2 The Cambodian Experience
63
2 The Cambodian Experience W. A. C. M. VAN DE PUT and I. M. EISENBRUCH CAMBODIA Along a muddy road some twenty kilometers from the town of Pursat there is a sign- board with information on psychosocial problems. We asked people about this, and were taken to the mee-phum, the village chief. He told us that this community had many problems. There were many people who felt hopeless about their lives, even so many years after the war and the Khmer Rouge regime. Some had simply given up, could not work any longer, and remained in their houses. People who were already poor became even poorer, and were even more hopeless. Other started drinking or gambling, and had violent fights at home or with others. Some were just feeling ill, could no longer care to look after their children. As mee-phum and head of the village development committee, our informant was sincerely interested in how things could get better. He had therefore been inter- ested when he was visited by two women who started talking to him about these kind of problems. They had proposed to discuss problems such as alcohol abuse, domestic violence, and feelings of hopelessness with the villagers. They had had several ani- mated discussions, and found that the presentations of the women had helped them see their problems in a different perspective. The women organized group meetings to further discuss specific problems. Some women from the village then started their own weekly ‘meetings’, and slowly people began to talk more about the gruesome events of the past and difficulties of more recent times. It turned out that this was not just causing old wounds to open, but actu- ally could make people feel better. People began to realize that they might help each other improving these conditions. A man who had now joined the discussion told us he had actually tried to stop drinking. He had not stopped completely. At times grief would still overcome him and he could not help himself but by drinking. But things had become much better now that he felt he could at least control himself to a degree. He could work again, and was better able to look after his family. The woman who then joined said she had learned a lot about emotional problems. After her husband died she started drinking heavily too. Now, she tried to 93 jong-02 10/26/01 1:40 PM Page 93
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of 2 The Cambodian Experience
2
The Cambodian Experience
W. A. C. M. VAN DE PUT and I. M. EISENBRUCH
CAMBODIA
Along a muddy road some twenty kilometers from the town of Pursat there is a sign-board with information on psychosocial problems. We asked people about this, andwere taken to the mee-phum, the village chief. He told us that this community hadmany problems. There were many people who felt hopeless about their lives, even somany years after the war and the Khmer Rouge regime. Some had simply given up,could not work any longer, and remained in their houses. People who were alreadypoor became even poorer, and were even more hopeless. Other started drinking orgambling, and had violent fights at home or with others. Some were just feeling ill,could no longer care to look after their children.
As mee-phum and head of the village development committee, our informantwas sincerely interested in how things could get better. He had therefore been inter-ested when he was visited by two women who started talking to him about these kindof problems. They had proposed to discuss problems such as alcohol abuse, domesticviolence, and feelings of hopelessness with the villagers. They had had several ani-mated discussions, and found that the presentations of the women had helped themsee their problems in a different perspective.
The women organized group meetings to further discuss specific problems. Somewomen from the village then started their own weekly ‘meetings’, and slowly peoplebegan to talk more about the gruesome events of the past and difficulties of morerecent times. It turned out that this was not just causing old wounds to open, but actu-ally could make people feel better. People began to realize that they might help eachother improving these conditions. A man who had now joined the discussion told ushe had actually tried to stop drinking. He had not stopped completely. At times griefwould still overcome him and he could not help himself but by drinking. But thingshad become much better now that he felt he could at least control himself to a degree.He could work again, and was better able to look after his family.
The woman who then joined said she had learned a lot about emotional problems. After her husband died she started drinking heavily too. Now, she tried to
93
jong-02 10/26/01 1:40 PM Page 93

help other families, and was enthusiastic about her weekly meetings with the women’sgroup. She said the new information on causes of suffering and the relation withthings that happened in the past had helped them to look again at problems and seethat something could be done. Not everything would be solved—but at least life hadbecome worth living at times.
INTRODUCTION
Cambodia had a history of violence and oppression when at the end of the1960s the country was torn apart by civil war. In 1975 the ‘Khmer Rouge’ startedtheir infamous nation-wide experiment in social engineering that has come to beknown as ‘the killing fields’. This affected every family, every community and allaspects of public life in Cambodia. Millions died, the country uprooted, religiouslife shattered and educational systems stopped. The Khmer Rouge regime of‘Democratic Kampuchea’ was toppled by Vietnamese troops in 1979, but ‘low-intensity-warfare’ continued throughout the 1980s. In the 1990s the political situa-tion slowly began to improve. After the second elections, in 1998, a process ofnormalization seems to have taken root in Cambodia, where the war has given wayto enduring poverty, the legacy of landmines, and a disastrous AIDS epidemic.
Much has been written about mental health problems of the hundreds ofthousands of Cambodians who fled to other countries (Eisenbruch, 1990a,b,1991; Boehnlein, 1985; Kinzie, 1997; Mollica, 1994). Less is known about howthe people in Cambodia cope with their experience. The authors of this chapterhad independently worked in Cambodia and were struck by the obvious psy-chological suffering of the population. In 1992, through discussions withCambodian representatives of the Ministry of Health, the Ministry of WomenAffairs, and the University of Phnom Penh, the idea for a psychosocial interven-tion program was born.
A program to implement the community mental health approach of theTranscultural Psychosocial Organization (TPO) was started in 1995, with the aimof identification, prevention and management of psychosocial problems (de Jong,1997). The program sought to develop interventions to enable people and commu-nities overcome traumatic events. In this chapter we describe the context, theimplementation and some of the results of this program. After a brief introductionof Cambodia’s recent history we sketch the cultural and social context in which weworked. We then describe how we attempted to develop and implement appropri-ate interventions that could complement the already existing local systems of care.
TRAUMA IN CAMBODIA
Cambodia is one of the many low-income countries that provided the battlefields for the cold war. It was, and still is, a rather homogenous society.
94 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 94

‘Pre-Revolutionary Cambodia was 80 percent peasant, 80 percent Khmer, and80 percent Buddhist. First, it was an overwhelmingly rural economy. Its villagesociety was decentralized, its economy unintegrated, dominated by subsistencerice cultivation. Compared to Vietnam, its villagers participated much less in village-organized activities. They were often described as individualistic; thenuclear family was the social core’ (Kiernan, 1996).
Warfare and cruelty have always been part of Cambodian history, as thebas-reliefs on the monuments of the Angkor period testify. From the perspectiveof the present day generations of Cambodians, the last decades have been a suc-cession of periods that each brought special difficulties.
Towards the end of the 1960s the whimsical Prince Sihanouk, who hadruled Cambodia as the 20th century version of the mythical-historical god-king,lost his grip on domestic developments and Cambodia was drawn into the war in Vietnam. The coup by Lon Nol in 1970 started a five-year civil war that killedat least 10% of the population. Many deaths were the effect of the Americanbombing campaigns that served little strategic purpose (Shawcross, 1979). The‘Khmer Rouge’, the sobriquet Sihanouk gave to the communist resistance in the1960s, recruited many young people from the destroyed villages. Social life wasbrought to a standstill, the eastern half of the country was destroyed and frontskept shifting. Hundreds of thousands fled to Phnom Penh, and when the city fellto the Khmer Rouge in April 1975, the people welcomed them vaingloriously assaviours from this horrible war.
‘Democratic Kampuchea’, as the country was formally named, turned outto be an unprecedented experiment in social engineering while it marked theonly period between 1970 and 1991 wherein the country was not at war. Thecomplete, absolute rule of the anonymous party (*‘Angkar’) over ordinary peoplewas mixed with intrigue, machination and ‘cleansing’ between factions of vari-ous revolutionary ideologies. It will always remain difficult to separate the massgraves made by Khmer Rouge cadres from the ditches used to bury the victimsof American bombs, but a total of 1.5 million is seen by many as an acceptableestimation of those put to death. This amounts to 25% of the Cambodian popu-lation of 1975.
The fabric of social life suffered under the unprecedented violence of civilwar in Cambodia, but the Khmer Rouge attempted to actively destroy it. Manypeople were killed for political reasons, but most deaths were the result of poli-cies aimed at transforming a traditional, family centered Asian society overnightinto a state-centered, self-supporting communist model (Vickery, 1984; Kiernan,1996). Urban groups exposed to hard labor in the rural areas were the first vic-tims. When communal eating was forced upon all families it was clear for allCambodians alike that the *Angkar was out for some new shape of society thatnobody could imagine or understand. Pagodas were destroyed. Monks weredefrocked and forced to marry. Traditional healers were used simply for their
THE CAMBODIAN EXPERIENCE 95
jong-02 10/26/01 1:40 PM Page 95

knowledge of herbs—but as servants, breaking the respect they had in villages.Mass marriages were arranged between men and women selected by the party.Families were torn apart. Many of the young Khmer Rouge cadres were givenpositions of authority over much older people, with a ‘license to kill’. Traditionalrituals were debunked by new party rituals. Traditional Cambodian life as peo-ple knew it was almost snuffed out.
On 7 January 1979, after 3 years, 8 months and 20 days, the state ofDemocratic Kampuchea was thrown over by Vietnamese troops. The horrors ofthe Khmer Rouge regime came to the attention of the world as refugees startedarriving in Thailand. Although clear signals about what was happening inCambodia had been given before (e.g. Ponchaud, 1978), there was now a world-wide outcry about the massive scale of terror and the enormous number of vic-tims. The scope of events seemed unique, autogenocide was coined as a term,and the ‘killing fields’ became famous.
Cold war logic made the Khmer Rouge, the enemy of the Vietnamese, anacceptable ally for Western powers for another eleven years. Aid was organizedfor refugees in camps at the border between Cambodia and Thailand. The ‘border camps’ housed up to 350,000 refugees until the repatriation of 1993. Ahuge variety of programs were set up by many international organizations inthese camps, while Cambodia itself remained unaided by the West, supportedinstead by Warsaw Pact countries (Myslewic, 1988).
The world fabricated an explanation of what had happened, and this‘Standard Total View’ (Vickery, 1984) reduced the complex Cambodian reality toa story of a harmonious, innocent, self-supporting society, made up of smiling people, that was suddenly disrupted by the terror of a group of barbarous commu-nists. It allowed all those for whom it was politically convenient to see the rule ofthe Khmer Rouge as a breach in timeless Khmer history. The context of a longexistence of cruelty in Khmer history and the more recent effect of the massivebombing campaign of the United Sates in 1972–3 escaped attention. The reliefand rehabilitation programs in the border camps, and later on in Cambodia,unconsciously adopted such a view. The representation of the suffering of theCambodian people in books, films and aid-programs was filtered through this two-dimensional version of reality. Thus a picture was built of Cambodians beingvictims of one of these extreme yet incomprehensible cases of ‘Asian cruelty’.
Meanwhile, in Cambodia, the Vietnamese control of the country causedintense fear amongst the population. Cambodian masters over decades hadlabelled the Vietnamese as the archenemy of the Cambodian people. Manyexpected no less than total eradication. Khmer Rouge guerillas penetrated deepinto the countryside and had bases everywhere. In the infamous K5 projectsmany Cambodians were dragooned by Vietnamese to build a fanciful bamboowall to keep out the Khmer Rouge in deforestation projects in highly malaria-endemic and mined areas—many did not survive.
96 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 96

Low intensity warfare continued to harass the population even after apeace agreement was brokered between the parties in Paris in 1991. A massivepeacekeeping, elections-enforcing and disarmament intervention by the UnitedNations in 1992–4 did not succeed in disarming the parties, but brought backthe refugees from the Thai border and organised elections in 1993. The coalitionpatchwork government blew up in July 1997.
The Khmer Rouge was holding out along the Northern and Eastern bor-ders. Within months of exposure and show trial in a jungle makeshift court roomby his former generals, Pol Pot expired in April 1998. Weeks later, twenty-threeyears after they had taken control of Cambodia, the Khmer Rouge ceased toexist as a military force. Elections were held in 1998, and at the time of writingCambodia has a government that seems to be the most stable since the time ofSihanouk in the 1960s.
The Need for a Cambodian Perspective
Cambodian history is complex and tragic. In order to find out whetherCambodian people could be helped to help themselves, one has to understandthe country, the culture, and its people at various levels. The orchestrated waythe Vietnamese authorities organized ‘days of hate’ and fabricated politicalexplanations strengthened the tendency of individual people to refer to ‘standardhistories’. This safe representation of what had happened to Cambodia as awhole served to avoid political risk, while there was little interest among familiesin details of what had happened to others. In understanding problems of peoplewe had to discover ‘local histories’. Some people considered the civil war and themassive bombarding a more difficult period than the Khmer Rouge years.Others suffered more after the fall of Pol Pot, when they were caught betweenwarring factions at the Thai border or were forced to join the ‘K5’ projects.
What are the coping mechanisms of all those that still function—how dopeople cope with loss, and what do they believe to be causes of illness and mis-fortune? When people try to explain how they have coped with the loss of achild, cultural concepts such as the ‘former mother’—the mother of the baby inits previous life who may reclaim the baby—are essential to know what peoplemean. And when people talk about hope, desperation, suicide, guilt, anger andacceptance, one needs to know what is meant.
THE CAMBODIAN EXPERIENCE 97
Foetal and Neonatal Death
People in rural areas have few options to avoid the loss of children and must believe in somecosmic and physical reality to make sense of the spectre of high infant mortality. Healers offerhope and a system of response for parents who would otherwise remain totally helpless in facingthe prospect of such loss.
jong-02 10/26/01 1:40 PM Page 97
Traditional beliefs and traditional healers of many kinds are essential in offeringpeople at least a thread of continuous identity in the massive turmoil that threat-ened their existence and their culture. Any intervention aimed at alleviation ofpsychological suffering needs to be complementary to—and at an absolute mini-mum, informed about, the work of these healers.
Coming to a full understanding of Cambodian tradition and culture is notthe objective of the project in Cambodia. The idea was to build a shared under-standing between the Cambodian and international members of the team.Based on literature, but much more on everyday conversations and workingexperience with villagers, we have tried to use these insights in the design ofinterventions. We will attempt to describe aspects of psychological and social suf-fering in Cambodia before we turn to these interventions.
PSYCHOSOCIAL AND MENTAL HEALTH PROBLEMS
In discussions with families throughout Cambodia everyday problems areeasily related to the events of the past. People who have given up hope andstopped functioning in the sense of being able to do their daily tasks are knownto all. Those that started drinking too much after the loss of a beloved one are tobe found in any village. Domestic violence is widespread. Sleeping disorders,recurrent nightmares—it is all so common that it is not seen to be any specialproblem that might be helped. Families with more severe problems in copingwith traumatic events of the past have, in many cases, lost all their possessions intheir search for help. These families are easily identified by anyone in any village.Roughly 20% of families in villages assessed were considered to be dysfunctionalby their fellow villagers, and this included anything from alcoholism to extremepoverty, from not being able to take care of children in the household to recur-rent violence, abuse or chronic disease.
These problems do not always seem directly related to gruesome events inthe past. To the outsider it even seems that many families blame past events forpresent-day problems that are found in any developing society: poverty, growingpressure on available land, a bad harvest or the impact of modern media on
98 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
Whether a fetus dies in utero or the infant dies in early life, the general term used is ‘dis-eased child’ (*?aarih koon). Usually, the postpartum ‘diseased child’ refers to one of two main sub-types. In the first, the child suffers from ‘child not harmonious’ (*koon min kaap). In the secondsubtype, in which the child died at the hands of ancestral spirits or its preceding mother, the con-dition includes ‘disease of the preceding mother’ (*?aarih mdaay daem) or as *‘skan of the disease ofthe preceding mother’. For the most part the healers attribute the child’s illness to defects in itsmother.
jong-02 10/26/01 1:40 PM Page 98

traditional values. The link between historical and social events and present dayindividual problems is easier understood when the effect of decades of civil war andsocial upheaval are taken into account, in a society that as such has been the focusof destruction. Whatever the material destruction wrought by bombs and artillery,the Khmer Rouge’s aimed target was destruction of traditional social, family andreligious life—resulting in a much deeper crater in the Cambodian psyche.1
In Cambodia the whole population, and not merely selected groups, livedthrough the years of horror. Only age might be used to distinguish betweengroups with different levels of exposure to traumatic experiences. But while somepeople are still haunted by memories of events that date back to the 1940s,others have experienced traumatic events recently, as the case of Vanna shows.
THE CAMBODIAN EXPERIENCE 99
Case: Older Woman in Kandaal Province
… After discussing the aim of our work with a teacher in (the village) the team was directedto an older lady named Vanna who was living opposite his house. According to the teacherVanna had problems, because she went bankrupt. The team found her in the space under hertraditional Khmer house. She had never left her house since she went bankrupt, some monthsago. Her business, transporting goods from the village to the market by oxcart, went bankruptafter one of the oxen she bought with borrowed money died. There was no more income, soVanna had to sell the other ox and the cart in order to pay her debts, and than still she owedmore money. She felt ashamed about that, and told us that she did not want to walk through thevillage anymore. Vanna belonged to a well-known family, her father had been the governor ofthe district when she was a young girl, and she felt awful about having lost everything.
When the team asked how she started the business she told that she needed an extra sourceof income after her son had married and went living with the family of his wife. She had twoother sons and a teenager daughter. Two years ago her elder son’s life ended upon standing of alandmine in the forest close to the village. Her younger son, still living with her, was severelymutilated in the same explosion, and his handicap rendered him almost unmarriageable. So shefelt she could not refuse when a family in the village offered to marry their daughter to him with-out asking a dowry—even though she felt the marriage might not be right. Her mind remained preoccupied with the landmine-accident that had changed so much. What still hurts her is how
1The destruction of religious, ritual and family life challenged people’s basic values and worldviews.In trauma-theory, this should lead to a compensatory search for meaning, which, when frustrated,leads to psychological and physical distress. Various theoretical approaches to explain the occur-rence of stress disorders include the use of a behavioral conditioning framework, or a focus on apsychodynamic perspective, or an information and emotional processing model, or a constructivistperspective, while others explore the social dimensions of people’s responses to traumatic events interms of the loss of resources (Meichenbaum, 1995). In all these theories ‘meaning’ is an essentialconcept: people need to rebuild their worldview in order to overcome trauma. The search formeaning has been made virtually impossible by the continuity of dramatic episodes in Cambodianhistory.
jong-02 10/26/01 1:40 PM Page 99

