Factors associated with gallstone disease in the MICOL experience
10
Original Articles Factors Associated With Gallstone Disease in the MICOL Experience A. F. ATTILI, R. CAPOCACCIA, N. CARULLI, D. FESTI, E. RODA, L. BARBARA, L. CAPOCACCIA, A. MENOTTI, L. OKOLICSANYI, G. RICCI, L. LALLONI, S. MARIOTTI, C. SAMA, E. SCAFATO, AND THE MICOL GROUP The epidemiological associations of gallstone disease were by age and sex have been extensively reported in a previous article, 1 and will be only briefly recalled here. This article evaluated in a general population sample of 29,584 individu- als (15,910 men and 13,674 women; age range, 30-39 years) analyzes and discusses the relationships between gallstone disease and the associated individual factors. belonging to 14 cohorts examined between December 1984 and April 1987. Subjects were screened for the presence of PATIENTS AND METHODS gallstones by gallbladder ultrasonography, completed a ques- tionnaire, and underwent a physical examination and blood Data Collection. The study protocol was prepared by the coordi- chemistry tests. Participants were considered to have gall- nating unit based on experience gained during the pioneering epide- stone disease if they had already had cholecystectomy or gall- miological studies performed in Italy by the Rome Group for the stones. Statistical associations were established by univariate Epidemiology and Prevention of Cholelithiasis (GREPCO) 2-5 and analysis of the age-standardized data and by stepwise multiple the Sirmione project. 6 The examination included an interview with logistic regression. Increasing age and body mass index and the administration of a standard questionnaire, followed by a physi- a maternal family history of gallstone disease were the most cal and ultrasonographic examination of the upper abdomen and a blood sampling for biochemical analyses. Field activities started in consistent associations (both at univariate and multivariate December 1984 and finished in April 1987. Details of the question- analysis and in both sexes) found in this study. Personal naire were given elsewhere. 1 Among others, questions relevant to history of dieting was associated with gallstone disease in the present study were the following: 1) Did your father or mother men, and at univariate analysis, in women. Decreasing serum ever suffer from gallstones or undergo cholecystectomy? 2) Do you total cholesterol levels and increasing serum triglycerides currently smoke cigarettes? If yes, how many a day and since when? were associated with gallstone disease in both sexes in the If not, have you ever smoked regularly? 3) Have you ever suffered multivariate analysis. In women, associations were also found from diabetes, gastric or duodenal ulcer, myocardial infarction or with a number of pregnancies and paternal family history angina, hepatic cirrhosis, Crohn’s disease, or hemolytic anemia? of gallstone disease. A slight but negative association with 4) Have you ever regularly assumed serum lipid – lowering drugs, contraceptive pill use was identified only at multivariate anal- aspirin, or antirheumatic drugs? If yes, which and for how long? and 5) Have you ever been on a slimming diet? Women were also ysis. Associations (investigated at univariate analysis) were asked about the number of pregnancies and use of estroprogestinic also found with diabetes, cirrhosis, angina or myocardial in- drugs. To estimate the prevalence of gallstone disease, the final farction, and peptic ulcer. There was no association with gallbladder status was recorded as follows: 1) normal at ultrasonog- smoking habits and use of aspirin or antirheumatic drugs. raphy; 2) presence of gallstones at ultrasonography; 3) presence of (HEPATOLOGY 1997; 26:809-818.) biliary sludge at ultrasonography; 4) previous cholecystectomy; and 5) inconclusive or doubtful. Gallstone disease was defined as the presence of conditions 2 or 4. A blood sample was obtained from The MICOL study (Multicenter Italian Study on Epidemi- each subject after an overnight fast to measure serum glucose, total ology of Cholelithiasis) was designed to obtain an overview and high-density lipoprotein cholesterol, triglycerides, and alanine of the distribution of gallstone disease in Italy for different transaminase. The same biochemical procedures and the same batch regions and age classes. For this purpose, 18 population sam- of reagents were used by all groups. A quality-control program on ples, covering most Italian regions, were enrolled in the all biochemical analyses was implemented under the supervision of the Biochemical Laboratory of the National Institutes of Health. study, with a total selected population of about 54,000 indi- Subjects. Details on participation rates were given elsewhere. 1 All viduals (men and women). Results on prevalence distribution analyses reported here refer to data for 29,584 individuals (15,910 men and 13,674 women) examined in 14 cohorts with a participa- tion rate above 50%. The mean prevalence of gallstones was 6.5% in men and 10.5% in women. The overall proportion of subjects Abbreviations: CI, confidence interval; BMI, body mass index; OR, odds ratio. From the MICOL (Multicenter Italian Study on Epidemiology of Cholelithiasis) having cholecystectomy was 3.0% in men and 8.4% in women. Research Group, Rome, Italy. Statistical Methods. All analyses reported in this article refer to Received December 23, 1996; accepted June 3, 1997. presence of gallstones or to gallstone disease as dependent variables. Supported by in part by the Italian National Research Council (Targeted Projects Data from men and women were analyzed separately. The univariate ‘‘Preventive and Rehabilitative Medicine’’ 1982-1987 and ‘‘Prevention and Control of analysis was performed for a number of factors possibly associated Risk factors’’ 1990-1995). with the disease. The age-adjusted prevalence was calculated by Address reprint requests to: Adolfo Francesco Attili, M.D., Largo Forano 3, 00199 applying the regression slopes for gallstones, cholecystectomy, and Rome, Italy. Fax: 39-6-444-0806. gallstone disease reported in a previous article by our group. 1 The Copyright q 1997 by the American Association for the Study of Liver Diseases. 0270-9139/97/2604-0001$3.00/0 odds ratios (OR) were calculated with reference to the lowest 809 AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology
Transcript of Factors associated with gallstone disease in the MICOL experience

Original Articles
Factors Associated With Gallstone Diseasein the MICOL Experience
A. F. ATTILI, R. CAPOCACCIA, N. CARULLI, D. FESTI, E. RODA, L. BARBARA, L. CAPOCACCIA, A. MENOTTI, L. OKOLICSANYI,G. RICCI, L. LALLONI, S. MARIOTTI, C. SAMA, E. SCAFATO, AND THE MICOL GROUP
The epidemiological associations of gallstone disease were by age and sex have been extensively reported in a previousarticle,1 and will be only briefly recalled here. This articleevaluated in a general population sample of 29,584 individu-
als (15,910 men and 13,674 women; age range, 30-39 years) analyzes and discusses the relationships between gallstonedisease and the associated individual factors.belonging to 14 cohorts examined between December 1984
and April 1987. Subjects were screened for the presence ofPATIENTS AND METHODSgallstones by gallbladder ultrasonography, completed a ques-
tionnaire, and underwent a physical examination and bloodData Collection. The study protocol was prepared by the coordi-chemistry tests. Participants were considered to have gall-
nating unit based on experience gained during the pioneering epide-stone disease if they had already had cholecystectomy or gall- miological studies performed in Italy by the Rome Group for thestones. Statistical associations were established by univariate Epidemiology and Prevention of Cholelithiasis (GREPCO)2-5 andanalysis of the age-standardized data and by stepwise multiple the Sirmione project.6 The examination included an interview withlogistic regression. Increasing age and body mass index and the administration of a standard questionnaire, followed by a physi-a maternal family history of gallstone disease were the most cal and ultrasonographic examination of the upper abdomen and a
blood sampling for biochemical analyses. Field activities started inconsistent associations (both at univariate and multivariateDecember 1984 and finished in April 1987. Details of the question-analysis and in both sexes) found in this study. Personalnaire were given elsewhere.1 Among others, questions relevant tohistory of dieting was associated with gallstone disease inthe present study were the following: 1) Did your father or mothermen, and at univariate analysis, in women. Decreasing serumever suffer from gallstones or undergo cholecystectomy? 2) Do youtotal cholesterol levels and increasing serum triglyceridescurrently smoke cigarettes? If yes, how many a day and since when?
were associated with gallstone disease in both sexes in the If not, have you ever smoked regularly? 3) Have you ever sufferedmultivariate analysis. In women, associations were also found from diabetes, gastric or duodenal ulcer, myocardial infarction orwith a number of pregnancies and paternal family history angina, hepatic cirrhosis, Crohn’s disease, or hemolytic anemia?of gallstone disease. A slight but negative association with 4) Have you ever regularly assumed serum lipid–lowering drugs,contraceptive pill use was identified only at multivariate anal- aspirin, or antirheumatic drugs? If yes, which and for how long?
