External beam radiation for retinoblastoma: Results, patterns of failure, and a proposal for...
8
Int. J. Radiation Oncology Biol. Phys., Vol. 35, No. I, pp. 12% 112, lYY6 Copyright C lYY6 Elsewer Science Inc. Printed in the USA. All rights reserved 0360.X)16/96 $lS.tK, + .(X) ELSEVIER l Brief Communication SSDI: 0360-3016(95)02133-7 EXTERNAL BEAM RADIATION FOR RETINOBLASTOMA: RESULTS, PATTERNS OF FAILURE, AND A PROPOSAL FOR TREATMENT GUIDELINES J. CARLOS HERNANDEZ, M.D.,* LUTHER W. BRADY, M.D.,* JERRY A. SHIELDS, M.D.,+ CAROL L. SHIELDS, M.D.,+ PATRICK DEPOTTER, M.D.,+ ULF L. KARLSSON, M.D.,* ARNOLD M. MARKOE, M.D.,* BEATRIZ E. AMENDOLA, M.D.* AND ARUN SINGH, M.D.+ *Department of Radiation Oncology, Hahnemann University, Philadelphia, PA, ‘Ocular Oncology Service. Wills Eye Hospital, Thomas Jefferson University, Philadelphia, PA Purpose: To analyze treatment results and patterns of failure following external beam radiation for retino- blastoma and propose treatment guidelines according to specific clinical variables. Methods and Materials: We analyzed 27 patients (34 eyes) with retinoblastoma who received external beam radiation as initial treatment at Hahnemann University Hospital from October 1980 to December 1991 and have been followed for at least 1 year. Of the 34 eyes, 14 were Groups I-II (Reese-Ellsworth classification), 7 were Group HI, and 13 were Groups IV-V. Doses ranged from 34.5-49.5 Gy (mean 44.3 Gy, median 45 Gy) in 1.5-2.0 Gy fractions generally delivered through anterior and lateral wedged pair fields. Results: At a mean follow up of 35.2 months (range 12-93 months), local tumor control was obtained in 44% (15 out of 34) of eyes with external beam radiation alone. Salvage therapy (plaque brachytherapy, cryotherapy, and/or photocoagulation) controlled an additional 10 eyes (29.5%), so that overall ocular survival has been 73.5%. Local tumor control with external beam radiotherapy alone was obtained in 78.5% (11 out of 14) of eyes in Groups I-II, but in only 20% (4 out of 20) of eyes in Groups III-V. A total of 67 existing tumors were identified prior to treatment in the 34 treated eyes and local control with external beam radiation alone was obtained in 87% (46 out of 53) of tumors measuring 15 mm or less and in 50% (7 out of 14) of tumors measuring more than 15 mm. When analyzing patterns of failure in the 19 eyes that relapsed, a total of 28 failure sites were identified and consisted of progression of vitreous seeds in seven instances (25% of failure sites) recurrences from previously existing tumors in 10 instances (36% of failure sites) and development of new tumors in previously uninvolved retina in 11 instances (39% of failure sites). Conclusions: 1) We find that external beam radiation to a dose of 45 Gy in fractions of 1.5 to 2.0 Gy provides adequate tumor control in retinoblastoma eyes Groups I-II (Reese-Ellsworth classification) or tumors measuring 15 mm in diameter or less. Eyes in more advanced group staging or containing tumors larger than 15 mm seem to require higher radiation doses. We propose treatment guidelines for external beam radiation of retinoblastoma that specifically take into account the important clinical variables of tumor stage and patient age. 2) External beam radiation does not prevent the appearance of new tumors in clinically uninvolved retina. Therefore, the traditional belief that external beam radiation can treat the retina “prophylactically” should be seriously questioned. Due to this finding and their significant less morbidity, focal treatment modalities (plaque brachytherapy, photocoagulation and/or cryotherapy), when clinically feasible, should be considered the treatment of choice for intraocular retinoblastoma. External beam radiation should be considered only when focal treatment modalities are not clinically indicated. Retinoblastoma, Radiotherapy, Failure patterns, Technique, Treatment guidelines. INTRODUCTION Retinoblastoma is the most common intraocular malig- nancy in childhood and second only to uveal melanoma as the most common primary intraocular malignancy (33). The tumor arises from multipotential retinal cells, which are capable of differentiating into specialized photorecep- tor cells. Although estimates vary, it occurs with a fre- Reprint requests to: J. Carlos Hemandez, M.D., Department of Radiation Oncology, University of Texas HSC at San Anto- nio, 7703 Floyd Curl Drive, San Antonio, TX 78229. Acknowledgements-The authors wish to thank David A. Lightfoot, M.A., Kathy Walsh, RTT, Sheila A. McGlynn, RTT, and Gary Antonelli, RTT, for their valuable assistance in the treatment of these patients. We also thank the Anesthesiology Department at Hahnemann University Hospital and specifically Dr. Joan Carroll for their close cooperation and expertise. Ms. Lucy Reina provided expert clerical assistance. Accepted for publication 3 August 1995. 125
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of External beam radiation for retinoblastoma: Results, patterns of failure, and a proposal for...

Int. J. Radiation Oncology Biol. Phys., Vol. 35, No. I, pp. 12% 112, lYY6
Copyright C lYY6 Elsewer Science Inc.
