
High folate intake is associated with lower breast cancer incidence in postmenopausal women in the...
10
See corresponding editorial on page 271. High folate intake is associated with lower breast cancer incidence in postmenopausal women in the Malmö Diet and Cancer cohort 1–3 Ulrika Ericson, Emily Sonestedt, Bo Gullberg, Håkan Olsson, and Elisabet Wirfa ¨lt ABSTRACT Background: Epidemiologic studies of associations between folate intake and breast cancer are inconclusive, but folate and other plant food nutrients appear protective in women at elevated risk. Objective: The objective was to examine the association between folate intake and the incidence of postmenopausal breast cancer. Design: This prospective study included all women aged 50 y (n 11699) from the Malmö Diet and Cancer cohort. The mean follow-up time was 9.5 y. We used a modified diet-history method to collect nutrient intake data. At the end of follow-up, 392 incident invasive breast cancer cases were verified. We used proportional hazard regression to calculate hazard ratios (HRs). Results: Compared with the lowest quintile, the incidence of inva- sive breast cancer was reduced in the highest quintile of dietary folate intake (HR: 0.56; 95% CI: 0.35, 0.90; P for trend 0.02); total folate intake, including supplements (HR: 0.56; 95% CI: 0.34, 0.91; P for trend 0.006); and dietary folate equivalents (HR: 0.59; 95% CI: 0.36, 0.97; P for trend 0.01). Conclusion: A high folate intake was associated with a lower inci- dence of postmenopausal breast cancer in this cohort. Am J Clin Nutr 2007;86:434 – 43. KEY WORDS Folate, breast cancer, obesity, body mass index, postmenopausal women, prospective study, diet INTRODUCTION Folate can be found in high concentrations in dark-green leafy vegetables, legumes, fruit, and liver (1). Folate is a coenzyme that carries one-carbon units and is thereby of great importance in the metabolism of amino acids and nucleotides (2). Two main mech- anisms link folate deficiency to cancer development: a reduced synthesis of S-adenosyl methionine (SAM), which results in aberrations in DNA methylation, and a reduced synthesis of the pyrimidine thymidylate, which results in the misincorporation of uracil into DNA. A third possible mechanism is impaired purine synthesis and subsequent changes in DNA (3). Epidemiologic studies have indicated that high folate intake may protect against colorectal cancer (4, 5) but also against cancer at other sites (6 –10). Current epidemiologic evidence of a relation between high folate intake and reduced breast cancer risk is, however, not conclusive. High folate intake was shown to be associated with a decreased risk of postmenopausal breast cancer in some studies (11–14), whereas this association was not confirmed in other studies (15–18). Other B vitamins are involved in folate metabolism. Vitamin B-12 acts as a cofactor to the enzyme methionine synthase, and both vitamin B-6 and riboflavin serve as cofactors for folate- dependent enzymes (19, 20). A study in Shanghai showed that the association between a high folate intake and a decreased risk of breast cancer was stronger among women with high intakes of vitamin B-12 and vitamin B-6 (13). The modifying effect of vitamin B-12 is supported by other studies (11, 14). Some studies indicate that the negative association between folate intake and breast cancer mainly appears among women at highest risk, ie, high consumers of alcohol. The detrimental in- fluence of alcohol on folate bioavailability is probably the most important explanation for this observation (16 –18). Obesity, however, is a well-known risk factor for breast cancer develop- ment, as is a high alcohol consumption (21, 22). Similar to many other studies, a previous report from the Malmö Diet and Cancer (MDC) study showed positive associations between BMI and breast cancer (23). Higher concentrations of endogenous sex hormones have been suggested to partly explain the increased risk of breast cancer among high consumers of alcohol (24). However, an elevated concentration of sex hormones is also a possible mechanism by which obesity can increase breast cancer risk (25, 26). In the Swedish mammography cohort, overweight women with high dietary intakes of ascorbic acid had a lower incidence of breast cancer (27), but the risk relation was reversed in lean women. Ascorbic acid, an antioxidant that may protect against DNA damage (28), is mainly found in fruit and vegeta- bles, as is folate. The aim of this study was to investigate whether folate intake is associated with postmenopausal breast cancer in women from the MDC cohort. This article also evaluates whether other nutri- ents influence the association between folate intake and breast cancer incidence. Finally, we wanted to examine whether the potential association between folate and breast cancer development was different among women who already had a higher breast cancer risk because they were overweight. 1 From the Department of Clinical Sciences, Lund University, Malmö, Sweden (UE, ES, BG, and EW), and the Department of Clinical Sciences, Lund University, Lund, Sweden (HO). 2 Supported by grants from the Swedish Cancer Society, the Swedish Medical Research Council, the City of Malmö, The Albert Påhlsson Foun- dation, and the Swedish Research Council Formas. 3 Reprints not available. Address correspondence to U Ericson, Nutritional Epidemiology, Clinical Research Center, Building 60, floor 13, Malmö Uni- versity Hospital, entrance 72, SE-205 02 Malmö, Sweden. E-mail: [email protected]. Received December 7, 2006. Accepted for publication March 21, 2007. 434 Am J Clin Nutr 2007;86:434 – 43. Printed in USA. © 2007 American Society for Nutrition at Niguarda Granda on December 1, 2007 www.ajcn.org Downloaded from
Transcript of High folate intake is associated with lower breast cancer incidence in postmenopausal women in the...

See corresponding editorial on page 271.
High folate intake is associated with lower breast cancer incidencein postmenopausal women in the Malmö Diet and Cancer cohort1–3
Ulrika Ericson, Emily Sonestedt, Bo Gullberg, Håkan Olsson, and Elisabet Wirfalt
ABSTRACTBackground: Epidemiologic studies of associations between folateintake and breast cancer are inconclusive, but folate and other plantfood nutrients appear protective in women at elevated risk.Objective: The objective was to examine the association betweenfolate intake and the incidence of postmenopausal breast cancer.Design: This prospective study included all women aged �50 y(n � 11699) from the Malmö Diet and Cancer cohort. The meanfollow-up time was 9.5 y. We used a modified diet-history methodto collect nutrient intake data. At the end of follow-up, 392 incidentinvasive breast cancer cases were verified. We used proportionalhazard regression to calculate hazard ratios (HRs).Results: Compared with the lowest quintile, the incidence of inva-sive breast cancer was reduced in the highest quintile of dietary folateintake (HR: 0.56; 95% CI: 0.35, 0.90; P for trend � 0.02); total folateintake, including supplements (HR: 0.56; 95% CI: 0.34, 0.91; P fortrend � 0.006); and dietary folate equivalents (HR: 0.59; 95% CI:0.36, 0.97; P for trend � 0.01).Conclusion: A high folate intake was associated with a lower inci-dence of postmenopausal breast cancer in this cohort. Am J ClinNutr 2007;86:434–43.
KEY WORDS Folate, breast cancer, obesity, body mass index,postmenopausal women, prospective study, diet
INTRODUCTION
Folate can be found in high concentrations in dark-green leafyvegetables, legumes, fruit, and liver (1). Folate is a coenzyme thatcarries one-carbon units and is thereby of great importance in themetabolism of amino acids and nucleotides (2). Two main mech-anisms link folate deficiency to cancer development: a reducedsynthesis of S-adenosyl methionine (SAM), which results inaberrations in DNA methylation, and a reduced synthesis of thepyrimidine thymidylate, which results in the misincorporation ofuracil into DNA. A third possible mechanism is impaired purinesynthesis and subsequent changes in DNA (3). Epidemiologicstudies have indicated that high folate intake may protect againstcolorectal cancer (4, 5) but also against cancer at other sites(6–10). Current epidemiologic evidence of a relation betweenhigh folate intake and reduced breast cancer risk is, however, notconclusive. High folate intake was shown to be associated witha decreased risk of postmenopausal breast cancer in some studies(11–14), whereas this association was not confirmed in otherstudies (15–18).
