
Herts Valleys Clinical Commissioning Group
212
Herts Valleys Clinical Commissioning Group Board meeting held in public Thursday 9 March 2017 2.00pm Conference Centre, Rothamsted Centre for Research and Enterprise, Harpenden, Herts, AL5 2JQ Note concerning HVCCG management of conflicts of interest. A conflict of interest occurs where an individual’s ability to exercise judgement, or act in a role is, could be, or is seen to be impaired or otherwise influenced by his or her involvement in another role or relationship. In some circumstances, it could be reasonably considered that a conflict exists even when there is no actual conflict. In these cases it is important to still manage these perceived conflicts in order to maintain public trust. Members and attendees of the Board are reminded of their responsibilities. To ensure transparency and openness, individuals should notify the Chair of any potential conflicts of interest in relation to agenda items, even if the interest is already formally recorded.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Herts Valleys Clinical Commissioning Group

Herts Valleys Clinical
Commissioning Group
Board meeting held in public
Thursday 9 March 2017 2.00pm
Conference Centre, Rothamsted Centre for
Research and Enterprise, Harpenden,
Herts, AL5 2JQ
Note concerning HVCCG management of conflicts of interest.
A conflict of interest occurs where an individual’s ability to exercise judgement, or act in a role is, could be, or is seen to be impaired or otherwise influenced by his or her involvement in another role or relationship. In some circumstances, it could be reasonably considered that a conflict exists even when there is no actual conflict. In these cases it is important to still manage these perceived conflicts in order to maintain public trust.
Members and attendees of the Board are reminded of their responsibilities.
To ensure transparency and openness, individuals should notify the Chair of any potential conflicts of interest in relation to agenda items, even if the interest is already formally recorded.

Herts Valleys Clinical Commissioning Group Agenda
Board Meeting Held in Public
Thursday, 9 March 2017 at 2.00pm at Rothamsted Centre for Research and
Enterprise, Harpenden, Herts, AL5 2JQ
In accordance with section 1 (2) Public Bodies (Admissions to Meetings Act 1960), The Board resolves that:
Representatives of the press, and other members of the public, be excluded from this meeting having
regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial
to the public interest.
Meeting in private 1.00 pm to 2.00 pm
Meeting in public 2.00 pm
Note to representatives of the press and members of the public
Members of the public are reminded that CCG Board meetings are meetings held in public, not public meetings. However, the Board provides members of the public at the start of each meeting the opportunity to ask questions that relate to the agenda items. The Chair will not normally allow more than one question per person due to time constraints. The time given over to questions will need to be limited in order for the board to cover their agenda fully within the given time
Members of the public are urged, if possible, to give notice of their questions at least 48 hours before the beginning of the meeting in order that a full answer can be provided; if notice is not given, an answer will be provided whenever possible but the relevant information may not be available at the meeting. If such information is not available, the CCG will provide a written answer to the question as soon as is practicable after the meeting.
The Secretary can be contacted by email ([email protected]), by telephone (01442 284074), or by post to: Board Secretary, Herts Valleys Clinical Commissioning Group, Hemel One, Boundary Way, Hemel Hempstead, HP2 7YU.
Administrative items Led by 1. Chair’s introduction Verbal – for information Nicolas Small 2. Interests to declare Verbal – for information Nicolas Small Link to registers of interest: http://hertsvalleysccg.nhs.uk/about-us/managing-conflicts-of-interest 3. Minutes of previous meeting
12 January 2017Attachments - for approval Nicolas Small
4. Matters arising and action log Attachment - for approval Nicolas Small 5. Accountable Officer’s report Attachment – for discussion Cameron Ward Strategic discussion 6. Financial plan 2017-18 to 2018-19 Attachment – for approval Caroline Hall 7. CCG contributions to adult social care Attachment – for approval Cameron Ward
Break 3.45 - 3.55

Herts Valleys Clinical Commissioning Group Agenda
Performance 8. Integrated Quality, Finance and
Performance report8a. Quality and performance8b. Finance
Attachment – for discussion Stuart Bloom Charles Allan Diane Curbishley Caroline Hall
9. Medical directorate report Attachment – for discussion David Buckle Governance and assurance 10. Equality and diversity annual report Attachment – for information Paul Curry 11. Communications and engagement Update Attachment – for information Juliet Rodgers 12. Board Assurance Framework Attachment – for discussion Rod While 13. Annual report 2016-17 process Attachment – for approval Caroline Hall
14. Investment Committee report Attachment – for information Paul Smith
15. Committee Chairs’ Reports and Committeeminutes
Attachment – for Information Committee Chairs
15.1 Patient and Public Involvement Committee –minutes 14/12/2016
Attachment – for Information Alison Gardner
15.2 Quality and Performance Committee – minutes 2/2/2017
Attachment –for information Stuart Bloom
15.3 Audit Committee minutes 12/01/2017 Attachment –for information Paul Smith 16. Risks identified during the meeting For Agreement Chair 17. Date and time of next meeting Verbal Chair
Thursday 11 May 2017 Nilands Conference Centre, Rosary Priory, 93 Elstree Road, Bushey Heath, Watford Herts, WD23 4EE

SPACER PAGE

SPACER PAGE

1
Meeting : NHS Herts Valleys CCG Board Meeting
Date : 12 January 2017
Time : 13.30 – 16.20
Venue : The South Hill Centre, Hemel Hempstead
Present: Nicolas Small (NS) Chairman (Hertsmere GP) Stuart Bloom (SB) - to B/14/17 Board Lay Member Alison Gardner (AG) Board Lay Member Paul Smith (PS) Board Lay Member Cameron Ward (CW) Interim Accountable Officer Trevor Fernandes (TF) Board GP Member (Dacorum) Mike Edwards (ME) Board GP Member (Hertsmere) Clair Moring (CM) Board GP Member (Watford and Three Rivers) Rami Eliad (RE) Board GP Member (Watford and Three Rivers) Richard Pile (RP) Board GP Member (St Albans and Harpenden) Mike Walton (MW) Board GP Member (St Albans and Harpenden) Thida Win (TW) Secondary Care Specialist Doctor Tad Woroniecki (TWo) Deputy Chief Finance Officer Diane Curbishley (DC) Director of Nursing and Quality In attendance: Hein Scheffer (HS) Director of Workforce Brian Gunson (BG) Health watch representative David Evans (DE) Programme Director - Your Care, Your Future David Buckle (DB) - to B/14/17 Medical Director Charles Allan (CA) Director of Contracting and Resilience Trudi Mount (TM) - to B/14/17 Head of IM&T and Estates Juliet Rodgers (JR) Associate Director, Communications and Engagement Caroline Sutherland (CS) Patient Representative Rod While (RW) Head of Corporate Governance There were six members of the public in attendance.
B/01/17 Welcome and apologies 1.1 Apologies for non-attendance were received from Thelma Stober and Caroline Hall. It was
noted that TWo was attending on behalf of Caroline Hall.
B/02/17 Call for questions 1.2 NS requested any questions from members of the public in respect of the agenda items. A
member of the public stated that he had he had submitted a question in respect of the disinvestment paper. It was noted that the question had not been received but NS noted that this would be responded to in due course.
DRAFT
Item 03

2
B/03/17 Declarations of interest 3.1 NS requested declarations of interest in respect of the agenda items, other than had been
reported previously, none were received.
B/04/17 Minutes of previous meetings 4.1 The board approved the minutes of the meeting on 10 November 2016 subject to an
amendment: B/93.2/16 stated that there were two GP systems in use in Hertfordshire, when in fact there are three.
4.2 The board approved the minutes of the extraordinary meeting which took place on 24 November 2016.
B/05/17 Action log 5.1 • B/56.6/16 – localising out of hours performance data. It was noted that this action
had been outstanding for some time and RW will discuss with CH to ensure that HUCaddress the issue as soon as possible.
• B/81.5/16 – BAF system IM&T risk. As this was being discussed at the meeting as partof the local digital road map, it was agreed that the action would be closed but thatthe BAF risk would continue to be monitored by the board.
• It was agreed that B/94.4/16 (progress on pathways) and B/94.5/16 (healthinequalities in STP) should be closed.
B/06/17 Patient story 6.1 DC introduced WW, a patient who had had experience of the Dacorum Holistic Healthcare
Team (DHHT) and the nurse who had been closely involved in his care. 6.2 The following points were made
• WW had been referred to DHHT by the GP for support as he appeared to havedifficulties looking after himself and was depressed.
• WW suffers from Sturge-Weber syndrome, together with bipolar disorder, epilepsy,glaucoma and Attention Deficit Hyperactivity Disorder (ADHD).
• He was admitted to hospital in August 2015 following a severe seizure.• He has difficulty remembering hospital appointments.• He had very poor living conditions with no heating and poor sleeping and cooking
facilities.• He was accompanied by the team to Langley House for physiotherapy and this has
helped his mobility.• He is on an ophthalmology pathway for his glaucoma.• DHHT have supported WW with weekly visits and telephone support, the team has
also assisted him with a simple meal programme and basic cooking skills.• Food bank vouchers have been supplied for both WW and his father. A local charity
was contacted by the team and two double beds were supplied to improve sleepingconditions.
• DHHT has also liaised with the local council and a new gas central heating system hasbeen installed as a result.
• Help has also been given to WW in completing Personal Independence Payment (PIP)paperwork and he was awarded the higher rate which has helped pay for gas,electricity and food.
• WW feels safe with the DHHT service and receives good continuity of care throughcontact with the same people. He was pleased with the passion and care shown bythe team and this is superior to what he has received from other agencies.
6.3 The following points were made in discussion: • DHHT is picking up social care issues and patients that appear to fall between
different services. Solutions are often non-medical but prevent admissions to hospital.

3
• All referrals to the service come from GPs.• DHHT is an example of Your Care, Your Future with care being delivered in the
community near to people’s homes.• It was noted that this service is only available in Dacorum and was a result of the
investment of improving capacity in primary care money. There is some overlap withwork done by the rapid response teams in other localities but DHHT appears to offerbenefits above and beyond what is provided by the rapid response teams.
6.4 The board thanked WW and his nurse for sharing their experiences. 6.5 ACTION: AS to ensure DHHT is reviewed alongside the review of rapid response
B/07/17 Accountable Officers (AO) report 7.1 CW introduced the paper with the following points:
• The overnight closure of the Hemel Hempstead urgent care centre is until furthernotice and discussions on future provision of urgent care in the area are taking place. This may require public consultation in April.
• The contracting process was brought forward by three months and a great deal ofwork had taken place to agree contracts and complete the operational plan.
7.2 NS stated that Kathryn Magson, the current accountable office in Richmond CCG, was joining the organisation as chief executive on 3 April 2017.
7.3 The following points were made in discussion: • PS stated that with a potential move to delegated commissioning, it was important
that any risks and audits were also transitioned to the CCG via a full handover. CW stated that this was part of the arrangement and the CCG was in dialogue with NHS England on this.
• PS stated that the board should have approved the health and safety policy ratherthan the executive. CW stated that we need to be clear on which policies the board would wish to reserve for its approval as the executive approved a large number of policies.
7.4 The board noted the AO report. 7.5 ACTION: CW to propose which policies should be approved by the board.
B/08/17 Operational plan 2017-19 8.1 TWo introduced the paper with the following key points:
• The board had discussed the plan at the confidential meeting in December 2016.• The plan was submitted to NHS England on 23 December along with the activity and
finance plans.• The plan starts with the assumption that we are not in financial balance and that we
are likely to miss our control total in 2016-17.• The plan allows for 3% activity growth before QIPP, tariff inflation, re-establishment
of the 1% transformation reserve, ensuring that 0.5% is not committed at the start ofthe year, re-establishment of contingency reserve of 0.5%, delivery of parity ofesteem requirements for mental health and the £3 per head to support the GPforward view.
• Allocation growth in the next two years is below 2% so the next two years will bechallenging with a QIPP requirement of £38m in 2017-18, which is 5% of our totalallocation.
• £33m of QIPP is identified so far.• A new coding structure for tariff in 2017-18 is being introduced and the impact is in
excess of £3m for Herts Valleys CCG.8.2 The following points were made in discussion:
• PS stated that there needed to be granularity around how the plan was going to bedelivered.

4
• TF stated that there remained a challenge around local workforce. CW stated that thisneeded to come back to the board as it was an important issue.
• CW noted that the plan included a full list of priorities, commencing January 2017 toensure smooth transition into the new financial year.
8.3 The board approved the operational plan 2017-19 and priorities for 2017/18. 8.4 ACTION: CW to discuss with HS a workforce report which will come back to the board.
B/09/17 STP / Your Care Your Future update 9.1 DE introduced the paper with the following points:
• Presented was the STP’s initial public document. The next stage is to finalisemobilisation plans.
• Further work is required on the governance associated with developing andsupporting the plan.
• The plan is being presented to the board for discussion and approval.• Your Care, Your Future is a significant part of the plan.
9.2 The following points were made in discussion: • There is a risk around specialist commissioning due to the fact that there is no
commissioning infrastructure within the STP. • CS stated that from the public point of view, this was an achievable and realistic plan.• There are further discussions with the public regarding Your Care, Your Future
organised over the next two months.9.3 The board approved the STP plan.
B/10/17 Local digital road map 10.1 TM made the following points in introducing the paper:
• This represents the digital strategy for the STP to support the transformationrequired.
• The senior responsible officer is Katie Fisher, CEO of West Herts Hospitals Trust(WHHT).
• There is an STP wide digital integrated care programme board which will be ensuringthat the strategy is implemented.
• The plan features four “big ticket” items:o Interoperabilityo Collaborative working environmento Joint business intelligenceo Urgent care dashboard.
• The plan acknowledges the importance of information governance in order to protectconfidentialities.
10.2 The following points were made by the board in discussion: • SB queried the lack of costs included in the plan. TM stated that this was because the
document was public facing. • PS noted that this was a direction of travel and spend on individual projects would
need to be approved in due course. • PS suggested that there needed to be a much greater emphasis on cyber security.• NS noted an on-going risk around the IT infrastructure of WHHT.
10.3 The board approved the local digital roadmap. 10.4 ACTION: TM to ensure that the risk of cyber security is addressed in the information
governance workstream. 10.5 ACTION: CW to address cyber security as a key corporate risk.
B/11/17 Operational planning guidance for GP forward view 11.1 DB introduced the paper with the following points
• The GP forward view (GPFV) was launched by NHS England in the spring as a new

5
approach to commissioning general practice, with a focus on funding and access. • A draft plan has already been submitted as part of the operational plan and a further
submission will be made in February.• There is big focus on online access to repeat prescriptions and appointments for
which there is great variance between practices.• A final decision has not been made by the CCG regarding the increased funding for
primary care via the £3 per head directive from NHS England.11.2 The following points were made in discussion:
• PS stated that the national audit office has published a review of attempts to improveGP access.
• It was recognised that there was an issue with recruitment of GPs that we would needto address.
• TF noted that in the current financial position there was a risk that the CCG would findit difficult to fund general practice to the extent required by the GPFV.
• CW stated that we needed to think about prioritisation of funds and that if we coulddemonstrate a better return on investment then general practice would receiveinvestment.
• PS stated that the GPs on the board clearly had interests in the discussion aboutfuture funding and we need to ensure that those interests are flagged prior to themeeting. NS agreed and that we should address this at future meetings.
11.3 The board noted the operational planning guidance for GP forward view.
B/12/17 Integrated Quality, Finance and Performance Report (IQFPR) 12.1 SB introduced the report with an overview of discussions that had taken place at the quality
and performance committee meeting on 5 January: • The board was asked to note that there was a detailed finance report to accompany
the full performance report in view of the current financial position of the CCG.• The financial element of the report is based on month 7. There is a likely deficit of
£8m which has been agreed with NHS England, but this is a challenge and theinvestment committee has been reviewing plans for 2017-18 and not the currentyear.
• Our QIPP target for 2017-18 is £38m and we will need to add to this target to ensurethat there is sufficient head room. This should be an additional 15%.
• WHHT have received feedback from the CQC and we await an update on this.• Herts Urgent Care is not delivering on some of the KPIs, with some deterioration over
the past two months. This needs to be addressed.• Issues with Royal Free 62 day cancer waits are being looked at in detail.
12.2 The following points were made in discussion: • CW stated that we expect to deliver a plan to achieve £38m within the next week;
£33m has currently been planned. Further schemes will be identified in phase 2 toachieve £45m.
• CW stated that two meetings have been held with the regional director who has beenencouraged by progress being made. Further savings are being sought for 2016-17.
• NS observed tireless energy amongst members of staff in developing plans to addressfinancial recovery at pace.
• PS considered that the report was too long which makes it difficult for the board tounderstand the key issues. He suggested there should be more gatekeeping in termsof what comes to board as the detail should be addressed at other meetings.
• CW suggested that we needed to get the balance right around board reporting andwhat needs to be in the public domain. We need to publish a detailed financial reportcurrently as we are in financial turnaround.
12.3 The board noted the Integrated Quality, Finance and Performance Report (IQFPR).

6
B/13/17 Medical director’s report 13.1 DB introduced the paper with the following points:
• He reminded GP prescribers that co-proxamol was no longer licensed and cost over£200 per pack. Whilst the number of prescriptions were few, this was not acceptable.
• He also requested board support to increase generic prescribing. 85% of prescriptionsare currently generic, so there is scope for improvement and there is savings potential of £260k per year.
13.2 The following points were made in discussion: • There are difficulties as patients sometimes insist on the branded form and are
concerned when the appearance of their medication changes. RP requested a directive from the CCG that GPs must prescribe generically.
• RE felt that we need to have an honest discussion with our patients.• PS stated that in this issue all GPs were conflicted and a declaration on this should
have been made on receipt of the papers. NS stated that this would need to beresolved outside of the meeting.
• PS again highlighted potential conflicts of interest13.3 The board noted the medical director’s report and that the discussion on generic prescribing
would be held at commissioning executive. 13.4 ACTION: NS/RW to address the issue of declaration of conflicts of interest.
B/14/17 Communications and engagement report 14.1 JR introduced the paper with the following key points:
• Events are taking place in each of the four localities to update people on Your Care,Your Future and hospital options and consider options on configuration of community services.
• We have experienced increased media activity over the last few weeks with coverageof the CCG’s withdrawal of discretionary adult social care funding and the temporary overnight closure of the urgent care centre at Hemel Hempstead.
14.2 The board noted the communications and engagement report.
B/15/17 Board Assurance Framework (BAF) 15.1 RW introduced the paper with the following points
• The BAF summary represents the position at the end of quarter 3.• We have recently received the outcome of an internal audit on risk management
which gave us a green amber rating – meaning the board can take reasonableassurance that effective processes are in place. The auditors stated that they hadseen evidence of best practice and RW recognised the key role played by riskmanager Katy Patrick and that her hard work had contributed greatly to this.
15.2 The following points were made in discussion: • NS stated that in the light of our changed financial situation we needed to critically
review our processes and how this particular BAF risk had been managed. • PS congratulated the team on the positive audit.• CA also recognised the inputs that had been provided to teams across the
organisation in driving improvements in our management of risk.15.3 The board noted the Board Assurance Framework.
B/16/17 Annual sustainability report and plan 16.1 CW introduced the report and plan with the following key points:
• This is part of an annual process to identify further improvements in sustainability.• It is important to note that the sustainability targets have remained the same, despite
the fact that the number of staff has increased. However we have managed toreduced our emissions despite this.
• The plan requires approval from the board.

7
16.2 The board approved the annual sustainability report and plan.
B/17/17 Investment committee report 17.1 PS introduced the report with the following points:
• The committee has been meeting fortnightly since 1 December 2016.• There have been some very productive meetings at which some very difficult
decisions had been considered. Both investments and disinvestments have beenapproved.
• The management team is to be commended for the speed with which materials havebeen development for the committee’s attention.
• The committee should be something that becomes part of core business of the CCG.17.2 The following points were made in discussion:
• We need to ensure that decisions are communicated in good time to relevant groups.• CW pointed out the flow chart which was now being followed.• Communications messages are being agreed with JR and messages will be
communicated in a timely way.• TF stated that GPs needed to be informed regarding any referrals that needed to be
curtailed.17.3 The board noted the investment committee report. 17.4 ACTION: Tracker spread sheet to be developed – RW
B/18/17 Committee chairs’ reports 18.1 AG noted on the PPI committee that the committee is looking to broaden the pool of
incoming patients to the PPI committee.
B/19/17 Additional risks identified in the meeting 19.1 It was agreed the risks around cyber security required a more rigorous review.
B/20/17 Next Board meeting 20.1 The next board meeting will take place on 9 March at 13.30, venue to be confirmed

SPACER PAGE

SPACER PAGE

Action Log Date of Meeting Subject Action Responsible
Officer
Due Date Comments Status
B/56.6/16 09.06.16 IQFPR
BI and Performance team to investigate the possibility of localising
performance data on out of hours.BI and Performance team to investigate the
possibility of localising performance data on out of hours.
C Hall 08.09.16 We have been advised by ENHCCG that go-live for patient level data is 29th June Open
B/07.5/17 12.01.17 Organisational Policies Establish which policies should be reserved for Board approvalC Ward
R While28.02.17
It is proposed that these should be Equality and Diversity Strategy and Health and Safety
polocyOpen
B/08.4/17 12.01.17 Workforce report Workforce report to be submitted for future Board meetingC Ward
H Scheffer09.03.17 Report submitted to Q&P 2 March and planned for Board in May 2017 Open
B/10.4/17 12.01.17 Cyber security riskEnsure that the risk of cyber security is addressed in the information
governance workstream.T Mount 09.03.17
IG Workstream asked to ensure this is included in programme. This will be monitored
at regular Local Digital Roadmap Board MeetingsOpen
B/10.5/17 12.01.17 Cyber security risk Address cyber security as a key corporate risk. C Ward 09.03.17 Open
B/13.4/17 12.01.17
Conflicts of interest Address the issue of declarations of conflicts of interest. R While 09.03.17 A link to declarations of interests registers has been added to the board agenda.
It is proposed that a standard statement be added to future minutes of board meetings
to the effect that "as board GPs are practicing local GPs a it is recognised that
discussions arise in which they may have a conflict and this would be declared at that
time".
Completed
B/17.4/17 12.01.17 Investment committee Tracker to be developed and shared R While 31.01.17 Complete Completed
Herts Valleys CCG Board Action Log
Item 04

SPACER PAGE

SPACER PAGE

Page 1 of 13
NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Accountable Officer’s report Agenda Item: 5
Purpose (tick one only) Decision or Approval ☐ Discussion ☒ Information ☐ Note ☐
Responsible Director(s) and Job Title
Cameron Ward Interim Accountable Officer
Author and Job Title Cameron Ward Interim Accountable Officer
Short Summary of Paper This paper provides an update for the Board on recent CCG developments
Recommendation(s) The Board is being asked to: - note and discuss the report
Engagement with Stakeholders/Patient/Public
N/A
Links to Strategic Objectives (tick all that apply)
Objective 1: We will continually improve engagement with patients, carers, the public and member practices so that they contribute to and influence our work and activities.
☒
Objective 2: We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to stay well and avoid ill health.
☒
Objective 3: We will work with health and social care partners to transform the delivery of care through the implementation of Your Care, Your Future, the strategic review in west Hertfordshire.
☒
Objective 4: We will ensure that there is a financially sustainable and affordable healthcare system in West Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR) What current risks does this report align to?
This report relates to all the strategic objectives of the Board
Risks What risks have been identified as a result of this report?
No further risks identified
Resource Implications None
Equality Impact Analysis N/A
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☐
Improved Patient Access and Experience ☐
A Representative and Supported Workforce
☐
Inclusive Leadership ☐

Page 2 of 13
Report History Which Groups or Committees have seen this report and when?
This is a regular report to Public Board meetings
Appendices NHS England assurance letter 24.02.17

Page 3 of 13
1.1 Your Care, Your Future
Significant progress has been made in developing the strategic outline case (SOC) for acute and
planned care configuration in west Hertfordshire. The SOC was presented to WHHT board on 2
February and was approved to go to outline business case (OBC) stage. As part of the NHS
Improvement and NHS England approval guidance the CCG and STP are required to sign a letter of
support for the SOC.
In order for HVCCG and STP to be in a position to support the Strategic Outline Case and write its
letter of support to the progress to outline business case stage we need to be assured in the
following areas:
The proposal in the SOC is in line with our Your Care, Your Future strategy
Activity assumptions are in line with our commissioning intentions (agreed clinical models and
activity assumptions)
Affordability from the commissioner perspective
Compliance with the reconfiguration guidance
The CCG has reviewed the document and written to WHHT with a series of queries that provide check
and challenge to the document and assumptions made within it. We have received responses from
WHHT that provide a some level of assurance but further clarity is required so that the CCG and STP
can be confident in signing up to a plan that is affordable to the system and deliver the best possible
outcomes required for patients long into the future. This focusses particularly on points 2 and 3
above.
Continued work will take place over the coming months to ensure that all plans outlined in the SOC
are affordable and deliverable within the current and future financial climate. Once the CCG is
confident that all the requirements are in place it will bring the final SOC to the Board for approval.
1.2 Your Care, Your Future Locality events
The Your Care, Your Future team has held information and engagement events in three of the four
localities in recent weeks. The events, which have been well attended, have focused on updating
people about plans to deliver more services in the community and shift provision away from hospitals
and gathering views on local needs.
Each of the events has been locally tailored with lead GPs updating on developments in their areas.
We have also been joined by other Your Care, Your Future partners. WHHT has updated on hospital
redevelopment plans and Hertfordshire Community Trust joined us at the St Albans and Harpenden
event to talk about proposals around community beds and the development of the health hub on the
Harpenden Memorial site. Public health colleagues have provided an analysis of local health needs
1. System leadership

Page 4 of 13
which differ between the localities. The health needs will be summarised into locality based
commissioning plans which will be coming to the May board meeting.
A date for the final event in Hertsmere has yet to be confirmed.
This engagement will be followed up by more focused discussions that will drill down to consider
future service provision at a very local level.
1.3 Implementation of pathways under Your Care, Your Future
Diabetes - the CCG has launched the multi-provider pathway collaborative process for an integrated
acute and community diabetes service. Good progress is being made by the providers in response to
the commissioning framework and specification with a launch of the new service from 1 October
2017.
Older People - commissioning a framework for older people is one of the high priority areas identified
under YCYF. The CCG has recently conducted an external review of the rapid response services across
three localities and the interdependencies of this service with the core community nursing and
therapy services. Following clinical discussion at Commissioning Executive, the Integrated Planned
and Primary Care Programme Board are tasked to develop a commissioning framework for older
people at locality level with general practice at the heart of this model as outlined in the YCYF models
of care. The core principles will be the same for each locality, including delivery of the framework via
the multi-provider pathway collaborative with the GP federations very much at the heart of it with
the other providers wrapped around it. It is proposed for this model to be agreed at each locality by
April 2017.
End of life care - good progress has been made on the delivery of the aspects of the revised end of
life care strategy, approved in November 2016.
From 3 April 2017 there will be a single referral centre for all referrals to palliative care for patients
who are registered with a GP, within the HVCCG. This is a collaborative approach with our current
providers for palliative care including Rennie Grove Hospice Care, The Hospice of St Francis, Peace
Hospice Care or Hertfordshire Community NHS Trust.
The West Hertfordshire Palliative Care Referral Centre will support the delivery of national priorities
and the outcomes of the Herts Valleys CCG palliative care and end of life care strategy for adults and
children 2016-21.
The service will promote and utilise the electronic palliative care co-ordination system (EPaCCS)
which was launched earlier this year to ensure all end of life patients are registered on the system
therefore enabling healthcare professionals to have access to a patient’s details and preferences at
the end of their life.
The palliative care referral centre will be based at Peace Hospice and will provide:
A single point of referral and triage for all palliative and end of life referrals
A single point of access via a central telephone number and email address

Page 5 of 13
Management of the electronic palliative care co-ordination system (EPaCCS)
An advice line to healthcare professionals and clinicians
An advice line for patients and carers (Year 2)
All referrals will be considered and managed by the referral centre multi-disciplinary team which
will be based at Peace Hospice Care in Watford. This team will consist of staff from The Hospice of
St Francis, Peace Hospice Care, Rennie Grove Hospice Care and Hertfordshire Community NHS
Trust. The aim of the Referral Centre is to rapidly respond with the appropriate Palliative Care
service regardless of where in the HVCCG the patient lives and to make this process much simpler,
easier and faster for all referrers.
1.4 West Hertfordshire Hospitals NHS Trust (WHHT) – revised CQC rating
It is really pleasing to see that, following a recent inspection, WHHT’s CQC rating has moved from
‘inadequate’ to ‘requires improvement’. The trust has seen a big increase in the number of individual
services graded as ‘good’ and a similarly significant drop in the number rated ‘inadequate’.
We are delighted to see such considerable improvement in our major acute trust; this is something
that will be making a real difference to local people. The trust does remain in special measures and
the reduced rating for the Hemel Hempstead site (as a result of care on Simpson ward), together with
the continued grading of the emergency department as inadequate are, of course, disappointing.
However colleagues at WHHT know what it is that they need to do to build on the considerable
achievements in order to make further improvements for the benefit of people living in west
Hertfordshire. We at Herts Valleys CCG will continue to work hard to support them in this.
1.5 Commissioning Executive:
Key areas of discussion and decisions made since the 12 January Board meeting
There have been 2 meetings of the Commissioning Executive since the last Accountable Officer (AO)
report was written. Below is a summary of key decisions and areas of discussion:
The Commissioning Executive agreed to support the move to generic prescribing subject to theproduction of a clear statement and exception process.
Approved the guidance on crushing tablets or opening capsules in a care home setting subjectto the production of a simple flow chart.
Ratified the recommendations of Herts Medicines Management Committee on treatments thatwere not subject to NICE Guidance.
Review of rapid response service
Quality premium 2017-18
Approved recommendation to the CCG of preferred bidder for wheelchair service

Page 6 of 13
1.6 Board private and development sessions
The following were the key areas of focus for Board development sessions held on 26 January and 23
February:
• Workshop facilitated by Nigel Edwards, CEO of the Nuffield Trust• Review of NHS staff survey• Review of internal CCG governance survey• Discretionary payments to Herts County Council• Draft GP practice estates plan
1.7 NHS England assurance
Our quarterly assurance meeting with NHS England (NHSE) took place on Friday 13 January 2017.
The meeting covered mental health, national performance standards, the STP and the CCG’s financial
position. A copy of our assurance letter issued on 24 February is attached as Appendix 1.
1.8 Update on delegated commissioning
The Board ratified member practices vote in favour of a move to full delegated commissioning
arrangements from 1 April 2017. This is to take delegated responsibility for commissioning primary
medical services (GP contracts) from NHS England.
The CCG’s formal application was supported by the NHS England (NHSE) (Central Midlands), Director
of Commissioning Operations prior to being submitted to NHS England centrally. The national
timescale for CCGS to be notified of the outcome of their applications was mid-January. This changed
to mid-February. On 14 February the CCG received formal confirmation from Paul Bauman, Chief
Financial Officer at NHS England that our application has been successful and the CCG can move to
delegated commissioning arrangements from 1 April 2017. This is subject to the CCG submitting a
completed Delegation Agreement with NHS England. David Buckle’s team are in the process of
preparing the delegation agreement with the NHSE (Central Midlands) area team ready for
submission in advance of the 8 March timescale.
There are weekly meetings in place with NHS England (Central Midlands) to ensure a smooth transfer
of commissioning arrangements to the CCG. It should be noted that NHSE remain statutorily
responsible for commissioning of primary medical services and the CCG will have to assure NHSE
through our assurance process that the CCG is effectively carrying out NHSE’s statutory functions.
This is good news for the CCG; it will enable us to continue to build on the good work with we are
doing with our GP clinical leads and member GP practices. We believe it is a key enabler for
progressing the CCGs clinical strategy Your Care, Your Future. It will assist with making local
commissioning decisions with all our contractors which we believe we are best placed to do; and to
do in a timely and responsive way. Being in delegated arrangements will assist in the delivery of the
GP Forward View for our practices and will support collaborative working with our neighbouring
CCGs. In our Hertfordshire and West Essex Sustainability and Transformation Plan footprint. East &
North Herts CCG chose to remain in joint commissioning arrangements and West Essex have also
received formal confirmation their application for delegated commissioning has been approved.

Page 7 of 13
Our member practices have been informed and stakeholders will be advised of the change in
commissioning arrangements. The terms of reference of the Joint Primary Medical Care Committee
(formerly Joint Commissioning Committee) will need to be revised and they will come to the next
Board meeting.
The Board will be kept updated and informed of our progress and delivery of our delegated
commissioning functions.
The CCG will receive the published allocation for general practice services, plus the 0.5% contingency.
The budget for 2016/17 is circa £71.1 million. The published budget confirmed by NHSE (Central
Midlands) for 2017/18 is £74,579 million (with 5.44% growth) and £77,325 million in 2018/19.
Individual GP practice income will continue to be paid by NHSE (Central Midlands) via the current
national arrangements through Capita. There is no risk that GP practices will not receive their
practice income from April 2017.
GP contract – General Medical Services (GMS) contracts are nationally negotiated each year between
the Department of Health, NHS England and General Practitioners Committee (GPC) and this will
continue to be the case. The negotiations for 2017/18 are currently taking place and the final
outcomes will be published by the NHS Confederation. The role of the CCG will be to implement the
nationally negotiated changes to the GMS contract, this includes contractual payments. The CCG will
be required to assure NHSE this has taken place.
The CCG will take over responsibility for the premises cost directions ie GP practices premises rent
reimbursements, premises and planning for new premises provision.
1.9 GP Federations
All four localities in west Hertfordshire have a GP federation covering their individual patient
populations with the majority of member practices being shareholders. These four existing GP
Federations (Dacorum, Herts Health, St Albans and Harpenden GP Federation and Direct Local
Health) have been working together to develop themselves into competent primary care providers
and are now in a position where they are about to formalise that relationship into one overarching
legal organisation covering all 68 practices and registered as HertsOne GP Federation. This
organisation is now registered with Companies House and is just in the process of completing its legal
requirements.
The establishment of HertsOne, will allow for more standardisation of primary care services and
outputs across the localities, more efficient use of resources with collaborations between the four
federations and is an attractive vehicle for NHS commissioners and member shareholders alike.
HertsOne as the overarching federation is now represented at the most senior transformation,
strategy and estates meetings alongside the other major local providers namely West Hertfordshire
Hospital NHS Trust (WHHT), Hertfordshire Partnership Foundation Trust (HPFT), Hertfordshire
Community Trust (HCT) and West Hertfordshire Adult Services, to complete the multi provider
collaborative vehicle for future commissioning of sustainable services across west Hertfordshire.

Page 8 of 13
2. Operational issues
The CCG has agreed to support a two year development plan for the establishment of HertsOne and
the continued development of the four locality federations given they are integral to the ability of the
CCG to implement Your Care, Your Future, Healthier Future, the Five Year Forward View, the GP
Forward View and deliver on its core access and quality standards for patients.
2.1 Nursing and quality - safeguarding
NHSE (Midlands and East) region required HVCCG to provide assurance around safeguarding
arrangements through up loading evidence to an electronic Safeguarding Assurance Tool (SAT). The
pilot was completed with evaluation through feedback/survey given to the NHSE team. Further plans
include development of the electronic tool for providers and GP practices.
A review of the section 11 tool was carried out to simplify, provide prompts, and align measurement
with CQC and Safeguarding Assurance Tool. The tool is used at the annual s11 visit to support
provider organisations to give assurance to the CCG on their safeguarding arrangements.
A number of workstreams led by members of the designated team are in development including:
FGM multi-agency pathway led by deputy designated nurse, in collaboration with a social
worker from Barnardos
Supervision task and finish group to review supervision across the partnership, following a
recommendation from a serious case review
Honour based violence/forced marriage policy
Discharge from Tier 4 mental health
Discharge of looked after children/care leavers with mental health team support from
emergency departments.
Primary care safeguarding children named GP vacancies are successfully recruited to across
Hertfordshire. The named GPs are supported by the specialist nurse within the Clinical
Commissioning Group’s safeguarding team.
NHSE funded level 3 safeguarding children training has been delivered to primary health practitioners
across Hertfordshire. These well attended conferences have incorporated current topics including
female genital mutilation (FGM), honour based violence, forced marriage and PREVENT.
Workshops have been offered to all practice nurses across Hertfordshire to support the recognition
and mandatory reporting of FGM.
The nurse specialist is working to support information sharing between primary care and
Hertfordshire Channel Panel which will be underpinned by a multi-agency channel information
sharing agreement and template created to support GPs to provide relevant information.
The deputy designated nurse for Looked after Children and Care Leavers (LAC & CL) has worked with
the Children in Care Council (CHICC) and CL health focus group on a podcast and comic strip

Page 9 of 13
explaining initial health assessment (IHA) to LAC/young people. She continues to increase
collaboration between health and children’s services through attendance at the risk management
panel to improve outcomes for Looked after Children and Care Leavers.
Further developments include four LAC GPs trained to undertake IHAs. Health Passports ‘My Care
Journey’ have been finalised and are due to be distributed to all Hertfordshire LAC and Care Leavers.
A specialist nurse is in post within HPFT to focus on transition of vulnerable children / young people
to adult services. Out of area delays in health assessments are being addressed by the LAC health
team delivering a 25 mile radius service to complete review health assessments (RHAs)
Further focussed work is required on systems and processes for information sharing between
secondary and primary care to ensure vulnerable families are supported.
A recent scope of all Hertfordshire GP practices revealed that not all were registered with nhs.digital
to submit data to the national dataset should FGM be disclosed or identified. Mandatory reporting
responsibilities require all GPs to provide data nationally so that consistent information on those
women and girls who have had FGM is recorded and to inform the commissioning of services
required. Support to increase these figures is being provided by named GPs for safeguarding children
and nurse specialists within the CCGs.
Dental checks for LAC are low compared to national benchmarking. Further scoping with
Hertfordshire Children’s Services colleagues is required to identify children with low compliance to
enable a targeted approach to improve compliance.
Hertfordshire Children’s Services colleagues continue to provide follow up to all teams/managers to
increase completion and return of the strength and difficulty questionnaires for LAC.
Phil Picton has stepped down from his role as Hertfordshire Safeguarding Children Board chair and a
newly appointed chair, Nicky Pace, has now commenced in post. Nicky comes to Hertfordshire with a
wealth of experience and has driven innovative practice in varying London boroughs.
2.2 Social prescribing(SP)
HVCCG hosted the first ever regional Social Prescribing Conference on Tuesday 7 February at
Shendish Manor, on behalf of NHSE and the National Social Prescribing Network. Over a hundred
delegates came from the whole of East Anglia, Essex, Bedfordshire, Luton and as far afield as
Northamptonshire, Swindon and Milton Keynes. They represented CCGs, local authorities, public
health, community pharmacy, the voluntary sector, GPs and SP projects themselves. Dr Michael
Dixon, the national NHSE SP Champion was the keynote speaker and Drs Nicolas Small and Marie-
Anne Essam both spoke about their positive experiences of using the Herts Valleys community
navigator scheme while Paul O’Hare, its manager, described how the project works and was
commissioned. The conference was very well received and work continues now with the
development of an East of England regional SP network (with funding from NHSE) and STP work to
develop the agenda further (Tim Anfilogoff for details). For presentations and notes of the
conference go to www.hertsvalleysccg.nhs.uk/socialprescribing. Tim continues to support the social
prescribing work at STP level and nationally through the national social prescribing network. Michael
Dixon’s email (noted below) demonstrated that Herts Valleys is leading this work.

Page 10 of 13
“Dear Tim
A big thank you and many congratulations on such a successful event in Hertfordshire yesterday. I
thought you had an audience (and a large one) of exactly the right mix and clearly all were animated
and keen to progress.
With your leadership skills, I see the East of England being a model of how regional leadership of
social prescription might progress. You have clearly got some real talents there – particularly Anne-
Marie and Nicholas. I was fascinated too to see that you have a representative from NHS England as
an SP lead for the East of England.
I think the future will be creative friction between what local SP and regional SP are doing, achieving,
thinking and driving and what nationally is being done by DH/NHS England and by the National
Prescribing Network. You expressed well that confluence between top and bottom and it will be
some achievement if we managed to make this a creative relationship rather than, as too often in the
past, an oppressive one!
I thought you had an excellent choice of speakers and enjoyed sharing the taxi and train home with
Neil Cleeveley.
I think we have some exciting times ahead and bless you for being such an effective leader.
With best wishes
Michael”
Dr Michael Dixon LVO, OBE, FRCGP, FRCC
Chair of Council, College of Medicine
2.3 Community navigator scheme
Community navigator scheme is still receiving many referrals. It has also supported the establishment
of a volunteer led social prescribing/low level community navigation project in the Maltings Surgery
in St Albans in partnership with the Maltings PPG and St Albans CVS.
The Frequent Attenders community navigator has left her position to take up a full time role with
Watford Community Housing Trust and we will be recruiting for a replacement for this position
(hosted by Watford Community Housing Trust) in the coming weeks. This will be a profiled
community navigator role and will not solely be looking at frequent attenders.
The community navigator scheme has been short listed for a Hertfordshire High Sheriff Award and
the outcome will be known on 16 March.
2.4 Continuous improvement
Following the all staff event in October 2016, Herts Valleys CCG has twelve continuous improvement
trained champions who are leading on a number of projects across the organisation. All projects go
through a rigid process of establishing measures, metrics and timelines against which targets and
outcomes are defined. The overall key objective of this programme is through cross team working to
generate efficiencies which when applied save both time and money. Projects include:

Page 11 of 13
The reviewing of payment processes within localities
The induction programme for new members of the Continuing Health Care team
Establishing quick wins for the operation restart project
Supporting Watford Workshop in reviewing their workforce documentation
The champions will provide quarterly updates to the Executive team and Board on the progress and
outcomes of their projects, with first update due in May 2017.
2.5 Staff health and wellbeing
Throughout February, over 70 members of staff took part in a team challenge by doing a virtual
walking/step challenge along route from Lands’ End to John O’Groats and for March the focus will be
to raise staff awareness on some of the months national health campaigns; including ovarian and
prostate cancer and the dangers of consuming too much salt.
2.6 Child and adolescent mental health services (CAMHS )
Seven innovative projects to boost the emotional health and wellbeing of children and young people
in Hertfordshire have been awarded funding from the Innovation Fund, set up as part of the
transformation of mental health services for children and young people in Hertfordshire.
The different early help schemes, including counselling for lesbian, gay, bisexual, transexual and
young people, joint parent-child therapy and coaching, counselling and cognitive behavioural therapy
for teenage boys at Dacorum’s education support centre, will be kicking off in coming weeks to test
new approaches and learn what really makes a difference. Young people helped decide which bids
should be funded, with schools, youth and community groups, charities, NHS and council
organisations among the 88 applicants.
Demand for Kooth.com, the online counselling website commissioned as early intervention for
Hertfordshire 10 to 25-year-olds last year, continues to grow, with more than 2,250 children and
young people registered by the end of December 2016. Feedback from young people and
professionals like GPs and school staff remains very positive.
Our work to give children and young people better emotional wellbeing health help by improving
links between schools and NHS mental health services was showcased at a national learning event.
The county’s two CAMHS schools link managers spoke at NHS England’s National Children and Young
People’s Mental Health services and schools link pilot learning event in London on Thursday 9
February. Around 100 delegates from across the country, including commissioners and education
staff, were at the London session to hear the headlines from the national pilot evaluation and join
workshops from a selection of pilot sites.
The new Community Perinatal Mental Health Team will be officially launched in April. The HPFT
team’s induction days run from March 14-17 but they have already started working with families.
Online information and leaflets for families and professionals, including pathways for GPS, are being
finalised.

Page 12 of 13
3. HR and organisational development and learning update
The refreshed CAMHS Transformation plan, Healthy Young Minds in Herts 2015-20 is online here and
the signposting website, www.healthyyoungmindsinherts.org.uk is being finalised, including a parent
carer survey here.
3.1 Chief Executive appointment update
The new Chief Executive for Herts Valleys CCG, Kathryn Magson will now commence in post on 16
March 2017, taking over from Cameron Ward.
3.2 Bedding down of HR and ODL shared service
Louise Thomas has been appointed as Assistant Director of HR and ODL and commenced in post on 3
January 2017. All vacancies are currently being appointed to. Work to embed consistent,
streamlined processes will commence in the spring and will form a specific project as part of the
CCG’s continuous improvement programme.
3.2 HR and ODL policy review update
A review of all HR and ODL policies is underway to ensure all policies are up to date, consistent and
compliant with all relevant legislation, statutory regulations, best practice guidance and NHS
directives. The updated policies will be launched by 1 April 2017 and will be complemented by a
suite of HR master classes which will launch by 1 May 2017.
3.4 HR and ODL forward plan
The HR and ODL forward plan has been developed and agreed. The plan will guide the work of the HR
and ODL team over the next year to ensure that the CCG is supported in achieving its strategic
objectives through the workforce.
3.5 Notice period consultation
A review of notice periods for staff took place with the aim to bring the CCG in line with other NHS
organisations and to ensure best practice. Following consultation, the new notice periods took effect
from 1 January 2017 and all staff have been informed.
3.6 Annual staff survey
The full results of the staff survey are now available to the CCG, albeit that they are still under
embargo until 7 March 2017. The headline results have been shared with the senior leadership team
and Board and also with the staff involvement group (SIG) on 28 February 2017. Full reports and
action plans will be devised and shared in due course.
3.7 Appraisals
The appraisal policy and paperwork has been revised as a result of feedback from the staff survey.
This is currently being agreed with SIG and will be launched later this month.

Page 13 of 13
3.8 Employee exit survey
A new online exit survey has been designed to help increase response rates and better inform the
CCG of the reasons that staff leave so that we can devise appropriate retention plans on a real time
basis. The proposals are in discussion with SIG at present.
3.9 Management graduate trainee scheme (MGT scheme)
The NHS Leadership Academy continue to host the MGT Scheme and an expression of interest has
been submitted on behalf of the CCG. The scheme will help ensure that each participant has the
best possible opportunities for a high quality learning experience with support during, and after, their
time on the Scheme. In turn, this will help the Academy ensure it is providing the NHS with high
quality leadership talent both now and in the future.
3.10 Pensions automatic enrolment
Preparations are underway in advance of the CCG’s staging date of 1 July 2017 to implement the
automatic enrolment of all staff to an appropriate pension scheme.
Terms/acronyms used in report
HVCCG Herts Valleys Clinical Commissioning Group
STP Sustainability and Transformation Plan
YCYF Your Care, Your Future
ENHCCG East & North Herts Clinical Commissioning Group
HR and ODL Human Resources and Organisational Development and Learning
LAC Looked After Children
CL Care Leavers
IHA Initial Health Assessment
CHICC Children in Care Council
FGM Female Genital Mutilation
RHA Review Health Assessment
SIG Staff Involvement Group
MGT Management Graduate Trainee



SPACER PAGE

SPACER PAGE

NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Financial Plan - Revised Agenda Item: 6
Purpose* (tick) Decision ☐ Approval ☒ Discussion ☐ Information ☐
Responsible Director(s) and Job Title
Caroline Hall, Chief Finance Officer
Author and Job Title Caroline Hall, Chief Finance Officer
Short Summary of Paper At its meeting in January 2017 the Board approved the CCG’s operational plan for 2017/18 to 2018/19. Included within this was the CCG’s financial plan for the same period. There has been a further iteration of the financial plan which was submitted to NHS England on 27 February 2017. This paper sets out the revised financial plan, the key assumptions made in its development and the risks to delivery.
Recommendation(s) The Board is being asked to: Approve the 2017/18 to 2018/19 revised financial plan.
Engagement with Stakeholders/Patient/Public
The financial plans include the financial impacts of strategic and operational strategies that have been discussed with stakeholders.
Links to Strategic Objectives (tick all that apply)
Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☐
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
List all relevant risk titles from the BAF and the CRR, together with reference number
BAF 2.2 Risk that we are unable to ensure high quality, safe and sustainable services for the population and patients of west Hertfordshire. 4.1 Risk that we do not deliver a financially sustainable health and social care system. 4.2 Risk that we do not deliver best value from the total CCG budget. 4.3 Risk that we do not achieve financial balance for 2016/17.
CRR SO4/03 - Risk that QIPP savings are not achieved as planned as a result of over-estimation of benefits and optimistic delivery timetables resulting in a threat to CCG of not achieving year-end balance. S04/22 - Risk that there are higher levels of hospital activity than planned/anticipated.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Fully addressed above
Resource Implications The resource implications are as set out in the paper.

Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☒
Improved Patient Access and Experience ☒
A Representative and Supported Workforce ☒
Inclusive Leadership ☒
Report History Which Groups or Committees have seen this report and when?
None previously
Appendices
*Purpose – definitions
For decision
This is where the board, committee or group is presented with a range of options and is asked to
decide which one to accept following discussion.
For approval
A specific recommendation, plan or document is presented, which the board, committee or group is
requested to approve. Discussion is not essential.
For information
Information is provided and it is important that the board, committee or group is aware of, and
understands the information and no decision is required. These items do not require discussion,
except for questions of clarification.
For discussion
The board, committee or group is asked to debate an issue, provide views, challenge and discuss as
appropriate. A decision may be made following the discussion although this is not always required.
An example is a progress report on a particular pathway. In this case the Board or Committee will be
asked to discuss and note the paper.

1
Herts Valleys CCG Financial Plan 2017/17 – 2018/19
Introduction
The CCG’s first financial plan for 2017 to 2019 was submitted to NHSE on 23 December 2016 and was presented to the January 2017 Board as part of the operation plan. Since then a further iteration of the financial plan has been developed and was submitted to NHSE on 27 February 2017. The key changes to the latest plan are that the starting point was updated to include the CCG’s forecast outturn at month 10 (previously month 8) and QIPP schemes have been further developed. The plan has also been amended to reflect contracts signed with providers.
As yet, we have not been asked to incorporate funds relating to the delegated commissioning of Primary Care.
This report sets out the key elements of the latest financial plan and describes the risks to delivery together with the mitigations currently in place.
Allocations
HVCCG receives an annual allocation from NHS England which it uses to commission services to meet the health and wellbeing needs for our population.
The following table shows how the CCG’s allocation grows over the next 2 years:
£'000 2016/17 2017/18 2018/19 Programme Baseline Allocation 733,574 753,601 775,410 Recurrent Changes In-Year 9 9 9 Running Cost Allocation 13,203 13,249 13,297 Total Notified Allocation 746,786 766,859 788,716
Non Recurrent Allocations 2016/17 2017/18 2018/19 Other Non-Recurrent allocations 6,962 (2,468) (2,507) In-Year drawdown/(drawup) (530) (100) (200) Total Non-Recurrent Allocation 6,432 (2,568) (2,707)
Total In-Year Allocation 753,218 764,291 786,009
Estimated registered population 638,289 645,128 652,117 Final per capita allocation 1,149 1,168 1,189 Final per capita growth 5.48% 1.64% 1.79% Final closing distance from target -2.64% -2.43% -2.01%
The closing distance from target shows that the CCG is now considered to be close to its target funding and will therefore be subject to ‘average’ levels of growth in future years. This is in contrast to the 6.7% received in 2016/17.

