Recent developments in functional and structural imaging of aphasia recovery after stroke

DISABILITY AND REHABILITATION, 1997; VOL. 19, NO. 6, 221-230
An evaluation of short-term group therapy for people with aphasia
SHELAGH M. BRUMFITT and PASCHAL SHEERAN
Accepted for publication: December 1996
Keywords group therapy, rehabilitation, aphasia.
Summary
This paper reports an evaluation of a group therapy intervention conducted with aphasic people (n = 6). The intervention comprised 10 sessions of approximately 90 min duration and included two participants with stuttering diffi- culties. The therapy programme consisted of communication activities within the group which encouraged sharing of personal experiences, videotaping of role-play activities for self- and group-evaluation and practice tasks completed ou1.side the group. Measures of functional communicative ability, attitudes to communication and psychological adjustment were obtained before and after the intervention. Findings showed significant improvements in communicative competence and attitudes to communication over the course of the intervention. Before the intervention self-esteem and communicative competence were highly intercorrelated. By the end of the therapy sessions the correlation between self-esteem and communicative com- petence was significantly smaller and was non-significant. This indicates that communicative function was not related to feelings of self-worth by the end of the intervention. Improve- ments in attitude to communication, greater attendance and completion of assignments were each predictive of reduced levels of depression. There was also evidence that stronger beliefs about the role of personal effort in improving speech were predictive of improvements in communication attitudes. A measure of satisfaction showed extremely positive evaluation of the intervention by participants. It is concluded that short- term group therapy can produce improvements in communi- cative abilities and attitudes, and have psychological benefits for participants. Several suggestions for future research are outlined.
Introduction
Clinical specialities of stuttering therapy and aphasia therapy both have a tradition of using group therapy. In general the type of therapy has had different aims, depending on the client group. Because of the need to
Authors: Shelagh M. Brumfitt (author for correspondence), Department of Speech Science, and Paschal Sheeran, Depart- ment of Psychology, University of Sheffield, 18/20 Claremont Crescent, Sheffield SIO ZTA, UK
acknowledge the interplay of fluency breakdown and psychological effects, stuttering therapy has frequently included psychological help in a group setting (e.g. refs 1 4 ) . Levy' reports a group approach with covert stutterers which focused on enabling the individual to identify personal therapeutic needs, desensitizing the stuttering behaviour and reconstruing of self as a more effective speaker. Similarly Sheehan's'. ' approach to therapy enables the individual to take responsibility for stuttering, and to learn that the reactions to the stutter are behaviours over which the individual can learn to exert control. Changing attitudes' and applying personal construct theorys to reconstruing self '*' are equally important parts of group work. As Stewart" points out, changes in attitude are inextricably linked to behaviour. Often these changes are helped by discussion activities but also tasks which encourage the speaker to take risks which might facilitate a new evaluation of self as a communicator (e.g. using the telephone after avoiding using it for many years). That is, where the individual conducts a new behavioural experiment and observes the positive outcomes of this action, then significant changes in attitude to communication can be achieved. Dalton," reviewing Fransella's work, discusses the importance of helping the stutterer to elaborate a new self, and using therapy to work towards the ideal self.
In contrast, therapy groups for aphasic people tend to focus on functional communicative tasks in which the reward for the speaker lies only in the achievement of the task. Although it may be implicit in aphasia therapy, evaluation of self is not strongly emphasized. Alterna- tively, groups may be organized to provide social support for both aphasic people and carers. Such support groups can have psychological benefits for those who attend. Rice et d.'* compared 'good' and 'poor' attenders at an evening support group on measures of psychosocial adjustment, and found that it was possible to distinguish between the two groups on tests of social dysfunction, somatic symptoms, anxiety and psychological well-being.
Wahrborg13 and Brurnfittl4 have reviewed the litera- ture on the use of psychotherapeutic groups for aphasic people. psychotherapy in this context focuses on enabling
0963-8288/07 $12.00 0 1997 Taylor & Francis Ltd
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

S. M . Brumfitt and P . Sheeran
the individual to come to terms with the enforced changes since the onset of the brain damage and aims to help the individual to respond more positively to rehabilitation. Much of the psychotherapeutic work with aphasic people was conducted in the US in the 1960s, and typically there was little formal evaluation of therapeutic outcomes. Lewis and Rosenberg” discuss the psychological effects of significant acquired brain damage (though not necessarily aphasic), and note problems with identity and low self-esteem. They point out that, in the past, research literature has concep- tualized negative feelings about self as an exclusively neurological symptom. They argue that self-esteem should be considered in terms of the personal impact of acquired brain damage upon the individual. Because low self-esteem and depression can result in poor motivation for rehabilitation, Lewis and Rosenberg argue that therapy should focus upon helping the patient express distress before attending to the preserved abilities. A psychotherapeutic group for aphasic people reported by Blackman16 is frequently cited. Here, the benefits of the group were described in terms of giving the aphasic person an opportunity to express hostility and anger in a safe context. The group was also described as enabling the individual to develop a ‘stronger sense of self’ (p. 156). No outcome measures are reported, but clearly the importance of sense of self was emphasized even in this early study. This emphasis has been underlined more recently by Brumfitt,” who argued that the theories individuals have about themselves may play an im- portant role in rehabilitation.