Printed in the USA. All rights reserved
0360.X)16/96 $lS.tK, + .(X)
ELSEVIER
l Brief Communication
SSDI: 0360-3016(95)02133-7
EXTERNAL BEAM RADIATION FOR RETINOBLASTOMA: RESULTS, PATTERNS OF FAILURE, AND A PROPOSAL FOR TREATMENT GUIDELINES
J. CARLOS HERNANDEZ, M.D.,* LUTHER W. BRADY, M.D.,* JERRY A. SHIELDS, M.D.,+
CAROL L. SHIELDS, M.D.,+ PATRICK DEPOTTER, M.D.,+ ULF L. KARLSSON, M.D.,*
ARNOLD M. MARKOE, M.D.,* BEATRIZ E. AMENDOLA, M.D.* AND ARUN SINGH, M.D.+
*Department of Radiation Oncology, Hahnemann University, Philadelphia, PA, ‘Ocular Oncology Service. Wills Eye Hospital, Thomas Jefferson University, Philadelphia, PA
Purpose: To analyze treatment results and patterns of failure following external beam radiation for retino- blastoma and propose treatment guidelines according to specific clinical variables. Methods and Materials: We analyzed 27 patients (34 eyes) with retinoblastoma who received external beam radiation as initial treatment at Hahnemann University Hospital from October 1980 to December 1991 and have been followed for at least 1 year. Of the 34 eyes, 14 were Groups I-II (Reese-Ellsworth classification), 7 were Group HI, and 13 were Groups IV-V. Doses ranged from 34.5-49.5 Gy (mean 44.3 Gy, median 45 Gy) in 1.5-2.0 Gy fractions generally delivered through anterior and lateral wedged pair fields. Results: At a mean follow up of 35.2 months (range 12-93 months), local tumor control was obtained in 44% (15 out of 34) of eyes with external beam radiation alone. Salvage therapy (plaque brachytherapy, cryotherapy, and/or photocoagulation) controlled an additional 10 eyes (29.5%), so that overall ocular survival has been 73.5%. Local tumor control with external beam radiotherapy alone was obtained in 78.5% (11 out of 14) of eyes in Groups I-II, but in only 20% (4 out of 20) of eyes in Groups III-V. A total of 67 existing tumors were identified prior to treatment in the 34 treated eyes and local control with external beam radiation alone was obtained in 87% (46 out of 53) of tumors measuring 15 mm or less and in 50% (7 out of 14) of tumors measuring more than 15 mm. When analyzing patterns of failure in the 19 eyes that relapsed, a total of 28 failure sites were identified and consisted of progression of vitreous seeds in seven instances (25% of failure sites) recurrences from previously existing tumors in 10 instances (36% of failure sites) and development of new tumors in previously uninvolved retina in 11 instances (39% of failure sites). Conclusions: 1) We find that external beam radiation to a dose of 45 Gy in fractions of 1.5 to 2.0 Gy provides adequate tumor control in retinoblastoma eyes Groups I-II (Reese-Ellsworth classification) or tumors measuring 15 mm in diameter or less. Eyes in more advanced group staging or containing tumors larger than 15 mm seem to require higher radiation doses. We propose treatment guidelines for external beam radiation of retinoblastoma that specifically take into account the important clinical variables of tumor stage and patient age. 2) External beam radiation does not prevent the appearance of new tumors in clinically uninvolved retina. Therefore, the traditional belief that external beam radiation can treat the retina “prophylactically” should be seriously questioned. Due to this finding and their significant less morbidity, focal treatment modalities (plaque brachytherapy, photocoagulation and/or cryotherapy), when clinically feasible, should be considered the treatment of choice for intraocular retinoblastoma. External beam radiation should be considered only when focal treatment modalities are not clinically indicated.
Retinoblastoma, Radiotherapy, Failure patterns, Technique, Treatment guidelines.
INTRODUCTION
Retinoblastoma is the most common intraocular malig- nancy in childhood and second only to uveal melanoma
as the most common primary intraocular malignancy (33). The tumor arises from multipotential retinal cells, which are capable of differentiating into specialized photorecep- tor cells. Although estimates vary, it occurs with a fre-
Reprint requests to: J. Carlos Hemandez, M.D., Department of Radiation Oncology, University of Texas HSC at San Anto- nio, 7703 Floyd Curl Drive, San Antonio, TX 78229. Acknowledgements-The authors wish to thank David A. Lightfoot, M.A., Kathy Walsh, RTT, Sheila A. McGlynn, RTT, and Gary Antonelli, RTT, for their valuable assistance in the
treatment of these patients. We also thank the Anesthesiology Department at Hahnemann University Hospital and specifically Dr. Joan Carroll for their close cooperation and expertise. Ms. Lucy Reina provided expert clerical assistance.
Accepted for publication 3 August 1995.
125

126 1. J. Radiation Oncology 0 Biology 0 Physics Volume 35, Number 1, 1996
quency of approximately 1 in 15,000 live births and in the United States 200 new cases occur each year (25). There seems to be no predisposition for race or sex, and the average age at diagnosis is 18 months. Due to earlier detection and improved treatment techniques, the mortal- ity from this disease in the US has decreased from over 90% to less than 10% over a few decades. As a result, greater efforts are being directed towards improving ocu- lar and visual prognosis in retinoblastoma survivors.
The management of retinoblastoma should be individual- ized according to specific clinical variables including stage, unilateral vs. bilateral disease, unifocal vs. multifocal involve- ment, tumor location, potential for vision, family history, and patient age. Treatment options include enucleation, external beam radiotherapy, plaque brachytherapy, photocoagulation, cryotherapy, and chemotherapy.
External beam radiation (EBR) is an effective treatment modality that can permit ocular preservation and visual potential. External beam radiation treatment parameters for retinoblastoma are not well defined. The literature reports a wide range of dose fractionation schedules, but the decision for their selection has been largely empirical (4, 5, 8, 19, 31). Failure rates following EBR alone are in the range of 40-70% (Table l), but salvage with the addition of focal treatment modalities permits an overall ocular survival of approximately 80%. Side effects from EBR tend to be dose related and include the production of orbital hypoplasia and an increase in the development of secondary nonocular malignancies, which are currently the most common cause of retinoblastoma deaths in the U.S. It is, therefore, important to more clearly define what are the optimal EBR treatment guidelines that will lead to more effective tumor control while minimizing poten- tial side effects.
We retrospectively reviewed our experience treating retinoblastoma patients with EBR to determine its effect on subsequent tumor control and to identify parameters predictive of outcome.
Table 1. Tumor control and ocular survival following external beam radiation (EBR) for retinoblastoma in different series
Series
No. eyes controlled Overall No. with EBR alone ocular eyes (%) survival*
Cassady et al. (5) 223 Lennox et al. ( 19) 107 Haye et al. (12) 84 Bedford et al. (4) 58 Schipper et al. (31) 54 Egbert et al., (8) 38 Thompson et al. (38) 34 Foote et al. (9) 25 Howarth et al. (17) 12 Current series 34
109 (49) 44 (41)
30 (52) 22 (41)
19 (56) Il(44) 4 (33)
15 (4)
69% 70% 60% 84% 81% 58% 70% 80%
100% 73%
* Results reflect tumor control with EBR plus salvage with focal treatment modalities.
METHODS AND MATERIALS
A total of 34 eyes in 27 patients with retinoblastoma received EBR as initial treatment at Hahnemann Univer- sity Hospital between October 1980 and December 199 1, and have been followed for at least 1 year. The group consists of 14 boys and 13 girls with a mean age at treatment of 13.6 months (range 2 weeks to 16 months). Twenty-three patients had no family history of retinoblas- toma (mean age 14.9 months) and 4 patients had a positive family history (mean age 6.3 months). Nineteen patients presented with bilateral involvement and 8 patients pre- sented with unilateral disease. In the 19 patients with bilateral involvement, a total of 26 eyes received external beam radiation, 10 eyes had been enucleated due to ad- vanced disease without visual potential, 1 eye (with one tumor) had been treated with plaque brachytherapy alone, and 1 eye (with one tumor) was treated with photocoagu- lation alone. Of the 34 eyes treated, 4 were Reese-Ells- worth (RE) Group I, 10 were RE Group 11, 7 were RE Group 111, 2 were RE Group IV and 11 were RE Group V (3 in RE Group Va and 8 in RE Group Vb.) Of interest, one of the patients with bilateral involvement additionally presented a pineal lesion by computed tomography (CT) and magnetic resonance imaging (MRI) compatible with the diagnosis of trilateral retinoblastoma.
