
Duration of hospitalization and appetite of HIV-infected South African children

Journal of Cardiac Failure Vol. 17 No. 1 2011
Review Articles
Hospitalization Epidemic in Patients With Heart Failure: RiskFactors, Risk Prediction, Knowledge Gaps, and Future Directions
GREGORY GIAMOUZIS, MD,1,2 ANDREAS KALOGEROPOULOS, MD,1 VASILIKI GEORGIOPOULOU, MD,1
SONJOY LASKAR, MD,1 ANDREW L. SMITH, MD,1 SANDRA DUNBAR, RN, DSN,1 FILIPPOS TRIPOSKIADIS, MD,2
AND JAVED BUTLER, MD, MPH1
Atlanta, Georgia; and Larissa, Greece
From the 1Emossaly, Larissa, Gr
Manuscript recAugust 3, 2010; r
Reprint requestUniversity Hospit30322, Tel: 404-
emory.eduSupported in p
Board grant entitlin Heart Failure.’’All decisions reSee page 62 for1071-9164/$ - s� 2011 Elseviedoi:10.1016/j.ca
ABSTRACT
Patients with heart failure (HF) are hospitalized over a million times annually in the United States. Hos-pitalization marks a fundamental change in the natural history of HF, leading to frequent subsequentrehospitalizations and a significantly higher mortality compared with nonhospitalized patients. Three-fourths of all HF hospitalizations are due to exacerbation of symptoms in patients with known HF.One-half of hospitalized HF patients experience readmission within 6 months. Preventing HF hospitaliza-tion and rehospitalization is important to improve patient outcomes and curb health care costs. To imple-ment cost-effective strategies to contain the HF hospitalization epidemic, optimal schemes to identifyhigh-risk individuals are needed. In this review, we describe the risk factors that have been associatedwith hospitalization risk in HF and the various multimarker risk prediction schemes developed to predictHF rehospitalization. We comment on areas that represent gaps in our knowledge or difficulties in inter-pretation of the current literature, representing opportunities for future research. We also discuss issueswith using HF readmission rate as a quality indicator. (J Cardiac Fail 2011;17:54e75)Key Words: Acute heart failure, risk factor, prognosis, risk prediction, outcome, model, hospitalization,rehospitalization.
Heart failure (HF) is a growing epidemic.1 Over 5 mil-lion individuals in the United States have HF, and morethan 550,000 are diagnosed annually.2 The complex arrayof physiologic, psychologic, social, and health care deliveryissues makes it a challenging chronic disease to manage.3,4
Over the past decade, the annual number of hospitalizationshas increased from 800,000 to O1 million for HF as a pri-mary, and from 2.4 to 3.6 million for HF as a primary or
ry University, Atlanta, Georgia and 2University of The-eece.eived December 12, 2009; revised manuscript receivedevised manuscript accepted August 16, 2010.s: Javed Butler, MD, MPH, Cardiology Division, Emoryal, 1365 Clifton Road, NE, Suite AT430, Atlanta, GA778-5273; Fax: 404-778-5285. E-mail: javed.butler@
art through an Emory University Heart and Vasculared ‘‘Novel Risk Markers and Prognosis Determination
garding this manuscript were made by a guest editor.disclosure information.ee front matterr Inc. All rights reserved.rdfail.2010.08.010
54
secondary diagnosis.5 Approximately 50% of HF patientsare rehospitalized within 6 months of discharge,6 and70% of rehospitalizations are related to worsening of previ-ously diagnosed HF.7 A recent analysis of all Medicare feesfor service readmission to hospitals for any cause showedHF to be the number 1 cause of rehospitalization.8 Heartfailure rehospitalization carries a significantly higher mor-tality risk compared with index hospitalization.9 Heart fail-ure is the primary reason for 12-15 million office visits and6.5 million hospital-days each year.10 With aging of thepopulation, HF rates and the associated rehospitalizationswill rise. By 2050, 1 in 5 persons in the United Stateswill be elderly11; 80% of patients hospitalized for HF areO65 years old.10 Furthermore, intense societal need for im-proving medical quality of care has shifted the focus from‘‘hard’’ outcome measures initially introduced (ie, all-causemortality) to ‘‘softer’’ outcomes; therefore, 30-day postdi-scharge HF readmission rates are now being consideredas quality measures.
To implement interventions to reduce HF rehospitaliza-tions cost-effectively, identification of high-risk individualsis essential. Numerous individual risk factors for HF

Risk Factors for Hospitalization in Heart Failure � Giamouzis et al 55
rehospitalization, assessed at various times related to indexhospitalization (admission, discharge, first follow-up visit,etc) have been reported. Importantly, identification oflow-risk individuals is also essential, because absence ofhigh risk does not necessarily indicate a low-risk patientwho can be safely discharged.12,13 Based on these factors,different multimarker risk-prediction models have been de-veloped to increase prediction accuracy and precision.14,15
However, gaps in our knowledge of the underlying patho-physiologic mechanisms pose difficulties in interpretingthe currently available excess of data. Furthermore, datain this respect are not always consistent. Given the hetero-geneous nature of the HF population, spanning from ische-mic to nonischemic, low to preserved ejection fraction,interfering with various comorbid conditions, a ‘‘one-size-fits-all’’ approach to risk stratification may not be appropri-ate and subpopulations may need to be targeted. Data basedonly on administrative records have been challenged,16,17
and addition of clinical information may improve riskprediction.18e22 Therefore, understanding the predictors,the timing of their appearance in the course of the syn-drome, their strength of association with certain outcomes,and in which specific subpopulations they predict risk is es-sential to devise effective prevention interventions to curbthe HF rehospitalization epidemic.In the present review, we provide a comprehensive over-
view of literature regarding individual predictors and themulti-marker risk models related to HF rehospitalizationrisk (Table 1). The details of individual risk factors are pre-sented in Supplementary Tables 2e4 (available online atwww.onlinejcf.com), where data are sorted by studies onindividuals with depressed, preserved, and unspecifiedejection fraction, respectively.
Literature Reviewed
In this review, we primarily list the studies and the riskfactors, and have created detailed tables to list more in-depth data, for references purposes. Considering the enor-mity of the topic, it was not possible to discuss the details,regarding either the risk factor’s strength of association oritss clinical and pathophysiologic significance, of eachand every individual risk factor. These would be topicsfor further focused reviews.Publications included in this review reported HF-specific
hospitalizations data as either primary or secondary out-come, or as part of a composite outcome with mortalityrate. To review data applicable to the current era of HFtherapy, we focused on studies published within the pastdecade. Ovid Medline, PubMed, and Scopus were searchedfrom January 1, 1999, to October 31, 2008, to identifyrelevant studies using the keywords: ‘‘heart failure,’’ ‘‘read-mission,’’ ‘‘rehospitalization,’’ ‘‘hospitalization,’’ ‘‘riskprediction,’’ ‘‘model,’’ ‘‘prognosis,’’ and ‘‘outcome.’’ Publi-cations eligible for inclusion reported on readmissionamong individual patients hospitalized for HF as a primary
outcome, secondary outcome, or part of a composite out-come. Only data from studies that included $100 patientswere included. NoneEnglish language studies, abstracts,pediatric studies, and publications without original data(reviews, letters, and editorials) were not included. Alsoexcluded were studies that reported results from caseseries, experimental studies, and those without quantifiedoutcomes.
Risk Factors for Hospitalization in Heart Failure
Sociodemographic
Heart failure rehospitalizations increase with age: A4-fold increase in 30-day readmission rate for elderlypatients $80 years23 and a 24% increase/10-year ageincrements in the annual readmission rate have been re-ported.24,25 Advanced age predicts readmission in multira-cial populations.26e30 Higher readmission rates have beenreported for both male4,24,25,31e33 and female34e37 gender;however, some studies have failed to replicate theseresults.38e41 Nonwhite race has been associated with a high-er risk,26,34 with higher rates in blacks and Latinos than inAsians and whites.42e45 Not all studies have confirmedthese findings.24,46e49 Risk is related to socioeconomic sta-tus50: A significant stepwise decrease in HF-related read-mission has been observed from the lowest to the highestincome quartile.51,52 Insurance status affects rehospitaliza-tion, with patients enrolled in a health maintenance organi-zation experiencing lower 6-month readmission rates thanMedicaid and Medicare patients.53 Lack of employmentis associated with readmissions,54,55 as is family statusand living alone.55,56 Smoking is associated with multiplereadmissions,56 although ‘‘smoker’s paradox’’ in hospital-ized HF patients has been reported, with current or recentsmoking being associated with a 23% lower risk-adjusted90-day rehospitalization risk.57 Current or past alcoholuse is an independent predictor of HF readmissions.55,56
Clinical
Several studies suggest higher readmission rates withischemic etiology.23,26,56,58e61 Some studies have reportedworse risk for patients with depressed ejectionfraction,58,62e64 whereas recent studies demonstrate similarrisk with preserved ejection fraction.47,65e70 Low systolicblood pressure is an independent predictor ofrehospitalization.60,71e73 A 2% increase in 60-day readmis-sion for every 1 mm Hg decrease has been reported.27,35,74
Similarly, 10 mm Hg decrease in diastolic pressure is asso-ciated with an 11% increase in cardiovascular mortality orHF rehospitalization.75 Increased heart rate has been shownto correlate with readmissions.76e79 Higher New YorkHeart Association functional class at discharge also predicts30-day and 1-year readmissions.25e27,56,80,81 Prior HF hos-pitalization is an independent risk factor for recurrentreadmissions.4,23,32,54,60,82e85 Prolonged length of stay
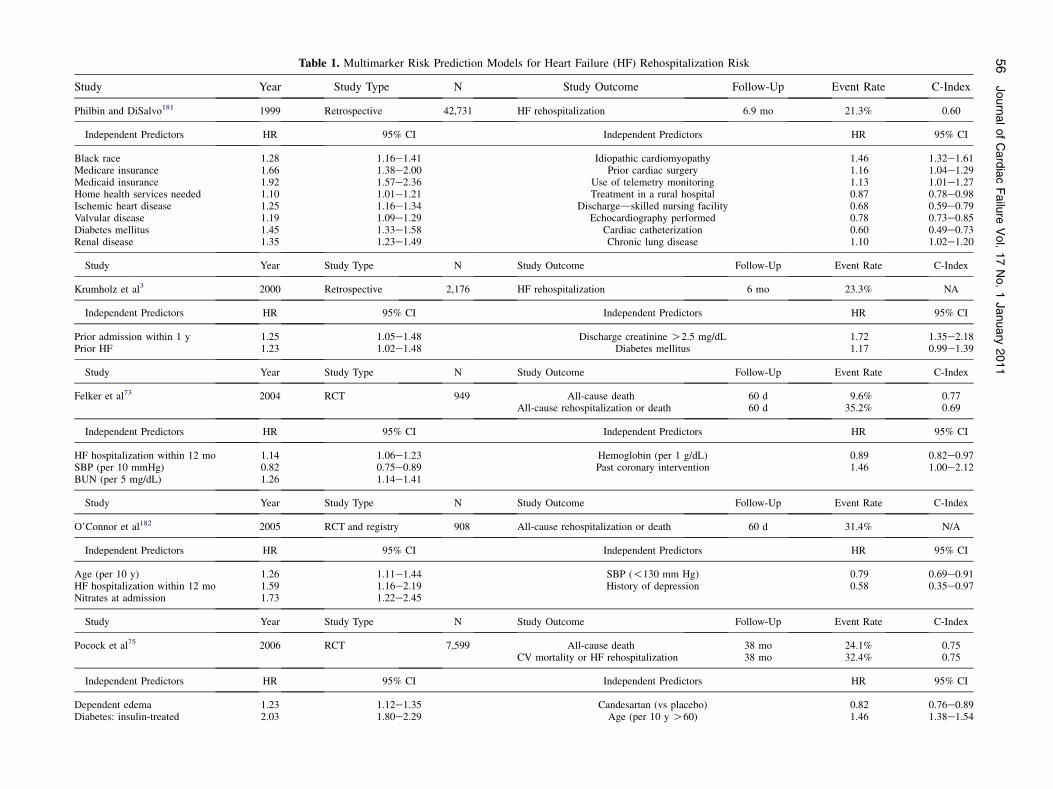
Table 1. Multimarker Risk Prediction Models for Heart Failure (HF) Rehospitalization Risk
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
Philbin and DiSalvo181 1999 Retrospective 42,731 HF rehospitalization 6.9 mo 21.3% 0.60
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
Black race 1.28 1.16e1.41 Idiopathic cardiomyopathy 1.46 1.32e1.61Medicare insurance 1.66 1.38e2.00 Prior cardiac surgery 1.16 1.04e1.29Medicaid insurance 1.92 1.57e2.36 Use of telemetry monitoring 1.13 1.01e1.27Home health services needed 1.10 1.01e1.21 Treatment in a rural hospital 0.87 0.78e0.98Ischemic heart disease 1.25 1.16e1.34 Dischargedskilled nursing facility 0.68 0.59e0.79Valvular disease 1.19 1.09e1.29 Echocardiography performed 0.78 0.73e0.85Diabetes mellitus 1.45 1.33e1.58 Cardiac catheterization 0.60 0.49e0.73Renal disease 1.35 1.23e1.49 Chronic lung disease 1.10 1.02e1.20
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
Krumholz et al3 2000 Retrospective 2,176 HF rehospitalization 6 mo 23.3% NA
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
Prior admission within 1 y 1.25 1.05e1.48 Discharge creatinine O2.5 mg/dL 1.72 1.35e2.18Prior HF 1.23 1.02e1.48 Diabetes mellitus 1.17 0.99e1.39
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
Felker et al73 2004 RCT 949 All-cause death 60 d 9.6% 0.77All-cause rehospitalization or death 60 d 35.2% 0.69
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
HF hospitalization within 12 mo 1.14 1.06e1.23 Hemoglobin (per 1 g/dL) 0.89 0.82e0.97SBP (per 10 mmHg) 0.82 0.75e0.89 Past coronary intervention 1.46 1.00e2.12BUN (per 5 mg/dL) 1.26 1.14e1.41
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
O’Connor et al182 2005 RCT and registry 908 All-cause rehospitalization or death 60 d 31.4% N/A
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
Age (per 10 y) 1.26 1.11e1.44 SBP (!130 mm Hg) 0.79 0.69e0.91HF hospitalization within 12 mo 1.59 1.16e2.19 History of depression 0.58 0.35e0.97Nitrates at admission 1.73 1.22e2.45
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
Pocock et al75 2006 RCT 7,599 All-cause death 38 mo 24.1% 0.75CV mortality or HF rehospitalization 38 mo 32.4% 0.75
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
Dependent edema 1.23 1.12e1.35 Candesartan (vs placebo) 0.82 0.76e0.89Diabetes: insulin-treated 2.03 1.80e2.29 Age (per 10 y O60) 1.46 1.38e1.54
56
JournalofCardiacFailure
Vol.17No.1January
2011

