Hepatic and portal vein thrombosis in cirrhosis: Possible role in development of parenchymal...
10
Hepatic and Portal Vein Thrombosis in Cirrhosis: Possible Role in Development of Parenchymal Extinction and Portal Hypertension IAN R. WANLESS, 1 FLORENCE WONG, 2 LAWRENCE M. BLENDIS, 2 PAUL GREIG, 3 E. JENNY HEATHCOTE, 2 AND GARY LEVY 2 Obliterative lesions in portal veins (PVs) and hepatic veins (HVs) of all sizes are known to occur in cirrhotic livers. PV lesions have generally been attributed to thrombosis, but the pathogenesis of the HV (veno-occlu- sive) lesions is unknown. We have studied 61 cirrhotic livers removed at transplantation to clarify the preva- lence, distribution, and pathogenesis of venous lesions, as well as the association of these lesions with other morphological features and clinical morbidity. Intimal fibrosis that is highly suggestive of healed HV or PV thrombosis was found in at least 70% and 36% of livers, respectively. The distribution of HV lesions was patchy and largely confined to veins between 0.1 and 3 mm in diameter, suggesting multifocal origin in small veins. PV lesions were more uniform throughout the liver, sug- gesting origin in large veins with propagation to the small veins. HV lesions were associated with regions of confluent fibrosis (focal parenchymal extinction), and PV lesions were associated with regional variation in the size of cirrhotic nodules and a history of bleeding varices. These observations suggest that thrombosis of medium and large PVs and HVs is a frequent occurrence in cirrhosis, and that these events are important in caus- ing progression of cirrhosis. (HEPATOLOGY 1995;21:1238- 1247.) Cirrhosis develops when parenchymal injury is fol- lowed by fibrous obstruction of sinusoids and adjacent small portal veins (PVs) and hepatic veins (HVs). Most cirrhotic livers have a uniform pattern of fibrous septa Abbreviations: PV, portal vein; HV, hepatic vein; FPE, focal parenchymal extinction. From the Departments of 1Pathology,'~Medicine, and 3Surgery,The Toronto Hospital, University of Toronto; and the Canadian Liver Pathology Reference Centre, Toronto, Canada. ReceivedAugust 19, 1994; accepted October 25, 1994. The Canadian Liver Pathology ReferenceCentre is supported by the Cana- dian Liver Foundation. This work was presented in part at the annual meeting of the American Association for the Study of Liver Diseases, Chicago, IL, November 6, 1993 (HEPATOLOGY 1993;18:112A), and at the biennial scientificmeeting of the In- ternational Association for the Study of the Liver, Cancdn, Mexico,May 23, 1994 (HEPATOLOGY 1994;19:139I). Address reprint requests to: Ian R. Wanless, MD, Department of Pathology, The Toronto Hospital, 200 Elizabeth St, Toronto, Canada, M5G 2C4. Copyright © 1995 by the American Association for the Study of Liver Diseases. 0270-9139/95/2105-000453.00/0 and regenerative nodules. However, we have noted re- gional variation in fibrosis in cirrhotic livers that is associated with obstruction of medium and large he- patic vessels. The purpose of the present study is to document the morphological and clinical features of these forms of regional parenchymal heterogeneity and obstructive lesions in PVs and HVs in cirrhotic livers. Our results suggest the vascular lesions are a result of thrombosis and regional parenchymal heterogeneity is secondary to vascular obstruction. Intrahepatic thrombosis may have an important influence on the natural history of cirrhosis. MATERIALS AND METHODS Sixty-one cirrhotic livers removed at time of transplanta- tion were studied. The patients were adults treated at The Toronto Hospital in 1992 or 1993. The specimens were unse- lected, except that livers with incomplete cirrhosis or cirrho- sis caused by HV thrombosis were excluded. Twenty-four liv- ers obtained at autopsy from patients without cirrhosis served as controls. Livers were examined grossly for weight, configuration, size of nodules, appearance of large PVs and HVs and regional heterogeneity in nodule size and parenchy- mal fibrosis. Histological blocks were obtained prospectively. The main HVs were sampled within 1 cm of their ostia, and the left and right PVs were sampled within 1 cm of the hilum. The main PV was sampled in most cases. Other blocks were taken from peripheral left and right lobes to show parenchyma; regions of maximal fibrosis were sampled. A mean of 17 blocks were obtained per liver. These were embedded in par- affin, sectioned, and stained with hematoxylin-eosin and elas- tic-trichrome. Iron, periodic acid-Schiff with diatase, and orcein stains were performed on one block from each liver. Grading for anatomic parameters is summarized in Table 1. Intimal fibrosis and luminal narrowing were graded (0 through 5) for each of the large veins (left, middle, and right HVs; left, right, and main PVs) and medium HVs and PVs from left and right lobes. Veins were called large if they were greater than 3 mm in diameter and medium if they were 0.2 to 3 mm in diameter. The gradings were defined as 1 (focal but definite intimal fibrosis), 2 (intimal fibrosis involving at least two-thirds of the circumference with luminal narrowing < 10%), 3 (intimal fibrosis with luminal narrowing approxi- mately 10% to 40%), 4 (intimal fibrosis with luminal nar- rowing 40% to 80%), and 5 (luminal narrowing >80%). For medium veins, the most severe lesion found in each lobe de- termined the grade for that lobe. Acute thrombi were sought but not included in the grading of luminal narrowing. 1238
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Hepatic and portal vein thrombosis in cirrhosis: Possible role in development of parenchymal...

Hepatic and Portal Vein Thrombosis in Cirrhosis: Possible Role in Development of Parenchymal Extinction
and Portal Hypertension
IAN R. WANLESS, 1 FLORENCE WONG, 2 LAWRENCE M. BLENDIS, 2 PAUL GREIG, 3 E. JENNY HEATHCOTE, 2 AND GARY LEVY 2
Obliterative l e s ions in portal ve ins (PVs) and hepat ic ve ins (HVs) of all s izes are k n o w n to occur in c irrhot ic livers. PV les ions h a v e general ly been attr ibuted to thrombosis , but the p a t h o g e n e s i s o f the HV (veno-occlu- sive) l es ions is u n k n o w n . We h a v e s tudied 61 c irrhot ic l ivers r e m o v e d at t ransp lantat ion to clarify the preva- lence, distribution, and p a t h o g e n e s i s o f v e n o u s les ions , as wel l as the as soc ia t ion of these les ions w i th o ther morpho log ica l features and cl inical morbidity. Int imal fibrosis that is h ighly sugges t ive of hea led HV or PV thrombos i s w a s found in at least 70% and 36% of livers, respect ively . The dis tr ibut ion o f HV les ions w a s patchy and largely conf ined to ve ins b e t w e e n 0.1 and 3 m m in diameter , sugges t ing mult i foca l origin in smal l veins. PV les ions w e r e more un i form t h r o u g h o u t the liver, sug- ges t ing origin in large ve ins w i th propagat ion to the smal l veins . HV les ions w e r e assoc ia ted wi th reg ions of conf luent f ibrosis (focal p a r e n c h y m a l ext inct ion) , and PV les ions w e r e assoc iated wi th reg ional var ia t ion in the s ize o f c irrhot ic nodules and a h is tory of b leeding varices. These observat ions sugges t that thrombos i s of m e d i u m and large PVs and HVs is a frequent occurrence in cirrhosis , and that these events are important in caus- ing progress ion of cirrhosis . (HEPATOLOGY 1995;21:1238- 1247.)
C i r r h o s i s d e v e l o p s w h e n p a r e n c h y m a l i n j u r y is fol- l o w e d b y f i b r o u s o b s t r u c t i o n o f s i n u s o i d s a n d a d j a c e n t s m a l l p o r t a l v e i n s (PVs) a n d h e p a t i c v e i n s (HVs) . M o s t c i r r h o t i c l i v e r s h a v e a u n i f o r m p a t t e r n o f f i b ro us s e p t a
Abbreviations: PV, portal vein; HV, hepatic vein; FPE, focal parenchymal extinction.
From the Departments of 1Pathology, '~Medicine, and 3Surgery, The Toronto Hospital, University of Toronto; and the Canadian Liver Pathology Reference Centre, Toronto, Canada.
Received August 19, 1994; accepted October 25, 1994. The Canadian Liver Pathology Reference Centre is supported by the Cana-
dian Liver Foundation. This work was presented in part at the annual meeting of the American
Association for the Study of Liver Diseases, Chicago, IL, November 6, 1993 (HEPATOLOGY 1993; 18:112A), and at the biennial scientific meeting of the In- ternational Association for the Study of the Liver, Cancdn, Mexico, May 23, 1994 (HEPATOLOGY 1994; 19:139I).