Assessing Psychosocial Problems by Participatory Action Research
The assessment of real problems for real people in villages was part of thetraining of the project team (see below). In assessing families and individualsshort versions of a more extensive battery of instruments were used, and thisenabled the construction of a culture-specific questionnaire used in a survey. Thefinal instrument included sections on demographics and social position, the ill-ness and health seeking history of the individual and the family, a narrativereport on personal history, traumatic events and coping styles. Sections of theWHO Composite International Diagnostic Interview (CIDI) were included.2
A specially developed instrument was used to gather data on how theCambodian people themselves would describe, explain and classify their prob-lems.3 In recording symptoms and signs, vernacular descriptions of the patient,the family, and traditional healers were used, in an attempt to avoid imposingwestern categories and which would be extrapolated to unreliable and invalidEnglish-Khmer translations of constructs of emotional experience and behavior.
Beyond the familiar categories of events as they are often listed in traumaquestionnaires, we asked for events that are typical for the situation inCambodia. This includes dead, sick or missing relatives, marital and family
100 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
she was not able to be with her son when he died. When the news of the accident came to thevillage, some neighbors took Vanna to the pagoda, to be with the monks who would know ‘howto keep her calm’. Her sons were brought to the hospital. When she heard about the accident sheran to the hospital, although the monks had warned her not to go. She saw her sons, and whenshe came out of the hospital, she was so confused that she did not pay attention and was hit by acar. After some days in the hospital recovering from her wounds she was brought back to thepagoda. The villagers had brought her there in the first place because they remembered herstrong emotional reaction in 1977, months after her second husband had been arrested byKhmer Rouge cadre (her first husband was killed by bombs in 1973). He had been too criticaland was accused of being a spy. After some months Vanna saw him pass by as a prisoner on anoxcart. She was upset and angry with the militia, and villagers had trouble controlling her—which they needed to do for her own safety. After Vanna’s husband came back from prison hewas a broken man and died a few months after the Vietnamese invasion. Faced with the burdenof bringing up the children on her own, her work kept her from thinking too much about thelosses suffered. She had to ‘keep going’. But when Vanna’s sons were blown up by the landmine,everything fell apart for her. Now, being bankrupt, she could not avoid thinking about all thathad happened to her, from the time her father was killed before her eyes by the ‘Khmer Serei’faction when she was only a small child in the late 1940’s. Vanna’s father was an important man,a chief of the district. The family had barely survived that loss. She could have never guessed, atthat time, that it was only the beginning.
2The probe flowchart was adapted to the Cambodian setting.3The Mental Distress Explanatory Model Interview was developed earlier, and adapted for this survey, by Dr. I. M. Eisenbruch.
jong-02 10/26/01 1:40 PM Page 100

related problems, gambling and domestic violence, social problems with neigh-bors or in-laws, and the presence of landmines and having land-mine victims inthe family. These are ‘new’ events, in the sense that they did not belong to therange of life-events to be included in a normal life pattern before the civil warstarted in 1970. The complex structures of many families in Cambodia, forexample, is a reflection of past traumas (forced Khmer Rouge marriages, lostrelatives who returned later, widowhood) and more recent traumas (abandon-ment of wife and small children by breadwinner). Poverty is a constant stressor,especially in the rural areas.
Qualitative information was gathered through group discussions and in thenarratives of the people met in the village where the teams set out to work.Group interviews were done in about a hundred *phum (villages) throughout thecountry. Topics included the history of these specific communities during differ-ent episodes, composition of the population, changes in daily life, and problemsthat were important for the villagers. Coping styles, idioms of distress, healingrituals and explanations for suffering were discussed in focus groups and in-depthinterviews with key informants such as healers, monks, village leaders, teachers,youth and elderly villagers. Next to the narrative section in the survey, patients(about 1,400 at the time of doing the survey) seen in the five clinics supported by the program throughout the country added information about the personalexperience of people who stayed in Cambodia, or had come back.
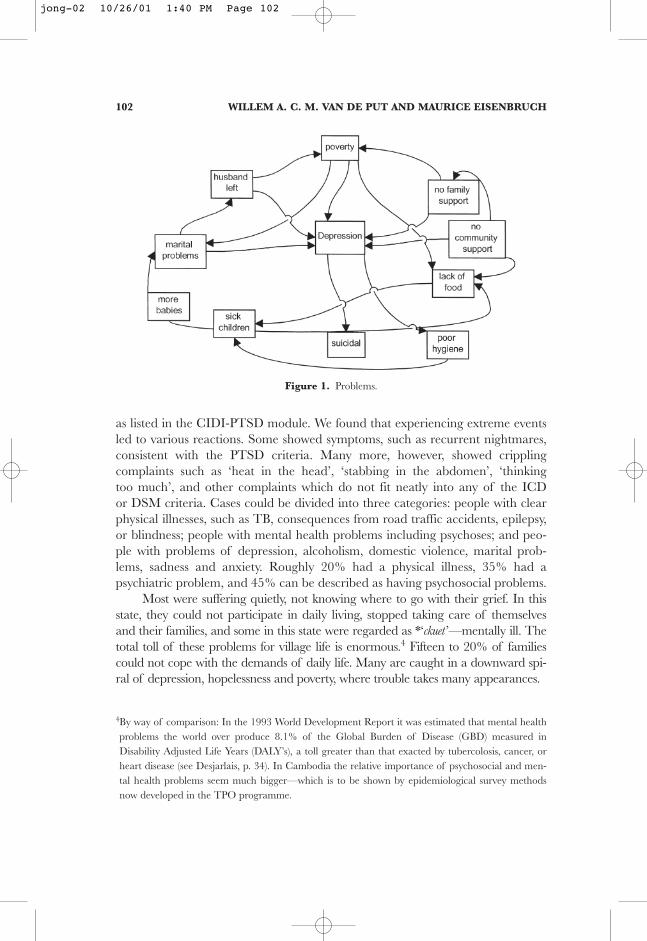
The survey was undertaken in three different districts throughout Cambodia.A team of especially trained interviewers accessed and conducted interviews inmore than 650 families. The age range in the survey was from 16 to 65. About half the total population of Cambodia is younger. A study into Cambodian per-ceptions of illness in children shows that many problems (Figure 1) in this field arenot easily recognized (Eisenbruch, 1994a). The overall majority of the populationhas been through events that are considered to be traumatic on any scale so fardeveloped, and those born after civil war and social terror are growing up in asociety where practically everyone has to cope with terrifying events.
This whole process of preparing the instruments and doing the survey helpedto identify and understand personal and community problems, and to select thehuman resources with which to work (as referral potential, or as trainees). Theresearch outcomes also provided basic knowledge needed for the development ofmonitoring instruments, and was instrumental in selecting specific areas of atten-tion and specific target sub-populations in the villages. The documented group dis-cussions, individual interviews, and observations of healing sessions recorded onvideotape, were used for training sessions with the core group.
In documenting the personal narrative of the cases, we took care not to pre-configure the trauma or to assume it to be a punctuation of their life historyduring the Pol Pot years. The villagers defined their problems themselves. We didnot find any respondent who did not experience at least several traumatic events
THE CAMBODIAN EXPERIENCE 101
jong-02 10/26/01 1:40 PM Page 101
as listed in the CIDI-PTSD module. We found that experiencing extreme eventsled to various reactions. Some showed symptoms, such as recurrent nightmares,consistent with the PTSD criteria. Many more, however, showed cripplingcomplaints such as ‘heat in the head’, ‘stabbing in the abdomen’, ‘thinkingtoo much’, and other complaints which do not fit neatly into any of the ICDor DSM criteria. Cases could be divided into three categories: people with clearphysical illnesses, such as TB, consequences from road traffic accidents, epilepsy,or blindness; people with mental health problems including psychoses; and peo-ple with problems of depression, alcoholism, domestic violence, marital prob-lems, sadness and anxiety. Roughly 20% had a physical illness, 35% had apsychiatric problem, and 45% can be described as having psychosocial problems.
Most were suffering quietly, not knowing where to go with their grief. In thisstate, they could not participate in daily living, stopped taking care of themselvesand their families, and some in this state were regarded as *‘ckuet ’—mentally ill. Thetotal toll of these problems for village life is enormous.4 Fifteen to 20% of familiescould not cope with the demands of daily life. Many are caught in a downward spi-ral of depression, hopelessness and poverty, where trouble takes many appearances.
102 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
Figure 1. Problems.
4By way of comparison: In the 1993 World Development Report it was estimated that mental healthproblems the world over produce 8.1% of the Global Burden of Disease (GBD) measured inDisability Adjusted Life Years (DALY’s), a toll greater than that exacted by tubercolosis, cancer, orheart disease (see Desjarlais, p. 34). In Cambodia the relative importance of psychosocial and men-tal health problems seem much bigger—which is to be shown by epidemiological survey methodsnow developed in the TPO programme.
jong-02 10/26/01 1:40 PM Page 102

THE CAMBODIAN EXPERIENCE 103
Lovesickness—Malevolent Power Over the Heart
Despite the apparently trivial label, lovesickness is a common and potentially serious mentalcondition. It shows the ways in which sense is made of community stress such as poverty, andsocial disharmony such as conflict in marriage. The Khmer word for love is *snae, and ‘madnessof lovesickness’ is *ckuət snae. There is the side of lovesickness in which the ritual specialist, in thiscase acting as sorcerer, *induces lovesickness. This action is known as *dak snae or ‘putting love’.The other side is the healer who acts to treat someone under the influence of a love-charm. Thisaction is known as *dah snae, or literally ‘dispelling the lovesickness’.
In Cambodia many men abandon wives and children for another woman, ‘marry her’ andhave children in another family, returning from time to time to Wife Number One, only toimpregnate her once more before wandering off again. These unfortunate women, knowneuphemistically as ‘widows’ and functionally female head-of-household, make up a big propor-tion of Cambodian villages.
At first, the victim daydreamed harmlessly about someone. In the second stage, the personfell hopelessly in love. At this stage the suitor simply craved love (or sex). Should she spurn hisardour, in vexation he hires a sorcerer to make her mad; if he can’t have her, nor will anyone else.
If lovesickness might seem a trivial issue, in which family members come to terms with tempo-rary lapses by a spouse, it can also be shorthand for potentially catastrophic family disruption.If a woman’s husband finds a ‘second wife’, the matter seldom rests there. In the course of our workwe observed commonly a pattern of a woman with young children and no husband to support them cascade into poverty (see below).
The abandoned wife, visited from time to time by her husband, is made pregnant oncemore, which only escalates her poverty when her husband next abandons her. All this com-pounds her depression and she may be driven to suicide. The combination of lack of economicmeans and social support, along with her depression and a poor level of domestic hygiene and alack of environmental stimulation for the children, can lead to malnutrition, chronic illness andpoor psychosocial development among the children. Her husband during his visits may alsobring with him the threat of syphilis and HIV/AIDS. Cambodia has an extraordinarily high rateof women as head-of-household, not simply because of a shortage of men, but because of thepattern we have sketched in this example. Lovesickness can help to frame this in local culturalterms, and shows how the traditional healers can possibly help to remoralise people who areotherwise deprived of power to influence their circumstances.
Ninety-six percent of the respondents reported exposure to at least onetraumatic event in their lives, and on average respondents had experienced 4 ofthese events. More than two thirds of respondents were exposed to several trau-matic events under Khmer Rouge rule. These events ranged from lack of foodand shelter (40%) to separation from the family (34%), to suffering from severeillness with no access to medical care (22%).
Males and females were exposed to the same extent, but age groups above22 reported significantly higher exposure. People in rural and border areasreported more events than people living in Phnom Penh. Thirty-six percentreported loss of a family member during the war and genocide, while 18%
jong-02 10/26/01 1:40 PM Page 103

witnessed the torture or murder of a family member. These numbers seem low,taking into account that many people reported torture as common practice dur-ing the Khmer Rouge time. Usually, severe torture and mass killing took place inremote areas away from potential witnesses (the ‘killing fields’). Next to that itwas highly unlikely that the person taken to torture would survive, while the KRused to kill all family members, including children, when people were listed astraitors.
Similarly, fifteen percent reported imprisonment or serious injury. Althoughthis figure seems high, it may not reflect the extent of imprisonment and tortureduring the KR time. The worst single example is the history of Toul Slengprison in Phnom Penh, where only seven survivors are known out of more than14,000 people imprisoned and killed (Chandler, 1999).
Exposure to war-related events declined after 1979. A temporal increasewas noted around 1985, which might be attributable to the ‘K5’ projects men-tioned above. Exposure to torture, injuries from landmines, imprisonment andwitnessing violence in the community still exist until the time of the study. At thebeginning of the 1980s Cambodia had a grossly imbalanced demographic struc-ture with areas where up to 65% of the population was female. In the study 29%of women were widows, or separated from their husbands, or divorced—and allthese women are called ‘widows’ in Cambodia.
Mental Disorders in Cambodia
The survey questionnaire included especially adapted cross-cultural instru-ments to measure prevalence of psychiatric disorders. The prevalence of anxietydisorder, posttraumatic stress disorder (PTSD) and major depression are ofspecific interest.
In a sample of 610 randomly selected Cambodians between fifteen andsixty-five years old, we found that lifetime prevalence of PTSD is 28%, and11.5% suffered major depression.5 In 9% of the respondents, PTSD and majordepression were present together. Disorders were more common in people whowere exposed to war events in the past or family and community violence today.Also, they are more common in older age groups than younger age groups. Theeffects of stress, grief and cognitive impairment caused by trauma were animportant risk factor for disorders. The prevalence was higher in geographicareas that witnessed more social-upheaval due to war events, as well as currentsocial structural change.
104 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
5Compared to an overview given by de Girolamo and McFarlane (de Girolamo and McFarlane,1996) these are high scores: Former political prisoners, Basoglu, 33% lifetime, 18% point; Laotianrefugees attending an Indochinese Psychiatric program (Moore & Boehnlein, 1991) 88%; Vietnamveterans formerly wounded in action (Pitman, Altman & Macklin) 32% point, 40% lifetime.
jong-02 10/26/01 1:40 PM Page 104

A quarter of all respondents reported at least one period of two weeks inwhich they felt sad or lost interest in their daily activities, and 11.5% met the criteria for at least one depressive episode (DSMIV-Major Depressive Episode).The prevalence in females was more than males (15.6% to 9.5%, chi �4.86,p � .05), and older age groups reported more depression than young. Suicide is the most serious consequence of depression and is estimated to happen in 15% of all depressed people. It is noteworthy that from all respondents inCambodia—not only the ones that scored on depression, 49.7% reported tohave been ‘thinking about death’, 20.3% reported suicidal thoughts, 14.4% hadplanned for suicide and 13.7% had actually attempted suicide.
The highest prevalence of PTSD (40%) is found in the middle-aged group(36–55). This is the group of which the youngest people were about ten years oldin 1970. One out of five of people born between 1972 and 1981 score on PTSD.The way people judge the quality of their life is not significantly related to theirscores on mental disorders.6
In the mental health clinics that were set up by the projects, it is significantthat posttraumatic stress disorder (PTSD) accounted for only 1.1% of the diag-nosis, as compared with the 28.4% found in the random sample of the popula-tion (20.6% for men, 34.2% for women). The reasons for the difference includethat people do not see signs and symptoms of PTSD as a reason to look for help(in the public health sector). As PTSD usually does not produce severe, incapaci-tating dysfunction in quite the same way as does a psychotic illness, a mentalhealth clinic would not be seen as an appropriate place to seek help. It could be expected that many with PTSD manifesting through somatic complaints(Kirmayer, 1996) would seek help in the traditional sector. They will be diag-nosed differently in the public health services, where health staff might easilyoverlook PTSD, due to the level of training and experience and the role of trans-ference as an obstruction in asking about trauma.
Forty percent of the sample showed anxiety disorder (14.4% for men,49.1% for women), and more than half of all people interviewed (53.4%) haveeither anxiety disorder, PTSD, mood disorder or somatoform disorder. Morethan one third of these people were not exposed to violence related traumaticevents. Do these high scores on concepts from western nosology point at a‘pathologic society’?
The constructs of PTSD and major depression are foreign to Cambodia.The popular Cambodian views of people suffering after the Khmer Rouge canbe summarized as ‘thinking too much’ or ‘headache’ or ‘Cambodian sickness’(Eisenbruch, 1991).
THE CAMBODIAN EXPERIENCE 105
6Based on the Cambodian adaptation of the short version of the WHO Quality of Life instrument(WHOQOL).
jong-02 10/26/01 1:40 PM Page 105

The important question may not be whether PTSD is cross-culturally validin Cambodia, but that a much deeper collective traumatization may not beexpressed as an individual complaint. Trauma tends to be pervasive, massive,chronic, complex and multilayered as the case examples show. Given the wide-spread nature of the traumatization due to war, the reactions would have cometo be accepted as a normal part of life (Somasundaram & Sivayokan, 1994). Theprevailing cultural idioms of distress including tiredness (*ohkumlang), thinking too
106 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
Madness of the Damaged Mind—A Khmer Rouge Creation?
Of all the types of mental disorders, the illness known as ‘madness of *the sa?te? ?aaram’seems to have a lot to do with stress, loss, bereavement, social and economic deprivation andfamily disruption—all of which lead to ‘thinking too much’ and to slow destruction of the mind.‘Madness of thinking too much’ was the final stage of a cascade, for which there were terms foreach stage. The person started with demoralization, literally ‘small heart’ (*tooc cət). This pro-gressed to worries, the thoughts literally ‘broken’—the term *khooc cət means literally ‘brokendown heart-mind’. This state progressed to *lap, a term implying distractibility and doubled as*lap lap to imply a progression of it. The epithet *‘aa’ is added, *aa-lap, to jeer at such a person.Further deterioration led to muddling and ‘lost and confused intellect or cognition’ (*vɔəŋveeŋsmaardəy). Anyone could have this mental state, not yet mentally ill.
A Cambodian traditional healer pays no less attention to how a person expresses thoughtsthan to what is thought. The indigenous terms for disorders of thinking have mainly to do withthe person’s speech. The healers also emphasized social context—did the speech upset people,and could they understand the person. Often, the abnormal content had to do with the Buddhistmoral code. A person’s talk was regarded as crazy if it put him outside the social fold. Patientswith thought disorders talked to themselves in rambling unrelated sentences, known as ‘no cadence or beat that bound them’. The term *rɔvəə-rɔviey refers to a scrambled series ofthoughts and, as a result, he can’t get started on anything. This thought disorder can progress to the more severe form, *vɔəŋveeŋ-vɔəŋvoan. The word *vɔəŋveeŋ on its own simply means to have lost one’s way, perhaps along the road. One difficulty for westerners in coming to grips with this concept is that the notion of *rɔvəə-rɔviey mixes disorders of thinking, perception,memory and concentration. The central feature is the social isolation and personal neglect, alongwith the gradual and chronic withdrawal and isolation. The healers are guarded in their opti-mism. They know the inexorable slide of such patients, few of whom have access to effectiveWestern antipsychotic medication, and they tend to avoid false claims (Eisenbruch, 1996). Theycan offer some calming medication, but it is not a cure. They offer some family support andcounseling.
‘Madness of the senses’ is often colored by memories of accumulating massive traumas andlosses that envelop the patient’s thinking—as indeed, of most ‘healthy’ Cambodians. A casecould be made that Cambodian ‘thinking too much’ is as much a local idiom of PTSD as ofschizophrenia, a proposition difficult to test in any war-torn society like Cambodia, which hasendured successive waves of trauma and loss over more than two decades. There is no one-to-one ‘discrete’ trauma followed by a posttraumatic reaction (Eisenbruch, 1991, 1992b, 1994a).Further work is needed to sort out the contributions, not only of PTSD, but of ongoing social-economic privation and lack of safety and security.
jong-02 10/26/01 1:40 PM Page 106

much (*kit chraen), and flashbacks of past traumas in the form of dreams andimagery which spill over into waking life (*sr amay), were so common as to beconsidered normal. Similarly the common occurrence of nightmares (71%), andwhat was termed depression or *pibak cet in 83% of Cambodian refugees in aThai border camp (Mollica & Jalbert, 1989) in apparently functioning adultscannot be considered pathological.
Summarised one could state that in Cambodia every household bears theconsequences of warfare, violence and repression. Individuals are often physi-cally and mentally scarred and have to cope with loss on many levels. Many findthemselves far away from what they consider to be their ‘home land’. In a coun-try where attachment to ancestors and their land is combined with a strongbelieve in reincarnation, it is striking to hear people say that the only hope theyhave left is not to be born as a Cambodian in the next life. Even more worryingis the significant number of people who have contemplated, and actuallyattempted, suicide, in a country where general belief holds that the very negativeconsequences of suicide have to be carried for the next five hundred lives. Peoplesee no use in talking to each other about the bad things in the past: everyone hadsimilar experiences and it is ‘better not to think about it’. ‘Good’ behavior iscomposed behavior, and when tears come, or anger, or outrage, it does not helpand isolates a person even more. People feel tired (*ah kamlang), they ‘think toomuch’ (*ki’t craen) or feel hopeless (*ah samkhum). On the other hand one findsextreme violence, lack of control mechanisms, sexual and domestic aggressionand crimes aimed at the most vulnerable people in society. In this atmosphere,sleeping disorders, nightmares, not being able to concentrate, a certain gloomi-ness covering everything, have become symptoms of normal life.
COPING IN CAMBODIA: SOCIO-CULTURAL CHARACTERISTICS
Cambodia has a wealth of indigenous ways of dealing with illness, mis-fortune, stress, poverty and conflict. Various types of healers offer help to peoplein distress. Traditional social mechanisms could help solve conflicts. Pagodas areresources for advice, help, and consolation. Public health and social care isanother potential resource for help. Currently systems of health care and socialwork are being developed and installed in Cambodia.
In order to develop sustainable and appropriate interventions, the projectaimed at strengthening the systems already in place, and made an effort to intro-duce complementary skills at the right levels, through the right people. Activeparticipation of the population is essential in installing sustainable care systems,and can only be achieved when new systems are complementary and acceptableto existing mutual support schemes.
THE CAMBODIAN EXPERIENCE 107
jong-02 10/26/01 1:40 PM Page 107

