Nail the Job Interview 101 Dynamite Answers to Interview ...
Upload
independentCategory
view
0download
0
Hospital inpatients� experiences of access to food: aqualitative interview and observational study
Smriti Naithani BSc MSc,* Kevin Whelan BSc MSc PhD,� Jane Thomas BSc MMedSci,�Martin C Gulliford MA FRCP FFPH§ and Myfanwy Morgan BA MA PhD FFPH–
*Research Assistant, Division of Health and Social Care Research, Department of Public Health Sciences, �Lecturer, Nutritional
Sciences Division, �Senior Lecturer, Nutritional Sciences Division, §Professor, Division of Health and Social Care Research,
Department of Public Health Sciences and –Reader, Division of Health and Social Care Research, Department of Public Health
Sciences, King�s College London, London, UK
Correspondence
Ms Smriti Naithani
Department of Public Health Sciences
King�s College London
Capital House
42 Weston St
London
SE1 3QD
UK
E-mail: [email protected]
Accepted for publication
2 January 2008
Keywords: access to services, food
service, hospital, hunger, patient
experience, qualitative
Abstract
Background Hospital surveys indicate that overall patients are
satisfied with hospital food. However undernutrition is common and
associated with a number of negative clinical outcomes. There
is little information regarding food access from the patients�perspective.
Purpose To examine in-patients� experiences of access to food in
hospitals.
Methods Qualitative semi-structured interviews with 48 patients
from eight acute wards in two London teaching hospitals. Responses
were coded and analysed thematically using NVivo.
Results Most patients were satisfied with the quality of the meals,
which met their expectations. Almost half of the patients reported
feeling hungry during their stay and identified a variety of
difficulties in accessing food. These were categorized as: organi-
zational barriers (e.g. unsuitable serving times, menus not
enabling informed decision about what food met their needs,
inflexible ordering systems); physical barriers (not in a comfort-
able position to eat, food out of reach, utensils or packaging
presenting difficulties for eating); and environmental factors (e.g.
staff interrupting during mealtimes, disruptive and noisy behav-
iour of other patients, repetitive sounds or unpleasant smells).
Surgical and elderly patients and those with physical disabilities
experienced greatest difficulty accessing food, whereas younger
patients were more concerned about choice, timing and the
delivery of food.
Conclusions Hospital in-patients often experienced feeling hungry
and having difficulty accessing food. These problems generally
remain hidden because staff fail to notice and because patients are
reluctant to request assistance.
doi: 10.1111/j.1369-7625.2008.00495.x
294 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303

Introduction
Undernutrition is common in hospital in-
patients, with a prevalence of between 13% and
40% reported in the UK1–3 and throughout the
world.4 Undernutrition is independently asso-
ciated with a number of negative clinical out-
comes, including increased complication rates,
mortality, longer hospital stays and increased
costs.5 Hospital admission can be associated
with a deterioration in the nutritional status of
both normally nourished and undernourished
patients.1 This arises from a range of factors
including the pathophysiological and metabolic
consequences of illness, together with a relative
failure of food intake. Ensuring that patients
receive adequate nutrition is therefore an
essential part of clinical care as recognized by
the recommendations of the Council of
Europe.4
In the United Kingdom, a number of reports
have identified inadequacies in dietary intake of
inpatients, including Hungry in Hospital6 and
more recently, Hungry to be Heard.7 In response
to these and other reports, the issue of food
access in hospitals has moved up the agenda of
professional bodies8 and the government.9 One
core standard recommends that �there should be
sufficient information to allow patients to access
appropriate food; food provided should meet
the patient�s needs, missed meals should be
replaced; assistance to eat and drink should be
provided where necessary; and food should be
appropriately presented and consumed in a
conducive environment�.9 These objectives are
currently being addressed through the National
Health Service Plan10 and the Better Hospital
Food initiative.11
The role of the doctor is underlined in the
report Nutrition and Patients: a Doctors
Responsibility8, which emphasizes that doctors
should be �familiar with relevant aspects of
food service to their patients and the impor-
tance of dietary intake�. Recent surveys indicate
that overall, patients reported a positive expe-
rience of their time in hospital.12,13 Since 2002,
the Inpatient surveys commissioned by the
Healthcare Commission have reported little
change in how patients have rated hospital
food. Over half of patients are said to be sat-
isfied with hospital food; 54% of patients rated
the food as �very good, or good� in 2006. The
survey also found that almost four-fifths of
patients (79%) said they were given a choice of
food while in hospital13. However there is little
information regarding the patient�s experience
of the organization and environmental factors
that affect their eating experience. The aim of
this study was therefore to investigate hospital
patients� experiences of access to food in terms
of satisfaction with meals and factors influenc-
ing their physical ability to eat and the quality
of meals.