and 5) Have you ever been on a slimming diet? Women were alsoysis. Associations (investigated at univariate analysis) wereasked about the number of pregnancies and use of estroprogestinicalso found with diabetes, cirrhosis, angina or myocardial in-drugs. To estimate the prevalence of gallstone disease, the finalfarction, and peptic ulcer. There was no association withgallbladder status was recorded as follows: 1) normal at ultrasonog-smoking habits and use of aspirin or antirheumatic drugs.raphy; 2) presence of gallstones at ultrasonography; 3) presence of(HEPATOLOGY 1997;26:809-818.)biliary sludge at ultrasonography; 4) previous cholecystectomy; and5) inconclusive or doubtful. Gallstone disease was defined as thepresence of conditions 2 or 4. A blood sample was obtained fromThe MICOL study (Multicenter Italian Study on Epidemi-each subject after an overnight fast to measure serum glucose, total
ology of Cholelithiasis) was designed to obtain an overview and high-density lipoprotein cholesterol, triglycerides, and alanineof the distribution of gallstone disease in Italy for different transaminase. The same biochemical procedures and the same batchregions and age classes. For this purpose, 18 population sam- of reagents were used by all groups. A quality-control program onples, covering most Italian regions, were enrolled in the all biochemical analyses was implemented under the supervision of
the Biochemical Laboratory of the National Institutes of Health.study, with a total selected population of about 54,000 indi-Subjects. Details on participation rates were given elsewhere.1 Allviduals (men and women). Results on prevalence distribution
analyses reported here refer to data for 29,584 individuals (15,910men and 13,674 women) examined in 14 cohorts with a participa-tion rate above 50%. The mean prevalence of gallstones was 6.5%in men and 10.5% in women. The overall proportion of subjectsAbbreviations: CI, confidence interval; BMI, body mass index; OR, odds ratio.
From the MICOL (Multicenter Italian Study on Epidemiology of Cholelithiasis) having cholecystectomy was 3.0% in men and 8.4% in women.Research Group, Rome, Italy. Statistical Methods. All analyses reported in this article refer to
Received December 23, 1996; accepted June 3, 1997. presence of gallstones or to gallstone disease as dependent variables.Supported by in part by the Italian National Research Council (Targeted Projects Data from men and women were analyzed separately. The univariate
‘‘Preventive and Rehabilitative Medicine’’ 1982-1987 and ‘‘Prevention and Control ofanalysis was performed for a number of factors possibly associated
Risk factors’’ 1990-1995).with the disease. The age-adjusted prevalence was calculated byAddress reprint requests to: Adolfo Francesco Attili, M.D., Largo Forano 3, 00199applying the regression slopes for gallstones, cholecystectomy, andRome, Italy. Fax: 39-6-444-0806.gallstone disease reported in a previous article by our group.1 TheCopyright q 1997 by the American Association for the Study of Liver Diseases.
0270-9139/97/2604-0001$3.00/0 odds ratios (OR) were calculated with reference to the lowest
809
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

810 ATTILI ET AL. HEPATOLOGY October 1997
TABLE 1. Age-Adjusted OR and 95% CI of Gallstones and Gallstone Disease by Decade for Men and Women
Men Women
Decades No. Gallstones Gallstone Disease No. Gallstones Gallstone Disease
30-39 4,027 1 (Ref) 1 (Ref) 3,434 1 (Ref) 1 (Ref)40-49 4,322 1.79 (1.41-2.27) 2.06 (1.67-2.52) 3,714 1.48 (1.24-1.78) 1.90 (1.65-2.20)50-59 4,393 3.37 (2.70-4.19) 3.82 (3.15-4.62) 3,833 2.08 (1.76-2.47) 2.53 (2.21-2.91)60-69 3,141 4.48 (3.59-5.59) 5.63 (4.65-6.83) 2,666 3.07 (2.58-3.65) 3.95 (3.43-4.54)
Abbreviation: Ref, reference population.
quartile for continuous variables or to the lowest category for cate- Higher levels were associated with a lower risk of gallstonegorical variables, except for occupational status, in which white- disease, but no further decrease was expected for serum cho-collar workers were used as the reference population. The associa- lesterol levels above 300 mg/dL. Serum cholesterol was alsotion between risk factors and prevalence of the disease was then negatively associated with both gallstones and gallstone dis-analyzed with multiple logistic regression analysis, and a stepwise ease in women, the relation being linear (Table 3). For gall-procedure was used to select the significant factors from the initial
stone disease, however, the strength of the association wasset of considered variables. Linear trends are described by the regres-modified by age (Fig. 3). The OR of gallstone disease, associ-sion coefficients and their corresponding SE and P values. To facili-ated with an increase of 20 mg/mL of serum cholesterol, wastate interpretation, higher-order terms are graphically presented inreduced with increasing age. For gallstones only, OR wasterms of ORs and corresponding 95% confidence bounds. These
were derived by the delta method from the information matrix. 0.97 (95% confidence interval [CI]Å 0.94-0.99), irrespectiveThey vanish at the factor’s value assumed as a reference for the of age.calculation of ORs. Regression models were also fitted to the data With regard to HDL serum cholesterol levels, the risk ofof single cohorts, showing that factors behaved in a sufficiently gallstone disease was higher in the lower quartile than in thesimilar way to allow pooled analysis. In the pooled regression model other quartiles in both sexes (Table 2). In women, an inversethe coefficients were supposed to be the same for all samples, and association was also observed for gallstones. In the multivari-the intercept was allowed to vary between populations to control
ate analysis no association was observed.possible confounding because of between-population variability ofSerum triglycerides were positively and significantly asso-unmeasured factors. Variables indicating previous diagnosis of other
ciated with gallstone disease only in women (Table 2). Indiseases such as myocardial infarction, peptic ulcer, or diabetesthe multivariate analysis (Table 3) serum triglycerides werewere excluded from the multivariate analysis. This decision was
made for the following reasons. 1) The underlying purpose of this positively associated with both gallstones and gallstone dis-work was to further increase our knowledge on gallstone disease ease in men. The ORs associated with an increase of 50 mg/in the general population. The low prevalence of these diseases and dL were 1.05 (95% CIÅ 1.02-1.08 ) in both cases. In women,the results of the univariate analysis clearly indicated that no rele- triglycerides were significantly associated with gallstone dis-vant proportion of gallstone disease might be attributed to any of ease, OR Å 1.06 (95% CI Å 1.02-1.10 ), but not with gall-these. The highest attributable risk was estimated for diabetes, that stones only.is 1.9. The corresponding values for peptic ulcer and myocardial
Body Mass Index. An increasing risk of gallstones or gall-infarction were 1.2 and 1.1, respectively. Therefore the occurrencestone disease with increasing body mass index (BMI) wasof these diseases cannot explain the gallstone disease prevalenceevident in women (Table 4). A similar but much less evidentlevels in the general population. 2) The association between thetrend was observed in men. BMI was also positively andpresence of two diseases may be misleading if the time sequence
between them is unknown. 3) The correlation between the preva- significantly associated with gallstone disease when control-lence of these diseases and other factors, as for instance betweenmyocardial infarction and age or serum lipids, could bias the esti-mates of the corresponding coefficients and yield meaningless re-sults. 4) Information about previous diagnosis was self-reported,and therefore much less accurate than for gallstone disease. In mul-tivariate analysis this lack of accuracy may affect the results as awhole.
RESULTS
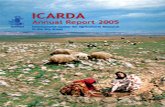
Age. An increased risk of gallstones and gallstone diseasewas observed for increasing ages in both sexes (Table 1). Inthe multivariate analysis the relation appeared curvilinear inmen (Fig. 1), a decreasing risk being observed for older ages.
