
Polyamidoamine dendrimer impairs mitochondrial oxidation in brain tissue

GRK2 Activity Impairs Cardiac Glucose Uptake and PromotesInsulin Resistance Following Myocardial Ischemia
Michele Ciccarelli, MD, PhD1,2, J. Kurt Chuprun, PhD1, Giuseppe Rengo, MD, PhD1,3, ErheGao, MD, PhD1, Zhengyu Wei, PhD1, Raymond J. Peroutka, BS1, Jessica Gold, PhD1, AnnaGumpert, PhD1, Mai Chen, MD, PhD1, Nicholas J. Otis, BS1, Gerald W. Dorn II, MD4, BrunoTrimarco, MD2, Guido Iaccarino, MD, PhD5, and Walter J. Koch, PhD1
1 George Zallie and Family Laboratory for Cardiovascular Gene Therapy, Center for TranslationalMedicine, Thomas Jefferson University, Philadelphia, PA, USA2 Department of Clinical Medicine and Cardiovascular Science, “Federico II” University of Naples,Italy3 Division of Cardiology, Fondazione “Salvatore Maugeri” – IRCCS – Istituto di Telese Terme –Italy4 Center for Pharmacogenomics, Department of Internal Medicine, Washington University Schoolof Medicine, St. Louis, MO, USA5 University of Salerno, Department of Medicine, Salerno, Italy Ciccarelli, GRK2 and CardiacMetabolism
AbstractBackground—Alterations in cardiac energy metabolism downstream of neurohormonalstimulation play a crucial role in the pathogenesis of heart failure (HF). The chronic adrenergicstimulation that accompanies HF is a signaling abnormality that leads to the up-regulation of Gprotein-coupled receptor kinase 2 (GRK2), which is pathological in the myocyte during diseaseprogression in part due to uncoupling of the β-adrenergic receptor (βAR) system. In this study weexplored the possibility that enhanced GRK2 expression and activity, as seen during HF, cannegatively affect cardiac metabolism as part of its pathogenic profile.
Methods and Results—Positron Emission Tomography (PET) studies revealed that transgenicmice with cardiac-specific overexpression of GRK2 negatively impacted cardiac metabolism byinhibiting glucose uptake and desensitization of insulin signaling, which increases after ischemicinjury and precedes HF development. Mechanistically, GRK2 interacts with and directlyphosphorylates insulin receptor substrate-1 (IRS1) in cardiomyocytes causing insulin-dependentnegative signaling feedback including inhibition of membrane translocation of the glucosetransporter, GLUT4. This identifies IRS1 as a novel non-receptor target for GRK2 and representsa new pathological mechanism for this kinase in the failing heart. Importantly, inhibition of GRK2activity prevents post-ischemic defects in myocardial insulin signaling and improves cardiacmetabolism via normalized glucose uptake, which appears to participate in GRK2-targetedprevention of HF.
Corresponding Author: Walter J. Koch, PhD, FAHA, W.W. Smith Professor of Medicine and Director, Center for TranslationalMedicine, Thomas Jefferson University, 1025 Walnut Street, Room 317, Philadelphia, PA 19107, 215-955-9982, FAX: 215-503-5731,[email protected] codes: Chronic Ischemic Heart Disease; Animal Models of Human disease; Biochemistry and Metabolism.Disclosures.None.
NIH Public AccessAuthor ManuscriptCirculation. Author manuscript; available in PMC 2012 May 10.
Published in final edited form as:Circulation. 2011 May 10; 123(18): 1953–1962. doi:10.1161/CIRCULATIONAHA.110.988642.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Conclusions—Our data provide novel insight into how GRK2 is pathological in the injuredheart. Moreover, it appears to be a critical mechanistic link within neurohormonal crosstalkgoverning cardiac contractile signaling/function through βARs and metabolism through the insulinreceptor.
KeywordsCardiac Metabolism; Glucose; Heart Failure; Ischemic Heart Disease; Cardiac PET
IntroductionDespite improvements in the treatment of heart failure (HF) the prognosis of this diseaseremains poor 1, 2. The reason that HF continues to worsen even in patients receiving optimaltherapy is unclear, however, there is increasing evidence that perturbations in cardiacmetabolism can contribute to the progression of cardiomyopathy as well as to a loss ofpharmacologic effectiveness 3, 4. Therefore, approaches targeting more efficient substrateutilization and preservation of cardiac metabolism are attractive therapeutic strategies 5. Inthe adult heart the major pathway for ATP production is fatty acid oxidation 6, 7 while therelative contribution of glucose increases during stress or injury, such as during exercise orischemia 5. During HF there is excessive uptake and myocardial free fatty acid accumulationwith reduced glucose utilization 8, 9. In animal models of HF and also in human diseasethese metabolic alterations reduce myocardial oxygen efficiency and lead to a depletion ofintracellular ATP 10, 11.
Insulin receptor signaling is critically involved in increasing glucose uptake in themyocardium and cardiac insulin resistance contributes to the development of left ventriculardysfunction by reducing cardiac efficiency through metabolic shift towards fatty acidsutilization12. Indeed, a profound state of insulin resistance has been found in the hearts ofob/ob mice and the ability of these hearts to modulate substrate utilization in response toinsulin and changes in fatty acid supply is altered 13. Importantly, normalization of cardiacmetabolism by overexpressing a human GLUT4 transgene in mice with insulin resistancerecovered the altered cardiac function observed in these animals 14, 15. Therefore, thesestudies indicate that cardiac insulin resistance reduces the metabolic efficiency of the heart,which can lead to contractile dysfunction. Moreover, insulin resistance is a known andrecognized phenomenon leading to HF16, as seen in positron emission tomographic (PET)studies showing that failing human myocardium has reduced glucose uptake and increasedfree fatty acid uptake 17.
Several hypotheses have been proposed to explain the association between altered cardiacmetabolism, insulin resistance, and HF, and among these there is a strong correlation withneurohormonal activation 18, 19, which increases plasma free fatty acid levels and inhibitsinsulin receptor signaling resulting in a loss of myocyte glucose uptake 20. An importantabnormality in the myocyte induced by neurohormonal activation in HF is the up-regulationof G protein-coupled receptor (GPCR) kinase 2 (GRK2), which classically phosphorylatesactivated GPCRs, such as the β-adrenergic receptors (βARs) in the heart, leading toattenuated signaling 21. In human HF, increased GRK2 is associated with lower cardiacfunction and prognosis 22, 23.