Address reprint requests to: Ian R. Wanless, MD, Department of Pathology, The Toronto Hospital, 200 Elizabeth St, Toronto, Canada, M5G 2C4.
Copyright © 1995 by the American Association for the Study of Liver Diseases.
0270-9139/95/2105-000453.00/0
a n d r e g e n e r a t i v e n o d u l e s . H o w e v e r , w e h a v e n o t e d re- g i o n a l v a r i a t i o n in f i b ros i s in c i r r h o t i c l i v e r s t h a t is a s s o c i a t e d w i t h o b s t r u c t i o n of m e d i u m a n d l a r g e he - p a t i c v e s s e l s . T h e p u r p o s e of t h e p r e s e n t s t u d y is to d o c u m e n t t h e m o r p h o l o g i c a l a n d c l i n i c a l f e a t u r e s of t h e s e f o r m s of r e g i o n a l p a r e n c h y m a l h e t e r o g e n e i t y a n d o b s t r u c t i v e l e s i o n s in P V s a n d H V s i n c i r r h o t i c l i ve r s .
O u r r e s u l t s s u g g e s t t h e v a s c u l a r l e s i o n s a r e a r e s u l t of t h r o m b o s i s a n d r e g i o n a l p a r e n c h y m a l h e t e r o g e n e i t y is s e c o n d a r y to v a s c u l a r o b s t r u c t i o n . I n t r a h e p a t i c t h r o m b o s i s m a y h a v e a n i m p o r t a n t i n f l u e n c e on t h e n a t u r a l h i s t o r y of c i r r h o s i s .
M A T E R I A L S A N D M E T H O D S
Sixty-one cirrhotic l ivers removed at t ime of t r ansp lan ta - t ion were studied. The pa t ien ts were adul t s t r ea ted at The Toronto Hospi ta l in 1992 or 1993. The specimens were unse- lected, except t ha t l ivers with incomplete cirrhosis or cirrho- sis caused by HV thrombosis were excluded. Twenty-four liv- ers obta ined at autopsy from pa t ien ts wi thout cirrhosis served as controls. Livers were examined grossly for weight, configuration, size of nodules, appearance of large PVs and HVs and regional heterogenei ty in nodule size and parenchy- mal fibrosis.
Histological blocks were obtained prospectively. The ma in HVs were sampled wi thin 1 cm of the i r ostia, and the left and r ight PVs were sampled wi thin 1 cm of the hilum. The ma in PV was sampled in most cases. Other blocks were t aken from per iphera l left and r ight lobes to show parenchyma; regions of maximal fibrosis were sampled. A mean of 17 blocks were obtained per liver. These were embedded in par- affin, sectioned, and s ta ined with hematoxyl in-eosin and elas- t ic-trichrome. Iron, periodic a c i d - S c h i f f wi th diatase, and orcein s ta ins were performed on one block from each liver. Grad ing for ana tomic pa r a me te r s is summar ized in Table 1. In t ima l fibrosis and luminal nar rowing were graded (0 th rough 5) for each of the large veins (left, middle, and r ight HVs; left, r ight , and ma in PVs) and med ium HVs and PVs from left and r ight lobes. Veins were called large if they were grea te r t han 3 m m in d iamete r and medium if they were 0.2 to 3 m m in diameter . The gradings were defined as 1 (focal but definite in t imal fibrosis), 2 ( int imal fibrosis involving at leas t two-thi rds of the circumference with luminal nar rowing < 10%), 3 ( in t imal fibrosis wi th luminal nar rowing approxi- ma te ly 10% to 40%), 4 ( int imal fibrosis wi th luminal nar- rowing 40% to 80%), and 5 ( luminal nar rowing >80%). For medium veins, the most severe lesion found in each lobe de- t e rmined the grade for t ha t lobe. Acute thrombi were sought but not included in the grading of lumina l narrowing.
1238
HEPATOLOGY Vol. 21, No. 5, 1995 WANLESS ET AL 1239
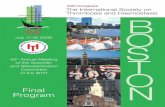
TABLE 1. S u m m a r y of A n a t o m i c G r a d i n g S y s t e m
Focal Parenchymal Extinction (% of lobar involvement on Parenchymal Fibrosis (on stained sections
Grade Vascular Disease gross appearance) at 5>< magnification)*
1 Focal intimal fibrosis < 10 Occasional broad fibrous septa 2 Intimal fibrosis involving 2/3 of circumference, 10-33 Many broad fibrous septa
< 10% luminal narrowing 3 10%-40% luminal narrowing >33 4 40%-80% luminal narrowing 5 >80% luminal narrowing
Confluent fibrosis at least 5 mm across
* Grade 0 fibrosis equals cirrhosis with uniformly narrow septa.
Parenchymal fibrosis was graded in two ways. Focal paren- chymal extinction (FPE) was defined as a grossly visible re- gion of severe parenchymal loss and fibrous replacement and was graded (0 through 3) for each lobe according to the ap- proximate percentage of involvement as 1 (< 10%), 2 (10% to 33%), or 3 (>33%). Parenchymal fibrosis was also graded by mounting all elastic-trichrome-stained slides on a light box and viewing them with a 5× lens. The fibrosis score of each slide was recorded (0 through 3) as 0 (cirrhosis with uniformly narrow septa), 1 (occasional broad fibrous septa), 2 (many broad fibrous septa), and 3 (confluent fibrosis at least 5 m m across). The fibrosis grade for the liver was the mean score of all slides.
Coronal slices of whole right lobes from 10 selected cir- rhotic livers were embedded in large paraffin blocks (up to 7 × 9 cm), and elastic-trichrome-stained sections were exam- ined to determine the topographic distribution of venous inti- mal fibrosis and parenchymal fibrosis. The location of all HVs at least 0.2 mm in diameter was marked. The HV external diameter was measured with an eyepiece graticule, and the percentage of narrowing was estimated to the nearest 10%. The parenchymal fibrosis in the region of each vein was graded on the large glass slides as described previously. Fig-
. ure 7 was produced by recording the location of fibrosis on a plastic overlay, digitizing both the overlay and the dotted slide, and superimposing the images using CorelDRAW (Corel Corporation, Ottawa, Canada). PV obstruction was es- t imated in 4 livers. For all portal tracts having arteries at least 0.03 mm in diameter, the smallest dimension of the PV lumen and the smallest outside dimension of the largest adjacent artery were measured and the PV/artery ratio was calculated. This method was used because PVs are often shrunken or not visible after thrombosis.
Clinical records were reviewed, without knowledge of ana- tomic findings, for history of variceal bleeding, esophageal sclerotherapy, portacaval anastomosis, and splenectomy. As- cites was graded as 1 (mild, treated with salt restriction only), 2 (moderate, treated and controlled with diuretics), or 3 (se- vere, resistant to diuretics or requiring large-volume para- centesis). The apparent origin was hepatitis C virus (14), primary biliary cirrhosis (9), primary sclerosing cholangitis (9), alcohol (7), hepatitis B virus (7), al-antitrypsin deficiency (3), hemochromatosis (2), autoimmunity (2), obesity (1), bili- ary atresia (1), and cryptogenic (6). Variceal bleeding had been treated using sclerotherapy in 19 patients. Five had a remote surgical shunt procedure, 2 had transjugular intrahe- patic portosystemic shunt insertion, and 9 had a splenectomy months or years before transplantation. The mean age was 49 (cirrhosis) and 69 (controls) with 66% and 46% men, re- spectively.
Statistical analysis was performed using Student's t-test (two-tailed) and X 2 test (two-tailed) or Fisher's exact test as computed by Microstat (Ecosoft Inc., Indianapolis, IN).
RESULTS
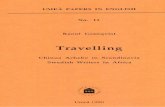
Prevalence of Lesions. Large I-IV disease (grades 3 t h r o u g h 5) was p r e sen t in one or more of the th ree ma jo r HVs in 10 l ivers (16.4%) (Fig. 1). At l eas t 80% n a r r o w i n g (grade 5) of an H V was p r e s e n t in 3 l ivers (4.9%). The p reva lence of lesions was s imi la r in the r ight , middle , and left veins, except t h a t g rade 4 and 5 lesions were not observed in the r igh t lobe. None of the controls h a d large H V disease g r e a t e r t h a n g rade 2.
M e d i u m H V disease (grades 3 t h r o u g h 5) was p r e sen t in 43 l ivers (70%) (r ight lobe, 36; left lobe, 33) (Fig. 1). None of the controls h a d m e d i u m H V disease g r e a t e r t h a n g rade 2. La rge H V disease cor re la ted wi th me- d ium H V disease in the s a m e lobe (Fig. 2). However , l a rge H V disease was u sua l ly less severe t h a n m e d i u m H V disease in the s a m e lobe.
