Antioxidant supplements for prevention of mortality in healthy ...
Upload
independentCategory
view
0download
0
Health Policy 92 (2009) 276–287
Contents lists available at ScienceDirect
Health Policy
journa l homepage: www.e lsev ier .com/ locate /hea l thpol
Hospital supplements in Belgium: Price variation and regulation
Ann Lecluysea,∗, Carine Van de Voordeb, Diana De Graevea,Erik Schokkaertc, Tom Van Ourtid,e,1
a Faculty of Applied Economics, University of Antwerp, Prinsstraat 13, 2000 Antwerpen, Belgiumb Belgian Health Care Knowledge Centre, Brussels, Belgiumc Department of Economics, KULeuven, Belgium and CORE, Université catholique de Louvain, Louvain, Belgiumd Erasmus School of Economics, Erasmus University Rotterdam, Rotterdam, The Netherlandse Tinbergen Institute, Burgemeester Oudlaan 50, 3062 PA Rotterdam, The Netherlands
a r t i c l e i n f o
Keywords:InpatientsFees and chargesHealth policyBelgium
a b s t r a c t
Objectives: Although there is a comprehensive public health insurance system in Belgium,out-of-pocket expenditures can be very high, mainly for inpatients. While a large partof the official price is reimbursed, patients are confronted with increased extra billing(supplements). Therefore, the government imposed various restrictions on the amount ofsupplements to be charged, related to the type of room and the patient’s insurance status.We investigate how prices are set and whether the restrictions have been effective.Methods: We use an administrative dataset of the Belgian sickness funds for the year 2003with billing data per hospitalisation and hospital characteristics. Boxplots describe thedistribution of several categories of supplements. OLS is used to explore the relationshipbetween hospital characteristics and extra billing.Results: There is a large and intransparent variation in extra billing practices among different
hospitals. Given the room type, supplements per day are smaller for patients qualifying forprotection, confirming that the regulation is applied quite well. However, because of theirlonger length of stay this does not result in lower supplements per stay for these patients.Conclusions: Currently the price setting behavior of providers lacks transparency. Protectiveregulation could be refined by taking into account the longer length of stay of vulnerablegroups.1. Introduction
The financial accessibility of a health care system is
directly related to the amount and the distribution ofout-of-pocket (OOP) payments. In the Belgian context, thelatter consist of official co-payments, payments for non-covered health care treatments/items, and extra payments∗ Corresponding author. Tel.: +32 0 3 2204878.E-mail address: [email protected] (A. Lecluyse).
1 Tom Van Ourti is a Postdoctoral Fellow of the Netherlands Organiza-tion for Scientific Research – Innovational Research IncentivesScheme – Veni.
0168-8510/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.healthpol.2009.04.004
© 2009 Elsevier Ireland Ltd. All rights reserved.
to providers on top of the customary fee agreed upon withthe health insurance. The two latter payments are called“supplements” in the Belgian terminology. This definitionis somewhat broader than the concepts of “balance billing”or “extra billing” used in countries like the US or Canada,which usually only refer to the charges paid by the patientin excess of the usual and customary rate paid by the healthplan.
While most studies on the financial accessibility of
health care focus on official co-payments or co-insurance,the effects of extra billing are studied to a much lesserextent. In a theoretical paper, Glazer and McGuire [1] pointout that extra billing may increase efficiency when theMedicare fee is set appropriately, because physicians will
lth Polic
rHiqtai
bniaobpda(iicpT[t‘epMfiQcitcpp
oospsctmtcba
teotwv
p
which also has to be paid by the patient. Moreover, thereare also services that are not covered by the compulsoryhealth insurance. For these items, there is no conventiontariff and the patient pays the full price out-of-pocket.
A. Lecluyse et al. / Hea
educe quality of care when extra billing is not allowed.owever, Kifmann and Scheuer [2] demonstrate that the
mpact on the patients’ welfare is unclear, as the positiveuality impact may be offset by the negative impact ofhe price to be paid by patients. Pauly [3] also argues thatn insurance system with extra billing will lead to pricencreases.
Existing empirical work has focused on the costs of extrailling for the patients. The first empirical papers, that didot take into account quality of care, showed that there
s an increasing cost for the patient when physicians arellowed to extra bill [4–6]. The results do not change whennly a (small) share of physicians is in a system of extrailling. Epp et al. [7] make a pre–post comparison of generalractitioners (GP) and specialists who ‘opted-out’ the Cana-ian system (and so gained allowance to extra bill) withmatched sample of those who remained in the system
and were not allowed to extra bill). Results show a dropn patient demand for opted-out GPs and specialists. Theres no loss in revenues for the physicians since extra billingompensates decreased demand. There is also evidence ofatients switching from opted-out to opted-in physicians.his observation is in line with the results of Northcott8] who carried out a survey in 1980 in Canada. He foundhat patients support the idea that physicians deserve anadequate compensation’, but are opposed to the system ofxtra billing. Finally, McKnight [9] analyses the impact onhysicians and patients of the restriction on extra billing foredicare beneficiaries in the US during the late 1980s. She
nds little evidence of a behavioral reaction of physicians.uality, assessed by the length of the consultation, is nothanged, nor is the quantity of service. The only declines found in the number of follow-up consultations. Sincehe out-of-pocket expenditures decreased significantly, sheoncluded that the restriction resulted in a transfer fromhysicians to patients and hence effectively protected theatient.
Belgium is an interesting case to study the impactf extra billing or, more broadly, supplements. Althoughfficial prices – reimbursements and co-payments – aretrongly regulated, there is a large degree of freedom inrice setting on top of these tariffs. The medical profes-ion is strongly in favor of this system. They consider theontrol over the price and mix of services at the heart ofheir entrepreneurial and clinical autonomy. The govern-
ent and the insurers on the other hand try to restricthe possibilities of extra billing in order to protect finan-ial accessibility for the patient. Protective regulation haseen introduced for some weaker socio-economic groupsnd is related to the choice of room type.
In this paper, we consider the effectiveness of this pro-ective (Belgian) regulation in reducing the price impact ofxtra billing.2 We analyze whether and how the practice
f extra billing differs between hospitals and whether pro-ective regulation leads to lower costs for the economicallyeaker patients. Our data reveals a large and intransparentariation in extra billing practices among different hospi-
2 We refer the reader to De Graeve et al. [10] for more results on costser individual.
y 92 (2009) 276–287 277
tals, but also suggests that this variation would have beenbigger in the absence of protective regulation. The reg-ulation leads to lower supplements per day for patientsqualifying for protection. Nevertheless, these patients havesimilar amounts of supplements per stay, due to a longerlength of stay.