Recent evidence suggests that GRK2 can have non-GPCR effects including playing anunidentified role in the regulation of insulin signaling in non-cardiac cells 24, 25. Moreover,increases in GRK2 activity following βAR stimulation inhibits insulin-dependent glucoseextraction 26. Therefore, we hypothesized that increased levels of GRK2, as seen during HF,directly induces myocardial insulin resistance and, given the importance of cardiac signaling
Ciccarelli et al. Page 2
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

for efficient metabolic substrate usage, we have studied the role of GRK2 in regulatingcardiac insulin signaling and metabolism in normal and post-ischemic myocytes and hearts.Our data reveal a role for GRK2 in HF pathogenesis that extends beyond the knownnegative effects on βAR signaling and cardiac contractility by demonstrating that GRK2 cancritically and negatively impact cardiac insulin signaling and metabolism.
MethodsExperimental Procedures
Experimental procedures were performed essentially as describedpreviously 27, 28. Anexpanded Methods section appears in the online-Data Supplement.
Statistical analyses—All experiments were performed at least in triplicate using cellisolates from different rats and the results were expressed as the mean±s.e.m. We used Prism4 and SPSS 17 to perform statistical analysis with two-tailed Student t-test for in-vitrostudies, and two way and repeated measure Anova with a Bonferroni post hoc test for the in-vivo studies. SPSS was used to evaluate the normal distribution according to the Levene testfor normality, and provide different p values for unpaired samples depending on normaldistribution. Even when the data is not normally distributed, we still found significantdifferences between means of different treatments and/or groups. A P< 0.05 was consideredstatistically significant.
RESULTSGRK2 levels influence in vivo cardiac glucose uptake
We first examined whether increased GRK2 in cardiomyocytes can alter in vivo glucoseuptake in the hearts of mice following insulin treatment. This is important since myocardialGRK2 up-regulation occurs acutely after ischemic injury 29 and may trigger furthersignaling defects. Therefore, we performed micro-PET using 18 -fluorodeoxyglucose (18-FDG) in transgenic mice with cardiac-specific GRK2 overexpression (Tg-GRK2 30) andtheir non-transgenic littermate controls (NLCs). An insulin injection produces a robustincrease in in vivo 18-FDG accumulation in the hearts of NLC mice, which is significantlylower in Tg-GRK2 mice (Fig. 1A). Mechanistically, GRK2 enhancement appears to cause aloss of insulin-dependent GLUT4 membrane translocation (Fig 1B).
GRK2 regulation of insulin signaling in cardiomyocytesDue to the above provocative in vivo results we explored molecular mechanisms involvingGRK2 and insulin signaling in cultured adult rat ventricular cardiomyocytes (ARVMs). Asexpected, when ARVMs were exposed to insulin, GLUT4 membrane translocation wasinduced as was the activation of the downstream kinase, Akt (Fig. 2A–C). Unexpectedly, wefound that insulin induced the membrane translocation of GRK2 (Fig 2A, D). The cause ofGRK2 membrane translocation after insulin administration is unclear but we next evaluatedwhether increased membrane GRK2 levels could alter downstream insulin receptorsignaling. To do this we pre-stimulated ARVMs with the βAR agonist isoproterenol (Iso) tocause Gβγ-dependent GRK2 translocation, which was evident in ARVMs (Fig. 2A, D).Interestingly, following Iso pre-treatment, insulin failed to induce GLUT4 translocation andthere was also significantly less insulin-dependent Akt activation (Fig. 2A–C).
To further explore how GRK2 levels may alter myocyte insulin signaling we overexpressedGRK2 in ARVMs using an adenovirus (ADGRK2). We found that increased GRK2 inARVMs attenuated insulin-stimulated Akt activation and GLUT4 membrane translocationcompared to control myocytes infected with ADGFP (Fig. 3A, B). Reduced GLUT4
Ciccarelli et al. Page 3
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

translocation is consistent with the above findings in Tg-GRK2 showing that enhancedGRK2 can lead to a loss of insulin-dependent in vivo cardiac glucose uptake. Indeed, wefound that insulin-dependent [H3]-deoxyglucose (2DOG) uptake in ARVMs wassignificantly attenuated by ADGRK2 (Fig. 3C).
GRK2 activity is required for attenuation of cardiomyocyte insulin signaling via directphosphorylation of IRS-1
Mechanistically, GRK2 could exert its inhibitory effect on insulin-dependent GLUT4translocation and cardiomyocyte glucose uptake and metabolism through differentpathways. GLUT4 membrane translocation has been shown to be dependent on Gαq/11signaling 25 and GRK2 has a known RGS domain within its amino-terminus that can interactdirectly with Gαq and inhibit its activity. Further, GRK2 has recently been shown to interactwith and inhibit Akt in endothelial cells 31. We conducted experiments to test these possiblemechanisms and found no evidence that GRK2 interacted with either of these proteins inARVMs, either basally or following stimulation of cells with insulin (data not shown).Therefore, we explored the possibility that GRK2 could regulate insulin signaling incardiomyocytes in other ways. Of note, kinase activity of GRK2 was necessary for thenegative regulation of insulin signaling, because the kinase-dead (K220R) GRK2 dominantnegative mutant (GRK2DN) failed to alter Akt activation (Fig. 4A) and GLUT4 membranetranslocation in response to insulin (Fig. 4B).
We next focused our attention to a potential regulatory role of GRK2 on insulin receptorsubstrate-1 (IRS1). This molecule moves to the plasma membrane following insulinstimulation and binds activated insulin receptors leading to Tyr phosphorylation andsubsequent activation of downstream signaling 21. IRS1 association with the insulin receptoralso initiates events that lead to the attenuation of insulin’s biological effects 32 throughphosphorylation of IRS1 at Ser307, which disrupts IRS1 binding to the insulin receptor andpromotes its proteasomal degradation 33. Of note, when IRS1 is phosphorylated at Ser307there is a reduction of Tyr612 phosphorylation and there appears to be a reciprocalrelationship between these two sites of post-translational modification 24, 33. A recent studyhas shown a physical interaction between GRK2 and IRS1 in adipocytes and muscle cellsunder basal conditions, which is disrupted by insulin treatment 34. However, ourexperiments in adult cardiac myocytes show that both GRK2 and IRS1 translocate to theplasma membrane. Moreover, they associate together and this interaction increases uponinsulin treatment of myocytes (Supplementary Figures 1A, B). Therefore, we pursued thehypothesis that increased GRK2 activity might enhance the feedback loop induced byinsulin via IRS1 inhibitory phophorylation. We observed that overexpression of GRK2 itselfsignificantly increased Ser307 phosphorylation of IRS1 under basal conditions and afterinsulin treatment compared to ADGFP infected cells (Fig 4C).
