A Rat Model for Sickle Cell-Mediated Vaso-occlusion in Retina
11
MICROVASCULAR RESEARCH 52, 270–280 (1996) ARTICLE NO. 0064 A Rat Model for Sickle Cell-Mediated Vaso-occlusion in Retina GERARD A. LUTTY,ANN PHELAN,* D. SCOTT MCLEOD, MARY E. FABRY,² AND RONALD L. NAGEL² The Wilmer Ophthalmological Institute and *the Division of Anesthesiology, Johns Hopkins University School of Medicine, Baltimore, Maryland 21287; and ² Albert Einstein School of Medicine, Bronx, New York Received June 11, 1996 Occlusions of the retinal vasculature are the initiating event in sickle cell retinopathy. In order to understand the mechanism(s) of sickle cell-mediated occlusion, a rat model was developed. Red blood cells (RBCs) from patients homozygous for hemoglobin (Hb) S (SS) or double heterozygous for Hb S and Hb C (SC) were separated on Percoll–Larex continuous density gradients, labeled with fluorescein isothiocyanate (FITC), and delivered via the left ventricle to anesthetized, ventilated rats. Blood gas levels were altered by changing inspired gas and moni- tored via a femoral arterial catheter. After the RBCs circulated for 5 min, animals were perfused with heparinized saline, the eyes enucleated, and the retinas removed and processed by our ADPase flatmount technique. The retinal vasculature was visualized under dark-field illumination and the FITC-RBCs visualized by fluorescence microscopy. Greater numbers of high-density SS cells (SS4, which consist of dense, dehydrated discocytes and irreversible sickled cells) were retained in the normal rat retinal vasculature than normal-density SS cells (SS2, which have the same density as normal AA cells, but consist of reticulocytes and young cells). Retention of SS4 cells was inversely dependent on the arterial oxygen tension. Most SS4s were retained in capillar- ies, but a few were observed within precapillary arterioles. The retained RBCs occupied the full lumenal diameter of vessels in most cases. In contrast, very few RBCs from SC donors (normal or high density) were retained in the normal retinal vasculature and retention did not increase significantly with hypoxia. This model demonstrates that high-density SS cells, which include irreversibly sickled cells, are retained in normal rat retinal vessels and that the number retained is oxygen dependent. Furthermore, it appears that trapping, not adhesion, is responsible for retention of RBCs in the normal retinal vasculature because there was preferential retention of SS4 cells, which are known to have lower adherence propensity, and the retained RBCs blocked the full diameter of the vessel. These results also demonstrate that the mechanism of vascular obstruction by SS and SC RBCs is different because low retention of SC cells was observed. The well-known propensity of SC patients to have retinal abnormalities must involve extraerythrocytic factors like increased hematocrit, induction of adhesive molecules and integrins, etc. q 1996 Academic Press, Inc. INTRODUCTION Sickle cell disease is caused by a point mutation in the hemoglobin gene, which results in hemoglobin that polymerizes when deoxygenated. Under these conditions, polymerization causes the erythrocyte to assume abnormal shapes, some of which are sickle-like, and become less deformable. The two most common b-globin mutations 270 0026-2862/96 $18.00 Copyright q 1996 by Academic Press, Inc. All rights of reproduction in any form reserved.