Diabetes: other 1.58 1.43e1.74 Pulmonary crackles 1.25 1.13e1.38EF (per 5% lower) 1.13 1.11e1.16 Rest dyspnea 1.20 1.10e1.31HF hospitalization within 6 mo 1.73 1.55e1.93 Female 0.83 0.76e0.91HF hospitalization beyond 6 mo 1.22 1.09e1.37 Atrial fibrillation 1.16 1.07e1.27Diagnosis of HF O2 years ago 1.31 1.20e1.43 BMI (per 1 kg/m2 decrease !27.5) 1.03 1.01e1.04Cardiomegaly 1.35 1.23e1.47 Mitral regurgitation 1.16 1.05e1.28NYHA functional class III 1.32 1.20e1.45 Previous MI 1.11 1.02e1.21NYHA functional class IV 1.54 1.25e1.89 Pulmonary edema 1.26 1.03e1.54DBP (per 10 mm Hg) 1.11 1.07e1.16 Heart rate (per 10/min) 1.08 1.05e1.11Bundle branch block 1.26 1.15e1.38
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
Yamokoski et al183 2007 RCT 373 Death 6 mo 19.3% N/AAll-cause rehospitalization 6 mo 49.3% 0.596
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
BUN at discharge N/A N/A High-dose diuretics N/A N/A
Study Year Study Type N Study Outcome Follow-Up Event Rate C-Index
Keenan et al184 2008 Retrospective 283919 All-cause rehospitalization 30 d 6.5% 0.60
Independent Predictors HR 95% CI Independent Predictors HR 95% CI
Past CAB surgery 0.93 0.91e0.96 History of HF 1.09 1.07e1.12Asthma 1.06 1.03e1.10 Other GI disorders 1.06 1.04e1.08Cardiorespiratory failure/shock 1.08 1.06e1.11 Peptic ulcer, hemorrhage, other GI disorders 1.07 1.05e1.10Arrhythmias 1.06 1.04e1.08 Severe hematologic disorders 1.15 1.10e1.21ACS 1.12 1.10e1.15 Nephritis 1.08 1.03e1.12Valvular and rheumatic disease 1.08 1.06e1.10 Metastatic cancer and acute leukemia 1.14 1.07e1.21Vascular disease 1.07 1.05e1.09 Liver and biliary disease 1.06 1.02e1.09Chronic atherosclerosis 1.09 1.06e1.11 End-stage renal disease/dialysis 1.16 1.11e1.22Other/unspecified heart disease 1.05 1.03e1.08 Decubitus or chronic skin ulcer 1.10 1.07e1.13Hemi- or paraplegia, paralysis,
functional disability1.04 1.01e1.08 Iron deficiency and other anemias and blood disease 1.09 1.06e1.11
Stroke 1.03 1.00e1.07 Pneumonia 1.09 1.06e1.11Disorders of fluid
electrolyte/acid-base1.12 1.09e1.14 Drug/alcohol abuse/dependence/psychosis 1.07 1.04e1.10
Chronic pulmonary disease 1.17 1.14e1.19 Other psychiatric disorders (depression excluded) 1.08 1.05e1.12Diabetes with complications 1.08 1.06e1.11 Fibrosis of lung and other chronic lung disorders 1.05 1.02e1.08Renal failure 1.15 1.13e1.18 Protein-calorie malnutrition 1.05 1.01e1.09Other urinary tract disorders 1.12 1.10e1.15
ACS, acute coronary syndrome; BMI, body mass index; BUN, blood urea nitrogen; CAB, coronary artery bypass; CI, confidence interval; CV, cardiovascular; DBP, diastolic blood pressure; EF, ejection frac-tion; GI, gastrointestinal; HR, hazard ratio; MI, myocardial infarction; NYHA, New York Heart Association; RCT, randomized control trial; SBP, systolic blood pressure.
RiskFactors
forHospita
lizatio
nin
HeartFailure
�Giamouzis
etal
57

58 Journal of Cardiac Failure Vol. 17 No. 1 January 2011
(O7 days) during index hospitalization portends higher6-month readmission rates4; when defined as O14 days,it confers a 3-fold increase risk.54 Physical signs of volumeoverload confer a 2-fold increased risk of 6-month readmis-sion in hospitalized HF patients.76 Also, signs of poor tissueperfusion, ie, ‘‘cold’’ state have a 2.5-fold higher risk.61 Inpatients with recent HF hospitalization, an objective clini-cal disease severity score was independently associatedwith annual risk for rehospitalization.29
Blood Tests
Lower admission hemoglobin level is associated witha higher risk.60,86 A 27% decrease in rehospitalization per2 g/dL increase in hemoglobin levels has been described.28
Similarly, a 2% higher risk of 1-year readmission for every1% lower admission hematocrit level has been reported.87
A 3 � 109/L increase in neutrophil count (approximately30% increase) is associated with a 25% increase in HF re-hospitalizations.28 The risk of HF rehospitalization afterhospital discharge increases by 8% per 3 mEq/L decreasein serum sodium levels.88 In another study, a 5 mEq/L in-crease conferred a 40% decrease in the 2-year HF rehospi-talization rate in patients with HF and preserved ejectionfraction.28 Total bilirubin levels predict risk in patientswith systolic dysfunction.27 A 2 mmol/L increase in admis-sion glucose confers a 6% increase in annual readmis-sions.89 A 25% increase in readmission per 1% increasein hemoglobin A1c levels has been reported.90 Both admis-sion84,85 and discharge36 serum creatinine levels have beencorrelated with readmission in patients with low84,85 orpreserved36 ejection fraction. A 39% increase in 6-monthreadmission rate per 1 mg/dL increase in serum creatininelevels has been reported.91 Similarly, increased blood ureanitrogen levels have been associated with higher readmis-sion rates28,92,93: A 2% risk per 1 mg/dL increase in admis-sion levels has been reported.32 Uric acid O7 mg/dL(420 mmol/L) in men and O6 mg/dL (360 mmol/L) inwomen with HF is associated with higher readmission ratesamong both hospitalized patients94 and outpatients.30
Several studies have reported the prognostic ability ofnatriuretic peptides.95e101 In a small single-center study,a B-type natriuretic peptide (BNP) level of O200 pg/mLprovided an optimal value in predicting HF readmission.102
Admission and discharge levels predict readmission in var-ious populations82,91,103e107 including those with systolicdysfunction,27,36 restrictive filling pattern,81 or chronic re-nal insufficiency.95 Although not consistently seen or uni-versally agreed upon, a reduction in natriuretic peptidelevels during hospitalization by O30%-40% has beenassociated with improved outcomes in somestudies.36,76,95,105,108e110 Postdischarge measurement alsoprovides risk stratification.29,111e113 Therefore, natriureticpeptideeguided therapy has been proposed,91,104,114,115
and several natriuretic peptideeguided trials have alreadybeen published. Even though their results are somewhat
conflicting, intense research interest in this fieldcontinues.114,116e118
Data on newer biomarkers are emerging. Elevated con-centration of cardiac troponin during HF hospitalization is astrong and consistent predictor of readmission.61,112,119e122
C-Reactive protein (CRP) levelsO0.9 mg/dL are associatedwith higher risk,123 and HF readmissions increase with in-creasing quartile of CRP124 or high-sensitivity CRP.120,125
Apolipoprotein A-I levels lower than !103 mg/dL areassociated with higher readmission rates independent ofhigh-density lipoprotein and BNP levels.126,127 Cystatin Cis also associated with higher risk irrespective of serumcreatinine.128 Other experimental biomarkers associatedwith HF rehospitalizations include advanced glycation end-products, such as pentosidine129 and soluble receptor,130
heart-type fatty acidebinding protein,102,131 serum renin,119
and serum procollagen type I levels.132
Other Tests
Prolonged QRS duration on electrocardiogram is an in-dependent predictor of HF morbidity.133,134 Increased car-diothoracic ratio on chest X-ray is associated with higherHF readmission rates.135 On echocardiography, severalstudies have reported lower readmission rates for patientswith higher ejection fraction26,29,30,35,81,120,136,137 A 2%fall in 6-month readmission rate per 1% increase in ejectionfraction has been reported.91 An increase of 1 mL/m2 in leftatrial volume index increases the risk of death or readmis-sion by 3%.138 Echocardiographically estimated systolicpulmonary arterial pressure has also been useful in predict-ing HF readmission.139 Right ventricular tissue Dopplerimaging predicts HF rehospitalization independently ofother Doppler diastolic function variables.140 Similarly, tis-sue Doppler imagingedetected mechanical dyssynchronypredicts HF readmission in patients with systolic dysfunc-tion and normal QRS duration.141 Finally, decreased heartrate variability,78,142e145 especially its very-low-frequencypower spectral components,146 is associated with higherrisk, and heart rate recovery after exercise provides addi-tional prognostic information.147
Comorbidity Burden
A large proportion of readmissions for HF are associatedwith comorbidities that precipitate, contribute to, or compli-cate HF admission,148 especially in the elderly.10 In a recentpopulation study, 39% of HF patients had $5 noncardiaccomorbidities and only 4% had HF alone.149
Cardiovascular
Presence of hypertension (admission systolic blood pres-sure O140 mm Hg) during HF hospitalization decreasesannual risk of HF readmission,24 especially in the elderly.59
In contrast, a history of hypertension (ie, documented anti-hypertensive treatment) is related to an increased risk.54
Angina pectoris is associated with a higher annual risk of

Risk Factors for Hospitalization in Heart Failure � Giamouzis et al 59
rehospitalization in black patients.136 Concomitantmyocardial infarction during HF hospitalization increasesannual readmission risk.24 Atrial fibrillation is common inHF and adversely affects hemodynamics.150,151 Severalstudies demonstrate that atrial fibrillation is associatedwith an increased risk of HF readmissions in patientswith low152 or preserved25,153 ejection fraction. Interest-ingly, rhythm control does not reduce risk for rehospitaliza-tion.154 Patients with valvular heart diseases, regardless ofsystolic function, have a 4-hold higher likelihood for HFrehospitalization.28
Noncardiovascular
Several studies have demonstrated a consistent associationbetween diabetes mellitus and increased rehospitalizationrates in HF with low66,155,156 or preserved66 ejection fractionor in multirace3,24,84,89,157 and in single-race26 populations.One study suggested an increased risk for black womenwith diabetes mellitus compared with men or nonblack pa-tients.136 Anemia is common in HF158: When defined as he-moglobin !12 g/dL, anemia is associated with higher HFreadmission.59,86,159e161 Hyponatremia, defined as serumsodium level !136 mEq/L, is a marker of increased 3-,83
6-,162 and 12-month122HF readmission. A history of renal in-sufficiency or the presence of elevated serum creatininelevels (O1.5 mg/dL) on admission are common in HF pa-tients163 and are associated with higher rates of HF rehospi-talization.24,55,164 Worsening renal function during HFhospitalization is also common,83 and regardless of the defi-nition used, it appears to predict independent risk for HF re-hospitalization.165,166 Cerebrovascular disease increases4-fold the likelihood of death or rehospitalization at 3monthsin patients hospitalizedwithHF.83History of stroke increasesthe annual mortality and readmission rate by 26% in HF pa-tients.24,167 Chronic obstructive pulmonary disease is associ-ated with higher risk,28,32,34,149 regardless of beta-blockeruse.168 Obstructive sleep apnea doubles169 and pulmonaryembolism quadruples83 the likelihood of HF readmission.Depression, present in almost one-half of chronic HF pa-tients,170,171 is associated with higher annual HF readmissionrates.55,170,172e174 Several scores have been used to quantifycumulative comorbidity burden: Higher HF readmissionrates have been reported for patients with higher Deyo co-morbidity score or Charlson comorbidity index.4,85
Quality of Life and Psychosocial Factors
Several self-assessment questionnaires quantify anindividual’s perception of their quality of life. A symptomstability score, based on either the Kansas City Cardiomy-opathy Questionnaire or the Minnesota Living withHeart Failure Questionnaire, correlates with the HFreadmission risk.34,175 Poor quality of life on the Notting-ham Health Profile is an independent predictor of readmis-sion among elderly HF patients.176 Higher readmissionrates have also been reported with worse 36-item Short
Form survey scores.84 Absence of emotional support or so-cial network among elderly hospitalized patients is a strongpredictor of increased readmission rate, especially amongwomen.85,177
Disease Management
Despite the fact that in the current therapeutic era morepatients are discharged on evidence-based medication, ad-herence to these therapies in the outpatient setting hasbeen shown to deteriorate over time.178 A targeted formaleducation and support intervention has been associatedwith a 44% decrease in the annual HF readmissionrate.179 A multidisciplinary team intervention, consistingof patient and family education, a prescribed diet, social-service consultation, medication review, and intensivefollow-up lead to improved quality of life and reduce HFreadmission rates.157 Poor follow-up is associated withhigher risk.54 A prepared follow-up plan with an appoint-ment scheduled in the HF clinic, provided to the patientupon discharge, decreases their likelihood for HF readmis-sion within 30 days after discharge.80 Health care providedby an HF-specialist reduces the risk for readmission com-pared with care provided by primary care physicians.56 Ahome-based telemanagement program has also been shownto reduce the annual HF readmission rate.180
Risk Prediction
Using administrative claims data, Philbin and DiSalvocreated a scoring system to quantify the annual HF-specific readmission risk among hospitalized HF patientsby using 16 variables (Table 1).181 This model had mar-ginal discriminative ability, with a C-index of 0.60.Krumholz et al. developed a model for readmission risk3:Among 32 variables examined, 4 emerged as independentpredictors of 6-month all-cause readmissions. Felkeret al. derived a model that predicted outcomes among pa-tients with decompensated HF.73 Among 41 variables eval-uated, 5 were predictive of death or readmission at 60 days.The discriminatory power of the model was better for themortality (C-index 0.77) but less for the composite endpoint including rehospitalization (C-index 0.69). O’Connoret al. combined data from a clinical trial and a registry tocreate a model to predict 60-day death or readmissionsamong hospitalized HF patients.182 Age, use of nitrates atadmission, and $1 admission for HF in the previous yearincreased risk, whereas systolic blood pressure !130mm Hg and, interestingly, a history of depression appearedto reduce risk. Pocock et al. developed a model from 7,599HF patients with preserved and decreased systolic func-tion.75 The final model included 21 predictor variablesfor cardiovascular death or HF rehospitalization. The 3most powerful predictors were age, diabetes mellitus, andejection fraction !45%. Yamokoski et al. created a modelto estimate the risk of death and readmission among

Fig. 1. The complex relationship between comorbidities and heart failure. Comorbid conditions may affect heart failure by causing it,exacerbating decompensation, masking symptoms, or affecting compliance with evidence-based medication.
60 Journal of Cardiac Failure Vol. 17 No. 1 January 2011
hospitalized patients with severe HF.183 The prognosticmodel again showed modest discrimination. Finally,Keenan et al. developed an administrative claimsebasedmeasure for profiling hospital performance for 30-dayall-cause readmission rates.184 The model included 37 vari-ables, and the C-index was only 0.60.
Overall, these models had modest C-indexes ofw0.60 forreadmission risk prediction regardless of whether they wereadministrative data181,184 or medical records based.183 Thisraises the possibility that either important predictors of HF re-admission are not present in suchdatabases or nonmedical fac-tors play a major role in HF rehospitalization risk.
Knowledge Gap and Future Directions
It is apparent from the aforementioned discussion thatdespite a multitude of known risk factors, actual predictionof HF rehospitalization is difficult, with at best only modestresults seen in the previous literature. Considering the in-ability to both reduce the national burden of HF rehospital-ization rate and the inability to accurately predictrehospitalization risk as opposed to combined rehospitaliza-tion and mortality risk, 4 issues need close scrutiny: impor-tance of comorbid conditions; lack of therapeutic options;importance of nonclinical factors; and assessment and treat-ment of congestion.
Importance of Comorbid Conditions
Comorbid conditions play a major role in HF progres-sion and risk for rehospitalization. Many comorbidities,
eg, diabetes mellitus or renal failure, may worsen HF,and HF may vice versa worsen the comorbid condition.Regarding HF rehospitalization risk, comorbidities mayaffect the risk by causing, exacerbating, or maskingHF, or by affecting compliance or health careeseekingbehaviors (Fig. 1). It is simplistic to assume that a diseasemanagement, as opposed to a patient management, ap-proach ignoring the huge comorbidity burden will reducerehospitalization risk. To complicate matters further, alladministrative and most clinical databases are incrediblyill equipped to truly assess the importance of comorbidityburden. For example, the Medicare database is based onadministrative codes and does not have the clinical infor-mation to put the information in its correct perspective,eg, HF may represent low or preserved left ventricularejection fraction, or ischemic or nonischemic etiology.Moreover, the degree of functional abnormality is notavailable (eg, peak VO2, 6-minute walking distance ,oreven the NYHA functional class), and it is well knownthat the clinical relevance of a peak VO2 of 10 mLkg�1 min�1 is different than that of 20 mL kg�1
min�1, though both conditions may be labeled as ‘‘heartfailure.’’ Finally, the administrative codes are largely pro-vided by hospital administrative and not medical staff.Therefore, database-related comorbidity assessment likelyunderestimates the role of comorbidities by inaccuratelyassessing:
True prevalence (eg, sleep apnea or depression).Disease severity (eg, risk may vary with worsening degreeof pulmonary function derangement, but such details arenot available).

