Giardiasis among different tribes of Orang Asli in Malaysia: Highlighting the presence of other...
10
Giardiasis among different tribes of Orang Asli in Malaysia: Highlighting the presence of other family members infected with Giardia intestinalis as a main risk factor Tengku Shahrul Anuar a , Hesham M. Al-Mekhlafi b , Mohamed Kamel Abdul Ghani c , Emelia Osman a , Azlin Mohd Yasin a , Anisah Nordin a , Siti Nor Azreen a , Fatmah Md Salleh a , Nuraffini Ghazali a , Mekadina Bernadus a , Norhayati Moktar a,⇑ a Department of Parasitology and Medical Entomology, Faculty of Medicine, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur, Malaysia b Department of Parasitology, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysia c Programme of Biomedical Sciences, School of Diagnostic and Applied Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur, Malaysia article info Article history: Received 14 May 2012 Received in revised form 6 July 2012 Accepted 9 July 2012 Available online 28 July 2012 Keywords: Giardiasis Giardia intestinalis Risk factors Orang Asli tribes Malaysia abstract The flagellate protozoan parasite, Giardia intestinalis, is widely distributed throughout the world with a high prevalence in developing countries in the tropics and subtropics, including Malaysia. Approximately 200 million people are infected with the parasite globally, with 500,000 new cases reported annually. This cross-sectional study was conducted among three tribes of Orang Asli communities in Selangor, Perak and Pahang states of Malaysia. The main objective was to determine the prevalence of and risk fac- tors for giardiasis. Stool samples were collected from 500 individuals aged between 2 and 74 years (males = 219, females = 281). The samples were examined with formalin–ether sedimentation and trichrome staining techniques. Socioeconomic data were collected through a pre-tested questionnaire. The overall prevalence of giardiasis was 20.0% with the highest prevalence in the Proto-Malays (33.3%) followed by Negritos (20.1%) and Senois (10.4%). The positive cases showed a decrease with increasing age and most of the positive cases were observed in individuals less than 24 years old. Males had signif- icantly higher prevalence than females (v 2 = 5.283, P = 0.022). Logistic regression analysis of the overall population studied and the Senoi tribe confirmed that being a child aged less than 15 years, being male, the consumption of raw vegetables and the presence of other family members infected with G. intestinalis were the main risk factors for giardiasis. The presence of other family members infected with G. intesti- nalis was the only risk factor highlighted in the Proto-Malay and Negrito tribes. Diarrhoea was signifi- cantly associated with giardiasis. However, the cause and effect relationship has yet to be determined. Thus, screening family members and treating the infected individuals are the main strategies that should be adopted by the public health authority in combating this infection in Orang Asli communities as well as health education regarding good personal and food hygiene practises. Ó 2012 Australian Society for Parasitology Inc. Published by Elsevier Ltd. All rights reserved. 1. Introduction Giardiasis is the most common intestinal protozoal infection worldwide and it occurs throughout the tropical and temperate re- gions. Prevalence varies between 2% and 5% in the developed coun- tries and up to 20% and 30% in the developing countries (Wilson, 1984; Farthing, 1994). In developed countries, giardiasis occurs sporadically and it is commonly described as a cause of diarrhoea among children in day-care centres (Polis et al., 1986) and travel- lers (Gray et al., 1994; Faustini et al., 2006). Giardiasis in developed countries is significantly associated with water; in some studies, Giardia intestinalis accounts for a high proportion (35.2% and 40.6%) of water-associated outbreaks of parasitic disease (Kourenti et al., 2007; Baldursson and Karanis, 2011). The distribution of giardiasis was found to be associated with geographic regions and a high incidence of giardiasis has been reported during the summer months (Addiss et al., 1992; Judy et al., 2001; Hoque et al., 2004). In developing countries, giardiasis is endemic and is usually considered a faecal–oral disease. Socio-demographic fac- tors such as poverty, poor personal hygiene and lack of proper san- itation have been identified as significant risk factors (Lai, 1992; Prado et al., 2003; Faustini et al., 2006; Naelah et al., 2011). In Malaysia, giardiasis is considered an endemic infection. The prevalence varies according to the population studied and the infection is predominantly seen in children, especially in the 0020-7519/$36.00 Ó 2012 Australian Society for Parasitology Inc. Published by Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ijpara.2012.07.003 ⇑ Corresponding author. Tel.: +60 3 9289 7312; fax: +60 3 2698 2640. E-mail addresses: [email protected], [email protected] (N. Moktar). International Journal for Parasitology 42 (2012) 871–880 Contents lists available at SciVerse ScienceDirect International Journal for Parasitology journal homepage: www.elsevier.com/locate/ijpara
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Giardiasis among different tribes of Orang Asli in Malaysia: Highlighting the presence of other...

International Journal for Parasitology 42 (2012) 871–880
Contents lists available at SciVerse ScienceDirect
International Journal for Parasitology
journal homepage: www.elsevier .com/locate / i jpara
Giardiasis among different tribes of Orang Asli in Malaysia: Highlightingthe presence of other family members infected with Giardia intestinalis as a mainrisk factor
Tengku Shahrul Anuar a, Hesham M. Al-Mekhlafi b, Mohamed Kamel Abdul Ghani c, Emelia Osman a,Azlin Mohd Yasin a, Anisah Nordin a, Siti Nor Azreen a, Fatmah Md Salleh a, Nuraffini Ghazali a,Mekadina Bernadus a, Norhayati Moktar a,⇑a Department of Parasitology and Medical Entomology, Faculty of Medicine, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur, Malaysiab Department of Parasitology, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysiac Programme of Biomedical Sciences, School of Diagnostic and Applied Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur, Malaysia
a r t i c l e i n f o
Article history:Received 14 May 2012Received in revised form 6 July 2012Accepted 9 July 2012Available online 28 July 2012
Keywords:GiardiasisGiardia intestinalisRisk factorsOrang Asli tribesMalaysia
0020-7519/$36.00 � 2012 Australian Society for Parahttp://dx.doi.org/10.1016/j.ijpara.2012.07.003
⇑ Corresponding author. Tel.: +60 3 9289 7312; faxE-mail addresses: [email protected], tsatab@
a b s t r a c t
The flagellate protozoan parasite, Giardia intestinalis, is widely distributed throughout the world with ahigh prevalence in developing countries in the tropics and subtropics, including Malaysia. Approximately200 million people are infected with the parasite globally, with 500,000 new cases reported annually.This cross-sectional study was conducted among three tribes of Orang Asli communities in Selangor,Perak and Pahang states of Malaysia. The main objective was to determine the prevalence of and risk fac-tors for giardiasis. Stool samples were collected from 500 individuals aged between 2 and 74 years(males = 219, females = 281). The samples were examined with formalin–ether sedimentation andtrichrome staining techniques. Socioeconomic data were collected through a pre-tested questionnaire.The overall prevalence of giardiasis was 20.0% with the highest prevalence in the Proto-Malays (33.3%)followed by Negritos (20.1%) and Senois (10.4%). The positive cases showed a decrease with increasingage and most of the positive cases were observed in individuals less than 24 years old. Males had signif-icantly higher prevalence than females (v2 = 5.283, P = 0.022). Logistic regression analysis of the overallpopulation studied and the Senoi tribe confirmed that being a child aged less than 15 years, being male,the consumption of raw vegetables and the presence of other family members infected with G. intestinaliswere the main risk factors for giardiasis. The presence of other family members infected with G. intesti-nalis was the only risk factor highlighted in the Proto-Malay and Negrito tribes. Diarrhoea was signifi-cantly associated with giardiasis. However, the cause and effect relationship has yet to be determined.Thus, screening family members and treating the infected individuals are the main strategies that shouldbe adopted by the public health authority in combating this infection in Orang Asli communities as wellas health education regarding good personal and food hygiene practises.