Transcript of A Rat Model for Sickle Cell-Mediated Vaso-occlusion in Retina

MICROVASCULAR RESEARCH 52, 270–280 (1996)ARTICLE NO. 0064
A Rat Model for Sickle Cell-MediatedVaso-occlusion in Retina
GERARD A. LUTTY, ANN PHELAN,* D. SCOTT MCLEOD,MARY E. FABRY,† AND RONALD L. NAGEL†
The Wilmer Ophthalmological Institute and *the Division of Anesthesiology, Johns HopkinsUniversity School of Medicine, Baltimore, Maryland 21287; and †Albert Einstein
School of Medicine, Bronx, New York
Received June 11, 1996
Occlusions of the retinal vasculature are the initiating event in sickle cell retinopathy. In orderto understand the mechanism(s) of sickle cell-mediated occlusion, a rat model was developed.Red blood cells (RBCs) from patients homozygous for hemoglobin (Hb) S (SS) or doubleheterozygous for Hb S and Hb C (SC) were separated on Percoll–Larex continuous densitygradients, labeled with fluorescein isothiocyanate (FITC), and delivered via the left ventricle toanesthetized, ventilated rats. Blood gas levels were altered by changing inspired gas and moni-tored via a femoral arterial catheter. After the RBCs circulated for 5 min, animals were perfusedwith heparinized saline, the eyes enucleated, and the retinas removed and processed by ourADPase flatmount technique. The retinal vasculature was visualized under dark-field illuminationand the FITC-RBCs visualized by fluorescence microscopy. Greater numbers of high-density SScells (SS4, which consist of dense, dehydrated discocytes and irreversible sickled cells) wereretained in the normal rat retinal vasculature than normal-density SS cells (SS2, which have thesame density as normal AA cells, but consist of reticulocytes and young cells). Retention of SS4cells was inversely dependent on the arterial oxygen tension. Most SS4s were retained in capillar-ies, but a few were observed within precapillary arterioles. The retained RBCs occupied the fulllumenal diameter of vessels in most cases. In contrast, very few RBCs from SC donors (normalor high density) were retained in the normal retinal vasculature and retention did not increasesignificantly with hypoxia. This model demonstrates that high-density SS cells, which includeirreversibly sickled cells, are retained in normal rat retinal vessels and that the number retainedis oxygen dependent. Furthermore, it appears that trapping, not adhesion, is responsible forretention of RBCs in the normal retinal vasculature because there was preferential retention ofSS4 cells, which are known to have lower adherence propensity, and the retained RBCs blockedthe full diameter of the vessel. These results also demonstrate that the mechanism of vascularobstruction by SS and SC RBCs is different because low retention of SC cells was observed. Thewell-known propensity of SC patients to have retinal abnormalities must involve extraerythrocyticfactors like increased hematocrit, induction of adhesive molecules and integrins, etc. q 1996
Academic Press, Inc.
INTRODUCTION
Sickle cell disease is caused by a point mutation in the hemoglobin gene, whichresults in hemoglobin that polymerizes when deoxygenated. Under these conditions,polymerization causes the erythrocyte to assume abnormal shapes, some of which aresickle-like, and become less deformable. The two most common b-globin mutations
270
0026-2862/96 $18.00Copyright q 1996 by Academic Press, Inc.All rights of reproduction in any form reserved.
AID MVR 1978 / 6z0a$$$121 10-23-96 07:41:32 mvra AP: MVR

271SICKLE CELL-MEDIATED VASO-OCCLUSION IN RETINA
are S and C, which represent changes at position 6 from glutamate to valine andglutamate to lysine, respectively. These two mutations are responsible for the twomost prominent, seriously affected genotypes: SS or sickle cell anemia and SC, thedouble heterozygote.
Sickle erythrocytes (red blood cells, RBCs) are believed to initiate vaso-occlusionsin most organ systems in sickle cell subjects. Experimental models have been devel-oped to investigate sickle RBC retention in peripheral microvasculatures. Kaul et al.have observed both adhesion and entrapment of fluorescently labeled sickle RBCs inpostcapillary venules in rat mesocecum (Kaul et al., 1989a). Using technicium-99m-labeled sickle RBCs, Fabry et al. have observed retention in several organ systems,resulting in occlusions, as determined by nuclear magnetic resonance imaging (MRI)(Fabry et al., 1989). Classification of sickle RBC type by density separation has beenused in experimental models to define the role of different sickle RBCs in vaso-occlusions (Kaul et al., 1983). The most dense cells (fraction 4, SS4) include theirreversibly sickled cells (ISCs), while a substantial population of the fraction 2 (SS2)or normal-density cells are sickle reticulocytes. Using density-defined cells in the exvivo mesocecum preparation, Kaul et al. observed deformable SS2 cells adheringpredominantly in postcapillary venules, while entrapment of SS4 cells was enhancedin the presence of adherent SS2 cells (Kaul et al., 1989a). The latter finding is inagreement with Fabry et al., who also observed adherence of SS2 cells using MRI,but found that SS2 adherence alone was not sufficient to cause occlusions (Fabry etal., 1992).