Other B vitamins are involved in folate metabolism. VitaminB-12 acts as a cofactor to the enzyme methionine synthase, and
both vitamin B-6 and riboflavin serve as cofactors for folate-dependent enzymes (19, 20). A study in Shanghai showed thatthe association between a high folate intake and a decreased riskof breast cancer was stronger among women with high intakes ofvitamin B-12 and vitamin B-6 (13). The modifying effect ofvitamin B-12 is supported by other studies (11, 14).
Some studies indicate that the negative association betweenfolate intake and breast cancer mainly appears among women athighest risk, ie, high consumers of alcohol. The detrimental in-fluence of alcohol on folate bioavailability is probably the mostimportant explanation for this observation (16–18). Obesity,however, is a well-known risk factor for breast cancer develop-ment, as is a high alcohol consumption (21, 22). Similar to manyother studies, a previous report from the Malmö Diet and Cancer(MDC) study showed positive associations between BMI andbreast cancer (23). Higher concentrations of endogenous sexhormones have been suggested to partly explain the increasedrisk of breast cancer among high consumers of alcohol (24).However, an elevated concentration of sex hormones is also apossible mechanism by which obesity can increase breast cancerrisk (25, 26). In the Swedish mammography cohort, overweightwomen with high dietary intakes of ascorbic acid had a lowerincidence of breast cancer (27), but the risk relation was reversedin lean women. Ascorbic acid, an antioxidant that may protectagainst DNA damage (28), is mainly found in fruit and vegeta-bles, as is folate.
The aim of this study was to investigate whether folate intakeis associated with postmenopausal breast cancer in women fromthe MDC cohort. This article also evaluates whether other nutri-ents influence the association between folate intake and breastcancer incidence. Finally, we wanted to examine whether thepotential association between folate and breast cancer developmentwas different among women who already had a higher breast cancerrisk because they were overweight.
1 From the Department of Clinical Sciences, Lund University, Malmö,Sweden (UE, ES, BG, and EW), and the Department of Clinical Sciences,Lund University, Lund, Sweden (HO).
2 Supported by grants from the Swedish Cancer Society, the SwedishMedical Research Council, the City of Malmö, The Albert Påhlsson Foun-dation, and the Swedish Research Council Formas.
3 Reprints not available. Address correspondence to U Ericson, NutritionalEpidemiology, Clinical Research Center, Building 60, floor 13, Malmö Uni-versity Hospital, entrance 72, SE-205 02 Malmö, Sweden. E-mail:[email protected].
Received December 7, 2006.Accepted for publication March 21, 2007.
434 Am J Clin Nutr 2007;86:434–43. Printed in USA. © 2007 American Society for Nutrition
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from

SUBJECTS AND METHODS
Study design
The MDC study is a prospective cohort study being conductedin Malmö, a city in the south of Sweden with �250 000 inhab-itants. In 1991, the MDC source population was defined as allpersons living in the City of Malmö and born between 1926 and1945. However, in May 1995, the cohort was extended to includeall women born between 1923 and 1950 and all men born be-tween 1923 and 1945. With this extension, 74 138 persons con-stituted the source population. The MDC study was approved bythe Ethical Committee at Lund University (LU 51–90). Details ofthe recruitment procedures and the cohort are described else-where (29). Briefly, the participants were invited by personalletters or came spontaneously after invitation by advertisement inlocal newspapers, in public places, or in primary health carecenters. Inadequate Swedish language skills and mental incapac-ity were the only exclusion criteria. The participants visited theMDC screening center twice. During the first visit, groups of 6–8participants were instructed on how to register meals in a menubook and how to fill out the diet questionnaire and the extensivequestionnaire covering socioeconomic and lifestyle factors.Nurses drew blood samples, recorded blood pressures, andmade anthropometric measurements. All questionnaires werecompleted at home. During the second visit, �10 d after thefirst visit, the socioeconomic questionnaire was checked anda dietary interview was conducted. In October 1996, whenrecruitment was closed, 28 098 participants had completed allbaseline examinations.
Study population
This study includes women who completed the baseline ex-aminations and were aged �50 y. An age criterion for menopausewas used because of missing values on self-reported cessation ofmenses, imprecise cessation of menses in combination with in-formation on menopausal hormone use among premenopausalwomen, and lack of detailed information on all women’s medicalhistory of hysterectomy. Fifty years was chosen as the definitionfor menopause (30), because the median natural age of meno-pause was 50.0 y in a subsample of 2898 women (without surgeryand hormone therapy) from the cohort (31). Because the age atdiagnosis was �55 y in 95% of the cases, we have reason tobelieve that very few women were premenopausal at diagnosis.All women with prevalent cancers at baseline, except those withcervix cancer in situ, were excluded. In total 11 699 women wereincluded. The average follow-up time was 9.5 y.
Breast cancer case definition and ascertainment
The Swedish Cancer Registry and the Southern Swedish Re-gional Tumor Registry provided data on case definition andascertainment until the end of follow-up (31 December 2003).Cases were women who received a diagnosis of invasive breastcancer during follow-up. Invasive cancer was defined as all can-cer except in situ cancer. Because in situ cancer does not essen-tially progress into invasive cancer (32), inclusion of in situcancer may obscure true associations between diet and seriousdisease. However, a sensitivity analysis including in situ cancerswas performed. Information on vital status was obtained from theNational Tax Board, which provides up-to-date information onvital status for all Swedish residents. Cases contributed person
time from the date of enrollment until the time of diagnosis.Noncases contributed person time from the date of enrollmentuntil death, migrating from Sweden or end of follow-up, which-ever was the first. A total of 392 invasive breast cancers weredocumented during 110 925 y of follow-up.
Dietary data
The MDC study used an interview-based, modified diet-history method that combined 1) a 7-d menu-book for registra-tion of lunch and dinner meals, cold beverages including alcohol,drugs, natural remedies, and nutrient supplements; 2) a 168-itemquestionnaire for assessment of meal pattern, consumption fre-quencies, and portion sizes of regularly eaten foods; and 3) a45-min complementary interview. The consistency of the infor-mation provided was carefully checked so that the questionnaireand menu book did not overlap.
The mean daily intake of foods was calculated on the basis offrequency and portion-size estimates from the questionnaire andmenu book. Food intake was converted to energy and nutrientintakes by using the MDC nutrient database, in which most of thenutrient information comes from PC-KOST2-93 from the Na-tional Food Administration in Uppsala, Sweden. The MDCmethod is described in detail elsewhere (33, 34). Nutrient intakesfrom supplements were calculated on the basis of the supplementconsumption recorded in the menu book. Supplement consump-tion was converted to nutrient intakes by using the MDC sup-plement database. This database contains information aboutnutrient contents in medical drugs, herbal remedies, and supple-ments consumed in the MDC study (35). The relative validity ofthe MDC method was evaluated in 1984–1985 in a sample ofMalmö residents (n � 105 women and 101 men aged 50–69 y)with the use of 18 d of weighed records, 3 d every second monthduring 1 y, as the reference method (36, 37). Pearson’s correla-tion coefficients in women, adjusted for total energy, betweenthe reference method and the MDC method were 0.75 for folate,0.69 for dietary fiber, 0.70 for carotene, and 0.71 for ascorbicacid.
Dietary variables
This study examined daily dietary and total intakes (includingsupplements) of energy and the following nutrients: folate (�g),vitamin B-12 (�g), vitamin B-6 (mg), riboflavin (mg), dietaryfiber (g), carotene (mg), and ascorbic acid (mg). Total folateintakes were calculated by adding folic acid intake from supple-ments to the intake from foods. In addition, dietary folate equiv-alents were calculated based on the assumption that the bioavail-ability of synthetic folic acid consumed in a meal is 1.7 times thebioavailability of food folate (38), ie, dietary folate equivalents ��g food folate � 1.7 � �g folic acid from supplements.