2
The 2017/18 to 2018/19 financial plan sets out how we will utilise these funds to support the strategy of the CCG. It also demonstrates how the CCG will return to in-year financial balance and deliver its control totals in both 2017/18 and 2018/19. The plan assumes that the CCG will not deliver its planned surplus in 2016/17. At this stage the CCG has been asked not to incorporate any element of deficit repayment into its plans.
Assumptions
In developing its expenditure plans the CCG has considered past levels of growth for its key areas of expenditure.
Growth levels have been applied to the forecast outturn at month 10 as follows:
Summary plan
The financial plan adheres to the business rules as set out in the planning guidance by:
i. the establishment of a 1% transformation reserve of which 0.5% remains uncommitted,ii. delivering its control totals in both 2017/18 and 2018/19iii. the re-establishment of a contingency reserve of 0.5%,iv. meeting the CCG’s requirement in terms of parity of esteemv. providing £3 per head to support the GP Forward view.
The Board is asked to note that in 2016/17 the CCG was required to set aside 1% of its allocation to support the national financial position. This sum currently remains uncommitted within the 2016/17 outturn. For 2017/18 and 2018/19 the CCG is only required to set aside 0.5% to which it must not commit its own expenditure. The remaining 0.5% is intended for non-recurrent transformation schemes.
Also, in the past the CCG has been required to deliver a 1% surplus each year. For this planning period the CCG has instead been set control totals such that it is expected to deliver a surplus of £100k in 2017/18 and £200k in 2018/19.
The summary financial plan as submitted to NHSE on 27 February 2017 is as follows:
Other Non Recurrent Cost Pressures
Gross Provider
Efficiency InflationNet tariff
inflation
Activity Growth
(Demog)
Activity Growth (Non-
Demog)
Acute Services -2.0% 2.8% 0.8% 1.1% 1.9%MH Services -2.0% 2.1% 0.1% 0.8% 0.0%Community services -2.0% 2.1% 0.1% 1.1% 0.4%Continuing Care Services 0.0% 4.6% 4.6% 1.0% 0.0%Primary Care Services 0.0% 4.2% 4.2% 1.1% 0.0%Other Programme Services 0.0% 1.7% 1.7% 0.2% 0.0%Primary Care Co-Commissioning 0.0% 0.0% 0.0% 0.0% 0.0%

3
The financial plan returns the CCG to financial balance on a recurrent basis from an underlying deficit position in 2016/17 of £5.9m.
QIPP
As noted above the CCG has received significantly less allocation growth in the 2 years of this plan when compared to previous years. The need to utilise this level of growth to meet all of the expected cost and activity growth, the business rules set out above and other planning requirements in addition to the need to return the CCG to in-year balance mean that there is a significant efficiency and savings requirement. The level of QIPP required to bring the financial plan back into balance is as follows:
Net QIPP Savings £ 000 2016/17 2017/18 2018/19 Recurrent (inclusive of full year effect) 10,930 38,024 25,103 % of Notified Resource 1.5% 5.0% 3.2%
Unidentified - 6,230 20,799 % Unidentified 0.0% 16.4% 82.9%
Revenue Resource Limit£ 000 2016/17 2017/18 2018/19Recurrent 746,786 766,859 788,716Non-Recurrent 6,432 (2,568) (2,707)Total In-Year allocation 753,218 764,291 786,009
Income and ExpenditureAcute 434,446 444,213 456,002Mental Health 79,919 81,466 83,824Community 66,492 63,944 66,183Continuing Care 31,140 30,497 32,174Primary Care 87,806 93,856 98,440Other Programme 48,212 33,539 32,729Primary Care Co-Commissioning - - -Total Programme Costs 748,015 747,515 769,352
Running Costs 13,203 12,941 12,713
Contingency - 3,835 3,944
Total Costs 761,218 764,291 786,009
£ 000 2016/17 2017/18 2018/19Underspend/(Deficit) In-Year Movement (8,000) - -
Net Risk (7,100) 0

4
Savings of £38m represents some 5% of the CCG’s resource limit and is significantly higher than that achieved in 2016/17.
As at 27 February the CCG had identified £32m of savings opportunities with £6.23m (16.4%) still to be identified.
£m Disinvestments / non continuation of expenditure 15 Continuing healthcare 3 Prescribing 2 Activity and contract related 12 Unidentified 6 Total QIPP requirement 38
At the point of signature no QIPP had been accepted as part of the contract values with acute trusts. To address this with West Hertfordshire Hospitals NHS Trust a joint QIPP Board has been established to identify, develop and agree schemes which will be incorporated into the contract from 1 April 2017.
Reserves
As part of the financial plan the CCG is holding a number of reserves. As noted within the business rules section above some of these are mandated and some must be held as uncommitted to support the national financial position.
Reserves held by the CCG are as follows:
Available to the CCG £m
Not Available to the CCG
£m
Total
£m 0.5% Reserve 3.8 3.8 0.5% Transformation Reserve 3.8 3.8 0.5% Contingency 3.8 3.8 Other 5.7 5.7
13.3 3.8 17.1
The reserves above are only available if the planned QIPP savings are delivered. The CCG Board has previously agreed that further investments to be funded from reserves should not be made until the QIPP savings and the overall financial position of the CCG allow it.

5
Risks
The financial plan as set out above can only ever be a statement of intent based on the knowledge available at a point in time. As the paper has set out a number of assumptions regarding activity growth and inflation have been made. There is an inherent risk within the plan that these assumptions prove to be inaccurate.
• Activity growth
One of the key assumptions within the plan is that a number of the QIPP schemes will mitigate and reduce the levels of activity that currently flow into the acute providers. Historically, activity growth has continued despite the existence of QIPP. Every 1% of acute activity growth above plan equates to approximately £4.4m.
In addition, assumptions have been made about the level of increases relating to the number of continuing healthcare packages. Whilst considerable work has been undertaken to ensure that eligibility reviews are carried out and that only relevant packages of care are charged to the CCG there is still the risk that the number of people eligible for care will increase above the levels included within the plan.
• Inflation and price risk
The Board has previously been made aware that the CCG is expecting an increase in acute tariff prices as a result of the move to HRG4+. The precise impact of this is not yet known but is expected to be in the region of £3.5m.
• QIPP delivery
As explained in the section on QIPP above the CCG has a significant QIPP target in 2017/18. In addition, delivery in 2016/17 was low despite an increased focus on the programme from October 2016 onwards. Whilst a number of schemes for 2017/18 are well developed a number still require significant work. Further schemes also need to be identified, developed and implemented.
In order to mitigate these risks the CCG is holding a number of reserves as set out above. In particular, the contingency reserve and part of the ‘other ‘reserves are being held to offset unplanned activity growth and the impact of HRG4+. Nevertheless, the CCG cannot rely on utilising its reserves to cover unplanned risks and must ensure that the QIPP programme delivers the full £38m. Achieving the QIPP programme should also allow for the establishment of funds to support the strategic aims of the CCG including Your Care, Your Future. Alongside this will be closer monitoring of acute contracts which are now in place. This allows earlier interventions when activity increases.
The level of risk inherent within the plan is recognised and as a result the CCG has included within its plan an assessment of net risk equivalent to £7.1m. This means that the CCG has made an assessment of the likely level of impact for each of its risks and the likelihood of them occurring. Under this assessment there is potentially £7.1m of risk for which no mitigations are yet in place.

6
Summary
The CCG’s latest 2017/18 financial plan has been developed using the 2016/17 forecast outturn as a start position. Assumptions regarding activity growth and inflation have been made using past trends and national guidance to inform the appropriate levels of uplift. As a result of lower levels of allocation growth than in previous years and the need to return to financial balance the levels of QIPP savings that need to be achieved are significantly higher than have historically been achieved.
In recognition of this the CCG has highlighted within the plan that it has a net risk of £7.1m.
There is no doubt that the delivery of the plan will present a significant challenge to the organisation especially in the 2017/18 financial year. Delivery will be dependent on rigorous financial control, the strict monitoring and management of provider contracts and a relentless focus on the delivery of QIPP.

SPACER PAGE

SPACER PAGE

NHS Herts Valleys Clinical Commissioning GroupBoard Meeting 9 March 2017
Item 7. CCG contributions to adult social care – paper to follow

SPACER PAGE

SPACER PAGE

NHS Herts Valleys Clinical Commissioning Group Board Meeting9 March 2017
Title Integrated quality performance and finance report Agenda Item: 8
Purpose (tick one only) Decision or Approval ☐ Discussion ☒ Information ☐
Responsible Director(s) and Job Title
Charles Allan- Director of Contracts and Resilience Caroline Hall - Chief Finance Officer Diane Curbishley –Director of Quality and Nursing
Author and Job Title Stephanie White – Performance Lead Short Summary of Paper This report provides an overview of performance across a number of domains,
namely; contract performance, quality, finance and programme performance. An integrated approach to performance involves coordinating all monthly data collections, producing a standard list of dashboards that are presented to the Quality and Performance Committee for a full discussion and assurance before a subset of this standard list is presented at the HVCCG Board and Commissioning executive committee.
The executive summary dashboards reflect the high priority key performance indicators identified which includes the recovery action plan/ trajectories (where applicable) and progress updates.
Key highlights: • CCG patients December performance compliant other than:
RTT and A&E Cancer – however very low patient numbers
• RNOH achieved 62 day standard in Nov and Dec• 6 KPI below and 6 above the national average• A&E continues to be a challenge• 2 week cancer referrals- confirming improvement (patient choice
related)
New reports are included : Community provider quarter success and challenge report for HUC, HPFT and HCT
Recommendation(s) The Committee is being asked to: • discuss and note the report
Engagement with Stakeholders/Patient/Public
Engagement has taken place with provider organisations.
Links to Strategic Objectives (tick all that apply) 1. Effective Engagement. We will continually improve engagements with member practices, patients, the
public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.☒
2. High Quality. We will commission safe, high quality services that meet the needs of the population, reducinghealth inequalities and supporting local people to avoid ill health and stay well.
☒
3. Transforming Delivery. Work with health and social care partners to transform the delivery of care throughthe implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
4. Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordablehealthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
Yes, this contributes evidence of assurance for the Board Assurance Framework in relation to: 1.1 “Risk that we do not engage effectively with a range of our patients, population and stakeholders” 1.2 “Risk that our member practices and other partners do not see the potential positive impact of their engagement with HVCCG” 2.1 “Risk that we do not deliver on all NHS Constitutional pledges, key national

targets and priorities” 2.2 “Risk that we are unable to ensure high quality, safe and sustainable services for the population and patients of west Hertfordshire” 2.3 “Risk that we do not close the health inequalities gap between the most and least deprived communities” 3.1 “ Risk that the joint submission to obtain additional capital resource to successfully transform the delivery of care in west Hertfordshire is unsuccessful” 3.2 “Risk that there will be insufficient support from local bodies and key stakeholders to transform the delivery of care in west Hertfordshire.” 3.3 “Risk that workforce issues will prevent us from transforming the delivery of care across the health and social care system” 4.1 “Risk that we do not deliver a financially sustainable health and social care system” “4.2 Risk that we do not deliver best value from the total CCG budget” 4.3 “Risk that we do not achieve financial balance for 2016/2017
This report mitigates risks on the Corporate Risk Register in relation to the following references: S01/24 Risk that public and stakeholders are not informed effectively S02/01 Risk of a lack of proportionate and effective controls on the use, sharing and publication of information SO2/15 Risk that the continuing healthcare (CHC) retrospective cases process is not able to deliver a desired outcome in a timely way S02/25 Risk of failure to deliver specific national targets n relation to dementia diagnosis S02/26 Risk to the CCG of not implementing the recommendations of Winterbourne View via the Transforming Care programme S02/30 Risk that patients are not assessed with a management plan and exited/admitted or discharged out of ED within 4 hours SO2/31 Risk that delayed transfers of care (DTOCs) are not reduced to the target of 2.5% SO2/32 Risk that the constitutional pledge to refer to treatment with 18 weeks at WHHT is not being met for our patients SO2/33 Risk that priority ambulance KPIs are not delivered for our patients. S03/02 Risk that localities will not be aligned with CCG strategic objectives S03/03 Risk of failure to ensure that Public Health is sufficiently embedded within the CCG programmes and localities S03/05 Risk that we fail to successfully transform health and social care through use of the Better Care Fund (BCF) S03/08 Risk that lack of available workforce in primary care prevents delivery of services identified as key to transformational change SO3/09 Risk that there will be a reduced level of provision for social care services S04/03 Risk that QIPP savings are not achieved as planned S04/22 Risk that there are higher levels of hospital activity than planned/anticipated S04/23 Risk that additional expenditure will occur that is not budgeted for.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
The executive summary dashboards reflect the high priority key performance indicators identified which includes the recovery action plan/ trajectories (where applicable) and progress updates.
Resource Implications Not applicable. This report provides a general update on key quality, performance and finance issues
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
There are no implications
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☒ Improved Patient Access and Experience ☒
A Representative and Supported Workforce
☒

Inclusive Leadership ☒
Report History Which Groups or Committees have seen this report and when?
9 March 2017 Quality and Performance Committee 28 February 2017 Senior Leadership Team
Appendices 10. Quality premium quarter 311 Workforce quarter 313 Environmental quarter 314 Better care fund quarter 315 Safe staffing quarter 316 Learning disability including transforming care quarter 318 System resilience progress update report19 Continuing health care quarter 3Glossary of terms
Chairs Quality and Performance Committee Report
Finance report The current financial forecast includes a number of significant risks which we expect could yet impact on the final outturn, including a number of unknowns in connection with provider contracts yet to be resolved. QIPP 2016/17 Current forecast is an end of year outturn of 51%. The risk around QIPP was flagged up some time ago and it is extremely disappointing that we have been unable to achieve better than this level despite the focus over the last few months. HUC Performance for December 2016 was the worst this year. There are significant concerns around on-going recruitment issues that have not been improved due to other opportunities that exist elsewhere, particularly for GPs. Apprenticeships It is very disappointing to note that so far only one apprentice is likely to be appointed in HR given that there are real opportunities for apprentices to contribute across the workforce including in primary care. This needs to be raised and discussed at Executive Team level, including exploring possible links to schools, including encouraging younger people to think of careers within the NHS. WHHT CQC report It is encouraging to see the CQC report further to the re-inspection in September 2016, with significant improvement being made in many areas. There is clearly still much to do with the CQC decision that WHHT ‘requires improvement’ but should stay in special measures in order to keep the pressure on for further improvement. QIPP 2017/18 The current level of QIPP worked up for 2017/18 is only at £31m, despite being reassured that by now we would have at least reached the target of £38m with a further 15% required on top as headroom. There are a number of QIPP plans within the £31m identified that are rag-rated ‘red’ and therefore give cause for concern that the £31m is not assured.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
9 March 2017 Integrated, quality and performance Board report
1. Purpose of this report
This report provides an overview of the key performance areas across a number of domains, namely; contract performance and quality and program performance. An integrated approach to performance involves coordinating all monthly data collections, producing a standard list of dashboards that are presented to the quality and performance committee for a full discussion and assurance before a subset of this standard list is presented at the HVCCG board.
1.1 Sections in this report The Integrated quality and performance report (IQPR) is a standardised set of dashboards with selected sections going to different groups, as described below:
Ref. Section
Available via HVCCG
intranet Board
Quality and performance committee
1 Introduction to the report
2 Key constitutional standards dashboard – funded via the sustainability and transformation fund
3
Performance against key national indicators (CCG view, acute trusts) full dashboards CCG patients
view CCG patients view
4 Quality dashboard /narrative quality exception
Quarterly stand-alone report and monthly dashboard/ exception verbal update
Appendices
5 Transformation / QIPP progress report Quarterly Stand-alone report
6 Digital road map
1 page summary of quarterly reports - appendix Quarterly
Half yearly- appendix
7 Health and wellbeing Annual- appendix
8 Quality premium Quarterly- appendix
9 Workforce Quarterly- Standalone document
10 Environmental Quarterly- appendix
11 Better care fund Quarterly- appendix 12 Safe staffing Quarterly- appendix
13 Learning disability including transforming care Quarterly-appendix
14 System resilience progress update report with
Ian
Monthly - appendix
15 Continuing health care (as of October 2016 report)
Quarterly - appendix
16 CCG assurance framework 2016-2017 including the six clinical priorities
Quarterly- appendix
17 Quarterly community provider success and challenge report
Quarterly from Q3
Quarterly from Q3 2016-2017
18 WHHT quality improvement plan
highlight report
Monthly- appendix
Item 8a

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
1.2 Based on comments received from HVCCG board and committee members the information provided to other
groups will be revised and will evolve over time.
A note about the data
1.3 The integrated quality performance and finance report includes a disparate range of indicators supported by a wide range of activity, finance, epidemiological and survey data and information. Whilst some metrics are related to short-term operational activity (e.g. A & E performance against the 4 hour target) others relate to longer term changes in outcomes. Consequently, not all metrics are updated monthly, partly due to data availability but also because a particular metric will not change significantly over the period of a month. The majority of the data is downloaded from the unify 2 website; this is where providers upload their data. Cancer waits data comes from the open exeter system , the data bases are live, so are constantly updated by the provider; therefore the data presented will reflect the position at the time of the data extraction. Four monthly stroke data from the sentinel stroke national audit program (SSNAP) and stroke monthly and delayed transfer of care ( DToC) comes from the provider performance reports. The East of England ambulance service sends their data to the HVCCG acute generic nhs.net email. 111 data source comes from sesui system that logs calls and Herts urgent care (HUC) data comes from the adastra system
As with performance reports in recent months the HVCCG are hampered by non-availability of patient identifiable
data.
A note about the narrative
1.4 The narrative within the dashboard reflect various information sources: trusts, community provider performance
reports, extracts from contract review meeting minutes, cancer action group, stroke leadership group, input from
programme leads, clinical leads and contract managers.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Executive summary: Key constitutional standards dashboard
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) that will give NHS the resources it needs as part of the five year forward view to sustain services. Trusts have agreed with NHS England and NHS Improvement a credible plan for maintaining delivery of core standards for patients, including the 4 hour A&E standard, the 18 week referral to treatment standard and for appropriate providers, the ambulance access standards. Key constitutional standards dashboard table below summarises the plan against actual performance for all of HVCCG main acute providers:
West Hertfordshire Hospital Trust:
Trusts Standards Threshold Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTD
Last 12 months
trend
Plan 83.0% 86.0% 88.0% 91.0% 93.0% 87.5% 88.6% 89.6% 91.0%
Actual 79.2% 85.9% 83.4% 83.2% 85.0% 85.2% 82.4% 84.0% 78.6% 83.7%
Plan No trajectories 88.9% 90.4% 91.7% 92.0%
Actual 88.6% 89.0% 88.5% 87.2% 87.2% 86.6% 87.4% 88.0% 86.9% 87.7%
Plan 0 0 0 0 0 0 0 0 0
Actual 2 1 0 0 1 0 0 0 0 4
Plan 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0%
Actual 99.9% 99.9% 100.0% 100.0% 100.0% 99.9% 99.9% 99.9% 100.0% 99.9%
Plan 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0%
Actual 87.2% 81.9% 86.9% 90.1% 88.7% 92.9% 87.0% 90.4% 94.9% 88.9%
99%
85%
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) for trusts to deliver against the agreed target recovery trajectories.
The table below summarises the plan against actual performance at Trust level view.
December data comments
A&E performance in December deteriorated to 77.8%, due to capacity issues particularly following the bank holiday period. Performance is still not in line with the revised trajectory to meet compliance.
Ambulance turnaround times deteriorated during December in line with increased demand and capacity issues. East of England Ambulance Service have continued to provide a hospital ambulance liaison
officer (HALO) cover and the cohorting of crews to monitor patients waiting in the corridor in order to release crews. The trust is also providing 2 queue nurses support to patients in the corridor.
An activity comparison of the current financial year (to 15/1/2017) with the same period last year has shown:
• Type 1 attendances are up by 6.4%,
• Ambulance arrivals are up by 8.0%,
• Admission rate from A&E (excluding ambulatory and frailty) is up by only 0.5 percentage points.
Front door flow, including acute assessment units
• An additional assessment area for GP patients was established during the period of peak demand and internal escalation
• In response to emergency pressures the trust has opened a number of additional surge beds which has also impacted on length of stay (LOS) and the ability to assess patients in a timely manner.
• STARRING (Rating) commenced in A&E in December
• Twilight service – the first substantive staff are now in post and working in the department. Efforts to try and fill unfilled shifts through NHS Professionals continue. Feedback has been very positive.
Hospital patient flow
• A clinical champion and a programme lead have been identified for SAFER and training is going well. The system held a “perfect (red to green)” week w/c 5th December and the learning has been shared
from this.
• The use of the patients lounge has increased and is now able to take 2 stretcher patients.
• Ward based multidisciplinary teams multidisciplinary teams (MDT) LOS review meetings continued through December
• The trust continues to work closely with the emergency care and improvement programme (ECIP) and system partners to improve flow both internally and externally.
East of England are working on a recovery plan to get people back on 999 vehicles and had met with SSG Healthcare to turn around performance with a working group including clinical representatives to
devise new initiatives.
Other initiatives are being evaluated eg halo, street triage as to how they fit into that recovery plan.
RTT
Planned reduction in elective activity over the Christmas & New Year break, combined with increased site pressures resulted in a deterioration against the 92% standard, with a submitted performance of
86.9% for December 2016 (88% November).
Elective medicine & women and children’s services (WACS) continue to meet the standard but surgery and clinical support have yet to achieve 92%.
The number of pathways between 0 and 18 weeks continues to reduce and this month, as a result of reduced activity, the backlog has increased slightly.
Outsourcing continues, with 791 patients currently considered appropriate, of which 419 have agreed to treatment with an alternative provider, 340 have been dated and 176 have been treated.
The tumour sites contributing to the breaches were lung, haematological, gynaecological and head and neck.
Reasons for breaches included patient choice, complex pathways that are accounted for in the standards. Other breach reasons are by tumour site:
Lung – there were capacity issues in diagnostics services internal and external to the trust, and also late referral out to Harefield. The pathway is now much better managed and the capacity issues at
Watford and Harefield have been resolved.
Urology – robot-assisted laparoscopic radical prostatectomy (RALP) & brachytherapy (BRACHY) waits are delaying patients significantly. This is being discussed with Herts Valleys CCG.
Gynae – Late referrals are coming into Watford via tertiary centre. A meeting is to be arranged with the cancer manager to discuss how this can be resolved.
Head and neck (H&N) - Complex patient pathway, patients needing several tests, MDTs and transferred between sites several times.
Please note: there are low patient numbers for many tumour sites and therefore compliance is vulnerable to a low number of breaches at tumour site level.
However it should be noted that aggregate performance is compliant and in line with the STF.
On track for performance compliance March 2017
Cancer 62 day: December is compliant .
West
Hertfordshire
Hospital Trust
(WHHT)
95%
92%
0
A&E 4 hour
standard
18-weeks RTT
Incomplete
Pathways
18-weeks RTT
Volume of 52
weeks breaches
Cancer 62 days
from GP referral
99% of Diagnostic
Pathways to be
Seen within 6-
weeks

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Executive summary: Key constitutional standards dashboard – funded via the Sustainability and transformation (continued):Royal free London:
Trusts Standards Threshold Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTD
Last 12 months
trend
Plan 90.0% 92.0% 93.0% 95.0% 95.0% 95.0% 92.0% 90.0% 91.0%
Actual 90.3% 92.5% 90.2% 91.3% 90.0% 87.9% 85.5% 85.0% 83.6% 90.4%
Plan 90.9% 91.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0%
Actual 90.4% 92.0% 92.2% 92.2% 92.0% 92.1% 92.2% 92.0% 92.1% 91.9%
Plan 5 5 5 5 5 5 0 0 0
Actual 4 2 4 2 3 5 2 2 0 24
Plan 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0%
Actual 99.7% 99.7% 99.7% 99.8% 99.6% 99.8% 99.8% 99.8% 99.1% 98.7%
Plan 79.7% 75.2% 76.1% 77.4% 78.1% 74.0% 78.0% 84.0% 85.0%
Actual 79.7% 80.9% 85.8% 75.8% 77.5% 78.0% 73.7% 82.1% 82.2% 79.3%
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) for trusts to deliver against the agreed target recovery trajectories.
The table below summarises the plan against actual performance at Trust level view.
99% of
Diagnostic
Pathways to be
seen within 6-
weeks
Cancer 62 days
from GP referral
Royal Free
London (RFL)
18-weeks RTT
Incomplete
Pathways
18-weeks RTT
Volume of 52
weeks breaches
A&E 4 hour
standard
December data commentsA&E
In December the combined trust outturned at 83.59% against the 95% standard. At site level, both the Royal Free hospital site and the Barnet hospital site failed the indicator outturning
at 85.21% and 76.68% respectively.
RFL have launched the safer, faster, better (SFB) programme to ensure that patients get home as soon as they are medically well enough.
“Improvement weeks” have been undertaken previously at the Royal Free London hospitals most recently back in January 2016 to help the flow of patients.
RFL decided to run an improvement week from Wednesday 4th – Tuesday 10th January on all Royal Free London sites, including the Royal Free hospital, Barnet hospital and Chase Farm
hospital.
Objectives of back to the floor were:
To rapidly get flow back in the whole system
To improve patient experience, safety, quality and flow throughout the trust
Placement of patients no longer requiring acute care into the appropriate environment
To increase front door turnaround and ensure a timely wrap around services response
To accelerate and improve discharge processes
To use the week to accelerate and embed known good practice
To engage staff and improve the working environment.
Cancer 62 day GP
National care improvement programme have conducted a review and RFL are awaiting the report to determine the revised plan and trajectories.
RFL recovery trajectory aimed for 83.8% in November and compliance in December.
Each non-compliant tumour site has a recovery plan (shared regularly with our North Central London (NCL) cancer lead) with actions identified to address the key areas of the patient
pathway. The chief operating officer continues to meet weekly with tumour site leads to ensure all pathways are analysed and delays addressed.
RFL have made good progress implementing key elements of our action plan this year to date, including:
- Lung straight to test pathways
- Prostate hot reporting, active in 3 clinics
- Teledermatology and dermatology one-stop clinics
- Renal and Hepatobiliary (HPB) one-stop clinics
- Improved MDT and root cause analysis (RCA) processes
We have also engaged in some backlog clearance. We believe that these have all made substantial improvements to our patient care.
However, we do not currently anticipate that we will return to standard in December. Outstanding actions that will affect performance include:
- Implementing hot reporting for the remaining 3 prostate clinics (of these, 2 are scheduled to start at the end of January)
- Increasing haematuria clinic capacity (due in January)
- Reducing turnaround times for histopathology results
- Identifying and addressing delays on inter-specialty pathways
- Increasing volumes on Lower GI straight to test pathways
85%
92%
0
99%
95%
Luton and Dunstable University Trust:
Trusts Standards Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTDLast 12 months
trend Plan 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0%
Actual 98.9% 98.7% 98.9% 99.1% 99.1% 99.1% 98.9% 99.0% 98.7% 99.0%Plan 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0%
Actual 94.2% 95.0% 94.8% 93.7% 92.9% 92.6% 92.2% 93.9% 93.1% 93.4%
Plan 0 0 0 0 0 0 0 0 0
Actual 0 0 0 0 0 0 0 1 0 1
Plan 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0%
Actual 99.2% 99.7% 99.1% 99.1% 99.0% 99.3% 99.6% 99.3% 99.1% 99.3%
Plan 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0%
Actual 85.6% 88.2% 86.7% 94.0% 87.5% 86.5% 88.0% 87.6% 89.0% 88.4%
Threshold
18-weeks RTT
Volume of 52
Weeks Breaches
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) for trusts to deliver against the agreed target recovery trajectories.
The table below summarises the plan against actual performance at Trust level view.
A&E 4 hour
standard18-weeks RTT
Incomplete
Pathways
December comments
Performance compliant
Above trajectories.Luton and
Dunstable
University Trust
(LDUT)
Cancer 62 days
from GP Referral
99% of Diagnostic
Pathways to be
Seen within 6-
weeks
85%
99%
0
95%
92%

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Executive summary: Key constitutional standards dashboard – funded via the Sustainability and transformation (continued):East and North Herts Trust (ENHT):
Trusts Standards Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTD
Last 12 months
trend
Plan 76.0% 77.0% 79.0% 81.0% 82.5% 85.0% 85.5% 86.0% 87.0%
Actual 81.1% 84.7% 84.7% 84.2% 82.5% 82.8% 88.0% 89.4% 85.4% 83.4%
Plan 92.0% 92.1% 92.4% 92.4% 92.5% 92.6% 92.6% 92.6% 92.6%
Actual 92.7% 93.0% 92.6% 92.8% 92.6% 92.1% 92.1% 92.1% 91.3% 92.5%
Plan 4 4 4 6 3 3 2 2 2
Actual 4 3 2 5 12 23 40 20 19
Plan 99.5% 99.5% 99.5% 99.5% 99.5% 99.5% 99.5% 99.5% 99.5%
Actual 99.9% 99.7% 99.7% 99.7% 99.5% 99.6% 99.7% 99.6% 99.2% 99.6%
Plan 78.0% 81.0% 85.0% 85.0% 74.0% 77.1% 77.9% 78.3% 83.3%
Actual 80.5% 81.5% 73.5% 76.5% 86.4% 63.9% 58.9% 67.2% 68.1% 70.1%
Threshold
East and North
Hospital Trust
(ENHT)
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) for trusts to deliver against the agreed target recovery trajectories.
The table below summarises the plan against actual performance at Trust level view.
A&E 4 hour
standard95%
18-weeks RTT
Volume of 52
Weeks Breaches
Cancer 62 days
from GP Referral85%
0
December comments
92%
18-weeks RTT
Incomplete
Pathways
99%
99% of Diagnostic
Pathways to be
Seen within 6-
weeks
A&E : ENHT did not achieve the 4 hour standard in December and failed the STF improvement trajectory, delivering 85.41% against a trajectory of 87%. Although performance was below the STF recovery
trajectory, December’s performance was a 5% improvement compared with the same period in 2015.
-This has now been escalated regionally with NHS England/NHS Improvement.
-There is a new triage process and a new chief operating officer in place.
-ECIP are also in as part of the ECIP remit regarding clinical leadership in A&E.
-There is a GP at the front door pilot in place from 01.01.17-31.03.17 with site actions and criteria in place.
Contract performance notice in place and action plan is currently being revised.
ENHT waiting over 52 weeks during December; these patients are a consequence of the current validation exercise. Application of clock stops 68 clock stops validated from June 15 and are highlighted in
52 week breaches. There were 100 breaches in December and 20 in January so RTT failed in December and January.
Each patient is being reviewed for any potential harm as a result of the delay in treatment and as yet none has been found.
1 x 52+ HVCCG patient- contract manager to raise penalty notice
62 day Performance
• The tumour sites of head and neck, upper gastrointestinal (GI) and urology have not achieved in either of the standards.
Corrective actions
• In order to sustainably deliver the cancer standard a number of key actions are required and in progress:
• Data and Information – the current cancer patient tracking list (PTL) is built from the cancer system (Infoflex), the reporting capabilities of Infoflex are not sufficiently developed to enable the detailed
level of 31 day patient tracking required. Therefore in conjunction with the Information team a new PTL is under construction that will enable a greater oversight of the patient’s entire cancer pathway.
• Performance is currently reported retrospectively, ENHT’s ability to forecast is currently very limited due to the processes used in our Infoflex system. The cancer and information teams are currently
developing a performance forecasting model.
• The data quality within the Infoflex system is poor, users have not been entering data in or close to real time and large volumes of data are recorded into free text fields making consistent reporting
almost impossible. Standard operating procedures (SOP) are being developed and implemented to ensure a standardised approach across both the Mount Vernon and Lister cancer teams.
• ENHT has historically not reported cancer performance separated between the Mount
Vernon and Lister sites; this reduces our ability to target performance, action is currently in progress to try and resolve this issue.
• The structure of the cancer division for those staff involved in PTL management and patient tracking needs to be reviewed. The current model fairly unique and does not support clarity of roles and
responsibilities
• Intensive support team (IST) completed their two day assessment of the service in December and the trust awaits the final report. From the verbal feedback received the actions above combined with the
larger cancer action plan appeared to cover the issues highlighted. The team highlighted two areas for immediate follow up of which both of these issues were immediately actioned and confirmation has
been received from the appropriate teams that processes have been changed.
Latest update at collaborative commissioning forum 14/2/17
Cancer 62 day – Contract performance notice in place as trust
Remedial action plan (RAP) has been received from the Trust
PTL 2 phases in place to rectify :
Phase 1 – infrastructure to be put in place for PTL. There is a regional escalation for cancer – RAP was to be submitted to ENCCG by Trust 14.02.17. ENHCCG to review and submit a revised trajectory by
tumour site.
Phase 2 - Interim management and support (IMAS) to come in to look at capacity and notes.
Royal National Orthopaedic Hospital (RNOH)
Trusts Standards Threshold Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTD Last 12 months trend
Plan
Actual
Plan tbc tbc 87.6% 88.2% 88.9% 88.7%
Actual 86.2% 88.0% 87.5% 87.5% 87.1% 87.6% 88.2% 88.1% 87.0% 87.5%
Plan tbc tbc 0 0 0 0 0 0 0
Actual 0 0 1 0 1 0 0 2 0 4
Plan tbc tbc 96.3% 97.4% 99.1% 99.0%
Actual 98.2% 97.4% 96.7% 96.3% 95.2% 96.3% 95.4% 95.7% 90.7% 95.6%
Plan tbc tbc 57.1% 71.4% 85.7% 85.0%
Actual No Data No Data No Data 38.5% 88.6% 84.6% 56.5% 100.0% 88.9% 57.8%
December comments
Royal National
Orthopaedic
Hospital (RNOH)
A&E 4 hour
standard95%
RTT: Overall RTT Performance is stable at 88.1%. We agreed a revised trajectory to compliance by 28/02/17 with NHS England and NHS Improvement at the escalation meeting on 12/10/16. The revised trajectory is
dependent on our continued drive to treat more patients at RNOH in a timely manner, to improve on our referral processes and continued efforts to outsource additional patients by 28/02/2017.
RNOH have made significant improvements and are compliant on many areas of the trust specialties: Peripheral nerve injury, paediatrics, cancer, sarcoma.
For sarcoma and cancer we have no breaches and are 100% compliant, the only trust nationally to achieve this.
RNOH currently have two patients in the system that are breaching over 50wks, RNOH contract lead does not believe they are HVCCG patients but I am awaiting confirmation.
Both of these are complex patients requiring 9 hours surgery each. The delays are due to firstly patient choice, and secondly a consultant being on paternity leave (only surgeon in the country able to do this procedure) and
the length of surgery means that surgery cannot be done on consecutive days.
RTT plans: RNOH are working closely with NHS England to develop and refresh this to ensure more sustainability going forward. RNOH have been asked to work with a demand and capacity model that is used by many other
trusts in London currently working through this and will be shared with HVCCG.
RNOH have a new RTT lead and we are hoping to put on a session that will be open to all CCGs to attend with an opportunity to ask questions on the model when it is ready.
Diagnostic waits:
Further deterioration due to recent spike in sarcoma referrals. Additional MRI outsourcing from December and additional ultrasound sessions continue.
A cobalt mobile scanner has started on site since yesterday. This has been funded by NHS England to help us get through increased demand for the service. Even before this, please note that RNOH latest position on UNIFY
will show that we have gone from 91% compliance to 96% last week, so improvements.
The new scanner will enable an additional 20 parts to be scanned per week
62 day Cancer: Achieved compliance as planned - first compliant month this financial year (Nov)-
4 x 62 day first treatments; all were treated within target.
Improvements made during the month were:
•Patient tracking list (PTL) meeting every week to track patients with clinical input from the consultant nurse.
•Increase in the tracking of the patients along the PTL rather than their care being managed through the meeting above.
•Telephone clinics since middle of August being run by the advanced nurse practitioner (ANP)which has resulted in the
discharging of more patients back to the referring district general hospital (DGH )when sarcoma has not been diagnosed.
•Increase in communication to the consultant team in the division in relation to 31 decision to treatment (DTT) and 62 day pathway patients.
•The schedulers have an increased awareness of the cancer target and patients are identified if they are on a cancer
target.
Contract manager has arranged contract review meetings with RNOH from the 8th of March to develop terms of reference (TOR) and performance reporting requirements.
18-weeks RTT
Incomplete
Pathways
18-weeks RTT
Volume of 52 Weeks
Breaches
0
99% of Diagnostic
Pathways to be
Seen within 6-
weeks
99%
92%
No A&E department
Cancer 62 days from
GP Referral85%
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) for trusts to deliver against the agreed target recovery trajectories.
The table below summarises the plan against actual performance at Trust level view.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Executive summary: Key constitutional standards dashboard – funded via the sustainability and transformation (continued):Buckinghamshire Healthcare Trust:
Trusts Standards Threshold Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTD Last 12 months trend
Plan 91.5% 95.0% 95.0% 97.1% 96.3% 95.5% 95.5% 95.3%
Actual 91.4% 89.4% 93.7% 91.8% 92.6% 91.9% 90.1% 87.9% 87.6% 91.8%
Plan 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0% 92.0%
Actual 92.0% 93.0% 92.1% 92.1% 91.7% 90.2% 89.5% 89.2% 88.8% 91.0%
Plan 0 0 0 0 0 0 0 0 0
Actual 1 0 0 0 0 1 0 0 0 2
Plan 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0%
Actual 99.8% 99.8% 99.8% 99.9% 99.5% 99.3% 100.0% 99.9% 99.7% 99.9%
Plan 86.2% 86.4% 86.9% 89.1% 85.3% 90.8% 88.1% 88.1% 90.0%
Actual 86.6% 84.0% 86.6% 79.5% 88.6% 79.2% 83.8% 84.4% 85.2% 84.1%
December comments
A&E 4 hour
standard95%
A&E :
Action plan agreed to improve performance managed through A&E delivery board.
New completion date: Q4, 2016/1
RTT :Growth in elective demand, especially in surgical specialties, has pushed BHT’s compliance against the 92% referral to treatment performance target down throughout Q3. The issue is predominantly focused around
rising demand. Cataract surgery (the trust’s most common surgical procedure) has seen referral numbers grow by over 50% from 15/16 outturn, leading to extended waits in both outpatients and theatres.
A RTT recovery program of work has been submitted which seeks to deliver sustainable RTT performance in Q4, based on the current known backlog. This plan focuses on five ‘hot spot’ areas :
general surgery, ophthalmology, paediatrics, trauma & orthopaedics (T&O) and oral surgery.
Actions:
• Sourcing of external spot purchase cataract activity – 400 cases due to be completed by the
end of December but there has been a slower than expected uptake by the BMI – 78 patients
completed to date – contract is now extended to end of February 2017
• Two cataract fellow’s recruited and in post (December 2016)
• Dedicated cataract only surgery in February (treat 127 cases) – excluding emergencies
• Cataract days rolled out to Wycombe and Amersham on Wednesdays (extra 40
slots/week)
• Outsourcing current oral surgery backlog (188 patients) to local dental practices
(January 2017)
Aim for compliance is by quarter 4.
Risks:
• Delayed speed of mobilization to outsource work and inability to divert out of area referrals in time
• Demand levels increasing further
• Delays in the Individual funding request procedure
• Capacity constraints and winter bed pressures resulting in the frequent cancellation of elective
surgery on the Stoke Mandeville Hospital (SMH) site on account of day surgery units (DSU) being used for an escalation area
Cancer 62 day: Performance compliant for Dec.
Actions:Thames Valley Cancer Network has issued a standard operating procedure (SOP )‘Cancer Pathways Inter Trust Transfer of Care’. The standard form for tertiary referrals is now being used.
Both the standard operating procedure (SOP) and the Cancer Access Policy have been adopted by BHT with effect from mid-November
HVCCG contract team will be working closely with BHT and the lead commissioner on this contract to develop a better understanding of key actions being taken to address under performance.
18-weeks RTT
Incomplete
Pathways
92%
18-weeks RTT
Volume of 52
Weeks Breaches
0
99% of Diagnostic
Pathways to be
Seen within 6-
weeks
99%
Cancer 62 days
from GP Referral85%
For 2016/17 NHS Improvement has allocated additional funding from the sustainability transformation funds (STF) for trusts to deliver against the agreed target recovery trajectories.
The table below summarises the plan against actual performance at Trust level view.
Buckinghamshire
Healthcare Trust
(BHT)
2. Key issues/ challenges and planned actionsWest Hertfordshire Hospitals Trust
Cancer 2 week waits following urgent GP referral for suspected cancer and 2 week waits and breast symptomatic where cancer is not suspected:
Indicator Trust Threshold 2015/2016 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-162016/2017
YTDLast 12 Months Dec data comments
Cancer 2 week waits following
urgent GP referral for
suspected cancer
WHHT - actual 93% 91.5% 81.0% 89.4% 90.8% 89.1% 94.5% 94.3% 90.1% Performance compliant for 2 consecutive months
Cancer 2 week waits - breast
symptomatic where cancer not
suspected
WHHT - actual 91.6% 44.8% 68.6% 88.3% 83.5% 88.3% 90.6% 78.6%
December is an improvement on November, up from 88.3% to 90.6% but is non-compliant.
The overall performance for this standard for Quarter 3 stands at 87.6 with 60 breaches to be validated. 51 patients breached due to patient cancellation, 7
administrative delays and 1 outpatient capacity and 1 recorded as other reason.
CGG have been informed and they will encourage GP’s to ensure before referring their patients are advised to ensure they are available for the next 2 weeks
HVCCG communications have gone out to practices about the need to ensure patients are available within two weeks of being referred.
This was also mentioned at the Herts-wide cancer update day beginning of February
93%

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Key issues/ challenges and planned actions:
East of England Ambulance Trust:
Indicator Trust Threshold 2015/2016 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-162016/2017
YTDLast 12 Months Dec data comments
Accountable
director
Responsible
managerClinical lead
East of England
ambulance
trust (EEAST )-
actual
60.5% 58.9% 62.2% 63.5% 63.6% 65.9% 62.2% 60.9%
EEAST Plan
EEAST - plan
EEAST - actual 71.3% 66.7% 68.5% 70.0% 70.20% 71.3% 69.9% 68.0%
Q2= 69.2% 72.8%
Ambulance category A -
red 2 (life threatening but
less time critical than red
1) response arriving <8
mins-EEAST
Ambulance category A -
red 1 (immediate life
threatening and most time
critical) response arriving
within 8 mins-EEAST
75%
75%
Charles AllanSharon
Kember
Dr Keith
Hodge
EEAST CCG operational performance group meeting 17th January 2017 update at meeting:
EEAST have experienced a very difficult festive period, followed by the previous week’s issues with severe delays at all acutes and finally the flood surge over the 12th –
14th January.
Some lessons learnt have been from managing the flood surge incident, namely the need for a defined list of vulnerable individuals which is shared between all services
and constantly maintained. EEAST advised that the development of digital roadmaps were currently underway which should assist with this going forward.
Senior contracts manager from lead commissioner will be attending an NHS England briefing on Friday 20th January, awaiting an update.
EEAST auditing R1 calls. Action: Share audit process of R1 calls with group.
Section 1 – Principles of Agreement
• demand: Nationally EEAST are still on the busiest ambulance response programme 1 (ARP1 )
Trusts.
• Capacity: small drop in rapid response vehicle (RRV) unit hour production (UHP)
since the summer, now close to 17.5K target line. Consideration should be made to reduction in hours and recent demand in the system.
Community first responders (CFR)
hours have had noticeable reduction in the past 4 weeks
February will also deliver a month of professional update (PU); staff have been encouraged to do overtime to accommodate this.
•Number of R1 patients responded to in 8 minutes: A reduction of 67 R1 patients for this week, providing the biggest drop in any one week. A reduction in R2 patients
also seen as R1 responses are prioritised.
• Weekend performance impact: No deterioration from the weekend, quality trauma discharge (QTD) figures have begun well. Discussion took place regarding
communicating to patients about conditions at A&E.
• National context: EEAST are middle of the pack this week for R1 performance, R2 performance reporting low this week, however A19 looks to be remaining
comparatively high.
Section 2 - recovery action plan (RAP) assumptions
Activity assumptions:
• Incident response count, YTD variance = 3.23%, and R1 and R2 incident response figures show YTD variance = 16.23% activity reduction in both red categories.
Section 3 – Improvements & efficiency
• Priority focus 1: Performance remains low in line with red demand.
• Priority focus 2: Rapid response vehicle (RRV) performance below 75%.
• Priority focus 3: Double staffed ambulance (DSA) Unit hour production (UHP) marginally up on last week, however private ambulance services (PAS) UHP down,
this was driven mainly by significant number of no shows by PAS crews. Sickness showing continued increase, reporting above 7.4%.
• Priority focus 4a: Sharp reduction A-to-H, which was one of the biggest influences in the trust's performance last week
• Priority focus 4c: Princess Alexandra Hospital (PAH) bucking the overall trend with upwards trend for arrival to handover (AtoH).
Priority focus 5: responses per incident (RPI) increased to 1.34 as demand reduced for R2.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Key issues/ challenges and planned actions:Hertfordshire Partnership Foundation Trust:
Indicator Threshold Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16Last 12
months
Accountable
director
Responsible
manager
Clinical
lead
Routine referrals to community mental health team
meeting 28 day wait≥98% 95.98% 95.57% 97.71% 91.75% 90.87% 92.66% 96.69% 87.25% 92.70%
Early memory diagnosis and support service referrals
meeting 6 week wait ≥90% 83.42% 85.03% 89.47% 96.33% 91.67% 93.97% 95.59% 98.04% 94.57%
Child and adolescent mental health services - percentage of
referrals meeting assessment waiting time standards -
routine (28 DAYS)≥95% 94.44% 95.59% 94.74% 92.59% 80.36% 100.00% 100.00% 100.00% 82.98% Charles Allan Simon Pattison
Dr
Mark
Allen
% of service users with an up to date risk assessment
(including learning disability & forensic (LD&F) & child and
adolescent mental health services (CAMHS) from April 201595% 94.89% 93.34% 93.88% 95.00% 94.77% 100.00% 94.61% 94.16% 94.14%
People with severe mental illness who have received a list
of physical checks (in-patients only)98% 95.35% 98.18% 98.15% 100.00% 100.00% 97.92% 100.00% 98.11% 100.00%
Number of people entering Improving access to
psychological therapies (IAPT) treatment
(Dec threshold
562)620 786 819 629 795 842 849 962 562
2% patients 1441
/12 months = per
month plan 120
120 120 120 120 120 120 120 120 120
Actual - numbers 106 113 112 109 114 87 96 103 tbc
Plan 50%50% 50% 50% 50% 50% 50% 50% 50% 50%
Actual - numbers 34.57% 37.70% 34.55% 50.00% 45.45% 42.47% 44.26% 46.30% tbc
Hertfordshire Partnership Foundation Trust
December comments
Waiting times
Performance of the trust’s single point of access (SPA) service impacts on many of the trust’s waiting
times, in particular those with a higher number of referrals such as child and adolescent mental health
services (CAMHS) and adult community teams’ routine waits. When performance falls in SPA, there is
a direct correlation with these services' performance the following month.
Over the past two years referral rates, incuding urgent to SPA, have been increasing, Therefore the
pressure to respond to these referrals within the necessary timescales has been significantly
exacerbated by high staff turnover within SPA in Q3, thus impacting on the ability of SPA to pass
routine referrals within 14 days, resulting in the decline in performance for CAMHS and adult
community. In January SPA performance has stabilised following immediate actions to address the
demand capacity gap and a recovery plan being implemented within the community teams that is
expected to deliver a balanced run rate position by the end of Q4.
Charles Allan Simon Pattison
Dr
Mark
Allen
Please refer to the dementia progress update for narrative
Due to the delays in SPA and a staff shortfall in the CAMHS Pod. A recovery plan is in place with
CAMHS staff clearing SPA breaches whilst SPA maintain the 14 day pass-on time. This is being
managed between a combination of staff working on bank and triaging remotely. Daily automated
reports are shared by SPA and a daily teleconference in place. The backlog in SPA is expected to be
cleared by 20th January 2017, which will result in an increased pressure on the community teams to
provide first appointments for these children.
Patient safety
Pressure within services to see people within waiting time thresholds and clearing backlogs that have
accumulated through the problems with SPA, has contributed to the decline as more assessment slots
have had to be found from a limited number of appointments available. There are known peaks of
risk assessments due in Q4, which will present a challenge for some services to meet this demand as
well as maintaining access levels.
To be reviewed at the contract review meeting on Wednesday 15th February 2017.
Charles Allan Simon Pattison
Dr
Mark
Allen
Any qualified provider (AQP) data for improving access to psychological therapies (IAPT ) access and recovery
access to IAPT via AQP/ IAPT counsellors
Charles Allan Simon Pattison
Dr
Mark
Allen
Recovery via AQP/ IAPT counsellors
Lea Vale's data has now been added to Q3, brining AQP access in line with anticpiated performance at
M9.
Nationally the recover rate for depression is lower than anxiety. Our AQP provision focussed upon the
Counselling for depression treatment modality and there it is expected that recovery rates are lower
than 50% target. A smaller number of providers who were successful at tender will see recovery rates
increase into Q4 and providers aware the expectation is for recovery rates above 50%.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Key issues/ challenges and planned actions:Herts Urgent Care:
Herts urgent care - Hertfordshire wide view
Indicator Threshold2015/2016 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16
2016/2017
YTDLast 12 Months Dec data comments
Accountable
director
Responsible
manager
Clinical
lead
Urgent home visits within
2 hours›95% 89.9% 90.2% 86.9% 93.9% 87.9% 89.4% 82.7% 88.5%
An increase in home visits for December 2016, compared to November Dec-16 2016. There were 2
weekday bank holidays in December, Acute in hours visiting service (AIHVS) impacted out of
hours (OOH) performance on some weekday evenings as 120 visits were passed into the OOH
period. Reduced visiting capacity in OOH across some weekends in December, 86% of the GP rota
was filled this month and there were 192 hours of sickness and 159 cancelled shifts.
Actions: HVCCG Director of contracts and resilience raised that areas that have been red for the
year need to have actions in place. The CCG will work with HUC around this in order to understand
what HUC need to improve performance. HVCCG requested that the report has to be clear on
what the improvement is for OOH and AIHVS. The CCG stated they needed to see forecasting to
have some idea of when improvement was going to start. Assurance is required by the CCG.
Please see HUC Q3 success and challenge report for further details on the action plan
Routine home visits
within 6 hours›95% 90.7% 87.7% 83.2% 90.8% 88.8% 88.3% 84.4% 87.7%
Procurement update:
Following a procurement process, the intergrated urgent care (IUC) contract has been awarded,
with standstill period until 20th January. The new service will commence in June 2017, with the
contracts teams in ENCCG and HVCCG working together on the mobilisation.
Action plan update :
The HVCCG IUC lead has emphasised that "AIHVS should not have a knock on effect on the Herts
Valleys OOH visiting resource and a remedial plan for out of hours needs to run in addition to the
AIHVS remedial plan.”
Please see HUC Q3 success and challenge report for further details on the action plan
Urgent face to face
consults within 2 hours›95% 89.3% 87.4% 92.8% 90.4% 86.7% 91.6% 89.0% 89.6%
An increase of 1216 cases for come to centre appointments from Dec-16 November this includes 2
weekday bank holidays. 86% of the GP rota was filled this month and there were 192 hours of
sickness and 159 cancelled shifts
Actions: see above
Dr Vipal
Parbat/ Dr
Keith
Hodge
Steve
Marshman as
of October
2016
Charles Allan
Herts Community Trust: Herts Community Trust (HCT)
refIndicator
Threshol
d2015/2016 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16
2016/2017
YTDLast 12 months Dec data comments
Accountable
director
Responsible
managerClinical lead
LQR 30
Average length of stay in HCT
community hospital for non-stroke
patients (trust view)
≤ 21 27.4 29.7 30.0 30.6 29.2 29.5 31.0 29.2 37.5 26.8 30.0
HCT were over the average length of stay (ALOS) thresholds for non-stroke. HCT
recorded a ALOS of 27 days for non-stroke patients, an improvement of six days on
previous month. There were five patients whose LOS was 80 days or over and of
these patients, three stayed over 100 days. One of these patients
was sub-acute and stayed for 146 days of which 109 were actual rehabbing days.
NB: Please see HCT Q3 success and challenge report for further details on the
action plan.
LQR 30
Average length of stay in HCT
community hospital for non-stroke
patients - HVCCG patient
≤ 21 29.4 30.6 34.5 32.3 29.6 31.2 33.0 30.3 37.7 25.9 31.8%
Non-stroke patients recorded a LOS of 26 days which improved to 19 days and
within threshold on the rehab pathway.
LQR 31
Community hospitals average
length of stay in HCT community
hospital non-stroke rehab
pathway only- HVCCG patient
≤ 19 19.9 20.5 19.5 22.3 19.9 22.1 20.5 19.0 22.4 19.0 20.6 Performance compliant for December
Charles Allan
As of
September
Steven
Marshman
Dr Clair Moring

