
Global aphasia without hemiparesis: lesion analysis and its mechanism in 11 Korean patients
6
Global aphasia without hemiparesis: lesion analysis and its mechanism in 11 Korean patients Oh Young Bang a , Kwang Gi Heo a , Yong Tae Kwak b , Phil Hyu Lee a , In Soo Joo a , Kyoon Huh a, * a Department of Neurology, College of Medicine, Ajou University, Woncheon-dong San 5, Paldal-ku, Suwon, Kyungki-do 442-749, South Korea b Department of Neurology, Yong-in Hyoja Geriatric Hospital, South Korea Received 21 March 2003; received in revised form 4 September 2003; accepted 8 September 2003 Abstract Background: Global aphasia without hemiparesis (GAWH) is a rare stroke syndrome. This study localized the lesion and examined the pathogenic mechanism in Korean patients with GAWH, and investigated whether areas of extensive hypoperfusion existed outside the diffusion-weighted imaging (DWI) lesions seen in these patients. Material and methods: Eleven patients were diagnosed with aphasia using the Western Aphasia Battery. To identify decreased perfusion, which might be functionally relevant to aphasia but not detected by DWI, single photon emission tomography (SPECT) was performed in five patients. To uncover the possible pathogenic mechanisms of ischemic stroke, vascular and cardiologic work-ups were performed in all of the patients. Results: The lesions seen on DWI varied, and included both inferior frontal and superior temporal (three), isolated inferior frontal (four) or superior temporal (one), subcortical (two), and even parieto- occipital (one) lesions. Brain SPECT did not reveal an extensive lesion of the peri-sylvian area outside the DWI lesion in any of the patients, except one with the subcortical lesions. Conclusion: Our results indicate that a single lesion in different locations may be sufficient to produce GAWH, and the lesion profile and stroke mechanism in GAWH are heterogeneous, suggesting that lesions to an area of complex functional anatomy result in aphasia. D 2003 Elsevier B.V. All rights reserved. Keywords: Aphasia; Hemiparesis; Diffusion weighted imaging; Single photon emission; Tomogram 1. Introduction Global aphasia without hemiparesis (GAWH) is a rare and striking stroke syndrome, because of the unusual dissociation between language and motor function. Global language impairment typically occurs after large peri-syl- vian lesions with infarction of both the frontal and temporal branches of the left middle cerebral artery. Ordinarily, contralateral hemiparesis occurs together with global apha- sia, due to the proximity of the cortical language centers and motor control areas [1]. Hanlon et al. [2] recently reviewed the lesion profile and mechanisms of non-Asian cases of GAWH, including 10 patients of theirs, and suggested that a single lesion and non- cardioembolic origin cause GAWH. Vignolo et al. [3] found that only 59% of their patients with global aphasia with hemiparesis had large left peri-sylvian lesions involving both Broca’s and Wernicke’s areas, whereas 30% had either anterior or posterior lesions and 11% had deep lesions of the insula and lenticular nucleus. Diffusion-weighted imaging (DWI) is the most sensi- tive tool for detecting fresh ischemic lesions that cannot be detected using conventional magnetic resonance imag- ing (MRI), and it also provides information that differ- entiates recent infarcts from chronic infarcts that are not associated with clinical deficits like aphasia. In addition, single photon emission tomography (SPECT) can identify decreased flow that may be functionally relevant to neurological symptoms that cannot be detected using computed tomography (CT) or MRI. This is particularly crucial for acute aphasia, when a defect detected by CT and MRI cannot be reliably used to differentiate various aphasia types [4]. Moreover, SPECT can be used to identify the remote effects of vascular lesions [5]. There- fore, DWI and SPECT together may provide instructive clues for understanding the lesion profile of GAWH and the functional anatomy of aphasia. 0022-510X/$ - see front matter D 2003 Elsevier B.V. All rights reserved. doi:10.1016/j.jns.2003.09.010 * Corresponding author. Tel.: +82-31-219-5175; fax: +82-31-219- 5178. E-mail address: [email protected] (K. Huh). www.elsevier.com/locate/jns Journal of the Neurological Sciences 217 (2004) 101 – 106
