Evaluation of Cardiology Training and Manpower Futures (of ...
Upload
independentCategory
view
3download
0
Rev Esp Cardiol. 2011;64(10):883–890
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Original article
How Beta-Blockers Are Used in Spain? Analysis of Limitations in Their Usein Internal Medicine and Cardiology: CARACTER-BETA Study
Xavier Garcia-Moll,a,* Lorenzo Facila,b Pedro Conthe,c Antonio Zapata,d Remei Artigas,d
Vicente Bertomeu,e and Jose Ramon Gonzalez-Juanatey,f on behalf of the CARACTER-BETAstudy investigators^
a Servicio de Cardiologıa, Hospital de la Santa Creu i Sant Pau, Barcelona, Spainb Servicio de Cardiologıa, Consorcio Hospital General Universitario de Valencia, Valencia, Spainc Servicio de Medicina Interna, Hospital General Universitario Gregorio Maranon, Madrid, Spaind Laboratorios Menarini, Badalona, Barcelona, Spaine Servicio de Cardiologıa, Hospital de San Juan, San Juan de Alicante, Alicante, Spainf Servicio de Cardiologıa, Hospital Clınico Universitario, Santiago de Compostela, A Coruna, Spain
Article history:
Received 31 January 2011
Accepted 29 May 2011
Available online 31 August 2011
Keywords:
Stable angina
Atrial fibrillation
Heart failure
Beta-blockers
A B S T R A C T
Introduction and objectives: Beta-blocker treatment has a class I indication, level of evidence A, in
guidelines for the treatment of heart failure, ischemic heart disease, and atrial fibrillation. However,
beta-blocker use continues to be less than optimal. In this study, beta-blocker use in Spain is analyzed in
patients with heart failure, ischemic heart disease, and atrial fibrillation.
Methods: Observational, epidemiologic, cross-sectional, multicenter study including 1608 patients with
heart failure, ischemic heart disease, and/or atrial fibrillation, recruited in 150 healthcare centers by
cardiologists and internal medicine specialists.
Results: Cardiologists enrolled 78.6% patients and internal medicine specialists 21.4%; 25.8% were
recruited at hospital discharge and 74.2% at outpatient centers. Men accounted for 77% of the sample,
and age was 68 (12) years. Of the total, 73% had ischemic heart disease, 42% heart failure, and 36% atrial
fibrillation (multiresponse variable). beta-blockers were given to 82.8% of those consulting in cardiology
compared to 71.6% of those treated in internal medicine (P<.0001). By pathology, the prescription rate
was 85.1% of patients with ischemic heart disease, 77.0% of those with heart failure, and 72.4% of those
with atrial fibrillation. Cardiology prescribed significantly more beta-blockers for ischemic heart disease
and heart failure than did internal medicine. Multivariate analysis showed that beta-blocker use
increased when the patient had ischemic heart disease, was treated by a cardiologist, and had
dyslipidemia, stroke, and/or left ventricular hypertrophy. Beta-blocker use decreased with age and with
a history of bronchospasm, asthma, bradycardia, chronic obstructive pulmonary disease, and/or
intermittent claudication.
Conclusions: There is still room for improvement in beta-blocker prescription in Spain for patients with
ischemic heart disease, heart failure, and/or atrial fibrillation.
� 2011 Sociedad Espanola de Cardiologıa. Published by Elsevier Espana, S.L. All rights reserved.
?
Como se usan los bloqueadores beta en Espana? Analisis de las limitaciones parasu uso en medicina interna y cardiologıa: estudio CARACTER-BETA
Palabras clave:
Angina estable
Fibrilacion auricular
Insuficiencia cardiaca
Bloqueadores beta
R E S U M E N
Introduccion y objetivos: El tratamiento con bloqueadores beta tiene una indicacion de clase I y nivel
de evidencia A en las guıas de tratamiento de insuficiencia cardiaca, cardiopatıa isquemica y
fibrilacion auricular. A pesar de ello, el uso de bloqueadores beta sigue siendo inferior a lo deseable.
El objetivo principal del estudio es analizar el uso de los bloqueadores beta en Espana en pacientes
con cardiopatıa isquemica, insuficiencia cardiaca, fibrilacion auricular.
Metodos: Estudio epidemiologico observacional, transversal y multicentrico, que incluye a
1.608 pacientes con cardiopatıa isquemica, insuficiencia cardiaca y/o fibrilacion auricular reclutados
en 150 centros sanitarios por cardiologos y medicos internistas.
Resultados: El 78,6% de los pacientes fueron incluidos en cardiologıa, y el 21,4%, en medicina interna; se
recogio al 25,8% en altas hospitalarias y al 74,2%, en consultas externas. El 67% eran varones. La media de
edad era 68 � 12 anos. El 73% tenıa cardiopatıa isquemica; el 42%, insuficiencia cardiaca, y el 36%, fibrilacion
auricular (variable multirrespuesta). El 82,8% de los tratados en cardiologıa recibio bloqueadores beta, frente
al 71,6% de los tratados en medicina interna (p < 0,0001). Por enfermedades, el 85,1% de los pacientes con
* Corresponding author: Servicio de Cardiologıa, Hospital de la Santa Creu i Sant Pau, Sant Antoni Maria Claret 167, 08025 Barcelona, Spain.
E-mail address: [email protected] (X. Garcia-Moll).^ The appendix lists the names of the investigators who participated in the first phase of the CARACTER-BETA study.