Methods
Study design
A qualitative approach using semi-struc-
tured interviews with hospital in-patients,
supplemented by informal observations of
mealtimes.
Study setting
The study was conducted on eight acute wards
across two London teaching hospital sites.
Each ward contained approximately 29 beds
comprising four patient bays (4–6 beds per
bay) and four single side rooms. Both hospi-
tals used a bulk-order system, whereby food is
prepared in the hospital kitchens, delivered in
bulk to individual wards and then reheated in
a heating trolley. At mealtimes the trolley was
wheeled into the ward corridor. A catering
assistant served patients� meals to nurses,
health-care assistants or support staff whose
responsibility it is to serve the food to patients
and provide assistance when required. At the
end of the meal the catering assistant collected
the plates. Breakfast was served between 7:30
and 8:00, lunch service began at 12:00 and
lasted 45 min and the evening meal service
began at 18:00 and was similar to lunch in
terms of the service, choice of food available
and duration.
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
295
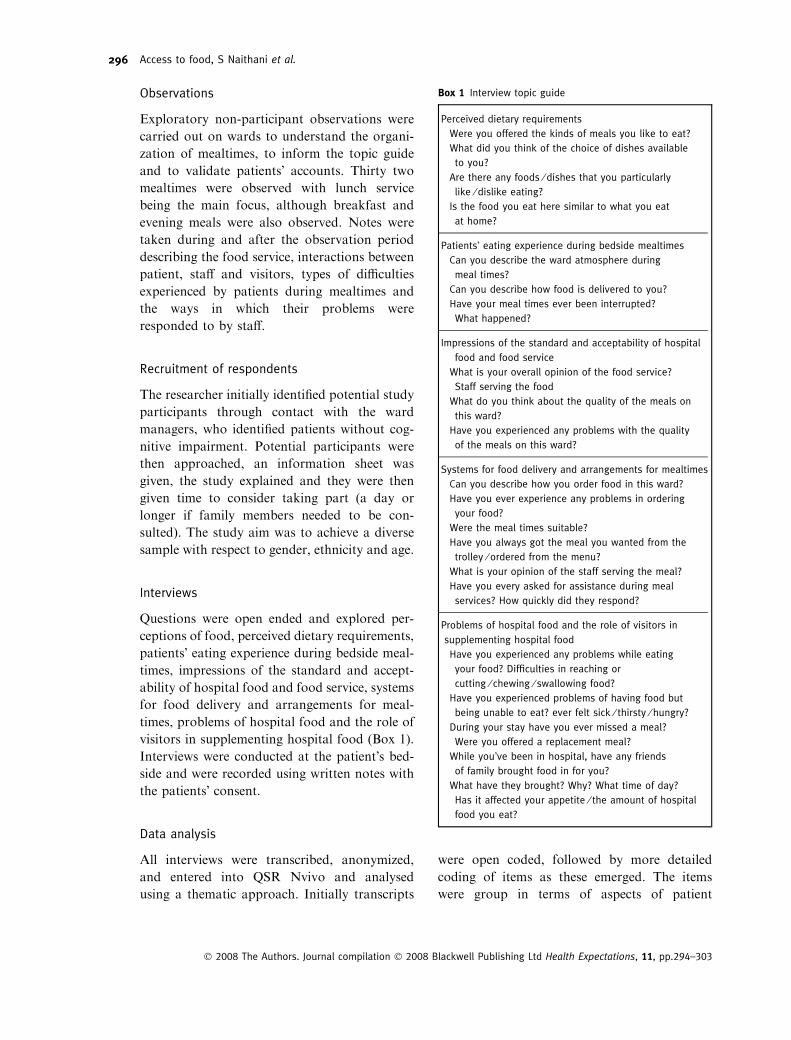
Observations
Exploratory non-participant observations were
carried out on wards to understand the organi-
zation of mealtimes, to inform the topic guide
and to validate patients� accounts. Thirty two
mealtimes were observed with lunch service
being the main focus, although breakfast and
evening meals were also observed. Notes were
taken during and after the observation period
describing the food service, interactions between
patient, staff and visitors, types of difficulties
experienced by patients during mealtimes and
the ways in which their problems were
responded to by staff.
Recruitment of respondents
The researcher initially identified potential study
participants through contact with the ward
managers, who identified patients without cog-
nitive impairment. Potential participants were
then approached, an information sheet was
given, the study explained and they were then
given time to consider taking part (a day or
longer if family members needed to be con-
sulted). The study aim was to achieve a diverse
sample with respect to gender, ethnicity and age.