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
2. Key issues/ challenges and planned actions:
Dementia update:
Dementia progress update :Accountable
director
Responsible
manager
Clinical
lead65+ Only (CFAS
II)30 - 64 (AS-
2014)Total
Estimated dementia prevalence in Herts
Valleys 6,778 364 6,990
67% target 4,519 244 4,683
Current estimated number diagnosed
(NHS England dementia diagnosis
workbook 16th Jan)
4,389 118 4,484
Additional diagnoses required to meet
target130 126 256
Estimated percentage diagnosed based on
new prevalence figures64.8%
Month Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Actual reporting via NHS England
workbook61.80% 62.80% 63.51% 64.5% 64.50% 64.50% 64.80% 64.80%
64.50% 65.00% 65.60% 66.20% 66.70% 67.30%
Dr Mark
Allen
We will continuously monitor performance against the following trajectory of improvement: This trajectory has now been updated using the dementia mortality rate from Public Health
England for Herts Valleys and the diagnostic capacity and rates from the new early memory diagnosis and support service (EMDASS) service model.
Diagnosis: where are we now?
Charles
Allan
Simon
Pattison
Revised trajectories from October 2016
Update:Performance reporting - 97% of patients are being seen within six weeks in the north-west and 83% in the south-west. At the end of December, 269 people were waiting to see a consultant. HPFT have increased the diagnostic sessions offered in excess of 30% per week in order to bring this number of people waiting down to a manageable level. Of the diagnostic sessions undertaken, 80% are receiving a diagnosis.
Practice visits : dementia estimated prevalence and diagnosis rate dashboard by practice to support to inform engagement with practices - progress to date means 14 practices have received a visit with a mental health lead, locality support and mental health commissioner and on-going regular communications via normal routes. Wave 2 has begun, with an additional 10 practices targeted due their 'gap' in expected diagnosis made
Action plan progress update: Implementation of the action plan has continued with respect of primary care
engagement actions. All localities apart from Dacorum have now received their dementia training/information session. GP's from other localities will be attending if they were unavailable at the time it was held in their locality.
3. HVCCG all acute providers at CCG patients view:
Indicator Plan2015/1
6Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 YTD
TRUST VIEW: Last 12
monthscomments for Dec
Cancer 2 week waits following urgent GP referral for
suspected cancer93% 95.1% 95.2% 93.1% 89.8% 84.3% 90.5% 91.5% 91.6% 94.5% 94.6% 91.6%
Cancer 2 week waits - breast symptomatic where cancer is
not suspected93% 91.3% 95.3% 90.7% 78.9% 56.5% 76.0% 91.1% 88.0% 90.4% 91.5% 84.3% Non-compliance is due to WHHT
Cancer 31 day - 1st definitive treatment from diagnosis 96% 98.1% 95.5% 97.1% 95.6% 97.7% 95.7% 96.2% 93.6% 98.1% 97.3% 96.3%
Cancer 31 day - subsequent treatment for cancer - surgery 94% 96.1% 96.2% 100.0% 100.0% 96.3% 100.0% 100.0% 95.7% 96.2% 97.0% 98.0%
Cancer 31 day - subsequent treatment for cancer - drugs 98% 98.7% 98.8% 100.0% 97.1% 100.0% 98.8% 96.7% 96.3% 97.6% 94.7% 97.8%Non-compliance is due to ENHT small
numbers
Cancer 31 day - subsequent treatment - radiotherapy 94% 95.8% 92.2% 92.5% 91.4% 93.7% 92.4% 90.1% 97.7% 92.3% 98.5% 93.3%
Cancer 62 days - 1st treatment following an urgent GP
referral85% 83.6% 83.9% 78.5% 83.3% 86.0% 80.5% 85.8% 82.1% 87.9% 92.4% 84.6%
Cancer 62 days - 1st treatment following referral from
screening service90% 94.1% 100.0% 93.3% 90.9% 89.5% 100.0% 96.4% 85.7% 100.0% 76.2% 92.1%
Non-compliance is due to WHHT small
numbers
Cancer 62 days - 1st treatment following consultants
decision to upgrade85% 86.2% 81.8% 94.1% 100.0% 82.4% 75.0% 78.6% 80.0% 85.0% 76.2% 84.1%
Non-compliance is due to WHHT and ENHT
very small numbers
18 week referral to treatment -incomplete pathway 92% 92.1% 91.0% 91.5% 90.8% 90.0% 89.8% 89.3% 89.0% 89.5% 90.6% 91.2%Non-compliance is due to WHHT, Bucks,
RNOH and ENHT
Number of patients waiting more than 52 weeks on
incomplete pathways0 3 3 5 4 3 4 0 0 1 23 Refers to ENHT
Diagnostic tests - % of patients waiting 6 weeks or less 99% 98.6% 99.7% 99.6% 99.5% 99.6% 99.3% 99.4% 99.8% 99.7% 99.3% 99.7%
A&E total time in department - less than 4 hours 95% 88.4% 83.1% 87.8% 86.1% 86.0% 86.8% 86.7% 84.5% 85.5% 81.5% 85.4%Non-compliance is due to WHHT, ENHT, RFL
and Bucks
Performance against key national indicators - CCG patients view for all Acute providers
3. Full dashboards for WHHT, RFL, ENHT, L&D, Bucks, RNOH– are available on the intranet:
http://hertsvalleysccg.nhs.uk/documents/business-intelligence-performance-and-information-governance/performance-reports
4. Quality key points: verbal update

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
5. Transformation and quality, innovation, productivity & prevention (QIPP) progress report:

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
5. Transformation and quality, innovation, productivity & prevention (QIPP) progress report (Continued)

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
5. Transformation and quality, innovation, productivity & prevention (QIPP) progress report (Continued)

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
5. Transformation and quality, innovation, productivity & prevention (QIPP) progress report (Continued)

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
6. Digital road map: n/a
7. Health and wellbeing report: annual appendix: n/a
8. Quality premium: quarter 3 report:
Measure
% of
quality
premium
£
equivalent
available
Baseline Target Time frameAchievement
Q3 16/17Comments RAG
Proportion of cancers diagnosed at stages 1 and 2 20% £587,5082013 = 51.1%, 2014 =
54.6%
Improve by 4 percentage
points to 58.6%
increase from 2015
to 2016n/a
Next release due Jun-17 - chasing
quarterly data from NHS England
GP Patient Survey - percentage of respondents who said they had a
good experience of making an appointment20% £587,508 July 15 = 77%, July 16 =
78.3%
Increase by 3 percentage
points to 81.3%
increase from July
16 to July 17n/a Next release July 2017
Increase in the proportion of GP referrals made by e-referrals 20% £587,508 March 16 = 39%Increase by 20 percentage
points to 59%
increase from Mar
16 to Mar 1747% Dec data
Improving antibiotic prescribing in primary and secondary care -
number of antibiotics per weighted antibiotic population
2015/16 = 1.03 per
weighted antibiotic pop1.16 1.04
Improving antibiotic prescribing in primary and secondary care -
number of co-amoxiclav, cephalosporins and quinolones as % of the
total selected antibiotics
2015/16 = 7.7% 10.0% 8.0%
LOCAL: % of patients aged 17+ with diabetes, as recorded on practice
disease registers10% £293,754 2014/15 = 5.08% 5.2%
increase from
14/15 to 16/175.27%
LOCAL: Reported prevalence of COPD on GP registers as % of
estimated prevalence10% £293,754 2014/15 = 57.36% 60%
increase from
14/15 to 16/1760%
LOCAL: % of patients returning to usual place of residence following
hospital treatment for stroke10% £293,754
2014/15 = 67.4%,
2015/16 = 68.6%72%
increase from
14/15 to 16/1771.5% 2016/17 Q3
TOTAL AWARD AVAILABLE £2,937,538
= £2,937,538 our weighted pop 1st April 2016 * £5 TOTAL MINUS AMBER RAG £1,175,015
**This may change if a provider meets its planned trajectory throughout the year TOTAL AFTER BREACHES** £293,754
Reason to deduct from award - current progress at CCG Target 2015/16 breach 14/15? £ reduction if breach reduction if breach Q3 2016/17 breach?
deficit/audit no £2,897,897 100%
Maximum 18 weeks from referral to treatment – incomplete standard 92% 92.1% yes £724,474 25% 90.6% yes
Maximum four hour waits in A&E departments 95% 88.4% yes £724,474 25% 81.5% yes
Maximum two month (62-day) wait from urgent GP referral to first definitive treatment for cancer85% 83.6% yes £724,474 25% 92.4% no
Maximum 8 minute response for Category A (Red 1) ambulance calls - CCG residents this year75% 65.3% yes £724,474 25% 64.4% yes
2015/16
(2016/17 results n/a till Sep 2017)
no reduction
needed from 15/16
to 16/17
Latest 4 Quarters
(Jan 16 - Dec 16)10% £293,754

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
9. Workforce: quarter 3 report
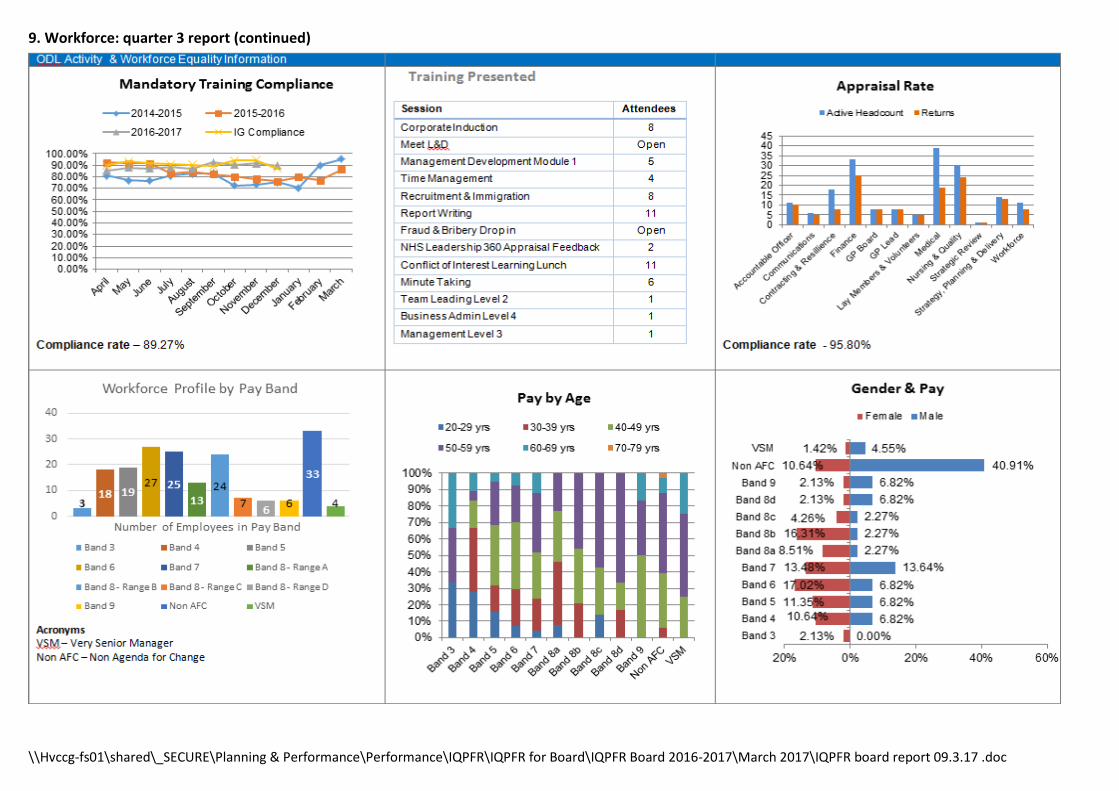
\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
9. Workforce: quarter 3 report (continued)

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
9. Workforce: quarter 3 report (continued)
Workforce narrative – Q3 Report
Workforce establishment & vacancy Rate By the end of this quarter, Herts Valley's vacancy rate was 19.83% with the total number of vacancies being 40. The actual working time equivalent (WTE) is currently 160 which is under the budgeted WTE of 199.
Current vacancies are within:
Contracting and resilience x 8
Finance, performance and corporate (FPC) x 7
Governing body x .5
Medical x 16
Nursing and quality x 6
Workforce x 3

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
9. Workforce: quarter 3 report (continued) Staff turnover This quarter highlights a turnover of 8.16% full time equivalent (FTE) which compared to Q3 15/16 (11.78%) is a slight reduction. During this quarter, 13 people left the organisation for the following reasons: -
1 End of fixed term contract
1 retirement
1 better reward package
1 lack of opportunities
3 work-life balance issues
6 promotions A trial of an electronic exit interview process is planned to enable a better understanding of the reasons for leaving given by staff. This will start to inform our retention strategies within the CCG. Agency/interim spend Agency and interim spend has continued to decline since October. Total spend YTD is £1,098,369.62. Further work around
reviewing the current interim headcount and recruiting on a permanent basis should result in a potential further decline by
the new financial year. Spend for Q3 is £490,071.00
Areas of highest spend for Q3 are contracting (@ £135k) and FPC (@ just about £135k)
Agency and interim spend continues to be monitored on a monthly basis.
Steps are in place to comply with NHS England guidance on agency spend for CCGs. Sickness absence The sickness absence trend has been steadily reducing and stands at 1.79% against the CCG’s national average of 2.59%; this highlights a significant reduction to the figures reported in Q3 15/16 of 4.19%. However, going forward there will be a continued focus on staff wellbeing with an aim to ensure early interventions with regards to sickness absence. Actions currently underway to address these issues are as follows:
A review of the Management of sickness absence policy
Monthly reports produced by workforce Information on attendance to highlight triggers that have been reached
Analysis to be undertaken of common reason for absence and linked to health and wellbeing champions
Human resources (HR) fundamental training being delivered to managers on sickness absence management
Promoting the employee assistance programme and health campaigns. Mandatory training compliance and appraisal rate Mandatory training compliance stands at 89.27% The appraisal and performance review policy is currently being reviewed and updated and will be launched around 31st March 2017. Other ODL Activities Education, training & development policy was developed and has been ratified and approved. A suite of HR masterclasses for staff and line managers has been developed by the HR & ODL team and will be launched in the spring. Equality data The equality and diversity annual report has been produced by the equality and diversity lead (Paul Curry) which showed that Herts Valleys was an organisation where the staff group is reasonably balanced, when compared to the local population and other CCGs. A full report is available on request.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
10. Environmental: quarter 3 report
Quarter 3, October - December 2016 summary progress report for sustainability (environmental dashboard)
key progress in quarter 3
key issues in quarter 3 Actions / timescales / learning
The overall organisational carbon footprint is predicted to
increase by 12,352 tCO2e on 2015/16 data by the end of Q4
(a smaller increase than last year, but we are working
towards a reduction).
Catering costs increased considerably on lastquarter, despite the CCG’s current financial position.However, some of the invoices paid related to theprevious quarter. Therefore, it would seem we didnot realise the reduction in catering costs initiallyindicated for last quarter. We need to look to reducethese costs by reducing catering requirements orusing more cost-effective venues. We did introduceauthorisation forms to try and manage this sometime ago but this has had no effect on spendingwhich continues to increase.
Although still on target, the rate of recycling wastehas reduced.
The sustainable development action plan (SDAP) hasbeen re-worked and sent through to the board forapproval. Therefore, limited work has beenundertaken on this during the last quarter.
The carbon footprint related to travel and the staffcommute remains a significant issue for us.
Sustainable development working group(SDWG) to discuss ideas in which cateringcosts might be reduced going forward.
Reporting on providers who have an SDMPand who use the good corporate citizen (GCC)to be extended to the Royal NationalOrthopaedic hospital. Negotiations to takeplace with those providers who do notcurrently have an SDMP in place or do not usethe GCC toolkit to ensure that appropriateaction is taken (2016/17)
“Recycling challenge” to be promoted for NHSsustainability day in March 2017 as a way toincrease recycling and reduce landfill waste.
Work to recommence on new SDAP now it hasbeen approved by the board.
New staff travel survey to be conducted inMarch 2017 at which time the distance of thecurrent staff commute will be recalculated.
Remaining on target to reach trajectory reductions on electric usage (however, this
is only based on one quarter’s winter usage), recycling and paper usage
Reducing water usage

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Environmental dashboard: APPENDIX A - HVCCG ENVIRONMENTAL DASHBOARD 2015/2016
Category Key performance indicators 2014/15 - 2019/20
Original
threshold
(tCO2e)
2014/15
(tCO2e)
2015/16
(tCO2e)
Quarter 1 Apr-
Jun 2016
(tCO2e)
Quarter 2 Jul-
Sep 2016
(tCO2e)
Quarter 3
Oct-Dec 2016
(tCO2e)
Quarter 4 Jan-
Mar 2017
(tCO2e) TREND COMMENTS STATUS
A target reduction of 3% for 14/15 and 5% per annum from 15/16 onwards 137,177 144,118 153,897 41,558 40,893 42,233
Annual equivalent measurement of 166,245 tCO2e so not currently meeting targets - increase
seen on Q1 & Q2 data
Plan 133,062 126,203 124,448 122,772 121,059 119,344 ↑
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards
17.76 29.04 22.78 3.23 1.28 8.66
Annual equivalent measurement of 17.56 tCO2e so currently not meeting targets. However,
this is not an accurate end of year reflection as only 1 quarter of winter usage is reflected.
Plan 17.23 16.35 16.12 15.9 15.68 15.46 ↑
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards81.29 41 47.88 7.27 9.38 9.63
Annual equivalent measurement of 35.04 tCO2e so currently meeting targets. Increase on Q1
& 2 figures - only 1 quarter of winter usage reflected in data.
Plan 78.85 74.85 73.83 72.81 71.8 70.79 ↑
A target reduction of 3% for 14/15 landfill and 5 % per annum from 15/16 onwards0.51 0.98 0.88 0.22 0.4 0.21
Annual equivalent measurement of 1.11 tCO2e, including an increase on Q1, so currently not
meeting targets, although current reduction on last year.
Plan 0.5 0.48 0.47 0.46 0.45 0.45 ↓
A target increase of 3% for 14/15 recycling and 5 % per annum from 15/16 onwards 0.07 0.11 0.14 0.02 0.03 0.02 Annual equivalent measurement of 0.09 tCO2e so currently on target.
Plan 0.07 0.08 0.08 0.09 0.09 0.09 ↓
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards 1.52 1.56 0.62 0.05 0.55 0.11 Annual equivalent measurement of 0.95 tCO2e so currently on target.
Plan 1.47 1.4 1.38 1.36 1.34 1.32 ↓
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards5.72 13.97 10.14 3.77 2.26 5.7
Annual equivalent measurement of 15.64 tCO2e currently significantly exceeding targets -
increase on last quarter.
Plan 5.55 5.26 5.19 5.12 5.05 4.97 ↑
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards
128.44 87.72 30.85 3.89 8.27 11.01
Annual equivalent measurement of 30.89 tCO2e so currently on target. Increase on Q1 but
reduction on same quarter last year.
Plan 124.59 118.17 116.56 114.95 113.35 111.75 ↑
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards 2.65 1.88 2.71 0.31 0.41 0.42
Annual equivalent measurement of 1.52 wte so currently on target. Slight increase on last
quarter but reduction on the same quarter last year.
Plan 2.48 2.35 2.31 2.28 2.25 2.22 ↑
A target reduction of 3% for 14/15 and 5 % per annum from 15/16 onwards
34.62 407.76 496.88 474 476 475
Annual equivalent measurement of 486 tCO2e so significantly above target. Business mileage
has remained the same this quarter but the carbon footprint is mostly made up of staff
commute. Currently showing a small reduction on last year.
Plan 33.59 31.86 31.43 31 30.57 30.13 ↑
A target reduction of 3% for 14/15 and 5% per annum from 15/16 onwards
23.59 14.27 14.74 2.21 2.46 3.51
Annual equivalent measurement of 10.91 tCO2e but based on spring/summer energy usage.
Slight reduction to data for Q1 highlighted in red due to reduction in electricity usage for that
quarter.
Plan 22.88 21.68 21.38 21.08 20.79 20.5 ↑
Increase in the proportion of providers that have sustainable development plans in place
to 100% by 2015/16* 80% 80% 80% 80% 80% 80%
Royal l national orthopaedic hospital (RNOH) added to portfolio of providers wef 1/4/16.
Reported annually.Plan 80% 100% 100% 100% 100% 100%
Increase in the proportion of providers that have completed the Good Corporate Citizen
Assessment to 100% by 2015/16* 40% 40% 80% 80% 80% 80% Royal Free (RF) and RNOH added to portfolio of providers wef 1/4/16. Reported annually.
Plan 40% 100% 100% 100% 100% 100%
75% compliance with current sustainable development action plan (SDAP) to be achieved.15 55 134 143 160 161
Currently slightly below target. However, work plan has been revised so ne trajectories will be
required for 17/18
Plan 21 137 147 157 167 177 ↑
* Calculated based on the following organisations: Barnet & Chase Farm Acute Hospital Trust; East of England Ambulance Service; Hertfordshire Community NHS Trust; Hertfordshire Partnership University NHS Trust; West Hertfordshire Hospitals NHS Trust
** No information has been provided by HCT in relation to the Avenue Clinic, therefore data for this site has been estimated based on that for Apsley 2
Overall carbon footprint
Gas
Paper products
Travel
Sustainability development action plan
Commissioning
Electric
Waste
Water & sanitation
Food & catering
Information and communication devices
Energy well to tank and transmission
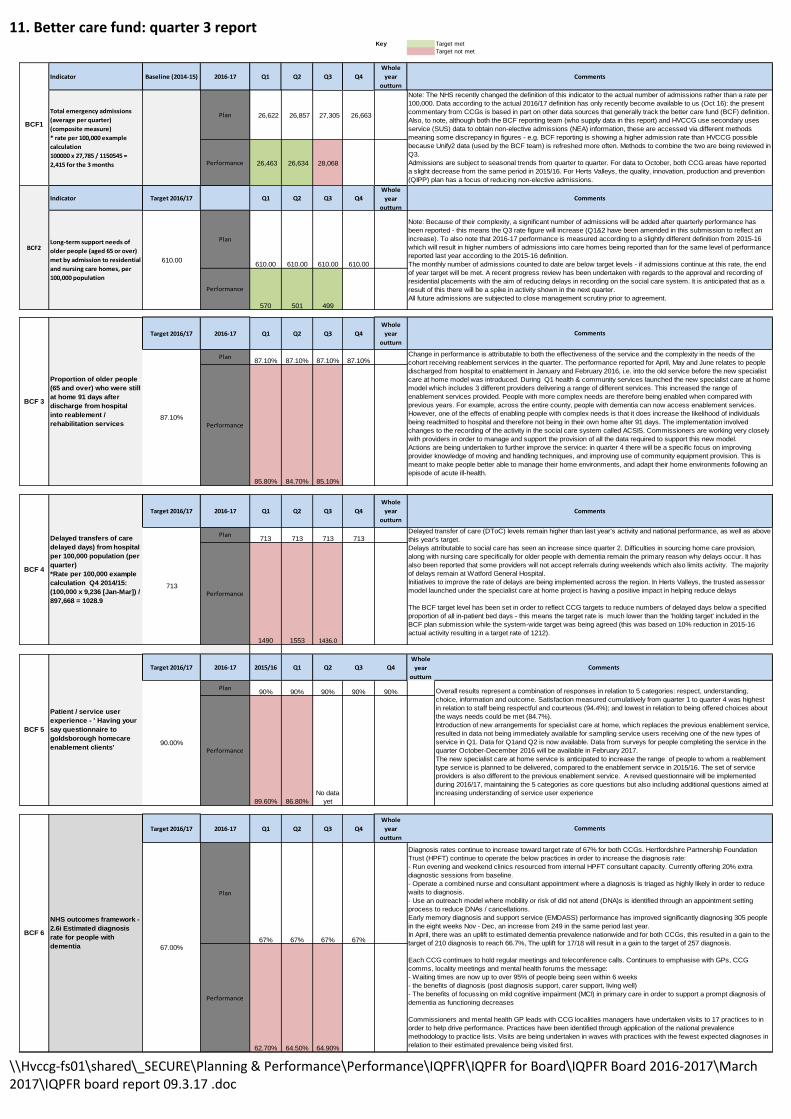
\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
11. Better care fund: quarter 3 reportKey Target met
Target not met
Indicator Baseline (2014-15) 2016-17 Q1 Q2 Q3 Q4
Whole
year
outturn
Plan 26,622 26,857 27,305 26,663
Performance 26,463 26,634 28,068
Indicator Target 2016/17 Q1 Q2 Q3 Q4
Whole
year
outturn
Plan
610.00 610.00 610.00 610.00
Performance
570 501 499
Target 2016/17 2016-17 Q1 Q2 Q3 Q4
Whole
year
outturn
Performance
85.80% 84.70% 85.10%
Target 2016/17 2016-17 Q1 Q2 Q3 Q4
Whole
year
outturn
Performance
1490 1553 1436.0
Target 2016/17 2016-17 2015/16 Q1 Q2 Q3 Q4
Whole
year
outturn
Performance
89.60% 86.80%
No data
yet
Target 2016/17 2016-17 Q1 Q2 Q3 Q4
Whole
year
outturn
Performance
62.70% 64.50% 64.90%
BCF 6
713
90%90%
67%
713
67%67.00%
Plan
67%
90.00%
BCF 4
713
BCF 5
713
Delayed transfers of care
delayed days) from hospital
per 100,000 population (per
quarter)
*Rate per 100,000 example
calculation Q4 2014/15:
(100,000 x 9,236 [Jan-Mar]) /
897,668 = 1028.9
Comments
87.10%
713
90%
67%
Diagnosis rates continue to increase toward target rate of 67% for both CCGs. Hertfordshire Partnership Foundation
Trust (HPFT) continue to operate the below practices in order to increase the diagnosis rate:
- Run evening and weekend clinics resourced from internal HPFT consultant capacity. Currently offering 20% extra
diagnostic sessions from baseline.
- Operate a combined nurse and consultant appointment where a diagnosis is triaged as highly likely in order to reduce
waits to diagnosis.
- Use an outreach model where mobility or risk of did not attend (DNA)s is identified through an appointment setting
process to reduce DNAs / cancellations.
Early memory diagnosis and support service (EMDASS) performance has improved significantly diagnosing 305 people
in the eight weeks Nov - Dec, an increase from 249 in the same period last year.
In April, there was an uplift to estimated dementia prevalence nationwide and for both CCGs, this resulted in a gain to the
target of 210 diagnosis to reach 66.7%, The uplift for 17/18 will result in a gain to the target of 257 diagnosis.
Each CCG continues to hold regular meetings and teleconference calls. Continues to emphasise with GPs, CCG
comms, locality meetings and mental health forums the message:
- Waiting times are now up to over 95% of people being seen within 6 weeks
- the benefits of diagnosis (post diagnosis support, carer support, living well)
- The benefits of focussing on mild cognitive impairment (MCI) in primary care in order to support a prompt diagnosis of
dementia as functioning decreases
Commissioners and mental health GP leads with CCG localities managers have undertaken visits to 17 practices to in
order to help drive performance. Practices have been identified through application of the national prevalence
methodology to practice lists. Visits are being undertaken in waves with practices with the fewest expected diagnoses in
relation to their estimated prevalence being visited first.
Delayed transfer of care (DToC) levels remain higher than last year's activity and national performance, as well as above
this year's target.
Delays attributable to social care has seen an increase since quarter 2. Difficulties in sourcing home care provision,
along with nursing care specifically for older people with dementia remain the primary reason why delays occur. It has
also been reported that some providers will not accept referrals during weekends which also limits activity. The majority
of delays remain at Watford General Hospital.
Initiatives to improve the rate of delays are being implemented across the region. In Herts Valleys, the trusted assessor
model launched under the specialist care at home project is having a positive impact in helping reduce delays
The BCF target level has been set in order to reflect CCG targets to reduce numbers of delayed days below a specified
proportion of all in-patient bed days - this means the target rate is much lower than the 'holding target' included in the
BCF plan submission while the system-wide target was being agreed (this was based on 10% reduction in 2015-16
actual activity resulting in a target rate of 1212).
Comments
Overall results represent a combination of responses in relation to 5 categories: respect, understanding,
choice, information and outcome. Satisfaction measured cumulatively from quarter 1 to quarter 4 was highest
in relation to staff being respectful and courteous (94.4%); and lowest in relation to being offered choices about
the ways needs could be met (84.7%).
Introduction of new arrangements for specialist care at home, which replaces the previous enablement service,
resulted in data not being immediately available for sampling service users receiving one of the new types of
service in Q1. Data for Q1and Q2 is now available. Data from surveys for people completing the service in the
quarter October-December 2016 will be available in February 2017.
The new specialist care at home service is anticipated to increase the range of people to whom a reablement
type service is planned to be delivered, compared to the enablement service in 2015/16. The set of service
providers is also different to the previous enablement service. A revised questionnaire will be implemented
during 2016/17, maintaining the 5 categories as core questions but also including additional questions aimed at
increasing understanding of service user experience
90%
Patient / service user
experience - ' Having your
say questionnaire to
goldsborough homecare
enablement clients'
BCF1
610.00
BCF2
BCF 3
87.10%
Total emergency admissions
(average per quarter)
(composite measure)
* rate per 100,000 example
calculation
100000 x 27,785 / 1150545 =
2,415 for the 3 months
Long-term support needs of
older people (aged 65 or over)
met by admission to residential
and nursing care homes, per
100,000 population
Proportion of older people
(65 and over) who were still
at home 91 days after
discharge from hospital
into reablement /
rehabilitation services
NHS outcomes framework -
2.6i Estimated diagnosis
rate for people with
dementia
Comments
Comments
Note: The NHS recently changed the definition of this indicator to the actual number of admissions rather than a rate per
100,000. Data according to the actual 2016/17 definition has only recently become available to us (Oct 16): the present
commentary from CCGs is based in part on other data sources that generally track the better care fund (BCF) definition.
Also, to note, although both the BCF reporting team (who supply data in this report) and HVCCG use secondary uses
service (SUS) data to obtain non-elective admissions (NEA) information, these are accessed via different methods
meaning some discrepancy in figures - e.g. BCF reporting is showing a higher admission rate than HVCCG possible
because Unify2 data (used by the BCF team) is refreshed more often. Methods to combine the two are being reviewed in
Q3.
Admissions are subject to seasonal trends from quarter to quarter. For data to October, both CCG areas have reported
a slight decrease from the same period in 2015/16. For Herts Valleys, the quality, innovation, production and prevention
(QIPP) plan has a focus of reducing non-elective admissions.
Comments
Note: Because of their complexity, a significant number of admissions will be added after quarterly performance has
been reported - this means the Q3 rate figure will increase (Q1&2 have been amended in this submission to reflect an
increase). To also note that 2016-17 performance is measured according to a slightly different definition from 2015-16
which will result in higher numbers of admissions into care homes being reported than for the same level of performance
reported last year according to the 2015-16 definition.
The monthly number of admissions counted to date are below target levels - if admissions continue at this rate, the end
of year target will be met. A recent progress review has been undertaken with regards to the approval and recording of
residential placements with the aim of reducing delays in recording on the social care system. It is anticipated that as a
result of this there will be a spike in activity shown in the next quarter.
All future admissions are subjected to close management scrutiny prior to agreement.
Comments
Change in performance is attributable to both the effectiveness of the service and the complexity in the needs of the
cohort receiving reablement services in the quarter. The performance reported for April, May and June relates to people
discharged from hospital to enablement in January and February 2016, i.e. into the old service before the new specialist
care at home model was introduced. During Q1 health & community services launched the new specialist care at home
model which includes 3 different providers delivering a range of different services. This increased the range of
enablement services provided. People with more complex needs are therefore being enabled when compared with
previous years. For example, across the entire county, people with dementia can now access enablement services.
However, one of the effects of enabling people with complex needs is that it does increase the likelihood of individuals
being readmitted to hospital and therefore not being in their own home after 91 days. The implementation involved
changes to the recording of the activity in the social care system called ACSIS. Commissioners are working very closely
with providers in order to manage and support the provision of all the data required to support this new model.
Actions are being undertaken to further improve the service: in quarter 4 there will be a specific focus on improving
provider knowledge of moving and handling techniques, and improving use of community equipment provision. This is
meant to make people better able to manage their home environments, and adapt their home environments following an
episode of acute ill-health.
87.10% 87.10% 87.10%Plan
Plan90%
Plan

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
12. Safe staffing: quarter 3 report
NB: All providers have actions in place to ensure they achieve safer staffing levels. Any accompanying exception reports will be detailed in the Q3 Quality Report` Data available from May 2015
Source: Nurse staff ing return - Unify2 - Published (NHS Choices)
Data available from May 2014
DCO Team
(Click down arrow to select DCO Team)
Org
codeTrust
Registered
midwives/n
urses Fill
Rate
HCA Staff
Fill Rate
Registered
midwives/
nurses Fill
Rate
HCA Staff
Fill Rate
Central Midlands RWH East & North Hertfordshire 100.08% 96.76% 80.13% 98.66% 92.83%
Central Midlands RY4 Hertfordshire Community NHS Trust 91.32% 127.89% 100.14% 154.59% 115.64%
Central Midlands RWR Hertfordshire Partnership NHS Foundation Trust 104.72% 125.67% 100.00% 100.00% 106.30%
Central Midlands RC9 Luton & Dunstable Hospital FT 88.00% 94.96% 99.23% 96.20% 94.12%
Central Midlands RWG West Hertfordshire Hospitals 74.99% 73.07% 100.00% 61.29% 80.16%
Other Trust HVCCG Commissionned RXQ Buckinghamshire Healthcare NHS Foundation Trust 100.00% 88.89% 100.00% 83.33% 96.43%
RAL Royal Free London NHS Foundation Trust 83.80% 89.56% 85.22% 98.25% 86.52%
RAN Royal National Orthopaedic Hospital NHS Trust 96.94% 98.19% 100.00% 100.00% 98.50%
Day Night
Overall
Fill Rate
Purely Indicative
threshold only - No
standards have been
set for this data
Less than 95%
Less than 90% or greater
than 150%
OCTOBER
2016-17

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
13. Learning disability including transforming: quarter 3 report
key progress in quarter 3 report Oct- Dec 2016
key issues in quarter 3 Actions / timescales / learning
Transforming care:
o Care and treatmentreview (CTR) and all ageavoidance admission
o Housing/accommodation/housing benefit Issues
o Discharge trajectories
Projects
Creative therapy in-patient andcommunity pilot
Circles
HPFT pilot servicescommenced foroffender andbehaviouralinvention andsupport
Social care crisisteam andcommunity crashpad – delayed asmarket unable torespond to the brief
Children and young people’s and adult leads in post leading On CTRs and admission avoidance work. Focus on community CTRs to support admission avoidance and also development of risk register – now known as admission avoidance register.
Continue to cause delays to discharge, escalated regionally and Nationally. Locally integrated accommodation commissioning team leading work to respond; project group set up to look at long term project work with in-house services around service provision for people with complex/high cost needs. Still awaiting confirmation re capital bid monies NHS England submitted in October, department of health capital bid failed. Work with providers in independent sector to reconfigure decommissioned community hospital for people with learning disabilities and autism continues. Herts transforming care partnership are attending and hosting a stall at a regional provider event on 22 Feb
Herts met Q3 for quarterly discharge targets. Child and adolescent mental health services (CAMHS) inpatient numbers currently 2: discharge plans for one person in place for both; one will be short spell in inpatient setting.
The work has now been completed. Positive outcomes in community pilot. The aim is to make this work sustainable; creative practitioners applied to join the provider list so that it can be purchased by use of individual budgets.
Two circles established and two circles in progress. Continuing to recruit volunteers.
Offending behaviour intervention team working well to brief. Early intervention practice development team name changed to positive partnerships team. Review of team following challenges with recruitment. Focus of team revisited in February: clear focus on prevention work, team working well positive feedback from users: support to individuals and providers, includes training.
Brief revised. Agreed to explore ‘proof of concept’ ideas with creative practitioners (creative therapies, application of positive behaviour supports) and shared lives. Aim now to ensure that creative practitioner work is sustainable and ensure practitioners are on provider register so that individuals can purchase via individual budgets health/social care as appropriate. Bid submitted for monies to develop shared lives model, a community provider has expressed interest also. With regard to prevention work a provider has approached Herts county council (HCC) with regard to utilising changing their residential service to supported living model and also to include community mobile outreach team to help prevent admission, the integrated accommodation team will lead on scoping this further with provider, integrated health & care commissioning team and operational teams.
Background summary In order to streamline action planning and measuring progress for learning disabilities (LD) in Hertfordshire it was decided to initiate an overarching learning disabilities delivery plan. This amalgamates actions from: the annual learning disability self-assessment framework which checks and rates the effectiveness of health, social care and community services for people with learning disabilities; Hertfordshire’s 2014 – 2019 joint commissioning strategy for LD and transforming care programme the national programme of work in response to Winterbourne view.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
key issues in quarter 3 Actions / timescales / learning
Specialist residential services(SRS)
New governance arrangements in place: provider & commissioners planning and assurance meeting in place, this meeting includes expert by experience family member from Herts and pan-regional oversight group established. The provider & commissioner assurance meeting aim is to have oversight of work plan for the service which includes person centred planning work being led by independent, advocacy organisation. This work will include individuals and their families as appropriate and feed into the assessment process led by social workers/care managers and the multi-disciplinary teams.
Children’s accommodationservices
Capital monies secured for Wynchlands and revenue funding agreed with education as part of multi-agency funding approach. Positive behaviour autism and learning disability mental health service reviewed now leading to further work around early identification, prevention and family support.
Health checks: (quality outcome framework) QoF register 2017/18: 2,708 Between April 2016 – December 2016: 540 health checks had been ‘claimed’. The number carried out is likely to be higher; In a recent questionnaire to practices which produced a return of 50%, 450 health checks had been completed up to December 2016 Historically, quarter 4 is when the majority of health checks are completed. Work to
support practices to work to the 70% target (and 75% by 2020) continues and the role of
the community LD link nurse within surgeries is beginning to demonstrate some effective
joint working. Contact with practices who have outstanding claims from 2015-16 is being
made. This will enable practices to amend their claim and receive payment for completion
of the health check.
key issues in quarter 3 Actions / timescales / learning
Annual self-assessment : A self- assessment working group continues meet quarterly. The completion of a self-assessment was not required for 2016/17. They will now be completed every 2 years. More detail about the 2017/18 assessment will be provided in the spring. Local data including screening was released by Improving Health and Lives (Public Health England) in December 2016, however this requires further analysis. In the meantime, the group are concentrating on refreshing a questionnaire that is sent to 1000 people with a learning disability in preparation for its distribution
Dementia project: Work continues to develop a service pathway for people with a LD who develop dementia. A further workshop has looked at how mainstream dementia services offer support where a person has a learning disability. Following last years’ HPFT LD commissioning for quality and innovation (CQUIN) involving the application of the ‘green light audit’ tool, audits from mainstream dementia services have been reviewed. Post-diagnostic support services have been re-procured and the new provider, together with the LD nurses, is participating in a number of training opportunities. 1) A 1-day course about supporting people with LD and dementia and/ or 2) virtual dementia tours. In addition, an introductory guide to dementia has been put into easy-read and is currently being reviewed prior to distribution.
Improving access topsychological therapies(IAPT)
Colleagues from Herts Partnership foundation trust (HPFT’s) IAPT provision are due to meet with the community learning disability nurses in order to provide the nurses with information about the service. Once the team have a better understanding of IAPT, it is anticipated that referrals will be made by the team where appropriate. In the meantime, the IAPT service has registered to be accredited to the purple star programme across the county. Training is imminent and will start with the Decorum hub.
Flu immunisation: Between September and December 2016, the LD community nurses held a flu jab campaign. The nurses developed materials including an easy-read invite and capacity documents for practices to be sent to the individuals/ carers. Unfortunately feedback from self-advocates indicates that this information was not widely distributed. A request to establish whether there has been an increase in take up of the flu jab amongst people with a LD has been made to the regional immunisation service. Data from ‘mede-analytics’ to understand admissions to hospital September – December 2016 for respiratory conditions has been received and is being analysed against the general population and last year’s data. In order to acquire local data directly from practices, a questionnaire was distributed. 50% of practices returned the questionnaire; details of number of flu vaccinations completed will be reported on Q4’s report.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
14. System resilience progress report:
LDB
Work
stream
Programme start date (Monday): 03/03/16
This week and next week : u
Sect. Ref. Task / milestonePlanned
Start
Planned
complete
Actual
completeDays Complete
Max End
Date
Comment
Date
16 16 Target =0.5 % of improvement to 95%
16 16.07 Milestone 1 - 0.1% achieved 01/08/16 31/08/16 30 no 31/08/16
16 16.08 Milestone 2 - 0.25% achieved 00/01/00
2 16.09 Milestone 3 - 0.5% target achieved 00/01/00
Programme start date (Monday): 03/03/16
This week and next week : u
Sect. Ref. Task / milestonePlanned
Start
Planned
complete
Actual
completeDays Complete
Max End
Date
Comment
Date
4 4 Target = 2.0% of improvement to 95%
4 4.07 Milestone 1 - 0.5% achieved 18/07/16 31/07/16 31/07/16 13 Yes 31/07/16
4 4.08 Milestone 2 - 1.25% achieved 18/08/16 31/08/16 31/08/16 13 Yes 31/08/16
2 4.09 Milestone 3 - 2.5% target achieved 19/09/16 30/09/16 11 No 30/09/16
Programme start date (Monday): 03/03/16
This week and next week : u
Sect. Ref. Task / milestonePlanned
Start
Planned
complete
Actual
completeDays Complete
Max End
Date
Comment
Date
7 7 Target = 0.5% of improvement to 95%
7 7.05 Milestone 1 - 0.1% achieved 10/03/16 10/04/16 10/03/16 0 Yes 10/04/16
7 7.06 Milestone 2 - 0.25% achieved 10/04/16 10/06/16 10/04/16 0 Yes 10/06/16
7 7.07 Milestone 3 - 0.5% target achieved 10/06/16 10/08/16 61 TBC 10/08/16
This project is under review and will be updated at the next report..
Comment / Constraints / Remedial actions
The red to green implementation had taken place during the perfect week which
had taken place on week of 7-13 December 2016 and had been considered a
success. The full report has been received and the perfect week will be repeated
in April in preparation for the Easter period.
The turnaround figures remained static and the project is proceeding.
Comment / Constraints / Remedial actions
Project ref: RP 16
3.
Am
bu
lan
ce R
esp
on
se
Pro
gra
mm
e
(Do
D a
nd
co
din
g p
ilo
ts)
4.
Imp
rov
ed
Pa
tie
nt
Flo
w
Project owner:
Clinical lead:
Project ref: RP 4
Project owner: EEAST / HVCCG / WHHT
Clinical lead: Dr David Gaunt
Recovery project
4.
Imp
rov
ed
Pa
tie
nt
Flo
w
Project name: 4th HALONumber of project tasks/milestones: 0
Comment / Constraints / Remedial actions
Project name: Lead Consultant / Early DischargeNumber of project tasks/milestones: 2
Clinical lead:
Project name: Ambulance turnaroundNumber of project tasks/milestones: 0
Project owner:
Project ref: RP 7
BACK

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
14. System resilience progress report (continued):
Programme start date (Monday): 03/03/16
This week and next week : u
Sect. Ref. Task / milestonePlanned
Start
Planned
complete
Actual
completeDays Complete
Max End
Date
Comment
Date
8 8 Target = 0.5% of improvement to 95%
8 8.05 Milestone 1 - 0.1% achieved 30/03/16 30/04/16 30/04/16 31 Yes 30/04/16
8 8.06 Milestone 2 - 0.25% achieved 30/04/16 30/05/16 30/05/16 30 Yes 30/05/16
8 8.07 Milestone 3 - 0.5% target achieved 30/05/16 30/07/16 61 No 30/07/16
Programme start date (Monday): 03/03/16
This week and next week : u
Sect. Ref. Task / milestonePlanned
Start
Planned
complete
Actual
completeDays Complete
Max End
Date
Comment
Date
5 5 Target=2.5% of improvement to 95%
5 5.12 Milestone 1 - 0.5% achieved 06/05/16 14/07/16 69 14/07/16
5 5.13 Milestone 2 - 1.5% achieved 07/05/16 14/08/16 99 14/08/16
5 5.14 Milestone 3 - 2.5% target achieved
08/05/16 30/09/16 145 30/09/16
Programme start date (Monday): 03/03/16
This week and next week : u
Sect. Ref. Task / milestonePlanned
Start
Planned
complete
Actual
completeDays Complete
Max End
Date
Comment
Date
11 11 Target = % of improvement to 95%
11 11.05 Milestone 1 - 0.1% achieved 30/06/16 30/06/16 30/06/16 0 Yes 30/06/16
11 11.06 Milestone 2 - 0.25% achieved 30/06/16 01/08/16 01/08/16 32 Yes 01/08/16
11 11.07 Milestone 3 - 0.5% target achieved 01/08/16 01/09/16 31 TBC 01/09/16
The twilight team is in place and is improving.
5.
Imp
rov
ed
Dis
cha
rge
5.
Imp
rov
ed
Dis
cha
rge
4.
Imp
rov
ed
Pa
tie
nt
Flo
w
Project owner: WHHT / HVCCG / HCT / HPUFT / HCC
Clinical lead: Dr Tammy Angel
The projects aligned to this work stream are still without any plans submitted to
the programme team. We have collated responses from previous requests for this
information but need to re-issue in order to have sight of timescales intended
impact and contribution toward the recovery plan.
While there is social work presence on site 7 days a week, there is still no
formal 7 day team. The implementation of this is now delayed until Feb '17
continuing health care (CHC) Review to be completed with actions by Dec '16
although increase in staffing not expected until March '17. This project is still
underway and staffing is in line with expectations.
Comment / Constraints / Remedial actions
Comment / Constraints / Remedial actions
Project name: Delay transfer of care (DToC) ReductionNumber of project tasks/milestones: 0
Project ref: RP 11
Comment / Constraints / Remedial actions
Due to operational pressures, Herts County Council are not reporting at this time.
Project owner:
Clinical lead:
Project ref: RP 8
Project name: Twilight TeamNumber of project tasks/milestones: 0
Project ref: RP 5
Project name: Stranded PatientsNumber of project tasks/milestones: 0
Project owner:
Clinical lead:

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
15. Continuing health care (CHC): quarter 3 report:
The national framework for NHS continuing healthcare and NHS funded nursing care sets out the principles and processes for
determining eligibility; the table below provides an overview of the framework and the progress update on the relevant
standards-
Status Actions Lead Evidence already in place to support standard Links to KPI Timeline
A
As part of the wider CHC improvement
plan the team will be developing a
standard operating procedure to ensure
consistency in process and assessment
Tracey
Brown
Commissioning policy and redress policy are
compliant with the national framework for
NHS CHC. Regular peer supervision is
arranged within the nurse assessors diaries to
discuss complex assessments.Ongoing
A
As part of the wider CHC improvement
plan the team will provide in reach to
the hospital team to support complex
discharges
Lucia
Contrino
A daily tracker is in place to manage all
referrals received. A commissioning process is
in place to ensure timely placements.
Ongoing
Y
Further work needs to take place
working with the children and young
peoples team to align processes
Tracey
Brown
The process for managing transition between
children and adults is articulated in the
commissioning policy Ongoing
Y
Bespoke training for clinical and non-
clinical staff forms part of the CHC
internal improvement plan. to be
commissioned.
Tracey
Brown
All staff to undertake CHC eLearning as part of
their induction plan. - training and
development is part of the wider CHC
improvement plan Ongoing
Status Actions Evidence already in place to support standard Links to KPI Timeline
Y
Commissioning policy will be updated
as part off the wider CHC improvement
plan.
Lucia
Contrino
The process for agreeing funding on receipt of
an appropriate fast track is articulated in the
commissioning policy
Ongoing
A
Regular audits are part of the wider CHC
improvement plan to ensure that fast
track referrals are appropriate.
Beau Klusko
Ongoing
Status Actions Evidence already in place to support standard Links to KPI Timeline
G
Care plan templates are being updated
as part of the wider CHC improvement
plan.
Nicola
Wilson
All patients have a written care plan saved
locally with the CCG in instances where the
patient remains in their own home. Standard is
met.
Y
Care plan templates are being updated
as part of the wider CHC improvement
plan.
Nicola
Wilson
Ongoing
Y
The process for timely authorisation of
care packaged is articulated in the
commissioning policy however there is
insufficient capacity re providers, we
are looking at options for block beds.
Lucia
Contrino
Ongoing
A
Work is in progress to develop a
procurement strategy to support the
commissioning of specialist packages.
Lucia
Contrino
Ongoing
A
x 4 band 7 nurses are to be recruited to
support case management intervention
for all CHC funded patients
Nicola
Wilson
A senior clinical lead has been appointed to
coordinate and lead the clinical team
Ongoing
Y
a backlog review team have been
commissioned to review all overdue
reviews between Jan - Mar 2017 - a
rolling programme of review activity
has been developed to run alongside
the backlog project
Nicola
Wilson
Historical fast tracks and high cost packages
were all reviewed in 2016 and completed
3) CHC reviews should
be undertaken after 3
months from the
initial decision and
annually thereafter
Ongoing
CHC assessment and decision making framework
Assessment and decision making; lawful, high quality and timelyStandard
Standard A1- Ensuring policies
are compliant with the
national framework to ensure
consistency of assessment
across the NHS
Standard A2: Assessment
process to facilitate timely
discharge from hospital and
specialist centres
1) Eligibility decision
needs to be made
within 28 days and
4. All applicants are
being notified of the
outcome following
eligibility decision
within 48 hours of
decision being made
2) Fast track decision
within 48 hours
Standard C6: Annual reviews
to include care package is
appropriate
Standard
Standard C1- all individuals in
receipt of NHS CHC have a
written care plan
Standard C2: Care planning is
person centred
Standard C3: Timely plan I
package put in place once
decision is reached
Standard C4: Appropriate
specialist package in place
Standard C5: Case
management arrangements in
place
Care and support
Standard A3: Transition
between children and adults
well managed
Standard A4: Trained &
competent assessors
Fast track
Standard
Standard F1-funding agreed
on the receipt of an
appropriate fast track
Standard F2: CCGs should
carefully monitor use of the
fast track tool and raise any
specific concerns with
clinicians, teams and
organisations
Coloured Compliance Status Indicator
Status Indicators are assigned by authorised Users to indicate their assessment of the current Compliance position of the service against the CHAT's Standards.
Green: Evidence available at the time of assessment shows that the Standard is met. Yellow: Evidence available at the time of assessment shows that the Standard is mostly met, or there is not sufficient Evidence to demonstrate the Standard is met. The impact on people who use services, visitors or staff is low. The action required is minimal. Amber: Evidence available at the time of assessment shows that the Standard is mostly met, or there is not sufficient Evidence to demonstrate the Standard is met. The impact on people who use services, visitors or staff is medium. The action required is moderate. Red: Evidence available at the time shows that the Standard is at risk of not being met or there is no available Evidence that the Standard is met. The impact on people who use services, visitors or staff is high. Action is required quickly. Grey: The Grey icon indicates that no Status has been set for the item or that it is not applicable to the service.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
15. Continuing health care: quarter 3 report:
The dashboard below highlights the priority key performance indicators for continuing health care:
Indicator
How indicator
maps to CHAT
standard
Threshold Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16
Last 12
Months CommentsAccountable
director
Responsible
manager
Clinical
lead
1. Eligibility decision
needs to be made within
28 days
A1, A2 100% 83.0% 87.0% 76.0% 88.0% 60.0% 68.0% 95.0% 57.0% 70.0%
The KPI is reflective of activity undertaken within the internal CCG CHC
team only. Herts County Council (HCC) manage the assessment of
community cases, and Hertfordshire Partnership Foundation Trust (HPFT)
manage assessments for mental health (MH) patients, previous reports
have only captured in house activity targets as there are no KPIs with
both our provider organisations to provide this information. Therefore the
data presented is reflective of cases managed within the team within
nursing homes. In April 2017 the community function will move in house
and reporting will be possible for all adult (non MH) CHC assessments.
.
2. Fast track decision
within 48 hoursF1,F2
National
93%92.0% 97.0% 88.0% 97.0% 72.0% 91.0% 100.0% 100.0% 99.0%
The CHC team has worked hard in the last quarter to develop processes
for agreeing fast tracks, we have met with refers and will continue to do
this. We are also in the process as part of the wider CHC improvement
plan to redevelop care plans and supportive information to assist with
commissioning care packages following fast track approval
3. CHC Reviews should be
undertaken after 3
months from the initial
decision and annually
thereafter
C6 100% 5.40% 6.60% 5.00%
The CHC service have not had clinical capacity to undertake all reviews
due to vacancies within the structure, and have been prioritising review
activity based on clinical need. The service has a backlog of reviews and
have commissioned a backlog team to clear these between Jan - March
2017. 11% in Q3 is descriptive of 43 reviews undertaken.
4. All applicants are being
notified of the outcome
following eligibility
decision within 48 hours
of a decision being made
A1 100% 84% 80% 76% 71% 80% 82%
The CHC team are reviewing all administration processes as part of the
wider CHC improvement plan, to include the review of template letters
and following feedback from patients and families of what "they need to
know" within an eligibility letter and sign posting to social care. Timeline
for completion 31/03/2017
Tracey
Brown
Dr
David
Buckle
Continuing health care key performance quarterly report.
Diane
Curbishley
0.00%
81.00%
11.00%
16. CCG IAF (improvement assessment framework) 2016-2017
NHS England CCG IAF January 2017 dashboard with a summary table that shows the 6 lowest and 6 above national average KPIs: comment comment
Provision of high quality care Maternal smoking at delivery
Cancer patient experience. Cancer diagnosed at early stage
Children and young people`s mental health
services transformation
NHSE responded to query
that this rating does not
reflect Q3 data where
improvements will be seen
Percentage of children aged 10-
11 classified as overweight or
obese
2014-2015 data
HVCCG 26.9% and England
average is 33.2%
Women’s experience of maternity services
Neonatal mortality and
stillbirths
2014-15 data
HVCCG 4.2 and England
average is 7.1
Digital interactions between primary and
secondary care Quality life of carers
2016 data
HVCCG 0.83 and England
average is 0.80
Primary care work force
Patient experience of GP
services
2016 Data
HVCCG 88.7% and England
average is 85.2%
See 6 clinical priority report
6 lowest performance quartile nationally 6 KPIs are above national average
Requested from NHSE the
England average to clarify
how this has been
benchmarked
Requested from NHSE the
England average to clarify
how this has been
benchmarked

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Full CCG improvement assessment framework: NHS England latest report

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
16. CCG IAF (improvement assessment framework) 2016-2017 (continued)
Six clinical priorities:
Clinical
priority area
Overall
ratingQ3 comments
Clinical
lead
Accountable
director
Responsible
programme/
manager
GP/ locality engagement/ communication update Q3
54.60% 82.3%- 69.40%
CancerNeeds
improvement
8.5
Dementia
Estimated diagnosis rate for
people with dementia.
of patients diagnosed with dementia whose
care plan has included receiving a face-to-
face review in the preceding 12 months.
New of cases of
cancer
diagnosed at
stage 1 and 2 as
a proportion of
all new cases of
cancer
diagnosed.
of people with
an urgent GP
referral
having first
definitive
treatment for
cancer within
62 days of
referral.
of adults
diagnosed with
any type of
cancer in a year
who are still
alive one year
after diagnosis.
of responses ,which were
positive to the question
"Overall, how would you
rate your care?".
79.70%
Nov data from NHS England for estimated diagnosis rate for people with dementia is 64.5%
Latest Jan data from NHS England for estimated diagnosis rate for people with dementia is 64.8%- see dementia report
for further update
Dementia care planning and post-diagnostic support- No national or local threshold. Annual reviews are in the local
incentive scheme, practice visits are being undertaken regarding case finding and updates on post diagnostic care
pathways.
2016-2017 CCG assurance framework
Herts valleys CCG rating for the six clinical priority areas
David Buckle
/Charles Allen
Planned and
primary care/ Avni
Shah
David Buckle
/Charles Allen
Mental Health
/Simon Pattison
Performing
well
79.70%
Dementia care planning and
post-diagnostic support
64.5% Nov 2016
Dr Phil
Sawyer
Dr Mark
Allen
Indicator ratings
1) CCG improvement assurance framework quarter 1 ,2 and 3 reported within the
integrated, quality, performance and finance report at quality and performance
committees.
2) GP forum – Q3 report to be presented at May forum
3) interloc meeting discontinued . Q3 report to go to the March primary care working
group ; the 4 clinical chairs and medical director attends and following meeting to be
cascaded to localities
4) Local incentive scheme for 2017-2018 Inclusion of the following KPIs within the
current CCG assurance framework where general practice has a direct influence on:
• Maternity: Percentage of children aged 10-11 classified as overweight or obese
• Diabetes patients that have achieved all the NICE recommended treatment targets:
Three (HbA1c, cholesterol and blood pressure) for adults and one (HbA1c) for children
• Diabetes patients that have achieved all the NICE recommended treatment targets:
Three (HbA1c, cholesterol and blood pressure) for adults and one (HbA1c) for children
• Diabetes: People with diabetes diagnosed less than a year who attend a structured
education course
• Learning disability: Proportion of people with a learning disability on the GP register
receiving an annual health check- direct enhanced service (DES) and outcome of general
medical services (GMS) contract negotiation 17/18 is that LD increase payment of £116-
£140 per patient for a health check. New developed template.
• Dementia care planning and post-diagnostic support - TBC
5) Clinical leads aligned to 6 priority areas and responsibilities has been captured within
the clinical lead job description
6) Standard item on the agenda and clinical leads to provide a progress update at the
quarterly clinical leads meetings, commenced from 27 October, next meeting will be in
May.
7) DXS :Plans to priorities pathways aligned to the 6 clinical priority areas to be
developed within the DXS template. Standard item on the DXS steering group agenda
and quarterly updates to be provided. Facilitators have provided support to practices to
use the DXS templates .
DXS work stream update
Diabetes - DXS cannot influence how the education programmes feed information back
to GP practices, but by including PIL explaining value of education it may encourage
more people to attend.
20170127 - Desmond Patient information leaflet (PIL) to be added to DXS
Cancer - further develop cancer pathways, and keys signs to watch out for in all clinical
pathways.
Cancer 62 day - GPs are prompted to print out the 2ww information leaflet from DXS.
This will hopefully reduce number of DNAs or rescheduled appointments that impact on
the achievement of this target.
LD –clinical lead is developing series of pathways to support improved care for people
with learning disabilities to upload on DXS.
Dementia -Inclusion of early memory diagnosis and support service (EMDASS) referral
form on DXS
20170127 -Referral form agreed with provider. Currently in build - scheduled for
14/02/17
All pathways refer to any additional reasonable adjustments that may be required to
support people with additional needs to be supported in the community wherever
possilbe.
8) subcommittee of primary care group ; Joint NHS England/ HVCCG committee to raise
on the 17/2/17 the communication approach of quarterly updates and the agreement
for the Q2 report to be cascaded to practices.
9) LIS action plan update : Dacorum 1 practice has increased by 10%= 62% 1 practice
reduced by 4% - visit booked by Dementia programme lead.
Watford and Three rivers- 1 x dementia actio plan
St albans and harpenden 3 practices; 1 practice has commenced an memory screening
service in Oct 2016
No further data update available from NHS England.
The data on 1 year survival time period reflects annual figures relating to patients diagnosed in 2013.
Update from cancer clinical lead :
HVCCG have therefore achieved 8.5/10 or 85% compared to national average of 87% or 8.7/10. The questions in the survey
relating to primary care where reassuringly positive for example 83% said they had only seen the GP once or twice before
referral compared to national average of 76%. And 73% said GP practice staff definitely did everything they could to support
patients compared to 63% national average. Areas where the survey was particularly weak were for example; only 695 of
patients said they were not talked about by hospital staff as if they were not there compared with national average of 81%.
Also only 9% of patients recalled being offered research opportunities compared with 28% national average. WHHT have
produced a report on this survey and devised an action plan which is being led by Michelle Sorley, lead cancer nurse to
implement this. The latest figure for Q2 16/17 shows that HVCCG is achieving 84.5% compared with 82.3% England with a
target of 85%. The trust has action plans which includes new diagnostic capacity to achieve this. The data of 69.4 for one
year survival refers to 2013 data which at the time compared with a national average of 70.2%. We hope that picking up
cancers earlier will show this percentage improving over future years.
NB:62 day : latest 92.4% Dec (CCG patients view) therefore performance compliant

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Six clinical priorities: quarter 3 report – (continued)
Clinical
priority area
Overall
ratingQ3 comments Clinical lead
Accountable
Director
Responsible
programme/
manager
GP/ locality engagement/ communication update Q3
56.50%
Q3 comments
2016-2017 CCG assurance framework
Herts valleys CCG rating for the six clinical priority areas
David Buckle/
Diane
Curbishley
Learning disability/
Simon Pattison
Dr Kirsten
Lamb
David Buckle
/Charles Allen
Not calculated
of diabetes patients have achieved
all the national institute for health
and excellence (NICE) recommended
treatment targets.
of people with diabetes
diagnosed for less than a
year who attended a
structured education course.
of GP practices
that
participated in
the national
diabetes audit.
Rate of inpatients per million GP
registered adult population for each
Transforming Care Partnership
(TCP). CCGs are then assigned the
score of the TCP they belong to.
of people with a learning disability who are
on the GP register and receiving an annual
health check during the year. Measured as a
percentage of the CCG’s registered learning
disability population.
Learning
disabilities.
Needs
improvement
Dr Nicola
Cowap
Please refer to the learning disability quarter 3 report for progress update
DiabetesNeeds
improvement
40.60%
64
3.90%
Indicator ratings
Comments as above
Planned and
primary care/ Avni
Shah
No further data update available from NHS England.
Structured education programme update
The recently released quality outcome framework (QoF) data for 2015/16 HVCCG GPs referred 94% of newly diagnosed
patients to a structured education programme, the challenge has been that as the data is pulled from the national diabetes
audit (NDA) on attendance GP practices do not currently code for this in practice so the `below` is not an accurate reflection
of the number of people who attended; in reality we are looking at 40 -50% of patient having attended. As the NDA doesn’t
look at provider information on who attended it does not pull this information.
Actions in place:
• HVCCG are working towards getting this coded within GP practice systems, but as NDA has annual changes in the data, this
will not be seen until the 2016/17 as the audit is completed this time next year. Update from clinical lead : HCT should be
sending out a letter when patients are discharged from DESMOND/fail to attend indicating how this should be coded. HVCCG
are raising awareness of this with primary care at forthcoming locality meetings, and asking for practices co-operation so
that NDA data more accurately reflects SE attendance in the future.
• Structured education Is being addressed at the structured education task & finish groups.
• HCT have conducted an audit no feedback as yet from HCT regarding the results of the audit, the next meeting of this group
is scheduled for 1st March.
• HVCCG are launching the DESMOND leaflet at the locality meetings and the GP newsletter that will be sent out imminently
• HVCCG are working with our provider of diabetes education sessions to ensure that details on who has attended education
sessions is fed back to primary care and recorded in the primary care patient record and thus included as part of the NDA
from where this statistic is gathered-
Results for the most recent NDA audit data collection. This relates to 2015/16 data collection so it is not very up-to-date and
does not really reflect any of the recent changes, and also only about 60% of practice have participated:-
Type 1 Rx targets: HVCCG recent audit 14/15 audit England 15/16
23% 22.2% 18.3%
Type 2 Rx targets: 40.6% 42.4% 40.4%
Achievement of all the national institute for health and excellence (NICE) recommended treatment targets update .
Improvement in treatment targets update comes via the NDA and Qof . Recent NDA data suggested that HVCCG is doing
better than the England average, and there has been slight improvement
Achievement of treatment targets is being addressed through the long term conditions specification which incentivised
practices for following up newly diagnosed patients, through QoF and also through the new service which will facilitate timely
access to specialist advice and our efforts to up skill primary care e.g. annual conference, diabetes web-site and planned
rolling programme of education.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Six clinical priorities: quarter 3 report – (continued)
Clinical
priority areaOverall rating Q3 comments Clinical lead
Accountable
Director
Responsible
programme/
manager
GP/ locality engagement/ communication update Q3
76.1 63.7 4.2
Q3 comments
25%70% 88%
Children and
young people’s
mental health
services
transformation
Crisis care
and liaison
mental
health
services
transforma
tion
Out of area
placements for
acute mental
health
inpatient care
David Buckle/
Charles Allen
Mental Health
/Simon Pattison
Dr Sara Khan
Dr Mark Allen
Indicator ratings
2016-2017 CCG assurance framework
Herts valleys CCG rating for the six clinical priority areas
57.40%78.1%- Nov 2016
England baseline 77.2%
Maternity Performing well
6.50%
Mental health
The score out of
100 for women’s
experience of
maternity services
based on the 2015
care quality
commission (CQC)
national maternity
services survey.
The score out of
100 for choices
offered to
women in
maternity
services based
on the national
maternity
services survey.
The rate of
stillbirths and
deaths within 28
days of birth per
1,000 live births
and stillbirths,
reported at CCG
of residence
level by calendar
year.
of women who were
smokers at the time of
delivery.
50.10%
IAPT recovery rate
Performing well
of people who were initially
assessed as “at caseness”, attended
at least two treatment contacts, are
coded as discharged and are
assessed as moving to recovery.
of people with first episode of psychosis,
starting treatment with a NICE-
recommended package of care and treated
within 2 weeks of referral.Comments as above
David Buckle/
Diane
Curbishley
Children, young
people and
maternity/ Liz Biggs
WHHT maternity visit on 8th December 2016- Please refer to quality stand alone document for update on Maternity visit
8th of December.
Smoking at time of delivery:
Specialist staff from Hertfordshire Stop Smoking Service (HSSS) provide monthly training for midwifery staff at WHHT,
including skills-based training in carbon monoxide monitoring and communications. A traffic light system is used to record
smoking status and subsequent actions in all women’s hand-held notes and midwives are encouraged to refer smoking
women and their partners to HSSS at every opportunity. Patient information is provided on HSSS, the love your bump
campaign, e-cigarettes and smoke free homes and cars. HSSS provide flexible, dedicated and intensive support to pregnant
women and their families, including information on e-cigarettes and the use of nicotine replacement therapy. They aim to
feedback to the midwife to ensure continuity of care. The quality of pregnancy stop smoking services in Hertfordshire has
increased; in 2014/15 the success rate of quitting successfully was 38%, in 2015/16 it was 43%.
Carbon monoxide monitoring will be repeated by midwives between 28 and 36 weeks gestation to provide a further
opportunity to identify and refer smokers for intensive specialist support.
Latest data reported from NHS England Nov 2016 78.1% for of people with first episode of psychosis, starting treatment with
a NICE-recommended package of care and treated within 2 weeks of referral. HVCCG now above England baseline figure of
77.2%
Episode of psychosis- work with HPFT to agree a funding model that moves towards full NICE compliance over 2017-18 and
2016/19 whilst delivering the 2 week referral target – The early intervention in psychosis (EIP) funding for HVCCG has been
agreed with HPFT into the 17/18 contract to deliver full nice compliance at £600,000. Number of new cases of psychosis
served year to date 93%.
In previous years, there has been a large push on promotion into Q4 to ensure the access target has been reached, the over
activity year to date can be viewed as ‘sessions in the bank’ to reduce the amount of resource required to promote the
service into Q4, enabling HPFT to focus their clinical resource on both access and recovery.
CCG improvement and assessment framework (IAF) MH transformation self-certification quarterly- UNIFY upload by
integrated health and care commissioning team (IHCCT) Q3 19th January 2017
This sets out the plans that are in place to implement the delivery of the set requirements for the following 3 KPIs: See HPFT
quarter 3 success and challenge report for an update
1- Children and young people’s mental health services transformation
2- Crisis care and liaison mental health services transformation
3- Out of area placements for acute mental health inpatient care
NB: No thresholds in place to date as the aim is to collate data nationally prior to setting targets.
Provision local data has the three monthly rolling average improving access to psychological therapies (IAPT) recovery rate at
52.8% in November of people who were initially assessed as “at caseness”, attended at least two treatment contacts, are
coded as discharged and are assessed as moving to recovery.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
17. Quarterly community provider success and challenge report: quarter 3 report
HPFT quarterly 3 report : success, challenges and 5 year view update
Key success in quarter 3 :
key challenges in quarter 3 : Actions / timescales / learning
1. EMDASS
2. Routine referrals tocommunity mentalhealth team meeting28 day wait
The early memory diagnosis and support service (EMDASS) has continued to offer up to 50% extra diagnosis sessions per week throughout Q3 in order to drive down the secondary waits from the initial nurse assessment. Despite this, there remained at the end of Q3, 260 people waiting to see a consultant, 120 of these had been waiting more than 12 weeks. The (did not attend) DNA rate for these sessions is over 20%. The service is undergoing an internal review to maximise efficiencies to drive down these waits with proposals due to commissioners in February.
Recent information over pressures on single point of access (SPA) and the impact on the national 28 day waiting time targets, HPFT presented a number of forums (GP leads 25 Jan 2017 and HPFT quality review meeting 26 Jan 2017) indicating the increase in referrals year on year. HPFT to undertake a review of processes, on average over the last 24 months, 34% of all referrals to adult community teams have been taken on for treatment by community initial assessment (IA) teams. Some of these referrals may have been taken on by other teams; and for a number of those not taken on, the triage and/or assessment may have been appropriate. However, the low take-on rates poses the question of whether these referrals are appropriate for secondary care. Whilst HPFT are clear that a single point of access is the correct access model, the utilisation of the service has become overwhelming, particularly as SPA currently has 40% workforce vacancy rate, due to retirement and people having worked there for more than 3 to 5 years. HPFT have proposed an action plan to make efficiencies in four areas:
Review of the telephone system, to move to a consistent core managementsystem, providing a menu of options for GPs and a more sophisticated systemwith greater data analysis potential.
Provide a range of options to GPs to reduce volume of referrals through SPA,such as exploring a “shared care” model through locality hub and spokemodels.
Analysis of frequent attenders/referrals via SPA.
Review of the governance and data collection requirements for all referrals /initial assessments
Key successes: 1. IAPTRecovery rate YTD 54.3% from provisional local data (50% target)
Access rate as projected moving from under-performing to meeting target from validated data in October 3.80% and continuing in excess of 4.0% in November from provisional local data. (3.75% 3 monthly rolling avg). The access target is on track with local service projections as access increases in Q3 and Q4 to these services.
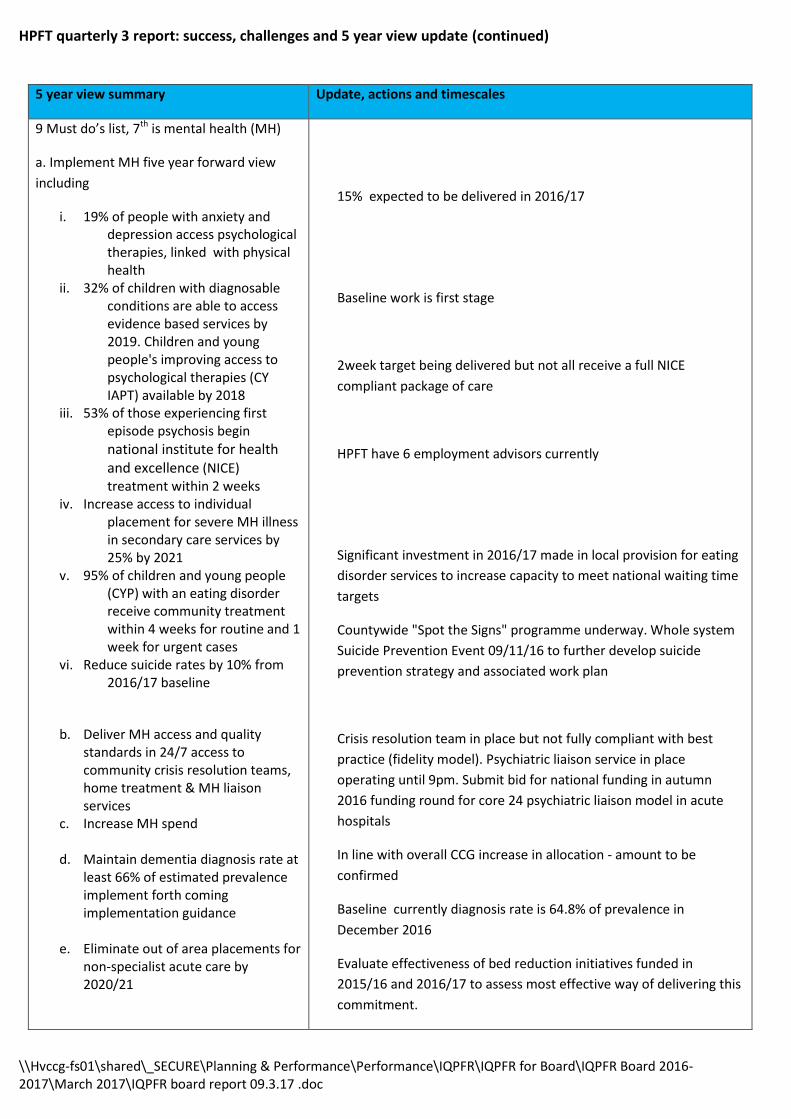
\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
HPFT quarterly 3 report: success, challenges and 5 year view update (continued)
5 year view summary Update, actions and timescales
9 Must do’s list, 7th is mental health (MH)
a. Implement MH five year forward view
including
i. 19% of people with anxiety anddepression access psychological therapies, linked with physical health
ii. 32% of children with diagnosableconditions are able to access evidence based services by 2019. Children and young people's improving access to psychological therapies (CY IAPT) available by 2018
iii. 53% of those experiencing firstepisode psychosis begin
national institute for health and excellence (NICE) treatment within 2 weeks
iv. Increase access to individualplacement for severe MH illness in secondary care services by 25% by 2021
v. 95% of children and young people(CYP) with an eating disorder receive community treatment within 4 weeks for routine and 1 week for urgent cases
vi. Reduce suicide rates by 10% from2016/17 baseline
b. Deliver MH access and qualitystandards in 24/7 access tocommunity crisis resolution teams,home treatment & MH liaisonservices
c. Increase MH spend
d. Maintain dementia diagnosis rate atleast 66% of estimated prevalenceimplement forth comingimplementation guidance
e. Eliminate out of area placements fornon-specialist acute care by2020/21
15% expected to be delivered in 2016/17
Baseline work is first stage
2week target being delivered but not all receive a full NICE
compliant package of care
HPFT have 6 employment advisors currently
Significant investment in 2016/17 made in local provision for eating
disorder services to increase capacity to meet national waiting time
targets
Countywide "Spot the Signs" programme underway. Whole system
Suicide Prevention Event 09/11/16 to further develop suicide
prevention strategy and associated work plan
Crisis resolution team in place but not fully compliant with best
practice (fidelity model). Psychiatric liaison service in place
operating until 9pm. Submit bid for national funding in autumn
2016 funding round for core 24 psychiatric liaison model in acute
hospitals
In line with overall CCG increase in allocation - amount to be
confirmed
Baseline currently diagnosis rate is 64.8% of prevalence in
December 2016
Evaluate effectiveness of bed reduction initiatives funded in
2015/16 and 2016/17 to assess most effective way of delivering this
commitment.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
HPFT quarter 3 report: success, challenges and 5 year view update (continued)
HCT quarterly report : successes and challenges Key success in quarter 3 : Oct – Dec 2016
key challenges in quarter 3 : Actions / timescales / lead /learning
1) Staff turnover and absence rate overthreshold.
2) Average length of stay in HCTcommunity hospital for non-stroke patients (trust view)
3) Average length of stay in HCTcommunity hospital for non-stroke patients - HVCCG patient
4) Community hospitals average lengthof stay in HCT community hospital non-stroke rehab pathway only- HVCCG patient
5) Children’s community nursing is overperforming which is affecting service delivery
1) HCT undertaking various options, with staff retention plan, including
“What makes you stay” survey for staff in hot spot areas.
2-4) The draft “Red to Green” plan was discussed in detail at the
transforming community services meeting on 6th February and will be
discussed further at the contract review meeting on 21st February.
The plan details various work streams, including learning from previous
schemes undertaken in acute trusts.
The overall aim of this plan is reduce length of stay, facilitate earlier
discharge or discharge on the estimated on the planned discharge date.
5) Deep dive into Children’s community nursing to come to the contract
review meeting on February 21st to look at options to manage demand and
maintain quality
Improvement assessment framework summary
Update, actions and timescales
CAMHS: Children and young people’s mental health services transformation
Crisis: crisis care and liaison mental health services transformation
Out of Area Treatments (OATS): Out of area placements for acute mental health inpatient care
- 4 Collaborative commissioning plans for tier 4 –met with NHS England twice and further meeting on 9th Jan to make further progress
- 5 Workforce plan –have some detail in the CAMHS transformation plan but not the fully worked up detail with Health Education England (HEE) about future training
- 1a and 1c - Not compliant on having a funded plan to deliver core 24 liaison psychiatry in acute hospitals – the bid currently being discussed would allow this
- 1d – Rapid assessment, interface and discharge (RAID) service meets these response times during the times it is operating but not outside those times. Again the bid for national funding discussed above would resolve this
- 2c Crisis resolution home treatment team fully staffed in line with national expectations – HPFT to baseline themselves against national expectations in 2017/18 to see how big the gap is (operating plan requirement is to meet this target by April 2019)
- 2e – crisis resolution and home treatment (CRHT) collecting outcome data – this is done in part but links to target above
- Partially compliant on having a plan in place to reduce out of area placements across all bed types. This is delegated to HPFT and they have plans to do this but this needs to be expanded to specifically cover all bed types.
Key successes: 1) Musculoskeletal (MSK) waiting times on a trajectory of improvement, with a 25% reduction in 18 week waits sinceOctober. 2) Community hospital - an improving percentage of patients having a planned discharge before midday3) Rapid response –EEAST to encourage direct referrals to the service by emergency care practitioner (ECP)’s andparamedics.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
HUC quarterly report : successes and challenges
Key success in quarter 3 : Oct- Dec 2017
key challenges in quarter 3 : Actions / timescales / lead /learning
1)Home visits
2) Urgent face to face
consults
HVCCG request for CCG
patient view level data
Action plan update: At the 9th February contract review meeting, HUC presented a paper on performance challenges and solutions. The plan covered 111 and out of hours. The following areas were broadly covered:
Challenges around staff retention, recruitment and sickness – with plans tomanage each area
Training – development of flexible courses and learning materials, and solvingissues related to part-time having to undertake full-time training
Rota patterns – adjusting rotas so that they match demand – eg more staffavailable at peak times
Managing GPs – recruitment and performance management
Actions on the plan run up until November and will be monitored through the
contract review meeting.
Home visits/urgent face to face consultations – this remains an issue and there has
been historical performance below expectation. It was explained this was down to
current structures and processes, but with newly procured integrated urgent care
(IUC) beginning on June 29th, performance will monitored going forwards with a
revised model.
Confirmation from ENHCCG that go-live for patient level data will be 29th June 2017
18. WHHT quality improvement plan: n/a
Key successes: 1) Clinical details of patients sent to practices by 8am next working day. - Continue to perform above ›95%2) Routine face to face consults within 6 hours. - Continue to perform above ›95%

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
APPENDIX
Glossary of terms for the integrated quality performance and finance report (IQPR)
Acronym Stands for Brief Definition
AD Assistant director Responsible for strategic and operational management for a
department/division. They will be responsible for compiling business
plans, developing strategy for their area of activity, ensuring
implementation and that performance targets and strategic objectives
are met.
AQN Activity query notice A notice setting out a query in relation to levels of referrals and/or activity to the provider.
AQP Any qualified provider A list of accredited providers that NHS patients can use.
AIVS Acute in hours visiting service Herts urgent care scheme providing a fast, efficient service that aims to keep people out of hospital and avoid the need to call 999 ambulances. Runs across east and north Hertfordshire.
BCF Better care fund A local single pooled budget to incentivise the NHS and local government to work more closely together around people, placing their well-being as the focus of health and care services.
CATT Crisis assessment and treatment team Mental health measured indicator (for number of referrals meeting a 4 hour wait).
CDU Clinical decisions unit An inpatient ward for emergency department patients, who require on-going observation and treatment, following assessment; who are expected to be discharged within 24 hours, once their treatment plan is completed.
CFR community first responders CFRs respond to local emergency calls and provide lifesaving first aid in those vital minutes before an ambulance arrives.
CHC Continuing health care NHS continuing healthcare is the name given to a package of care that is arranged and funded solely by the NHS for individuals who are not in hospital and have been assessed as having a "primary health need".
CLO Chief locality officer Responsible to manage locality wide issues.
CPN Contract performance notice If the co-coordinating commissioner believes that the provider has failed or is failing to comply with any obligation on its part under this contract it may issue a contract performance notice to the provider.
CQC Care quality commission The regulator for all health and social care services in England.
CQN Contract query notice Contract query notice: a notice setting out in detail, the nature of a query either by the commissioner or the provider in relation to performance or non-performance of a contractual obligation.
CQRM Clinical quality review meeting A meeting between the commissioner and provider of health services to review all the quality measures
CQUIN Commissioning for quality and innovation The key aim of the CQUIN framework is to secure improvements in the quality of services and better outcomes for patients, a principle fully supported at all levels of the hospital
CTR Care and treatment review Care and treatment reviews have been developed as part of NHS England’s commitment to transforming the services for people with learning disabilities and/ or autism who display behavior that challenges, including those with a mental health condition.
DGH District general hospital Major secondary care facilities available to UK residents, which provide an array of diagnostic and therapeutic services. While some clinics may be staffed by senior registrars in certain specialties, DGHs are not regarded as teaching hospitals.
DNA Did not attend When a patient does not attend an appointment.
DQIP Data quality improvement plan Allows the commissioner and the provider to agree a local plan to
improve the capture, quality and flow of data to support both the
commissioning and contract management process.
DTOC Delayed transfer of care Refers to delays in transfer of care of acute and non-acute (including community and mental health) patients.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Glossary of terms for the integrated quality and performance report (IQPR) (continued)
Acronym Stands for Brief Definition
DXS DXS care pathways DXS care pathways are structured plans of care; designed to support the implementation of CCG designated clinical guidelines and protocols. They provide detailed NHS best evidence guidance for each stage in the management of a patient with a specific condition and are built around diagnostic codes.
EEAST East of England ambulance trust The trust covers the six counties which make up the east of England - Bedfordshire, Cambridgeshire, Essex, Hertfordshire, Norfolk and Suffolk and provides a range of services, but is best known for the 999 emergency services.
ECIP Emergency care and improvement programme
Clinically led programme that offers intensive practical help and support to 28 urgent and emergency care systems leading to safer faster and better care for patients.
ECPs Emergency care practitioner Allows patients to be treated at home or in their home surrounds, without being transported to a hospital emergency department if it is not necessary.
EIP Early intervention in psychosis Early intervention in psychosis is a clinical approach to those experiencing symptoms of psychosis for the first time. It forms part of a new prevention paradigm for psychiatry and is leading to reform of mental health services, especially in the united kingdom.
EMDASS Early memory diagnosis and support service
Mental health measured indicator (for number of referrals meeting a 6 week wait).
ENHT East and north Herts NHS trust A large provider of acute health care services to HVCCG patients.
ENHCCG East and North Hertfordshire clinical commissioning group
The organisation responsible for commissioning (planning, designing and paying for) NHS services. The CCG serves over half a million people (580,000) registered at 60 GP practices across east and north Hertfordshire.
FNC Funded nursing care Care provided by a registered nurse for people who live in a care home.
FOI Freedom of information The Freedom of information Act 2000 provides public access to information held by public authorities. It does this in two ways: public authorities are obliged to publish certain information about their activities; and members of the public are entitled to request information from public authorities.
GCC Good corporate citizen A corporation that accepts the importance of being collectively responsible for its local community and environment as an integral part of their core business.
HALO Hospital ambulance liaison officer Post in place to support pressures in the west Herts hospitals NHS trust ambulance service.
HCA Health care assistant Healthcare assistants help with the day-to-day care of patients, either in hospitals or in patients' homes.
HCAI Healthcare associated infection Includes MRSA and clostridium difficile.
HRG Healthcare resource group Healthcare resource groups (HRGs) are standard groupings of clinically
similar treatments which use common levels of healthcare resource.
HRGs help organisations to understand their activity in terms of the types
of patients they care for and the treatments they undertake.
HCT Hertfordshire community trust Provides a wide range of care in people's homes, community settings and in its community hospitals.
HSCIC Health and social care information centre (now known as NHS Digital)
The national provider of information, data and IT systems for commissioners, analysts and clinicians in health and social care.
HUC Herts urgent care Delivers urgent health care services in Hertfordshire.
HVCCG Herts valleys clinical commissioning Group The NHS organisation responsible for commissioning (planning, designing and buying) health services on behalf of people who live in Hertfordshire’s council districts of Dacorum, Hertsmere, St Albans, Three Rivers and Watford.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Glossary of terms for the integrated quality and performance report (IQPR) (Continued)
Acronym Stands for Brief Definition
IAPT Improving access to psychological therapies The improving access to psychological therapies (IAPT) programme supports the frontline NHS in implementing national institute for health and clinical excellence (NICE) guidelines for people suffering from depression and anxiety disorders.
ICO Information commissioner’s office Office responsible for the enforcement of the data protection act 1998, and also responsible for freedom of information.
IDAT Involuntary drug and alcohol treatment The IDAT program is a structured drug and alcohol treatment program that provides medically supervised withdrawal, rehabilitation and supportive interventions for identified patients.
IST Intensive support team A small core team who manage the programme and assignments and provide the NHS with specialist advice in the delivery of operational standards.
ITP Inter trust referral policy Inter trust referral policy for transfers.
IHCCT Integrated health care and commissioning team
Commissions services for adults and children with mental health problems and adults with learning disabilities in Hertfordshire.
IPA Integrated point of access The integrated point of access is a single point of contact for Hertfordshire GP’s and other health and social care professionals to access adult community health and social care services and refer for either community nursing or social care referrals . This portal is for professional referrals only.
JCT Joint commissioning team Procures and monitors a range of health and social care support services
KPI Key performance indicator Measure by which success or failure is determined.
L&D Luton and Dunstable University Hospital NHS Foundation Trust
A large provider of acute health care services to HVCCG patients.
LAS London ambulance service The London ambulance service (LAS) is a national health service trust that is responsible for answering and responding to medical emergencies in Greater London.
LOS Length of stay Refers to a patient’s length of time in hospital.
MCI Mild cognitive impairment A condition in which someone has minor problems with cognition - their mental abilities such as memory or thinking
MDT Multidisciplinary teams A group of professionals from one or more clinical disciplines who together make decisions regarding recommended treatment of individual patients. Multidisciplinary teams may specialise in certain conditions, such as cancer.
Monitor Health sectors regulator that works closely with the care quality commission (CQC)
Monitor helps hospitals and other providers to develop and improve performance, respond better and faster to changing patient needs and challenges.
MSA Mixed sex accommodation Unjustified mixing in relation to sleeping accommodation.
NCL North Central London Clinical Commissioning Groups (CCGs) in north central London (Barnet, Camden, Enfield, Haringey and Islington)
NEPTS Non-emergency patient transport service Provides transport for patients who have a medical reason which means they are not able to travel for treatment by another method.
NHSE NHS England The main aim of NHS England is to improve the health outcomes for people in England.
NHSI National health service improvement Responsible for overseeing foundation trusts and NHS trusts, as well as independent providers that provide NHS-funded care. NHSI offers the support the providers need to give patients consistently safe, high quality, compassionate care within local health systems that are financially sustainable
NHSP NHS Professionals Specialist organisation within the NHS recruiting and supplying temporary doctors, nurses, and corporate staff
NICE national institute for health and excellence NICE's role is to improve outcomes for people using the NHS and other
public health and social care services by providing national guidance and
advice.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Glossary of terms for the integrated quality and performance report (IQPR) (Continued)
Acronym Stands for Brief Definition
NICE National institute for health and excellence NICE's role is to improve outcomes for people using the NHS and other
public health and social care services by providing national guidance and
advice.
OOH Out of hours Outside normal surgery hours.
POD Point of delivery Hospital or health care facility that is designated to support disaster
situations in a specific geographic area.
PTL Patient tracking lists A PTL contains the data required to manage patients’ pathways, by showing clearly which patients are approaching the maximum waiting time so operational staff (e.g. staff booking appointments or admissions for patients) can offer dates according to clinical priority and within maximum waiting times.
PTS Patient transport service Provides pre-planned non-emergency transport for patients who have a
medical condition that would prevent them from travelling to a treatment
center by any other means, or who require the skills of an ambulance
care assistant during the journey.
QIPP Quality, innovation, productivity and prevention
A large-scale programme developed by the department of health to drive forward quality improvements in NHS care, at the same time to provide efficiency savings.
QN Queue nurse Assists with the offloading of ambulances particularly in times where there are capacity pressures in the A&E department. The patient can be cared for by the queue nurse in a designated area and the crew can be released, once a cubicle becomes available the patient can then be transferred.
RAID Rapid assessment, interface and discharge This service is delivered by Herts partnership foundation trust (HPFT) and enables faster identification of mental health needs among hospital inpatients of all ages – as well as benefitting people arriving at accident and emergency. This will help to reduce the time that some people need to stay in hospital, prevent unnecessary re-admission and encourage faster recovery from mental and physical illness.
RAP Remedial action plan A recognised action plan implemented to tackle identified areas of concern.
RCA Root cause analysis A method of problem solving used for identifying the root causes of faults or problems.
RFL Royal free London A large provider of acute health care services to HVCCG patients.
RNOH Royal l national orthopedic hospital A specialist orthopedic hospital.
RPI Responses per incident Ambulance resources deployed per incident
RRV Rapid response vehicle Rapid response vehicles are designed to reach the patient as soon as possible. They are usually smaller vehicles that can travel through traffic faster than an ambulance
RTT Referral to treatment time National 18 week referral rate to treatment target.
SBU Strategic business unit Building firm foundations of clinical quality and maximising operational effectiveness without compromising the trust’s financial position.
SCN Strategic clinical network Bring together those who use, provide and commission the service to make improvements in outcomes for complex patient pathways.
SDIP Service development improvement plan The development of an SDIP for a department ensures that a department
is continuously addressing the improvement of service delivery.
SDMP Sustainable development management plan
A document that clarifies objectives on sustainable development helps to set out a plan of action.
SI Serious incident An incident where one or more patients, staff members, visitors or member of the public experience serious or permanent harm, alleged abuse or a service provision is threatened.

\\Hvccg-fs01\shared\_SECURE\Planning & Performance\Performance\IQPFR\IQPFR for Board\IQPFR Board 2016-2017\March 2017\IQPFR board report 09.3.17 .doc
Glossary of terms for the integrated quality and performance report (IQPR) (Continued)
Acronym Stands for Brief Definition
SIRI Serious incident requiring investigation Serious incidents requiring investigation are usually but not exclusively within a hospital.
SLA Service level agreement Agreement between a service provider (either internal or external) and the end user that defines the level of service expected from the service provider.
SLT Senior leadership team HVCCG senior management team that meet fortnightly.
SMART Specific, measurable, achievable, realistic and time related.
Method used to ensure project/performance goals meet these objectives.
SMH Stoke Mandeville Hospital Stoke Mandeville Hospital is a large National Health Service hospital in Aylesbury, England. It is part of Buckinghamshire Healthcare NHS Trust.
SOP Standard operating procedures Step by step instructions to assist staff to carry out routine operations/ specific pieces of work.
SPA Single point of access A central place, site or phone number (e.g., 999, NHS direct, GP out-of-hours, NHS 111) which provides a gateway to a range of health and social services.
SQPR Service quality performance report Report highlighting key performance indicators.
SRIG System resilience implementation group (SRIG has been superseded by the programme board)
(SRIG) will ensure accountability is taken by the owner organisation for projects to be implemented and ensure escalation to system resilience group when any of the above schemes are showing high risk.
SRG System resilience group SRG will follow up areas identified via the programme board in relation to system resilience schemes.
SSNAP Sentinel stroke national audit programme Single source of stroke data in England, Wales and Northern Ireland.
STF Sustainability and transformation fund NHS funding which will support financial balance, the delivery of the five year forward view, and enables new investment in key priorities.
SUS Secondary uses service The secondary uses service is designed to provide anonymous patient based data for purposes other than direct clinical care such as healthcare planning, commissioning, public health, clinical audit and governance, benchmarking, performance improvement, medical research and national policy development.
TCI Treatment come in date Relates to 52+ week waiters and TCI refers to patients receiving an appointment.
TCP Transforming care partnership Tasked with transforming care for people with a learning disability and/or autism. It is made up of people who use the services, their families, providers of services, clinical commissioning groups, local authorities and NHS England specialised commissioning hubs.
TDA Trust development authority The NHS trust development authority provides support, oversight and governance for all NHS Trusts to deliver high quality services.
TEC Technology enabled care Use of technologies such as telehealth, telecare, telemedicine, telecoaching and self-care to transform the way patients engage in and control their own healthcare and empowering patients to manage it.
VTE Venous thromboembolism A disease that includes both deep vein thrombosis (DVT) and pulmonary embolism (PE).
WHHT West Herts Hospitals NHS Trust A large provider of acute health care services to HVCCG patients.
WRES Workforce race equality standard Tool to measure improvements in the workforce with respect to black and minority ethnic (BME) staff with many of the methods being transferable to focusing on other groups.