In the next section, we summarize the most importantcharacteristics of the Belgian health insurance system. Thethird section describes the data and methods. In Section 4,the results with respect to variation in price setting behav-ior are presented. Section 5 evaluates the effectiveness ofthe protective mechanisms. The final section concludes.
2. The Belgian health insurance system3
Belgium has a centralised compulsory health insur-ance system organized through sickness funds and with(dominantly) fee-for-service remuneration for providers.Co-payments are imposed to limit moral hazard, while atthe same time protective measures have been introducedout of a concern for equality of access. First, some specificgroups of patients have a right to so-called ‘preferential sta-tus’. This right is assigned automatically to persons andtheir dependents belonging to specific social categories(such as the elderly and the handicapped), provided thegross taxable income of the family does not exceed a yearlylimit. For these patients co-payments are reduced (andhence reimbursements are increased) for all types of healthcare. The amount of the reduction depends on the typeof expenditure (GP, specialist, drugs,. . .).4 Second, a sys-tem of maximum billing puts an income-dependent cap onannual co-payments at the level of the household. Third,some lump sum subsidies have been installed to compen-sate people who can be expected to have high medicalexpenditures (e.g. people with a chronic illness or receivingpalliative treatment at home).
Reimbursements and co-payments in the compulsorysystem are strongly regulated through a complex processof negotiations with the various actors involved (sicknessfunds, representatives of health care professionals,. . .), allwithin preset budgetary limits. The resulting ‘conventiontariff’ (the Belgian terminology for the negotiated price)consists of the co-payment and the reimbursement. OOPpayments in Belgium, however, are not limited to co-payments. Health care providers consider the conventiontariff as a kind of social tariff, and are not obliged to abideby it in all circumstances. If providers charge a fee on top ofthe convention tariff, the difference between the total feecharged and the convention tariff is called a supplement,
3 This section is based on De Graeve et al. [10].4 It is important to emphasize that granting this “preferential status” is
not within the discretion of the providers. The reduction of co-payments isgranted to all people with certain well-specified observable characteris-tics. These observable characteristics are linked to morbidity (expectedhealth care expenditures) and to income, but there is no selection on(unobservable) morbidity characteristics.

278 A. Lecluyse et al. / Health Policy 92 (2009) 276–287
Fig. 1. Structure of health care prices.
Table 1Summary of regulation with respect to inpatient supplements (2003 situation).
Type of supplement Type of room
Common room Two-person room Single room
Fee supplementPhysician/dentist subscribed No No YesPhysician/dentist not subscribed Yes, but protected persons Yes, but protected persons YesOther subscribed No No NoOther not subscribed Yes, but protected persons Yes, but protected persons Yes
Room supplement No Yes, with maximum Yes
g on ty
ed item
tients can be charged for certain products delivered by thehospital pharmacist such as a personal thermometer, anti-decubitus materials, lip salve, bath oil and so on. These
Material supplement Yes or no, dependin
Other supplements (including drugs) Yes, for used/order
Examples are non-covered implants, some drugs or para-pharmaceutical items, non-covered esthetical surgery andalso diverse non-medical items for inpatients such as thecosts of a refrigerator or telephone in the hospital room.The composition of health care prices in Belgium is shownin Fig. 1.
Traditionally, there has been a large degree of freedomfor the providers to determine whether supplements willbe charged and at which level they are set. However, inorder to protect the patient, inpatient supplements haveincreasingly been regulated. Table 1 provides a summary.As our data refer to the 2003 situation, we focus on theregulation that was in place in that year. A distinction ismade between fee, room, material and other supplements.
The amount of fee supplements depends on the type ofroom, the type of patient and also on whether or not thephysician subscribed to the convention tariff. The hospitalis obliged to set a (freely chosen) maximum supplement(which may vary between hospitals); this maximum has tobe mentioned on the admission form signed by the patient.Any health care provider (physician, dentist or other) whodoes not subscribe to the convention tariff can freely deter-mine the amount of fee supplements, irrespective of thechoice of room of the patient and within the maximumset by the hospital. In addition, convention tariffs have tobe respected in two-person or common rooms for specificgroups (e.g. beneficiaries of preferential status and theirdependents, patients eligible for the mentioned lump sumsor entitled to a lump sum for the handicapped). Supple-
ments cannot be charged for patients staying in a singleor two-person room if they did not have a free choice ofroom type (e.g. because of medical or technical necessity,because of unavailability of a two-person or common room,or when the patient is admitted to an emergency unit orpe of device
s
intensive care unit beyond her control). For health careproviders who subscribe to the convention tariff, a distinc-tion is made between physicians and dentists on the onehand, and other health care providers on the other hand.The latter are never allowed to charge supplements, whilethe former can charge supplements in a single room (exceptwhen the patient is in a single room beyond her control).
Room supplements can be charged in a single ortwo-person room. The amount of the supplement for atwo-person room is limited (D19.34 in 2003 linked to theconsumer price index). In a single room there is no legallydetermined upper limit. Similar to the regulation of feesupplements, no supplement can be charged in a singleroom/two-person room if this room was not freely chosenby the patient.5
The regulation of material supplements (for implants,devices or osteosynthetic material) is rather complicatedand specific to each type of implant or material. For someimplants or materials, no supplements can be charged; forothers, supplements are limited; and for some they areunlimited. Regulation is always linked to the device andnot to the (vulnerable status of the) beneficiary or to thetype of room.
Finally, other supplements may apply. Over-the-counterdrugs are not reimbursed, not even during hospitalisationand are denoted as drug supplements. In addition inpa-
are referred to as parapharmaceutical supplements. Diverse
5 Furthermore, from 2006 onwards no room supplements can becharged to vulnerable patients.

A. Lecluyse et al. / Health Policy 92 (2009) 276–287 279
Table 2Some summary statistics of subsample of inpatients.
Total sample Inpatients
All No prefstata Prefstat All No prefstat Prefstat
N (number of patients) 271,813 224,414 47,399 36,760 25,992 10,768% Females 52.01 50.71 60.01 57.34 56.37 60.22p-value of equality test <0.0001 0.1888Average age 40.23 37.65 56.05 49.50 45.16 62.48p-value of equality test <0.0001 <0.0001% Without health care costs 5.38 5.60 4.32p-value of equality test <0.0001Average expendituresb 1595.52 1227.14 3851.01 3111.19 2770.65 4127.19p
tatus.ents.
ssfd
3
facsveanhpFtaisciiicoaq(thpscsbiwttth
The absolute amounts of supplements per hospital staycannot directly be interpreted as prices. They reflect effectsof morbidity (longer hospital stays) on the one hand and ofregulatory measures and supply-side behavior (price set-
6 Paramedical fees are not taken into account in this category. The reg-
-value of equality test <0.0001
a No prefstat = without preferential status; prefstat = with preferential sb In this table, expenditure is the sum of reimbursements and co-paym
upplements contain charges for non-medical products orervices, such as telephone, television, refrigerator, bedor accompanying person, drinks outside the meals, hair-resser, laundry.