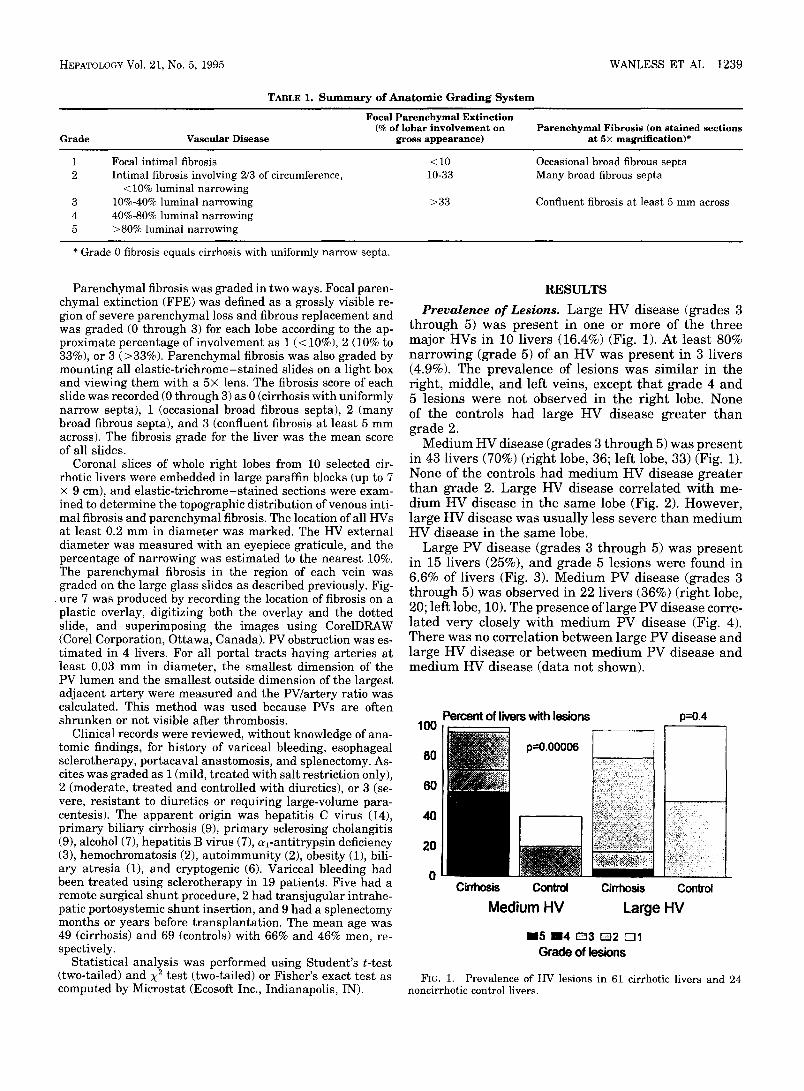
La rge PV disease (grades 3 t h r o u g h 5) was p r e s e n t in 15 l ivers (25%), and g rade 5 lesions were found in 6.6% of l ivers (Fig. 3). M e d i u m PV disease (grades 3 t h r o u g h 5) was observed in 22 l ivers (36%) (r ight lobe, 20; left lobe, 10). The p resence of l a rge PV disease corre- l a ted ve ry closely wi th m e d i u m PV disease (Fig. 4). The re was no cor re la t ion be tween large PV disease and large H V disease or be tween m e d i u m PV disease and m e d i u m H V disease (da ta not shown).
100
80
60
40
20
Percent of livers with lesions p=0.4
FIG. 1.
Cirrhosis C o n t r o l Cirrhosis Control
Medium HV Large HV
BB5 BB4 D 3 D 2 E31 Grade of lesions
Prevalence of HV lesions in 61 cirrhotic livers and 24 noncirrhotic control livers.
1240 WANLESS ET AL HEPATOLOGY May 1995
4 . 4
o 3 . " " , 3
lm - W e-
( lee
" 0 . - - , , . , . , - , . , • • - J O
e e
e l e
eee eee
ee •
i
• e e
eee ee
e e e e • •
0 1 2 3 4 5 M e d i u m - s i z e d hepat ic ve ins
FIG. 2. Correlation between disease in large and medium HVs. Each dot represents the grading of medium HVs and large HVs in the same lobe (P < .01 [)/2 = 46.6; d f = 25]).
0 1 2 3 4 5 M e d i u m - s i z e d portal ve ins
FIG. 4. Correlation between disease in large and medium PVs. Each dot represents the grading of medium PVs and large PVs in the same lobe (P < .0001 [X 2 = 96.4; d f = 25]).
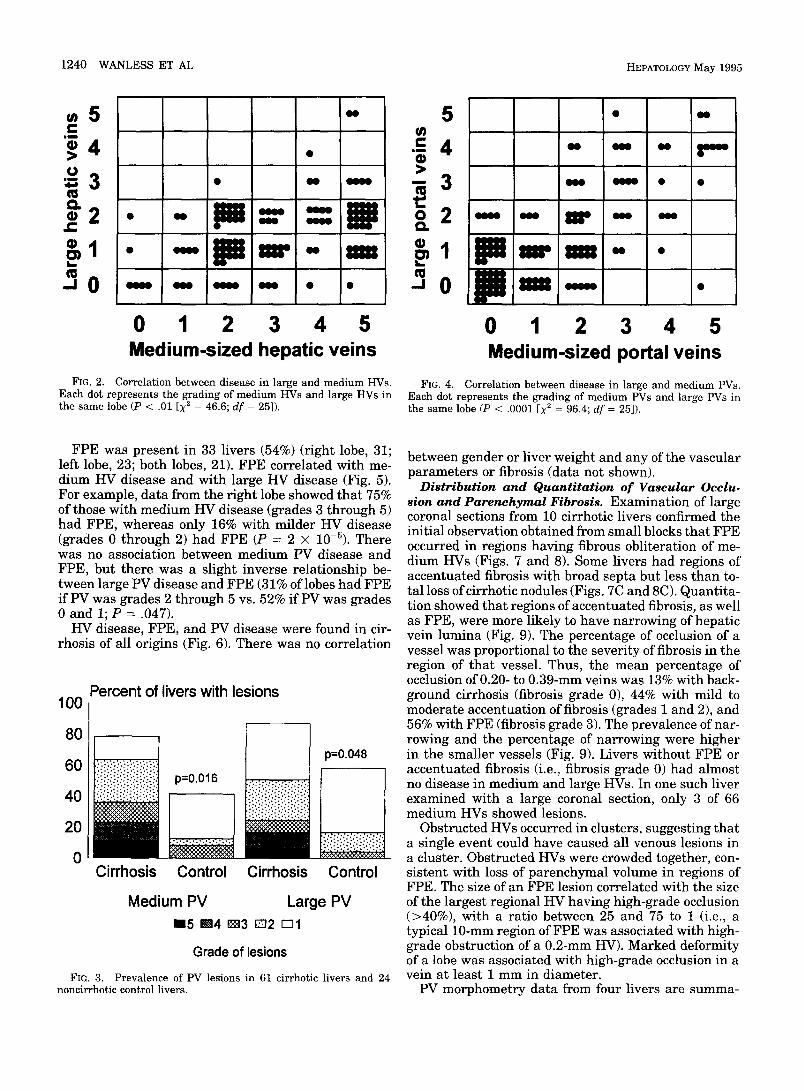
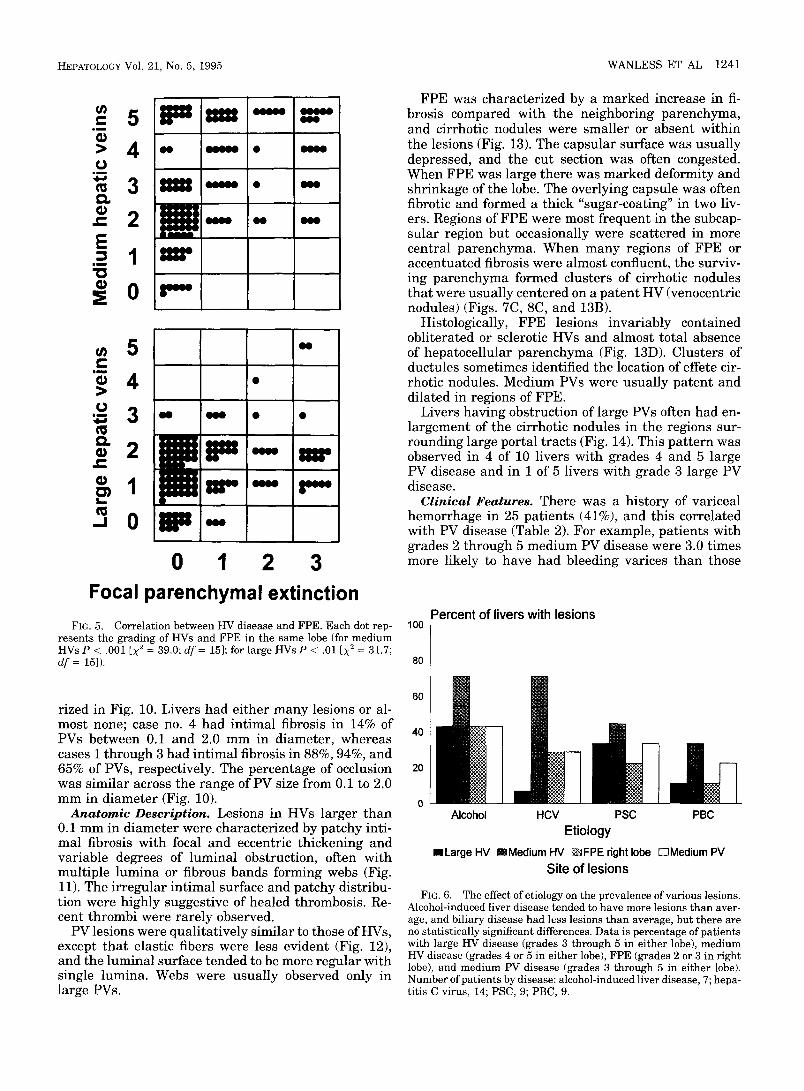
FPE was present in 33 livers (54%) (right lobe, 31; left lobe, 23; both lobes, 21). FPE correlated with me- dium HV disease and with large HV disease (Fig. 5). For example, data from the right lobe showed that 75% of those with medium HV disease (grades 3 through 5) had FPE, whereas only 16% with milder HV disease (grades 0 through 2) had FPE (P = 2 × 10-5). There was no association between medium PV disease and FPE, but there was a slight inverse relationship be- tween large PV disease and FPE (31% of lobes had FPE i fPV was grades 2 through 5 vs. 52% i fPV was grades 0 and I; P = .047).