To address this potential specific role of GRK2 in myocyte insulin signaling, we studiedlevels of phospho-Ser307 IRS1 in isolated cells from NLC, Tg-GRK2 and cardiac-specificGRK2 knockout (KO) mice 27 after insulin administration. Fig. 4D shows that increasedcardiac GRK2 in Tg-GRK2 ARVMs results in increased basal and insulin-stimulated IRS1pSer307 levels while GRK2KO myocytes have attenuated insulin-stimulatedphosphorylation of IRS1 at Ser307 compared to NLC myocytes. Importantly, an in vitrokinase assay shows that purified GRK2 directly phosphorylates purified GST-IRS1 atSer307 (Fig. 4E). The physiological relevance of GRK2 phosphorylation of Ser307 ininsulin signaling regulation was explored by using an IRS1 in which Ser307 was mutated toalanine, which could not be phosphorylated by GRK2 (Supplementary Fig 1C).Overexpression of this mutated IRS1 by adenovirus (ADIRS1mt) in neonatal rat ventricularcardiomyocytes (NRVMs) removes the ADGRK2 inhibitory effects on insulin-mediated
Ciccarelli et al. Page 4
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

activation of Akt (Fig 4F) and GLUT4 translocation to the membrane (Supplementary Fig.1D).
Consistent with GRK2 activity inducing Ser307 phosphorylation of IRS1, an inhibitoryphosphorylation, we found that GRK2, but not the kinase-dead GRK2 mutant (K220R), alsoreduced the stimulatory-signaling Tyr612 phosphorylation in ARVMs (Supplementary Fig.1E).
Cardiac glucose uptake defects precede HF development after MI and both are augmentedwith GRK2 up-regulation
With our findings that increased GRK2 levels in myocytes negatively affects insulinsignaling, we next sought to determine if this translates to the pathogenesis of HF. Todetermine whether GRK2-mediated loss of glucose metabolism occurs in compromisedmyocardium, we used micro-PET to follow 18-FDG uptake after myocardial infarction(MI). Left coronary artery ligation induced a reproducible left ventricular (LV) infarct in Tg-GRK2, GRK2KO and NLC mice as previously described 27 (data not shown). All groupsshowed increased 18-FDG uptake 1 week after MI consistent with the heart increasing to themore protective glucose metabolism 5. However, the acute post-MI glucose uptake responsewas significantly reduced in Tg-GRK2 mice compared to NLC (Fig. 5A). Further, aprogressive reduction in glucose uptake after MI is observed in both NLC and Tg-GRK2mice, which accompanies progressive post-MI cardiac dysfunction and LV remodeling asmeasured by echocardiography (Fig. 5B). In cardiac GRK2KO mice, there was an initiallower glucose uptake response acutely after MI, however, in vivo glucose uptake remainedstable throughout the study period and this resulted in significantly higher uptake comparedto the NLC group at 6–8 weeks post MI (Fig. 5A). Interestingly, as in ARVMs (Fig. 3C),attenuated cardiac glucose uptake in vivo over time was significantly attenuated with GRK2overexpression and this worsened metabolic effect was most evident 1–3 weeks post-MI(Fig. 5A). This data shows that higher levels of myocardial GRK2 cause acute post-MIdefects in glucose metabolism that are evident before LV dysfunction appears andaccordingly, Tg-GRK2 mice have significantly worse cardiac function and remodelingchronically after MI while cardiac GRK2KO mice showed a preserved glucose utilization,resulting in preserved cardiac volume and function (Fig. 5B,C).
βARKct improves insulin signaling in adult cardiomyocytesOur data indicate that excess GRK2 produces serious modifications in cardiac glucoseuptake and insulin signaling in vivo and in vitro. Inhibition of GRK2 activity through thecarboxyl terminal domain of GRK2 (βARKct) has previously rescued several models ofHF21, 29. In light of the above data showing, in particular, the protective role of myocardialGRK2 loss on cardiac metabolism, we hypothesized that the beneficial effect of βARKct inrescuing cardiac function during HF could be due, at least in part, to a favorable effect oncardiac metabolism. Indeed, transgenic mice with cardiac βARKct expression (Tg-βARKct)have significantly lower inhibitory IRS1 Ser307 phosphorylation induced by insulin (Fig.6A), similar to data in cardiac-specific GRK2 KO mice (Fig 4D). Therefore, βARKct has thepotential to enhance insulin signaling and we tested this hypothesis by introducing βARKctin ARVMs via an adenovirus (ADβARKct). We found that βARKct expression restores andenhances Akt phosphorylation as well as a downstream target of Akt, GSK3β, whencompared to levels found in ADGRK2 and ADGFP treated myocytes, respectively (Fig6B,C).
Ciccarelli et al. Page 5
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

AAV6-βARKct gene therapy prevents GRK2-mediated defects in cardiac glucosemetabolism prior to the rescue of subsequent HF
Next, we asked whether inhibiting GRK2 could lift the negative effects of this kinase on invivo myocardial insulin signaling and measured myocardial glucose uptake and insulinresponses in post-MI rat hearts that expressed βARKct. To do this, we injected AAV6-GFPor AAV6-βARKct into the myocardium of rats during surgery to induce a MI as we havedone previously 28. Then, we serially measured in vivo glucose uptake in the heart viamicro-PET along with LV dimension and function via echocardiography and LVcatheterization. As expected, our method of cardiac gene transfer led to chronic and robustβARKct expression in the rat heart (Supplementary Fig. 2A). AAV6-βARKct deliverycompared to AAV6-GFP did not produce any significant differences in cardiac function andvolume in sham-treated rats (data not shown), therefore in our data presentation we onlyshow one sham control group.
