
HƯỚNG DẪN SỬ DỤNG Tài liệu được xác ... - Trang thiết bị y tế
15
HƯỚNG DẪN SỬ DỤNG Tài liệu được xác nhận bằng chữ ký số Hà Nội, ngày 12 tháng 01 năm 2021 Người đại diện hợp pháp của cơ sở GIÁM ĐỐC Trịnh Diệu Hương
-
Upload
khangminh22 -
Category
Documents
-
view
8 -
download
0
Transcript of HƯỚNG DẪN SỬ DỤNG Tài liệu được xác ... - Trang thiết bị y tế

HƯỚNG DẪN SỬ DỤNG
Tài liệu được xác nhận bằng chữ ký số
Hà Nội, ngày 12 tháng 01 năm 2021 Người đại diện hợp pháp của cơ sở
GIÁM ĐỐC
Trịnh Diệu Hương

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 1 / 7
HƯỚNG DẪN SỬ DỤNG
Thuốc thử dùng cho xét nghiệm định lượng protein toàn phần
Tên sản phẩm Mã sản phẩm Quy cách đóng gói
URINARY/CSF PROTEIN OSR6170 Hộp 4 lọ x 19 mL + 1 lọ x 3 mL
Chỉ dùng trong chẩn đoán in vitro
NGUYÊN LÝ XÉT NGHIỆM
MỤC ĐÍCH SỬ DỤNG
Thuốc thử sử dụng trong xét nghiệm đo màu quang học để định lượng protein toàn phần có trong nước tiểu
và dịch não tủy (CSF) người trên các máy phân tích của hãng Beckman Coulter.
TÓM TẮT VÀ GIẢI THÍCH
Tham khảo (1)
Xét nghiệm protein toàn phần trong nước tiểu đóng vai trò quan trọng trong chẩn đoán và điều trị các bệnh
có liên quan đến thận, tim và chức năng tuyến giáp. Các bệnh này thường đặc trưng bởi protein niệu với 4
dạng chính: (a) tăng tính thấm cầu thận (protein niệu do cầu thận) (b) giảm tái hấp thu ở ống thận (protein
niệu do ống thận) (c) tăng nồng độ protein có trọng lượng phân tử thấp (quá tải protein niệu) (d) xuất hiện
bất thường của protein trong đường dẫn niệu (protein niệu sau thận). Tăng nồng độ protein niệu cũng có
thể xuất hiện sau hoạt động thể lực nặng hoặc trong các tình trạng sau: tăng sinh globulin miễn dịch đơn
dòng, thận ứ nước, biến chứng thận do tiểu đường và nhiễm trùng đường niệu.
Định lượng protein toàn phần trong dịch não tủy đóng vai trò quan trọng trong việc phát hiện tăng tính thấm
của hàng rào máu não với protein huyết tương hoặc tăng sinh các globulin miễn dịch nội màng. Tăng tính
thấm của hàng rào máu não có thể do u não, xuất huyết nội sọ, nhiễm khuẩn hoặc viêm màng não do virus,
viêm não hoặc bại liệt. Xác định tình trạng tăng sinh globulin miễn dịch nội màng có vai trò quan trọng
trong chẩn đoán bệnh gây hủy bao myelin của sợi thần kinh (demyelinating) như bệnh xơ cứng rải rác.
PHƯƠNG PHÁP
Tham khảo (1,2,3)
Đỏ pyrogallol kết hợp với molybdat tạo thành phức hợp màu đỏ có độ hấp thụ tối đa ở bước sóng 470nm.
Xét nghiệm dựa trên sự thay đổi độ hấp thụ khi phức hợp đỏ pyrogallol-molybdat gắn với các nhóm amino
của phân tử protein, hình thành phức hợp màu xanh tím có độ hấp thụ tối đa ở bước sóng 600 nm. Độ hấp
thụ của phức hợp này tỷ lệ thuận với nồng độ protein có trong mẫu.
MẪU BỆNH PHẨM
LOẠI MẪU
Sử dụng mẫu bệnh phẩm nước tiểu và dịch não tủy.

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 2 / 7
Mẫu nước tiểu: Lấy mẫu bệnh phẩm nước tiểu 24 giờ hoặc 12 giờ không chứa chất bảo quản. (4,5,6)
Độ ổn định của mẫu: (7) Xét nghiệm mẫu mới lấy hoặc mẫu được bảo quản ở 2-8oC trong vòng 48 giờ.
Mẫu nước tiểu có chứa hemoglobin có thể cho kết quả cao giả.
Mẫu dịch não tủy: Hãng Beckman Coulter khuyến cáo mẫu cần được chứa trong các dụng cụ trơn.
