
Evolution of liver transplantation in Europe: Report of the European Liver Transplant Registry
13
REVIEW Evolution of Liver Transplantation in Europe: Report of the European Liver Transplant Registry Rene ´ Adam, * Paul McMaster, † John G. O’Grady, ‡ Denis Castaing, § Jurgen L. Klempnauer, Neville Jamieson, ¶ Peter Neuhaus, # Jan Lerut, ** Mauro Salizzoni, †† Stephen Pollard, ‡‡ Ferdinand Muhlbacher, §§ Xavier Rogiers, Juan Carlos Garcia Valdecasas, ¶¶ Joaquin Berenguer, ## Daniel Jaeck, *** Enrique Moreno Gonzalez, ††† and the European Liver Transplant Association The European Liver Transplant Registry (ELTR) cur- rently allows for the analysis of 44,286 liver transplanta- tions (LTs) performed on 39,196 patients in a 13-year period. After an exponential increase, the number of LTs is plateauing due to a lack of organs. To cope with this, alternatives to cadaveric LT, such as split LT, domino LT, or living-related LT (LRLT) are being used increasingly. They now account for 11% of all procedures. One of the most important findings in the evolution of LT is the considerable improvement of results along time with, for the mean time, a one-year survival of 83%, all indications confounded. The improvement is particularly significant for cancers. This improvement is mainly represented by hepatocellular carcinoma, with a gain of 17% for 5-year survival rate from 1990 to 2000. Increasingly, older donors are used to augment the donor pool and older recipients are transplanted due to improved results and a better selection of patients. More than two thirds of deaths and three quarters of retransplantations occurred within the first year of transplantation. Retransplantation is associated with much less optimal results than first LT. One of the prominent features of recent years is the devel- opment of LRLT. LRLT is now performed by almost half of the European centers. As with split LT or domino LT, LRLT aims to provide more patients to be transplanted. Special attention is paid to reducing the risk for the donor, which is now estimated to be 0.5% mortality and 21% postoperative morbidity. (Liver Transpl 2003;9: 1231-1243.) T he European Liver Transplant Registry (ELTR) has cumulated data concerning 46,530 liver trans- plantations (LTs) in 41,522 patients from 124 centers in 21 countries from May 1968 to December 2001 (Fig. 1). These data give a comprehensive overview of the status and evolution of LT in Europe. Both number of transplant centers and annual number of LTs per- formed in Europe have gradually increased since the ELTR was created (Fig. 2). The following analysis was undertaken using ELTR data from January 1988 to December 2001 (44,286 LTs, 39,196 patients). Janu- ary 1988 was chosen because it corresponds to the dif- fusion of cyclosporine-based immunosuppression and standardization of the surgical procedure. Background of the ELTR The ELTR is a Service of the European Liver Trans- plant Association, which is part of the European Society for Organ Transplantation. The ELTR represents more than 95% of overall European data compared with pub- lished official figures. 1 To encourage completion, an ELTR Expert Committee decided intentionally to limit the two-part questionnaire to the most relevant items. The first part of the questionnaire includes 34 items From the *European Liver Transplant Registry; §Ho ˆpital Paul Brousse, Villejuif; ***Centre Hospitalier Re ´gional Universitaire de Stras- bourg, Strasbourg, France; †The Queen Elizabeth Hospital, Birming- ham; ‡King’s College Hospital, London; ¶Addenbrooke’s Hospital, Cam- bridge; ‡‡St Jame’s and Seacroft University Hospital, Leeds, UK; Medizinische Hochschule Hannover, Hannover; #Charite ´ Campus, Virchow Klinikum, Berlin; Universitatskrankenhaus Eppendorf, Hamburg, Germany; **Cliniques Universitaires Saint Luc, Brussels, Belgium; ††Centro de Trapianti di Fegato, Torino, Italy; §§Klinishe Abteilung fu ¨r Transplantation, Wien, Austria; ¶¶Hospital Clinic I Pro- vincial de Barcelona; ##Hospital Universitario La Fe, Valencia; and †††Hospital 12 de Octubre, Madrid, Spain. The order of the 16 coauthors was determined according to the decreasing number of liver transplantations recorded in the European Liver Transplant Registry. The registry is supported in part by a grant from Novartis, Fujisawa, and Roche; and logistic support of the Paul Brousse Hospital (Assistance Publique, Ho ˆpitaux de Paris). The European Liver Transplant Registry is a service of the European Liver Transplant Association. Address reprint requests to Rene ´ Adam, MD, PhD, Centre He ´pato- biliaire, Ho ˆpital Paul Brousse, 12-14 Av Paul-Vaillant-Couturier, BP 200, F-94804 Villejuif Cedex, France. Telephone: 331-4559-3288; FAX: 331-4559-3857; E-mail: [email protected] Copyright © 2003 by the American Association for the Study of Liver Diseases 1527-6465/03/0912-0001$30.00/0 doi:10.1016/j.lts.2003.09.018 1231 Liver Transplantation, Vol 9, No 12 (December), 2003: pp 1231-1243
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Evolution of liver transplantation in Europe: Report of the European Liver Transplant Registry

REVIEW
Evolution of Liver Transplantation in Europe: Report ofthe European Liver Transplant Registry
Rene Adam,* Paul McMaster,† John G. O’Grady,‡ Denis Castaing,§
Jurgen L. Klempnauer,� Neville Jamieson,¶ Peter Neuhaus,# Jan Lerut,**