Interviews
Questions were open ended and explored per-
ceptions of food, perceived dietary requirements,
patients� eating experience during bedside meal-
times, impressions of the standard and accept-
ability of hospital food and food service, systems
for food delivery and arrangements for meal-
times, problems of hospital food and the role of
visitors in supplementing hospital food (Box 1).
Interviews were conducted at the patient�s bed-
side and were recorded using written notes with
the patients� consent.
Data analysis
All interviews were transcribed, anonymized,
and entered into QSR Nvivo and analysed
using a thematic approach. Initially transcripts
were open coded, followed by more detailed
coding of items as these emerged. The items
were group in terms of aspects of patient
Box 1 Interview topic guide
Perceived dietary requirements
Were you offered the kinds of meals you like to eat?
What did you think of the choice of dishes available
to you?
Are there any foods ⁄ dishes that you particularly
like ⁄ dislike eating?
Is the food you eat here similar to what you eat
at home?
Patients� eating experience during bedside mealtimes
Can you describe the ward atmosphere during
meal times?
Can you describe how food is delivered to you?
Have your meal times ever been interrupted?
What happened?
Impressions of the standard and acceptability of hospital
food and food service
What is your overall opinion of the food service?
Staff serving the food
What do you think about the quality of the meals on
this ward?
Have you experienced any problems with the quality
of the meals on this ward?
Systems for food delivery and arrangements for mealtimes
Can you describe how you order food in this ward?
Have you ever experience any problems in ordering
your food?
Were the meal times suitable?
Have you always got the meal you wanted from the
trolley ⁄ ordered from the menu?
What is your opinion of the staff serving the meal?
Have you every asked for assistance during meal
services? How quickly did they respond?
Problems of hospital food and the role of visitors in
supplementing hospital food
Have you experienced any problems while eating
your food? Difficulties in reaching or
cutting ⁄ chewing ⁄ swallowing food?
Have you experienced problems of having food but
being unable to eat? ever felt sick ⁄ thirsty ⁄ hungry?
During your stay have you ever missed a meal?
Were you offered a replacement meal?
While you�ve been in hospital, have any friends
of family brought food in for you?
What have they brought? Why? What time of day?
Has it affected your appetite ⁄ the amount of hospital
food you eat?
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
296
satisfaction with food, their eating experience
and perceived problems during mealtimes. The
data were mapped onto the some dimensions of
access;14 these included physical barriers,
organizational and environmental factors. For
each aspect both positive and negative experi-
ences were categorized together with the ways
in which their problems were responded to by
staff. Each stage of the analysis coding and
interpretations discussed with the team and a
consensus reached.
Ward managers gave informed consent to the
researcher being present as an observer and con-
ducting interviews with staff after they received
written information about the study. Ethical
approval was granted by the hospital trust.
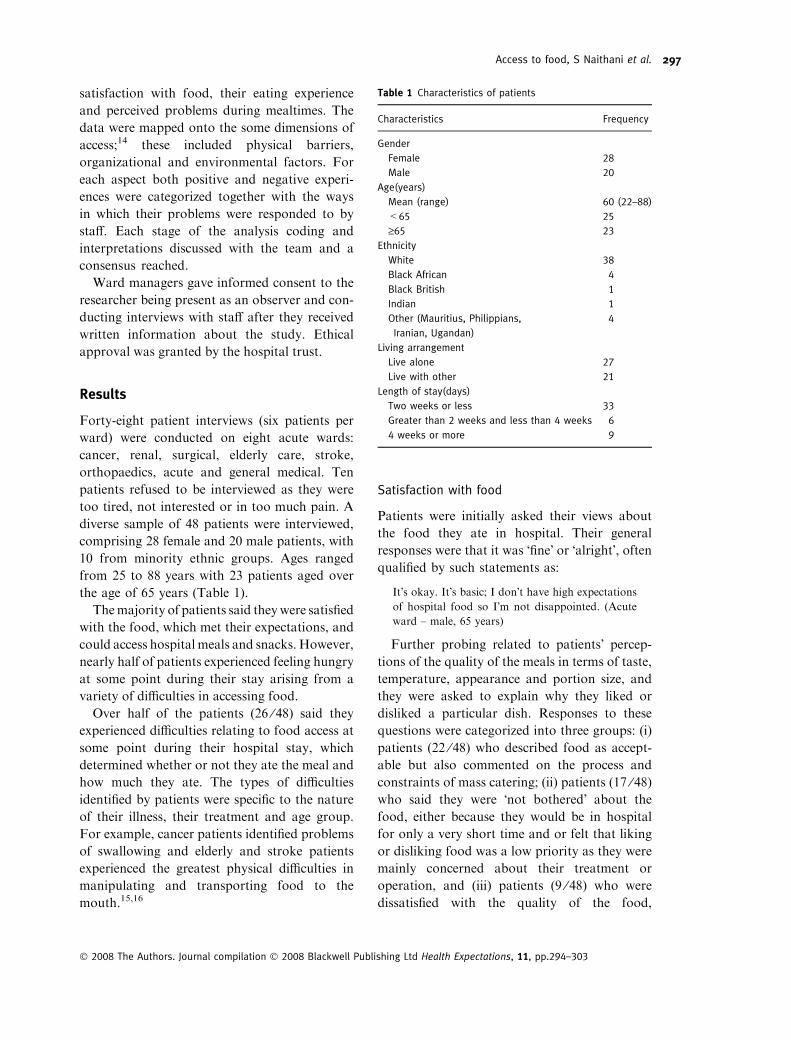
Results
Forty-eight patient interviews (six patients per
ward) were conducted on eight acute wards:
cancer, renal, surgical, elderly care, stroke,
orthopaedics, acute and general medical. Ten
patients refused to be interviewed as they were
too tired, not interested or in too much pain. A
diverse sample of 48 patients were interviewed,
comprising 28 female and 20 male patients, with
10 from minority ethnic groups. Ages ranged
from 25 to 88 years with 23 patients aged over
the age of 65 years (Table 1).
