
External rotation lag sign revisited: Accuracy for diagnosis of full thickness supraspinatus tear
6
External rotation lag sign revisited: Accuracy for diagnosis of full thickness supraspinatus tear Filippo Castoldi, MD a , Davide Blonna, MD a, *, Ralph Hertel, MD b a University of Turin Medical School; Mauriziano ‘‘Umberto I’’ Hospital, Turin, Italy b Shulterzentrum, Lindenhofspital, Bern, Switzerland Hypothesis: This study reassessed the sensitivity and the specificity of the external rotator lag sign (ERLS) for diagnosis of supraspinatus tears in a large cohort of patients. Materials and methods: The ERLS was used to assess 401 consecutive patients with 406 painful shoulder conditions. The clinical diagnosis was controlled either arthroscopically or by open surgery. Results: For isolated full-thickness supraspinatus tears, the ERLS had a sensitivity of 56% and a specificity of 98%. When the lesion involved the infraspinatus and the teres minor the sensitivity improved substan- tially. There was a strong correlation between the extension of the tear and the amount of the lag. The lag increased from 7 for an isolated rupture of the supraspinatus tendon to 26 in case of extension to the teres minor. Conclusion: The ERLS is highly specific and acceptably sensitive for diagnosis of full-thickness tears, even in case of an isolated lesion of the supraspinatus tendon. Level of evidence: Level 2; prospective cohort treatment study. Ó 2009 Journal of Shoulder and Elbow Surgery Board of Trustees. Keywords: External rotation lag sign; rotator cuff tear; supraspinatus tear Diagnosis, interpretation, and subsequent management of the rotator cuff tear can be challenging to clinicians, even with the use of ultrasonography or magnetic resonance imaging (MRI). Although preoperative imaging is useful to detect rotator cuff tears and estimate the size, physical examination remains essential. Physical examination of the rotator cuff can be performed using 2 types of tests, generally known as integrity tests: those that determine whether a movement can be achieved actively, often asso- ciated with force measurements, and those that assess if a passive position can be maintained in space (the lag signs). Jobe and Moynes 5 first reported that the function of the supraspinatus could be isolated at physical examination. Unfortunately, this test can be easily biased by pain. In fact, because the supraspinatus tear is usually part of a painful syndrome, the Jobe sign will produce a high rate of false- positive results. This results in a low specificity in the discrimination of the different stages of the impingement syndrome. 9,14 An ideal test for the supraspinatus integrity, if the test is based on biomechanical laws and free of confounding elements, should not only have a high sensitivity and speci- ficity for a full-thickness tear but should also be negative in case of partial-thickness tear. The external rotation lag sign (ERLS) described by Hertel et al 1 in 1996 was designed to *Reprint requests: Davide Blonna, University of Turin Medical School, Mauriziano ‘‘Umberto I’’ Hospital, Largo Turati 62, 10128 Turin, Italy. E-mail address: [email protected], [email protected] (D. Blonna). J Shoulder Elbow Surg (2009) -, 1-6 www.elsevier.com/locate/ymse 1058-2746/2009/$36.00 - see front matter Ó 2009 Journal of Shoulder and Elbow Surgery Board of Trustees. doi:10.1016/j.jse.2008.11.007 ARTICLE IN PRESS
Transcript of External rotation lag sign revisited: Accuracy for diagnosis of full thickness supraspinatus tear

*Reprint req
Mauriziano ‘‘Um
E-mail addre
Blonna).