. Data and methods
We used an administrative dataset of the sickness fundsor 2003. Since in principle all persons living in Belgiumre insured by one of the sickness funds, their joint dataover the whole population. From this population a randomample of about 300,000 individuals was drawn. Each indi-idual had a chance of 1/40 of being included in the sample,xcept for the elderly (65 and older) that had a chance ofbout 1/20. This oversampling was applied to get a largerumber of observations for the elderly, which on averageave larger health care expenditures. In our analysis sam-ling weights were used to maintain representativeness.or all the individuals in the sample we have, besides allhe demographic and socio-economic information that isvailable at the level of the sickness funds, also detailednformation on health care expenditures. The latter con-ist of reimbursements by the health insurance system,o-payments and supplements. The data allow us to relatenpatient health care expenditures to the individual staysn the hospital. Since registration of supplements is obligedn the hospital sector, our data on the overall out-of-pocketost of inpatient stays are quite reliable. As the magnitudef supplements is much smaller in the ambulatory sectornd the data on ambulatory supplements are of much loweruality, we focus our analysis on the cost per inpatient stayexcluding day care). A patient can have more hospitalisa-ions within a year: while 36,760 individuals in the samplead an inpatient stay, we have information on 54,919 hos-italisations. Table 2 shows that, compared to the totalample, our subsample of inpatients is older on average andontains more females and individuals with preferentialtatus (29.29% versus 17.44%). The average amount of reim-ursements and co-payments in the sample of inpatients
s about twice as high as in the total sample. Individuals
ith preferential status have significantly larger expendi-ures than individuals without preferential status in theotal sample as well as in the sample of inpatients andhey are significantly less likely to have no reimbursedealth care costs: 4.32% of them did not need health care
<0.0001
as compared to 5.60% of those without preferential sta-tus.
Expenditures for all medical interventions during hos-pitalisation have been aggregated into five categories:physician/dental fees,6 drugs, materials, room, and diversesupplements. The information in the administrative datasetwas combined with information on hospital characteris-tics: size, province and type of hospital (general, chronicor psychiatric hospital). Although there is no direct infor-mation on morbidity and income of the patients, we canapproximate their economic and health situation witha variety of indirect indicators. We lack information onsupplemental hospital insurance. Because such insurancemainly refunds supplements and co-payments for hospi-tal stays, the amount paid by the patients out of their ownpocket may be considerably reduced. Therefore, in somecases, our data will overestimate the financial burden onthe patient.
For the patient, what matters in the first place is thetotal absolute amount paid out-of-pocket. Co-paymentsare fixed by law, however, and we are mainly interestedin the effect of supplements and in the price settingbehavior of the providers. We will therefore focus on thelatter. We will first describe the practice of price set-ting (taking into account the regulation) by looking morecarefully at the calculated unit supplement prices for thefive aggregated categories of care. We will then analyzehow the price setting behavior differs between hospitalsusing OLS-regression with our (limited) information onprovider characteristics as explanatory variables. We willfinally investigate whether the protective regulation leadsto lower OOP for the protected groups by calculating meansupplements per day and per stay.
ulation prohibits the paramedical staff to charge supplements if theysubscribe to the convention tariff. Since almost all of them subscribe theconvention, there are hardly any supplements for this type of care. Wedo not show separate results for paramedical supplements. The amounts(reimbursements, co-payments and supplements) related to paramedicalfees are however still included in total expenditures.
280 A. Lecluyse et al. / Health Policy 92 (2009) 276–287
Table 3Relative unit supplement prices (2003).
All hospitalisations Hospitalisations wheresupplements are charged
N Relative unitsupplement price
N Relative unitsupplement price
Mean Median Mean Median
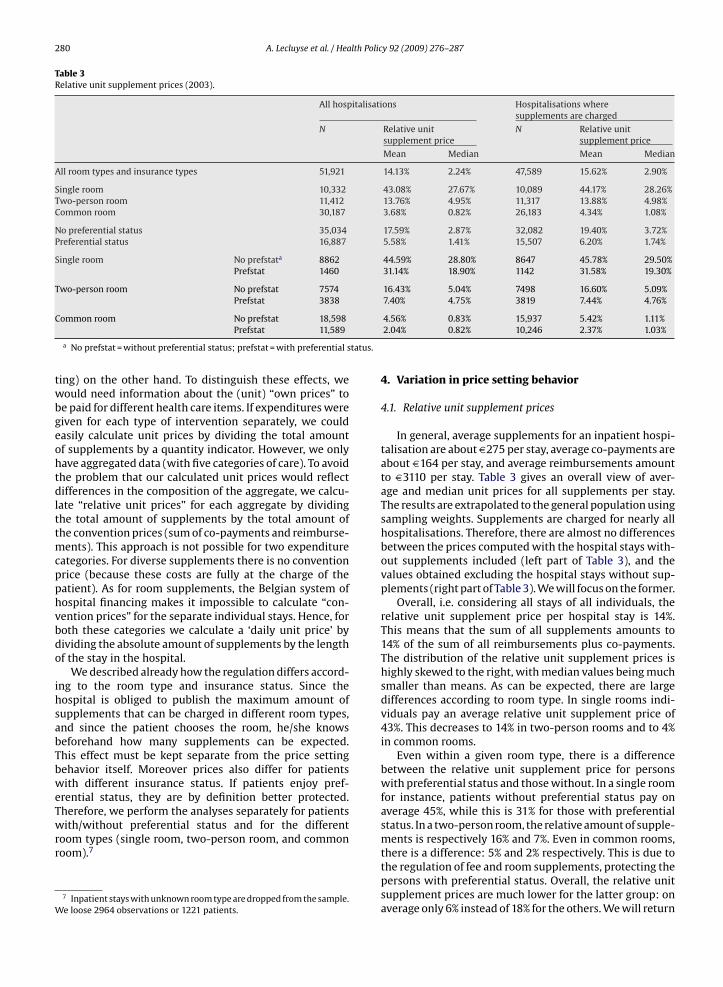
All room types and insurance types 51,921 14.13% 2.24% 47,589 15.62% 2.90%
Single room 10,332 43.08% 27.67% 10,089 44.17% 28.26%Two-person room 11,412 13.76% 4.95% 11,317 13.88% 4.98%Common room 30,187 3.68% 0.82% 26,183 4.34% 1.08%
No preferential status 35,034 17.59% 2.87% 32,082 19.40% 3.72%Preferential status 16,887 5.58% 1.41% 15,507 6.20% 1.74%
Single room No prefstata 8862 44.59% 28.80% 8647 45.78% 29.50%Prefstat 1460 31.14% 18.90% 1142 31.58% 19.30%
Two-person room No prefstat 7574 16.43% 5.04% 7498 16.60% 5.09%Prefstat 3838 7.40% 4.75% 3819 7.44% 4.76%
tatus.