In this section we will describe the existing resources for help used bythe population, and present them in the context of special characteristics ofCambodian society. We will start with a helicopter view on society, and descentto have a closer look at the structure of communities and the world view ofpeople in these communities. In the next section we shall then explain how wemodeled interventions in accordance with the existing resources.
Understanding ‘Communities’ in Cambodia
To understand psychosocial problems in Cambodia it is necessary to con-sider long time characteristics of this society as well as present circumstances.Any separation between causes and effects where causes are defined in historical,and effects in psychological terms, is superficial. The notion that historic eventscaused the breakdown of the fabric of social life and traumatized the society asa whole is only one part of reality. The equally bitter other part is that someelements of the original structure of society gave room for catastrophic develop-ments. In thinking about community work one needs to be aware of this.
Most social scientists who have worked to any extent in Cambodia agree thatthe level of social integration in Cambodia is unique (Chandler, 1993; Delvert,1961; Ebihara, 1968; Martel, 1975; Ovesen, J., Trankell, I. & Ojendal, J., 1995;Porée-Maspero, 1962; Thion, 1993; Van de Put, 1992).7 For centuries, Cambodia
108 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
7Some quotes:
‘Que les phums soient miniscules ou qu’ils groupent plusieurs centaines de maisons, un fait apparaitcertain: 1’absence d’une communaute rurale. Pas de maison commune. Pas de terrain commune’(Delvert, 1961).
The majority of families that live in that phum will be found scattered over the rural area, usually ingroups of 8 to 12 houses. These are the ‘kroms’ (� group) that are inhabited by members of thesame family in matrilineal line. These kroms can be considered the core of social life in Cambodia,where 85% of the population lives in rural areas. Within these kroms, every nuclear family runs it’sown household. (Van de Put, 1992)
The weakness, or the outright lack of institutional links among individuals may lead someone inauthority, facing any form of challenge, to resort to immediate and violent retaliation. This is proba-bly a result of the traditional basic education, handed down from the ancient times when a majorityof the people were slaves of the rulers, which insists that authority should never, and cannot be,challenged—for any reason whatsoever. (Thion, 1993, p. 166)
Cambodian proverbs and didactic literature are filled with references to the helplessness of the indi-vidual and to the importance of accepting power relationships as they are. (Chandler, 1993–1, p. 105).
The Cambodian communal institution was far from having the same strong internal cohesion thatwas so noticeable in neighboring Vietnam. The real nucleus of the Khmer village is the pagoda.The difference in political organization is obvious at first sight even today. (Thion, 1993, p. 25)
jong-02 10/26/01 1:40 PM Page 108

was made up of families who lived scattered over the country. Nowadays peopleare found in villages (*phum), and these are often seen as the basic unit for socialchange by rehabilitation or development programs. Yet the memory of living insmaller, scattered units is vivid in Cambodia: the *phum is not necessarily anatural habitat.
In Cambodia, Thailand and Vietnam alike, as in any peasant society, accessto land is essential. Whereas pressure on the land by growing numbers of peopleforced the Thais and Vietnamese to keep up a strict system of social behavior,the Cambodians numbered far less and did not have to deal with large land-ownership until late in the 20th century. There was not the same need for com-munal organization as a collective defense mechanism as in the neighbouringcountries. The Khmers lived in scattered compounds, containing less than tenhouses. Relatives would be living together in an uxorilocal system—where hus-bands would join the families of their wives. These units of extended familieswere separated by dense forest.
Beginning under the French administration, people were forced to rebuildtheir houses following orders for relocation given by subsequent regimes, whileDemocratic Kampuchea reorganized public space completely. This process(Greve, 1993; Davenport, 1995) led to the clusters of houses one sees nowadaysall over the countryside, the *phums, and these cannot simply be taken as the nat-ural focus of community interventions.
To come to a better understanding of what constitutes a community inCambodia we assessed more than a hundred *phums. We looked for people andfamilies with common interests, and potential mutual benefit in relationshipswith each other. The assessments led us to distinguish between vertical and hori-zontal structures in a groups living in the same area. Vertical relationships wereto be found in any *phum between different income groups. Relative wealth waslinked to ones position in this system that was loosely structured on the basis ofkinship and links to the spiritual world in the area of birth. Horizontal relations,between people in the same income group, were less developed and less clear.
In order to identify individual people willing to work with us, composegroups willing to collaborate, organize effective self-help groups and to assess thepresence of vulnerable families, we found it was useful to distinguish betweenthree different types of *phums. There are ‘old’ *phums where a number of fami-lies have managed to stay together over time, without ‘newcomers’. Having expe-rienced hardships as a group, mostly related, there is a sense of continuity andsolidarity. Here people would have their social networks mainly intact, and tradi-tional healers could be accessed by all. Nevertheless, in these phums people havenot found ways of helping each other cope with extreme emotions. In thesephums interventions such as psycho-education sparked initiative and group dis-cussions had considerable impact on the coping strategies used, as we will discussbelow under ‘community interventions’.
THE CAMBODIAN EXPERIENCE 109
jong-02 10/26/01 1:40 PM Page 109

Another type is the *mixed phum, where ‘new’ people joined the old core ofrelated families.8 In these *phums it was effective to create bonds between theolder and newer groups by ‘re-installing’ traditional links between people in needand traditional resources.
A third type is the ‘new’ *phum. Created often for returnees, or, in the1980’s, for families in need of new land to work on, or, in the 1970’s, for reasonsof security and control, psychosocial problems are often serious in these *phums.Yet there is limited access to traditional resources, because healers, leaders andteachers do not belong to the same group. In these phums it was important tobring together people with shared interests, who would not necessarily have pre-vious contact between them. Interventions such as psycho-education, group workand individual counseling were then productive per income group.
To understand the context of psychological suffering and some natural cop-ing styles in Cambodia, we will narrow our focus and ‘zoom in’ to have a moredetailed look at life within these *phums.
Order and Hierarchy. Amidst all confusion and chaos in Cambodiasince the end of the 1960s it is essential to realize that Cambodian cosmology isbased on strict order. This order is normative, and translates in a hierarchicalsociety. Order is preserved by proper behavior, by acting and behaving accordingto ones role in social life. Order is contrasted with wilderness. The well arrangedorder (*robab rap roy) and the wilderness (*prey) marks the difference between theuntamed forest, the wild, and the cultivated, civilized, the predictable, thearranged (Chandler, 1996). The word for ‘normal’ is the same word for ‘to be’(*chea), and is the same word for healing. One gas to strive for order, and keep thedangerous wilderness at bay.
This importance of order, of respect for hierarchy, of the careful balance inman-occupied and cultivated land and wilderness, helps to explain the impact offorced relocation from cities and villages to ‘the fields’ or ‘the forest’ that hap-pened all over Cambodia in the Khmer Rouge time. It also clarifies the literalmeaning of being ‘marginalised’ when the poorest are always to be found in theoutskirts of any community—far away from the ordered center, close to the eviland danger of the unordered wilderness. And it stresses the importance of the‘right behavior’ and the position of the ‘self ’ in Cambodian cosmology.
110 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
8New people were the people who had been ordered to leave the cities by the Khmer Rouge, versusthe ‘old people’ who were supposed to be the original, real Khmer peasants in the rural areas.
Violations of Codes of Conduct
There are disorders which are caused by violations of conduct: by people against theirancestors, by healers against former masters (*koh kruu), or by misconduct, or by marital or com-munity dysfunction (*ckuət cue cambuə). Acute psychotic reactions can be involved.
jong-02 10/26/01 1:40 PM Page 110

Fixed Roles and Choice in Relationships. The core of Cambodianvalues delineates proper conduct, proper for one’s position in society. There is acomplex set of rules and regulations for the right behavior. One needs to knowhow to play the role of the mother, the father, the son, the cousin, client, orpatron. Hierarchy is a condition for order, and prevails in interpersonal relations.An example came in a conversation with a high ranking official in the ministry ofjustice, who had been beaten and abused when he was in prison just a yearbefore. When asked about any feelings of revenge to his abusers who were nowhis subordinates, he was surprised and said he would take action against themonly when they stopped their abusive behavior towards prisoners—for thatwas how they were supposed to act. The role prescribes and justifies behavior.Tortures need not be revenged, as long as they were part of an overall imposedsystem. But immediate revenge is in place when ones role is mocked, when one isinsulted in public, made ridiculous by people who have no right to do so.
This is not a unique Cambodian characteristic—one finds it in any Asiansociety. The special Cambodian characteristic is related to the above-mentionedlevel of social integration. Not being forced by socio-economic circumstancesto develop and maintain relationships based on mutual dependency, there hasalways been a choice in engaging in certain relationships. Within any existingrelation the rules are strict, but one can choose not to engage in that relation-ship—without the consequences that would lead to social exclusion in Thailandor Vietnam.
THE CAMBODIAN EXPERIENCE 111
Magical Action Illness—Malevolent Power to Harm the Body
At the level of the village and community, individuals and groups inevitably come into con-flict, reflected in the category of illness called ‘magical action’ or ‘magical human intervention’.Modernisation, bringing in its wake complications in work, marriage and sexual relations,induces its own forms of social strain, and ‘referrals’ to traditional healers because of sorceryshow no signs of decreasing. With the loss of the predictable social structure imposed by
The person’s own ancestral spirits, the *cue cəmbuə may induce madness of the ancestralspirits when they invade a person or withdraw their protection against spirits from the lowerworld. It is often brought on by relapse in conduct and the patient may know it. If, for a example,a young single woman commits a sexual indiscretion, she is violated but so is her family, includ-ing her ancestors. In retribution, her ancestral spirits makes her or her father mad. The *kruu willdiagnose it as caused by the ancestral spirits (remember how an individual problem will alsoaffect the family, and eventually the community).
Ancestor madness seems to be grouped in three types. It can be based on genetic inheri-tance, or on violations of expected codes of conduct and respect towards parents and ancestors,or on punishment inflicted by spirits for similar violations.
jong-02 10/26/01 1:40 PM Page 111

Shifting Social Values, Growing Individual Confusion. The age-old notion of order, and the certainty that comes with obeying the order, is shift-ing. As long as roles where clear, there would be certainty on when they wereplayed rightly or wrongly. The change in the last decades brought the need fornew roles and new definitions to Cambodia.
Correct behavior was and still is important in social life. People adjustbehavior, language, and appearance, to the status and role they have in relationto people in their company. Codes of conduct are important, and we have seen
112 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
communism, and the advent of UNTAC and a market economy, the social strain went up and sodid the level of accusation. One might say, ironically, that where sorcery is replaced as a meansto blow off social strain, it is replaced by a tendency towards indiscriminate or disproportionateviolence—two friends playing cards, or a married couple, suddenly in disagreement, and oneblowing the other to bits at point blank range with a B-40 rocket launcher.
The common Cambodian disorder known as ‘magical human interference’ relates to whatis usually described as sorcery. It is a key marker of social and domestic disharmony and, at thesame time that its ritual treatment acts to restore social harmony. Beyond that, what psychiatristsmight term as psychosomatic or somatoform disorders could be interpreted by the patient andfamily as a sign of a community disorder and, if not promptly treated, can turn into a chronicdisability, misunderstood and misdiagnosed by western health services.
Magical sorcery is common in Southeast Asian societies. In Cambodia, magical humanintervention leads to the acute onset of bizarre and socially disruptive behavior that, it wouldseem, can be ameliorated by the healer. The common signal that alerts the patient is a dream,which notifies him that something magical is in the process of invading his house, or his body—and the full-blown physical and mental symptoms follow the next day. The hallmarks of peoplesuffering from magical human interference are swelling of the abdomen and, too, migratorystabbing pains.
One can blame magical action initiated by people—as opposed to spirits—if community rela-tionships break down. The terms make sense according to the agent (non-human or human); themechanism (invading spirits, a spell, or projected foreign bodies); the physical effect (disrupted bodyelements, causing swelling; pain, caused by the effects of foreign objects).
The healers are unconcerned with localizing the culprit. The resolution of communityproblems does not call for that and, more important than showing the victim who had done himin, the community has to see the sick person reintegrated in the course of the healing ritual.
A dramatic condition calls for a dramatic solution. This illness is the leitmotif of communityrivalries and jealousies—and healers, as part of the community, cannot escape professional rival-ries. The protagonists avoid the local healer, preferring to travel to a healer further away wherethey can reveal their problems with less chance of local gossip getting back to family and neigh-bors. For their part, patients who have been troubled by multiple episodes of ‘magical humanintervention’ say that they have visited many healers in different localities, and no one, patient orhealer, seems perturbed.
‘Illness of magical human interference’ is one of the most common disorders identified byhealers. Whereas ‘ancestral spirit disorders’ can give rise to a variety of secondary illnesses, ‘mag-ical human interference’ seems to be a result of trouble between the victim and someone in theircommunity. The use of magic to induce illness reflects a need by people to control their socialand personal environment.
jong-02 10/26/01 1:40 PM Page 112

THE CAMBODIAN EXPERIENCE 113
many clients for whom breaking the code of conduct was the origin of their ill-ness (‘incompatibility of sleeping’ or *toah damneek—see below). The traditionalhealers can only be powerful (that is, effective) only if they follow their codes ofconduct. At the same time, such adherence has to be maintained in a societywhich seems to be ‘on the loose’ as a whole.
Whereas patronage, kinship, and the religious obligations used to organizesocial life in the past, short-term mutual interest between individual families isnowadays acting as an organizing principle for community life.9 The relative iso-lation in which extended families lived made avoidance a rational alternative tocomplex systems of ‘conflict management’, and while heads of families used totry to limit the consequences of smoldering conflict, nowadays these mechanismsfor social control have disappeared in many villages.
Domestic Violence
As an example of change in response to problems one may look at the problem of domesticviolence. Little is known about the prevalence of domestic violence before 1975, but informantstold us that in the past, excessive brutal behavior within the family would not be tolerated. Peoplewho were able to put a stop to it were the elderly, provided that the original infrastructure of thevillage would be intact. People like the *aacaa, the Buddhist ritual assistant and functionary in thepagoda, had real authority in the village, and could use their influence with heads of the families(of which they themselves would often be one) to end unacceptable breaches of conduct.
In the turmoil between 1970 and 1979 traditional uxorilocality was disrupted. Nowadayseconomic factors are decisive in deciding whether a newly married couple will live close to her orhis parents—if there are parents (Nepote, 1992). This has consequences for the resources avail-able to the women that end up in the village of their husbands—especially so if the marriagebreaks down or the husband dies. Going ‘home’, back to their village of origin, is not a realoption, since the woman is not seen as the responsibility of her kin once she found a husbandand another place to live. As one village leader commented about his frustration at seeing howhis son-in-law used physical violence against his own daughter, who lived with her husband’s par-ents: ‘there is nothing I can do. They were married, with my consent. The husband is her master.I cannot interfere’.
Thus a rather ‘natural’ protective mechanism in favor of women has disappeared, and isnot replaced by an alternative. Where there used to be the safety-net of well known and oftenrelated resources for help for the woman, such as the traditional healer and the *aacaa, nowadaysmany widowed or abandoned women find themselves living in an environment where they ‘donot belong’.
9See Thion, 1993, p. 152: kinship relations seem to be modeled on patron–client relationships, andused to promote individual ambitions.
Once we understood these mechanisms, we were able to find solutions forthese problems. Women in distress could be linked to resources in their villages(see case study below). Repairing these traditional links was at once one of themore appreciated and successful interventions of the Cambodian project team,
jong-02 10/26/01 1:40 PM Page 113

114 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
as an illustration of the usefulness of a ‘new approach’ to well known problemsin traditional settings.
Much confusion results from the loss of role models and the balance whichneeds to be found by each individual between playing his role in traditional,strictly hierarchical Cambodian society and the present day chaos. AssessingCambodian community from this angle helps in interpreting the use—or thelack—of social networks in coping, while at the same time providing the neces-sary background information to develop community level interventions.
Why would all this be important? First, it sheds light on the complex knot ofcause-and-effect in recent Cambodian history. This ‘looseness’ in relationshipswas strengthened through the upsetting civil war in the early 1970s, while theKhmer Rouge went further and actually forced people to see themselves as indi-viduals without any social responsibility but to the ‘Angka’—the ‘organization’.Assuming responsibility for even family members or friends was enough forinstant execution. There is an uncomfortable continuity in the loose structure oftraditional society (Evers, 1969, 1980), the age-long absolute rule by a distantmonarch, the lack of models for conflict resolution and lack of societal capacityfor organized resistance to totalitarian control. It could be argued that the suc-cess of the Khmer Rouge, a movement that numbered probably no more thanabout 60,000, mostly adolescent members, in mastering a society of 6 million foralmost four years, has much to do with this fragmented character of society.Traditional bonds of trust between people were fragile, which in itself allowedthe Khmer Rouge to destroy these fragile bonds even further.
Second, this forced erosion of bonds between people in Cambodia seemsrelated to the difficulty in making sense of what has happened and creating newcoping mechanisms. The traditional ways of living together have changed sooften and so quickly, that there has been no time to find new rules. In many casespeople found that as soon as warfare would cease to be the common threat, inse-curity would come from within the community.
The political order imposed by the Khmer Rouge regime did not replacethe old cosmological order—here continuity reached its limits. In traditionalsociety order and hierarchy was balanced by a minimum of social responsibilityand cohesion. People who had fled the last stronghold of the Khmer Rouge in1997 had secretly continued performing the rituals explicitly forbidden by theirnew leaders for almost thirty years.
The Cambodian Self. The Western concept of the self is described as‘… a bounded, unique, more or less integrated motivational and cognitive uni-verse, a dynamic centre of awareness, emotion, judgement, and action organizedinto a distinctive whole and set contrastively both against other such wholes andagainst its social and cultural background. … is a peculiar idea within the contextof world cultures’ (Geertz, 1983). Cambodian culture constitutes another percep-tion of the self.
jong-02 10/26/01 1:40 PM Page 114

THE CAMBODIAN EXPERIENCE 115
Then point here is not that Cambodia would be a ‘collectivist’ society as con-trasted to an individualistic society (Kirn, Triandis, Kagitcibasi, Choi & Yoon,1994). Cambodians individuals do not see themselves as ‘set contrastively’ againsttheir social and cultural background, but rather think of themselves in terms of thesum of their relationships and ambitions. Relationships include family, friends,colleagues, authorities as well as relationships with the spiritual world. As shownabove, the individual strives to lead a life following the roles that have been pro-vided by birth. But at the same time it is personal ambition that defines each indi-viduals choice in which relationships to engage in—and which not.
Karma and Reincarnation. The worldview of individuals people isshaped by the classical Theravada Buddhist doctrine as much as the beliefs inthe supernatural world (Choulean, 1986). These beliefs are seamlessly woventogether, and influence people’s ambivalent responses to misfortune, poverty,psychosocial misery and mental disorders. An illustration of this effective mix-ture of religious doctrine and animistic beliefs is the fact that the *neak tha, thespirit that is a symbol of man’s domestication of the wilderness, is often pre-sented and honored in the (Buddhist) pagoda.10
The boxes on mental illness in Cambodia throughout this chapter showthat illness is contextualised by the patient’s network of family, kin, neighbors,and the general community. What stands out is the large number of polymor-phous spirits; the poor classification which straddles the world of the living andthe dead; their immaturity and childishness; their ill-defined and unpredictablerole as gatekeepers of moral behavior; and their capricious tendency to causeharm. The guardian spirits define not only where people may go in their envi-ronment, but also how they should behave. In spite of the recent modernization,the Cambodian beliefs in the guardian spirits appear to be firmly entrenchedand are perhaps the last to be relinquished as an explanation for illness.
The spiritual world is therefore very much ‘real’. Everyday decisions canoften not be taken without consulting a medium, e.g. about the right time androute for a funeral. Karma and reincarnation are important aspects in daily life,too. People know that there will be more lives, in which they will bear the conse-quences of their behavior in this life. The theoretical texts of the Theravada tra-dition offer a basis to assess the self as an active and morally responsible agent,notwithstanding the explanation of the person, the I, as only conventional truth.Ultimate truth is in impersonal elements of existence (*dhamma) (Collins, 1982).Fascinating as they are, these theoretical considerations are beyond the interest ofmost people in daily life. What counts is the effect of the belief in *kamma (badkarma) and *b’aap bon (good karma) in reincarnation in Cambodia.
The continuation of life and moral consequence may be illustrated by theexample of the survivor of the civil war and the Khmer Rouge who managed to
10Lecture Ang Choulean, July 2000, Phnom Penh.
jong-02 10/26/01 1:40 PM Page 115