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Global aphasia without hemiparesis: lesion analysis and its mechanism in 11 Korean patients

www.elsevier.com/locate/jns
Journal of the Neurological Sciences 217 (2004) 101–106
Global aphasia without hemiparesis: lesion analysis and its
mechanism in 11 Korean patients
Oh Young Banga, Kwang Gi Heoa, Yong Tae Kwakb, Phil Hyu Leea, In Soo Jooa, Kyoon Huha,*
aDepartment of Neurology, College of Medicine, Ajou University, Woncheon-dong San 5, Paldal-ku, Suwon, Kyungki-do 442-749, South KoreabDepartment of Neurology, Yong-in Hyoja Geriatric Hospital, South Korea
Received 21 March 2003; received in revised form 4 September 2003; accepted 8 September 2003
Abstract
Background: Global aphasia without hemiparesis (GAWH) is a rare stroke syndrome. This study localized the lesion and examined the
pathogenic mechanism in Korean patients with GAWH, and investigated whether areas of extensive hypoperfusion existed outside the
diffusion-weighted imaging (DWI) lesions seen in these patients. Material and methods: Eleven patients were diagnosed with aphasia using
the Western Aphasia Battery. To identify decreased perfusion, which might be functionally relevant to aphasia but not detected by DWI,
single photon emission tomography (SPECT) was performed in five patients. To uncover the possible pathogenic mechanisms of ischemic
stroke, vascular and cardiologic work-ups were performed in all of the patients. Results: The lesions seen on DWI varied, and included both
inferior frontal and superior temporal (three), isolated inferior frontal (four) or superior temporal (one), subcortical (two), and even parieto-
occipital (one) lesions. Brain SPECT did not reveal an extensive lesion of the peri-sylvian area outside the DWI lesion in any of the patients,
except one with the subcortical lesions. Conclusion: Our results indicate that a single lesion in different locations may be sufficient to produce
GAWH, and the lesion profile and stroke mechanism in GAWH are heterogeneous, suggesting that lesions to an area of complex functional
anatomy result in aphasia.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Aphasia; Hemiparesis; Diffusion weighted imaging; Single photon emission; Tomogram
1. Introduction
Global aphasia without hemiparesis (GAWH) is a rare
and striking stroke syndrome, because of the unusual
dissociation between language and motor function. Global
language impairment typically occurs after large peri-syl-
vian lesions with infarction of both the frontal and temporal
branches of the left middle cerebral artery. Ordinarily,
contralateral hemiparesis occurs together with global apha-
sia, due to the proximity of the cortical language centers and
motor control areas [1].
Hanlon et al. [2] recently reviewed the lesion profile and
mechanisms of non-Asian cases of GAWH, including 10
patients of theirs, and suggested that a single lesion and non-
cardioembolic origin cause GAWH. Vignolo et al. [3] found
that only 59% of their patients with global aphasia with
0022-510X/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.jns.2003.09.010
* Corresponding author. Tel.: +82-31-219-5175; fax: +82-31-219-
5178.
E-mail address: [email protected] (K. Huh).
hemiparesis had large left peri-sylvian lesions involving
both Broca’s and Wernicke’s areas, whereas 30% had either
anterior or posterior lesions and 11% had deep lesions of the
insula and lenticular nucleus.
Diffusion-weighted imaging (DWI) is the most sensi-
tive tool for detecting fresh ischemic lesions that cannot
be detected using conventional magnetic resonance imag-
ing (MRI), and it also provides information that differ-
entiates recent infarcts from chronic infarcts that are not
associated with clinical deficits like aphasia. In addition,
single photon emission tomography (SPECT) can identify
decreased flow that may be functionally relevant to
neurological symptoms that cannot be detected using
computed tomography (CT) or MRI. This is particularly
crucial for acute aphasia, when a defect detected by CT
and MRI cannot be reliably used to differentiate various
aphasia types [4]. Moreover, SPECT can be used to
identify the remote effects of vascular lesions [5]. There-
fore, DWI and SPECT together may provide instructive
clues for understanding the lesion profile of GAWH and
the functional anatomy of aphasia.