Mauro Salizzoni,†† Stephen Pollard,‡‡ Ferdinand Muhlbacher,§§ Xavier Rogiers,��
Juan Carlos Garcia Valdecasas,¶¶ Joaquin Berenguer,## Daniel Jaeck,***
Enrique Moreno Gonzalez,††† and the European Liver Transplant Association
The European Liver Transplant Registry (ELTR) cur-rently allows for the analysis of 44,286 liver transplanta-tions (LTs) performed on 39,196 patients in a 13-yearperiod. After an exponential increase, the number of LTsis plateauing due to a lack of organs. To cope with this,alternatives to cadaveric LT, such as split LT, domino LT,or living-related LT (LRLT) are being used increasingly.They now account for 11% of all procedures. One of themost important findings in the evolution of LT is theconsiderable improvement of results along time with, forthe mean time, a one-year survival of 83%, all indicationsconfounded. The improvement is particularly significantfor cancers. This improvement is mainly represented byhepatocellular carcinoma, with a gain of 17% for 5-yearsurvival rate from 1990 to 2000. Increasingly, olderdonors are used to augment the donor pool and olderrecipients are transplanted due to improved results and abetter selection of patients. More than two thirds ofdeaths and three quarters of retransplantations occurredwithin the first year of transplantation. Retransplantationis associated with much less optimal results than first LT.One of the prominent features of recent years is the devel-opment of LRLT. LRLT is now performed by almost halfof the European centers. As with split LT or domino LT,LRLT aims to provide more patients to be transplanted.Special attention is paid to reducing the risk for thedonor, which is now estimated to be 0.5% mortality and21% postoperative morbidity. (Liver Transpl 2003;9:1231-1243.)
The European Liver Transplant Registry (ELTR)has cumulated data concerning 46,530 liver trans-
plantations (LTs) in 41,522 patients from 124 centersin 21 countries from May 1968 to December 2001(Fig. 1). These data give a comprehensive overview ofthe status and evolution of LT in Europe. Both numberof transplant centers and annual number of LTs per-formed in Europe have gradually increased since theELTR was created (Fig. 2). The following analysis wasundertaken using ELTR data from January 1988 toDecember 2001 (44,286 LTs, 39,196 patients). Janu-ary 1988 was chosen because it corresponds to the dif-
fusion of cyclosporine-based immunosuppression andstandardization of the surgical procedure.
Background of the ELTR
The ELTR is a Service of the European Liver Trans-plant Association, which is part of the European Societyfor Organ Transplantation. The ELTR represents morethan 95% of overall European data compared with pub-lished official figures.1 To encourage completion, anELTR Expert Committee decided intentionally to limitthe two-part questionnaire to the most relevant items.The first part of the questionnaire includes 34 items
From the *European Liver Transplant Registry; §Hopital PaulBrousse, Villejuif; ***Centre Hospitalier Regional Universitaire de Stras-bourg, Strasbourg, France; †The Queen Elizabeth Hospital, Birming-ham; ‡King’s College Hospital, London; ¶Addenbrooke’s Hospital, Cam-bridge; ‡‡St Jame’s and Seacroft University Hospital, Leeds, UK;�Medizinische Hochschule Hannover, Hannover; #Charite Campus,Virchow Klinikum, Berlin; ��Universitatskrankenhaus Eppendorf,Hamburg, Germany; **Cliniques Universitaires Saint Luc, Brussels,Belgium; ††Centro de Trapianti di Fegato, Torino, Italy; §§KlinisheAbteilung fur Transplantation, Wien, Austria; ¶¶Hospital Clinic I Pro-vincial de Barcelona; ##Hospital Universitario La Fe, Valencia; and†††Hospital 12 de Octubre, Madrid, Spain.
The order of the 16 coauthors was determined according to thedecreasing number of liver transplantations recorded in the EuropeanLiver Transplant Registry.
The registry is supported in part by a grant from Novartis, Fujisawa,and Roche; and logistic support of the Paul Brousse Hospital (AssistancePublique, Hopitaux de Paris). The European Liver Transplant Registryis a service of the European Liver Transplant Association.
Address reprint requests to Rene Adam, MD, PhD, Centre Hepato-biliaire, Hopital Paul Brousse, 12-14 Av Paul-Vaillant-Couturier, BP200, F-94804 Villejuif Cedex, France. Telephone: �331-4559-3288;FAX: �331-4559-3857; E-mail: [email protected]
Copyright © 2003 by the American Association for the Study ofLiver Diseases
1527-6465/03/0912-0001$30.00/0doi:10.1016/j.lts.2003.09.018
1231Liver Transplantation, Vol 9, No 12 (December), 2003: pp 1231-1243

regarding date and indication for LT, donor and recip-ient blood group compatibility, technical aspects of LT,and immediate postoperative immunosuppressiontherapy. The second part (11 items) concerns graft andpatient outcome and immunosuppressive regimen fol-low-up. Participation in the ELTR is voluntary, and astandard computerized database is provided to contrib-uting centers with a detailed instruction handbook forthe collection of accurate and uniform data. To avoidspelling and typing errors, all items are pull-downmenus, except for names of transplant recipients anddates. Centers send a copy of their database twice a year.Data then are subjected to checks for completeness andconsistency. Comprehensive logical intra-updates andinter-updates are performed routinely.