� 2012 Australian Society for Parasitology Inc. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Giardiasis is the most common intestinal protozoal infectionworldwide and it occurs throughout the tropical and temperate re-gions. Prevalence varies between 2% and 5% in the developed coun-tries and up to 20% and 30% in the developing countries (Wilson,1984; Farthing, 1994). In developed countries, giardiasis occurssporadically and it is commonly described as a cause of diarrhoeaamong children in day-care centres (Polis et al., 1986) and travel-lers (Gray et al., 1994; Faustini et al., 2006). Giardiasis in developedcountries is significantly associated with water; in some studies,
sitology Inc. Published by Elsevier
: +60 3 2698 2640.lycos.com (N. Moktar).
Giardia intestinalis accounts for a high proportion (35.2% and40.6%) of water-associated outbreaks of parasitic disease (Kourentiet al., 2007; Baldursson and Karanis, 2011). The distribution ofgiardiasis was found to be associated with geographic regionsand a high incidence of giardiasis has been reported during thesummer months (Addiss et al., 1992; Judy et al., 2001; Hoqueet al., 2004). In developing countries, giardiasis is endemic and isusually considered a faecal–oral disease. Socio-demographic fac-tors such as poverty, poor personal hygiene and lack of proper san-itation have been identified as significant risk factors (Lai, 1992;Prado et al., 2003; Faustini et al., 2006; Naelah et al., 2011).
In Malaysia, giardiasis is considered an endemic infection.The prevalence varies according to the population studied andthe infection is predominantly seen in children, especially in the
Ltd. All rights reserved.

872 T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880
underprivileged community (Norhayati et al., 1998; Al-Mekhlafiet al., 2005; Mohammed et al., 2008). In addition to socio-demo-graphic factors, a recent study in Malaysia identified drinking tapwater and consuming raw vegetables as risk factors for giardiasis(Mohammed et al., 2008). A significant association of giardiasiswith protein-energy malnutrition (wasting) has also been reportedin Malaysia (Al-Mekhlafi et al., 2005).
The present study was conducted to examine the epidemiologyand risk factors of giardiasis among different tribes of Orang Asli inMalaysia (Proto-Malay, Negrito and Senoi). We believe that this isthe first study to explore the epidemiology and risk factors of giar-diasis in three Orang Asli tribes in Malaysia. A clear understandingof the epidemiology and identifying the risk factors of giardiasis inthe different Orang Asli tribes may help in the implementation ofspecific control and preventive strategies of giardiasis in Orang Aslicommunities.
2. Materials and methods
2.1. Study area and study population
The present study was carried out from June to December 2011in three different states of Peninsular Malaysia without discrimi-nating age or gender. Specific villages within the locations of Jelebu(2� 550 N latitude, 102� 40 E longitude), Gerik (5� 260 N latitude,101� 70 E longitude) and Temerloh (3� 430 N latitude, 102� 220 E lon-gitude) in Malaysia were included in this study (Fig. 1).
Parit Gong village, Jelebu, Negeri Sembilan state is considered asub-urban area with a population of 496 inhabitants. Most of theresidents are primarily involved in farming and rubber tapping.There are also many individuals who are engaged in commercialand professional activities such as teaching and government ser-vice (Department of Orang Asli Development (JAKOA), 2011. Re-search and Development Division: Information Database, JelebuDistrict, Negeri Sembilan, Malaysia). The main sub-tribe residingin this area is the Temuan and they belong to the Proto-Malay tri-bal group.
RPS Air Banun area, Gerik, Perak state is considered a remotearea, located in a valley approximately 40 km from the town ofGerik. The occupations of the inhabitants include farmers, rubbertappers and some do odd jobs such as selling forest products.The area comprises five villages with 10–15 households in each(Department of Orang Asli Development (JAKOA), 2011. Researchand Development Division: Information Database, Gerik District,Perak, Malaysia). The main sub-tribe residing in this area is theJahai which belongs to the Negrito tribal group.
Pasu village, Temerloh, Pahang state is considered a sub-urbanarea which is within 10 km from the town of Kuala Krau. Out of625 residents, 65% are farmers and rubber tappers while theremainders are mostly government and private workers (Depart-ment of Orang Asli Development (JAKOA), 2011. Research andDevelopment Division: Information Database, Temerloh District,Pahang, Malaysia). The main sub-tribe residing in this area is theJahut and they belong to the Senoi tribal group.
2.2. Structured questionnaire
A structured questionnaire was developed in English and thentranslated to Bahasa Melayu (the national language for Malaysia).The questionnaire was pre-tested among Orang Asli individualswho were admitted to Gombak Hospital, Selangor state. Trainedresearch assistants interviewed participants in person, askingquestions on demographic data (i.e., age, gender and education le-vel), socioeconomic background (i.e., occupation, household in-come and educational status), behavioural risks (i.e., personal
hygiene such as hand washing and food consumption), environ-mental sanitation and living condition characteristics (i.e., typesof water supply, latrine system, sewage disposal system and pres-ence of domestic animals). Participants were also asked if they haddiarrhoea and symptoms of gastroenteritis (i.e., vomiting, nausea,abdominal pain, watery stools and blood or mucus stools). For chil-dren, the questionnaire was completed by interviewing their par-ents or the guardian who had given informed consent.
