Host defence factors and prognosis in hairy cell leukemia
13
Leukemia Research Vol. 6. No. 5. pp. 625-637. 1982. 0145-2126/82/050625-13503.00/0 Printed in Great Britain. © 1982 Pergamon Press Ltd. HOST DEFENCE FACTORS AND PROGNOSIS IN HAIRY CELL LEUKEMIA EVAN M. HERSH, JORGE QUESADA, MICHAEL J. KEATING, SHELLY RASMUSSEN, SAMUEL G . MURPHY, CHARLES GSCHWIND a n d JOHN MORGAN Department of Clinical Immunology and Biological Therapy, The University of Texas System Cancer Center. M.D. Anderson Hospital and Tumor Institute, Houston, TX 77030, U.S.A. (Received 22 March 1982. Accepted 5 April 1982) -Abstract--Host defence parameters were characterized in 20 patients with hairy cell leukemia {HCL) and were related to hematological, clinical and prognostic variables. The diagnosis was confirmed by examination on the bone marrow by light and electron microscopy, and by staining for tartrate-resistam acid phosphatase. The major findings were markedly impaired delayed type hypersensitivity to recall antigens (mean skin test diameter in ram, HCL: 4.5, acute myelogenous leukemia: 17.4. normal: 14.8); low lymphocyte blastogenic responses to pokeweed mitogen (patients: 2.33 × 103 counts per rain per culture, normals: 15.11 and concanavalin A {patients: 5.3 × 103 counts per min, normals: 31.9); low peripheral blood adherent monocytes (patients: 2.7 × 104/ml, normals: 14.8), low serum lysozyme (patients: 1.8 #g/ml, normals: 5.8) and virtually absent antibody-dependent cellular cytotoxicity ADCC to human erythrocytes {patients: 1.6°,o target cell lysis, normals: 8.7). In vitro addition of allogeneic monocytes restored the pokeweed mitogen and concanavalin A responses in 10 cases. There were significant negative correlations between the extent of bone marrow involvement with leukemia and several host defence par- ameters including ADCC to chicken erythrocytes (p = 0.002), delayed type hypersensitivity (p = 0.005), ADCC to the human leukemia CEM cell line (p = 0.3) and concanavalin A response (p = 0.03). Variables predicting prognosis included serum lysozyme (p = 0.008), ADCC to CEM (p = 0.009), delayed type hypersensitivity (p = 0,03), adherent monocytes (p = 0.04), concanava- lin A response (p = 0.05) and platelet count (p = 0.05). These data indicate the important role of host defence parameters in the course of HCL and indicate the important role of host defence parameters in the course of HCL and indicate pathways for the study of the fundamental nature of the disease and its management. INTRODUCTION HAlaY CELL leukemia (HCL) has been described previously as a heterogeneous, but well defined, clinical entity characterized by leukemic infiltration of the bone marrow, a relatively long clinical course, a poor response to chemotherapy, occasional prolonged clinical improvement after splenectomy [3] and a high incidence of systemic infections [24]. Some of these infections are with unusual organisms such as atypical mycobacteria. This has suggested that there is a major component of host defence failure in this disease [13]. The nature of the leukemic cell has been the subject of considerable debate and indeed the leukemic cells express different surface markers in different patients. However, the typical case shows a leukemic cell with the characteristics of a phagocytic B cell [9]. These cells are readily identified by their content of tartrate-resistant acid phosphatase 1-19] and have a typical electron microscopic picture of multiple hair-like projections from the cell surface [3]. Abbre~'iations: ADCC, antibody-dependent cellular cytotoxicity; Cand, Candida; Con-A, concanavalin A; DTH, delayed type hypersensitivity; Derm, dermatophytin; HCL, hairy cell leukemia; HRBC, human red blood cells: KLH. keyhole limpet hemocyanin: PHA, phytohemagglutinin; PWM, pokeweed mitogen; PPD, purified protein derivative: Var. varidase. 625
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Host defence factors and prognosis in hairy cell leukemia
Leukemia Research Vol. 6. No. 5. pp. 625-637. 1982. 0145-2126/82/050625-13503.00/0 Printed in Great Britain. © 1982 Pergamon Press Ltd.
HOST DEFENCE FACTORS A N D PROGNOSIS IN HAIRY CELL LEUKEMIA
EVAN M. HERSH, JORGE QUESADA, MICHAEL J. KEATING, SHELLY RASMUSSEN, SAMUEL G. MURPHY, CHARLES GSCHWIND and JOHN MORGAN
Department of Clinical Immunology and Biological Therapy, The University of Texas System Cancer Center.
M.D. Anderson Hospital and Tumor Institute, Houston, TX 77030, U.S.A.
(Received 22 March 1982. Accepted 5 April 1982)
-Abstract--Host defence parameters were characterized in 20 patients with hairy cell leukemia {HCL) and were related to hematological, clinical and prognostic variables. The diagnosis was confirmed by examination on the bone marrow by light and electron microscopy, and by staining for tartrate-resistam acid phosphatase. The major findings were markedly impaired delayed type hypersensitivity to recall antigens (mean skin test diameter in ram, HCL: 4.5, acute myelogenous leukemia: 17.4. normal: 14.8); low lymphocyte blastogenic responses to pokeweed mitogen (patients: 2.33 × 103 counts per rain per culture, normals: 15.11 and concanavalin A {patients: 5.3 × 103 counts per min, normals: 31.9); low peripheral blood adherent monocytes (patients: 2.7 × 104/ml, normals: 14.8), low serum lysozyme (patients: 1.8 #g/ml, normals: 5.8) and virtually absent antibody-dependent cellular cytotoxicity ADCC to human erythrocytes {patients: 1.6°,o target cell lysis, normals: 8.7). In vitro addition of allogeneic monocytes restored the pokeweed mitogen and concanavalin A responses in 10 cases. There were significant negative correlations between the extent of bone marrow involvement with leukemia and several host defence par- ameters including ADCC to chicken erythrocytes (p = 0.002), delayed type hypersensitivity (p = 0.005), ADCC to the human leukemia CEM cell line (p = 0.3) and concanavalin A response (p = 0.03). Variables predicting prognosis included serum lysozyme (p = 0.008), ADCC to CEM (p = 0.009), delayed type hypersensitivity (p = 0,03), adherent monocytes (p = 0.04), concanava- lin A response (p = 0.05) and platelet count (p = 0.05). These data indicate the important role of host defence parameters in the course of HCL and indicate the important role of host defence parameters in the course of HCL and indicate pathways for the study of the fundamental nature of the disease and its management.
INTRODUCTION
HAlaY CELL leukemia (HCL) has been described previously as a heterogeneous, but well defined, clinical entity characterized by leukemic infiltration of the bone marrow, a relatively long clinical course, a poor response to chemotherapy, occasional prolonged clinical improvement after splenectomy [3] and a high incidence of systemic infections [24]. Some of these infections are with unusual organisms such as atypical mycobacteria. This has suggested that there is a major component of host defence failure in this disease [13].
The nature of the leukemic cell has been the subject of considerable debate and indeed the leukemic cells express different surface markers in different patients. However, the typical case shows a leukemic cell with the characteristics of a phagocytic B cell [9]. These cells are readily identified by their content of tartrate-resistant acid phosphatase 1-19] and have a typical electron microscopic picture of multiple hair-like projections from the cell surface [3].
Abbre~'iations: ADCC, antibody-dependent cellular cytotoxicity; Cand, Candida; Con-A, concanavalin A; DTH, delayed type hypersensitivity; Derm, dermatophytin; HCL, hairy cell leukemia; HRBC, human red blood cells: KLH. keyhole limpet hemocyanin: PHA, phytohemagglutinin; PWM, pokeweed mitogen; PPD, purified protein derivative: Var. varidase.
625
626 EVAN M. HERSH et al.
The prognosis of the patients seen at the M.D. Anderson Hospital is poor with a median survival of 30 months (Stewart et al., unpublished). Patients who presented with major systemic infection and those who presented at initial diagnosis with a hemoglobin under 10 g had survivals of one and three months respectively.
Increasing attention is being directed to the host defence failure because of the serious nature of the infectious complications. Certainly a component of this can be explained by the granulocytopenia which is characteristic of the disease. The patients also manifest monocytopenia and show a reduced mononuclear phase of the cutaneous inflammatory response as studied by the skin window technique [22]. In addition, variable degrees of deficiency in delayed hypersensitivity [16] and in lymphocyte blastogenic response to phytohemagglutinin (PHA) [21] have been described. We have previously reported two cases of HCL in whom there was a characteristic defect of low serum lysozyme, low monocyte-macrophage precursors in the peripheral blood and absent antibody-depen- dent cellular cytotoxicity (ADCC)to human red blood cells (HRBC) [12]. The latter is a monocyte-mediated function. We also noted low lymphocyte blastogenic responses to pokeweed mitogen (PWM) and concanavalin A (Con-A). These were restored in t'itro by the addition of allogenic monocytes.