116 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
become a successful businessman. This man, who does not feel the need to sharehis wealth with his parents, or other relatives apart from wife and children, seeshis survival and material success as proof of his good deeds in the past, in previ-ous lives. He managed to gather enough *b’aap bon to achieve what he hasachieved today—and in his eyes, other people must have failed to do so.
So while karma and predestiny shape the present life, actions towards capri-cious deities may push one across the knife edge, with retaliatory action possiblyresulting in misery and mental affliction. One has to be careful, and one needstraditional healers of many kinds to deal with the spiritual world—be it to knowhow to prevent misery or to deal with the effects of spiritual actions. And at thesame time, many older people devote time to ‘make merit’, to build up *b’aap bonfor the next life. Some people go live at the pagoda, temporarily or for good.The *doon chhi (buddhist nuns) are women who have chosen the spiritual life.Their quest for enlightening is an individual path, as fits exactly in TheravadaBuddhism, where the role of Boddhishatva who returns on the threshold of theNirvana to help others reach the same level of insight does not exist. Therefore itneeds to be understood that the pagoda is always there for people who choosethe religious path—but one should not assume that the monks or the *doon chhicould be turned into ‘community activists’.
Example of The Use Some Women Make of a Pagoda: The Doon Cii (Nuns)
In the north west of the country there is a fertile province, Battambang, that for many yearswas the landmine-pocked battleground for the civil war with the Khmer Rouge. Ek Phnom is adistrict of that province. In Wat Ek Phnom, a well-known pagoda, there is a group of Buddhistnuns. The teacher of the *doon cii (nuns) living here is Pun Sim, 75 years old. She was trained atWat Toul Tong, in Phnom Penh, in the 1960s and 70s. She originally came from Ek Phnom, andwas sent back there by the KR in 1975. Wat Ek Phnom was destroyed, and in 1980 she wasamong the four women who started the rehabilitation of the *Wat. A *doon cii center was started,and at some time the number of women present rose to more than 70. Women come from allover Cambodia to Wat Ek Phnom. Most of the women follow the *sel pram, (five Buddhist pre-cepts), some follow the eight Buddhist precepts, and some *sel dap (ten precepts). A monkin theory strives to adhere to the full 227 Buddhist precepts; laymen strive to observe five basicprecepts, and some lay people at certain stages of their lives, like these *doon chhi, undertake tofollow eight or ten.
There are women who stay in the *Wat for a certain period of time, and there are womenwho stay for the rest of their lives. They have all come to the Wat to make merit. Wrong deedshave to be made good by making merit at the end of life. Younger women may feel that theyhave to make merit at some point in their lives too. Many women come for three months, theLenten season. Then they go back home again, and some of them will come back for anotherthree months the next year. At *Cool Wosa (Lenten) there are more *doon cii than during the rest ofthe year, usually about 50 or 60 in Wat Ek Phnom.
Pinn Simm is the teacher. Her supreme master is Sah Matak Virihea Pok Soi, who resides in*Wat Andouk. As in *Wat Andouk, Ek Phnom also receives women who have mental health or
jong-02 10/26/01 1:40 PM Page 116

THE CAMBODIAN EXPERIENCE 117
These notions of individuality and continuity had to be acknowledged inunderstanding the suffering and coping mechanisms of individual people. Theimportance of relations with the ancestors helps to explain the suffering of peo-ple who were never able to organize for the necessary rituals at the death of fam-ily members. The notions of ‘making merit’ and the effect it may have on thenext life, as well as the certainty that no deeds will remain without consequences,are important notions in understanding psychological problems as well as poten-tial solutions. In the interventions we used these notions, as we will show below.
The Community Resources (Figure 2)
The Traditional Healing System. Healers and monks practice tradi-tional healing methods all over Cambodia. Most communes have a Buddhist
psycho-social problems. They can be helped if they want to learn about the Buddhist way of life,the rules, the codes of conduct, the explanations of suffering (*toah). Women who want to cometo the *Wat are welcome, even if they have nothing, if they are in debt. Pinn Simm said, after wediscussed our work with her, that TPO is trying to help ‘from the outside’, while the *doon ciiapproach the problem from the inside. But, she said, at *Wat Ek Phnom they also have to beginat the outside. A woman who is depressed needs to be dressed and fed, before they can startworking on the ‘inside’.
Figure 2. Problems and relevant resources.
jong-02 10/26/01 1:40 PM Page 117

118 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
pagoda and most villages have at least one healer. The label ‘traditional sector’ initself does not mean very much when the vast difference between various types ofhealers is taken into consideration. There are the Buddhist monks (*preah sang),their ritual assistants and much-respected heads of families, (*aacaa), and some-times nuns (*doon cii) in the pagoda. There are male, and sometimes female, tradi-tional healers (*kruu boran or *kruu khmer). There are female, and sometimes male,mediums (*kruu chool ruub). There are lay healers, fortunetellers, and traditionalbirth attendants (*cmap). Monks and traditional healers have often had many yearsof training and developed skills in some specialized aspect of healing. Some arerenowned, for example, for treating children’s diseases or illnesses brought on byhuman interference such as sorcery; many are experts in pharmacological treat-ment, gathering plants outside their houses, which they sometimes prepare inelaborate pharmacies. Each sort of traditional healer offers a particular targetintervention: the monks, for example, tend to focus on advice and calming peo-ple’s anxieties; the *kruu, the trained healers, provided medication and magical rit-uals to help rid people of invading spells and spirits and, through the public ritual,to reintegrate the person into the local community; the mediums, mostly women,offered an intercession with the ancestors and in this way acted as remoralizingcounselors for women who cannot face their future; the traditional birth attendants
Sick Healers
Violations of moral codes can be committed by ordinary people and by monks and *kruuwho are entrusted with the transmission of cultural knowledge. There are particular forms ofmadness associated with violation of moral codes. The *kruu’s former *guru can take his errantdisciple out of the intergenerational chain, and in the process cultural transmission is vouchsafed.These mental disorders of moral turpitude serve cultural survival by ensuring that thoseentrusted with cultural knowledge—monks and *kruu—are kept in line.
Wrong kruu, or Brahmanic MalpracticeThe most popular term for this condition was simply ‘wrong *kruu’ or sometimes as ‘mad-
ness of wrong *kruu’—if the healer fell ill with ‘wrong *kruu’ inevitably he went mad. The illnessbeing caused by the former master stationing on the head of the *kruu, it was not surprising thatthe symptoms began in the head. Generally the sick healer became disinhibited, shouting whilewalking all around the house. If no one knew how to prepare the offering, the disabled *kruu,lucid or not, would remain insane.
Nearly every healer had the same ‘emergency response’ when they felt the premonitorysigns of ‘wrong *kruu’. He or she rushed to prepare the offering and think of the good deeds ofthe former master. One had to get the angry former master on side as quickly as possible. Theoffering was called literally the ‘equipment’(*rɔəndap) for the former master, a different construc-tion than more common ways to express offerings made by people to deities.
Sickness of the Monk Who Deviated to the Left, or Buddhist MalpracticeIf ‘wrong *kruu’ is the hallmar of illness striking down the *kruu for Brahmanic malpractice,
‘madness of the dhamma’ is the equivalent for the monks for committing Buddhist malpractice.
jong-02 10/26/01 1:40 PM Page 118

THE CAMBODIAN EXPERIENCE 119
help families through difficulties around childbirth and the puerperium. All heal-ers have to follow strict rules of moral conduct.
In some provinces there are exceptionally successful healers, some based inBuddhist pagodas, whose fame extends throughout Cambodia. Some of thesemonks, and *kruu, manage up to ten or fifteen inpatients, and some healers seemore than one hundred patients per day. These healers do not claim that theycan cure all serious psychiatric illnesses, but they believe they can amelioratesymptoms in a majority of cases. For the most part, patients do not pay morethan they have to pay to visit the local hospital.
The more experienced traditional healers know their limitations and avoidtreating cases of what would be called chronic psychoses in western nosology(Eisenbruch, 1994b). They help the family to understand why a person may havedeveloped *çhkuet (literally ‘mad’) and in this way, open the door for reintegrationof the patient into the community.
A female *kruu may also work as a TBA, combining the technical skill ofmidwifery with the cosmic power of the healer, especially when it involveswomen’s illnesses. The traditional birth attendants are nearly always women.They reinforce the cultural prescriptions for pregnancy and childbirth which,when violated, are believed to lead to puerperal forms of insanity.
Mediums (*kruu chool ruub) have their clients mainly coming from considerabledistances. In their own villages, the magic of their performance may be hinderedby their personal ties to the community, while the personal character of many ofthe relational problems people take to the medium may cause them to cover some‘safe’ distance from their homes. Mediums are usually women, sometimes men.Not only do the mediums act as general psychosocial supports, but they may alsohelp to ameliorate the problems of patients afflicted by serious and acute psychi-atric derangement such as ‘magical human intervention’ and spirit possession.
The medium focuses on the management of nagging and intractable psy-chosocial problems. In serious situations, such as a woman abandoned by her hus-band for another, with no livelihood or means to raise her four small children,shunned by her local village, at the bottom of a cycle of poverty, profoundlydemoralised and depressed, the *kruu is a resource for help. The mediums, oftenwomen who experienced severe problems themselves and where then called by a
The most popular term was ‘madness of the dhamma’ (*ckuət thoa). The root cause was thatthe practitioner tried too hard, with the wrong reasons, using the wrong techniques, or with thewrong instruction, to transcend consciousness. The culprit in practicing Buddhist dhamma mayunwittingly have ‘deviated to the left’, the expression denoting a violation from the rule, set up bytheir meditation teacher.
‘Madness of the dhamma’ affected those within the orbit of the Buddhist pagoda—elderly‘nuns’, ritual assistants, those who observed the 10 Precepts, as well as the ordained monks—while living under the influence of the pagoda where the dhamma was so concentrated.
jong-02 10/26/01 1:40 PM Page 119

120 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
spirit (*yee) to serve as their medium for healing, help people to find the cause theirproblem. They relate their clients to a cosmological setting shared by client andmedium. The *yee can speak freely, through the medium, and is not tied to socialrules or etiquette. The often strict hierarchy in social positions does not apply tothe spirit. This may lead to a ‘break-through’ in communication when a familysituation seems hopelessly blocked. Relational problems can be more openly dis-cussed and sometimes solved with the help of the spirit through the medium. Thisdiscussion in itself is a special characteristic of the medium. People can talk to heror him. It is an opportunity to talk about the problems at hand, which one doesnot find easily in Cambodian society. The traditional healer or the monks knowwhat needs to be done: their social status limits verbal contact with the client.
There is at least one *kruu in nearly every village. The *kruu, like the monks,are an integral part of the community, highly respected among most villagers. Ifmonks and *kruu carry out similar healing rituals, the monks are seen to be spiri-tual healers, the *kruu the medical ones. Within the project we tried to avoid the‘category fallacy’ (Kleinman, 1977) by working as much as possible within thecultural belief system, offering medical treatment only for the more severe symp-toms or illnesses that did not find help elsewhere.
Other Resources in the Traditional Community. Traditionally, pub-lic life centred around the market and the pagoda, which was the original venue ofthe schools. Traditional resources for help included, next to the monks and the tra-ditional healers, the teachers in a village, the people involved in village associations,official authorities, or people with a special position in the *phum. The mostrespected villagers are members of the ‘pagoda committee’, and together with the*achaa, the ritual assistant of the monks who is also in the pagoda committee, thesemen are family leaders and the locus of social control. These men are also impor-tant in ‘associations’, which can be seen as models for organizing mutual support.Examples of associations and ways of working together are: the ‘pots and pansgroup’ (*samakum chaan chhnang); the funeral association; construction associations;rice bank groups, and parents associations. The presence and functioning of theseassociations is closely related to the type of *phum (see above): the closer the relation-ships between the people who make up a community (the ‘old’ *phum) the higherthe level of functioning associations. Another avenue for social support is given withthe habit of reciprocal work, usually called ‘*provas dai ’ (giving a ‘helping hand’).
There are official authorities, such as the village chief (*mee-phum) and mem-bers of the various committees. There are also informal leaders, people who arerespected, and who act as patrons for others (e.g. the *mee-kchal ). Families need torelate to the village authorities inorder to begin finding solutions for very practi-cal problems such as access to land. In case of domestic problems, some peoplemay also need the assistance of authorities, e.g. in cases of domestic violence. Allthese local resources have roles in Cambodian society, and they can be effectivein alleviating psychosocial distress.
jong-02 10/26/01 1:40 PM Page 120

The Public Health System. The Cambodian context includes resourcesbeyond those traditionally provided in the community. In assessing the potentialsolutions people might use modern systems need to be included. State providedsystems of care were weak in all respects. Ministries of women’s affairs, socialwelfare and veterans, culture and religion, and rural development existed sincethe United Nations Transitional Authorities in Cambodia were installed in 1992.It would be beyond the focus of this chapter to give a detailed overview of theefforts made in all these ministries to set up systems of care for the most vulnera-ble groups in society. What all these have in common is a fundamental lack ofmeans to effectively cater for the large target groups. In view of the efforts madeby the project to contribute to sustainable solutions for psychosocial problems,we need to make one exception here for allophatic health services. There is over-lap of course in psychosocial problems and rural and urban poverty, social exclu-sion and education. The illness metaphors and somatization used by individualsto understand their psychological suffering and find effective coping styles to alle-viate it point at the health sector as a avenue for developing effective interven-tions. We will therefore briefly sketch the health system and its problems inCambodia here, which should provide the contextual background for the inter-ventions in the health sector as they are described below.
When the Khmer Rouge took over in 1975, the one mental hospital,*Takmou, providing mainly custodial care, was closed, as were most other medicalservices. Few traditional healers and monks who had provided some care for thementally ill (Eisenbruch, 1994a), were allowed to continue. After the fall of theKhmer Rouge regime in 1979 public health care was modelled on the experi-ence in Vietnam. This effort to introduce a nation-wide system resulted in asituation where too many staff had had too little training, and were ill placedthroughout the country lacking financial means and supervision. Although thetraditional healing sector was affected by the years of war and terror, it was ableto take a central place in the options for health care after 1979. In 1995, at thetime the project started, psychiatric care was simply non-existing.
In general the health status of the Cambodian population is still among thepoorest in the world. Average life expectancy is 54.4 years, much lower than inneighboring countries such as Vietnam (61.3 years), and Thailand (66 years).Maternal mortality rate is estimated at 900 per 100,000 live births, the highest inthe region. Acute respiratory infections, malaria, and, increasingly, HIV relatedillnesses are the main causes of mortality. HIV prevalence in adults reached analarming 4% by the end of 1999, the highest in Asia, and comparable to countriessuch as Ghana and Nigeria (UNAIDS, 2000). Fertility rate with 5.2 children is,after Laos PDR, the highest in Asia (Demographic Survey of Cambodia, 1996).
There is thus a very high burden of disease in Cambodia, and still a veryweak infrastructure to address it. Seeking care in government health facilities isunattractive for most patients, because of its time-consuming and unpredictablecharacter. Staff is often absent, the waiting time is long, and when people are
THE CAMBODIAN EXPERIENCE 121
jong-02 10/26/01 1:40 PM Page 121

seen by health staff they face an often disrespectful attitude and unpredictablecosts (Van de Put, 1992).
Cambodians privately spend a lot of money to seek health care. This out-of-pocket contribution amounts to 82% of total health care expenditure, or US$33.3 per capita per year (World Bank, 1999), and constitutes with 13.2% ofGDP far more than many households can afford. One illness episode can ruin afamily, especially when they desperately need treatment with immediate effect torestore the working capacity of one of the family members. The population canhardly judge the real effect of the huge variety of health services offered in thetraditional, private and public sectors.
Utilisation of public health facilities is on average throughout Cambodia0.35 contacts per capita per year, which is dramatically below the WHO interna-tional standard of 0.60 for rural areas, and well below the contact rates asobserved in the region (World Bank, 1999). Also the number of patients admit-ted in government health facilities is low, due to the absence of staff, poorhygienic conditions, lack of drugs, etc. In 1997, no more than one third of thenecessary structures were in place, the health sector was seriously under-funded,and health staff received extremely low salaries (on average 15 USD/month—whereas average monthly household expenditure is 262 USD in Phnom Penhand 80 USD in the rural areas).
Low salaries not only makes it difficult for health workers to concentrate ontheir public duties, but also severely limits the effect of training efforts on behaviorchange in health workers. Experience in other projects since 1997 shows thattraining only yields results when combined with an incentive system that directlyrelates financial benefits with quality outcome of work. (Soeters & Griffiths, 2000).
The efforts of the project to help install basic mental health skills in inte-grated primary and secondary care (Somasundaram, Van de Put, Eisenbruch &De Jong, 1998) are described below. For now it is important to stress that peoplesuffering from the psychological consequences of stress as well as the mentally illcould only find relief within the traditional sector as described above. Therewere no alternative choices, and there was no system in place capable to deliversocial or medical services.
Coping in Cambodia and the Need for Interventions
We have presented some of the existing resources in the community withinthe context of characteristics of Cambodian culture and society. Given this vari-ety of traditional resources, one might question the need for new interventions.We will conclude the first half of this chapter by showing this need as related tothe characteristics of Cambodian coping styles. We will use the remaining part
122 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 122

THE CAMBODIAN EXPERIENCE 123
of the chapter to show how we have tried to overcome these barriers or even usesome of them in developing appropriate interventions.
Cambodian Culture. The worldview of Cambodians stresses the con-tinuous cycle of lives, the importance of *b’aap bon (good karma) in reincarna-tion, and the reality of the impact of spirits and ancestors on the environment.The importance of conducting the right rituals for the dead and the need torestore disturbed relations with the spiritual world are essential elements of cop-ing. These essential elements need to be the point of departure for any effectiveapproach to help people help themselves—it is not sufficient just to be aware ofthese beliefs. In our community approach we have stressed these elements as willbe shown below under ‘community interventions’.
Spirit Madness—Messing with the Non-human World
One has to propitiate one’s guardian spirits by making the expected offerings. But one canalso become ill if one interfered with the guardian spirits of a neighbor, even if this was doneindirectly. In this way, madness of guardian spirits shares with madness of magical action thefunction of stabilizing community relations. Trouble in the community starts at home and thehouse spirit is the detonator in the guardian spirit bomb.
Madness caused by spirits was remarkable in that the patient spoke in the strange, some-times high-pitched voice of the spirit. The most marked disturbances were in mood. They werecapable of outbursts of murderous destruction. Madness of spirits, like madness of magicalaction, tended to be an acute illness.
Before attacking the spirits, the healer had first to ‘put the patient’s mind back together’—toassemble the brain’s four body elements and to refresh the patient’s perceptions and memory(dah sa?te?). After that, he could worry about the spirits, using a sequence of Pali stanzas to tiethem up with one; expel them with one; chase them away with one; made them break up anddisperse into little pieces (*bɑmbaek) with one; dissipate them with one (*kɑmcat); stab them withone; and melt and liquefy (*rumliey) with another.
People quarrel and love, fall ill and recover, and all these human experiences, centred natu-rally on pathogenic processes in the patient’s body, invariably take place along with the involve-ment of spirits and the supernatural. To oversimplify the formula, hurt or offended ancestorscause ancestral madness; offended people cause magical human interference illness or sorcery;and hurt or offended spirits cause spirit madness.
As said, for most Cambodians traditional health beliefs still prevail.Although it was clear from the outset that the construct ‘psychosocial’ was for-eign to Cambodians, people had no difficulty in discussing the variety of prob-lems they had to deal with—in which they did not distinguish easily betweenphysical, mental or spiritual problems. Behaviour and health are embedded inbeliefs about natural and supernatural forces in the environment of the villageand the surrounding fields and forests. While traditional views on the world and
jong-02 10/26/01 1:40 PM Page 123

the according life perspective are severely shaken, the health beliefs as they areillustrated in the textboxes throughout this chapter remain the main frameworkof meaning.
This means that these health beliefs need to be taken into considerationwhen looking for additional interventions. This requires careful translation andcomparison of indigenous health beliefs and international concepts of psychiatryand psychology. A major effort was made in initial training and subsequentdevelopment of training materials to be used by others in Cambodia, as is shownbelow under ‘training’.
The traditional sector is strong in Cambodia. People in the traditional sec-tor make ideal resources for any community health programme because of therespect and familiarity given to the traditional healers in Khmer society, the rele-vance of explanatory belief systems and cosmology of the traditional sector, theacceptance by the general population, their wide availability in even the remotestvillage and the common use made of their services by those seeking help.
It would seem that the healers might act as ‘trauma therapists’ in manycountries recovering from war. Traditional healers provide a means for peopleto resolve their personal sadness and their problems in the community moreacceptable than the methods brought by the West. And more than that, thetraditional methods are themselves a way of combating feelings of cultural losscaused by ongoing modernization and development projects. As new health serv-ices take off in Cambodia, we had hoped that the healers could work alongsidethem, with no detriment to either.
Social Setting and Social Change. There are also limits to what canbe achieved by the healers within a changing society. There can be a social mis-match, an inability of the healer to deal with what was also part of her/his per-sonal experience, and a mismatch in meaning and interpretation in traditionalversus international taxonomies of illness.
On the level of a social mismatch it is important that the difference in socialstructure between villages leads to various levels of access for Cambodians to tra-ditional healers. Many people have been displaced because they have eitherreturned form refugee camps, were forcibly removed from their own land andhad no chance to go back there, or went to live in the village of a husband wholater left them. These people do not live in what should be their own, naturalenvironment. Their attachment within their communities is different, and theyoften have less access to local helpers.
More important is that all healers, whether medium, *kruu, or monk, haveshared the Cambodian history with their clients. For some of the healers theevents of the past decades have even been especially difficult, because they weretargets of prosecution (monks and traditional healers). Mediums (*kruu chool ruub)usually become mediators between the spiritual and human world at the request
124 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 124