HV disease, FPE, and PV disease were found in cir- rhosis of all origins (Fig. 6). There was no correlation
Percent of livers with lesions 100
80
60
40
20
0 Cirrhosis Control Cirrhosis
p=0.048
' . : . : . : . : . : . : . : . : . : .
Control
Medium PV Large PV m5 B=4 m3 E22 ~1
Grade of lesions
FIG. 3. Prevalence of PV lesions in 61 cirrhotic livers and 24 noncirrhotic control livers.
between gender or liver weight and any of the vascular parameters or fibrosis (data not shown).
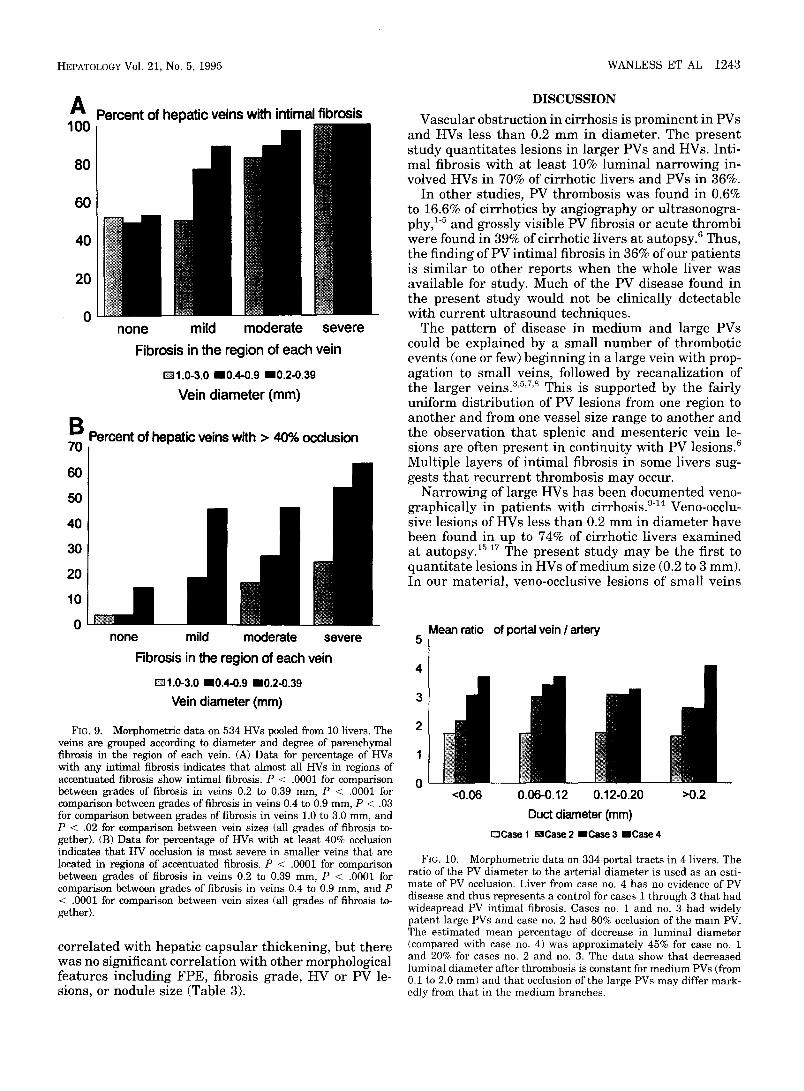
Distribution and Quanti tat ion of Vascular Occlu- sion and Parenchymal Fibrosis. Examination of large coronal sections from 10 cirrhotic livers confirmed the initial observation obtained from small blocks that FPE occurred in regions having fibrous obliteration of me- dium HVs (Figs. 7 and 8). Some livers had regions of accentuated fibrosis with broad septa but less than to- tal loss of cirrhotic nodules (Figs. 7C and 8C). Quantita- tion showed that regions of accentuated fibrosis, as well as FPE, were more likely to have narrowing of hepatic vein lumina (Fig. 9). The percentage of occlusion of a vessel was proportional to the severity of fibrosis in the region of that vessel. Thus, the mean percentage of occlusion of 0.20- to 0.39-mm veins was 13% with back- ground cirrhosis (fibrosis grade 0), 44% with mild to moderate accentuation of fibrosis (grades 1 and 2), and 56% with FPE (fibrosis grade 3). The prevalence of nar- rowing and the percentage of narrowing were higher in the smaller vessels (Fig. 9). Livers without FPE or accentuated fibrosis (i.e., fibrosis grade 0) had almost no disease in medium and large HVs. In one such liver examined with a large coronal section, only 3 of 66 medium HVs showed lesions.
Obstructed HVs occurred in clusters, suggesting that a single event could have caused all venous lesions in a cluster. Obstructed I-tVs were crowded together, con- sistent with loss of parenchymal volume in regions of FPE. The size of an FPE lesion correlated with the size of the largest regional HV having high-grade occlusion (>40%), with a ratio between 25 and 75 to 1 (i.e., a typical 10-mm region of FPE was associated with high- grade obstruction of a 0.2-mm HV). Marked deformity of a lobe was associated with high-grade occlusion in a vein at least 1 mm in diameter.
PV morphometry data from four livers are summa-
HEPATOLOGY Vol. 21, No. 5 ,1995 WANLESS ET AL 1241
5 M m
3 ~ A
K ~ X X X m •
E= 1 ==,
0 z"-
N
N
2 [JnF z z -
1 = = =
" 0 IZ l= , "
0 1 2 3 Focal parenchymal extinction
FIG. 5. Correlation between HV disease and FPE. Each dot rep- resents the grading of HVs and FPE in the same lobe (for medium HVs P < .001 [X: = 39.0; df = 15]; for large HVs P < .01 [X 2 = 31.7; df = 15]).
rized in Fig. 10. Livers had either many lesions or al- most none; case no. 4 had intimal fibrosis in 14% of PVs between 0.1 and 2.0 mm in diameter, whereas cases I through 3 had intimal fibrosis in 88%, 94%, and 65% of PVs, respectively. The percentage of occlusion was similar across the range of PV size from 0.1 to 2.0 mm in diameter (Fig. 10).