Common room No prefstat 18,598Prefstat 11,589
a No prefstat = without preferential status; prefstat = with preferential s
ting) on the other hand. To distinguish these effects, wewould need information about the (unit) “own prices” tobe paid for different health care items. If expenditures weregiven for each type of intervention separately, we couldeasily calculate unit prices by dividing the total amountof supplements by a quantity indicator. However, we onlyhave aggregated data (with five categories of care). To avoidthe problem that our calculated unit prices would reflectdifferences in the composition of the aggregate, we calcu-late “relative unit prices” for each aggregate by dividingthe total amount of supplements by the total amount ofthe convention prices (sum of co-payments and reimburse-ments). This approach is not possible for two expenditurecategories. For diverse supplements there is no conventionprice (because these costs are fully at the charge of thepatient). As for room supplements, the Belgian system ofhospital financing makes it impossible to calculate “con-vention prices” for the separate individual stays. Hence, forboth these categories we calculate a ‘daily unit price’ bydividing the absolute amount of supplements by the lengthof the stay in the hospital.
We described already how the regulation differs accord-ing to the room type and insurance status. Since thehospital is obliged to publish the maximum amount ofsupplements that can be charged in different room types,and since the patient chooses the room, he/she knowsbeforehand how many supplements can be expected.This effect must be kept separate from the price settingbehavior itself. Moreover prices also differ for patientswith different insurance status. If patients enjoy pref-erential status, they are by definition better protected.Therefore, we perform the analyses separately for patients
with/without preferential status and for the differentroom types (single room, two-person room, and commonroom).77 Inpatient stays with unknown room type are dropped from the sample.We loose 2964 observations or 1221 patients.
4.56% 0.83% 15,937 5.42% 1.11%2.04% 0.82% 10,246 2.37% 1.03%
4. Variation in price setting behavior
4.1. Relative unit supplement prices
In general, average supplements for an inpatient hospi-talisation are about D275 per stay, average co-payments areabout D164 per stay, and average reimbursements amountto D3110 per stay. Table 3 gives an overall view of aver-age and median unit prices for all supplements per stay.The results are extrapolated to the general population usingsampling weights. Supplements are charged for nearly allhospitalisations. Therefore, there are almost no differencesbetween the prices computed with the hospital stays with-out supplements included (left part of Table 3), and thevalues obtained excluding the hospital stays without sup-plements (right part of Table 3). We will focus on the former.
Overall, i.e. considering all stays of all individuals, therelative unit supplement price per hospital stay is 14%.This means that the sum of all supplements amounts to14% of the sum of all reimbursements plus co-payments.The distribution of the relative unit supplement prices ishighly skewed to the right, with median values being muchsmaller than means. As can be expected, there are largedifferences according to room type. In single rooms indi-viduals pay an average relative unit supplement price of43%. This decreases to 14% in two-person rooms and to 4%in common rooms.
Even within a given room type, there is a differencebetween the relative unit supplement price for personswith preferential status and those without. In a single roomfor instance, patients without preferential status pay onaverage 45%, while this is 31% for those with preferentialstatus. In a two-person room, the relative amount of supple-ments is respectively 16% and 7%. Even in common rooms,
there is a difference: 5% and 2% respectively. This is due tothe regulation of fee and room supplements, protecting thepersons with preferential status. Overall, the relative unitsupplement prices are much lower for the latter group: onaverage only 6% instead of 18% for the others. We will return
A. Lecluyse et al. / Health Policy 92 (2009) 276–287 281
Fig. 2. (a) Relative unit supplement prices for fee supplements (exclusive paramedical supplements). (b) Relative unit supplement prices for drug supple-ments. (c) Relative unit supplement prices for material supplements. (d) Daily unit supplement price for room supplements. (e) Daily unit supplement pricefor diverse costs.

282 A. Lecluyse et al. / Health Policy 92 (2009) 276–287
(Contin
Fig. 2.to the effectiveness of the social protection mechanisms inthe next section.
Fig. 2a–e shows boxplots8 for the different categories ofcare. In Fig. 2a–c the relative supplement price is shown formedical fees (without paramedical fees), drugs and mate-rial, and Fig. 2d–e shows the daily supplement for roomsupplements and diverse costs. In each case, there is askewed distribution (with long right tails and a medianmuch smaller than the mean). The notes to Fig. 2a–e givethe p-values for the significance testing of the differences inunit prices according to preferential status and room type.
There clearly is a large variation between the different
subcategories of supplements. First, while overall supple-ments for medical fees are a relatively small percentageof the convention price (12.40%), we see a large variationaccording to room type and insurance type of the patient8 For readability, the scaling differs for the different boxplots. The upperhinge of the box indicates the 75th percentile of the data set, and the lowerhinge the 25th percentile. The ends of the whiskers indicate the 10th and90th percentiles.
ued ).
(Fig. 2a). As expected, relative unit prices are highest inthe single rooms where on average a supplement of about51.33% (relative to the convention price) is charged. Thisdrops to 4.95% in two-person rooms and to 0.74% in com-mon rooms. Also as expected, patients with preferentialstatus have to pay significantly less supplements (3.69%of the convention price) as compared to those withoutpreferential status (15.92%). Furthermore, the interactionbetween room type and insurance status is consistent withthe regulation. The more detailed results reported in DeGraeve et al. [10] show in addition a large variation amongsubgroups of medical disciplines. For example, gynaecolo-gists charge on average 100% supplements in single rooms.
On the contrary, drug supplements, material supplementsand diverse supplements do not show these strong differ-ences according to room type (Fig. 2b, c and e). As theregulation here does not distinguish between the room
types, this result is as expected. Moreover, the differencesaccording to insurance status are not significant.Fig. 2d shows that the regulation is well applied for roomsupplements: there is a large variation linked to the roomtype and the insurance status of the patients. Patients with-

lth Polic
otrvtuami
4
utiianbtOptt
‘asofttmvfhpf
rdorhstsiaissDis
ac
tus and room type. To put the numbers in perspective we
A. Lecluyse et al. / Hea
ut preferential status and/or residing in a single room payhe highest room supplements per day. While, on average,oom supplements per day are not very large (D9.54), theyary between D27 and D34 in single rooms depending onhe insurance status of the patient. In line with the reg-lation, the amount of room supplements does not varyccording to insurance status in the other room types. It isuch lower in two-person rooms (D11–12) and (almost) nil
n common rooms.