In terms of aetiology there is only the most tenuous link between aphasia and stuttering (1.e. the link is usually observed in acquired stuttering) and in practice many clinicians treat the two groups of patients as discrete types. The model of therapy is very different. The aphasic person is referred in a hospital setting, where therapy addresses the short-term, acute needs of orient- ing to what has happened, and remediating the language problem. The stuttering person may decide for himself or herself to come for help, and this decision may be induced by social pressure, such as coping with the speaking demands of a job. Aphasia therapy may have to focus on all aspects of linguistic functioning so that the person may need instruction in regaining reading skills as well as speaking ability. Moreover, the aphasic person has to adapt to rehabilitation at the same time as dealing with the memory of having had an intact communicative system. Frequently this is reported as a grief reaction.’* The therapy for the stutterer is more specific, dealing exclusively with the fluency dimension of speech and personal and social responses to this difficulty.
In the long term, however, both stuttering and aphasic patients have to cope in society with a chronic com- munication problem which other people may find incomprehensible. It is well recognized, in the field of fluency treatment, that work conducted in the clinical setting needs to be carried over into everyday life. This issue of ‘transfer and maintenance’ is implicit in a therapy plan.’g~20 This is by no means so well established in aphasia therapy, though Glozman and Tsyganok’l note that ‘the results obtained by a speech therapist in the course of individual activities often are not trans- ferred to the sphere of social contact beyond the classroom’ (p. 16). They report that aphasic people may develop negative emotional responses to speaking be- cause of the social discomfort they experience when attempting to speak outside a controlled clinical setting. Thus, there is some explicit acknowledgement of the significance of self-esteem and how it could affect responses to rehabilitation. The therapeutic significance of self-esteem has not, however, been fully explored.
In general, the acute needs of the aphasic person are such that establishing basic communicative ability is the foremost target. Yet it is clear that aphasic people may survive for many years without further illness. Psycho- social and emotional problems may be found many years after the original brain We would argue that the aphasic person’s well-being depends upon how well he/she is able to cope with communicative demand and pressure in much the same way as the long-term stutterer. Previous studies have not examined the potential of group therapy approaches used with stutterers for aphasic individuals.
The present study
The aim of the present study was to set up an intervention group for aphasic people which would have the same structure and aims as therapeutic groups for long-term stutterers. The particular aim of the group was to offer aphasic people an opportunity to experiment in communicative assignments which could improve (a) their communicative competence, (b) their attitude to communication and (c) their self-esteem and well-being. Because the present study was exploratory, and was designed to investigate whether participants’ scores would improve over the course of the intervention, a within-subjects design was employed. It is important to acknowledge that ours is not a formal experimental design, and that the lack of a control group limits the generalizations that can be drawn from the present study.
222
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

Group therapy for
The therapy programme
There were three main parts to the programme:
1. Communicative activities within the group which encouraged sharing of personal experiences
The theoretical rationale for this approach was that this would simultaneously address both linguistic and personal difficulties (cf. ref. 15). Such activities were also anticipated to have benefits in terms of encouraging identification with other group members and increasing cohesiveness within the group. The communicative activities were also intended to encourage self-evaluation based upon coniparison of the individuals’ ability and attitude with those of others. (‘social c~mparison’).’~ Two people with stuttering difficulties were included in the group for this reason, though results from these individuals are not reported here. The significance of comparisons with others is well established in psycho- logical research, and social comparisons have been shown to enhance people’s sense of competence, self- esteem and task performance in a variety of settings (see ref. 25, for review).
2. Videotaping of role-play activities for self- and group-evaluat ion
Theoretically, the opportunity to gain feedback about the individual’s own communicative performance would encourage self-evaluation and facilitate modification of communicative behaviours. Although it is commonly used in stuttering therapy as a means of increasing transfer and maintenance skills,26 this technique has been less available to the aphasic person. The way in which the individual interpreted experiences in the group was viewed as crucial. There is evidence that behaviour change is more successful if the individual can be helped to view new experiences in effective ways; that is, by not overlooking or discounting small successes.*’ Since communicative change is often very subtle, focusing attention on new, but small changes in behaviour was recognized as important.
3. Practice tasks to be completed outside the group as homework
This activity conforms to the transfer and maintenance approaches employed in stuttering therapy.*O Practice tasks focused on helping the person cope with a variety of communicative environments and on developing competence in communicative behaviours which in-
aphasic people
creased in complexity. Although, in stuttering therapy, transfer is used to develop a specific fluency technique, it was decided that the process of transfer could be usefully applied to the aphasic person who, during recovery or adjustment, was continually testing out his or her aphasic communicative behaviours.
Group therapy sessions were led by the same therapist (the first author) and were aimed to address both individual and group needs wherever possible. Although the group was largely task-oriented, concentrating especially on communicative function, attention was given to the group process and decisions about activities were made by the group as a whole. This conforms to Fawcus’s approach,’* which underlines the need to include both work on tasks as well as addressing the psychosocial needs among groups for communicatively disordered people.