1
NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Finance Report 2016/17 – Month 10 Agenda Item: 8b
Purpose* (tick) Decision ☐ Approval ☐ Discussion ☒ Information ☐
Responsible Director(s) and Job Title
Caroline Hall, Chief Finance Officer
Author and Job Title Julie Dean, Head of Financial Planning & Reporting
Short Summary of Paper At month 10 the CCG is reporting an adverse variance against plan of £15.6m (£13m at month 9). It is now acknowledged that in-year break-even will not happen and a revised control total of £8m variance from plan has been agreed. This remains a challenging target and relies on recovery actions being achieved.
Recommendation(s) The Board is being asked to: Note financial performance for 2016/17.
Engagement with Stakeholders/Patient/Public
Engagement has taken place with provider organisations
Links to Strategic Objectives (tick all that apply) Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☐
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☐
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☐
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
The report is aligned specifically to the following risks on the 2016/17 Board Assurance Framework:
4.1 Failure to deliver a financially sustainable health and social care system 4.2 Failure to deliver best value from the total CCG budget 4.3 Failure to achieve the agreed control total for 2016/17.
This report provides an update on risks relating to finance and identifies mitigating actions where applicable in relation to: S04/03 S04/22 S04/23 (these risks relate to achievement of financial targets)
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Emerging risk: There is a significant risk that the CCG may exceed the revised control total.
Resource Implications Not applicable. This report provides a general update on key finance issues and performance.
2
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
There are no implications.
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☐ Improved Patient Access and Experience ☐
A Representative and Supported Workforce ☐
Inclusive Leadership ☐
Report History Which Groups or Committees have seen this report and when?
Headline messages about month 10 have been shared with the Executive Team on 21 February 2017 and Q&P on 2 March 2017.
Appendices

3
Finance Report 2016/17 – Month 10
1. Executive Summary and Purpose of the Report
This paper provides a 2016/17 finance update as at the end of January 2017 (month 10).The CCG is currently reporting an in-year deficit of £15.2m (£15.6m variance from plan),which reflects significant over-performance in acute services and continuing carepartially offset by underspends elsewhere. The cumulative deficit (including the surpluscarried forward from 2015/16) is £9.4m year to date, compared with a planned surplus of£6.3m. A recovery plan has been implemented however it is clear that the CCG will notachieve breakeven in year despite additional efforts to identify further mitigations. TheCCG has therefore agreed a revised adverse forecast variance from plan of £8m. Thisremains a challenging target to achieve with significant risk of non-achievement.
2. Summary dashboard of financial duties – RAG rated
3. CCG allocation table
The CCG received £2.4m of non-recurrent funding in month 10, as detailed in the table above.
The CCG is also expecting revenue allocations this year for:-
• Improving Access to general practice• Prime Ministers Challenge Fund
To DateForecast Outturn
Do not exceed revenue resource limit Red GreenAchieve in-year control total Red RedDo not exceed cash limit Green GreenDo not exceed running cost allocation Amber GreenCompliance with Better Payments Practice Code Amber Amber
Revenue Resource
£000
Running Costs £000
Allocation at month 9 745,116 13,203Changes in month:MoD - Out of hours 7IAPT Expansion Wave 1 160ACC - Royal Free vanguard Q4 funding 1,842ACC - Royal Free vanguard 3rd qtr local evaluation funding 50CYP WL & WT Reduction: 2nd tranche 133Non-recurrent allocation to mitigate impact of NHS PS move to market rents 248
Allocation at month 10 747,556 13,203

4
4. Summary financial position – as at 31 January 2017 (Month 10)
The CCG has recorded an in year deficit of £15.2m year to date compared to a planned in year surplus of £0.4m (variance £15.6m). The cumulative deficit at month 10, which takes the brought forward surplus into account, is £9.4m, compared to a planned surplus of £6.3m.
The CCG is forecasting a deficit variance from plan of £8m. Additional mitigations have been identified to get to this revised control total (see below for further details) however this remains a challenging target to achieve.
Acute The majority of the CCG’s expenditure variance relates to expenditure at acute providers.
The table below shows the acute budget and expenditure broken down by provider. The expenditure is based on month 8 freeze and month 9 flex data where this is available. Based on this data, the CCG is estimating over-performance of £18.5m on acute services year to date with a forecast over-performance of £15.8m. QIPP savings are included in provider budgets where agreed in contracts but £12.1m has not been attributed to individual providers and is shown towards the bottom of the table in ‘acute reserves’.
The contract value for West Herts Hospital NHS Trust (WHHT) does not include expected annual QIPP savings of £9.5m. The Trust’s monitoring data is indicating contract under-performance of £0.9m year to date when we might expect under-performance due to QIPP of around £7.9m indicating significant over-performance compared to plan.
The forecast outturn for acute services is over-performance of £15.8m (4%) after additional recovery plan mitigations of £5.5m. If the mitigations do not materialise then there is a risk that over-performance could be in the region of £21m (5%).
DescriptionAnnual budget
(ISFE)(£000)
YTD budget (£000)
YTD Actual (£000)
YTD Variance (£000)
Forecast (£000)
Forecast Variance
(£000)
Programme Allocation 740,545 609,828 609,828 0 740,545 0
Programme CostsAcute 418,682 348,018 366,496 (18,478) 434,446 (15,764)Mental Health / LD 82,642 68,599 66,893 1,706 79,919 2,723Community Services 66,635 55,529 55,366 163 66,492 143Continuing Care / FNC 27,692 23,076 28,660 (5,584) 31,140 (3,448)Prescribing 76,972 64,462 61,754 2,708 73,985 2,987Other Primary Care 16,237 13,564 12,775 789 15,298 939Reserves & non-recurrent programmes 27,878 17,428 15,106 2,322 24,998 2,880Other Programme Costs 23,777 19,132 17,948 1,184 21,737 2,040Total costs 740,515 609,808 624,998 (15,190) 748,015 (7,500)
Programme Surplus / (Deficit) 30 20 (15,170) (15,190) (7,470) (7,500)
Running Cost Allocation 13,203 11,003 11,003 0 13,203 0Running Costs 12,703 10,584 11,033 (449) 13,203 (500)
Running Cost Surplus / (Deficit) 500 419 (30) (449) 0 (500)
TOTAL IN YEAR SURPLUS / (DEFICIT) 530 439 (15,200) (15,639) (7,470) (8,000)
Prior Year Surplus brought forward 7,011 5,843 5,843 0 7,011 0
TOTAL CUMULATIVE SURPLUS 7,541 6,282 (9,357) (15,639) (459) (8,000)

5
Acute expenditure table
Mental health / learning disabilities The under-performance on mental health of £1.7m year to date largely relates to slippage on investments. The released funds are not being reinvested this financial year due to the overall finances of the CCG.
Continuing healthcare Continuing care is over-performing by £5.6m year to date. The position reflects current commitments on the continuing healthcare database together with the above anticipated increase in the NHS funded nursing care (FNC) rate and a further £1.1m relating to 2015/16 that was not accrued at the time. The CCG is currently conducting a data cleanse of the CHC database to ensure that the commitments recorded are up to date and accurate.
BUDGET ACTUAL VARIANCE VAR. % BUDGET ACTUAL VARIANCE VAR. %TOP 6 CONTRACTS:
West Hertfordshire Hospitals243,406 203,152 202,250 902 0% 243,406 242,367 1,039 0%
Royal Free London 48,243 40,202 41,288 (1,085) (3%) 48,243 49,428 (1,185) (2%)
Luton And Dunstable 19,500 16,250 17,715 (1,465) (9%) 19,500 21,259 (1,759) (9%)
East And North Hertfordshire14,678 12,232 12,580 (348) (3%) 14,678 15,099 (421) (3%)
Buckinghamshire Healthcare14,316 11,930 11,840 90 1% 14,316 14,209 107 1%
Royal National Orthopaedic 8,321 6,934 6,600 334 5% 8,321 7,920 400 5%
OTHER CONTRACTS:University College London 9,109 7,591 8,516 (925) (12%) 9,109 10,221 (1,112) (12%)Imperial College Healthcare 6,895 5,746 6,624 (878) (15%) 6,895 7,949 (1,054) (15%)The Hillingdon Hospitals 5,227 4,356 4,886 (530) (12%) 5,227 5,863 (636) (12%)Royal Brompton & Harefield 4,236 3,530 3,359 171 5% 4,236 4,030 206 5%Moorfields Eye Hospital 3,990 3,325 3,617 (292) (9%) 3,990 4,341 (350) (9%)London North West Healthcare 4,477 3,730 3,767 (37) (1%) 4,477 4,521 (45) (1%)Guys And St Thomas 2,207 1,839 1,995 (156) (8%) 2,207 2,394 (187) (8%)Great Ormond Street Hospital 1,023 852 770 82 10% 1,023 924 98 10%Barts Health 2,046 1,705 1,765 (60) (4%) 2,046 2,094 (48) (2%)Other NHS Contacts less than £1m 4,262 3,552 3,814 (262) (7%) 4,262 4,579 (317) (7%)SUB-TOTAL NHS CONTRACTS 391,935 326,926 331,386 (4,460) (1%) 391,935 397,198 (5,264) (1%)
East Of England Ambulance 17,076 14,230 14,989 (759) (5%) 17,076 18,068 (992) (6%)
TOTAL INDEPENDENT SECTOR CONTRACTS
9,565 7,971 9,785 (1,814) (23%) 9,565 11,743 (2,178) (23%)
TOTAL OTHER ACUTE HEALTHCARE
8,471 7,059 7,208 (149) (2%) 8,471 8,653 (182) (2%)
ACUTE RESERVES (8,365) (8,168) 3,128 (11,297) 138% (8,365) 4,312 (12,678) 152%
GRAND TOTAL 418,682 348,018 366,496 (18,478) (5%) 418,682 439,974 (21,292) (5%)
Mitigations 0 0 0 0 0 (5,528) 5,528
REVISED GRAND TOTAL 418,682 348,018 366,496 (18,478) (5%) 418,682 434,446 (15,764) (4%)
PROVIDERANNUAL BUDGET
YTD POSITION (£'000) FULL YEAR POSITION (£'000)

6
5. Reserves
The 1% non-recurrent requirement of £7.4m remains uncommitted and must remain so at this stage to mitigate financial risk across the wider NHS and will only be released on a decision by HM Treasury. This is not anticipated until later in the financial year, if at all in 2016/17. The forecast outturn assumes this funding is not available to mitigate the CCG in-year deficit.
The CCG 0.5% contingency of £3.8m has been utilised to mitigate the £3m impact from repayment of the system risk share with the balance supporting the in-year position. The balance of other reserves is also supporting the financial position and is not available for investment.
6. QIPP
Planned £000
Delivered £000
Variance £000
Delivery to date 15,807 8,383 7,424 Forecast outturn 21,620 10,700 10,920
Number Value £000
Schemes over delivering to date 2 3,022 Schemes on target to date 4 2,607 Schemes under delivering to date 27 2,755 Schemes abandoned 2 0
The Children’s A&E workstream was abandoned in August 2016 as children’s A&E attendances had increased by 7.2% on the 15/16 baseline with a plan to reduce by 2% against the 15/16 baseline. The Children’s Paediatric Urgent Care Pathway workstream was abandoned in December 2016.
7. Run rate and underlying position
Within the reported 2016/17 financial position are a number one-off or non-recurrentincome and expenditure items. Once these are taken into account the true, underlyingposition of the CCG is revealed. The table below shows an underlying deficit of £5,247k,which equates to 0.7% of the recurrent revenue allocation. This means the CCG hasrecurrent expenditure that is higher than its recurrent allocation. It is acknowledged thatan underlying surplus of between 1 and 2% indicates a sustainable financial position.The CCG’s 2017/18 financial plan aims to restore the underlying position to this level.This requires the CCG to reduce its ongoing expenditure through the successful deliveryof QIPP schemes.
1%£000
0.5% Contingency
£000Other£000
Total£000
Balance at start of year 7,336 3,760 5,000 16,096Utilised to date (FOT) 3,000 3,387 6,387Supporting the financial position 760 1,613 2,373Uncommitted 7,336 0 0 7,336

7
Underlying position
Recurrent Underlying
Surplus/ (Deficit)
Non Recurrent
Forecast Surplus/ (Deficit)
(£000) (£000) (£000)
16/17 published allocation 733,574 733,574Post Mth07 Recurrent Transfers 9 9Running Cost Allocation 13,203 13,203NR: -
Return of Surplus/(Deficit) 7,011 7,011 Co-Commissioning NR Allocation -
Other Non Recurrent allocations 6,962 6,962
TOTAL ALLOCATION 746,786 13,973 760,759
Acute services 437,183 (2,737) 434,446Mental Health Services 80,235 (316) 79,919Community Health services 65,427 1,065 66,492Continuing Care services 31,368 (228) 31,140Prescribing 74,710 (725) 73,985Other Primary Care 15,288 10 15,298Other Programme services 6,618 (466) 6,152BCF Expenditure 18,085 (2,500) 15,585Reserves & Non Recurrent Programmes 9,979 15,019 24,998Running costs 13,140 63 13,203Contingency - - TOTAL APPLICATION OF FUNDS 752,033 9,185 761,218
CUMULATIVE SURPLUS/ (DEFICIT) (5,247) (459)(0.70%) (0.06%)
Surplus/(Deficit) In-Year Movement: (7,470)Surplus/(Deficit) b/f: 7,011
2016/17 - month 10
NHS Herts Valleys CCG

8
8. Better payments practice code (BPPC)
The cumulative number of invoices paid within payment terms (15 days for NHS and 30 days for non NHS) is 96%. The number of NHS invoices paid within 15 days is below target at 86% but payment of non NHS invoices remains above target at 98%.
Year To Date Period Covered Apr-16 to Jan-17
Number of Bills Paid Value of Bills PaidIn Total Within In Total Within Period Target % Period Target %
£'000 £'000Non NHS 18,053 17,701 98% 154,632,283.56 151,168,091.04 98%NHS 3,401 2,924 86% 407,922,038.09 399,801,571.62 98%Total 21,454 20,625 96% 562,554,321.65 550,969,662.66 98%

9
9. Statement of financial position (SOPF)
The CCG has no fixed assets or long term liabilities so the SOFP only includes information on current assets and liabilities, offset by the general fund.
10. Cash
This table shows cash utilisation year to date and an expected cash profile for the remainder of the year. It shows that £623m of the £760m expected to be available (82%) has been drawn-down to date, leaving £137m (18%) undrawn balance. The drawdown in January was £0.4m less than forecast. The cash available to the CCG includes £8m to cover payments associated with the forecast variance. If the actual variance is higher there may be an impact on cash-flow however it is envisaged that this will be managed through delaying the payment of over-performance invoices.
Asset /Liability 31 January 2017
31 March 2016
£000 £000Non-current assets: 0 0
Current assets:Trade and other receivables 2,409 4,889Cash and cash equivalents -36 163Total current assets 2,373 5,052
Total assets 2,373 5,052
Current liabilities:Trade and other payables -52,433 -44,796Provisions -523 -652Total current liabilities -52,956 -45,448
Non-Current Assets plus/less Net Current Assets/Liabilities -50,583 -40,396
Financed by Taxpayers’ EquityGeneral fund -50,583 -40,396Total taxpayers' equity: -50,583 -40,396
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Total£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Forecast Drawdowns inc Top Slice for Drugs @ M6 61,327 62,759 59,251 61,983 64,903 63,965 61,065 62,531 64,065 63,216 64,365 70,435 759,865
Actual drawdown 55,500 56,500 53,000 56,000 58,500 57,400 54,500 57,800 55,800 56,500 561,500Actual top slice 5,827 6,259 6,251 5,983 6,403 5,999 6,122 6,049 6,039 6,302 61,234
61,327 62,759 59,251 61,983 64,903 63,399 60,622 63,849 61,839 62,802 0 0 622,734Diff 0 0 0 0 0 566 443 -1,318 2,226 414 137,131
Undrawn balance 137,131Proportion remaining 18.0%
Amendments to Forecast DrawdownM6 - Additional 526k allocation to be drawn down in JanM8 - Additional 1,466k allocation (3,091k actual less forecast 1,625k) to be drawn down in Nov M9 - Additional 1,256k allocation resulting from ACF1 (M6) exercise to be drawn down in M12M9 - Additional 8m central support provided as part of ACF1 exercise to be drawn down in M9, M11 and M12

10
11. Recovery plan
The recovery plan developed in August has proved insufficient to achieve breakeven andtherefore further actions have been developed to address the financial challenge. Inparticular, the recovery plan relied on an improvement in QIPP delivery but this isproving difficult to achieve. An updated recovery plan is provided below, showingremaining mitigations with a current unmitigated risk of £8m. There is acceptance thatthe position is unlikely to improve further and therefore the CCG is now forecasting anadverse variance compared to plan of £8m. This remains challenging to achieve.
12. Risks and mitigating actions
The current forecast of an £8m variance from plan is based on current performance,various assumptions including how activity may change over the remaining months ofthe year and recovery actions. There is a risk that these assumptions prove inaccurateor unachievable.
The current unmitigated forecast is a deficit of £18.6m. Mitigations totalling £10.6m areset out in the recovery plan leaving current net risk of £8m. Additional mitigations maybe required if these savings do not materialise, otherwise the revised control total will bebreached.
13. Recommendation and conclusion
Board members are asked to note the 2016/17 financial position, which shows that at theend of January the CCG has an in-year adverse variance against plan of £15.6m and istherefore £15.6m behind the planned year to date surplus target and significantly behindthe recovery plan trajectory. It is now clear that the CCG will not achieve breakeven inyear despite additional efforts to identify further mitigations. The CCG has thereforeagreed a revised adverse variance from plan of £8m. This remains challenging toachieve and performance will need to be closely monitored over the remaining months ofthe year. There is now however a significant risk that the revised control total will not beachieved.
Herts Valleys CCG - Financial Risk Assessment LikelyAs at 16 February - based on month 10 finance report £m
Current Forecast Variance to plan -18.62
Recovery Plan (1) RAG RatingNon-STF related contract penalties and sanctions 0.03 Additional CCG allocation (Quality premium) 0.82 National Prescribing Profile changes 0.20
1.05 Recovery Plan (2)
Programme slippage 0.75 Scheme underspends 1.40 GP IT underspend 0.12 Resolution of disputed items 0.20 Additional contract challenges 0.25 Additional acute mitigations 3.85 CHC review 1.85 Additional CHC savings 1.15
9.57
Agreed revised control total -8.00

SPACER PAGE

SPACER PAGE

1
NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Medical Directorate Report Agenda Item: 9
Purpose* (tick) Decision ☐ Approval ☐ Discussion ☒ Information ☒
Responsible Director(s) and Job Title
David Buckle, Medical Director
Author and Job Title Michelle Campbell, Head of Primary Care Sarah Crotty, Head of Pharmacy & Medicines Optimisation Team
Short Summary of Paper This paper provides the Board with an update on the work being undertaken in both the Primary Care Team and Pharmacy and Medicines Optimisation Team (PMOT) within the Medical Directorate.
Recommendation(s) The Board is being asked to: Note the content of the paper
Engagement with Stakeholders/Patient/Public None Links to Strategic Objectives (tick all that apply) Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☒
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
BAF: 1.1 Risk that we fail to engage effectively with our patients, population and stakeholders 1.2 Risk that member practices do not see the potential positive impact of their engagement with HVCCG 2.2 Risk that we are unable to ensure high quality, safe and sustainable services for the population and patients of west Hertfordshire 4.1 Risk that we do not deliver a financially sustainable health and social care system 4.2 Risk that we do not deliver best value from the total CCG budget 4.3 Risk that we do not achieve financial balance for 2016/17
SO1/04 Failure to engage and communicate effectively with member practices could lead to lack of support, poor performance and threat to reputational risk, also a failure to meet organisational objectives SO4/23 Risk that additional expenditure will occur that is not budgeted for SO4/03 Risk that QIPP savings are not achieved as planned

2
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Financial risks identified in both Primary Care and PMOT areas.
Mitigation: - Monthly monitoring of all activity and expenditure against Primary Care Plus and
PMOT budgets - Additional PMOT financial savings areas will be identified if existing plans are
not on track to be delivered Resource Implications
None
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
N/A
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☒ Improved Patient Access and Experience ☒
A Representative and Supported Workforce ☒
Inclusive Leadership ☐
Report History Which Groups or Committees have seen this report and when?
None
Appendices None
*Purpose – definitions
For decision This is where the board, committee or group is presented with a range of options and is asked to decide which one to accept following discussion. For approval A specific recommendation, plan or document is presented, which the board, committee or group is requested to approve. Discussion is not essential. For information Information is provided and it is important that the board, committee or group is aware of, and understands the information and no decision is required. These items do not require discussion, except for questions of clarification. For discussion The board, committee or group is asked to debate an issue, provide views, challenge and discuss as appropriate. A decision may be made following the discussion although this is not always required. An example is a progress report on a particular pathway. In this case the Board or Committee will be asked to discuss and note the paper

3
Introduction
The Medical Directorate report provides the Board with a brief overview of the work of the two teams that form the directorate – The Pharmacy and Medicines Optimisation teams (PMOT) and Localities and Primary Care Development. The main workstreams discussed below illustrate some of the ways our teams and clinical colleagues are taking forward the strategic priorities of the organisation. The report covers the above for the months of January and February 2017.
Localities/Primary Care Team
1. Delegated commissioning
An update is provided in the Accountable Officer’s Board report.
2. CCG commissioned services from general practice
Increasing Capacity in Primary Care schemes continue until 31 March 2017 with St Albans andHarpenden, Watford and Three Rivers and Hertsmere localities offering additional appointmentsduring core hours. Additional appointments are also available at the weekend in the Watfordand Three Rivers locality, with the extension to the GP Access Service (GPAS) pilot involving alllocality practices. Up to the end of January 2017 an additional 35,131 appointments have beenmade available during the week with an average of 94% uptake. An additional 1,941appointments were available to patients at the weekend with an average of 94% uptake (acrossthe additional practices in Watford delivering the GPAS).
The contract for the Dacorum Holistic Healthcare Team continues until December 2017.
A Commissioning Framework is being developed that supports the delivery of the currentPrimary Care Plus (PC Plus), Local Incentive Scheme and the Member Practice CommissioningAgreement. This will simplify the payment and monitoring processes for general practice withinour existing PC Plus Budget. The first draft will be circulated to the CCG Practice Manager Forumand engagement with member practices will be managed through locality commissioningmeetings.
3. Procurements and Consultations
The procurement process for the two APMS Contracts for Meadowell Surgery in Watford andNew Surgery in Tring is due to commence in the next few weeks. As this is later than anticipated,the contracts with the existing providers have been extended to allow sufficient time for theprocurement process to be completed.
The formal consultation on West Herts Medical Centre is due to start in the next few weeks andthe outcome will be reported to the NHS England/CCG Joint Primary Medical ServicesCommissioning Committee.
4. GP Forward View
A detailed plan covering the implementation of the GP Forward View (GPFV) has been preparedand submitted to NHS England. The final draft of the plan is due to be submitted in March 2017.
4
Localities are continuing to engage with member practices on how they can support the delivery of the GPFV priorities.
5. GP Resilience Programme
The programme is intended to identify areas of development and support which will increasepractice resilience.
NHS England (Central Midlands) has received 27 expressions of interest from Herts Valleyspractices of which 23 were supported in principle. Practices were informed of the outcome inDecember 2016. Of the 23 practices:
• 16 require a diagnostic review;• 5 requested funding to consider new models of care i.e. the potential recruitment of a
clinical pharmacist;• 2 practices have required emergency section 96 (s96) funding to achieve urgently
required sustainability.
The CCG and GP practices are currently waiting to progress this programme of work. The LMC has developed a local diagnostic review toolkit across Hertfordshire, Luton and Bedfordshire and there are 56 GP practices waiting to undergo the reviews. The CCG believes this process will identify how we can work collaboratively to support general practice.
Pharmacy and Medicines Optimisation Team (PMOT)
The Medicines Optimisation Team is now almost fully staffed for the first time in some months, with all but one vacant post appointed to. There will however be a period where new staff are learning the HVCCG ways of doing things. Soon, we will have more capacity to develop supportive work for practices in 2017/18, to improve our ScriptSwitch (support software on practice systems providing prescribing safety advice and cost effective alternatives) profile and to work collaboratively with both our GP practices and localities.
Coming soon:
• Local Incentive scheme (now at the final draft stage).• Local advice on antibiotics (reducing the use of trimethoprim – because we have
considerable local antibiotic resistance, and there is national drivers to encouragenitrofurantoin use, where possible. This initiative should help us to work towards achievingour targets in the NHS England Quality Premium scheme 2017/18).
• We predict the annual spend on ‘specials’ in HVCCG will be as much as £750k. Specials areprescriptions that have to be specifically made and dispensed for a named patient. We arereviewing this spend as we believe significant savings could be made.
• Working with practice staff to review and stop oral nutritional supplements where a foodfirst approach is appropriate.
• In Q1 2017, we plan to reinstate annual GP practice visits by a pharmacist from our team todiscuss prescribing and medicines optimisation – focusing on the changes which willmaximise our ability to stay under budget while improving the quality of care aroundmedicines.

SPACER PAGE

SPACER PAGE

NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Equality & Diversity Annual Report (Workforce Data) Agenda Item: 10
Purpose* (tick) Decision ☐ Approval ☐ Discussion ☐ Information ☒
Responsible Director(s) and Job Title
Hein Scheffer, Director of Workforce
Author and Job Title Paul Curry, Equality and Diversity Lead Short Summary of Paper This report presents the annual workforce equality data. Publication of this data by
21 January each year is a requirement of the Equality Act 2010. The report shows an organisation where the staff group is reasonably balanced, when compared to the local population and other CCGs.
Recommendation(s) The Board is being asked to: Note the contents and findings of the report
Engagement with Stakeholders/Patient/Public
State briefly and engagement activities and relevant outcomes of that engagement
Links to Strategic Objectives (tick all that apply) Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☒
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☐
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☐
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
1.3 Risk that we have an unengaged staff body. 2.1 Risk that we do not deliver on all NHS Constitutional pledges, key national targets and priorities. 2.3 Risk that we do not close the health inequalities gap between the most and least deprived communities.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Any risk of not meeting the statutory requirement to publish workforce equality data will be met by the publication of this report.
Resource Implications None

2
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
No equality impact analysis is required. This report provides baseline equality data. When used with the staff survey results to produce a Workforce Race Equality Standard report and action plan an equality impact analysis will be undertaken on that report and action plan.
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☐ Improved Patient Access and Experience ☐
A Representative and Supported Workforce ☒
Inclusive Leadership ☐
Report History Which Groups or Committees have seen this report and when?
Executive Quality and Performance Committee
Appendices 1. Summary report2. Workforce Information Analysis – Herts Valleys CCG Equality & Diversity
Report 2016

3
Appendix 1
Summary Report
Herts Valleys Clinical Commissioning Group (HVCCG) workforce equality & diversity report.
This report is produced in order to comply with one of the data publication requirements of the Equality Act 2010, which states that annual workforce data should be published by 21 January each year.
We have a duty to publish a range of equality data, as well as our workforce data. For example, our Annual Report includes a section on equalities. By April 2017 we will also publish our Workforce Race Equality Standard report and be working towards a new equality and diversity strategy and action plan and a report on progress against the NHS Equality Delivery System (EDS2). We will bring the findings from the different reports together to produce an overview report on equality and diversity, looking at the system wide impact of our policies and practices. This will ensure that we meet all the data publication requirements of the Equality Act.
We present our findings alongside local workforce or population data available from Hertfordshire County Council. This can be a useful indicator of how we compare to the population we serve. Data analysis. On the 30th November 2016, when this data was produced, we employed 182 people. Overall, the workforce data for HVCCG does not produce any ’red flags’. There is a general balance between the expectations for a CCG workforce when compared to other CCG workforces (1) and when looking at the local working age population. A few interesting indicators are:
• Increase in proportion of the workforce in Band 6 and 7 for both sexes from last year.• General reduction in people not declaring equality group status, which is a positive
trend that should be encouraged.• Age: Increases in 20-39 and 40-49.• Reasons for leaving: staff in the younger age groups are likely to leave for
promotion/better reward packages, which indicated that there may be issues aroundretaining staff. Voluntary resignation in 50-65 age groups looks like it tends to be fora better work/life balance. Males are more likely to resign for promotion/better rewardpackages and Females more likely to resign for work life balance.
• Excluding Non-AfC staff*, who are all part time, 21% of female employees work parttime and 7% of male employees work part time.
• The NHS defines Black and minority ethnic (BME) as everyone who self-identifiestheir ethnicity as other than white British. Our BME employment rate, 25.27%, ishigher than the Herts valleys CCG population BME rate of 11.01%. 24% of our non-AfC staff* are Black and Minority Ethnic.
* Staff on non-AfC grades refers to very senior managers and those on ad hoc salarygrades: this group would include clinical leads

4
Workforce Race Equality Standard (WRES) The NHS Workforce Race Equality Standard (WRES) has been developed as a tool to measure improvements in the workforce with respect to BME staff with many of the methods being transferable to focusing on other groups. It is an NHS initiative that has been conceived by the national NHS Equality & Diversity Council; through collaboration with NHS staff and independent researchers. The challenge is to ensure BME staff are treated fairly and their talents valued and developed. The WRES CCG Technical Guidance states:
“CCGs are required to have “due regard” to the WRES in respect of their own workforce. It is recognised that the small size of many CCGs means that a literal application and interpretation of the indicators should be approached with caution” “CCGs should pay due regard to the WRES both as an indication they are complying with their Public Sector Equality Duty and in order to demonstrate that as commissioners they also take the intent of the WRES seriously.”
When looking at our performance as an employer, a key indicator from the WRES is the relative likelihood of a BME applicant being appointed once shortlisted. This is important because to be shortlisted the applicant has shown that they are likely to meet the criteria for the post applied for. Using the data we have, we are able to say that in 2016 you were statistically more likely to be appointed from shortlisting if you were a BME applicant than a White applicant. If you are a BME employee you are more likely to be working full time and if you leave us voluntarily it is more likely to be for promotion or a better reward package than your White colleagues.
From July 2016 CCGs are required to publish a WRES report and action plan. WRES indicators include results from the Staff Survey, which can give a clearer picture of what it is like to work for the organisation if staff are in a minority group. The staff survey results are likely to be available in February 2017 and a separate WRES report will be produced in the New Year, when the data is available. Conclusion
This workforce data report shows an organisation where the staff group is reasonably balanced, when compared to the local population and other CCGs.
Recommendations
The committee is recommended to note the contents and findings of the report.

5
Workforce Information Analysis – Herts Valleys CCG Appendix 2
Equality & Diversity Report 2016
Report Author: Paul Curry
Author Job Title: Equality and Diversity Lead
Supported by: Selina Jassal, Workforce Information Manager
December 2016

6
Table of Contents SECTION 1 INTRODUCTION ........................................................................................................... 3
1.1 Introduction ............................................................................................................................. 3
SECTION 2 ORGANISATIONAL PROFILE .................................................................................. 3-5
2.1 Gender .................................................................................................................................... 3
2.2 Disability .................................................................................................................................. 4
2.3 Ethnic Origin ............................................................................................................................ 4
2.4 Age .......................................................................................................................................... 4
2.5 Religion / Belief ....................................................................................................................... 4
2.6 Sexual Orientation ................................................................................................................... 5
2.7 Marital Status .......................................................................................................................... 5
2.8 Maternity ................................................................................................................................. 5
2.9 Leavers ................................................................................................................................... 5
SECTION 3 PAY GRADE COMPARISONS ..................................................................................... 6
3.1 Pay Grade Comparisons ......................................................................................................... 6
SECTION 4 RECRUITMENT & SELECTION ................................................................................... 6
4.1 Recruitment & Selection .......................................................................................................... 6
SECTION 5 TRAINING & DEVELOPMENT ..................................................................................... 6
5.1 Training & Development .......................................................................................................... 6
APPENDIX 1 – Workforce Data Overview ...................................................................................... 7
APPENDIX 2 – Pay Grade Comparison – Protected Characteristics ...................................... 8-10
APPENDIX 3 – Recruitment & Selection Overview ..................................................................... 11
APPENDIX 4 – Leavers Overview ................................................................................................ 12
APPENDIX 5 – Leaving Reasons – Protected Characteristics .............................................. 13-14
APPENDIX 6 - Mandatory Training Participation Rates by Protected Characteristics ...…...15
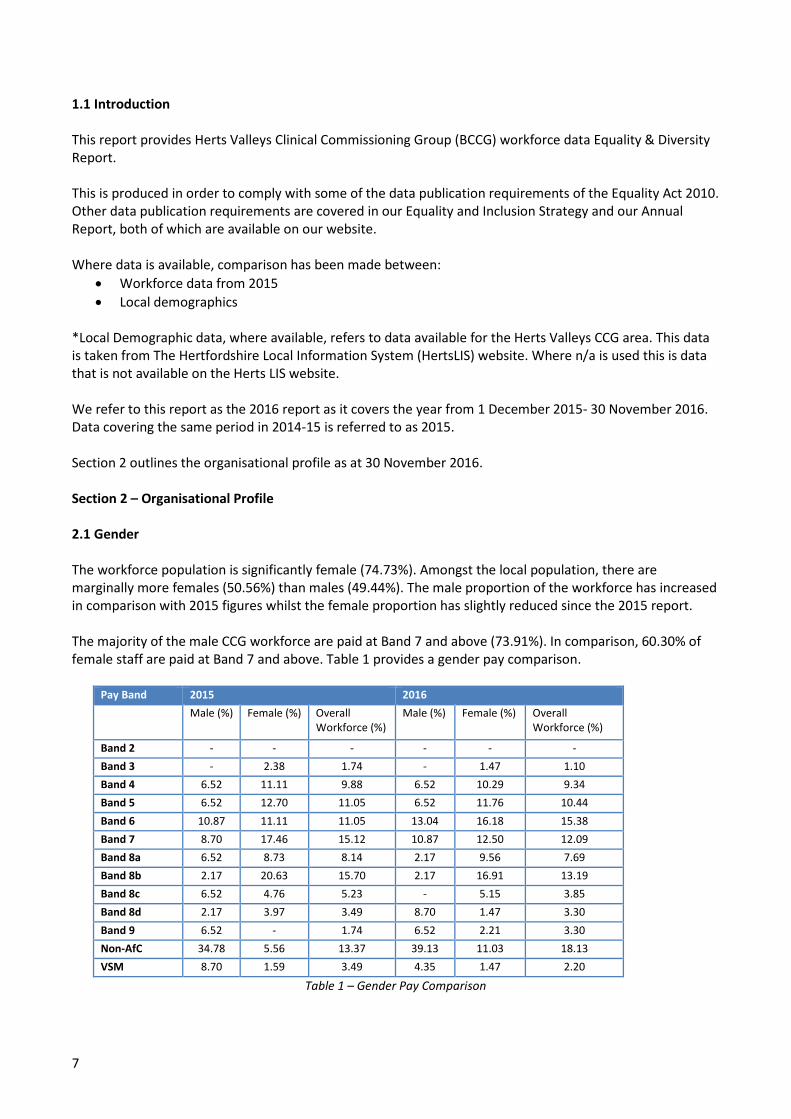
7
1.1 Introduction
This report provides Herts Valleys Clinical Commissioning Group (BCCG) workforce data Equality & Diversity Report.
This is produced in order to comply with some of the data publication requirements of the Equality Act 2010. Other data publication requirements are covered in our Equality and Inclusion Strategy and our Annual Report, both of which are available on our website.
Where data is available, comparison has been made between: • Workforce data from 2015• Local demographics
*Local Demographic data, where available, refers to data available for the Herts Valleys CCG area. This datais taken from The Hertfordshire Local Information System (HertsLIS) website. Where n/a is used this is data that is not available on the Herts LIS website.
We refer to this report as the 2016 report as it covers the year from 1 December 2015- 30 November 2016. Data covering the same period in 2014-15 is referred to as 2015.
Section 2 outlines the organisational profile as at 30 November 2016.
Section 2 – Organisational Profile
2.1 Gender
The workforce population is significantly female (74.73%). Amongst the local population, there are marginally more females (50.56%) than males (49.44%). The male proportion of the workforce has increased in comparison with 2015 figures whilst the female proportion has slightly reduced since the 2015 report.
The majority of the male CCG workforce are paid at Band 7 and above (73.91%). In comparison, 60.30% of female staff are paid at Band 7 and above. Table 1 provides a gender pay comparison.
Pay Band 2015 2016 Male (%) Female (%) Overall
Workforce (%) Male (%) Female (%) Overall
Workforce (%)
Band 2 - - - - - - Band 3 - 2.38 1.74 - 1.47 1.10 Band 4 6.52 11.11 9.88 6.52 10.29 9.34 Band 5 6.52 12.70 11.05 6.52 11.76 10.44 Band 6 10.87 11.11 11.05 13.04 16.18 15.38 Band 7 8.70 17.46 15.12 10.87 12.50 12.09 Band 8a 6.52 8.73 8.14 2.17 9.56 7.69 Band 8b 2.17 20.63 15.70 2.17 16.91 13.19 Band 8c 6.52 4.76 5.23 - 5.15 3.85 Band 8d 2.17 3.97 3.49 8.70 1.47 3.30 Band 9 6.52 - 1.74 6.52 2.21 3.30 Non-AfC 34.78 5.56 13.37 39.13 11.03 18.13 VSM 8.70 1.59 3.49 4.35 1.47 2.20
Table 1 – Gender Pay Comparison

8
2.2 Disability
The number of employees declaring a disability has remained nominally static from the 2015 report.
Disability Status 2015 Workforce Profile (%)
2016 Workforce Profile (%)
Local Demographic (%)
Yes 4.65 4.95 14.01 No 80.23 84.62 85.99 Undeclared 15.12 10.44 0.00
Table 2 – Disability Profile Comparison
2.3 Ethnic Origin
The majority of the workforce is white (69.23%). BME staff make up 25.27% of the workforce. Statistics of new starters (between 1 December 2015 – 1 December 2016) reveal that the majority of new appointees were white (58.57%). Table 3 provides further detail.
Table 3 – Ethnic Origin Comparison
2.4 Age
There have been slight increases in the 20-39 and 40-49 age groups. Currently 42.31%% of the workforce is aged 50-65 years, slightly lower than in 2015.
Age Band 2015 Workforce Profile (%)
2016 Workforce Profile (%)
Local Demographic (%)
Under 20 - - 25.1 20-39 22.09 25.82 26.01 40-49 27.33 31.32 15.57 50-65 50.00 42.31 17.91 65+ 0.58 0.55 15.41 Undeclared - - -
Table 4 – Age Profile 2.5 Religion / Belief
The group with the highest representation amongst the workforce is Christianity (39.56%), with 47.14% of new appointees also belonging to this group.
Religion / Belief 2015 Workforce Profile (%)
2016 Workforce Profile (%)
Local Demographic (%)
Atheism 13.37 13.19 24.41 Christianity 36.63 39.56 57.03 Hinduism 5.81 4.95 0.8 Islam 0.58 1.10 3.82 Other 8.72 29.89 3.91 Undeclared 34.88 31.32 7.33
Table 5 – Religion / Belief Comparison
Ethnic Origin 2015 Workforce Profile (%)
2016 Workforce Profile (%)
Local Demographic (%)
White 69.77 69.23 85.45 BME 21.51 25.27 11.01 Undeclared 8.72 5.49 -

9
2.6 Sexual Orientation As with previous workforce reporting statistics, LGB disclosure rates continue to be minimal. Whilst the majority declared as heterosexual (73.08%), 24.73% chose not to disclose their sexual orientation. Table 6 provides further details. Sexual Orientation 2015 Workforce
Profile (%) 2016 Workforce Profile (%)
Local Demographic (%)
LGB 1.74 2.20 1.7 Heterosexual 69.19 73.08 93.7 Undeclared 29.07 24.73 -
Table 6 – Sexual Orientation 2.7 Marital Status The highest represented group amongst employees are Married / Civil Partnership (63.19%) followed by Single (21.98%). Around 6.59% of employees chose not to declare their marital status. Marital Status 2015 Workforce
Profile (%) 2016 Workforce Profile
Local Demographic (%)
Married / Civil Partnership 59.88 63.19 50.76 Single 21.51 21.98 31.98 Legally Separated 1.74 1.10 Not available Divorced 6.98 5.49 8.26 Widowed 0.58 1.65 6.46 Undeclared 9.30 6.59 -
Table 7 – Marital Status 2.8 Maternity Five members of staff were on maternity leave during 2016; currently two employees have returned during 2016, giving a return rate of 40.00%. One employee did not return to work due to an end of fixed term contract. The other two members of staff are still on maternity leave. 2.9 Leavers There were 58 leavers during 1 December 2015 – 1 December 2016; the most frequent reason for leaving was ‘promotion’ (27.59%), followed by ‘work life balance’ at 20.69% and thirdly, ‘retirement age’ (10.34%). Table 8 summarises all leaving reasons. An overview of leavers by characteristic is available in appendix 4 and 5 Leaving Reason 2016 Leavers (%) Voluntary resignation – promotion 27.59 Voluntary resignation – work life balance 20.69 Retirement age 10.34
Voluntary resignation – other/not known 10.34 Voluntary resignation – relocation 6.90 Voluntary resignation – better reward package 6.90
End of fixed term contract 5.17
Redundancy – compulsory 5.17
Voluntary resignation – lack of opportunities 3.45
Voluntary early retirement – with actuarial reduction 1.72
Voluntary resignation – child dependents 1.72
Table 8 – Leaving Reasons

10
Section 3 – Pay Grade Comparisons
3.1 Pay Grade Comparisons
An analysis of pay grades (including working hours) was conducted for the following characteristics:
• Gender• Ethnicity• Disability
The use of Agenda for Change payscales ensures that staff receive equal pay for the same job.
Detailed information regarding pay in relation to characteristics is available in appendix 2
4.1 Recruitment & Selection
Data on applications received and shortlisting information of job applicants was extracted from NHS Jobs, where CCG vacancies are processed. Applications sent to Recruiting Managers only provide employment history and qualifications.
Appendix 3 provides details of job applicant success rates by characteristic. Job applications reported on are from the period 1 December 2015 – 1 December 2016.
5.1 Training & Development
A breakdown of mandatory training participation rates by protected characteristics (as at August 2015) is provided in Appendix 6.

Appendix 1 - Workforce Data Overview
Characteristic 2015Workforce Data (%) 2016 Workforce Data (%) Local Demographic (%) Gender
Male 26.74 25.27 49.34 Female 73.26 74.73 50.66
Disability Status Yes 4.65 4.95 14.01 No 80.23 84.67 85.99 Undeclared 15.12 10.44 -
Ethnicity White 69.77 69.23 85.45 BME 21.51 25.27 11.01 Undeclared 8.72 5.49 -
Age Band Under 20 - - 25.1 20 to 39 22.09 25.82 26.01 40 to 49 27.32 31.32 15.57 50 to 65 50.00 42.31 17.91 65 + 0.58 0.55 15.41 Undeclared - - -
Religion Atheism 13.37 13.19 24.41 Christianity 36.63 39.56 57.03 Hinduism 5.81 4.95 0.8 Islam 0.58 1.10 3.82 Other 8.72 29.89 3.91 Undeclared 34.88 31.32 7.33
Sexual Orientation LGB 1.74 2.20 1.7 Heterosexual 69.19 73.08 93.7 Undeclared 29.07 24.73 -
Marital Status Married / Civil Partnership 59.88 63.19 50.76 Single 21.51 21.98 31.98 Separated 1.74 1.10
Divorced 6.98 5.49 8.26 Widowed 0.58 1.65 6.46
Undeclared 9.30 6.59 0.00

Appendix 2 – Pay Grade/Working Hours – Protected Characteristics
Payscale Working Hours Gender
Female Male Band 2 Full Time - -
Part Time - - Band 3 Full Time 1 -
Part Time 1 - Band 4 Full Time 11 2
Part Time 3 1 Band 5 Full Time 14 3
Part Time 2 - Band 6 Full Time 17 6
Part Time 5 - Band 7 Full Time 12 5
Part Time 5 - Band 8 - Range A Full Time 7 1
Part Time 6 - Band 8 - Range B Full Time 20 1
Part Time 3 - Band 8 - Range C Full Time 7 -
Part Time - - Band 8 - Range D Full Time 2 4
Part Time - - Band 9 Full Time 3 3
Part Time - - Non-AfC Full Time - -
Part Time 15 18 VSM Full Time 2 1
Part Time - 1 Grand Total 136 46

Appendix 2 – Pay Grade/Working Hours – Protected Characteristics (continued)
Payscale Working Hours
BME Undeclared White Grand Total
Band 2 Full Time - - - -
Part Time - - - -
Band 3 Full Time 1 - - 1
Part Time - - 1 1
Band 4 Full Time 7 1 5 13
Part Time 1 - 3 4
Band 5 Full Time 5 1 11 17
Part Time - - 2 2
Band 6 Full Time 10 1 12 23
Part Time - 1 4 5
Band 7 Full Time 3 1 13 17
Part Time 1 - 4 5
Band 8 - Range A Full Time 4 1 3 8
Part Time 3 1 2 6
Band 8 - Range B Full Time 2 1 18 21
Part Time - - 3 3
Band 8 - Range C Full Time - - 7 7
Part Time - - - -
Band 8 - Range D Full Time - - 6 6
Band 9 Full Time 1 1 4 6
Non-AfC Full Time - - -
Part Time 8 1 24 33
VSM Full Time - - 3 3
Part Time - - 1 1

14
Appendix 2 – Pay Grade/Working Hours – Protected Characteristics (continued)
Payscale Working Hours Disability - No Undeclared Disability - Yes Grand Total Band 2 Full Time - - - -
Part Time - - - - Band 3 Full Time 1 - - 1
Part Time 1 - - 1 Band 4 Full Time 12 1 - 13
Part Time 4 - - 4 Band 5 Full Time 14 2 1 17
Part Time 1 - 1 2 Band 6 Full Time 20 2 1 23
Part Time 5 - - 5 Band 7 Full Time 12 2 3 17
Part Time 4 - 1 5 Band 8 - Range A Full Time 7 1 - 8
Part Time 6 - - 6 Band 8 - Range B Full Time 17 3 1 21
Part Time 3 - - 3 Band 8 - Range C Full Time 7 - - 7 Band 8 - Range D Full Time 6 - - 6 Band 9 Full Time 5 1 - 6 Non-AfC Full Time - - - -
Part Time 25 7 1 33 VSM Full Time 3 - - 3
Part Time 1 - - 1

15
Appendix 3 – Recruitment & Selection Overview
Applications Shortlisted Appointed Gender Male 831 160 14 Female 3,102 637 49 Undisclosed 24 8 -
Disability Yes 136 38 - No 3,768 752 63 Undisclosed 53 15 -
Ethnicity White 2,058 420 25 BME 1,791 357 38 Undisclosed 108 28 -
Age Group Under 20 89 7 - 20-29 years 1,283 224 11 30-39 years 1,087 244 18 40-49 years 797 163 19 50-59 years 604 146 13
60-64 years 85 16 2
65+ years 11 5 - Undisclosed 1 - -
Religion / Belief Atheism 373 77 10 Christianity 1,842 81 9 Hinduism 281 400 32 Islam 536 56 4 Other 501 86 3 Undisclosed 424 105 3
Sexual Orientation LGB 87 15 3 Heterosexual 3,550 717 59 Undisclosed 320 73 1
Marital Status Married / Civil Partnership 1,634 339 35 Single 1,854 355 21 Legally Separated 42 6 1 Divorced 235 55 3 Widowed 39 13 2 Undisclosed 153 37 1

16
Appendix 4 – Leavers Overview
Characteristic Leavers (2015) 2016 Leavers Gender
Male 10 16 Female 38 42 Undeclared - -
Disability Yes - 2 No - 50 Undeclared 48 6
Ethnic Origin White 34 35 BME 13 19 Undeclared 1 4
Age Band Under 20 - - 20 to 39 5 17 40 to 49 13 13 50 to 65 28 11 65+ - -
Religion / Belief Atheism 9 9 Christianity 18 24 Hinduism 1 6 Islam - 2 Other 4 4 Undeclared 16 13
Sexual Orientation LGB - 2 Heterosexual 33 48 Undeclared 15 8
Marital Status Married / Civil Partnership 28 31 Single 9 16 Legally Separated / Divorced / Widowed 8 6 Undeclared 3 5

17
Appendix 5 – Leaving Reasons – Protected Characteristics Leaving Reason Female % Male % Voluntary resignation – promotion 21.43 43.75 Voluntary resignation – work life balance 26.19 6.25 Retirement age 11.90 6.25 Voluntary resignation – other/not known 11.90 6.25 Voluntary resignation – relocation 7.14 6.25 Voluntary resignation – better reward package 2.38 18.75 End of fixed term contract 7.14 - Redundancy – compulsory 7.14 - Voluntary resignation – lack of opportunities 2.38 6.25 Voluntary early retirement – with actuarial reduction 2.38 - Voluntary resignation – child dependents - 6.25 Leaving Reasons – Gender Leaving Reason White % BME % Undisclosed % Voluntary resignation – promotion 17.14 47.37 25.00 Voluntary resignation – work life balance 22.86 15.79 25.00 Retirement age 14.29 5.26 - Voluntary resignation – other/not known 11.43 - 50.00 Voluntary resignation – relocation 8.57 5.26 - Voluntary resignation – better reward package 2.86 15.79 - End of fixed term contract 5.71 5.26 - Redundancy – compulsory 5.71 5.26 - Voluntary resignation – lack of opportunities 5.71 - - Voluntary early retirement – with actuarial reduction 2.86 - - Voluntary resignation – child dependents 2.86 - -
Leaving Reasons – Ethnicity Leaving Reason Atheism % Christianity % Islam % Other % Undisclosed % Voluntary resignation – promotion 11.11 25.00 50.00 75.00 23.08 Voluntary resignation – work life balance 22.22 33.33 - - 7.69 Retirement age 11.11 12.50 - 25.00 7.69 Voluntary resignation – other/not known - 8.33 - - 30.77 Voluntary resignation – relocation 22.22 4.17 - - 7.69 Voluntary resignation – better reward package - 8.33 50.00 - - End of fixed term contract 11.11 - - - 7.69 Redundancy – compulsory - 4.17 - - 7.69 Voluntary resignation – lack of opportunities 11.11 4.17 - - - Voluntary early retirement – with actuarial reduction 11.11 - - - - Voluntary resignation – child dependents - - - - 7.69
Leaving Reasons – Religion / Belief
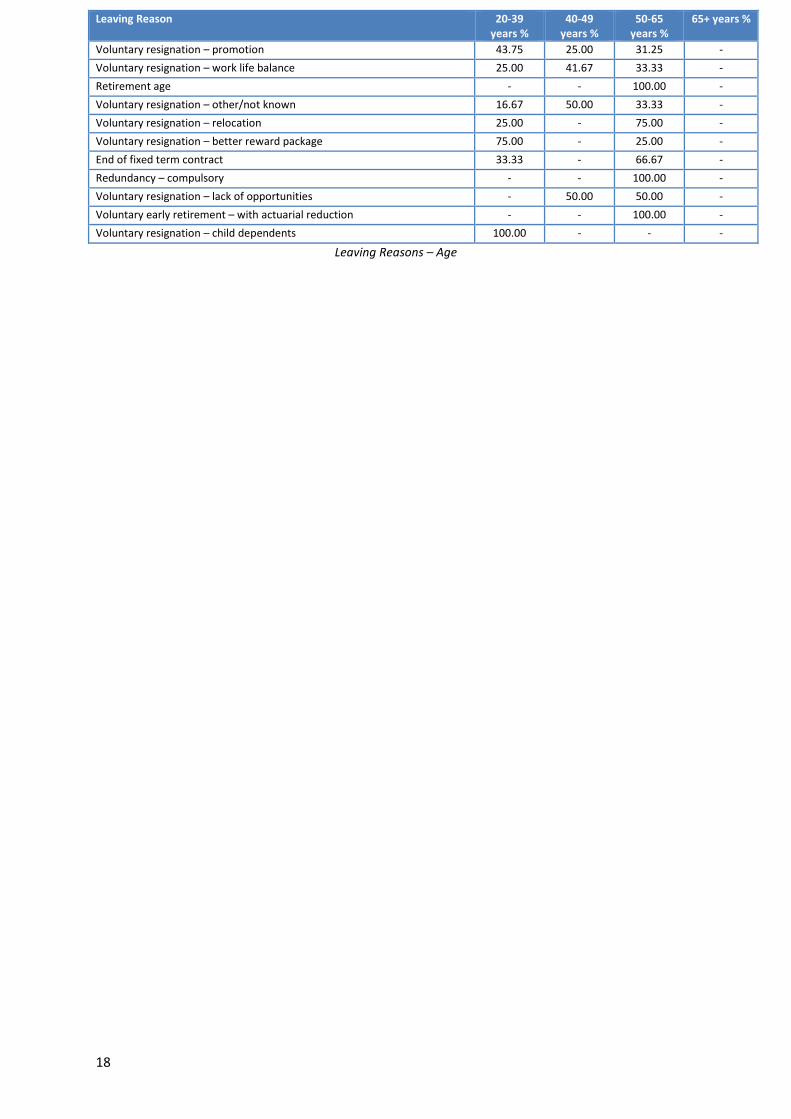
18
Leaving Reasons – Age
Leaving Reason 20-39 years %
40-49 years %
50-65 years %
65+ years %
Voluntary resignation – promotion 43.75 25.00 31.25 - Voluntary resignation – work life balance 25.00 41.67 33.33 - Retirement age - - 100.00 - Voluntary resignation – other/not known 16.67 50.00 33.33 - Voluntary resignation – relocation 25.00 - 75.00 - Voluntary resignation – better reward package 75.00 - 25.00 - End of fixed term contract 33.33 - 66.67 - Redundancy – compulsory - - 100.00 - Voluntary resignation – lack of opportunities - 50.00 50.00 - Voluntary early retirement – with actuarial reduction - - 100.00 - Voluntary resignation – child dependents 100.00 - - -

19
APPENDIX 6 - Mandatory Training Participation Rates by Protected Characteristics
Age 20-29 30-39 40-49 50-59 60-69 70-79 No 18.18% 0.00% 35.90% 25.49% 28.57% 0.00% Yes 81.82% 100.00% 64.10% 74.51% 71.43% 100.00%
Gender Female Male No 18.69% 43.33% Yes 81.31% 56.67%
Ethnicity BME Undisclosed White No 21.88% 22.22% 25.00% Yes 78.13% 77.78% 75.00%
Disability No Undisclosed Yes No 19.82% 52.94% 22.22% Yes 80.18% 47.06% 77.78%
Religion & Belief
Atheism Christianity Hinduism Islam Other Undisclosed
No 27.78% 17.54% 20.00% 0.00% 23.08% 32.56% Yes 72.22% 82.46% 80.00% 100.00% 76.92% 67.44%
Sexual Orientation
Heterosexual LGB Undisclosed
No 19.19% 25.00% 38.24% Yes 80.81% 75.00% 61.76%
Marital Status
Divorced Legally Separated
Married/Civil Partnership
Single Undisclosed Widowed
No 30.00% 50.00% 25.32% 18.75% 25.00% 0.00% Yes 70.00% 50.00% 74.68% 81.25% 75.00% 100.00%

SPACER PAGE
SPACER PAGE

Page 1 of 5
NHS Herts Valleys Clinical Commissioning GroupBoard Meeting 9 March 2017
Title Communications and Engagement Report Agenda Item: 11
Purpose (tick one only) Decision or Approval ☐ Discussion ☐ Information ☒
Responsible Director(s) and Job Title
Juliet Rodgers, Associate Director of Communications and Engagement.
Author and Job Title Juliet Rodgers, Associate Director of Communications and Engagement. Short Summary of Paper This paper summarises key communications and engagement activities since the last
board meeting in public Recommendation(s) The board is being asked to:
To note communications and engagement activities for the period. Engagement with Stakeholders/Patient/Public
The report includes a key section on how patients, carers and public are involved in the work of the CCG.
Links to Strategic Objectives (tick all that apply) Objective 1: We will continually improve engagement with patients, carers, the public and member practices so that they contribute to and influence our work and activities.
☒
Objective 2: We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to stay well and avoid ill health.
☐
Objective 3: We will work with health and social care partners to transform the delivery of care through the implementation of Your Care, Your Future, the strategic review in west Hertfordshire.
☒
Objective 4: We will ensure that there is a financially sustainable and affordable healthcare system in West Hertfordshire.
☐
Board Assurance Framework (BAF) and Corporate Risk Register (CRR) What current risks does this report align to?
Activities reported here provide evidence of work to engage with public, staff and membership – key issues on Board Assurance Framework.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Work reported here mitigates risk in the corporate register around engagement with the public in e.g. service re-design; relationships; and reputational risk.
Resource Implications Within existing resources. Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
Our engagement work seeks to include our diverse communities. An Equality Analysis was completed for the public participation strategy.
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☒ Improved Patient Access and Experience ☒
A Representative and Supported Workforce ☒
Inclusive Leadership ☒
Report History Which Groups or Committees have seen this report and when?
None
Appendices None.