.2. Determinants of variation in unit supplement prices
We now present the results of OLS-estimations with thenit supplement prices of the different categories of care ashe dependent variable and observable hospital character-stics as explanatory variables. Because of the differencesn regulation, the sample is split by type of room and insur-nce status of the patient.9 Of course, this approach doesot offer a complete “explanation” for the price settingehavior of the hospitals, which may also be influenced byheir financial situation or by their quality of treatment.ur only purpose is to get a better idea about the trans-arency of the supplements, i.e. in how far they are linkedo hospital characteristics which are easily observable tohe patients.
Table 4 shows the results with as reference categoryan inpatient hospital stay in the province of Antwerp in
general hospital with 250–500 beds’. Except for roomupplements per day in single and two-person rooms,bservable hospital characteristics explain only a smallraction of the variation in prices. In several cases (wherehe adjusted R2 is shaded), these characteristics do not addo the explanation of the variation and the F-test for the full
odel is not significant. The large fraction of unexplainedariation suggests that the market is not very transparentor the patients, in that observable characteristics of theospital itself do not tell much about the unit supplementrices charged. Other conclusions can be summarized asollows.
First, there is a large geographical variation for fee andoom supplements. In line with the regulation, the largestifferences are found in single rooms and for patients with-ut preferential status. For example, compared to Antwerp,elative medical fee supplements in Brussels are about 43%igher in a single room for patients without preferentialtatus and 40% higher for those with preferential status. Inwo-person rooms, the difference in extra billing is a lotmaller (about 22%) for the former and it becomes insignif-cant for the latter. Room supplements per day also varyccording to the province. Again the variation is largestn single rooms, but it is smaller according to insurancetatus. For example, room supplements are largest in Brus-
els: patients without (with) preferential status pay about51 (D49) more per day in single rooms, and D5 (D6) moren two-person rooms. For drug supplements and materialupplements we do not observe such geographical differ-
9 We did not include patient characteristics since the dependent vari-ble is a unit supplement price, removing the need for a morbidityorrection.
y 92 (2009) 276–287 283
entiation. Diverse supplements per day do not vary muchby region either.
Second, the type of hospital matters. Fee supplements,with the exception of paramedical fees, are between 8% and10% higher in chronic hospitals if the patient stays in a two-person or single room respectively. In psychiatric hospitals,significantly lower relative fee supplements are charged ina single room for patients with preferential status. Also, therelative drug supplements are significantly lower in psy-chiatric hospitals. This can be explained by the regulation.In general and chronic hospitals, non-reimbursed pharma-ceuticals, such as painkillers or sleeping pills, are to be paidout-of-pocket as a supplement. For patients in psychiatrichospitals, however, these drugs are included in the dailylump sum – which is considered as a co-payment. Third,psychiatric hospitals charge lower room supplements perday. Patients in single rooms pay about D18 less per day ina psychiatric hospital than in a general hospital. The differ-ence is D7 per day for two-person rooms irrespective of theinsurance status of the patient.
After controlling for the other effects, the size of thehospital also matters: smaller hospitals (less than 250beds) charge significantly lower fee supplements. We findan increasing trend for room supplements: larger hospi-tals charge significantly larger room supplements per dayin single (+D6) and two-person rooms (+D2) and smallerhospitals charge significantly less (varying from −D5 to−D1). Conform the regulation, we found no difference forcommon rooms. Finally, diverse costs per day are also sig-nificantly higher in hospitals with more than 500 beds.Given the paucity of available data, it is not easy to explainthese differences. Some hypotheses may be formulated,however. First, the market power of the smaller hospitals ismost probably more limited. Secondly, the level of supple-ments may be linked to the reputation of the medical staffand to the level of comfort of the (mainly) single rooms,which may be lower in smaller hospitals that are often olderand less well equipped.
5. Effectiveness of the protective mechanisms
A first component in the regulation of supplementsis the explicit differentiation between the different roomtypes. Table 3 has shown that this regulation indeed works.Patients can freely choose their type of room and those whoopt for a two-person room or for a common room pay sig-nificantly lower supplements. A second component in theregulation is the protection of the weaker socio-economicgroups with preferential status. Here, our results are lesscomforting.
Table 5 gives an overview of the supplements to be paidper hospital stay and per day, according to insurance sta-
add the respective amounts of reimbursements10 and co-payments. At first sight, most of the results are in line withwhat could be expected given the regulation. Overall, the
10 Due to the hospital financing system, the reimbursement of an indi-vidual hospital stay is not directly available in the data and had to beestimated. See the technical note in appendix 1 in De Graeve et al. [10] formore details.

284A
.Lecluyseet
al./Health
Policy92
(2009)276–287
Table 4Determinants of unit supplement prices charged by the hospital.
