
High prevalence at computed coronary tomography of non-calcified plaques in asymptomatic HIV...
8
High prevalence at computed coronary tomography of non-calcified plaques in asymptomatic HIV patients treated with HAART: A meta- analysis Fabrizio D'Ascenzo a, i, *, 1 , Enrico Cerrato a, i , Andrea Calcagno d , Walter Grossomarra a , Flavia Ballocca a , Pierluigi Omed e a , Antonio Montefusco a , Simona Veglia b , Umberto Barbero a , Sebastiano Gili a , Margherita Cannillo a , Martina Pianelli a , Elisa Mistretta a , Alessio Raviola a , Davide Salera a , Domenica Garabello b , Massimo Mancone f , Vicente Estrada g , Javier Escaned g, i , Daniela De Marie h , Antonio Abbate c , Stefano Bonora d , Giuseppe Biondi Zoccai e, i , Claudio Moretti a, i , Fiorenzo Gaita a a Division of Cardiology, Department of Medical Sciences, University of Turin, Italy b Division of Radiology, Turin, Italy c VCU Pauley Heart Center, Richmond, VA, USA d Division of Infectious Disease, Amedeo di Savoia Hospital, Turin, Italy e Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italy f Policlinico Umberto I “Sapienza”, University of Rome, Italy g Hospital Clinicos San Carlos, Madrid, Spain h Division of Cardiology, Hospital Maria Vittoria, Italy i Cardiogroup.org Collaborative Group, Italy article info Article history: Received 23 October 2014 Received in revised form 13 February 2015 Accepted 7 March 2015 Available online 16 March 2015 Keywords: HIV Non calcific plaques HAART CCT abstract Introduction: Asymptomatic patients with human immunodeficiency virus (HIV) infection are at increased risk of vascular disease. Whether asymptomatic HIV patients have increased prevalence or structural differences in coronary artery plaques is not clear. Methods: Pubmed, Cochrane and Google Scholar were searched for articles evaluating asymptomatic HIV patients evaluated with coronary computed tomography. The prevalence of coronary stenosis (defined as >30% and >50%), of calcified coronary plaques (CCP) viewed as more ‘stable’ plaques, and of non-calcified coronary plaques (NCP) viewed as more ‘vulnerable’ plaques were the end points of interest. Results: 9 studies with 1229 HIV patients and 1029 controls were included. No significant differences were detected about baseline cardiovascular risk profile. The prevalence of significant coronary stenosis >30% or >50% did not differ between HIVþ and HIV- patients (42% [37e44] and 46% [35e52] with an Odds Ratio [OR] of 1.38 [0.86e2.20] for >30% stenosis) and (15% [9e21] and 14% [7e22] with an OR of 1.11 [0.81e1.52]), respectively. The prevalence of calcified coronary plaques (CCP) (31% [24e32] and 21% [14e30] with an OR of 1.17 [0.63e2.16]) also did not differ among HIVþ and HIV- patients. On the contrary rates of NCP were >3-fold higher in HIV-positive patients [58% (48e60) and 17% (14e27) with an OR of 3.26 (1e30-8.18)], with an inverse relationship with CD4 cell count at meta-regression (Beta 0.20 [-0.35-0.18], p 0.04). Conclusion: Asymptomatic HIV patients present a similar burden of coronary stenosis and calcified coronary artery plaques but significantly higher rates of non-calcific coronary plaques at computed to- mography. The association between HIV infection, reduced CD4 cell counts and higher prevalence on * Corresponding author. Division of Cardiology, Department of Internal Medicine, Turin, Italy. E-mail address: [email protected] (F. D'Ascenzo). 1 www.cardiogroup.org. Contents lists available at ScienceDirect Atherosclerosis journal homepage: www.elsevier.com/locate/atherosclerosis http://dx.doi.org/10.1016/j.atherosclerosis.2015.03.019 0021-9150/© 2015 Elsevier Ireland Ltd. All rights reserved. Atherosclerosis 240 (2015) 197e204
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of High prevalence at computed coronary tomography of non-calcified plaques in asymptomatic HIV...