The most frequent presenting finding was leukocoria in 16 patients (60%) followed by strabismus in 6 patients (22%), visual difficulties in 2 patients, routine screening because of family history in 2 patients, and as an inciden- tal finding following head trauma in 1 patient. The mean duration of presenting findings prior to diagnosis was 1.7 months.
In addition to history, physical examination, and rou- tine blood work, all patients underwent examination under anesthesia with indirect ophthalmoscopy and scleral de- pression to determine the size, number, and location of tumors. Tumor thickness was determined by ultrasonogra- phy. Detailed drawings and retinal photographs were ob- tained in all patients to complete documentation. The di- agnosis of retinoblastoma could be made clinically in all patients without need for fine needle aspiration biopsy. Retinal examination of the parents and siblings was also performed. In those patients seen from 1980 to 1989 (17 patients), staging workup consisted additionally of com- puted tomography (CT) and/or magnetic resonance im- aging (MRI) of the brain and orbits, lumbar puncture with spinal fluid cytology, bone marrow aspirate, and chromosome analysis. None of these patients presented evidence of extraocular disease. In those patients seen after 1989 (10 patients), staging workup included CT and/ or MRI of the brain and orbits and chromosome analysis, but lumbar puncture and bone marrow aspirate were not routinely done unless there was clinical or radiographic suspicion of optic nerve or extraocular extension. Only one patient in this group presented extraocular disease, detected by head CT, consisting of pineal involvement
External beam radiation for reninoblastoma: results. patterns 0 J. C. HERNANDEZ et al. 127
(trilateral retinoblastoma) and no additional areas of tu- mor involvement were detected following lumbar punc-
ture and bone marrow aspirate. Others have also noted the low yield of routine lumbar punctures and bone marrow aspirates in patients with limited intraocular retinoblas- toma (27).
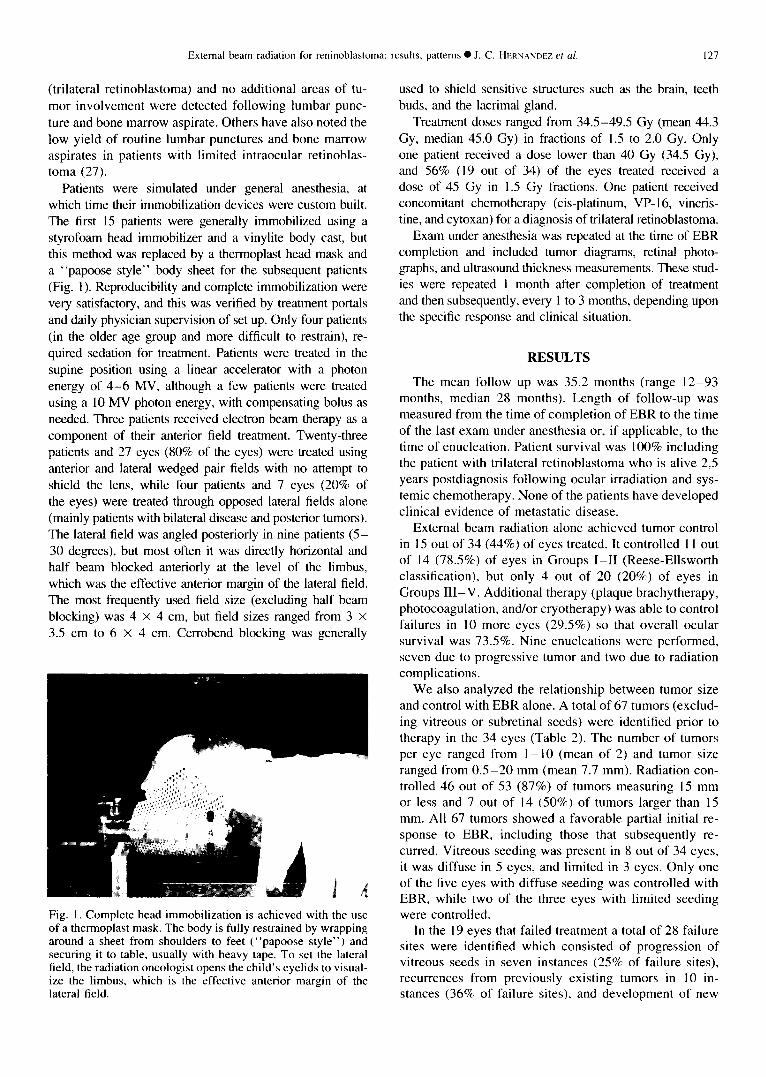
Patients were simulated under general anesthesia, at which time their immobilization devices were custom built. The first 15 patients were generally immobilized using a Styrofoam head immobilizer and a vinylite body cast, but this method was replaced by a thermoplast head mask and a “papoose style” body sheet for the subsequent patients (Fig. 1). Reproducibility and complete immobilization were very satisfactory, and this was verified by treatment portals and daily physician supervision of set up. Only four patients (in the older age group and more difficult to restrain), re- quired sedation for treatment. Patients were treated in the supine position using a linear accelerator with a photon energy of 4-6 MV, although a few patients were treated using a 10 MV photon energy, with compensating bolus as needed. Three patients received electron beam therapy as a
component of their anterior field treatment. Twenty-three patients and 27 eyes (80% of the eyes) were treated using anterior and lateral wedged pair fields with no attempt to shield the lens, while four patients and 7 eyes (20% of the eyes) were treated through opposed lateral fields alone (mainly patients with bilateral disease and posterior tumors). The lateral field was angled posteriorly in nine patients (5- 30 degrees), but most often it was directly horizontal and half beam blocked anteriorly at the level of the limbus, which was the effective anterior margin of the lateral field. The most frequently used field size (excluding half beam blocking) was 4 x 4 cm, but field sizes ranged from 3 X
3.5 cm to 6 x 4 cm. Cerrobend blocking was generally
Fig. 1. Complete head immobilization is achieved with the use of a thermoplast mask. The body is fully restrained by wrapping around a sheet from shoulders to feet (“papoose style”) and securing it to table, usually with heavy tape. To set the lateral field, the radiation oncologist opens the child’s eyelids to visual- ize the limbus, which is the effective anterior margin of the lateral field.
used to shield sensitive structures such as the brain, teeth buds, and the lacrimal gland.