Fig. 1. DWI and brain SPECT findings in each group of patients. Black and white images, schematic drawings of the DWI lesions. Color images, brain SPECT
findings. Red lines represent the anterior and posterior margin of precentral gyrus.
O. Young Bang et al. / Journal of the Neurological Sciences 217 (2004) 101–106102

O. Young Bang et al. / Journal of the Neurological Sciences 217 (2004) 101–106 103
Fewer than 30 patients with GAWH have been described
previously [2]. To the best of our knowledge, no studies of
GAWH using DWI and SPECT have been reported. Further-
more, the pathogenic mechanismsmay vary depending on the
localization of the lesions and with ethnic group. The objec-
tives of this study were to localize the lesions and determine
the pathogenic mechanisms in Korean patients with GAWH,
and to investigate whether extensive areas of hypoperfusion
outside the DWI lesions existed in these patients.
Table 1
Characteristics of patients
Case Sex/age Handedness Work up for mechanisms of stroke
Angiographic Cardiologic
Classical lesion group
1 M/60 Right Normal MRA A-Fib, normal TTE
and TEE
2 M/79 Right Normal MRA A-Fib, normal TTE
3 F/59 Left Normal on TFCA Normal TEE
Non-classical lesion group
(1) Single lesion group
4a F/64 Right Left EC ICA
stenosis on TFCA
Normal TTE
5 M/62 Right Normal MRA A-Fib, akinetic left
ventricle segment
on TTE
6b F/43 Right Bilateral IC ICA
occlusion on TFCA
Normal TEE
7 F/80 Right Normal on MRA Normal TTE
8 M/79 Right Normal MRA Normal TTE
(2) Extra-sylvian lesion group
9c F/62 Right Left EC ICA
occlusion on TFCA
Normal TTE
10c F/75 Right Left EC ICA
occlusion on MRA
Normal TTE
11 F/58 Right Proximal MCA
stenosis on TFCA
Trivial valvular hear
disease on TEE
IC: intracranial, EC: extracranial, ICA: internal carotid artery, MCA: middle
cerebral artery, A-Fib: atrial fibrillation, MRA: magnetic resonance
angiography, TFCA: transfemoral conventional angiography, TTE: trans-
thoracic echocardiogram, TEE: transesophageal echocardiogram.a Asymptomatic old infarcts on right hemisphere.b Probable Moyamoya disease.c Previous right hemiparesis, but no sequale.
2. Materials and methods
We studied 11 consecutive patients with GAWH (4 men
and 7 women; age, 43–80 years; all but one were right-
handed). The Medical Research Council (MRC) scale was
used to assess their motor strength: on this scale, ‘0’
indicates no movement, ‘1’ movement only if gravity is
removed, ‘2’ weakness against gravity, ‘3’ weakness against
slight resistance, ‘4’ weakness against stronger resistance,
and ‘5’ normal strength. Each patient was also assessed
using the National Institutes of Health Stroke Scale (NIHSS)
[6]. All the subjects had normal scores bilaterally for the
upper extremity, hand, and lower extremity motor items of
the MRC and NIHSS. None had facial weakness. The
Western Aphasia Battery (WAB) [7,8] established the apha-
sic subtype and severity of aphasia, including subscales for
fluency, comprehension, repetition, and naming, during the
acute (within 3 days after stroke onset) and postacute (4 and
8 weeks after stroke onset) stages.
To uncover the possible pathogenic mechanisms of is-
chemic stroke, all the patients were examined using MRI (1.5
T, Sigma, GE), electro- and echocardiography, and conven-
tional or magnetic resonance angiography. DWI was per-
formed in the axial plane (TR: 10,000 ms, TE: 104 ms, slice
thickness: 7 mm, and no gap) within 3 days after stroke onset
in all of the patients. An extensive work-up, including
coagulopathy studies, was performed in two patients youn-
ger than 60 years old (patients 3 and 6). Using the results of
the work-up, the etiological subtypes of ischemic stroke were
classified using the criteria of Adams et al. [9]. To define
whether there was an extensive lesion outside the DWI
lesion, a Tc-99 m HMPAO brain SPECT study was also
performed in selected patients (within 7 days after stroke
onset). The existence and extent of the area of hypoperfusion
were determined by visual inspection by a neuroradiologist
who did not know the clinical status of the subjects.