Themajority of patients said theywere satisfied
with the food, which met their expectations, and
could access hospital meals and snacks. However,
nearly half of patients experienced feeling hungry
at some point during their stay arising from a
variety of difficulties in accessing food.
Over half of the patients (26 ⁄48) said they
experienced difficulties relating to food access at
some point during their hospital stay, which
determined whether or not they ate the meal and
how much they ate. The types of difficulties
identified by patients were specific to the nature
of their illness, their treatment and age group.
For example, cancer patients identified problems
of swallowing and elderly and stroke patients
experienced the greatest physical difficulties in
manipulating and transporting food to the
mouth.15,16
Satisfaction with food
Patients were initially asked their views about
the food they ate in hospital. Their general
responses were that it was �fine� or �alright�, oftenqualified by such statements as:
It�s okay. It�s basic; I don�t have high expectations
of hospital food so I�m not disappointed. (Acute
ward – male, 65 years)
Further probing related to patients� percep-
tions of the quality of the meals in terms of taste,
temperature, appearance and portion size, and
they were asked to explain why they liked or
disliked a particular dish. Responses to these
questions were categorized into three groups: (i)
patients (22 ⁄48) who described food as accept-
able but also commented on the process and
constraints of mass catering; (ii) patients (17 ⁄48)who said they were �not bothered� about the
food, either because they would be in hospital
for only a very short time and or felt that liking
or disliking food was a low priority as they were
mainly concerned about their treatment or
operation, and (iii) patients (9 ⁄48) who were
dissatisfied with the quality of the food,
Table 1 Characteristics of patients
Characteristics Frequency
Gender
Female 28
Male 20
Age(years)
Mean (range) 60 (22–88)
<65 25
‡65 23
Ethnicity
White 38
Black African 4
Black British 1
Indian 1
Other (Mauritius, Philippians,
Iranian, Ugandan)
4
Living arrangement
Live alone 27
Live with other 21
Length of stay(days)
Two weeks or less 33
Greater than 2 weeks and less than 4 weeks 6
4 weeks or more 9
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
297

regarding it as unhealthy (e.g. fried), not cooked
to their personal taste, not served attractively or
not smelling appetising. An opinion held by over
half (6 ⁄10) of minority ethnic patients. Elderly
patients� were reported to be dissatisfied and put
off by the portion sizes, with even the standard
size regarded as too large particularly during
periods of inactivity and when they experiences a
loss of appetite.
Organizational barriers
Frequently cited (25 ⁄48) causes of patients
feeling hungry were that hospital food was not
available after admission, between meal times
and after their treatment.
When I came here on this ward they said I had to
wait and see a doctor, we waited for ages I didn�tget to sleep till 12 and all that time we waited I
didn�t have anything to eat. I was hungry. I asked
the nurse for a cup of tea and she gave me one but
I didn�t have anything to eat. (Care of the Elderly
ward – female, 69 years)
Another difficulty was the early time of the
evening meal:
I do get hungry around 8 or 9 o�clock, that�sbecause they serve dinner too early. That�swhen I get really hungry. They do give us a cup
of tea and some biscuits but that isn�t enough
really. I�m still hungry. (Stroke ward – male,
81 years)
Patients also reported a lack of access to
snacks and drinks between meals, and some
patients who were offered snacks considered that
the amount provided was inadequate. Two
patients reported that a lack of food resulted in
them feeling very agitated and finding it difficult
to rest.