Room type Prefstata R2adj Intercept Vlaams-Brabant
West-Flanders
East-Flanders
Limburg Brussels Brabant-Wallon
Hainaut Liège Luxemburg Namur Chronhospb
Psychhospc
<250 Beds >500 Beds
Relative medical fee supplements (exclusive paramedical supplements)Single room No 0.080 0.5113** −0.0783 −0.0428 −0.0415 −0.1649** 0.4279** 0.2636* −0.0605 0.2537** 0.0314 0.0224 0.1021** 0.0996 −0.0747* −0.0485*
Yes 0.098 0.3909** 0.0579 −0.0518 0.0721 −0.1231* 0.3981* 0.4500 −0.0892 0.2883** 0.2153 −0.0471 0.0687 −0.3766** −0.0443 −0.0731
Two-person room No 0.106 0.0492** 0.0029 −0.0349** 0.0177* −0.0338** 0.2158** −0.0095 −0.0273* 0.0212 −0.0492** −0.0527** 0.0780** 0.1349 −0.0404** −0.0015Yes 0.049 0.0157** 0.0105 −0.0115* 0.0071 −0.0106 0.0402 −0.0233 −0.0119* −0.0098 −0.0157** −0.0164** 0.0406 −0.0083 −0.0138* −0.0021
Common room No 0.006 0.0190** −0.0132 −0.0125 −0.0117 −0.0109 0.0158 −0.0184** −0.0138 −0.0052 −0.0187** −0.0226* 0.0309 0.0034 −0.0063* −0.0029Yes 0.003 0.0069 −0.0017 −0.0057 −0.0031 −0.0037 −0.0025 −0.0067 −0.0058 −0.0057 −0.0061 −0.0089 0.0210 −0.0013 −0.0036 −0.0011
Relative drug supplementsSingle room No 0.004 0.8123** −0.2480 0.1203 0.0968 −0.0646 0.0912 −0.3774** −0.0248 0.0090 −0.0420 0.0161 0.0158 −0.7804** −0.0409 −0.1931*
Yes −0.001 0.2743 −0.0444 0.2204 −0.1197 −0.1553 −0.0185 0.0753 −0.1048 0.2388 0.0993 −0.0282 −0.0160 −0.2739** −0.0201 0.2082
Two-person room No −0.001 0.6892 −0.3928 −0.4675 −0.5945 −0.3524 −0.5523 −0.2801 −0.4551 −0.4907 −0.0341 −0.3642 −0.1991 −0.1885 −0.0366 0.3156Yes −0.002 0.2638** −0.0267 0.0186 0.0075 0.0204 −0.0412 −0.0753 −0.0321 0.0405 0.0240 0.1582 0.1085 −0.2564** −0.0289 0.0269
Common room No 0.003 0.4529** −0.1653 −0.0316 −0.0538 −0.0316 0.1273 −0.0411 0.0603 0.0047 0.0199 0.0205 0.0232 −0.4124** −0.0166 −0.0304Yes 0.001 0.2741** −0.0480 −0.0196 0.0525 −0.0405 0.8398 0.3579 0.1102 0.0565 0.0542 0.1009 −0.0207 −0.3369** −0.0429 0.0725
Relative material supplementsd
Single room No −0.001 0.6830** −0.1542 0.2452 0.1953 −0.2667 −0.0338 −0.4138 0.0514 −0.0007 −0.0218 −0.2257 −0.2436 −0.0748Yes 0.009 0.4247 1.1539 0.4101 −0.0193 0.1067 0.0626 −0.1255 0.1574 0.1023 −0.3898 −0.2810 −0.0738 −0.2571
Two-person room No 0.009 1.0975* −0.2964 −0.3187 −0.2497 −0.6277 0.2979 −1.2169* −0.0571 −0.4124 −0.3913 −0.9329 0.8599 −0.3992Yes −0.003 0.4391 −0.0327 0.0616 0.4753 −0.1956 0.0236 −0.4266 −0.1917 −0.1126 −0.2358 −0.2838 0.0186 −0.0199
Common room No 0.000 0.3707 0.0208 −0.2377 0.0020 0.0871 4.7121 −0.0428 −0.1939 −0.1698 0.2060 −0.0377 0.4129 0.3678Yes 0.003 0.5757* −0.3297 −0.2731 −0.2857 −0.4749 −0.2433 −0.4802 −0.2739 −0.3356 0.0110 −0.4617 0.1244 0.1165
Room supplements per daySingle room No 0.398 26.63** 14.02** −7.22** −6.60** −6.04** 51.47** 29.09** 0.74 7.92** 7.42** 11.11** −2.30 −18.48** −5.38** 5.80**
Yes 0.438 21.95** 15.50** −5.67** −2.31 −1.21 48.81** 19.98 1.74 7.27** 9.58* 10.00** −5.47 −18.39** −1.06 5.41**
Two-person room No 0.301 10.46** 5.33** −1.53** 0.45 −0.68 5.43** 6.87** 0.08 3.78** 6.81** −8.00** 1.56** −6.67** −0.80* 2.08**
Yes 0.313 9.78** 6.20** −1.74** 1.07* 0.39 6.34** 7.03** 1.52 4.01** 7.08** −7.42** 0.64 −7.47** −1.29** 2.05**
Common room No 0.000 0.00 0.00 0.00 0.00 0.00 0.03 0.00 0.03 0.00 0.00 0.00 −0.01 0.00 −0.01 0.00Yes −0.001 0.01 −0.01 0.00 −0.01 0.00 −0.01 −0.01 0.00 −0.01 −0.01 −0.01 0.00 0.00 0.00 0.00
Diverse supplements per daySingle room No 0.011 4.81** 1.81 1.50 0.04 −0.05 1.71 8.78 11.87** −3.01* 20.20 1.08 −2.28 −5.45** −2.57 3.39*
Yes 0.012 1.95 7.79 1.78 −0.50 −1.94 32.27 4.01 9.62 −4.28 13.00 4.71 −5.84 −3.39 −0.24 7.86*
Two-person room No 0.002 5.42* −2.44 −2.86 −0.31 −2.62 −2.47 19.23 −3.57 −0.14 1.97 −0.70 −1.88 −2.29 −2.57 3.34Yes 0.003 1.25 2.17 0.20 −0.26 0.59 2.29 1.01 0.68 2.47 0.71 5.00* −2.37** −2.62** 0.46 3.33*
Common room No 0.003 2.98** 2.59 1.93 0.84 0.19 −0.56 0.59 −1.47 −1.69 −0.12 1.55 −1.44 −3.11** −0.11 2.28**
Yes 0.009 2.70** 1.39 −0.40 0.40 0.61 −0.61 −0.58 −1.80* −1.90** 0.03 2.11 0.21 −1.87** 0.17 0.69
Shaded area: F-test for the model as a whole is not significant (p > 0.0001).a Prefstat = preferential status.b Chron hosp = chronic hospital, i.e. a geriatric hospital, or a hospital that specializes in specific services such as palliative care and rehabilitation.c Psych hosp = psychiatric hospital.d Due to multicollinearity problems, we leave out the dummies for type of hospital.* Significance of p < 0.001.
** Significance of p < 0.0001.
A. Lecluyse et al. / Health Policy 92 (2009) 276–287 285
Table 5Average absolute amounts of reimbursements, co-payments and supplements per inpatient stay and per inpatient day, according to room type andpreferential insurance status.