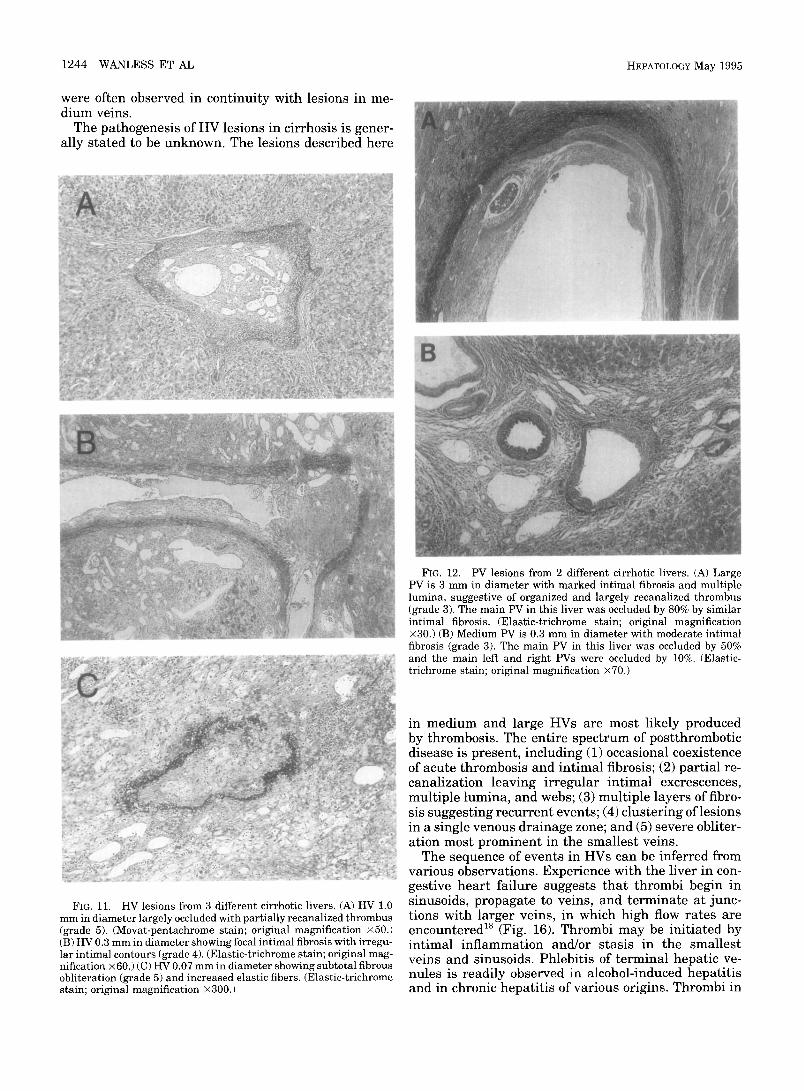
Anatomic Description. Lesions in HVs larger than 0.1 mm in diameter were characterized by patchy inti- mal fibrosis with focal and eccentric thickening and variable degrees of luminal obstruction, often with multiple lumina or fibrous bands forming webs (Fig. 11). The irregular intimal surface and patchy distribu- tion were highly suggestive of healed thrombosis. Re- cent thrombi were rarely observed.
PV lesions were qualitatively similar to those of HVs, except that elastic fibers were less evident (Fig. 12), and the luminal surface tended to be more regular with single lumina. Webs were usually observed only in large PVs.
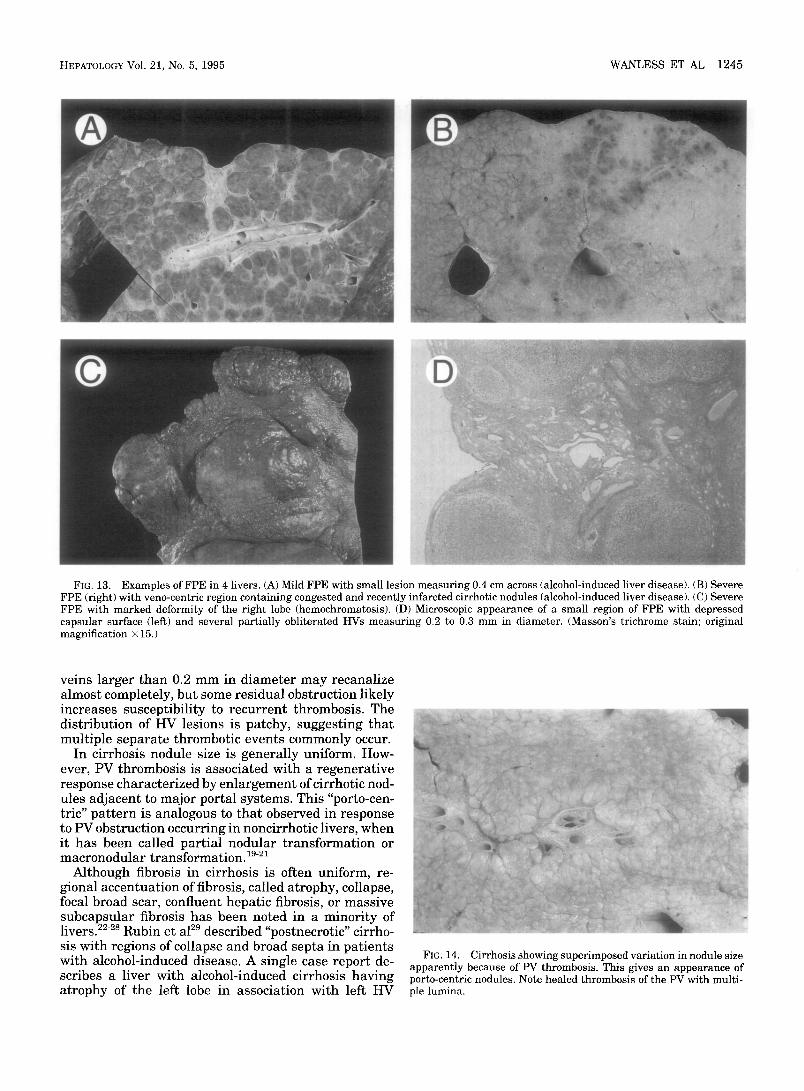
FPE was characterized by a marked increase in fi- brosis compared with the neighboring parenchyma, and cirrhotic nodules were smaller or absent within the lesions (Fig. 13). The capsular surface was usually depressed, and the cut section was often congested. When FPE was large there was marked deformity and shrinkage of the lobe. The overlying capsule was often fibrotic and formed a thick "sugar-coating" in two liv- ers. Regions of FPE were most frequent in the subcap- sular region but occasionally were scattered in more central parenchyma. When many regions of FPE or accentuated fibrosis were almost confluent, the surviv- ing parenchyma formed clusters of cirrhotic nodules that were usually centered on a patent HV (venocentric nodules) (Figs. 7C, 8C, and 13B).
Histologically, FPE lesions invariably contained obliterated or sclerotic HVs and almost total absence of hepatocellular parenchyma (Fig. 13D). Clusters of ductules sometimes identified the location of effete cir- rhotic nodules. Medium PVs were usually patent and dilated in regions of FPE.
Livers having obstruction of large PVs often had en- largement of the cirrhotic nodules in the regions sur- rounding large portal tracts (Fig. 14). This pat tern was observed in 4 of 10 livers with grades 4 and 5 large PV disease and in 1 of 5 livers with grade 3 large PV disease.
Clin ica l Features . There was a history of variceal hemorrhage in 25 patients (41%), and this correlated with PV disease (Table 2). For example, patients with grades 2 through 5 medium PV disease were 3.0 times more likely to have had bleeding varices than those
Percent of livers with lesions 100
80
60
40
20
Alcohol HCV PSC PBC
Etiology
ULarge HV mMedium HV ~ F P E right lobe I~Medium PV
Site of lesions
FIG. 6. The effect of etiology on the prevalence of various lesions. Alcohol-induced liver disease tended to have more lesions t han aver- age, and biliary disease had less lesions t han average, but there are no statistically significant differences. Data is percentage of pat ients with large HV disease (grades 3 through 5 in ei ther lobe), medium HV disease (grades 4 or 5 in ei ther lobe), FPE (grades 2 or 3 in r ight lobe), and medium PV disease (grades 3 through 5 in ei ther lobe). Number of pat ients by disease: alcohol-induced liver disease, 7; hepa- titis C virus, 14; PSC, 9; PBC, 9.