THE CAMBODIAN EXPERIENCE 125
of a spirit who came to their assistance when they experienced severe personalproblems, often the same emotional problems as their clients have.11 While thismay actually help some of the healers to help these clients, many healers saidclearly that they felt powerless when faced by problems related to extreme vio-lence, repression and warfare.
This emotional difficulty is related to the fact that the traditional taxonomy ofproblems applied by the different healers is often ill fitted for dealing with theresults of modern warfare and extreme violence. There are examples of how heal-ers adapt their explanations and tools, but health beliefs are shifting in general,patterns of health seeking behavior are changing, and healers are now in competi-tion with other sectors that offer help. Next to a confrontation between explana-tory models this includes a more vulgar aspect: healers have to maintain theirfamilies as small independent entrepreneurs within a rapidly changing society.
The competitors from other sectors have their share of problems too. Aswas said in the discussion of the public health care system, there are manyreasons why institutional weakness prevents successful introduction of new skills.There is a clear need for integrated basic psychiatry in primary care, but at thetime the necessary conditions of a motivated, salaried and skilled staff weresimply non-existent. Yet a beginning had to be made, and below we will brieflydescribe the efforts made.
We found that there was no clear unique concept of a community inCambodia. The social turmoil of the last decades resulted in villages with differ-ent social structures. In these social structures the notions of hierarchy andimportance of order prevailed in many of the more traditional villages, while inothers different groups would have different access to local resources.
This meant we had to adapt the composition of intervention teams in dif-ferent types of communities. We also had to adapt the selection mechanisms forparticipants in group sessions, and we had to adapt the logic of using differenttraining modules in a different order in different communities. These elementsare described below under ‘community interventions’.
11A woman in Prok Da, Ponhea Leu district, was abandoned by her *Boramey, her spirit, when wecame to see her for another visit. Her spirit had been the spirit of a two year old child, who helpedher heal people for about one-and-a-half year. This woman had many problems herself, and thespirit had asked her to act as its medium in return for helping her. The *kruu chool ruub, the mediumherself, had become well known in the past months, and had seen hundreds of clients who oftencame from far to see her. But now she was tired of being a medium, and wanted the spirit to findsomeone else. She begged the spirit to leave her alone, and indeed the spirit agreed to move toanother medium. The woman knows who the new medium for this spirit is, someone in a villagenot very far from hers. Others in the village told us that the women stopped being a medium aftershe had had some problems with patients, who were not satisfied by the results of the treatmentreceived.
jong-02 10/26/01 1:40 PM Page 125

126 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
In a society ‘on the move’ rural communities are changing, and urban cen-tres change even faster. The dynamics of fast modernisation and influence ofglobal developments through the media requires new role models and mixes uptraditional patterns of respect, obedience and social control. New ‘roles’ had tobe defined for effective helpers, which would bridge the traditional requirementswith the demands of change.
This meant that the relationship between the various people able to helpothers had to be studied in order to ensure productive referral. It also meant thatespecially in individual encounters such as counseling sessions a new role couldonly be defined by developing new skills, as is further explained under ‘counseling’.
‘Helpers’ in Cambodia ask for assistance: healers as well as health staffneed assistance, sometimes for their own problems, often in dealing with theirclients. There is confusion among many of the healers about the appropriatenessof traditional concepts for modern problems. The health staff cannot cope withthe psychosocial and mental health problems of their patients. But most impor-tantly, there are the obvious needs of many individual Cambodians, families andcommunities.
THE INTERVENTION APPROACH
In February 1995 a project was started on the assumption that theCambodian people could be helped in coping with the past.12 The projectwanted to support individuals, families and communities in coping with trauma.The idea was to introduce community workers (teachers, health workers, andothers) to basic theoretical and practical knowledge in the field of psychosocialinterventions, and to develop psychosocial care as an aspect of community workand general health policy.
We formed a core group of Cambodians who were offered culturallyappropriate and relevant training, monitoring and supervision, based on thedaily experience of assessing existing problems and identifying realistic solutionsin the field of psychosocial problems in the community. We developed, testedand evaluated culturally sensitive guidelines and manuals for improved detection,assessment, management and prevention of psychosocial problems on the basisof the reached understanding with the core group.
12The project was started by the International institute for psychosocial and socio-ecological research(IPSER). In 1996 the organization changed its name to Transcultural Psychosocial Organization(TPO). The project was funded by the government of the Netherlands, and ran until November2000. Since that time, the project continues its activities as an independent Cambodia NGO: TPOCambodia.
jong-02 10/26/01 1:40 PM Page 126

THE CAMBODIAN EXPERIENCE 127
Subsequently we extended the training to other community workers. Afterbeing familiar with the curriculum and the practical work in case management,the core group was trained in didactic skills and trained others, who wereselected according to the results of the action research within the project.
In working close with the University of Phnom Penh, the project strength-ened domestic action research capacity. Students participated in the community-based activities, and their activities were incorporated in their training. Theywere also involved in various types of action research.
Interventions
We found individuals in need of mental health services, and others in needto break their social isolation. We found families in need of moral and material.There are healers and monks who are looking for ways to understand what ishappening to society, in order to be able to improve support to families in theircommunity. There are communities struggling with psychosocial problems, andindividuals and families who are looking for others a sense of community. Theprogram set out to develop interventions for these needs. In this section of thechapter we will describe these interventions and the difficulties we had in devel-oping and implementing them. The interventions can be summarized in amatrix (Table 1).
Four elements are basic in this intervention model:
1 to create awareness concerning psycho-social and mental health prob-lems, by producing appropriate materials and training local healthworkers and NGO staff in psycho-education;
2 to support community rebuilding and strengthen the existing sectors onthe basis of information on the right match between problems andresources, by installing referral potential and collaboration between dif-ferent sectors;
3 to better equip the existing resources, by offering training, based onan especially developed manual, to different groups such as teachers,health staff, healers and NGO community workers;
4 to add appropriate new resources at different levels, including mentalhealth clinics at the provincial and district level; trained villagers inteams to refer families and provide psycho-education; self-help groupswhere women and men find a ‘niche’ in village life where they areallowed to talk about their emotions.
Before we discuss these different interventions we have to elaborate on whatwas the essential method of the program: training Cambodian people. The orig-inal intention was to find a group of people with a clear interest in doing psy-chosocial work and to start practical work with these people as soon as possible.
jong-02 10/26/01 1:40 PM Page 127
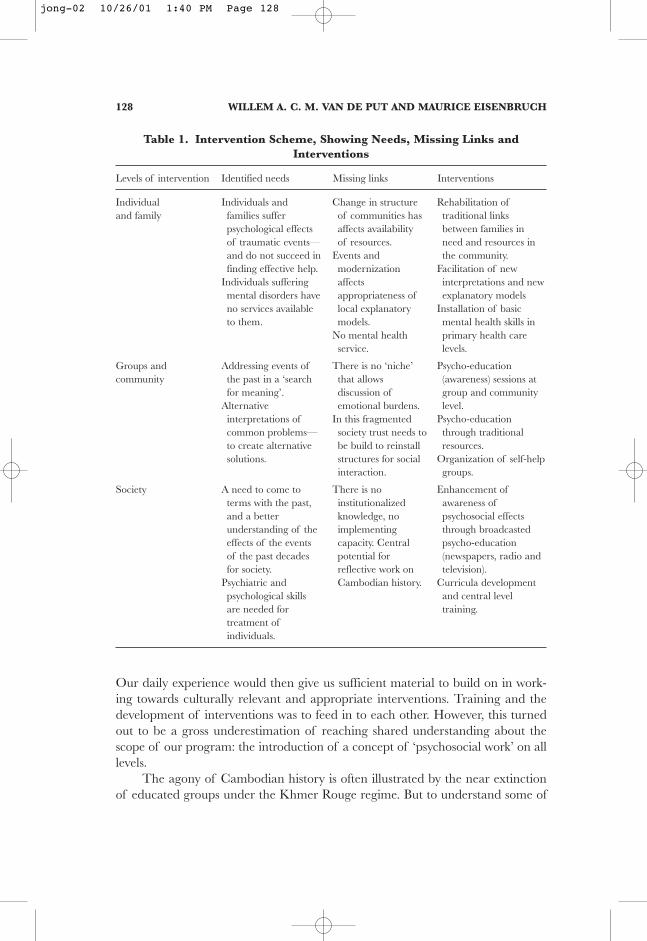
128 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
Our daily experience would then give us sufficient material to build on in work-ing towards culturally relevant and appropriate interventions. Training and thedevelopment of interventions was to feed in to each other. However, this turnedout to be a gross underestimation of reaching shared understanding about thescope of our program: the introduction of a concept of ‘psychosocial work’ on alllevels.
The agony of Cambodian history is often illustrated by the near extinctionof educated groups under the Khmer Rouge regime. But to understand some of
Table 1. Intervention Scheme, Showing Needs, Missing Links andInterventions
Levels of intervention Identified needs Missing links Interventions
Individual Individuals and Change in structure Rehabilitation ofand family families suffer of communities has traditional links
psychological effects affects availability between families inof traumatic events— of resources. need and resources inand do not succeed in Events and the community.finding effective help. modernization Facilitation of new
Individuals suffering affects interpretations and newmental disorders have appropriateness of explanatory modelsno services available local explanatory Installation of basicto them. models. mental health skills in
No mental health primary health careservice. levels.
Groups and Addressing events of There is no ‘niche’ Psycho-educationcommunity the past in a ‘search that allows (awareness) sessions at
for meaning’. discussion of group and communityAlternative emotional burdens. level.interpretations of In this fragmented Psycho-educationcommon problems— society trust needs to through traditionalto create alternative be build to reinstall resources.solutions. structures for social Organization of self-help
interaction. groups.
Society A need to come to There is no Enhancement ofterms with the past, institutionalized awareness ofand a better knowledge, no psychosocial effectsunderstanding of the implementing through broadcastedeffects of the events capacity. Central psycho-educationof the past decades potential for (newspapers, radio andfor society. reflective work on television).
Psychiatric and Cambodian history. Curricula developmentpsychological skills and central levelare needed for training.treatment ofindividuals.
jong-02 10/26/01 1:40 PM Page 128

the issues in training, developments before 1975 and after 1979 are also impor-tant. Traditional education in pagoda schools was replaced throughout the 1950sand 1960s by a government installed educational system. Historians (e.g.Chandler, 1993) have described the weaknesses of this system before 1970.Whereas the main role of education in the colonial era was preparing people totake up roles as ‘fonctionnaires’, for which little technical know-how or analyticalskills were needed, throughout the 1960s the gap between the content of educa-tion and the demands of society became clear. Some schoolteachers in PhnomPenh recoginised this in the 1950s and 1960s, and this actually marked thebeginning of the movement of which these teachers were to become leaders, theKhmer Rouge.
But also these teachers were firmly imbedded in the previously discussedhierarchical roles in Cambodia, and the traditional position of importance ofthe teacher was never questioned. This strict hierarchy made exchange of ideasor discussions between teacher and pupil unlikely if not impossible. Criticalquestions were seen as not polite—they were potentially embarrassing.
What could have gradually developed into a more modernized system ofeducation and adapted teaching and learning skills was stopped short by warfare.In the civil war years (1970–75) many people were barred from education forvery practical reasons, and after April 1975 the rice fields became the Universityfor the whole of the population, according to Pol Pot.
The subsequent presence of the Vietnamese caused fear which, howeverirrational or unjustified it may have been, had a paralyzing effect on society.The educational system had to be rebuilt amidst lack of material, lack of trainedstaff, and a deep sense of insecurity about what would happen next inCambodia. New teachers as well as students at the time found that the best wayto avoid danger was to accept what was offered with skepticism. The traditionalimportance of playing the given role in society to perfection was now turned intoa caricature. Curricula were followed strictly. The teacher would write texts fromhis textbook on the blackboard, and students would copy. The teachers wouldspeak, the students would repeat. Teaching became a ritual based on the experi-ence of the old traditional religious schools: the copying and chanting of texts.After the texts were being used this way, they became instantly meaningless.Pages from notebooks would be torn out at the end of the day to wrap food orroll cigarettes. Only empty pages represented some value: they had still to beused in the training ritual, for one day.
One of the consequences was that many people kept using the same copingstyle which had helped them to survive the Khmer Rouge era, characterized byquiet, low-profile, non-confrontational acceptance. The bureaucratic system inall levels of government encouraged reserved behavior, where one would do aswas told, follow rules and regulations, forms and protocols to the letter. Initiativewas discouraged, obedience the norm. The educational system in the 1980s was
THE CAMBODIAN EXPERIENCE 129
jong-02 10/26/01 1:40 PM Page 129

constructed in a situation where strict communist bureaucratic rules came ontop of traditional hierarchy and the experience of Khmer Rouge authority. Thisstrengthened the already existing tradition of non-critical acceptance in educa-tional settings.
The status of texts is a complex matter in Cambodian society. Secular textsare mainly seen as administrative tools of control. The detailed documentsproduced in torture centers (Tuol Sleng most notably) and the role of the pressare two examples on different ends of a continuum (Chandler, 1999; Mehta,1997). Written confessions quite obviously held no truth but functioned as thejustification of immediate killing, and the newspapers were mainly used—andtolerated—as channels for provocative and phony accusations. In both examples,the written word does not mean much. The spoken word is much more impor-tant. Truth and meaning are in the words people speak, not in the words peoplewrite. The chanting of Pali texts is important—not reading them. And this hasconsequences for training programs as well as action research in Cambodia.
In doing action research in Cambodia, language is an important tool ofcommunication, but is by no means the only aspect of it. Language itself reflectssome of the aspects of social life that are important in Cambodia, and it alsoreproduces these aspects. In every-day life Cambodia, the presentation of what issaid, or ‘how things are said’, is at least as important as the content of the message.
The role people have according to status, which shapes the conversation,can easily lead to misunderstanding. Roles of people change: a woman can be anemployee, and employer, a mother, a wife, and a daughter, and has to act accord-ingly at different times of the day. People talk in accordance with the role theytake at a specific time and place. This role influences not only what they say, butalso how they say it. The westerners ‘obsession with truth’, and the methods usedin finding, or creating a version of, the truth, are often incompatible with specificculture-bound ways of communicating.
When questionnaires are done about the needs of people, the answers caneasily be misinterpreted without anyone being aware of it. People may say yeswhen they mean no, and everybody may understand—except the interpreter-researcher at the end of the line, who feeds the answers into the computer, andreduces all meaning to digital information. Too often one finds examples ofassumptions based on superficial understanding, not only of what has been said,but also on how it has been said. Examples are studies concerning reproductivehealth (the reports say that women report an overwhelming need for contracep-tives, but in practice most women refuse to use means even when offered free intheir own house); the selection of trainees for NGO programs (incentives offeredmake it attractive for a patron in the phum to ensure that his clients benefit from these—although they may not be the implementers looked for); medicalmisinterpretation (the patient-doctor role does not allow a patient to reportcomplaints which she or he could, and would, easily discuss with the same doctor
130 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 130

THE CAMBODIAN EXPERIENCE 131
outside the medical space). Answers given to questionnaires are a mix of politeness,curiosity and specific interests. Everyday in the newspapers there are examples ofhow confusion exists about the meaning of what has been said. Not only thecontent, but the show-element of talking, the rhetoric of repetition, the ‘chant-ing’ of messages is often not picked up by the foreigner, or the Cambodianresearcher who follows ‘orders’ from the methodological textbook.
Issues of meaning and traditional learning styles have played a huge rolein the pilot phase of the project. The initial exchange of information betweenCambodian and expatriate members of the team took much more time thanexpected. The expatriate trainers noticed an inability to read with comprehen-sion, to access information, poorly developed skills in analyzing and synthesizing,a lack of concepts and perspective, a fear of not being right, and an expectationthat there were strict rules to be found which would tell the core group what todo in any circumstances. The core group members noticed a lack of languageskills, a fuzzy set of ideas about what should be done exactly, a disregard for theclassroom as the proper venue for training, and a confusing desire of wanting tobe colleagues and employers at the same time. The notion of supervision wasdifficult to distinguish from control, and especially the idea of a ‘cybernetic loopof information’, fine-tuning interventions or creating new interventions on thebasis of experience, was difficult to implement.
Thus we learned that the insights slowly gained in aspects of Cambodiansociety could immediately be applied to our own work. The general lack of trust,the silence about emotions in hierarchical situations and the extreme carefulnessin avoiding unpleasant comments in an unsafe setting were all having their effectin our daily work. It took a long time to establish the trust that allowed for inter-nal evaluation in a constructive manner.
With hindsight one easily sees the reasons for this. Basic skills such as reportwriting or planning work schedules can be taught and learned. Much more difficult and time-consuming is to first adjust to the idea that some knowledgeis not, and cannot be, precise, in the sense of technical factuality or political correctness.13 Then was has to feel comfortable enough with this idea to use accu-mulated experience and self-written reports as a basis to change interventions.
In the end, we managed to bridge the gap by applying the age-old way oflearning that seems universal: role modeling—which is how traditional healershave always been trained. The core group became more confident as they slowlyfamiliarized themselves with casework, and especially as they helped writing themanual (see below). After basic trust had been established, we found common
13Some trainees were disappointed when there were no straightforward answers to questions such as‘how many times does a woman with four dead children need counseling, as compared with awoman who has two dead children?’ Some took the reply that there is no definite, context-freeanswer to this as a sign that a better teacher was needed: someone who would know.
jong-02 10/26/01 1:40 PM Page 131
ground in the exchange of opinions and experience that led towards new initia-tives, and the development of new interventions. We used well known elementsin culture, such as stories, the traditional relations between people, and weworked with various traditional healers. The challenge was in deliberately creat-ing something new by combining older and newer elements.
In the first four months of the program, the focus was on an exchange ofinformation: the core group was introduced to mental health and psychologicalconcepts, while the expatriate team was informed on the social context andpersonal experience of problems of the heart-mind—the Cambodian expressionclosest to psychosocial problems. The core group started working in clusters ofvillages in the provinces of Kandaal, Kampong Speu, and Battambang. Practicaltraining was done in the field. The work in the villages offered new material fordiscussion and learning sessions every day. It was in this stage that mutual under-standing was beginning to grow.
Production of Culturally Competent Materials. One of the chal-lenges in the project was the production of teaching material. Next to posters,videos, radio and television appearances and verbal modules, the way to reachtrainees, health authorities, and other organizations was to develop a curriculaand texts on community mental health. Curricula for health staff were devel-oped for the Ministry of Health, according to the guidelines of the ‘minimal andcomplementary package of activities’ under the health reform plan. In these cur-ricula we could use the experience gained in endless discussions on communitymental health, in combination with international expertise on primary mentalhealth care. The most time-consuming and complicated work was in the devel-opment of a community mental health manual.
The UNHCR/WHO Mental Health for Refugees Manual (De Jong &Clarke, 1996) was used as a source of inspiration for a new manual, especiallydeveloped for the situation in Cambodia. The structure includes the most com-mon and important part of the community workers responsibility and offers acomplete range of possible psychosocial interventions to be chosen according tothe needs of the client. Although theoretically, academically and to some extentclinically, the demarcation between major (psychosis) and minor mental disor-ders (psycho-social, for which the Khmer term ‘wrecked heart-mind’ or *khooc cetis appropriate) is not all that clear cut, the distinction is helpful for teachingabout mental illness at a basic level. Subtle psychological concepts had to beintroduced for the first time and the need was for simple and clear lessons thatcould be easily understood.
Specially given the lack of skills and material in the western sector, it wasfelt to be important to include lessons learnt in co-operation and research intothe traditional sector in the manual. Thus throughout the manual there is specialattention for local idioms of distress, the locally used taxonomy of mental disorder,
132 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 132