Energy-adjusted variables were obtained by regressing in-takes of all nutrients on total energy intake (39). Quintiles ofnutrient residuals were used as exposure categories. Consump-tion of folic acid–containing supplements (yes or no) was basedon information about the current use of supplements from themenu book.
Other variables
In September 1994, the processing of dietary data was slightlyaltered (34). Method version (indicating data collection before or
FOLATE INTAKE AND BREAST CANCER 435
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from

after 1 September 1994) and season of data collection were ex-amined as potential confounders of dietary relations. Informationon age was obtained from the personal identification number.Age was divided into 5-y categories. The smoking status of theparticipants was defined as smokers (including irregular smok-ers), exsmokers, and never-smokers. Information on total alco-hol consumption was converted into a 4-category variable.Women reporting zero consumption in the menu book and indi-cating no consumption of any type of alcohol during the previousyear were categorized as zero reporters. The other categoryranges were �15 g alcohol/d (low), 15–30 g alcohol/d (medium),and �30 g alcohol/d (high). Alcohol intake was also dichoto-mized (�4.7 or �4.7 g/d). Leisure-time physical activity wasassessed by using a questionnaire adapted from the MinnesotaLeisure Time Physical Activity Questionnaire (40, 41). Thenumber of minutes per week of 18 different activities was mul-tiplied by an activity-specific intensity coefficient, and an overallleisure-time physical activity score was created. The score wasdivided into tertiles and categorized as low, medium, or high.Household activities were estimated in hours per week and di-vided into 4 groups with cutoffs every 10 h (0–9, 10–19, 20–29,or �30).
The participants were divided into 4 categories according totheir highest level of education (�8 y, 9–10 y, 11–13 y, oruniversity degree). Classification of the socioeconomic indexwas based on information on job title, tasks, and position at work.The procedure was adapted from that of the 1989 Swedish pop-ulation census (42). In this study, the information was collapsedinto 5 categories: blue-collar workers, white-collar workers(low, medium, or high), and self-employed. The retired and un-employed categories were classified according to their positionbefore retirement or unemployment.
Weight was measured to the nearest 0.1 kg by using a balance-beam scale while the subjects were wearing light clothing and noshoes. Standing height was measured with a fixed stadiometercalibrated in centimeters. Body mass index (BMI; in kg/m2) wascalculated from a direct measurement of weight and height and a3-category variable was created (BMI � 25, 25–29, or �30).BMI was also dichotomized (�25 or �25).
Age at menarche and age at menopause were used as contin-uous variables. Lactation was reported as the total number ofmonths for all children. Years with menstrual cycles was the timespan between menarche and menopause accounting for interrup-tions for pregnancies and lactation. The duration of contraceptivepill use (in y) was divided into 4 categories, with zero consump-tion as the lowest category. Current hormone replacement ther-apy (HRT; yes or no) was based on the questionnaire item,“Which medications do you use on a regular basis? ”, in combi-nation with information on drug use from the 7-d menu book(43). Age at birth of first child was divided into 4 categories withan additional category for women with no children. Parity wasthe number of children with no children in the lowest category,and 4 or more in the highest.
Statistical analysis
The SPSS statistical computer package (version 11.5; SPSSInc, Chicago, IL) was used for all statistical analyses. All nutrientand food variables were log transformed (10-log) to normalizethe distribution before analysis. A very small amount (0.01) wasadded before transformation to handle zero intakes.
The baseline status of established risk factors and potentialconfounders was examined in cases and noncases with Cox pro-portional hazard regression or analysis of variance. All modelswere adjusted for age. Models including dietary data were alsoadjusted for method version and season. Energy-adjusted partialcorrelation coefficients between intakes (dietary and total) offolate and other nutrients were computed.
Cox proportional hazard regression examined quintiles of fo-late intake (regressed on total energy) in relation to hazard ratios(HRs) of invasive breast cancer. Adjustments were made for agecategory, method version, season, and energy with the residualmethod (39). A second model included adjustments for vitaminB-12, vitamin B-6, and riboflavin. In the third multivariatemodel, adjustments were also made for established risk factorsand potential confounders (ie, weight, height, leisure-time phys-ical activity, household work, smoking, alcohol, socioeconomicstatus, age at menopause, and HRT). These covariates were iden-tified from the literature or previously indicated potential con-founding of the folate–breast cancer association within the MDCcohort (44, 45). To evaluate the probability that folate is a gen-uine risk factor for breast cancer, independent of other plant foodcomponents, the full model was also repeated with adjustmentsfor either intake of ascorbic acid, carotene, or dietary fiber. Fi-nally, analysis with the full model was stratified on the dichot-omous BMI variable (�25 and �25) and on alcohol intake (�4.7and �4.7 g/d). Sensitivity analyses were made for age (�55 y),for alcohol intake (�15 g/d), and by inclusion of in situ cancers.All steps were repeated for dietary folate intakes (excluding folicacid from supplements), total folate intakes, and dietary folateequivalents.
RESULTS
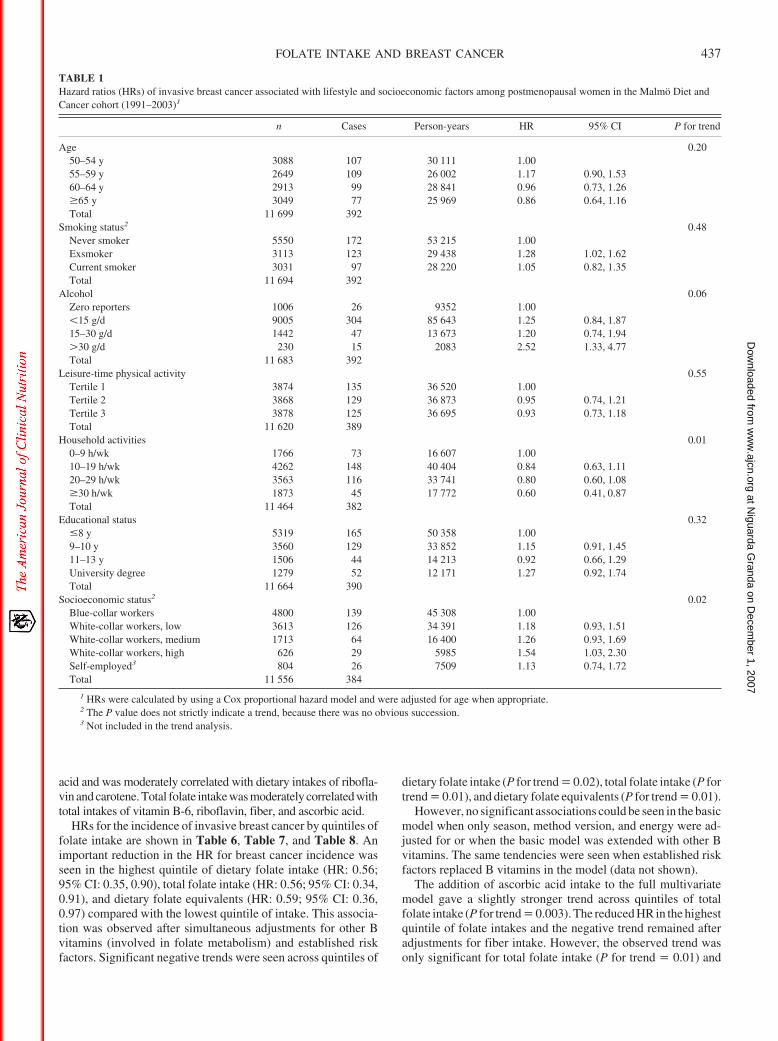
Age-adjusted breast cancer HRs of the study cohort are pre-sented in relation to lifestyle and socioeconomic factors in Table1. Exsmokers had a higher breast cancer incidence than did neversmokers, and women with an alcohol intake �30 g/d had a higherbreast cancer incidence than did zero consumers. High white-collar workers had a higher incidence than did blue-collar work-ers. Women who spent much time on household work had a lowerincidence (�30 h/wk compared with �10 h/wk), but the differ-ence was no longer significant after adjustment for age at meno-pause and parity (data not shown).