2.3. Faecal examination
Following the administration of the questionnaire, a widemouth screw-capped container pre-labelled with the individual’sname and code was distributed to each participant for the collec-tion of a faecal sample the next day. Their ability to recognise theirname was counter-checked. The participant was instructed toscoop a thumb sized faecal sample, using a provided scoop, intothe container. Then, the container was placed into a zip-lockedplastic bag. Parents and guardians were instructed to monitor theirchildren during the sample collection in order to ensure that theyplaced their faecal samples into the correct container. Approxi-mately 10 g of each faecal specimen was kept in a 15 mL centrifugetube containing 3 mL Polyvinyl Alcohol (PVA). The collected faecalsamples were processed and examined for the presence of G. intes-tinalis cysts and/or trophozoites by the formalin–ether sedimenta-tion and trichrome staining techniques and then examined byusing a microscope at magnifications of 400 and 1000� (Fleckand Moody, 1993). Specimens were reported to be positive if cystsand/or trophozoites were detected by any of the two techniques.All positive cases were treated with metronidazole prescribed bythe medical personnel from the Ministry of Health, Malaysia.
2.4. Statistical analyses
Data were entered in Microsoft Access and were cross-checkedby the technical staff in order to ensure that data were entered cor-rectly. Statistical analysis was performed using SPSS version 20(SPSS, Chicago, IL, USA). For descriptive analysis, rate (percentage)was used to describe the characteristics of the studied population,including the prevalence of G. intestinalis. A Chi-squares test (v2)was used to test the associations between the variables. In the uni-variate analysis, the dependent variable was prevalence of G. intes-tinalis, while the independent variables were demographic andsocioeconomic factors, behaviour risks, environmental sanitation,living condition characteristics and gastrointestinal symptoms.All variables that were significantly associated with the prevalenceof G. intestinalis in the univariate model were included in a logisticregression analysis to identify the risk factors for G. intestinalis. Foreach statistically significant factor, an Odds Ratio (OR) and 95%confidence interval (CI) were computed by the univariate and mul-tivariate logistic regression analyses. The level of statistical signif-icance was set as P < 0.05.
2.5. Ethical considerations
Prior to data collection, the study protocol (Reference Number:UKM 1.5.3.5/244/FF-165-2011) was reviewed and approved by theEthics Committee of Universiti Kebangsaan Malaysia Medical Cen-tre (UKMMC) and permission for field work was obtained from theDepartment of Orang Asli Development (JAKOA). Village meetingswere held and village authorities and villagers were handed de-tailed explanations of the aims, procedures, potential risks andbenefits of the study. During the meeting, they were also informedthat their identity and personal information would be kept strictlyconfidential, and they could withdraw from the study at any pointof time without citing reasons for doing so. If they agreed to

Fig. 1. Map showing the location of the villages in Peninsular Malaysia involved in the study (triangles).
T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880 873
participate, their consent was obtained in written form (signatureor thumbprint for those who were illiterate) or parents were ap-proached for consent on behalf of their children.
3. Results
3.1. Demographic characteristics
The general characteristics of the Orang Asli (Aborigine)communities who participated in this study are shown in Table1. Overall, 500 individuals aged from 2 to 74 years participated inthis study with a median age of 18 years (interquartile range
(IQR) 9–35); and consisted of 150 (30.0%) Proto-Malays, 139(28.0%) Negritos and 211 (42.0%) Senois. More than 40% of the par-ticipants were children aged less than 15 years and more than halfof the participants were females (56.2% females and 43.8% males).Overall, the studied population came from a low socioeconomicbackground with more than half having less than 6 years of formaleducation. A high percentage of household income of less thanRM500.00 was predominantly seen in the Negrito (82.7%) andSenoi (60.7%) tribes. Most (95.3%) houses in Proto-Malay villageshad piped water supplies and toilet facilities; conversely pipedwater supplies and safe sewage disposal facilities were lacking inthe villages of the Negrito and Senoi tribes.

Table 1General characteristics of the Orang Asli communities that participated in this study.
Characteristics/tribes Overall n (%) Proto-Malay n (%) Negrito n (%) Senoi n (%)
Age groups (years)<15 221 (44.2) 59 (39.3) 72 (51.8) 90 (42.7)15–24 73 (14.6) 17 (11.3) 22 (15.8) 34 (16.1)25–44 131 (26.2) 48 (32.0) 29 (20.9) 54 (25.6)45–74 75 (15.0) 26 (17.3) 16 (11.5) 33 (15.6)
GenderMale 219 (43.8) 66 (44.0) 66 (47.5) 87 (41.2)Female 281 (56.2) 84 (56.0) 73 (52.5) 124 (58.8)
Socioeconomic statusFather’s education (<6 years) 222 (74.0) 54 (66.7) 68 (77.3) 100 (76.3)Mother’s education (<6 years) 232 (56.2) 53 (65.4) 77 (87.5) 102 (77.9)Low monthly household income (<RM500) 260 (52.0) 17 (11.3) 115 (82.7) 128 (60.7)Working mothers 153 (51.0) 45 (55.6) 33 (37.5) 75 (57.3)Large family (P8 members) 171 (34.2) 32 (21.3) 63 (45.3) 76 (36.0)Supplied with piped water 357 (71.4) 143 (95.3) 76 (54.7) 138 (65.4)Presence of toilet at household) 308 (61.6) 143 (95.3) 48 (34.5) 117 (55.5)
Total 500 (100) 150 (100) 139 (100) 211 (100)
RM = Malaysian Ringgit (US$1 = RM3.17 at 16 July 2012).
Table 2Prevalence of giardiasis among different Orang Asli tribes according to age groups and gender.