Risk Factors for Hospitalization in Heart Failure � Giamouzis et al 61
Adequacy of therapy (eg, it is possible that individuals withdiabetes mellitus have a different risk based on hemoglobinA1c levels).
These limitations may preclude accurate risk predictionand risk attenuation, underscoring the need for better as-sessment and treatment of comorbidities in future.
Assessment and Treatment of Congestion
Many hospitalized HF patients lose little or no weightduring hospitalization,185 although data from clinical trialpopulations differ from registry or observational data inthis respect.186 However, it may be inaccurately assumedthat all patients with decompensated HF have significantfluid overload, and in those who do have significant fluidoverload, that it will be possible to get rid of the excessfluid adequately, safely, and in a short time. Effective,safe, and timely diuresis is related to a complex interactionof hemodynamics and fluid compartment interactions(intra- vs extravascular volume and oncotic pressure). Cur-rent surrogates of volume assessment, eg, pulmonary arteryocclusive pressure or the natriuretic peptide levels, may notalways represent the volume status, and even if they did,when they can be safely optimized without complicationssuch as hypotension or renal failure is poorly understood.Although a recent consensus statement proposes a methodof assessment,187 real-life assessment of congestion con-tinues to be debated, and how to decongest patients effec-tively and safely is not well known.
Importance of Nonclinical Factors
It is possible, and likely, that nonclinical factors, espe-cially in the elderly, play a major role in HF worsening re-quiring hospitalization. Important risk factors may not beavailable in clinical or administrative databases unlessspecifically measured, eg, compliance with medications.Most risk scores do not account for the influence of patientself-care behavior or social vulnerabilities; withoutpaying specific attention to these as preventive interventiontargets, medical interventions per se may not reach their fullpotential.
Lack of Therapeutic Options
Data with therapies that have been proven to improve re-hospitalization risk are primarily for systolic dysfunctionand were almost exclusively generated in the chronic outpa-tient setting. Unfortunately, there continues to be a lack ofscientifically proven data supporting therapies that, whentargeted specifically at acute decompensated HF patients,prevent the risk for readmission. Furthermore, there is norandomized trial for the management of diastolic HF thatreduces readmission rate, although diastolic dysfunction ac-counts for O50% of HF, especially among the elderly pop-ulation.188 Data in this respect are largely either related todisease management programs189e191 or based on observa-tional data.192 The lack of successful therapy to date maybe partially driven by the lack of understanding of the
taxonomy of acute decompensated HFsyndromes,2,7,12,193e195 which likely represent several var-ied pathophysiologies necessitating different therapeuticapproaches. Perhaps no other area of major cardiovascularpublic health impact is less well understood than decom-pensated HF, underscoring the need for intense focused re-search in this area.
Other Issues
Several other issue regarding heart failure rehospitaliza-tion risk, prediction, and the use of these data merit high-light.
Outcome
Different investigators have assessed varying outcomes,eg, prediction of hospitalization versus rehospitalization,rehospitalization alone versus combined with mortality,and prediction of all-cause versus cardiovascular versusHF-specific rehospitalizations. Because the predictors ofmortality versus all-cause versus HF-specific rehospitaliza-tion may vary, synthesizing a summary conclusion based oncurrent literature, though important to implement specificstrategies for lowering this epidemic, is difficult. Neverthe-less, end points other than HF rehospitalization, such as all-cause rehospitalization, may provide extremely importantinformation regarding specific HF populations (eg, the el-derly HF patients with preserved ejection fraction, wheremore than one-half of rehospitalizations have been attrib-uted to noncardiovascular causes).
Time Period
Different studies have reported risk for 30-, 90-, 180-, or365-day outcomes. It is possible that short-term outcomesare related to in-hospital care, intermediate-term outcomesto postdischarge care, and long-term outcomes to other pa-tient- and provider-related factors. Data from these variousstudies therefore may not be directly comparable.
Timing of Risk Factor Measurement
When a particular risk factor is measured for risk predic-tion in the spectrum of illness and presentation merits atten-tion. This is especially important for the clinical (ie,congestion, body weight) and laboratory (admission or dis-charge values vs dynamic changes) parameters. There isa great variability in the timing of assessment of a particularrisk factor among different studies, and these risk factorsmay predict risk at one particular time point and not theother.
Diversity
Considerable data indicate that both biologic/diseasee andhealth care deliveryerelated disparities exist based on gen-der,24,25,32,35,132 race/ethnicity,26,42,43,45 and age.23e28,30,132
This may be particular important for nonclinical risk factors,including patient perception, belief system, and compliance.

62 Journal of Cardiac Failure Vol. 17 No. 1 January 2011
Predictors in these various groupsmay vary requiring inquiryof specific race/ethnicityerelated data.
Intention
Risk models for primary prevention are most optimal ifthey are parsimonious and specific. In contrast, models topredict mortality to allocate advanced therapies need tobe sensitive and complexity is less of a concern. BecauseHF readmission risk prediction can have various motivesand may differ for patients, providers, payers, or re-searchers, the need and quality of the prediction modelmay differ correspondingly.
Readmission and Quality of Care
There is intense societal focus on improving medicalquality of care.42,196e199 Initial quality measures were pro-cess related, and subsequently ‘‘hard’’ outcome measureswere introduced, eg, mortality. However, new measures,such as 30-day postdischarge HF readmission rates, are cur-rently used as quality measures. This consideration raisesseveral concerns. The published risk-adjusted HF readmis-sion predictions models are not optimal for accurate riskprediction for reasons stated above. Performance of othermodels that are currently unpublished in peer-reviewedjournals cannot be judged. In addition, there are no gold-standard rules for when a person should be admitted withHF, and patients may be hospitalized for borderline clinicalor nonclinical social reasons, eg, inadequate family support,assisted-living infrastructures, primary care physician avail-ability, etc. Finally, quality measures such as HF readmis-sion rate might precipitate provider behaviors regardingresisting admissions; this may be a safety concern.
Conclusion
Heart failure rehospitalization clearly marks a fundamen-tal change in the natural history of the syndrome, signifi-cantly increasing subsequent mortality and morbidity.Preventing HF rehospitalization is important to improve pa-tient outcomes and curb health care costs. However, to im-plement such cost-effective strategies, optimal schemes toidentify high-risk individuals, as well as low-risk patientsfor safe discharge, are needed. Numerous risk factorshave been associated with HF rehospitalization risk. Basedon these factors, different multimarker risk predictionmodels were developed to predict HF readmission risk.However, these data, for multiple reasons cited above, arelimited in their application. Further studies to assess the un-derlying pathophysiologic mechanisms and develop newtherapeutic options and better risk prediction schemes areneeded to curb this epidemic.
Disclosures
None.
References
1. Roger VL, Weston SA, Redfield MM, Hellermann-Homan JP,
Killian J, Yawn BP, et al. Trends in heart failure incidence and sur-
vival in a community-based population. JAMA 2004;292:344e50.
2. Gheorghiade M, Pang PS. Acute heart failure syndromes. J Am Coll
Cardiol 2009;53:557e73.
3. Krumholz HM, Chen YT, Wang Y, Vaccarino V, Radford MJ,
Horwitz RI. Predictors of readmission among elderly survivors of ad-
mission with heart failure. Am Heart J 2000;139(1 Pt 1):72e7.
4. Krumholz HM, Parent EM, Tu N, Vaccarino V, Wang Y, Radford MJ,
et al. Readmission after hospitalization for congestive heart failure
among Medicare beneficiaries. Arch Intern Med 1997;157:99e104.
5. Fang J, Mensah GA, Croft JB, Keenan NL. Heart failureerelated hospi-
talization in theU.S., 1979 to 2004. JAmColl Cardiol 2008;52:428e34.
6. Butler J, Kalogeropoulos A. Worsening heart failure hospitalization
epidemic we do not know how to prevent and we do not know
how to treat!. J Am Coll Cardiol 2008;52:435e7.
7. Gheorghiade M, Zannad F, Sopko G, Klein L, Pina IL, Konstam MA,
et al. Acute heart failure syndromes: current state and framework for
future research. Circulation 2005;112:3958e68.
8. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among
patients in the Medicare fee-for-service program. N Engl J Med
2009;360:1418e28.
9. Stewart S, MacIntyre K, Hole DJ, Capewell S, McMurray JJ. More
‘‘malignant’’ than cancer? Five-year survival following a first admis-
sion for heart failure. Eur J Heart Fail 2001;3:315e22.10. Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al.
Heart disease and stroke statisticsd2008 update: a report from the
American Heart Association Statistics Committee and Stroke Statis-
tics Subcommittee. Circulation 2008;117:e25ee146.
11. White House Conference on Aging;. The booming dynamics of aging.
Available at: http://www.whcoa.gov. Retrieved December 6, 2006.
12. Collins S, Storrow AB, Kirk JD, Pang PS, Diercks DB,
Gheorghiade M. Beyond pulmonary edema: diagnostic, risk stratifi-
cation, and treatment challenges of acute heart failure management
in the emergency department. Ann Emerg Med 2008;51:45e57.
13. Collins SP, Storrow AB. Acute heart failure risk stratification: can we
define low risk? Heart Fail Clin 2009;5:75e83.
14. McKay NL, Deily ME. Comparing high- and low-performing hospi-
tals using risk-adjusted excess mortality and cost inefficiency. Health
Care Manage Rev 2005;30:347e60.15. Pine M, Jordan HS, Elixhauser A, Fry DE, Hoaglin DC, Jones B,
et al. Enhancement of claims data to improve risk adjustment of hos-
pital mortality. JAMA 2007;297:71e6.16. Iezzoni LI, Ash AS, Shwartz M, Daley J, Hughes JS,
Mackiernan YD. Predicting who dies depends on how severity is
measured: implications for evaluating patient outcomes. Ann Intern
Med 1995;123:763e70.17. Davis RB, Iezzoni LI, Phillips RS, Reiley P, Coffman GA, Safran C.
Predicting in-hospital mortality. The importance of functional status
information. Med Care 1995;33:906e21.
18. Pine M. Results of laboratory tests for improving risk adjustment for
comparisons of hospitals’ outcomes. Am Clin Lab 1999;18:10e1.
19. Fry DE, Pine MB, Jordan HS, Hoaglin DC, Jones B, Meimban R.
The hazards of using administrative data to measure surgical quality.
Am Surg 2006;72:1031e7; discussion 1039e48.
20. Pine M, Norusis M, Jones B, Rosenthal GE. Predictions of hospital
mortality rates: a comparison of data sources. Ann Intern Med
1997;126:347e54.21. Fry DE, Pine M, Jordan HS, Elixhauser A, Hoaglin DC, Jones B,
et al. Combining administrative and clinical data to stratify surgical
risk. Ann Surg 2007;246:875e85.
22. Pine M, Jones B, Lou YB. Laboratory values improve predictions of
hospital mortality. Int J Qual Health Care 1998;10:491e501.
23. Kossovsky MP, Sarasin FP, Perneger TV, Chopard P, Sigaud P,
Gaspoz J. Unplanned readmissions of patients with congestive heart