1242 WANLESS ET AL HEPATOLOGY May 1995
A
!! iiii iii!i iii iiiii i iii iiii i ii!iii !iiii i iiiiiiiiiii i i i! ii!iiii i!iiiiii iiiii i ii~ i i~*-'!i ~ i i i ii ~iiiiiiliiiiiiiiiiliiiiiiiiiiiiiiiiii!iiiiii~i ii~i!:!!!!::̧:̧!ii!!!~!ii~iiii!:!:! .......
patient data (Fig. 15) showed that many patients with bleeding varices had evidence of intrahepatic PV occlu- sion even when the main or first order PVs had less than 10% narrowing of their lumina. There was no correlation between HV disease and variceal bleeding (Table 2).
There was a history of ascites in 79% of patients; in 38% of patients ascites was severe (grade 3). Ascites
. . . . . . . . . . P " . . . . . . . . 7 . . . .
[ ] Cirrhotic parenchyma with broad fibrous septa
Focal parenchymal extinction (densely fibrotic liver)
o 0 0 0 0 0 O • o o 0 •
Normal 10-70% <'10% >70%
> 1.0 mm
0,6-'1,0 mm
0,2-0.6 mm
Vein diameter
Percent occlusion of hepatic veins
FIG. 7. Diagrams mapping the location of all HVs at least 0.2 mm in diameter, luminal occlusion, and focal accentuation of paren- chymal fibrosis. (A and B) Pat ient with cirrhosis and severe FPE. The pat ient was a 42-year-old man with hepati t is C virus cirrhosis, severe bleeding varices, and no ascites. (A) Right lobe. The HVs with high-grade obstruction are clustered and crowded together in regions of severe FPE. The main HVs were widely patent but with mild int imal fibrosis. (B) Left lobe. Many HVs with no int imal fibrosis are located in regions without FPE. (C) Pat ient with cirrhosis related to hemochromatosis. There is no well-defined region of FPE but wide- spread geographic accentuation of fibrosis tha t correlates with the location of HV lesions. Veins greater t han 0.3 mm in diameter have part ial occlusion suggesting recanalized thrombus, but many HV between 0.1 and 0,3 mm in diameter have high-grade obstructive lesions.
with grades 0 or 1 PV disease (53.8% vs. 18.2%; P = .012). This relation was still present after the 12 patients with prior splenectomy and/or portacaval anastomosis were excluded. Examination of individual
FIG. 8. Liver slices adjacent to those analyzed in Fig. 7. (A) Marked FPE involves half of the cross sectional area. (B) The left lobe has minimal FPE (left). (C) Cirrhosis with minimal FPE but with large geographic areas showing moderate accentuation of fibrosis and some residual small cirrhotic nodules. The regions without accentua- tion of fibrosis are often centered on the hepatic venous drainage.
HEPATOLOGY Vol. 21, No. 5, 1995
A Percent of hepatic veins with intimai fibrosis 100
80
60
40
20
0 none mild moderate severe
Fibrosis in the region of each vein
D1.0-3 .0 lB0.4-0.9 ==0.2-0.39
Vein diameter (mm)
R " - Percent of hepatic veins with > 40% occlusion 70
60
50
40
30
20
10
none mild moderate severe
Fibrosis in the region of each vein
D1.0-3.0 IB0.4-0.9 ==0.2-0.39
Vein diameter (ram)
FIG. 9. Morphometric data on 534 HVs pooled from 10 livers. The veins are grouped according to diameter and degree of parenchymal fibrosis in the region of each vein. (A) Data for percentage of HVs with any intimal fibrosis indicates that almost all HVs in regions of accentuated fibrosis show intimal fibrosis. P < .0001 for comparison between grades of fibrosis in veins 0.2 to 0.39 mm, P < .0001 for comparison between grades of fibrosis in veins 0.4 to 0.9 mm, P < .03 for comparison between grades of fibrosis in veins 1.0 to 3.0 mm, and P < .02 for comparison between vein sizes (all grades of fibrosis to- gether). (B) Data for percentage of HVs with at least 40% occlusion indicates that t tV occlusion is most severe in smaller veins that are located in regions of accentuated fibrosis. P < .0001 for comparison between grades of fibrosis in veins 0.2 to 0.39 mm, P < .0001 for comparison between grades of fibrosis in veins 0.4 to 0.9 mm, and P < .0001 for comparison between vein sizes (all grades of fibrosis to- gether).
correlated with hepatic capsular thickening, but there was no significant correlation with other morphological features including FPE, fibrosis grade, HV or PV le- sions, or nodule size (Table 3).
WANLESS ET AL 1243
DISCUSSION
Vascular obstruction in cirrhosis is prominent in PVs and HVs less than 0.2 mm in diameter. The present s tudy quanti tates lesions in larger PVs and HVs. Inti- mal fibrosis with at least 10% luminal narrowing in- volved HVs in 70% of cirrhotic livers and PVs in 36%.
In other studies, PV thrombosis was found in 0.6% to 16.6% of cirrhotics by angiography or ultrasonogra- phy, 1-5 and grossly visible PV fibrosis or acute thrombi were found in 39% of cirrhotic livers at autopsy. ~ Thus, the finding ofPV intimal fibrosis in 36% of our patients is similar to other reports when the whole liver was available for study. Much of the PV disease found in the present s tudy would not be clinically detectable with current ultrasound techniques.
The pat tern of disease in medium and large PVs could be explained by a small number of thrombotic events (one or few) beginning in a large vein with prop- agation to small veins, followed by recanalization of the larger veins. 3'5'7's This is supported by the fairly uniform distribution of PV lesions from one region to another and from one vessel size range to another and the observation that splenic and mesenteric vein le- sions are often present in continuity with PV lesions. ~ Multiple layers of intimal fibrosis in some livers sug- gests that recurrent thrombosis may occur.
Narrowing of large HVs has been documented veno- graphically in patients with cirrhosis. 9-14 Veno-occlu- sive lesions of HVs less than 0.2 mm in diameter have been found in up to 74% of cirrhotic livers examined at autopsy. ~5-17 The present s tudy may be the first to quanti tate lesions in HVs of medium size (0.2 to 3 mm). In our material, veno-occlusive lesions of small veins
Mean ratio of portal vein / artery 5
4
2
0 <0.06 0.06-0.12 0.12-0.20 >0.2
Duct diameter (mm) rTCase 1 inCase 2 ==Case 3 ==Case 4
FIG. 10. Morphometric data on 334 portal tracts in 4 livers. The ratio of the PV diameter to the arterial diameter is used as an esti- mate of PV occlusion. Liver from case no. 4 has no evidence of PV disease and thus represents a control for cases 1 through 3 that had widespread PV intimal fibrosis. Cases no. 1 and no. 3 had widely patent large PVs and case no. 2 had 80% occlusion of the main PV. The estimated mean percentage of decrease in luminal diameter (compared with case no. 4) was approximately 45% for case no. 1 and 20% for cases no. 2 and no. 3. The data show that decreased luminal diameter after thrombosis is constant for medium PVs (from 0.1 to 2.0 mm) and that occlusion of the large PVs may differ mark- edly from that in the medium branches.
1244 WANLESS ET AL HEPATOLOGY May 1995
were often observed in continuity with lesions in me- dium veins.
The pathogenesis of HV lesions in cirrhosis is gener- ally stated to be unknown. The lesions described here
FIG. 12. PV lesions from 2 different cirrhotic livers. (A) Large PV is 3 mm in diameter with marked intimal fibrosis and multiple lumina, suggestive of organized and largely recanalized thrombus (grade 3). The main PV in this liver was occluded by 80% by similar intimal fibrosis. (Elastic-trichrome stain; original magnification x30.) (B) Medium PV is 0.3 mm in diameter with moderate intimal fibrosis (grade 3). The main PV in this liver was occluded by 50% and the main left and right PVs were occluded by 10%. (Elastic- trichrome stain; original magnification x70.)
FIG. 11. HV lesions from 3 different cirrhotic livers. (A) HV 1.0 mm in diameter largely occluded with partially recanalized thrombus (grade 5). (Movat-pentachrome stain; original magnification x50.) (B) HV 0.3 mm in diameter showing focal intimal fibrosis with irregu- lar intimal contours (grade 4). (Elastic-trichrome stain; original mag- nification x60.) (C) HV 0.07 mm in diameter showing subtotal fibrous obliteration (grade 5) and increased elastic fibers. (Elastic-trichrome stain; original magnification x300.)
in medium and large HVs are most likely produced by thrombosis. The entire spectrum of postthrombotic disease is present, including (1) occasional coexistence of acute thrombosis and intimal fibrosis; (2) partial re- canalization leaving irregular intimal excrescences, multiple lumina, and webs; (3) multiple layers of fibro- sis suggesting recurrent events; (4) clustering of lesions in a single venous drainage zone; and (5) severe obliter- ation most prominent in the smallest veins.