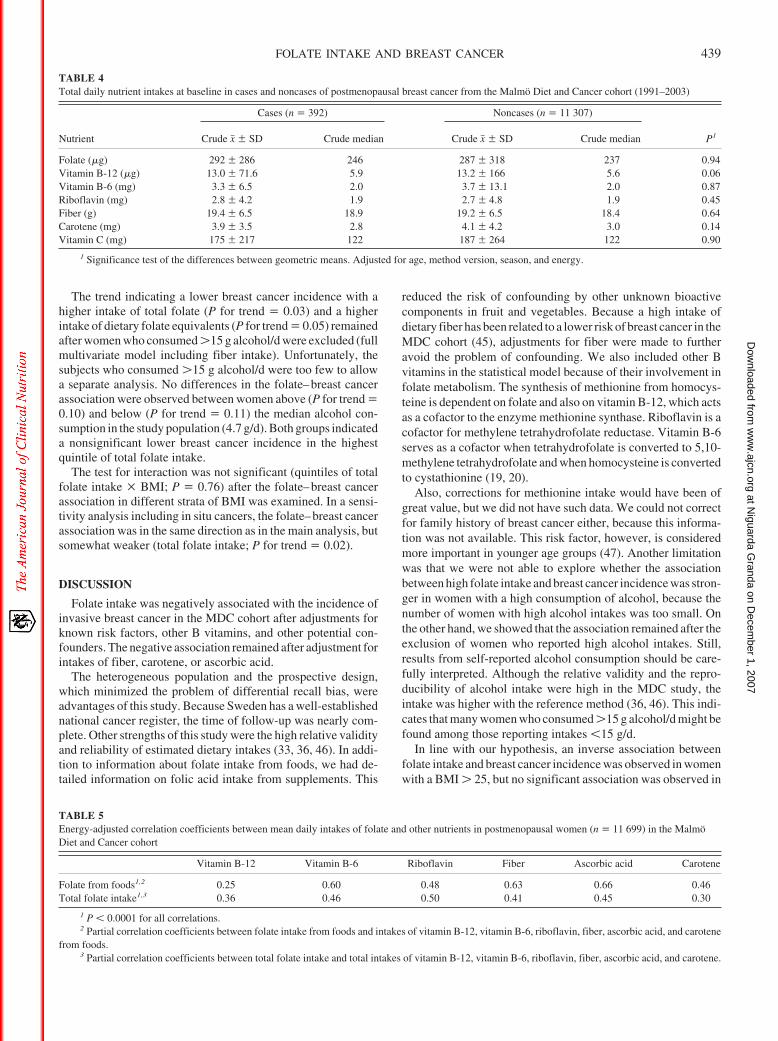
Current HRT was also a significant risk factor for invasivebreast cancer (Table 2). Use of contraceptive pills for �16 y wasassociated with a higher incidence of breast cancer. However, theincrease was no longer significant after HRT and age at meno-pause were controlled for (data not shown). Age at menopausewas higher in cases than in noncases (P for trend � 0.04), butwhen the total number of years with menstrual cycles was com-puted, a slightly stronger association was seen (P for trend �0.03) (Table 3). Both height and weight were significantlyhigher in cases than in noncases. Total mean daily intakes of Bvitamins, fiber, carotene, and ascorbic acid did not significantlydiffer between cases and noncases in a basic model with adjust-ments for age, method version, and season (Table 4). The totalmedian intake of folate in the study population was 238 �g/d.
Partialcorrelationcoefficientsbetweenintakesof folateandothernutrients are shown in Table 5. Dietary folate intake was stronglycorrelated with dietary intakes of vitamin B-6, fiber, and ascorbic
436 ERICSON ET AL
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from
acid and was moderately correlated with dietary intakes of ribofla-vin and carotene. Total folate intake was moderately correlated withtotal intakes of vitamin B-6, riboflavin, fiber, and ascorbic acid.
HRs for the incidence of invasive breast cancer by quintiles offolate intake are shown in Table 6, Table 7, and Table 8. Animportant reduction in the HR for breast cancer incidence wasseen in the highest quintile of dietary folate intake (HR: 0.56;95% CI: 0.35, 0.90), total folate intake (HR: 0.56; 95% CI: 0.34,0.91), and dietary folate equivalents (HR: 0.59; 95% CI: 0.36,0.97) compared with the lowest quintile of intake. This associa-tion was observed after simultaneous adjustments for other Bvitamins (involved in folate metabolism) and established riskfactors. Significant negative trends were seen across quintiles of
dietary folate intake (P for trend � 0.02), total folate intake (P fortrend � 0.01), and dietary folate equivalents (P for trend � 0.01).
However, no significant associations could be seen in the basicmodel when only season, method version, and energy were ad-justed for or when the basic model was extended with other Bvitamins. The same tendencies were seen when established riskfactors replaced B vitamins in the model (data not shown).
The addition of ascorbic acid intake to the full multivariatemodel gave a slightly stronger trend across quintiles of totalfolate intake (P for trend � 0.003). The reduced HR in the highestquintile of folate intakes and the negative trend remained afteradjustments for fiber intake. However, the observed trend wasonly significant for total folate intake (P for trend � 0.01) and
TABLE 1Hazard ratios (HRs) of invasive breast cancer associated with lifestyle and socioeconomic factors among postmenopausal women in the Malmö Diet andCancer cohort (1991–2003)1
n Cases Person-years HR 95% CI P for trend
Age 0.2050–54 y 3088 107 30 111 1.0055–59 y 2649 109 26 002 1.17 0.90, 1.5360–64 y 2913 99 28 841 0.96 0.73, 1.26�65 y 3049 77 25 969 0.86 0.64, 1.16Total 11 699 392
Smoking status2 0.48Never smoker 5550 172 53 215 1.00Exsmoker 3113 123 29 438 1.28 1.02, 1.62Current smoker 3031 97 28 220 1.05 0.82, 1.35Total 11 694 392
Alcohol 0.06Zero reporters 1006 26 9352 1.00�15 g/d 9005 304 85 643 1.25 0.84, 1.8715–30 g/d 1442 47 13 673 1.20 0.74, 1.94�30 g/d 230 15 2083 2.52 1.33, 4.77Total 11 683 392
Leisure-time physical activity 0.55Tertile 1 3874 135 36 520 1.00Tertile 2 3868 129 36 873 0.95 0.74, 1.21Tertile 3 3878 125 36 695 0.93 0.73, 1.18Total 11 620 389
Household activities 0.010–9 h/wk 1766 73 16 607 1.0010–19 h/wk 4262 148 40 404 0.84 0.63, 1.1120–29 h/wk 3563 116 33 741 0.80 0.60, 1.08�30 h/wk 1873 45 17 772 0.60 0.41, 0.87Total 11 464 382
Educational status 0.32�8 y 5319 165 50 358 1.009–10 y 3560 129 33 852 1.15 0.91, 1.4511–13 y 1506 44 14 213 0.92 0.66, 1.29University degree 1279 52 12 171 1.27 0.92, 1.74Total 11 664 390
Socioeconomic status2 0.02Blue-collar workers 4800 139 45 308 1.00White-collar workers, low 3613 126 34 391 1.18 0.93, 1.51White-collar workers, medium 1713 64 16 400 1.26 0.93, 1.69White-collar workers, high 626 29 5985 1.54 1.03, 2.30Self-employed3 804 26 7509 1.13 0.74, 1.72Total 11 556 384
1 HRs were calculated by using a Cox proportional hazard model and were adjusted for age when appropriate.2 The P value does not strictly indicate a trend, because there was no obvious succession.3 Not included in the trend analysis.
FOLATE INTAKE AND BREAST CANCER 437
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from

dietary folate equivalents (P for trend � 0.01). The results did notsubstantially change when carotene replaced fiber in the multi-variate model.