Page 2 of 5
NHS Herts Valleys Clinical Commissioning GroupBoard Meeting 9 March 2017
1. Introduction and purpose of paperThis paper summarises the communications and engagement activity for the previous period.
2. Public facing campaignsWe have just concluded the final phase of our local promotion of the national Stay Well this Winter campaign where we reminded people that it wasn’t too late to get the flu jab. We also encouraged people to seek help and advice from their local community pharmacist at the first signs of illness.
More recently we have focused our campaign activities on promoting Patient Online, encouraging patients to register for this service. We have handed out information at roadshows and public events, including the Your Care, Your Future locality meetings. There was also a presentation to the public and patient involvement committee (PPI), information to staff and all our regular bulletins to members and stakeholders. We also issued a press release and one of our patient practice group reps did a slot on a community radio show.
We have also supported national public health campaigns such as Dry January, Be Clear on Cancer, Time to Talk and Feeling Good Week.
3. Patient and public participation
We have launched our engagement on the review of urgent care services which starts with a survey asking local people about their views and experiences of urgent care services in this area. We are asking as many people as possible to complete the survey before it closes at the end of March.
The PPI development session on 6 March ‘Community Support – let’s get connected’ focuses on local community and support groups and organisations. We will be exploring how these groups can work with practice patient groups, sharing information and support and influencing health services.
Colleagues spoke at a meeting of Hertbeats recently. This is a St Albans community group and up to 40 people came to talk about issues around how the NHS works, with a focus on financial challenges and our Your Care, Your Future programme.
Your Care, Your Future information and engagement events are taking place each of the four localities in west Hertfordshire in the first three months of 2017. The events are focusing on plans to provide more integrated health and care services in communities and reduce trips to hospital. Locality GPs and GP board members are playing a lead role in highlighting what is already happening to develop care closer to home and updating on future plans. Each event has looked at public health profiles and local health needs-related priorities.
The first three events in Dacorum, Watford and Three Rivers and St Albans and Harpenden were well attended with a good level of engagement. Feedback from those submitting comments has been positive. They have rated the events very/quite useful (82% Dacorum

Page 3 of 5
NHS Herts Valleys Clinical Commissioning GroupBoard Meeting 9 March 2017
and 100% Watford and Three Rivers) and all those commenting would consider attending future events. Information about the St Albans and Harpenden event is being collated.
We are arranging a date for the Hertsmere one which will be advertised as soon as we have details. The first three events reached a broadly similar demographic to previous events, though the make-up of the Watford and Three Rivers audience was slightly younger and more diverse. Efforts will continue during 2017 to engage with a more diverse range of people and organisations, particularly younger people and those with ‘protected characteristics’ who have been less well represented in feedback to date. We will be working with members of the Your Care, Your Future communications and engagement group, which includes Healthwatch Hertfordshire, to help achieve this.
A summary of the health needs will be contained within locality-focussed commissioning plans and these will be discussed at the next board meeting in May.
There has been a positive reaction to the Your Care, Your Future newsletter issued in early February. This updated readers on acute hospital reconfiguration, development of new care pathways and promoted the locality events.
Patients have continued to send in letters expressing their views on acute hospital transformation plans and to lobby for a new hospital on a greenfield site. Since the preferred option was announced in October, 22 letters have been received: 16 from local residents (some of these are people writing two or more times); three from MPs (Mike Penning and David Gauke) and three from national/regional NHS offices to assist with responses to enquiries. We have responded to all letters.
We are running a public survey with East and North Hertfordshire CCG during March, to gather views from local people about priorities in healthcare in the future, given the considerable ongoing financial challenges for everyone. We hope to raise awareness and to gain some insight to support further work in the coming months around commissioning policies.
4. Media coverageWe have continued to receive media enquiries and see coverage on our decision not to repeat the payment of additional discretionary funding to Hertfordshire County Council’s social care budget. The Watford Observer has carried a couple of brief articles, quoting HCC’s cabinet member for adult care, Colette Wyatt-Lowe, followed by a more extensive piece on 17 February which quoted extensively from the Herts Valleys statement.
That same week, the Hemel Gazette featured a two-page special headlined ‘Health cash row goes all the way to Westminster’ about HCC’s consideration of a possible referral to the Secretary of State for Health. There were quotes from county councillors and the feature included a lengthy section of the Herts Valleys statement.
In addition the issue was discussed on BBC Three Counties Radio on the Andy Collins Show on Thursday 19 January. It included interviews with Cllr Tindall, Geoff Brown of Healthwatch

Page 4 of 5
NHS Herts Valleys Clinical Commissioning GroupBoard Meeting 9 March 2017
Hertfordshire, Colette Wyatt-Lowe and our board GP Dr Trevor Fernandes. Broadcast coverage also included a piece on BBC London TV on 20 February.
Your Care, Your Future- related items including acute hospital transformation and locality meetings also featured in local newspapers. In broad terms the Hemel Hempstead Gazette continues to champion the campaign to build a new hospital on a greenfield site, whereas the Watford Observer has supported plans for the redevelopment of the current Watford and St Albans sites. Most of the negative coverage has been on letters pages, and we have responded publicly to many of these.
We have issued media releases on: Patient Online, Your Care, Your Future locality events, Hertfordshire’s pharmacy survey, new provider of Hertfordshire urgent care and our recent regional social prescribing event.
5. Staff communications and engagementWe held our first staff learning afternoon – a new session introduced to encourage staff to attend short sessions run by colleagues on a specific topic or work area. Topics at our first afternoon session were stakeholder engagement, NHS counter fraud and the Freedom of Information Act.
We continue to hold well-attended monthly face-to-face staff briefings led by Cameron Ward with short “pop-ups” from colleagues to provide updates on a range of projects and issues. Last month this included a slot from GP board member Dr Richard Pile who talked about prevention of poor health and what we, as commissioners, are doing to contribute towards this aim. We regularly brief staff on our financial position.
6. Member practice communications and engagementOur most recent GP forum that took place on Thursday 16 February was well attended with around 100 representatives present. The agenda included: delegated commissioning and general practice five year forward view; the local financial position; locality commissioning and GP federation updates; and a session on DXS (portal for GP referral forms). GPs also had the opportunity to hear from and meet Kathryn Magson, Herts Valleys’ new chief executive who joins on 16 March.
Readership of the weekly e-bulletin for member practice continues to increase and requests from providers and community groups to contribute content remains high.
7. Other
Hertfordshire County Council health scrutiny committee We attended a special day-long session at HCC’s health scrutiny meeting early in February to address issues arising out of our decision not to make an additional discretionary payment to their social care budget.

Page 5 of 5
NHS Herts Valleys Clinical Commissioning GroupBoard Meeting 9 March 2017
360 stakeholder survey The annual NHS England-commissioned survey of the stakeholders of all CCGs launched earlier this year – following feedback about the timing. The survey seeks feedback from the full range of stakeholders, including our GP membership, partner organisations and patient representatives. This year the survey was run earlier than previously and closed at the end of February. We expect to be getting results in time for a discussion at the May board meeting. Social media On social media we have been tweeting about Feeling Good Week, effective use of antibiotics, reminders about our Your Care, Your Future events, cold weather advice on how to Stay Well This Winter and A&E under pressure. We are approaching 4,000 followers on Twitter. We continue to monitor and, where appropriate, contribute to health-related discussions on community facebook pages in Watford, Three Rivers and Dacorum. These are the districts with the most active pages. There was some especially interesting discussion following the Your Care, Your Future locality meeting in Dacorum, some of it favourable in terms of feeding back that the session helped people to understand the complexities of the plans and proposals under discussion.

SPACER PAGE

SPACER PAGE
1
NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Board Assurance Framework 2016/17 Q4 (position at 28 February 2017)
Agenda Item: 12
Purpose (tick one only) Decision or Approval ☒ Discussion ☐ Information ☐
Responsible Director(s) and Job Title
Rod While, Head of Corporate Governance
Author and Job Title Katy Patrick, Risk Manager
Short Summary of Paper The paper presents in summary the Board Assurance Framework (BAF) - Appendix 1 with assurances and actions updated to mid- Q4 (28 February 2017). The paper also outlines a proposal for review of the BAF for 2017/18.
Recommendation(s) The Board is being asked to:
Review and discuss the BAF 2016/17 to date. Approve the outcome of the review of BAF risks for 2017/18.
Engagement with Stakeholders/Patient/Public
N/A
Links to Strategic Objectives (tick all that apply)
Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☒
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
All of the risks on the Board Assurance Framework (BAF) and Corporate Risk Register (CRR) are relevant.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
N/A
Resource Implications There are no additional funding implications.
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
N/A

2
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☒
Improved Patient Access and Experience ☒
A Representative and Supported Workforce ☒
Inclusive Leadership ☒
Report History Which Groups or Committees have seen this report and when?
The Q4 (26 January position) has been presented to the Quality &Performance Committee, Executive Team and Audit Committee.
Appendices Appendix 1 BAF Summary presentation
1. Introduction
1.1 The board assurance framework (BAF), as part of the fundamental core of HVCCG’s internal
control systems, identifies all risks which potentially impact on achievement of the CCG’s four
strategic objectives. The nature and relative sizes of these risks are set out in Section 2.1 below.
1.2 This paper provides the Board with a summary of the updated BAF for 2016/17 and the
quarter 4, 28 February 2017 position, following meetings with individual risk owners, the executive
team and assistant directors. Changes made to the BAF since quarter 1 2016/17 are set out in
section 2.2 below.
1.3 The BAF summary at Appendix 1 outlines specific control measures that the CCG has put in place
to manage the identified risks and the independent assurances relied upon by the Board to
demonstrate that these are operating effectively. This report includes graphs showing individual risk
movements over time.
1.4 Whilst this framework identifies the significant potential risks which may threaten achievement
of the CCG’s strategic objectives, any related risks requiring specific mitigating actions are cross-
referenced and documented fully within the CCG’s corporate risk register.
1.5 The BAF and CRR are reviewed monthly with individual risk owners and reported at least
quarterly through the Board and its Committees.
1.6 SLT members have been asked to consider any additions or alterations required to the strategic
risks on the BAF, particularly in the light of the ten priorities for 2017-18 agreed as part of the
operational plan at the January Board meeting. Only one change - to the risk description for BAF 2.3
has been proposed - as noted below.
2. Strategic risks in Q4, at 28 February 2017.2.1 Relative positions of threats to strategic objectives.
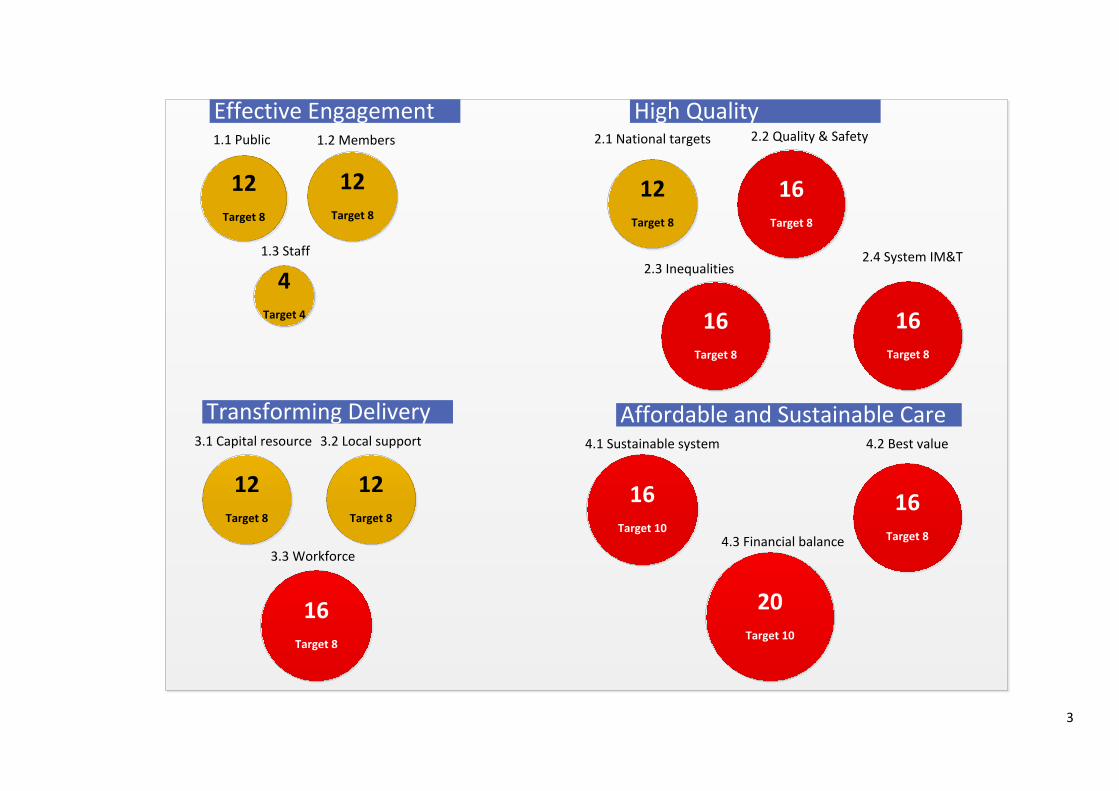
3
12Target 8
12Target 8
4Target 4
1.1 Public 1.2 Members
1.3 Staff
12Target 8
16Target 8
16Target 8
2.1 National targets 2.2 Quality & Safety
2.3 Inequalities2.4 System IM&T
12Target 8
3.1 Capital resource
12Target 8
3.2 Local support
16Target 8
3.3 Workforce
16Target 10
20Target 10
16Target 8
4.1 Sustainable system 4.2 Best value
4.3 Financial balance
Effective Engagement High Quality
Transforming Delivery Affordable and Sustainable Care
16Target 8
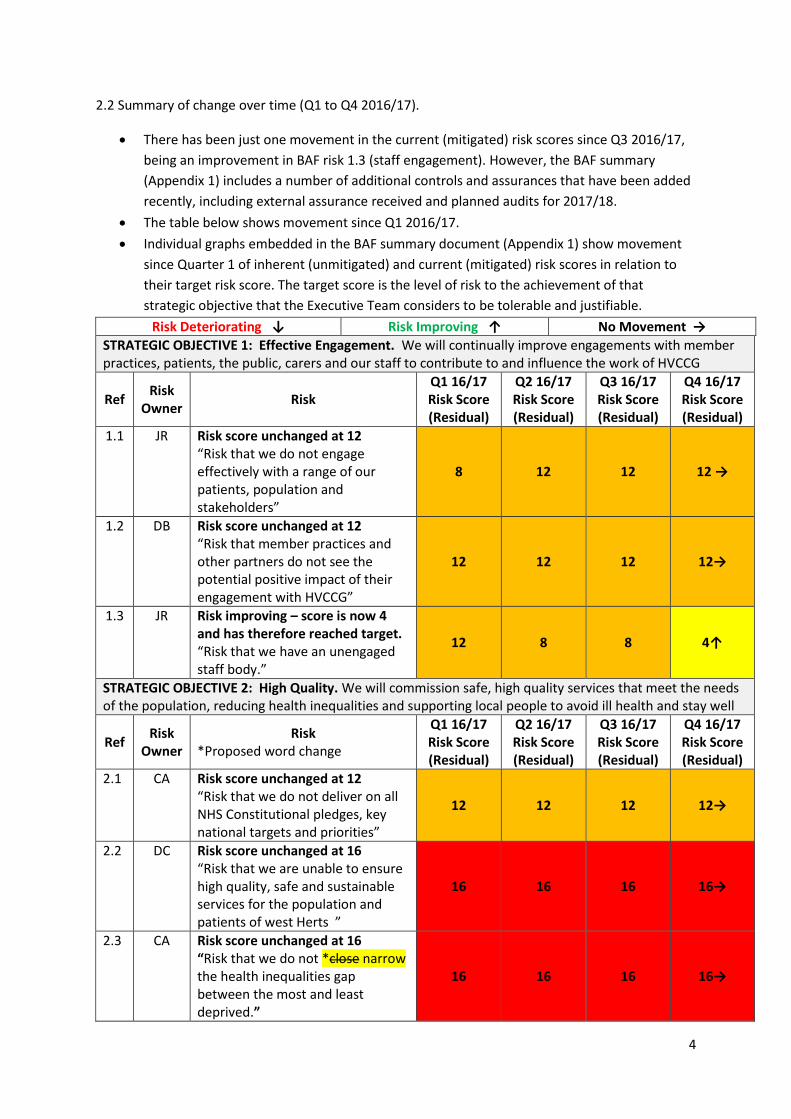
4
2.2 Summary of change over time (Q1 to Q4 2016/17).
There has been just one movement in the current (mitigated) risk scores since Q3 2016/17,
being an improvement in BAF risk 1.3 (staff engagement). However, the BAF summary
(Appendix 1) includes a number of additional controls and assurances that have been added
recently, including external assurance received and planned audits for 2017/18.
The table below shows movement since Q1 2016/17.
Individual graphs embedded in the BAF summary document (Appendix 1) show movement
since Quarter 1 of inherent (unmitigated) and current (mitigated) risk scores in relation to
their target risk score. The target score is the level of risk to the achievement of that
strategic objective that the Executive Team considers to be tolerable and justifiable.
Risk Deteriorating ↓ Risk Improving ↑ No Movement →
STRATEGIC OBJECTIVE 1: Effective Engagement. We will continually improve engagements with member practices, patients, the public, carers and our staff to contribute to and influence the work of HVCCG
Ref Risk
Owner Risk
Q1 16/17 Risk Score (Residual)
Q2 16/17 Risk Score (Residual)
Q3 16/17 Risk Score (Residual)
Q4 16/17 Risk Score (Residual)
1.1 JR Risk score unchanged at 12 “Risk that we do not engage effectively with a range of our patients, population and stakeholders”
8 12 12 12 →
1.2 DB Risk score unchanged at 12 “Risk that member practices and other partners do not see the potential positive impact of their engagement with HVCCG”
12 12 12 12→
1.3 JR Risk improving – score is now 4 and has therefore reached target. “Risk that we have an unengaged staff body.”
12 8 8 4↑
STRATEGIC OBJECTIVE 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well
Ref Risk
Owner Risk
*Proposed word change
Q1 16/17 Risk Score (Residual)
Q2 16/17 Risk Score (Residual)
Q3 16/17 Risk Score (Residual)
Q4 16/17 Risk Score (Residual)
2.1 CA Risk score unchanged at 12 “Risk that we do not deliver on all NHS Constitutional pledges, key national targets and priorities”
12 12 12 12→
2.2 DC Risk score unchanged at 16 “Risk that we are unable to ensure high quality, safe and sustainable services for the population and patients of west Herts ”
16 16 16 16→
2.3 CA Risk score unchanged at 16 “Risk that we do not *close narrow the health inequalities gap between the most and least deprived.”
16 16 16 16→

5
2.4 CH Risk score unchanged at 16 “Risk of lack of adequate system capability in the management and security of information, data and technology”
20 16 16 16→
STRATEGIC OBJECTIVE 3: Transforming Delivery. Work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the strategic review in west Hertfordshire
Ref Risk
Owner Risk
Q1 16/17 Risk Score (Residual)
Q2 16/17 Risk Score (Residual)
Q3 16/17 Risk Score (Residual)
Q4 16/17 Risk Score (Residual)
3.1 CA Risk score unchanged at 12 “Risk that the joint submission to obtain additional capital resource to successfully transform the delivery of care in west Hertfordshire is unsuccessful.”
12 12 12 12 →
3.2 CA Risk score unchanged at 12 “Risk that there will be insufficient support from local bodies and key stakeholders to transform the delivery of care in west Hertfordshire.”
12 12 12 12 →
3.3 CA Risk score unchanged at 16 “Risk that workforce issues will prevent us from transforming the delivery of care across the local health and social care system.”
12 16 16 16 →
STRATEGIC OBJECTIVE 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in West Hertfordshire
Ref Risk
Owner Risk
Q1 16/17 Risk Score (Residual)
Q2 16/17 Risk Score (Residual)
Q3 16/17 Risk Score (Residual)
Q4 16/17 Risk Score (Residual)
4.1 CH Risk score unchanged at 16 “Risk that we do not deliver a financially sustainable health and social care system.
20 16 16 16→
4.2 CH Risk score unchanged at 16 “Risk that we do not deliver best value from the total CCG budget”
16
16
16
16→
4.3
CH Risk score unchanged at 20 “Failure to achieve the agreed control total for 2016/17”
15 20 20 20→
3. Recommendations
The Committee is asked to review and discuss the BAF 2016/17 current position, and approve the proposal from SLT that there is only one change to the BAF for 2017/18.
1. Board Assurance Framework 2016/17 at 28 February 2017, summary presentation.

STRATEGIC OBJECTIVE 1: Effective Engagement. We will continually improve engagement with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
BAF RISK 1.1 Risk that we do not engage effectively with a range of our patients, population and stakeholders. CAUSES: (A) Lack of commitment, (B) Unclear approach and absence of strategy, (C) Availability of funding, (D) Limited workforce capacity and capability. ASSURANCE SUMMARY Q4 2016/17 (Feb): Quarter 4 includes many patient and public stakeholder engagement initiatives, including: locality conversation events; consultation to support development of new models of care for unplanned, urgent and emergency services; understanding and input for the local digital strategy; steering group for integrated personal commissioning; support for Patient Online. The Communications and Engagement team are also involved in dissemination of information to stakeholders on an on-going basis about such matters as: the CCG's financial position; the move to delegated commissioning; discussions with partners about joint commissioning. A range of media are employed, including the Stakeholder Briefing; face-to-face meetings; press releases; presentations to a variety of groups and response to individual correspondence.
Inherent Risk Residual Risk Target Risk
16 12 8
RISK OWNER: Associate Director of Communications & Engagement RISK LEAD: Associate Director of Communications & Engagement
CONTROLS 1. Public Participation Strategy and Implementation Planprovides consistency of process (B)
2. Joint Commissioning Teams helps engagement withstakeholders (A), (B)
3. Patient representatives at Locality Meetings (A)
4. Patient & Public Involvement Representative attendsHVCCG Board; Lay Board Member with Lead for Patient Engagement in place.(A) 5. Public Board meetings (A)6. Communications and Engagement Strategy in place (B)
7. Engagement with key public groups and monitoring atPublic Participation & Involvement Committee. (Chaired by Lay Member) (A), (B) 8. Monitoring at Commissioning Executive and HVCCGBoard (A), (B), (C), (D)
9. Your Care, Your Future (A), (B), (C), (D)
10.Your Care, Your Future Clinical Engagement Subgroup(A), (B), (D)
11. Planned and Primary Care Network chaired by HealthWatch meets bi- monthly (A), (B)
12. Local Medical Committee, Local PharmaceuticalCommittee and West Herts Clinical Engagement Group feeds into HVCCG Programme Board (A), (B) 13. Service redesign/ transformation groups have
ASSURANCES 1.Public Participation Strategy approved by Commissioning Executiveand HVCCG Board (+) 1.Each Public Participation & Involvement Committee receives areport on progress against the Implementation Plan (+) 1. 2014/15 NHS England Stakeholder Survey (+)2. Progress reports to Public Participation & Involvement Committeeand HVCCG Board (+) 2. 2014/15 NHS England Stakeholder Survey (+)3. Progress reports to Public Participation & Involvement Committeeand HVCCG Board (+) 4. Communication & Engagement Report to HVCCG Board (+)
5. Part 1 Board Meeting open to public with papers online (+)6. Updates on stakeholder and public participation provided to PublicParticipation & Involvement Committee and HVCCG Board (+) 7. Public Participation & Involvement Committee reporting to HVCCGBoard (+)
8. Commissioning Executive and Board fully assured thattransformation of services has taken into account a fair representation of stakeholders (+) 9. Clinical Engagement Subgroup and Your Care, Your Future feedsinto the Commissioning Executive Meeting and each HVCCG Board Meeting (+) 10. Clinical Engagement Subgroup and Your Care, Your Future feedsinto the Commissioning Executive Meeting and each HVCCG Board Meeting (+) 11. Planned and Primary Care Network agendas set by Healthwatchand HVCCG jointly. The Network reports to the Planned and Primary Care Programme which reports to the Commissioning Executive. (+) 12. Programme Board has extended attendance invitation to all mainproviders for Part 2 Programme Board (+)
13. Stakeholders involved in redesigning of services from
ACTION PLAN & UPDATES 1.Implementation of the updatedstrategy produced by the Your Care, Your Future Communications & Engagement Group for the current phase of the programme. 2. Engagement over next phase isunderway with a focus on local services: - Conversation events have been held in Dacorum, Watford & Three Rivers and St Albans & Harpenden localities. Events well attended in Dacorum (31 Jan); Watford & Three Rivers (8 Feb); and St Albans & Harpenden (28 Feb). The Hertsmere engagement event is being planned for end of March 3. The strategic outline case for acutereconfiguration has been approved by the WHHT Board and supported by the HCC Scrutiny Committee. A report on engagement was included as part of the SOC report. Feedback from NHS England supports a review of plans to take into account the current financial circumstances. 4. Considerable engagement via localmedia on current issues such as acute reconfiguration 5. Continued correspondence withindividuals on key YCYF issues 6. YCYF newsletter issued7. Stakeholder letters issued8. Patient representation on Hemelhub project team
COMPLETION DATE 1. March 2017
2. Jan to Mar 2017
3. SOC review by June 2017

relevant patient and other stakeholder representatives who are involved in the redesigning of services (A), (B)
14. All business cases are presented to highlight time andresource required in order to ensure objectives of transforming services are delivered (A), (C), (D) 15. Re-launched Equality and Quality Impact Assessment(A) 16. Senior Managers attend Health Scrutiny Meetings andHealth & Wellbeing Boards (A), (B) 17. Enhanced monitoring and reporting mechanismsdeveloped (A), (B) 18. Your Care, Your Future intensive engagement overhospital options appraisal has taken place (A), (B) 19. Exec summary of STP plan published and circulatedboth internally & externally (A), (B) 20. Update on HVCCG financial situation was discussed ata Board meeting in public and at the Patient & Public Participation Committee and communicated in two stakeholder letters (A), (B) 21. New approach to expanding involvement via practiceparticipation groups agreed by PPI
development to procurement. E.g. enhanced respiratory services, ongoing engagement with public and stakeholders on Gynaecology and Cardiology and all Your Care, Your Future work streams. (+) 14. Business case submissions reviewed by Commissioning Executive(+)
15. All policies and policy revisions include the EQIA (+)
16. Reports to the Commissioning Executive and HVCCG Board fromHealth Scrutiny Meetings and Health Wellbeing Boards (+) 17. Quality Alert System; Locality and GP briefings; Performance Packs(+) 18. Public Participation & Involvement Committee, GP Forum, HVCCGBoard (+) 19. Intranet, STP Website, stakeholder comms
20. Public Participation & Involvement Committee, HVCCG Boardstakeholder communications.
21. PPI minutes
9. PPI committee discussions oncurrent issues such as social care funding 10. Investment committee decisionsconveyed to PPI committee 11.Engagement underway to informthe development of future models of urgent care by gathering information on patient and public experience of using unplanned, urgent and emergency services, including: - West Herts Medical Centre - NHS 111 - Minor injuries unit at St Albans - Urgent Care Centre in Hemel Hempstead - Accident & Emergency in Watford. Patient representation on the group. 12. Engagement with patient forumsis planned to ensure their understanding of the Local Digital Roadmap and help them to play and active part in helping the STP to use technology to the best advantage of patients. 13. A steering group is being formedcomprising representatives of many ages from a variety of agencies to help progress the integrated personal commissioning project. 14. Materials and information arebeing provided to support awareness-raising and promotion of Patient Online. 15.Survey launching – with ENHCCG(and likely to become STP-wide initiative) to gather public views of priorities in a financially challenging environment.
11. end March 2017
12. April 2017
15. March 2017

CORPORATE RISK REGISTER LINKS RISK MOVEMENT
SO1/24 Risk that public and stakeholders are not informed effectively.
0
2
4
6
8
10
12
14
16
18
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 1: Effective Engagement. We will continually improve engagement with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
BAF RISK 1.2 Risk that member practices and other partners do not see the potential positive impact of their engagement with HVCCG CAUSES: (A) Failure to communicate effectively, (B) Pressures in general practice, (C) Unclear approach and absence of strategy ASSURANCE SUMMARY Q4 2016/17 (Feb): GP Forum 16 February 2017 was well attended. The GP Forum, held six monthly, is the only event at which all of our practices are represented. These meetings are therefore an important opportunity for the CCG to explain their plans and answer questions.
Inherent Risk Residual Risk Target Risk
20 12 8
RISK OWNER: Medical Director RISK LEAD: Associate Director of Communications & Engagement
CONTROLS 1. Your Care, Your Future has been developed withsignificant engagement through programmes of care, enablers and localities (A), (B), (C)
2. Member Practice Engagement Plan and Communications& Engagement Strategies in place (A), (B), (C)
3. GP Forums, weekly bulletins, GP intranet and PracticeManagers Forum all facilitate two-way discussion and information sharing (A), (B) 4. Locality Board structure and management arrangementsin place to increase engagement. Monthly locality briefings capture highlights from meetings (A), (B)
5. Bi-monthly Training, Education, Research and LearningGroup in place chaired by HVCCG Chair (A), (B), (C) 6. Joint commissioning of primary medical services withNHS England (B), (C)
7. Annual practice visits to engage member practices andenhance quality of Primary Care led by Executives, Locality Officers and Locality Clinical Leads (A), (B), (C)
8. Investment of £1.5m over three years to increasecapacity in primary care (supporting additional appointments) and a holistic assessment team in Dacorum (B), (C) 9. Stakeholder engagement activity reported separatelythrough the Accountable Officer report to the Board on a
ASSURANCES 1.The Member Practices' Commissioning Agreement (MPCA)has been revised for 2016/17 and is under consultation to ensure Membership engagement at locality, practice and CCG level (+) 1. Annual NHS England 360° Stakeholder Survey (+)2. The Member Practices' Commissioning Agreement (MPCA)has been revised for 2016/17 and is under consultation to ensure Membership engagement at locality, practice and CCG level (+) 2. InterLoc meetings discuss concerns and share good practicewith GP practices (+) 2. Annual NHS England 360° Stakeholder Survey (+)2. Amber/Green Internal Audit Opinion for Member PracticeEngagement 3. Practice Manager Forum introduced following engagementwith GPs (+). Six monthly feedback from GPs was positive (+)
4. All work undertaken on the Plan on a Page is reportedmonthly to Locality Board Meeting and reported for information to HVCCG Board quarterly. Locality Chairs are also members of the Commissioning Executive (+) 5. Practice Nurse and GP Education Programme secured fundingthrough the Health Education Programme 2015/16 (+) 6. All clinical programmes led by a clinician who has extensiveclinical engagement and a representative from all localities. This strengthens the synergy with the Strategy (Your Care, Your Future) (+) 7. Practice visit from May 2015 gave in-depth insight into the'real' pressures in primary care. This led to action on how HVCCG can support member practices during CQC visits through the sharing of best practice to raise standards (+) 8. Evaluation of year one has shown positive outcomes (+)
9. Accountable Officer’s reports to Board (+)
ACTION PLAN & UPDATES 1. To work with localities and GPs asproviders to find alternative models of care. 2. To work closely with the LMC to helpinform alternative models of care. 3. To plan for 2017/18 and delegatedcommissioning.
COMPLETION DATE 1. Ongoing from Apr 2016
2. Ongoing from Apr 2016
3. Mar 2017

monthly basis (A), (C) 10. Quality Alert System (A)
11. Weekly GP bulletin (A)12. Periodic QIPP briefings (A)13. Plan developed for joint practice visits with NHSE2016/17 (A), (B) 14. GP intranet overhauled (A)15. Localities bulletin reviewed (A)
10. QAS quarterly reports to Quality & Performance Committee(+) 11. Communications Team emails (+)12. Communications Team emails (+)
CORPORATE RISK REGISTER LINKS RISK MOVEMENT
SO1/24 Risk that public and stakeholders are not informed effectively.
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 1: Effective Engagement. We will continually improve engagement with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
BAF RISK 1.3 Risk that we have an unengaged staff body. CAUSES: Failure to implement internal communications strategy (A) Failure to adhere to specific timetables for circulation (B) ASSURANCE SUMMARY Q4 2016/17 (Feb): There is a whole range of different activities in place to ensure that we communicate and engage with our staff. We continue to develop those activities and to listen to suggestions about how we can improve. We have increased the frequency of all-staff face-to-face briefings and they are now monthly. NHS staff survey 2016 results received. Staff involvement group will have this as a key focus over the next few months. SLT to address key issues identified. Staff also receive the broader stakeholder bulletin and regular information about items featured in the national or local press. One Brief is disseminated through all teams by the Senior Leadership Team, with all staff being afforded the opportunity to raise queries in writing and receive responses.The Executive team meeting on 23 February recommended that the current risk score should be reduced to the target score of 4, to reflect the progress made during 2016/17 with staff engagement. It is recommended that this risk should remain on the BAF in order to ensure that the progress made is sustained.
Inherent Risk Residual Risk Target Risk
16 4 4
RISK OWNER: Associate Director of Communications & Engagement RISK LEAD: Associate Director of Communications & Engagement
CONTROLS 1. Staff involvement group2. All staff meetings & staff briefings3. Team briefing
4. Staff wellbeing and social activities
5. Director breakfasts6. Staff surveys7. Refreshing internal communications plan8. Intranet overhauled and re-launched9. Updated internal communications & engagement planhas been discussed and agreed at the staff involvement group and includes actions following NHS staff survey 2016.
ASSURANCES 1. Minutes of Staff Involvement Group2. Standard staff communications channels3. OneBrief delivered at team meetings, feedback collated andreported on, published on intranet 4. Wellbeing noticeboards and displays, publicity for activitiesvia standard staff communications channels 5. Standard staff communications channels6. Standard staff communications channels7. Minutes of Staff Involvement Group8. New intranet site9. Minutes of Staff Involvement Group10. NHS staff survey – and results
ACTION PLAN & UPDATES 1. Staff involvement group working onstaff suggestions. 2. Staff involvement group considering andleading on actions to be taken as result of recent 2016 staff survey results. 3.Staff involvement group reviewingrevised appraisal paper work and exit interview approach. 4. New members joined staff involvementgroup – full complement. 5. Continuous improvement project beingtaken forward. 6. Development of CE staff briefings andembedding regular monthly sessions
COMPLETION DATE 1. On-going
2. March 2017
3. March 2017
CORPORATE RISK REGISTER LINKS RISK MOVEMENT
0
2
4
6
8
10
12
14
16
18
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target
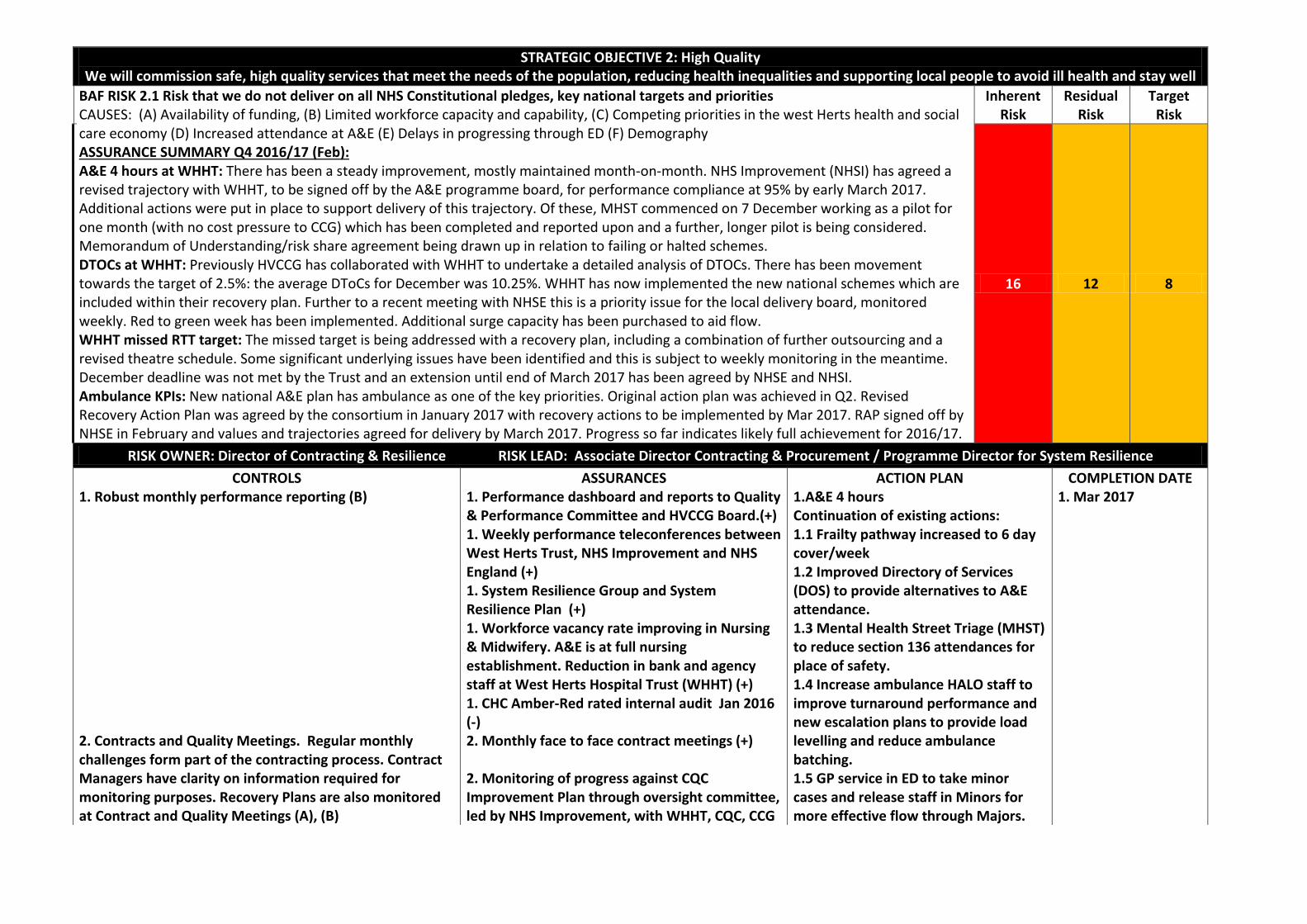
STRATEGIC OBJECTIVE 2: High Quality We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well
BAF RISK 2.1 Risk that we do not deliver on all NHS Constitutional pledges, key national targets and priorities CAUSES: (A) Availability of funding, (B) Limited workforce capacity and capability, (C) Competing priorities in the west Herts health and social care economy (D) Increased attendance at A&E (E) Delays in progressing through ED (F) Demography ASSURANCE SUMMARY Q4 2016/17 (Feb): A&E 4 hours at WHHT: There has been a steady improvement, mostly maintained month-on-month. NHS Improvement (NHSI) has agreed a revised trajectory with WHHT, to be signed off by the A&E programme board, for performance compliance at 95% by early March 2017. Additional actions were put in place to support delivery of this trajectory. Of these, MHST commenced on 7 December working as a pilot for one month (with no cost pressure to CCG) which has been completed and reported upon and a further, longer pilot is being considered. Memorandum of Understanding/risk share agreement being drawn up in relation to failing or halted schemes. DTOCs at WHHT: Previously HVCCG has collaborated with WHHT to undertake a detailed analysis of DTOCs. There has been movement towards the target of 2.5%: the average DToCs for December was 10.25%. WHHT has now implemented the new national schemes which are included within their recovery plan. Further to a recent meeting with NHSE this is a priority issue for the local delivery board, monitored weekly. Red to green week has been implemented. Additional surge capacity has been purchased to aid flow. WHHT missed RTT target: The missed target is being addressed with a recovery plan, including a combination of further outsourcing and a revised theatre schedule. Some significant underlying issues have been identified and this is subject to weekly monitoring in the meantime. December deadline was not met by the Trust and an extension until end of March 2017 has been agreed by NHSE and NHSI. Ambulance KPIs: New national A&E plan has ambulance as one of the key priorities. Original action plan was achieved in Q2. Revised Recovery Action Plan was agreed by the consortium in January 2017 with recovery actions to be implemented by Mar 2017. RAP signed off by NHSE in February and values and trajectories agreed for delivery by March 2017. Progress so far indicates likely full achievement for 2016/17.
Inherent Risk
Residual Risk
Target Risk
16 12 8
RISK OWNER: Director of Contracting & Resilience RISK LEAD: Associate Director Contracting & Procurement / Programme Director for System Resilience
CONTROLS 1. Robust monthly performance reporting (B)
2. Contracts and Quality Meetings. Regular monthlychallenges form part of the contracting process. Contract Managers have clarity on information required for monitoring purposes. Recovery Plans are also monitored at Contract and Quality Meetings (A), (B)
ASSURANCES 1. Performance dashboard and reports to Quality& Performance Committee and HVCCG Board.(+) 1. Weekly performance teleconferences betweenWest Herts Trust, NHS Improvement and NHS England (+) 1. System Resilience Group and SystemResilience Plan (+) 1. Workforce vacancy rate improving in Nursing& Midwifery. A&E is at full nursing establishment. Reduction in bank and agency staff at West Herts Hospital Trust (WHHT) (+) 1. CHC Amber-Red rated internal audit Jan 2016(-) 2. Monthly face to face contract meetings (+)
2. Monitoring of progress against CQCImprovement Plan through oversight committee, led by NHS Improvement, with WHHT, CQC, CCG
ACTION PLAN 1.A&E 4 hours Continuation of existing actions: 1.1 Frailty pathway increased to 6 day cover/week 1.2 Improved Directory of Services (DOS) to provide alternatives to A&E attendance. 1.3 Mental Health Street Triage (MHST) to reduce section 136 attendances for place of safety. 1.4 Increase ambulance HALO staff to improve turnaround performance and new escalation plans to provide load levelling and reduce ambulance batching. 1.5 GP service in ED to take minor cases and release staff in Minors for more effective flow through Majors.
COMPLETION DATE 1. Mar 2017

3. Monitoring by the RTT Programme Board and HVCCGQuality & Performance Committee (B), (C) 4. Financial policies, data sharing and data access policiesin place. (B) 5. Integrated Plan. (HCC and partnership CCGs) (A), (B), (C)
6. System Resilience Group monitoring Urgent andPlanned Care dashboard. (A), (B) 7. Fortnightly performance meetings with NHSImprovement and NHS England. (B)
8. Collaborative work on workforce planning: both short-term fixes and longer-term plans are being worked up. (B), (C) 9. CQC Improvement Plan for West Herts Hospital Trust.(A), (B), (C)
10. Internal Audit of urgent care sustainability 2016/17 (A)– (F)
11. Terms of Reference for the A&E Local Delivery Board(HVCCG's Urgent Care Programme Board) have been reviewed and made more robust in relation to ownership, accountability and delivery against schemes.
and the Deanery (+)
3.Audit activity and assurance demonstrates that the system is working (+) 4. Internal Audit Plan monitoring and review aspart of the internal audit cycle(+) 5. Acute Contracting & PerformanceManagement Green rated Internal Audit January 2016 (+) 6. Reports to, and monitoring from the Quality &Performance Committee (+) 7. Reported to SRG Group and in summary toIntegrated Quality, Performance and Finance Report (IQPFR) 8. Reporting to SRG.
9. NHS Improvement led multi-partnershipOversight Group established to gain assurance that the CQC improvement action plan is robust and that appropriate actions are in place to deliver agreed outcomes and demonstrate improvement. (Chaired by the NHS Improvement Portfolio Director and attended by HVCCG Accountable Officer and Director of Nursing & Quality). Membership also includes NHSE, Healthwatch, Health Education England and the GMC/ LMC.
10. Urgent Care Sustainability internal auditreports partial assurance December 2016 with all recommendations agreed and implemented by Feb 2017.
1.6 Review of co-ordinated discharge services. 1.7 Route cause analysis across organisations to understand flow blockages. 1.8 Respiratory in-reach consultant to facilitate on site assessment in ED. 1.9 Improved performance against target of 5 patients per hour. 1.10 Re-establishment of discharge to assess in social care. 1.11 Establishment of community bed discharge resource to allow for closure of surge areas in acute trust. 1.12 Formal MoU/risk share agreement to be developed relating to failing and halted schemes. 2. DTOCs2.1. 7 day working is part of the recovery plan 2.2. Care home trusted assessor is to be employed to reduce delays caused by waiting for care homes to assess 2.3. Discharge to assess (DTA) model being re-introduced on a multi-disciplinary level to effect greater flow and remove surge areas currently in constant operation in the acute trust. 2.4. Establishment of a community bed discharge resource to allow for closure of surge areas in the acute trust. 2.5. Increasing specialist care at home resource. 2.6. Frailty pathway increased to 6 day cover/week 2.7. Route cause analysis in train to understand reason for continued under-performance 2.8. HCA team in place to facilitate early discharge for stranded patients.
2. Mar 2017

3. RTT 18 weeks3.1 Revised recovery action plan agreed with WHHT, NHSE and NHSI to March 2017 3.2 The Trust has identified over 200 patients to be directly outsourced and HVCCG are overseeing the tracking and monitoring of the progress. 4. Ambulance KPIs (Red 1 & Red 2)1. Revised Recovery Action Plan (RAP)prepared to address Red 1 & Red 2 by March 2017. Agreed by the consortium in January 2017. 2. Current action plan achieved Q2.
3. Mar 2017
4.Mar 2017
CORPORATE RISK REGISTER LINKS RISK MOVEMENT SO2/01 Risk of a lack of proportionate and effective controls on the use, sharing and publication of information.
SO2/15b Risk that CHC performance is inadequate.
SO2/25 Risk of failure to deliver specific national targets in relation to Dementia Diagnosis.
SO2/30 Risk that patients are not assessed with a management plan and exited/admitted or discharged out of the Emergency Department (ED) within 4hrs.
S02/31 Risk that we do not reduce delayed transfers of care (DTOCs) to the target of 2.5%.
SO2/32 Risk that we do not deliver on the constitutional pledge to refer to treatment within 18 weeks at WHHT.
SO2/33 Risk that we do not deliver on priority ambulance KPIs. 0
2
4
6
8
10
12
14
16
18
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 2: High Quality We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well
BAF RISK 2.2 Risk that we are unable to ensure high quality, safe and sustainable services for the population and patients of west Hertfordshire. CAUSES: (A) Poor systems for monitoring and escalating provider quality issues, (B) Responsiveness of HVCCG, (C) Ambiguity over quality assurances required from partners, (D) Poor quality of assurances from providers commissioned directly and indirectly, (E) Availability of funding, (F) Limited workforce capacity and capability ASSURANCE SUMMARY Q4 2016/17 (Feb): Monthly oversight group meetings and quality assurance visits continue. There are however, positive assurances that the Trust is maintaining safe services with positive outcomes. Mortality rates are lower than the national average and improvement has been made in targets around cancer and diagnostics. The CQC report on their re-inspection carried out in September 2016 has now been received and is publicly available from 1 March 2017. Rating has improved overall from 'inadequate' to 'requires improvement'. Improvement has been seen and acknowledged, with some areas such as maternity moving from 'inadequate' to 'good'. The Trust remains in special measures due to some unsatisfactory findings for one ward in Hemel Hospital which was judged 'inadequate'. The CQC reported that at the time of the inspection it was not possible to judge how sustained the improvements were. A re-inspection is likely to be carried out in key areas within six months. Current risk score remains at 16 until sustained improvements are reported by the CQC and WHHT is removed from special measures.
Inherent Risk Residual Risk Target Risk
20 16 8
RISK OWNER: Director of Nursing & Quality RISK LEAD: Head of Quality Assurance
CONTROLS Following West Herts Hospital Trust's CQC serious concerns report: 1. NHS Improvement led multi-partnership OversightGroup established to gain assurance that the CQC improvement action plan is robust and that appropriate actions are in place to deliver agreed outcomes and demonstrate improvement. (Chaired by the NHS Improvement Portfolio Director and attended by HVCCG Accountable Officer and Acting Director of Nursing & Quality). Membership also includes NHSE, Healthwatch, Health Education England and the GMC/ LMC.) (A) - (F) 2. TDA Improvement Director in place at WHHT to providesupport, clear direction and to ensure adequate progress is made in line with CQC recommendations. (A) - (F) 3. Monitoring of quality and safety of services through themonthly integrated Quality and Contract Review meetings chaired by the Director of Nursing & Quality (A), (B), (C), (D)
4. CQUINS in place (B), (D)5. The CCG Infection Control Nurse attends the West HertsInfection Control Committee and West Herts link to the Herts Health Economy Infection Control Group (A), (B) (C), (D) 6. Programme of quality/assurance visits agreed andplanned for 2016/17 (A), (B), (C), (D) 7. HVCCG working with WHHT to implementrecommendations from the review of SI governance.(A),
ASSURANCES
1. Monthly report to the Quality & Performance Committee bythe Acting Director of Nursing and programme of quality assurance visits implemented. (+) 1. Monitoring of progress against CQC Improvement Planthrough oversight committee, led by NHSI, with WHHT, CQC, CCG and the Deanery. Positive verbal feedback from NHSI (+)
2. Monthly report to the Quality & Performance Committee bythe Acting Director of Nursing and programme of quality assurance visits implemented. (+) 3. Recent SSNAP data (Sentinel Stroke National AuditProgramme) show significant qualitative improvement. (+) 3. Performance report on national and local KPIs to ExecutiveTeam, Quality & Performance Committee and HVCCG Board (quarterly). Exception reports to the bi-monthly Local Area Team Quality surveillance group (bi-monthly). (+) 3. Workforce vacancy rate improving in Nursing andMidwifery. A&E is at full nursing establishment. Reduction in bank and agency staff at WHHT (+) 4. CQUIN overall achievement 2016/17 (-)5. Infection control action plan in place monitored by InfectionControl Committee attended by CCG (monthly). Infection control cases monitored against national KPI (monthly) (+)
6. Quality Report to Quality & Performance Committee.(+)
7. Monthly report to the Quality & Performance Committee bythe Director of Nursing and programme of quality assurance
ACTIONS & PROGRESS
1. WHHT CQC Improvement Plan monitoredat NHSI oversight committee. Monthly reports to Q&P on progress.
COMPLETION DATE
1. Ongoing weekly milestonemonitoring.