High prevalence at computed coronary tomography of non-calcifiedplaques in asymptomatic HIV patients treated with HAART: A meta-analysis
Fabrizio D'Ascenzo a, i, *, 1, Enrico Cerrato a, i, Andrea Calcagno d, Walter Grossomarra a,Flavia Ballocca a, Pierluigi Omed!e a, Antonio Montefusco a, Simona Veglia b,Umberto Barbero a, Sebastiano Gili a, Margherita Cannillo a, Martina Pianelli a,Elisa Mistretta a, Alessio Raviola a, Davide Salera a, Domenica Garabello b,Massimo Mancone f, Vicente Estrada g, Javier Escaned g, i, Daniela De Marie h,Antonio Abbate c, Stefano Bonora d, Giuseppe Biondi Zoccai e, i, Claudio Moretti a, i,Fiorenzo Gaita a
a Division of Cardiology, Department of Medical Sciences, University of Turin, Italyb Division of Radiology, Turin, Italyc VCU Pauley Heart Center, Richmond, VA, USAd Division of Infectious Disease, Amedeo di Savoia Hospital, Turin, Italye Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italyf Policlinico Umberto I “Sapienza”, University of Rome, Italyg Hospital Clinicos San Carlos, Madrid, Spainh Division of Cardiology, Hospital Maria Vittoria, Italyi Cardiogroup.org Collaborative Group, Italy
a r t i c l e i n f o
Article history:Received 23 October 2014Received in revised form13 February 2015Accepted 7 March 2015Available online 16 March 2015
Keywords:HIVNon calcific plaquesHAARTCCT
a b s t r a c t
Introduction: Asymptomatic patients with human immunodeficiency virus (HIV) infection are atincreased risk of vascular disease. Whether asymptomatic HIV patients have increased prevalence orstructural differences in coronary artery plaques is not clear.Methods: Pubmed, Cochrane and Google Scholar were searched for articles evaluating asymptomatic HIVpatients evaluated with coronary computed tomography. The prevalence of coronary stenosis (defined as>30% and >50%), of calcified coronary plaques (CCP) viewed as more ‘stable’ plaques, and of non-calcifiedcoronary plaques (NCP) viewed as more ‘vulnerable’ plaques were the end points of interest.Results: 9 studies with 1229 HIV patients and 1029 controls were included. No significant differenceswere detected about baseline cardiovascular risk profile. The prevalence of significant coronary stenosis>30% or >50% did not differ between HIVþ and HIV- patients (42% [37e44] and 46% [35e52] with anOdds Ratio [OR] of 1.38 [0.86e2.20] for >30% stenosis) and (15% [9e21] and 14% [7e22] with an OR of1.11 [0.81e1.52]), respectively. The prevalence of calcified coronary plaques (CCP) (31% [24e32] and 21%[14e30] with an OR of 1.17 [0.63e2.16]) also did not differ among HIVþ and HIV- patients. On thecontrary rates of NCP were >3-fold higher in HIV-positive patients [58% (48e60) and 17% (14e27) withan OR of 3.26 (1e30-8.18)], with an inverse relationship with CD4 cell count at meta-regression(Beta "0.20 [-0.35-0.18], p 0.04).Conclusion: Asymptomatic HIV patients present a similar burden of coronary stenosis and calcifiedcoronary artery plaques but significantly higher rates of non-calcific coronary plaques at computed to-mography. The association between HIV infection, reduced CD4 cell counts and higher prevalence on
* Corresponding author. Division of Cardiology, Department of Internal Medicine,Turin, Italy.
E-mail address: [email protected] (F. D'Ascenzo).1 www.cardiogroup.org.
Contents lists available at ScienceDirect
Atherosclerosis
journal homepage: www.elsevier .com/locate/atherosclerosis
http://dx.doi.org/10.1016/j.atherosclerosis.2015.03.0190021-9150/© 2015 Elsevier Ireland Ltd. All rights reserved.
Atherosclerosis 240 (2015) 197e204

non-calcific coronary artery plaques may shed light into the pathogenesis in HIV-associated coronaryartery disease, stressing the importance of primary prevention in this population.
© 2015 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Life expectancy of human immunodeficiency virus (HIV) pa-tients dramatically increased thanks to highly active antiretroviraltherapy (HAART) [1]. Physicians managing these patients areshifting towards a more global assessment of clinical conditions,with a particular attention of development of both clinical andsubclinical cardiovascular disease [2,3].
HIV patients, actually, are exposed for many years to thecontinuous interaction between traditional risk factors, coronaryHIV infection, immune-mediated response and the still debatedeffect of HAART [3,4].
In acute coronary syndrome (ACS) settings, this peculiar path-ological pattern has led to a higher risk of coronary adverse events;several challenges have been identified in those patients, such asdrug to drug interaction with new antiaggregants or statins andcompliance to medications [4e6].
Consequently, primary care is becoming crucial, both to preventsubclinical impairment of systolic and diastolic dysfunction [5] andto reduce number of cardiovascular adverse events [3]. Even sub-clinical atherosclerosis has been related with risk for cardiovascularevents in the general population [7,8], and particular for thosepresenting with non-calcified plaques due to a higher risk ofrupture [9]. An increased use of coronary computed tomography(CCT) has been reported, both to measure coronary artery calcium(CAC) and to evaluate the prevalence and features of coronaryplaques, in order to accurately address pharmacological and inter-ventional strategies [10e12].
Some studies have found a higher prevalence of subclinicalatherosclerosis in HIV-positive patients [13e15] but the results arenot consistent. Consequently we performed a systematic review tounderstand the prevalence and the peculiarities of coronary pla-ques in asymptomatic HIV-positive patients.
2. Methods
The Cochrane Collaboration and Meta-analysis Of ObservationalStudies in Epidemiology (MOOSE) [18] was followed during elab-oration of the present analysis.
2.1. Search strategy and study selection
Pertinent articles were searched in Medline, Cochrane Library,Biomed Central and Google Scholar in keeping with establishedmethods [16] with Mesh strategy: ((coronary computed tomogra-phy) OR (CCT)) AND (hiv OR aids OR (human AND immunodefi-ciency AND virus)).
Two independent reviewers (F.DA, E.C.) first screened retrievedcitations at the title and/or abstract level, with divergences resolvedafter consensus. If potentially pertinent, they were then appraisedas complete reports according to the following explicit selectioncriteria. Studies were included if (i) investigating with CCTasymptomatic HIV and non HIV patients (ii) with more than 90% ofpatients treated with HAART. Exclusion criteria was (i) absence ofnon HIV controls.
2.2. Data extraction
Two unblinded independent reviewers (G.B.-Z, F.DA, and E.C.)abstracted the following data on pre-specified forms: authors,journal, year of publication, location of the study group, baselinefeatures, type and timing of antiretroviral therapy, and protocols ofCCT. The prevalence of coronary stenosis (more than 30% and morethan 50%), of calcified coronary (CCP), of non-calcified coronaryplaques (NCP) and of Coronary Artery Calcification Score (CAC)more than 0 were the end points of interest.