Room type Insurance Per stay Per day
Reimb Co-pay Suppl Reimb Co-pay Suppl
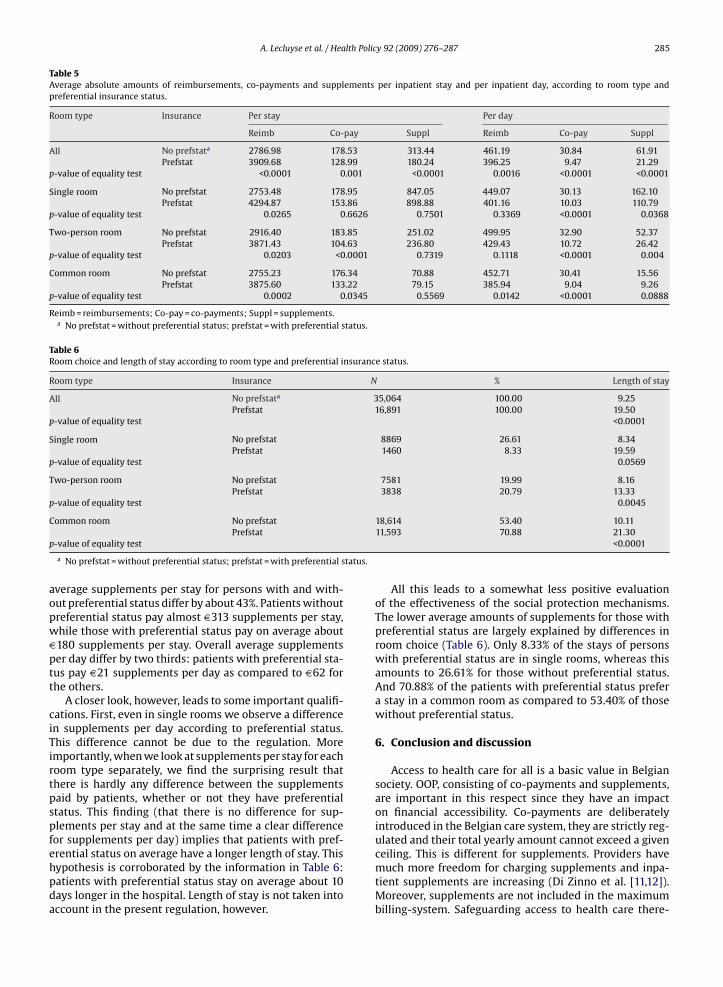
All No prefstata 2786.98 178.53 313.44 461.19 30.84 61.91Prefstat 3909.68 128.99 180.24 396.25 9.47 21.29
p-value of equality test <0.0001 0.001 <0.0001 0.0016 <0.0001 <0.0001
Single room No prefstat 2753.48 178.95 847.05 449.07 30.13 162.10Prefstat 4294.87 153.86 898.88 401.16 10.03 110.79
p-value of equality test 0.0265 0.6626 0.7501 0.3369 <0.0001 0.0368
Two-person room No prefstat 2916.40 183.85 251.02 499.95 32.90 52.37Prefstat 3871.43 104.63 236.80 429.43 10.72 26.42
p-value of equality test 0.0203 <0.0001 0.7319 0.1118 <0.0001 0.004
Common room No prefstat 2755.23 176.34 70.88 452.71 30.41 15.56Prefstat 3875.60 133.22 79.15 385.94 9.04 9.26
p-value of equality test 0.0002 0.0345 0.5569 0.0142 <0.0001 0.0888
Reimb = reimbursements; Co-pay = co-payments; Suppl = supplements.a No prefstat = without preferential status; prefstat = with preferential status.
Table 6Room choice and length of stay according to room type and preferential insurance status.
Room type Insurance N % Length of stay
All No prefstata 35,064 100.00 9.25Prefstat 16,891 100.00 19.50
p-value of equality test <0.0001
Single room No prefstat 8869 26.61 8.34Prefstat 1460 8.33 19.59
p-value of equality test 0.0569
Two-person room No prefstat 7581 19.99 8.16Prefstat 3838 20.79 13.33
p-value of equality test 0.0045
C
p
tatus.
aopwDptt
ciTirtpspfehpda
ommon room No prefstatPrefstat
-value of equality test
a No prefstat = without preferential status; prefstat = with preferential s
verage supplements per stay for persons with and with-ut preferential status differ by about 43%. Patients withoutreferential status pay almost D313 supplements per stay,hile those with preferential status pay on average about180 supplements per stay. Overall average supplementser day differ by two thirds: patients with preferential sta-us pay D21 supplements per day as compared to D62 forhe others.
A closer look, however, leads to some important qualifi-ations. First, even in single rooms we observe a differencen supplements per day according to preferential status.his difference cannot be due to the regulation. Moremportantly, when we look at supplements per stay for eachoom type separately, we find the surprising result thathere is hardly any difference between the supplementsaid by patients, whether or not they have preferentialtatus. This finding (that there is no difference for sup-lements per stay and at the same time a clear differenceor supplements per day) implies that patients with pref-
rential status on average have a longer length of stay. Thisypothesis is corroborated by the information in Table 6:atients with preferential status stay on average about 10ays longer in the hospital. Length of stay is not taken intoccount in the present regulation, however.18,614 53.40 10.1111,593 70.88 21.30
<0.0001
All this leads to a somewhat less positive evaluationof the effectiveness of the social protection mechanisms.The lower average amounts of supplements for those withpreferential status are largely explained by differences inroom choice (Table 6). Only 8.33% of the stays of personswith preferential status are in single rooms, whereas thisamounts to 26.61% for those without preferential status.And 70.88% of the patients with preferential status prefera stay in a common room as compared to 53.40% of thosewithout preferential status.
6. Conclusion and discussion
Access to health care for all is a basic value in Belgiansociety. OOP, consisting of co-payments and supplements,are important in this respect since they have an impacton financial accessibility. Co-payments are deliberatelyintroduced in the Belgian care system, they are strictly reg-ulated and their total yearly amount cannot exceed a given
ceiling. This is different for supplements. Providers havemuch more freedom for charging supplements and inpa-tient supplements are increasing (Di Zinno et al. [11,12]).Moreover, supplements are not included in the maximumbilling-system. Safeguarding access to health care there-
lth Polic
286 A. Lecluyse et al. / Heafore necessitates addressing supplements as well. In recentyears, more attention has indeed been given to the reg-ulation of extra billing in the Belgian hospital sector. Theprotection is focused on weaker socio-economic groupsand is differentiated according to the type of room.
A limitation of our analysis is the fact that we lackinformation on supplemental hospital insurance. This typeof voluntary insurance reimburses co-payments and extrabilling when the patient is hospitalised. The total shareof individuals with supplemental hospital insurance was62.40% in 2001, but it is likely to be higher in 2003. Take-upof such insurance shows a strong social gradient; individ-uals that are higher educated, in higher income classes,employed, and without preferential status are more likelyto have supplemental hospital insurance (Schokkaert et al.[13]). Moreover, it is well known that Belgian physicians dif-ferentiate their extra billing policy between patients withand without supplemental coverage. As such, it is likelythat we overestimated the out-of-pocket costs of hospi-talised patients with supplemental hospital insurance. Thisis especially the case in single and two-person rooms wheremore supplements are charged.