Cẩn thận khi lấy mẫu dịch não tủy để tránh tạp nhiễm máu vào mẫu bệnh phẩm trong quá trình lấy mẫu.
Độ ổn định của mẫu dịch não tủy: (4) xét nghiệm mẫu mới lấy hoặc mẫu được bảo quản ở 4oC trong vòng
72 giờ.
Tương tự với các phương pháp theo nguyên lý tạo màu, xét nghiệm các mẫu nước tiểu có chứa các globulin
miễn dịch chuỗi nhẹ (ví dụ Protein Bence-Jones) có thể cho kết quả protein thấp giả. Trường hợp nghi ngờ
mẫu có chứa các protein này, khuyến cáo cô đặc mẫu và tiến hành phân tích điện di. (1)
Ngược lại, khi xét nghiệm mẫu nước tiểu từ các bệnh nhân được điều trị bằng các chất thay thế huyết tương
có bản chất polypeptid. Các chất thay thế này có thể được bài tiết vào nước tiểu và dẫn đến kết quả protein
niệu cao. Trường hợp nghi ngờ mẫu có chứa các polypeptid này, khuyến cáo cô đặc mẫu và tiến hành phân
tích điện di.
THUỐC THỬ
CẢNH BÁO VÀ THẬN TRỌNG
Tuân thủ các biện pháp phòng ngừa thường quy khi xử lý tất cả các thuốc thử trong phòng xét nghiệm.
Chất hiệu chuẩn: Các nguyên liệu sinh học có nguồn gốc từ người chứa trong sản phẩm đã được kiểm tra
và cho kết quả âm tính đối với kháng thể kháng virus viêm gan C (anti-HCV), virus HIV 1/2 (anti-HIV 1/2)
và kháng nguyên bề mặt virus viêm gan B (HbsAg) bằng các phương pháp được FDA chấp thuận. Tuy
nhiên, hiện chưa có phương pháp nào có thể đảm bảo chắc chắn rằng các sản phẩm có nguồn gốc từ máu
người không chứa các tác nhân lây nhiễm, do đó, cần thao tác với sản phẩm như nguồn có nguy cơ lây
nhiễm.
Thải bỏ tất cả các chất thải theo quy định của khu vực.
CÁC THÀNH PHẦN PHẢN ỨNG
Nồng độ cuối cùng của các thành phần phản ứng:
Thuốc thử R1: Chất hiệu chuẩn:
Đỏ pyrogallol 47 μmol/L Albumin huyết thanh người 0,50 g/L
Natri molybdat 320 μmol/L Chất bảo quản
Acid succinic 50 mmol/L
Natri benzoat 3,5 mmol/L
Natri oxalat 1,0 mmol/L
Methanol 0,8 % w/v

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 3 / 7
Nồng độ của các thành phần phản ứng trong thuốc thử được ghi trên nhãn của bộ xét nghiệm là nồng độ
thực trong từng lọ R1/R2. Nồng độ của các thành phần thuốc thử ghi trong Tài liệu hướng dẫn sử dụng là
nồng độ cuối cùng của các thành phần trên trong cu-vét phản ứng sau khi thêm R1, mẫu bệnh phẩm.
PHÂN LOẠI NGUY CƠ THEO GHS
Urinary/CSF Protein R1 NGUY HIỂM
H370 Có thể gây tổn thương các cơ quan.
P260 Tránh hít phải hơi thuốc thử.
P308+P311 Nếu đã tiếp xúc hoặc nghi ngờ phơi nhiễm: Liên hệ
với bác sĩ.
Methanol 1 – 2%
Urinary/CSF Protein
Calibrator
CẢNH BÁO
H317 Có thể gây phản ứng dị ứng da.
H412 Ảnh hưởng có hại lâu dài đối với môi trường thủy sinh.
P273 Tránh thải bỏ ra môi trường.
P280 Đeo găng tay, mặc quần áo bảo hộ và sử dụng thiết bị
bảo vệ mắt/mặt.
P333+P313 Nếu bị kích ứng da hoặc phát ban: Yêu cầu chăm
sóc/tư vấn y tế.
P362+P364 Cởi quần áo nhiễm bẩn và giặt sạch trước khi sử dụng.
Khối phản ứng: 5-cloro-2-methyl-4-isothiazolin -3-on
[EC# 247-500-7] và 2-methyl-4-isothiazolin-3-on
[EC# 220-239-6](3:1) < 0,05%
Bảng dữ liệu an toàn có sẵn tại techdocs.beckmancoulter.com
CHUẨN BỊ THUỐC THỬ
Thuốc thử R1 đã sẵn sàng để sử dụng và có thể đặt trực tiếp vào khoang hóa chất của thiết bị. Bảo quản
thuốc thử R1 tránh ánh sáng trực tiếp. Chất hiệu chuẩn đã sẵn sàng để sử dụng.