Overall Proto-Malay Negrito Senoi
n positive n tested % positive n positive n tested % positive n positive n tested % positive n positive n tested % positive
Age groups (years)<15 59 221 26.7 23 59 39 22 72 30.6 14 90 15.615–24 20 73 27.4 10 17 58.8 4 22 18.2 6 34 17.625–44 16 131 12.2 13 48 27.1 1 29 3.4 2 54 3.745–74 5 75 6.7 4 26 15.4 1 16 6.2 0 33 0
GenderMale 54 219 24.7 24 66 36.4 16 66 24.2 14 87 16.1Female 46 281 16.4 26 84 31 12 73 16.4 8 124 6.5
Total 100 500 20 50 150 33.3 28 139 20.1 22 211 10.4
874 T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880
3.2. Prevalence of giardiasis
The prevalence and distribution of giardiasis is shown in Table2. It was evident that of 500 individuals studied, 20.0% were posi-tive for G. intestinalis infection; the Proto-Malays harboured moreG. intestinalis (33.3%) followed by Negritos (20.1%) and Senois(10.4%). Overall, the positive cases showed a decrease with increas-ing age and most of the positive cases were observed in individualsof less than 24 years old. Similar findings were observed in the Pro-to-Malay, Negrito and Senoi tribes. The overall prevalence of giar-diasis was significantly higher in males (v2 = 5.283, P = 0.022), withsimilar observations seen in all tribes.
3.3. Risk factors for G. intestinalis infection
Univariate analysis identified being aged less than 15 years,being male and being a consumer of raw vegetables and fresh fruitas the main risk factors for the overall population studied (Table 3).In Proto-Malays, drinking untreated water, bathing and washing inthe river, indiscriminate defecation, outdoor sewage disposal andeating raw vegetables were identified as risk factors for giardiasis(Table 4). In Negritos, being aged less than 15 years, drinking un-treated water, bathing and washing in the river, indiscriminatedefecation, working mothers and a household monthly income ofless than RM500 were the risk factors for G. intestinalis infection(Table 5). In Senois, being aged less than 15 years, being maleand eating raw vegetables were the risk factors for giardiasis (Table6). The presence of other family members infected with G. intesti-nalis was the only risk factor that contributed to all tribes studied
(Tables 3–6). Logistic regression analysis of the overall populationstudied again confirmed that being aged less than 15 years, beingmale, eating raw vegetables and the presence of other family mem-bers infected with G. intestinalis as the risk factors for giardiasis.Similar observations were identified in the Senoi tribe. However,the presence of other family members infected with G. intestinaliswas the only risk factor confirmed in the Proto-Malay and Negritotribes.
Table 7 highlights the association of diarrhoea and other gastro-enteritis symptoms with giardiasis. Diarrhoea was the significantsymptoms associated with giardiasis observed in all tribes, whilediarrhoea (v2 = 13.527, P < 0.001) and other gastroenteritis symp-toms (v2 = 18.638, P < 0.001) were significantly associated withgiardiasis in the overall population studied.
4. Discussion
The prevalence rate of giardiasis among the Orang Asli inMalaysia has remained relatively similar over the years and ourstudy confirmed that this infection is still a significant infectionin these communities. The overall prevalence rate of giardiasis inthis study was 20.0% and it was mostly in agreement with previousreports from Malaysia (Al-Mekhlafi et al., 2005; Mohammed et al.,2008). Recent studies in developing countries elsewhere have re-ported prevalence rates of 17.7% and 27.3% (Izabella de et al.,2011; Naelah et al., 2011). The positive cases showed a decreasewith increasing age and most of the positive cases were observedin individuals less than 24 years old. This observation was seen

Table 3Potential risk factors associated with Giardia intestinalis infection among the overall population studied (univariate analysis, n = 500).
Variables No. examined Infected (%) OR (95% CI) P-value
Age (years)<15 221 26.7 1.45 (1.13,1.86) 0.001a,b
P15 279 14.7 1
GenderMale 219 24.7 1.28 (1.02,1.60) 0.022a,b
Female 281 16.4 1
Drinking untreated waterYes 209 19.7 1No 291 20.2 1.02 (0.79,1.31) 0.892
Bathing and washing in the riverYes 143 25.2 1.15 (0.98,1.34) 0.067No 357 17.9 1
Not washing hands after playing with soil or gardeningYes 197 20.4 1.02 (0.85,1.22) 0.855No 303 19.7 1
No domestic petsYes 191 20.8 1.04 (0.86,1.25) 0.716No 309 19.5 1
Indiscriminate defecationYes 192 20.8 1.03 (0.87,1.23) 0.713No 308 19.5 1
Sewage disposalOutdoor 240 19.2 1Common drainage 260 20.8 1.05 (0.83,1.33) 0.654
Eating with handsYes 328 19.9 1No 172 20.2 1.01 (0.86,1.18) 0.924
Consuming raw vegetablesYes 238 25.6 1.45 (1.11,189) 0.002a,b
No 262 14.7 1
Eating fresh fruitsYes 395 22.9 1.98 (1.19,3.30) 0.005a
No 105 11.2 1
Father’s educationNon-educated (<6 years) 222 27.5 1.52 (0.91,2.55) 0.095Educated (>6 years) 78 17.9 1
Mother’s educationNon-educated (<6 years) 232 25.9 1.18 (0.71,1.96) 0.524Educated (>6 years) 68 22.1 1
Working mothersYes 153 28.8 1.25 (0.93,1.68) 0.125No 147 21.1 1
Household membersP8 171 19.9 1<8 329 20.1 1.01 (0.74,1.37) 0.962
Household monthly income6RM500 260 19.6 1>RM500 240 20.4 1.03 (0.83,1.27) 0.823
Other family members infected with giardiasisYes 136 51.5 2.78 (2.06,3.77) <0.001a,b
No 364 8.2 1
RM = Malaysian Ringgit (US$1 = RM3.17 at 16 July 2012).Reference group marked as Odds Ratio (OR) = 1.CI = Confidence interval.
a Significant association (P < 0.05).b Variables were confirmed by logistic regression as significant predictors of giardiasis.