One tissue affected by sickle RBC-initiated occlusions is retina, where vaso-occlu-sions are the initial event in sickle cell retinopathy. Sickle cell retinopathy occursmost frequently in SC subjects and S subjects with b-thalassemia and least frequentlyin SS subjects (Goldberg, 1976, 1977; Serjeant, 1985). The opposite appears to betrue in other organ systems in that vaso-occlusion-initiated pathology occurs in othersystems more commonly in SS subjects than in SC subjects (Powars, 1994). Thereason for this paradox is unclear, but SC subjects have a higher hematocrit (Hct)than SS subjects and, therefore, SC blood has greater viscosity, which has beenimplicated in the higher incidence of retinopathy (Serjeant et al., 1986). Clinically,the initial sites of vaso-occlusion in retina appear to be arteriolar bifurcations predomi-nantly in peripheral retina, as determined by fluorescein angiography (Raichand etal., 1977). The lumenal diameter of retinal capillaries (3.5–6 mm), however, is lessthan the RBC diameter (Wise et al., 1971), so RBCs must deform to traverse themicrovasculature. One would anticipate, therefore, that poorly deformable sickle RBCsmight have difficulty traversing retinal precapillary arterioles and capillaries and be-come trapped. This phenomenon has indeed been observed directly in the mesocecum(Kaul et al., 1989) and similar preparations (Klug et al., 1977; La Celle, 1977) inwhich ISCs obstruct precapillary sphincters.
Histopathologically, retinal occlusions in young SS subjects have been observed atprecapillary arteriolar bifurcations but, with age, all vessels in the retinal vascularhierarchy may become occluded (McLeod et al., 1993). As a result of vaso-occlusions,neural retina becomes ischemic and is believed to release diffusible angiogenic factorswhich stimulate neovascularization, a hallmark of proliferative sickle cell retinopathy.
The purpose of this study was to develop an experimental model in which to studyretention of sickle RBCs in retina. The rat was chosen because its retinal vessels havelumenal diameters similar to those of human retinal vessels and substantial information
AID MVR 1978 / 6z0a$$$121 10-23-96 07:41:32 mvra AP: MVR

272 LUTTY ET AL.
on sickle RBC retention has already been accrued in other vasculatures of the rat(Kaul et al., 1989a,b; Fabry et al., 1992; Aldrich et al., 1996). In this study, sickleRBCs were fluorescently labeled and administered via the left ventricle. After salineperfusion, the retinas were removed from the eyes and incubated for ADPase activity,which forms a lead reaction product in blood vessels facilitating visualization of theretinal vasculature (Lutty et al., 1992). Therefore, sickle RBCs in retinal flatmountscan be visualized by fluorescence microscopy and the blood vessel hierarchy demon-strated by dark-field illumination of the lead ADPase reaction product.
In this initial study, we evaluated the retention of normal density, fraction 2, andhigh density, fraction 4, cells from SS and SC subjects in the normal rat retinalvasculature. We also determined the effects of varying blood gases on sickle RBCretention. Our results demonstrate that human SS4 cells are retained in the normal ratretinal vasculature predominantly at the capillary level and that the retention is directlyrelated to blood oxygen levels. We also found no significant retention of SC cells inthe normal rat retinal vasculature.
METHODS
Blood was obtained from subjects at the Bronx Comprehensive Sickle Cell Center,Bronx, NY. Erythrocytes from sickle cell subjects were isolated from blood by Pallfilters (Pall Biomedical, Inc., Glen Cove, NY) and then Percoll–Larex density gradientseparated as previously described (Fabry et al., 1992). Control erythrocytes fromnormal subjects (AA RBCs) were isolated by passing the blood through a Pall filter.After storage and shipment at 47 overnight, the cells were washed in phosphate-buffered saline (PBS) twice and then labeled with fluorescein isothiocyanate (FITC;Research Organics Inc., Cleveland, OH), 0.1 ml of packed cells/2.0 ml of 0.1% FITCin PBS, for 1 hr at room temperature by the procedure of Butcher et al. (1980).