THẬN TRỌNG
Chất bảo quản natri azide có thể tạo thành các hợp chất gây nổ trong đường ống kim loại.
Tham khảo thông tin trong NIOSH: Nguy cơ gây nổ của azide (8/16/76).
Để tránh tích tụ hợp chất azide, sau khi đổ bỏ thuốc thử chưa được pha loãng, xả đường ống
với nhiều nước. Thải bỏ sản phẩm chứa natri azide theo quy định của khu vực.

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 4 / 7
ĐỘ ỔN ĐỊNH VÀ BẢO QUẢN
1. Thuốc thử và chất hiệu chuẩn chưa mở ổn định đến hết hạn sử dụng ghi trên nhãn khi được bảo quản
ở 2-8oC.
2. Sau khi mở, thuốc thử được bảo quản trong khoang hóa chất của thiết bị sẽ ổn định trong 90 ngày.
Chất hiệu chuẩn đã mở nắp ổn định cho đến khi hết hạn sử dụng ghi trên nhãn với điều kiện nút cao
su và nắp được đóng lại ngay sau khi sử dụng để tránh tạp nhiễm. Bảo quản chất hiệu chuẩn ở 2-8oC.
HIỆU CHUẨN
CHẤT HIỆU CHUẨN CẦN CUNG CẤP
Sử dụng chất hiệu chuẩn được cung cấp sẵn trong bộ xét nghiệm. Tham khảo nhãn sản phẩm để biết giá trị
gán của chất hiệu chuẩn. Chất hiệu chuẩn được truy xuất nguồn gốc theo tiêu chuẩn ban đầu, dựa trên quy
trình chuẩn bị chất hiệu chuẩn sử dụng albumin huyết thanh người tinh khiết theo phương pháp trọng lượng.
Hiệu chuẩn lại xét nghiệm trong các trường hợp sau:
Thay đổi lô thuốc thử hoặc khi giá trị kiểm chứng thay đổi đáng kể;
Bảo dưỡng toàn bộ hoặc thay thế một bộ phận quan trọng của thiết bị.
KIỂM CHỨNG (QC)
Sử dụng các chất kiểm chứng có giá trị được xác định bởi hệ thống Beckman Coulter.
Mỗi phòng xét nghiệm nên tự thiết lập tần suất kiểm chứng riêng. Tuy nhiên, quy trình GLP (Good
laboratory practice – Thực hành tốt phòng xét nghiệm) khuyến cáo nên chạy kiểm chứng vào mỗi ngày xét
nghiệm mẫu bệnh phẩm hoặc vào mỗi thời điểm thực hiện hiệu chuẩn xét nghiệm/chạy mẫu trắng.
Kết quả kiểm chứng thu được ở từng phòng xét nghiệm có thể khác với giá trị trung bình cho trước. Khuyến
cáo mỗi phòng xét nghiệm nên tự xác định giá trị và khoảng giá trị kiểm chứng kỳ vọng đặc hiệu cho từng
chất phân tích, dựa trên nhiều lần chạy để phù hợp với yêu cầu riêng. Giá trị kỳ vọng cần nằm trong dải
chấp nhận tương ứng (được cung cấp trong tài liệu liên quan tới sản phẩm).
Nếu nhận thấy kết quả kiểm chứng thay đổi theo xu hướng hoặc đột ngột, cần kiểm tra lại toàn bộ thông số
cài đặt.
Mỗi phòng xét nghiệm cần xây dựng hướng dẫn cho các hành động khắc phục cần thực hiện khi kết quả
kiểm chứng nằm ngoài giới hạn cho phép.
QUY TRÌNH XÉT NGHIỆM
Tham khảo Tài liệu hướng dẫn sử dụng máy phân tích AU của Beckman Coulter để có hướng dẫn chi tiết
cho từng xét nghiệm cụ thể trên từng máy phân tích với các loại mẫu được liệt kê trong phần Mục đích sử
dụng.
TÍNH TOÁN KẾT QUẢ
Máy xét nghiệm của Beckman Coulter tự động tính toán nồng độ của protein toàn phần có trong mẫu.

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 5 / 7
Máy phân tích tự động trả kết quả theo đơn vị SI (g/L). Để chuyển sang đơn vị mg/dL, nhân kết quả với
hệ số 100.