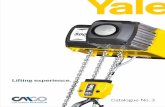
Serum Lipids. An inverse relationship was observed be-tween total serum cholesterol levels and the risk of gallstonesor gallstone disease (Table 2). In the multivariate analysis,cholesterol level in men was negatively associated with gall-stone disease, with a nonlinear shape (Fig. 2), showing astronger association at lower cholesterol levels. With respectto a mean value of 250 mg/dL, the odds of gallstone disease FIG. 1. Estimated ORs (and 95% CI) of gallstones in men as a function
of years of age, as derived from logistic regression analysis.rose steeply for decreasing values of serum cholesterol.
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

HEPATOLOGY Vol. 26, No. 4, 1997 ATTILI ET AL. 811
stones or gallstone disease was significantly higher amongmanagers or pensioners than in the reference population (Ta-ble 6). Among women, housewives had an increased proba-bility of gallstones.
Slimming Diet. On the questionnaire, 1,423 men and 2,069women responded yes to the question, Were you ever on aslimming diet? Men who had been on a slimming diet pre-sented an increased risk for gallstones or gallstone disease(OR Å 1.47 [95% CI Å 1.21-1.78] and OR Å 1.59 [95% CIÅ 1.35-1.86]) A similar, but less evident, association wasobserved in women (OR Å 1.18 [95% CI Å 1.05-1.32]). Inmultivariate analysis (Table 3), the association between aslimming diet and gallstone disease was also controlled forthe BMI level, which is a candidate confounding factor. Theresulting ORs for men were still statistically significant: 1.33(95% CI Å 1.07-1.65) and 1.38 (95% CI Å 1.15-1.69), re-spectively, for gallstones and gallstone disease were estimated
FIG. 2. Estimated ORs (and 95% CI) of gallstone disease as a function in this case. At multivariate analysis no association resultedof total serum cholesterol levels, as derived from logistic regression analysis.
for women.Smoking. Both at univariate and multivariate analysis,
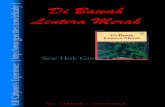
smoking was not a factor associated with gallstones or gall-ling, with multivariate analysis (Table 3), for the other covari-stone disease.ates. The estimated OR in men associated with a unitary
Aspirin and Other Antirheumatic Drugs. A particularly lowincrease of BMI was 1.03 (95% CI Å 1.01-1.05) for bothrisk for gallstones was observed in the 139 women replyinggallstones and gallstone disease. In women, the correspond-positively to the question, Have you ever regularly used aspi-ing value for gallstones was 1.06 (95% CI Å 1.05-1.07),rin or other antirheumatic drugs?, and indicating a use ofwhereas the relation with gallstone disease, shown in Fig. 4,over 60 months (Table 7). However, a reduced risk of gall-was nonlinear. In fact at BMI equal to 16 the OR associatedstone disease was observed in both sexes if they had takenwith a unitary increase of the factor was 1.10 (95% CI Åaspirin or antirheumatic drugs for less than 12 months.1.09-1.11 ); the corresponding value for BMI Å 36 was 1.04
Hypolipidemic Drugs. No association was noted between re-(95% CI Å 1.01-1.06). When estimated with respect to theported regular use of hypolipidemic drugs and risk for gall-mean level (BMI Å 26), the OR of having gallstones for astones or gallstone disease in both sexes.unitary increase was 1.07 (95% CI Å 1.05-1.09)
Family History. Each participant was invited to respond toEducation. Among the factors measured in this study, edu-the question, Did your father or mother ever suffer fromcation may be considered the best indicator of socioeconomicgallstones or have their gallbladder surgically removed?status. An increasing risk of having gallstones and gallstoneAmong those responding yes for the mother, an increaseddisease with higher educational qualifications was observedrisk of gallstones or gallstone disease was observed in bothin men (Table 5). This was not the case with women. Multi-sexes (Table 8). Women whose father had clinically diag-variate analysis (Table 3) confirmed the results of the univari-nosed gallstone disease also had an increased risk of gallstoneate analysis.
Occupation. In men, the age adjusted OR of having gall- disease that was even higher for women reporting a history
TABLE 2. Age-Adjusted OR of Gallstones and Gallstone Disease by Quartiles of Serum Levels of Total Serum Cholesterol,HDL Cholesterol, and Triglycerides for Men and Women
Men Women
Quartiles No. Gallstones Gallstone Disease Quartiles No. Gallstones Gallstone Disease
Total cholesterol71-189 3,531 1 (Ref) 1 (Ref) 66-185 2,870 1 (Ref) 1 (Ref)190-219 3,643 0.84 (0.70-1.00) 0.86 (0.74-1.00) 186-216 2,851 0.93 (0.79-1.10) 0.91 (0.80-1.00)220-250 3,629 0.76 (0.64-0.94) 0.73 (0.63-0.85) 217-250 2,688 0.90 (0.77-1.07) 0.93 (0.82-1.06)251-647 3,581 0.72 (0.60-0.87) 0.66 (0.57-0.78) 251-920 2,658 0.78 (0.66-0.93) 0.77 (0.68-0.88)
HDL cholesterol6-39 3,722 1 (Ref) 1 (Ref) 7-45 2,615 1 (Ref) 1 (Ref)40-46 3,365 1.01 (0.84-1.20) 0.87 (0.75-1.01) 46-54 2,838 0.76 (0.66-0.89) 0.79 (0.70-0.89)47-55 3,648 0.86 (0.72-1.03) 0.78 (0.67-0.91) 55-64 2,691 0.78 (0.65-0.90) 0.82 (0.73-0.92)56-98 3,649 0.84 (0.70-1.01) 0.73 (0.63-0.85) 65-98 2,932 0.76 (0.65-0.89) 0.70 (0.62-0.79)
Triglycerides10-86 3,612 1 (Ref) 1 (Ref) 17-69 2,957 1 (Ref) 1 (Ref)87-122 3,629 0.98 (0.82-1.18) 1.00 (0.86-1.16) 70-94 2,721 1.23 (1.04-1.46) 1.18 (1.03-1.36)123-179 3,570 0.92 (0.77-1.10) 0.99 (0.85-1.15) 95-134 2,748 1.22 (1.03-1.45) 1.23 (1.08-1.40)180-6,014 3,573 0.89 (0.74-1.07) 0.94 (0.80-1.09) 135-9,801 2,641 1.16 (0.97-1.37) 1.31 (1.15-1.49)
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

812 ATTILI ET AL. HEPATOLOGY October 1997
TABLE 3. Logistic Regression Analysis. Regression Coefficients, Corresponding Standard Errors, and P Values for Single Factorsand Interactions, Significantly Associated With Gallstones and Gallstone Disease
Gallstones Gallstone Disease
Factor Coefficient SE P Coefficient SE P
MenAge .1825 .0374 õ.001 .1894 .0319 õ.001Age2 0.0013 .0004 õ.001 0.0013 .0003 õ.001BMI .0300 .0102 õ.01 .0300 .0086 õ.001Cholesterol 0.0039 .0008 õ.001 0.0133 .0038 õ.001Cholesterol2 .00002 .00001 õ.05Triglycerides .0010 .0003 õ.01 .0010 .0003 õ.001Slimming diet .2875 .110 õ.01 .3209 .0927 õ.001FamiliarityMother .5788 .101 õ.001 .6316 .0849 õ.001Education
None-elementary 0 0Junior high .2479 .082 õ.01 .2610 .0692 õ.001High school-university .3751 .175 õ.05 .2291 .154 NS
WomenAge .0449 .0034 õ.001 .0756 .0117 õ.001BMI .0570 .0066 õ.001 .1390 .0419 õ.001BMI2 0.0014 .0007 õ.05Cholesterol 0.0016 .0007 õ.05 0.0054 .0028 õ.05Cholesterol* age 0.00015 .0005 õ.01Triglycerides .0011 .0004 õ.001N of pregnancies
0 0 01 0.0010 .115 n.s. .1377 .0932 n.s.2 .0777 .101 n.s. .2367 .0827 õ.013 .1141 .111 n.s. .2871 .0904 õ.001ú3 .2347 .116 õ.05 .3563 .0961 õ.001
Pill use 0.2079 .0865 õ.05FamiliarityMother .3564 .0875 õ.001 .4720 .0670 õ.001Father .3675 .182 õ.05 .6536 .129 õ.001
NOTE. Age2, BMI2, and Cholesterol2 are quadratic terms; Cholesterol* age is interaction between cholesterol and age (see Fig. 3).