Risk Factors for Hospitalization in Heart Failure � Giamouzis et al 63
failure: do they reflect in-hospital quality of care or patient character-
istics? Am J Med 2000;109:386e90.
24. Blackledge HM, Newton J, Squire IB. Prognosis for South Asian and
white patients newly admitted to hospital with heart failure in the United
Kingdom: historical cohort study. BMJ 2003;327(7414):526e31.
25. Koitabashi T, Inomata T, Niwano S, Nishii M, Takeuchi I, Nakano H,
et al. Paroxysmal atrial fibrillation coincident with cardiac decom-
pensation is a predictor of poor prognosis in chronic heart failure.
Circ J 2005;69:823e30.
26. Lee R, Chan SP, Chan YH, Wong J, Lau D, Ng K. Impact of race on
morbidityandmortality inpatientswithcongestiveheart failure: a study
of the multiracial population in Singapore. Int J Cardiol 2009;134:
422e5.
27. Shinagawa H, Inomata T, Koitabashi T, Nakano H, Takeuchi I,
Naruke T, et al. Prognostic significance of increased serum bilirubin
levels coincident with cardiac decompensation in chronic heart fail-
ure. Circ J 2008;72:364e9.
28. Berry C, Hogg K, Norrie J, Stevenson K, Brett M, McMurray J.
Heart failure with preserved left ventricular systolic function: a hospi-
tal cohort study. Heart 2005;91:907e13.
29. Pascual-Figal DA, Domingo M, Casas T, Gich I, Ordonez-Llanos J,
Martinez P, et al. Usefulness of clinical and NT-proBNP monitoring
for prognostic guidance in destabilized heart failure outpatients. Eur
Heart J 2008;29:1011e8.
30. Pascual-Figal DA, Hurtado-Martinez JA, Redondo B, Antolinos MJ,
Ruiperez JA, Valdes M. Hyperuricaemia and long-term outcome after
hospital discharge in acute heart failure patients. Eur J Heart Fail
2007;9:518e24.
31. Alla F, Al-Hindi AY, Lee CR, Schwartz TA, Patterson JH,
Adams KF Jr. Relation of sex to morbidity and mortality in patients
with heart failure and reduced or preserved left ventricular ejection
fraction. Am Heart J 2007;153:1074e80.
32. Harjai KJ, Thompson HW, Turgut T, Shah M. Simple clinical vari-
ables are markers of the propensity for readmission in patients hos-
pitalized with heart failure. Am J Cardiol 2001;87:234e7.
33. Nieminen MS, Harjola VP, Hochadel M, Drexler H, Komajda M,
Brutsaert D, et al. Gender related differences in patients presenting
with acute heart failure. Results from EuroHeart Failure Survey II.
Eur J Heart Fail 2008;10:140e8.
34. Howie-Esquivel J, Dracup K. Effect of gender, ethnicity, pulmonary
disease, and symptom stability on rehospitalization in patients with
heart failure. Am J Cardiol 2007;100:1139e44.
35. MielniczukLM,TsangSW,DesaiAS,NohriaA,LewisEF, Fang JC, et al.
Theassociationbetweenhigh-dosediuretics andclinical stability in ambu-
latory chronic heart failure patients. J Card Fail 2008;14:388e93.36. Bettencourt P, Azevedo A, Fonseca L, Araujo JP, Ferreira S,
Almeida R, et al. Prognosis of decompensated heart failure patients
with preserved systolic function is predicted by NT-proBNP varia-
tions during hospitalization. Int J Cardiol 2007;117:75e9.
37. Frazier CG, Alexander KP, Newby LK, Anderson S, Iverson E,
Packer M, et al. Associations of gender and etiology with outcomes
in heart failure with systolic dysfunction: a pooled analysis of 5 ran-
domized control trials. J Am Coll Cardiol 2007;49:1450e8.
38. LeeWY,CapraAM, JensvoldNG,Gurwitz JH,GoAS.Gender and risk
of adverse outcomes in heart failure. Am J Cardiol 2004;94:1147e52.
39. Opasich C, De Feo S, Ambrosio GA, Bellis P, Di Lenarda A, Di
Tano G, et al. The ‘‘real’’ woman with heart failure. Impact of sex
on current in-hospital management of heart failure by cardiologists
and internists. Eur J Heart Fail 2004;6:769e79.
40. Sheppard R, Behlouli H, Richard H, Pilote L. Effect of gender on
treatment, resource utilization, and outcomes in congestive heart fail-
ure in Quebec, Canada. Am J Cardiol 2005;95:955e9.
41. Vaccarino V, Chen YT, Wang Y, Radford MJ, Krumholz HM. Sex
differences in the clinical care and outcomes of congestive heart fail-
ure in the elderly. Am Heart J 1999;138(5 Pt 1):835e42.
42. Rathore SS, Foody JM, Wang Y, Smith GL, Herrin J, Masoudi FA,
et al. Race, quality of care, and outcomes of elderly patients hospi-
talized with heart failure. JAMA 2003;289:2517e24.
43. Afzal A, Ananthasubramaniam K, Sharma N, al-Malki Q, Ali AS,
Jacobsen G, et al. Racial differences in patients with heart failure.
Clin Cardiol 1999;22:791e4.
44. Philbin EF, DiSalvo TG. Influence of race and gender on care pro-
cess, resource use, and hospital-based outcomes in congestive heart
failure. Am J Cardiol 1998;82:76e81.
45. Alexander M, Grumbach K, Remy L, Rowell R, Massie BM.
Congestive heart failure hospitalizations and survival in California:
patterns according to race/ethnicity. Am Heart J 1999;137:
919e27.
46. Gambassi G, Agha SA, Sui X, Yancy CW, Butler J, Giamouzis G,
et al. Race and the natural history of chronic heart failure: a propen-
sity-matched study. J Card Fail 2008;14:373e8.
47. Agoston I, Cameron CS, Yao D, Dela Rosa A, Mann DL, Deswal A.
Comparison of outcomes of white versus black patients hospitalized
with heart failure and preserved ejection fraction. Am J Cardiol 2004;
94:1003e7.
48. Deswal A, Petersen NJ, Souchek J, Ashton CM, Wray NP. Impact of
race on health care utilization and outcomes in veterans with conges-
tive heart failure. J Am Coll Cardiol 2004;43:778e84.
49. Echols MR, Felker GM, Thomas KL, Pieper KS, Garg J, Cuffe MS,
et al. Racial differences in the characteristics of patients admitted for
acute decompensated heart failure and their relation to outcomes: re-
sults from the OPTIME-CHF trial. J Card Fail 2006;12:684e8.
50. Osler M, Gerdes LU, Davidsen M, Bronnum-Hansen H, Madsen M,
Jorgensen T, et al. Socioeconomic status and trends in risk factors for
cardiovascular diseases in the Danish MONICA population,
1982e1992. J Epidemiol Community Health 2000;54:108e13.
51. Philbin EF, Dec GW, Jenkins PL, DiSalvo TG. Socioeconomic status
as an independent risk factor for hospital readmission for heart fail-
ure. Am J Cardiol 2001;87:1367e71.
52. Rathore SS, Masoudi FA, Wang Y, Curtis JP, Foody JM,
Havranek EP, et al. Socioeconomic status, treatment, and outcomes
among elderly patients hospitalized with heart failure: findings
from the National Heart Failure Project. Am Heart J 2006;152:
371e8.
53. Philbin EF, DiSalvo TG. Managed care for congestive heart failure:
influence of payer status on process of care, resource utilization, and
short-term outcomes. Am Heart J 1998;136:553e61.
54. Tsuchihashi M, Tsutsui H, Kodama K, Kasagi F, Setoguchi S,
Mohr M, et al. Medical and socioenvironmental predictors of hospital
readmission in patients with congestive heart failure. Am Heart J
2001;142:E7.
55. Faris R, Purcell H, Henein MY, Coats AJ. Clinical depression is com-
mon and significantly associated with reduced survival in patients
with nonischaemic heart failure. Eur J Heart Fail 2002;4:541e51.
56. Evangelista LS, Doering LV, Dracup K. Usefulness of a history of to-
bacco and alcohol use in predicting multiple heart failure readmis-
sions among veterans. Am J Cardiol 2000;86:1339e42.
57. Fonarow GC, AbrahamWT, Albert NM, Stough WG, Gheorghiade M,
Greenberg BH, et al. A smoker’s paradox in patients hospitalized for
heart failure: findings from OPTIMIZE-HF. Eur Heart J 2008;29:
1983e91.
58. Babayan ZV,McNamara RL, Nagajothi N, Kasper EK, Armenian HK,
PoweNR, et al. Predictors of cause-specific hospital readmission in pa-
tients with heart failure. Clin Cardiol 2003;26:411e8.59. Ezekowitz JA, Bakal JA, Kaul P, Westerhout CM, Armstrong PW.
Acute heart failure in the emergency department: short and
long-term outcomes of elderly patients with heart failure. Eur J Heart
Fail 2008;10:308e14.
60. Felker GM, Gattis WA, Leimberger JD, Adams KF, Cuffe MS,
Gheorghiade M, et al. Usefulness of anemia as a predictor of death
and rehospitalization in patients with decompensated heart failure.
Am J Cardiol 2003;92:625e8.
61. Perna ER, Macin SM, Cimbaro Canella JP, Alvarenga PM, Rios NG,
Pantich R, et al. Minor myocardial damage detected by troponin T is
a powerful predictor of long-term prognosis in patients with acute de-
compensated heart failure. Int J Cardiol 2005;99:253e61.

64 Journal of Cardiac Failure Vol. 17 No. 1 January 2011
62. Pernenkil R, Vinson JM, Shah AS, Beckham V, Wittenberg C,
Rich MW. Course and prognosis in patients O or 5 70 years of
age with congestive heart failure and normal versus abnormal left
ventricular ejection fraction. Am J Cardiol 1997;79:216e9.63. Harjai KJ, Nunez E, Turgut T, Shah MP, Humphrey JS, Newman J,
et al. The independent effects of left ventricular ejection fraction
on short-term outcomes and resource utilization following hospitali-
zation for heart failure. Clin Cardiol 1999;22:184e90.64. DautermanKW,GoAS,Rowell R,Gebretsadik T, Gettner S,Massie BM.
Congestive heart failure with preserved systolic function in a statewide
sample of community hospitals. J Card Fail 2001;7:221e8.65. Malki Q, Sharma ND, Afzal A, Ananthsubramaniam K, Abbas A,
JacobsonG, et al. Clinical presentation, hospital length of stay, and read-
mission rate in patients with heart failure with preserved and decreased
left ventricular systolic function. Clin Cardiol 2002;25:149e52.66. MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL,
Young JB, et al. Impact of diabetes on outcomes in patients with low
and preserved ejection fraction heart failure: an analysis of the Cande-
sartan inHeart Failure:Assessment ofReduction inMortality andMor-
bidity (CHARM) programme. Eur Heart J 2008;29:1377e85.
67. Fonarow GC, Stough WG, Abraham WT, Albert NM,
Gheorghiade M, Greenberg BH, et al. Characteristics, treatments,
and outcomes of patients with preserved systolic function hospital-
ized for heart failure: a report from the OPTIMIZE-HF Registry.
J Am Coll Cardiol 2007;50:768e77.
68. Ahmed A, Roseman JM, Duxbury AS, Allman RM, DeLong JF. Cor-
relates and outcomes of preserved left ventricular systolic function
among older adults hospitalized with heart failure. Am Heart J
2002;144:365e72.
69. Smith GL, Masoudi FA, Vaccarino V, Radford MJ, Krumholz HM.
Outcomes in heart failure patients with preserved ejection fraction:
mortality, readmission, and functional decline. J Am Coll Cardiol
2003;41:1510e8.
70. Tsutsui H, Tsuchihashi M, Takeshita A. Mortality and readmission of
hospitalized patientswith congestive heart failure and preserved versus
depressed systolic function. Am J Cardiol 2001;88:530e3.
71. Brophy JM, Dagenais GR, McSherry F, Williford W, Yusuf S. A mul-
tivariate model for predicting mortality in patients with heart failure
and systolic dysfunction. Am J Med 2004;116:300e4.
72. Levy WC, Mozaffarian D, Linker DT, Sutradhar SC, Anker SD,
Cropp AB, et al. The Seattle Heart Failure Model: prediction of sur-
vival in heart failure. Circulation 2006;113:1424e33.
73. Felker GM, Leimberger JD, Califf RM, Cuffe MS, Massie BM,
Adams KF Jr, et al. Risk stratification after hospitalization for de-
compensated heart failure. J Card Fail 2004;10:460e6.
74. Filippatos G, Rossi J, Lloyd-Jones DM, Stough WG, Ouyang J,
Shin DD, et al. Prognostic value of blood urea nitrogen in patients hos-
pitalized with worsening heart failure: insights from the Acute and
Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic
Heart Failure (ACTIV in CHF) study. J Card Fail 2007;13:360e4.
75. Pocock SJ, Wang D, Pfeffer MA, Yusuf S, McMurray JJ,
Swedberg KB, et al. Predictors of mortality and morbidity in patients
with chronic heart failure. Eur Heart J 2006;27:65e75.
76. Bettencourt P, Azevedo A, Pimenta J, Frioes F, Ferreira S, Ferreira A.
N-Terminal-pro-brain natriuretic peptide predicts outcome after hospi-
tal discharge in heart failure patients. Circulation 2004;110:2168e74.77. Kingwell BA, Thompson JM, Kaye DM, McPherson GA,
Jennings GL, Esler MD. Heart rate spectral analysis, cardiac norepi-
nephrine spillover, and muscle sympathetic nerve activity during hu-
man sympathetic nervous activation and failure. Circulation 1994;90:
234e40.
78. Stefenelli T, Bergler-Klein J, Globits S, Pacher R, Glogar D. Heart
rate behaviour at different stages of congestive heart failure. Eur
Heart J 1992;13:902e7.
79. Triposkiadis F, Karayannis G, Giamouzis G, Skoularigis J,
Louridas G, Butler J. The sympathetic nervous system in heart failure
physiology, pathophysiology, and clinical implications. J Am Coll
Cardiol 2009;54:1747e62.
80. Armola RR, Topp R. Variables that discriminate length of stay and
readmission within 30 days among heart failure patients. Lippincotts
Case Manage 2001;6:246e55.
81. Feola M, Aspromonte N, Milani L, Bobbio M, Bardellotto S,
Barro S, et al. Plasma brain natriuretic peptide predicts short-term
clinical outcome in heart failure patients with restrictive filling pat-
tern. J Card Fail 2008;14:420e5.
82. Gackowski A, Isnard R, Golmard JL, Pousset F, Carayon A,
Montalescot G, et al. Comparison of echocardiography and plasma
B-type natriuretic peptide for monitoring the response to treatment
in acute heart failure. Eur Heart J 2004;25:1788e96.83. Darze ES, Latado AL, Guimaraes AG, Guedes RA, Santos AB, de
Moura SS, et al. Acute pulmonary embolism is an independent pre-
dictor of adverse events in severe decompensated heart failure pa-
tients. Chest 2007;131:1838e43.
84. Rodriguez-Artalejo F, Guallar-Castillon P, Pascual CR, Otero CM,
Montes AO, Garcia AN, et al. Health-related quality of life as a pre-
dictor of hospital readmission and death among patients with heart
failure. Arch Intern Med 2005;165:1274e9.
85. Rodriguez-Artalejo F, Guallar-Castillon P, Herrera MC, Otero CM,
Chiva MO, Ochoa CC, et al. Social network as a predictor of hospital
readmission and mortality among older patients with heart failure.
J Card Fail 2006;12:621e7.86. Young JB, Abraham WT, Albert NM, Gattis Stough W,
Gheorghiade M, Greenberg BH, et al. Relation of low hemoglobin
and anemia to morbidity and mortality in patients hospitalized with
heart failure (insight from the OPTIMIZE-HF registry). Am J Cardiol
2008;101:223e30.
87. Kosiborod M, Smith GL, Radford MJ, Foody JM, Krumholz HM.
The prognostic importance of anemia in patients with heart failure.
Am J Med 2003;114:112e9.
88. Gheorghiade M, Abraham WT, Albert NM, Gattis Stough W,
Greenberg BH, O’Connor CM, et al. Relationship between admission
serum sodium concentration and clinical outcomes in patients hospi-
talized for heart failure: an analysis from the OPTIMIZE-HF registry.
Eur Heart J 2007;28:980e8.
89. Berry C, Brett M, Stevenson K, McMurray JJ, Norrie J. Nature and
prognostic importance of abnormal glucose tolerance and diabetes in
acute heart failure. Heart 2008;94:296e304.
90. Gerstein HC, Swedberg K, Carlsson J, McMurray JJV,
Michelson EL, Olofsson B, et al. The hemoglobin A1c level as a pro-
gressive risk factor for cardiovascular death, hospitalization for heart
failure, or death in patients with chronic heart failure: an analysis of
the Candesartan in Heart Failure: Assessment of Reduction in Mor-
tality and Morbidity (CHARM) Program. Arch Intern Med 2008;
168:1699e704.
91. Valle R, Aspromonte N, Carbonieri E, d’Eri A, Feola M,
Giovinazzo P, et al. Fall in readmission rate for heart failure after im-
plementation of B-type natriuretic peptide testing for discharge deci-
sion: a retrospective study. Int J Cardiol 2008;126:400e6.
92. Shenkman HJ, Zareba W, Bisognano JD. Comparison of prognostic
significance of amino-terminal pro-brain natriuretic peptide versus
blood urea nitrogen for predicting events in patients hospitalized
for heart failure. Am J Cardiol 2007;99:1143e5.
93. Giamouzis G, Kalogeropoulos AP, Georgiopoulou VV, Agha SA,
Rashad MA, Laskar SR, et al. Incremental value of renal function
in risk prediction with the Seattle Heart Failure Model. Am Heart J
2009;157:299e305.
94. Niizeki T, Takeishi Y, Arimoto T, Okuyama H, Nozaki N, Hirono O,
et al. Hyperuricemia associated with high cardiac event rates in the
elderly with chronic heart failure. J Cardiol 2006;47:219e28.
95. Pimenta JM, Almeida R, Araujo JP, Azevedo A, Frioes F, Rocha-
Goncalves F, et al. Amino terminal B-type natriuretic peptide, renal
function, and prognosis in acute heart failure: a hospital cohort study.
J Card Fail 2007;13:275e80.
96. Green SM, Redmond P, Januzzi JL, Aleryani S, Lee-
Lewandrowski E, Sluss P, et al. The impact of amino-terminal proebrain natriuretic peptide testing on hospital length of stay and