Based on the cerebral lesions on DWI, we divided these
patients into three groups: (a) lesions in both the left
superior temporal and inferior frontal gyrus (the classical
lesion group), (b) a lesion in either the left inferior frontal
gyrus or the left superior temporal gyrus (the single lesion
group), and (c) a subcortical or cortical lesion outside the
peri-sylvian area (the extra-sylvian lesion group).
The SPECT patterns and possible mechanisms of stroke
were compared among the groups.
3. Results
All of the patients had large acute infarcts; however, the
locations of the infarcts on DWI varied (Fig. 1): three
(patients 1–3) were classified in the classical lesion group,
five (patients 4–8) in the single lesion group, and three
(patients 9–11) in the extra-sylvian lesion group. The
precentral gyrus was spared in all of the patients (Fig. 1).
However, two patients with subcortical lesions (patients 9
and 10) showed possible involvement of the motor pathway
in the deep brain structure on DWI, and were characterized
by the presence of a previous history of involvement of the
motor pathway and improvement without any motor deficit.
A SPECT study was performed in five patients who did not
show concurrent involvement of both the left inferior frontal
and left superior temporal gyrus (three of the single lesion
group, and one each of the extra-sylvian and classical lesion
groups). However, brain SPECT did not reveal any exten-
sive lesions of the peri-sylvian area outside the DWI lesions
in any of the patients, except one (patient 10) with the
subcortical lesions (Fig. 1).
Table 1 lists the demographic data and results of the
etiologic evaluation. Of the 11 patients, only three met the
criteria for cardioembolic ischemic stroke, and large artery
O. Young Bang et al. / Journal of the Neurological Sciences 217 (2004) 101–106104
disease of the relevant vessels was more prevalent (five
patients) in our patients with GAWH. Moreover, the path-
ogenic mechanism of stroke differed with the location of the
lesion on DWI. Two of the three patients with infarcts in
both the left superior temporal and inferior frontal gyrus (the
classical lesion group) had a potential source of cardioemb-
olism, whereas all the patients in the extra-sylvian lesion
group had large arterial occlusive lesions: two patients with
subcortical lesions (patients 9 and 10) had occlusive lesions
of the extracranial internal carotid artery and one patient
with an occipito-parietal lesion (patient 11) had a proximal
middle cerebral arterial occlusive lesion. One patient (pa-
tient 3 in the classical lesion group), a left-handed woman,
had a right hemispheric lesion, but no clear etiology. For the
single lesion group, the mechanisms of ischemic stroke were
variable: extracranial internal carotid arterial stenosis, atrial
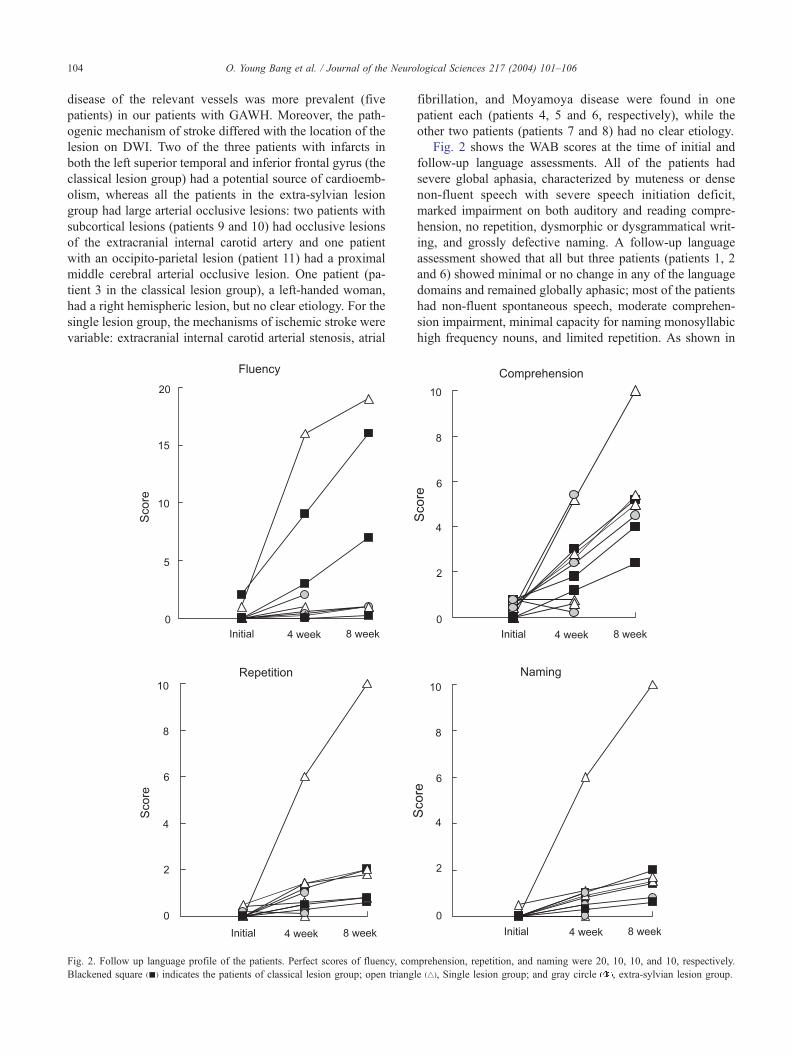
Fig. 2. Follow up language profile of the patients. Perfect scores of fluency, com
Blackened square (n) indicates the patients of classical lesion group; open triang