Nineteen percent of the women consumed folic acid– con-taining supplements. Consumption of folic acid– containingsupplements was independently associated with a lower HRfor invasive breast cancer (0.63; 95% CI: 0.43, 0.94) in the fullmultivariate model with adjustment for dietary folate. How-ever, the association between dietary folate intake and breastcancer was not influenced by the consumption of folic acid–
containing supplements (data not shown). Supplement con-sumption tended to be more frequent in women with highdietary folate intakes (22% in the highest quintile comparedwith 15% in the lowest quintile).
The analysis was repeated with the exclusion of womenyounger than 55 y at baseline. The significant reduction in the HRin the highest quintile of dietary folate equivalents was strength-ened (HR: 0.48; 95% CI: 0.28, 0.84; P for trend � 0.004) in thissubsample and did not substantially change after adjustment forfiber intake, carotene, and ascorbic acid.
TABLE 2Hazard ratios (HRs) of invasive breast cancer associated with reproductive and anthropometric factors among postmenopausal women in the Malmö Dietand Cancer cohort (1991–2003)1
n Cases Person-years HR 95% CI P for trend
Duration of contraceptive pill use 0.010 6980 214 65 551 1.001–5 y 1680 52 16 241 0.93 0.68, 1.286–15 y 1806 67 17 285 1.14 0.86, 1.51�16 y 1031 54 9863 1.58 1.16, 2.16Total 11 497 387
Hormone replacement therapyNo 8611 233 80 420 1.00Yes 2377 126 22 261 1.92 1.54, 2.39Total 10 988 359
Age at birth of first childNo children 1440 47 13 203 1.24 0.83, 1.83�20 y 1882 53 17 780 1.00 0.152
20–25 y 4131 139 39 256 1.20 0.88, 1.6525–30 2959 99 28 140 1.20 0.86, 1.68�30 1066 40 10 066 1.39 0.92, 2.09Total 11 478 378
Parity (number of children) 0.510 1440 47 13 203 1.001 2496 79 23 586 0.94 0.65, 1.342 4674 160 44 501 0.99 0.71, 1.373 2009 73 19 083 1.05 0.73, 1.52�4 870 19 8177 0.64 0.38, 1.10Total 11 489 378
BMI 0.41�25 5861 183 56 060 1.0025–30 4069 147 38 372 1.20 0.96, 1.49�30 1747 62 16 308 1.19 0.89, 1.59Total 11 677 392
1 Values were calculated by using a Cox proportional hazard model and were adjusted for age.2 Test for trend in women with at least one child.
TABLE 3Anthropometric and reproductive characteristics among cases and noncases of postmenopausal breast cancer in the Malmö Diet and Cancer cohort(1991–2003)1
No. of cases/noncases Cases Noncases P2
Weight (kg) 392/11 285 69.6 11.63 68.2 11.7 0.02Height (cm) 392/11 286 163.9 5.6 163.1 6.0 0.03Age at menarche (y) 386/11 211 13.6 1.4 13.6 1.5 0.99Age at menopause (y) 339/9981 49.9 4.7 49.4 4.5 0.04Duration of lactation (mo) 323/9758 8.0 7.6 8.3 8.7 0.67Time between menarche and menopause (y) 335/9925 36.3 4.8 35.7 4.7 0.04Years with menstrual cycles (y)4 323/9758 34.3 4.7 33.7 4.9 0.03
1 Values were adjusted for age.2 ANOVA.3 x� SD (all such values).4 Pregnancies and lactation were accounted for.
438 ERICSON ET AL
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from
The trend indicating a lower breast cancer incidence with ahigher intake of total folate (P for trend � 0.03) and a higherintake of dietary folate equivalents (P for trend � 0.05) remainedafter women who consumed �15 g alcohol/d were excluded (fullmultivariate model including fiber intake). Unfortunately, thesubjects who consumed �15 g alcohol/d were too few to allowa separate analysis. No differences in the folate–breast cancerassociation were observed between women above (P for trend �0.10) and below (P for trend � 0.11) the median alcohol con-sumption in the study population (4.7 g/d). Both groups indicateda nonsignificant lower breast cancer incidence in the highestquintile of total folate intake.
The test for interaction was not significant (quintiles of totalfolate intake � BMI; P � 0.76) after the folate–breast cancerassociation in different strata of BMI was examined. In a sensi-tivity analysis including in situ cancers, the folate–breast cancerassociation was in the same direction as in the main analysis, butsomewhat weaker (total folate intake; P for trend � 0.02).
DISCUSSION
Folate intake was negatively associated with the incidence ofinvasive breast cancer in the MDC cohort after adjustments forknown risk factors, other B vitamins, and other potential con-founders. The negative association remained after adjustment forintakes of fiber, carotene, or ascorbic acid.
The heterogeneous population and the prospective design,which minimized the problem of differential recall bias, wereadvantages of this study. Because Sweden has a well-establishednational cancer register, the time of follow-up was nearly com-plete. Other strengths of this study were the high relative validityand reliability of estimated dietary intakes (33, 36, 46). In addi-tion to information about folate intake from foods, we had de-tailed information on folic acid intake from supplements. This
reduced the risk of confounding by other unknown bioactivecomponents in fruit and vegetables. Because a high intake ofdietary fiber has been related to a lower risk of breast cancer in theMDC cohort (45), adjustments for fiber were made to furtheravoid the problem of confounding. We also included other Bvitamins in the statistical model because of their involvement infolate metabolism. The synthesis of methionine from homocys-teine is dependent on folate and also on vitamin B-12, which actsas a cofactor to the enzyme methionine synthase. Riboflavin is acofactor for methylene tetrahydrofolate reductase. Vitamin B-6serves as a cofactor when tetrahydrofolate is converted to 5,10-methylene tetrahydrofolate and when homocysteine is convertedto cystathionine (19, 20).
Also, corrections for methionine intake would have been ofgreat value, but we did not have such data. We could not correctfor family history of breast cancer either, because this informa-tion was not available. This risk factor, however, is consideredmore important in younger age groups (47). Another limitationwas that we were not able to explore whether the associationbetween high folate intake and breast cancer incidence was stron-ger in women with a high consumption of alcohol, because thenumber of women with high alcohol intakes was too small. Onthe other hand, we showed that the association remained after theexclusion of women who reported high alcohol intakes. Still,results from self-reported alcohol consumption should be care-fully interpreted. Although the relative validity and the repro-ducibility of alcohol intake were high in the MDC study, theintake was higher with the reference method (36, 46). This indi-cates that many women who consumed �15 g alcohol/d might befound among those reporting intakes �15 g/d.
In line with our hypothesis, an inverse association betweenfolate intake and breast cancer incidence was observed in womenwith a BMI � 25, but no significant association was observed in
TABLE 4Total daily nutrient intakes at baseline in cases and noncases of postmenopausal breast cancer from the Malmö Diet and Cancer cohort (1991–2003)
Nutrient
Cases (n � 392) Noncases (n � 11 307)
P1Crude x� SD Crude median Crude x� SD Crude median
Folate (�g) 292 286 246 287 318 237 0.94Vitamin B-12 (�g) 13.0 71.6 5.9 13.2 166 5.6 0.06Vitamin B-6 (mg) 3.3 6.5 2.0 3.7 13.1 2.0 0.87Riboflavin (mg) 2.8 4.2 1.9 2.7 4.8 1.9 0.45Fiber (g) 19.4 6.5 18.9 19.2 6.5 18.4 0.64Carotene (mg) 3.9 3.5 2.8 4.1 4.2 3.0 0.14Vitamin C (mg) 175 217 122 187 264 122 0.90
1 Significance test of the differences between geometric means. Adjusted for age, method version, season, and energy.
TABLE 5Energy-adjusted correlation coefficients between mean daily intakes of folate and other nutrients in postmenopausal women (n � 11 699) in the MalmöDiet and Cancer cohort
Vitamin B-12 Vitamin B-6 Riboflavin Fiber Ascorbic acid Carotene
Folate from foods1,2 0.25 0.60 0.48 0.63 0.66 0.46Total folate intake1,3 0.36 0.46 0.50 0.41 0.45 0.30
1 P � 0.0001 for all correlations.2 Partial correlation coefficients between folate intake from foods and intakes of vitamin B-12, vitamin B-6, riboflavin, fiber, ascorbic acid, and carotene
from foods.3 Partial correlation coefficients between total folate intake and total intakes of vitamin B-12, vitamin B-6, riboflavin, fiber, ascorbic acid, and carotene.