Risk Factors for Hospitalization in Heart Failure � Giamouzis et al 65
morbidity in patients with acute decompensated heart failure. Arch
Pathol Lab Med 2007;131:473e6.
97. FonarowGC, PeacockWF, Phillips CO,GivertzMM,LopatinM.Admis-
sionB-type natriuretic peptide levels and in-hospitalmortality in acute de-
compensated heart failure. J Am Coll Cardiol 2007;49:1943e50.
98. Kirk V, Bay M, Parner J, Krogsgaard K, Herzog TM, Boesgaard S,
et al. N-Terminal proBNP and mortality in hospitalised patients
with heart failure and preserved vs. reduced systolic function: data
from the prospective Copenhagen Hospital Heart Failure study
(CHHF). Eur J Heart Fail 2004;6:335e41.
99. Fonarow GC, Peacock WF, Horwich TB, Phillips CO, Givertz MM,
Lopatin M, et al. Usefulness of B-type natriuretic peptide and cardiac
troponin levels to predict in-hospital mortality from ADHERE. Am J
Cardiol 2008;101:231e7.
100. Harrison A, Morrison LK, Krishnaswamy P, Kazanegra R, Clopton P,
Dao Q, et al. B-Type natriuretic peptide predicts future cardiac events
in patients presenting to the emergency department with dyspnea.
Ann Emerg Med 2002;39:131e8.
101. Fisher C, Berry C, Blue L, Morton JJ, McMurray J. N-terminal pro B
type natriuretic peptide, but not the new putative cardiac hormone re-
laxin, predicts prognosis in patients with chronic heart failure. Heart
2003;89:879e81.
102. Niizeki T, Takeishi Y, Arimoto T, Takahashi T, Okuyama H,
Takabatake N, et al. Combination of heart-type fatty acid binding
protein and brain natriuretic peptide can reliably risk stratify patients
hospitalized for chronic heart failure. Circ J 2005;69:922e7.103. Cheng V, Kazanagra R, Garcia A, Lenert L, Krishnaswamy P,
Gardetto N, et al. A rapid bedside test for B-type peptide predicts
treatment outcomes in patients admitted for decompensated heart
failure: a pilot study. J Am Coll Cardiol 2001;37:386e91.104. Valle R, Aspromonte N, Giovinazzo P, Carbonieri E, Chiatto M,
di Tano G, et al. B-Type natriuretic peptideeguided treatment for
predicting outcome in patients hospitalized in sub-intensive care
unit with acute heart failure. J Card Fail 2008;14:219e24.105. Ferreira S, Almeida R, Guerrero H, Lourenco-Ferreira S, Fonseca L,
Rocha R, et al. Prognosis of decompensated heart failure: role of NT-
proBNP. Rev Port Cardiol 2007;26:535e45.106. Logeart D, Thabut G, Jourdain P, Chavelas C, Beyne P, Beauvais F,
et al. Predischarge B-type natriuretic peptide assay for identifying pa-
tients at high risk of re-admission after decompensated heart failure.
J Am Coll Cardiol 2004;43:635e41.107. Hamada Y, Tanaka N, Murata K, Takaki A, Wada Y, Oyama R, et al.
Significance of predischarge BNP on one-year outcome in decom-
pensated heart failuredcomparative study with echo-Doppler in-
dexes. J Card Fail 2005;11:43e9.108. Cournot M, Leprince P, Destrac S, Ferrieres J. Usefulness of in-
hospital change in B-type natriuretic peptide levels in predicting
long-term outcome in elderly patients admitted for decompensated
heart failure. Am J Geriatr Cardiol 2007;16:8e14.
109. Verdiani V, Ognibene A, Rutili MS, Lombardo C, Bacci F, Terreni A,
et al. NT-ProBNP reduction percentage during hospital stay predicts
long-term mortality and readmission in heart failure patients. J Car-
diovasc Med (Hagerstown) 2008;9:694e9.
110. Cournot M, Mourre F, Castel F, Ferrieres J, Destrac S. Optimization
of the use of B-type natriuretic peptide levels for risk stratification at
discharge in elderly patients with decompensated heart failure. Am
Heart J 2008;155:986e91.
111. Nishii M, Inomata T, Takehana H, Naruke T, Yanagisawa T,
Moriguchi M, et al. Prognostic utility of B-type natriuretic peptide
assessment in stable low-risk outpatients with nonischemic cardio-
myopathy after decompensated heart failure. J Am Coll Cardiol
2008;51:2329e35.
112. Ishii J, Cui W, Kitagawa F, Kuno T, Nakamura Y, Naruse H, et al.
Prognostic value of combination of cardiac troponin T and B-type na-
triuretic peptide after initiation of treatment in patients with chronic
heart failure. Clin Chem 2003;49:2020e6.
113. Pfister R, Diedrichs H, Schiedermair A, Rosenkranz S, Hellmich M,
Erdmann E, et al. Prognostic impact of NT-proBNP and renal
function in comparison to contemporary multi-marker risk scores
in heart failure patients. Eur J Heart Fail 2008;10:315e20.
114. Giamouzis G, Giannakoulas G, Tsarpalis K, Agha SA,
Georgiopoulou V, Kalogeropoulos A, et al. Natriuretic peptideeguided levosimendan therapy for heart failure: a promising new ap-
proach. Int J Cardiol 2008;128:91e3. author reply 94e6.
115. Dokainish H, Zoghbi WA, Ambriz E, Lakkis NM, Quinones MA,
Nagueh SF. Comparative cost-effectiveness of B-type natriuretic pep-
tide and echocardiography for predicting outcome in patients with
congestive heart failure. Am J Cardiol 2006;97:400e3.
116. Troughton RW, Frampton CM, Yandle TG, Espiner EA,
Nicholls MG, Richards AM. Treatment of heart failure guided by
plasma aminoterminal brain natriuretic peptide (N-BNP) concentra-
tions. Lancet 2000;355(9210):1126e30.
117. Pfisterer M, Buser P, Rickli H, Gutmann M, Erne P, Rickenbacher P,
et al. BNP-guided vs symptom-guided heart failure therapy: the Trial
of Intensified vs Standard Medical Therapy in Elderly Patients With
Congestive Heart Failure (TIME-CHF) randomized trial. JAMA
2009;301:383e92.118. Jourdain P, Jondeau G, Funck F, Gueffet P, Le Helloco A, Donal E,
et al. Plasma brain natriuretic peptideeguided therapy to improve
outcome in heart failure: the STARS-BNP multicenter study. J Am
Coll Cardiol 2007;49:1733e9.119. Nishio Y, Sato Y, Taniguchi R, Shizuta S, Doi T, Morimoto T, et al.
Cardiac troponin T vs other biochemical markers in patients with
congestive heart failure. Circ J 2007;71:631e5.120. Xue C, Feng Y, Wo J, Li Y. Prognostic value of high-sensitivity
C-reactive protein in patients with chronic heart failure. N Z Med J
2006;119(1245):U2314.
121. Setsuta K, Seino Y, Takahashi N, Ogawa T, Sasaki K, Harada A, et al.
Clinical significance of elevated levels of cardiac troponin T in pa-
tients with chronic heart failure. Am J Cardiol 1999;84:608e11.
122. del Carlo CH, Pereira-Barretto AC, Cassaro-Strunz C, Latorre
Mdo R, Ramires JA. Serial measure of cardiac troponin T levels
for prediction of clinical events in decompensated heart failure.
J Card Fail 2004;10:43e8.
123. Alonso-Martinez JL, Llorente-Diez B, Echegaray-Agara M,
Olaz-Preciado F, Urbieta-Echezarreta M, Gonzalez-Arencibia C.
C-Reactive protein as a predictor of improvement and readmis-
sion in heart failure. Eur J Heart Fail 2002;4:331e6.
124. Anand IS, Latini R, Florea VG, Kuskowski MA, Rector T, Masson S,
et al. C-Reactive protein in heart failure: prognostic value and the
effect of valsartan. Circulation 2005;112:1428e34.
125. Tang WH, Shrestha K, van Lente F, Troughton RW, Martin MG,
Borowski AG, et al. Usefulness of C-reactive protein and left ventric-
ular diastolic performance for prognosis in patients with left ventric-
ular systolic heart failure. Am J Cardiol 2008;101:370e3.
126. Iwaoka M, Obata JE, Abe M, Nakamura T, Kitta Y, Kodama Y, et al.
Association of low serum levels of apolipoprotein A-I with adverse
outcomes in patients with nonischemic heart failure. J Card Fail
2007;13:247e53.
127. Giamouzis G, Butler J. Relationship between heart failure and lipids:
the paradigm continues to evolve. J Card Fail 2007;13:254e8.
128. Arimoto T, Takeishi Y, Niizeki T, Takabatake N, Okuyama H,
Fukui A, et al. Cystatin C, a novel measure of renal function, is an
independent predictor of cardiac events in patients with heart failure.
J Card Fail 2005;11:595e601.
129. Koyama Y, Takeishi Y, Arimoto T, Niizeki T, Shishido T,
Takahashi H, et al. High serum level of pentosidine, an advanced
glycation end product (AGE), is a risk factor of patients with heart
failure. J Card Fail 2007;13:199e206.
130. Koyama Y, Takeishi Y, Niizeki T, Suzuki S, Kitahara T, Sasaki T, et al.
Soluble Receptor for advanced glycation end products (RAGE) is
a prognostic factor for heart failure. J Card Fail 2008;14:133e9.
131. Arimoto T, Takeishi Y, Shiga R, Fukui A, Tachibana H, Nozaki N,
et al. Prognostic value of elevated circulating heart-type fatty acid
binding protein in patients with congestive heart failure. J Card
Fail 2005;11:56e60.

66 Journal of Cardiac Failure Vol. 17 No. 1 January 2011
132. Ruiz-Ruiz FJ, Ruiz-Laiglesia FJ, Samperiz-Legarre P, Lasierra-
Diaz P, Flamarique-Pascual A, Morales-Rull JL, et al. Propeptide
of procollagen type I (PIP) and outcomes in decompensated heart
failure. Eur J Intern Med 2007;18:129e34.133. Danciu SC, Gonzalez J, Gandhi N, Sadhu S, Herrera CJ, Kehoe R.
Comparison of six-month outcomes and hospitalization rates in heart
failure patients with and without preserved left ventricular ejection
fraction and with and without intraventricular conduction defect.
Am J Cardiol 2006;97:256e9.
134. Wang NC, Maggioni AP, Konstam MA, Zannad F, Krasa HB,
Burnett JC Jr, et al. Clinical implications of QRS duration in patients
hospitalized with worsening heart failure and reduced left ventricular
ejection fraction. JAMA 2008;299:2656e66.
135. Giamouzis G, Sui X, Love TE, Butler J, Young JB, Ahmed A. A
propensity-matched study of the association of cardiothoracic ratio
with morbidity and mortality in chronic heart failure. Am J Cardiol
2008;101:343e7.
136. Ofili EO,MayberryR,Alema-MensahE, SaleemS,HamiraniK, JonesC,
et al. Gender differences and practice implications of risk factors for fre-
quent hospitalization for heart failure in an urban center serving predom-
inantly African-American patients. Am J Cardiol 1999;83:1350e5.
137. Agha SA, Kalogeropoulos AP, Shih J, Georgiopoulou VV,
Giamouzis G, Anarado P, et al. Echocardiography and risk prediction
in advanced heart failure: incremental value over clinical markers.
J Card Fail 2009;15:586e92.
138. Popescu BA, Popescu AC, Antonini-Canterin F, Rubin D,
Cappelletti P, Piazza R, et al. Prognostic role of left atrial volume
in elderly patients with symptomatic stable chronic heart failure:
comparison with left ventricular diastolic dysfunction and B-type
natriuretic peptide. Echocardiography 2007;24:1035e43.
139. Shalaby A, Voigt A, El-Saed A, Saba S. Usefulness of pulmonary ar-
tery pressure by echocardiography to predict outcome in patients re-
ceiving cardiac resynchronization therapy heart failure. Am J Cardiol
2008;101:238e41.
140. Dokainish H, Sengupta R, Patel R, Lakkis N. Usefulness of right ven-
tricular tissue Doppler imaging to predict outcome in left ventricular
heart failure independent of left ventricular diastolic function. Am J
Cardiol 2007;99:961e5.
141. Cho GY, Song JK, Park WJ, Han SW, Choi SH, Doo YC, et al. Me-
chanical dyssynchrony assessed by tissue Doppler imaging is a pow-
erful predictor of mortality in congestive heart failure with normal
QRS duration. J Am Coll Cardiol 2005;46:2237e43.
142. Boveda S, Galinier M, Pathak A, Fourcade J, Dongay B,
Benchendikh D, et al. Prognostic value of heart rate variability in
time domain analysis in congestive heart failure. J Interv Card Elec-
trophysiol 2001;5:181e7.
143. Adamson PB, Smith AL, Abraham WT, Kleckner KJ, Stadler RW,
Shih A, et al. Continuous autonomic assessment in patients with
symptomatic heart failure: prognostic value of heart rate variability
measured by an implanted cardiac resynchronization device. Circula-
tion 2004;110:2389e94.
144. Ho KK, Moody GB, Peng CK, Mietus JE, Larson MG, Levy D, et al.
Predicting survival in heart failure case and control subjects by use of
fully automated methods for deriving nonlinear and conventional in-
dices of heart rate dynamics. Circulation 1997;96:842e8.
145. la Rovere MT, Pinna GD, Maestri R, Mortara A, Capomolla S, Febo O,
et al. Short-term heart rate variability strongly predicts sudden cardiac
death in chronic heart failure patients. Circulation 2003;107:565e70.
146. Hadase M, Azuma A, Zen K, Asada S, Kawasaki T, Kamitani T, et al.
Very low frequency power of heart rate variability is a powerful pre-
dictor of clinical prognosis in patients with congestive heart failure.
Circ J 2004;68:343e7.
147. Arena R, Guazzi M, Myers J, Peberdy MA. Prognostic value of heart
rate recovery in patients with heart failure. Am Heart J 2006;151
(851):e7e13.
148. Brown AM, Cleland JG. Influence of concomitant disease on patterns
of hospitalization in patients with heart failure discharged from Scot-
tish hospitals in 1995. Eur Heart J 1998;19:1063e9.
149. Braunstein JB, Anderson GF, Gerstenblith G, Weller W, Niefeld M,
Herbert R, et al. Noncardiac comorbidity increases preventable hos-
pitalizations and mortality among Medicare beneficiaries with
chronic heart failure. J Am Coll Cardiol 2003;42:1226e33.150. Middlekauff HR, Stevenson WG, Stevenson LW. Prognostic signifi-
cance of atrial fibrillation in advanced heart failure. A study of 390
patients. Circulation 1991;84:40e8.
151. Rivero-Ayerza M, Scholte op Reimer W, Lenzen M, Theuns DA,
Jordaens L, Komajda M, et al. New-onset atrial fibrillation is an in-
dependent predictor of in-hospital mortality in hospitalized heart fail-
ure patients: results of the EuroHeart Failure survey. Eur Heart J
2008;29:1618e24.
152. Ahmed A, Thornton P, Perry GJ, Allman RM, DeLong JF. Impact of
atrial fibrillation on mortality and readmission in older adults hospi-
talized with heart failure. Eur J Heart Fail 2004;6:421e6.153. Olsson LG, Swedberg K, Ducharme A, Granger CB, Michelson EL,
McMurray JJ, et al. Atrial fibrillation and risk of clinical events in
chronic heart failure with and without left ventricular systolic dys-
function: results from the Candesartan in Heart FailureeAssessment
of Reduction in Mortality and Morbidity (CHARM) program. J Am
Coll Cardiol 2006;47:1997e2004.
154. Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, et al.
Rhythm control versus rate control for atrial fibrillation and heart
failure. N Engl J Med 2008;358:2667e77.
155. Greenberg BH, Abraham WT, Albert NM, Chiswell K, Clare R,
StoughWG, et al. Influence of diabetes on characteristics and outcomes
in patients hospitalized with heart failure: a report from the Organized
Program to Initiate Lifesaving Treatment in Hospitalized Patients
With Heart Failure (OPTIMIZE-HF). Am Heart J 2007;154: 277e1e8.
156. Giamouzis G, Triposkiadis F, Butler J. Metformin use in patients
with diabetes mellitus and heart failure: friend or foe? J Card Fail
2010;16:207e10.
157. Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE,
Carney RM. A multidisciplinary intervention to prevent the readmis-
sion of elderly patients with congestive heart failure. N Engl J Med
1995;333:1190e5.
158. Felker GM, Adams KF Jr, Gattis WA, O’Connor CM. Anemia as
a risk factor and therapeutic target in heart failure. J Am Coll Cardiol
2004;44:959e66.
159. Berry C, Norrie J, Hogg K, Brett M, Stevenson K, McMurray JJ. The
prevalence, nature, and importance of hematologic abnormalities in
heart failure. Am Heart J 2006;151:1313e21.
160. Luthi JC, Flanders WD, Burnier M, Burnand B, McClellan WM.
Anemia and chronic kidney disease are associated with poor out-
comes in heart failure patients. BMC Nephrol 2006;7:3.
161. Kosiborod M, Curtis JP, Wang Y, Smith GL, Masoudi FA, Foody JM,
et al. Anemia and outcomes in patients with heart failure: a study
from the National Heart Care Project. Arch Intern Med 2005;165:
2237e44.
162. Milo-Cotter O, Cotter G, Weatherley BD, Adams KF, Kaluski E,
Uriel N, et al. Hyponatraemia in acute heart failure is a marker of in-
creased mortality but not when associated with hyperglycaemia. Eur
J Heart Fail 2008;10:196e200.
163. Akhter MW, Aronson D, Bitar F, Khan S, Singh H, Singh RP, et al.
Effect of elevated admission serum creatinine and its worsening on
outcome in hospitalized patients with decompensated heart failure.
Am J Cardiol 2004;94:957e60.
164. McClellan WM, Langston RD, Presley R. Medicare patients with
cardiovascular disease have a high prevalence of chronic kidney dis-
ease and a high rate of progression to end-stage renal disease. J Am
Soc Nephrol 2004;15:1912e9.
165. Metra M, Nodari S, Parrinello G, Bordonali T, Bugatti S, Danesi R,
et al. Worsening renal function in patients hospitalised for acute heart
failure: clinical implications and prognostic significance. Eur J Heart
Fail 2008;10:188e95.
166. Logeart D, Tabet JY, Hittinger L, Thabut G, Jourdain P, Maison P, et al.
Transient worsening of renal function during hospitalization for acute
heart failure alters outcome. Int J Cardiol 2008;127:228e32.