J Shoulder Elbow Surg (2009) -, 1-6
1058-2746/2009
doi:10.1016/j.jse
ARTICLE IN PRESS
www.elsevier.com/locate/ymse
External rotation lag sign revisited: Accuracy fordiagnosis of full thickness supraspinatus tear
Filippo Castoldi, MDa, Davide Blonna, MDa,*, Ralph Hertel, MDb
aUniversity of Turin Medical School; Mauriziano ‘‘Umberto I’’ Hospital, Turin, ItalybShulterzentrum, Lindenhofspital, Bern, Switzerland
Hypothesis: This study reassessed the sensitivity and the specificity of the external rotator lag sign(ERLS) for diagnosis of supraspinatus tears in a large cohort of patients.Materials and methods: The ERLS was used to assess 401 consecutive patients with 406 painful shoulderconditions. The clinical diagnosis was controlled either arthroscopically or by open surgery.Results: For isolated full-thickness supraspinatus tears, the ERLS had a sensitivity of 56% and a specificityof 98%. When the lesion involved the infraspinatus and the teres minor the sensitivity improved substan-tially. There was a strong correlation between the extension of the tear and the amount of the lag. The lagincreased from 7� for an isolated rupture of the supraspinatus tendon to 26� in case of extension to the teresminor.Conclusion: The ERLS is highly specific and acceptably sensitive for diagnosis of full-thickness tears,even in case of an isolated lesion of the supraspinatus tendon.Level of evidence: Level 2; prospective cohort treatment study.� 2009 Journal of Shoulder and Elbow Surgery Board of Trustees.
Keywords: External rotation lag sign; rotator cuff tear; supraspinatus tear
Diagnosis, interpretation, and subsequent managementof the rotator cuff tear can be challenging to clinicians,even with the use of ultrasonography or magnetic resonanceimaging (MRI). Although preoperative imaging is useful todetect rotator cuff tears and estimate the size, physicalexamination remains essential. Physical examination of therotator cuff can be performed using 2 types of tests,generally known as integrity tests: those that determinewhether a movement can be achieved actively, often asso-ciated with force measurements, and those that assess if
uests: Davide Blonna, University of Turin Medical School,
berto I’’ Hospital, Largo Turati 62, 10128 Turin, Italy.
ss: [email protected], [email protected] (D.
/$36.00 - see front matter � 2009 Journal of Shoulder and Elbo
.2008.11.007
a passive position can be maintained in space (the lagsigns).
Jobe and Moynes5 first reported that the function of thesupraspinatus could be isolated at physical examination.Unfortunately, this test can be easily biased by pain. In fact,because the supraspinatus tear is usually part of a painfulsyndrome, the Jobe sign will produce a high rate of false-positive results. This results in a low specificity in thediscrimination of the different stages of the impingementsyndrome.9,14