FOLATE INTAKE AND BREAST CANCER 439
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from

normal-weight women. However, the power to detect an inter-action between BMI and folate intake was low, and the test forinteraction was not significant. Consequently, we cannot excludethat the observed differences between strata were due to chance.
Four case-control studies suggest that high folate intakes areassociated with a decreased risk of postmenopausal breast cancer(11–13, 48), and a Scottish study indicated a nonsignificant neg-ative association (49). In 2 case-control studies, folate intakecould not be related to postmenopausal breast cancer (15, 50).High dietary folate intake was recently associated with a de-creased risk of postmenopausal breast cancer in women from alarge French cohort (14), and a nested case-control study fromDenmark reported that total folate intakes �300 �g/d indicate anincreased risk, albeit nonsignificant (51). Results from mostother prospective studies do not support the overall inverse as-sociation between folate intake and postmenopausal breast can-cer observed in this study (15–18, 52). In fact, 4 cohort found nosignificant relations (15–17, 52). In addition, a study from amulticenter cohort in the United States showed that high totalintakes are related to a significantly increased risk (18). How-ever, most cohort studies observed a decreased risk with high
folate intakes in women with a moderate to high consumption ofalcohol (16, 17, 52). In a Danish study, an increased breast cancerrisk was only associated with alcohol consumption in womenwith low folate intakes (51). To the best of our knowledge, nostudy has previously investigated whether the relation betweenfolate intake and breast cancer is different between overweightwomen and normal-weight women. Yet, in another Swedishstudy, a high intake of ascorbic acid was only related to a lowerrisk of breast cancer in overweight women (27).
Our findings of an association between high folate intake andlower breast cancer incidence confirm the biological hypothesisthat low intakes of folate enhance the development of breastcancer. Folate in a reduced form, 5-MTHF, acts as a methyl donorin the synthesis of methionine, which is needed for the synthesisof SAM. SAM is the most important methyl donor in biologicalreactions, including DNA methylation (3). Changes in DNAmethylation patterns are an early event in carcinogenesis andmay influence gene silencing (53, 54). Folate is also involved inDNA synthesis and repair; folate deficiency has been related toelevated uracil incorporation to DNA and subsequent chromo-some breaks, which may contribute to an increased risk of cancer
TABLE 6Hazard ratios (and 95% CIs) of invasive breast cancer across quintiles of dietary folate intake in women aged �50 y from the Malmö Diet and Cancercohort (1991–2003)1
Quintiles of dietary folate intake
P for trend21 2 3 4 5
Median (�g) 153 194 218 249 302No. of cases/person-years3 72/21 564 77/22 035 86/22 058 84/22 576 73/22 691Basic model4 1.00 1.03 (0.75, 1.43) 1.15 (0.84, 1.57) 1.09 (0.80, 1.50) 0.93 (0.67, 1.29) 0.69Model with B vitamins5 1.00 1.07 (0.77, 1.50) 1.18 (0.83, 1.67) 1.10 (0.76, 1.59) 0.81 (0.54, 1.22) 0.25Full model6 1.00 0.85 (0.59, 1.24) 0.94 (0.64, 1.38) 0.88 (0.58, 1.33) 0.56 (0.35, 0.90) 0.02
1 Hazard ratios were calculated by using a Cox proportional hazard model and were adjusted for energy with the residual method.2 Tests for trend of quintile medians.3 Basic model.4 Adjusted for age, method version, season, and total energy.5 Basic model with additional adjustment for quintiles of vitamin B-12 from foods, quintiles of vitamin B-6 from foods, and quintiles of riboflavin from
foods.6 Model as in footnote 5 with additional adjustment for weight, height, leisure-time physical activity, household work, smoking, socioeconomic status, age
at menopause, hormone replacement therapy, and alcohol intake.
TABLE 7Hazard ratios (and 95% CIs) of invasive breast cancer across quintiles of total folate intake in women aged �50 y from the Malmö Diet and Cancer cohort(1991–2003)1
Quintiles of total folate intake
P for trend21 2 3 4 5
Median (�g) 160 204 236 284 456No. of cases/person-years3 71/21 587 78/22 124 85/22 104 84/22 691 74/22 418Basic model4 1.00 1.06 (0.77, 1.46) 1.16 (0.84, 1.58) 1.10 (0.80, 1.51) 0.98 (0.71, 1.36) 0.67Model with B vitamins5 1.00 1.11 (0.80, 1.56) 1.22 (0.86, 1.72) 1.11 (0.76, 1.61) 0.84 (0.55, 1.29) 0.18Full model6 1.00 0.99 (0.68, 1.44) 1.01 (0.68, 1.50) 0.94 (0.62, 1.43) 0.56 (0.34, 0.91) 0.006
1 Hazard ratios were calculated by using a Cox proportional hazard model and were adjusted for energy with the residual method.2 Tests for trend of quintile medians.3 Basic model.4 Adjusted for age, method version, season, and total energy.5 Basic model with additional adjustment for quintiles of total vitamin B-12 intake, quintiles of total vitamin B-6 intake, and quintiles of total riboflavin
intake.6 Model as in footnote 5 with additional adjustment for weight, height, leisure-time physical activity, household work, smoking, socioeconomic status, age
at menopause, hormone replacement therapy, and alcohol intake.
440 ERICSON ET AL
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from

(55). Overweight women might have an increased need for DNArepair in mammary epithelial cells because of an elevated pro-liferative activity (56) caused by higher concentrations of estro-gens (26). Also, high concentrations of insulin may be respon-sible for the increased risk of breast cancer in overweight women(57). Because high folate intakes have been shown to be relatedto increased insulin sensitivity and reduced insulin concentra-tions (58), a protective effect of folate in overweight women isplausible. Although folate is involved in DNA repair, ascorbicacid is an antioxidant that may prevent DNA damage by scav-enging free radicals (28). However, the antioxidative propertiesof ascorbic acid may also increase the stability of folate duringfood preparation and digestion (59).
It is possibly the rather low folate intake in this population that,unlike most other cohort studies, enables us to detect an overallinverse association between folate intake and postmenopausalbreast cancer. In the Nurses’ Health Study (NHS), the total folateintake in the first quintile was in range of that in this study, but theNHS used the second quintile as a reference category (17). In 3published cohort studies, cutoffs between the first and secondintake categories of total folate ranged from 210 to 335 �g/d,compared with 178 �g/d in this study population, and cutoffsbetween the highest intake groups ranged from 400 to 853 �g/d,compared with 349 �g/d in this study population (15, 18, 51).The study of French women by Lajous et al (14) had no infor-mation on total folate intake but detected an inverse associationdespite higher dietary intakes than in our study. However, thegreatest risk reduction seemed to occur after the first quintile ofdietary folate intake (14). In the present study, only in the highestquintile of total folate intake did the median intake (456 �g)exceed the Nordic recommended daily intake of 300 �g folate.Consequently, the negative associations observed in the presentstudy were not achieved at unrealistic intakes. It might be pos-sible, by several methods, to increase the folate intake in thisstudy population. In Sweden, most supplements with folic acidcontain 400 �g, which is in line with the amount related to lowerbreast cancer incidence in this study. In addition, Sweden has notyet come to a decision concerning the mandatory folic acid for-tification of foods. With regard to the contradictory results fromdifferent studies, including an American study that indicated anincreased risk at total intakes much higher than in our study (18),
an increased consumption of fruit and vegetables would be asafer way to increase folate intakes. The consumption of fruit andvegetables is relatively low in Sweden compared with that inother European countries, but is similar to consumption in theUnited States (60, 61). On the other hand, a trend toward a higherconsumption of fruit and vegetables has been observed (62, 63).