BÁO CÁO KẾT QUẢ
KHOẢNG THAM CHIẾU
Nước tiểu (1) 0,05 – 0,08 g/ngày khi nghỉ ngơi
Giá trị có thể tăng tới 0,30 g/ngày khi tập luyện
Dịch não tủy (Người trưởng thành) (1) 0,15 – 0,45 g/L
Dịch não tủy (Trẻ sơ sinh < 1 tháng) (1) 0,15 – 1,30 g/L
Giá trị kỳ vọng có thể thay đổi theo tuổi, giới tính, loại mẫu, chế độ ăn và vùng địa lý. Mỗi phòng xét
nghiệm nên tự xác định giá trị kỳ vọng riêng cho quần thể tương ứng, trong trường hợp cần thiết có thể tự
xác định khoảng tham chiếu riêng theo quy trình GLP. Để sử dụng cho mục đích chẩn đoán, kết quả xét
nghiệm phải được đánh giá kết hợp với tiền sử bệnh, thăm khám lâm sàng và các thông tin khác của bệnh
nhân.
LƯU Ý QUY TRÌNH XÉT NGHIỆM
CÁC YẾU TỐ GÂY NHIỄU
Các nghiên cứu được tiến hành trên máy AU cho biết các chất được trình bày dưới đây gây nhiễu xét
nghiệm Urinary/CSF Protein với mức độ <10%:
Chất gây nhiễu Nồng độ xét nghiệm được
(mmol/L)
Nồng độ xét nghiệm được
(g/L)
Amoni 139
Ascobat 1,1
Bilirubin 0,3
Acid Citric 10
Creatinin 26
Cu2+ 1,6
Fe3+ 1,1
Gentamycin 0,04
Glucose 277
Acid oxalic 7,8
Acid tartaric 13
Tobramycin 0,04
Acid Uric 18
Tham khảo tài liệu Young (9) trong mục Tài liệu tham khảo để có thêm thông tin về các chất gây nhiễu.
ĐẶC TÍNH HIỆU NĂNG
ĐẶC TÍNH HIỆU NĂNG

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 6 / 7
Dữ liệu được cung cấp đại diện cho hiệu năng của xét nghiệm trên các hệ thống AU của Beckman Coulter.
Dữ liệu thu được từ các phòng xét nghiệm có thể không giống với các kết quả này.
ĐỘ TUYẾN TÍNH
Xét nghiệm tuyến tính trong dải nồng độ 0,01 – 2,00 g/L.
ĐỘ NHẠY
Nồng độ tối thiểu có thể phát hiện được trên máy AU là 0,005 g/L.
Nồng độ tối thiểu có thể phát hiện được là nồng độ protein toàn phần thấp nhất có thể đo được, phân biệt
từ mức 0 của chất hiệu chuẩn. Nồng độ này được tính toán bằng giá trị trung bình tuyệt đối cộng với 3SD
(dựa trên 20 lần xét nghiệm lặp lại mẫu không chứa chất phân tích).
SO SÁNH PHƯƠNG PHÁP
Một nghiên cứu (sử dụng mẫu bệnh phẩm nước tiểu) để so sánh xét nghiệm Urinary/CSF Protein OSR6x70
trên máy AU với một xét nghiệm protein trong nước tiểu/dịch não tủy thương mại khác, thu được kết quả
phân tích hồi quy tuyến tính dưới đây:
y = 0,957x + 0,009 r = 0,998 n = 108 Dải mẫu = 0,01 – 1,99 g/L
ĐỘ TIN CẬY
Ước lượng độ tin cậy của xét nghiệm dựa trên khuyến cáo của NCCLS (10) phù hợp với hiệu năng điển
hình. Dữ liệu dưới đây thu được từ xét nghiệm 3 mẫu trộn nước tiểu tiến hành trong 20 ngày trên máy AU.
n = 80
Trong cùng lần chạy Toàn phần
Trung bình g/L SD CV
%
SD CV %
0,14 0,002 1,5 0,003 1,8
0,44 0,003 0,8 0,010 2,3
1,60 0,017 1,0 0,042 2,6

Hướng dẫn sử dụng OSR6170 Urinary/CSF Protein
Phiên bản cập nhật tháng 5/2020 Trang 7 / 7
TÀI LIỆU THAM KHẢO
1. Tietz NW. Textbook of clinical chemistry, 2nd ed. Philadelphia: WB Saunders Company, 1994.
2. Fujita Y, Mori I, Kitano S. Color reaction between pyrogallol red molybdenum (VI) complex and
protein. Bunseki Kagaku 1983;32:379-386.