An ideal test for the supraspinatus integrity, if the test isbased on biomechanical laws and free of confoundingelements, should not only have a high sensitivity and speci-ficity for a full-thickness tear but should also be negative incase of partial-thickness tear. The external rotation lag sign(ERLS) described by Hertel et al1 in 1996 was designed to
w Surgery Board of Trustees.
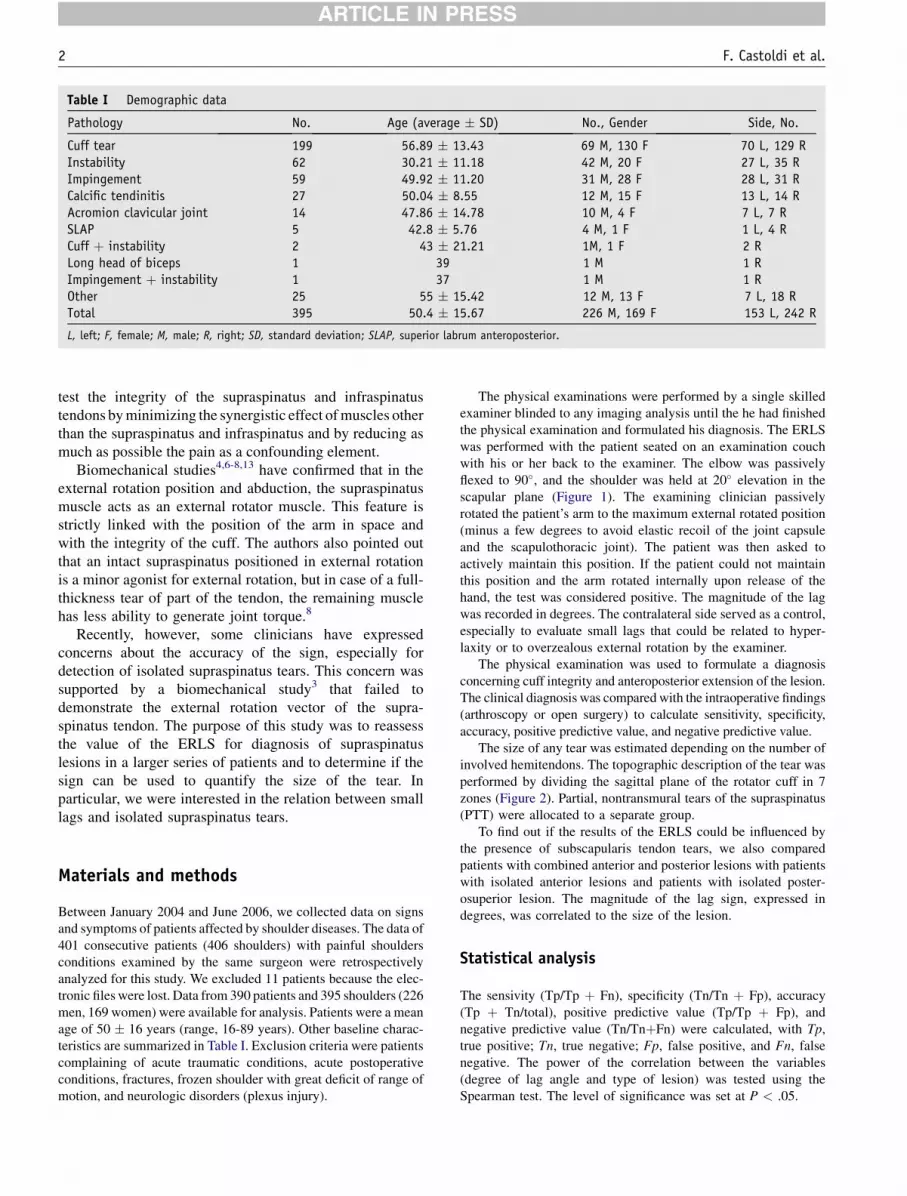
Table I Demographic data
Pathology No. Age (average � SD) No., Gender Side, No.
Cuff tear 199 56.89 � 13.43 69 M, 130 F 70 L, 129 RInstability 62 30.21 � 11.18 42 M, 20 F 27 L, 35 RImpingement 59 49.92 � 11.20 31 M, 28 F 28 L, 31 RCalcific tendinitis 27 50.04 � 8.55 12 M, 15 F 13 L, 14 RAcromion clavicular joint 14 47.86 � 14.78 10 M, 4 F 7 L, 7 RSLAP 5 42.8 � 5.76 4 M, 1 F 1 L, 4 RCuff þ instability 2 43 � 21.21 1M, 1 F 2 RLong head of biceps 1 39 1 M 1 RImpingement þ instability 1 37 1 M 1 ROther 25 55 � 15.42 12 M, 13 F 7 L, 18 RTotal 395 50.4 � 15.67 226 M, 169 F 153 L, 242 R
L, left; F, female; M, male; R, right; SD, standard deviation; SLAP, superior labrum anteroposterior.
2 F. Castoldi et al.
ARTICLE IN PRESS
test the integrity of the supraspinatus and infraspinatustendons by minimizing the synergistic effect of muscles otherthan the supraspinatus and infraspinatus and by reducing asmuch as possible the pain as a confounding element.
Biomechanical studies4,6-8,13 have confirmed that in theexternal rotation position and abduction, the supraspinatusmuscle acts as an external rotator muscle. This feature isstrictly linked with the position of the arm in space andwith the integrity of the cuff. The authors also pointed outthat an intact supraspinatus positioned in external rotationis a minor agonist for external rotation, but in case of a full-thickness tear of part of the tendon, the remaining musclehas less ability to generate joint torque.8
Recently, however, some clinicians have expressedconcerns about the accuracy of the sign, especially fordetection of isolated supraspinatus tears. This concern wassupported by a biomechanical study3 that failed todemonstrate the external rotation vector of the supra-spinatus tendon. The purpose of this study was to reassessthe value of the ERLS for diagnosis of supraspinatuslesions in a larger series of patients and to determine if thesign can be used to quantify the size of the tear. Inparticular, we were interested in the relation between smalllags and isolated supraspinatus tears.