In the current study, we extend these observations to a group of 20 patients with HCL. The observed abnormalities in serum lysozyme, monocyte-macrophage precursors, ADCC and HRBC and lymphocyte blastogenic responses to Con-A and PWM are confirmed. The described abnormalities correlated with each other, with the extent of disease and with the prognosis of the patients. The implications of these findings for therapy, and future directions of investigation of host defence abnormalities in HCL are discussed.
MATERIALS AND METHODS
Patients
Twenty patients with the diagnosis of HCL were studied. The diagnosis was made by light and electron microscopic examination of the peripheral blood and bone marrow, and by the presence of cells containing tartrate-resistant acid phosphatase on cytochemical staining. In cases with splenectomy, and in cases that had undergone liver biopsy, histopathological examination of these organs also revealed the presence of HCL infiltration. None of the patients were on therapy when studied.
Therapy after the first visit to M. D. Anderson and the first immunological evaluation consisted of weekly i.v. methanol extraction residue of BCG (MER} plus either allogeneic leukocyte transfusions or lithium carbonate in an attempt to improve marrow granulopoesis in nine patients, prednisone and halotestin in one patient. intermittent anthracyeline therapy in two patients and no therapy in eight patients. Two patients underwent splenectomy after their first host defence evaluation and were subsequently in the no-therapy group. Thirteen other patients had undergone splenectomy prior to the start of evaluation and follow-up.
Laboratory examination Clinical evaluation included complete physical examination, complete blood count, platelet count, bone
marrow aspiration and biopsy, histochemical and electron microscopic examination of the bone marrow, complete clinical chemistries, chest X-ray and liver spleen scan.
Delayed type hypersensitivity (DTH) was measured to the recall antigens dermatophytin lDerm), varidase or streptokinase-streptodornase (Vat), Candida (Cand). mumps and purified protein derivative (PPD), using stan- dard doses as previously described [18]. Primary DTH was measured by the administration of 100tlg of keyhole limpet hemocyanin (KLH) i.d. and testing with this dose two weeks later, as previously described [8]. Delayed hypersensitivity responses were measured in mm as the average of two right-angle diameters of induration at 48 hr after placement of the tests [18]. Hyporesponsiveness was defined as development of DTH to less than two of the battery of antigens. A positive reaction was defined as 5 mm induration or greater.
Leukocyte counts Leukocyte counts were made on peripheral blood smears and on cytocentrifuge preparations stained with
Wright-Giemsa stain. These preparations were also evaluated by phagocytosis of latex particles, Sudan black stain [4] and non-specific esterase stain [26] done on both the whole blood and the FicolI-Hypaque density solution centrifuged mononuclear cells. T cells were determined by the E-rosette method [I]. B cells were

Host defence in hairy cell leukemia 627
determined by fluorescence with 5S rabbit anti-human lgM and 5S rabbit anti-human IgD [25]. One hundred cell differential counts were done on each preparation and the results were recorded as the percentage of cells used to calculate the absolute cell count when appropriate.
Lymphocyte blastooenesis
Lymphocyte blastogeneic responses were measured using the standard microculture system as previously described [17]. Wells contained 1.5 x 105 peripheral blood lymphocytes in 0.2 ml of RPM1 1640 with 20~o normal human AB serum. After 42 or 64 h in culture at 37°C in 5~, CO2 and air, 1/~Ci of [~H]thymidine (sp. act. 1.9 Ci/mmol) was added for 8 h and the cultures were harvested with an automatic cell harvester onto fibreglass filter discs. The incorporated radioactivity was counted in a liquid scintillation counter. Culture sets consisted of triplicates which were not stimulated, and triplicates which were stimulated with PHA, Con-A and PWM as previously described [17]. The mitogens were added in a volume of 0.02 ml per well. The PHA was used as a 1 : 100 dilution of the stock solution from Difco Laboratories. The PWM was used as a 1:20 dilution of the stock from Grand Island Biologicals and the Con-A concentration was 4 ~g/well.
For monocyte restoration of blastogenesis, allogeneic adherent monocytes were used. To collect these, FicolI-Hypaque separated peripheral blood mononuelear cells from normal human subjects were washed three times in Hank's balanced salt solution (HBSS) and were incubated in plastic flasks for 45 rain at 37°C in RPMI 1640 with 1~'o autologous serum. At the end of this culture period, the nonadherent cells were washed off the plastic surface, the adherent cells were released by a 15rain incubation at room temperature with 30mM lidocaine, washed twice in RPM1 1640 and added to the microwells, in triplicate sets, at a concentration of 3 × 104 monocytes per microwell in 0.2 ml of RPMI 1640 with 20~o human AB serum without lymphocytes or with added patient lymphocytes, as described above. All of the allogeneic monocyte-containing cultures were also incubated alone or stimulated with PHA, PWM and Con-A. Incubation, thymidine incorporation, har- vesting, counting and evaluation of the monocyte-containing cultures were carried out as described above. Net counts per min were the counts in the stimulated cultures minus the counts in the appropriate unstimulated controls.
Serum lysozyme Serum lysozyme was determined by using the Worthington Diagnostics Lysozyme Reagent Kit as previously
described [12]. Briefly. the test measures the rate at which a suspension of Micrococcus lysodecticus is lysed. The kit contains a vial of lyophilized substrate and a vial of lysozyme standard which are reconstituted with distilled water. The standard was used to prepare a standard curve for the substrate and all subsequent determinations using the substrate were compared to the curve generated. A volume of 300tA of serum or standard was added to 3 ml of substrate, and absorbance readings at 550 nm were taken after 0.5 and 3 rain. The difference in optical density was computed and the amount of lysozyme present was determined from the standard curve.
Cellular cytotoxicity assays The ADCC assay was carried out as a modification of the method of Poplack et al. [20]. Target erythrocytes
were collected fresh weekly and stored in Alsever's solution• Erythrocytes were labelled after being washed twice in Hank's balanced salt solution. Erythrocytes (2 x l0 ~) were incubated with 100 #Ci of sodium s tchro- mate (51Cr) in 0.3 ml for 40 rain at 37cC. Labelled cells were washed three times in HBSS and diluted appropri- ately. The reaction mixture consisted of 0.1 ml of RPMI 1640 with 5~ fetal calf serum (FCS) plus glutamine and penicillin-streptomycin, and containing l x 105 mononuclear cells (collected by Ficoll-Hypaque density solution centrifugation), 0.1 ml of erythrocyte suspension containing 3 x 10 ~ erythrocytes, and 0.05 ml of anti- serum in a Linbro round bottomed microtitre plate. For chicken erythrocytes (CRBC) the antiserum was a 1 : 800 dilution of a rabbit antiserum made by weekly immunization of rabbits for four weeks. For human type B erythrocytes IHRBC) the antiserum was a l:15 dilution of DADE anti-B antiserum (Dude Company, Miami, FIoridal. For ADCC to the nucleated human T-leukemia cell line (CEM), 5 x l06 washed CEM cells in 0.5 ml of HBSS with 5°o FCS were incubated with 100pCi of 51Cr for 40rain at 37°C. They were then washed three times and used for the ADCC assay. For this assay. 1 x l05 peripheral blood mononuclear cells from the patients and I x 104 labelled cells were mixed with a final 1:1000 dilution of antiserum in a total volume of 0.2 ml and incubated in a Linbro round bottomed microtitre plate. The antiserum used was a rabbit antiserum made by weekly immunization of rabbits with viable CEM cells for three weeks. The l:1000 dilution was selected because it was non-cytolytic without leukocytes and gave a 50~o lysis with the leukocytes of normal donors. For all of the above, triplicate cultures were incubated in a 37~C incubator for 4 h. They were then centrifuged and one half of the culture supernatant was counted for chromium release• Cultures without antibody and total chromium content of the cultures were utilized as controls, and specific lysis was calculated by the following fomula:
Supernatant counts per rain with antibody - supernatant counts per rain without antibody x 100.
Total counts per rain in the culture
Spontaneous cell-mediated cytotoxicity (SCMCI by the natural killer cells was determined using Ficoll- Hypaque separated mononuclear cells and the CEM human T-cell leukemia and the K562 human myeloid leukemia cell lines as the targets [23]. The target cells were labelled with 100/JCi of 51Cr as described above.