1885-5857/$ – see front matter � 2011 Sociedad Espanola de Cardiologıa. Published by Elsevier Espana, S.L. All rights reserved.
doi:10.1016/j.rec.2011.05.027

X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890884
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
cardiopatıa isquemica, el 77% con insuficiencia cardiaca y el 72,4% con fibrilacion auricular. Cardiologıa
prescribio significativamente mas bloqueadores beta que medicina interna en cardiopatıa isquemica e
insuficiencia cardiaca. El analisis multivariable mostro que los bloqueadores beta aumentan si se padece
cardiopatıa isquemica, se es tratado por un cardiologo, se tiene dislipemia, accidente cerebrovascular y/o
hipertrofia ventricular izquierda. Disminuyen los bloqueadores beta con la edad, el broncospasmo y el asma
bronquial, la bradicardia, la enfermedad pulmonar obstructiva cronica y/o la claudicacion intermitente.
Conclusiones: Todavıa existen margenes de mejora en la prescripcion de bloqueadores beta a pacientes
con cardiopatıa isquemica, insuficiencia cardiaca y/o fibrilacion auricular en Espana.
� 2011 Sociedad Espanola de Cardiologıa. Publicado por Elsevier Espana, S.L. Todos los derechos reservados.
Abbreviations
ACEI: angiotensin converting enzyme inhibitor
AF: atrial fibrillation
BB: beta-blockers
CHF: chronic heart failure
INTRODUCTION
Cardiovascular diseases constitute an important public healthproblem. These severe chronic conditions, particularly ischemicheart disease and cerebrovascular disease, are the main cause ofdeath in our society.1
The prevalence of some of these conditions, for example, chronicheart failure (CHF), is continuously increasing (around 10% in thepopulation older than 70 years),2 affecting the quality of life andsurvival of patients. The prognosis of patients with heart disease hasimproved with the advances in preventing cardiovascular riskfactors and in treatments, but mortality and morbidity rates remainvery high. This is due, in part, to improper use of medication with aproven beneficial effect on cardiovascular disease in general, such asantiplatelet agents, lipid-lowering drugs, angiotensin-convertingenzyme inhibitors (ACEIs), and beta-blockers (BBs).3,4
BB treatment has a significant role in cardiovascular disease,being used for years because of its anti-ischemic, antiarrhythmic,and antihypertensive properties. The favorable effects of adrener-gic blockade have been recently established in patients with heartfailure.5 The benefits and clinical indications for BB use have beenclearly established in several European and American guidelinesfor the diagnosis and treatment of these conditions (eg, CHF, stableangina, atrial fibrillation [AF]),6–8 and there is consensus on theiruse with a class I indication, level of evidence A, in the treatment ofchronic ischemic heart disease, CHF, and AF (in this last indication,together with nondihydropyridine calcium channel blockers).Nonetheless, adherence to the guidelines in general and to the useof BBs in particular remains less rigorous that would be desirableand is very disparate between European countries.9–11
The main objective of this study is to determine the therapeuticuse of BBs for class I indications, level of evidence A (ischemic heartdisease, CHF, and/or AF) in the clinical practice of specialistsprescribing treatment for these patients. The secondary aims are toevaluate which factors determine the use of BBs and whether thereare differences regarding the medical specialties in which thesepatients are treated.
METHODS
CARACTER-BETA is a multicenter, cross-sectional, observationalstudy, performed under the aegis of the Hypertension Section ofthe Spanish Society of Cardiology and conducted in Spain.
COPD: chronic obstructive pulmonary disease
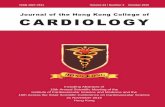
A total of 1608 consecutive patients were recruited in150 centers from across the country. The geographic distributionof participants by autonomous communities is shown in Figure 1.The recruiting physicians were internal medicine specialists andcardiologists, working in outpatient clinics and hospital wards.
Physicians were chosen from all over Spain, and participation ofthe patients included by autonomous community was propor-tionate to the demographic weight of each community within thetotal in Spain (Fig. 1). Patients were consecutively recruited and thenumber that each participating physician could include waslimited to minimize the possibility of selection bias. The inclusioncriteria were the following: signed informed consent; age olderthan 18 years; having been diagnosed of and treated for ischemicheart disease, CHF, and/or AF; and attending regular follow-upvisits in an outpatient clinic or having received a hospitaldischarge. With regard to the heart failure criterion, the conditionhad to be in a stable phase because the indication for BBs inunstable heart failure is class IIb, level of evidence C.
The exclusion criteria were current participation in a clinicaltrial involving BBs or presence of any abnormality that couldcompromise the ability to provide written informed consent forparticipation and/or fulfill the procedures required for the study.
Among the 1608 patients initially enrolled, 1582 (98.38%)patients were ultimately eligible for the analysis. Patients wereconsidered invalid for the analysis if they did not fulfill one or moreof the proposed selection criteria (n=17), had no record of treatmentof any kind (n=7), or were receiving more than one BB (n=2).
The study was approved by an independent ethics committee(Ethics Committee for Clinical Research, Hospital de San Juan de
Alicante) on 28 March 2007 and was carried out in keeping with theethics requirements expressed in the Declaration of Helsinki.Patients were informed before recruitment, and they received aninformation form and signed an informed consent for participationbefore the study was initiated. The data collected were identifiedby codes, and confidentiality was maintained in accordance withOrganic Law 15/1999 (13 December) for the protection of personaldata, and Royal Decree 994/1999 (11 June) regarding securitymeasures for computer files containing personal data.