The sequence of events in HVs can be inferred from various observations. Experience with the liver in con- gestive heart failure suggests that thrombi begin in sinusoids, propagate to veins, and terminate at junc- tions with larger veins, in which high flow rates are encountered is (Fig. 16). Thrombi may be initiated by intimal inflammation and/or stasis in the smallest veins and sinusoids. Phlebitis of terminal hepatic ve- nules is readily observed in alcohol-induced hepatitis and in chronic hepatitis of various origins. Thrombi in
HEPATOLOGY Vol. 21, No. 5, 1995 WANLESS ET AL 1245
FIG. 13. Examples of FPE in 4 livers. (A) Mild FPE with small lesion measuring 0.4 cm across (alcohol-induced liver disease). (B) Severe FPE (right) with veno-centric region containing congested and recently infarcted cirrhotic nodules (alcohol-induced liver disease). (C) Severe FPE with marked deformity of the right lobe (hemochromatosis). (D) Microscopic appearance of a small region of FPE with depressed capsular surface (left) and several partially obliterated HVs measuring 0.2 to 0.3 mm in diameter. (Masson's trichrome stain; original magnification × 15.)
veins larger than 0.2 mm in diameter may recanalize almost completely, but some residual obstruction likely increases susceptibility to recurrent thrombosis. The distribution of HV lesions is patchy, suggesting that multiple separate thrombotic events commonly occur.
In cirrhosis nodule size is generally uniform. How- ever, PV thrombosis is associated with a regenerative response characterized by enlargement of cirrhotic nod- ules adjacent to major portal systems. This "porto-cen- tric" pat tern is analogous to that observed in response to PV obstruction occurring in noncirrhotic livers, when it has been called partial nodular transformation or macronodular transformation. 19-21
Although fibrosis in cirrhosis is often uniform, re- gional accentuation of fibrosis, called atrophy, collapse, focal broad scar, confluent hepatic fibrosis, or massive subcapsular fibrosis has been noted in a minority of livers. 22-2s Rubin et a129 described "postnecrotic" cirrho- sis with regions of collapse and broad septa in patients with alcohol-induced disease. A single case report de- scribes a liver with alcohol-induced cirrhosis having atrophy of the left lobe in association with left HV
FIG. 14. Cirrhosis showing superimposed variation in nodule size apparently because of PV thrombosis. This gives an appearance of porto-centric nodules. Note healed thrombosis of the PV with multi- ple lumina.
1246 WANLESS ET AL HEPATOLOGY May 1995
TABLE 2. P r e v a l e n c e o f H i s t o r y o f B l e e d i n g V a r i c e s C o r r e l a t e d With V a s c u l a r L e s i o n s
Grade 0-1 Grade 2-5 Vessel Lesions Vessel Lesions
(%) (%) P
All patients, n = 61 Medium PV 18.2 53.8 Large PV 26.7 54.8 Medium HV 33.3 41.4 Large HV 23.1 45.8
Excluding prior portacaval anastamosis and splenectomy, n = 49
Medium PV 10.5 46.7 Large PV 25.0 42.9 Medium HV 33.3 32.6 Large HV 23.1 36.1
TABLE 3. P r e v a l e n c e o f A s c i t e s C o r r e l a t e d With V a r i o u s H e p a t i c L e s i o n s
Low-Grade High-Grade Lesion (%) Lesion (%) P
Capsular thickening* 41.9 77.8 .012 FPEt 55.5 71.4 NS
.012 Large HVs$ 56.9 70.0 NS
.046 Medium HVs$ 61.1 58.1 NS NS Large PVs$ 58.7 60.0 NS NS Medium PVs$ 61.5 54.6 NS
.016 NS NS NS
NOTE. The data are expressed as the percentage of pat ients hav- ing a history of bleeding varices among those with low-grade or high- grade vascular lesions in ei ther the left or r ight lobes.
Abbreviation: NS, not significant.
thrombosisJ ° It is likely that all these lesions represent FPE superimposed on established cirrhosis. Hales et al 2~ found HV obliteration within such lesions and sug- gested the venous lesions were secondary to the scars. We confirm the association of extinction and HV le- sions, but it seems more likely that the venous lesions are primary and the extinction is secondary.
The clinical significance of secondary HV thrombosis in cirrhosis is not certain. There is no evidence from our data to suggest that lesions of medium or large HVs are important in the genesis of ascites. However, most of our patients had moderate to severe ascites so that a type 2 error may have occurred.
5 A u) C "3 4 A
NOTE. The data are expressed as the percentage of pat ients hav- ing moderate to severe ascites among those with low-grade or high- grade lesions.
Abbreviation: NS, not significant. * Low grade = 0; high grade = 1 through 3. t Low grade = 0-1, high grade = 2-3, in ei ther the left or r ight
lobes. $ Low grade = 0-2, high grade = 3-5, in e i ther the left or r ight
lobes.
>
2
L-
Lesions in medium and large PVs correlated with a history of variceal bleeding. It is possible that PV thrombosis contributes to the development of clinical portal hypertension in patients with cirrhosis by in- creasing resistance in the large and medium PVs or by causing obliteration of small intrahepatic collateral veins. Patients with cirrhosis and partial or complete obstruction of the PV often have bleeding varices at presentation, 3'31 although we are not aware of con- trolled studies defining the importance of PV thrombo-
J
eins A e A • •
ee A ewe.. ee • ~ R ~ Focal parenchymal extinction
ee (me • &
• A A
0 1 2 3 4 5 Medium-sized portal veins
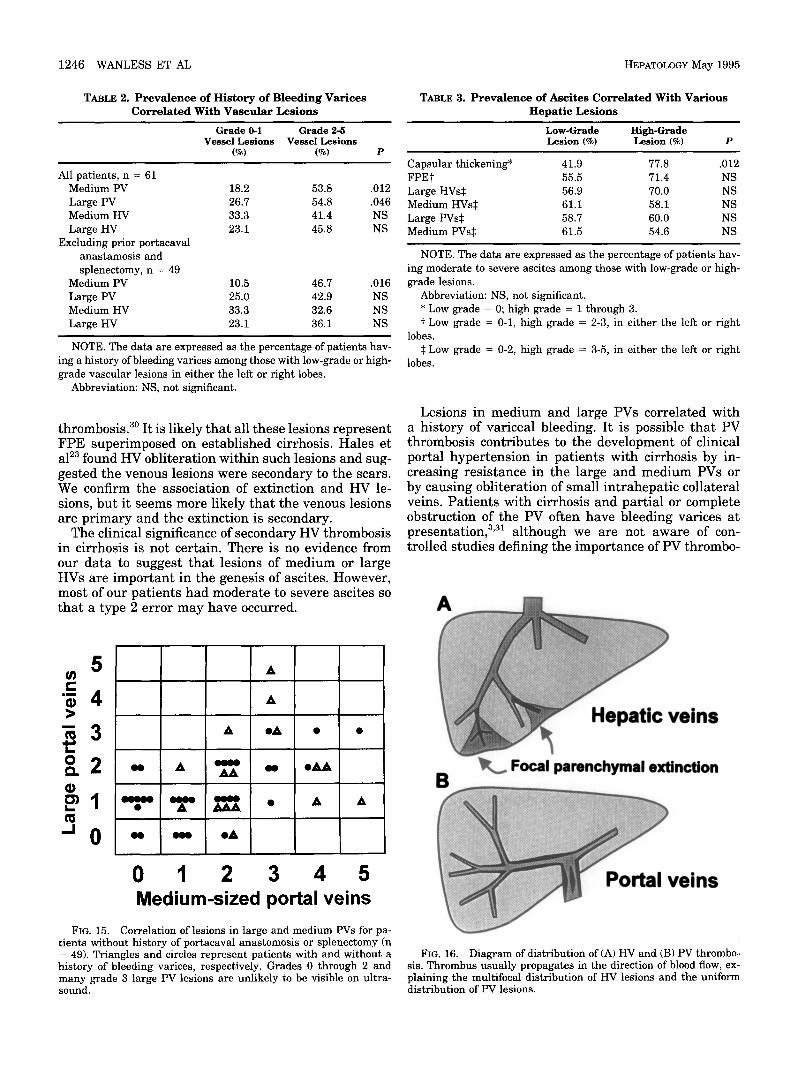
FIG. 15. Correlation of lesions in large and medium PVs for pa- t ients without history of portacaval anastomosis or splenectomy (n = 49). Triangles and circles represent pat ients with and without a history of bleeding varices, respectively. Grades 0 through 2 and many grade 3 large PV lesions are unlikely to be visible on ultra- sound.
veins
FIG. 16. Diagram of distribution of (A) HV and (B) PV thrombo- sis. Thrombus usually propagates in the direction of blood flow, ex- plaining the multifocal distr ibution of HV lesions and the uniform distribution of PV lesions.