and there is a special unit on local resources to fit the local context. In the chap-ter about relaxation exercises it was thought appropriate to introduce the age-oldBuddhist practices of mindful breathing (Ana Pana Sati) and meditation, as wellas local massage techniques.
The manual has been titled Community Mental Health in Cambodia, andexists in a Khmer and English version (Somasundaram, D. J., Kail, K., Van dePut, W. A. C. M., Eisenbruch, M., & Thomassen, L., 1997). The contents of themanual include units on helping skills, the community and its resources, stressand relaxation, psychosocial problems, major mental disorders, children, alcoholand drug problems, and epilepsy and head injury.
There were many technical problems in translating from English to Khmerand vice-versa. Many English psychological words had no equivalent in Khmer.A whole Khmer vocabulary for psychological terms had to be created. Part ofthis effort resulted in and benefited from the Psychology Dictionary brought outby the Department of Psychology, University of Phnom Penh. Some terms hadto be literally coined and short explanations included in the text.
Training using this draft was first given for the program team, who thenused the draft for training a variety of trainees, who were then followed-up toascertain what they were doing with the training. The feedback from the team,the trainees, their follow-up assessment and comments from experts in the fieldwere used to prepare the pre-final draft. Before the core group started the firstbatch of training for village workers a preparatory session of the material wasorganized. In these sessions the units were reviewed word-by-word, and the coregroup had many suggestions on the appropriate terminology, and added exam-ples based on their own experience in the villages. Back-translation was checkedagain. In this process the core group made the last steps to becoming familiarwith the units of the manual.
Field-testing the manual involved several topics. First, the selection of thetrainees is a test in itself. By follow-up and monitoring the core group checks howthe villagers saw the training, how they use this new knowledge, and how thiseffects their communities. Another point for field-testing is how to match thecontent of the manual with the different levels of education of the trainees.Different levels of understanding call for fine-tuned didactic skills and trainingstyles. Specific training in didactic skills for the core group helped them to adaptthe training to the groups selected.
On the basis of this manual the core group has been training a total ofsome 1600 people up to 1999. Training is still ongoing. The trainees are varioushealth staff, NGO staff, ministerial staff, traditional healers, formal and informalvillage leaders, other villagers and students.
We shall now turn to the interventions these people were trained in. We willbegin at the community level, and descend to the level of the individual. Thuswe can describe the work of the program in a natural order: we enter a village,
THE CAMBODIAN EXPERIENCE 133
jong-02 10/26/01 1:40 PM Page 133

134 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
identify problems, and apply interventions. When relevant we will refer to thecharacteristics we have identified in the first part of the chapter, and show howwe tried to overcome difficulties and be complementary to existing resources.
Community Interventions: Entering the Village
First contact in any community was with the local authorities, respecting theimportance of hierarchy and order. The team explains the ideas of trying tocollect information about the problems of the ‘heart-mind’ (*paññyeahaa plav cet)families are facing. The history of the particular village is discussed with some ofthe leaders at the house of one of them, and anyone standing around quicklyjoins in. Soon demarcation lines in the social structure of the *phum are clear.Especially vulnerable groups are identified, and the *phum will be one of thethree types mentioned above.
If a tight group is encountered, it is easy to contact healers and other resourcesfor help, and organize group sessions where the problems of the ‘heart-mind’ arediscussed. Materials for psycho-education have been developed, and the posters,videotapes and presentations on special modules allow people to shift the angle ofinterpretation of their daily problems. Building on the existing relations in the
husbandleft
maritalproblems
sickchildren
poverty
PagodaPagoda
Depression
no familysupport
no communitysupport
poorhygiene
lack offood
NGO
suicidal
provideinformation,
refer toservice
Healtheducation
familyplanning
aacaa, orother
resources
refer toservice,provide
information
contact ortrain
resources
contactand trainresources
Healthcare
Kruu
morebabies
refer toNGO, trainNGO staff
providecounseling
Mentalhealth
Trainhealth
workers
NGO
Figure 3. Problems, resources and interventions.
jong-02 10/26/01 1:40 PM Page 134

village, the team can begin organizing training for interested helpers in the com-munity, and group work (see below) comes almost automatically.
In mixed villages the approach has to be more careful. The different groupsare best approached separately, and the team finds out through interviews ofkey informants (teachers, village leaders, monks) what the local history is. Inthese phums building individual relationships between healers or helpers andpeople in need meant building up a sense of mutual trust that is the basis forgroup sessions. In ‘new *phum’ the most effective approach is for the team to startindividual casework and identify individuals who have common interests. Oncethey are brought together, psycho-education is given for various groups, and rela-tionships begin to be possible.
In all villages, people tell the team about the problems in either their ownfamily or direct relatives, and usually agree with the suggestion of the team to goto the house where the problems are. These initial discussions about the projectin the beginning phase of the program helped to develop material for psycho-education later on. At the house of one of the identified families, the discussionabout the problems and their causes is continued. The family is asked what wasdone to find solutions, and if possible, the informant is asked to come along tothe house, market, or hospital where help was found. There the healer, healthworker or any other resource is asked to comment upon the problem and giveher/his views about the causes and potential healing chances. Since the overallmajority of people have visited several of the health sectors, it is often possible toreconstruct the health-seeking path and see a number of the helpers involved inthe reported problem.
If possible, the next step in help-seeking behavior is followed. Sometimessuggestions are made. This involves the team actively in the help-seeking behav-ior of some patients, and allows them in other cases to be part of the search forhelp. These visits provide documented information on help-seeking behavior andcurrent beliefs in the individual, family and healer.
The next step is thus defined by the type of village entered, and can consistof either psycho-education for anyone interested, and/or individual case workaimed at strengthening local resources for help, or individual case-work thatbuilds a basis for a group approach.
We will discuss these related interventions separately, but will first presentan example of how the teams were able to successfully break through culturallymediated patterns of expectations and dependency.
Breaking the Cycle of Poverty and Depression: the ‘IsolatedWoman’. To give an example of how this works in practice, we present a caseexample of a pregnant woman whom we shall call Somaly, living in extremelypoor conditions with four children at the edge of a *phum where her husbandwas born. He had left her after the fourth child was born. He now lived with
THE CAMBODIAN EXPERIENCE 135
jong-02 10/26/01 1:40 PM Page 135
another woman, but every now and then he would come back, and Somalyalways hoped he would stay. Problems would start within a few days, however.The last time the man left, he had taken the last valuables and left her pregnantand beaten up. The malnourished and weak children did not go to school. Theyhad scabies. The woman did not have any relatives in the village. Her motherlived about 10 km away, and would sometimes visit her. The mother was in noposition to offer material support, since she hardly had enough for herself.
This woman was one of the many widows, *mee-may, a term also used forabandoned women in Cambodia. Living isolated in a village where she was notoriginally from, she belonged to a group we had come to see as one of the mostvulnerable in rural areas. She seemed to be in really hopeless situation. In thefirst flowchart, put together in the course of discussion with the team after theyhad seen the woman, one sees how the problems are all related, and how itwould not help to suppose that one problem solved at the time would not comeback quickly afterwards. The related problems are like a downward spiral, whichneeds to be stopped.
1. Problems. At first the team found it difficult to get away from theexpectations given with the roles they felt they had in this community. As peoplewith positions, jobs, and therefore rich as compared to the villagers, they felt theyshould confirm this status by giving presents. Embarrassed and shy at first con-tact because they felt ashamed for having no material support to offer, theybecame somewhat more confident when they realized how happy the womanwas when they returned for a second, and third visit. But what was to be done?One way to begin is to look for the simplest problem, and start there. One of theteam showed the woman how she could treat the scabies by washing the childrenwith water, boiled with the leaves of the tamarind tree.
The team was suspicious. Would one really have to teach the woman howto do things that were so common in Cambodia—and would she actually dothem and keep doing them? If so, more women might be in need of this simpleadvice. The traditional birth attendant (*cmab) would be the right person to dothis, as we had found in our interviews with healers. In the same vein, the grouprealized that one could relate all the different problems to different resources inthe community. There could be organizations working in the area in fields suchas health education, health care, family spacing, food programs, income genera-tion and small credit schemes. There is the pagoda, there are the traditionalhealers, the older people, teachers, the *phum leaders. All these people can beseen as resources available—if one would just know what to ask them and howto stimulate them to help. The second flowchart shows the resources related tothe problems.
2. Problems and resources. For marital problems, one can go to the *kruu.For the food situation one could look at the rice bank or other initiatives. Animportant part of facilitating interventions thus became mapping these various
136 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 136

resources. The different sectors for help need to be localised, people need to befound and asked what one could do in a situation like this.
It is possible to find the traditional sector, the public health sector, the com-munity development sector, but what is there for problems such as depressionand suicidal behavior? Many problems can be referred, but that in itself was notseen as sufficient. Some part of the problem seemed to need new interventions.There was no referral option for mental health problems of this woman in thisspecific situation. Here was a role for the program—installing basic psychiatricskills in primary care (see below). Next to that, Somaly was a ‘new person’ in this*phum, which meant no more than that none of the community leaders wererelated to her. But this severely affected her access to normal local resources.This was a typical situation of where traditional relations could be re-invented.
3. Problems, resources, and interventions. The above scheme shows theresources for the various interventions needed. Now it could be seen how theactivities of the team relate to the problems of the woman. The team kept visit-ing Somaly, and listened to her. They were themselves impressed by the effect ofthis activity, which was seen as ‘nothing’ at first, but laid the first foundation for‘talk therapy’—a modest beginning of counseling skills, something very new inCambodia (see below). The initial fear that Somaly would want to have nothingto do with them once she found there was no material support proved to bewrong.
The tip about the tamarind tree leaves worked well. The children were get-ting better. Somaly, in talking with the team, came to realize that she was not theonly one in this situation. Shame, hopelessness and the conviction that helpcould only be expected from people who were far better of had prevented herform recognizing others in similar positions. Somaly began to talk to others, andtook more care of her children. It seemed like the team had succeeded in findinga way ‘in’—breaking through the cycle of causation.
One day, her mother was visiting when the team was there. The team askedthe mother what she would have done if a similar situation had occurred whenshe was young, in the 1960’s. The mother responded that a situation such as thiswould be unthinkable then. The chief of the *phum, the older men, and espe-cially the *aacaa would not have allowed such behavior from a young man (thehusband). Somaly would have found support from the community against a manwho was clearly behaving out of bounds—and this would have been easierbecause she would have lived in her own village, where her husband had joinedher. The team then asked why Somaly would not try to go and talk to the *aacaa,but both mother and daughter said that this could not be done. When asked why,they said that they felt to be too poor to go to the *aacaa and ask his help.
Later the team visited the *aacaa and talked about his role in the phum.He was proud to have the team coming to the pagoda to talk to him, and complained that few people seemed to want his advise anymore. He felt his status
THE CAMBODIAN EXPERIENCE 137
jong-02 10/26/01 1:40 PM Page 137

138 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
as *aacaa, which used to be a respected position only open for the best of theolder men, had inflated since his father had been one. The team told him aboutthe woman, and her hesitations to come to him for advise. The *aacaa explainedthat he would be delighted to see what he could do, as long as the woman wouldrespect his position as an *aacaa and come to him—she could not expect a manof his position to go to her house to offer his support. The roles had to be playedwell. When this message was brought back to Somaly, she eventually gatheredcourage and went to see the *aacaa.
This contact was a turning point in a process of re-socialization for Somaly.Not all her problems were solved, but her isolation had become less. She nowhad contact with other women, with whom she could share work and help inlooking after the children. She was now known to the *aacaa, and had betteraccess to the pagoda and the monks. Village committees were helpful in gettingthe children to school. The vicious cycle had been broken, and was turnedupward.
In this approach we made full use of the information on explanatory mod-els used by people in distress. The explanatory models pointed the way to theright resources for help. Knowing these resources, and knowing what they didand how they could be approached, helped us bridge the gap between a womanin distress and the community around her. Knowledge on the role-play and hier-archy informed us about thresholds in accessing various resources for Somaly.The characteristics of a mixed phum helped in realizing why in this communitya special intervention was needed to restore age-old Cambodian communityrelations.
The mix of problems Somaly had to cope with reflected what we earliercalled the banality of psychosocial problems. Her problems seem no differentfrom those of many women in other countries. Yet the context in which she hadto cope with them was laden with the effects of war and the breakdown of sociallife. Her husband’s behaviour is no longer as remarkable as it was in hermother’s youth. Her social position in her village is a direct result of warfare.Her lack of access to a community and her depressed state counted for a loss ofeven the simplest folk treatments.
Flow charts as shown above, based on real experience, where used as atraining device; as the beginning of a map of a district to show where problemsand resources are; and as an inventory of intervention possibilities. Exploringsocial structures showed the most productive composition of teams of village volunteers for psychosocial work. Being offered a role as a helper for others further helped women like Somaly, and important villagers such as the *aacaafelt recognized when included. Both had a keen interest in participating in training: the women because it helped them understand and act upon their ownsituation, the *aacaa because it raised his status and gave him ideas on how tohelp others. The women were happy to do outreach work: visiting marginalised
jong-02 10/26/01 1:40 PM Page 138

families brought them social contacts. They felt safe under the protection oftheir colleagues in the ‘village team’, important people such as the *aacaa or vil-lage leader, who in turn enjoyed being consulted by families sent to them by thewomen.
Mapping local resources also brought the team to community workersinvolved in other programs. We co-operated with local and international organi-zations that implemented community development programs in many sectors.We managed to establish contact between these programs and the populationwho would benefit most of them via the local counterparts. In that way commu-nity development programs benefited from a motivated target group, while themost vulnerable people benefited from the development program. This way theproject had a preventive impact on psychosocial problems by offering people realchances to improve their well being.
The experience with Somaly showed the team that talking and listening washelpful. This notion in turn helped the team to move away from more traditionalideas of helping, which consisted mainly of providing material aid and using thehierarchical role to order behavior change.
Psycho-Education
In the approach towards the total community, in group work and in sessionswith individuals, psychos-education is essential. In the ‘old *phums’ an initialdiscussion with the village chief and the crowd that would immediately gatheraround his house was enough to set a date for a village-wide session on psycho-education. People in these villages have easy access to their local resources forhelp. The interest in discussing the ‘heart-mind’ problems was nevertheless enormous.
One important aim of psycho-education was to help people see their prob-lems in a fresh way. The vicious cycle of depression and poverty leads to a seriesof problems as shown in the case of Somaly. Unraveling this knot was a processpeople highly enjoyed in group sessions. It helped to distinguish between thedifferent aspects of a problematic situation, and made people think again aboutwhat kind of help might be available. An example is how women are affected by*toah, which can only be healed by the kruu, but at the same time have abdomi-nal problems that need medical care. Treatment offered by different sectors caneasily be complementary.
A clear example of the need for complementarity is in perinatal andpostnatal disorders. These are widespread across cultures, but little is known ofindigenous taxonomies, explanatory models, or local treatment methods used toameliorate or prevent them. The Khmer term *toah means ‘to be different’, ‘inconflict’, ‘incompatible’, or ‘to quarrel’. Perinatal disorders can be viewed aspartial solutions to sociomoral predicaments. The illnesses provide women, who
THE CAMBODIAN EXPERIENCE 139
jong-02 10/26/01 1:40 PM Page 139

have few options over how they work, eat, and cohabit, with a socially acceptable‘way out’ to signal their distress and to find partial support from the traditionalhealers. These disorders involve many symptoms, while the causes for these symp-toms are seen differently by traditional and western healers. In order to heal theperson, the symptoms as well as the cause need to be treated. Sometimes thetraditional healer may not be able to treat the symptoms. Sometimes the doctormay not be able to treat the cause.
Using posters and video material in psycho-education sessions helpedpeople look at their own problems from a slightly different angle. Domestic vio-lence and alcoholism now became symptoms of underlying causes ratherthan unavoidable facts of life. An alternative idea of causality where abnormalsituations caused normal reactions helped people think of alternative ways ofcoping, such as sharing experiences and finding help with local resources for spe-cial parts of their problems. Psycho-education helped people to make moreeffective use of available resources, and also facilitated new approaches.
Relaxation Techniques. As a practical part of psycho-education relax-ation techniques were introduced. Promoting body-awareness and encouragingthe use of body-oriented techniques like relaxation exercises and breathing exer-cises was also used in individual encounters in counseling. The following fourmethods were adapted to suit the culture and religion of the Cambodian com-munity (see also the chapter on Sri Lanka):
• Breathing Exercises. Buddhist Mindful breathing or Ana Pana Sati.• Muscular Relaxation. A variation of Jacobson’s Progressive Muscular
Relaxation, the technically similar Yogic exercise, Shanti or Sava Asanaor the Buddhist Mindful body awareness was used.
• Repetition of Words. A meaningful word, phrase or verse is repeatedover and over to oneself.
• Meditation. Various meditation practices known in Cambodia, such as*Samadhi and *Vipassana meditation were used.
Using traditional methods of massage like *Thveu Saasay to produce profoundrelaxation is both culturally familiar and effective. Therapy with relaxation meth-ods, being non-pharmacological, is safe, cheap, non-toxic and has no side-effects.
The benefits to these practices are not confined to producing relaxation.When methods are culturally familiar, they tap into past childhood, communityand religious roots and thus release a rich source of associations that can behelpful in therapy and the healing process. Although these techniques do no for-mal psychotherapy, they may accomplish what psychotherapy attempts to do byreleasing cultural and spiritual restorative processes. One way is by teaching thetraditional practices to large groups in the community, in pagodas, communitycenters, and as part of the curricula in schools. This is be promotive, preventive
140 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 140

and curative. When people come together to learn and practice these methods ina Pagoda under a senior *aacaa or monk, the atmosphere is therapeutic andsocially healing. Apart from the actual practice of the methods, people interactin a healthy way, support each other, find meaning for their problems and suffer-ing through the religious doctrines on Karma and suffering.
Staff of ministries of rural development, women’s affairs, and social welfareand NGO staff are trained in organizing psycho-education sessions. Some of themonks are eager to use parts of the manual in their chants at funerals and at otheroccasions. The core group members themselves directly reach some 5000 peopleper year in psycho-education sessions for groups. The numbers reached by min-istry and NGO staffer monks are not easily available, but should be many more.
Psycho-education was used as a means to reach groups of villagers whogathered to hear about a different way to look at familiar problems. It was alsoused within self-help groups to open discussions, and as well as a tool in individ-ual treatment. In the ‘old *phums’ one of the effects of psycho-education is aninterest in self-help groups. In the ‘new *phums’ individual case managementbuilds relationships and leads to group work.
Group Work
The group approach is not only appropriate because so many peoplerequire help, but is necessary to facilitate a joint process of coming to terms withthe past. Since problems people face are often related to a process of findingsome kind of meaning, or at least an acceptable explanation, for the events ofthe past and the present, and this calls for discussion, exchange of opinions, andmutual reinforcement. The fact that people actually help themselves, prevents anextra layer of ‘psychosocial workers’ and facilitates (re)building social networks.
In the composition of groups and the gradual transition from facilitatedgroup work to self-help groups, it is important to know the local history and thetype of village. According to Kinzie (1997) group therapy is a ‘professionally ledtherapeutic activity occurring in a group setting employing techniques varyingfrom educational to those in which specific interactional and dynamic issues areexamined’. He notes that in group therapy with Cambodian people cultural val-ues such as respect for authority, the need for smooth relationships and the tradi-tional interdependent family relationships are important in the psychotherapeuticrelationship, and would pose difficulties for a positive outcome (Kinzie, 1997).There would be no cultural analogue to the type of self-disclosure required inindividual psychotherapy in any of the Asian healing ceremonies. Asians wouldbe reluctant to speak about themselves publicly. Group processes may be lessstraightforward than in the West.
We found that a group approach to deal with problems was not only possi-ble and effective, but also embedded in culture itself.
THE CAMBODIAN EXPERIENCE 141
jong-02 10/26/01 1:40 PM Page 141