Statistical Analysis and Sample Calculation
The main study variable was the percentage of patients who, atthe time of the visit, were receiving pharmacological treatment inkeeping with the guidelines of the European Society of Cardiology,in particular regarding BB use (treated/untreated, indicated/notindicated because of a contraindication).
Sample Size Calculation
The sample size was calculated assuming maximal uncertainty orindifference (p=q=0.5) related to the therapeutic approach in the useof BBs, because of the fact that precise, homogeneous data werenot available. Therefore, based on inclusion of 1800 patients in thestudy, it was calculated that a precision of 2.3% would be achieved

Andalusia
Aragon
Asturias
Balearic lslands
Valencian community
Canary Islands
Cantabria
Castile-La Mancha
Castile and León
Catalonia
Extremadura
Galicia
La Rioja
Community of Madrid
Murcia
Navarre
Basque country
11.9%
13.7%
14.8%
7.9%
10.5%
Figure 1. Distribution of the patients included by autonomous communities.
X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890 885
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
in estimating a percentage by a normal bilateral asymptotic95% confidence interval, assuming that the percentage would be50% and setting the patient loss rate due to incomplete data at 10%.Nonetheless, following a quality control process of the data obtained,1582 patients were ultimately included in the study. Because thepremise of maximum uncertainty or indifference was not met inthe study, but instead was P=.804 and q=0.196, and assuming thesame confidence interval, the degree of precision reached wascalculated at 1.96%, which was better than the initial target.
Statistical Analysis
The descriptive statistics included the distribution of frequen-cies, measures of central tendency, standard deviation, andcalculation of 95% confidence intervals. Bivariate analysis ofcategorical values was performed by comparing contingencytables, using the x2 test with variables of a nominal type and theFisher exact test when appropriate. Continuous variables that metthe assumptions of normality for dichotomous variables wereanalyzed with the Student t test and variables with more than2 categories, by analysis of variance. Variables with a non-normaldistribution were analyzed with the Mann-Whitney U test andKruskal-Wallis test, respectively. The principal study variable, BBuse, underwent descriptive evaluation and logistic regression
Table 1Demographic Characteristics of the Study Population
Cardiology
Men, % 67
Age, years 66.6
Systolic pressure, mmHg 133.8 (19.7)
Diastolic pressure, mmHg 76.4 (11.5)
Heart rate, bpm 70 (13)
Hypertension, % 70
Diabetes mellitus, % 28
Dyslipidemia, % 63.4
Stroke, % 7.6
LVH on ECG, % 42.9
Intermittent claudication, % 5.8
COPD, % 9.7
COPD, chronic obstructive pulmonary disease; ECG, electrocardiography; LVH, left ven
Data expressed as the mean (standard deviation), unless otherwise indicated.
analysis using the stepwise method and including all factors thatcould have an influence on BB prescription. Significance was set ata two-tailed P value of .05.
RESULTS
A total of 1608 patients from across the country were recruited,and 1582 (98.38%) patients fulfilled the selection criteria forinclusion in the analysis. Of the patients included, 79% were fromcardiology (1244 patients vs 338 patients from internal medicine),26% had been discharged from hospital, and 74% were fromoutpatient clinics.
The baseline characteristics of the population studied areshown in Table 1 and the baseline analytical parameters aresummarized in Table 2.
Mean age of the study patients was 67.5 (11.6) years, two-thirdswere men, and the mean body mass index was 28.35 (4.15). Thebody mass index was �25 in 81.1% of patients. Mean abdominalgirth was 97.8 (13.18) cm, and 47.7% of patients had criteriafor abdominal obesity (men, >102 cm; women, >88 cm). Theprevalence of hypertension was 72.2%, diabetes mellitus 31.7%,and dyslipidemia 62.8%.
Patients seen in cardiology were younger (66.6 [11.6] vs 70.8[10.9] years in internal medicine; P<.0001) and there was a higher
Internal medicine P
60 .0027
70.8 <.0001
138.1 (18.9) .001
78.9 (18.9) .0007
74 (12) <.0001
81.1 <.0001
45.3 <.0001
60.4 NS
17.8 <.0001
47.4 .037
11.8 .0003
12.1 .19
tricular hypertrophy.

Table 2Baseline Laboratory Data of the Study Population
Analytic parameters Mean (SD) range
Hematocrit, % 40.4 (5.95) 10.8-60
Hemoglobin, g/dL 14.1 (3.98) 1.2-53
Creatinine, mg/dL 1.1 (0.45) 0.1-8.7
Total cholesterol, mg/dL 189.11 (42.16) 79-346
HDLc, mg/dL 45.44 (13.45) 10-137
LDLc, mg/dL 113.76 (35.64) 24-268
Triglycerides, mg/dL 143.91 (79.44) 28-1085
Glucose, mg/dL 113.43 (37.53) 20.9-470
Glycohemoglobin, % 6.84 (1.59) 1-14.2
Sodium, mEq/L 139.86 (3.71) 105-153
Potassium, mEq/L 4.39 (0.5) 2.9-6.4
BNP, pg/mL; median (95% CI) range 77.5 (213.99-750.44) 15-6100
BNP, B-type natriuretic peptide; CI, confidence interval; HDLc, high-density
lipoprotein cholesterol; LDLc, low- density lipoprotein cholesterol; SD, standard
deviation.
X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890886
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
percentage of men (68.7% vs 59.4% in internal medicine; P<.003).These differences were also seen according to the heart diseaseunder study: patients with ischemic heart disease were signifi-cantly younger (66.8 [11.6] years vs 70.2 years for patients withheart failure and 70.8 years for those with AF; P<.0001) and weremore often men (72.4% vs 59.6% of patients with heart failure and56.9% of those with AF).