Male Sprague–Dawley rats (Harlen, Frederick, MD) weighing 200–250 g wereanesthetized with pentobarbital (intraperitoneal 50 mg/kg) and a tracheotomy wasperformed. Ventilation was controlled and supplemental O2, room air, or nitrogenwas administered through the tracheotomy using a Harvard Rodent Ventilator (TV Å1.5 cm3/kg, RR Å 100) to manipulate blood gas values. Femoral and tail arteries werecatheterized to draw samples for blood gas analysis (Acid Base laboratory ABL-3, Radiometer, Copenhagen, Denmark) and to monitor blood pressure via pressuretransducer recording (Gould recording systems, Cleveland, OH), respectively. A me-dian sternotomy was performed to expose the left ventricular chamber of the heart.Rectal temperatures were measured by a YSI thermometer and the temperature wasregulated by heat lamp at 377 { 1.07. FITC-labeled red cells (300 ml, Hct 10) wereinjected into the left ventricle using a tuberculin needle and syringe. Once the needlewas placed into the left ventricular space, 0.5 cc of blood was withdrawn to ensureproper placement of the needle in the ventricle. The mixed rat blood with the labeledRBCs was then slowly injected into the left ventricle over a 1-min time interval. After5 min circulation of labeled cells, the carotid arteries were cannulated bilaterally, thejugular veins were cut, and the brain and eyes perfused clear of blood with 30 ml ofheparinized PBS through each carotid at a rate of 1 ml/min.
Eyes were enucleated immediately and retinas excised and fixed in 2% paraformal-dehyde in 0.1 M cacodylate, pH 7.4. After washing with 0.1 M cacodylate with 5%sucrose, the retinas were incubated for ADPase activity as previously described (Lutty
AID MVR 1978 / 6z0a$$$122 10-23-96 07:41:32 mvra AP: MVR

273SICKLE CELL-MEDIATED VASO-OCCLUSION IN RETINA
et al., 1992). The retinas were viewed as flatmounts on a Zeiss IM microscope witha 16X oil immersion objective. The lead ADPase reaction product was viewed bydark-field illumination and then the light source switched to view the fluorescentRBCs. The total number of retained, FITC-labeled RBCs was determined for eachretina and the cell counts for both retinas from an animal were averaged to give thenumbers presented.
RESULTS
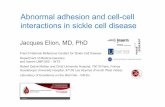
The rat retinal vasculature is a bilayered vasculature with the primary or superficialvasculature lying in the innermost tissue or nerve fiber layer and consisting of arteriesand veins with a limited capillary network. Arterioles feed the secondary or deepvasculature in the inner nuclear layer, which is composed mostly of capillaries andvenules, which anastomose with veins of the primary vasculature. All components ofthe vascular hierarchy are ADPase positive, but arteries and arterioles have the greatestactivity, which appears to ring the blood vessels (Fig. 1A). Capillaries have the leastactivity, with lumenal diameters comparable to human retinal capillaries (3.5–6.0 mmdiameter) (Wise et al., 1971). Because the vasculature is bilayered, the number offluorescently labeled cells in a retina was determined by focusing between the primaryand the secondary vasculature in each microscopic field. Most sickle RBCs wereretained in retinal capillaries (average lumenal diameter 5.4 mm) (Figs. 1 and 2). Thecells appeared to occupy the full extent of the capillary lumens.
In preliminary experiments we determined that changes in blood pressure between50 and 120 mmHg did not significantly affect the number of cells retained. We alsodetermined that the number of cells retained was comparable after 5 and 15 mincirculation, but far fewer cells were observed after 30 min circulation. Hematocrits(Hct, i.e. the volume of packed cells) of injected cells between 10 and 45 wereevaluated and we found that Hct 10 resulted in a sufficient number of retained cellsfor statistical analysis, but Hct 30 or greater yielded too many cells in retina to countin some instances and boxcarring or logjams of labeled cells, making exact cellnumber determinations difficult. Therefore, in the experiments presented, the cellswere administered at Hct 10 and circulated for 5 min under normal blood pressure(80–125).