Materials and methods
Between January 2004 and June 2006, we collected data on signsand symptoms of patients affected by shoulder diseases. The data of401 consecutive patients (406 shoulders) with painful shouldersconditions examined by the same surgeon were retrospectivelyanalyzed for this study. We excluded 11 patients because the elec-tronic files were lost. Data from 390 patients and 395 shoulders (226men, 169 women) were available for analysis. Patients were a meanage of 50 � 16 years (range, 16-89 years). Other baseline charac-teristics are summarized in Table I. Exclusion criteria were patientscomplaining of acute traumatic conditions, acute postoperativeconditions, fractures, frozen shoulder with great deficit of range ofmotion, and neurologic disorders (plexus injury).
The physical examinations were performed by a single skilledexaminer blinded to any imaging analysis until the he had finishedthe physical examination and formulated his diagnosis. The ERLSwas performed with the patient seated on an examination couchwith his or her back to the examiner. The elbow was passivelyflexed to 90�, and the shoulder was held at 20� elevation in thescapular plane (Figure 1). The examining clinician passivelyrotated the patient’s arm to the maximum external rotated position(minus a few degrees to avoid elastic recoil of the joint capsuleand the scapulothoracic joint). The patient was then asked toactively maintain this position. If the patient could not maintainthis position and the arm rotated internally upon release of thehand, the test was considered positive. The magnitude of the lagwas recorded in degrees. The contralateral side served as a control,especially to evaluate small lags that could be related to hyper-laxity or to overzealous external rotation by the examiner.
The physical examination was used to formulate a diagnosisconcerning cuff integrity and anteroposterior extension of the lesion.The clinical diagnosis was compared with the intraoperative findings(arthroscopy or open surgery) to calculate sensitivity, specificity,accuracy, positive predictive value, and negative predictive value.
The size of any tear was estimated depending on the number ofinvolved hemitendons. The topographic description of the tear wasperformed by dividing the sagittal plane of the rotator cuff in 7zones (Figure 2). Partial, nontransmural tears of the supraspinatus(PTT) were allocated to a separate group.
To find out if the results of the ERLS could be influenced bythe presence of subscapularis tendon tears, we also comparedpatients with combined anterior and posterior lesions with patientswith isolated anterior lesions and patients with isolated poster-osuperior lesion. The magnitude of the lag sign, expressed indegrees, was correlated to the size of the lesion.
Statistical analysis
The sensivity (Tp/Tp þ Fn), specificity (Tn/Tn þ Fp), accuracy(Tp þ Tn/total), positive predictive value (Tp/Tp þ Fp), andnegative predictive value (Tn/TnþFn) were calculated, with Tp,true positive; Tn, true negative; Fp, false positive, and Fn, falsenegative. The power of the correlation between the variables(degree of lag angle and type of lesion) was tested using theSpearman test. The level of significance was set at P < .05.

Figure 1 Correct execution of the external rotation lag sign test. The shoulder is held at 20� elevation in the scapular plane.
Figure 2 Sagittal plane of the rotator cuff and the humeral head.Subscapularis: 1, lower portion; 2, upper portion. Supraspinatus:3, anterior portion; 4, posterior portion. Infraspinatus: 5, superiorportion; 6, inferior portion. Teres minor: 7.
External rotation lag sign 3
ARTICLE IN PRESS
Results
PTT of the supraspinatus
As expected, the ERLS was not able to identify PTT of thesupraspinatus. The very low number of true-positive resultsdetermined a sensitivity of only 12%; however, the speci-ficity was nearly 100% owing to a high percentage of true-negative results (Table II). The presence of a subscapularistear slightly increased the sensitivity of the test, but thisdetermined a similar increase in false-positive results andtherefore a loss in accuracy.
Isolated supraspinatus full-thickness tear
An isolated lesion of the anterior half of the supraspinatus(zone number 3) could not be identified by the ERLS (lowsensitivity). The results are similar to PTT (Table II). As weobserved for the PTT, the sensitivity of the test wasimproved by an associated subscapularis lesion. Thesensitivity improved immensely when the tear extended tothe posterior portion of the supraspinatus (zone 4), withoutaffecting the specificity of the test. The ERLS had a sensi-tivity of 56% and a specificity of 98% for isolated lesions ofzone 3 and 4 (complete lesion of the supraspinatus). Thesensitivity increased to 62% and specificity decreased to93% for lesions that included the subscapularis (zone 1 and2; Table II). Considering the true-positive results, theaverage rotational angle (or lag angle) for an isolatedsupraspinatus rupture (zones 3 and 4) was 7.35� � 3.12�.