Echocardiography was performed in 89.8% of the studypatients, with no differences between those seen in cardiologyor in internal medicine. Mean left ventricular ejection fraction was55% (55% in ischemic patients, 49% in those with CHF, and 55% inpatients with AF). This was an older population, in which theprevalence of heart failure with preserved ventricular function wasnotable, above all in patients consulting in internal medicine.
With respect to the patients’ habits, 23% consumed alcohol,although only 3% of the total population (11.8% of those who drankalcohol) admitted to drinking more than 80 mg per day. Among thetotal, 15.3% were active smokers of a mean of 16.1 (9.9) cigarettesper day, and 40.4% practiced some type of physical exercise.Patients consulting in cardiology smoked somewhat less (15.6[10.2] cigarettes vs 18.5 [7.9] in internal medicine) and exercisedmore (44.4% vs 25.8% in internal medicine).
BB were prescribed to 85.1% of patients with ischemic heartdisease, 77% of those with CHF, and 72.4% of those with AF. Ingeneral, patients with ischemic heart disease consulted more oftenwith cardiologists (74% vs 67.5% in internal medicine), whereasinternal medicine specialists treated a larger number of patientswith CHF (52.1% vs 39% in cardiology) and/or AF (40.8% vs 34.1%).
Use of BBs was similar in hospitals and in the outpatient setting(82.3% at hospital discharge and 79.6% in outpatient clinics). However,BB use was significantly higher in cardiology than in internalmedicine (82.8% vs 71.6%; P<.0001). Furthermore, most cardiologistscontemplated BB use, and among patients who did not receive them,there was a specific reason in 63.2% and in 11% it was because ofintolerance (in internal medicine, 51.8% and 10.8%, respectively).Thus, no reason was given in 25.9% of patients who were not treatedwith BBs in cardiology (37.4% in internal medicine; P=.05).
Reasons for Not Prescribing Beta-Blockers
BB were not prescribed in 19.6% of all patients: in 5.7%, it wasnot considered to be indicated, in 11.7% it was not prescribedbecause of a specific reason, and in 2.1%, it was indicated, but nottolerated by the patients.
The reasons why BB treatment was not prescribed in cardiologyand internal medicine are shown in Figure 2, In internal medicine,an ‘‘unfavorable social situation’’ was given as the main limitationto prescribing BBs. It is worthy of note that the presence of arespiratory disorder was more often the reason for not prescribingBBs in cardiology than in internal medicine, despite the fact thatthere is a higher prevalence of these disorders in patients treatedby internal medicine specialists. In contrast, bradycardia anddiabetes mellitus were more important reasons for not prescribingthese drugs in internal medicine than in cardiology.
Beta-Blockers in Ischemic Heart Disease
The most common condition under study was ischemic heartdisease (72.6% of patients), in which BB use was high, alwaysexceeding 80%. No differences in prescribing these drugs wereobserved between outpatient treatment and at hospital discharge(84.0% vs 87.9%, respectively). However, their use was morefrequent in cardiology than in internal medicine (86.3% vs 80.3%;P<.05). The most commonly used combined regimen was a BB,ACEI, antiplatelet agent, and lipid-lowering drug (42.1% of patientswith ischemic heart disease).
Beta-Blockers in Heart Failure
Among the patients included, 41.8% had CHF. New York HeartAssociation functional class II was the most common (54.5%),accounting for 46% of hospital admissions during the year prior tothe study. A depressed ejection fraction (left ventricular ejectionfraction <35%) was documented in 46%. Use of BBs was less intensein patients with CHF, with no significant variation betweenoutpatient prescription and hospital discharge (76.9 vs 77%).Similar to what was seen in ischemic heart disease, CHF patientstreated in cardiology received BBs more often than patients treatedin internal medicine (81.7% vs 64.2%; P<.00005). The mostcommonly used combination was a BB, ACEI/angiotensin IIreceptor antagonist, antiplatelet/anticoagulant, diuretic, andlipid-lowering drug (46.4% of CHF patients).
Beta-Blockers in Atrial Fibrillation
Among the total series, 35.5% of patients had AF. The diagnosisof this condition had been made in the 3 years before the study(interquartile range, 1-6 years). In 55.6%, AF was permanent, and25.2% of patients had undergone cardioversion in the previous2 years. Treatment with BBs was similar in both settings underconsideration (outpatient, 71.6%; hospital discharge, 74.8%) and inboth medical specialties (cardiology, 74.3%; internal medicine,66.7%). The most commonly prescribed combination was a BB,ACEI/angiotensin II receptor antagonist, and an anticoagulant(23.1% of FA patients).
Other Treatment
The treatments patients received are summarized in Figure 3.Proper use of the other drug groups is evident, such as lipid-lowering drugs, antiplatelet agents, ACEI, and angiotensin IIreceptor antagonists. These findings are consistent with recentlypublished data in Spanish registries of ischemic heart disease.12
Independent Predictors of Beta-Blocker Use
The use or not of BBs was considered the dependentvariable, and the following variables were considered explicative

5.5
0.8
0
0
0.8
1.6
5.5
4.7
3.2
5.5
6.3
11.0
15.8
14.2
22.8
26
4.7
4.7
7.0
4.7
9.3
4.7
11.6
9.3
9.30
30.2
14.0
34.9
0 5 10 15 20 25 30 35 40
Others
Erectile dysfunction
Cognitive deterioration
Hypotension
AV block
Muscle fatigue
Depresion
Diabetes
Arterial disease
COPD
Bradycardia
Bronchial asthma
Unfavorable social situation
Internal medicine
Cardiology
Difficulties with follow-up
P=.33
P=.02
P=.45
P=.28
P=.00
P=.32
P=.00
P=.11
P=1.00
P=.19
P=.10
P=.16
P=.16
P=.19
Patients, %
Figure 2. Reasons why beta-blockers were not indicated in patients for whom their use was considered. AV, atrioventricular; COPD, chronic obstructive pulmonarydisease.