fibrillation, and Moyamoya disease were found in one
patient each (patients 4, 5 and 6, respectively), while the
other two patients (patients 7 and 8) had no clear etiology.
Fig. 2 shows the WAB scores at the time of initial and
follow-up language assessments. All of the patients had
severe global aphasia, characterized by muteness or dense
non-fluent speech with severe speech initiation deficit,
marked impairment on both auditory and reading compre-
hension, no repetition, dysmorphic or dysgrammatical writ-
ing, and grossly defective naming. A follow-up language
assessment showed that all but three patients (patients 1, 2
and 6) showed minimal or no change in any of the language
domains and remained globally aphasic; most of the patients
had non-fluent spontaneous speech, moderate comprehen-
sion impairment, minimal capacity for naming monosyllabic
high frequency nouns, and limited repetition. As shown in
prehension, repetition, and naming were 20, 10, 10, and 10, respectively.
le (4), Single lesion group; and gray circle , extra-sylvian lesion group.

O. Young Bang et al. / Journal of the Neurological Sciences 217 (2004) 101–106 105
Fig. 2, there was a tendency to show more improvement in
comprehension and, in some patients (patients 1, 2 and 6) in
fluency, than in repetition or naming.
4. Discussion
Earlier reports suggest that multiple lesions involving the
anterior and posterior language area, but sparing the motor
cortex, are necessary to cause GAWH, and that GAWH is
highly indicative of embolic etiology [10,11]. However,
various lesion locations and pathogenic mechanisms have
been described in non-Asian cases of GAWH. Some reports
indicate that GAWH is not pathognomonic of embolism,
and that GAWH is also heterogeneous with respect to the
lesion profile [2,12].
In this study, similar variation in lesion location was
observed; only 3 of the 11 patients with GAWH had typical
classical lesions, and GAWH occurred more commonly with
a single lesion in the peri-sylvian area (either the inferior
frontal gyrus or superior temporal gyrus) or even the extra-
sylvian area. These results are in good agreement with
previously reported cases with global language impairment,
in which a single cortical lesion or deep brain lesion plus an
extensive lesion could cause global aphasia, suggesting the
highly heterogeneous location of the lesion in GAWH [3].
Moreover, with the help of SPECT, we attempted to
document possible extensive perfusion defects in the peri-
sylvian area in the patients with a single lesion, but failed to
do so. Therefore, our SPECT results strongly suggest that a
single lesion in either the left inferior frontal or superior
temporal gyrus can cause global aphasia. One case with a
subcortical lesion showed an extensive perfusion defect
outside the DWI lesions on brain SPECT. Cortical hypo-
perfusion in the peri-sylvian areas has been reported to be
crucial for the development of subcortical global aphasia
[13].