MI induces progressive dilatation and LV dysfunction (Supplementary Fig 2C,D-Table 1)and consistent with human and animal models of HF, we found a progressive increase inmyocardial GRK2 levels after MI (Supplementary Fig 2B). Rats treated with AAV6-βARKct had significantly improved post-MI cardiac function and significantly lessremodeling throughout the 12 weeks of study (Supplementary Fig 2C,D and SupplementaryTable 1) with respect to the AAV6-GFP group. When we assessed in vivo glucose uptakepost-MI via micro-PET, we found that MI caused an acute defect in 18-FDG uptake incontrol AAV6-GFP treated rats and this metabolic abnormality was evident before anycardiac dysfunction or remodeling was found (Fig. 6D), a finding that was similar to theabove studies in mice (Fig. 5). Interestingly, AAV6-βARKct treated rats actually had normalmyocardial glucose uptake 3 weeks post-MI and this was significantly improved over post-MI GFP treated rats throughout the study (Fig 6D). To evaluate the potential in vivomechanism of the above PET results, we took a cohort of 3 week post-MI rats andchallenged them with insulin to measure GLUT4 membrane localization and found thissignificantly blunted in GFP-treated rats, however, AAV6-βARKct treated animals hadsignificantly improved insulin responsiveness (Fig. 6E).
DiscussionOur data adds significantly to the dynamic role of GRK2 in the pathogenesis of HF as ituncovers a new mechanism upon which up-regulated GRK2 in the injured myocardiumpromotes ventricular dysfunction. Importantly, enhanced GRK2 activity not only negativelyimpacts cardiac contractile function after myocardial injury but it is also causes abnormalcardiac metabolism. Further, GRK2 may represent a molecular link between the excessiveneurohormonal activation that follows cardiac stress and initiation of defects in myocyteenergy substrate utilization. Of note, our data reveals that GRK2 inhibition via βARKctexpression or its gene deletion in myocytes corrects metabolic alterations observed duringthe early stages of post-ischemic HF. This facilitates myocyte usage of glucose which is aprotective metabolic substrate, and delays the development of HF.
As observed in our micro-PET studies the modification in cardiac glucose uptake is an earlyevent after induction of MI. In particular, the initial increase is followed by a progressivereduction, which is then accompanied by a progressive cardiac dilation and reducedfunction. This behavior observed in NLC control mice is significantly modified in mice withaltered GRK2 levels in myocytes. Tg-GRK2 mice with enhanced GRK2 cardiac expressionsignificantly reduces protective myocyte glucose uptake while cardiac-targeted GRK2KOmice have preserved glucose uptake throughout the 8 weeks post-MI. Given the higherefficiency of glucose in ATP production and the lower impact in oxidative stress with
Ciccarelli et al. Page 6
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

respect to other substrates, we show that GRK2-mediated pathogenesis in HF is mediated atleast in part through negative alterations in cardiac metabolism.
Our findings once again highlight the deleterious effect of increased GRK2 levels thataccompany myocardial ischemia, and most importantly, confirm the importance ofidentifying strategies aimed specifically to reduce its activity in the heart as potential HFtherapy. Moreover, GRK2 inhibition with the βARKct, which has been demonstrated torescue or prevent animals models of HF and also improves contractile function of failinghuman ventricular myocytes 28, 35, has beneficial effects that extend beyond the functionalrecovery of βARs and contractility. Indeed, previous studies showed that GLUT4overespression improves cardiac function in mice with cardiac insulin resistance 14, 15 andhere we demonstrate that lowering GRK2 during HF improves glucose uptake and delaysthe development of the disease. We attribute at least part of the improvement to restoredinsulin-stimulated GLUT4 membrane translocation. GRK2 also represents the firstidentification of a molecule that represents a nodal link between excessive neurohormonalstimulation and metabolic abnormalities, supporting the hypothesis that strategies aimed topreserve myocardial metabolism could be beneficial in the treatment or prevention of HF.
Insulin signaling is known to be protective in the heart by inhibiting apoptosis and oxidativestress 36 and is also an important regulator of cardiac mass 37. These effects are primarilymediated by activation of PI3K-Akt and inhibition of GSK3β 38. Based on the results of thisstudy, injury-induced increases in GRK2 within the cardiomyocyte may increase oxidativestress, which expands our mechanistic understanding of why Tg-GRK2 mice progress morerapidly to HF. Therefore, GRK2 clearly has effects in the myocyte that extend beyondGPCR-mediated functions improving our mechanistic understanding of the pathologicalnature of GRK2 in the heart.
Of interest, recent studies have described a correlation between insulin resistance andincreased levels of GRK2 in pathological conditions. In particular, Garcia-Guerra et al. haverecently found that overexpression of either GRK2 or the kinase-dead mutant reduce insulinsensitivity in myoblasts and adipocytes, 34 and that finding was consistent with otherstudies25, 31 that suggested a kinase independent mechanism was involved, possibly bysequestering molecules involved in insulin signaling, such as Gαq/11, Akt, and IRS1.However, our data demonstrates for the first time that the catalytic activity of GRK2 isfundamental and a requirement in post-ischemic cardiac metabolic alterations - in particular,the dampening insulin signaling.
The finding that Ser307 of IRS1 is a target for GRK2 phosphorylation in cardiomyocytessignificantly increases the overall knowledge about regulation of insulin signaling inphysiology and pathology. Several serine residues within IRS1 are involved in thephysiological mechanism of IRS1 inhibition; however Ser307 has specific properties andcharacteristics that make it particularly interesting as a target of GRK2. This site is foundproximal to the IRS1 phospho-Tyr binding domain and Ser307 phosphorylation rapidlyreduces its affinity for binding to the insulin receptor 33, a process that resembles βARdesensitization. Thus, GRK2 appears to directly modulate signaling through this non-GPCRand participates in the physiological regulation of insulin signaling. Accordingly, GRK2inhibition reduces insulin-mediated Ser307 phosphorylation and improves signaling and as aresult can improve glucose uptake and insulin resistance in the injured cardiomyocyte.Indeed, elevated levels of phospho-Ser307 of IRS1 have been observed in animal models ofinsulin resistance and the equivalent Ser 312 site in human IRS1 has been demonstrated tobe hyperphosphorylated in insulin-resistant subjects 39, 40. Therefore, our findings canhypothetically be extended beyond the heart and suggests that βARKct gene therapy could
Ciccarelli et al. Page 7
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

be employed for the possible treatment of reduced skeletal muscle and liver glucose uptakeas is observed in type II Diabetes.