They didn�t offer my anything, they didn�t check on
me and see if I was hungry, if I wanted anything to
eat…. I�m glad I had something before I came
because I didn�t have anything after that, nothing
come to think of that…. I was hungry; I didn�tsleep that night. (Surgical ward – female, 51 years)
The solution for some patients was for family
members to bring food in for them. For three
patients, outside meals were regarded as the
main meal of the day.
Always evening meal, my wife can only visit in the
evenings. She will bring me a variety of things,
from M&S sandwiches, cold meat and cooked
dinners, like casseroles, pies. I never go hungry.
She brings that every day so I don�t have to worry
about going hungry. (Surgical ward – male,
56 years)
Ordering system
All patients were able to accurately describe the
system for ordering meals and reported it to be
simple and straightforward. However 16
patients experienced difficulties in ordering
meals, with the most common problem (12 ⁄16)being that menus did not provide enough
information about the ingredients used and the
nutritional value of meals to allow them to make
an informed decision about which meal met
their needs.
I�m diabetic, I have to be careful when I choose
what food to eat. Here it is difficult to tell which
foods are good and which are bad. There isn�tenough information on the sheet so you can�t get aclear idea of what is in the food and in my case
whether it is suitable for me, suitable for a dia-
betic…. I get my wife to have a look at it and she�lltell me what is good and what is bad. She has some
difficulty with it as well because she can only guess
whether the food is low in sugar or not. (Stroke
ward – male, 81 years)
Another problem for patients with visual
impairments or poor literacy was the usefulness
of menus if assistance was not given. Observa-
tional data revealed that these types of problems
were more likely to be avoided or corrected
quickly on wards where food service was
supervised by a senior staff member or sup-
ported by a longstanding catering assistant.
Serving times
Over a third of patients (19 ⁄48) reported that
meals were served at times that were not con-
sistent with their normal habits. Although
patients often considered that breakfast was
served too early, this was not perceived as a
major problem because breakfast was not the
most important meal of the day. The majority of
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
298

patients considered the evening meal as their
main meal. As a result of early service of the
evening meal (6 pm), a few patients (8 ⁄48) eitherskipped their meal or were unable eat the meal
and as a result felt hungry later in the evening.
Enough time to eat
The majority of patients said they had enough
time finish their meal. However post-surgical
patients and patients with difficulties in eating
due to disability or age commented that there
was insufficient time to eat. Although patients
said they were not overtly pressured from staff
to stop eating, they felt rushed and compelled to
stop eating when staff returned to collect their
plates.
It takes a long time to eat because I have to use
my left hand. Picking up food and cutting is a bit
tricky. I can do, I don�t need help but it takes a
long time… usually the time they give would be
sufficient but because I have to use my other hand
eating takes longer. I�m sure they would give us
more time but when the lady comes round with
the trolley collecting up the plates I tend to give
her mine even when I haven�t finished. I feel I
have to. She looks fed up and I get the impression
that she wouldn�t be too happy if I ask her to
come back later. (Care of the elderly ward – male,
76 years)
Physical barriers
Physical barriers to eating presented difficulties
for a many elderly patients (9 ⁄48) and post-
surgical patients (7 ⁄48). These included inap-
propriate seating and trolley positioning result-
ing in food being placed out of reach and
patients experiencing difficulties in transporting
food to mouth; and being given inappropriate
utensils to feed themselves.
The only problem with dessert is using the des-
sertspoon. They are so big and I can�t open my
mouth wide enough because of all the sores, they
will start to weep or bleed and it�s actually really
painful. I can�t use it. (Cancer ward – female,
86 years)
Observational data supported this but also
identified that patients with visual or hearing
impairments were not always aware that food
and drink had been served.
Help and assistance
Elderly patients, post-surgical patients and those
with physical disabilities faced greater barriers
to eating compared with other patients and more
often expressed dissatisfaction with lack of
support during mealtimes.
Observations revealed that this often meant
that assisting and monitoring patients during
meal times was often sidelined as a low priority
activity. Staff were seen to complete paper work,
change beds and arrange care plans during
mealtimes.
Twelve patients required assistance and nine
of them reported difficulties in getting staff
attention and felt that problems reported to
support staff were not always followed up.
They rarely walk around the bay during meal times.