(B), (C), (D)
8. Monitoring of Serious Incidents and Never Events tohorizon scan by identifying trends and themes across providers. Close liaison with providers through the Integrated Quality Lead for JCT ) (A), (B), (C), (D), (F)
9. Review of governance structure at WHHT andrecruitment to the majority of new governance posts including Serious Incident management. (F) 10. New Associate Medical Director in post at WHHTleading on Maternity (A), (C), (D), (F) 11. CQC Improvement Plan for West Herts Hospital Trust.(A) - (F)
12. TDA clinical review conducted on 12th February 2016.(A), (D) 13. Clinical review completed 24 June 2016 (A), (D)16. CQC re-inspected Sept 2016 - WHHT CQC reportreceived February 2017. WHHT remains in special measures subject to review within 6 months' time. Following Hertfordshire NHS Community Trust’s (HCT) CQC requires improvement report: 14. CQC re-inspected Q1 2016/17 - HCT rated 'Good'.All Trusts 15. Data Quality Improvement Plans include requirementsaround accuracy of data and reporting.
visits implemented. (+) 7. Slight improvement in training figures for safeguardingchildren. L1 is slightly below target at 93% & L2 now 96% which is within target. 8. Serious incident overdue backlog reduced from 45 in July2015 to zero in January 2016. October 2016 no backlog but some RCAs not within national time frames due to request from WHHT for extensions. (+) 8. Herts & Beds-wide workforce programme in place. (+)8. 2016/17 Q1 & Q2 WHHT no never events. (+)9. Herts & Beds-wide workforce programme in place. (+)
11. Monthly report to the Quality & Performance Committee bythe Director of Nursing and programme of quality assurance visits implemented. (+) 11. HSMR at WHHT has fallen to below national average (+)
13. Monitoring through CQRM (+)
15. Monitoring through CQRM (+) RISK MOVEMENT
CORPORATE RISK REGISTER LINKS
SO4/22 Risk that there are higher levels of hospital activity than planned/anticipated.
SO4/23 Risk that additional expenditure will occur which is not budgeted for.
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
BAF RISK 2.3 Risk that we do not close the health inequalities gap between the most and least deprived communities. CAUSES: (A) Lack of focused investment on strategies for prevention, early intervention and diagnosis, (B) Limited workforce capacity and capability for implementation ASSURANCE SUMMARY Q4 2016/17 (Feb): Increased focus on prevention development is ongoing to close the gap of prevalence between expected and observed. Data analysis is being developed at sub-locality level.
Inherent Risk Residual Risk Target Risk
16 16 8
RISK OWNER: Director of Contracting & Resilience RISK LEAD: Programme Director, Planned & Primary Care
CONTROLS 1. Clinical Strategy focuses on prevention identifyinggroups at risk and approaches for increased intervention (A), (B)
2. Your Care Your Future Strategy and programme in place(A), (B)
3. All localities have a Local Commissioning Plan whichhighlights health inequalities (A), (B)
4. Business Cases completed and agreed (A), (B)
5. HCC Prevention Strategy (A)6. Primary Care & Community Implementation Plan (A), (B)7. Hub Strategy focuses on areas of health inequalities andhubs will play a key role in prevention within localities (A) 8. Locality plans and Member Practice CommissioningAgreements (MPCAs) and future models of care have been developed using the Your Care Your Future (YCYF) eight identified population groups and ‘tartan rug’ locality profiles which identify priority issues against national benchmarking.
ASSURANCES 1. Clinical Strategy monitored by the clinical programmes andreported quarterly to the Clinical Executive. Clinical Executive reports to the HVCCG Board. (+) 1. Increase in number of deprived wards in the CCG area. (-)2. Prevention is a key feature of the Case for Change in Your CareYour Future Strategy. Strategic outline case agreed by all parties (+) 2. Partnership working. (+)2. Increase in number of deprived wards in the CCG area. (-)3. Local Commissioning Plan updates and progress reported toHVCCG Board. (+) 3. Increase in number of deprived wards in the CCG area. (-)4. Prevention is one of the priorities in the business cases agreedfor 2016/17 (+) 4. Increase in number of deprived wards in the CCG area. (-)5. Reports to Health & Wellbeing Board (+)6. Reports to Programme Board (+)7. Fortnightly team meetings with all providers, reported to theEstates Strategy Group (+) 8. Locality Plans on a page and MPCAs.
ACTION PLAN & UPDATES 1.Implementation of identified areas andend to end pathways with a focus on prevention. 2. Focus of hub development is on areasof deprivation: a) Borehamwoodb) South Oxhey3. Data analysis is being developed at sub-locality level.
COMPLETION DATE 1.Apr 2017
2a. Q3 2016/17 2b. Q4 2016/17
3. Q4 2016/17 - Q2 2017/18

RISK MOVEMENT
CORPORATE RISK REGISTER LINKS
SO2/09 Risk to CCG in relation to resourcing delivery of joint co-commissioning of primary medical services.
SO2/15b. Risk that CHC performance is inadequate.
SO2/25 Risk of failure to deliver specific national targets in relation to dementia diagnosis.
S02/26 Risk to the CCG of not implementing the objectives of Building the Right Support via the Transforming Care Programme.
0
2
4
6
8
10
12
14
16
18
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
BAF RISK 2.4 Risk of lack of adequate system capability in the management and security of information, data and technology CAUSES: (A) Historic under-investment in IT, (B) Historic lack of vision of using IT to support clinical services (C) Lack of joined up approach across providers. ASSURANCE SUMMARY Q4 2016/17(Feb): All providers are meeting regularly to discuss this risk. There is an understanding that funding is limited and there is a need to collaborate. The local digital road map implementation group has been established. Hertfordshire Digital Integrated Care Programme Board comprises a core delivery board and an extended board of wider stakeholders. Target risk score of 8 has an expected achievement date of March 2019. The programme is on track with in-year milestones and plans are being progressed around the shared care record with a local pilot using the “medical information gateway” that will commence in Q1 2017/18.
Inherent Risk
Residual Risk Target Risk
20 16 8
RISK OWNER: Chief Finance Officer RISK LEAD: Head of IM &T
CONTROLS 1. IM&T Strategy (A), (B), (C )2. Local Digital Roadmap with inter-operability as akey deliverable (C )
3. IT systems reviewed as part of tender processfor new providers (A), (B) 4. Contracts (A), (B)5. Hertfordshire Digital Integrated CareProgramme Board (C )
6. Head of IM&T meets with WHHT (A), (B), (C )7. WHHT has a new datacentre (A), (B), (C)8. Hertfordshire and west Essex Local DigitalRoadmap (LDR) published on STP website (A), (B), (C) 9. STP capital bid includes investment in IM&T (A),(B) 10. Head of IM&T attends fortnightly STPtechnology work stream meeting (A), (B), (C)
ASSURANCES 1. Strategy approved by Board2. Digital Road Map submitted as part of STP2. Digital Road Map is signed up to by all providers2. Monitoring of Digital Maturity Index throughprogramme board and reports to Commissioning Exec and HVCCG Board 3. Procurement records
4. Contract documentation and negotiation records5. Reports to the Hertfordshire Chief Executives Group5. Regular feedback on the project to HVCCG throughthe Accountable Officer’s report. 6. Updates to Exec and SLT7. Oversight group8. Report requesting approval of Local Digital Roadmap(LDR) to HVCCG Board Jan 2017 prior to publication on STP website. 9,10. STP updates to HVCCG Board and STP groups
ACTION PLAN 1. Chief Finance Officer & Head ofIM&T to work with Executive and providers to secure further information and assurances. Full plans including update on baseline assessment of digital maturity index of all providers reported to HVCCG Board Jan 2017. Both community and mental health trusts already have a full Electronic Patient Record (EPR) and have plans to progress these systems with the addition of bed management and offline working. Acute trusts have plans to progress this for the 2020 paperless deadline, either through deployment of an integration engine or through a full EPR system. 2. The LDR has been extended tocover the whole STP footprint with plans signed off by all partners and published on the STP website mid-January 2017. 3. A shared care record is currentlybeing developed with local providers. A local pilot using the “medical information gateway” will commence in Q1 2017/18. All
COMPLETION DATE 1.From Apr 2016
2. Jan 2017
3.Q1 2017/18

organisations have appropriate IG toolkit compliance and established policies for IG, data security, cyber crime and business continuity plans. The national NHSMail2 migration programme outlines plans for other collaborative tools.
CORPORATE RISK REGISTER LINKS RISK MOVEMENT
SO2/01 A lack of proportionate and effective controls on the use, sharing and publication of information.
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west
Hertfordshire.
BAF RISK 3.1 Risk that the joint submission to obtain additional capital resource to successfully transform the delivery of care in west Hertfordshire is unsuccessful. CAUSES: (A) Failure to make a compelling case for transformation, (B) Failure to communicate effectively with national bodies, key stakeholders and patients, (C) Limited workforce capacity and capability, (D) Requirement for an Estates Strategy ASSURANCE SUMMARY Q4 2016/17 (Feb): Initial feedback did not include any decision about capital funding. NHSE has, however, indicated that the capital pot available for investment over the next five years is limited and could potentially not meet the demands identified in the STP. HVCCG are currently remodelling Your Care, Your Future figures in line with the current financial position. The reviewed plans will then be aligned with the Strategic Outline Case for acute reconfiguration and plans for capital expenditure in the STP plan. Proposals to be presented to HVCCG Board on 29 June 2017.
Inherent Risk
Residual Risk
Target Risk
20 12 8
RISK OWNER: Director of Contracting and System Resilience RISK LEAD: Programme Director Your Care, Your Future
CONTROLS 1.Clear prioritisation mechanisms in place for the STP process - revenue and capital (A), (B), (C)
2. CCG is developing a draft Estates Strategytogether with the Estates Group which reports to the Commissioning Executive and Board (D) 3. Accountable Officer attends the ChiefExecutives Sustainability & Transformation Plan (STP) Group (A), (B) 4. Quality Assurance meetings with NHSE (A),(B), (C), (D) 5. Chief Finance Officer attends FARG (A), (B)6. Submission 21 Oct 2016
7. HVCCG Chair attends the STP Chairs’ Group8. PwC review of STP governance presented toChairs’ Group Feb 2017 9. Progress reports on STP governance to theHVCCG Audit Committee
ASSURANCES 1. Funds for transformation are enhancing primary andcommunity services (+) 1. Increased engagement and partnership from all partnersacross the health and social care health economy evidenced by signing of Strategic Outline Case. (+) 2. The development of an Estates Strategy (+)
3. Minutes from the Group (+)
4. Outcomes reported (+)
5. Minutes from the Group (+)6. Report on the Pt 1 process and key outline to the Boardin Public for 10 Nov to the Board in Public 7. Plan for Pt2 will be shared in closed Board 10 Nov8. Chairs’ Group minutes (+)8. PwC report (+)9. Audit Committee minutes (+)
ACTION PLAN 1. Strategic outline implementation
starting from April 2016.2. Development of Memorandum of
Understanding proposed to Chairsgroup by Audit Committee and inPwC governance review.
COMPLETION DATE 1.April 2017.
2.2017/18

RISK MOVEMENT
CORPORATE RISK REGISTER LINKS
SO3/02 Risk that localities will not be aligned with CCG objectives.
SO3/03 Risk of failure to ensure that Public Health is sufficiently embedded within the CCG programmes and localities.
SO3/05 Risk that we fail to successfully transform health and social care through use of the Better Care Fund.
SO3/08 Risk that we are unable to deliver the services identified as key to transformational change due to lack of available workforce in primary care.
SO3/09 Risk that there will be increased pressure on health services due to a reduced level of provision for social care services
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target
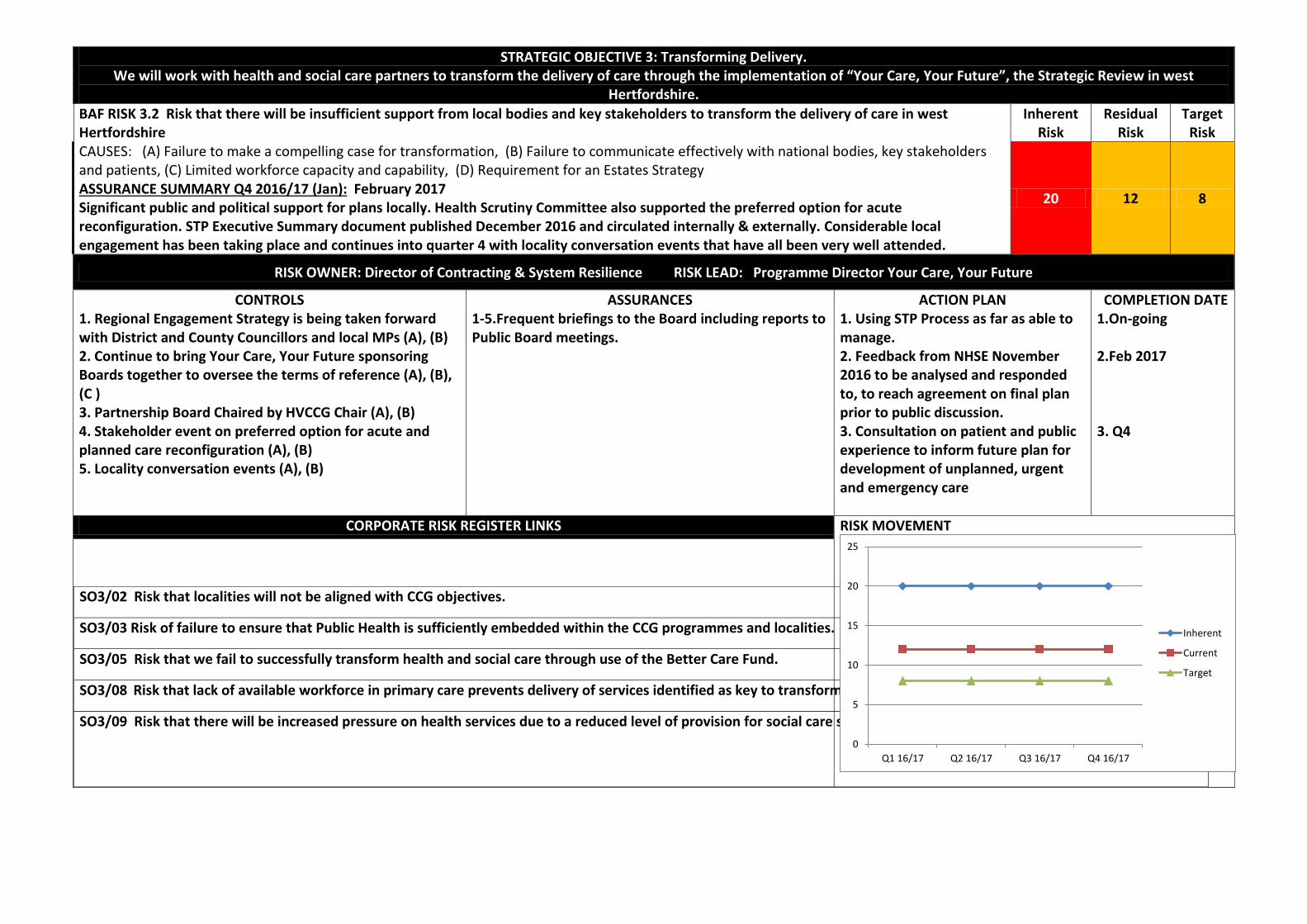
STRATEGIC OBJECTIVE 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west
Hertfordshire.
BAF RISK 3.2 Risk that there will be insufficient support from local bodies and key stakeholders to transform the delivery of care in west Hertfordshire CAUSES: (A) Failure to make a compelling case for transformation, (B) Failure to communicate effectively with national bodies, key stakeholders and patients, (C) Limited workforce capacity and capability, (D) Requirement for an Estates Strategy ASSURANCE SUMMARY Q4 2016/17 (Jan): February 2017 Significant public and political support for plans locally. Health Scrutiny Committee also supported the preferred option for acute reconfiguration. STP Executive Summary document published December 2016 and circulated internally & externally. Considerable local engagement has been taking place and continues into quarter 4 with locality conversation events that have all been very well attended.
Inherent Risk
Residual Risk
Target Risk
20 12 8
RISK OWNER: Director of Contracting & System Resilience RISK LEAD: Programme Director Your Care, Your Future
CONTROLS 1. Regional Engagement Strategy is being taken forwardwith District and County Councillors and local MPs (A), (B) 2. Continue to bring Your Care, Your Future sponsoringBoards together to oversee the terms of reference (A), (B), (C ) 3. Partnership Board Chaired by HVCCG Chair (A), (B)4. Stakeholder event on preferred option for acute andplanned care reconfiguration (A), (B) 5. Locality conversation events (A), (B)
ASSURANCES 1-5.Frequent briefings to the Board including reports to Public Board meetings.
ACTION PLAN 1. Using STP Process as far as able tomanage. 2. Feedback from NHSE November2016 to be analysed and responded to, to reach agreement on final plan prior to public discussion. 3. Consultation on patient and publicexperience to inform future plan for development of unplanned, urgent and emergency care
COMPLETION DATE 1.On-going
2.Feb 2017
3. Q4
CORPORATE RISK REGISTER LINKS RISK MOVEMENT
SO3/02 Risk that localities will not be aligned with CCG objectives.
SO3/03 Risk of failure to ensure that Public Health is sufficiently embedded within the CCG programmes and localities.
SO3/05 Risk that we fail to successfully transform health and social care through use of the Better Care Fund.
SO3/08 Risk that lack of available workforce in primary care prevents delivery of services identified as key to transformational change.
SO3/09 Risk that there will be increased pressure on health services due to a reduced level of provision for social care services
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 3: Transforming Delivery Work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire
BAF RISK 3.3 Risk that workforce issues prevent us from transforming the delivery of care across the local health and social care system. CAUSES: (A) Unclear approach and absence of strategy, (B) Limited workforce capacity and capability, (C) Workforce culture not congruent with required changes, (D) Poor communication with health and social care partners ASSURANCE SUMMARY Q4 2016/17 (Feb): Aligning to all strategic plans for the implementation of Your Care, Your Future. WPEG has identified current new ways of working and hard to recruit areas. This work will be developed by the new Local Workforce Action Board (LWAB). To be taken forward within the CCG by Director of Workforce in consultation with Director of Contracting & Resilience and Planned and Primary Care team working on the multi-provider pathway collaborative. MPPC submission for the diabetes pathway in February to include workforce plan and provide a model for the development of other pathways.
Inherent Risk
Residual Risk
Target Risk
20 16 8
RISK OWNER: Programme Director Your Care, Your Future RISK LEAD: Associate Director of Workforce
CONTROLS 1. A new HR&ODL Strategy developed withfour strands: Leadership Culture; Workforce Planning, Recruitment & Retention; Learning & Development; Policies, Procedures & Systems. (A), (B), (C), (D)
2. A new Service Level Agreement has beensigned by the AOs of HVCCG, BCCG and LCCG, that sets out the HR&ODL services, which is implemented via the approved HR&ODL Strategy. 3. The CCG partakes in the local workforceaction board (LWAB). This has replaced the former group, WPEG. The focus is on four strands, being: Trainees; Recruitment & Retention; Our People; New Ways of Working. The Director of Workforce is the SRO for new ways of working across Beds & Herts. (A), (B), (C), (D) 4. Current new ways of working locally,regionally and nationally were identified by WPEG in a report tabled on 17.11.16. 5. Workforce strategy reviewed.
ASSURANCES 1. HR&ODL Strategy approved at the BoardDevelopment meeting on 26 May 2016 Accountable Officer or Director of Nursing & Quality will evaluate KPIs defined at quarterly 3 CCG AOs Tripartite meetings (+) 1. Progress against the HR & ODL Strategy is to bereported quarterly via Q&P and bi-monthly to the Accountable Officers’ Forum 2. Monitored via Q&P and the Accountable Officers’forum.
3. Progress reported to local workforce action board(LWAB) bi-monthly (+) 3. National Primary Care workforce data highlightsgaps amongst nurses and GPs (-) 3. The Integrated Care Boards are not clear what theimpact on the workforce would be following integration or the creation of new models of care (-)
ACTION PLAN & UPDATES 1. Further work is required to developworkforce changes alongside pathway design: in particular providing clarity over roles and changes in competencies. Initial report from the WPEG to be taken forward in new LWAB (Local Workforce Action Board). 2. Local workforce action board (LWAB) willdevelop WPEG work that identified recruitment hotspots to improve further recruitment and retention. First meeting December 2016 3. Director of Workforce to collaborate withDirector of Contracting & Resilience to draw up a specific action plan for Q4 2016/17 that defines the new models of care, pathways and workforce requirements in detail. 4. Multi provider pathway collaborativesubmission for diabetes pathway at the end of February will include an action plan for workforce. Learning from that first example will be built into the other new pathways.
COMPLETION DATE 1. Mar 2017
2. From Dec 2016
3. Mar 2017
4. Feb 2017

CORPORATE RISK REGISTER LINKS RISK MOVEMENT
SO3/02 Risk that localities will not be aligned with CCG objectives.
SO3/03 A failure to ensure that Public Health is sufficiently embedded within the CCG programmes and localities.
SO3/05 Risk that we fail to successfully transform health and social care through use of the Better Care Fund.
SO3/08 Risk that we are unable to deliver the services identified as key to transformational change due to lack of available workforce in primary care.
SO3/09 Risk that there will be increased pressure on health services due to a reduced level of provision for social care services
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 4: Affordable & Sustainable Care We will ensure that there is a financially sustainable and affordable healthcare system in West Hertfordshire.
BAF RISK 4.1 Risk that we do not deliver a financially sustainable health and social care system. CAUSES: (A) Reliant upon the engagement of partners in a common financial strategy for both STP (5 years) and Your Care Your Future (10 years), (B) Additional financial uncertainty related to the requirement that utilisation of 1% of CCG non-recurrent spend remains fully uncommitted to create a system risk reserve with spending subject to HM Treasury approval. ASSURANCE SUMMARY Q4 2016/17 (Feb): February 2017 It is now clear how the ST Fund plays into Yr5 STP share, but initial feedback on submission review received 15.11.16 does not include any decision about capital funding. NHSE has, however, indicated that the capital pot available for investment over the next five years is limited and could potentially not meet the demands identified in the STP. The Your Care, Your Future (YCYF) risk report to the Audit Committee on 12 January highlighted the developing interdependency between YCYF and the STP. The report states that there is a high risk associated with insufficient headroom to invest or reallocate resources. The controls identified to manage this risk include financial transparency across the health and care system. HVCCG is now remodelling Your Care, Your Future to reflect the difficult financial situation. The review proposals will be presented to the Board in June 2017 and the outcome fed into the Strategic Outline Case and the STP. 1% non-recurrent requirement of £7.5m remains uncommitted pending decision by H M Treasury. Forecast outturn assumes this funding is not available to mitigate the CCG in-year deficit.
Inherent Risk
Residual Risk
Target Risk
25 16 10
RISK OWNER: Chief Finance Officer RISK LEAD: Director of Development
CONTROLS 1.CFO membership of STP Finance Group meeting for Your Care, Your Future 2. STP draft plan submitted 30 June 2016
3. STP “do nothing” finance templatesubmitted 30 June 2016 4. STP Lead appointed5. STP updated plan submitted 21 Oct 20166. Separate work streams established foracute, community, primary care and prevention 7. Strategic and implementation risk registersfor YCYF
ASSURANCES 1. Minutes from new STP Finance group willbe reported to HVCCG Board 2. Feedback in letter from NHSE July andNovember 2016 does not include any decision about capital finance (-) 3,4,5,6. Board reports
7. Reported to the audit committee (+)
ACTION PLAN 1. Re-modelling of YCYF to reflect the difficultfinancial situation. 2. Mapping of outcome of the YCYF to plans for SOCand STP.
COMPLETION DATE 1. June 2017
2. July 2017

CORPORATE RISK REGISTER LINKS RISK MOVEMENT
SO3/09: Risk that there will be increased pressure on health services due to a reduced level of provision for social care services.
S04/03: Risk that QIPP savings are not achieved as planned.
0
5
10
15
20
25
30
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 4: Affordable & Sustainable Care We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
BAF RISK 4.2 Risk that we do not deliver best value from the total CCG budget. CAUSES: (A) Lack of ownership of individual schemes; (B) Lack of consistent programme management approach; (C) Failure to identify schemes early enough; (D) Failure to identify alternative schemes for lost savings; (E) Not adopted RightCare methodology or part of Wave 1 CCGs; (F) (F) We do not derive the benefits available from engagement with the programme boards. ASSURANCE SUMMARY Q4 2016/17 (Feb): Estimated QIPP delivery to date (M10) is 66%. Weekly escalation meetings review both the financial recovery plan and individual QIPP schemes with delivery leads and directors. CHC plan in place to address issues identified in the internal investigation by March 2017. Internal auditors have identified the need for better oversight and ownership of QIPP schemes by programme boards. Revised Terms of Reference have been sent to the next meeting of all programme boards by the Head of Corporate Governance. Review of QIPP processes and business case process on-going to bring about improvements.
Inherent Risk Residual
Risk Target Risk
20 16 8
RISK OWNER: Chief Finance Officer RISK LEAD: Assistant Director of Transformation & Planning/Programme Director, Financial Turnaround
CONTROLS 1. Clinical and Programme Leads are inplace to ensure that schemes are monitored with BI Data (A), (C)
2. Transformation/QIPP & Planning Lead inplace (A), (B), (C)
3. Monthly reporting of both activity andfinancial cost to identify areas of further concern (B), (C)
ASSURANCES 1. Monthly feedback to Executive Boardand Quality & Performance Committee regarding provider performance (+) 1. Monthly NHS England assessment ofCCG QIPP (+) 1. Internal Audit Opinion for ContinuingHealthcare Amber/Red (-) 1. Providers who have accepted a controltotal giving them access to the Sustainability & Transformation Fund are not subject to 'double jeopardy' (-) 2. Monthly progress reporting on projectsincluding QIPP to Quality & Performance Committee (+) 2. NHS England quarterly comparisons ofMidlands & East CCGs QIPP achievement (+) 2. Potential variance against budget of -£6.6m identified for Continuing Healthcare (CHC): £1.1m relates to 2015/16; c. £1m relates to funded nursing care (FNC) price increase. Forecasting only 15% QIPP delivery for CHC (-) 2.QIPP estimated performance YTD 66% (-) 3. Annual Internal Audit review (+)3. Green-rated Internal Audit Opinion forKey Financial Controls, Financial Planning
ACTION PLAN & UPDATES 1. Additional QIPP, decommissioning in-year and delayingnon-committed expenditure to provide headroom to mitigate financial risk and meet obligations 2. Transformation Projects are continually under review toensure delivery of savings. 3. Programme of weekly escalation meetings to review FRPand QIPP with delivery leads and directors from November 2016. 4. Review of QIPP processes from identification to delivery.5. Review of business case process.6. Governance review to strengthen role of programmeboards in driving and ensuring accountability for schemes. 7. QIPP also to be raised consistently at all of the clinicallocality meetings.
COMPLETION DATE 1. Ongoing
2. Ongoing
3. From Nov 2016
4. On-going5. On-going6. Feb 2017
7. On-going

4. Monitored by the Quality &Performance Committee (A), (B), (C)
5. Internal and external QIPP meetings (A),(C)
6. Monthly financial reporting on QIPP toNHS England (C) 7. Project Monitoring Team (A), (C)8. Monthly meetings between AccountableOfficer and QIPP Programme Clinical Leads (A), (B), (C) 9. Risk Mitigation Plan (A), (B), (C)10. Internal PMO process for monthlychecking of transformation and QIPP project milestones (C) 11. Introduction of GP performance datapacks so any areas of concern can be highlighted and support given in primary care (A) 12. Close monitoring of all contracts (C)
13. Line by line review of expenditure fromApril 2016, benchmarked against other CCGs (A), (B), (C) 14. NHSE sharing QIPP data from otherCCGs in the region (B), (C) 15. Rationale for business cases isevidence-based, using e.g. Right Care data sets (B), (C) 16. Transformation projects are continuallyunder review to ensure delivery of savings (A), (B) 17. Implementation of a formalisedprogramme of projects to achieve targeted
& Reporting and Acute Contracting & Performance Management. Amber/Green Internal Audit Opinion for Governance and Payroll (+) 4. Monthly QIPP report showing the statusof all schemes is in place (+) 4. NHSE QIPP review 16.6.165. Financial Turnaround Group and Q&Pscrutiny (+) 5. External review (by ex CFO) of CCGexpenditure compared with peer group CCGs, expected by July 2016
12 Financial Turnaround Group and Q&P scrutiny (+) 13 Financial Turnaround Group and Q&P scrutiny (+)
14 Financial Turnaround Group and Q&P scrutiny (+)

savings has been introduced. Part of this formal approach is the compliance of written business cases with supporting evidence. (A), (B), (C), (D), (E) 18. Feedback received on detailed reviewof expenditure together with benchmarking against other CCGs. Conclusions included in recommendations in the Financial Recovery Plan along with service restrictions. (B), (C), (D) 19. Programme of weekly escalationmeetings to review FRP as well as QIPP with delivery leads and directors from November 2016.(A), (B), (C), (D), (E) 20. CHC plan in place to address thebacklog and scope the exact size of the budgetary challenge by March 2017. 21. Alignment with NHSE menu ofopportunities - advice from regional turnaround lead 22. Joint QIPP board with WHHTestablished. 23. Internal workshops to identifyadditional savings 24. Right care/best value/better careanalysis 25. Complete workbooks and QIA & EQIAprocess for all 2017/18 QIPP schemes 26. Further assurance on Macphersonreport has been developed and is now being cascaded through SLT. CORPORATE RISK REGISTER LINKS
S04/03: Risk that QIPP savings are not achieved as planned
RISK MOVEMENT
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

STRATEGIC OBJECTIVE 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
BAF RISK 4.3 Risk that we do not achieve the agreed control total for 2016/17 CAUSES: (A) Acute activity levels and/or (B) Financial values of activity above those detailed in the 2016/17 financial plan. ASSURANCE SUMMARY Q4 2016/17 (Feb): Acute over-performance is estimated as £18.5m to date. Continuing Healthcare over performance is at £6.6m. This is being partially managed by the Financial Recovery Plan and proactive oversight of activity flows. Further analysis is being undertaken to understand the causes of increased activity. However, NHS England have acknowledged that the CCG is unlikely to achieve a year end position better than £8m variance to plan and the control total has been revised accordingly. At M10 £6.6m of recovery actions have been identified in the Financial Recovery Plan. Month 10 finance report shows £15.6m adverse variance against plan and QIPP delivery to date is estimated as 66%. An Investment Committee of the HVCCG Board has been established and a Turnaround Director appointed. The Accountable Officer has created a programme of weekly escalation meetings to review both the financial recovery plan and individual QIPP schemes with delivery leads and directors. Further plan submitted on 23 December 2016 with another submission due on 24 February 2017. Two escalation meetings have taken place with NHS England with further meetings to be managed by the NHSE local team. Return to in-year balance is forecast in the financial plan for 2017/18 with QIPP delivery of £38m required.
Inherent Risk
Residual Risk
Target Risk
20 20 10
RISK OWNER: Chief Finance Officer RISK LEAD: Deputy Director Contracting and Procurement
CONTROLS 1. NHS Standard Contracts for 2016/17 (A), (B)
2. Activity and Finance schedules (A), (B)
3. CCG Financial Plan 2016/17 (A), (B)
ASSURANCES 1. Meeting monitoring activity and financialperformance (Monthly) (+) 1. Penalties more acknowledged by providers1. NHS England routine monitoring of financialposition (Monthly) (+) 1. Internal Audit Opinion on CHC Amber-Red(-)1. CHC expenditure volatile and difficult topredict (-) 2. Reports to Quality & PerformanceCommittee (Monthly) (+) 2. Internal audit review (Annual) (+)2. Reports of provider Trusts to their ownBoards (WHHT - monthly. Others are a mixture of monthly, bi-monthly and quarterly) (+) 2. Green-rated Internal Audit Opinion for KeyFinancial Controls, Financial Planning & Reporting and Acute Contracting & Performance Management. Amber/Green Opinion for Governance & Payroll (+) 3. Internal audit of commissioning plans(Annual) (+)
ACTION PLAN 1. Further analysis is being undertaken to understandthe causes of increased activity 2. Review of QIPP processes from identification todelivery. 3. Revision of business case process.
COMPLETION DATE 1. On-going
2. On-going
3. On-going

4. Monitored by the Quality & PerformanceCommittee (A), (B) 5. Internal monthly meetings betweenAccountable Officer and Contract Leads (A), B)
6. External monitoring meetings and activityreports (A), (B) 7. Provision of activity reports to localities andpractices (A), (B) 8. Strategic outline business case for YourCare, Your Future signed by all parties 21st October 2015 (A), (B) 9. Monthly review of Running Cost Allowanceand individual programme budgets (A), (B) 10. Board level scrutiny of financial plans (A),(B) 11. Increased focus of internal and externalmonitoring meetings holding providers more closely to contract (A) 12. Increased focus on contract challenges:finalising old queries; raising additional queries (B) 13. Weekly escalation meetings introduced toreview FRP and QIPP with delivery leads and directors (A), (B) 14. Investment Committee review of spendareas (A), (B) 15. Contract challenge reviews escalated (A),(B) 16. CHC finance review accelerated (B)
17. Joint QIPP Board with WHHT established(A)
3. NHS England Regional deep dive process. (+)4. Contract performance report regularly toExecutive Team (Monthly) (+) 5. Financial Turnaround Meeting and Q&PCommittee monitoring of QIPP schemes (Weekly and Monthly) (+) 6. Contracting and quality meeting minutes (+)
7. Sent monthly by email (+)
8. Financial Effectiveness Group monitoring ofmitigation plan (Monthly) (+)
9. Reported in monthly finance reports (+)
10. Board minutes (+)
11. Minutes of contracting and qualitymeetings (+)
12. Written record of challenges (+)
13. Action notes from weekly financialturnaround meetings (+)
14. Investment Committee minutes, trackerand published decision register (+) 15. Written record of escalation (+)
16. Action plan in place and progress reportedto the Q&P Committee (+) 17. Minutes from the joint board and reportsto the Q&P Committee (+)

RISK MOVEMENT
CORPORATE RISK REGISTER LINKS
S04/22: Higher levels of hospital activity than planned/anticipated.
S04/23: Risk that additional expenditure will occur which is not budgeted for.
0
5
10
15
20
25
Q1 16/17 Q2 16/17 Q3 16/17 Q4 16/17
Inherent
Current
Target

SPACER PAGE

SPACER PAGE

NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title 2016/17 Annual Report and Accounts – proposed approval process
Agenda Item: 13
Purpose* (tick) Decision ☐ Approval ☒ Discussion ☐ Information ☐
Responsible Director(s) and Job Title
Caroline Hall Chief Finance Officer
Author and Job Title Caroline Hall Chief Finance Officer
Short Summary of Paper The nationally prescribed 2016/17 Annual Report and Accounts timetable envisages that draft documents will be made available to the CCG’s external auditors, BDO, and to NHS England by noon on Friday 21 April 2017.
The external audit process is due to be completed, and audited Annual Reports and Accounts, including relevant signatures, certificates and the auditors’ opinion statements, submitted to NHS England by noon on Wednesday 31 May 2017.
These dates do not align with planned Board meetings in public since the final report will not be discussed with the external auditors until 18 May 2017 at the Audit Committee, or confirmed with the Chair and Accountable Officer until 25 May 2017: following today’s meeting the next Board meeting is scheduled for 11 May 2017. Therefore, the Board is asked to approve the use of the ‘Emergency powers and urgent decisions’ provision of the Constitution to enable the Chair and Accountable Officer to approve the audited Annual Report and Accounts for 2016/17 on the advice of the Audit Committee, following its meeting on 18 May 2017. The external auditors plan to present the findings of the audit at this meeting and agree any necessary amendments to the draft documents prior to signature and provision of certificates and opinion statements. Provision has been made for a final teleconference between the external auditors, Chair of the Audit Committee and Chief Finance Officer on Tuesday 30 May 2017, if this is required.
All Board members will also be invited to attend the Audit Committee meeting on 18 May 2017 for this item should they so wish.
In the event that the Chair of the Audit Committee believes that it is not appropriate for approval to be given without discussion by the full Board, an extra Board meeting will need to be arranged at short notice between 18 May and 30 May 2016.
This proposal mirrors the actions taken to obtain approval to the 2013/14, 2014/15 and 2015/16 audited Annual Report and Accounts.
Recommendation(s) The Board is being asked to: The Board is asked to agree to the use of the ‘Emergency powers and urgent decisions’ provision to enable the audited Annual Report and Accounts for 2016/17 to be approved by the Audit Committee on the Board’s behalf prior to the submission deadline, as set out above.
Engagement with Stakeholders/Patient/Public
None.
Links to Strategic Objectives (tick all that apply)
Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☒

Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
The Annual Report and Accounts will refer to the assurances provided during 2016/17 to manage critical business risks and the financial performance of the CCG will be disclosed in the accounts.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
No new risks identified
Resource Implications No additional resource implications
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
N/A
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☐
Improved Patient Access and Experience ☐
A Representative and Supported Workforce ☐
Inclusive Leadership ☐
Report History Which Groups or Committees have seen this report and when?
None – the principle of the suggested approval arrangements has been discussed by the Audit Committee.
Appendices None
*Purpose – definitions
For decision
This is where the board, committee or group is presented with a range of options and is asked to
decide which one to accept following discussion.
For approval
A specific recommendation, plan or document is presented, which the board, committee or group is
requested to approve. Discussion is not essential.
For information

Information is provided and it is important that the board, committee or group is aware of, and
understands the information and no decision is required. These items do not require discussion,
except for questions of clarification.
For discussion
The board, committee or group is asked to debate an issue, provide views, challenge and discuss as
appropriate. A decision may be made following the discussion although this is not always required.
An example is a progress report on a particular pathway. In this case the Board or Committee will be
asked to discuss and note the paper.

SPACER PAGE

SPACER PAGE

1
NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Investment Committee Report Agenda Item: 14
Purpose* (tick) Decision ☐ Approval ☐ Discussion ☐ Information ☒
Responsible Director(s) and Job Title
Paul Smith Investment Committee Chair
Author and Job Title Rod While Head of Corporate Governance
Short Summary of Paper The paper summarises outcomes from the first four meetings of the investment committee
Recommendation(s) The Board is being asked to: Note the report
Engagement with Stakeholders/Patient/Public
Individual reports to the investment committee will have been subject to engagement but not this report.
Links to Strategic Objectives (tick all that apply) Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☒
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
Decisions made by the investment committee potential impact on all risks on the Board Assurance Framework and the Corporate Risk Register.
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Not applicable to this report
Resource Implications Not applicable to this report
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
All decisions made by the investment committee are subject to equality impact analyses
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☐ Improved Patient Access and Experience ☐
A Representative and Supported Workforce ☐
Inclusive Leadership ☐

2
Report History Which Groups or Committees have seen this report and when?
None
Appendices Appendix 1 Disinvestment / service change / investment flowchart
*Purpose – definitions
For decision This is where the board, committee or group is presented with a range of options and is asked to decide which one to accept following discussion. For approval A specific recommendation, plan or document is presented, which the board, committee or group is requested to approve. Discussion is not essential. For information Information is provided and it is important that the board, committee or group is aware of, and understands the information and no decision is required. These items do not require discussion, except for questions of clarification. For discussion The board, committee or group is asked to debate an issue, provide views, challenge and discuss as appropriate. A decision may be made following the discussion although this is not always required. An example is a progress report on a particular pathway. In this case the Board or Committee will be asked to discuss and note the paper.

3
1. BackgroundIn response to the CCG being formally placed in financial turnaround, the investment committee was approved by the CCG Board, alongside terms of reference and committee criteria on 24 November.
The approved terms of reference state that the committee has the following remit: “To review and assess potential service investments and disinvestments in line with NHS Herts Valleys Clinical Commissioning Group’s strategy. This will include assessing business cases focusing on the return on investment and value for money to improve health and reduce health inequalities”.
Committee membership comprises two lay members, two Board GPs, the Accountable Officer and the Chief Finance Officer.
2. ProgressEight meetings of the committee have been held between 1 December and 5 January in order to review planned future investments and progress on recent investments to establish evidence of outcomes.
Decisions on the following services have been made by the committee
Investments Disinvestments / service changes • Your Care, Your Future/transformation fund• 4th Hospital ambulance liaison officer• Emergency Care Practitioner• Care Home Implementation Team• Perinatal and IAPT early implementer
funding• Leg ulcer service• CHC back log - short term staff investment• Transforming care underspend (carry over to
2017-18 for continuation of transformingcare programme*
• Rapid assessment intervention and discharge(RAID)*
• GP Federations*
• Social care discretionary monies• Stroke• Demographic and non-demographic contract
growth• GP in emergency department• Integrated point of access• Direct access MRI (contract end)• AQP physiotherapy• AQP vasectomy• AQP Ophthalmology• Integrated assessment and discharge team
Sports and exercise medical service• Discharge to assess beds*• Family safeguarding*• People transferring from NHS England specialist
commissioning, without funding following theperson*
• Rapid response service*
*Decisions made since the last Board report on 12 January 2017.

4
Appendix 1
Disinvestment / investment
Process start
Desk based work
Assurance / monitoring
Decision point
Idea on potential savings scheme to Ian Armitage.
List as part of QIPP
ExecutiveFirst pass review
No further action Rejected
Programme BoardsCYPM / MHLD / planned and primary care / system
resilience
Engagement with stakeholders (patients, localities, MPs, HCC, district councils, finance, BI, contracting, medical
director, nursing and quality)Complete business case ensuring sign off from Medical
Director, Director of Nursing and Quality and CFO.Complete EQIA
Recommended for further work
Commissioning Executive orJoint Primary Medical
Services Commissioning Committee
Review proposal
Business case
No further action
Not approved
Investment CommitteeConsideration of business case
Recommended & >£50kNot approved
Commissioning lead prepares implementation plan with
contracting, finance, BI, comms & engagement and planning &
transformation
Recommended and <£50k
Approved
Monitor implementation
progress at financial turnaround
meetings
QIPP headline progress reported
at Executive. Cause for any shortfalls
established
Any shortfall in delivery due to clinical reasons to be review by
Commissioning Executive
QIPP Report at Q&PReview of investment
scheme
Q&P report to Board
Potential investment
Investment
SPACER PAGE

SPACER PAGE

NHS Herts Valleys Clinical Commissioning Group Board Meeting 9 March 2017
Title Committee Chairs’ Reports and Committee minutes Agenda Item: 15
Purpose (tick one only) Decision or Approval ☐ Discussion ☐ Information ☒
Responsible Director(s) and Job Title
Cameron Ward Accountable Officer
Author and Job Title Committee Chairs: Alison Gardner, Stuart Bloom
Short Summary of Paper The Committee Chairs’ report summarises key discussions, areas of assurance and decisions from the most recent Patient and Public Involvement and Quality & Performance committee meetings.
Also included are ratified minutes from Committee meetings. Recommendation(s) The Board is being asked to:
Note this report
Engagement with Stakeholders/Patient/Public
Not applicable
Links to Strategic Objectives (tick all that apply) Objective 1: Effective Engagement. We will continually improve engagement s with member practices, patients, the public, carers and our staff to contribute to and influence the work of Herts Valleys CCG.
☒
Objective 2: High Quality. We will commission safe, high quality services that meet the needs of the population, reducing health inequalities and supporting local people to avoid ill health and stay well.
☒
Objective 3: Transforming Delivery. We will work with health and social care partners to transform the delivery of care through the implementation of “Your Care, Your Future”, the Strategic Review in west Hertfordshire.
☒
Objective 4: Affordable & Sustainable Care. We will ensure that there is a financially sustainable and affordable healthcare system in west Hertfordshire.
☒
Board Assurance Framework (BAF) and Corporate Risk Register (CRR)
What current risks does this report align to?
All BAF and CRR risks apply
Risks (e.g. patient safety, financial, legal) What risks have been identified as a result of this report? How are they being mitigated?
Not applicable
Resource Implications Not applicable
Equality Impact Analysis (indicate the key points the analysis has identified relevant to decision required)
Not applicable
Equality Delivery System (identify which goal your proposal / paper supports)
Better Health Outcomes ☒ Improved Patient Access and Experience ☒
A Representative and Supported Workforce ☒
Inclusive Leadership ☒

Report History Which Groups or Committees have seen this report and when?
Not applicable
Appendices Committee minutes 15.1 Patient and Public Involvement Committee – 14 December 2016 15.2 Quality and Performance Committee – 2 February 2017 15.3 Quality and Performance Committee – 12 January 2017

3
Chairs report: March 2017
Quality and Performance Committee Dates of Meetings Chair Executive Lead
2 March 2017 Stuart Bloom Caroline Hall / Charles Allan
Finance report The current financial forecast includes a number of significant risks which we expect could yet impact on the final outturn, including a number of unknowns in connection with provider contracts yet to be resolved. QIPP 2016/17 Current forecast is an end of year outturn of 51%. The risk around QIPP was flagged up some time ago and it is extremely disappointing that we have been unable to achieve better than this level despite the focus over the last few months. HUC Performance for December 2016 was the worst this year due to high demand. There are significant concerns around on-going recruitment issues that have not been improved due to other opportunities that exist elsewhere, particularly for GPs. Apprenticeships It is very disappointing to note that so far only one apprentice is likely to be appointed in HR given that there are real opportunities for apprentices to contribute across the workforce including in primary care. Further opportunities are being explored and will be pursued at Executive Team level, including exploring possible links to schools, including encouraging younger people to think of careers within the NHS. WHHT CQC report It is encouraging to see the CQC report further to the re-inspection in September 2016, with significant improvement being made in many areas. There is clearly still much to do with the CQC decision that WHHT ‘requires improvement’ but should stay in special measures in order to embed changes for further improvement. QIPP 2017/18 The current level of QIPP worked up for 2017/18 is only at £31m, despite being reassured that by now we would have at least reached the target of £38m with a further 15% required on top as headroom. There are a number of QIPP plans within the £31m identified that are rag-rated ‘red’ and therefore give cause for concern that the £31m is not assured. Further work continues to validate schemes and identify additional proposals.

4
Patient and Public Involvement Committee Dates of Meeting Chair Executive Lead
15 February 2017 Alison Gardner Juliet Rodgers
Tad Woroniecki and Charles Allen led comprehensive, practical and forthright discussions on the challenges of our financial position and winter pressures. Patient Representatives offered constructive challenge, suggestions and ideas and strong support for our efforts to return to financial balance and commission our providers effectively whilst supporting their efforts to meet service delivery and improvement targets. Our Patient Representatives valued the opportunity to learn in detail about the constraints and stresses that we are dealing with and are keen to do whatever they can to support our efforts to inform opinion in the localities.
Half term had led to a significant number of executive contributors to the committee being unavailable to attend the meeting but Louise Manders led discussions on Your Care Your Future and the Participation and Engagement highlight report on behalf of David Evans, Juliet Rodgers and Heather Aylward. In particular Patient Representatives noted the emerging local flavour of the delivery of elements of YCYF.
The Chair noted the quality and range of the papers and reports submitted by patients involved in HVCCG business and service development activities as well as the usual comprehensive locality reports. These reports demonstrate the ‘sharp end’ of our patient involvement activity – but they also remind us of the need to broaden our patient participation beyond the usual committed local groups and individuals.
Finally Patient Representatives were briefed on the re-design of the musculoskeletal service and a drive to get more patients registered for Patient on-line. In both cases useful suggestions and feedback on existing arrangements were offered by patient representatives and Dipesh Songara and Trudi Mount were invited to come back to the committee as and when they were available – and were also invited to use Representatives as a resource outside committee as appropriate.

5
Joint Primary Medical Services Commissioning Committee Dates of Meeting Chair Executive Lead
26 January 2017 Thelma Stober David Buckle
The following areas were discussed at the January meeting:
• The committee agreed that confirmation of all interests as well as ‘no interests’ should be declared in writing in advance of the meeting. Thisrequirement also applies to staff
• The need to ensure that practices were advised of the need for GP partners, CCG clinical leads, attendees of locality committees and any othersinvolved in commissioning to complete the NHS England on-line conflicts of interest training once this was available.
• The primary care risk log was presented by NHS England. Due to confidentialities, this item will always be discussed at the private section of thecommittee meetings.
• The committee received a progress report on arrangements for delegated primary medical services commissioning and noted an ongoing riskaround resourcing. A memorandum of understanding (MoU) with NHS England is being developed to help address this. The MoU should bebrought to the Committee prior to completion
• Progress report on estates and technology transformation fund (ETTF) and the committee noted the current status of schemes relating to anumber of local practices.
• Summary of the draft commissioning framework for 2017-18. This will provide a simplified and consistent approach to the reporting andpayment processes for individually commissioned services provided by practices.
• NHS England provided an update on the position in respect of the APMS contracts for New Surgery, West Herts Medical Centre and MeadowellSurgery. The committee was concerned about apparent delays in procurement and suggested that NHS England should consider extending thecurrent contracts for a further 3 months to 1 October 2017. This would provide NHSE with additional time to complete the tenderdocumentation and commence the procurements.
• Update report on improving GP practice resilience programme• Update on operational plan and draft GP forward view plan which needs to be finalised and signed off by the CCG Board in March.• The committee approved a revised dispute policy for payments made to practices.

6
Audit Committee Dates of Meeting Chair Executive Lead
23 February 2017 Paul Smith Caroline Hall
Key points for the Board to note:
• The decision register is being kept up to date. There is a question over how we give greater visibility to conflict of interest management atlocality level.
• The Committee noted that the CCG complied with NHS England’s information governance toolkit. This was supported by internal audit work.• The Committee had requested a whistleblowing update to get assurance that the process was in place and that staff knew how to use it.
Evidence was provided by HR that gave assurance on this.• The Committee discussed the areas of judgement and estimate that would be reflected in the annual accounts and was content that the
approach was robust and defendable. The format of the annual report also was noted. A draft of the governance statement was consideredand in discussion it was suggested that we would need to include reference to the overall financial position, potential concerns aroundcontinuing health care data quality and financial tracking, and issues relating to social care spending and the governance around it. Thegovernance statement also detailed the responsibilities of localities, and in discussion the Committee felt that more evidence would be requiredof how those responsibilities have been discharged so as to form a view on whether any further comment was necessary in the statement.
• The 2017/18 audit plan was agreed. Any interested board members can request a copy of the plan.• The internal auditors reported on two audits carried out since the last audit committee; primary care commissioning – reasonable assurance,
and cyber security (reasonable assurance). The Committee noted the two reports and the proposed management actions.• The Committee agreed the counter fraud plan for 2017/18, and noted progress against the current year plan. A few investigations were
ongoing, but there is nothing significant to report to the Board.• The Board Assurance Framework was reviewed and in discussion, the Committee suggested that the scoring of the risk of ineffective
engagement with stakeholders should take account of positive patient engagement as well as issues around social care funding and therelationship with the county council.