Risk Factors for Hospitalization in Heart Failure � Giamouzis et al 67
167. Mujib M, Giamouzis G, Agha SA, Aban I, Sathiakumar N,
Ekundayo OJ, et al. Epidemiology of stroke in chronic heart failure
patients with normal sinus rhythm: findings from the DIG stroke sub-
study. Int J Cardiol 2009 May 11. [Epub ahead of print].
168. Mascarenhas J, Lourenco P, Lopes R, Azevedo A, Bettencourt P. Chronic
obstructivepulmonarydisease in heart failure. Prevalence, therapeutic and
prognostic implications. Am Heart J 2008;155:521e5.
169. Kasai T, Narui K,Dohi T,YanagisawaN, Ishiwata S, OhnoM, et al. Prog-
nosis of patientswith heart failure and obstructive sleep apnea treatedwith
continuous positive airway pressure. Chest 2008;133:690e6.
170. Parissis JT, Nikolaou M, Farmakis D, Bistola V, Paraskevaidis IA,
Adamopoulos S, et al. Clinical and prognostic implications of self-
rating depression scales and plasma B-type natriuretic peptide in hos-
pitalised patients with chronic heart failure. Heart 2008;94:585e9.
171. Lesman-Leegte I, Jaarsma T, Sanderman R, Linssen G, van
Veldhuisen DJ. Depressive symptoms are prominent among elderly
hospitalised heart failure patients. Eur J Heart Fail 2006;8:634e40.
172. Rumsfeld JS, Havranek E, Masoudi FA, Peterson ED, Jones P,
Tooley JF, et al. Depressive symptoms are the strongest predictors
of short-term declines in health status in patients with heart failure.
J Am Coll Cardiol 2003;42:1811e7.
173. Vaccarino V, Kasl SV, Abramson J, Krumholz HM. Depressive
symptoms and risk of functional decline and death in patients with
heart failure. J Am Coll Cardiol 2001;38:199e205.
174. Jiang W, Alexander J, Christopher E, Kuchibhatla M, Gaulden LH,
Cuffe MS, et al. Relationship of depression to increased risk of mor-
tality and rehospitalization in patients with congestive heart failure.
Arch Intern Med 2001;161:1849e56.
175. O’Loughlin C, Murphy NF, Conlon C, O’Donovan A, Ledwidge M,
McDonald K. Quality of life predicts outcome in a heart failure dis-
ease management program. Int J Cardiol 2010;139:60e7.
176. Mejhert M, Kahan T, Persson H, Edner M. Predicting readmissions
and cardiovascular events in heart failure patients. Int J Cardiol
2006;109:108e13.177. Krumholz HM, Butler J, Miller J, Vaccarino V, Williams CS, Mendes de
LeonCF, et al. Prognostic importance of emotional support for elderly pa-
tients hospitalized with heart failure. Circulation 1998;97:958e64.178. Butler J, Arbogast PG, Daugherty J, Jain MK, Ray WA, Griffin MR.
Outpatient utilization of angiotensin-converting enzyme inhibitors
among heart failure patients after hospital discharge. J Am Coll Car-
diol 2004;43:2036e43.179. Krumholz HM, Amatruda J, Smith GL, Mattera JA, Roumanis SA,
Radford MJ, et al. Randomized trial of an education and support in-
tervention to prevent readmission of patients with heart failure. J Am
Coll Cardiol 2002;39:83e9.180. Giordano A, Scalvini S, Zanelli E, Corra U, Longobardi GL,
Ricci VA, et al. Multicenter randomised trial on home-based telema-
nagement to prevent hospital readmission of patients with chronic
heart failure. Int J Cardiol 2009;131:192e9.
181. Philbin EF, DiSalvo TG. Prediction of hospital readmission for heart
failure: development of a simple risk score based on administrative
data. J Am Coll Cardiol 1999;33:1560e6.182. O’ConnorCM,StoughWG,GallupDS,HasselbladV,GheorghiadeM.
Demographics, clinical characteristics, and outcomes of patients hos-
pitalized for decompensated heart failure: observations from the
IMPACT-HF registry. J Card Fail 2005;11:200e5.183. Yamokoski LM, Hasselblad V, Moser DK, Binanay C, Conway GA,
Glotzer JM, et al. Prediction of rehospitalization and death in severe
heart failure by physicians and nurses of the ESCAPE trial. J Card
Fail 2007;13:8e13.184. Keenan PS, Normand S-LT, Lin Z, Drye EE, Bhat KR, Ross JS, et al. An
administrative claimsmeasure suitable for profiling hospital performance
on the basis of 30-day all-cause readmission rates among patients with
heart failure. Circ Cardiovasc Qual Outcomes 2008;1:29e37.
185. Mehta RH, Rogers JG, Hasselblad V, Tasissa G, Binanay C,
Califf RM, et al. Association of weight change with subsequent out-
comes in patients hospitalized with acute decompensated heart fail-
ure. Am J Cardiol 2009;103:76e81.
186. Blair JE, Khan S, Konstam MA, Swedberg K, Zannad F,
Burnett JC Jr, et al. Weight changes after hospitalization for worsen-
ing heart failure and subsequent re-hospitalization and mortality in
the EVEREST trial. Eur Heart J 2009;30:1666e73.187. Gheorghiade M, Follath F, Ponikowski P, Barsuk JH, Blair JE,
Cleland JG, et al. Assessing and grading congestion in acute heart
failure: a scientific statement from the acute Heart Failure Committee
of the Heart Failure Association of the European Society of Cardiol-
ogy and endorsed by the European Society of Intensive Care Medi-
cine. Eur J Heart Fail 2010;12:423e33.
188. Aurigemma GP, Gaasch WH. Clinical practice. Diastolic heart fail-
ure. N Engl J Med 2004;351:1097e105.
189. Yu DS, Thompson DR, Lee DT. Disease management programmes
for older people with heart failure: crucial characteristics which im-
prove post-discharge outcomes. Eur Heart J 2006;27:596e612.190. Gohler A, Januzzi JL, Worrell SS, Osterziel KJ, Gazelle GS, Dietz R,
et al. A systematic meta-analysis of the efficacy and heterogeneity of
disease management programs in congestive heart failure. J Card Fail
2006;12:554e67.191. Gonseth J,Guallar-Castillon P,Banegas JR,Rodriguez-Artalejo F. The ef-
fectiveness of disease management programmes in reducing hospital re-
admission in older patients with heart failure: a systematic review and
meta-analysis of published reports. Eur Heart J 2004;25:1570e95.192. Abraham WT, Adams KF, Fonarow GC, Costanzo MR, Berkowitz RL,
LeJemtel TH, et al. In-hospitalmortality in patientswith acute decompen-
sated heart failure requiring intravenous vasoactive medications: an anal-
ysis from the Acute Decompensated Heart Failure National Registry
(ADHERE). J Am Coll Cardiol 2005;46:57e64.
193. Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS,
Ganiats TG, et al. 2009 focused update: ACCF/AHA guidelines for
the diagnosis and management of heart failure in adults: a report
of the American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines: developed in collab-
oration with the International Society for Heart and Lung Transplan-
tation. Circulation 2009;119:1977e2016.
194. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ,
Ponikowski P, Poole-Wilson PA, et al. ESC Guidelines for the diag-
nosis and treatment of acute and chronic heart failure 2008: the Task
Force for the Diagnosis and Treatment of Acute and Chronic Heart
Failure 2008 of the European Society of Cardiology. Developed in
collaboration with the Heart Failure Association of the ESC (HFA)
and endorsed by the European Society of Intensive Care Medicine
(ESICM). Eur Heart J 2008;29:2388e442.
195. Triposkiadis F, Parissis JT, Starling RC, Skoularigis J, Louridas G.
Current drugs and medical treatment algorithms in the management
of acute decompensated heart failure. Expert Opin Investig Drugs
2009;18:695e707.
196. Fonarow GC, Abraham WT, Albert NM, Gattis Stough W,
Gheorghiade M, Greenberg BH, et al. Influence of a performance-
improvement initiative on quality of care for patients hospitalized
with heart failure: results of the Organized Program to Initiate Life-
saving Treatment in Hospitalized Patients With Heart Failure (OPTI-
MIZE-HF). Arch Intern Med 2007;167:1493e502.
197. Rathore SS, Foody JM, Wang Y, Herrin J, Masoudi FA, Havranek EP,
et al. Sex, quality of care, and outcomes of elderly patients hospital-
ized with heart failure: findings from the National Heart Failure Pro-
ject. Am Heart J 2005;149:121e8.
198. Ko DT, Tu JV, Masoudi FA, Wang Y, Havranek EP, Rathore SS, et al.
Quality of care and outcomes of older patients with heart failure hos-
pitalized in the United States and Canada. Arch Intern Med 2005;
165:2486e92.
199. Philbin EF, Rocco TA, Lindenmuth NW, Ulrich K, McCall M,
Jenkins PL, MISCHF Study Investigators. The results of a random-
ized trial of a quality improvement intervention in the care of patients
with heart failure. Am J Med 2000;109:443e9.
200. Chung ES, Lin G, Casey DE Jr, Bartone C, Menon S, Saghir S, et al.
Relationship of a quality measure composite to clinical outcomes for
patients with heart failure. Am J Med Qual 2008;23:168e75.
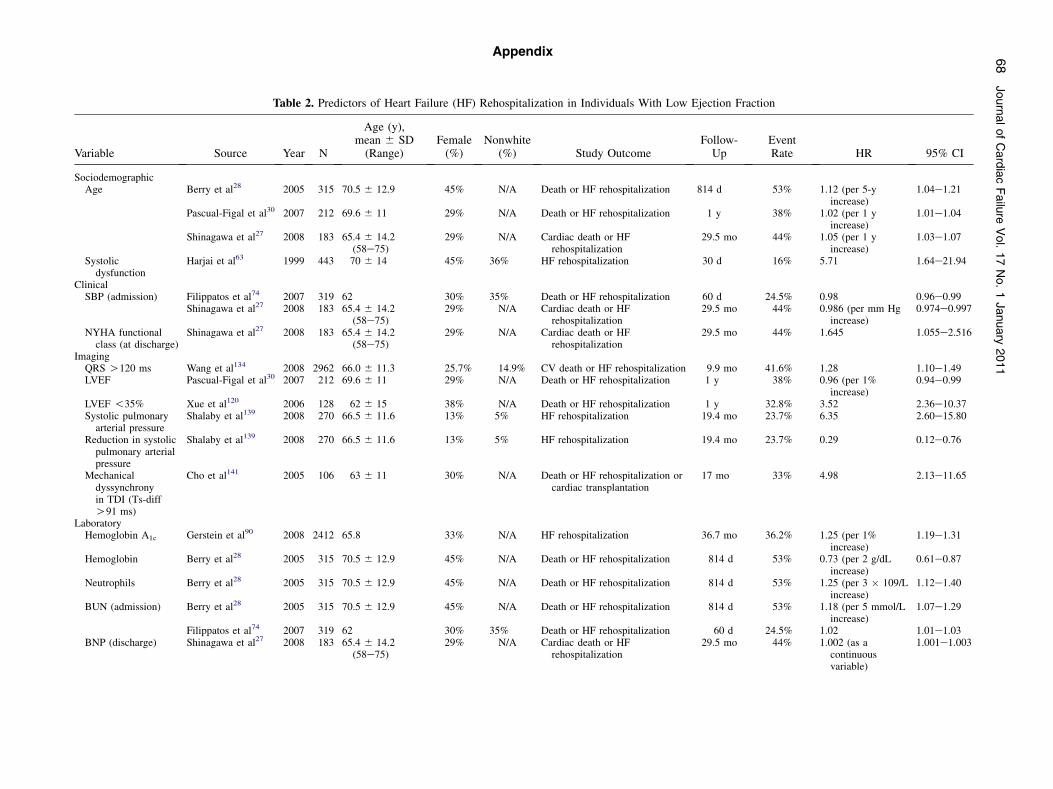
Table 2. Predictors of Heart Failure (HF) Rehospitalization in Individuals With Low Ejec Fraction
Variable Source Year N
Age (y),mean 6 SD(Range)
Female(%)
Nonwhite(%) Study Outcome
Fo
SociodemographicAge Berry et al28 2005 315 70.5 6 12.9 45% N/A Death or HF rehospitalization 81
Pascual-Figal et al30 2007 212 69.6 6 11 29% N/A Death or HF rehospitalization 1
Shinagawa et al27 2008 183 65.4 6 14.2(58e75)
29% N/A Cardiac death or HFrehospitalization
29
Systolicdysfunction
Harjai et al63 1999 443 70 6 14 45% 36% HF rehospitalization 3
ClinicalSBP (admission) Filippatos et al74 2007 319 62 30% 35% Death or HF rehospitalization 6
Shinagawa et al27 2008 183 65.4 6 14.2(58e75)
29% N/A Cardiac death or HFrehospitalization
29
NYHA functionalclass (at discharge)
Shinagawa et al27 2008 183 65.4 6 14.2(58e75)
29% N/A Cardiac death or HFrehospitalization
29
ImagingQRS O120 ms Wang et al134 2008 2962 66.0 6 11.3 25.7% 14.9% CV death or HF rehospitalization 9LVEF Pascual-Figal et al30 2007 212 69.6 6 11 29% N/A Death or HF rehospitalization 1
LVEF !35% Xue et al120 2006 128 62 6 15 38% N/A Death or HF rehospitalization 1Systolic pulmonary
arterial pressureShalaby et al139 2008 270 66.5 6 11.6 13% 5% HF rehospitalization 19
Reduction in systolicpulmonary arterialpressure
Shalaby et al139 2008 270 66.5 6 11.6 13% 5% HF rehospitalization 19
Mechanicaldyssynchronyin TDI (Ts-diffO91 ms)
Cho et al141 2005 106 63 6 11 30% N/A Death or HF rehospitalization orcardiac transplantation
17
LaboratoryHemoglobin A1c Gerstein et al90 2008 2412 65.8 33% N/A HF rehospitalization 36
Hemoglobin Berry et al28 2005 315 70.5 6 12.9 45% N/A Death or HF rehospitalization
Neutrophils Berry et al28 2005 315 70.5 6 12.9 45% N/A Death or HF rehospitalization
BUN (admission) Berry et al28 2005 315 70.5 6 12.9 45% N/A Death or HF rehospitalization
Filippatos et al74 2007 319 62 30% 35% Death or HF rehospitalizationBNP (discharge) Shinagawa et al27 2008 183 65.4 6 14.2
(58e75)29% N/A Cardiac death or HF
rehospitalization29
Appendix 68
Journal
tion
llow-Up
EventRate HR 95% CI
4 d 53% 1.12 (per 5-yincrease)
1.04e1.21
y 38% 1.02 (per 1 yincrease)
1.01e1.04
.5 mo 44% 1.05 (per 1 yincrease)
1.03e1.07
0 d 16% 5.71 1.64e21.94
0 d 24.5% 0.98 0.96e0.99.5 mo 44% 0.986 (per mm Hg
increase)0.974e0.997
.5 mo 44% 1.645 1.055e2.516
.9 mo 41.6% 1.28 1.10e1.49y 38% 0.96 (per 1%
increase)0.94e0.99
y 32.8% 3.52 2.36e10.37.4 mo 23.7% 6.35 2.60e15.80
.4 mo 23.7% 0.29 0.12e0.76
mo 33% 4.98 2.13e11.65
.7 mo 36.2% 1.25 (per 1%increase)
1.19e1.31
814 d 53% 0.73 (per 2 g/dLincrease)
0.61e0.87
814 d 53% 1.25 (per 3 � 109/Lincrease)
1.12e1.40
814 d 53% 1.18 (per 5 mmol/Lincrease)
1.07e1.29
60 d 24.5% 1.02 1.01e1.03.5 mo 44% 1.002 (as a
continuousvariable)
1.001e1.003
ofCardiacFailure
Vol.17No.1January
2011