142 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
Ancestral Spirit Illness—Violations of Moral Hygiene in the Family
The transition from childhood to early adulthood is the critical period when the person’supbringing will be tested—not only in terms of how they will respond to the developmental pres-sure to become sexually active, but also whether their choice of marriage partner will be themost propitious. Any community misfortune can be traced to the couple’s miscreance, so parentshave to guard their daughters for everyone’s sake. This belief helps to explain the elaborate mar-riage ceremonies that inform the ancestral spirits that a particular couple are properly togetherand that no offence should be taken when they begin to have sex. The fit between the partnersshapes the sort of descendants they in turn will raise, so naturally their ancestors keep a watchfuleye during his phase. It is also a testing time for the parents who, after all, were accountable forrearing the children and for their character development.
The most common general term for family lineage is ‘family line’ (*puuc). Families in whichan illness run are designated ‘leprosy family’, tuberculosis family’ or simply ‘illness family’.Another popular related term is ‘family line’ or ‘family tree’ (*trɑkool) which refers to the race orthe clan. Another widely known term is ‘mum-dad ancestral spirits’ (*mee baa) which designates,too, the parents and the representatives of the bride and groom during the marriage ceremony.This term is reserved to delineate close relationships within two generations of the person.Healers have an additional vocabulary. The ‘line of the family lineage’ (*cuə cɑmbuə) takes inassumed ancestral links to a person.
In ‘wrong to the ancestral line’ (*khoh cue cɑmbue), the illness stems from the remote ancestralline some generations removed from the patient. The victim can be any direct descendant of theculprit, in any generation, with no implication that the patient has done wrong. And the prelimi-nary illness can be arrested when the victim apologizes on behalf of the family line and offeringpropitiation in apology to the ancestral spirits. In the second taxon, the illness stems from anancestral spirit one generation removed from the patient and their still-living forebears andknown in Khmer as ‘mum-dad ancestral spirits’ (*mee baa); the victim was the wrong-doer or theirparent, spouse, or sibling. The group covered domestic conflicts.
The preliminary stage of illness can be divided along several lines:
• The origin of the illness, or punishment: remote generations of the ancestral spirits ofthe family line, or the immediate ancestral sprits
• The identity of the violator of the code of conduct• Whether the victim, or the patient, was necessarily the culprit who had committed the
infraction• The clinical features of the illness• Whether there was a time limit during which the culprit could admit guilt or perform
the necessary propitiatory offerings to the ancestral spirits• Expected course and outcome (death, recovery, or chronicity).
The ancestral spirits, in their capacity as moral policemen and in withdrawing protection,leave the descendant open to the depredations, such as sorcery attack, initiated by the aggrievedfamily against him. In this way, the person’s ancestors act in concert with the community.
There are three components to the diagnosis of illness from ancestral spirits. One proce-dure, ‘augury with the chicken egg’, was used to detect who in a family group had committed theoffence, a critical question when ‘wrong to the mum-dad spirits’ was suspected, but irrelevantwhen the patient was afflicted by ‘line of illness’ because the culprit, one of the patient’s forebears,was long dead. Astrological prediction, known as (*tiey) or literally ‘seeing divination’ (*tɔəh tiey),
jong-02 10/26/01 1:40 PM Page 142

THE CAMBODIAN EXPERIENCE 143
By taking the social structures of the communities in account, and organizegroups accordingly, we could prevent some of the constraints Kinzie found.Once people have been selected from the same social strata, being in compara-ble positions, we find that sharing emotions turns out to be an enormous relief.People have to feel safe in this new setting, and begin to talk about the dailyproblems everybody shares. The facilitator helps to create an atmosphere oftrust, and uses modules of psycho-education to start a discussion about problemsof another order, the problems that cause much more emotional discomfort thenthe usual daily things.
The group sessions in Cambodia proved to provide a setting where, for thefirst time ever, people have an opportunity to talk about their emotions. Groupsof women or men need a safe setting, a facilitator who can introduce the topic,and not much more to begin a process of finding out what actually happened tothem, and why. This cannot be overestimated: in a society where any attempt to come to terms with the past has been frustrated by a complex knot of socio-cultural and political reasons, organizing group talk about the events of the pastsimply offered an excuse that was eagerly used by many to finally ‘just talk’.
was a method used to determine which ancestral spirit had been wronged and offended and hadcaused the illness, but the healer did not disclose his logical steps to the patient. In another procedure, ‘examining the healing manuals’, also employed to diagnose which ancestral spirit was angered, the patient’s personal history was important, and the patient followed the logicaldeductions used by the healer. If a person was already ill, the manuals could help explain why;if they were in good health, the manuals warned of their proneness—everyone had their Achillesheel.
TreatmentThe spectrum of ancestral spirit disorders can be treated by a ritual sequence that follows
roughly this order:General vaccination of the whole community. The calendrical ritual offerings to the ancestral spir-
its, performed on behalf of the whole community, in a ritual known as ‘erecting the pavilion’(*laəŋrɔən). This ceremony, rather than curing an individual patient, helps everyone.
Before the patient has been cured of first-stage illness. Treatment focuses on the clarification of theproblem and with appeasement through dialogue of ancestral spirits. Ritual offering to theancestral spirits, known by the general term (*saen): these rituals include calling the protectiveancestral spirit to possess the medium and reveal the nature of the patient’s offence (*bɑñcoan?aarak); and ‘feasting the ancestral spirit’ (*lieŋ ?aarak).
Immediately after the cure of the first-stage illness. Treatment focuses on termination of issues to dowith the ancestral spirit. The patient, if a promise has been made to the ancestral spirit, mustdischarge it and announce that it has been discharged (*lie bamnan). Treatment then focuses onminimizing the sequelae of the illness caused by invading wild spirits unconnected to the ances-tral line.
Follow up. Defensive manoeuvres to prevent attack by wild spirits unrelated to the ancestralspirits: these include the use of magical yantra designs.
jong-02 10/26/01 1:40 PM Page 143

In group sessions people often repeat stories from the past. It is as if the storiesneed to be repeated until they start making some sense.
Group members start offering each other very pragmatic mutual support.They help each other find work, look after each other’s children, or simplycomfort each other. This works well as long as no label is used to describe theseactivities, such as solidarity, group-work, friendship, brotherhood, or social sup-port. These terms have all been abused by one or another totalitarian system inthe past.
The group setting, which allows its participants for the first time to talkfreely about their daily emotional problems, is seen by most of them as too pre-cious to be risked by the potential problems related to communal business. Therepetition of life stories serves the purpose of finding meaning for what hashappened, and, of course, the process of rebuilding mutual trust requires time.Some of the self-help groups slowly create new networks of friends that stretchmuch farther than the *phum. And once they are connected, introduced to eachother, these networks develop quickly and start functioning as communities withmutual support. Some 2000 people are reached per year in groups facilitated byteam members. Some of these groups quickly require no more facilitation andturn into self-help groups. Others function for some time and then dissolve, butnot without having at least given people an opportunity to start building support-ive relationships. And these are used to find practical solutions leading to addi-tional income, shared responsibilities, and a sense of belonging.
Counseling
One of the most common interventions in psychotherapy and psychosocialwork is the supportive verbal contact between the helper and the client, of whichcounseling is one type. Supportive verbal contact takes place in the sessions withmediums (kruu chool ruub), and although the client contacts a supernaturalentity through the medium, the idea of verbal healing already exists in theCambodian context. The team found people also appreciated talking and listen-ing about problems without the supernatural context, and we set out to see ifcounseling techniques could be used in Cambodia.
There are reasons to question the potential use of these techniques (Van dePut et al., 1998a). People do not talk easily amongst each other about emotionaldistress. The general feeling is that one should not think, and certainly not talkabout traumatic events. They should be forgotten. Talk would open up oldwounds in the listener, and the result would just be more pain. Even in the ‘old*phums’ relatives avoid to discuss traumatic events.
In counseling sessions the client is invited to talk about her/his personal life.As said before, the quality of a life has much to do with the perfection of playingones role according to now it should be’. Legends and stories provide a mold to
144 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 144

THE CAMBODIAN EXPERIENCE 145
shape reality in communicable ways, and are important for constructing rolemodels. Truth is constructed in a careful process where hierarchy and role-expectations are respected or even cautiously mocked, in order to present theoften chaotic reality in a polished way.14 To the western listener who comparesnotes of various counseling sessions with one client, this results in confusionabout what actually happened and sometimes outright frustration.
Another difficulty is related to the importance of regulated behavior andcommunication, and helps to explain the success of the mediums. Open discus-sion aimed at solving conflicts is usually avoided. The strength of the mediums isin their ability to allow people to communicate directly with spirits who arebeyond conventional limitations in communication. Problem solving withoutsupernatural assistance is different. When heads of families used to meet in orderto find ways to prevent escalating conflicts they would not aim at taking away thecause of the conflict. Finding acceptable ways for all parties to let the conflict rest,in other words, defining the proper way to behave in a crisis situation is moreimportant to than ‘tackling the roots of the problem’. Finally, the social hierarchytends to rule out the emphatic relationship required for counseling.
Nevertheless, contacts as described in the case of Somaly made the teamsee that verbal contact had effect. People actually liked contact with ‘strangers’such as the team, because, they said, they could not talk about emotions andproblems in the village. As we went along, we learned to respect that in counsel-ing sessions people were actually reconstructing their lives, as they did in groupsessions (see below). The positive results helped the team accept a new role,where empathy was not prevented by hierarchical expectations.
In describing common factors in brief psychotherapeutic approaches,Garfield (1997) lists the following basic general therapeutic factors: helping theclient to understand his problem, the therapeutic relationship, emotional release,reinforcement of client responses, helping clients to confront a problem, givinginformation, reassurance of the client, promoting successful coping, and emo-tional involvement of the client. These factors actually do apply in Cambodia,but were not easily transformed in practical counseling skills.
The two biggest barriers taken in installing counseling skills were related:the new role a counselor has to assume in order to be effective, and the ability toimprovise. They are related in, again, the tension between fixed roles and poten-tial loose behavior. The team initially wanted a clear protocol, prescribing indetail what to do under which circumstances. It was difficult to accept the theo-retical concept of counseling as a skilled improvisation in unpredictable, unique
14In Cambodian culture, stories, including life-stories, are not expected to simply reflect what hap-pened. People tend to reconstruct the story of their own lives until it fits in a culturally and sociallydesirable standard story. This tendency was reinforced by the communist ritual of creating falseautobiographies: in self-criticism sessions, or worse, in prisons under torture.
jong-02 10/26/01 1:40 PM Page 145

situations, where the aim is not to offer clear-cut solutions but helping peoplethink about their problems.
Working on counseling skills is at the same time highly relevant, because itattempts to find answers to this tension between rigid answers to new problems,a given fact in a modernizing society as Cambodia. And it also turned out to bea very productive area to build mutual understanding between the Cambodianand international members of the team. It was a basis for developing a commonlanguage for describing helping activities.
After four years, the efforts to introduce counseling as a skill to the membersof the core-group were successful. Core-group members are functioning as ade-quate professional helpers. Counseling techniques include problem analysis, situ-ation analysis, incident exploration, detailed discussion of a traumatic memory,and giving reassurance through psycho-education (cf Van der Veer, 1998b). Theteam is effective in supporting clients with a variety of complaints, symptomsand problems, such as physical complaints without an identifiable physical cause,post-traumatic symptoms, depressive complaints, marital problems, substanceabuse and so on. Also, they have been able to share their knowledge with others.Last but not least, all team members seem to be better equipped to deal withtheir own problems related to traumatic experiences in the past.
Core-group members today are involved in counseling contacts up to about15 sessions, with frequencies varying between twice a week and once a month.Clients can be referred for medication or a second opinion. Cases are discussedin regular team meetings. Some team members have specialized in attendingspecial categories of clients, including landmine victims, terminal aids-patients,homeless women and so on. It must be noted, however, that they achieved theseskills after a prior education ranging between nursing school and a completedstudy in medicine or psychology, followed by three years of training within theprogram. We have not found a shortcut to create counseling skills in ‘crashcourses’ in Cambodia.
In the coming years the needs for counseling are huge, for example due tothe continuously growing amount of land mine victims and the explosive AIDSepidemic. It is clear that counseling offers a valuable additional resource for manyin Cambodia. But training counselors is a complicated process that should not beunderestimated. The program works closely with the Royal University of PhnomPenh, where introductory courses in counseling were introduced at the depart-ment of psychology, where they are now regularly taught by department lecturers.
Psychiatric Services
It was no surprise that at the start of field work the first problems presentedby villagers to the teams were patients with psychotic disorders, causing consider-able distress to themselves and their surroundings. Faced with many who were
146 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 146

THE CAMBODIAN EXPERIENCE 147
severely deteriorated, sometimes chained up, the program had first to attend to these, which were seen by communities as a priority and a test for the newworkers’ credibility.
There was no existing psychiatric care within the public health care systemin Cambodia at the start of the project. The public health system itself was weakin terms of skilled staff, funding, and utilization. In view of the efficacy of thetraditional sectors in dealing with common psychosocial stress and eventualrehabilitation of mentally ill patients, the program set out to interfere as little aspossible with existing traditional healing networks and sought to encourage theiruse while offering its own treatment. Western biomedicine is capable of recog-nizing and effectively treating severe neuro-psychiatric disorders such as schizo-phrenia and major affective disorders as well as epilepsy. Primary health workerscan be given basic training to manage the majority of mental health problemswith a few inexpensive drugs (De Jong, 1987, 1996; WHO, 1990).
Well aware of the weaknesses of the Cambodian public health system asdescribed above, we decided to begin mental health clinics in the District Hospitalsin the areas we worked in (Somasundaram et al., 1999). Implementation of thehealth coverage plan designed by the Ministry of Health requires a clear defini-tion of the services at each level within the health system. The MOH defined a‘minimal package of activities’ for health centers and a ‘complementary packageof activities’ for referral hospitals, which were finalized in 1998 and 1999. TheTPO project provided the mental health material for these, and the staff at localhospitals was trained accordingly. In each hospital, 10 medical staff was given
Examples of Mental Illness in Cambodia: Madness ofWrecked Brains and Nerves
The most common term for this illness is ‘madness of the nerve tubules’ (*ckuət sɑɑ sayprɑsaat). It arises from any condition in which the brain and nervous system are injured. Womenoften were anxious about a sick child, or because the husband had run off with a ‘second wife’.
The patients spoke, sometimes to themselves, in a disorganized and careless way aboutthings that weren’t true, a condition termed (*pde�h-pdaah). They spoke deliriously (*rɔvəə-rɔviey).There were persistent headaches. There is a fear among Cambodians of abnormal sensationsaround the temples; the temple is literally ‘wearing a flower in the ear’. People are also terrifiedof problems around the back of the neck, as it is believed that this is the junction of the nervetubules ascending to the brain and, if injured, the brain will be damaged too. There were othersomatic sensations, such as tightness in the chest, a sense of ‘weak’ respiratory movements, heatin the chest, and the heart raced.
Damaged or disrupted nerve tubules needed direct treatment—the most direct was to applya burning wick to the skin in the method of moxibustion. Since the disease is believed to stemfrom overheated nerves, some healers prescribe ‘cooling medicine’ followed by ritual pouring oflustral water.
jong-02 10/26/01 1:40 PM Page 147

148 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
training in basic mental health care. Psychiatric specialist supervision, supportfrom the TPO team and supply of psychotropic drugs were provided. The clinicsopened one day a week, under supervision. It proves difficult to offer psychiatricservices on an integrated basis in the outpatient clinics. The motivational prob-lems of staff, who receive no extra salary or other incentive, is the biggest con-straint in installing regular and reliable service. As we mentioned above, theaverage salary of a health worker amounts to about 10% of what is needed toreach an income which can sustain a small household. Not many staff are inter-ested in giving more time without extra pay. Most of the clinics so far keep offer-ing psychiatric services on a one-morning-per-week basis. But in some clinicsstaff sows a personal interest and enthusiasm. Here the number of people seenkeeps growing steadily over the months—incidentally proving that health work-ers attitude is one of the main constraints in utilization of health services inCambodia. On average, each clinic sees about sixty patients every day theyopen. The clinics staffed by enthusiastic health workers see over a hundred eachday they open. Patients often travel from far to reach the out-patient in district orreferral hospitals. The catchment area of the four clinics officially covers some350,000 people, but patients come from far beyond the catchment area. There areno beds available for psychiatric care in Cambodia. The four clinics set up by theteam attracted 1524 new cases in 1999, and managed some 10,000 follow-up visits.
From the point of view of western nosology, the most common psychiatricconditions treated in the clinics were anxiety (26.1%), depression (19.8%) andschizophrenia (16.6%).15 Psychosis was diagnosed in 12.9% of patients, and thisincluded both acute psychosis and many cases later re-diagnosed as schizophre-nia on long-term follow-up. Those receiving the diagnosis of schizophrenia hadobvious chronic symptoms of self-neglect, deterioration in functioning, loss oftouch with reality, withdrawal or grossly abnormal behavior, hallucinations in theauditory or visual modality and strange beliefs of persecutory or religious nature.The hallucinations and delusions were often related to local events and culturebut with bizarre twists and clearly not shared by others. Much of the paranoiainvolved traumatic events in the past.
There was a high number of epileptic patients (14.8%), mostly generalizedtonic clonic seizures.
15Based on the diagnoses of 9.950 patients seen in 1999, when diagnostic skills of staff were deemedsufficient to yield data for monitoring purposes.
Pig Madness—Epilepsy as a Psychosocial, Even Mental Disorder
The rural patients generally prefer traditional healers to treat epilepsy. This was partly a reflec-tion of the cost of attending the clinic, and that the clinics until recently were not stocked withany form of anticonvulsant medication. Everyone knows about ‘pig madness’, the local idiom for
jong-02 10/26/01 1:40 PM Page 148
THE CAMBODIAN EXPERIENCE 149
Therapeutic interventions for major mental disorders in the clinics includedpharmacotherapy, crisis intervention, counseling, behavioral-cognitive methods,relaxation techniques, psycho-education, and emotive methods. When possiblefamilies were referred to selected traditional resources, group therapy or familytherapy. Psychological forms of treatment like counseling, relaxation exercisesand other non-pharmacological forms of therapy were encouraged to be usedfor the appropriate conditions, particularly the minor mental health disorders(Somasundaram, 1997).
The majority of patients received medication. Chlorpromazine, haloperi-dol, amitriptyline and imipramine covered most serious mental disorders, whilebenzhexol was needed for side effects. As epileptic patients also came in largenumbers to the mental health clinic, phenobarbitone and phenytoin were added.
The interventions were often used in combination as the following caseillustrates:
Theary, a 44 year old married lady with 6 children complained of having headaches for thelast ten years due to ‘thinking too much (*kit craBn)’. When asked what she thought too muchabout, she recounted an incident that happened in 1973. She had been carrying food for com-batants when she had suddenly seen ‘big’ tanks coming towards her. There had been heavyshelling with death and destruction all around her. Many of her relations and friends were killed.She saw corpses, body parts such as hands and fingers, blood and people crying out in pain.Heavy bombing had followed and she had taken shelter in a bunker, which collapsed under thebombing. She had been buried under the sand, suffered head injury and lost consciousness. Shecame to in the hospital but could not remember for how long she had been unconscious. She haddifficulty in remembering many of the details of what happened. She tried not to remember andoften suppressed her memories (‘forced them out of her mind’). Sometimes she could notremember anything, while at other times she had vivid recollections of the scene, particularlywhen she saw military personnel or heard loud explosions. At these times she became very fright-ened. She had frequent nightmares of the event both at night and when she slept in the day.
She became markedly distressed when recounting her past experience, her hands shakingvisibly. She resisted trying to remember, saying she didn’t want to remember. She had been givena responsible position during the Khmer Rouge regime, being in charge of the Children’s unit inher area, and had been unusually harsh. She admitted during subsequent counseling sessionsthat she feared retributions from those who had been affected in her village. She did not wish totalk about this time.
In 1979, Vietnamese soldiers had come, fired some shots in the air, and taken her husbandaway. She had become severely frightened, her body shaking terribly. Now her appetite is poorand she is not able to work as before. She has attacks of fainting lasting two hours or more, a few
epilepsy, in which the person has a sudden seizure. Given the presumed brain disorder, healersused moxibustion in an effort to reverse the disturbance—to get the pig out of the patient. Theritual transformed the pig into an image of the patient, and the patient metaphorically becamethe pig. After performing moxibustion, the healers gave medicine, sometimes to cool the febrilepatient.
jong-02 10/26/01 1:40 PM Page 149
150 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
It is difficult to evaluate the effect of introducing basic psychiatry. The prelim-inary results suggest that after the first flush of treatment, most patients improve tothe extent that they can lead reasonably productive lives (Somasudaram et al.,1998). One evident outcome of starting western psychiatric clinics with theobjective of providing a source of medication for the more severe mental ill-nesses in the community was that the clinic soon outstripped this basic functionand began to attract all types of psychosocial problems.
In a country without any psychiatric inpatient or outpatient servicespatients often are a severe burden to their families and their community, not tomention their own suffering. Basic psychiatry proved to be helpful to alleviatethese situations. The challenge is in installing these services in a sustainableand user-friendly way. Motivation of health staff running the clinic, follow-upoptions in the community, and the awareness of the local population are equallyimportant determinants for the effective use of these services. As we mentionedabove, motivation levels connected to low salaries limit the effect of trainingefforts in general on behavior change and increased skills in health workers. Butrecent experience in introducing health financing schemes in Cambodia hasnow shown results in increased utilization of public health services (Soeters &Griffiths, 2000). The combination of this effect with growing awareness withinthe population and increased options for follow-up within the community allowsbasic psychiatry to be installed properly—and the experience of the projectshows how this can technically be done.
CONCLUSIONS
The experience gained in the TPO program reaffirms the reality that peopleundergo a series of traumas as they either move from war to border camps, toresettlement, to repatriation, to internal displacement, or are exposed to a seriesof traumatic episodes in their home country. Resettlement, even from the awfulconditions of the camps, does not necessarily bring relief (Muecke & Sassi,1992). The work of the program runs consistent with the findings that people in
times every month. She often has chest pain, with a heavy pressure as if a heavy weight is on her,making it difficult to breathe (she said this started after she had been buried in the sand). Shestarted neglecting her self-care, sometimes crying and feeling sad.
She was started on imipramine, counseling, relaxation exercises and participation in women’sgroup was arranged. She improved quickly, her appetite and sleep returning to normal and fre-quency of re-experiencing decreased markedly. However she remained very sensitive and vulnera-ble to reminders of the trauma, and becomes distressed whenever it was brought up. Attempts aremade to gradually desensitize her to the trauma using a behavioral-cognitive technique.
jong-02 10/26/01 1:40 PM Page 150