628 EvA~ M. HERsn et al.
The effector target cells ratio was 50:1 with 5 × 10 '~ effector mononuclear cells in a total volume of 0.25 ml of RPMI 1640, and l&/o FCS. Incubation time of triplicate cultures was 4h at 37:C. Release of ~Cr and estimation of the percentage specific lysis was calculated as described above.
Peripheral blood adherent monoc)'tes
The assay for adherent monocytes in the peripheral blood was carried out as a modification of the method of Currie and Hedley 17]. Mononuclear leukocytes were collected by Ficoll-Hypaque density solution centrifu- gation. The cells were washed twice with HBSS and resuspended in RPMI 1640 supplemented with penicillin streptomycin and glutamine, The cell suspension was adjusted to 2 x 106 cells per ml and 100,ul were added to the microwells of flat bottomed microculture plates. Also 100/A of autologous serum was added to each well. After 7 days of incubation in a humidified 37~C CO2 atmosphere, all wells were thoroughly washed with HBSS to remove non-attached cells and debris. Then 50/~1 of white cell lysing agent (Scientific Products. McGraw Park, lllinois) were added to each well and incubation was carried out for 30 s. The contents of the wells were then aspirated and the number of released nuclei per well were enumerated using a Coulter counter. The number of adherent monocytes per ml of blood was then calculated.
Statistical methods
Patients' immunological data were compared to normal control subjects' immunological data by Stud6nt's t-test and the chi-square test 1,14]. Blastogenic responses to mitogens and the restorative effect of allogeneic monocytes on blastogenic responses were evaluated by comparing appropriate replicate sets by Student's t-test.
Correlations between pairs of variables were determined by examining plots of the data and correlation coefficients 114]. The Mann-Whitney test [14] was used to compare values of a variable between pairs of patient subgroups. For example, patients who had died were compared with patients who had not died with respect to a number of laboratory and immunological parameters. Survival curves were calculated and plotted using the technique of Kaplan and Meier 115]. Survival curves for different patient subgroups were compared using a generalized Wilcoxon test [10] and a two-tailed p value. A logistic regression analysis [5] was used to relate laboratory and immunological parameters to prognosis. Good prognosis patients were defined as those with stable disease or better following treatment. Poor prognosis patients were defined as those who developed progressive disease or who died. Cox's regression model 1,61 was used to relate laboratory and immunological parameters to survival.
R E S U L T S
The pa t ien t s had a m e d i a n age o f 54 years r ang ing from 24 to 70. On ly three pa t ien ts were unde r age 40. All o f the pa t i en t s were male. Th i r t een o f the pa t ien t s had prev ious ly u n d e r g o n e sp l enec tomy before referral to M.D. A n d e r s o n H o s p i t a l and two underwent s p l e n e c t o m y after their first visit and hos t defence eva lua t ion . O n l y five of the 15 splenec- t omized pa t ien ts had any benefi t f rom s p l e n e c t o m y in t e rms o f increased g ranu locy te or p la te le t counts . Six of the pa t ien ts had m a j o r infect ions at the t ime of first admis s ion to M.D. A n d e r s o n Hosp i t a l . O n l y two o f those failed_ to recover f rom their infect ion and
d ied du r ing the first hosp i ta l admiss ion . A to ta l o f five o f the s tudy subjects have d ied and 15 r ema in alive.
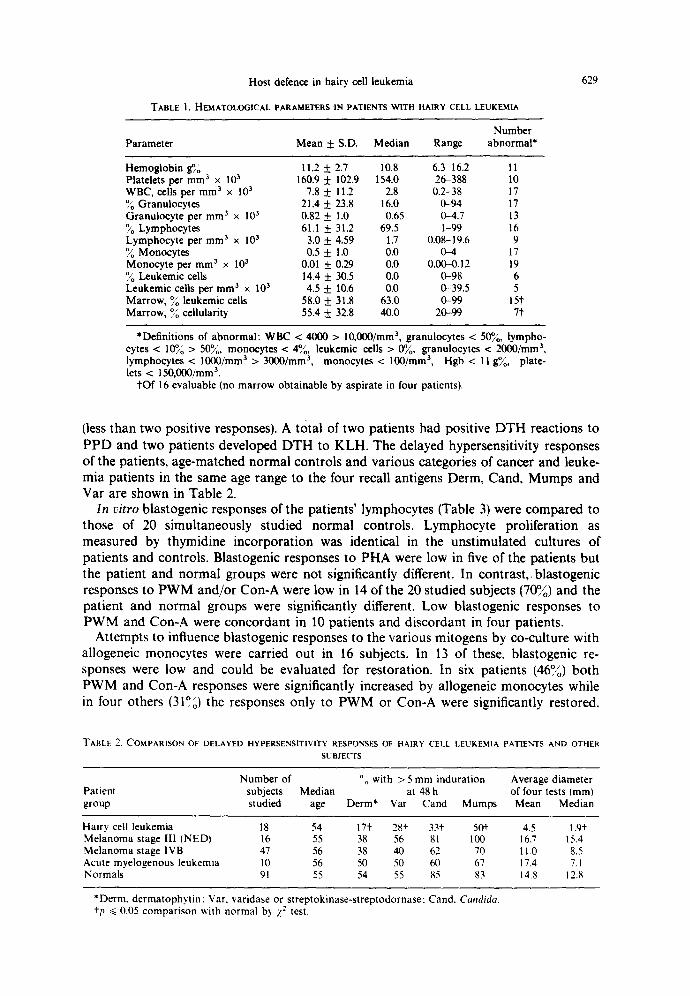
The hema to log i ca l charac te r i s t i cs of the pa t ien ts a re given in Tab le 1 (means, med ian values and ranges). The m e a n whi te coun t was 7800/ram 3 with 21.4°o polys, 61.1°,o lymphocy te s , 0.5% m o n o c y t e s and 14.3°,o l eukemic cells. However , 17 pa t ien ts had white coun t s be low 4000 and 13 pa t ien ts had abso lu t e g ranu locy te counts be low 1000. O n l y five pa t ien ts had l eukemic cells de tec tab le in the pe r iphe ra l b lood . The mean he mog lob in was 11.2 g~o and the mean p la te le t coun t was 160,000/mm 3. Seven pa t ien t s had pla te le t coun t s be low 100,000 and th ree had pla te le t coun t s be low 50,000. The m a r r o w cel lu lar i ty ave raged 559/00 with 58~o leukemic cells. However , no m a r r o w could be o b t a i n e d by a sp i r a t i on in four of the 20 cases (dry tap).
H a l f o f the pa t ien ts had an e levated a lka l ine p h o s p h a t a s e (greater than 85 i.u.) and it was over 250i .u . in four of the pat ients . Otherwise , b l o o d chemis t r ies were essent ia l ly normal .
De layed hypersens i t iv i ty was eva lua ted in 18 of the 20 pa t ien ts and found to be s ignif icant ly d imin i shed . F ive pa t ien ts were a l lergic to al l the recall ant igens. Three a d d i t i o n a l pa t ien ts reac ted on ly to the m u m p s ant igen and two a dd i t i ona l pa t ien ts reac ted only to P P D . Thus, I0 ou t of 18 or (55.5%) o f the subjects were hyporespons ive
Host defence in hairy cell leukemia
TABLE 1. HEMATOLOGICAL PARAMETERS IN PATIENTS WITH HAIRY CELL LEUKEMIA
629
Number Parameter Mean 4- S.D. Median Range abnormal*
Hemoglobin g~g 11.2 4- 2.7 10.8 6.3-16.2 11 Platelets per m m 3 x 103 160.9 4- 102.9 154.0 26-388 10 WBC, cells per m m 3 x 103 7.8 4- 11.2 2.8 0.2-38 17 o/ Granulocytes 21.4 + 23.8 16.0 0-94 17 Granulocyte per m m 3 × 103 0.82 + 1.0 0.65 0-4.7 13 °1,o Lymphocytes 61.1 _+ 31.2 69.5 1-99 16 Lymphocyte per mm 3 x 103 3.0 + 4.59 1.7 0.08-19.6 9 o~/o Monocytes 0.5 _+ 1.0 0.0 0-4 17 Monocyte per m m 3 x 10 a 0.01 4- 0.29 0.0 0.00-0.12 19 ~o Leukemic cells 14.4 + 30.5 0.0 0-98 6 Leukemic cells per m m 3 x 103 4.5 4- 10.6 0.0 0-39.5 5 Marrow, ~o leukemic cells 58.0 + 31.8 63.0 0-99 15"t Marrow, ~o cellularity 55.4 + 32.8 40.0 20-99 7"t"
*Definitions of abnormal: WBC < 4000 > lO,O00/mm 3, granulocytes < 50%, lympho- cytes < 10~/o > 50~0, monocytes < 4Yo, leukemic cells > 0%, granulocytes < 2000/ram a, lymphocytes < 1000/mm 3 > 3000/mm 3, monocytes < 100/mm 3, Hgb < 11 gYo, plate- lets < 150,000/mm 3.