The type of SS RBC that was retained in the greatest numbers under all conditionswas SS4 (dense SS cells) (Fig. 3). SS4 cells were retained in greater numbers thanSS2 cells from the same donors and in far greater numbers than SC2 or SC4 cells(Fig. 4). For all cell types, the majority of the cells retained were observed in capillaries(5.4 mm average lumenal diameter at site of retention), although some retention inprecapillary arterioles was also observed. The retention of the SS4 cells was inverselyrelated to blood oxygen: the lower the pO2, the more cells retained (Fig. 3). Thistrend was not observed for SS2, SC2, or SC4 cells in general (Figs. 3 and 4). Thenumber of AA RBCs from normal subjects retained in retina was between 2 and 14cells and seemed unrelated to blood gas values (data not shown).
In some experiments, three populations of cells from a donor were used on thesame day: SS2, SS4, and ‘‘total RBCs’’ (cells isolated from blood by Pall filter butnot density separated). In these experiments, retention of total RBCs was comparableor greater than SS4 cells and retention was related to oxygen tension, suggesting thatthe SS4 cells were responsible for retention in this experiment (Fig. 5). When this
AID MVR 1978 / 6z0a$$$122 10-23-96 07:41:32 mvra AP: MVR

274 LUTTY ET AL.
10-23-96 07:41:32 mvra AP: MVR

275SICKLE CELL-MEDIATED VASO-OCCLUSION IN RETINA
FIG. 2. Multiple exposure micrograph showing an area in the far peripheral primary capillary networksimultaneously demonstrates fluorescently labeled cells and blood vessels. The SS4 RBCs (arrows) appearto occupy the entire lumenal diameter of these capillaries. Magnification, 1201.
experiment was performed with cells from SC donors, the total RBCs retained in-creased with hypoxia in all donors, but there was no consistent trend for SC2 or SC4cells in normoxic and hypoxic animals.
As with most measurements of the properties of sickle red cells, there was consider-able interdonor variance in extent of the increase in sickle RBC retention when corre-lated with blood hypoxia. For SS4 cells, increased retention with hypoxia was almostalways observed but with variable slopes, although there was one exception (donorMH) (Fig. 6). In contrast, there was no correlation with blood oxygen for SS2 cells.Retention of SC4 cells from five donors did increase as blood oxygen decreased, withonly one donor showing no change in number retained under normoxic and hypoxicconditions; however, the largest number of SC4 cells retained in any retina was 30compared to 25–550 SS4 cells. Finally, similar to SS2 cells, a minimal number ofSC2 cells were retained in retinal vessels and there was no consistent trend in thenumber retained under normoxic versus hypoxic conditions.
FIG. 1. ADPase-incubated, flatmounted retinas viewed with dark-field illumination (A, C) to show thevasculature and with fluorescence microscopy (B, D) to demonstrate the distribution of fluorescein-labeledSS4 cells. (A) Area of the primary vasculature in the nerve fiber layer showing a small artery (thick arrow),arterioles, and capillaries (arrowheads). (B) A fluorescently labeled SS4 cell at a bifurcation of a capillary(thin arrow). Area in the primary vasculature with a small vein (curved arrow) shown with dark-field (C)and fluorescence (D) demonstrates a sickled RBC in a straight segment of a capillary prior to a bifurcation(thin arrow in D). Magnification, 1001.
AID MVR 1978 / 6z0a$$$122 10-23-96 07:41:32 mvra AP: MVR

276 LUTTY ET AL.
FIG. 3. Number of SS2 (h) and SS4 (m) cells retained in the retinal vasculature as a result of changingarterial pO2. Data points represent the average number of cells from both eyes of each animal.
DISCUSSION
We have developed a model for evaluating sickle erythrocyte-mediated retinal vaso-occlusions in rat. In healthy animals with a normal retinal vasculature, SS4 or denseSS cells were retained in the greatest number. SS2, SC2, and SC4 cells were retainedin numbers only twofold greater than those of AA (normal) RBCs or less. The numberof SS4 cells retained increased dramatically under hypoxic conditions for most donors.The reason for this could be that polymerization occurs rapidly in this population ofSS RBCs under hypoxic conditions and that the polymerization process is reversedslowly (Eaton et al., 1994).