cTnT (O1.8 mg/L) Tang et al125 2008 136 57 6 14 24% N/A Death, cardiac transplantation,and HF rehospitalization
33 mo N/A 2.61 1.96e4.31
hsCRP (O3.2 mg/L) Tang et al125 2008 136 57 6 14 24% N/A Death, cardiac transplantation,and HF rehospitalization
33 mo N/A 3.81 2.14e9.35
Total bilirubin(admission levelsO1.2 mg/dL)
Shinagawa et al27 2008 183 65.4 6 14.2(58e75)
29% N/A Cardiac death or HFrehospitalization
29.5 mo 44% 1.90 1.32e2.72
ComorbidityDiabetes mellitus MacDonald et al66 2008 7599 66.0 6 11.4 32% 9% HF rehospitalization 37.7 mo 155 per 1,000
patient-y1.64 1.44e1.86
Valve disease Berry et al28 2005 315 70.5 6 12.9 45% N/A Death or HF rehospitalization 814 d 53% 3.72 1.68e8.24Hyperuricemia[discharge UAO7 mg/dL in menand 6 mg/dL inwomen]
Pascual-Figal et al30 2007 212 69.6 6 11 29% N/A Death or HF rehospitalization 1 y 38% 1.64 1.06e2.55
Depression Parissis et al170 2008 156 65 6 12 (35e76) 17% N/A Death or HF rehospitalization 6-mo 39.4% 1.074 (per 1 pointincrement inZung scale)
1.009e1.142
BNP, V-type natriuretic peptide; cTnT, cardiac troponin T; hsCRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; TDI, tissue Doppler imaging; other abbreviations as in Table 1.
Table 3. Predictors of Heart Failure (HF) Rehospitalization in Individuals With Preserved Ejection Fraction
Variable Source Year NAge (y), mean 6
SD (IQR) Female Nonwhite Study OutcomeFollow-UpPeriod
EventRate HR 95% CI
ImagingQRS O120 ms Danciu et al133 2006 217 71 (63-80) 47% 57% Death or rehospitalization 6 mo 56% 1.15 N/ALaboratoryHemoglobin A1c Gerstein et al90 2008 2412 65.8 33% N/A CV death or HF rehospitalization 36.7 mo N/A 1.25 (per 1%
increase)1.20e1.31
Serum sodium Berry et al28 2005 130 72.6 6 12.4 62% N/A Death or HF rehospitalization 814 d 42% 0.60 (per 5 mmol/Lincrease)
0.43e0.84
BUN Berry et al28 2005 130 72.6 6 12.4 62% N/A Death or HF rehospitalization 814 d 42% 1.81, per 5 mmol/Lincrease
1.46e2.24
Serum Creatinine Bettencourt et al36 2007 224 74.6 6 10.5 67% N/A Death or rehospitalization 6 mo 43% 1.33 1.08e1.64NT-pro-BNP (admission-
discharge difference)Bettencourt et al36 2007 224 74.6 6 10.5 67% N/A Death or rehospitalization 6 mo 43% 7.79 2.03e29.86
ComorbidityDiabetes mellitus MacDonald et al66 2008 7599 66.0 6 11.4 32% 9% HF rehospitalization 37.7 mo 117 per 1,000
patient-y2.04 1.68e2.47
Angina pectoris Ofili et al136 1999 1200 64 6 16 (19e99) 51% 94% All-cause rehospitalization 12 mo 56% 1.87 1.06e3.32COPD Berry et al28 2005 130 72.6 6 12.4 62% N/A Death or HF rehospitalization 814 d 42% 9.86 4.48e21.7Valve disease Berry et al28 2005 130 72.6 6 12.4 62% N/A Death or HF rehospitalization 814 d 42% 3.96 1.67e9.38
COPD, chronic obstructive pulmonary disease; IQR, interquartile range; NT-pro-BNP, N-terminal proeB-type natriuretic peptide; other abbreviations as in Table 1.
RiskFactors
forHospita
lizatio
nin
HeartFailure
�Giamouzis
etal
69

Table 4. Predictors of Heart Failure (HF) RehospitalizationdEjection Fraction Unspecified
Variable Source Year N Age (y) Female Nonwhite End Point Follow-UpEventRate HR 95% CI
SociodemographicAge Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 1.24 (per 10-y
increase)1.20e1.28
Koitabashi et al25 2005 427 65.8 6 13.5 36% N/A HF rehospitalization 34 mo 34.9% 1.03 (per 1-yincrease)
1.02e1.05
Lee et al26 2008 668 66 6 12 32.6% 100% Death or HF rehospitalization 2 y 29.6% 1.02 (per 1-yincrease)
1.01e1.04
Ruiz-Ruiz et al132 2007 111 73.4 6 7.9 46.8% N/A HF rehospitalization 21 mo 48.6% 1.059 (per 1-yincrease)
1.006e1.115
Age ($80 y) Kossovsky et al23 2000 442 75.6 6 11.2 48% N/A HF rehospitalization 31 d N/A 3.90 1.30e12.00Gender (female) Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 0.92 0.85e0.98
Mielniczuk et al35 2008 183 55.5 6 15 49% N/A Death or HF rehospitalization 1y 47% 2.43 1.00e4.40Gender (male) Harjai et al32 2001 443 70 6 14 45% 36% HF rehospitalization 30 d 15.8% 2.70 1.40e5.40
Ruiz-Ruiz et al132 2007 111 73.4 6 7.9 46.8% N/A HF rehospitalization 21 mo 48.6% 2.08 1.08e4.00Koitabashi et al25 2005 427 65.8 6 13.5 36% N/A HF rehospitalization 34 mo 34.9% 1.53 1.02e2.28
Race (nonwhite) Afzal et al43 1999 163 66.0 N/A 69% All-cause rehospitalization 6 mo 23.4% 1.83 N/ALee et al26 2008 668 66 6 12 32.6% 100% Death or HF rehospitalization 2 y 29.6% 1.65 1.04e2.63
Race (black) Alexander et al45 1999 90,316 73.2 53% 25% All-cause rehospitalization 1 y 60.1% 1.07 1.04e1.10Rathore et al42 2003 29,732 79.5 6 0.2 60% 11.6% All-cause rehospitalization 1 y 65% 1.09 1.06e1.13
Socioeconomicstatus (expressedas householdincome)
Philbin et al51 2001 41,776 74 6 13 57% 18% HF rehospitalization 6 mo 21.5% 1.18 (lowest v.highestquartile)
1.10e1.26
Socioeconomicstatus (residence-based)
Rathore et al52 2006 25,086 78.8 6 0.1 57.7% 15.5% All-causerehospitalization
1 y 68.0% 1.08 (lowest vshighestquartile)
1.03e1.12
Smoking (current) Evangelista et al56 2000 753 69 6 11.7(33e99)
2% 39.4% Multiple (O1) HF readmissions 1 y 29.2% 1.82 1.17e2.82
Fonarow et al57 2008 48,612 73.1 52% 26% All-cause rehospitalization 60 and 90 d 29% 0.77 0.63e0.94Alcohol use (current) Evangelista et al56 2000 753 69 6 11.7
(33e99)2% 39.4% Multiple (O1) HF readmissions 1 y 29.2% 5.92 3.83e9.13
Alcohol use (history) Faris et al55 2002 396 53 6 15(15e86)
26% 17% Rehospitalization 48 mo Rate, 1.7/patient-year
2.5 1.30e5.00
Living alone Evangelista et al56 2000 753 69 6 11.7(33e99)
2% 39.4% Multiple (O1) HF readmissions 1 y 29.2% 2.09 1.42e3.09
Faris et al55 2002 396 53 6 15(15e86)
26% 17% Rehospitalization 48 mo Rate, 1.7/patient-y
3.6 1.08e12.2
Social network(low vs high)
Rodriguez-Artalejoet al85
2006 371 77.2 6 6.7 58.2% N/A Rehospitalization 6 mo 36.4% 1.98 1.07e3.68
Lack of occupation Tsuchihashi et al54 2001 230 69 6 14 40% N/A HF rehospitalization 1 y 35.0% 2.59 1.22e5.48Faris et al55 2002 396 53 6 15
(15e86)26% 17% Rehospitalization 48 mo Rate, 1.7/
patient-year2.20 1.00e4.80
ClinicalIschemic etiology Babayan et al58 2003 493 N/A N/A N/A All-cause rehospitalization 1 year 56.6% 1.40 1.11e1.79
Evangelista et al56 2000 753 69 6 11.7(33e99)
2% 39.4% Multiple (O1) HF readmissions 1 y 29.2% 3.99 2.58e6.18
Ezekovitz et al59 2008 10,415 79.5 (73e85) 50.4% N/A All-cause rehospitalization 30 d 20.2% 1.36 1.12e1.67Lee et al26 2008 668 66 6 12 32.6% 100% Death or HF rehospitalization 2 y 29.6% 1.62 1.07e2.47
Previous myocardialrevascularization
Kossovsky et al23 2000 442 75.6 6 11.2 48% N/A HFrehospitalization
31 d N/A 3.00 1.50e6.10
70
JournalofCardiacFailure
Vol.17No.1January
2011

Previous MI Perna et al61 2005 184 64.5 6 13.2 39.7% N/A HF rehospitalization 3 y 75% 1.99 1.02e3.90Systolic dysfunction Babayan et al58 2003 493 N/A N/A N/A HF rehospitalization 12 mo N/A 2.44 1.46e4.08
Dauterman et al64 2001 782 78 54% 15% HF rehospitalization 1 y N/A 1.22 1.00e1.50Prior admission for
HF (anytime)Darze et al83 2007 198 69.4 6 13.5 44% N/A Death or rehospitalization 3 mo 46% 3.40 1.60e7.60
Prior admission forHF (last y)
Felker et al60 2003 906 68 30% 36% Death or rehospitalization 60 d 11.6% 1.14 1.06e1.23Rodriguez-Artalejo
et al842005 394 77.2 6 6.6 56.1% N/A HF rehospitalization 6 mo 35.0% 1.88 1.24e2.83
Tsuchihashi et al54 2001 230 69 6 14 40% N/A HF rehospitalization 1 y 35.0% 3.29 1.77e6.13Prior hospitalization
for any causeRodriguez-Artalejo
et al852006 371 77.2 6 6.7 58.2% N/A Rehospitalization 6 mo 36.4% 1.50 1.01e2.28
Prior hospitalizationfor any cause(last 6 mo)
Harjai et al32 2001 443 70 6 14 45% 36% HF rehospitalization 30 d 15.8% 1.30 1.20e1.40
Length of stay(O14 d)
Tsuchihashi et al54 2001 230 69 6 14 40% N/A HF rehospitalization 1 y 35.0% 3.21 1.22e8.46
Previous diagnosisof HF
Kossovsky et al23 2000 442 75.6 6 11.2 48% N/A HF rehospitalization 31 d N/A 4.50 2.30e8.80
History ofpercutaneouscoronaryintervention
Felker et al60 2003 906 68 30% 36% Death or rehospitalization 60 d 11.6% 1.46 1.00e2.12
SBP (admission level) Felker et al60 2003 906 68 30% 36% Death or rehospitalization 60 d 11.6% 0.88 (per10 mm Hgincrease)
0.82e0.97
SBP (clinical visit) Mielniczuk et al35 2008 183 55.5 6 15 49% N/A Death or HF rehospitalization 1 y 47% 0.95 (per1 mm Hgincrease)
0.92e0.98
Poor tissue perfusion Perna et al61 2005 184 64.5 6 13.2 39.7% N/A HF rehospitalization 3 y 75% 2.46 1.31e4.60Volume overload Bettencourt et al76 2004 182 73.0 6 11.0 53% N/A Death or rehospitalization 6 mo 43% 1.87 1.08e3.23Higher discharge
NYHAfunctional class
Armola and Topp.80 2001 179 70.2 N/A N/A HF rehospitalization 30 d 23.5% N/A N/AEvangelista et al56 2000 753 69 6 11.7
(33e99)2% 39.4% Multiple (O1) HF readmissions 1 y 29.2% 2.57 1.86e3.55
Feola et al81 2008 250 73 34% N/A Death or rehospitalization 6 mo 56.4% 1.50 1.06e2.11Koitabashi et al25 2005 427 65.8 6 13.5 36% N/A HF rehospitalization 34 mo 34.9% 1.63 1.11e2.39
NYHA functionalclass II vs I
Lee et al26 2008 668 66 6 12 32.6% 100% Death or HF rehospitalization 2 y 29.6% 2.20 1.24e3.89
NYHA functionalclass III-IV vs I
Lee et al26 2008 668 66 6 12 32.6% 100% Death or HF rehospitalization 2 y 29.6% 2.99 1.60e5.62
ImagingCardiothoracic ratio
(O0.50)Giamouzis et al135 2008 5,164 64 6 11 19% 9.5% HF rehospitalization 37 mo 41% 1.27 1.13e1.44
LVEF (discharge) Feola et al81 2008 250 73 34% N/A Death or rehospitalization 6 mo 56.4% 0.98 0.97e0.99LVEF (admission) Valle et al91 2008 315 77 6 9 53% N/A HF rehospitalization 6 mo 28.6% 0.983 (per 1%
increase)0.961e0.992
LVEF (clinical visit) Mielniczuk et al35 2008 183 55.5 6 15 49% N/A Death or HF rehospitalization 1 y 47% 0.95 (per 1%increase)
0.93e0.97
LAVi Dokainish et al140 2007 100 57 6 12 45% N/A Cardiac death or rehospitalizationfor worsening HF
527 6 47 d 46% N/A N/A
RVTDI Dokainish et al140 2007 100 57 6 12 45% N/A Cardiac death or rehospitalizationfor worsening HF
527 6 47 d 46% N/A N/A
(continued on next page)
RiskFactors
forHospita
lizatio
nin
HeartFailure
�Giamouzis
etal
71