X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890 887
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
variables: sex, age, cardiovascular diseases under study (ischemicheart disease, CHF, and AF or atrial flutter), specialty (patienttreated in cardiology/internal medicine) and various concomitantdiseases (hypertension, diabetes mellitus, dyslipidemia, stroke, leftventricular hypertrophy, hepatic failure, second- or third-degreeatrioventricular block, history of bronchospasm and bronchialasthma, bradycardia, hypotension, chronic obstructive pulmonarydisease [COPD] and intermittent claudication). Multiple regressionanalysis was used to determine which variables were indepen-dently associated with BB use (Table 3). We entered in the modelvariables showing differences between using and not using BBs aswell as variables with differences between internal medicine andcardiology to adjust for the various baseline characteristics of thepatients in these two settings. We saw that as the age of the patientincreased, the probability of being prescribed a BB decreased, andthat the same was true for a history of respiratory conditions,bradycardia, and intermittent claudication. In contrast, if a patientwith ischemic heart disease and/or a history of dyslipidemia,stroke, and/or left ventricular hypertrophy consulted in cardiology,the probability of receiving BB treatment increased. The Hosmer-Lemeshow test indicated that the regression model had satisfac-tory goodness-of-fit (P=.8808), ie, the degree to which thepredicted probability coincides with the observed probability.Lastly, the ROC curve obtained with the model showed gooddiscrimination (P=.758).
DISCUSSION
BB use in Spain has improved over the past decade. Data fromthe Spanish registries PREVESE I and II (patients with acutemyocardial infarction), 3C program (patients at discharge follow-ing an acute coronary syndrome), PRIAMHO (acute coronary
syndrome with ST segment elevation), and DESCARTES (acutecoronary syndrome without ST segment elevation) show BB use in50% to 60% of patients with acute ischemic heart disease.13–18
Furthermore, in the more recent studies BB use is seen to increase,as shown in Table 4, which also includes data from theEUROASPIRE and TRECE registries.19–22 In the present study, weobserved an increase in the use of these drugs for ischemic heartdisease (more than 80% of patients) and for CHF (around 75%). Theischemic heart disease data are in line with the overall results fromEUROASPIRE III (around 80%),19 in which the data were collected2 years before those from the present study. The specific data forSpain, however, were lower (around 60%).
In the present study, we found differences in BB use accordingto the attending specialty (cardiology or internal medicine) andaccording to the setting (hospital discharge or outpatienttreatment). Overall, BBs were used more in cardiology than ininternal medicine, whether to treat ischemic heart disease, CHF, orAF. Although in AF the difference showed a trend similar to that ofthe other 2 disease groups, it did not reach statistical significance,likely because of the smaller number of patients included. Thedifference was, however, very evident in the treatment of heartfailure, in which 64.2% of patients treated in internal medicinereceived BBs compared to 81.7% of those treated in cardiology,with both values being lower than the BB use reported in therecently published SHIFT study.23 A part of the treatmentdifferences between specialties can be explained by the differingbaseline characteristics of the patients treated in each of them.For example, the percentage of women was higher in internalmedicine, and women received BBs less frequently thanmen. Nonetheless, patients treated in internal medicine had ahigher prevalence of cardiovascular risk factors (older age anda higher prevalence of hypertension and diabetes) and moreextracardiac manifestations of atherosclerotic disease (stroke and

Table 3Multiple Regression Analysis to Identify Variables That IndependentlyExplained the Use or Not of Beta-Blockers in Study Patients
Effect OR (95% CI) P
Constant 8.3 (2.98-23.13) <.0001
Age, years 0.97 (0.96-0.98) .0003
Ischemic heart disease 2.3 (1.6-3.31) <.0001
Follow-up by cardiology 1.7 (1.24-2.34) .001
Dyslipidemia 1.72 (1.28-2.3) .0002
Stroke 1.64 (1.02-2.66) .041
Left ventricular hypertrophy 1.51 (1.13-2.03) .0051
History of bronchospasm and
bronchial asthma
0.22 (0.13-0.38) <.0001
Bradycardia 0.28 (0.15-0.54) .0002
COPD 0.39 (0.26-0.6) <.0001
Intermittent claudication 0.35 (0.22-0.57) <.0001
CI, confidence interval; COPD, chronic obstructive pulmonary disease; OR, odds
ratio.
Other variables entered in the model that were not statistically significant: diabetes
mellitus, atrial fibrillation, hypertension, hypotension, heart failure, hepatic failure,
and sex.
80
70
60
50
40
30
20
10
0ACEI
ARBsCCB
Anticoagulant
Antiplatelet
Diuretics
Digoxin
Nitrates
Lipid-lowering drugs
Antidiabetics
Cardiology Internal medicine
Pat
ient
s, %
Figure 3. Other treatments received by the patients in this study. ACEI, angiotensin-converting enzyme inhibitor; ARBs, angitesin receptor blockers; CCB, calciumchannel blocker.