Our data, together with other reported cases [2,14],
suggest that GAWH cannot be considered pathognomic
for embolic stroke. In our study, atherosclerotic lesions
affecting either intra- or extra-cranial arteries were more
common than cardioembolic sources, although this might
have been caused by the low prevalence of cardioembolic
stroke (10.9%) among the stroke patients seen during the
study period. In this study, atherosclerotic disease was
found exclusively in the patients in the non-classical
lesion group, whereas most of the patients with the
classical lesion pattern on DWI had cardioembolic sour-
ces, suggesting that the location of the lesion on DWI
differs with the pathogenic mechanism of stroke. Al-
though only a small number of patients were included
in our study, in Korean patients with GAWH, there is a
tendency to the non-classical lesion pattern (73%, 8 of 11
patients) and a reduced association with a cardioembolic
source (27%, 3 of 11 patients), as compared to non-Asian
GAWH (about half of the patients had the classical lesion
pattern and a cardioembolic source) [2,10–12,14]. Further
studies with more patients are needed.
As shown in Fig. 1, none of our patients had involvement
of the precentral motor cortex. The DWI finding of subcor-
tical lesions in patients with GAWH (patients 9 and 10) was
unexpected. Using three-dimensional data on the lesions,
von Keyserlingk et al. [15] reported that parts of the deep
white matter were spared in patients with global aphasia, but
no hemiparesis. We do not know why the patients with a
subcortical lesion in our study (patients 9 and 10) did not
manifest hemiparesis, despite the likely involvement of the
motor pathway seen on DWI. A common finding in these
two patients was that they were thought to have had
previous involvement of the motor pathway and recovered.
Brain SPECT (patient 10) showed global left hemispheric
hypoperfusion (Fig. 1). Neuroimaging studies in stroke
patients indicate altered poststroke activation patterns,
which suggest functional reorganization or ‘‘brain plastici-
ty’’ [16]. An issue of particular interest is the role of the
motor cortex ipsilateral to the affected hand when patients
move this hand. Evidence for ipsilateral involvement, in
addition to contralateral activation, has been reported in
positron emission tomography (PET) [17,18] and functional
MRI studies [19–21], but with a focus of activity in the
ipsilateral premotor cortex [18,19,22]. Although we did not
perform functional imaging to document functional reorga-
nization, ‘cortical plasticity’, i.e., right hemispheric control
of right limb motor functions, could have played a role in
the development of GAWH in our patients.
Varying degrees of improvement after GAWH have been
reported; the improvement can be either rapid [11,12] or
poor [2]. Our patients could not be characterized by exten-
sive recovery of language function uniformly. Although the
language profile and recovery are reported to depend on the
location of the lesion [2], we could not confirm this finding,
probably due to the short interval of the follow-up assess-
ment of language function.
Our study has some limitations. First, we examined only
a small number of patients because of the rarity of this
syndrome. Second, due to the high frequency of vascular
death, fatal recurrent stroke, or myocardial infarction, espe-
cially in patients with large-artery disease (five patients), we
could not conduct a long-term follow-up examination.
Third, a more extensive work-up to deduce the mechanism,
such as a transesophageal echocardiogram, was not per-
formed in all of the patients, because of poor cooperation.
Conventional angiography was not performed in patients
older than 75 years or in those with sources of cardioemb-
olism, and hemostatic markers of prothrombotic tendency,
including protein C, protein S, antithrombin III, and anti-
phospholipid antibodies, were checked only in those youn-
ger than 60 years old. Finally, the brain SPECT study was
performed only in selected patients.
In conclusion, our results indicate that although the
patients with acute GAWH all appeared similar on neurolog-
ical examination, the lesion profile and stroke mechanism in
O. Young Bang et al. / Journal of the Neurological Sciences 217 (2004) 101–106106
GAWH are heterogeneous. A single lesion, in either a cortical
or subcortical area, in the absence of an extensive perfusion
defect, may cause GAWH, suggesting the complex functional
anatomy of aphasia. The localization of the lesions may also
differ depending on the pathogenic mechanism.