1 | P a g e
Meeting : NHS Herts Valleys CCG Patient and Public Involvement Committee Meeting
Date : 14 December 2016
Time : 10.06 – 12.30
Venue : Apsley Meeting Room, Hemel One
Present:
Alison Gardner (AG) Lay Board Member, Meeting Chair
Colin Barry (CB) Patient Representative (Watford and Three Rivers)
Helen Clothier (HC) Patient Representative (St Albans and Harpenden) (from PPI/102/16 to PPI/104.2/16)
Brian Gunson (BG) Healthwatch Hertfordshire Representative
Juliet Rodgers (JR) Associate Director, Communications and Engagement
Gavin Ross (GR) Patient Representative (St Albans and Harpenden)
Caroline Sutherland (CS) Patient Representative (Hertsmere)
John Wigley (JW). Patient Representative (St Albans and Harpenden)
In attendance:
Laura Abel (LA) Corporate Governance Support Manager (Secretary to the Committee)
Heather Aylward (HA) Public Engagement Manager
Lynn Dalton (LD) Assistant Director of Localities and General Practice Development (for items PPI/105-106/16)
David Evans (DE) Programme Director, Your Care, Your Future (from PPI/99/16 to PPI/104.2/16)
Louise Manders (LM) Head of Programme Communication and Engagement Your Care, Your Future (from PPI/99/16 to PPI/104.2/16)
Simon Marshall (SM) Community Partnership Training Officer, East of England Ambulance Service NHS Trust (EEAST) (observer)
Tad Woroniecki (TW) Deputy Chief Finance Officer (for item PPI/103/16)
PPI/99/16 Chairman’s introduction and apologies for absence (Chair)
99.1
99.2
AG welcomed everyone to the meeting and introductions were made for the benefit of SM, who was attending the meeting as part of his shadowing of HA. The committee were pleased to welcome back CB.
Apologies had been received from Robert Hillyard (RH), Kevin Minier (KM), Margaret Morgan (MM), and Mike Walton (MW).
PPI/100/16 Declarations of interests (Chair)
100.1 There were no new interests declared.
PPI/101/16 Minutes of previous meeting (Chair)
101.1 The minutes were agreed as an accurate record of the meeting held on 19 October 2016.
PPI/102/16 Matters arising and action log (Chair)
102.1 It was agreed that completed (green) actions would be closed and open (red/amber) actions were
Approved 15.02.17
Item 15.1

2 | P a g e
discussed in turn.
102.2 PPI/53.5/16 PPI Gluten free prescribing – variation in the costs of gluten free products available to the NHS and commercially Further to the update provided at the meeting held on 17 August 2016, JR had again spoken to the medicines optimisation team and the Medical Director. She confirmed that the CCG had no influence over the cost paid by the NHS for gluten free products and it was agreed that it was important to focus on issues where the CCG could make a difference. It was agreed to close the action.
102.3 The Committee noted the action updates.
PPI/103/16 Finance Update (Deputy Chief Finance Officer)
103.1 TW presented an update on the financial position of the CCG, highlighting that at month 7(end October) the CCG was reporting a deficit against plan of £9.5m which was a deteriorationfrom the £6.9m reported at month 6 (end September). The financial recovery plan wastherefore at risk, prompting further discussions with NHS England and a need for additionalrecovery actions to be identified.
Factors included:o An underlying problem at end of 2015/16;o A price increase in the national tariff (the amount paid to providers under PBR),
compared to previous net tariff reductions;o over-performance in acute services and continuing care; ando non-achievement of all the planned QIPP savings.
The CCG was now in financial turnaround and being closely monitored by NHS England.
An investment committee had been established to ensure that all new investments deliveredvalue for money, and to look more closely at and potentially disinvest from services that werenot delivering value for money or the benefits intended. It was noted that there werewidespread financial difficulties across the NHS at this time.
AG stressed that it was important for the correct messages to be communicated and to reportfacts.
103.2 The following points were discussed:
In response to a question from JW, TW explained the CCG funding formula, which was mostlybased on the size and age of the CCG population, and also included other factors suchdeprivation and rurality.
In response to a question from CB about the robustness of the recovery plan, TW explainedthat:
o NHS England’s finance team had reviewed the CCG’s figures and had concluded thatthe YTD position and forecasts were generally reliable;
o trend data, e.g. around winter, had been factored into the forecasts;o forecasts were updated using ‘real’ data once available;o the individual elements of the recovery plan were rated Red / Amber / Green (RAG);o NHS England had recognised a net financial risk of £8m; ando The impact of an overspend of £8m in 2016/17 onto 2017/18 was significant both in
terms of the higher underlying expenditure and the necessity to “repay” the £8m in2017/18.
The recent decision not to make an extra discretionary payment to Herts County Council in2017/18 for social care commissioned services over and above the amount mandated to bepaid to the Better Care Fund (a pooled fund to help deliver more joined up health and socialcare) was discussed.
DE explained that the county council had been unable to demonstrate how the additionalfunding would make a significant impact on health services, e.g. in reducing delayed transfersof care.
BG noted that it was important to mitigate the inaccurate media coverage and stressed thatthis was part of strategic discussions across the STP footprint about the provision of services to

3 | P a g e
patients.
JR added that she had produced a paper for the extraordinary board meeting held on24 November 2016 that outlined broadly the plans to ensure engagement with local peoplearound financial recovery issues and to keep people informed. She would circulate this(attached as appendix 1 to the minutes).
The committee thanked TW for his update and clear explanation of the financial issues facingthe CCG.
103.3 The Committee noted the financial update.
103.4 ACTION: J Rodgers to circulate paper outlining key communication and engagement principles as part of the financial recovery programme.
PPI/104/16 Your Care, Your Future / Sustainability and Transformation Plan updates (Programme Director, Your Care, Your Future and Head of Programme Communication and Engagement Your Care, Your Future)
104.1 DE and LM provided an update on recent and planned communication and engagementaround YCYF and the STP.
Now that the acute hospital option had been agreed, it was important for everyone to worktogether to deliver it.
The new link for the YCYF website is: http://hertsvalleysccg.nhs.uk/your-care-your-future
The Hertfordshire and West Essex Sustainability and Transformation Plan was launched on 12December 2016 (www.healthierfuture.org.uk).
Patient representatives were invited to YCYF engagement events that would take place in2017 in each of the four localities. The first event would take place in Hemel Hempstead on31 January and Geoff Brown, CEO of Healthwatch Hertfordshire, had agreed to chair.
104.2 The Committee noted the Your Care, Your Future and STP updates.
PPI/105/16 Future of West Herts Medical Centre and the development of urgent care centres (Assistant Director of Localities and General Practice Development)
105.1 LD explained that the services currently offered at West Herts Medical Centre (WHMC) werecommissioned by NHS England (NHSE) rather than by Herts Valleys CCG.
There were circa 1,800 patients registered with WHMC, which also saw non-registeredpatients (circa 11,000 attendances per year).
The contract was an alternative provider medical services (APMS) contract which was timelimited, rather than a general medical services (GMS) contract which was an on-going contract(in perpetuity) between the GP contractor and NHSE.
The two contractual options at the end of the extended contract would be to:1. Close WHMC to registered patients and non-registered attenders and assist patients
to re-register with a new practice; or2. Re-procure (competitively tender) the contract.
A wide consultation by NHS England and Herts Valleys would be undertaken involving bothpatients and practices in Dacorum. This was planned to commence towards the end of January2017.
In response to a question from JW about an urgent care centre at St Albans Hospital, DEexplained that now that the acute option had been agreed, we were able to consider otherservice provision, including the urgent care service, across the patch.
105.2 The Committee noted the update in respect of urgent care centres.
PPI/106/16 Outcome of the vote on delegated commissioning of primary care medical services (Assistant Director of Localities and General Practice Development)
106.1 LD reminded the committee that NHS England currently commissioned GP practice contracts.
Since April 2014, CCGs had been given the option to either:o influence;o jointly commission; or

4 | P a g e
o fully commission GP services.
GPs had been assured that the GMS contract would continue to be nationally negotiated andwas a protected budget.
In October the CCG board had voted to recommend to member practices moving to fulldelegated commissioning of GP practice contracts from April 2017.
The Local Medical Committee had facilitated the ballot of all GP practices (one practice, onevote) and the majority outcome had been in favour of delegated commissioning.
A formal application had been submitted to NHS England on 6 December 2016 and theirdecision would be communicated in January 2017 following a due diligence process to ensurethat the CCG was capable of undertaking delegated commissioning.
If approved, shadow arrangements would be in place between January and April 2017.
The advantages were noted to be:o more informed decision making, based on local knowledge; ando support for the re-design of community services and the delivery of YCYF.
106.2 The Committee noted that HVCCG GP practices had voted in favour of delegated commissioning.
D Evans, L Manders and L Dalton left the meeting
PPI/107/16 Proposals to develop and broaden participation and patient participation update (Associate Director Communications and Engagement and Public Engagement Manager)
107.1 HA presented a number of initiatives to develop and broaden the range of people who activelyengaged with the CCG.
AG and HA had attended a meeting with the Chair of the Rothschild House Surgery patientparticipation group (which had practices in Tring and in Pitstone, which sits in Aylesbury ValeCCG) on 12 December 2016. Other participants at the meeting had been Aylesbury Vale CCGand Bucks healthcare providers. This was noted to have been a very successful discussionabout cross-CCG boundary commissioning.
Other suggestions about how to engage hard to reach groups were welcomed and should besubmitted to HA.
107.2 The Patient Participation update was noted.
107.3 ACTION: Suggestions about how to engage with hard to reach people/communities to be submitted to HA – ALL
PPI/57/16 Finance Update – Annual Report and Accounts 2015-16 (Chief Finance Officer)
PPI/108/16 Locality reports on patient and public involvement (Patient Representatives)
108.1 Dacorum – no report received.
108.2 Hertsmere – CS advised that the next meeting of the same day urgent care appointment service pilot would be on 3 January 2017.
108.3 St Albans and Harpenden – The meeting held on 30 November was noted to have been a great success and JW was commended on how well it had been chaired.
108.4 Watford and Three Rivers – Due to CB’s recent hospital admission, there was no written report from the locality. However, CB noted that the NHS winter pressures meeting held on 17 November had been useful. AG, HA and Sarah Hill, Chief Locality Officer for Watford and Three Rivers, had been discussing additional representation from the locality and would update the committee shortly.
108.5 The Committee noted the reports from the locality patient groups.
PPI/109/16 Update on patient representative involvement in HVCCG business meetings (Patient Representatives)
109.1 Young people takeover day was agreed to have been a great success. This was a priority group
to engage with.
109.2 The Committee noted the report from C Sutherland and H Clothier.

5 | P a g e
PPI/110/16 Any Other Business (Chair)
110.1 GR highlighted the recently reported cases involving Herts Valleys patients with eating
disorders being sent to Glasgow for treatment. This was noted to be specialist commissioning
undertaken by NHS England and outside of Herts Valleys’ remit. JR agreed to provide an
update on this issue.
There was no other AOB.
110.2 ACTION: J Rodgers to provide an update on specialist commissioning around treatment for eating disorders.
PPI/111/16 Risks identified during the meeting
111.1 There were no new risks identified during the meeting.
PPI/112/16 Items for cascade to the localities
112.1 Broadening patient participation – HA to provide
STP engagement activities and YCYF website – LM to provide
112.2 ACTION: B Gunson to circulate the STP presentation to the committee.
PPI/113/16 Date and time of next meeting
10.00-13.00, Wednesday 15 February 2017.

1 | P a g e
Meeting : QUALITY AND PERFORMANCE COMMITTEE Date : 02/02/17 Time : 10.00am Venue : Apsley Meeting Room, Hemel One
Present: Stuart Bloom (SB) Board Lay Member and Meeting Chair Charles Allan (CA) Director of Contracting and Resilience Diane Curbishley (DC) Director of Nursing & Quality Trevor Fernandes (TF) GP Board Member (Dacorum) Alison Gardner (AG) Board Lay Member Caroline Hall (CH) Chief Finance Officer (from QP/23.2/17) Clair Moring (CM) GP Board Member (Watford & Three Rivers) Richard Pile (RP) GP Board Member (St Albans & Harpenden) Thida Win (TW) Secondary Care Consultant to the Board In attendance: Margaret Morgan (MM) Patient Representative Katy Patrick (KP) Risk Manager (Minutes) Caroline Sutherland (CS) Patient Representative to the Board Miranda Sutters (MS) Locum Consultant in Public Health (from QP/5.1/17) Cameron Ward (CW) Interim Accountable Officer (QP/18/17 to QP/21/17 & from QP/23.2/17). Rod While (RW) Head of Corporate Governance (QP/18/17 to QP/25/17)
QP/18/17 Welcome and apologies for absence (SB) 18.1 • The Chair welcomed colleagues to the meeting.
• The Chair noted that a poor pack of papers had been circulated in advance of themeeting that lacked information about financial and QIPP plans for 2017/18. CWcommented that this work is being progressed on a daily basis and a paper would betabled today.
18.2 • Apologies for absence were received from Annette Keen.
QP/19/17 Declarations of interests (SB) 19.1 • No conflicts of interest were declared to the Chair in advance of the meeting by
committee members.• No interests were declared by attendees in relation to agenda items.
QP/20/17 Minutes of previous meeting (SB) 20.1 The minutes of the previous meeting were reviewed and approved. 20.2 The minutes were approved as an accurate record of the meeting of 5 January 2017.
QP/21/17 Matters arising and action log (SB) 21.1 The action log was reviewed.
QP/179.10/16 CA has asked Simon Pattison to monitor the HPFT 24 hour waits for urgent referrals to CMHT. Nothing is currently being reported as an exception. Action to be closed. QP/07.9/17 CA will confirm the urgent care clinical lead with the CCG Chair on Friday, 3 February 2017. QP/11.3/17 The service level agreement with East & North Herts CCG to provide a service for
Final Approved Minutes
Item 15.2

2 | P a g e
Individual Funding Requests has been amended and will be signed by David Buckle, Medical Director on his return from leave on 7 February 2017.
CW left the meeting QP/22/17 Serious Incidents report 2016/17 Q3 (DC) 22.1 • DC noted that the report includes detail of the two never events flagged to the
Committee in January. Investigation of these incidents is on the 60-day pathway tocompletion.
• An alert has been raised in relation to a death related to use of cot sides in thecommunity. The patient was discharged home from West Herts Hospital Trust(WHHT) with cot sides. A great many agencies were involved in the care of thispatient so the matter has been raised as a HVCCG serious incident initially, in order toidentify the biggest contributing factors. Gathering all the necessary information islikely to take longer than the usual 60 days. NHS England (NHSE) has been madeaware. This is the second occurrence nationally involving cot sides in a patient’s ownhome. Such incidents are considered to be entirely preventable. Nursing homes havereceived a message from the CCG confirming that they should assess each patient’sneeds and risks individually.
22.2 The following points were raised in discussion: • It would be useful to include a brief note about the cot sides alert in the GP bulletin.• WHHT has made significant progress with the prevention and management of
pressure ulcers. There has, however, been a recent cluster. The Nursing & Qualityteam are working to review these as a group and record lessons learned.
22.3 The Committee noted the update on serious incidents. 22.4 ACTION: Include information about the cot sides alert in the GP bulletin (DC)
QP/23/17 Quality alert system (QAS) update 2016/17 Q3 (DC) 23.1 • Figures remain high with the system being well used by GPs.
• Real progress has been made with trusts who are demonstrating much betterengagement with quality reports and understanding that the purposes are to identifythemes and trends.
• WHHT now include a quality section in every newsletter.• Some alerts are still being challenged as ‘inappropriate’. These often present an
opportunity for GP education, for example in relation to the Consultant to Consultantreferral policy, or education of hospital doctors, for example where they are askingGPs to write a sickness certificate. Some alerts have arrived with the wrong providerfollowing pathway changes.
CH and CW joined the meeting 23.2 The following points were raised in discussion:
• Hertfordshire Community Trust report that 40 per cent of the quality alerts theyreceive are for services that they no longer provide. GPs need to be reminded of the up-to-date contact details.
• Letters to GPs from consultants are not necessarily ‘inappropriate’ but rather, poorlyworded. For example, a consultant should be asking the GP to review a patient discharged by them in the light of information provided, not requesting that the patient is referred by the GP on to other specific services.
• It is good to see that some positive steps have been made with the system.• There are still frequent concerns reported about incomplete, late and/or inaccurate
discharge summaries. This is a serious matter that needs to be given priority.• There is no national standard by which discharge summaries are measured or
financial penalties available in the contracts. Concerns about the quality of dischargesummaries is something that has been raised frequently at clinical partnership groupmeetings but the messages do not seem to be getting through, so a differentapproach may be required. The importance of accurate and timely information being

3 | P a g e
received by GPs should perhaps be flagged directly to registrars at the trusts. It may be helpful to offer the trusts written examples of what information is crucial, what else a GP would reasonably expect to receive, as well as what information is not necessary.
• The Emergency Care Improvement Plan includes work on professional standards that is being overseen by national colleagues. These improvements are also part of the Urgent Care and A&E recovery plan. They can also be raised in relation to data quality challenges.
23.3 The Committee noted the update on QAS. 23.4 ACTION: Check that information about contact details for providers made available to GPs is
up-to-date (DC) 23.5 ACTION: Raise concerns about discharge summaries in connection with information and
data quality challenges and be clear about what is expected (CA) QP/24/17 Month 9 finance report (CH) 24.1 • CH noted that the report circulated prior to the meeting is now in a new format with
less focus on the year-to-date position. • A set of slides was tabled to update the committee on recent developments. • The CCG’s financial position and achievement of the target control total of £8m
variance from plan remains extremely challenging. • The main contributory areas are in acute and CHC.
24.2 The following points were raised in discussion: • There are still large risks in the financial recovery plan. There are two key areas of
focus at present: - CHC data cleanse; - challenges to ensure correct charging and appropriate application of
penalties. • The CCG has a further assurance meeting with NHSE on 3 February. The exact amount
of the control total, originally discussed as being within a range from £8m to 10m, will be explored at that meeting.
• Contracting, BI and finance teams are working together to try and identify reasons for over-performance in acute and any particular specialisms of note. This information is not yet available. New reporting from February will include more narrative.
• If the CCG does not achieve the control total that it agrees with NHSE the main consequences will be additional scrutiny and reporting as well as a referral to the Secretary of State. It is anticipated that the more robust plans that are in place for recovery and a QIPP target of £38m (plus additional schemes up to (£45m) will mean that NHSE are willing to allow HVCCG to have time to put these in place. However, any marginal increase in activity could have a huge impact over the next few months.
• The CCG plans to work collaboratively with providers to improve system performance and the financial position. A change in behaviours will be needed in order to make improvements.
• The total acute figure includes a great number of providers, including those in the independent sector. Efforts to divert activity away from WHHT have resulted in increased activity in other providers, but the costs are the same.
• Activity is very high across the country, with increased numbers of very ill people attending hospital. It is important to benchmark HVCCG against other CCGs nationally, but this does not alter our statutory financial duties.
• There is no easy solution to the long delays experienced in receiving data from the national reporting system.
24.3 The Committee considered the further report tabled. • Slide 13 sets out the recovery plan for 2017/18 with a QIPP target of £38m (£33m so
far identified) and other opportunities.

4 | P a g e
• A significant proportion of the QIPP plan involves disinvestment and there istherefore a degree of confidence about delivery in the key savings area.
• HVCCG is meeting weekly with WHHT at a QIPP board to cement plans prior to thestart of the new financial year.
• It is critical not only for the CCG, but also for WHHT, to divert those patients who donot need to attend the hospital to more appropriate services.
• It continues to be very important to maintain pace through the weekly financialturnaround and QIPP meetings.
24.4 The following points were raised in discussion: • The lack of any falls work for older people is a concern that will be picked up with CW
at another meeting.• The bringing forward of contract timetables offers an opportunity in Q1 of 2017/18 to
begin work on what should be in the contracts for 2018/19.• GPs need advance notice of meetings with WHHT in order to be able to attend
regularly.• There will be a focus on hospital prescribing for bio-similar drugs.• There are still some areas to be tightened up in relation to procedures of low clinical
value.• Discussions and decisions made at the Investment Committee are summarised in the
table on page 8. Consideration of some opportunities is pending. The main reason forsetting up this committee was so that additional schemes could be consideredquickly. Next steps will be to evaluate all CCG investments from the £700m+allocation.
24.5 The Committee noted the M9 update on finance. 24.6 ACTION: Share future meeting dates with WHHT with TF (CW)
QP/25/17 Transformation and QIPP report (CH) 25.1 • The Committee were asked to note the performance summary.
• QIPP performance is only part of the financial picture.• The new format of reporting is less detailed but includes intelligence with the factual
reporting about which schemes are working, which are not and the actions beingtaken.
25.2 The following points were raised in discussion: • The more focused style is helpful.• The Chair noted that it is concerning that there are only a few weeks left this financial
year and still a big gap in the QIPP plan for 2017/18. £33m of £38m has beenidentified so far, with a further £7m of schemes required for headroom. The 2017/18plan needs to be fully worked up and in place before the start of the new financialyear.
25.3 The Committee noted the Transformation and QIPP report. RW left the meeting QP/26/17 Integrated quality and performance report (CA/DC) 26.1 • CA noted that A&E departments were busy nationally over Christmas and New Year
with neighbouring CCGs all under significant and continuing pressure.• One surgical ward has been closed due to the respiratory outbreak (report on care
homes discussed later).• Pressure in the hospitals is having an effect on the RTT targets with electives
cancelled on a number of days in the last few months. The CCG is looking at how theycan support moves to outsourced providers.
• CA tabled the monthly reporting timetable for acute contracts for information inrelation to the timescales for receipt of data.
CH left the meeting 26.1 contd. • The Royal Free London (RFL) has not achieved the return to standard anticipated for

5 | P a g e
62 day cancer waits. There have been many efforts to improve this performance but the new appointments have not had the impact expected. The national team is now looking for reasons why there has been no movement.
• The consortium’s revised recovery action plan for East of England Ambulance ServiceTrust (EEAST) is now with NHSE and NHS Improvement for sign off. Locally, west Herts has made use of Hospital Ambulance Liaison Officers (HALOs), but the recovery plan is looking again at how to get maximum numbers of personnel on 999 vehicles and an evaluation of HALOs is therefore being carried out. There are some concerns with the overall plan as it still relies on recruitment and retention of staff which is an area where EEAST have not achieved targets in the past. Further discussion is underway about what it might be possible to do locally.
• CA noted that the standstill period for the integrated urgent care procurement haspassed with no challenges and the result will be shared in a communication with the Board. The move to mobilisation will be from 24 February, earlier than originally expected.
• HPFT have been missing the 28 day target which they report is due to a huge increasein referrals. The increase correlates with the time they started self-referrals. This has been discussed at SLT and it seems that it is only the initial phone calls that are a problem, not the services then delivered.
26.2 The following points were raised in discussion: • It is important that EEAST not only look at capacity and capability but also actively
triage the use of ambulance services to prevent patients being conveyed inappropriately. HVCCG are trying to push for a standard 8% ‘hear and treat’ in the EEAST contract.
• We need to also make sure that contacts for alternative services are included inEEAST’s Directory of Services. The evaluation of rapid response services is to be discussed later today. E&NHCCG has had some positive outcome data from using an emergency care practitioner (ECP) in a car.
• Significant progress has been made on the 52 week waits at RFL with just a fewanomalies remaining.
• In-hours visits are still being passed over to the out-of-hours staff at HUC (125 inNovember) when they should be sent back to the practices in E&N Herts. HVCCG have stated that this must cease immediately. Under the new contract these services will be contractually separate. Need to check whether the update promised by 20 January was received.
26.3 • DC had no quality issues to flag from the report• The outcome of the CQC re-inspection is awaited with the checks for factual accuracy
completed. HVCCG has written a letter outlining how we would continue to supportthe Trust if necessary. A quality summit is scheduled for 24 February 2017 to discussthe outcomes.
26.4 The Committee noted the IQPFR. 26.5 ACTION: Error for correction in the section on HUC procurement: action plan should read
‘May 2016 to January 2017’(CA/Stephanie White) 26.6 ACTION: Check whether HUC returned the requested responses to E&NHCCG by 20 January
2017 (CA)
QP/27/17 Respiratory outbreak in care homes (DC) 27.1 • 21 care homes have been affected in west Hertfordshire with only 8 affected in east
and north Hertfordshire. Two further homes have been added since the report wascirculated, but the rate has now slowed.
• 7 care homes remain closed with two of them now undertaking deep-cleaning andpreparing to re-open. There are no scheduled re-opening dates for the other 5homes.

6 | P a g e
• The Nursing & Quality team has been involved in a lot of communication interfacewith the East of England Health Protection team, Public Health England (PHE) andcare home challenges around prescribing and screening.
27.2 The following points were raised in discussion: • Communications came out, via fax, late on a Friday afternoon asking for prescribing of
prophylaxis for care home residents. There was a time lag with passing on the national messages from PHE and the subsequent dispensing of prescriptions that meant many would be ineffective.
• Lessons have been learned about working with the Health Protection team and theMemorandum of Understanding will be reviewed in the light of recent events.
• One surgical ward has been closed at WHHT with patients infected in all three bays aswell as staff.
27.3 The Committee noted the briefing.
QP/28/17 Committee work plan (SB) 28.1 • An update on the Continuing Healthcare action plan has been scheduled for 2 March
2017. • Future finance reports to include an update from the Investment Committee.
28.2 The Committee noted the updated work plan. 28.3 ACTION: Arrange for the inclusion of an Investment Committee update in the M10 finance
report, showing what has been agreed and delivery (CH)
QP/29/17 Risks identified during the meeting (SB) 29.1 • Financial risks continue to be of concern.
QP/30/17 Items for cascade to localities (SB) 30.1 • As a result of the continued use of the quality alert system (QAS) by GPs, providers
are reporting more regularly on quality issues.• The CCG are aware of the issue relating to prescribing for care homes. This is part of
on-going discussions with Public Health England about creating a clearer pathway.
QP/31/17 Any other business (SB) 31.1 • MS raised a query about local plans for vascular surgery and stroke. A draft strategy
will be going to the Commissioning Executive in two weeks’ time. MS to liaise with CAand Avni Shah.
31.2 ACTION: Discuss stroke strategy paper with MS (CA)
QP/32/17 Next meeting (SB) 32.1 2 March 2017, Apsley meeting room, 2nd floor, Hemel One, 10.00am

1 | P a g e
Meeting : Audit Committee Date : Thursday January 12 2017 Time : 10.00am Venue : Apsley meeting room, Hemel One, Hemel Hempstead
Present:
Paul Smith (PS) Audit Chair & Board Lay Member
Stuart Bloom (SB) Board Lay Member
Alison Gardner (AG) Board Lay Member
Rami Eliad (RE) Board GP Member, Watford and Three Rivers
Mike Edwards (ME) Board GP Member, Hertsmere
Daniel Carlton-Conway (DCC) GP Locality Chair, St Albans and Harpenden
In attendance:
Lisa Clampin (LC) Lead Partner, East Anglia / Head of Public Sector Assurance, BDO
Diane Curbishley (DC) Director of Nursing and Quality (AC/09/17 & AC/18/17 only)
Sarah Howe (SH) Manager, Internal Audit, RSM
Ed Knowles (EK) Assistant Director, Integrated Healthcare (AC/11/17 & AC/17-18/17 only)
Katy Patrick (KP) Risk Manager (Minutes)
Jo Reeder (JRe) Personal Health Budget lead (AC/18/17 only)
Cameron Ward (CW) Interim Accountable Officer
Rod While (RW) Head of Corporate Governance
Tad Woroniecki (TW) Deputy Chief Finance Officer
AC/01/17 Welcome, introductions & apologies for absence (PS)
1.1 PS welcomed attendees.
Apologies for absence were received from Caroline Hall, Alison Langridge and CliveMakombera.
AC/02/17 Declarations of Interest (PS)
2.1 There were no interests declared in relation to the agenda items.
AC/03/17 Minutes of previous meeting (PS)
3.1 The Committee reviewed the minutes of the previous meeting.
3.2 The minutes of 13 October 2016 were approved as an accurate record of the meeting.
AC/04/17 Matters Arising and Action Log (PS)
4.1 The Committee reviewed the action log and noted the following:
AC/19.8/16 A policy on confidential papers, using the NHS England classificationsystem, will be finalised within the next four weeks. Outcomes of RSM’s audit oflocalities will inform the content of the policy.
AC/98.5/16 RW to explain to Hein Scheffer the committee’s requirements forwhistleblowing updates, which are to include both data and assurance that the policy isworking in the organisation.
All other outstanding items were included on the agenda for this meeting.
4.2 ACTION: Advise HS of the Committee’s requirements for whistleblowing updates (RW)
Final Approved Minutes
Item 15.3

2 | P a g e
AC/05/17 Gifts and Hospitality Register (RW)
5.1 RW noted that the register is the latest version and it has been made clear which itemshave not been seen before.
There is one minor error to note: HSJ sponsorship was £300 not £301.
5.2 The following points were raised in discussion:
The fee noted for KB refers to a speaking engagement.
GP forum attendance and fees payable are a separate issue to be picked up at theInvestment Committee.
5.3 The Committee noted the Gifts and Hospitality Register which is updated on an on-going basis.
AC/06/17 Decision Register (RW)
6.1 The decision register now includes the whole of Q3 2016-17, including InvestmentCommittee decisions.
This version of the register has not yet been published as it is important that this isco-ordinated with provider discussions. The register will be published prior to the nextBoard meeting, but the published version will only include matters where a finaldecision has been taken.
6.2 The following points were raised in discussion:
It would be useful if items that are intended as savings are shown in brackets todistinguish them from expenditure.
6.3 The Committee noted the decision register which now captures all Committees.
6.4 ACTION: Future versions of the register to highlight savings amounts with the use of brackets (RW)
AC/07/17 Conflict of interests (COI) self-certification (RW)
7.1 CCGs are now required to make annual and quarterly submissions on a simple templateto self-certify their compliance with new COI guidance. This is the second quarterlysubmission.
No breaches have been reported. All relevant information is captured on the websitelink.
The outcome of the internal audit of COI is not yet known.
7.2 The following points were raised in discussion:
It is helpful to confirm that all the necessary arrangements are in place.
The management of conflicts of interest is working well operationally, with conflictshandled sensibly in meetings and participants only excluded when decisions are beingmade.
It would be useful to include the link to registered interests on Board agendas.7.3 The Committee noted the COI self-certification document.
7.4 ACTION: Add link to published register of interest to future Board agendas (RW)
AC/08/17 Business critical models: Macpherson recommendations (CW)
8.1 The paper addresses the validity of models used by the CCG and whether or not theyare sufficiently robust.
The CCG needs a method by which to judge whether models are sufficientlyaccurate/kept up to date/reviewed periodically.
Those recommendations in the Macpherson report that are relevant to CCGs have beenadopted together with some additional measures.
The recommendations and good practice included in this summary paper will beincorporated into revision of the business case processes.
8.3 The Committee supported the recommendations which are an important discipline that will improve confidence in the numbers upon which the CCG relies for decision making. An

3 | P a g e
update in 6 months’ time was requested.
8.4 ACTION: Add update in six months’ time to the committee planner (KP)
DC joined the meeting
AC/09/17 Continuing healthcare (CHC) review (CW/RW/DC)
9.1 This is the second time that difficulties have been encountered with CHC and it isimportant that lessons are learned across the organisation.
The Executive Team decided that it would be helpful to conduct a detailed internalinvestigation of CHC processes and systems. It was agreed that an external review wasunnecessary, but it was important that the Audit Committee had oversight of thereport, its conclusions and recommended actions.
Everyone involved in the investigation was open and honest about the difficultiesuncovered.
Two key issues were identified:- internal processes;- internal communication, particularly between the CHC and Finance teams.
There are a number of recommendations that have a wider organisational impact,particularly in relation to QIPP schemes.
9.2 DC commented on the report.
The review of CHC processes and systems was welcomed. Significant concerns aboutCHC have been expressed over the past few years, before the current problems wereuncovered. It is useful to highlight the issues and plan forward, but not all of theproblems are yet fully understood.
Recommendations and responses are detailed in Appendix 1, have been agreed by theCFO and reviewed by the Executive Team.
An intensive period of work has been put in place over the next three months to bringsystems up to date.
Under the QIPP scheme, 70 backlog reviews have been conducted already in January sothe work is moving rapidly. Processes in last year’s QIPP scheme were not sufficientlyrobust but they have been strengthened this year.
The CCG team are working closely with the local authority to get commitment thatfunding for every individual will be from the right source by 1 April 2017.
The team, supported by Phil Church the Turnaround Director, has committed to gainingan absolute understanding of CHC expenditure by the end of February 2017. The mainchallenge is that when invoices come in, the CHC system is not adequate enough forthe finance team to be able to marry them up.
Communication between the two directorates has also been flagged as an issue and DCand the CFO have committed to improving liaison with immediate effect. Finance staffare already embedded as part of the CHC team.
9.2 The following points were made in discussion:
The projected £6.25M variance will be quality assured by the end of February.
DC has overriding responsibility for CHC but needs involvement of colleagues in thefinance team.
Weekly checks are currently conducted on the variance.
Phil Church has brought external finance resource into the CHC team this week andthey are partly looking at reconciliation
DCC joined the meeting
9.2 contd.
It is concerning to note that convincing, but erroneous, verbal and written assuranceswere given to DC by the interim Assistant Director that the QIPP target was on trackand would be delivered.
DC was aware that there was an over spend of approximately £1.8m and understoodthe reasons for that figure. Further overspends were not reported. There is a good dealof confidence in the new Assistant Director who has vast experience. The seniorstructure has also been changed so that both the Director and the Deputy Director of

4 | P a g e
Nursing & Quality are over CHC. The structure underneath has also been changed with more clinical input at an operational level.
Going forward, learning for the CCG is that further assurance is required. There arelinks here to the business critical models item. Experience from elsewhere is useful. Theorganisation will also be raising the profile of looking at performance with the seniorleadership team reviewing a range of indicators.
A letter to the former interim AD has been proposed, advising her of the problems thathave come to light. The Director of Workforce has reservations about this because ofthe difficulty of knowing specifically what was done.
The report highlights two issues, of staff morale and location of the team, that arebeing taken forward with an options paper coming to the Executive Team on 24January. There will be significant challenges associated with bringing an additional teamof 33 people into Hemel One.
The proposed improvement plan will come to Q&P to provide assurance.
The vacancy rate in the team has halved since the new AD joined HVCCG as she hasattracted staff to come and work with her. Risks to business and delivery are beingconsidered in relation to all vacancies.
A lot of work has been scheduled for completion by the end of March, but there areinterim staff in place to tackle the backlog and this will therefore have no impact onbusiness as usual.
This is a critical item for year end. If all of this work is completed as planned uncertaintyabout the figures will be removed.
This document may not need to be confidential going forward, but it is important tosequence actions. CH and DC as lead directors to agree what may be shared and whenfor the purposes of wider learning.
9.3 The Committee noted the review of CHC and action plan.
9.4 ACTION: Agree with CH what may be shared and when (DC)
AC/10/17 STP governance (RW)
10.1 There is agreement among audit chairs across the country that current governancearrangements for STPs are not ideal.
Currently, all decision making has to be referred back to 12 individual Boards, sinceneither the joint executive group nor the programme board are recognised inlegislation. There is a Chairs’ oversight group, chaired by Nicolas Small and supportedby RW, but there is no appetite for delegation.
There is also no co-ordination in the way that the organisations involved are regulated,being at an organisational not STP level.
A number of other areas are putting in place a memorandum of understanding (MoU)and initial discussions about this have taken place with Tom Cahill, the STP lead.
PwC are conducting a review of STPs that will cover governance among other thingsand may make some useful recommendations.
10.2 The following points were raised in discussion:
It is a concern that we seem to be moving away from the clinically led model of CCGs toa lack of clinical involvement in STPs. There is a meeting being held with clinical leadson Friday 13 January where the best method to ensure that the clinical voice is heard inSTPs will be discussed.
It is important to get programme governance set up first, before trying to agree anMoU between all organisations. The meeting in February will provide an opportunity torevisit this and PwC recommendations will hopefully also help with this discussion.
In the absence of any other formal governance arrangements, an MoU would be anadvance.
10.3 The Committee noted the update on STP governance and endorsed the proposal of an MoU.
10.4 ACTION: Communicate the Committee’s endorsement of an MoU to the STP Chairs’ group
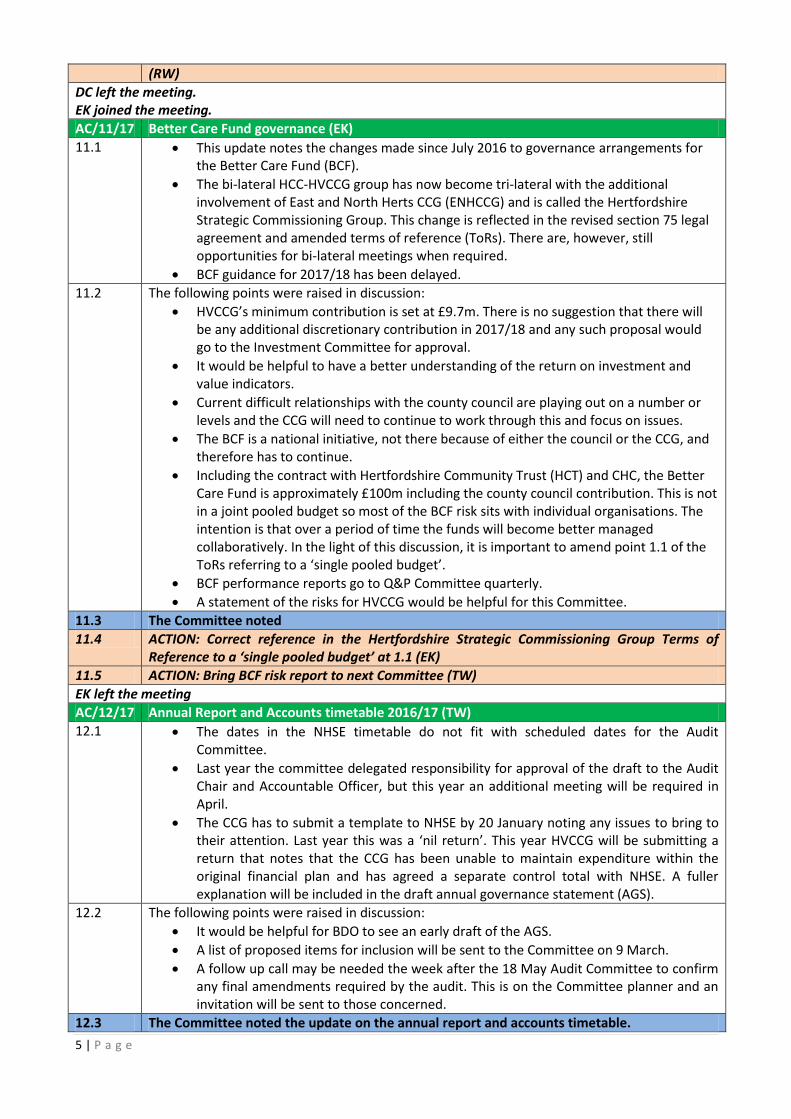
5 | P a g e
(RW)
DC left the meeting. EK joined the meeting.
AC/11/17 Better Care Fund governance (EK)
11.1 This update notes the changes made since July 2016 to governance arrangements forthe Better Care Fund (BCF).
The bi-lateral HCC-HVCCG group has now become tri-lateral with the additionalinvolvement of East and North Herts CCG (ENHCCG) and is called the HertfordshireStrategic Commissioning Group. This change is reflected in the revised section 75 legalagreement and amended terms of reference (ToRs). There are, however, stillopportunities for bi-lateral meetings when required.
BCF guidance for 2017/18 has been delayed.
11.2 The following points were raised in discussion:
HVCCG’s minimum contribution is set at £9.7m. There is no suggestion that there willbe any additional discretionary contribution in 2017/18 and any such proposal wouldgo to the Investment Committee for approval.
It would be helpful to have a better understanding of the return on investment andvalue indicators.
Current difficult relationships with the county council are playing out on a number orlevels and the CCG will need to continue to work through this and focus on issues.
The BCF is a national initiative, not there because of either the council or the CCG, andtherefore has to continue.
Including the contract with Hertfordshire Community Trust (HCT) and CHC, the BetterCare Fund is approximately £100m including the county council contribution. This is notin a joint pooled budget so most of the BCF risk sits with individual organisations. Theintention is that over a period of time the funds will become better managedcollaboratively. In the light of this discussion, it is important to amend point 1.1 of theToRs referring to a ‘single pooled budget’.
BCF performance reports go to Q&P Committee quarterly.
A statement of the risks for HVCCG would be helpful for this Committee.
11.3 The Committee noted
11.4 ACTION: Correct reference in the Hertfordshire Strategic Commissioning Group Terms of Reference to a ‘single pooled budget’ at 1.1 (EK)
11.5 ACTION: Bring BCF risk report to next Committee (TW)
EK left the meeting
AC/12/17 Annual Report and Accounts timetable 2016/17 (TW)
12.1 The dates in the NHSE timetable do not fit with scheduled dates for the AuditCommittee.
Last year the committee delegated responsibility for approval of the draft to the AuditChair and Accountable Officer, but this year an additional meeting will be required inApril.
The CCG has to submit a template to NHSE by 20 January noting any issues to bring totheir attention. Last year this was a ‘nil return’. This year HVCCG will be submitting areturn that notes that the CCG has been unable to maintain expenditure within theoriginal financial plan and has agreed a separate control total with NHSE. A fullerexplanation will be included in the draft annual governance statement (AGS).
12.2 The following points were raised in discussion:
It would be helpful for BDO to see an early draft of the AGS.
A list of proposed items for inclusion will be sent to the Committee on 9 March.
A follow up call may be needed the week after the 18 May Audit Committee to confirmany final amendments required by the audit. This is on the Committee planner and aninvitation will be sent to those concerned.
12.3 The Committee noted the update on the annual report and accounts timetable.

6 | P a g e
12.4 ACTION: Arrange an additional short Audit Committee meeting to review and approve the draft ARA prior to submission on 21 April (KP)
12.5 ACTION: Send invitation for teleconference to agree any final changes with BDO prior to the final submission (KP)
12.6 ACTION: Share early draft of AGS with BDO (TW)
AC/13/17 External Audit update (LC)
13.1 It is still early in the audit process, but meetings have taken place with CW in Octoberand with PS today.
A report on the outcome of BDO’s risk assessment process and a statement of theplanned audit strategy will come to the next Committee, together with an indication ofwhen the audit will take place.
Dates will be agreed with the finance team.
13.2 The Committee noted the external audit update.
AC/14/17 Internal Audit Plan (SH)
14.1 SH introduced the draft internal audit plan for 2017/18 that has been reviewed withExecutive Directors.
Section 4 of the report notes questions that the Committee might wish to considerwhen deciding whether the plan meets their requirements.
14.2 The following points were raised in discussion:
In the current financial circumstances, with the Investment Committee sometimesmaking decisions to disinvest, it is important to consider the impact on healthinequalities. For this reason the Equality and Quality Impact Assessment (EQIA) hasbeen amended.
As there are proposed changes to the CCG’s business planning process it may behelpful to build in an audit to review how it is working in 2017/18.*
The next review planned of cyber security is in 2019/20, but a recent review wasundertaken as part of the 2016/17 plan and this will be reported to the Committee inMarch.
The audit of provider contract management needs to include sufficiently detailedassurance about the monitoring arrangements for providers.*
There has been some discussion about the most appropriate timing for an audit of co-commissioning. If it took place early if would be an advisory piece but would havelittle evidence to review. This can be removed from the 2017/18 plan.*
As collaborative arrangements are so key to transformation there might be anargument for bringing this audit forward but there was pressure to include otherthings in the plan. A paper could be brought to the Committee by the Directorinstead.
14.3 The Committee noted the audit plan for 2017/18 and broadly agreed the content with the clarifications and amendments noted above*.
14.4 ACTION: Re-engage with CH and CW to discuss proposal to audit the new business case process (SH)
14.5 ACTION: Re-visit the Provider Contract Management plan with Charles Allan and ensure that the CCG’s monitoring arrangements are covered in sufficient detail in the scope (SH)
14.6 ACTION: Delay the audit of primary care co-commissioning (SH)
14.7 ACTION: Bring assurance paper to the next Committee on collaborative arrangements (CA)
AC/15/17 Internal Audit Progress Report (SH)
15.1 The report refers to three final audit reports.
The audit of information governance has now been finalised and all other audits areon track for completion by March.

7 | P a g e
74% of the evidence uploaded in relation to recommendations has been validated.There are no concerns relating to the other 24% - this is simply a timing issue.
There have been no further breaches of the 20 working day limit for the submission ofmanagement responses.
The audit of Urgent Care Sustainability returned an amber-red opinion which isunsurprising given the current performance issues such as the A&E and delayedtransfers of care targets. Recommendations have been made in relation to formalscrutiny of schemes included in the recovery plan and risk sharing arrangements.Most actions have already been implemented or are underway.
The audit of Financial Planning and QIPP also returned an amber-red opinion with onehigh-priority recommendation relating to business cases. The medium-priorityrecommendations included a review of the budget setting processes, EQIA, deadlinesand accountabilities for QIPP actions.
15.2 The following points were made in discussion:
There have been weaknesses in the QIPP processes in the past, but a significantamount of work has been undertaken over the past few months to address these. TheInvestment Committee has helped with this. The business case process is undergoinga review that will be concluded by the end of the month.
The Executive Team has discussed the budget setting timetable and process report.
15.3 The risk management audit noted improvements and best practice and returned anamber-green opinion. A recommendation has been made to embed the monthlyreview of directorate risk registers at all team meetings.
15.4 The following points were made in discussion:
The Board has discussed Institute of Risk Management research on ‘ExtendedEnterprise’ and the implications for the CCG in the context of the STP and sharedownership of some system risks. The paper has been shared with Tom Cahill and itsapplication for HVCCG is being pursued.
15.3 The Committee noted the internal audit progress report.
AC/16/17 Internal audit report recommendations tracker (KP)
16.1 There are six internal audit recommendations outstanding. Three of these relate toCHC and the issues discussed in relation to the review paper. The others have beensubject to a slight delay due to pressures associated with the planning and contractinground being brought forward this year.
16.2 The Committee noted the report.
EK joined the meeting
AC/17/17 Review of risk related to Your Care, Your Future implementation (EK)
17.1 The risk register for Your Care, Your Future (YCYF) implementation has been recentlyredrafted and re-formatted and is now reported on the HVCCG risk register template.
YCYF is a system-wide change project but it has been established that the principlerisks should be reflected across HVCCG’s organisational risk registers.
The programme delivery approach focuses on three main developments: redesign ofacute provision; redesign of clinical pathways; and development of hubs.
There are also key enablers such as an appropriately trained workforce and improvedIT infrastructure. HVCCG Director of Workforce is working with Director of Contractingand Resilience on an action plan and risk mitigation in relation to workforce.
Section 4 of the report outlines areas of high risk associated with the project.- To all intents and purposes, YCYF is the delivery of the STP in west Hertfordshire.
However, there is still some formalisation of STP governance and decision making to be agreed. For this reason the current risk score remains relatively high.
- There is a risk related to insufficient financial headroom to invest or reallocate resources which may make the forecast savings figures ambitious. Mitigation is largely dependent upon financial transparency across the system and a need to

8 | P a g e
agree upon how limited resources may best be spent across the system. For these reasons the current risk score is relatively high.
- Another significant risk relates to the acute work stream and the ambition for new models of care (NMCs) and pathways to be sufficiently developed to achieve a shift in activity. Mitigation includes an in depth review of the scope of activity shift required, plus a detailed assessment of whether the plans for NMCs are ambitious enough. This currently remains a high risk.
17.2 The following points were raised in discussion:
This report is very timely on two levels:- New processes for business cases should help to reduce the risks around delivery
in NMCs - The Multi-Partner Pathway Collaborative (MPPC) will be a vehicle to help with the
cultural change needed to deliver collaborative arrangements and agree resource allocation.
Baseline principles need to be agreed, in order that there are no double payments forservices. There is a clear message to providers that we pay on actual delivery.
DC and JRe joined the meeting
17.2 contd. Whenever an opportunity arises to bid for additional funds and we think we have agood case the CCG does pursue it. For example, Children and Adolescent MentalHealth Services have been successful with several significant bids and a number ofother bids have been made in relation to the STP.
Progress with acute reconfiguration and the hubs are both clearly affected by NHSE’sstatement that capital funding is subject to clear constraints. The partners need toconsider contingency plans if the level of funding we have bid for in the strategicoutline case is not sufficiently compelling.
17.3 The Committee noted the update on YCYF implementation risks.
17.4 ACTION: Consider what contingency plans might be added to the STP and YCYF risk registers (EK)
AC/18/17 Personal health budgets (DC/JRe)
18.1 This paper presents current assurance around the CCG’s financial and operationalprocesses for personal health budgets (PHBs).
PHBs were implemented in Herts Valleys two years ago. In 2015/16 there were 29 andin the current year to date there have been 47 approved so it would appear to be agrowing area.
HVCCG was recently successful in a bid to pilot Integrated PersonalisedCommissioning (IPC).
18.2 The following points were raised in discussion:
Although there has been an increase in expenditure on PHBs, all recipients arecurrently CHC patients and costs are, on average, cheaper when converted to a PHB.There is confidence in the numbers for the indicative budget which are based onrobust methodology. This is not impacted by the separate CHC financial issues.Scrutiny of PHB has been significantly more intensive with smaller numbers ofpatients. This work will continue to be developed as numbers move towardsmateriality and lessons will be learned from the CHC problems.
All new cases are subject to financial monitoring with subsequent monitoring carriedout at least quarterly and then annually by Essex Coalition of Disabled People (ECDP).All of this monitoring is up to date. There is a dedicated PHB nurse and all money isprocessed by ECDP as direct payments or held and administered on the patient’sbehalf. Monthly management accounts are received with monthly reconciliation ofbank statements. In cases where a risk assessment concludes that there is a higherfinancial risk for an individual, monitoring will be conducted more frequently.
ECDP provide a PHB service for a number of other CCGs and the local authority and

9 | P a g e
HVCCG has been happy with the service. Nevertheless, independent assurance about their financial controls should be sought by HVCCG to ensure that they are looking after this money properly. The finance team meet with them regularly and will be asked to seek formal external assurance.
A recent patient story to the Board suggested that a better quality of care isexperienced with PHBs.
It is important, especially as the number of PHB awards is expected to continue rising,that the CCG has firm assurance that the forecast savings are real. The IPC groupbeing established will have stronger governance arrangements with more robustplanning. Social care has 20 years of experience with PHBs and there is learning aboutvalue for money for the CCG from this experience on a larger scale.
As the use of PHBs for long term conditions will present more challenges in terms ofproving their cost-effectiveness it will be useful to develop better governance now.
18.3 The Committee noted the update on PHB processes.
18.4 ACTION: Seek independent external assurance about ECDP financial controls (TW)
DC and JRe left the meeting EK left the meeting
AC/19/17 Board Assurance Framework 2016-17, Q3 (KP)
19.1 No current risk scores have changed on the Board Assurance Framework (BAF) but KPhas worked with risk owners and leads to improve assurances and develop actions.For example an action plan is being developed collaboratively between HR andPlanned and Primary Care to address workforce requirements of the new clinicalpathways.
At the next Risk Management Group meeting in February the senior leadership teamwill have the opportunity to discuss the YCYF implementation risks presented to theCommittee today and how they impact individual directorates.
The Risk Management Group was not quorate in December due to competingdemands for a number of ADs in relation to the planning and contracting round.
19.2 The following points were raised in discussion:
More frequent work force updates have been requested by Q&P (currently receivedquarterly).
19.3 The Committee noted the 2016-17 Q3 BAF update.
AC/20/17 Review of risk management strategy and procedure (KP)
20.1 The paper proposes revision of the risk definition at section 3 of the strategy to bringit in line with the ISO 31000 risk framework that has been adopted by HVCCG.
The ISO definition acknowledges that risk exists on a spectrum ranging from positive(an opportunity) to negative (a threat).
This definition also has more relevance to the current risk context with our extendedenterprise in the STP.
20.2 The Committee accepted the proposed amendments to HVCCG’s risk definition.
AC/21/17 Review of bad debt right offs, tender waivers and losses & compensations (TW)
21.1 TW confirmed that there were none to report that he was aware of.
21.2 The Committee noted the update.
AC/22/17 Committee work plan (KP)
22.1 The plan for 2017/18 has been developed in consultation with RSM.
LC noted that the planner for March includes BDO external audit plan and fees whichwas a PSAA contractual requirement under the former arrangements, but is no longerrequired.
22.2 The Committee work plan was noted.

10 | P a g e
22.3 ACTION: Remove the item noted above from the planner (KP)
AC/23/17 Items for cascade to localities (PS)
23.1 The Committee did not note any items for cascade.
AC/24/17 Date and time of next meeting (PS)
24.1 9 March 2017, 10.00am Plus additional meeting on 20 April 2017, 11.00am




