The retention of SS4 cells appeared to be due to trapping and not adhesion. TheSS4 fraction contains the ISCs, which are the most rigid of the SS RBC types. Thecells were retained most often in capillaries and retained cells totally filled the lumens.SS4 cells were also retained in perfused lung preparations under hypoxic conditionsbut, when the perfusate was made normoxic, the cells were released from the microvas-culature, suggesting mechanical trapping (Aldrich et al., 1996). The results in lungwere not unexpected because the lung vasculature, unlike blood vessels in most otherorgans, constricts in response to hypoxia (Voelkel, 1986). In retina, however, onemight assume that dilation would occur under hypoxic conditions because this hasbeen demonstrated in retinal arteries and veins (Hickam et al., 1966). Therefore, theincrease in the number of SS4 cells retained under hypoxic conditions suggests thatpolymer formation is responsible for the mechanical retention.
AID MVR 1978 / 6z0a$$$122 10-23-96 07:41:32 mvra AP: MVR

277SICKLE CELL-MEDIATED VASO-OCCLUSION IN RETINA
FIG. 4. Number of SC2 (h) and SC4 (m) cells retained in the retinal vasculature as a result of changingpO2.
Retention of SS4 but not SS2 cells in our model differs from what has been observedin the mesocecum. In ex vivo preparations of that vasculature, SS2 cells adhere mostprominently in postcapillary venules (Kaul et al., 1989a). When SS2 cells adhere,SS4 cells can obstruct the lumen behind them. An additive effect was observed inour model when retention of total RBCs was compared to retention of SS2 or SS4cells alone, but for SS subjects the retention appeared to be influenced by SS4 andnot SS2 cells. However, in the normal rat retinal vasculature, adhesion of SS2 cellswas not observed.
Pilot studies with rats pretreated with lipopolysaccharide (LPS, 0.2 mg/kg body wt)24 hr prior to experimentation demonstrate that substantial numbers of SS2 cells willadhere in the rat retinal vasculature under normoxic conditions but only after theendothelium is stimulated with cytokines (Lutty et al., 1996). Administration of LPSis known to upregulate the release of TNF-a and IL-1, which can stimulate adhesionmolecule expression by endothelial cells (Vadas et al., 1992).
Variation in red cell retention between donors is not surprising. First, HbF levelsdiffer between patients and the HbF level controls the rate of sickling (Bertles et al.,1968). Second, the concentration of HbS in a given cell (which is directly proportionalto the red cell density) determines the delay time of polymerization in that cell(Mozzarelli et al., 1987) and high-density cells (SS4) will have much shorter delaytimes. The percentage of high-density cells varies widely from patient to patient (Fabryet al., 1984). The percentage of high-density cells also decreases after the onset of
AID MVR 1978 / 6z0a$$$122 10-23-96 07:41:32 mvra AP: MVR

278 LUTTY ET AL.
FIG. 5. Comparison of SS2, SS4, and total RBCs (T/RBCs) from one donor in retinal vessels fromnormoxic and hypoxic animals. Total RBCs represent the entire RBC population, i.e., without densityseparation.
FIG. 6. Summary of the average number of SS4 cells retained in the retinal vasculature with the donorindicated. Lines connect the cell numbers from all animals administered cells from the same donor in thesame experiment. Note that donor KC, for example, was used on two separate occasions.
AID MVR 1978 / 6z0a$$1978 10-23-96 07:41:32 mvra AP: MVR

279SICKLE CELL-MEDIATED VASO-OCCLUSION IN RETINA
painful crisis (Fabry et al., 1984; Ballas, 1992), but patients who had experienced acrisis within the past month were excluded as donors in this study.
Finally, it seems surprising that SS4, not SC2 or SC4 cells, were the most retainedcell population in the rat retina because SC subjects are reported to have a higherincidence of proliferative retinopathy than is expected from their otherwise mild sys-temic course. The higher incidence of retinopathy in SC subjects than in SS subjectshas been attributed to a higher Hct in SC subjects yielding higher blood viscosity(Serjeant et al., 1986), but hematocrit was kept constant in our study. Serjeant hasalso speculated that the higher incidence of proliferative sickle cell retinopathy maybe deceptive because there may be a more rapid rate of autoinfarction of the neovascu-larization in SS subjects, giving the clinical impression that there is less neovasculariza-tion (Serjeant, 1985).