So when I�ve wanted their help they�re not around
or I�d have to wait a long time before I could get
someone�s attention. I can�t really be bothered to
wait so I get on with it. I do what I can, the things I
can reach and cut I eat, the things I can�t I leave.(Orthopaedic ward – female, 57 years)
When I�ve needed my food cutting or if I�vedropped something . . . sometimes they�ve forgot-
ten and I have to ask them again. Once I waited for
over 10 minutes before someone came and helped
me. It�s difficult sometimes to get their attention
because they don�t always come into the room… I
can see they are still around but they seem to be
doing paper work or something. (Stroke ward –
female, 81 years)
Observations made during meal times indi-
cated that if meals were left, the assumption
made by staff was that patients did not want
them and so they were removed. However, the
reason for some patients was that they were
unable to feed themselves.
Five of the 12 patients who experienced
physical difficulties were reluctant to inform staff
and felt powerless to complain:
I was having my dressing changed when lunch
came. They asked me if I wanted my food to be
served. I said yes because the nurse said it wouldn�t
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
299

take long but it did. By the time she�d finished my
food had gone cold, well it was lukewarm and
everyone else had finished eating. I wasn�t happyabout that but what can you do. I like my food to
be hot; the food was lukewarm. I ate it anyway
because I was hungry but the food was spoilt, it had
gone cold. (Orthopaedic ward – female, 51 years)
Environmental factors
Patients were asked to describe the environment
on the ward during meal times. Five out of the
eight wards were perceived as noisy. Patients
staying in general and emergency wards identi-
fied particular noise problems, in terms of the
sounds of equipment and the movement of
patients and different medical staff through the
wards at meal times. Patients (13 ⁄48) also stated
that the disruptive behaviour of other patients,
the repetitive sounds of equipment and
unpleasant smells had a negative effect on meal
consumption and the overall eating experience.
It has been noisy; staff are always rushing in and
out of the bays… The lady in the end bed she�s gotsome problem with her bowels. While I was having
my lunch she used the commode, which is off
putting… but what made it worse is that they left it
by the side. The smell was awful. That put me right
off my food. It made me heave at one point, I kept
my eyes locked on the window and tried to think
about something else just to distract me and stop
me from being sick. (Acute ward – female,
34 years)
Altogether eleven patients� described the
working practices of staff during meal times as
disruptive:
When they put things in that bin (points to bin at
the entrance of the bay) the lid when it comes
down makes an awful bang sound. It goes on at
night as well. It�s really irritating. It�s so loud. Staff
sometimes clean the floor around you when you�reeating that can be annoying. (Elderly ward –
female, 82 years)
Some patients also identified interruptions by
doctors as a factor responsible of temporarily
stopping or preventing them from eating their
meal.
The doctor came round, I think she was running
late, she said she would only be a little while and I
could have me lunch brought in but she said for
ages. By the time she left my food had gone cold,
so I didn�t eat it. (General medical – male 76 years)
Discussion
This study indicates that the overall quality of
food is acceptable to the majority of patients
and supports existing studies measuring inpa-
tients� satisfaction with hospital food.14,17
Patients� responses about food acceptability
were however often influenced by their low
expectations of hospital food and food provi-
sion, their understanding of the constraints of
the processes of mass catering, their high regard
of medical treatment over importance of food
taste and the ability to seek out alternative ways
to access food of their choice. However the
current study goes beyond this and takes into
consideration factors outside of the food itself
that impact upon the patients� experience, andidentified organizational, physical, and envi-
ronmental barriers have a major impact on
patients� experiences of mealtimes in hospital.
Over half the patients felt hungry at some
point during their stay in hospital, with this
being widespread across men and women and
different age groups. This was partly the result
of limited availability of food outside of meal
times, especially immediately following admis-
sion where patients may have missed their
evening meal. Other common problems were
that breakfast and the evening meal were viewed
as being too early, with little food being avail-
able between meals. Some patients were looking
to eat in ways that would promote their health,
but were not enabled to contribute to their own
care in this way because of features of the meal
delivery system in hospital. For example some
patients experienced difficulties choosing meals
or specials diets because of a lack of information
available. Whereas for others difficulties arose
through not being able to reach food, manipu-
late utensils or to feed themselves, which was
particularly important if they were given insuf-
ficient time to finish eating or if needed help was
not provided. This corresponds with findings
from the 2006 Healthcare commission survey
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
300

which indicated that 20% patients said they did
not get enough help from staff to eat their meals.
Of those patients who needed help to eat their
meals, fewer said they always received it.13
Our study indicated that physical, organiza-
tional and environmental factors affecting the
quality of hospital meal times were widespread,
and included interruptions for medical or nurs-
ing care, noises and smells from other patients,
or cleaning being carried out around the
patients� beds.The Protected Mealtimes scheme introduced
in 2001 is an initiative aimed at improving the
eating experience for patients in hospital, from
presentation of food to assistance at mealtimes.