Treatment doses ranged from 34.5-49.5 Gy (mean 44.3 Gy, median 45.0 Gy) in fractions of 1.5 to 2.0 Gy. Only one patient received a dose lower than 40 Gy (34.5 Gy), and 56% (19 out of 34) of the eyes treated received a dose of 45 Gy in 1.5 Gy fractions. One patient received concomitant chemotherapy (cis-platinum, VP- 16, vincris- tine, and cytoxan) for a diagnosis of trilateral retinoblastoma.
Exam under anesthesia was repeated at the time of EBR completion and included tumor diagrams, retinal photo- graphs, and ultrasound thickness measurements. These stud- ies were repeated 1 month after completion of treatment and then subsequently, every 1 to 3 months, depending upon the specific response and clinical situation.
RESULTS
The mean follow up was 35.2 months (range 12-93 months, median 28 months). Length of follow-up was measured from the time of completion of EBR to the time of the last exam under anesthesia or, if applicable, to the time of enucleation. Patient survival was 100% including the patient with trilateral retinoblastoma who is alive 2.5 years postdiagnosis following ocular irradiation and sys- temic chemotherapy. None of the patients have developed clinical evidence of metastatic disease.
External beam radiation alone achieved tumor control in 15 out of 34 (44%) of eyes treated. It controlled 1 1 out of 14 (78.5%) of eyes in Groups I-II (Reese-Ellsworth classification), but only 4 out of 20 (20%) of eyes in Groups III-V. Additional therapy (plaque brachytherapy, photocoagulation, and/or cryotherapy) was able to control failures in 10 more eyes (29.5%) so that overall ocular survival was 73.5%. Nine enucleations were performed, seven due to progressive tumor and two due to radiation complications.
We also analyzed the relationship between tumor size and control with EBR alone. A total of 67 tumors (exclud- ing vitreous or subretinal seeds) were identified prior to therapy in the 34 eyes (Table 2). The number of tumors per eye ranged from 1 - 10 (mean of 2) and tumor size ranged from 0.5-20 mm (mean 7.7 mm). Radiation con- trolled 46 out of 53 (87%) of tumors measuring 15 mm or less and 7 out of 14 (50%) of tumors larger than 15 mm. All 67 tumors showed a favorable partial initial re- sponse to EBR, including those that subsequently re- curred. Vitreous seeding was present in 8 out of 34 eyes, it was diffuse in 5 eyes, and limited in 3 eyes. Only one of the five eyes with diffuse seeding was controlled with EBR, while two of the three eyes with limited seeding were controlled.
In the 19 eyes that failed treatment a total of 28 failure sites were identified which consisted of progression of vitreous seeds in seven instances (25% of failure sites), recurrences from previously existing tumors in 10 in- stances (36% of failure sites), and development of new

128 I. J. Radiation Oncology l Biology 0 Physics Volume 3.5, Number I, 1996
Table ‘2. Tumor control following external beam radiation (EBR) alone according to tumor size
Tumor size (maximum basal
diameter)
<5 mm 5.1-10 mm 10.1-15 mm >15 mm
Total
Number of tumors
32 14 7
14
67
Number of tumors controlled
with EBR alone (%)
28 (87.5) 13 (93) 5 (71.5) 7 (50)
53 (79)
tumors in previously uninvolved retina in 11 instances (39% of failure sites). Failures from previously existing tumors were more frequent in large tumors (7 out of 14 or 50% of tumors measuring > 15 mm recurred) com- pared to smaller tumors (7 out of 53 or 21.5% of tumors 5 15 mm recurred).
Complications requiring enucleation occurred in 2 of the 34 eyes. Both eyes presented initially with large tu- mors and both received plaque brachytherapy for recur- rence in addition to EBR. The first developed neovascu- la~zation and hemo~hage and the second developed glau- coma. Lens changes were analyzed in the 34 treated eyes. Of the 10 eyes followed from 12 to 24 months, 3 were enucleated and none of the remaining 7 evaluable eyes showed lens changes. Of the 16 eyes followed from 24- 36 months, 5 were enucleated, and of the 11 evaluable eyes, 7 (64%) showed early posterior subcapsular lens changes, which did not affect visual acuity. Of the eight eyes followed for more than 36 months, one was enucle- ated, and all seven evaluable eyes (100%) showed poste- rior subcapsular lens changes, which required lens extrac- tion in three cases. In the three cases, surgery was per- formed without difficulty and the patients were prescribed aphakic lenses. No significant anterior segment complica- tions have been noted so far in our series. Longer follow- up is required to assess other therapy-related events such as orbital hypoplasia and secondary malignant neoplasms.
DISCUSSION
It is important to define guidelines for the treatment of retinoblastoma with external beam radiation (EBR) that will lead to more effective tumor control while decreasing potential side effects. Impo~ant treatment variables in- clude total dose, fractionation, and treatment technique. Important patient variables include extent of disease, pa- tient age, potential for useful vision, and heritable vs. nonheritable disease.
A clear dose response for control of retinoblastoma with EBR has not been documented. More than half of our patients were treated to a dose of 45 Gy using a relatively low dose per fraction of 1.5 Gy in an attempt to decrease late side effects. Our rest-&s in terms of tumor control and ocular survival compare favorably with those
in other series where higher doses per fraction were used (Table 1). Cassady el al. in the largest U.S. series of retinoblastoma patients treated with EBR, found no sig- nificant difference in local tumor control when doses of 32.5 to 35 Gy were used compared to doses of 40 to 45 Gy (fractions of 3.3 to 4.0 Gy administered three times per week) even after correcting for tumor stage (5). They did not correct for technique used, even though kilovolt- age energy was used for the first 4 years of the study (ipsilateral temporal and contralateral nasal oblique fields) while megavoltage energy was used for the remaining 5 years (single lateral field with ante~or margin at the bony cantus). Messmer ef ul., however, reported a higher recur- rence rate of 49% in 71 retinoblastoma eyes treated with EBR to a dose of approximately 40 Gy (range 37-41 Gy), compared to a 22% recurrence rate in 40 eyes treated to a dose of 50 Gy (range 49-51 Gy) even though the latter group had significantly larger tumors (23). The frac- tionation schedule was not stated. Similarly, a high failure rate (8 out of 12 eyes or 67% recurrences) was reported in one series that used comparatively low EBR doses of 35-45 Gy in 2.0 Gy fractions (17). Therefore, it is reasonable to assume that even though a clear dose re- sponse for control of retinoblastoma has not been docu- mented, there is a dose threshold below which the failure rate would become excessive. Failure rates seem to be- come higher at doses below 40 Gy in fractions of 2.0 Gy or less.