2.3. Internal validity and quality appraisal
Unblinded independent reviewers (G.B.-Z, F.DA, and E.C.) eval-uated quality of included studies on pre-specified forms. Modifyingthe MOOSE items to take into account the specific features ofincluded studies [15e18], we separately abstracted and appraisedstudy design, setting, data source, as well as risk of analytical, se-lection, adjudication, detection, and attrition bias (expressed aslow, moderate, or high risk of bias, as well as incomplete reportingleading to inability to ascertain the underlying risk of bias). For thequality assessment of the selected studies we used the Newcastle-Ottawa Scale (NOS) for Assessing the Quality of NonrandomizedStudies in Meta-Analysis [19].
2.4. Data analysis and synthesis
Continuous variables are reported as mean (standard deviation)or median (range). Categorical variables are expressed as n/N (%).Statistical pooling was performed according to a random-effectmodel with generic inverse-variance weighting, computing riskestimates with 95% confidence intervals, using RevMan 5 (TheCochrane Collaboration, The Nordic Cochrane Centre, and Copen-hagen, Denmark). Meta-regression analysis for the impact oftraditional risk factors and HIV features on the primary end pointwas performed with random effect with Comprehensive Meta-Analysis after computation of the event rate. All confidence in-tervals were of 95%). Standard hypothesis testing was set at thetwo-tailed 0.05 level.
3. Results
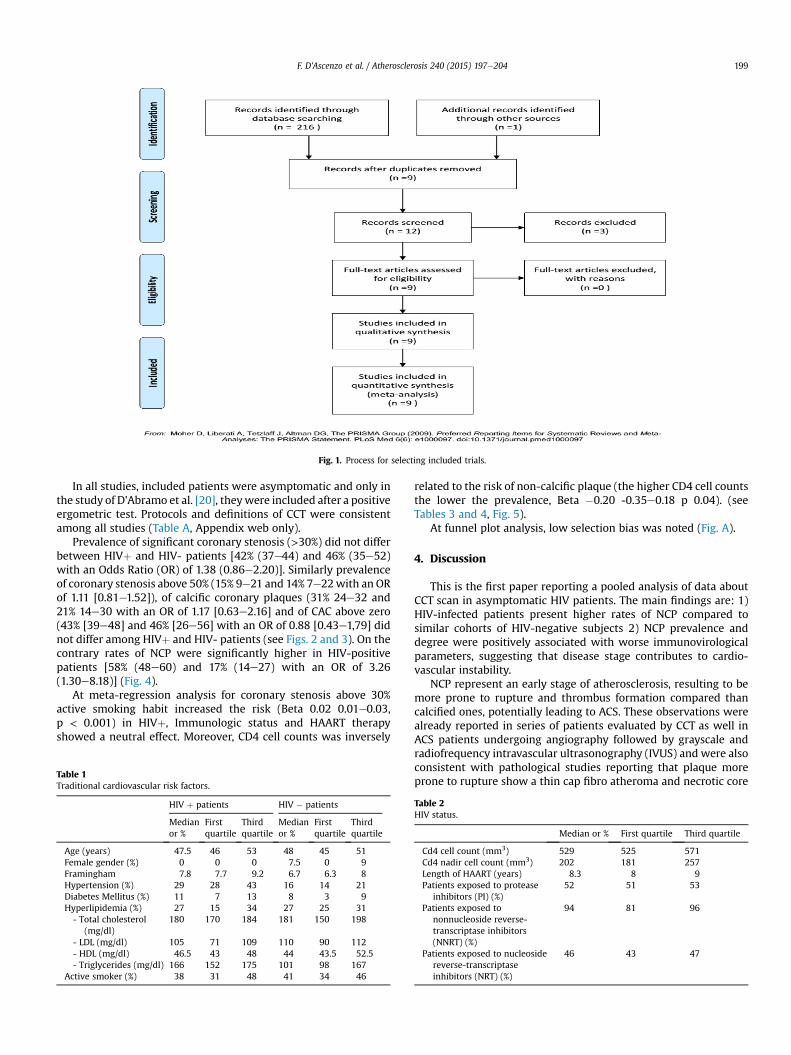
217 studies were first screened at abstract level, and afterevaluation 9 studies with 1229 HIV patients and 1029 controls wereincluded [20e28]. (see Fig. 1). Eight studies out of nine were pro-spective: eight were performed in the USA and one in Europe.
Baseline features of the included patients are reported in Table 1.HIV patients were more frequently of male gender, with higherrates of diabetes mellitus and of hypertension in the includedstudies, but without significant differences.
Concerning immunovirological variables these patients hadbeen on HAART for 8.3 (8e9) years, with a CD4þ T lymphocyte cellcount of 529/mm3 (525e571) and a CD4þ nadir of 201 cells/mm3(181e257). 52% (51e53) have been exposed to Protease Inhibitors(PI), 94% (81e96) to nonnucleoside reverse-transcriptase inhibitors(NNRT) and 46% (43e47) to nucleoside reverse-transcriptase in-hibitors (NRTIs) (Table 2).
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204198
In all studies, included patients were asymptomatic and only inthe study of D'Abramo et al. [20], theywere included after a positiveergometric test. Protocols and definitions of CCT were consistentamong all studies (Table A, Appendix web only).