of disease in both parents. To avoid the possible bias in which we limited the univariate analysis to this last group. The ORfor gallstones (not shown here) were almost identical to thosesubjects with already-diagnosed gallstones or with cholecys-
tectomy may be more aware of similar problems in their obtained in the unselected group. Multivariate analysis con-firmed the abovementioned results. Estimated ORs in womenparents than subjects who are unaware of having gallstones,with paternal family history were 1.44 (95% CI Å 1.01-2.06)for gallstones and 1.92 (95% CI Å 1.49-2.48) for gallstonedisease, and 1.43 (95% CI Å 1.20-1.70) and 1.60 (95% CIÅ 1.41-1.83), respectively, for maternal family history. In
TABLE 4. Age-Adjusted OR of Gallstones and the GallstoneDisease by Quartiles of BMI for Men and Women
BMIQuartiles No. Gallstones Gallstone Disease
Men15-24.0 3,679 1 (Ref) 1 (Ref)24.1-26.2 3,687 1.04 (0.86-1.25) 1.04 (0.89-1.22)26.3-28.5 3,547 1.08 (0.90-1.31) 1.18 (1.01-1.39)28.6-48.0 3,471 1.20 (1.00-1.44) 1.24 (1.06-1.46)
Women12-22.7 2,914 1 (Ref) 1 (Ref)22.8-25.2 2,825 1.16 (0.96-1.40) 1.14 (0.98-1.31)25.3-28.6 2,731 1.42 (1.18-1.69) 1.48 (1.29-1.70)
FIG. 3. OR (and 95% CI) of gallstone disease in women associated with 28.7-55.5 2,597 1.86 (1.57-2.21) 2.03 (1.77-2.31)an increase of 10 mg/dL of total serum cholesterol according to age.
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

HEPATOLOGY Vol. 26, No. 4, 1997 ATTILI ET AL. 813
TABLE 5. Age-Adjusted OR of Gallstones, and the Gallstone Disease and 95% CI by Education Level
Men WomenEducational
Level No. Gallstones Gallstone Disease No. Gallstones Gallstone Disease
None 1,056 1 (Ref) 1 (Ref) 2,056 1 (Ref) 1 (Ref)Primary 7,301 1.19 (0.93-1.54) 1.21 (0.98-1.49) 6,921 1.08 (0.93-1.25) 1.18 (1.05-1.33)Middle 3,879 1.35 (1.04-1.75) 1.43 (1.15-1.78) 2,331 1.16 (0.98-1.39) 1.18 (1.03-1.36)High school 2,774 1.57 (1.20-2.04) 1.60 (1.28-2.01) 1,826 1.08 (0.90-1.31) 1.01 (0.87-1.17)University 837 1.83 (1.33-2.51) 1.69 (1.29-2.21) 457 0.91 (0.66-1.25) 0.84 (0.65-1.08)
men, only this last factor was significant, with estimated ORs Peptic Ulcer. A total of 1976 men and 797 women (12.4%and 5.8% of the examined population, respectively) declaredof 1.78 (95% CI Å 1.46-1.03) for gallstones and 1.88 (95%
CI Å 1.59-2.22) for gallstone disease. that they had suffered in the past or were presently sufferingfrom peptic ulcer. In men, an increased risk for gallstones andDiabetes. In this study, 756 men and 568 women (4.7%
and 4.2% of the examined population, respectively) were gallstone disease was present in those presenting a history ofpeptic ulcer (Table 9). The opposite was found for womenaware of being diabetic. A higher risk for gallstones and
gallstone disease among diabetic men and women was evi- with regard to gallstones and gallstone disease.Parity. An increased risk for gallstone disease was observeddent (Table 9). The results were not different when 232 men
and 92 women with serum glucose levels above 140 mg/dL with increasing number of pregnancies (Table 10). An in-creased risk for gallstones was only observed in women with(although they had declared that they were not diabetic)
were included. four or more pregnancies. When controlling in the multivari-ate analysis for the other covariates (Table 3), the estimatedCirrhosis. In this study, 65 men and 18 women were aware
of being cirrhotic at the moment of examination. In both ORs for gallstones were 1.00 (95% CI Å 0.79-1.25), 1.08(95% CI .89-1.32), 1.12 (95% CI Å 0.9-1.39), and 1.26 (95%sexes a significant increase in risk for gallstone disease was
evident (Table 9). CI Å 1.01-1.58) for women with one, two, three, and morethan three pregnancies, with respect to the nulliparous. TheHemolytic Anemia. A total of 290 men and 278 women were
aware of having hemolytic anemia. Most of these were in- corresponding values for gallstone disease were 1.15 (95%CI Å 0.95-1.38), 1.26 (95% CI Å 1.08-1.49), 1.33 (95% CIcluded in cohorts from Sinnai (Sardinia) and Codigoro (Fer-
rara), where there is a high prevalence of beta thalassemia. Å 1.12-1.59) and 1.42 (95% CI Å 1.18-1.72), respectively.Oral Contraceptives. At univariate analysis, use of oral con-In men, a higher risk of gallstones or gallstone disease was
observed in patients with hemolytic anemia than in the refer- traceptives was not associated with gallstones or gallstonedisease. No association was noted even stratifying for theence population (Table 9). No association was observed in
women. time-length of pill use or for the most commonly used typesof oral contraceptives containing different amounts of estro-Myocardial Infarction or Angina. On the survey, 523 men and
209 women (3.3% and 1.5% of the examined population, gen and progestin. At multivariate analysis (Table 3), a nega-tive association between gallstone disease and use of oralrespectively) responded yes to the question, Have you ever
suffered from myocardial infarction or angina? With the ex- contraceptives was observed (OR, 0.81; 95% CIÅ 0.68-0.96).ception of gallstones in women, the results consistently indi-
DISCUSSIONcated an increased risk for gallstones and gallstone diseaseThe overall participation rate in the present study wasin those with a previous history of angina or myocardial
lower than that obtained in previous epidemiological studiesinfarction (Table 9).on gallstone disease performed in Italy. This result was tosome extent predictable. Of course, the possibility that aparticipation bias might have influenced the results cannotbe excluded in principle. However, a serious bias is unlikelyto have occurred for several reasons. First of all, the programwas presented to the invited participants as a general programof preventive medicine, with no mention of the specific goal.Moreover, most of the prevalent subjects were unaware ofhaving gallstones. After excluding the four cohorts with thelowest sample size, the correlation between participationamong the 14 cohorts contributing to the pooled sample andprevalence was negative for women and near zero for men.Because the results obtained regarding associated factorswere highly consistent between the two sexes, the existenceof a sex-specific bias seems unlikely.
Quality control studies were performed to test the reliabil-ity of ultrasonographic7 and chemical laboratory findings.Ultrasonography had a very good interobserver agreementon the definite presence or absence of gallstones, and less so
FIG. 4. Estimated OR of gallstone disease in women according to BMI. for doubtful diagnoses. Quality control of serum cholesterol,
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

814 ATTILI ET AL. HEPATOLOGY October 1997
TABLE 6. Age-Adjusted OR of Gallstones and the Gallstone Disease and 95% CI by Occupational Status
Men Women
No. Gallstones Gallstone Disease No. Gallstones Gallstone Disease
White-collar w 5,999 1 (Ref) 1 (Ref) 2,749 1 (Ref) 1 (Ref)Manager 701 1.66 (1.25-2.19) 1.57 (1.23-2.00) 100 1.04 (0.50-2.18) 0.89 (0.48-1.64)Blue-collar w 6,487 0.93 (0.79-1.08) 1.01 (0.89-1.15) 2,417 0.90 (0.73-1.11) 1.01 (0.86-1.18)Pensioner 2,449 1.27 (1.01-1.60) 1.31 (1.12-1.54) 1,588 0.96 (0.76-1.21) 1.09 (0.92-1.31)Unemployed 132 0.80 (0.35-1.83) 0.72 (0.35-1.49) 51 NC 1.04 (0.46-2.32)Housewife 6,649 1.16 (0.98-1.37) 1.16 (1.02-1.32)
Abbreviation: NC, not calculable.
triglycerides, and glucose measurements showed nonnegligi- study. In a case control study, Scragg et al.,15 too, reportedthe presence of an inverse association, which was obscured inble interlaboratory effects. Regression analyses of obtained
versus expected measures showed regression slopes generally the multivariate analysis by plasma insulin and triglycerides.Serum triglyceride levels were associated with gallstone dis-between 0.9 and 1.1. Of the 16 laboratories of the centers
belonging to the pooled sample, only three centers showed ease in women both at univariate and multivariate analysis.In men the association was evident only after controlling forregression slopes outside these limits for triglycerides (b Å
0.868, bÅ 0.888, and bÅ 1.151) and two centers for glucose multiple factors in the multivariate analysis. The interactionwith age, observed by Scragg et al.15 and the GREPCO study,5(b Å 1.196, and b Å 0.685).