In our study, we found that tumor control rates were closely related to tumor size and Reese-Ellsworth (RE) group staging. We obtained a relatively satisfactory tumor control rate of 78.5% for early stage tumors (RE Groups I-II), but a control rate of only 20% for more advanced tumors (RE Groups III-V) following EBR alone with doses of approximately 45 Gy in 1.5 to 2.0 Gy per frac- tion. The correlation between tumor stage and tumor con- trol is consistent with the results reported in other series. Cassady et al. obtained a tumor control rate of 73% in eyes RE Groups I-III vs. a 20% control rate in eyes Groups IV-V following EBR alone (5). McCormick et al. obtained local control in 83% of eyes RE Groups I- III vs. 35% in 31 eyes Groups IV-V treated without lens sparing (20). Foote et al. reported tumor control in only 2 out of IO eyes classified as RE Groups IV-V following EBR alone (9). Using EBR and focal therapy, Egbert et al. were able to save 80% of eyes in RE Groups I-III, but only 29% of those in Groups IV-V (8). In the previ- ous series, similar doses were used to treat the higher stage tumors and the lower stage ones. Furthermore, in our series we found a favorable control rate of 87% for tumors measuring 15 mm or less and a less favorable control rate of 50% in tumors larger than 15 mm. Simi- larly, Foote et al. were able to control 91% (53 out of 58) of tumors measuring 16 mm or less and only 67% (4 out of 6) of tumors larger than 16 mm using doses of approximately 45 Gy in 1.8 Gy fractions (9). In an analy- sis of 290 eyes treated by EBR and other conservative

External beam radiation for reninoblastoma: results, patterns 0 J. C. HF.RNANIXL et a/. 129
methods, DeSutter et al. found a success rate of 9 1% in tumors smaller than 6.5 mm, 94.5% success rate in tumors 6.5- 16 mm, 7 1.4% in tumors larger than 16 mm and 33% when the tumor was larger than half the retina (6). DeSutter et af.‘s high success rates include EBR in addi- tion to focal salvage modalities.
By reviewing the above data, it is evident that treatment results following EBR are closely related to stage and tumor size. Doses of approximately 45 Gy in 1.5 to 2.0 Gy per fraction appear to provide satisfactory results for eyes in Groups I-II Reese-Ellsworth classification or con- taining tumors smaller than 16 mm. In these patients, higher radiation doses seem unnecessary and can result in increased morbidity. In contrast, patients with larger tumors have poor control rates with EBR at these doses and in these cases increasing the dose could potentially improve outcome.
Relative to vitreous seeding, Hopping et al. stated a difference in visual prognosis when the seeding was local- ized vs. diffuse (15, 16). DeSutter et ul., in an analysis of 590 retinoblastoma cases, found a treatment failure rate of 75% for tumors with diffuse vitreous seeding, 25% with localized vitreous seeding and 17.5% when vitreous seeding was absent (6). Therefore, although the Reese- Ellsworth staging system does not take this difference into account, not all cases of vitreous seeding have the same prognostic impact. Although our patient numbers are too small to make similar correlations, two of our three eyes with localized vitreous seeding were controlled with EBR alone, while only one of five eyes with diffuse vitreous seeding was controlled.
Although an increase in tumor dose could theoretically result in improved tumor control, there is a dose threshold above which potential ocular complications would be- come unacceptable. Parsons et al., in an analysis of 74 adult patients whose field of radiation included the eye, found only one severe retinal injury at doses of 50 Gy conventional fractionation while all but one patient who received doses in the 60 Gy range (1.7 to 2.0 Gy per fraction) developed severe retinal injury (24). There were few patients in the 50 to 55 Gy range, but it was clear that in adults, the sigmoid dose curve for ocular complications became steep between 50 and 60 Gy. Less information is available on ocular radiation tolerance in children. In a series of 81 retinoblastoma eyes treated with EBR, Messmer et al. found that within a dose range of 36-51 Gy, the location of the tumor (36%) or cataract (15%) were the main factors responsible for poor visual acuity, whereas radiation retinopathy and/or optic neuropathy oc- curred in only three eyes (which in addition had received ‘“Co plaques) (22). In children treated for retinoblastoma, Egbert et ul. had a 21% (8 out of 38 eyes) rate of enucle- ation for radiation complications following doses of 50 to 60 Gy fractionated over 3.5 to 6 weeks (8). This high enucleation rate suggests a rise in radiation complications above doses of 50 Gy. In contrast, there were no enucle- ations for radiation complications in the series reported
by Foote et al. (9) (39 to 51Gy at 1.8 to 3.0 Gy per fraction); or Thompson et al. (38), (30 to 50 Gy at 10 Gy per week in three to five fractions) after the first course
of EBR. It is difficult to make radiobiological compari- sons from series to series, because different fractionation schemes were used even within the same institutions. However, the data suggests that, like in adults, a greater risk for ocular complications exists in children when doses higher than 50 Gy in 2.0 Gy fractions are used.
We also believe that patient age should be taken into consideration when determining EBR schedules for retino- blastoma. Younger patients are at a higher risk of developing radiation-induced side effects. The visual acuity of a full- term baby at birth is only 20 out of 400 (10). This is attrib- uted to the short diameter of the newborn eye and retinal immaturity, although incomplete myelination of the optic nerve may also be a factor. Of all ocular structures at the time of birth, the retina is the least developed functionally. Specifically, the macula is the last retinal area to complete development and even after birth, the macular cones elon- gate and undergo other histological changes (18). The mac- ula is not fully mature until approximately 4 months after birth (21). Patients in their first months of life, therefore, seem more susceptible to radiation-induced complications, particularly those that can affect their central vision. Unfor- tunately, even patients whose disease is diagnosed at an early age (first 6 months of life) can commonly present with advanced intraocular stage (3). We believe that due to their higher vulnerability to radiation-induced side effects, partic- ular caution is warranted when treating patients younger than 6 months.
Based on the considerations discussed above, the Hah- nemann University/Wills Eye Group has developed gen- eral guidelines for the treatment of retinoblastoma with external beam radiation that take into account the im- portant clinical variables of tumor stage and patient age (Table 3). Patients younger than 6 months with tumors smaller than 16 mm are treated to a dose of 40-45 Gy in 1.5 Gy fractions (doses closer to 40 Gy in newborns and patients with a low tumor burden and doses closer to 45 Gy in patients closer to 6 months of age and with a higher tumor burden). Patients younger than 6 months with any tumor equal to or larger than 16 mm or with
Table 3. Hahnemann/Wills guidelines for the treatment of retinoblastoma with external beam radiation
Age
Stage <6 months ~6 months
40-45 Gy in 45 Gy in 1.5-2.0 Tumors < 16 mm 1.5 Gy fr Gy fr Any tumor 2 16 mm or
localized vitreous 48 Gy in 1.5 50 Gy in 1.5-2.0 Gy seeding Gy fr fr
Diffuse vitreous seeding or tumor involving 49.5 Gy in 50-54 Gy in 1.5- 2 l/2 of retina 1.5 Gy fr 2.0 Gy fr

130 I. J. Radiation Oncology 0 Bioiogy l Physics Volume 35. Number I, 1996
localized vitreous seeding are treated to a dose of 48 Gy in 1.5 Gy fractions. Patients younger than 6 months with extensive vitreous seeding or tumor involving half or more of the retina are treated to a dose of 49.5 Gy in I .5 Gy fractions. Patients older than 6 months with tumors smaller than 16 mm are treated to a dose of 45 Gy in 1.5-2.0 Gy fractions. Patients older than 6 months with any tumor equal to or larger than 16 mm or with localized vitreous seeding are treated to a dose of 50 Gy in 1.5-2.0 Gy fractions. Patients older than 6 months with extensive vitreous seeding or tumor involving half or more of the retina are also treated to a dose of 50-54 Gy in 1.5-2.0 Gy fractions depending upon overall tumor burden and age. We should point out that we have not found tumor location anterior to the equator to be an adverse prognos- tic factor following EBR with anterior and lateral compo- nents so this variable is not factored in our choice of dose. Finally, in bilateral cases, each eye is assessed indi- vidually and the worse affected eye is not routinely enu- cleated.