The group met on one morning per week for 10 weeks and sessions lasted approximately 1; h. Sessions were held at the Philippa Cottam Communication Clinic, University of Sheffield, which had good facilities for group work, including several rooms with video and sound links to observation rooms. All three types of task were used in the group, and the complexity of the tasks increased over time. For example, in the initial stages a difficult task was identified during group discussions, and an assignment was organized around it (e.g. a specific shopping task). In the later stages group members were encouraged to work independently on tasks which they defined as challenging or difficult. For example, one subject made the decision to answer the telephone instead of waiting for her husband to do it.
HYPOTHESES
Four questions guided the present study.
The first question concerned the success of the intervention measured in terms of statistically identifiable changes over time. It was important to establish whether this therapeutic approach could demonstrate statistically significant changes in communicative competence, attitude to communi- cation, and psychological adjustment. The second question concerned the relationship between communicative competence and attitudes, and participants’ levels of self-esteem and well- being. The key issue here was whether individuals who demonstrate improvement in communicative competence also demonstrated improvements in psychological adjustment.
223
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

S. M . Brumfitt and P. Sheeran
(3) The third question concerned factors predictive of improvement and practice. Partridge and John- stonZ9 have shown that people with more internal beliefs about control over recovery (i.e. that the self has a key role in the recovery process) show improved outcomes during the course of therapy. Thus a greater belief in personal control over communicative competence might predict better outcome in the present context. Attendance and commitment to the group have also been shown to be significant factors in improvement" and were therefore also explored.
(4) Finally, the fourth question looked at the indi- vidual's perception of the group therapy and predictors of satisfaction. Clearly this has im- portant implications for the development of further groups for people with communicative problems.
Method
PARTICIPANTS AND PROCEDURE
Advertisements were placed in a newsletter for the national charity ADA (Action for Dysphasic Adults). Districts including Sheffield and surrounding areas were notified of the project. Since it was thought likely that a seriously impaired aphasic speaker would have con- siderable difficulty with the group setting, participants were selected following referral by a speech and language therapist. People with previous psychiatric history or a serious physical disability were excluded from the study.
Table 1 describes characteristics of the obtained sample. Three men and three women were recruited. Two of the men were classed as fluent aphasics (Clients 1 and 9, two women and one man were mixed aphasics (Clients 2, 3 and 6) and one woman was a non-fluent aphasic (Client 4). One person (Client 1) was being regularly monitored by a speech and language therapist, while the remainder were post-acute therapy. The auditory verbal comprehension subscale of the Western
Table 1 Sample characteristics
Aphasic Battery3' was used to determine participants' general level of auditory comprehension. Participants' comprehension scores were satisfactory, ranging from 140 to 198 (out of 200) with a mean of 163.8 (SD = 21.6). Participants were told that the purpose of the study was to enhance their existing skills and help them to manage more successfully in their everyday lives. Motivation to attend was high; this was indicated by the fact that four out of the six subjects travelled to the sessions from surrounding towns, financing themselves.
Ages ranged from 21 to 52 with a mean age of 42.3 years. Five of the six people had associated hemiplegia, but only two of the five needed support while walking. One person was in employment - the youngest in the group who had found work in an office in the company where he had worked pre-morbidly as an electrician. One man had taken early retirement prior to the cerebro- vascular accident. Two of the women had been house- wives, and the other two participants were unable to work because of their disability (both wanted to work). Five of the participants were in the first 3 years post- onset. The remaining woman had been aphasic for 12 years but was extremely keen to improve her abilities.
Measures were taken before the first meeting and, where appropriate, 10 weeks later, after the last meeting. Measures were administered by eight final-year post- graduate speech and language therapists (the same therapist did not work with the same participant at both time points).
EVALUATION MEASURES Measures of communication
Functional communication profile (FCP).31 The purpose of the functional communication profile is to gain as much information as possible about a person's residual language function in the simplest manner and to produce a quantifiable result. The profile consists of a list of 45 communicative behaviours which relate to everyday life. Assessment is divided into dimensions of speaking, understanding, reading, movement and other (e.g.
WAB auditory Marital Time since comprehension Age
Client Se.x bears) status onset Lesion Hemiplegia Employment score
I Male 52 Married I year 1 month Left No No 167 2 Female 48 Married 1 year 4 months Left Yes N o I40 3 Female 50 Married 1 year 2 months Left Yes No 162
5 Male 44 Married 3 years 2 months Left N o N o 198 6 Male 21 Single 2 years 5 months Left No Yes I42
Note. WAB = Western Aphasia Battery. Scores on the auditory comprehension subscale range from 0 to 200.
4 Female 39 Single 10 years Left Yes No 174
224
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

Group therapy for aphasic people
handling money). Each dimension includes a subset of tasks which the assessor rates ‘normal’, ‘good’, ‘fair’, ‘poor’ or ‘zero’. Detailed instructions are provided to determine the numerical value of each rating. Overall scores are expressed as a percentage, with higher scores indicating better communicative function. The FCP has been shown to have good test-retest reliability3’ and construct validity33 and was considered to offer the best basic profile which could be completed in the relatively short time available for testing.