3. Watanabe N, Kamei S, Ohkubo A, Yamanaka M, Ohsawa S,Makino K, Tokuda K. Urinary protein as
measured with pyrogallol red-molybdate complex manually and in Hitachi 726 automated analyser.
Clin Chem 1986;32:1551-1544.
4. Tietz NW. Clinical guide to laboratory tests, 3rd ed. Philadelphia: WB Saunders Company, 1995:518-
520.
5. NCCLS. Urinalysis and collection, transportation and preservation of urine specimens; approved
guideline – second edition. NCCLS document GP16-A2; 2001.
6. Young DS. Effects of preanalytical variables on clinical laboratory tests, 2nd ed. AACC Press, 1997.
7. First MR. Renal Function. In: Kaplan LA, Pesce, AJ, eds. Clinical chemistry: theory, analysis and
correlation, 3rd ed. St. Louis: Mosby-Year Book, 1996:484-504.
8. Pena C, Martinez-Bru C, Homs R, Planella T, Cortes M. Effect of plasma replacement therapy on
determinations of urine protein concentration [Letter]. Clin Chem 1998;44:359-360.
9. Young DS. Effects of drugs on clinical laboratory tests, 5th ed. AACC Press, Washington D.C, 2000.
10. NCCLS. Evaluation of precision performance of clinical chemistry devices; approved guideline.
NCCLS document EP5-A;1999.
Cơ sở sản xuất: Beckman Coulter Ireland Inc.
Địa chỉ: Lismeehan, O’Callaghan’s Mills, Co. Clare, Ireland
Chủ sở hữu sản phẩm: Beckman Coulter, Inc.
Địa chỉ: 250 S. Kraemer Blvd., Brea, CA 92821 USA.

AU UPInstructions For Use© 2020 Beckman Coulter, Inc. All rights reserved.
Urinary/CSF ProteinOSR6170 4 x 19 mL R1, 1 x 3 mL CalibratorOSR6270 4 x 52 mL R1, 1 x 3 mL Calibrator
For in vitro diagnostic use only.
ANNUAL REVIEW
Reviewed by Date Reviewed by Date
PRINCIPLEINTENDED USE
Photometric colour test for the quantitative determination of total protein in human urine and cerebrospinal fluid (CSF)on Beckman Coulter analysers.
SUMMARY AND EXPLANATION
Reference1
Measurement of total protein in urine is important in the diagnosis and treatment of diseases associated with renal,cardiac and thyroid function. These diseases are often characterised by proteinuria of which there are four main types:(a) increased glomerular permeability (glomerular proteinuria) (b) defective tubular reabsorption (tubular proteinuria) (c)increased concentration of low molecular weight protein (overload proteinuria) (d) abnormal secretion of protein into theurinary tract (postrenal proteinuria). Increased levels of urinary protein may also be present following strenuous exerciseor in the following conditions: monoclonal gammopathies, nephritis, diabetic nephropathy or urinary tract infections.
The measurement of total protein in CSF is important in detecting increased permeability of the blood/brain barrierto plasma proteins or to detect increased intrathecal production of immunoglobulins. Increased permeability of theblood brain barrier may result from conditions such as brain tumour, intracerebral haemmorhage or by inflammationcaused by bacterial or viral meningitis, encephalitis or poliomyelitis. Determination of increased intrathecal synthesis ofimmunoglobulins is important in the diagnosis of demyelinating diseases such as multiple sclerosis.
METHODOLOGY
Reference1,2,3
Pyrogallol red is combined with molybdate to form a red complex with a maximum absorbance at 470nm. The assayis based on the shift in absorption that occurs when the pyrogallol red-molybdate complex binds basic amino groups ofprotein molecules. A blue-purple complex is formed with a maximum absorbance at 600 nm. The absorbance of thiscomplex is directly proportional to the protein concentration in the sample.
Instructions For Use BLOSR6X70 09 English UP MetaboliteMAY 2020 Page 1 of 7

SPECIMENTYPE OF SPECIMEN
Urine or cerebrospinal fluid.
Urine: A 24 hour or 12 hour urine specimen with no preservative is preferred.4,5,6
Sample Stability:7 Analyse fresh otherwise stable stored at 2…8°C for up to 48 hours.
Urine samples contaminated by haemoglobin will result in a falsely elevated value.
CSF: Beckman Coulter recommends that CSF samples be collected in plain collection devices.
In the case of CSF samples care should be taken to avoid blood contamination during collection.
Sample Stability:4 Analyse fresh, otherwise stable stored at 4°C for up to 72 hours.