The ELTR has developed partnerships with themain European Organ Sharing Organisations: UKTransplant in the United Kingdom; Organizacion
Nacional de Transplantes in Spain; the EurotransplantFoundation, which includes Austria, Belgium, Ger-many, Luxemburg, Slovenia, and The Netherlands;and Scandiatransplant, which includes Denmark, Fin-land, Norway, and Sweden. These relationships repre-sent an additional way to control the quality of bothELTR and Organ Sharing Organisation data. Periodicmeetings and workshops are organized by the ELTRCommittee, ELTR Expert Committee, and contribu-tors to review the questionnaire and update the proce-dures of data collection and analysis. Twice a year, anELTR report is sent to participating centers, with asummary of results presented as tables and figures.Main data are available in the ELTR Web site (www.eltr.org) and have been published.2 In addition, theELTR database recently allowed the development of arisk model for LT mortality according to donor andrecipient characteristics and transplant procedure.3
Figure 1. Number of LTs performed in each country in Europe (May 1968 to December 2001).
1232 Adam et al

This model can be used prospectively for an individualpatient profile and to perform risk-adjusted compari-sons of patient outcomes among centers.
To ensure the reliability of the scientific analysis ofall data, a control of adequacy between the ELTR ques-tionnaire and patient charts is performed by randomlyconduced audit visits. Seven hundred thirty-four filesfrom 21 centers were audited between June 1998 andJune 2001. The ELTR completeness rate was 95%, andthe consistency rate between charts and the ELTR was98%. Agreement between the ELTR and chart reviewwas very good for all conditions. No significant corre-lation was found between quality of data and experienceof visited centers. Results of audit visits indicate thatELTR data are reliable and scientific results of theELTR can be considered credible and representative ofLT in Europe.4
Results of LT in Europe
Main Indications for LT in Europe
Main indications for LT in Europe with the corre-sponding survival rates at 1, 5, and 10 years are listed inTable 1. Cirrhosis is the most frequent indication(50%), mainly related to either viral infection (24%),with 16% hepatitis C virus infection, or alcohol abuse
(18%). Cirrhosis is followed by three indications: cho-lestatic disease (13%), primary liver tumors (10%), andacute hepatic failure (9%). Cholestatic disease is repre-sented mainly by primary biliary cirrhosis (8%), biliaryatresia (5%), and primary sclerosing cholangitis (4%).Biliary atresia is the most frequent indication (56%) inthe pediatric population, followed by metabolic disease(21%). Hepatocellular carcinoma is the most frequentcancer (8%). Virus-related fulminant hepatitis is themost frequent cause of acute hepatic failure (2%) inEurope.
The percentage of main indications for LT haschanged significantly with time. Whereas cancers rep-resented 50% of indications before 1980, they currentlyrepresent no more than 10%. Conversely, acute hepaticfailure that led anecdotally to LT before 1986 has sincebecome a recognized indication for LT (Fig. 3).
Overall Patient Survival