Overall, our data show that GRK2 inhibition clearly delays the reduction in glucose uptakeand protects insulin signaling in the heart, preserving cardiac dimension and function. Thesedata support the novel hypothesis that part of the therapeutic effect of GRK2 inhibition inHF includes correction of abnormal cardiac metabolism.
Supplementary MaterialRefer to Web version on PubMed Central for supplementary material.
AcknowledgmentsWe thank Dr. M. Thakur and K. Devadalas of the Jefferson PET core facility for conducting the PET imaging andanalysis of Micro-PET data. We also thank Filomena Severino and Dr Daniela Femminella for their technicalsupport and encouragement.
Funding Resources
This work was supported in part by US National Institutes of Health grants R01 HL085505, R37 HL61690 and P01HL075443 (Project 2) (to W.J.K.) and a fellowship from the Great Rivers Affiliate of the American HeartAssociation (to M.C.).
References1. Braunwald E. The Denolin lecture. Congestive heart failure: a half century perspective. Eur Heart J.
2001; 22:825–836. [PubMed: 11350092]2. Jessup M, Brozena S. Heart failure. N Engl J Med. 2003; 348:2007–2018. [PubMed: 12748317]3. Neubauer S. The failing heart--an engine out of fuel. N Engl J Med. 2007; 356:1140–1151.
[PubMed: 17360992]4. Ingwall JS, Weiss RG. Is the failing heart energy starved? On using chemical energy to support
cardiac function. Cir Res. 2004; 95:135–145.5. Ashrafian H, Frenneaux MP. Metabolic modulation in heart failure: the coming of age. Cardiovasc
Drugs Ther. 2007; 21:5–7. [PubMed: 17285357]6. Bing RJ, Siegel A, Ungar I, Gilbert M. Metabolism of the human heart. II. Studies on fat, ketone
and amino acid metabolism. Am J Med. 1954; 16:504–515. [PubMed: 13148192]7. Wisneski JA, Gertz EW, Neese RA, Mayr M. Myocardial metabolism of free fatty acids. Studies
with 14C-labeled substrates in humans. J Clin Invest. 1987; 79:359–366. [PubMed: 3805273]8. Lommi J, Kupari M, Yki-Jarvinen H. Free fatty acid kinetics and oxidation in congestive heart
failure. Am J Cardiol. 1998; 81:45–50. [PubMed: 9462605]9. Taylor M, Wallhaus TR, Degrado TR, Russell DC, Stanko P, Nickles RJ, Stone CK. An evaluation
of myocardial fatty acid and glucose uptake using PET with [18F]fluoro-6-thia-heptadecanoic acidand [18F]FDG in Patients with Congestive Heart Failure. J Nucl Med. 2001; 42:55–62. [PubMed:11197981]
10. Horn M, Remkes H, Stromer H, Dienesch C, Neubauer S. Chronic phosphocreatine depletion bythe creatine analogue beta-guanidinopropionate is associated with increased mortality and loss ofATP in rats after myocardial infarction. Circulation. 2001; 104:1844–1849. [PubMed: 11591624]
11. Neubauer S, Krahe T, Schindler R, Horn M, Hillenbrand H, Entzeroth C, Mader H, Kromer EP,Riegger GA, Lackner K. 31P magnetic resonance spectroscopy in dilated cardiomyopathy andcoronary artery disease. Altered cardiac high-energy phosphate metabolism in heart failure.Circulation. 1992; 86:1810–1818. [PubMed: 1451253]
12. Peterson LR, Waggoner AD, Schechtman KB, Meyer T, Gropler RJ, Barzilai B, Davila-RomanVG. Alterations in left ventricular structure and function in young healthy obese women:
Ciccarelli et al. Page 8
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

assessment by echocardiography and tissue Doppler imaging. J Am Coll Cardiol. 2004; 43:1399–1404. [PubMed: 15093874]
13. Mazumder PK, O’Neill BT, Roberts MW, Buchanan J, Yun UJ, Cooksey RC, Boudina S, AbelED. Impaired cardiac efficiency and increased fatty acid oxidation in insulin-resistant ob/ob mousehearts. Diabetes. 2004; 53:2366–2374. [PubMed: 15331547]
14. Belke DD, Larsen TS, Gibbs EM, Severson DL. Altered metabolism causes cardiac dysfunction inperfused hearts from diabetic (db/db) mice. Am J Physiol Endocrinol Metab. 2000; 279:E1104–1113. [PubMed: 11052966]
15. Semeniuk LM, Kryski AJ, Severson DL. Echocardiographic assessment of cardiac function indiabetic db/db and transgenic db/db-hGLUT4 mice. Am J Physiol Heart Circ Physiol. 2002;283:H976–982. [PubMed: 12181126]
16. Boudina S, Bugger H, Sena S, O’Neill BT, Zaha VG, Ilkun O, Wright JJ, Mazumder PK,Palfreyman E, Tidwell TJ, Theobald H, Khalimonchuk O, Wayment B, Sheng X, Rodnick KJ,Centini R, Chen D, Litwin SE, Weimer BE, Abel ED. Contribution of impaired myocardial insulinsignaling to mitochondrial dysfunction and oxidative stress in the heart. Circulation. 2009;119:1272–1283. [PubMed: 19237663]
17. Witteles RM, Tang WH, Jamali AH, Chu JW, Reaven GM, Fowler MB. Insulin resistance inidiopathic dilated cardiomyopathy: a possible etiologic link. J Am Coll Cardiol. 2004; 44:78–81.[PubMed: 15234411]
18. Kostis JB, Sanders M. The association of heart failure with insulin resistance and the developmentof type 2 diabetes. Am J Hypertens. 2005; 18:731–737. [PubMed: 15882558]
19. Zucker IH. Novel mechanisms of sympathetic regulation in chronic heart failure. Hypertension.2006; 48:1005–1011. [PubMed: 17015773]
20. Opie LH, Thandroyen FT, Muller C, Bricknell OL. Adrenaline-induced “oxygen-wastage” andenzyme release from working rat heart. Effects of calcium antagonism, beta-blockade, nicotinicacid and coronary artery ligation. J Mol Cell Cardiol. 1979; 11:1073–1094. [PubMed: 522135]
21. Iaccarino G, Koch WJ. Transgenic mice targeting the heart unveil G protein-coupled receptorkinases as therapeutic targets. Assay Drug Dev Technol. 2003; 1:347–355. [PubMed: 15090200]
22. Iaccarino G, Barbato E, Cipolletta E, De Amicis V, Margulies KB, Leosco D, Trimarco B, KochWJ. Elevated myocardial and lymphocyte GRK2 expression and activity in human heart failure.Eur Heart J. 2005; 26:1752–1758. [PubMed: 16055494]
23. Bonita RE, Raake PW, Otis NJ, Chuprun JK, Spivack T, Dasgupta A, Whellan DJ, Mather PJ,Koch WJ. Dynamic changes in lymphocyte GRK2 levels in cardiac transplant patients: abiomarker for left ventricular function. Clin Transl Sci. 2008; 3:14–18. [PubMed: 20443948]
24. Shahid G, Hussain T. GRK2 negatively regulates glycogen synthesis in mouse liver FL83B cells. JBiol Chem. 2007; 282:20612–20620. [PubMed: 17517892]