As with all dye based methods, analysis of urine samples containing immunoglobulin light chains (i.e. Bence-JonesProtein) may result in the underestimation of protein. Where such samples are suspected it is recommended that thesample be concentrated and further analysed via electrophoresis.1
Discrepancies may arise when analysing total urine protein in samples from patients who have been treated withpolypeptide-based plasma substitutes.8 The polypeptides from the plasma substitute may be excreted into the urineand result in an elevated total urine protein result. Where such samples are suspected it is recommended that thesample be concentrated and further analysed via electrophoresis.
Specimen storage and stability information provides guidance to the laboratory. Based on specific needs, each laboratorymay establish alternative storage and stability information according to good laboratory practice or from alternativereference documentation.
REAGENTSWARNING AND PRECAUTIONS
Exercise the normal precautions required for handling all laboratory reagents.
Calibrator: Biological materials of human origin contained in the calibrator were tested for anti-HCV, HbsAg and Anti-HIV1/2 on a single donor basis using FDA approved methods and were found to be non-reactive. As there is no known testmethod that can offer complete assurance that products derived from human blood will not transmit infectious agents,this product should be handled as a potentially infectious material.
Dispose of all waste material in accordance with local guidelines.
REACTIVE INGREDIENTS
Final concentration of reactive ingredients:
R1 Calibrator
Pyrogallol Red 47 µmol/L Human Serum Albumin 0.50 g/L
Sodium Molybdate 320 µmol/L Also contains preservatives
Succinic Acid 50 mmol/L
Sodium Benzoate 3.5 mmol/L
Sodium Oxalate 1.0 mmol/L
Methanol 0.8% w/v
UP Metabolite English Instructions For Use BLOSR6X70 09Page 2 of 7 MAY 2020

The concentrations of the reactive components of the reagents shown on the kit label are the actual concentrations inthe individual R1/R2 vials. The reagent composition which is shown in the Instructions For Use is the final concentrationof these components in the reaction cuvette after addition of R1, Sample, and R2.
CAUTION
Sodium azide preservative may form explosive compounds in metal drain lines.See NIOSH Bulletin: Explosive Azide Hazard (8/16/76).To avoid the possible build-up of azide compounds, flush wastepipes withwater after the disposal of undiluted reagent. Sodium azide disposal must be inaccordance with appropriate local regulations.
GHS HAZARD CLASSIFICATION
Urinary/CSF Protein R1 DANGER
H370 Causes damage to organs.
P260 Do not breathe vapours.
P308+P311 If exposed or concerned: Call a doctor/physician.
Methanol 1 - 2%
Urinary/CSF Protein Calibrator WARNING
H317 May cause an allergic skin reaction.
H412 Harmful to aquatic life with long lasting effects.
P273 Avoid release to the environment.
P280 Wear protective gloves, protective clothing and eye/faceprotection.
P333+P313 If skin irritation or rash occurs: Get medicaladvice/attention.
P362+P364 Take off contaminated clothing and wash it before use.
reaction mass of: 5-chloro-2-methyl-4-isothiazolin -3-one[EC# 247-500-7] and 2-methyl-4-isothiazolin-3-one [EC#220-239-6](3:1) < 0.05%
Safety Data Sheet is available at techdocs.beckmancoulter.com
REAGENT PREPARATION
R1 is ready for use and can be placed directly on board the instrument. Protect R1 from direct sunlight. The Calibratoris ready for use.
Instructions For Use BLOSR6X70 09 English UP MetaboliteMAY 2020 Page 3 of 7

STORAGE AND STABILITY
1. The unopened reagent and calibrator are stable until the expiration date printed on the label when stored at 2…8°C.
2. Once open, reagent stored on board the instrument is stable for 90 days. The opened calibrator is stable until theexpiration date on the label, provided that the stopper and cap are replaced immediately after each use to avoidcontamination and the calibrator is stored at 2…8°C.
CALIBRATIONCALIBRATOR REQUIRED
Use Calibrator provided in the kit. For value assigned to the calibrator please refer to bottle label. The calibrator istraceable to a primary standard which is prepared gravimetrically using reagent grade human serum albumin.
Recalibrate the assay when the following occur:
Change in reagent lot or significant shift in control values;
Major preventative maintenance was performed on the analyser or a critical part was replaced.
QUALITY CONTROLControl material with values determined by this Beckman Coulter system may be used.
Each laboratory should establish its own control frequency however good laboratory practice suggests that controls betested each day patient samples are tested and each time calibration/blanking is performed.
The results obtained by any individual laboratory may vary from the given mean value. It is therefore recommended thateach laboratory generates analyte specific control target values and intervals based on multiple runs according to theirrequirements. These target values should fall within the corresponding acceptable ranges given in the relevant productliterature.