H~ihnernun~~ll.~ EBR technique
In addition to total dose and fractionation, technique is an important variable in the treatment of retinoblastoma. Lens-sparing techniques have resulted in higher recur- rence rates when compared to techniques that include an anterior field component. McCormick, et al. reported a 67% failure rate with the use of a lens-sparing technique compared to a 17% failure rate when it was not used (20). Foote et ul. also reported a high failure rate of 7 I % when a lens-sparing technique was used compared to 36% when it was not used (9). Schipper et al. have described the use of a lateral field technique that attempts to avoid marginal misses while sparing the lens (30). Localization is obtained by using suction contact lenses that immobi- lize each eye and are connected to a rigid metal arm, which is fixed to the accelerator gantry. Their results in a series of 39 patients showed good tumor control (Table I), but 18 patients developed posterior cataracts in spite of the use of this technique (31). This is not surprising, considering the negligible distance that exists between the posterior aspect of the lens and the ora set-rata (only 1-2 mm). A significant disadvantage of Schipper’s tech- nique is that it requires general anesthesia for each treat- ment so that children are treated three times per week at doses per fraction of 3 Gy or higher to avoid frequent inductions. Schmid et al. found a correlation between radiation comp1ications and the use of high doses per fraction (32). Of 45 patients with retinoblastoma treated with EBR, 10 developed radiation retinopathy, and this complication correlated significantly with the use of hy- pofractionaton 0, < 0.01). Our technique allowed us ex- cellent immobilization without need for general anesthe- sia. This permitted us the use of fraction sizes of less than 2.0 Gy, which theoretically would decrease the likeli- hood of late side effects. By any technique, radiation- induced cataracts are very difficult to avoid, but if they develop and interfere with vision, they can be treated surgically with minimal morbidity.
We have elected to generally use anterior and lateral field components with no attempt to spare the lens to treat the entire retina. The lateral field is a photon field, which is half-beam blocked anteriorly. A 4 MV photon energy is preferred, but if another energy is used bolus may be considered for the lateral held, depending upon the photon energy used and the soft tissue thickness measured on the CT scan. The effective anterior margin of this half- beamed lateral field is placed at the limbus, which is verified by the treating physician each day. This way, we are able to spare most of the anterior segment from the lateral field (Fig. 2). After the margins of the lateral field have been set, the patient is treated with his/her eyes closed (tape may be used to close them) so that the minor lacrimal glands and the anterior part of the eyelids can be spared. For treatment of the anterior field we include the orbit and a small margin around it to correct for pen- umbra. The main lacrimal gland is blocked from the ante- rior field. When designing the anterior field it is important to remember that the sagittal length of the eye at 6 months postnatally is approximately 18.2 mm and at 12 months postnatally it is 20.6 mm (IS). Therefore, there is the possibility of underdosing the anterior retina when using linear accelerator-based photons (D,,,,, 12- 15 mm). An alternative is the use of electrons for the anterior compo- nent of the treatment (in this situation the eyelids are taped open during treatment of this field to avoid their effect as bolus). The electron energy chosen depends upon the actual eyeball length as per ultrasound and/or CT scan. Although the use of electrons anteriorly will result in an increased gradient dose to the anterior segment and palpebral lacrimal glands, these structures will be ex- cluded from the lateral photon field component and, there-
I r’ / / I I I /
Fig. 2. Diagram illustrating the area treated through the lateral EBR field for retinoblastoma. The held is half-beam blocked anteriorly and shaped in all directions by the block, not the collimator, to minimize penumbra. After the anterior margin of the lateral field has been confirmed to be at the hmbus by the treating physician, the patient’s eyes are closed for treatment so a portion of the palpebral lacrimal structures can be spared. The cornea and most of the anterior segment are also spared from the Iateral field component. No attempt is made to spare the lens.
External beam radiation for reninoblastoma: results, patterns 0 J. C. HERNANDEL et al. 131
fore, will only receive a portion of the total dose (Fig. 1). Please note that we would not advise delivering the entire treatment course through a single anterior electron field. An additional advantage of using electrons for the anterior field component is the avoidance of unnecessary brain irradiation from a photon exit dose. One should remember that brain myelination is basically a postnatal event that progresses steadily over the first few years of life and that the volume of brain receiving exit photon radiation can be considerable (at birth the orbital opening comprises almost 50% of the height of the face compared to approximately 30% in the adult) (7). Although to date no neurologic morbidity from this exit photon dose has been documented, it would seem prudent to avoid it if possible.