25. Usui I, Imamura T, Babendure JL, Satoh H, Lu JC, Hupfeld CJ, Olefsky JM. G protein-coupledreceptor kinase 2 mediates endothelin-1-induced insulin resistance via the inhibition of bothGalphaq/11 and insulin receptor substrate-1 pathways in 3T3-L1 adipocytes. Mol Endocrinol.2005; 19:2760–2768. [PubMed: 15994203]
26. Cipolletta E, Campanile A, Santulli G, Sanzari E, Leosco D, Campiglia P, Trimarco B, IaccarinoG. The G protein coupled receptor kinase 2 plays an essential role in beta-adrenergic receptor-induced insulin resistance. Cardiovasc Res. 2009; 84:407–415. [PubMed: 19620130]
27. Raake PW, Vinge LE, Gao E, Boucher M, Rengo G, Chen X, DeGeorge BR Jr, Matkovich S,Houser SR, Most P, Eckhart AD, Dorn GW 2nd, Koch WJ. G protein-coupled receptor kinase 2ablation in cardiac myocytes before or after myocardial infarction prevents heart failure. Circ Res.2008; 103:413–422. [PubMed: 18635825]
28. Rengo G, Lymperopoulos A, Zincarelli C, Donniacuo M, Soltys S, Rabinowitz JE, Koch WJ.Myocardial adeno-associated virus serotype 6-betaARKct gene therapy improves cardiac functionand normalizes the neurohormonal axis in chronic heart failure. Circulation. 2009; 119:89–98.[PubMed: 19103992]
29. Rockman HA, Koch WJ, Lefkowitz RJ. Seven-transmembrane-spanning receptors and heartfunction. Nature. 2002; 415:206–212. [PubMed: 11805844]
Ciccarelli et al. Page 9
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

30. Koch WJ, Rockman HA, Samama P, Hamilton RA, Bond RA, Milano CA, Lefkowitz RJ. Cardiacfunction in mice overexpressing the beta-adrenergic receptor kinase or a beta ARK inhibitor.Science. 1995; 268:1350–1353. [PubMed: 7761854]
31. Liu S, Premont RT, Kontos CD, Zhu S, Rockey DC. A crucial role for GRK2 in regulation ofendothelial cell nitric oxide synthase function in portal hypertension. Nat Med. 2005; 11:952–958.[PubMed: 16142243]
32. Sun XJ, Goldberg JL, Qiao LY, Mitchell JJ. Insulin-induced insulin receptor substrate-1degradation is mediated by the proteasome degradation pathway. Diabetes. 1999; 48:1359–1364.[PubMed: 10389839]
33. Aguirre V, Werner ED, Giraud J, Lee YH, Shoelson SE, White MF. Phosphorylation of Ser307 ininsulin receptor substrate-1 blocks interactions with the insulin receptor and inhibits insulin action.J Biol Chem. 2002; 277:1531–1537. [PubMed: 11606564]
34. Garcia-Guerra L, Nieto-Vazquez I, Vila-Bedmar R, Jurado-Pueyo M, Zalba G, Diez J, Murga C,Fernandez-Veledo S, Mayor F Jr, Lorenzo M. G Protein-Coupled Receptor Kinase 2 (Grk2) Playsa Relevant Role in Insulin Resistance and Obesity. Diabetes. 2010; 59:2407–2417. [PubMed:20627936]
35. Williams ML, Hata JA, Schroder J, Rampersaud E, Petrofski J, Jakoi A, Milano CA, Koch WJ.Targeted beta-adrenergic receptor kinase (betaARK1) inhibition by gene transfer in failing humanhearts. Circulation. 2004; 109:1590–1593. [PubMed: 15051637]
36. Aikawa R, Nawano M, Gu Y, Katagiri H, Asano T, Zhu W, Nagai R, Komuro I. Insulin preventscardiomyocytes from oxidative stress-induced apoptosis through activation of PI3 kinase/Akt.Circulation. 2000; 102:2873–2879. [PubMed: 11104747]
37. Decker RS, Cook MG, Behnke-Barclay M, Decker ML. Some growth factors stimulate culturedadult rabbit ventricular myocyte hypertrophy in the absence of mechanical loading. Circ Res.1995; 77:544–555. [PubMed: 7641324]
38. Markou T, Cullingford TE, Giraldo A, Weiss SC, Alsafi A, Fuller SJ, Clerk A, Sugden PH.Glycogen synthase kinases 3alpha and 3beta in cardiac myocytes: regulation and consequences oftheir inhibition. Cell Signal. 2008; 20:206–218. [PubMed: 17993264]
39. Werner ED, Lee J, Hansen L, Yuan M, Shoelson SE. Insulin resistance due to phosphorylation ofinsulin receptor substrate-1 at serine 302. J Biol Chem. 2004; 279:35298–35305. [PubMed:15199052]
40. Morino K, Petersen KF, Dufour S, Befroy D, Frattini J, Shatzkes N, Neschen S, White MF, Bilz S,Sono S, Pypaert M, Shulman GI. Reduced mitochondrial density and increased IRS-1 serinephosphorylation in muscle of insulin-resistant offspring of type 2 diabetic parents. J Clin Invest.2005; 115:3587–3593. [PubMed: 16284649]
Ciccarelli et al. Page 10
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Clinical Perspective
A large number of studies have demonstrated that the increased level of G protein-coupled receptor kinase 2 (GRK2) seen in injured myocardium has deleterious effects onthe progression of heart failure (HF). Importantly, GRK2 lowering is associated withimproved cardiomyocyte signaling and function in failing human hearts mechanicallyunloaded with assist devices. However, the mechanisms through which GRK2 promotesHF or why its inhibition is therapeutic have not been fully elucidated. Interestingly,therapies targeting the neurohormonal axis, such as β-blockers, can attenuate cardiacremodeling and improve prognosis in patients with HF and these drugs can significantlydecrease GRK2 in the heart. On the other hand, agents aimed to directly increase cardiaccontractility have failed. Thus, it appears that GRK2 lowering and inhibition, which doesimprove contractility, must have additional effects on pathological components of HFdevelopment to account for the overwhelming positive effects seen in various animalmodels. The current study provides the first evidence that there is a close relationshipbetween GRK2 activity and unfavorable modifications of cardiac metabolism, includinginsulin resistance and a loss of glucose uptake that can occur after ischemic injury andthrough the progression to HF. Indeed, we have identified IRS1 as a novel substrate ofGRK2 kinase activity that can attenuate insulin signaling in the myocyte. These data alsoinclude the demonstration that insulin resistance and defective glucose uptake appear inthe early stages of HF, suggesting the use of therapies aimed at restoring correctmetabolic substrate utilization in the myocyte as soon as possible after ischemic injury. Inthis scenario, lowering GRK2, which is known to be up-regulated acutely aftermyocardial injury, appears to be a feasible and exciting approach to maintain metabolichomeostasis in the myocyte, which may contribute significantly in preventing thedevelopment of subsequent ischemic HF.