If any trends or sudden shifts in values are detected, review all operating parameters.
Each laboratory should establish guidelines for corrective action to be taken if controls do not recover within the specifiedlimits.
TESTING PROCEDURE(S)Refer to the appropriate Beckman Coulter AU analyser User Guide/Instructions For Use (IFU) for analyser-specific assayinstructions for the sample type as listed in the Intended Use statement.
CALCULATIONSThe Beckman Coulter analysers automatically compute the total protein concentration of each sample.
REPORTING RESULTSREFERENCE INTERVALS
Urine1 0.05 – 0.08 g/day at rest
Value may increase to up to 0.30 g/day following exercise.
CSF (Adults)1 0.15 – 0.45 g/L
CSF (newborn <1month)1 0.15 – 1.30 g/L
UP Metabolite English Instructions For Use BLOSR6X70 09Page 4 of 7 MAY 2020

Expected values may vary with age, sex, sample type, diet and geographical location. Each laboratory should verifythe transferability of the expected values to its own population, and if necessary determine its own reference intervalaccording to good laboratory practice. For diagnostic purposes, results should always be assessed in conjunction withthe patient's medical history, clinical examinations and other findings.
PROCEDURAL NOTESINTERFERENCES
Results of studies conducted on the AU400, AU600/AU640, and AU2700/AU5400 show that the following substancesinterfere with this Urinary/CSF Protein procedure by < 10%:
Substance Level Tested(mmol/L)
Level Tested (g/L)
Ammonia 139
Ascorbate 1.1
Bilirubin 0.3
Citric Acid 10
Creatinine 26
Cu2+ 1.6
Fe3+ 0.01
Gentamycin 0.02
Glucose 277
Oxalic acid 5.8
Tartaric Acid 13
Tobramycin 0.03
Uric Acid 18Refer to Young9 for further information on interfering substances.
PERFORMANCE CHARACTERISTICSPERFORMANCE CHARACTERISTICS
Data contained within this section is representative of performance on Beckman Coulter systems. Data obtained in yourlaboratory may differ from these values.
LINEARITY
The test is linear within a concentration range of 0.01 – 2.00 g/L.
SENSITIVITY
The lowest detectable level on an AU analyser was estimated at 0.005 g/L.The lowest detectable level represents the lowest measurable level of total protein that can be distinguished from zero. It is calculated as the absolute mean plus three standard deviations of 20 replicates of an analyte-free sample.
Instructions For Use BLOSR6X70 09 English UP MetaboliteMAY 2020 Page 5 of 7
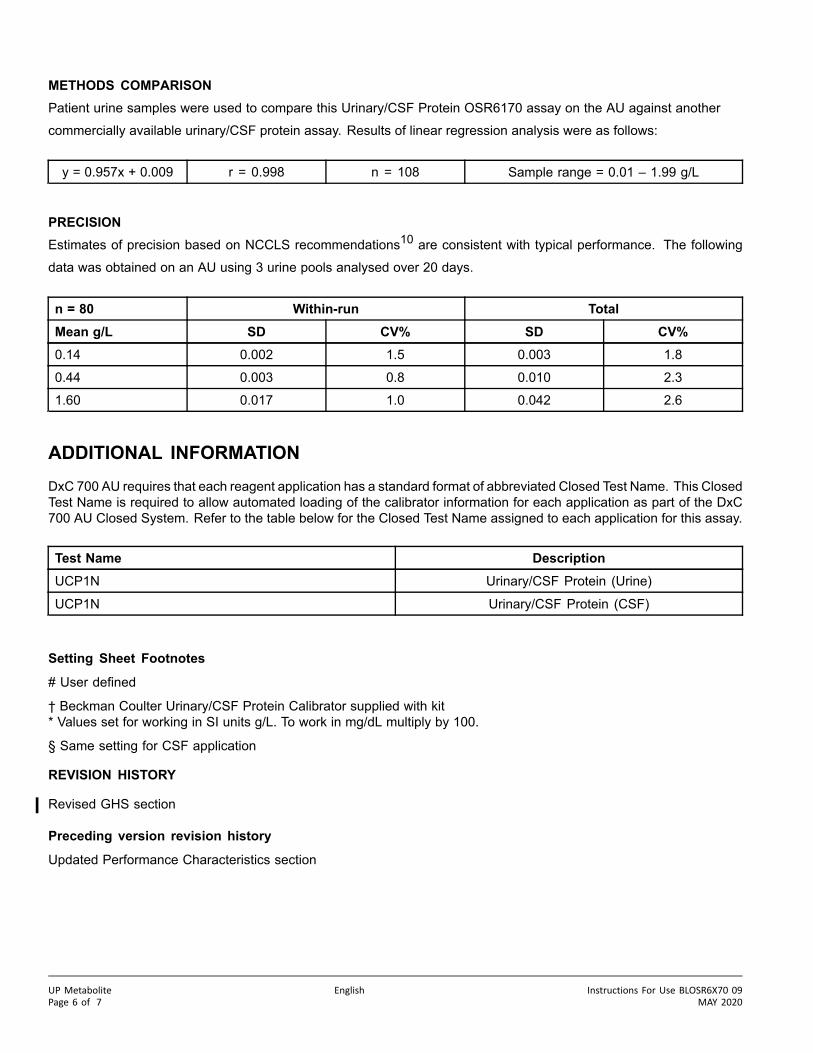
METHODS COMPARISONPatient urine samples were used to compare this Urinary/CSF Protein OSR6170 assay on the AU against another commercially available urinary/CSF protein assay. Results of linear regression analysis were as follows:
y = 0.957x + 0.009 r = 0.998 n = 108 Sample range = 0.01 – 1.99 g/L