Prevalence of significant coronary stenosis (>30%) did not differbetween HIVþ and HIV- patients [42% (37e44) and 46% (35e52)with an Odds Ratio (OR) of 1.38 (0.86e2.20)]. Similarly prevalenceof coronary stenosis above 50% (15% 9e21 and 14% 7e22with an ORof 1.11 [0.81e1.52]), of calcific coronary plaques (31% 24e32 and21% 14e30 with an OR of 1.17 [0.63e2.16] and of CAC above zero(43% [39e48] and 46% [26e56] with an OR of 0.88 [0.43e1,79] didnot differ among HIVþ and HIV- patients (see Figs. 2 and 3). On thecontrary rates of NCP were significantly higher in HIV-positivepatients [58% (48e60) and 17% (14e27) with an OR of 3.26(1.30e8.18)] (Fig. 4).
At meta-regression analysis for coronary stenosis above 30%active smoking habit increased the risk (Beta 0.02 0.01e0.03,p < 0.001) in HIVþ, Immunologic status and HAART therapyshowed a neutral effect. Moreover, CD4 cell counts was inversely
related to the risk of non-calcific plaque (the higher CD4 cell countsthe lower the prevalence, Beta "0.20 -0.35e0.18 p 0.04). (seeTables 3 and 4, Fig. 5).
At funnel plot analysis, low selection bias was noted (Fig. A).
4. Discussion
This is the first paper reporting a pooled analysis of data aboutCCT scan in asymptomatic HIV patients. The main findings are: 1)HIV-infected patients present higher rates of NCP compared tosimilar cohorts of HIV-negative subjects 2) NCP prevalence anddegree were positively associated with worse immunovirologicalparameters, suggesting that disease stage contributes to cardio-vascular instability.
NCP represent an early stage of atherosclerosis, resulting to bemore prone to rupture and thrombus formation compared thancalcified ones, potentially leading to ACS. These observations werealready reported in series of patients evaluated by CCT as well inACS patients undergoing angiography followed by grayscale andradiofrequency intravascular ultrasonography (IVUS) and were alsoconsistent with pathological studies reporting that plaque moreprone to rupture show a thin cap fibro atheroma and necrotic core
Fig. 1. Process for selecting included trials.
Table 1Traditional cardiovascular risk factors.
HIV þ patients HIV " patients
Medianor %
Firstquartile
Thirdquartile
Medianor %
Firstquartile
Thirdquartile
Age (years) 47.5 46 53 48 45 51Female gender (%) 0 0 0 7.5 0 9Framingham 7.8 7.7 9.2 6.7 6.3 8Hypertension (%) 29 28 43 16 14 21Diabetes Mellitus (%) 11 7 13 8 3 9Hyperlipidemia (%) 27 15 34 27 25 31- Total cholesterol
(mg/dl)180 170 184 181 150 198
- LDL (mg/dl) 105 71 109 110 90 112- HDL (mg/dl) 46.5 43 48 44 43.5 52.5- Triglycerides (mg/dl) 166 152 175 101 98 167
Active smoker (%) 38 31 48 41 34 46
Table 2HIV status.
Median or % First quartile Third quartile
Cd4 cell count (mm3) 529 525 571Cd4 nadir cell count (mm3) 202 181 257Length of HAART (years) 8.3 8 9Patients exposed to protease
inhibitors (PI) (%)52 51 53
Patients exposed tononnucleoside reverse-transcriptase inhibitors(NNRT) (%)
94 81 96
Patients exposed to nucleosidereverse-transcriptaseinhibitors (NRT) (%)
46 43 47
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204 199

with an overlying thin fibrous cap [32,33].Previous CCT studies reported a higher prevalence of NCP in
intermediate-risk asymptomatic patients, especially in those withsignificantly higher level of C-reactive protein, cholesterol (totaland low-density lipoprotein) as well as a trend for a higher prev-alence of diabetes mellitus [34]. Our analysis includes a youngpopulation (median age of 47 years) with a low prevalence ofdiabetes and a moderate prevalence of hyperlipidemia (11% and27% respectively). Despite these characteristics, the prevalence ofNCP was 3-fold higher compared with similar Framingham-basedscore non-HIV population (58% vs. 17%) and comparable to theone reported in recent study [35] by Park et al. (NCP rate ¼ 56%).
We reported a CAC score value higher than zero in less than halfof subjects. Even if CAC score of zero was associated with very lowrisk of cardiac events, NCP plaque cannot be detected on non-
contrast cardiac scans, used to measure CAC levels. Previousstudies utilizing CCT to estimate the extent of coronary artery dis-ease in HIV patients assessed only CAC by scoring without exploredirectly the lumen caliber or plaques burden [36,37]. Although theCAC scoring is a well defined marker for atherosclerotic lesions andcardiac event risk in non-HIV population, it may not provide areliable valuation of early atherosclerosis in young HIV patients inwhom calcifications are absent: our finding demonstrate that asignificant proportion of patientswith coronaryatherosclerosismaybe missed using only calcium score criterion. Thus we stressed theadditional value of adopting CCT over CAC scoring alone for theassessment of coronary tree in young HIV-positive patients; sinceCCP probably reflects advanced stable atherosclerosis while iden-tifying NCP seem crucial in this group of patients.
Additionally we reported a significant correlation between low
Fig. 2. Incidence of CCT findings in HIV and control patients.
Fig. 3. Risk of coronary stenosis more than 30% (above) and 50% (below).