The lack of SC cell trapping in the microcirculation, under the conditions of ourexperiments, could be due to the lower number of very dense cells observed in SCblood and their smaller diameter, both well-established factors which influence thehemodynamic properties of blood (Kaul et al., 1983). Alternatively, the obstructionby SC cells might require the involvement of extraerythrocytic factors. Preliminarydata (Lutty et al., 1996) suggest strongly that exposure of the retinal microcirculatoryendothelium to LPS is accompanied by a very dramatic increase in SC RBC retentionand that this retention is by adhesion and not entrapment as is the case for SS4 cells.
We conclude from this study that high-density SS cells, which include irreversiblysickled cells, are retained in normal retinal vessels of the rat and that the numberretained is oxygen dependent. In contrast, very few SC cells of any density are retained,which suggests that SC RBCs may not be retained in the retinal vasculature of normalrats or that a high Hct of SC cells is required for retention. Therefore, adhesion ofsickle erythrocytes may not be a feature of retinal vaso-occlusion in the steady-state,but endothelial activation may be an important modulating phenomenon in SC subjects.Finally, the model we have developed will be useful in determining the effects ofHct, modulators of vasotonia, cytokines, and adhesion molecules on sickle cell-medi-ated vaso-occlusion in the retinal vasculature.
ACKNOWLEDGMENTS
The authors acknowledge the excellent technical assistance of Sandra Suzuka, Carol Merges, MichaelaKunz, Sylvia Crone, and Rachel Brownstein. This work was supported by NIH Grants HL45922 (G.L.),EY01765 (Wilmer Institute), and HL38655 (R.L.N.). Dr. Lutty is an American Heart Association EstablishedInvestigator.
REFERENCES
Aldrich, T. K., Dhuper, S., Patwa, N. S., Makolo, E., Suzuka, A., Najeebi, S. A., Santhanakrishnan, S.,Nagel, R. L., and Fabry, M. E. (1996). Pulmonary entrapment of sickle cells: The role of regional alveolarhypoxia. J. Appl. Physiol. 80, 531–539.
Ballas, S. K. (1992). Red blood cell changes during the evolution of the sickle cell painful crises. Blood79, 2154–2163.
Bertles, J. F., and Milner, F. A. (1968). Irreversibly sickled erythrocytes: A consequence of the heteroge-neous distribution of hemoglobin types in sickle-cell anemia. J. Clin. Invest. 47, 1731–1741.
Butcher, E. C., and Weissman, I. L. (1980). Direct fluorescent labeling of cells with fluorescein or rhodamineisothiocyanate. I. Technical aspects. J. Immunol. Methods 37, 97–108.
AID MVR 1978 / 6z0a$$$122 10-23-96 07:41:32 mvra AP: MVR

280 LUTTY ET AL.
Eaton, W. A., and Hofrichter, J. (1994). Sickle hemoglobin polymerization. In Sickle Cell Disease: BasicPrinciples and Clinical Practice (S. H. Embury, R. P. Hebbel, N. Mohandas, and M. H. Steinberg, Eds.),pp. 53–87. Raven Press, New York.
Fabry, M. E., Benjamin, L., Lawrence, C., and Nagel, R. L. (1984). An objective sign in painful crisis insickle cell anemia: The concomitant reduction of high density red cells. Blood 64, 559–563.
Fabry, M. E., Fine, E., Rajanayagam, V., Factor, S. M., Gore, J., Sylla, M., and Nagel, R. (1992). Demonstra-tion of endothelial adhesion sickle cells in vivo: A distinct role for deformable sickle cell discocytes.Blood 79, 1602–1611.
Fabry, M. E., Mears, J. G., Patel, P., Schaefer-Rego, K., Carmichael, L. D., Martinez, G., and Nagel, R. L.(1984). Dense cells in sickle cell anemia: The effects of gene interaction. Blood 64, 1042–1046.
Fabry, M. E., Rajanayagam, V., Fine, E., Holland, S., Gore, J. C., Nagel, R. L., and Kaul, D. K. (1989).Modeling sickle cell vaso-occlusion in the rat leg: Quantification of trapped sickle cells and correlationwith 31P metabolic and 1H magnetic resonance imaging changes. Proc. Natl. Acad. Sci. USA 86, 3808–3812.