"tOf 16 evaluable (no marrow obtainable by aspirate in four patients).
(less than two positive responses). A total of two patients had positive DTH reactions to PPD and two patients developed DTH to KLH. The delayed hypersensitivity responses of the patients, age-matched normal controls and various categories of cancer and leuke- mia patients in the same age range to the four recall antigens Derm, Cand, Mumps and Var are shown in Table 2.
In vitro blastogenic responses of the patients' lymphocytes (Table 3) were compared to those of 20 simultaneously studied normal controls. Lymphocyte proliferation as measured by thymidine incorporation was identical in the unstimulated cultures of patients and controls. Blastogenic responses to PHA were low in five of the patients but the patient and normal groups were not significantly different. In contrast,, blastogenic responses to PWM and/or Con-A were low in 14 of the 20 studied subjects (70~o) and the patient and normal groups were significantly different. Low blastogenic responses to PWM and Con-A were concordant in 10 patients and discordant in four patients.
Attempts to influence blastogenic responses to the various mitogens by co-culture with allogeneic monocytes were carried out in 16 subjects. In 13 of these, blastogenic re- sponses were low and could be evaluated for restoration. In six patients (46%) both PWM and Con-A responses were significantly increased by allogeneic monocytes while in four others (31°~,) the responses only to PWM or Con-A were significantly restored.
TABLE 2, COMPARISON OF DELAYED HYPERSENSITIVITY RESPONSES OF HAIRY CELL LEUKEMIA PATIENTS AND OTHER
SUBJECTS
Number of Oo with > 5 mm induration Average diameter Patient subjects Median at 48 h of four tests (ram) group studied age Derm* Var Cand Mumps Mean Median
Hairy cell leukemia 18 54 17"I 28"i 33.1. 50+ 4.5 1.9"i Melanoma stage II1 (NEDt 16 55 38 56 81 100 16.7 15.4 Melanoma stage IVB 47 56 38 40 62 70 11.0 8.5 Acute myelogenous leukemia 10 56 50 50 60 67 17.4 7.1 Normals 91 55 54 55 85 83 14.8 12.8
*Derm. dermatophyt in : Var. varidase or streptokinase-streptodornase: Cand. Capldida. +p ~< 0.05 comparison ~vith normal by Z" test.
630 EVAN M. HERSH et al.
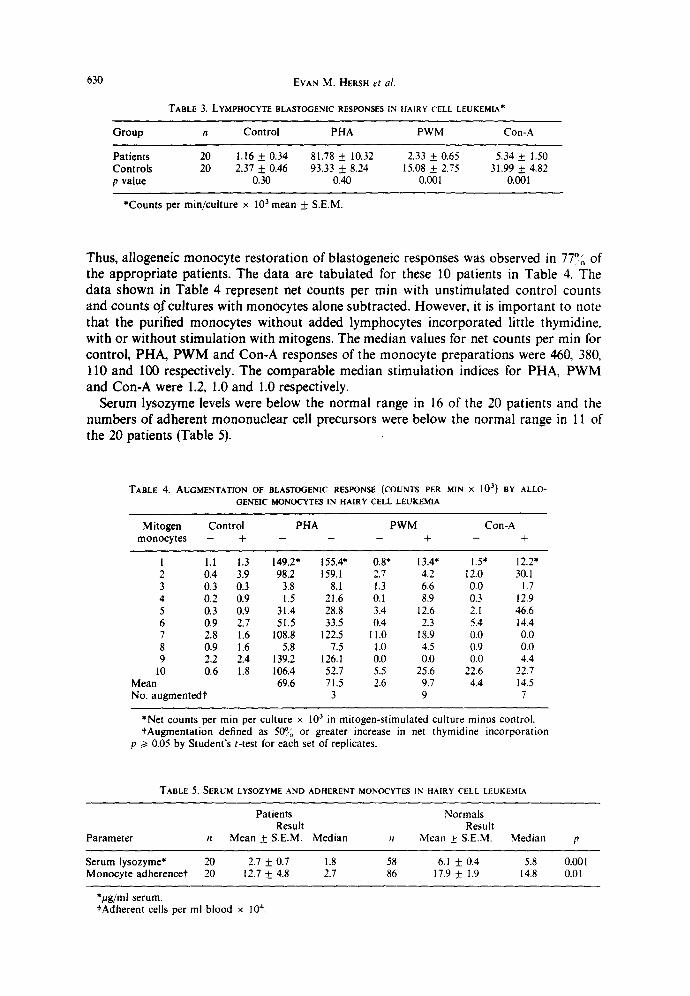
TABLE 3, LYMPHOCYTE BLASTOGENIC RESPONSES IN HAIRY CELL LEUKEMIA*
Group n Control PHA PWM Con-A
Patients 20 1.16 + 0.34 81.78 + 10.32 2.33 + 0.65 5.34 _+ 1.50 Controls 20 2.37 _+ 0.46 93.33 4- 8.24 15.08 + 2.75 31.99 + 4.82 p value 0.30 0.40 0.001 0.001
*Counts per rain/culture × 103 mean ~ S.E.M.
Thus, allogeneic monocyte restoration of blastogeneic responses was observed in 77°0 of the appropriate patients. The data are tabulated for these 10 patients in Table 4. The data shown in Table 4 represent net counts per min with unstimulated control counts and counts qfcultures with monocytes alone subtracted. However, it is important to note that the purified monocytes without added lymphocytes incorporated little thymidine. with or without stimulation with mitogens. The median values for net counts per min for control, PHA, PWM and Con-A responses of the monocyte preparations were 460, 380, 110 and 100 respectively. The comparable median stimulation indices for PHA, PWM and Con-A were 1.2, 1.0 and 1.0 respectively.
Serum lysozyme levels were below the normal range in 16 of the 20 patients and the numbers of adherent mononuclear cell precursors were below the normal range in 11 of the 20 patients (Table 5).
TABLE 4. AUGMENTATION OF BLASTOGENIC RESPONSE (COUNTS PER MINx 10 3) BY ALLO- GENEIC MONOCYTES IN HAIRY CELL LEUKEMIA
Mitogen Control PHA PWM Con-A monocytes - + - + - + - +
1 l.l 1.3 149.2" 155.4" 0.8* 13.4" 1.5" 12.2" 2 0.4 3.9 98.2 159.1 2.7 4.2 12.0 30. l 3 0.3 0.3 3.8 8.1 1.3 6.6 0.0 1.7 4 0.2 0.9 1.5 21.6 0.l 8.9 0.3 12.9 5 0.3 0.9 31.4 28.8 3.4 12.6 2.1 46.6 6 0.9 2.7 .51.5 33.5 0.4 2.3 5.4 14.4 7 2.8 1.6 108.8 122.5 I 1.0 18.9 0.0 0.0 8 0.9 1.6 5.8 7.5 1.0 4.5 0.9 0.0 9 2.2 2.4 139.2 126.1 0.0 0.0 0.0 4.4
10 0.6 1.8 106.4 52.7 5.5 25.6 22.6 22.7 Mean 69.6 71.5 2.6 9.7 4.4 14.5 No. augmentedt 3 9 7
*Net counts per min per culture x 103 in mitogen-stimulated culture minus control. tAugmentation defined as 5~Y/o or greater increase in net thymidine incorporation
p /> 0.05 by Student's t-test for each set of replicates.
TABLE 5. SERUM LYSOZYME AND ADHERENT MONOCYTES IN HAIRY CELL LEUKEMIA
Patients Normals Result Result
Parameter , Mean _+ S.E.M. Median n Mean _+ S.E.M. Median p
Serum lysozyme* 20 2.7 4- 0.7 1.8 58 6.1 _ 0.4 5.8 0.001 Monocyte adherencet 20 12.7 + 4.8 2.7 86 17.9 + 1.9 14.8 0.0l
*itg/ml serum. tAdherent cells per ml blood x 104.