HEPATOLOGY Vol. 21, No. 5, 1995 WANLESS ET AL 1247
sis i n p a t i e n t s w i t h c i r rhos i s . A n a l t e r n a t e i n t e r p r e t a - t i on of ou r d a t a is t h a t p a t i e n t s w i t h severe p o r t a l h y p e r t e n s i o n c a u s e d b y c i r rhos i s a re p r e d i s p o s e d to h a v e s e c o n d a r y P V t h r o m b o s i s b e c a u s e of m a r k e d s ta - sis, h y p o t e n s i o n , or effects of t h e r a p e u t i c m a n e u v e r s . Howeve r , e x a m i n a t i o n of ou r d a t a a f t e r r e m o v i n g pa- t i e n t s w i t h h i s t o r y of s p l e n e c t o m y or p o r t a c a v a l a n a s t o - mos i s d id n o t r e m o v e t he a s s o c i a t i o n b e t w e e n PV dis- ease a n d b l e e d i n g var ices . A role for s c l e r o t h e r a p y is m o r e di f f icul t to exc lude b e c a u s e few p a t i e n t s w i t h o u t s c l e r o t h e r a p y a re a v a i l a b l e to se rve as cont ro ls . M e s e n - te r ic t h r o m b o s i s h a s b e e n d i a g n o s e d s h o r t l y a f t e r s c l e r o t h e r a p y i n s eve ra l p a t i e n t s , b u t t h i s is a r a r e c o m p l i c a t i o n t h a t w a s c l in i ca l ly f o u n d on ly once in a se r ies of 799 s c l e r o t h e r a p y p rocedure s . 32
Acknowledgment: We t h a n k K. E k e m for exce l l en t t e c h n i c a l a s s i s t a n c e .
R E F E R E N C E S
1. Okuda K, Ohnishi K, Kimura K, Matsutani S, Sumida M, Goto N, Musha H, et al. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study of 708 patients. Gastroenterol- ogy 1985;89:279-286.
2. Boyer JL, Sen Gupta KP, Biswas SK, Pal NC, Basu Mallick KC, Iber FL, Basu AK. Idiopathic portal hypertension. Comparison with the portal hypertension of cirrhosis and extrahepatic portal vein obstruction. Ann Intern Med 1967;66:41-68.
3. Belli L, Sansalone CV, Aseni P, Romani F, Rondinara G. Portal thrombosis in cirrhosis. A retrospective analysis. Ann Surg 1986; 302:286-291.
4. Kage M, Arakawa M, Fukuda K, Kojiro M. Pathomorphologic study on the extrahepatic portal vein in idiopathic portal hyper- tension. Liver 1990; 10:209-216.
5. Gaiani S, Bolondi L, Bassi SL, Zironi G, Siringo S, Barbara L. Prevalence of spontaneous hepatofugal portal flow in liver cirrhosis. Clinical and endoscopic correlation in 228 patients. Gastroenterology 1991; 100:160-167.
6. Hou PC, McFadzean AJS. Thrombosis and intimal thickening in the portal system in cirrhosis of the liver. J Pathol Bact 1965;89:473-480.
7. Knockaert DC, Robaeys GK, Cox EJ, Marchal GJ. Suppurative pylethrombosis: a changing clinical picture. Gastroenterology 1989; 97:1028-1030.
8. Benhamou JP. Transient portal hypertension. In: Okuda K, Ben- hamou JP, eds. Portal hypertension. Clinical and physiological aspects. Tokyo: Springer-Verlag, 1991:363-364.
9. Viamonte M, Jr, Warren WD, Fomon JJ. Liver panangiography in the assessment of portal hypertension in liver cirrhosis. Radiol Clin North Am 1970;8:147-167.
10. Smith GW, Westgaard T, Bjorn-Hansen R. Hepatic venous angi- ography in the evaluation of cirrhosis of the liver. Ann Surg 1971; 173:469-480.
11. Miller F J, Jr, Maddrey WC, Sheff RN, Harrington DP, White RI, Jr. Hepatic venography and hemodynamics in patients with alcoholic hepatitis. Radiology 1975; 115:313-317.
12. Bookstein JJ, Appelman HD, Walter JF, Foley WD, Turcotte JG,
Lambert M. Histological-venographic correlates in portal hyper- tension. Radiology 1975; 116:565-573.
13. Takayasu K, Musha H, Nakazima Y, Okuda K. Clinical evalua- tion of hepatic vein catheterization--differential diagnosis of liver cirrhosis from other liver diseases based on venograms. Jpn J Gastroenterol 1978;75:1623-1633.
14. Futagawa S, Fukasawa M, Musha H, lsomatsu T, Koyama K, Ito T, Horisawa M, et al. Hepatic venography in noncirrhotic idiopathic portal hypertension. Radiology 1981; 141:303-309.
15. Goodman ZD, Ishak KG. Occlusive venous lesions in alcoholic liver disease: a study of 200 cases. Gastroenterology 1982; 83:786-796.
16. Nakanuma Y, Ohta G, Doishita K. Quantitation and serial sec- tion observations of focal veno-occlusive lesions of hepatic veins in liver cirrhosis. Virchows Arch A Pathol Anat Histopathol 1985;405:429-438.
17. Burt AD, MacSween RNM. Hepatic vein lesions in alcoholic liver disease: retrospective biopsy and necropsy study. J Clin Pathol 1986; 39:63-67.
18. Wanless IR, Liu JL, Butany J. Role of thrombosis in the patho- genesis of congestive hepatic fibrosis (cardiac cirrhosis) HEPA- TOLOGY 1995;21:1232-1237.
19. Sherlock S, Feldman CA, Moran B, Scheuer PJ. Partial nodular transformation of the liver with portal hypertension. Am J Med 1966;40:195-203.
20. Wanless IR, Lentz JS, Roberts EA. Partial nodular transforma- tion of liver in an adult with persistent ductus venosus. Arch Pathol Lab Med 1985; 109:427-432.
21. Wanless IR, Peterson P, Das A, Boitnott JK, Moore GW, Bernier V. Hepatic vascular disease and portal hypertension in polycy- themia vera and agnogenic myeloid metaplasia: a clinicopatho- logical study of 145 patients examined at autopsy. HEPATOLOGY 1990; 12:1166-1174.
22. Karsner HT. Morphology and pathogenesis of hepatic cirrhosis. Am J Clin Pathol 1943; 13:569-606.
23. Hales MR, Allan JS, Hall EM. Injection-corrosion studies of nor- mal and cirrhotic livers. Am J Pathol 1959;35:909-941.
24. Baggenstoss AH. Post-necrotic cirrhosis. Morphology, etiology, and pathogenesis. In: Popper H, Schaffner F, eds. Progress in liver diseases. Vol 1. New York: Grune &Stratton, 1961:14-38.
25. Edmondson HA. Pathology of alcoholism. Am J Clin Pathol 1980;74:725-742.
26. Harbin WP, Robert NJ, Ferrucci JT, Jr. Diagnosis of cirrhosis based on regional changes in hepatic morphology. A radiological and pathological analysis. Radiology 1980; 135:273-283.
27. Naschitz JE, Enat R, Yeshurun D, Eisenberg D, Baruch Y, Bas- san L, Misselevitch I, et al. Massive subcapsular fibrosis of the liver: ultrasonic and computed tomographic characteristics. J Clin Gastroenterol 1991; 13:470-474.
28. Ohtomo K, Baron RL, Dodd GD, Federle MP, Miller WJ, Camp- bell WL, Confer SR, et al. Confluent hepatic fibrosis in advanced cirrhosis: appearance at CT. Radiology 1993; 188:31-35.
29. Rubin E, Krus S, Popper H. Pathogenesis ofpostnecrotic cirrho- sis in alcoholics. Arch Pathol Lab Med 1962;73:288-299.
30. Lehmann H, Kaiserling E, Schlaak M. Left hepatic lobe atrophy and partial Budd-Chiari syndrome in a patient with alcoholic liver cirrhosis. Hepatogastroenterol 1982;29:3-5.
31. Kew MC, Varma RR, Dos Santos HA, Scheuer PJ, Sherlock S. Portal hypertension in primary biliary cirrhosis. Gut 1971; 12: 830-834.
32. Thatcher BS, Sivak MV, Ferguson DR, Petras RE. Mesenteric venous thrombosis as a possible complication of endoscopic sclerotherapy: a report of two cases. Am J Gastroenterol 1986;81:126-129.