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204200

CD4 cell counts and risk of NCP. The association between CD4 cellcount and cardiovascular disease has already been previously re-ported and it may be related to immune-dysfunction (immuneactivation and immune senescence) or to the prevalence of otherinfection potentially affecting endothelial cells (cytomegalovirus,HHV-8, and others) [38e40]. Similarly, previous studies reported alow CD4þ count to be associated with a high prevalence of carotidartery plaques [41]: our findings strengthen these observationssupporting the hypothesis of a systemic inflammatory dysregula-tion in HIV-positive patients.
The only other variable that showed a positive interaction on therisk of coronary stenosis was active smoking status, accordingly tothe higher risk of smoker-related comorbidities previously re-ported in HIV-infected than uninfected patient. Notably, thesesubgroup are actually an attractive target for a “multi-disease”screening since that recent studies are currently investigating the
Fig. 4. Risk of non calcified, of calcified and of CAC more than 0 (from above to below).
Table 3Meta-regression analysis on traditional cardiovascular risk factors and HIV status on finding of coronary stenosis (more than 30%).
HIV þ patients HIV " patients
Beta LCI UCI p Beta LCI UCI P
Age 0.02 "0.06 0.11 0.57 "0.15 "0.31 "0.02 <0.001Female gender "0.008 "0.03 0.02 0.55 0.011 "0.01 0.25 0.34Framingham "0.03 "0.14 0.08 0.64 "0.17 "0.49 0.14 0.45Hypertension "0.0007 "0.03 0.02 0.94 "0.02 "0.06 0.005 0.47Diabetes Mellitus "0.01 "0.06 0.02 0.24 "0.14 "0.21 0.15 0.45Hyperlipidemia "0.01 "0.04 0.02 0.41 "0.01 "0.03 0.01 0.33Total cholesterol (mg/dl) 0.25 "0.01 0.35 0.56 0.02 "0.03 0.07 0.39LDL (mg/dl) 0.001 "0.03 0.04 0.99 "0.01 "0.15 0.12 0.89HDL (mg/dl) 0.05 "0.26 0.15 0.19 0.11 "0.06 0.34 0.21Triglycerides "0.002 "0.01 0.008 0.68 0.01 "0.01 0.04 0.49Active smoker 0.02 0.01 0.03 <0.001 0.06 "0.21 0.09 0.56Cd4 cell count (logit) 0.02 "0.01 0.06 0.97Cd4 nadir cell count (logit) "0.001 "0.005 0.007 0.83Length of HAART (years, logit) 0.19 "0.21 0.24 0.19PPI 0.003 "0.21 0.45 0.45NNRT "0.02 "0.024 0.61 0.67NRT 0.001 "0.005 0.008 0.58
Table 4Meta-regression analysis on traditional cardiovascular risk factors and HIV status onfinding of non-calcific coronary plaque.
HIV þ patients
Beta LCI UCI p
Age 0.09 "0.09 0.14 0.67Female gender "0.008 "0.03 0.02 0.11Framingham "0.03 "0.14 0.08 0.98Hypertension "0.0007 "0.03 0.02 0.78Diabetes Mellitus "0.01 "0.06 0.02 0.25Hyperlipidemia "0.01 "0.04 0.02 0.67Active smoker 0.04 "0.01 0.09 0.07Cd4 cell count (logit) "0.02 "0.09 0.01 0.04Cd4 nadir cell count (logit) "0.002 "0.11 0.21 0.45Length of HAART (years, logit) 0.19 "0.21 0.24 0.34PPI 0.003 "0.21 0.45 0.76NNRT 0.05 "0.41 0.78 0.15NRT 0.005 "0.05 0.01 0.58
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204 201

role of CT for lung cancer prevention in HIV-positive smokers evenif with sparse results [42e44].
Clinical implications of present study may be of interest forphysicians, cardiologists, infective disease specialists and generalpractitioners. Plaque characteristics observed using CCT underlinethe vulnerable atherosclerotic pattern of HIV-positive subjects,suggesting the need of aggressive primary prevention programs inthis specific population. These data highlight the importance ofaddressing modifiable cardiovascular risk factors to optimize long-term health in the setting of HIV infection comorbidities. Althoughnot confirmed in randomized controlled trial, statins use may becrucial, for their effect on plaques stability. A parallel focus onsmoking cessation is important, considering the interaction on therisk of coronary stenosis demonstrated from several studies.Furthermore several data report the underuse of aspirin in primaryprevention [45] in high-risk HIV-positive patients despite height-ened awareness regarding elevated cardiovascular risk, althoughthe absence of randomized controlled trials may explain suchconduct.
Finally even if a CCT based approach for primary prevention hasnever been suggested to improve prognosis, these results mayadvise HIV physicians to evaluate and to focus on plaque charac-teristics in order to select appropriate primary prevention strategies
4.1. Limitations
Our study shares several limitations. Unfortunately it was notpossible to reportabout long-termfollow-uporhardclinical events in
this population.Moreoverwedonot have detailed data aboutHAARTregimen and almost all patients are male making it impossible toappraise specific differences. Third, we reported incidence of coro-nary stenosismore than 30% considering our aim to focus onplaques’features independentlyof thedegreeof stenosis. Finally, the potentialbenefit by CCT needs to be weighted against its safety related to ra-diation exposure in asymptomatic young patients. Moreover asdemonstrated in Table B, most of the included studies were of highquality, with an accurate definition of control population.