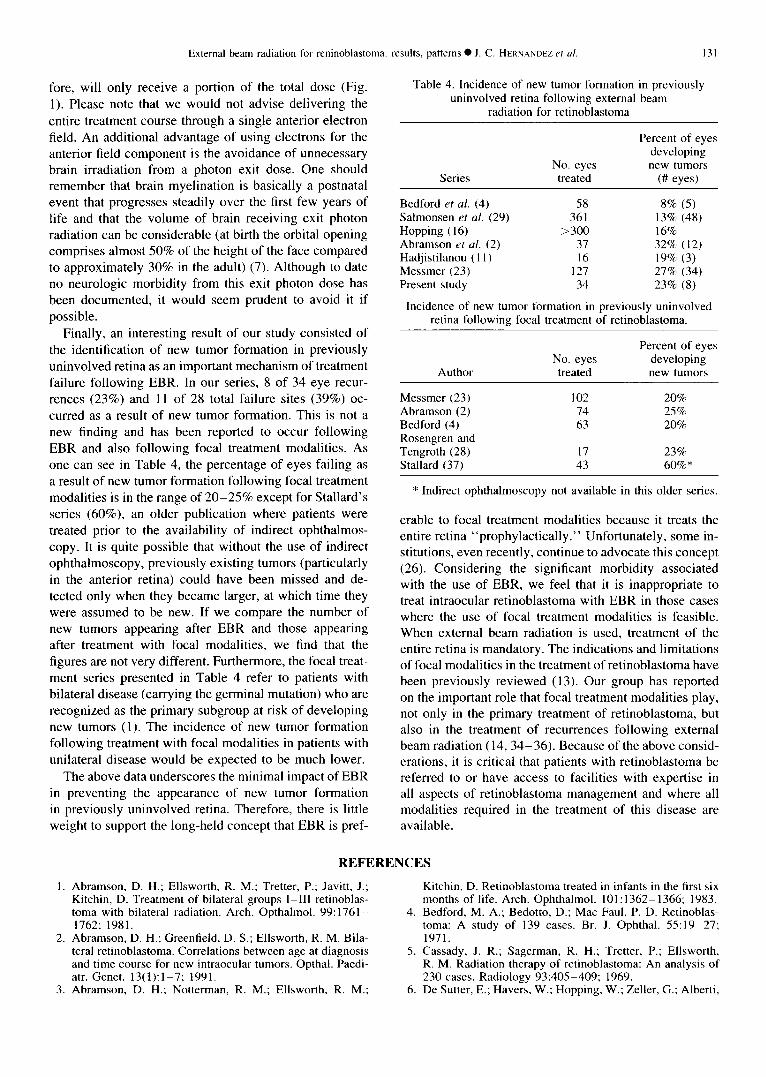
Finally, an interesting result of our study consisted of the identification of new tumor formation in previously uninvolved retina as an important mechanism of treatment failure following EBR. In our series, 8 of 34 eye recur- rences (23%) and 11 of 28 total failure sites (39%) oc- curred as a result of new tumor formation. This is not a new finding and has been reported to occur following EBR and also following focal treatment modalities. As one can see in Table 4, the percentage of eyes failing as a result of new tumor formation following focal treatment modalities is in the range of 20-25% except for Stallard’s series (60%), an older publication where patients were treated prior to the availability of indirect ophthalmos- copy. It is quite possible that without the use of indirect ophthalmoscopy, previously existing tumors (particularly in the anterior retina) could have been missed and de- tected only when they became larger, at which time they were assumed to be new. If we compare the number of new tumors appearing after EBR and those appearing after treatment with focal modalities, we find that the figures are not very different. Furthermore, the focal treat- ment series presented in Table 4 refer to patients with bilateral disease (carrying the germinal mutation) who are recognized as the primary subgroup at risk of developing new tumors (1). The incidence of new tumor formation following treatment with focal modalities in patients with unilateral disease would be expected to be much lower.
The above data underscores the minimal impact of EBR in preventing the appearance of new tumor formation in previously uninvolved retina. Therefore, there is little
weight to support the long-held concept that EBR is pref-
Table 4. Incidence of new tumor formation in previously uninvolved retina following external beam
radiation for retinoblastoma
Percent of eyes developing
No. eyes new tumors Series treated (I# eyes)
Bedford et al. (4) 58 8% (5) Salmonsen ef al. (29) 361 13% (48) Hopping ( 16) >300 16% Abramson et al. (2) 37 32% (12) Hadjistilanou ( I 1) 16 19% (3) Messmer (23) 127 27% (34) Present study 34 23% (8)
Incidence of new tumor formation in previously uninvolved retina following focal treatment of retinoblastoma.
Percent of eyes No. eyes developing
Author treated new tumors
Messmer (23) 102 20% Abramson (2) 74 25% Bedford (4) 63 20% Rosengren and Tengroth (28) 17 23% Stallard (37) 43 60%*
* Indirect ophthalmoscopy not available in this older series.
erable to focal treatment modalities because it treats the entire retina “prophylactically.” Unfortunately, some in- stitutions, even recently, continue to advocate this concept (26). Considering the significant morbidity associated with the use of EBR, we feel that it is inappropriate to treat intraocular retinoblastoma with EBR in those cases where the use of focal treatment modalities is feasible. When external beam radiation is used, treatment of the entire retina is mandatory. The indications and limitations of focal modalities in the treatment of retinoblastoma have been previously reviewed (13). Our group has reported on the important role that focal treatment modalities play, not only in the primary treatment of retinoblastoma, but also in the treatment of recurrences following external beam radiation (14,34-36). Because of the above consid- erations, it is critical that patients with retinoblastoma be referred to or have access to facilities with expertise in all aspects of retinoblastoma management and where all modalities required in the treatment of this disease are available.
REFERENCES
Abramson, D. H.; Ellsworth, R. M.; Tretter, P.; Javitt, J.; Kitchin, D. Treatment of bilateral groups I-III retinoblas- toma with bilateral radiation. Arch. Opthalmol. 99: 1761- 1762; 1981.
4.
Abramson, D. H.; Greenfield, D. S.; Ellsworth, R. M. Bila- teral retinoblastoma. Correlations between age at diagnosis and time course for new intraocular tumors. Opthal. Paedi- atr. Genet. 13(1):1-7; 1991.
5.
Abramson, D. H.; Notterman, R. M.; Ellsworth, R. M.; 6.
Kitchin, D. Retinoblastoma treated in infants in the first six months of life. Arch. Ophthalmol. 101: 1362- 1366; 1983. Bedford, M. A.; Bedotto, D.; Mac Faul, P. D. Retinoblas- toma: A study of 139 cases. Br. J. Ophthal. 55: 19-27; 1971. Cassady, J. R.; Sagerman, R. H.; Tretter, P.; Ellsworth, R. M. Radiation therapy of retinoblastoma: An analysis of 230 cases. Radiology 93:405-409; 1969. De Sutter, E.; Havers, W.; Hopping, W.; Zeller, G.; Alberti,

132 I. J. Radiation Oncology 0 Biology 0 Physics Volume 35. Number I, 1996
7.
8.
W. The prognosis of retinoblastoma in terms of globe sav- ing treatment. A computer assisted study. Part I. Ophthal. Paediatr. Genet. 8(2):77-84; 1987. Doxanas, M. T.; Anderson, R. C. Clinical orbital anatomy. Baltimore, MD: Williams and Wilkins; 1970. Egbert, P. R.; Donaldson, S. S.; Moazed, K.; Rosenthal, A. R. Visual results and ocular complications following radiotherapy for retinoblastoma. Arch. Ophthalmol. 96: 1826- 1830; 1978. Foote, R. L.; Garretson, B. R.; Schomberg, P. J.; Buskirk, S. J.; Robertson, D. M.; Earle, J. D. External beam radiation for retinoblastoma: Patterns of failure and dose response analysis. Int. J. Radiat. Oncol. Biol. Phys. 16:823-830; 1989.