Host defence in hairy cell leukemia
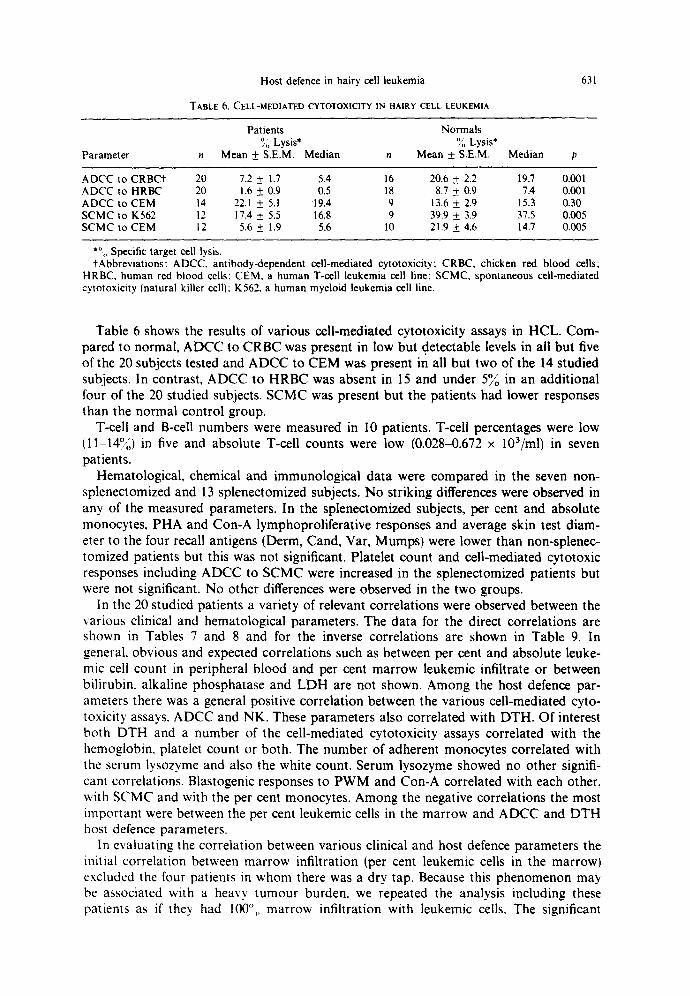
TABLE 6. CELL-MEDIATED CYTOTOXIC1TY IN HAIRY CELL LEUKEMIA
631
Patients Normals )~, Lysis* ~, Lysis*
Parameter n Mean + S.E.M. Median n Mean +_ S.E.M. Median p
ADCC to CRBC't 20 7.2 + 1.7 5.4 16 20.6 + 2.2 19.7 0.001 ADCC to HRBC 20 1.6 + 0.9 0.5 18 8.7 + 0.9 7.4 0.001 ADCC to CEM 14 22.1 + 5.1 19.4 9 13.6 + 2.9 15.3 0.30 S C M C to K562 12 17.4 + 5.5 16.8 9 39.9 -!-_ 3.9 37.5 0.005 SCMC to CEM 12 5.6 + 1.9 5.6 10 21.9 + 4.6 14.7 0.005
. o Specific target cell lysis. tAbbrevia t ions : ADCC. ant ibody-dependent cell-mediated cytotoxicity; CRBC, chicken red blood cells;
HRBC, h u m a n red blood cells: CEM, a h u m a n T-cell leukemia cell line; SCMC, spontaneous cell-mediated cytotoxicity (natural killer cell); K562, a h u m a n myeloid leukemia cell line.
Table 6 shows the results of various cell-mediated cytotoxicity assays in HCL. Com- pared to normal, ADCC to CRBC was present in low but detectable levels in all but five of the 20 subjects tested and ADCC to CEM was present in all but two of the 14 studied subjects. In contrast, ADCC to HRBC was absent in 15 and under 5~o in an additional four of the 20 studied subjects, SCMC was present but the patients had lower responses than the normal control group.
T-cell and B-cell numbers were measured in I0 patients. T-cell percentages were low (1 oj 1-14. o) in five and absolute T-cell counts were low (0.028-0.672 x 103/ml) in seven patients.
Hematological, chemical and immunological data were compared in the seven non- splenectomized and 13 splenectomized subjects. No striking differences were observed in any of the measured parameters. In the splenectomized subjects, per cent and absolute monocytes, PHA and Con-A lymphoproliferative responses and average skin test diam- eter to the four recall antigens (Derm, Cand, Var, Mumps) were lower than non-splenec- tomized patients but this was not significant. Platelet count and cell-mediated cytotoxic responses including ADCC to SCMC were increased in the splenectomized patients but were not significant. No other differences were observed in the two groups.
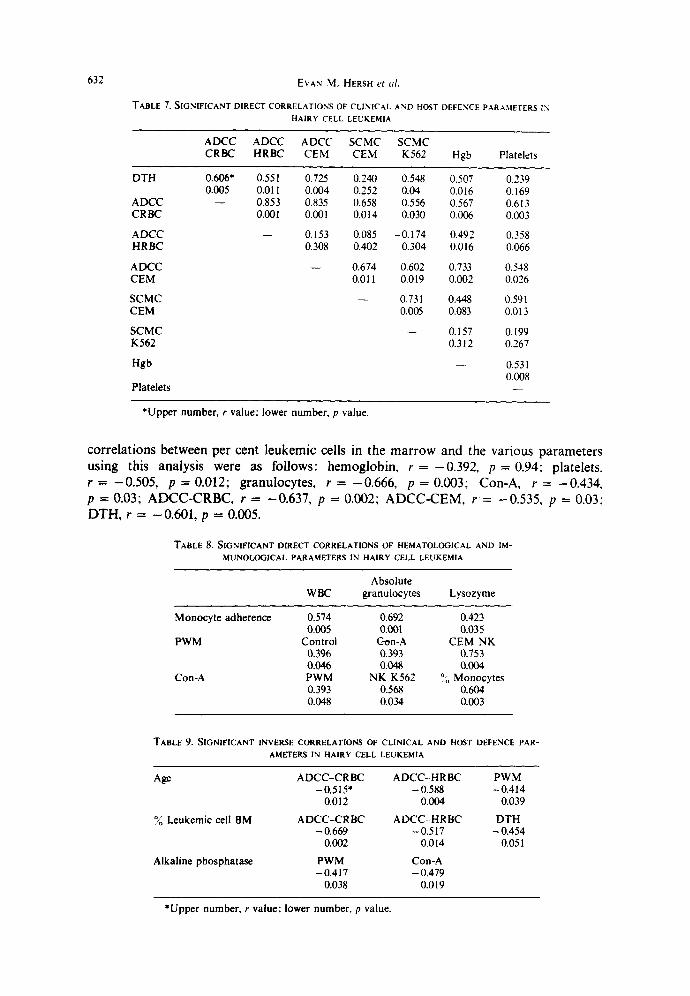
In the 20 studied patients a variety of relevant correlations were observed between the various clinical and hematological parameters. The data for the direct correlations are shown in Tables 7 and 8 and for the inverse correlations are shown in Table 9. In general, obvious and expected correlations such as between per cent and absolute leuke- mic cell count in peripheral blood and per cent marrow leukemic infiltrate or between bilirubin, alkaline phosphatase and LDH are not shown. Among the host defence par- ameters there was a general positive correlation between the various cell-mediated cyto- toxicity assays, ADCC and NK. These parameters also correlated with DTH. Of interest both DTH and a number of the cell-mediated cytotoxicity assays correlated with the hemoglobin, platelet count or both. The number of adherent monocytes correlated with the serum lysozyme and also the white count. Serum iysozyme showed no other signifi- cant correlations. Blastogenic responses to PWM and Con-A correlated with each other, with SCMC and with the per cent monocytes. Among the negative correlations the most important were between the per cent leukemic cells in the marrow and ADCC and DTH host defence parameters.