When all indications are considered during the entirestudy period, patient survival rates are 80% at 1 year,70% at 5 years, and 62% at 10 years. Survival hasimproved regularly year after year, reaching 83% at 1year in 2001 compared with 76% in 1990 to 1994 andonly 34% before 1985 (Fig. 4). Currently, at 5 years,the patient survival rate is 72%. The improvement con-
Figure 2. Evolution of 28,783 LTs performed in Europe since May 1968. Arrows indicate the year the first LT wasperformed in indicated countries.
1233European Liver Transplant Registry Report

Table 1. Primary Indications for LT in Europe and Corresponding Survival
Indication for LTNo. of
Patients
Percentage Survival Rate (%)
OfDisease
OfTotal
1 Yr 5 Yr 10 Yr
Graft Patient Graft Patient Graft Patient
Acute hepatic failure 3709 9 60 65 52 59 53 55Virus 837 23 2 63 66 52 57 47 54Drug 544 15 1 61 63 53 57 46 53Toxic 106 3 0.3 70 73 69 70 69 70Postoperative/traumatic 51 1 0.1 39 45 28 35 — —Unknown/others 2,171 59 6 57 64 51 58 49 54
Cholestatic disease 5,213 13 78 82 69 77 61 70Primary biliary cirrhosis 2,959 57 8 79 83 71 77 64 69Primary sclerosing cholangitis 1,731 33 4 78 83 65 75 54 66Secondary biliary cirrhosis 271 5 1 70 74 59 69 54 62Others 252 5 1 79 83 71 79 69 76
Congenital biliary disease 2,350 6 75 83 69 78 66 74Extrahepatic biliary atresia 1,963 84 5 75 83 69 79 67 78Others 387 16 1 76 83 69 77 58 69
Cirrhosis 19,719 50 79 82 66 71 57 63Virus-related cirrhosis (Hepatitis) 9,486 48 24 81 83 69 72 60 66
Virus B 2,410 12 6 79 80 65 70 59 64Virus C 5,977 30 15 79 81 62 67 52 57Virus BD 640 3 2 88 91 81 85 76 83Virus BC 380 2 1 78 83 63 71 58 67Virus BCD 79 0.4 0.2 91 92 79 85 74 78
Alcoholic cirrhosis 6,950 35 18 81 83 69 72 56 59Autoimmune cirrhosis 991 5 3 76 81 65 72 58 65Others 2,292 12 6 71 74 62 69 55 58
Primary liver tumors 4,104 10 70 74 47 49 38 38Hepatocellular carcinoma and cirrhosis 2,789 68 7 78 79 54 58 44 47Hepatocellular carcinoma and noncirrhotic liver 543 13 1 66 67 37 39 27 27Hepatic cholangiocellular carcinoma 196 5 1 60 62 23 29 20 21Biliary tract carcinoma (Klatskin) 177 4 0.5 65 66 29 30 18 18Hepatoblastoma 71 2 0.2 79 80 68 70 59 60Epithelioid hemangioendothelioma 66 2 0.2 84 86 61 63 61 63Hepatocellular carcinoma, fibrolamellar 32 1 0.1 67 70 32 34 — —Angiosarcoma 16 0.4 0.04 60 65 — — — —Other liver malignancies 214 5 1 — — — — — —
Secondary liver tumors 314 1 71 73 33 37 20 21Carcinoid 103 33 0.3 76 78 40 43 29 31Other neuroendocrine 59 19 0.2 72 74 43 45 — —Colorectal 22 7 0.1 75 78 25 30 — —Gastrointestinal, noncolorectal 10 3 0.03 81 83 — — — —Nongastrointestinal 12 4 0.03 58 61 — — — —Others 108 34 0.3 — — — — — —
Metabolic diseases 2,401 6 79 83 70 77 63 71Familial amyloidotic polyneuropathy 534 22 1 82 85 69 76 54 63Wilson’s disease 362 15 1 79 84 74 81 64 74�1-Antitrypsin deficiency 281 12 1 81 83 70 78 68 71Hemochromatosis 250 10 1 71 72 59 64 — —Cystic fibrosis 109 5 0.3 82 85 70 78 — —Byler disease 103 4 0.3 82 84 82 83 82 83Primary hyperoxaluria 95 4 0.2 81 84 75 78 75 76Tyrosinemia 52 2 0.1 89 92 74 82 74 82Crigler-Najjar 30 1 0.1 87 90 79 81 — —Glycogen storage disease 24 1 0.1 80 82 76 78 — —Others 561 23 1 — — — — — —
Budd-Chiari 391 1 66 73 58 68 52 63Benign liver tumors or polycystic disease 352 1 81 82 73 77 64 65
Polycystic disease 218 62 1 83 85 77 80 70 73Solid tumor 134 38 0.3 77 79 68 73 57 57
Parasitic disease 43 0.1 65 67 58 68 — —Other liver disease 600 2 70 73 60 60 52 52Total 39,196 100 76 83 63 71 55 63
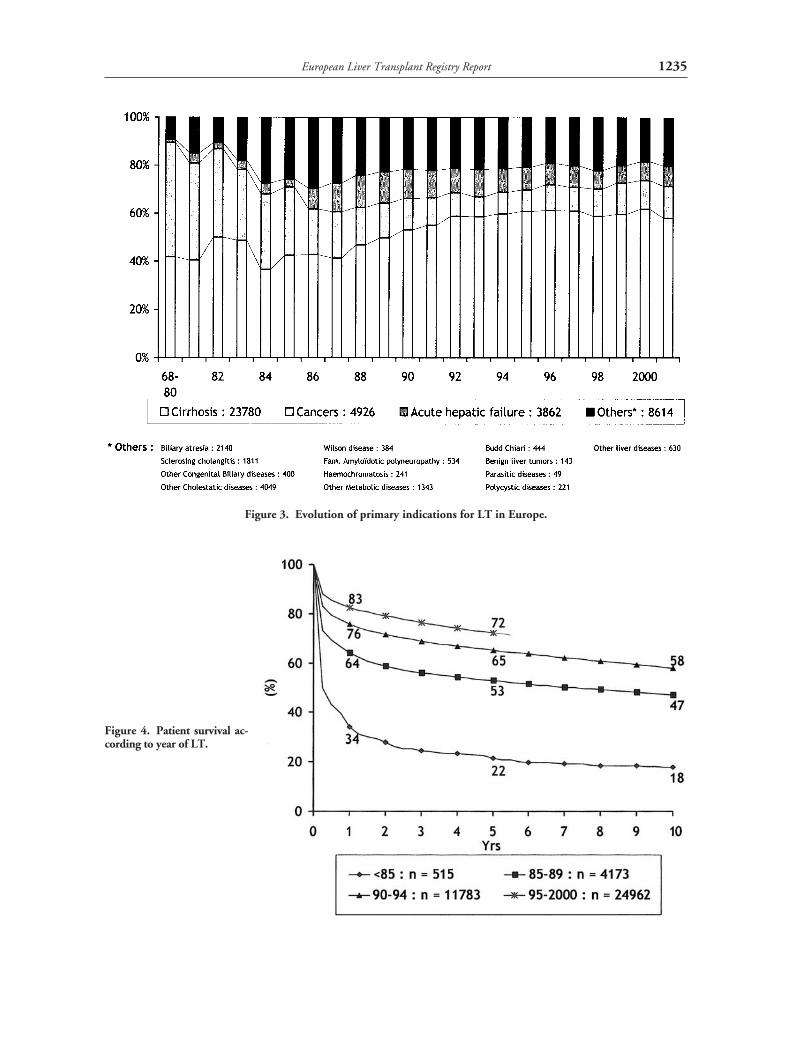
Figure 3. Evolution of primary indications for LT in Europe.