5. Conclusion
In this comprehensive meta-analysis, NCP was more prevalentand extensive in asymptomatic HIV-infected patients, especially inpresence of lower CD4 cell counts. This finding provides new detailson the differences in atherosclerotic process in HIV-infected pa-tients, stressing the importance of primary prevention in thispopulation. On the other hand the use of CCT may be considered inthe future, if supported by larger prospective studies, as a com-plementary tool to evaluate high risk patients, both for traditionalcardiovascular risk factors as well for severity of HIV infection.
Appendix
Fig. 5. Meta regression analysis for HIV þ patients (smoking habits), and HIV- (age) on coronary stenosis more than 30% and on non calcific plaque (Cd4þ).
Table ACCT's protocols.
Slice Analysis Non-calcified plaque
Post, 14 64 slice in 3 centers320-row in 1 center
modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
D'Abramo, 13 64 slice modified 15-segment model of theAmerican Heart Association
e
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204202

Table A (continued )
Slice Analysis Non-calcified plaque
Hwang, 13 64 slice in modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
Zanni, 13 64 slice modified 15-segment model of theAmerican Heart Association
mean minimal attenuation less than 40 Hounsfield Units
Duarte, 12 64 slice modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
Pereyra, 12 e e e
Burdo, 11 64 slice modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
Fitch, 10 64 slice modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
Lo, 10 64 slice modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
Robinson, 10 64 slice modified 15-segment model of theAmerican Heart Association
any discernible structure that could be clearly assignable to thevessel wall, with a CT density less than the contrast enhancedcoronary lumen but greater than the surrounding connective tissue,and identified in at least 2 independent planes.
Table BOttawa scale for included studies.
Selection:e Adequate case definition: 9/10e Representativeness of the cases: 9/10e Selection of controls: 9/10 community Controls; 1/10 hospital controlse Definition of controls: 9/10 no History of disease
Comparability:e Study controls for cardiovascular risk factors: 9/10e Study controls for cardiologist indications: 1/10
Exposure:e Ascertainment: 10/10 secure (cct protocols)e Same methods ascertainment: 10/10
Fig. A. Funnel plot.
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204 203

References
[1] M.J. Burgess, M.J. Kasten, Human immunodeficiency virus: what primary careclinicians need to know, Mayo Clin. Proc. 88 (12) (2013 Dec) 1468e1474.
[2] K.C. Dabhadkar, Bellam N Polypill strategy for primary prevention of cardio-vascular disorders, Drugs Today (Barc) 49 (5) (2013 May) 317e324.
[3] G.A. Burkholder, A.R. Tamhane, J.L. Salinas, M.J. Mugavero, J.L. Raper,A.O. Westfall, et al., Underutilization of aspirin for primary prevention ofcardiovascular disease among HIV-infected patients, Clin. Infect. Dis. 55 (11)(2012 Dec) 1550e1557.
[4] E. Cerrato, F. D'Ascenzo, G. Biondi-Zoccai, A. Calcagno, S. Frea, W. GrossoMarra, et al., Cardiac dysfunction in pauci symptomatic human immunodefi-ciency virus patients: a meta-analysis in the highly active antiretroviraltherapy era, Eur. Heart J. 34 (19) (2013 May) 1432e1436.
[5] F. D'Ascenzo, E. Cerrato, D. Appleton, C. Moretti, A. Calcagno, N. Abouzaki,G. Vetrovec, T. Lhermusier, D. Carrie, B. Das Neves, J. Escaned, S. Cassese,A. Kastrati, A. Chinaglia, R. Belli, D. Capodanno, C. Tamburino, F. Santilli,G. Parodi, A. Vachiat, P. Manga, L. Vignali, M. Mancone, G. Sardella, F. Fedele,J.J. DiNicolantonio, P. Omed!e, S. Bonora, F. Gaita, A. Abbate, G.B. Zoccai,Percutaneous coronary intervention and surgical revascularization in HIVDatabase (PHD) Study investigators Prognostic indicators for recurrentthrombotic events in HIV-infected patients with acute coronary syndromes:use of registry data from 12 sites in Europe, South Africa and the UnitedStates, Thromb. Res. 134 (3) (2014 Sep) 558e564, http://dx.doi.org/10.1016/j.thromres.2014.05.037. Epub 2014 Jun 2.
[6] F. D'Ascenzo, E. Cerrato, G. Biondi-Zoccai, C. Moretti, P. Omed!e, F. Sciuto, et al.,Acute coronary syndromes in human immunodeficiency virus patients: ameta-analysis investigating adverse event rates and the role of antiretroviraltherapy, Eur. Heart J. 33 (7) (2012 Apr) 875e880.
[7] R. Detrano, A.D. Guerci, J.J. Carr, D.E. Bild, G. Burke, A.R. Folsom, et al., Coronarycalcium as a predictor of coronary events in four racial or ethnic groups,N. Engl. J. Med. 358 (2008) 1336e1345.
[8] F. D'Ascenzo, P. Agostoni, A. Abbate, D. Castagno, M.J. Lipinski, G.W. Vetrovec,et al., Atherosclerotic coronary plaque regression and the risk of adversecardiovascular events: a meta-regression of randomized clinical trials,Atherosclerosis 226 (1) (2013 Jan) 178e185.
[9] G.W. Stone, A. Maehara, A.J. Lansky, B. de Bruyne, E. Cristea, G.S. Mintz, et al.,PROSPECT Investigators. A prospective natural-history study of coronaryatherosclerosis, N. Engl. J. Med. 364 (3) (2011 Jan 20) 226e235.