In evaluating the correlation between various clinical and host defence parameters the initial correlation between marrow infiltration (per cent leukemic cells in the marrow) excluded the four patients in whom there was a dry tap. Because this phenomenon may be associated with a heavy tumour burden, we repeated the analysis including these patients as if they had 100°,, marrow infiltration with leukemic cells. The significant
632 EVAN M. HERSH et al.
TABLE 7. SIGNIFICANT DIRECT CORRELATION'S OF CLINICAL AND HOST DEFENCE PARAMETERS IN HAIRY CELL LEUKEMIA
ADCC ADCC ADCC SCMC SCMC CRBC HRBC CEM CEM K562 Hgb Platelets
DTH 0,606* 0,551 0.725 0.240 0.548 0.507 0.239 0.005 0.011 0,004 0.252 0.04 0.016 0,169
ADCC - - 0.853 0,835 0.658 0.556 0.567 0,613 CRBC 0.001 0.001 0.014 0.030 0.006 0,003
ADCC - - 0.153 0.085 -0.174 0.492 0.358 HRBC 0.308 0.402 0.304 0.016 0.066
ADCC - - 0.674 0.602 0.733 0,548 CEM 0.011 0.019 0.002 0.026
SCMC - - 0.731 0.448 0.591 CEM 0.005 0.083 0.013
SCMC - - 0,157 0.199 K562 0.312 0.267
Hgb - - 0.531 0.008
Platelets
*Upper number, r value; lower number, p value.
correlations between per cent leukemic cells in the marrow and the various parameters using this analysis were as follows: hemoglobin, r = - 0 . 3 9 2 , p = 0.94; platelets, r = - 0 . 5 0 5 , p = 0.012; granulocytes, r = - 0 . 6 6 6 , p =0 .003; Con-A, r = - 0 . 4 3 4 , p = 0.03; ADCC-CRBC, r = -0.637, p = 0.002; ADCC-CEM, r = -0.535, p = 0.03; DTH, r = -0.601, p = 0.005.
TABLE 8. SIGNIFICANT DIRECT CORRELATIONS OF HEMATOLOGICAL AND IM- MUNOLOGICAL PARAMETERS IN HAIRY CELL LEUKEMIA
Absolute WBC granulocytes Lysozyme
Monocyte adherence 0.574 0.692 0.423 0.005 0.001 0.035
PWM Control C~on-A CEM NK 0.396 0.393 0.753 0.046 0.048 0.004
Con-A PWM NK K562 ° o Monocytes 0.393 0.568 0.604 0.048 0.034 0,003
TABLE 9. SIGNIFICANT INVERSE CORRELATIONS OF CLINICAL AND HO~T DEFENCE PAR- AMETERS IN HAIRY CELL LEUKEMIA
Age ADCC-CRBC ADCC-HRBC -0.515" -0.588
0.012 0.004
% Leukemic cell BM ADCC-CRBC ADCC H R B C -0.669 -0.517
0.002 0.014
Alkaline phosphatase PWM Con-A -0.417 -0.479
0.038 0.019
PWM - 0.414
0.039
DTH - 0.454
0,051
*Upper number, r value: lower number, p value.
Host defence in hairy cell leukemia
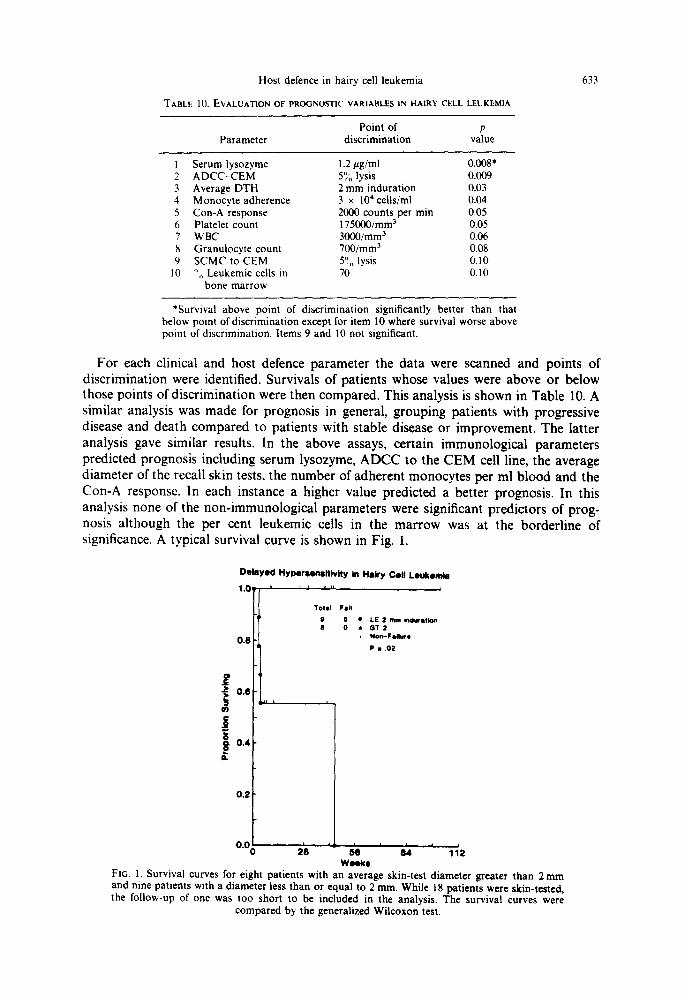
"I'ABLE 10. EVALUATION OF PROGNOSTIC VARIABLES IN HAIRY CELL LEUKEMIA
633
Point of p Parameter discrimination value
1 Serum lysozyme 1.2/ag/ml 0.008* 2 A D C C - C E M 5°/0 lysis 0.009 3 Average DTH 2 m m indurat ion 0.03 4 Monocyte adherence 3 x 10' cells/ml 0.04 5 Con-A response 2000 counts per rain 0.05 6 Platelet count 175000/mm 3 0.05 7 WBC 3000/mm 3 0.06 8 Granulocyte count 700/mm 3 0.08 9 S C M C to CEM 5°. lysis 0.10
10 0,, Leukemic cells in 70 0.10 bone marrow
*Survival above point of discrimination significantly better than that below point of discrimination except for item 10 where survival worse above point of discrimination. Items 9 and 10 not significant.
For each clinical and host defence parameter the data were scanned and points of discrimination were identified. Survivals of patients whose values were above or below those points of discrimination were then compared. This analysis is shown in Table 10. A similar analysis was made for prognosis in general, grouping patients with progressive disease and death compared to patients with stable disease or improvement. The latter analysis gave similar results. In the above assays, certain immunological parameters predicted prognosis including serum lysozyme, ADCC to the CEM cell line, the average diameter of the recall skin tests, the number of adherent monocytes per ml blood and the Con-A response. In each instance a higher value predicted a better prognosis. In this analysis none of the non-immunological parameters were significant predictors of prog- nosis although the per cent leukemic cells in the marrow was at the borderline of significance. A typical survival curve is shown in Fig. 1.
Delayed Hyl)ersenaitivtty in Hairy Coil Leukemia
1"(~ it'l t *l I I II II I 0.8
0"1
~ 0.4
0.2
0.0
T O t a l F l l i l
9 5 • LE 2 mm |hm~'st~on 8 0 • GT 2 i N o n . - F l i i l u r e
P : .02
~'8 ie ' ~ ' , h Wicks
FIG. 1. Survival curves for eight patients with an average skin-test diameter greater than 2 m m and nine patients with a diameter less than or equal to 2 ram. While 18 patients were skin-tested, the follow-up of one was too short to be included in the analysis. The survival curves were
compared by the generalized Wilcoxon test.