T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880 875
in Proto-Malay, Negrito and Senoi tribes. This finding was consis-tent with the recently published report that included a study ofall age groups (Mohammed et al., 2008). The possible reasons forthis age-specific prevalence of giardiasis are probably related toan individual’s sanitary behaviours and their dependence on andcontact with older family members. The younger age groups ofchildren are more susceptible to infection as they may eat indis-criminately or in the current study, it most likely resulted from
close contact with other family members who were infected. Forchildren in older age groups, exposure to infection was mostlythrough the habit of playing with soil, not washing their hands be-fore eating, as well as high levels of direct transmission of thisinfection within the family from members who were carriers.The lack of effective immunity in children has also being postu-lated to explain this age-specific pattern. Following acute giardia-sis, the host immune response is triggered to overcome the
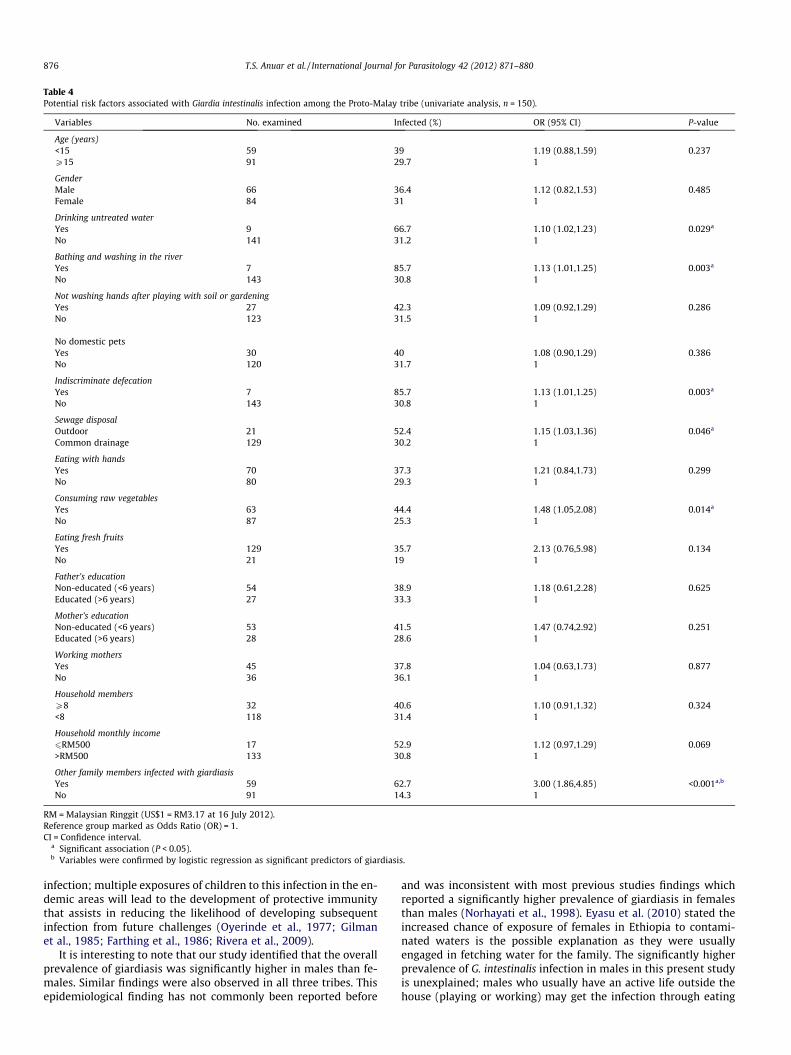
Table 4Potential risk factors associated with Giardia intestinalis infection among the Proto-Malay tribe (univariate analysis, n = 150).
Variables No. examined Infected (%) OR (95% CI) P-value
Age (years)<15 59 39 1.19 (0.88,1.59) 0.237P15 91 29.7 1
GenderMale 66 36.4 1.12 (0.82,1.53) 0.485Female 84 31 1
Drinking untreated waterYes 9 66.7 1.10 (1.02,1.23) 0.029a
No 141 31.2 1
Bathing and washing in the riverYes 7 85.7 1.13 (1.01,1.25) 0.003a
No 143 30.8 1
Not washing hands after playing with soil or gardeningYes 27 42.3 1.09 (0.92,1.29) 0.286No 123 31.5 1
No domestic petsYes 30 40 1.08 (0.90,1.29) 0.386No 120 31.7 1
Indiscriminate defecationYes 7 85.7 1.13 (1.01,1.25) 0.003a
No 143 30.8 1
Sewage disposalOutdoor 21 52.4 1.15 (1.03,1.36) 0.046a
Common drainage 129 30.2 1
Eating with handsYes 70 37.3 1.21 (0.84,1.73) 0.299No 80 29.3 1
Consuming raw vegetablesYes 63 44.4 1.48 (1.05,2.08) 0.014a
No 87 25.3 1
Eating fresh fruitsYes 129 35.7 2.13 (0.76,5.98) 0.134No 21 19 1
Father’s educationNon-educated (<6 years) 54 38.9 1.18 (0.61,2.28) 0.625Educated (>6 years) 27 33.3 1
Mother’s educationNon-educated (<6 years) 53 41.5 1.47 (0.74,2.92) 0.251Educated (>6 years) 28 28.6 1
Working mothersYes 45 37.8 1.04 (0.63,1.73) 0.877No 36 36.1 1
Household membersP8 32 40.6 1.10 (0.91,1.32) 0.324<8 118 31.4 1
Household monthly income6RM500 17 52.9 1.12 (0.97,1.29) 0.069>RM500 133 30.8 1
Other family members infected with giardiasisYes 59 62.7 3.00 (1.86,4.85) <0.001a,b
No 91 14.3 1
RM = Malaysian Ringgit (US$1 = RM3.17 at 16 July 2012).Reference group marked as Odds Ratio (OR) = 1.CI = Confidence interval.
a Significant association (P < 0.05).b Variables were confirmed by logistic regression as significant predictors of giardiasis.
876 T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880
infection; multiple exposures of children to this infection in the en-demic areas will lead to the development of protective immunitythat assists in reducing the likelihood of developing subsequentinfection from future challenges (Oyerinde et al., 1977; Gilmanet al., 1985; Farthing et al., 1986; Rivera et al., 2009).
It is interesting to note that our study identified that the overallprevalence of giardiasis was significantly higher in males than fe-males. Similar findings were also observed in all three tribes. Thisepidemiological finding has not commonly been reported before
and was inconsistent with most previous studies findings whichreported a significantly higher prevalence of giardiasis in femalesthan males (Norhayati et al., 1998). Eyasu et al. (2010) stated theincreased chance of exposure of females in Ethiopia to contami-nated waters is the possible explanation as they were usuallyengaged in fetching water for the family. The significantly higherprevalence of G. intestinalis infection in males in this present studyis unexplained; males who usually have an active life outside thehouse (playing or working) may get the infection through eating

Table 5Potential risk factors associated with Giardia intestinalis infection among the Negrito tribe (univariate analysis, n = 139).