Supraspinatus, infraspinatus, and teres minor tears
The sensitivity of the ERLS was improved significantlywhen a lesion extended into the infraspinatus or into theteres minor. For combined lesions of zones 3, 4, and 5, thesensitivity was 65%. For combined lesion of zones 3 to 6,the sensitivity was as high as 97% (Table II). The ERLS
showed the best sensitivityd100%din case of teres minorlesions, with a specificity of 93% and an overall accuracy of93%.
Correlation between magnitude of lag and exten-sion of the tear
The extension of the tear has an effect on the amount of lagsign. When the data from the true-positive results wereconsidered, the angular lag increased from 7.35� � 3.12�
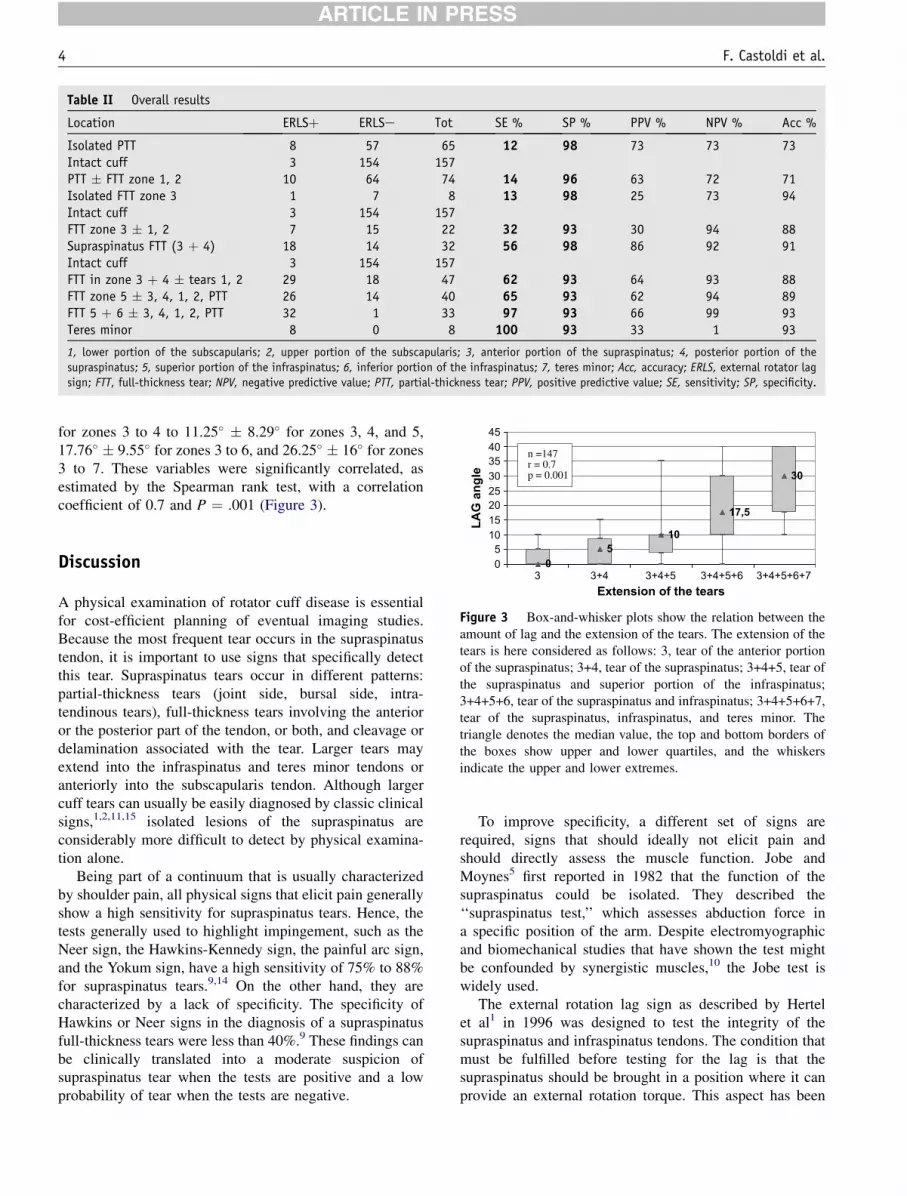
Table II Overall results
Location ERLSþ ERLSe Tot SE % SP % PPV % NPV % Acc %
Isolated PTT 8 57 65 12 98 73 73 73Intact cuff 3 154 157PTT � FTT zone 1, 2 10 64 74 14 96 63 72 71Isolated FTT zone 3 1 7 8 13 98 25 73 94Intact cuff 3 154 157FTT zone 3 � 1, 2 7 15 22 32 93 30 94 88Supraspinatus FTT (3 þ 4) 18 14 32 56 98 86 92 91Intact cuff 3 154 157FTT in zone 3 þ 4 � tears 1, 2 29 18 47 62 93 64 93 88FTT zone 5 � 3, 4, 1, 2, PTT 26 14 40 65 93 62 94 89FTT 5 þ 6 � 3, 4, 1, 2, PTT 32 1 33 97 93 66 99 93Teres minor 8 0 8 100 93 33 1 93
1, lower portion of the subscapularis; 2, upper portion of the subscapularis; 3, anterior portion of the supraspinatus; 4, posterior portion of the
supraspinatus; 5, superior portion of the infraspinatus; 6, inferior portion of the infraspinatus; 7, teres minor; Acc, accuracy; ERLS, external rotator lag
sign; FTT, full-thickness tear; NPV, negative predictive value; PTT, partial-thickness tear; PPV, positive predictive value; SE, sensitivity; SP, specificity.
17,5
30
202530354045
G a
ng
le
n =147r = 0.7 p = 0.001
4 F. Castoldi et al.