References
[1] Damasio AR. Aphasia. N Engl J Med 1992;326:531–9.
[2] Hanlon RE, Lux WE, Dromerick AW. Global aphasia without hemi-
paresis: language profile and lesion distribution. J Neurol Neurosurg
Psychiatry 1999;66:365–9.
[3] Vignolo LA, Boccardi E, Caverni L. Unexpected CT-scan findings in
global aphasia. Cortex 1986;22:55–69.
[4] De Deyn PP, Dierckx RA, Alavi A, et al. A textbook of SPECT in
neurology and psychiatry. London: John Libbey & Company, 1997.
[5] Hillis AE, Wityk RJ, Barker PB, et al. Subcortical aphasia and neglect
in acute stroke: the role of cortical hypoperfusion. Brain 2002;125:
1094–104.
[6] Brott T, Adams HP, Olinger CP, et al. Measurement of acute cerebral
infarction. A clinical examination scale. Stroke 1989;20:864–70.
[7] Ferro J, Kertesz A. Comparative classification of aphasic disorders.
J Clin Exp Neuropsychol 1987;9:365–75.
[8] Kertesz A.Western aphasia battery. Orlando: Grune and Stratton, 1982.
[9] Adams HP, Bendixen BH, Kappelle J, et al. Classification of subtype
of acute ischemic stroke. Definitions for use in a multicenter clinical
trial. Stroke 1993;24:35–41.
[10] VanHorn G, Hawes A. Global aphasia without hemiparesis: a sign of
embolic encephalopathy. Neurology 1982;32:403–6.
[11] Tranel D, Biller J, Damasio H, et al. Global aphasia without hemi-
paresis. Arch Neurol 1987;44:304–8.
[12] Deleval J, Leonard A, Mavroudakis N, et al. Global aphasia without
hemiparesis following prerolandic infarction. Neurology 1989;39:
1532–5.
[13] Okuda B, Tanaka H, Tachibana H, Kawabata K, Sugita M. Cerebral
blood flow in subcortical global aphasia. Perisylvian cortical hypo-
perfusion as a crucial role. Stroke 1994;25:1495–9.
[14] Legatt AD, Rubin MJ, Kaplan LR, Healton EB, Brust JCM. Global
aphasia without hemiparesis: multiple etiology. Neurology 1987;37:
201–5.
[15] von Keyserlingk AG, Naujokat C, Niemann K, et al. Global apha-
sia—with and without Hemiparesis. A linguistic and CT scan study.
Eur Neurol 1997;38:259–67.
[16] Johansson BB. Brain plasticity and stroke rehabilitation. The Willis
lecture. Stroke 2000;31:223–30.
[17] Weiller C, Ramsay SC, Wise RJS, Friston KJ, Frackowiak RSJ. In-
dividual patterns of functional reorganization in the human cerebral
cortex after capsular infarction. Ann Neurol 1993;33:181–9.
[18] Seitz RJ, Knorr U, Azari NP, Herzog H, Freund HJ. Visual network
activation in recovery from sensorimotor stroke. Restor Neurol Neu-
rosci 1999;14:25–33.
[19] Cramer SC, Nelles G, Benson RR, Kaplan JD, Parker RA, Kwong
KK, et al. A functional MRI study of subjects recovered from hemi-
paretic stroke. Stroke 1997;28:2518–27.
[20] Cao Y, D’Olhaberriague L, Vikingstad EM, Levine SR, Welch KMA.
Pilot study of functional MRI to assess cerebral activation of motor
function after poststroke hemiparesis. Stroke 1998;29:112–22.
[21] Carey JR, Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey L, Rund-
quist P, et al. Analysis of fMRI and finger tracking training in subjects
with chronic stroke. Brain 2002;125:773–88.
[22] Nelles G, Spiekermann G, Jueptner M, Leonhardt G, Muller S, Ger-
hard H, et al. Evolution of functional reorganization in hemiplegic
stroke: a serial positron emission tomographic activation study. Ann
Neurol 1999;46:901–9.




