Variables No. examined Infected (%) OR (95% CI) P-value
Age (years)<15 72 30.6 2.57 (1.24,5.32) 0.002a
P15 67 9 1
GenderMale 66 24.2 1.28 (0.81,2.03) 0.252Female 73 16.4 1
Drinking untreated waterYes 69 27.8 2.27 (1.09,4.73) 0.009a
No 70 10 1
Bathing and washing in the riverYes 63 31.7 2.14 (1.17,3.92) 0.002a
No 76 10.5 1
Not washing hands after playing with soil or gardeningYes 91 22 1.26 (0.67,2.38) 0.458No 48 16.7 1
No domestic petsYes 69 24.7 1.69 (0.86,3.33) 0.092No 70 13 1
Indiscriminate defecationYes 91 26.4 2.28 (1.09,7.07) 0.012a
No 48 8.3 1
Sewage disposalOutdoor 106 21.7 1.41 (0.60,3.33) 0.413Common drainage 33 15.2 1
Eating with handsYes 105 20.6 1.09 (0.50,2.40) 0.823No 34 18.8 1
Consuming raw vegetablesYes 113 20.2 1.01 (0.42,2.45) 0.984No 26 20 1
Eating fresh fruitsYes 122 20.5 1.18 (0.36,3.82) 0.784No 17 17.6 1
Father’s educationNon-educated (<6 years) 68 32.4 2.25 (0.72,7.01) 0.13Educated (>6 years) 20 15 1
Mother’s educationNon-educated (<6 years) 77 28.6 1.06 (0.31,3.67) 0.929Educated (>6 years) 11 27.3 1
Working mothersYes 33 42.4 1.59 (1.04,2.54) 0.024a
No 55 20 1
Household membersP8 63 20.6 1.03 (0.70,1.51) 0.895<8 76 19.7 1
Household monthly income6RM500 115 23.5 5.80 (1.09,6.31) 0.032a
>RM500 24 4.2 1
Other family members infected with giardiasisYes 46 47.8 3.66 (1.79,7.49) <0.001a,b
No 93 6.5 1
RM = Malaysian Ringgit (US$1 = RM3.17 at 16 July 2012).Reference group marked as Odds Ratio (OR) = 1.CI = Confidence interval.
a Significant association (P < 0.05).b Variables were confirmed by logistic regression as significant predictors of giardiasis.
T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880 877
and drinking contaminated food or water outside the house or itmay be associated with increased contact with farm and pet ani-mals and recreational water. A similar finding was observed byRivera et al. (2009).
To date there is only one cross-sectional community-basedstudy that was undertaken to determine the prevalence of giardi-asis among different tribes of Orang Asli (Dunn, 1972). The studywas carried out in all age groups of Orang Asli and the overall
prevalence of giardiasis was reported as 11.1%; 12.4% of Proto-Ma-lay (Temuan), 9.3% of Negrito and 5.7% of Senoi (Semelai) tribeswere infected with G. intestinalis, respectively. The overall preva-lence of giardiasis and prevalence according to the tribes fromthe study were very low compared with the present study. How-ever, the distribution of infection between different tribes is simi-lar; the highest prevalence was still observed in Proto-Malays(33.3%) followed by Negritos (20.1%) and Senois (10.4%). It is

Table 6Potential risk factors associated with Giardia intestinalis infection among the Senoi tribe (univariate analysis, n = 211).
Variables No. examined Infected (%) OR (95% CI) P-value
Age (years)<15 90 15.6 1.64 (1.06,2.89) 0.036a,b
P15 121 6.6 1
GenderMale 87 16.1 1.69 (1.09,2.97) 0.024a,b
Female 124 6.5 1
Drinking untreated waterYes 131 11.5 1.23 (0.65,2.33) 0.503No 80 8.6 1
Bathing and washing in the riverYes 73 13.7 1.22 (0.82,1.81) 0.258No 138 8.7 1
Not washing hands after playing with soil or gardeningYes 79 11.4 1.07 (0.74,1.53) 0.722No 132 9.8 1
No domestic petsYes 92 10.9 1.04 (0.70,1.55) 0.853No 119 10.1 1
Indiscriminate defecationYes 94 10.6 1.02 (0.68,1.52) 0.928No 117 10.3 1
Sewage disposalOutdoor 113 10.6 1.02 (0.63,1.66) 0.922Common drainage 98 10.2 1
Eating with handsYes 153 11 1.19 (0.53,2.66) 0.699No 58 8.9 1
Consuming raw vegetablesYes 62 16.9 1.43 (1.01,2.19) 0.039a,b
No 149 7.5 1
Eating fresh fruitsYes 144 12.1 1.33 (0.71,2.51) 0.343No 67 8 1
Father’s educationNon-educated (<6 years) 100 18 2.61 (0.68,10.09) 0.118Educated (>6 years) 31 6.5 1
Mother’s educationNon-educated (<6 years) 102 15.7 1.13 (0.44,2.89) 0.802Educated (>6 years) 29 13.8 1
Working mothersYes 75 17.3 1.26 (0.67,2.38) 0.447No 56 12.5 1
Household membersP8 76 10.5 1.01 (0.72,1.40) 0.972<8 135 10.4 1
Household monthly income6RM500 128 11.7 1.26 (0.67,2.39) 0.446>RM500 83 8.4 1
Other family members infected with giardiasisYes 31 35.5 1.79 (1.17,2.72) <0.001a,b
No 180 6.1 1
RM = Malaysian Ringgit (US$1 = RM3.17 at 16 July 2012).Reference group marked as Odds Ratio (OR) = 1.CI = Confidence interval.
a Significant association (P < 0.05).b Variables were confirmed by logistic regression as significant predictors of giardiasis.
878 T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880
interesting to note that in spite of better housing conditions andadequate provision of basic amenities, the Proto-Malays showeda higher prevalence of giardiasis compared with Negrito and Senoiwho experience poorer sanitary conditions. A study in Brazil re-ported that giardiasis and soil-transmitted helminthes (STH) canstill persist and continue to infect people who have good housingconditions and free access to public health care and education (Iza-bella de et al., 2011). In this study, six significant variables which
included drinking untreated water, bathing and washing in the riv-er, indiscriminate defecation, outdoor sewage disposal, eating rawvegetables and the presence of other family members infected withgiardiasis were observed as significant risk factors in the univariateanalysis for the Proto-Malay tribe. However, these variables lostthe strength of association with only the presence of other familymembers infected with giardiasis retained as a significant risk fac-tor in the logistic regression model. Considering these findings, it is

Table 7The association of diarrhoea and gastroenteritis symptoms with Giardia intestinalis infection among Proto-Malays, Negritos, Senois and the overall population studied.