Our results show that in practice hospitals (seem to)respect the regulation. First, supplements are predomi-nantly charged in private rooms, to a lesser extent intwo-person rooms, and far less in common rooms. Second,the overall relative unit supplement price and the overalltotal amount of supplements to be paid per stay or per dayare lower for patients with preferential status. At the sametime, however, there is a large variation in price settingbehavior which cannot be explained by observable hospitalcharacteristics.
While overall averages suggest that patients with prefer-ential status are to some extent protected, a deeper analysisshows that this is not solely the result of the regulation.While for each type of room, the absolute amount of sup-plements per day is indeed lower thanks to the regulation,the absolute amount of supplements per stay does notdiffer according to insurance status. These apparently con-tradictory findings can be explained easily. First, patientswith preferential status are more likely to choose a com-mon room (with full protection against supplements) andonly a small part chooses a single room (with no protec-tion against supplements). Second, those patients tend tohave longer stays. This may be partly explained by the factthat patients with preferential status are on average sickerand poorer than other patients. Alternatively, it could wellbe that individuals without preferential status want to behospitalised for a shorter period, due to their higher oppor-tunity cost in terms of income lost. Moreover, they are morehighly educated on average and could therefore be moreefficient in choosing the best health care trajectory.
Our results have two important policy implications.First, prices vary greatly and observable hospital charac-teristics explain only a minor part of that variation. Whileit is somewhat reassuring that for room supplements – that
are a large part of the total supplements – 30% (two-personroom) to 40% (single room) of the variation among hospi-tals can be explained, the situation is much worse for feesupplements. Probably, the internal contracts between thephysician and the hospital play an important role in they 92 (2009) 276–287
price setting with respect to fee supplements. As Corens[14] indicates, specialists share their (official) fees with thehospital to compensate for the use of equipment and space.The degree of sharing depends on several factors, such asthe number of specialists in the specialty, the reputationof hospital and physician, the experience of the physician,etc. Moreover, in most hospitals, all fees are pooled andredistributed monthly. In any case, price setting is ratherintransparent both for the regulator and for the patients,despite the fact that hospitals are obliged to declare theirextra billing policy. Policies should be developed to improvethis transparency.
Second, our results showed that the regulation is notvery effective in safeguarding vulnerable patients fromlarge out-of-pocket costs: although the relative supple-ment prices and absolute amounts per day are lower, theabsolute amount of supplements per stay is not differ-ent between protected and non-protected patients. Sincepatients with preferential status have longer hospital stays,policy makers should consider how the regulation couldtake into account the length of the hospital stay.
Since currently supplements are highly linked to pri-vate rooms and our results show a social stratification inthe choice of room type, in which patients with preferen-tial status mostly choose common rooms, those patientsare better protected against extra billing. Yet the diverg-ing prices according to room type together with the socialstratification of room choice can endanger equity: policymakers should ascertain that this situation will not lead todifferences in the quality of care and service in the differenttypes of rooms [15].
Acknowledgements
This article is derived from De Graeve D, Lecluyse A,Schokkaert E, Van Ourti T, Van de Voorde C (2006). Eigenbetalingen in de Belgische gezondheidszorg. De impact vansupplementen. Equity and Patient Behaviour (EPB). Brussel:Federaal Kenniscentrum voor de gezondheidszorg (KCE);KCE reports 50 A (D/2006/10.273/68).
References
[1] Glazer J, McGuire TG. Should physicians be permitted to ‘balance bill’patients? Journal of Health Economics 1993;12:239–58.
[2] Kifmann M, Scheuer F. Balance billing: the patients’ perspective.Mimeo; 2006.
[3] Pauly MV. Insurance reimbursement. In: Cuyler AJ, Newhouse JP,editors. Handbook of health economics, vol. 1. Amsterdam: ElsevierScience B.V; 2000. p. 537–60.
[4] Paringer L. The Medicare assignment rates of physicians: theirresponses to changes in reimbursement policy. Health Care FinancingReview 1980;1:75–89.
[5] Mitchell JB, Cromwell J. Physician behavior under the Medicareassignment option. Journal of Health Economics 1982;1:245–64.
[6] Zuckerman S, Holahan J. The role of balance billing in Medicare physi-cian payment reform. In: Frech III HE, editor. Regulating doctors’ fees:competition, benefits and controls under medicare. Washington D.C:AEI Press; 1991. p. 143–69.
[7] Epp MJ, Vining AR, Collins-Dodd C, Love E. The impact of direct andextra billing for medical services: evidence from a natural experiment
in British Columbia. Social Science of Medicine 2000;51:691–702.[8] Northcott HC. Extra-billing and physician remuneration: a paradox.Canadian Public Policy 1982;8:200–6.
[9] McKnight R. Medicare balance billing restrictions: Impactson physicians and beneficiaries. Journal of Health Economics2007;26:326–41.

lth Polic
[
[
[
[
Health Economics 2009, forthcoming.
A. Lecluyse et al. / Hea
10] De Graeve D, Lecluyse A, Schokkaert E, Van Ourti T, Van de VoordeC. Eigen betalingen in de Belgische gezondheidszorg. De impact vansupplementen, Equity and Patient Behaviour (EPB). Brussel: Feder-aal Kenniscentrum voor de gezondheidszorg (KCE), KCE reports 50A;2006.
11] Di Zinno T, Huchon J, Laasman J-M. Coûts hospitaliers: nature,
ampleur et évolution des frais à charge du patient hospitalisé enhôpital général. Etudes et analyses. Bruxelles: UNMS; 2005. Availablefrom: http://www.mutsoc.be/NR/rdonlyres/EB601C3F-C7EC-43C2-B567-0D3A2F04E94B/0/Etudesupplementhopitaux2005.pdf.12] Di Zinno T, Huchon J, Laasman J-M, Vanoverloop J. Coûts hospitaliers:nature, ampleur et évolution des frais à charge du patient hospitalisé
[
[
y 92 (2009) 276–287 287
en hôpital général. Etudes et analyses. Bruxelles: UNMS; 2006. Avail-able from: http://www.mutsoc.be/NR/rdonlyres/40085978-12E4-4C5B-A19D-582A46F7A0D5/0/couts hospitaliers2006.pdf.
13] Schokkaert E, Van Ourti T, De Graeve D, Lecluyse A, Van de VoordeC. Supplemental health insurance and equality of access in Belgium.
14] Corens D. Health system review, vol. 9. Belgium: Health Systems inTransition;; 2007, 1–172.
15] van de Glind I, de Roode S, Goossensen A. Do patients in hospi-tals benefit from single rooms? A literature review. Health Policy2007;84:153–62.
Copyright © 2022 FDOKUMEN