Our study confirms previous observations of the GREPCO was not evident.The positive association with BMI was evident in bothstudies2,3 showing that age is linearly related to gallstone
disease. This observation suggests that the age trend of the sexes, confirming that obesity is a key factor in the pathogen-esis of gallstones. A slightly curvilinear relationship betweenincidence is flat or only slightly increasing (the rate of in-
crease needed to compensate a possible cohort effect). gallstone disease and BMI was present in women. The qua-dratic relationship between gallstone disease prevalence andWith regard to serum lipids, our study shows an inverse
relationship between serum total cholesterol levels and gall- BMI in women indicates a sort of saturation effect: the associ-ation is higher in slim or normal subjects, losing strength asstones. This particularly applies to men. Similar results were
observed in two Danish9-10 and one Japanese study.11 The the factor’s level increases.Our study shows that educational level is positively associ-GREPCO reported similar results in women.5 At variance,
the Sirmione project,6 the Framingham study,12 and Diehl et ated with gallstone disease in men but not in women. Manag-ers were at increased risk for gallstone disease. Similar resultsal.13 reported no such association. A specific contribution of
the present study is the possibility, arising from the large were observed by Maurer et al.16 in Hispanic populationsof the United States, whereas Diehl et al.,17 in multivariatenumber of individuals examined, of a more detailed modeling
of the shape of the considered relationships. Thus it is possi- analysis, found an inverse association between socioeco-nomic indicators and clinical gallbladder disease in women.ble to observe that, in men, no substantial change in gallstone
disease prevalence is associated with further increases in se- No definite association was noted between gallstone dis-ease and smoking habits. Similar results emerged in therum cholesterol over a threshold level of about 300 mg/mL.
In turn, the interaction effect with age indicates that serum GREPCO study,5 whereas a positive association with smok-ing habits was observed in two studies18-19 investigating clini-cholesterol levels are negatively associated with the preva-
lence of the disease in women only at later ages. As far as cal gallbladder disease.Men and women who had been on a slimming diet inHDL cholesterol is concerned, an inverse association was
found at univariate analysis with gallstone disease in both the past were at increasing risk of gallstone disease. Thisassociation was present in men also after controlling for mul-sexes. This result is in keeping with previous observations
of Petitti,14 Jorgensen,10 and Thijs.9 In the multivariate analy- tiple confounding factors (including BMI) in the multivariateanalysis. Various factors could induce gallstone formationsis this association was absent. Thus it appears to be noninde-
pendent. An identical result was observed in the GREPCO during weight reduction dieting.20 Among these, the most
TABLE 7. Age-Adjusted OR of Gallstones, and the Gallstone Disease and 95% CI by Previous Use of Aspirin or Antirheumatic Drugs
Men Women
No. Gallstones Gallstone Disease No. Gallstones Gallstone Disease
Never used 14,493 1 (Ref) 1 (Ref) 11,836 1 (Ref) 1 (Ref)°1 year 606 0.73 (0.50-1.07) 0.66 (0.50-0.90) 645 0.64 (0.47-0.87) 0.74 (0.59-0.93)1.1-5 years 727 1.08 (0.80-1.45) 0.99 (0.80-1.30) 1,027 0.80 (0.64-1.00) 0.86 (0.73-1.02)ú5 years 57 NC NC 139 0.44 (0.21-0.95) 0.76 (0.48-1.21)
Abbreviation: NC, not calculable.
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

HEPATOLOGY Vol. 26, No. 4, 1997 ATTILI ET AL. 815
TABLE 8. Age-Adjusted OR of Gallstones and the Gallstone Disease and 95% CI by Parental History of Gallstone Disease
Men WomenFamily History
Disease No. Gallstones Gallstone Disease No. Gallstones Gallstone Disease
None 12,620 1 (Ref) 1 (Ref) 10,792 1 (Ref) 1 (Ref)Mother 1,567 1.72 (1.43-2.06) 1.76 (1.51-2.05) 1,315 1.29 (1.10-1.50) 1.59 (1.41-1.79)Father 371 1.38 (0.94-2.02) 1.36 (0.98-1.88) 337 1.21 (0.86-1.68) 1.71 (1.34-2.18)Both 75 0.65 (0.20-2.08) 1.59 (0.82-3.11) 78 1.14 (0.56-2.28) 2.59 (1.62-4.12)
important are probably a reduced gallbladder contraction and father had an increased frequency of gallstones, cholecystec-tomy, or gallstone disease. Although a recall bias cannot beincreased biliary cholesterol output. To date an increased
risk for gallstones has been recognized only for rapid and completely excluded, the same results were obtained limitingthe analysis to subjects unaware of having gallstones. Bothintense weight loss.21-30 We do not believe that the men who
had followed a diet had necessarily followed an intensive genetic and environmental mechanisms could explain thisfinding.program of weight reduction. Thus our results draw attention
to dieting as a small but epidemiologically increasing risk Our data confirm previous observations of an increasedrisk of gallstones among those suffering from diabetes,13,18,52factor for developing gallstones.
Although some experiences are negative,31-33 the use of cirrhosis,53-61 or hemolytic anemia.62 Although a recall biascannot be excluded, a pathogenic role of these conditionsaspirin24,34-36 or other antirheumatic drugs37 is commonly
thought to be protective against gallstone formation, the through various mechanisms is conceivable. Diabetics couldform cholesterol gallstones more frequently because of a re-mechanism postulated being the reduction of mucus produc-
tion from the gallbladder. In our study a particularly low duced gallbladder contraction and increased biliary cholesterolsecretion. Increased biliary secretion of unconjugated bilirubinprevalence of gallstones in 139 women who took aspirin or
antirheumatic drugs for more than 5 years was evident. It might lead to an increased formation of pigment stones incirrhosis and hemolytic anemia. The associations observed inshould be pointed out, however, that the protective effect of
these drugs was not time related, because this also emerged this study with peptic ulcer (men) and myocardial infarctionor angina are more controversial. However, in these cases, too,for regular use for less than 12 months. It could be queried
how such a short period of time could exert such a prolonged a recall bias might be involved, as suggested by a lower ORin gallstones (mostly unaware of having gallstones) than inand persistent protection against gallstone formation.
Use of hypolipidemic drugs38 or oral contraceptives16,39-50 gallstone disese (which also includes subjects already submit-ted to cholecystectomy). For myocardial infarction, at least, aare thought to be a risk for the formation of gallstones. No
association was noted between gallstone disease and previous common pathogenic mechanism may be presumed.Data regarding parity lend further confirmation to the factuse of hypolipidemic drugs in the present study. Moreover,
duration and composition of oral contraceptives was not re- that pregnancy is a condition associated with an increasedrisk of gallstone disease. The mean number of pregnancieslated to gallstone disease in the univariate analysis. Indeed,
in the multivariate analysis, the association with gallstone in Italy is approximately two. If the formation of gallstonesduring pregnancy could be prevented, prevalence of gallstonedisease was negative. A recent careful review by Thijs51 of
the literature on epidemiological studies concludes that this disease in women would be reduced by approximately 20%.In conclusion, this study, performed on a very large popu-association is slight and transient. The apparent contradic-
tion between recent epidemiological studies might be ex- lation, has identified several factors that are significantly as-sociated with gallstone disease. The knowledge of these fac-plained by the fact that the association between gallstone
disease and the use of oral contraceptives emerged when high tors, and in particular BMI, serum triglycerides, slimmingdiet, family history, diabetes, and pregnancy, whether or notestrogen doses were used, whereas recent studies enrolled
women who mostly use a medium-low estrogen dose. they will be confirmed as risk factors in the ongoing longitu-dinal phase of the MICOL study, represents the essentialSubjects with known gallstone disease in their mother or
TABLE 9. Age-Adjusted OR of Gallstones, and the Gallstone Disease and 95% CI by Some Clinically Diagnosed Diseases
Disease Sex No. With Disease Gallstones Gallstone Disease
Diabetes Men 756 1.52 (1.18-1.96) 1.54 (1.24-1.91)Women 568 1.63 (1.29-2.06) 1.92 (1.60-2.31)
Cirrhosis Men 65 NC 3.15 (1.79-5.55)Women 18 NC 3.43 (1.35-8.71)
Hemolytic anemia Men 290 1.72 (1.17-2.52) 1.43 (1.01-2.04)Women 276 0.89 (0.59-1.33) 0.88 (0.64-1.21)
Myocardial infarction or angina Men 523 1.81 (1.36-2.41) 1.99 (1.57-2.52)Women 209 1.28 (0.85-1.92) 1.76 (1.30-2.38)
Peptic ulcer Men 1,976 1.30 (1.09-1.56) 1.59 (1.38-1.84)Women 797 0.67 (0.51-0.88) 0.83 (0.68-1.00)
NOTE. For each disease and sex the reference population was constituted by subjects without the disease.Abbreviation: NC, not calculable.