Goldberg, M. F. (1976). Retinal vaso-occlusion in sickling hemoglobinopathies. Birth Defects 12, 475–515.
Goldberg, M. F. (1977). Retinal neovascularization in sickle cell retinopathy. Trans. Am. Acad. Ophthalmol.Otolaryngol. 83, 409–431.
Hickam, J. B., and Frayser, R. (1966). Studies of the retinal circulation in man. Observations on vesseldiameter, arteriovenous oxygen difference, and mean circulation time. Circulation 33, 302–316.
Kaul, D., Fabry, M., and Nagel, R. (1989a). Microvascular sites and characteristics of sickle cell adhesionto vascular endothelium in shear flow conditions: Pathophysiological implications. Proc. Natl. Acad. Sci.USA 86, 3356–3360.
Kaul, D., Fabry, M., Windisch, P., Baez, S., and Nagel, R. (1983). Erythrocytes in sickle cell anemia areheterogeneous in their rheological and hemodynamic characteristics. J. Clin. Invest. 72, 22–31.
Kaul, D. K., Fabry, M. E., and Nagel, R. L. (1989b). Erythrocytic and vascular factors influencing themicrocirculatory behavior of blood in sickle cell anemia. Ann. N.Y. Acad. Sci. 565, 316–326.
Klug, P. P., and Lessin, L. S. (1977). Microvascular blood flow of sickled erythrocytes. Blood Cells 3,263–272.
La Celle, P. L. (1977). Oxygen delivery to muscle cells during capillary occlusion by sickled erythrocytes.Blood Cells 3, 273–282.
Lutty, G. A., and McLeod, D. S. (1992). A new technique for visualization of the human retinal vasculature.Arch. Ophthalmol. 110, 267–276.
Lutty, G. A., Phelan, A., McLeod, D. S., Merges, C., Suzuka, S. M., Fabry, M. E., and Nagel, R. L. (1996).A rat model for retinal vascular occlusion by human sickle erythrocytes. Invest. Ophthalmol. Vis. Sci.37, S659.
McLeod, D., Goldberg, M., and Lutty, G. (1993). Dual perspective analysis of vascular formations in sicklecell retinopathy. Arch. Ophthalmol. 111, 1234–1245.
Mozzarelli, A., Hofrichter, J., and Eaton, W. A. (1987). Delay time of hemoglobin S polymerization preventsmost cells from sickling in vivo. Science 237, 500–506.
Powars, D. R. (1994). Natural history of disease: The first two decades. In Sickle Cell Disease: BasicPrinciples and Practice (S. H. Embury, R. P. Hebbel, N. Mohandas, and M. H. Steinberg, Eds.), pp.395–412. Raven Press, New York.
Raichand, M., Goldberg, M. F., Nagpal, K. C., Goldbaum, M. H., and Asdourian, G. K. (1977). Evolutionof neovascularization in sickle cell retinopathy. Arch. Ophthalmol. 95, 1543–1552.
Serjeant, B. E., Mason, K. P., Acheson, R. W., Maude, G. H., Stuart, J., and Serjeant, G. R. (1986). Blood rheologyand proliferative retinopathy in homozygous sickle cell disease. Br. J. Ophthalmol. 70, 522–525.
Serjeant, G. R. (1985). Sickle Cell Disease. Oxford Univ. Press, Oxford.
Vadas, M. A., Gamble, J. R., and Smith, W. B. (1992). Regulation of myeloid blood cell–endothelialinteraction by cytokines. In Adhesion. Its Role in Inflammatory Disease (J. M. Harlan and D. Y. Liu,Eds.), pp. 65–81. Freeman, New York.
Voelkel, N. F. (1986). Mechanisms of hypoxic pulmonary vasoconstriction. Am. Rev. Respir. Dis. 133,1186–1195.
Wise, G. N., Dollery, C. T., and Henkind, P. (1971). The Retinal Circulation. Harper and Row, New York.
AID MVR 1978 / 6z0a$$$123 10-23-96 07:41:32 mvra AP: MVR