Figure 4. Patient survival ac-cording to year of LT.
1235European Liver Transplant Registry Report

cerns all indications, but particularly LT for cancers(Fig. 5).
The critical period for post-LT outcome is repre-sented by the first 6 months: 58% of deaths and 68% ofre-LTs occur within the 6 months after LT (Fig. 6). In48% of cases, re-LT is indicated in the month afterprimary LT, and one third of patients who die do sowithin the first month after LT.
Survival of Pediatric Versus Adult LiverTransplant Recipients
Eleven percent of LTs have been performed in pediatricpatients (�15 years), with 4% of children younger than2 years. Five-year survival in children is significantlybetter than in adults (76% v 68%; P � .0001). In thepediatric population, 5-year survival rates are 75% forchildren younger than 2 years and 77% for those aged 3to 15 years.
Survival According to Indication for LT
The 5-year patient survival rate is significantly better forcirrhosis (71%) than for primary liver tumors (49%;P � .001) and acute hepatic failure (59%; P � .001).The greater survival rates obtained in metabolic diseases(77%) and cholestatic diseases (73%) occur partlybecause of the high percentage of children in thesegroups. Details of survival rates at 1, 5, and 10 yearsaccording to primary indication are listed in Table 1.
Survival According to Donor and RecipientCharacteristics
Donor characteristics. The majority of donors weremale (61%). Eighty-one percent were younger than 55years, whereas 5% were older than 65 years. Graft sur-vival when organs were procured from donors youngerthan 55 years was significantly greater than that withorgans from donors older than 65 years (63% v 52% at5 years; P � .0001). An increasing percentage of liversare coming from donors older than 60 years (2% in1991, 10% in 1996, and 20% in 2001), in relation tothe increasing gap between a growing waiting list and arelatively stable donor pool (Fig. 7).
Recipient age. In addition to the already mentionedbetter survival of pediatric versus adult liver transplantrecipients, an influence of recipient age is noted foradults. Survival rates are 71% for adults aged 16 to 45years, 67% for those aged 46 to 60 years, and 63% forthose older than 60 years. However, average age oftransplant recipients has increased steadily during thelast decade, and patients older than 60 years, who rep-
Figure 5. Patient survival according to indication for andyear of LT.
1236 Adam et al

Figure 6. Mortality and re-LT; percentage per period and cumulative proportions.
Figure 7. Evolution of donor age in Europe.
1237European Liver Transplant Registry Report

resented less than 5% in the 1980s, represented approx-imately 20% of transplant recipients in 2001 (Fig. 8).
Blood group type matching. Ninety-two percent of LTswere isogroup, and 7% were compatible. Only 1% wereincompatible and restricted to urgent procedures. Inemergencies, isogroup and compatible LTs have similarsurvival. Incompatible LTs have a decreased 5-yeargraft survival rate of 24% compared with isogroup andcompatible LTs; 48% and 46%, respectively (P �.0001). However, use of these incompatible grafts inemergency indications allows an approximately 50%survival rate in patients otherwise destined to a fataloutcome.
In elective conditions, isogroup LTs have a better5-year survival rate than compatible LT (65% v 57%;P � .0001).
Survival According to Surgical Technique
More than 99% of LTs were performed orthotopically,and 89% of grafts were full size. Alternative proceduresto full-size LTs have been used increasingly in recentyears, represented by reduced livers (5%), split livers(4%) living donors (1.6%), and domino transplants(0.4%). Survival at 5 years was similar between split-liver and reduced-liver grafts (57% and 56%), but less
than that of total-liver grafts (61%; P � .0001). How-ever, split-liver transplantation in experienced centershad results similar to full-size LTs.3 Auxiliary graftsrepresented 0.4% of overall LTs, with a graft survivalsimilar to that of nonauxiliary grafts in urgent indica-tions (5-year survival rates, 45% v 47%), but not inelective cases (47% v 64%; P � .0001). Graft survivalwas better when cold ischemia time was less than 12hours and University of Wisconsin solution was usedfor preservation (P � 0.001).
Living Related LT in Europe
The ELTR has accumulated data concerning 806 livingrelated LTs (LRLTs) performed in 46 centers from 15countries from October 1991 to December 2001 (Fig.1). There were 359 LRLTs performed in adults and 446LRLTs performed in children. By the last 2 years, adultLRLT largely exceeded pediatric LT (286 v 128 proce-dures). The graft used was mainly the right liver foradults (93%) and left-liver lobe for children (84%). Thedonor surgical mortality rate was 0.5%, with four post-operative deaths related to pulmonary embolism (onedeath), sepsis (two deaths), and cardiac failure (onedeath). Donor morbidity accounted for 21% of earlypostoperative complications, greater for right-liver
Figure 8. Evolution of recipient age in Europe.