[10] A.H. Ellims, G. Wong, J.M. Weir, P. Lew, P.J. Meikle, A.J. Taylor, Plasma lip-idomic analysis predicts non-calcified coronary artery plaque in asymptom-atic patients at intermediate risk of coronary artery disease, Eur. Heart J.Cardiovasc Imaging 15 (8) (2014) 908e916.
[11] F. D'Ascenzo, E. Cerrato, G. Biondi-Zoccai, P. Omed!e, F. Sciuto, D.G. Presutti, etal., Coronary computed tomographic angiography for detection of coronaryartery disease in patients presenting to the emergency department with chestpain: a meta-analysis of randomized clinical trials, Eur. Heart J. CardiovascImaging 14 (8) (2013 Aug) 782e789.
[12] V. Kamperidis, M.A. de Graaf, A. Broersen, W. Ahmed, G. Sianos, V. Delgado, etal., Prognostic value of aortic and mitral valve calcium detected by contrastcardiac computed tomography angiography in patients with suspicion ofcoronary artery disease, Am. J. Cardiol. 113 (5) (2014 Mar 1) 772e778.
[13] P.Y. Hsue, J.C. Lo, A. Franklin, A.F. Bolger, J.N. Martin, S.G. Deeks, D.D. Waters,Progression of atherosclerosis as assessed by carotid intima-media thicknessin patients with HIV infection, Circulation 109 (2004) 1603e1608.
[14] J.S. Currier, M.A. Kendall, W.K. Henry, B. Alston-Smith, F.J. Torriani, P. Tebas,Y. Li, et al., Progression of carotid artery intima-media thickening in HIV-infected and uninfected adults, AIDS 21 (2007) 1137e1145.
[15] C. Grunfeld, J.A. Delaney, C. Wanke, J.S. Currier, R. Scherzer, M.L. Biggs, et al.,Preclinical atherosclerosis due to HIV infection: carotid intima-medial thick-ness measurements from the FRAM study, AIDS 23 (2009) 1841e1849.
[16] D. Moher, A. Liberati, J. Tetzlaff, D.G. Altman, PRISMA Group. Preferredreporting items for systematic reviews and meta-analyses: the PRISMAstatement, BMJ 339 (2009 Jul 21) b2535, http://dx.doi.org/10.1136/bmj.b2535.
[17] D. Moher, D.J. Cook, S. Eastwood, I. Olkin, D. Rennie, D.F. Stroup, Improving thequality of reports of meta-analyses of randomised controlled trials: theQUOROM statement. Quality of reporting of Meta-analyses, Lancet 354 (9193)(1999 Nov 27) 1896e1900.
[18] D.F. Stroup, J.A. Berlin, S.C. Morton, I. Olkin, G.D. Williamson, D. Rennie, et al.,Meta-analysis of observational studies in epidemiology: a proposal forreporting. Meta-analysis of observational Studies in epidemiology (MOOSE)group, JAMA 283 (15) (2000 Apr 19) 2008e2012.
[19] http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.[20] W.S. Post, M. Budoff, L. Kingsley, F.J. Palella Jr., M.D. Witt, X. Li, et al., Asso-
ciations between HIV infection and subclinical coronary atherosclerosis, Ann.Intern Med. 160 (7) (2014 Apr 1) 458e467, http://dx.doi.org/10.7326/M13-1754.
[21] A. D'Abramo, C. D'Agostino, A. Oliva, M. Iannetta, G. D'Ettorre, F. Vullo, et al.,
Early atherosclerosis in HIV infected subjects on suppressive antiretroviraltreatment: role of osteoprotegerin, ISRN AIDS 5 (2013 Dec) 737083.
[22] M.V. Zanni, S. Abbara, J. Lo, B. Wai, D. Hark, E. Marmarelis, S.K. Grinspoon,Increased coronary atherosclerotic plaque vulnerability by coronarycomputed tomography angiography in HIV-infected men, AIDS 27 (8) (2013May 15) 1263e1272. AIDS. 2012 Nov 28;26(18):2409-12.
[23] F. Pereyra, J. Lo, V.A. Triant, J. Wei, M.J. Buzon, K.V. Fitch, et al., Increasedcoronary atherosclerosis and immune activation in HIV-1 elite controllers,AIDS 26 (18) (2012 Nov 28) 2409e2412.
[24] J.J. Hwang, J. Wei, S. Abbara, S.K. Grinspoon, J. Lo, Receptor activator of nuclearfactor-kB ligand (RANKL) and its relationship to coronary atherosclerosis inHIV patients, J. Acquir Immune Defic. Syndr. 61 (3) (2012 Nov 1) 359e363.
[25] H. Duarte, J.R. Matta, N. Muldoon, H. Masur, C. Hadigan, A.M. Gharib, Non-calcified coronary plaque volume inversely related to CD4(þ) T-cell count inHIV infection, Antivir. Ther. 17 (4) (2012) 763e767.
[26] T.H. Burdo, J. Lo, S. Abbara, J. Wei, M.E. DeLelys, F. Preffer, et al., Soluble CD163,a novel marker of activated macrophages, is elevated and associated withnoncalcified coronary plaque in HIV-infected patients, J. Infect. Dis. 204 (8)(2011 Oct 15) 1227e1236.
[27] K.V. Fitch, J. Lo, S. Abbara, B. Ghoshhajra, L. Shturman, A. Soni, et al., Increasedcoronary artery calcium score and noncalcified plaque among HIV-infectedmen: relationship to metabolic syndrome and cardiac risk parameters,J. Acquir Immune Defic. Syndr. 55 (4) (2010 Dec) 495e499.