Audits indicate that where this scheme has been
implemented patients report greater satisfaction
with their meals and fewer interruptions.18
However in many cases this scheme has not been
fully implemented and surveys indicate that
patients� still experience interruptions by hospi-
tal providers during mealtimes.6,19,20 Studies
implementing a Protected Mealtimes scheme
have often shown that this can lead to tension
between nursing staff who try to ensure it works
and medical colleagues who are not convinced of
its value.21 Our study supports this, with
patients� accounts or observation identifying
occasions when Protected Mealtimes were not
fully implemented by all health-care staff work-
ing within the wards. In some wards it appeared
more difficult to implement Protected Meal-
times, for example on surgical and acute wards
surgeons were seen consulting during mealtimes
and on the renal ward patient�s dialysis treat-
ment clashed with meal service.
Whereas previous studies have shown that
undernutrition increased with and longer length
of stay,22,23 in our study, short stay patients (less
than 2 weeks) reported more problems arising
from the quality of food and food service during
mealtimes compared with long stay patients
(longer than a month). Reasons may be that
long stay patients may have already learned
coping strategies and therefore be better
prepared to deal with potential difficulties com-
pared with short stay patients or that family and
friends provide food and assistance while eating.
Studies that have attempted to address prob-
lems of undernutrition have highlighted the
importance of reducing organizational, physical
and environmental barriers to accessing hospital
food. For example a trial among patients on
elderly wards, showed that eating at a dining
table increased their energy intake,24 and pro-
tected them from interruption during mealtimes
leading to improve nutritional status (less weight
loss and improved mid-arm circumference).25
The current study supports the importance of
organizational and environmental factors and
indicates that these have significant influences on
access to food among all ages and not only
elderly patients.
Strengths and limitations of study
A strength of this study was that it included
different types of wards and included both
elderly and young patients with a wide range of
medical conditions. A limitation is that the study
was carried out in only two hospitals, both of
which used bulk ordering systems. Different
food service systems can result in differences in
food consumption and food wastage26,27 and it
is possible that they may have different impli-
cations for patients� experiences of food access,
choice and other aspects of patient care. A sec-
ond limitation was that only those patients who
were able to give informed consent and were well
enough to be interviewed were recruited.
Patients who were too ill to participate, or
unable to consent, may well be those with
additional problems of food access and at the
greatest risk of undernutrition. A third limita-
tion of the study was that interviews focused on
the problems and barriers patients experienced
at mealtimes and did not explore in depth what
they found positively helpful or their thoughts
about potential solutions to the difficulties they
experienced.
Conclusions
Currently nutritional care has a low priority in
hospitals.6, 7 Our study indicates that all
age groups experienced organizational and
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
301

environmental barriers during mealtimes on
hospital wards and many elderly and post-surgi-
cal patients had physical difficulties in eating
while a more general difficulties was the unavail-
ability of food between meals and the missing of
meals. These problems led to many patients
feeling hungry at some point during their hospital
stay. However, these difficulties of accessing food
often remain hidden because staff fail to notice
and patients are reluctant to request assistance.
This indicates that patients� eating experience andnutritional care requires adherence with the
principles of Protected Mealtimes where other
activities are not undertaken on the ward while
meals are served or eaten and increased attention
to identifying and addressing patients� needs forassistance. However in circumstances where this
is not practical an alternative solution would be
to positively suggest to patients that they might
enjoy their food more if it was taken away and
kept hot while the doctor spoke with them. This
flexible approach requires the organization and
availability of sufficient staff able to assist with
ordering and feeding and increased importance
assigned to this aspect of patient care, as well as
good co-ordination of activities among catering
assistants, nurses and domestic staff.
Acknowledgement
This research was supported by the Guy�s and St
Thomas� Charity.
Declarations
1. This study was approved by the research
Ethics Committee of Guy�s Hospital,
London.
2. The Guy�s and St Thomas� Charity funded
the study.
3. None of the authors is aware of any conflict
of interest with respect to this paper.
References
1 McWhirter JP, Pennington CR. Incidence and
recognition of malnutrition in hospital. BMJ, 1994;
308: 945–948.
2 Kelly IE, Tessier S, Cahill A et al. Still hungry in
hospital: identifying malnutrition in acute hospital
admissions. QJM, 2000; 93: 93–98.
3 Edington J, Boorman J, Durrant ER et al. Prevalence
of malnutrition on admission to four hospitals in
England. Clinical Nutrition, 2000; 19: 191–195.
4 Council of Europe Committee of Experts on
Nutrition FSaCP. Food and Nutritional Care in
Hospitals: How to Prevent Under-Nutrition.
Strasbourg: Council of Europe Publishing, 2003.