chronic- or postconflict situations do best if they keep a grip on their culturalidentity (Cheung, 1995; Berry, 1991; Moon & Pearl, 1991; Eisenbruch, 1986).Our findings underscore the need for public mental health programs to givecareful consideration to the long-term consequences of post-war adjustment,and how people show cultural as well as personal losses (Schindler, 1993; Lipson,1991; Lipson, 1993). All this has implications for trauma theory and also forpublic mental health interventions. The program in Cambodia strives for cultur-ally competent clinical management, for it is known that the right treatment inthe wrong cultural garb, with the best of intentions, may further undermineidentity and might exacerbate signs of PTSD (Schreiber, 1995).
Local resources should be utilized. The experience in Cambodia supportsthe growing literature attesting the value of traditional healers as ‘trauma thera-pists’ in countries recovering from war (Gibbs, 1994; Wilson, 1989; Taussig,1986; Bracken, Giller, & Summerfield, 1995). It seems that they provide a meansthat for some is more agreeable than the methods brought by the classical publichealth and psychiatry. People need to have access to their local resources. Dif-ferent circumstances, from closed areas like refugee camps and open situationswhere the displaced population has more access to its own local resources andecosystem, have pointed out the hazards of adopting any single preconceivedblueprint.
At the same time there was a need to introduce new interventions, and thisneed was seen both by Cambodians in general as by healers of different sectors.Drawing lessons from the initial interventions of the program as well as the con-textual studies done, it was clear that any sustainable intervention technique hadto be fully imbedded and complementary to existing explanatory models, and beinstalled in the right group of helpers. This chapter has attempted to present ageneral amalgam of work done in these different contexts, and the case exam-ples serve to demonstrate how local culture and history stamps the training andthe interventions.
The experience shows that it is not enough to come and train local staff.Like all foreign programs, this one runs the risk of leaving the research in thehands of foreign experts at the expense of the local staff. By involvement of localstaff as far as possible, the program has sought to minimize this inevitable haz-ard. More information is now gathered about the outcome of interventions, todifferentiate types of mental distress and their attributes with reference to theirpredicted time course and healing without intervention.
The psychosocial problems found in communities, families and individualsin Cambodia are often not recognized and have a paralyzing effect on socialrehabilitation. Although mental health clinics are helpful for individuals thatneed medical treatment and their families, their coverage is limited and the solu-tion they offer does not match the overall majority of the problems people have.The essential question remains how certain characteristics of Cambodian society
THE CAMBODIAN EXPERIENCE 151
jong-02 10/26/01 1:40 PM Page 151
are causes as well as effects of what has happened—and the challenge—asshown by this chapter—is how this knowledge might be harnessed to developinterventions aimed at reconciliation and rehabilitation.
REFERENCES
Berry, J. W. (1991). Refugee adaptation in settlement countries: An overview with an emphasis onprimary prevention. In F. L. Ahearn Jr. & J. L. Athey (Eds.), Refugee children: Theory, research, andservices (pp. 20–38). Baltimore, MD: Johns Hopkins University Press.
Boehnlein, J. K., Kinzie, J. D., Ben, R., & Fleck, J. (1985). One-year follow-up study of posttraumaticstress disorder among survivors of Cambodian concentration camps. American Journal ofPsychiatry, 142(8), 956–959.
Bracken, P. J., Geiller, J. E., & Summerfield, D. (1995). Psychological responses to war and atrocity:The limitations of current concepts. Social Science and Medicine, 40, 1073–1082.
Brody, E. B. (1994). Psychiatric diagnosis in sociocultural context. Journal of Nervous and Mental Disease,182, 253–254.
Chandler, D. P. (1991). The tragedy of Cambodian history: Politics, war and revolution since 1945. New Haven,CT: Yale University Press.
Chandler, D. P. (1993). A history of Cambodia (2nd ed.). Chiang May, Thailand: Silkworm Books.Chandler, D. P. (1999). Voices from S-21: Terror and history in Pol Pot’s secret prison. Chiang May, Thailand:
Silkworm Books.Chandler, D. P., & Kiernan, B. (Eds.) (1983). Revolution and its aftermath in Kampuchea: Eight essays.
New Haven, CT: Yale University Southeast Asia Studies.Choulean, A. (1986). Les etres surnaturels dans la religion populaire khmère [Supernatural beings in the folk
religion of the Khmer]. Paris: Cedoreck.Collins, S. (1982). Selfless persons: Imagery and thought in Theravada Buddhism. Cambridge, England:
Cambridge University Press.Davenport, P., Healy, J., & Malone, K. (1995). Vulnerable in the village: A study of returnees in Battambang
Province, Cambodia, with a focus on strategies for the landless. Phnom Penh, Cambodia: UNHCR,Lutheran World Services and Japan Sotoshu Relief Committee.
De Jong, J. T. V. M. (1987). A descent into African psychiatry. Amsterdam: Royal Tropical Institute.De Jong, J. T. V. M. (1996). A comprehensive public mental health programme in Guinea-Bissau: A
useful model for African, Asian and Latin-American countries. Psychological Medicine, 26, 97–108.De Jong, J. T. V. M. (1997). TPO program for the identification, management, and prevention of psychosocial and
mental health problems of refugees and victims of organized violence within primary health care of adults andchildren. Amsterdam: Transcultural Psychosocial Organization. Internal document.
De Jong, J. T. V. M., & Clarke, J. (Eds.) (1996). Mental health for refugees. Geneva: World HealthOrganization.
Delvert, J. (1961). Le paysan cambodgien_ [The Cambodian peasant]. Paris: Mouton.Desjarlais, R., Eisenberg, L., Good, B., & Kleinman, A. (1995). World mental health: Problems and priori-
ties in low-income countries. New York: Oxford University Press.Ebihara, M. (1968). Svay, a Khmer village in Cambodia. Unpublished doctoral dissertation, Columbia
University, New York.Eisenbruch, M. (1990a). Classification of natural and supernatural causes of mental distress:
Development of a Mental Distress Explanatory Model Questionnaire. Journal of Nervous andMental Disease, 178(11), 712–719.
Eisenbruch, M. (1990b). Report of preliminary study of mental health in Cambodia. Document submitted toUNHCR Geneva.
152 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 152

Eisenbruch, M. (1991). From post-traumatic stress disorder to cultural bereavement: Diagnosis ofSoutheast Asian refugees. Social Science and Medicine, 33(6), 673–680.
Eisenbruch, M. (1992a). The ritual space of traditional healing in Cambodia. Bulletin d’École Françaisd’Extreme-Orient, 79(2), 283–316.
Eisenbruch, M. (1992b). Towards a culturally sensitive DSM: Cultural bereavement in Cambodianrefugees and the traditional healer as taxonomist. Journal of Nervous and Mental Disease, 181(1), 8–10.
Eisenbruch, M. (1994a). Resources and limitations in meeting the health needs of the Cambodian population.Paper presented at the conference Mental Health Education for Medical Doctors in Cambodia,Phnom Penh, Cambodia.
Eisenbruch, M. (1994b). The taxonomy of the psychoses in Cambodia. Paper presented at the GeigyTranscultural Psychiatry Symposium, 1–3 December, Perth, Australia.
Eisenbruch, M. (1996). The indigenous taxonomy of psychiatric disorders in Cambodia. In H. Vistosky, F. Lieh Mak, & J. J. López-Ibor, Jr. (Eds.), X World Congress World Psychiatric Association,Madrid, August 23–28, 1996: Addendum (p. 22). Amsterdam: Elsevier Biomedical.
Eisenbruch, M., & Handelman, L. H. (1989). Development of a culturally appropriate ExplanatoryModel Schedule for Cambodian refugee patients. Journal of Refugee Studies, 2(2), 243–56.
Evers, H. D. (Ed.) (1969). Loosely structured social systems: Thailand in comparative perspective (Cultural reportseries no. 17). New Haven, CT: Yale University Southeast Asia Studies.
Evers, H. D. (Ed.). (1980). Sociology of South-East Asia: Readings on social change and development.Kuala Lumpur, Malaysia: Oxford University Press.
Geertz, C. (1983). Local knowledge. New York: Basic Books.Gibbs, S. (1994). Post-war social reconstruction in Mozambique: Re-framing children’s experience of
trauma and healing. Disasters, 18, 268–276.Greve, H. S. (1993). Land tenure and property rights in Cambodia. Report to UNTAC, Phnom Penh,
Cambodia.Kiernan, B. (1996). The Pol Pot regime: Race, power and genocide in Cambodia under the Khmer Rouge.
New Haven, CT: Yale University Press.Kim, U., Triandis, H., KagitÇibas, Ç., Choi, S., & Yoon, G. (1994). Individualism and Collectivism: theory,
method, and applications. Thousand Oaks, CA: Sage Publications.Kinzie, J. D. (1990). The ‘concentration camp syndrome’ among Cambodian refugees. In D. A. Ablin
& M. Hood (Eds.), The Cambodian agony. Armonk, NY: M.E. Sharpe.Kirmayer, L. J. (1996). Confusion of the senses: Implications of ethnocultural variations in somato-
form and dissociative disorders for PTSD. In A. J. Marsella, M. J. Friedman, E. T. Gerrity & R. M. Scurfield (Eds.), Ethnocultural aspects of posttraumatic stress disorder (pp. 131–163). Washington,DC: American Psychological Association.
Kleber, R., Figley, C., & Gersons, B. (Eds.) (1995). Beyond trauma: Cultural and societal dynamics.New York: Plenum Press.
Kleinman, A. M. (1980). Patients and healers in the context of culture. Berkeley, CA: University ofCalifornia Press.
Lipson, J. G. (1991). Afghan refugee health: Some findings and suggestions. Qualitative Health Research,1, 349–369.
Lipson, J. G. (1993). Afghan refugees in California: Mental health issues. Issues in Mental HealthNursing, 14(4), 411–423.
Marsella, A. J., Friedman, M. J., Gerrity, E. T., & Scurfield, R. M. (Eds.) (1996). Ethnocultural aspects ofposttraumatic stress disorder. Washington, DC: American Psychological Association.
Martel, G. (1975). Lovea, village des environs d’Angkor: aspects demographiques, economiques et sociologiquesde monde rural cambodgien dans la province de Siem Reap [Lovea, neighboring village of Angkor:Demographic, economical and sociological aspects of rural Cambodian society in the provinceof Siem Reap]. Paris: L’Ecole Française d’Extreme-Orient.
Mehta, H. C. (1997). Cambodia silenced: The press under six regimes. Bangkok, Thailand: White Lotus.
THE CAMBODIAN EXPERIENCE 153
jong-02 10/26/01 1:40 PM Page 153

Ministry of Planning (1996). Demographic survey of Cambodia—1996. Phnom Penh, Cambodia:National Institute of Statistics.
Mollica, R. (1994). Southeast Asian refugees: Migration history and mental health issues. In A. J. Marsella, T. Bornemann, S. Ekbald, & J. Orley (Eds.), Amidst peril and pain: The mental healthand well-being of the world’s refugees (pp. 83–100). Washington, DC: American PsychologicalAssociation.
Mollica, R., & Jalbert, R. (1989). Community of confinement: The mental health crisis in Site Two (displacedpersons camp on the Thai border). Alexandria, VA: World Federation for Mental Health.
Moon, J. H., & Pearl, J. H. (1991). Alienation of elderly Korean American immigrants as related toplace of residence, gender, age, years of education, time in the U.S., living with or without chil-dren, and living with or without a spouse. International Journal of Aging and Human Development,32(2), 115–124.
Muecke, M. A., & Sassi, L. (1992). Anxiety among Cambodian refugee adolescents in transit and inresettlement. Western Journal of Nursing Research, 14, 267–291.
Myslewiec, E. (1988). Punishing the poor: The international isolation of Cambodia. Oxford, England: Oxfam.Nepote, J. (1992). Parente et organization sociale dans le Cambodge moderne et contemporain [Kinship and social
organisation in contemporary Cambodia]. Nantes, France: Edition Olizane.Ovesen, J., Trankell, I., & Ojendal, J. (1995). When every household is an island: social organisation and power
structures in rural Cambodia. Stockholm: Swedish International Development Cooperation Agency.Ponchaud, F. (1978). Cambodia year zero. London: Alien Lane.Porée-Maspero, E. (1962). Étude sur les rites agraires des cambodgien [Study into Cambodian rural rituals].
Paris: Mouton.Project Against Domestic Violence (1996). Household survey on domestic violence in Cambodia. Phnom
Penh, Cambodia: Ministry of Women’s Affairs.Schindler, R. (1993). Emigration and the black Jews of Ethiopia: Dealing with bereavement and loss.
International Social Work, 36(1), 7–19.Schreiber, S. (1995). Migration, traumatic bereavement and transcultural aspects of psychological
healing: Loss and grief of a refugee woman from Begameder County in Ethiopia. British Journalof Medical Psychology, 68(2), 135–142.
Schriever, S. H. (1990). Comparison of beliefs and practices of ethnic Viet and Lao Hmong con-cerning illness, healing, death and mourning: Implications for hospice care with refugees inCanada. Journal of Palliative Care, 6(1), 42–49.
Shawcross, W. (1985). The quality of mercy. Glasgow, Scotland: William Collins Sons.Somasundaram, D. J. (1996). Post-traumatic responses to aerial bombing. Social Science and Medicine,
42(11) 1465–1471.Somasundaram, D. J., Kail, K., Van de Put, W. A. C. M., Eisenbruch, M., & Thomassen, L. (1997).
Community mental health in Cambodia. Phnom Penh, Cambodia: Transcultural PsychosocialOrganization.
Somasundaram, D. J., & Sivayokan, S. (1994). War trauma in a civilian population. British Journal ofPsychiatry, 156, 524–527.
Somasundaram, D. J., Van de Put, W. A. C. M., Eisenbruch, M., & De Jong, J. T. V. M. (1999).Starting mental health in Cambodia. Social Science and Medicine, 48, 1029–1046.
Taussig, M. (1986). Shamanism, colonialism, and the wild man: A study in terror and healing. Chicago:University of Chicago Press.
Thion, S. (1993). Watching Cambodia. Bangkok, Thailand: White Lotus.United Nations Development Programme. (1996). Cambodian human development report 1997. Phnom
Penh, Cambodia.United Nations Research Institute for Social Development (1993). Rebuilding war torn societies: Report of
the workshops on the Challenges of Rebuilding War torn Societies and the Social Consequences of the PeaceProcess in Cambodia, Geneva, 27–30 April 1993. Geneva.
154 WILLEM A. C. M. VAN DE PUT AND MAURICE EISENBRUCH
jong-02 10/26/01 1:40 PM Page 154
THE CAMBODIAN EXPERIENCE 155
Van de Put, W. A. C. M. (1992). Empty hospitals, thriving business: Utilization of health services and healthseeking behaviour in two Cambodian districts. Amsterdam: Medicines sans Frontières Holland.
Van de Put, W. A. C. M., Hema, N., Sovandara, S. C., Renol, K. K., & Eisenbruch, M. (1996).Psycho-social problems and the use of community resources in Cambodia. Paper presented at theInternational Conference on Khmer Studies, Royal University of Phnom Penh, Cambodia.
Van de Put, W. A. C. M., Somasundaram, D., Eisenbruch, I. M., Kall, K., Soomers, R., &Thomassen, L. (1997). Facts and thoughts on the first years 1995–1997. Phnom Penh, Cambodia:Transcultural Psychosocial Organization.
Van de Put, W. A. C. M. & Van der Veer, G. (in press). Counseling in Cambodia. Mind & human inter-action (University of Virginia, Center for the Study of Mind and Human Interaction).
Van der Kolk, B. A., McFarlane, A. C., & Weisaeth, L. (Eds.) (1996). Traumatic stress: The effects of over-whelming experience on mind, body, and society. New York: Guilford Press.
Vickery, M. (1984). Cambodia: 1975–1982. Boston, MA: South End Press.Wilson, J. P. (1989). Trauma, transformation and healing: An integrative approach to theory, research and post-
traumatic therapy. New York: Brunner/Mazel.World Health Organization (1975). Organization of mental health services in developing countries. (Technical
report series no. 564). Geneva.World Health Organization (1981). Report from the WHO collaborative study of strategies for extending mental
health care. Geneva.World Health Organization (1990). The introduction of a mental health component into primary health care.
Geneva.World Health Organization (1994). Primary health care concepts and challenges in a changing world: Alma Ata
revisited. Geneva.World Health Organization (1996). Diagnostic and management guidelines for mental disorders in primary
care—ICD-10 Chapter V Primary Care Version. Geneva.
jong-02 10/26/01 1:40 PM Page 155