634 EVAN M. HERSH et al.
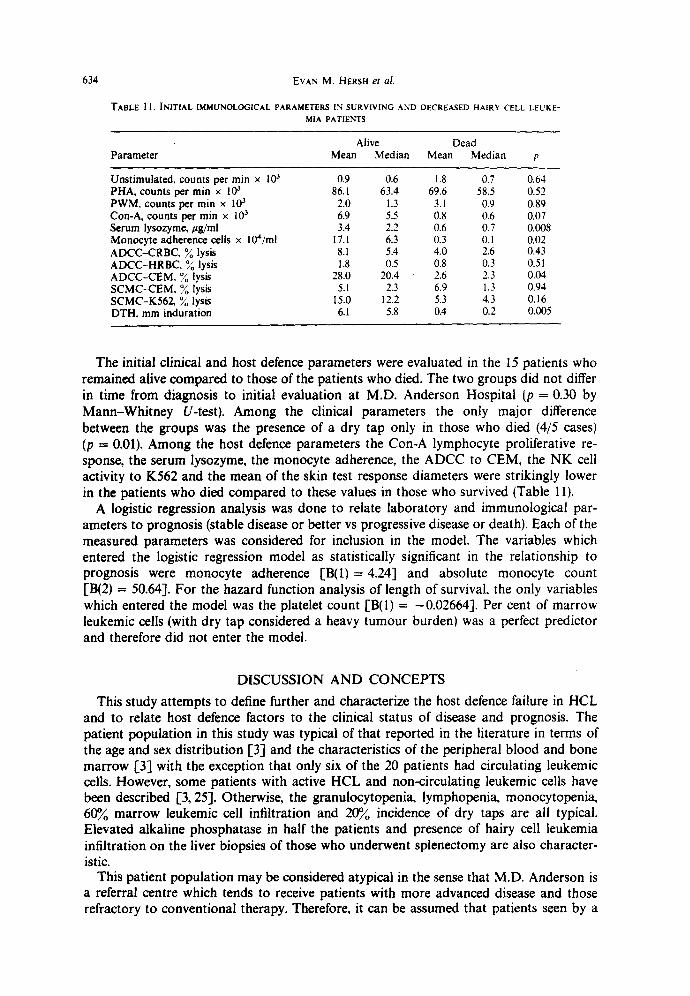
TABLE 1 1. INITIAL IMMUNOLOGICAL PARAMETERS IN SURVIVING AND DECREASED HAIRY CELL LEUKE- MIA PATIENTS
Alive Dead Parameter Mean Median Mean Median p
Unstimulated, counts per m i n x 103 0.9 0.6 1.8 0.7 0.64 PHA, counts per min x 103 86.1 63.4 69.6 58.5 0.52 PWM, counts per rain x 10 J 2.0 1.3 3.1 0.9 0,89 Con-A, counts per rain x 103 6.9 5.5 0.8 0.6 0.07 Serum lysozyme, gg/ml 3.4 2.2 0.6 0. 7 0.008 Monoeyte adherence cells x 104/ml 17.1 6.3 0.3 0.1 0.02 ADCC-CRBC. ~g lysis 8.1 5.4 4.0 2.6 0.43 ADCC-HRBC, ~ lysis 1.8 0.5 0.8 0.3 0.51 ADCC-CEM, o//o lysis 28.0 20.4 2.6 2.3 0.04 SCMC-CEM, ~o lysis 5.1 2.3 6.9 1.3 0.94 SCMC-K562, ~o lysis 15.0 12.2 5.3 4.3 0.16 DTH. mm induration 6.1 5.8 0.4 0.2 0.005
The initial clinical and host defence parameters were evaluated in the 15 patients who remained alive compared to those of the patients who died. The two groups did not differ in time from diagnosis to initial evaluation at M.D. Anderson Hospital (p = 0.30 by Mann-Whitney U-test). Among the clinical parameters the only major difference between the groups was the presence of a dry tap only in those who died (4/5 cases) (p = 0.01). Among the host defence parameters the Con-A lymphocyte proliferative re- sponse, the serum lysozyme, the monocyte adherence, the ADCC to CEM, the NK cell activity to K562 and the mean of the skin test response diameters were strikingly lower in the patients who died compared to these values in those who survived (Table 11).
A logistic regression analysis was done to relate laboratory and immunological par- ameters to prognosis (stable disease or better vs progressive disease or death). Each of the measured parameters was considered for inclusion in the model. The variables which entered the logistic regression model as statistically significant in the relationship to prognosis were monocyte adherence [B(1)= 4.24] and absolute monocyte count [B(2) = 50.64]. For the hazard function analysis of length of survival, the only variables which entered the model was the platelet count [B(I) = -0.02664]. Per cent of marrow leukemic cells (with dry tap considered a heavy tumour burden) was a perfect predictor and therefore did not enter the model.
DISCUSSION AND CONCEPTS
This study attempts to define further and characterize the host defence failure in HCL and to relate host defence factors to the clinical status of disease and prognosis. The patient population in this study was typical of that reported in the literature in terms of the age and sex distribution [3] and the characteristics of the peripheral blood and bone marrow I'3] with the exception that only six of the 20 patients had circulating leukemic cells. However, some patients with active HCL and non-circulating leukemic cells have been described 1'3, 25]. Otherwise, the granulocytopenia, lymphopenia, monocytopenia, 60% marrow leukemic cell infiltration and 20% incidence of dry taps are all typical. Elevated alkaline phosphatase in half the patients and presence of hairy cell leukemia infiltration on the liver biopsies of those who underwent splenectomy are also character- istic.
This patient population may be considered atypical in the sense that M.D. Anderson is a referral centre which tends to receive patients with more advanced disease and those refractory to conventional therapy. Therefore, it can be assumed that patients seen by a
Host defence in hairy cell leukemia 635
hematologist and subjected to a splenectomy, who entered a complete or partial remis- sion or who stabilized with good counts, would be less likely to be referred than those with progress disease. In this regard, 13 patients had undergone splenectomy prior to their first evaluation. However, comparison of the splenectomized and non-splenecto- mized patients in terms of hematological, chemical and immunological data revealed no striking differences. Indeed, the only trends we noted involved the per cent and absolute monocytes counts, the PHA and Con-A responses, and the average skin test diameter, and these were not significant. These were depressed in the splenectomized compared to the non-splenectomized subjects. Two additional patients underwent splenectomy after their initial evaluation. It is of interest that only five of the 15 splenectomized patients showed any hematological or clinical improvement after splenectomy.
In our initial study of two patients with hairy cell leukemia [12], a spectrum of immunological and host defence parameter abnormalities were identified, including im- paired delayed hypersensitivity to recall antigens, low PWM and Con-A lymphocyte blastogenic responses, low serum lysozyme, a low number of adherent monocytes in the peripheral blood and a selective deficiency in ADCC to HRBC with preservation of measurable reactivity of ADCC to CRBC.
In this study of 20 patients with hairy cell leukemia, these observations have been confirmed. Thus, HCL patients had more depressed delayed hypersensitivity than age- matched patients with stage IVB melanoma, or acute myelogenous leukemia. PWM and Con-A responses were significantly depressed. Serum lysozyme, monocyte adherence and ADCC to HRBC were also significantly lower than normal controls. In addition to ADCC to CRBC, we also measured ADCC to nucleated human cells, namely the CEM cell line, and found this to be normal. SCMC cell activity to the K562 and to the CEM cell lines were present but low. These two cell lines were utilized because one is sensitive and the other relatively resistant to lysis by NK cells. In addition, the per cent and absolute T cells were measured in 10 of the 20 patients and were found to be profoundly depressed in six.
The other important finding in our initial report of two patients was that the deficiency in response to PWM and Con-A was corrected by culturing the patients' leukocytes in the presence of normal allogeneic adherence monocytes. In the current study, this was evaluable in 13 patients who had depressed PWM or Con-A responses. Restoration of both responses was seen in six of the patients and of one or the other in an additional four patients. Thus, we have confirmed the fact that the deficient responses to PWM and Con-A are caused by a deficiency in monocytes and can be restored by the addition of adherent cells. This suggests that the administration of allogeneic monocytes or stimu- lation of monocytes production in the patients' marrow might improve their immune reactivity as well as other aspects of the disease.
The low level of serum lysozyme, reduced number of circulating adherent monocytes, virtually absent ADCC activity to the HRBC target, and low PWM and Con-A re- sponses can all be explained by reduced numbers of monocytes. Whether the function of the remaining monocytes is normal is uninvestigated at present. Presumably the low monocytes relate to impaired bone marrow production of these cells although increased utilization, shortened circulation half-life or sequestration has not been ruled out. It is harder to explain why these patients manifest lymphopenia, T- and B-cell deficiency and impaired SCMC cell activity. Whether this represents a failure of the marrow to produce adequate numbers of lymphocyte precursors, whether bone marrow produced monocytes are necessary for the production of adequate numbers of lymphocytes is not known. It is also possible that shortened half-life or sequestration explains this finding.
It was of interest to investigate correlations between the various clinical parameters, correlations between the various immunological parameters and correlations between the
636 EVAN M. HERSH et al.
clinical and immunological parameters. Among the clinical parameters, age correlated inversely with ADCC activity. This is the reverse of what we have previously observed in patients with cancer and other types of leukemia [11]. Age and ADCC activity correlated directly in that study. Manifestations of the effects of the tumour cell burden including the per cent leukemic cells in the bone marrow and the serum alkaline phosphatase (presumably reflecting liver involvement) correlated inversely with ADCC, average delayed hypersensitivity response and with lymphocyte proliferative responses to PWM and Con-A. These presumably reflect either an indirect effect of the tumour burden mediated by soluble factors as well as an effect mediated by the deficiency of monocytes.
There was a strong direct correlation between delayed hypersensitivity and the various ceU-mediated cytotoxicity parameters and interestingly between these parameters and the hemoglobin and the platelet count. The reason for this latter correlation is not clear at this time, but may relate to the common denominator of the tumour burden.
As noted above, four patients had dry taps and the per cent leukemic cells in the bone marrow could not be evaluated. However, since dry taps probably relate to an extensive tumour burden and a packed bone marrow, correlations were also done based on the assumption, there was a strong inverse correlation between the per cent leukemic cells in the marrow and hematological parameters including hemoglobin, platelet and granulo- cyte counts and immunological parameters including Con-A response, ADCC responses and delayed hypersensitivity.