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

816 ATTILI ET AL. HEPATOLOGY October 1997
TABLE 10. Age-Adjusted OR of Gallstones, Gallstone Disease, gini V. Field Staff: Angelelli G, Elba, S Mossa A, Noviello M, andand 95% CI by Number of Pregnancies Petruzzi J. †VII Como. Cohort: Mozzate Divisione di Medicina In-
terna, Ospedale di Niguarda, Milano Director: G. Ideo. PrincipalNo. Gallstones Gallstone DiseaseInvestigator: Ideo G and Caspani B. Biochemical Staff: M. CavalleriField Staff: Caspani B, Molteni A, Stefini A, Molteni G B, Albonico0 1,883 1 (Ref) 1 (Ref)D, Alfieri G, Gola D, Guanziroli M, Carrara G, Snider L, Restelli G.1 2,633 0.95 (0.78-1.16) 1.17 (0.99-1.37)†VIII Ferrara. Cohort: Codigoro Istituto di Clinica Medica, Uni-2 5,024 1.05 (0.88-1.25) 1.35 (1.17-1.56)versita di Ferrara e I Divisione Medicina Arcispedale S Anna, Fer-3 2,459 1.09 (0.89-1.33) 1.37 (1.16-1.61)rara. Director: Alvisi V. Principal Investigator: Pazzi P. Biochemical¢4 1,644 1.53 (1.24-1.88) 1.70 (1.43-2.02)Staff: Guerra G and Franze D. Field Staff: Pavani F, Massari M,Putinati S, Vincenzi M, Laterza A, Ferraresi D, Caberletti I, AndreatiC, Trevisani L, Bozzolani G, Zangirolami A, Sighinolfi D, StabelliniG, and D’Ambrosi A. IX Firenze. Cohort: Poggio Caiano Istitutobasis for planning programs aimed at preventing gallstoneclinica Medica IV, Universita di Firenze. Director: Gentilini P. Prin-disease in selected or even in the general population.cipal investigators: Buzzelli G, Curradi F. Biochemical Staff: IgnestiC. Field Staff: Bandini P, La Villa L, Arena U, Smorlesi C, BonechiAcknowledgment: This article is dedicated to ProfessorC, Coletta D, Mondanelli D, Parronchi G, Mondelli L, and CalabreseLes Schoenfield in recognition of his achievements and ac-E. †X Milano Cohort: Carimate Catt. di Medicina Interna, Istitutocomplishments over the last four decades. The text was ed-di Scienze Biomediche ‘‘S. Paolo,’’ Universita di Milano. Director:ited for English by M. J. Crowley.Podda M. Biochemical Staff: Allieri V. Principal Investigator: ZuinM. Field Staff: Battezzati PM, Bertolini E, Crosignani A, De FazioAPPENDIXC, Grandinetti G, Camisasca M, Caserta C, Petroni ML, RoccucciP. †XI Modena Cohort: Modena S. Lazzaro Istituto Clinica Medica
COMPOSITION OF THE MICOL RESEARCH GROUP I, Universita di Modena. Director: Carulli N. Principal Investigators:Policy Board. Barbara L, Capocaccia L, Menotti A, Muntoni S, Loria P and Menozzi D. Biochemical Staff: Grossi G. Field Staff:
and Ricci G. Medici G, Tripodi A, Ronucci L, Montanari M, Di Donato P, IoriSteering Committee. Attili A F, Capocaccia R, Carulli N, Festi M, Digrisolo A, Iori R, Boraldi V, Gollini D, and Sacche C. †XII
D, Lalloni L, Okoliksanyi L, Roda E, and Sama C. Modena Cohort: Modena Madonnina Istituto Clinica Medica, Uni-Editorial Board. Attili A F, Capocaccia R, Carulli N, Lalloni L, versita di Modena. Director: G. Salvioli. Principal Investigator: Lugli
Okoliksanyi L, Roda E, Sama C, and Taroni F. R. Biochemical Staff: Carbonieri A and Gaetti E. Field Staff: Nasi G,Biochemical Quality Control Staff. Director: Morisi G. Staff: Bu- Tondelli E, Boccaletti B, Frignani A, Pradelli J. XIII Napoli Cohort:
ongiorno A M, Laboratory of Clinical Biochemistry, National Health Afragola Istituto Medicina Interna e Malattie Metaboliche, II Fa-Institute, Rome. colta, Universita di Napoli. Director: Mancini M. Principal Investiga-
Biostatistical Analysis Staff. Director: Menotti A. Staff: Attili AF, tors: Farinaro E and Contaldo F. Biochemical Staff: De Biase G. FieldCapocaccia R, Mariotti S, Scafato E, and Valente F, Laboratory of Staff: Maturo N, Cecere A, Fusco D, Di Biase G. †XIV Padova.Epidemiology and Biostatistics, National Health Institute, Rome. Cohort: Montegrotto T. Istituto Medicina Interna, Universita di Pa-
Echographic Standardization. Coordinators: Festi D and Lalloni dova. Directors: Okolicsanyi L and Crepaldi G. Principal Investiga-L. tors: Burlina A, Nassuato G, Zacchi G, and Rampazzo G. Biochemical
Operative Units Participating in the Cross-Sectional Field Activi- Staff: De Franchis G and Di Vitofrancesco N. Field Staff: Angelinities*. †I. Bari Cohort: Bari Clinica Medica I, Universita di Bari. G, Fragasso A, Iemmolo RM, Lirussi F, Orlando R, Passera D, Straz-Directors: Albano O, Palasciano G. Principal Investigators: Calo Ga- zabosco M, and Toso S. †XV Pietra Ligure (SV). Cohort: Pietrabrieli G, Portincasa P, and Tardi S. Biochemical Staff: Vendemiale Ligure Ospedale S. Corona, Divisione di Medicina Generale, PietraG and Velardi A. Field Staff: Baldassarre G, Belfiore A, Morelli M, Ligure. Director: G. Marenco. Principal Investigator: Marenco G.Origlia G, Palmieri V, and Vinciguerra V, †II Bologna. Cohort: Lo- Biochemical Staff: Santorirella L. Field Staff: Colombo P, Artom A,jano (Bo) Clinica Medica I, Policlinico S, and Orsola. Universita di Giudici A, Cipriani A, and Folco U. †XVI Roma. Cohort: Tivoli IIBologna Director: Barbara L. Principal Investigator: Roda E. Biochemi- Cattedra di Gastroenterologia, Clinica Medica III, Universita dical Staff: Benassi MS and Forni M. Field Staff: D. Festi, R. Frabboni, Roma ‘‘La Sapienza’’. Director: Capocaccia L. Principal Investigator:A. M. Morselli-Labate, M. C. Nacchiero, S. Parro, G. Pollini, M. Attili AF. Biochemical Staff: Pinto G. Field Staff: De Santis A, GinanniRossi, A. G. Rusticali, C. Sama, G. Tassinari, G. Cane, B. Crino, O. Corradini S, Scafato E, De Luca C, Romiti A, Cantagalli A, PortoMasiello, D. Panuccio, A. Romani, R. Romanelli †III Bologna Cohort: D, Capri R, Giuliani E, Giambenedetti F, Rosati A, Gualandi S,Brisighella Cattedra di Gerontologia, Universita di Bologna Director: and Pallotto P, †XVII Rome Cohort: Ronciglione Istituto di TerapiaProf. Descovich G. C. Principal Investigators: Dormi A and Magri Medica Sistematica, Universita di Roma ‘‘La Sapienza’’. Director:G. L. Biochemical Staff: Sangiorgi Z, Copparoni G, La Regina C, and Ricci G. Principal Investigator: Lalloni L. Biochemical Staff: AntoniniMeotti C. Field Staff: Benassi B, Borlotti ML, Cavina A, Ceccardi M, R, Cantini R, Giocca S, Mazzarella B, Pacioni F, and Zucca A. FieldCeredi C, D’Addato S, Descovich B, De Simone G, Faggioli E, Gaddi Staff: Argento G, Azzarri A, Bava L, Bucci A, Conti R, De Felici I,A, Minardi A, Matteucci A, Negro G, Rimondi S, Sisca GB, Stagni Degano D, Graziani G, Martini L, Montali A, Palombo P, PellicciaE, Vici D, Vigna M. IV Bolzano Cohort: Bolzano Divisione di Gas-