1238 Adam et al

(34%) than left-lobe donation (10%; P � .001). Com-pared with cadaveric LTs, there were significantly morecancers (23% v 10%), fewer acute hepatic failures (4%v 8%), and fewer re-LTs (1% v 10%). The overall5-year graft survival rate was 75%, better for childrenthan for adults (80% v 66% at 3 years). Whereas sur-vival of LRLT was better than cadaveric LT for children(80% v 70%; P � .001), it was similar for adults (66%v 68% at 3 years). Graft size had no prognostic influ-ence in children, but significantly affected the outcomeof adults (3-month graft loss, 21% for right livers, 50%for left livers, 69% for left lobes; P � .001). Overall,graft loss included more primary nonfunction (21% v13%) and technical complications (21% v 13%) afterLRLT than after cadaveric LT (P � .01).
Re-LT and Death
Main causes of re-LT. Re-LT was indicated in 4,216cases (9.5%), mainly for technical complications,mostly vascular (33%); primary nonfunction (27%);
and rejection (mainly chronic; 22%). Recurrence ofprimary disease (mostly nontumoral) was concerned inonly 8% of cases (Table 2).
Five-year graft survival rates for the second and thirdLTs were 42% and 37%, respectively. Rates was signif-icantly lower (P � .0001) than those for primary LT(63%; Fig. 9). In emergency situations, the differencein survival between primary LT and a second LT,although still significant (P � .001), was reduced (52%v 37%; data not shown).
Main causes of mortality. Main causes of death in the8,557 patients (�19%) who died after primary LT orre-LT were, by decreasing order, such general causes asmultiple organ failure and cerebrovascular, cardiovas-cular, pulmonary, and renal complications (30%); sep-sis (20%); recurrence of primary disease (mostly cancer;17%); technical complications (mostly hemorrhageand vascular; 6%); and rejection (4%; Table 3). Intra-operative deaths represented 5%, and primary non-function represented 3% of all deaths.
Table 2. Cause of Re-LT After the First LT in Europe
Cause of Re-LT
Time of Re-LT
Total
Percentage
1Day
1Week
1Month
6Months
1Year
3Years
5Years
�5Years
OfComplication
OfTotal
Primary nonfunction 85 621 188 0 0 0 0 0 894 100 27Technical 10 194 341 286 91 107 40 25 1,093 0 0
Vascularcomplications 8 179 303 193 48 39 15 11 796 73 24
Biliary complications 0 1 17 79 43 66 25 12 243 22 7Hepatic infarction 0 11 18 12 0 2 0 1 43 4 1Hemorrhage 2 3 3 2 0 0 0 1 11 1 0.3
Sepsis 0 6 6 12 6 6 4 4 44 100 1Bacterial infection 0 4 2 9 4 1 1 0 21 48 1Viral infection 0 1 1 1 2 3 2 3 13 30 0.4Fungal infection 0 0 2 1 0 2 0 0 5 11 0.1Sepsis not designated 0 1 1 1 0 0 1 1 5 11 0.1
Rejection 3 36 118 177 154 169 52 32 741 100 22Chronic 0 0 0 135 141 160 51 31 518 70 16Acute 2 32 105 26 8 6 1 1 181 24 5Not designated 1 4 13 16 5 3 0 0 42 6 1
Recurrence of disease 0 2 4 41 49 87 37 49 269 100 8Nontumoral 0 2 4 41 49 80 34 47 257 96 8Tumoral 0 0 0 0 0 7 3 2 12 4 0.4
Tumor de novo 1 2 2 6 2 1 1 1 16 100 0.5Other causes 9 24 55 64 25 34 12 27 250 100 7
Hepatic 5 12 27 43 9 17 10 24 147 59 4Nonhepatic 4 12 28 21 16 17 2 3 103 41 3
Unknown cause 0 5 8 11 4 5 0 1 34 100 1Total 108 890 722 597 331 409 146 139 3,341 100 0
NOTE. Complications correspond to the first cause of failure declared according to time of occurrence.
1239European Liver Transplant Registry Report

DiscussionWith more than 40,000 recorded LTs all over Europe,the ELTR currently is one of the most important data-bases to evaluate results of LT. It is representative of LTin Europe (95% of LTs performed). Owing to accuratecontrol of data, including audit visits to randomlyselected centers, its scientific value recently has beenemphasized.5-7
More than 4,000 LTs per year currently are per-formed in Europe. After an exponential growth fromthe 1980s, the number of yearly LTs is plateauing fromapproximately 4 years because of the lack of organs. Tocope with a donor shortage that presently represents themost important limiting factor of LT, such alternativesto cadaveric LT as split, domino, or living related LTsare increasingly used, accounting for 11% of all proce-dures. Although more technically demanding, thesetechniques give results similar to those for cadaveric LTand allow a larger number of patients to undergo LT.
One of the most important findings in the evolutionof LT is the significant improvement in results withtime; presently, a 1-year survival rate of 83%, all indi-cations confounded, in relation to greater technical
expertise, better selection of patients, and improvedpost-LT management of complications and immuno-suppressive therapy. The improvement is particularlysignificant for cancers, represented mainly by hepato-cellular carcinoma, with a gain of 17% in 5-year sur-vival rates from 1990 to 2000.
Donor and recipient age influence the quality ofresults, shown by a previous analysis of ELTR datafocused on mortality after LT.3 However, they are notprominent factors in mortality. Therefore, evolutionshows that older donors are increasingly used to aug-ment the donor pool, and older recipients increasinglyundergo LT owing to improved results and better selec-tion of patients.