Ciccarelli et al. Page 11
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1. GRK2 levels influence in vivo cardiac glucose uptake(A) Tg-GRK2 and NLC mice were studied by PET to evaluate cardiac glucose uptake afterintraperitoneal injection of insulin (Ins, 0.075U/Kg, IP). Ins significantly increases glucoseuptake however this response was attenuated in BK12 mice (*, P<0.05, Ins vs Basal, §,P<0.05, TG-GRK2 vs NLC, n=8 per group). (B) Plasma membrane GLUT4 protein levelsfrom Tg-GRK2 and NLC hearts. Animals were injected with Ins as above and sacrificed 15min later. GLUT4 levels on the plasma membrane were increased by Ins in NLC butattenuated in TG-GRK2. GLUT4 level was normalized to the membrane protein Gβ (*,P<0.05, Ins vs Basal, §, P<0.05, fold of increased translocation to the membrane, TG-GRK2vs NLC, n=3 per group).
Ciccarelli et al. Page 12
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2. Interplay between βAR and insulin receptor signalingARVMs were stimulated with Ins (0.1 μM for 10 min) with or without pre-treatment withthe βAR agonist isoproterenol (Iso, 10μM for 5 min). Membrane fractions were preparedand blotted for signaling proteins. (A) Representative western blot showing membraneGLUT4, pAkt and GRK2. Gβ blotting was used as loading control. (B–D) Bar Chartsshowing GLUT4 translocation (*, P<0.05 Ins vs. Basal, n=3; **, n.s, Iso+Ins vs Iso, n=3pergroup), Akt was activated in response to Ins but attenuated with Iso pretreatment (§ P<0.05,fold activation, Iso+Ins vs. Ins alone, n=3 per group) and GRK2 translocation induced byIns with or without Iso pretreatment (*§, P<0.05 Ins, Iso and Iso+Ins vs Basal, n=3 pergroup).
Ciccarelli et al. Page 13
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
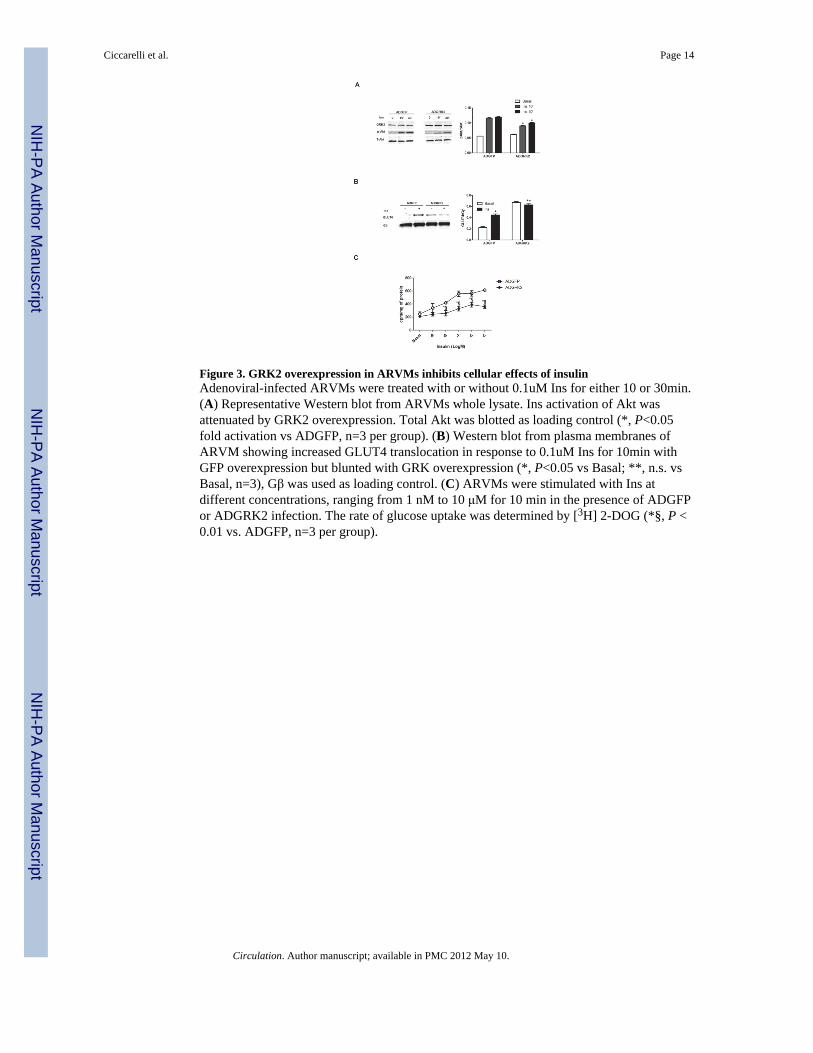
Figure 3. GRK2 overexpression in ARVMs inhibits cellular effects of insulinAdenoviral-infected ARVMs were treated with or without 0.1uM Ins for either 10 or 30min.(A) Representative Western blot from ARVMs whole lysate. Ins activation of Akt wasattenuated by GRK2 overexpression. Total Akt was blotted as loading control (*, P<0.05fold activation vs ADGFP, n=3 per group). (B) Western blot from plasma membranes ofARVM showing increased GLUT4 translocation in response to 0.1uM Ins for 10min withGFP overexpression but blunted with GRK overexpression (*, P<0.05 vs Basal; **, n.s. vsBasal, n=3), Gβ was used as loading control. (C) ARVMs were stimulated with Ins atdifferent concentrations, ranging from 1 nM to 10 μM for 10 min in the presence of ADGFPor ADGRK2 infection. The rate of glucose uptake was determined by [3H] 2-DOG (*§, P <0.01 vs. ADGFP, n=3 per group).