In summary, our results indicate that high folate intakes areassociated with a lower incidence of postmenopausal breast can-cer. These findings could not be explained by intakes of othernutrients found in the same foods as folate.
We thank the staff and participants of the Malmö Diet and Cancer Study.The authors’ responsibilities were as follows—UE: wrote the manuscript,
performed the data analysis, and contributed to the study design; ES: helpedrevise the manuscript; BG: gave statistical advice, contributed to the studydesign, and helped revise the manuscript; HO: gave advice on matters relatedto oncology and helped interpret the results and revise the manuscript; EW:contributed to the study design and helped interpret the results and revise themanuscript. No conflicts of interest were reported.
REFERENCES1. Nordic Council of Ministers. Nordic nutrition recommendations 2004.
Copenhagen, Denmark: Nordic Council of Ministers, 2004.2. Stover PJ. Physiology of folate and vitamin B12 in health and disease.
Nutr Rev 2004;62:S3–12; discussion S13.3. Choi SW, Mason JB. Folate and carcinogenesis: an integrated scheme.
J Nutr 2000;130:129–32.4. Giovannucci E. Epidemiologic studies of folate and colorectal neopla-
sia: a review. J Nutr 2002;132(suppl):2350S–5S.5. Sanjoaquin MA, Allen N, Couto E, Roddam AW, Key TJ. Folate intake
and colorectal cancer risk: a meta-analytical approach. Int J Cancer2005;113:825–8.
6. Prinz-Langenohl R, Fohr I, Pietrzik K. Beneficial role for folate in theprevention of colorectal and breast cancer. Eur J Nutr 2001;40:98–105.
7. Eichholzer M, Luthy J, Moser U, Fowler B. Folate and the risk ofcolorectal, breast and cervix cancer: the epidemiological evidence.Swiss Med Wkly 2001;131:539–49.
8. Stevens VL, Rodriguez C, Pavluck AL, McCullough ML, Thun MJ,Calle EE. Folate nutrition and prostate cancer incidence in a large cohortof US men. Am J Epidemiol 2006;163:989–96.
9. Pelucchi C, Galeone C, Talamini R, et al. Dietary folate and risk ofprostate cancer in Italy. Cancer Epidemiol Biomarkers Prev 2005;14:944–8.
10. Larsson SC, Hakansson N, Giovannucci E, Wolk A. Folate intake andpancreatic cancer incidence: a prospective study of Swedish women andmen. J Natl Cancer Inst 2006;98:407–13.
TABLE 8Hazard ratios (and 95% CIs) of invasive breast cancer across quintiles of dietary folate equivalents in women aged �50 y from the Malmö Diet and Cancercohort (1991–2003)1
Quintiles of dietary folate equivalents
P for trend21 2 3 4 5
Median (�g) 160 204 237 287 582No. of cases/person-years3 71/21 593 78/22 107 89/22 121 77/22 748 77/22 356Basic model4 1.00 1.06 (0.77, 1.46) 1.21 (0.89, 1.66) 1.00 (0.73, 1.39) 1.02 (0.74, 1.41) 0.77Model with B vitamins5 1.00 1.11 (0.79, 1.55) 1.27 (0.90, 1.79) 1.00 (0.68, 1.45) 0.88 (0.57, 1.37) 0.26Full model6 1.00 0.99 (0.68, 1.44) 1.04 (0.71, 1.55) 0.86 (0.56, 1.31) 0.59 (0.36, 0.97) 0.01
1 Hazard ratios were calculated by using a Cox proportional hazard model and were adjusted for energy with the residual method.2 Tests for trend of quintile medians.3 Basic model.4 Adjusted for age, method version, season, and total energy.5 Basic model with additional adjustment for quintiles of total vitamin B-12 intake, quintiles of total vitamin B-6 intake, and quintiles of total riboflavin
intake.6 Model as in footnote 5 with additional adjustment for weight, height, leisure-time physical activity, household work, smoking, socioeconomic status, age
at menopause, hormone replacement therapy, and alcohol intake.
FOLATE INTAKE AND BREAST CANCER 441
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from
11. Lajous M, Lazcano-Ponce E, Hernandez-Avila M, Willett W, Romieu I.Folate, vitamin B(6), and vitamin B(12) intake and the risk of breastcancer among Mexican women. Cancer Epidemiol Biomarkers Prev2006;15:443–8.
12. Negri E, La Vecchia C, Franceschi S. Re: dietary folate consumption andbreast cancer risk. J Natl Cancer Inst 2000;92:1270–1.
13. Shrubsole MJ, Jin F, Dai Q, et al. Dietary folate intake and breast cancerrisk: results from the Shanghai Breast Cancer Study. Cancer Res 2001;61:7136–41.
14. Lajous M, Romieu I, Sabia S, Boutron-Ruault MC, Clavel-Chapelon F.Folate, vitamin B(12) and postmenopausal breast cancer in a prospectivestudy of French women. Cancer Causes Control 2006;17:1209–13.
15. Feigelson HS, Jonas CR, Robertson AS, McCullough ML, Thun MJ,Calle EE. Alcohol, folate, methionine, and risk of incident breast cancerin the American Cancer Society Cancer Prevention Study II NutritionCohort. Cancer Epidemiol Biomarkers Prev 2003;12:161–4.
16. Rohan TE, Jain MG, Howe GR, Miller AB. Dietary folate consumptionand breast cancer risk. J Natl Cancer Inst 2000;92:266–9.
17. Zhang S, Hunter DJ, Hankinson SE, et al. A prospective study of folateintake and the risk of breast cancer. JAMA 1999;281:1632–7.
18. Stolzenberg-Solomon RZ, Chang SC, Leitzmann MF, et al. Folate in-take, alcohol use, and postmenopausal breast cancer risk in the Prostate,Lung, Colorectal, and Ovarian Cancer Screening Trial. Am J Clin Nutr2006;83:895–904.
19. Lamprecht SA, Lipkin M. Chemoprevention of colon cancer by calcium,vitamin D and folate: molecular mechanisms. Nat Rev Cancer 2003;3:601–14.
20. Powers HJ. Interaction among folate, riboflavin, genotype, and cancer,with reference to colorectal and cervical cancer. J Nutr 2005;135(suppl):2960S—6S.
21. Singletary KW, Gapstur SM. Alcohol and breast cancer: review of ep-idemiologic and experimental evidence and potential mechanisms.JAMA 2001;286:2143–51.
22. Friedenreich CM. Review of anthropometric factors and breast cancerrisk. Eur J Cancer Prev 2001;10:15–32.
23. Lahmann PH, Lissner L, Gullberg B, Olsson H, Berglund G. A prospec-tive study of adiposity and postmenopausal breast cancer risk: theMalmo Diet and Cancer Study. Int J Cancer 2003;103:246–52.
24. Onland-Moret NC, Peeters PH, van der Schouw YT, Grobbee DE, vanGils CH. Alcohol and endogenous sex steroid levels in postmenopausalwomen: a cross-sectional study. J Clin Endocrinol Metab2005;90:1414–9.
25. Pike MC. Reducing cancer risk in women through lifestyle-mediatedchanges in hormone levels. Cancer Detect Prev 1990;14:595–607.
26. McTiernan A, Rajan KB, Tworoger SS, et al. Adiposity and sex hor-mones in postmenopausal breast cancer survivors. J Clin Oncol 2003;21:1961–6.
27. Michels KB, Holmberg L, Bergkvist L, Ljung H, Bruce A, Wolk A.Dietary antioxidant vitamins, retinol, and breast cancer incidence in acohort of Swedish women. Int J Cancer 2001;91:563–7.