What has not changed with time is the critical periodof the first 6 months and, more generally, the first yearto determine the final outcome of the transplant recip-ient. More than two thirds of deaths and more thanthree fourths of re-LTs occurred within the first yearafter LT.
When required in approximately 7% of patients,re-LT is associated with much less optimal results thanthe first LT. However, no team considers this a suffi-
Figure 9. Graft survival (%)according to number of LTs.
1240 Adam et al

cient reason to not perform a new LT, suggesting that asort of moral contract with the patient has a role to play,in addition to strict consideration of the optimal use oforgans. Interestingly, third and fourth LTs are not associ-ated with results much worse than those of second LTs.
One of the prominent features of recent years is thedevelopment of LRLT, now performed by almost halfthe centers. As with split LT, LRLT aims to providemore patients with transplants,but with special atten-tion to decrease as much as possible risks for the donor,now estimated to be 0.5% for mortality and 21% forpostoperative morbidity.
In conclusion, LT presently has reached the age ofmaturity. Indications are oriented to more optimal useof the limited donor pool. Survival is still increasing
gradually in relation to greater expertise in the surgicalprocedure and management of immunosuppressivetherapy. Alternatives to conventional use of cadavericfull-size liver grafts are expanding to palliate the organshortage. This latter development probably will repre-sent the key issue in the near future, to avoid patientdeath on the waiting list and offer LT to patients cur-rently not benefitting from this therapy.
Acknowledgment
The authors thank Vincent Karam (Data Manager) and Vale-rie Delvart (Biostatistician) for collection quality control andstatistical analysis of ELTR data and all the contributing cen-ters, listed next.
Table 3. Post-LT Mortality After First LT in Europe
Cause of death
Time of Death
Total
Percentage
1Day
1Week
1Month
6Months
1Year
3Years
5Years
�5Years
OfComplication
OfTotal
Intraoperative death 391 0 0 0 0 0 0 0 391 100 5Primary nonfunction 52 122 88 0 0 0 0 0 262 100 3Technical 71 75 171 114 30 43 15 15 534 100 6
Hemorrhage 57 47 58 39 6 8 2 1 218 41 3Vascular
complications 13 18 101 41 11 16 9 1 210 39 2Biliary complications 0 2 4 30 13 16 3 12 80 15 1Hepatic infarction 1 8 8 4 0 3 1 1 26 5 0.3
Sepsis 6 69 514 785 148 135 36 54 1,747 100 20Bacterial infection 1 23 161 236 51 48 15 32 567 32 7Fungal infection 0 7 79 97 14 11 2 3 213 12 2Viral infection 0 2 15 84 10 13 2 4 130 7 2Sepsis not designated 5 37 259 368 73 63 17 15 837 48 10
Rejection 1 12 61 73 69 97 32 24 369 100 4Chronic 0 0 0 42 61 90 32 22 247 67 3Acute 1 11 57 26 5 6 0 1 107 29 1Not designated 0 1 4 5 3 1 0 1 15 4 0.2
Recurrence of disease 0 2 10 189 326 606 223 126 1,482 100 17Tumoral 0 0 1 122 215 392 134 66 930 63 11Nontumoral 0 2 9 67 111 214 89 60 552 37 6
Tumor de novo 1 0 5 49 87 194 134 109 579 100 7General causes 198 335 680 650 150 235 107 191 2,546 100 30
Cardiovascular 89 88 135 106 35 64 44 81 642 25 8Cerebrovascular 48 114 123 115 28 54 11 27 520 20 6Pulmonary 17 37 143 177 33 40 17 28 492 19 6Gastrointestinal 12 15 59 53 15 25 14 19 212 8 2Renal 0 7 29 29 12 16 12 24 129 5 2Multiple organ failure 32 74 191 170 27 36 9 12 551 22 6
Other causes 12 60 102 129 78 109 56 45 591 100 7Unknown cause 2 3 11 14 5 10 7 4 56 100 1Total 734 678 1,642 2,003 893 1,429 610 568 8,557 100 100
NOTE. Complications correspond to first declared cause of death according to date it occurred.