Table 4. (Continued)
Variable Source Year N Age (y) Female Nonwhite End Point Follow-UpEventRate HR 95% CI
Mitral peak earlydiastolic flowvelocity/TD earlydiastolic velocity
Dokainish et al140 2007 100 57 6 12 45% N/A Cardiac death or rehospitalizationfor worsening HF
527 6 47 d 46% N/A N/A
LaboratoryBNP (admission levelO200 pg/mL)
Niizeki et al102 2005 186 67 6 12 41% N/A Cardiac death or rehospitalizationfor worsening HF
18 mo 23.7% 2.41 1.02e5.73
NT-pro-BNP ($30%increase duringhospitalization)
Bettencourt et al76 2004 182 73.0 6 11.0 53% N/A Death orrehospitalization
6 mo 43% 5.96 3.23e11.01
NT-pro-BNP(in-hospitalvariation !30%)
Bettencourt et al76 2004 182 73.0 6 11.0 53% N/A Death or rehospitalization 6 mo 43% 2.03 1.14e3.64Pimenta et al95 2007 283 72.8 6 11.7 51.9% N/A Death or rehospitalization 6 mo 43.5% 2.68 1.54e4.68
NT-pro-BNP anddecreased renalfunction(in-hospitalvariation !30%)
Pimenta et al95 2007 283 72.8 6 11.7 51.9% N/A Death or rehospitalization 6 mo 43.5% 2.54 1.49e4.33
BNP (discharge) Feola et al81 2008 250 73 34% N/A Death or rehospitalization 6 mo 56.4% 1.006 1.004e1.009Ferreira et al105 2007 304 72.7 6 11.6 53.9% N/A Death or rehospitalization 6 mo 43% 2.02 1.28e3.20Koitabashi et al25 2005 427 65.8 6 13.5 36% N/A HF rehospitalization 34 mo 34.9% 1.002 1.001e1.003Logeart et al106 2004 114 69.4 6 14.4 30.7% N/A All-cause rehospitalization 6 mo 37% 1.25 (per
100 ng/Lincrease)
1.16e1.34
BNP (discharge level!250 pg/mL)
Valle et al91 2008 315 77 6 9 53% N/A HF rehospitalization 6 mo 28.6% 0.271 0.141e0.523
NT-pro-BNP anddecreased renalfunction (dischargevalue abovemedian)
Pimenta et al95 2007 283 72.8 6 11.7 51.9% N/A Death or rehospitalization 6 mo 43.5% 2.53 1.27e5.03
NT-proBNP(follow-up)
Pfister et al113 2008 290 64 (54e72) 20% N/A All-cause mortality,rehospitalizationfor ADHF and urgentcardiac transplantation
498 d 22.4% 1.9 (perincrease of1 SD of logNT-proBNP)
1.50e2.40
BNP (in-hospitaldecrease O30%vs no variation)
Ferreira et al105 2007 304 72.7 6 11.6 53.9% N/A Death or rehospitalization 6 mo 43% 2.24 1.37e3.66
BNP (in-hospitalincrease O30%vs decrease O30%)
Ferreira et al105 2007 304 72.7 6 11.6 53.9% N/A Death or rehospitalization 6 mo 43% 3.85 2.24e6.63
BNP (predischargeBNP $360 pg/mLand decrease!50% duringhospitalization)
Cournot et al110 2008 157 83 6 6 49% N/A Death orrehospitalizationfor worsening HF
3, 12,and 18 mo
48%, 76%,84%
5.97 2.98e11.94
BNP (2 mo afterinitiation oftherapy)
Ishii et al112 2003 100 68 6 11 44% N/A Death or rehospitalization forworsening HF or MI
1 y 44% 3.11 (log BNPper 10-foldincrease)
1.61e6.01
72
JournalofCardiacFailure
Vol.17No.1January
2011

BNP (O160 ng/L2 mo after initiationof therapy)
Ishii et al112 2003 100 68 6 11 44% N/A Death or rehospitalization forworsening HF or MI
1 y 44% 2.35 1.14e4.84
cTnT $0.10 ng/mL(within 24 h ofadmission)
Perna et al61 2005 184 64.5 6 13.2 39.7% N/A HF rehospitalization 3 y 75% 1.74 1.05e2.90
cTnT ($0.01 ng/mLduringhospitalizationfor ADHF)
Nishio et al119 2007 145 66.6 6 1.6 27% N/A Death or HF rehospitalization 1 y 19.3% 1.88 1.04e3.62
cTnT (2 mo afterinitiation oftherapy)
Ishii et al112 2003 100 68 6 11 44% N/A Death or hospitalization for worsening HF or MI
1 y 44% 2.07 (per 0.1mg/L increase)
1.43e3.01
cTnT (O0.001 mg/L2 mo after initiationof therapy)
Ishii et al112 2003 100 68 6 11 44% N/A Death or hospitalization forworsening HF or MI
1 y 44% 3.08 1.59e5.98
Hemoglobin(admission level)
Felker et al60 2003 906 68 30% 36% Death or rehospitalization 60 d 11.6% 0.88 (per 1 g/dLincrease)
0.82e0.97
Young et al86 2008 48,612 73.2 6 13.95 51.6% 25.9% Death or rehospitalization 60e90 d 36.2% 1.088 (per 1 g/dLdecrease)
1.044e1.134
Kosiborod et al87 2003 2,281 79 6 8 58% 10% All-cause rehospitalization 1 y N/A 1.02 (per 1%decrease)
1.01e1.03
Hemoglobin A1c Gerstein et al,90 2008 2,412 65.8 33.0% N/A Death or rehospitalizationfor worsening HF
36.7 mo N/A 1.25 (per 1%increase)
1.20e1.31
Serum sodium(admission level)
Gheorghiade et al88 2007 5,791 73 52% 26% Death or rehospitalization 60e90 d 36.4% 1.08 1.026e1.136
Glucose (admissionlevel, continuousvariable)
Berry et al89 2008 454 N/A 51% N/A Death or hospitalization forworsening HF
12 mo 36.3% 1.06, per2 mmol/Lincrease
1.02e1.10
Abnormal glucosetolerance
(admissionlevel $6 mmol/L)
Berry et al89 2008 454 N/A 51% N/A Death or hospitalization forworsening HF
12 mo 46% 1.61 1.07e2.41
Serum creatinine(admission level)
Rodriguez-Artalejo et al85
2006 371 77.2 6 6.7 58.2% N/A Rehospitalization 6 mo 36.4% 1.31 (per1 mg/dLincrease)
1.05e1.63
Rodriguez-Artalejo et al84
2005 394 77.2 6 6.6 56.1% N/A HF rehospitalization 6 mo 35.0% 1.33 (per1 mg/dLincrease)
1.09e1.64
Serum creatinine(discharge level)
Valle et al91 2008 315 77 6 9 53% N/A HF rehospitalization 6 mo 28.6% 1.39 (per1 mg/dLincrease)
1.09e1.77
\BUN (admissionlevel)
Felker et al60 2003 906 68 30% 36% Death or rehospitalization 60 d 11.6% 1.28 (per5 mg/dLincrease)
1.14e1.41
Harjai et al32 2001 443 70 6 14 45% 36% All-cause rehospitalization 30 d 26.2% 1.02 (per1 mg/dLincrease)
1.004e1.030
BUN (admission levelO28 mg/dL)
Shenkman et al92 2007 257 69 6 17 40% 32% Death or hospitalizationfor worsening HF
30 d 28.4% 1.83 1.03e3.24
CRP Anand et al124 2005 4,202 62.5 6 11 20% 9% First morbid eventa 12 mo 1.53 1.28e1.84Serum cystatin C Arimoto et al128 2005 140 66 6 13 38% N/A Cardiac death or HF
rehospitalization480 d 23% 1.94, per
increaseof one SD
1.29e6.64
(continued on next page)
RiskFactors
forHospita
lizatio
nin
HeartFailure
�Giamouzis
etal
73

Table 4. (Continued)
Variable Source Year N Age (y) Female Nonwhite End Point Follow-UpEventRate HR 95% CI
Heart-type fatty acidebinding protein(O4.3 ng/mL)
Arimoto et al131 2005 179 67 6 12 39% N/A Cardiac death or HFrehospitalization
20 mo 25% N/A N/A
Niizeki et al102 2005 186 67 6 12 41% N/A Cardiac death or HFrehospitalization
18 mo 23.7% 5.42 2.20e13.32
Serum pentosidine(log)
Koyama et al129 2007 141 66 6 13 37.6% N/A Cardiac death or HFrehospitalization
479 d 22.7% 1.88 (per1 SDincrease)
1.23e2.69
Koyama et al130 2008 160 69 6 12 40.6% N/A Cardiac death or HFrehospitalization
872 d 30% 1.59 (per1 SDincrease)
1.11e1.29
sRAGE (log) Koyama et al130 2008 160 69 6 12 40.6% N/A Cardiac death or HFrehospitalization
872 d 30% 1.90 (per1 SDincrease)
1.16e3.09
Renin Nishio et al119 2007 145 66.6 6 1.6 27% N/A Death or HF rehospitalization 1 y 19.3% 2.38 1.22e5.05Serum PIPO124 ng/mL
Ruiz-Ruiz et al132 2007 111 73.4 6 7.9 46.8% N/A HF rehospitalization 21 mo 48.6% 1.015 1.006e1.024
ComorbidityHypertension(history)
Tsuchihashi et al54 2001 230 69 6 14 40% N/A HF rehospitalization 1 y 35.0% 1.99 1.06e3.72
Diabetes mellitus Berry et al89 2008 454 N/A 51% N/A Death or HF rehospitalization 12 mo 48% 1.88 1.22e2.88Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 1.11 1.02e1.21Lee et al26 2008 668 66 6 12 32.6% 100% Death or HF rehospitalization 2 y 29.6% 1.80 1.25e2.60Rodriguez-
Artalejo et al842005 394 77.2 6 6.6 56.1% N/A HF rehospitalization 6 mo 35.0% 1.45 1.02e2.06
Anemia Berry et al159 2006 528 72 6 13 50% N/A Death or HF- rehospitalization 814 d 54% 1.40 1.04e1.89Ezekovitz et al59 2008 10,415 79.5 (73e85) 50.4% N/A All-cause rehospitalization 30 d 20.2% 1.30 1.00e1.69
Anemia (Htc #24%) Kosiborod et al161 2005 50,405 79.4 6 0.05 59% 15.6% HF rehospitalization 1 y N/A 1.21 (Htc#24% vs HtcO44%)
1.04e1.38
Anemia (admissionHb !12 g/dL)
Luthi et al160 2006 955 75.4 6 12.8 45.7% N/A All-cause rehospitalization 30 d 13.4% 1.60 1.00e2.58
Hyponatremia(admission Na!135 mEq/L)
Milo-Cotter et al162 2008 331 75.8 6 10.3 49% N/A Death or HF- rehospitalization 6 mo 46% N/A N/A
Concomitant AMI Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 1.13 1.02e1.24Concomitantparoxysmal AF
Koitabashi et al25 2005 427 65.8 6 13.5 36% N/A HF rehospitalization 34 mo 34.9% 2.30 1.30e4.05
Hypertension Ezekovitz et al59 2008 10,415 79.5 (73e85) 50.4% N/A All-cause rehospitalization 30 d 20.2% 0.74 0.60e0.91Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 0.88 0.82e0.94
Stroke (yes vs no) Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 1.26 1.12e1.41Cerebrovasculardisease
Darze et al83 2007 198 69.4 6 13.5 44% N/A Death or rehospitalization 3 mo 46% 4.10 1.60e10.90
Hyponatremia(!136 mEq/L)
Darze et al83 2007 198 69.4 6 13.5 44% N/A Death or rehospitalization 3 mo 46% 3.70 1.60e8.50
Renal insufficiency Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 1.57 1.44e1.72Faris et al55 2002 396 53 6 15
(15e86)26% 17% Rehospitalization 48 mo Rate, 1.7/
patient-year2.80 1.20e6.60
McCellan et al164 2004 755 75.7 6 10.9(30e100)
60.2% 29.7% Rehospitalization 30 d 32% 1.70 1.18e2.44
Acute renal failure Darze et al83 2007 198 69.4 6 13.5 44% N/A Death or rehospitalization 3 mo 46% 2.70 1.40e5.30
74
JournalofCardiacFailure
Vol.17No.1January
2011

WRF (both a $25%and a $0.3 mg/dLincrease in sCrfrom admission)
Metra et al165 2008 318 68 6 11 40% N/A CV death or HFrehospitalization
480 d 48% 1.47 1.13e1.81
Atrial dibrillation Blackledge et al24 2003 5,789 77.5 50% 12.6% Death or rehospitalization 1 y 49% 0.94 0.88e1.00Acute pulmonary
embolismDarze et al83 2007 198 69.4 6 13.5 44% N/A Death or rehospitalization 3 mo 46% 4.00 1.10e15.10
Depression Faris et al55 2002 396 53 6 15(15e86)
26% 17% Rehospitalization 48 mo Rate, 1.7/patient-year
1.25 1.07e1.90
Depression (major) Jiang et al174 2001 357 63 6 13 38% 30% HF rehospitalization 1 y 60.5% 2.98 1.17e7.59COPD Harjai et al32 2001 443 70 6 14 45% 36% HF rehospitalization 30 d 15.8% 2.20 1.10e4.50Charlson comorbidity
indexRodriguez-
Artalejo et al852006 371 77.2 6 6.7 58.2% N/A Rehospitalization 6 mo 36.4% 1.13 (per
1-pointincrease)
1.02e1.26
Social/PsychologicReadiness-for-
dischargecriteria
Kossovsky et al23 2000 442 75.6 6 11.2 48% N/A HF rehospitalization 31 d N/A 1.23 1.06e1.42
Follow-up plan Armola and Topp80 2001 179 70.2 N/A N/A HF rehospitalization 30 d 23.5% 0.33 N/APoor follow-up visits
(!1/mo or none)Tsuchihashi et al54 2001 230 69 6 14 40% N/A HF rehospitalization 1 y 35.0% 4.87 2.01e11.78
HF performancemeasures
Chung et al200 2008 400 N/A N/A N/A All-cause rehospitalization 6 mo N/A 0.74 0.57e0.97
Primary carephysician
Evangelista et al56 2000 753 69 6 11.7(33e99)
2% 39.4% Multiple (O1) HFreadmissions
1 y 29.2% 2.41 1.57e3.67
Home-basedtelemanagementprogram
Giordano et al180 2008 460 57 6 10 15% N/A HF rehospitalization 1 y 19% 0.50 0.34e0.73
SF-36 physicalsummary score
Rodriguez-Artalejo et al84
2005 394 77.2 6 6.6 56.1% N/A HF rehospitalization 6 mo 35.0% 1.59 1.12e2.26
AF, atrial fibrillation; CRP, C-reactive protein; Htc, hematocrit; PIP, propeptide of procollagen type I; sCr, serum creatinine; LAVi, left atrial volume index; RVTDI, right ventricular tissue Doppler imaging;sRAGE, soluble receptor for advanced glycation end products; TD, tissue Doppler; WRF, worsening of renal function;other abbreviations as in Tables 1-3.
RiskFactors
forHospita
lizatio
nin
HeartFailure
�Giamouzis
etal
75
Copyright © 2022 FDOKUMEN




