Tribe/characteristics No. examined Infected (%) v2 P-value
Proto-MalayDiarrhoea 6.66 0.010a
Yes 14 64.3No 136 30.1
Other symptoms of gastroenteritis 3.01 0.083Yes 72 40.3No 78 26.9
NegritoDiarrhoea 4.76 0.029a
Yes 11 45.5No 128 18
Other symptoms of gastroenteritis 0.52 0.47Yes 19 26.3No 120 19.2
SenoiDiarrhoea 3.98 0.046a
Yes 22 22.7No 189 9
Other symptoms of gastroenteritis 3.54 0.06Yes 23 21.7No 188 9
Overall populationDiarrhoea 13.53 <0.001a
Yes 47 40.4No 453 17.9
Other symptoms of gastroenteritis 18.64 <0.001a
Yes 114 34.2No 386 15.8
a Significant association (P < 0.05).
T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880 879
logical to postulate that there was high transmission occurringwithin the family and infected family members served as a sourceof infection. The infection is probably transmitted directly throughhuman-to-human contact. However, accidental ingestion of cystsin drinking water or raw vegetables cannot be ruled out in thisenvironment where the carrier rates are high, and personal andfood hygiene levels are always compromised. Thus, screening andtreating family members, especially those aged less than 24 yearsis crucial as almost 66% of infected individuals are identified in thatage group.
Logistic regression analysis of the Senoi tribe identified childrenaged less than 15 years, being male, eating raw vegetables and thepresence of other family members infected with G. intestinalis asthe risk factors for giardiasis. The presence of other family mem-bers infected with G. intestinalis was the only risk factor identifiedin Proto-Malay and Negrito tribes. Individuals residing in the Pro-to-Malay, Negrito and Senoi villages with the presence of otherfamily members infected with G. intestinalis were at a 10.9-fold,12.18-fold and 13.24-fold higher risk of getting giardiasis, respec-tively. To the best of our knowledge, there is a paucity of studiesreported on the association of presence of other family membersinfected with G. intestinalis as a risk factor for giardiasis. Norhayatiet al. (1998) reported individuals with family members infectedwith G. intestinalis were 3.8 times more likely to be infected com-pared with individuals not at risk. A similar finding was also re-ported by Chute et al. (1987). In the Senoi tribe, the logisticregression model identified children less than 15 years old, malesand those consuming raw vegetables were at 9.65-fold, 6.05-foldand 7.50-fold higher risk of infection with giardiasis, respectively.Consuming raw vegetables was first reported in Malaysia as oneof the risk factor for giardiasis in the Orang Asli community byMohammed et al. (2008). Consuming these raw vegetables withcontaminated hands or without sufficient washing of the vegeta-bles was postulated as an explanation of the association. Besidesscreening and treating other family members infected with G.
intestinalis, health education on good personal and food hygienepractises are highly recommended for the prevention and controlof giardiasis in the Senoi tribe.
The present study showed a significant association betweengiardiasis and diarrhoea but not with other symptoms of gastroen-teritis such as vomiting, nausea and abdominal discomfort. Thisassociation was observed in all of the three tribes. Analysis of theoverall population studied indicated a strong association betweendiarrhoea and other symptoms of gastroenteritis with giardiasis.Similar observations have been reported previously (Mohammedet al., 2008). Lokman et al. (2007) reported that G. intestinalis wasthe most common parasite isolated in an acute diarrheal illnessoutbreak caused by rotavirus in the Orang Asli community. Thus,in the present study the cause and effect relationship was not pos-sible to determine due to the limitation of the cross-sectional de-sign used in this study. On the other hand, no attempt was madeto rule out other bacterial or viral causes of diarrhoea. Giardiasispresents with a wide spectrum of clinical expression and mostinfections are asymptomatic or with mild clinical features; diar-rhoea is the most frequent symptom seen in giardiasis. Acute giar-diasis is usually a self-limiting illness; prolonged diarrhoea withmalnutrition and growth failure in young children that is usuallyseen in chronic illness have been described before (Sackey et al.,2003; Al-Mekhlafi et al., 2005). A study by Al-Mekhlafi et al.(2005) reported giardiasis as a strong predictor of significant wast-ing in children of Orang Asli.
In conclusion, our findings highlight that giardiasis is still a pub-lic health problem in Orang Asli communities and a significantlyhigh prevalence rate of giardiasis is observed among the Proto-Ma-lay tribe. The presence of other family members infected with G.intestinalis is the significant risk factor identified in all tribes. In-fected family members served as the source of infection and directtransmission through human-to-human contact is postulated asthe main mode of transmission. Based on these findings, we sug-gest identifying and treating the carriers and infected individuals

880 T.S. Anuar et al. / International Journal for Parasitology 42 (2012) 871–880
within the family as the main strategy in the control and preven-tion of giardiasis in all Orang Asli tribes. In addition, health educa-tion pertinent to good personal and food hygiene practise mayhelp in reducing the prevalence of giardiasis in Orang Aslicommunities.
Acknowledgements
We gratefully acknowledge the Department of Orang AsliDevelopment (JAKOA), Ministry of Rural and Regional Develop-ment, Kuala Lumpur, Malaysia for granting us permission to con-duct this research. We also thank all of the participants fromParit Gong village, Pasu village and the RPS Air Banun area for theircommitment and contribution in providing their faecal samples.The work presented in this paper was funded by the UKMMCFundamental Research Grant (FF-165-2011), Special Research Uni-versity Grant (UKM-GUP-2011-316) and Geran Galakan PenyelidikMuda (GGPM-2011-080) from the Universiti Kebangsaan Malaysia.During this project, T.S.A. also received fellowship support from theMinistry of Higher Education, Malaysia and Graduate ResearchAssistantship scheme from the Universiti Kebangsaan Malaysia.
References
Addiss, D.G., Davis, J.P., Roberts, J.M., Mass, E.E., 1992. Epidemiology of giardiasis inWinconsin: increasing incidence of reported cases and unexplained seasonaltrends. Am. J. Trop. Med. Hyg. 47, 13–17.
Al-Mekhlafi, H., Azlin, M., Nor Aini, U., Shaik, A., Sa’iah, A., Fatmah, M.S., Ismail, M.G.,Ahmad Firdaus, M.S., Aisah, M.Y., Rozlida, A.R., Norhayati, M., 2005. Giardiasis asa predictor of childhood malnutrition in Orang Asli children in Malaysia. Trans.R. Soc. Trop. Med. Hyg. 99, 686–691.