Ciccarelli et al. Page 14
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 4. Mechanism of inhibitory effects of GRK2 on insulin signaling in myocytes(A–B) ARVMs were infected with ADGFP, ADGRK2, or kinase-dead GRK2(ADGRK2DN) and stimulated with Ins (0.1 μM for 10 min). (A) Representativeimmunoblot in whole cell lysates showing reduced pAkt level when GRK2 is overexpressed(*, fold activation, P<0.01 vs ADGFP and ADGRK2DN, n=3 per group). (B) Ins-stimulatedGLUT4 membrane levels in ARVMs is attenuated with GRK2 overexpression (*, P<0.05 vsBasal; **, n.s. vs Basal, n=3) (C) IRS1 was immunoprecipitated from whole lysate ofARVMs infected with ADGFP or ADGRK2 and stimulated with Ins as above. Top panel,representative immunoblot for p-ser307 showing increased p-ser307 with ADGRK2treatment. Lower panel is total IRS-1 (* P<0.05 vs ADGFP, n= 3). (D) Level of p-Ser307 ofIRS1 was evaluated by immunoprecipitation of equal amount of IRS1 from isolatedmyocytes of NLC, Tg-GRK2 and cardiac GRK2 KO mice after stimulation with Ins (10−7
M, 10 min). Representative blots for GRK2, pSer307 IRS1 and total IRS1 are shown.Reduced and increased levels of pSer307IRS1 were respectively observed in GRK2KO andTg-GRK2 versus NLC (*, P<0.01, fold of activation, GRK2KO vs NLC, n=3; **, P <0.01,Tg-GRK2 vs NLC, n=3 per group). (E) GRK2 phosphorylates IRS1 at Ser307. An in-vitrokinase assay was performed with purified GST-IRS1 alone (none) or in the presence of ATPor ATP plus purified GRK2. Representative blot from 3 independent assays (top panel) anddensitometric analysis (lower panel) are shown. (*, P<0.05, fold activation vs ATP andnone) (F) NRVMs were co-infected with either ADIRS1wt or ADIRS1 mutant Ser307Ala(mt) in addition to ADGFP or ADGRK2 and stimulated with Ins as above. Representativeimmunoblot showing p-Akt levels is provided (*, P<0.01, fold activation vsADGRK2+ADIRS1wt, n=3 per group).
Ciccarelli et al. Page 15
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 5. Cardiac glucose uptake in post-MI mice(A) 18-FDG cardiac uptake in NLC Tg-GRK2 and cardiac-specific GRK2KO mice underSham conditions and 1–8 weeks post-MI. Shown at top are representative micro-PETimages where infarct is clearly visible and histogram below quantifies 18-FDG uptake inmyocardium (*, P<0.05, TG-GRK2 vs NLC; §, P<0.05, GRK2KO vs NLC, n=12 pergroup). (B–C) LV diameter at diastole and Ejection fraction (EF) in NLC, Tg-GRK2 andGRK2KO mice determined by echocardiography serially after MI. (*, P<0.01, Tg-GRK2 vsNLC; §, P<0.01, GRK2KO vs NLC, n=12, per group).
Ciccarelli et al. Page 16
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 6. Inhibition of GRK2 in myocytes and myocardium restores normal insulin signalingand prevents defective in vivo glucose uptake post-MI(A) Level of Ins-stimulated pSer307 in IRS1 immunoprecipitated from adult mouseventricular myocytes isolated from NLC, Tg-GRK2, or Tg-βARKct mice (*, P<0.01 vsNLC, n=3; §, P<0.01, Tg-βARKct vs NLC, n=3 per group). (B) ARVMs were infected witheither ADGFP, ADGRK2 or ADβARKct. Representative blots for p-Akt and t-Akt areshown (*, P <0.01, fold increase in activation, ADGRK2 vs ADGFP, n=3;**, P <0.01, foldincrease in activation, ADβARKct vs ADGRK2 and ADGFP, n=3 per group). (C)Representative western blot from ARVMs whole lysate infected as in (A) and stimulatedwith Ins showing pGSK3β and total-GSK3β (*, P <0.01, fold increase in activation,ADGRK2 vs ADGFP, n=3; **, P <0.01, fold increase in activation, ADβARKct vsADGRK2, n=3). (D) Global rat myocardial in vivo glucose uptake evaluated by micro-PETin Sham and 1, 3, 6, and 12 weeks post-MI rats treated with AAV6-GFP or AAV6-βARKct(*, P<0.05, vs AAV6GFP, n=8 per group). (E) Rats 3 weeks post MI and Sham weresacrificed 15 min after an IP injection of insulin (0.075 U/Kg) and hearts removed. Plasma
Ciccarelli et al. Page 17
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

membranes were prepared to evaluate GLUT4 levels as shown in a representative blot (*,P<0.05 vs Basal; §, P< 0.05 vs Basal, n=3 per group).
Ciccarelli et al. Page 18
Circulation. Author manuscript; available in PMC 2012 May 10.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Copyright © 2022 FDOKUMEN




