ARTICLE IN PRESS
for zones 3 to 4 to 11.25� � 8.29� for zones 3, 4, and 5,17.76� � 9.55� for zones 3 to 6, and 26.25� � 16� for zones3 to 7. These variables were significantly correlated, asestimated by the Spearman rank test, with a correlationcoefficient of 0.7 and P ¼ .001 (Figure 3).
0
5
10
051015
3 3+4 3+4+5 3+4+5+6 3+4+5+6+7Extension of the tears
LA
Figure 3 Box-and-whisker plots show the relation between theamount of lag and the extension of the tears. The extension of thetears is here considered as follows: 3, tear of the anterior portionof the supraspinatus; 3+4, tear of the supraspinatus; 3+4+5, tear ofthe supraspinatus and superior portion of the infraspinatus;3+4+5+6, tear of the supraspinatus and infraspinatus; 3+4+5+6+7,tear of the supraspinatus, infraspinatus, and teres minor. Thetriangle denotes the median value, the top and bottom borders ofthe boxes show upper and lower quartiles, and the whiskersindicate the upper and lower extremes.
Discussion
A physical examination of rotator cuff disease is essentialfor cost-efficient planning of eventual imaging studies.Because the most frequent tear occurs in the supraspinatustendon, it is important to use signs that specifically detectthis tear. Supraspinatus tears occur in different patterns:partial-thickness tears (joint side, bursal side, intra-tendinous tears), full-thickness tears involving the anterioror the posterior part of the tendon, or both, and cleavage ordelamination associated with the tear. Larger tears mayextend into the infraspinatus and teres minor tendons oranteriorly into the subscapularis tendon. Although largercuff tears can usually be easily diagnosed by classic clinicalsigns,1,2,11,15 isolated lesions of the supraspinatus areconsiderably more difficult to detect by physical examina-tion alone.