Baldursson, S., Karanis, P., 2011. Waterborne transmission of protozoan parasites:Review of worldwide outbreaks – an update 2004–2010. Water Res. 45, 6603–6614.
Chute, C.G., Smith, R.P., Baron, J.A., 1987. Risk factors of endemic giardiasis. Am. J.Public Health 77, 585–587.
Dunn, F.L., 1972. Intestinal parasitisms in Malayan Aborigines (Orang Asli). Bull.World Health Organ. 46, 99–113.
Eyasu, T., Beyene, P., Tekola, E., 2010. Prevalence of giardiasis and cryptosporidiosisamong children in relation to water sources in selected villages of Pawi specialdistrict in Benishangul-Gumuz Region, Northwestern Ethiopia. Ethiop. J. HealthDev. 24, 205–213.
Farthing, M.J.G., Mata, L., Urrutia, J.J., Kromal, R.A., 1986. Natural history of Giardiainfection of infants and children in rural Guatemala and its impact on physicalgrowth. Am. J. Clin. Nutr. 43, 393–403.
Farthing, M.J.G., 1994. Giardiasis as a disease. In: Thompson, R.C.A., Reynoldson, J.A.,Lymbery, A.J. (Eds.), Giardia: From Molecules to Disease. CAB International,Wallingford, UK, pp. 15–37.
Faustini, A., Marinacci, C., Fabrizi, E., Marangi, M., Recchia, O., Pica, R., Giustini, F., LaMarca, A., Nacci, A., Panichi, G., Perucci, C.A., 2006. The impact of CatholicJubilee in 2000 on infectious diseases. A case–control study of giardiasis, Rome,Italy 2000–2001. Epidemiol. Infect. 134, 649–658.
Fleck, S.L., Moody, A.H., 1993. Diagnostic Technique in Medical Parasitology, 11thed. Cambridge U.P., Cambridge.
Gilman, R.H., Brown, K.H., Visvesvara, G.S., Modal, G., Greenberg, B., Sack, R.B.,Brandt, F., Khan, M.U., 1985. Epidemiology and serology of Giardia lamblia in adeveloping country: Bangladesh. Trans. R. Soc. Trop. Med. Hyg. 79, 469–473.
Gray, S.F., Gunnell, D.J., Peters, T.J., 1994. Risk factors for giardiasis: a case–controlstudy in Avon and Somerset. Epidemiol. Infect. 113, 95–102.
Hoque, M.E., Hope, V.T., Scragg, R., Michael, B., Rupendra, S., 2004. A descriptiveepidemiology of giardiasis in New Zealand and gaps in surveillance data. N. Z.Med. J. 117, 1–13.
Izabella de, O.P., Milton Ferreira de, C., Adalberto, M., Flavia, A.C.P., Clarice, A., Luiz,C.R., Sandra, H.C.T., Elaine, S.C., 2011. Prevalence and risk factors of giardiasisand soil-transmitted helminthiasis in three municipalities of SoutheasternMinas Gerais State, Brazil. Parasitol. Res. 108, 1123–1130.
Judy, D.G., Pascal, M., Jeff, B.W., Anna, M.L., Shammon, E.M., Julie, S., Jeffrey, J.A., Rob,K.M., Dean, M., Scott, A.M.E., 2001. A descriptive analysis of giardiasis casesreported in Ontario, 1990–1998. Can. J. Public Health 92, 361–365.
Kourenti, C., Karanis, P., Smith, H., 2007. Waterborne transmission of protozoanparasites: A worldwide review of outbreaks and lesson learnt. J. Water Health92, 361–365.
Lai, K.P.F., 1992. Intestinal protozoan infections in Malaysia. Southeast Asian J. Trop.Med. Public Health 23, 578–586.
Lokman, H.S., Gan, C.C., Malkit, K., Noor Azian, M.Y., Chong, C.K., Shaari, N.,Zainuddin, W., Chin, C.N., Sara, Y., Lye, M.S., 2007. Parasitic infections amongOrang Asli (Aborigine) in the Cameron Highlands, Malaysia. Southeast Asian J.Trop. Med. Public Health 38, 415–419.
Mohammed, A.K.M., Lim, Y.A.L., Surin, J., Wan, K.L., Al-Mekhlafi, H.M., 2008. Riskfactors for endemic giardiasis: highlighting the possible association ofcontaminated water and food. Trans. R. Soc. Trop. Med. Hyg. 102, 465–470.
Naelah, A.A., Mohammed, A.K.M., Rohela, M., Lim, Y.A.L., 2011. Factors associatedwith high prevalence of intestinal protozoan infections among patients inSana’a City, Yemen. PLoS One 6, e22044.
Norhayati, M., Penggaben, M., Oothuman, P., Fatmah, M.S., 1998. Prevalence andsome risk factors of Giardia duodenalis infection in a rural community inMalaysia. Southeast Asian J. Trop. Med. Public Health 29, 735–738.
Oyerinde, J.P.O., Ogunbi, O., Alonge, A.A., 1977. Age and sex distribution of infectionswith Entamoeba histolytica and Giardia intestinalis in the Lagos population. Int. J.Epidemiol. 6, 231–234.
Polis, M.A., Tuazon, C.U., Alling, D.W., Talmanis, E., 1986. Transmission of Giardialamblia from day care center to the community. Am. J. Public Health 76, 1142–1144.
Prado, M.S., Strina, A., Barreto, M.L., Oliveira-Assis, A.M., Paz, L.M., Cairncross, S.,2003. Risk factors for infection with Giardia duodenalis in pre-school children inthe city of Salvador. Brazil. Epidemiol. Infect. 131, 899–906.
Rivera, R.C., Leal, Y.A., Mulia, L.Y., Delgado, A.G., Pierrers, G.O., Conyer, R.T., Munoz,O., 2009. Seroepidemiology of giardiasis in Mexico. Am. J. Trop. Med. Hyg. 80, 6–10.
Sackey, M.E., Weigel, M.M., Armijos, R.X., 2003. Predictors and nutritionalconsequences of intestinal parasitic infections in rural Ecuadorian children. J.Trop. Pediatr. 49, 17–23.
Wilson, A., 1984. Mysterious Giardia. World Health Organization, Geneva.