The relationship of the clinical and immunological parameters to prognosis was evalu- ated in three ways. First, by scanning the ranked data, points of discrimination were identified and the prognosis of patients whose values fall above and below these points of discrimination were compared. Each variable was evaluated independently. With this analysis, the most important prognostic variables were the serum lysozyme level, the ADCC to CEM, the average diameter of the delayed hypersensitivity reactions to the skin-test antigens, the monocyte adherence, the Con-A response and the marrow per cent leukemic cells. None of the other clinical or host defence variables predicted prognosis. The second approach was to compare the initial clinical and immunological parameters between the 15 patients who survived and the five patients who died. Important in this analysis was that the time from diagnosis to first immunological study was the same for the two groups. By this analysis, the most important prognostic variables for survival were the average delayed hypersensitivity response to the six antigens, the serum lyso- zyme, the per cent leukemic cells in the bone marrow, the per cent peripheral blood lymphocytes, the monocyte adherence and the ADCC to CEM. In the third approach, logistic regression analyses were done to relate laboratory and immunological par- ameters to prognosis. The important prognostic variables appeared to be the absolute monocyte count, monocyte adherence and platelet count. However, logistic regression analyses must be interpreted with caution, because of the small number of patients, because only three patients had a partial remission and because only five patients expired.
Overall, important prognostic factors relating to host defence have been identified in a disease in which infection is a major cause of death. This offers the potential for an attempt to improve these host defence factors as a major approach to an understanding and therapy of the disease. Thus, a major objective of research into the nature of this disease should be directed towards understanding the monocyte deficiency. What is the cause of the quantitative deficiency and do the remaining monocytes have normal func- tion? Since monocyte numbers are low, is RES function impaired in HCL? The second major question would relate to the lymphocyte deficiency. We have documented lympho- penia, low T-cell rosettes and impaired lymphocyte-mediated cytotoxicity suggesting quantitative and qualitative defects. The etiology of these is not understood. Whether
Host defence in hairy cell leukemia 637
there are changes in lymphocyte subsets is not known. The above outlined observations have suggested that biological approaches to therapy of HCL may be useful. This is also suggested by the high risk of chemotherapy in these patients. Attempts to stimulate proliferation of normal cells in the marrow and to restore lymphocyte number and function should be high priority areas for therapeutic research.
Acknowled,qements Supported by Grants CA-05831. CA-16672 and CA-14528 from the National Cancer Institute. National Institutes of Health. Bethesda. MD 20205 IU.S.A.I. Dr. Murphy was a scholar of the Leukemia Society of America.
REFERENCES 1. BACH .11 F. (1973) Evaluation of T cells and thymic serum factors in man using the rosette technique.
Transplantation 16, 196. 2, BURNS G. S.. CAWLEV J. C., BARKER C. R., GOLDS'tONE A. H. & HAYHOF F. G. J. (19771 New evidence
relating to the nature and origin of the hairy cell leukemic reticuloendotheliosis. Br. J. Hemat. 36, 71. 3. CA'rOVSKV D. (1977t Hairy cell leukemia and prolymphocytic leukemia. Clin. Hemat. 6, 245. 4. COLLINS R. D.. LEECH J. H.. WALDRON J. A., FLEXNER J. M. & GUCK A. D. 11976) Diagnosis of hematopoe-
tic, mononuclear and lymphoid cell neoplasms. In Manual of Clinical hnmunology (Ros~ N. R. & FRIEDMAN H., Eds.h p. 718. Am. Soc, Microsis Vol., Washington.
5. Cox D. R. 11970) Anah,sis of Binary Data. Methuen, London. 6. Cox D. R. 11972) Regression models and life tables. JI. R. statist. Soc. Series B, 34, 187. 7. CUP, RtE G. A. & HEDLEY D. W. 11977) Monocytes and macrophages in malignant melanoma. I. Peripheral
blood macrophage precursors, Br. J. Cancer 36, 1. 8. CURTIS J. E.. HERSCH E. M., HARRIS J. E.. McBRID~ C. M. & FRI-IREICH E. J, 11970) The human primary
immunc response to keyhole limpet hemocyanin: interrelationship to delayed hypersensitivity, antibody response and in vitro blast transformation. Clin, exp. hnnnm. 6, 473.
9. Ft; S. M., Wr~CHES'r~R R. J., Rm K. R. & KUN KEL H. G. 0974) Hairy cell leukemia: proliferation of a cell with phagocytic and B-lymphocyte properties. Scan. J. Immun. 3, 847.
t0. GFHAN E. A, (19651 A generalized Wilcoxon test for comparing arbitrarily singly-censored samples. Biome- trika 52, 203.
11. HEkSH E. M., Mt:RVm' S. G., Gux'rERMAN J. U., MORGAN J., QUESADA J.. ZANDER A. & StEWARt D. 11982) Antibody dependent cell-mediated cytotoxicity in human cancer: characterization of patient leukocyte activity and treatment effects.
12. HERSrt E. M.. Mt:RVHV S.. ZAYDER A., DICKE K.. STEWART D. J., TOKI H. & LA'rREILLE J. (1980) Host blood deficiency in hairy cell leukemia and its correction by leukocyte transfusion. Blood 56, 526.
13. Ht:NDER C. P., TA>;~ENBAUM H., CHURCHILL W. H.. MALONEV W. C. & SCHUR P. H. 11977) Immunologic abnormalities in patients with malignant lymphoproliferative diseases. J. natn. Cancer Inst. 58, 1185.
14. JFRROLD H. ZAR 11974) Biostatistical Analysis. Prentice-Hall, Englewood Cliffs, New Jersey. 15. KAPLAX E. L. & M~IER P. 11958) Nonparametric estimation from incomplete observations. J. Am. statist.
.4ss. 53, 457. 16. LA~G J. M.. OBERLANG F. & MORS R. 11974) Immunity cellulaire et leucemies a tricholeukocytes. Nour.
Pressc Med. 3, 2578, 17. LEWlYSKI U.. MAVLIGIT G. M.. Gt'TTERMAN J. U. & HERSH E. M. 11977) interaction between repeated skin
testing with recall antigens and temporal fluctuations of in vitro lymphocyte blastogenesis in cancer patients, Clin. hmnun, hmnunopath. 7, 77.
18. MORRIS D. L., HERSn E. M., Hm B. P., GUTTERMAX J. U.. MARSHAI-L M. M. & M^vLworr G. (19781 Recall antigen delayed-type hypersensitivity in melanoma and acute leukemia patients and their associates. Cam'er Rc.~. 39, 219.
19. NAX,A K.. JAFFI: E. S.. SOBAY; E. J.. BI~AYLAY R. C. & BERARD C. W. 11977) Hairy cell leukemia: enzyme histochemical characterization with special reference to splenic stromal changes. Cancer 39, 2323.
20. POPLACK D O,. BOYSARD G. C., HOLIMA~ B. J. & BLAESE R. M. 11976) Monocyte mediated antibody- dependent cellular cytotoxicity: a clinical test of monocyte function. Blood 48, 809.
21. Rtmx A. D.. DObGLAS D.. CHESSlY L. N., GLADE P. R. & DAMESHEK W, (1969) Chronic reticulolymphocy- tic leukemia: reclassification of 'Leukemic reticuloendotheliosis" through functional characterization of the circulating mononuclear cells. Am. J. Med. 47, 149.
22. SFSHADRI R. S.. BROW~< E. J. & Zn't'RSKV A. (19761 Leukemia reticuloendotherliosis: a failure of monocyte production. N. Emil. J. Med. 295, 181.
23. T,,K,XSt GI M.. RAMSEYER A. & TAICASL'GI J. 11977) Decline of natural nonselective cell-mediated cytotoxicity m patients with tumor progression. Cancer Res. 37, 413.
24. ~,VEINSTFIN R. A.. Gl:t.MAX E. GOLOMB H. M. 11978) Disseminated atypical mycobacterial infection in hairy cell leukemia. Lancet i i , 1052.
25 Wt~(nES'rEg R. J. & Ross G. 11976) Methods for enumerating lymphocyte populations. In Manual of Clinical hmnunolotly (Rose N. R. & FRIEDMAX H., Eds./. American Society of Hematology, Washington.
26. Y asl L. T., LI C. Y. & CROSBV W. H. (1971~ C xtochemical identification of monocytes and granulocytes, Am. J. elm. Path. 55. 283.