28. Ferguson LR, Philpott M, Karunasinghe N. Dietary cancer and preven-tion using antimutagens. Toxicology 2004;198:147–59.
29. Manjer J, Carlsson S, Elmstahl S, et al. The Malmo Diet and CancerStudy: representativity, cancer incidence and mortality in participantsand non-participants. Eur J Cancer Prev 2001;10:489–99.
30. Morabia A, Flandre P. Misclassification bias related to definition ofmenopausal status in case-control studies of breast cancer. Int J Epide-miol 1992;21:222–8.
31. Wirfalt E, Mattisson I, Gullberg B, Olsson H, Berglund G. Fat fromdifferent foods show diverging relations with breast cancer risk in post-menopausal women. Nutr Cancer 2005;53:135–43.
32. Sanders ME, Schuyler PA, Dupont WD, Page DL. The natural history oflow-grade ductal carcinoma in situ of the breast in women treated bybiopsy only revealed over 30 years of long-term follow-up. Cancer2005;103:2481–4.
33. Callmer E, Riboli E, Saracci R, Akesson B, Lindgarde F. Dietary as-sessment methods evaluated in the Malmo food study. J Intern Med1993;233:53–7.
34. Wirfalt E, Mattisson I, Johansson U, Gullberg B, Wallstrom P, BerglundG. A methodological report from the Malmo Diet and Cancer study:development and evaluation of altered routines in dietary data process-ing. Nutr J 2002;1:3.
35. Elmståhl S, Wallström, P., Berglund, G., Janzon, L., Johansson, U.,Larsson, S.A., Mattisson, I. The use of dietary supplements in relation todietary habits in a Swedish middle-aged population. Scand J Nutr 1994;38:94–97.
36. Riboli E, Elmstahl S, Saracci R, Gullberg B, Lindgarde F. The MalmoFood Study: validity of two dietary assessment methods for measuringnutrient intake. Int J Epidemiol 1997;26(suppl):S161–73.
37. Elmstahl S, Riboli E, Lindgarde F, Gullberg B, Saracci R. The MalmoFood Study: the relative validity of a modified diet history method andan extensive food frequency questionnaire for measuring food intake.Eur J Clin Nutr 1996;50:143–51.
38. Yang TL, Hung J, Caudill MA, et al. A long-term controlled folatefeeding study in young women supports the validity of the 1.7 multiplierin the dietary folate equivalency equation. J Nutr 2005;135:1139–45.
39. Willett W, Stampfer MJ. Total energy intake: implications for epidemi-ologic analyses. Am J Epidemiol 1986;124:17–27.
40. Taylor HL, Jacobs DR Jr, Schucker B, Knudsen J, Leon AS, DebackerG. A questionnaire for the assessment of leisure time physical activities.J Chronic Dis 1978;31:741–55.
41. Richardson MT, Leon AS, Jacobs DR Jr, Ainsworth BE, Serfass R.Comprehensive evaluation of the Minnesota Leisure Time Physical Ac-tivity Questionnaire. J Clin Epidemiol 1994;47:271–81.
42. National Bureau of Statistics. Occupations in population and housingcensus 1985 (FoB 85) according to Nordic standard occupational clas-sification (Nordisk yrkesklassificering NYK) and Swedish socio-economic classification (Socioekonomisk indelning SEI). Stockholm,Sweden: Statistics Sweden, 1989 (in Swedish).
43. Merlo J, Berglund G, Wirfalt E, et al. Self-administered questionnairecompared with a personal diary for assessment of current use of hormonetherapy: an analysis of 16,060 women. Am J Epidemiol 2000;152:788–92.
44. Manjer J, Berglund G, Bondesson L, Garne JP, Janzon L, Malina J.Breast cancer incidence in relation to smoking cessation. Breast CancerRes Treat 2000;61:121–9.
45. Mattisson I, Wirfalt E, Johansson U, Gullberg B, Olsson H, Berglund G.Intakes of plant foods, fibre and fat and risk of breast cancer—a pro-spective study in the Malmo Diet and Cancer cohort. Br J Cancer 2004;90:122–7.
46. Elmstahl S, Gullberg B, Riboli E, Saracci R, Lindgarde F. The MalmoFood Study: the reproducibility of a novel diet history method and anextensive food frequency questionnaire. Eur J Clin Nutr 1996;50:134–42.
47. Loman N, Johannsson O, Kristoffersson U, Olsson H, Borg A. Familyhistory of breast and ovarian cancers and BRCA1 and BRCA2 mutationsin a population-based series of early-onset breast cancer. J Natl CancerInst 2001;93:1215–23.
48. Graham S, Hellmann R, Marshall J, et al. Nutritional epidemiology ofpostmenopausal breast cancer in western New York. Am J Epidemiol1991;134:552–66.
49. Sharp L, Little J, Schofield AC, et al. Folate and breast cancer: the roleof polymorphisms in methylenetetrahydrofolate reductase (MTHFR).Cancer Lett 2002;181:65–71.
50. Thorand B, Kohlmeier L, Simonsen N, Croghan C, Thamm M. Intake offruits, vegetables, folic acid and related nutrients and risk of breast cancerin postmenopausal women. Public Health Nutr 1998;1:147–56.
51. Tjonneland A, Christensen J, Olsen A, et al. Folate intake, alcohol andrisk of breast cancer among postmenopausal women in Denmark. EurJ Clin Nutr 2005.
52. Sellers TA, Kushi LH, Cerhan JR, et al. Dietary folate intake, alcohol,and risk of breast cancer in a prospective study of postmenopausalwomen. Epidemiology 2001;12:420–8.
53. Kim YI. Nutritional epigenetics: impact of folate deficiency on DNAmethylation and colon cancer susceptibility. J Nutr 2005;135:2703–9.
54. Duthie SJ, Narayanan S, Sharp L, Little J, Basten G, Powers H. Folate,DNA stability and colo-rectal neoplasia. Proc Nutr Soc 2004;63:571–8.
55. Blount BC, Mack MM, Wehr CM, et al. Folate deficiency causes uracilmisincorporation into human DNA and chromosome breakage: impli-cations for cancer and neuronal damage. Proc Natl Acad Sci U S A1997;94:3290–5.
56. Dumitrescu RG, Cotarla I. Understanding breast cancer risk— where dowe stand in 2005? J Cell Mol Med 2005;9:208–21.
442 ERICSON ET AL
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from

57. Kuhl H. Breast cancer risk in the WHI study: the problem of obesity.Maturitas 2005;51:83–97.
58. Setola E, Monti LD, Galluccio E, et al. Insulin resistance and endothelialfunction are improved after folate and vitamin B12 therapy in patientswith metabolic syndrome: relationship between homocysteine levelsand hyperinsulinemia. Eur J Endocrinol 2004;151:483–9.
59. McNulty H, Pentieva K. Folate bioavailability. Proc Nutr Soc 2004;63:529–36.
60. Agudo A, Slimani N, Ocke MC, et al. Consumption of vegetables, fruit
and other plant foods in the European Prospective Investigation intoCancer and Nutrition (EPIC) cohorts from 10 European countries. PublicHealth Nutr 2002;5:1179–96.
61. Krebs-SmithSM,KantorLS.Chooseavarietyoffruitsandvegetablesdaily:understanding the complexities. J Nutr 2001;131(suppl):487S–501S.
62. Becker W. Dietary guidelines and patterns of food and nutrient intake inSweden. Br J Nutr 1999;81(suppl):S113–7.
63. Groth MV, Fagt S. [Trends in dietary habits in Denmark and Swedensince the 1960s]. Ugeskr Laeger 2001;163:425–9 (in Danish).
FOLATE INTAKE AND BREAST CANCER 443
at Niguarda G
randa on Decem
ber 1, 2007 w
ww
.ajcn.orgD
ownloaded from




