Attitude to communication scale (S24).34 The S24 meas- ures people’s attitudes towards communication, and has been widely used with the stuttering population.:’’ The scale consists of statements such as: ‘I find it easy to talk with almost anyone’; ‘I am sometimes embarrassed by the way I talk’; and ‘ I find it very easy to look at my audience while speaking to a group’. A true/false response is required for each statement. Higher scores indicate more disordered attitudes towards communi- cation. The measure had face validity for aphasic people. To take account of the aphasic person’s potential difficulty with comprehension, each item was spoken aloud, face to face with the subject. Visual or written stimuli were used as aids to comprehension. None of the subjects had significant comprehension difficulties.
Stutterer’s self-ratings of reactions to speech situations scale.36 This scale consisted of 30 speaking situations which the individual is required to rate on two five-point scales. In the modified version employed here,:” the individual rates situations in terms of ‘Avoidance ’ and ‘Reaction’. For example, in the case of the item ‘ Introducing myself (face-to-face) ’ the individual rates how likely he/she would be to avoid this situation and how much he/she would enjoy speaking in this situation. On the Avoidance scale responses range from : ‘ I avoid this situation every time I possibly can’ (5) to ‘I never try to avoid this situation and have no desire to avoid i t ’ (1). On the Reaction scale responses range from: ‘I very much dislike speaking in this situation’ (5) to ‘I definitely enjoy speaking in this situation’ (1). Higher scores on the Avoidance scale indicate greater avoidance, while higher scores on the Reaction scale indicate more negative evaluations of speaking situations.
Measures of psychological adjustment
Rosenberg self-esteem scale (RSE).38 This Guttman scale is a unidimensional index of global self-esteem. It consists of 10 statements, five of which are phrased in a positive direction (e.g. ‘I feel that I’m a person of worth,
at least on an equal plane with others’), and five which are negatively phrased (e.g. ‘All in all, I am inclined to feel that I’m a failure’). The statements are rated on a four-point scale ranging from ‘strongly agree’ to ‘strongly disagree’. The reliability and validity of the RSE is well e~tablished.~’
Hospital anxiety and depression scale (HADS).40 This 14- item self-assessment scale is a reliable instrument for detecting anxiety and depression in adult^.^' It has also been shown to be a valid measure of these disorders of moods, and is commonly used as a screening instrument in general hospital practice.40 The scale includes seven anxiety items (e.g. ‘I feel tense or wound up’) and seven depression items (e.g. ‘I look forward with enjoyment to things ’). Four-point scales are used for response options (e.g. ‘not at all’, ‘occasionally’, ‘quite often’, ‘very often’).
Satisfaction measure
A seven-item scale was used to measure satisfaction with the intervention at the end of the last session. Respondents indicated their agreement/disagreement with statements on five-point scales (‘strongly agree’ to ‘strongly disagree’). The statements employed were ‘I feel the group has given me increased confidence’, ‘I felt able to participate in the activities in the group quite well’, ‘It was useful to see myself on video practising different sorts of conversations’, ‘ Meeting other people with similar problems was helpful to me’, ‘I found it helpful to talk in the group about situations I had been in during the week’, ‘I do not avoid as many situations as I used to, since coming to the group’, and ‘It was useful to be with people who had different communi- cation problems to me’.
Predictive measures
Statements of intent. Two statements were designed to measure intentions to attend the group and to practise tasks at home after every session (‘I am confident that coming here [to the group] would be ...’ and ‘I am confident that doing practice tasks at home every week would be...’). Five-point Likert scales were used for responses (‘extremely easy’ to ‘extremely difficult’).
Recovery locus of control scale (RLOC).” This is a nine- item scale which measures two factors: beliefs about the role of the self in the process of recovery (internal beliefs), and beliefs about the role of external factors in recovery (external beliefs). The scale has satisfactory reliability
225
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

S. M . Brumjitt and P. Sheeran
and has been shown to be predictive of behavioural outcomes in health setting^.^' Five items are used to measure internal beliefs (e.g. ‘ Improving my speech is a matter of my own determination rather than anything else’) and four items are used to measure external beliefs (‘My own contribution to my improvement in my speech doesn’t amount to much’). Four of the items on the scale were altered slightly: the term ‘recovery’ was changed to ‘improvement in my speech’ in order to make the scale relevant to this client group. Five-point Likert scales (‘strongly agree’ to ‘strongly disagree’) were used to measure responses. The RLOC was administered before the intervention only.
Practice tasks. Homework assignments were checked each week and the number of completed tasks was recorded for each participant. The sorts of tasks were based on difficulties identified by the group members, and included assignments such as going into a shop to purchase a newspaper or using the telephone.
Attendance. 10) was recorded.
The number of meetings attended (out of
Results
ATTENDANCE AND PRACTICE
The attendance for this group was very good, with all members attending at least 50 % of the sessions and one person attending all ten. The mean attendance rate was 8.5 sessions with a range of 5 to 10. The mean number of practice tasks completed was 6.8 (range 4 to 9).