F, Prosperi G, Quattrini B, Ricci P, Ricciardi F, Santoboni G, Scarnotroenterologia, Ospedale Generale Regionale, Bolzano. Director: Do-
A, Valeo M, and Azzari L. XVIII Verona. Cohort: Verona Istitutobrilla G. Principal Investigators: G. De Pretis, S. Amplatz. BiochemicalClinica Medica, Universita di Verona. Directors: Scuro LA andStaff: Gaspa U. Field Staff: Benvenuti S, Di Fede F, Felder M, andAngelini G. Principal Investigator: Angelini G. Biochemical Staff:Ortore P. †V Cagliari Cohort: Sinnai Divisione di Medicina Interna,Zatti M. Field Staff: Antolini G, Bonioli A, Bottona E, Castagnini A,Centro per le Malattie Dismetaboliche e la lotta contro l’Arterioscle-Degani G, di Stefano G, Fratta Pasini A, Lavarini E, Montagnoli G,rosi, Ospedale Brotzu, Cagliari Director: Muntoni S. Principal Inves-Perbellini S, Pisani G, Rigo L, Rizzini P, Sandrini T, Sciortino M,tigator: Pintus F. Biochemical Staff: F. Pintus. Field Staff: Pintus P,Tallon N, Zordan D.*Mascia P, Ganga E, Ganga R, Tronci P, and Cabiddu G F. †VI
Castellana Grotte Cohort: Castellana Grotte Ospedale Spec. in Gas-troenterologia, IRCCS, Castellana Grotte Director: Giorgio I. Princi- † Cohorts who contributed to the pooled sample reported in this article.pal Investigator: Misciagna G. Biochemical Staff: Messa C and Man-
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

HEPATOLOGY Vol. 26, No. 4, 1997 ATTILI ET AL. 817
on the formation of lithogenic bile and gallstones during loss of weightREFERENCES[Comments]. N Engl J Med 1988;319:1567-1572.
1. Attili AF, Carulli N, Roda E, Barbara L, Capocaccia L, Menotti A, Okolic- 25. Everhart JE. Contributions of obesity and weight loss to gallstone dis-sanyi L, et al. Epidemiology of gallstone disease in Italy: prevalence ease. Ann Intern Med 1993;119:1029-1035.data of the multicenter Italian study on cholelithiasis (M.I.COL.). Am 26. Worobetz LJ, Inglis FG, Shaffer EA. The effect of ursodeoxycholic acidJ Epidemiol 1995;141:158-165. therapy on gallstone formation in the morbidly obese during rapid
2. Rome Group for the Epidemiology and Prevention of Cholelithiasis. weight loss. Am J Gastroenterol 1993;88:1705-1710.The epidemiology of gallstone disease in Rome, Italy, Part I. Prevalence 27. Hofmann AF. Primary and secondary prevention of gallstone disease:data in men. HEPATOLOGY 1988;8:904-906. implications for patient management and research priorities. Am J Surg
3. Rome Group for the Epidemiology and Prevention of Cholelithiasis. 1993;165:541-548.Prevalence of gallstone disease in an Italian adult female population. 28. Shiffman ML, Sugerman HJ, Kellum JH, Brewer WH, Moore EW. Gall-Am J Epidemiol 1984;119:796-805. stones in patients with morbid obesity. Relationship to body weight,
4. Rome Group for the Epidemiology and Prevention of Cholelithiasis. weight loss and gallbladder bile cholesterol solubility. Int J Obes 1993;Epidemiology of gallstone disease in Italy: comparison between a rural 17:153-158.and urban female population. Ital J Gastroenterol 1987;19:129-133. 29. Marks JW, Stein T, Schoenfield LJ. Natural history and treatment with
5. Rome Group for the Epidemiology and Prevention of Cholelithiasis. ursodiol of gallstones formed during rapid loss of weight in man. DigThe epidemiology of gallstone disease in Rome, Italy. Part II. Factors Dis Sci 1994;39:1981-1984.associated with the disease. The Rome Group for Epidemiology and 30. Weinsier RL, Wilson LJ, Lee J. Medically safe rate of weight loss forPrevention of Cholelithiasis (GREPCO). HEPATOLOGY 1988;8:907-913. the treatment of obesity: a guideline based on risk of gallstone forma-
6. Barbara L, Sama C, Morselli Labate AM, Taroni F, Rusticali AG, Festi tion. Am J Med 1995;98:115-117.D, et al. A population study on the prevalence of gallstone disease: the 31. Kurata JH, Marks JW, Abbey D. One gram of aspirin per day does notSirmione Study. HEPATOLOGY 1987;7:913-917. reduce risk of hospitalization for gallstone disease. Dig Dis Sci 1991;
7. Festi D, Lalloni L, Taroni F, Barbara L, Menotti A, Ricci G, and the 36:1110-1115.MICOL study group. Inter and intra-observer variation in ultrasono- 32. Kupfer RM, Northfield TC. Effect of sodium acetyl salicylate on choles-graphic detection of gallstones: the Multicenter Italian study on epide- terol saturation of fasting gall bladder bile, with and without chenicmiology of cholelithiasis (M.I.COL.). Eur J Epidemiol 1989;5:51-57. acid. Br J Clin Pharmacol 1983;15:114-116.
8. the MICOL group. Prevalence of gallstone disease in 18 Italian popula- 33. Cohen BI, Mosbach EH, Ayyad N, Yoshii M, McSherry CK. Aspirintion samples: first results from the MICOL study. In: Capocaccia L, Ricci does not inhibit cholesterol cholelithiasis in two established animalG, Angelico F, Angelico M, Attili AF, Lalloni L, eds. Recent Advances
models. Gastroenterology 1991;101:1109-1116.in the Epidemiology and Prevention of Gallstone Disease. Dordrecht:
34. Lee SP, Carey MC, LaMont JT. Aspirin prevention of cholesterol gall-Kluwer, 1991:37-44.
stone formation in prairie dogs. Science 1981;211:1429-1431.9. Thijs C, Knipschild P, Brombacher P. Serum lipids and gallstones: a
35. Sahlin S, Ahlberg J, Einarsson K, Danielsson A. The effect of aspirin oncase-control study. Gastroenterology 1990;99:843-849.gallbladder epithelium and bile composition in patients with gallstones.10. Jorgensen T. Gallstones and plasma lipids in a Danish population. ScandEur J Gastroenterol Hepatol 1992;4:1019-1024.J Gastroenterol 1989;24:916-922.