X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890888
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
intermittent claudication); hence, one could infer the opposite:because they had a higher risk profile, internal medicine patientsshould show a greater prevalence of BB treatment than those incardiology. As to the setting in which patients were treated, at
Table 4Evolution of Beta-Blocker Treatment Over the Past 15 Years in Ischemic Heart Dis
PREVESE I13 EUROASPIRE I19,a Programa 3C15 PREVESE
Year 1994 1995 1998 1998
Patients, n 1329 4863 3074 2054
Beta-blockers, % 33.3 53.7 (34.7) 37.4 45.1
a Between parentheses, data for Spain.b Between parentheses, data for ischemic heart disease.
discharge from hospital or on an outpatient basis, this factor had asmaller impact on BB prescription.
It was interesting to note that the reasons for not prescribingBBs differed between cardiology and internal medicine. One of thestated causes, ‘‘unfavorable social situation’’, could be interpretedas an umbrella category that would encompass various conditions.It was found that cardiologists cite COPD more often than internalmedicine specialists as a reason for not prescribing these drugs(38.6% vs 23.3%), whereas internists cite bradycardia more often(30.2% vs 14.2%). Furthermore, it is worthy of note that diabetesmellitus remains a reason for not indicating treatment in 11.6% ofpatients in internal medicine and 6.3% of those in cardiology. Thesedifferences may be explained by the type of disease: COPD istreated more commonly in internal medicine, whereas bradycardiais seen and treated more often in cardiology.
The matter in which there were significant differences betweenthe two specialties was in the percentage of patients for whom BBtreatment was not contemplated: 25.9% in cardiology and 37.4% ininternal medicine, a statistically significant difference on whichefforts should be focussed to improve daily clinical practice.
Multivariate analysis showed various areas in which the BBprescription rate can be improved. A series of variables that havebeen historically related to a ‘‘contraindication’’ for BB treatment(eg, respiratory disease or intermittent claudication) are nowconsidered free of this contraindication (with the exception ofrespiratory disease with a potential for bronchospasm). Anothervariable, age, is a classic in interventional studies. In the present
ease Registries
II16 EUROASPIRE II20,a EUROASPIRE III21,a TRECE22 CARACTER BETAb
1999 2006 2006 2008
5556 8966 2897 1582
63 (47) 80 (60) 64.5 80.4 (85.1)

X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890 889
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
study, it was reaffirmed that as age increased, treatment decreased,in this case BBs, despite the published evidence on BB use inpatients of advanced age.24
The limitations of this study are those inherent to anyobservational registry that does not allow a stratified adjustmentof the patients. Furthermore, there is some selection bias related tononrandomized recruitment of the participating medical specia-lists, as well as a unbalanced representation of acute phase(at discharge) and ambulatory patients included, which coulddetract from the external validity.
CONCLUSIONS
The data from this study show that the BB use for cardiovasculardiseases in which treatment with these drugs is highly recom-mended by scientific societies has improved in Spain with respectto previous registries. Nevertheless, there are still significantdifferences between cardiology and internal medicine, even afteradjusting for the baseline characteristics between patients treatedin these two specialties. The reasons for not prescribing BBs differbetween cardiologists and internal medicine specialists, and thereremains a considerable number of patients in whom the use ofthese drugs is not contemplated even though there is a clearindication, particularly outside the cardiology setting. These data,the first obtained in a nationwide study, show that there is stillroom for improvement in BB prescription in Spain, in particular forpatients with CHF or AF.
FUNDING
This project was funded by an unrestricted grant fromLaboratorios Menarini S.A.
CONFLICTS OF INTERESTS
Antonio Zapata and Remei Artigas are employed in the MedicalDepartment of Menarini, the laboratory that provided an unrest-ricted grant to carry out this study.
APPENDIX A. INVESTIGATORS PARTICIPATING IN THE FIRSTPHASE OF THE CARACTER-BETA STUDY