COMPARISON OF PRE- AND POST-INTERVENTION
EVALUATION MEASURES
Table 2 presents the mean scores before and after the intervention for measures of communicative competence
Table 2 being. measures before and after the intervention
Mean scores for the communication, self-esteem and well-
Time1 Time2 t- Values p- Values
FCP 68.13 72.38 2.543 0.03 S24 13.83 10.17 1.309 0 1 2 Avoidance 71.83 67.17 1.144 0.15 Reaction 78.00 69.33 2.229 004 Self-esteem 30.33 27.17 1.256 0.13 Anxiety 6.67 5.50 0.1 I9 0.46 Depression 6.50 6.33 0.150 0.44
On all measures a reduction in the mean indicates improvement, with the exception of the Taylor Sarno communication profile and the Rosenberg self-esteem scale, in both of which higher scores indicate progress.
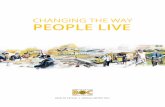
Depression s 0 1 2 3 4 5 6
Number of Participants
Figure 1 Number of participants showing improved post-intervention scores on measures of communicative competence, attitude to communication and psychological adjustment.
(FCP), attitude to communication (S24, Avoidance and Reaction) and self-esteem and well-being (RSE, HADS). Paired t-tests (one-tailed) were used to determine the significance of differences between scores at time1 and time2. A significant difference was found between the time1 and time2 scores for the Taylor Sarno Com- munication Profile ( t = 2.54, p = 0.03) and for the measure of Reactions to Speech Situations ( t = 2.23, p = 0.04). Thus, the primary purpose of the intervention was achieved : significant improvements in communicative behaviour following the group therapy sessions were obtained, and there were more positive evaluations of speaking situations at time2 than timel.
Although the direction of change was positive for all of the other measures (except self-esteem), no other statistically significant changes were found between mean scores at time1 and time2. One difficulty with comparison of mean scores, however, is that this procedure may mask the number of respondents showing improved scores. Figure 1 shows the number of participants whose communication and psychological adjustment scores improved over the course of the intervention. Improve- ments on all seven measures were observed for at least 50 YO of participants and on most measures 66-83 % (2-D of participants demonstrated improved scores.
RELATIONSHIPS BETWEEN COMMUNICATIVE COMPETENCE AND ATTITUDE TO COMMUNICATION AND PSYCHOLOGICAL
ADJUSTMENT
Our second aim was to investigate the relationship between changes in communicative competence, attitude
226
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

Group lherapy for aphasic people
to communication and psychological adjustment. In order to compute change scores for each variable, the difference between the time1 and time2 scores was calculated for each participant. Correlations were then conducted between the change scores computed for different variables.
Significant relationships were found between changes scores on the Taylor Sarno functional communication profile and changes in Reaction scores ( r = -0.955, p < 0.05) and, to a lesser extent, Avoidance scores ( r = -0.762, p < O.OS).t Improvements in communicative competence were therefore associated with less avoidance and more positive evaluations of speaking situations. This finding is consistent with Stewart’slO view that attitude to communication and communicative be- haviour are inextricably intertwined.
The relationship between communicative behaviour and self-esteem demonstrated an interesting temporal dynamic. At timel the Taylor Sarno functional com- munication profile and the Rosenberg self-esteem scale were significantly associated ( r = 0.736, p < 0.05). At time2, however, there was no longer a significant relationship between the two scales ( r = 0.422, p < 0.01). The difference between the two rs was statistically significant ( t = 3.43, p < 0.05). Thus, before group therapy, communicative behaviour was closely bound up with self-esteem for participants in the present study; however, by the end of the intervention communicative behaviour and level of self-esteem were independent of each other. This finding may suggest that a benefit which participants gained by the end of the intervention was a broadening of the basis of their self-esteem - self-esteem is no longer related to communicative behaviour at time2 but is, presumably, related to other factors instead.
PREDICTORS OF IMPROVEMENT IN COMMUNICATION AND PSYCHOLOGICAL ADJUSTMENT
Improvements in Depression scores were related to improvements in both Reaction ( r = 0 .738 ,~ < 0.05) and Avoidance scores ( r = 0.791, p < 0.01). Unfortunately, correlations between two change scores do not tell us which variable is causing change in the other. In order to determine whether changes in communicative behaviour were producing changes in depression, or whether changes in depression were producing changes in
~ ~~~~~~~
t It should be noted that increased scores on the FCP indicate improvement in communicative behaviour, while decreases in Avoidance and Reaction scores indicate an improvement in responses to comniunicative situations. Thus, the negative correlation obtained here indicates that improvements on the FCP are related to improvements in Avoidance and Reaction.
Table 3 Partial correlation coefficients between avoidance, reaction and depression scores
Controlling Predictor Criterion .for . . . r P
Avoidance Depression (time2)
Reaction Depression (timel)
Depression Avoidance (timel)
Depression Reaction (time 1)
Depression 0.89 0.02
Depression 0.76 0.07
Avoidance 0.73 0.08
Reaction 0.73 0.08
(timel)
(time 1)
(time 1)
(time 1)
communicative behaviour, partial correlation analyses were undertaken. Support for the causal effect of an independent variable would be obtained if the inde- pendent variable was significantly correlated with the time2 scores or the dependent variable after controlling for timel scores on the dependent variable (see, e.g. ref. 42).