Being part of a continuum that is usually characterizedby shoulder pain, all physical signs that elicit pain generallyshow a high sensitivity for supraspinatus tears. Hence, thetests generally used to highlight impingement, such as theNeer sign, the Hawkins-Kennedy sign, the painful arc sign,and the Yokum sign, have a high sensitivity of 75% to 88%for supraspinatus tears.9,14 On the other hand, they arecharacterized by a lack of specificity. The specificity ofHawkins or Neer signs in the diagnosis of a supraspinatusfull-thickness tears were less than 40%.9 These findings canbe clinically translated into a moderate suspicion ofsupraspinatus tear when the tests are positive and a lowprobability of tear when the tests are negative.
To improve specificity, a different set of signs arerequired, signs that should ideally not elicit pain andshould directly assess the muscle function. Jobe andMoynes5 first reported in 1982 that the function of thesupraspinatus could be isolated. They described the‘‘supraspinatus test,’’ which assesses abduction force ina specific position of the arm. Despite electromyographicand biomechanical studies that have shown the test mightbe confounded by synergistic muscles,10 the Jobe test iswidely used.
The external rotation lag sign as described by Hertelet al1 in 1996 was designed to test the integrity of thesupraspinatus and infraspinatus tendons. The condition thatmust be fulfilled before testing for the lag is that thesupraspinatus should be brought in a position where it canprovide an external rotation torque. This aspect has been

External rotation lag sign 5
ARTICLE IN PRESS
supported by independent biomechanical investigations.4,6-8,13
Furthermore, recent studies8 demonstrated that even in thepresence of a tear that does not involve the entire tendon,the remaining cuff has a reduced ability to generate jointtorque. Walsh et al15 assessed the clinical value of thehornblower sign and of Neer’s dropping sign. Theyconcluded that the dropping sign and the hornblower signwere positive and highly accurate for detection of largeruptures but not really useful for small ruptures.
The different appreciation of similar signs might be dueto critical differences in the test position as well as in theamount of lag that the clinician is searching for. Small lagsof 5� to 10� are not readily visible if one expects a largedropping (Neer)12 in the order of 20� and more. We highlyrecommend testing the contralateral side, which mightclarify the situation, especially for the inexperiencedobserver. Our activity has led us to understand that elicitingthe ERLS requires a certain amount of practice and dedi-cation. The fine nature of the ERLS is somehow compa-rable to the difficult pivot shift sign for anterior cruciateinsufficiency.
Few reports have been published on the diagnostic valueof the rotator cuff signs, and particularly of the lag sign,other than the Hertel study. Park et al14 reported similarresult in sensitivity and specificity between the supra-spinatus muscle test and the infraspinatus muscle test, butthey did not routinely evaluate the ERLS in each patientand did not distinguish among different extensions ofthickness tears. They found that a combination of a painfularc sign, drop-arm sign, and positive infraspinatus muscletest produced the best posttest probability (91%) for full-thickness rotator cuff tears. We agree with these authorsthat a combination of several signs, including the history aswell as the conventional radiographic signs, will dramati-cally improve our diagnostic accuracy, probably to a levelwhere additional imaging is only necessary to determinethe degree of degeneration of the tendon and muscular cuff;that is, to determine reparability in grey zone patients.
In our series for isolated full-thickness tears of thesupraspinatus, the ERLS had a specificity of 98% anda sensitivity of 56%. This greatly outweighs the Jobe sign,especially when considering that in our study the pretestprobability for a full-thickness lesion in zone 3 and 4 wasonly about 17% instead of 41%.14
Limitations of this study are (1) its retrospective nature,(2) measuring of the lag is subjective and not quantified byan instrument, (3) the influence of a concomitant symp-tomatic long head of the biceps on the accuracy of theERLS was not analyzed, and (4) the test was performed byan experienced surgeon, thus introducing a positive biascompared with a less experienced person. Nevertheless, webelieve that this study demonstrated the validity of theERLS as an accurate sign for the diagnosis of an isolatedsupraspinatus tear in experienced hands.
The increasing magnitude of lag sign with increasinganteroposterior extension of the rupture seems to be
affected by a ‘‘waterfall effect’’: a sudden increase of thelag when the lesion extends into regions 6 and 7. Thisexponential reduction of torque might be explained by thesudden destabilization of the mechanical fulcrum whena critical size of the rupture is reached.8 An associatedlesion of the subscapularis may lead to an abnormalincrease of passive external rotation, which may producea false-positive ERLS. This explains the increased sensi-tivity and the decreased specificity of the ERLS when thesupraspinatus tear is associated with a subscapularis tear.