23.
9. 24.
10.
Il.
25.
26.
12. 27.
13. 28.
14.
30.
15.
Greenwald, M. J. Visual development in infancy and child- hood. Pediatr. Clin. North Am. 30:977-993; 1983. Hadgistilanou, T.; Greco, G.; Frezzoti, R. Recurrent and new tumors during conservative treatment of bilateral reti- noblastoma. Ophthal. Paediatr. Genet. 12(2):79-84; 1991. Haye, C.; Desjardins, L.; Elmaleh, C.; Schlienger, P.; Zucker, J. M.; Laurent, M. Prognosis and treatment of reti- noblastoma, 105 cases treated at Institut Curie. Ophthal. Paediatr. Genet. 10: 15 1 - 155; 1989. Hemandez, J. C.; Brady, L. W.; Shields, J. A. Shields, C. L. DePotter, P. Radiotherapy of ocular tumors. In: Tob- ias, J. S.; Thomas, P. R., eds. Current radiation oncology, 1st ed. London: Edward Arnold Publishers; 1994. Hemandez, J. C.; Brady, L. W.; Shields, J. A.; Shields, C. L.; Amendola, B. E. Plaque brachytherapy in the treat- ment of retinoblastoma. In: Alberti, W.; Sagerman, R. H., eds. Radiotherapy of intraocular and orbital tumors. Berlin: Springer Verlag; 1993. Hopping, W. The new Essen prognosis classification for conservative sight-saving treatment of retinoblastoma. In: Intraocular tumors. Berlin: Akademieverlag; 1983:497- 502.
29.
31.
16. Hopping, W.; Alberti, W.; Havers, W.; Passarge, E.; Zeller, G.; DeSutter, E. Das Retinoblastoma. In: Lund, 0. E.; Waubke, T. N., eds. Die Augenerkrankungen in Kinde- salter. Stuttgart: Enke; 1985:199-217. Howarth, C.; Meyer, D.; Hustu, 0.; Johnson, W. W.; Shanks, E.; Pratt, C. Stage-related combined modality treat- ment of retinoblastoma. Cancer 48:851-858; 1980. Isenberg, S. H. The eye in infancy. Chicago: Year Book Med. Publishers, Inc.; 1989:40. Lennox, E. L.; Draper, G. J.; Sanders, B. M. Retinoblas- toma: A study of natural history and prognosis of 268 ‘cases. Br. Med. J. 3:731-734; 1975. McCormick, B.; Ellsworth, R.; Abramson, D.; Haik, B.; Tome, J.; Grabowski, E.; LoSasso, T. Radiation therapy for retinoblastoma: Comparison of results with lens-sparing vs. lateral beam techniques. Int. J. Radiat. Oncol. Biol. Phys. 15:567-574; 1988. McDonell, J. M. Ocular embriology and anatomy. In: Ryan, S. J., ed. Retina. St. Louis, MO: C. V. Mosby Company; 1989. Messmer, E. P.; Fritze, H.; Mohr, C.; Heinrich, T.; Sa-
32.
17. 33.
34.
18.
19. 35.
36. 20.
21.
22.
37.
38.
verwein, W.; Havers, W.; Hersthemke, B.; Hopping, W. Long-term treatment effects in patients with bilateral retino- blastoma: Ocular and mid-facial findings. Graefe’s Arch. Clin. Exp. Ophthalmol. 229:309-3 14; 199 1. Messmer, E. P.; Saverwein, W.; Heinrich, T.; Hopping, W.; Klueter-Reckmann, D.; Bomfeld, N.; Sack, H.; Forster, J.; Havers, W. New and recurrent tumor foci following local treatment as well as external beam radiation in eyes of patients with hereditary retinoblastoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 228:426-43 1; 1990. Parsons, J. T.; Fitzgerald, C. R.; Hood, C. I.; Ellingwood, K. E.; Bova, P. J.; Million, R. R. The effects of irradiation on the eye and optic nerve. Int. J. Radiat. Oncol. Biol. Phys. 9:609-622; 1983. Pendegrass, T. W. Incidence of retinoblastoma in the U.S. Arch. Ophthalmol. 98: 1204- 12 10; 1980. Plowman, P. N.; Kingston, J. E.; Hungerford, J. D. Prophy- lactic retinal radiotherapy has an exceptional place in the management of familial retinoblastoma. Br. J. Cancer 68:743-745; 1993. Pratt, C. B.; Meyer, D.; Chenaille, P.; Crom, D. B. The use of bone marrow aspirations and lumbar punctures at the time of diagnosis of retinoblastoma. J. Clin. Oncol. 7: 140- 143; 1989. Rosengren, B.; Tengroth, B. Retinoblastoma treated with a CO60 applicator. Acta. Radiol. Ther. Phys. Biol. 16:l IO- 116; 1977.
Salmonsen, P. C.; Ellsworth, R. M.; Kitchin, F. D. The occurence of new retinoblastoma after treatment. Trans. Am. Acad. Ophthalmol. Otolaryngol. 86:837-840; 1979. Schipper, J. An accurate and simple method for megavol- tage radiation therapy of retinoblastoma. Radiother. Oncol. 1:31-41; 1983. Schipper, J.; Tan, K. E.; Van Peperzeel, H. A. Treatment of retinoblastoma by precision megavoltage radiation therapy. Radiother. Oncol. 3:117-132; 1985. Schmid, C.; Coucke, P.; Balmer, A.; Wellman, D.; Guil- lemin, C.; Mirimanoff, R. Retinoblastoma: A retrospective study of external beam radiation at CHUV-Lausanne. Schweiz Med. Wschr. 1225:45; 1992. Shields, J. A.; Shields, C. L. Intraocular tumors: A text and atlas. Philadelphia, PA: W. B. Saunders Company; 1992. Shields, J. A.; Shields, C. L.; Parsons, H.; Giblin, M. E. The role of photocoagulation in the management of retino- blastoma. Arch. Ophthalmol. 108:205-208; 1990. Shields, J. A.; Parsons, H.; Shields, C. L.; Giblin, M. E. The role of cryotherapy in the management of retinoblas- toma. Am. J. Ophthalmol. 108:260-264; 1989. Shields, C. L.; Shields, J. A.; DePotter, P.; Minelli, S.; Hemandez, J. C.; Brady, L. W.; Cater, J. R. Plaque radio- therapy in the management of retinoblastoma. Use as pri- mary and secondary treatment. Ophthalmology lOO(2): 216-224; 1993. Stallard, H. B.; Doyne Memorial lecture. The conservative treatment of retinoblastoma. Trans. Ophthalmol. Sot. UK 82:473-535; 1962. Thompson, T. W.; Small, R. C.; Stein, J. J. Treatment of retinoblastoma. Am. J. Roentgenol. 14:16-23; 1972.