Table 3 presents the results of the analysis. Overall, it appears that improvements in communicative behaviour are responsible for improvements in depression scores, rather than the other way round. A significant as- sociation was obtained between Avoidance change and depression at time2 controlling for depression at time1 (JI = 0.021). Changes in Reaction scores were also mar- ginally associated with Depression at time2 controlling for Depression at time1 (p = 0.07). The corresponding partial correlations between depression and communi- cative behaviour at time2 controlling for communicative behaviour at time1 were also marginally significant (JI = 0.08). However, these significance levels were less than those obtained for the analyses in which communicative behaviours were the independent variable. These findings do not rule out the possibility that changes in depression cause changes in communicative behaviour. They suggest only that the direction of influence is stronger from communicative behaviour to depression in the present study.
Internal locus of control over improvement predicted changes in both Avoidance behaviour ( r = 0.775, p < 0.05) and Reaction to communicative situations ( r = 0.764, p < 0.05). Participants who believed that their own efforts were the most important factor in improved speech were likely to show increases in positive evalu- ations, and less avoidance of speech situations. These findings suggest that the modified version of the recovery locus of control scale2’ employed here would be a valid measure for selecting participants who are most likely to demonstrate positive changes in attitudes to communi- cation, and could be used for this purpose in future group therapy studies.
227
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

S. M . Brumfitt and P . Sheeran
We also observed a number of significant predictors of changes in depression scores. Better attendance, and greater completion of homework tasks were both associated with improvements in depression scores ( r values = 0.858 and 0.770, respectively; p values < 0.05). Thus, simply attending group therapy and completing assigned work both had positive psychological benefits for participants.
Satisfaction with the intervention
Responses to the satisfaction measure indicated a very positive evaluation of the group therapy sessions. The mean response across the seven statements was 4.15 (out of 5 ) while the mean for individual questions ranged from 3.7 to 4.6. Answers to the satisfaction questions were above the scale-midpoints in all cases.
Positive changes in communicative behaviour and self- esteem were both correlated with greater endorsement of the item ‘The group has given me increased confidence’ ( r values = 0.731 and 0.758, respectively, p values < 0.05). Thus, changes in communicative competence and feelings of self-worth were reflected in reports of increased confidence at the end of intervention. Improve- ments in depression scores were also significantly associated with responses to the item ‘It was useful to be with people who had different communication problems to me’ ( r = 0.740, p < 0.05). This finding would seem to vindicate our including two participants with stuttering difficulties in the group therapy sessions.
Discussion
The main objective of the present study was to evaluate the effects of a group therapy intervention on functional communication behaviour, attitude to com- munication, self-esteem and well-being. We were able to demonstrate statistically significant changes in both functional communication scores and evaluations of communicative situations over the course of the in- tervention. Although statistically significant changes on other variables were not obtained, positive changes on all measures were observed for the majority of participants.
Very little research has been conducted which evalu- ates communication behaviour following inter~ention.‘~ The findings obtained here are encouraging : the aphasic sample employed made substantial changes to their communicative behaviour. Importantly, the major changes were found in the ‘speaking’ section of the FCP. It can be argued that the format of the group and the facilitation techniques employed here, encouraged group members to be more experimental in their speaking
attempts, which in turn led to positive changes. For example, one person moved from a rating of ‘poor’ for ‘saying greetings’ to a rating of ‘good’ over the course of the intervention. While there is some debate about how communicative behaviour should be assessed, and how measures of such behaviour differ from communicative assessments which examine language processing, Wor- ral143 notes that the rationale for the FCP has stood the test of time. We believe that results obtained here using the Taylor Sarno profile are reliable and valid. Future interventions might usefully include additional assess- ments of communication behaviour as well as this measure.
One of the most intriguing findings obtained here concerned changes in the relationship between com- municative behaviour and self-esteem over the course of the intervention. Before the intervention, self-esteem was strongly related to communicative behaviour. By the end of the group therapy sessions self-esteem and com- municative behaviour were no longer significantly re- lated. We must presume that, at the end of the intervention, self-esteem was related to factors other than communicative behaviour. For people with long- term aphasic difficulties this has important implications, since it suggests that a group therapy intervention may enable the individual to feel better, independently of whether changes in communication occur. This finding is also consistent with current aims of aphasia therapy, which include ‘facilitation of accommodation to changed communication skills ’.44
There were significant indications that this type of intervention may be useful in bringing about increased feelings of well-being. Those participants who attended regularly and those who practised regularly, were more likely to report reductions in depressive symptomatology over the 10 weeks. Changes in reaction to, and avoidance of, speaking situations and behaviours were also associ- ated with the improvements in depression scores. Partial correlation analyses appeared to support the view that changes in Avoidance and Reaction were responsible for reduced depression, rather than changes in depression producing changes in communicative attitudes among the present sample.
Participants in the present study were not clinically depressed people, however, nor was the intervention primarily focused on improving depression levels. The possibility of a causal role for improvements in de- pression, therefore, cannot be ruled out. This issue warrants future research. It should also be noted that, while depression is a well-established factor in psycho- logical studies of chronic conditions (e.g. ref. 45), psychological well-being is rarely mentioned or assessed
228
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

Group therapy for aphasic people
in speech and language therapy outcomes. The present study strongly suggests that future evaluation studies benefit from including assessments of this type.