[28] J. Lo, S. Abbara, L. Shturman, A. Soni, J. Wei, J.A. Rocha-Filho, K. Nasir, et al.,Increased prevalence of subclinical coronary atherosclerosis detected bycoronary computed tomography angiography in HIV-infected men, AIDS 24(2) (2010 Jan 16) 243e253.
[32] G.W. Stone, A. Maehara, A.J. Lansky, B. de Bruyne, E. Cristea, G.S. Mintz, et al.,A prospective natural-history study of coronary atherosclerosis, N. Engl. J.Med. 364 (3) (2011 Jan 20) 226e235.
[33] R. Virmani, A.P. Burke, A. Farb, F.D. Kolodgie, Pathology of the vulnerableplaque, J. Am. Coll. Cardiol. 47 (2006) C13eC18.
[34] J. Hausleiter, T. Meyer, M. Hadamitzky, A. Kastrati, S. Martinoff, A. Sch€omig,Prevalence of noncalcified coronary plaques by 64-slice computed tomogra-phy in patients with an intermediate risk for significant coronary artery dis-ease, J. Am. Coll. Cardiol. 48 (2) (2006 Jul 18) 312e318.
[35] G.M. Park, S.W. Lee, Y.R. Cho, C.J. Kim, J.S. Cho, M.W. Park, S.H. Her, J.M. Ahn,J.Y. Lee, D.W. Park, S.J. Kang, Y.H. Kim, C.W. Lee, E.H. Koh, W.J. Lee, M.S. Kim,K.U. Lee, J.W. Kang, T.H. Lim, S.W. Park, S.J. Park, J.Y. Park, Coronary computedtomographic angiographic findings in asymptomatic patients with type 2diabetes mellitus, Am. J. Cardiol. 113 (5) (2014 Mar 1) 765e771.
[36] Q. Meng, J.A. Lima, H. Lai, D. Vlahov, D.D. Celentano, S.A. Strathdee,K.E. Nelson, K.C. Wu, S. Chen, W. Tong, S. Lai, Coronary artery calcification,atherogenic lipid changes, and increased erythrocyte volume in black injec-tion drug users infected with human immunodeficiency virus-1 treated withprotease inhibitors, Am. Heart J. 144 (4) (2002 Oct) 642e648.
[37] R. Talwani, O.M. Falusi, C.F. Mendes de Leon, J.L. Nerad, S. Rich, L.A. Proia,B.E. Sha, K.Y. Smith, H.A. Kessler, Electron beam computed tomography forassessment of coronary artery disease in HIV-infected men receiving antire-troviral therapy, J. Acquir Immune Defic. Syndr. 30 (2) (2002 Jun 1) 191e195.
[38] K. Sacre, P.W. Hunt, P.Y. Hsue, E. Maidji, J.N. Martin, S.G. Deeks, et al., A role forcytomegalovirus-specific CD4þCX3CR1þ T cells and cytomegalovirus-induced T-cell immunopathology in HIV-associated atherosclerosis, AIDS 26(7) (2012 Apr 24) 805e814.
[39] A.K. Steele, E.J. Lee, J.A. Manuzak, S.M. Dillon, J.D. Beckham, et al., Microbialexposure alters HIV-1-induced mucosal CD4þ T cell death pathways Ex vivo,Retrovirology 11 (2014 Feb 4) 14.
[40] M.V. Zanni, T. Kelesidis, M.L. Fitzgerald, J. Lo, S. Abbara, B. Wai, et al., HDLredox activity is increased in HIV-infected men in association with macro-phage activation and noncalcified coronary atherosclerotic plaque, Antivir.Ther. 19 (8) (2014 Feb 17) 805e811.
[41] R.C. Kaplan, L.A. Kingsley, S.J. Gange, L. Benning, L.P. Jacobson, Lazar J,AnastosK, Tien PC, Sharrett AR, Hodis HN. Low CD4þ T-cell count as a majoratherosclerosis risk factor in HIV-infected women and men, AIDS 22 (13)(2008 Aug 20) 1615e1624.
[42] M. Calvo-S#anchez, R. Perell#o, I. P#erez, et al., Differences between HIV-infectedand uninfected adults in the contributions of smoking, diabetes and hyper-tension to acute coronary syndrome: two parallel case-control studies, Hiv.Med. 14 (2013) 40e48.
[43] A. Hulbert, C.M. Hooker, J.C. Keruly, T. Brown, K. Horton, E. Fishman, et al.,Prospective CT screening for lung Cancer in a high-risk Population: HIV-positive smokers, J. Thorac. Oncol. 9 (6) (2014 Jun) 752e759.
[44] Detrano R1, A.D. Guerci, J.J. Carr, D.E. Bild, G. Burke, A.R. Folsom, et al., Cor-onary calcium as a predictor of coronary events in four racial or ethnic groups,N. Engl. J. Med. 358 (2008) 1336e1345.
[45] G.A. Burkholder, A.R. Tamhane, J.L. Salinas, M.J. Mugavero, J.L. Raper,A.O. Westfall, et al., Underutilization of aspirin for primary prevention ofcardiovascular disease among HIV-infected patients, Clin. Infect. Dis. 55 (11)(2012 Dec) 1550e1557.
F. D'Ascenzo et al. / Atherosclerosis 240 (2015) 197e204204




