Carlos Pons de Beristain, Carme Amoros, Mohammad ElsahebDaaboul, Pere Alvarez Garcıa, Josep Pinar Sopena, Nicolas OrtegaLopez, Carlos Lafuente Gormaz, Antonio Castilla Nunez, FermınMartınez Garcıa, Salvador Moreno Honorato, M. Luz Cardo Maeso,Manuel Rayo Gutierrez, Alejandro Berenguel Senen, FernandoLopez Sanchez, Jorge Raul Castro Dorticos, Jesus Saavedra Falero,Oscar Gonzalez Lorenzo, Jose Antonio Nunez Gamero, VilmaMonagas Miller, Veronica Suberviola Sanchez-Caballero, AlbertoChocamo Higueras, Luis Miguel Cuadrado Gomez, FlorentinoGarcıa Gonzalez, Francisco Alonso Montero, Jose Luis AlvarezCuesta, Eddi Velasquez Arias, Jose Carlos Porro Fernandez,Fernando Samaniego Rodrıguez, Jose Marıa Martınez Dıaz, JuanaFreire Corzo, Milagros Pedreira Perez, Jose Enrique Lopez Paz, RosaMarıa Campo Perez, Marıa Bastos Fernandez, M. Dolores MartınezRuiz, Eduardo Caballero Dorta, Egon Gross Kasztovits, EfrenMartınez Quintana, Federico Segura Villalobos, Xavier Garcıa-Moll, Jose Manuel Garcıa Ruiz, Alvaro Gonzalez Franco, MarıaDolores Martın Cid, Jose Sergio Hevia Nava, Vicente BarrialesAlvarez, Gonzalo Marcos Gomez, Sabino Antonio Saez, AndresPerez Garrido, Manuel Maestre Garcıa, Alfredo Luis Michan Dona,Juan Manuel Adriasens Abad, Miguel Angel Rico Corral, Roman
Calvo Jambrina, Gonzalo Baron Esquivias, Juan Andreu Alvarez,Jose Antonio Bernal Bermudez, Marıa Amalia Acuna Lorenzo,Humberto Mendoza Ruiz De Zuazu, Teresa M. Perez Sanz, JoseJavier Moreno Palomares, Luis Marıa Alvarez Gallego, VirginiaMontero Gato, Javier Cabezon Gutierrez, Juan Marıa IrigoyenRodrıguez, Miren Morillas Bueno, Julio Martınez Flores, JavierAndres Novales, Juan Jose Villareal, Angel Brea Yernando, ImadEldin Yousef Hat Hat, Joaquın Canoves Femenia, Antonio ToralNoguera, Juan Quiles Granado, Juan Lujan Martınez, Miguel GarcıaMartınez, Javier Pereira Garcıa-Tizon, Ernesto Ortiz Vecino, JesusGrandes Ibanez, Francisco Alonso Valladares, Jesus Segovia Castro,Manuel Rodrıguez Revuelta, Jaime Fernandez-Duenas Fernandez,Francisco Javier Rivera Guzman, Eduardo Carmona Nimo, MartınRuiz Ortiz, Fernando Olaz Preciado, Juan Marıa Arnedillo Pardo,Juan Perez Calvo, Fidel Sardana Cardiel, Julio Sanchez Alvarez, JorgeParra Ruiz, Jose Luis Ramos Cortes, Hipolito Pousibet Sanfeliu,Carmelo Ruiz Ortiz, Antonio Jesus Martın de la Higuera, Jorge M.Alegret, Guillermo Federico Mazzanti, Pedro Castellanos Llauger,Lluis Carles Olivan Sayrol, Moises Cadierno Carpintero, AgustınArdiaca Capell, Miguel Angel Saanchez-Corral Mena, Ramon deCastro Aritmendiz, Rosa Gilabert Gomez, Vicente Oliver Morena,Julio Nunez Villota, Pau Federico Zaragoza, Pablo Aguar Carrascosa,Araceli Rosello Serralta, Carlos Garcıa Palomar, Lorenzo Facila Rubio,M. Jose Bosch Campos, Pedro Rollan Garcıa, Juan Cosin Sales, RafaelCuenca Luque, Ramon Boixeda Viu, Edgardo Kaplinsky, Julio CarballoGarrido, Joan Sala Montero, Rosa Piulats Egea, Francisco MartıRamon, Carlos Alberto Valle Gort, Julio Jesus Ferrer Hita, MiguelBethencourt Munoz, Angel Montiel Trujillo, Juan Robledo Carmona,Eloy Rueda Calle, Carlos Gomez Navarro, Marıa Guil Garcıa, AlvaroRubio Alcaide, Juana Nunez Morcillo, Joan Torres Marques, JoseMarıa Gamez Martınez, Jose Marıa Turiel Martınez, Ines MollerBustinza, Alberto Riera Garcia, Jose Alonso Gonzalez, FranciscoGonzalez Vilchez, Salvador Diez-Aja Lopez, Santiago CantabranaMiguel, Juana Marıa Gallego Garcıa, Jose Manuel Rubio Campal,Honorio Gervas Pabon, Jorge Oria Vidal, Javier David Romero Roldan.
REFERENCES
1. Villar Alvarez F, Banegas Banegas JR, Rodrıguez Artalejo F, Del Rey Calero J.Mortalidad cardiovascular en Espana y sus comunidades autonomas (1975-1992). Med Clin (Barc). 1998;110:321–7.
2. Anguita Sanchez M, Crespo Leiro MG, De Teresa Galvan E, Jimenez Navarro M,Alonso-Pulpon L, Muniz Garcıa J; on behalf of the PRICE Study Investigators.Prevalencia de la insuficiencia cardiaca en la poblacion general espanola mayorde 45 anos. Estudio PRICE. Rev Esp Cardiol. 2008;61:1041–9.
3. Beaulieu MD, Blais R, Jacques A, Battista RN, Lebeau R, Brophy J. Are patientssuffering from stable angina receiving optimal medical treatment? QJM.2001;94:301–8.
4. Komajda M, Follath F, Swedberg K, Cleland J, Aguilar JC, Cohen-Solal A, et al.;Study Group on Diagnosis of the Working Group on Heart Failure of theEuropean Society of Cardiology. The EuroHeart Failure Survey programme–asurvey on the quality of care among patients with heart failure in Europe. Part 2:treatment. Eur Heart J. 2003;24:464–74.
5. Lopez-Sendon J, Swedberg K, McMurray J, Tamargo J, Maggioni AP, Dargie H,et al.; Task Force on Beta-Blockers of the European Society of Cardiology. Expertconsensus document on beta-adrenergic receptor blockers. Eur Heart J.2004;25:1341–62.
6. Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M, et al.; TaskForce for the Diagnosis and Treatment of Chronic Heart Failure of the EuropeanSociety of Cardiology. Guidelines for the diagnosis and treatment of chronicheart failure: executive summary (update 2005): The Task Force for theDiagnosis and Treatment of Chronic Heart Failure of the European Society ofCardiology. Eur Heart J. 2005;26:1115–40.
7. Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al.ACC/AHA/ESC: Guıa de practica clınica 2006 para el manejo de pacientes confibrilacion auricular. Version resumida. Rev Esp Cardiol. 2006;59:1329.
8. Fox K, Alonso Garcia MA, Ardissino D, Buszman P, Camici PG, Crea F, et al.Guidelines on the management of stable angina pectoris. Executive summary.The Task Force on the Management of Stable Angina Pectoris of the EuropeanSociety of Cardiology. Eur Heart J. 2006;27:1341–81.
9. Beaulieu MD, Brophy J, Jacques A, Blais R, Battista RN, Lebeau R. Physicians’attitudes to the pharmacological treatment of patients with stable anginapectoris. QJM. 2005;98:41–51.

X. Garcia-Moll et al. / Rev Esp Cardiol. 2011;64(10):883–890890
Document downloaded from http://www.revespcardiol.org, day 28/09/2012. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
10. Komajda M, Lapuerta P, Hermans N, Gonzalez-Juanatey JR, Van Veldhuisen DJ,Erdmann E, et al. Adherence to guidelines is a predictor of outcome in chronicheart failure: the MAHLER survey. Eur Heart J. 2005;26:1653–9.
11. Daly C, Clemens F, Lopez Sendon JL, Tavazzi L, Boersma E, Danchin N, et al. Theinitial management of stable angina in Europe, from the Euro heart Survey. EurHeart J. 2005;26:1011–22.
12. Ferreira-Gonzalez I, Permanyer-Miralda C, Marrugat J, Heras M, Cunat J, CiveiraE, et al.; on behalf of the MASK study investigators. Estudio MASCARA (Manejodel Sındrome Coronario Agudo. Registro Actualizado). Resultados globales. RevEsp Cardiol. 2008;61:803–16.
13. De Velasco JA, Cosın J, Lopez-Sendon JL, De Teresa E, De Oya M, Carrasco JL, et al.;on behalf of the PREVESE Study Investigators Group. La prevencion secundariadel infarto de miocardio en Espana. Estudio PREVESE. Rev Esp Cardiol.1997;50:406–15.
14. Cabades A, Lopez-Bescos L, Aros F, Loma-Osorio A, Bosch X, Pabon P, et al.Variabilidad en el manejo y pronostico a corto y medio plazo del infarto agudode miocardio en Espana. El estudio PRIAMHO. Rev Esp Cardiol. 1999;52:767–75.
15. De Velasco JA, Llargues E, Fito R, Sala J, Del Rıo A, De los Arcos E, et al.; on behalfof the Programa de Cuidado Coronario Continuado (3C) Investigators Group.Prevalencia de los factores de riesgo y tratamiento farmacologico al altahospitalaria en el paciente coronario. Resultados de un registro multicentriconacional (Programa 3C). Rev Esp Cardiol. 2001;54:159–68.
16. De Velasco JA, Cosın J, Lopez-Sendon JL, De Teresa E, De Oya M, Sellers G. Nuevosdatos sobre la prevencion secundaria del infarto de miocardio en Espana.Resultados del estudio PREVESE II. Rev Esp Cardiol. 2002;55:801–9.
17. Aros F, Cunat J, Loma-Osorio A, Torrado E, Bosch X, Rodrıguez JJ, et al.; on behalfof the PRIAMHO II Study Investigators. Tratamiento del infarto agudo de
miocardio en Espana en el ano 2000. El estudio PRIAMHO II. Rev Esp Cardiol.2003;56:1165–73.
18. Bueno H, Bardajı A, Fernandez-Ortiz A, Marrugat J, Martı H, Heras M; on behalfof DESCARTES Study Investigators. Manejo del sındrome coronario agudo sinelevacion del segmento ST en Espana. Estudio DESCARTES (Descripcion delEstado de los Sındromes Coronarios Agudos en un Registro Temporal Espanol).Rev Esp Cardiol. 2005;58:244–52.
19. EUROASPIRE Study Group. EUROASPIRE. A European Society of Cardiologysurvey of secondary prevention of coronary heart disease: Principal results.Eur Heart J. 1997;18:1569–82.
20. EUROASPIRE Study Group. Lifestyle and risk factor management and use of drugtherapies in coronary patients from 15 countries. Principal results from EURO-ASPIRE II. Euro Heart Survey Programme. Eur Heart J. 2001;22:554–72.
21. Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U; on behalf ofEUROASPIRE Study Group. EUROASPIRE III: A survey on the lifestyle, risk factorsand use of cardioprotective drug therapies in coronary patients from twentytwo European countries. EUROASPIRE Study Group. Eur J Cardiovasc PrevRehabil. 2009;16:121–37.
22. Bertomeu V, Cordero A, Quiles J, Mazon P, Aznar J, Bueno H. Control de losfactores de riesgo y tratamiento de los pacientes con cardiopatıa isquemica:registro TRECE. Rev Esp Cardiol. 2009;62:807–11.
23. Swedberg K, Komajda M, Bohm M, Borer JS, Ford I, Dubost-Brama A, et al.; SHIFTInvestigators. Ivabradine and outcomes in chronic heart failure (SHIFT): arandomised placebo-controlled study. Lancet. 2010;376:875–85.
24. Flather MD, Shibata MC, Coats AJS, Van Veldhuisen DJ, Parkhomenko A, BorbolaJ, et al.; SENIORS Investigators. Randomized trial to determine the effect ofnebivolol on mortality and cardiovascular hospital admission in elderlypatients with heart failure (SENIORS). Eur Heart J. 2005;26:215–25.
Copyright © 2022 FDOKUMEN