Our findings suggest that internal locus of improve- ment could be an important discriminating criterion in setting up groups for aphasic people. This scale measures beliefs about the role of personal effort in bringing about improvement. Stronger beliefs in the self as the locus of improvement were found to be related to improvements in both avoidance behaviours and reactions to com- municative situations. Thus, those people who had a strong belief in their own effectiveness would respond better to this type of intervention.
It is important to note the good attendance rate for the group. Four of the group members travelled a substantial distance to meetings - something which can be viewed as a marker both of a high level of motivation to attend the sessions and of the high value placed on attendance. Findings from the satisfaction measure support this conclusion. Evaluations of the group therapy were extremely positive on all seven of the dimensions assessed. These findings provide strong support for the view that future interventions of this type would be likely to be seen as extremely valuable by aphasic individuals.
In evaluating the project as a whole it is important to point out that several significant findings were obtained here despite the small-scale and short-term nature of the intervention. In the first instance it is difficult to demonstrate statistically significant associations among such a small sample. Secondly, 10 weeks could have been too short a time period to demonstrate change with this type of client group, in terms of both communicative enhancement and psychological adjustment. Many people find it difficult to make wholly positive interpre- tations of their experiences during the course of therapy, and find they need greater time for the effects to become clear in their own minds. Discussing the work of Goldfried and Robins,” M a d d u ~ , ~ ~ for example, noted the tendency for clients to discount or ignore the importance of success experiences particularly if they were small and subtle. This study suggests, however, that it is possible for short-term group therapy conducted with a small group to demonstrate statistically significant improvements in areas of clinical importance.
Traditionally there has been little evaluation of outcome in group therapy for aphasic people, and this is partly owing to the methodological problems in assessing people who have significant communication deficits. Participants in the present study were sufficiently skilled communicators to be able to respond to the evaluation questionnaire. Whether the results obtained here can be extrapolated to the severely impaired aphasic population
requires further exploration. Our findings certainly warrant further research using other aphasic samples.
While the findings obtained here are certainly sugges- tive, it is important to acknowledge a significant limitation of the study; namely, the lack of a control group. While we have been able to demonstrate changes from pre- to post-test among the present sample, because we have not employed a formal experimental design we cannot conclusively state that these changes resulted from our short-term group therapy intervention. It is possible that a control group who did not receive our intervention could have demonstrated equivalent improvements over the same time period. What we can conclude, however, is that the present intervention is capable of demonstrating changes in communicative ability and attitudes towards communication. Further research should be directed towards a randomized controlled trial which includes both experimental and control groups. Such a trial should also track participants’ progress over a longer period than the present study, in order to ensure that improvements in communicative ability, attitudes to- wards communication, and psychological adjustment are maintained over time.
In conclusion, there are some important points to make about traditional measurement approaches used in aphasia therapy. In general, improvements are measured exclusively in terms of the dimension of communicative ability. Although this encompasses a broad area, it does not entirely take account of the aphasic person’s intrapsychic and interpersonal experiences. Whatever their disability, people in group therapy experience feelings, have attitudes and interact with others. These psychological issues require greater acknowledgement and attention. While both communication skills training and psychosocial work is seen as appropriate in groups for aphasic people, these two strands of therapy have still not been integrated. We need more intervention research in this area which investigates the relationship between psychological adjustment and communicative behaviour, and greater examination of beliefs about the self as a factor in communicative improvements.
References
1 Fransella F. Stuttering: not a symptom but a way of life. British Journal of Communication Disorders 1970; 5 : 22-29.
2 Fransella F. Personal Change and Reconstruction. London: Aca- demic Press, 1972.
3 Evesham M. Teaching stutterers the skill of fluent speech. British Journal of Disorders of Communication 1983; 18: 31-39.
4 Hayhow R, Levy C. Working with stuttering. Bicester: Winslow Press, 1989.
5 Levy C. Interiorised stuttering: a group therapy approach. In: Levy C (ed.) Sturtering Therapy: Practical Approaches. London: Croom Helm, 1987: 85-101.
229
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.

S. M . Brumjitt and P . Sheeran
6 Sheehan JG. Current issues on stuttering and recovery. In: Gregory HH (ed.) Controversies about Stuttering Therapy. Baltimore: University Park Press, 1979: 175-209.
7 Sheehan JG. Theory and treatment of stuttering as an approach avoidance conflict. In: Shanes GH & Rubin H (eds) Stuttering Then and Now. Ohio: Merrill, 1986: 95-111.
8 Stewart T. The relationship of attitudes and intentions to behave to the acquisition of fluent speech behaviour by stammerers. British Journal of Disorders of Communication 17: 3-13.
9 Kelly G. The Psychology of Personal Constructs. New York: Norton, 1955.
10 Stewart T. Positive attitudes to fluency; a group therapy pro- gramme. In: Levy C (ed.) Stuttering Therapies; Practical Ap- proaches. London: Croom Helm, 1987: 85-92.
1 1 Dalton P. Counselling People with Communication Problems. London: Sage, 1994.
12 Rice B, Paul1 A, Muller D. An evaluation of a social support group for spouses and aphasic adults. Aphasiology 3 : 247-256.