This study confirmed the clinical validity of the ERLSfor diagnosis of an isolated tear of the supraspinatus.Nevertheless attempts at biomechanically reproducing thesign failed to measure a significant lag sign in case ofisolated supraspinatus lesion.3 Although we have no clearexplanation for this finding, we believe that methodologicerrors could be imputed. These are some basic facts toconsider when setting up experimental studies on lag signs:lag signs do not test weakness of a given musculotendinousunit. A lag occurs only if the patient cannot activelymaintain a given position in space. Certainly, a minimum offorce is required to maintain a position against gravity, butbeyond this, no higher force is required. We believe thatfurther efforts must be done to create adequate model toinvestigate the ERLS.
Conclusions
The ERLS is a useful sign for the diagnosis of isolated fullthickness tears of the supraspinatus tendon. It is highlyspecific and offers a good sensitivity. When integrated withother signs, symptoms, and tests, it provides a precise pictureof the lesion including its size and allows the surgeon toefficiently plan further investigations and treatment.
References
1. Hertel R, Ballmer FT, Lombert SM, Gerber C. Lag signs in the diagnosis
of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-13.
2. Holtby R, Razmjou H. Validity of the supraspinatus test as a single
clinical test in diagnosing patients with rotator cuff pathology.
J Orthop Sports Phys Ther 2004;34:194-200.
3. Hurschler C, Wulker N, Windhagen H, Hellmers N, Plumhoff P.
Evaluation of the lag sign tests for external rotator function of the
shoulder. J Shoulder Elbow Surg 2004;13:298-304.
4. Jenp YN, Malanga GA, Growney ES, An KN. Activation of the rotator
cuff in generating isometric shoulder rotation torque. Am J Sports Med
1996;24:477-85.
5. Jobe FW, Moynes DR. Delineation of diagnostic criteria and rehabili-
tation program for rotator cuff injuries. Am J Sports Med 1982;10:336-9.
6. Kelly BT, Kadrmas WR, Speer KP. The manual muscle examination
for rotator cuff strength. An electromyographic investigation. Am J
Sports Med 1996;24:581-8.
7. Kronberg M, Nemeth G, Brostrom LA. Muscle activity and coordi-
nation in the normal shoulder. An electromyographic study. Clin
Orthop Relat Res 1990;257:76-85.

6 F. Castoldi et al.
ARTICLE IN PRESS
8. Langenderfer JE, Patthanacharoenphon C, Carpenter JE, Hughes RE.
Variation in external rotation moment arms among subregions of
supraspinatus, infraspinatus, and teres minor muscles. J Orthop Res
2006;24:1737-44.
9. MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic
accuracy of the Hawkins and Neer subacromial impingement signs. J
Shoulder Elbow Surg 2000;9:299-301.
10. Malaga GA, Jenp YN, Growney ES, An KN. EMG analysis of
shoulder positioning in testing and strengthening the supraspinatus.
Med Sci Sports Exerc 1996;28:661-64.
11. Murrell GA, Walton JR. Diagnosis of rotator cuff tears. Lancet 2001;
357:769-70. Erratum in: Lancet 2001;357:1452.
12. Neer CS. Anatomy of shoulder reconstruction. In: Neer CS, editor. Shoulder
reconstruction. Philadelphia: WB Saunders Company; 1990. p. 1-39.
13. Otis JC, Jiang CC, Wickiewicz TL, Peterson MG, Warren RF,
Santner TJ. Changes in the moment arms of the rotator cuff and
deltoid muscles with abduction and rotation. J Bone Joint Surg Am
1994;76:667-76.
14. Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic
accuracy of clinical tests for the different degrees of subacromial
impingement syndrome. J Bone Joint Surg Am 2005;87:1446-55.
15. Walch G, Boulahia A, Calderone S, Robinson AH. The ‘dropping’ and
‘hornblower’s’ signs in evaluation of rotator-cuff tears. J Bone Joint
Surg Br 1998;80:624-8.




