PRECISIONEstimates of precision based on NCCLS recommendations10 are consistent with typical performance. The following data was obtained on an AU using 3 urine pools analysed over 20 days.
n = 80 Within-run TotalMean g/L SD CV% SD CV%0.14 0.002 1.5 0.003 1.8
0.44 0.003 0.8 0.010 2.3
1.60 0.017 1.0 0.042 2.6
ADDITIONAL INFORMATIONDxC 700 AU requires that each reagent application has a standard format of abbreviated Closed Test Name. This ClosedTest Name is required to allow automated loading of the calibrator information for each application as part of the DxC700 AU Closed System. Refer to the table below for the Closed Test Name assigned to each application for this assay.
Test Name DescriptionUCP1N Urinary/CSF Protein (Urine)
UCP1N Urinary/CSF Protein (CSF)
Setting Sheet Footnotes
# User defined
† Beckman Coulter Urinary/CSF Protein Calibrator supplied with kit* Values set for working in SI units g/L. To work in mg/dL multiply by 100.
§ Same setting for CSF application
REVISION HISTORY
Revised GHS section
Preceding version revision history
Updated Performance Characteristics section
UP Metabolite English Instructions For Use BLOSR6X70 09Page 6 of 7 MAY 2020

REFERENCES1. Tietz NW. Textbook of clinical chemistry, 2nd ed. Philadelphia: WB Saunders Company, 1994.
2. Fujita Y, Mori I, Kitano S. Color reaction between pyrogallol red molybdenum (VI) complex and protein. BunsekiKagaku 1983;32:379-386.
3. Watanabe N, Kamei S, Ohkubo A, Yamanaka M, Ohsawa S,Makino K, Tokuda K. Urinary protein asmeasured with pyrogallol red-molybdate complex manually and in Hitachi 726 automated analyser. Clin Chem1986;32:1551-1544.
4. Tietz NW. Clinical guide to laboratory tests, 3rd ed. Philadelphia: WB Saunders Company, 1995:518-520.
5. NCCLS. Urinalysis and collection, transportation and preservation of urine specimens; approved guideline - secondedition. NCCLS document GP16-A2; 2001.
6. Young DS. Effects of preanalytical variables on clinical laboratory tests, 2nd ed. AACC Press, 1997.
7. First MR. Renal Function. In: Kaplan LA, Pesce, AJ, eds. Clinical chemistry: theory, analysis and correlation, 3rded. St. Louis: Mosby-Year Book, 1996:484-504.
8. Pena C, Martinez-Bru C, Homs R, Planella T, Cortes M. Effect of plasma replacement therapy on determinationsof urine protein concentration [Letter]. Clin Chem 1998;44:359-360.
9. Young DS. Effects of drugs on clinical laboratory tests, 5th ed. AACC Press, Washington D.C, 2000.
10. NCCLS. Evaluation of precision performance of clinical chemistry devices; approved guideline. NCCLS documentEP5-A;1999.
Beckman Coulter Ireland Inc., Lismeehan, O’Callaghan’s Mills Co. Clare, Ireland (001) 703-527-3887
Beckman Coulter, Inc., 250 S. Kraemer Blvd., Brea, CA 92821 U.S.A.www.beckmancoulter.com
Instructions For Use BLOSR6X70 09 English UP MetaboliteMAY 2020 Page 7 of 7




