13 Wahrborg P. Assessment and Management of Emotional and Psychosocial Reactions to Brain Damage and Aphasia. London : Whurr, 1995.
14 Brumfitt SM. Psychotherapy in aphasia. In: Code C & Muller D (eds) Treatment of Aphasia: From Theory to Practice. London: Whurr, 1995: 000-000.
15 Lewis L, Rosenberg SJ. Psychoanalytic psychotherapy with brain injured adult psychiatric patients. Journal of Nervous and Mental Disease 1990; 178: 69-77.
16 Blackman N. Group psychotherapy with aphasics. Journal of Nervous and Mental Disease 1950; 3 : 154163.
17 Brumfitt SM. Losing your sense of self: what aphasia can do. Aphasiology 1993; 7: 569-591.
18 Tanner D, Gerstenberger D. The grief response in neuropathologies of speech and language. Aphasiology 1988; 2: 79-84.
19 Florance CL, Shames GH. Stuttering treatment: issues in transfer and maintenance. Seminars in Speech, Language and Hearing 1980; 1: 375-388.
20 Ryan BP. Maintenance programs in progress. In Boberg E (ed.) Maintenance of Fluency. Amsterdam: Elsevier, 198 1 : 5671.
21 Glozman ZM, Tsyganok AA. Some aspects of personality change in aphasia. Soviet Neurology and Psychiatry 1983; 16: 15-26.
22 Thomsen IV. Late outcome of very severe blunt head trauma: a 10-1 5 year second follow up. Journal of Neurology, Neurosurgery and Psychiatry 1984; 47: 260-268.
23 Wahrborg P, Borenstein P. Progressive psychological deterioration in aphasic and non aphasic stroke patients. In: Wahrborg P (ed.) Assessment and Management of Emotional and Psychosocial Re- actions to Brain Damage and Aphasia. London: Whurr, 1988.
24 Festinger L. A theory of social comparison processes. Human Relations 1954; 7: 117-140.
25 Suls J, Wills TA. Social Comparisons: Contemporary Theory and Research. Hillsdale, NJ: Erlbaum, 1991.
26 Wells GB. Stuttering Treatment: A Comprehensive Clinical Guide. Princeton, NJ: Prentice Hall, 1987.
27 Goldfried MR, Robins C. On the facilitation of self-efficacy. Cognitive Therapy and Research 1982; 6 : 361-380.
28 Fawcus M. Group Encounters in Speech and Language. London: Whurr, 1991.
29 Partridge C, Johnson M. Perceived control over recovery from physical disability : measurement and prediction. British Journal of Clinical Psychology 1989; 28: 53-59.
30 Kertesz A. Western Aphasia Battery. London: Grune and Stratton, 1982.
31 Sarno MT. The Functional Communication Profile: Manual of Directions. Rehabilitation Monographs 1975; 42: 1-32.
32 Greenberg FR. Functional communication ability and responses to a structured langauge test in dysphasic adults. Paper presented at the American Congress of Physical Medicine and Rehabilitation, San Francisco, 1966.
33 Schhlanger B, Arnold B, Brotkinn R, Kilpatrick I, Miller R. Relationships between the communicative functioning of aphasics and performance on varied tasks. Paper presented at the Meeting of the American Speech and Hearing Association, Washington DC, 1966.
34 Andrews G, Cutler J. Stuttering therapy: the relation between changes in symptom level and attitudes. Journal of Speech and Hearing Disorders 1974; 39: 312-319.
35 Dalton P. (ed.) Approaches to the Treatment ofstuttering. London: Croom Helm, 1983.
36 Johnson W, Darley FL, Spriestersbach DC. Diagnostic Method.7 in Speech Pathology. New York: Harper & Row, 1963.
37 Hayhow R. The assessment of stuttering and the evaluation of treatment. In: Dalton P. (ed.) Approaches to the Treatment of Stuttering. London: Croom Helm, 1983: 1547.
38 Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press, 1965.
39 Blascovich J, Tomaka J. Measures of self-esteem. In: Robinson JP, Shaver PR & Wrightsman LS (eds) Measures of Personality and Social Psychological Attitudes. San Diego, CA : Academic Press,
40 Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica 1983; 67: 361-370.
41 Goldberg D. Identifying psychiatric illness among general medical patients. British Medical Journal 1985; 1: 161-162.
42 Gerrard M, Gibbons FX, Bushman B. The relationship between perceived vulnerability to HIV and precautionary sexual behavior. Psychological Bulletin 1996 (In press).
43 Worrall L. The functional communication perspective. In Code C & Muller D (eds) Treatment of aphasia; from theory to practice. London; Whurr; 1995.
44 Byng S. What is aphasia therapy? In Code C & Muller D (eds) Treatment of Aphasia: From Theory to Practice. London: Whurr, 1995.
45 Kent G. Impairment, disability and psychological well being. The Psychologist 1995; 412413.
46 Maddux JE. Self efficacy. In: Snyder CR & Forsyth DR (eds) Handbook of Social and Clinical Psychology. New York : Pergamon, 1991 : 57-77.
1991: 171-188.
230
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Car
olin
a on
01/
30/1
5Fo
r pe
rson
al u
se o
nly.
Copyright © 2022 FDOKUMEN