to the design of the BABY HUG study, acquisition of data, analysis and interpretation of data, revisingthe manuscript, final approval, and accountability for the work; Dr Goldsmith contributed to data analysis and interpretation of data, numerous critical revisions/critiques of the article, final approval, and agreed to be accountable for all aspects of the work including resolution of queries; Dr Casella contributed to the designof the BABY HUG study, acquisition of data, analysis and interpretation of data, revising the manuscript, final approval, and accountability for the work; Ms Reedcontributed to the conduct of the study, acquisition of data, interpretation of data, revising the manuscript, final approval, and accountability for the work; DrRogers contributed to the conception and design, acquisition and interpretation of data, drafting and revision of the manuscript, final approval, and accountabilityfor the work; Dr Waclawiw contributed to designing the study, data analysis and interpretation of the results, assistance with substantial review and revision of themanuscript, final approval, and accountability for the work; and Dr Thompson made substantial contributions to the statistical design of the study and themanuscript, and he was responsible for the longitudinal analyses and for several drafts of this manuscript.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-0917
doi:10.1542/peds.2014-0917
Accepted for publication Jun 19, 2014
Address correspondence to Sohail Rana, MD, Department of Pediatrics and Child Health, Howard University, 2041 Georgia Ave, NW, Washington, DC 20060. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Casella has received an honorarium and travel expenses in the past and presently receives salary support through Johns Hopkins forproviding consultative advice to Mast Pharmaceuticals (previously Adventrx Pharmaceuticals) regarding a proposed clinical trial of an agent for treating vaso-occlusive crisis in sickle cell disease. He is an inventor and a named party on a patent and licensing agreement to ImmunArray for a panel of brain biomarkers forthe detection of brain injury. He has filed a provisional patent for a potential treatment of sickle cell disease; the other authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING: Supported by the National Heart, Lung, and Blood Institute/National Institutes of Health contracts N01-HB-07150 to N01-HB-07160, with partial support ofthe Best Pharmaceuticals for Children Act and the National Institute of Child Health and Human Development. Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
472 RANA et al by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-0917; originally published online August 25, 2014;Pediatrics
and Bruce ThompsonWaclawiwGoldsmith, James F. Casella, Caroline K. Reed, Zora R. Rogers, Myron A.
Sohail Rana, Patricia E. Houston, Winfred C. Wang, Rathi V. Iyer, JonathanHydroxyurea and Growth in Young Children With Sickle Cell Disease
ServicesUpdated Information &
/peds.2014-0917http://pediatrics.aappublications.org/content/early/2014/08/19including high resolution figures, can be found at:
Supplementary Material
0/peds.2014-0917.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2014/08/2Supplementary material can be found at:
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by Lorelle Bradley on September 11, 2014pediatrics.aappublications.orgDownloaded from