36. Das A, Baijal SS, Saraswat VA. Effect of aspirin on gallbladder motility11. Shinchi K, Kono S, Honjo S, Imanishi K, Hirohata T. Serum lipids andin patients with gallstone disease. Dig Dis Sci 1995;40:1782-1785.gallstone disease. A study of self-defense officials in Japan. Ann Epide-
37. Hood K, Gleeson D, Ruppin DC, Dowling RH. Prevention of gallstonemiol 1993;3:614-618.recurrence by non-steroidal anti-inflammatory drugs. Lancet 1988;2:12. Friedman GD, Kamel WB, Dawber TR. The epidemiology of gallbladder1223-1225.disease: observation in the Framingham study. J Chron Dis 1966;19:
38. Bateson MC, Maclean D, Ross PE, Bouchier IAD. Clofibrate therapy273-292.and gallstone induction. Am J Dig Dis 1978;23:623-628.13. Diehl AK, Stern MP, Ostrower VS, Friedman PC. Prevalence of clinical
39. Braverman DZ, Johnson ML, Kern FJ. Effects of pregnancy and contra-gallbladder disease in Mexican-American, Anglo, and black women.ceptive steroids on gallbladder function. N Engl J Med 1980;302:362-South Med J 1980;73:438-441, 443.364.14. Friedman GD, Petitti DB, Klatsky AL. Association of a history of gall-
40. Strom BL, Tamragouri RN, Morse ML, Lazar EL, West SL, Strolley PD,bladder disease with a reduced concentration of high-density-lipopro-Jones JK. Oral contraceptives and other risk factors for gallbladdertein cholesterol. N Engl J Med 1981;304:1394-1398.disease. Clin Pharmacol Ther 1986;39:335-341.15. Scragg RKR, Calvert GD, Oliver JR. Plasma lipids and insulin in gall
41. Jarnfelt-Sampsioe A, Eriksson B, Leissner KH, Samsioe G. Gallbladderstone disease: a case-control study. Br Med J 1984;289:521-525.disease related to use of oral contraceptives and nausea in pregnancy.16. Maurer KR, Everhart JE, Knowler WC, Shawker TH, Roth HP. RiskSouthern Med J 1985;78:1040-1043.factors for gallstone disease in the Hispanic populations of the United
42. Everson GT, McKinley C, Lawson M, Johnson M, Kern F, Jr. GallbladderStates. Am J Epidemiol 1990;131:836-844.function in the human female: effect of the ovulatory cycle, pregnancy,17. Diehl AK, Rosenthal M, Hazuda HP, Comeaux PJ, Stern MP. Socioeco-and contraceptive steroids. Gastroenterology 1982;82:811-819.nomic status and the prevalence of clinical gallbladder disease. J Chron
43. Evron S, Frankel M, Diamant Y. Biliary disease in young women andDis 1985;38:1019-1026.its association with pregnancy or oral contraceptives. Int Surg 1982;18. Diehl AK, Haffner SM, Hazuda HP, Stern MP. Coronary risk factors67:448-450.and clinical gallbladder disease: an approach to the prevention of gall-
44. Di Padova C, Campana ZG, Podda M. Cholesterol supersaturation ofstones? Am J Public Health 1987;77:841-845.bile in women during oral contraceptive use. Ital J Gastroenterol 1978;19. Stampfer MJ, Maclure KM, Colditz GA, Manson JE, Willett WC. Risk10:62-63.of symptomatic gallstones in women with severe obesity. Am J Clin
45. Grodstein F, Colditz GA, Hunter DJ, Manson JE, Willett WC, StampferNutr 1992;55:652-658.MJ. A prospective study of symptomatic gallstones in women: relation20. Bennion LJ, Grundy SM. Risk factors for the development of cholelithia-with oral contraceptives and other risk factors. Obstet Gynecol 1994;sis in man. N Engl J Med 1978;299:1161-1167.84:207-214.21. Shiffman ML, Sugerman HJ, Kellum JH, Brewer WH, Moore EW. Gall-
46. Thijs C, Leffers P, Knipschild P. Oral contraceptive use and the occur-stones in patients with morbid obesity. Relationship to body weight,rence of gallstone disease—a case-control study. Prev Med 1993;22:weight loss and gallbladder bile cholesterol solubility. Int J Obes 1993;122-131.17:153-158.
47. Bennion LJ, Mott DM, Howard BV. Oral contraceptives raise the choles-22. Yang H, Petersen GM, Roth MP, Schoenfield LJ, Marks JW. Risk factorsterol saturation of bile by increasing biliary cholesterol secretion. Metab-for gallstone formation during rapid loss of weight. Dig Dis Sci 1992;olism 1980;29:18-22.37:912-918.
48. Van der Werf SD, Van Berge Henegouwen GP, Ruben AT, Palsma DM.23. Shiffman ML, Sugerman HJ, Kellum JM, Brewer WH, Moore EW. Gall-Biliary lipids, bile acid metabolism, gallbladder motor function andstone formation after rapid weight loss: a prospective study in patientssmall intestinal transit during ingestion of a sub-fifty oral contraceptive.undergoing gastric bypass surgery for treatment of morbid obesity. AmJ Hepatol 1987;4:318-326.J Gastroenterol 1991;86:1000-1005.
49. Petitti DB, Sidney S, Perlman JA. Increased risk of cholecystectomy in24. Broomfield PH, Chopra R, Sheinbaum RC, Bonorris GG, Silverman A,Schoenfield LJ, Marks JW. Effects of ursodeoxycholic acid and aspirin users of supplemental estrogen. Gastroenterology 1988;94:91-95.
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology

818 ATTILI ET AL. HEPATOLOGY October 1997
50. Kern F, Jr., Everson GT, DeMark B, McKinley C, Showalter R, Braver- 56. Acalovschi M, Badea R, Pascu M. Incidence of gallstones in liver cirrho-sis. Am J Gastroenterol 1991;86:1179-1181.man DZ, Szczepanik van Leeuven P, et al. Biliary lipids, bile acids,
and gallbladder function in the human female: effects of contraceptive 57. La Vecchia C, Negri E, D’Avanzo B, Franceschi S, Boyle P. Risk factors forgallstone disease requiring surgery. Int J Epidemiol 1991;20:209-215.steroids. J Lab Clin Med 1982;99:798-805.
51. Thijs C, Knipschild P. Oral contraceptives and the risk of gallbladder 58. Fornari F, Civardi G, Buscarini E, Cavanna L, Imberti D, Rossi S, SholliG, et al. Cirrhosis of the liver. A risk factor for development of cholelithi-disease: a meta-analysis. Am J Public Health 1993;83:1113-1120.
52. Hanis CL, Hewett-Emmett D, Kubrusly LF, Maklad MN, Douglas TC, asis in men. Dig Dis Sci 1990;35:1403-1408.59. Schwesinger WH, Kurtin WE, Levine BA, Page CP. Cirrhosis and alco-Mueller WH, Barton SA, et al. An ultrasound survey of gallbladder
disease among Mexican Americans in Starr County, Texas: frequencies holism as pathogenetic factors in pigment gallstone formation. Ann Surg1985;201:319-322.and risk factors. Ethn Dis 1993;3:32-43.
53. Abdel Rahman HA, Hafez AS, Maymoun NM, el Gendy SD, Abdo AS, Yonis 60. Acalovschi M, Badea R, Dumitrascu D, Varga C. Prevalence of gallstonesin liver cirrhosis: a sonographic survey. Am J Gastroenterol 1988;83:AM, Abdel Aziz S. Risk factors of gallstone disease in a sample of patients
in Benha City. J Egypt Public Health Assoc 1993;68:205-227. 954-956.61. Iber FL, Caruso G, Polepalle C, Kuchipudi V, Chinoy M. Increasing54. Fornari F, Imberti D, Squillante MM, Squassante L, Civardi G, Buscarini
E, Cavanna L, et al. Incidence of gallstones in a population of patients prevalence of gallstones in male veterans with alcoholic cirrhosis. AmJ Gastroenterol 1990;85:1593-1596.with cirrhosis. J Hepatol 1994;20:797-801.
55. Conte D, Barisani D, Mandelli C, Bodini P, Borzio M, Pistoso S, Segala 62. Soloway RD, Trotman BW, Maddrey WC, Nakayama F. Pigment gall-stone composition in patients with hemolysis or infection/stasis. DigM, et al. Cholelithiasis in cirrhosis: analysis of 500 cases. Am J Gas-
troenterol 1991;86:1629-1632. Dis Sci 1986;31:454-460.
AID Hepa 0037 / 5p27$$$721 09-10-97 12:16:22 hepas WBS: Hepatology