5 Correia MI, Waitzberg DL. The impact of malnutri-
tion on morbidity, mortality, length of hospital stay
and costs evaluated through a multivariate model
analysis. Clinical Nutrition, 2003; 22: 235–239.
6 Association of Community Health Councils for
England and Wales. Hungry in Hospital? London:
CHC, 1997.
7 Age Concern. Hungry to be Heard. The Scandal of
Malnourished Older People in Hospital. London: Age
Concern, 2006.
8 Report of a working party of the Royal College of
Physicians. Nutrition and Patients. A doctor�sResponsibility. London: Royal College of Physicians,
2002.
9 Department of Health. Patient Focused Benchmarks
for Clinical Governance. London: NHS Modernisa-
tion Agency ⁄Department of Health, 2003.
10 Department of Health. The NHS Plan: A Plan for
Investment, A Plan for Reform. London: HMSO, 2000.
11 NHS Estates. Better Hospital Food. 2007. Source.
Available at: http://195.92.246.148/nhsestates/
better_hospital_food/bhf_content/introduction/
home.asp, accessed on 22 May 2007.
12 Department of Health. Acute Inpatient Survey:
National Overview 2001 ⁄ 02. London: HMSO, 2003.
Available at: http://www.dh.gov.uk/en/
Publicationsandstatistics/Publications/Publications
Statistics/DH_4066592, accessed on 22 May 2007.
13 Healthcare Commission. Inpatients: The Views of
Hospital Inpatients in England. Key findings
from the 2006 survey. Available at: http://
www.healthcarecommission.org.uk, accessed on 22
May 2007.
14 Gulliford M, Munoz JF, Morgan M et al. What does
�access to health care� mean? Journal of Health
Services Research & Policy, 2002; 7: 186–188.
15 Westergren A, Karlsson S, Anderson P, Ohlsson O,
Hallberg IR. Eating difficulties, need for assisted
eating, nutritional status and pressure ulcers in
patients admitted for stroke rehabilitation. Journal
of Clinical Nursing, 2001; 10: 257–269.
16 O�Hara PA, Harper DW, Kangas M, Dubeau J,
Borsutzky C, Lemire N. Taste, temperature, and
presentation predict satisfaction with foodservices in
a Canadian continuing-care hospital. Journal of the
American Dietetic Association, 1997; 97: 401–405.
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
302

17 Stanga Z, Zurfluh Y, Roselli M, Sterchi AB, Tanner
B, Knecht G. Hospital food: a survey of patients�perceptions. Clinical Nutrition, 2003; 22: 241–246.
18 Robinsion G, Goldstein M, Levine GM. Impact of
nutritional status on DRG length of stay. JPEN.
Journal of Parenteral and Enteral Nutrition, 1987; 11:
49–51.
19 Beth Horwell. Protected Mealtimes and Visiting
Hours, Elderly ward, YH, Audit Report 2006. York
Hospital NHS Trust, June 2006.
20 Commission for Patient and Public Involvement in
Health. Shaping Health. PPI Forums joining forces to
tackle NHS Food. Food Watch August–October 2006:
National Summary.
21 Savage J, Scott C Patients� Nutritional Care in Hos-
pital: An Ethnographic Study of Nurses� Role and
Patients� Experiences. London: RCN, 2005. Available
at: http://www.rcn.org.uk/downloads/research/insti-
tute/PatientsNutritionalCareInHospital.doc, accessed
22 May 2007.
22 Wade DT, Hewer RL. Motor loss and swallowing
difficulty after stroke: frequency, recovery and prog-
nosis. Acta Neurologica Scandinavica, 1987; 76: 50–
54.
23 Anderson MD. Malnutrition and length of stay – a
relationship? Henry Ford Hospital Medical Journal,
1985; 34: 190–193.
24 Wright L, Hickson M, Frost G. Eating together is
important: using a dining room in an acute elderly
medical ward increases energy intake. Journal of
Human Nutrition and Dietetics, 2006; 19: 23–26.
25 Das AK, McDougall T, Smithson JA, West RM.
Benefits of family mealtimes for nursing home resi-
dents: protecting mealtimes may similarly benefit el-
derly inpatients. BMJ, 2006; 332: 1334–1335.
26 Wilson A, Evans S, Frost G. A comparison of the
amount of food served and consumed according to
meal service system. Journal of Human Nutrition and
Dietetics, 2000; 13: 271–275.
27 Hickson M, Fearnley L, Thomas J, Evans S. Does a
new steam meal catering system meet patient
requirements in hospital? Journal of Human Nutrition
and Dietetics, 2007; 20: 476–485.
Access to food, S Naithani et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd Health Expectations, 11, pp.294–303
303
Copyright © 2022 FDOKUMEN