1241European Liver Transplant Registry Report

Contributing centers: Addenbrooke’s Hospital (N. Jamie-son), Cambridge, UK; Centro de Trapianti di Fegato (M.Salizzoni), Torino, Italy; Centro Trapianti di Fegato (V.Memeo), Bari, Italy; Charite-Universitatsklinikum zu Berlin(P. Neuhaus), Berlin, Germany; Children’s Memorial HealthInstitute (P. Kalicinski), Warsaw, Poland; Chirurgische Uni-versitatsklinik und Poliklinik (W. Timmermann), Wurzburg,Germany; C.H. Princesse Grace (C. Huguet), Monte-Carlo,Monaco; Centre Hospitalo-Universitaire de Caen (P. Segol),Caen, France; Centre Hospitalo-Universitaire de Grenoble(C. Letoublon), Grenoble, France; Centre Hospitalo-Univer-sitaire de Liege (M. Meurisse), Liege, Belgium; Centre Hos-pitalo-Universitaire Nancy (P. Boissel), Vandoeuvre, France;Centre Hospitalo-Universitaire Vaudois (M. Gillet), Lau-sanne, Switzerland; Centre Hospitalo-Universitaire Necker(Y. Revillon), Paris, France; Clinica Puerto de Hierro (J.Ardaiz), Madrid, Spain; Clinica Universitaria de Navarra(J.A. Cienfuegos), Pamplona, Spain; Cliniques UniversitairesSaint-Luc (J. Lerut), Brussels, Belgium; CSU de Bellvitge (E.Jaurrieta), Barcelona, Spain; Klinikum Rechts der IsarMunchen (M. Stangl), Munchen, Germany; University Hos-pital Freiburg (G. Kirste), Freiburg, Germany; CUK GHsEssen (C. Broelsch), Essen, Germany; CUK Innsbruck (R.Margreiter), Innsbruck, Austria; Dijkzigt Hospital (S.W.Schalm), Rotterdam, The Netherlands; Eberhard-Karls-Uni-versitat Tubingen (R. Viebahn), Tubingen, Germany; Free-man Hospital (P. Groom), Newcastle-upon-Tyne, UK;Friedrich Schiller Universitat Jena (J. Scheele), Jena, Ger-many; Georg August Universitat Gottingen (B. Ringe), Got-tingen, Germany; Hopital Purpan (P. Broue), Toulouse,France; Hopital de la Conception (Y.P. Letreut), Marseille,France; Hopital de Pontchaillou (K. Boudjema), Rennes,France; Hopital Erasme (M. Gelin), Brussels, Belgium; Hopi-tal Rangueil (G. Fourtanier), Toulouse, France; HopitalHautepierre (D. Jaeck), Strasbourg, France; Hopital JeanMinjoz (G. Mantion), Besancon, France; Hopital Dupuytren(B. Descottes), Limoges, France; Hopital Beaujon (J.Belghiti), Clichy, France; Hopital Calmette (F.R. Pruvot),Lille, France; Hopital Cantonal Universitaire de Geneve (P.Morel), Geneva, Switzerland; Hopital Cochin (D. Houssin),Paris, France; Hopital de la Croix-Rousse (C. Ducerf), Lyon,France; Hopital du Kremlin-Bicetre (F. Gauthier), Le Krem-lin-Bicetre, France; Hopital E. Herriot (O. Boillot), Lyon,France; Hopital G&R Laennec (J. Visset), Nantes, France;Hopital Henri Mondor (D. Cherqui), Creteil, France; Car-diovascular Institute Dedinje (B. Radevic), Beograd, Yugosla-via; Hopital de la Timone Enfants (A. Delarue), Marseille,France; Hopital Pasteur Nice (A. Bourgeon), Nice, France;Hopital Paul Brousse (D. Castaing), Villejuif, France; Hopi-tal Pitie-Salpetriere (L. Hannoun), Paris, France; HopitalSaint Antoine (R. Parc), Paris, France; Hopital Saint-Eloi (J.Domergue), Montpellier, France; Hopital Saint Roch (J.Guggenheim), Nice, France; Hopital Tripode (J. Saric), Bor-deaux, France; Hospitais da Universidade de Coimbra (D.L.Furtado), Coimbra, Portugal; Hospital 12 de Octubre (E.
Moreno Gonzales), Madrid, Spain; Hospital Central de Astu-rias (D.I. Gonzalez Pinto), Oviedo, Spain; Hospital Clinic IProvincial de Barcelona (G. Valdecasas), Barcelona, Spain;Hospital Clinico Universitario de Zaragoza (T. Serrano),Zaragoza, Spain; Hospital Clınico Universitario Santiago deCompostela (E. Varo), La Coruna, Spain; Hospital de Cruces(J.O. de Urbina), Baracaldo-Vizcaya, Spain; Hospital Gal deSanto Antonio (M.C. Pereira), Porto, Portugal; Hospital Gre-gorio Maranon (C. Kempin), Madrid, Spain; Hospital Infan-til Barcelona (V. Martinez Ibanez), Barcelona, Spain; Hospi-tal Infantil La Paz (J.T. Larrucea), Madrid, Spain; HospitalNtra Sra de Candelaria (A. Soriano), Santa Cruz de Tenerife,Spain; Hospital Ramon y Cajal (E. de Vicente Lopez),Madrid, Spain; Hospital Regional Carlos Haya (A. de laFuente Perucho), Malaga, Spain; Hospital Virgen de laArrixaca (F. Sanchez Bueno), El Palmar, Spain; Hospital Uni-versitario La Fe (J. Berenguer), Valencia, Spain; HospitalMarques de Valdecilla (L.A. Herrera), Santander, Spain; Hos-pital Universitario Reina Sofia (C. Pera), Cordoba, Spain;Hospital Universitario Virgen de la Nieves (D. Ramia Angel),Granada, Spain; Hospital Universitario Rio Hortega (G.Sanchez Antolin), Valladolid, Spain; Hospital Virgen delRocio (A. Bernardos), Sevilla, Spain; Hotel Dieu, CHU deClermont-Ferrand (J. Chipponi), Clermont-Ferrand, France;Huddinge Hospital (B.G. Ericzon), Huddinge, Sweden;I.C.C. Bologna (A. Cavallari), Bologna, Italy; Istituto diChirurgia Generale I (A. Maffei Faccioli), Padova, Italy; Isti-tuto Nazionale Tumori Milano (Mazaferro), Milano, Italy;Johannes Gutenberg Univiversity Mainz Klinikum (G.Otto), Mainz, Germany; King’s College Hospital (J.G.O’Grady), London, UK; Klinikum der Christian AlbrechtsUniversity (B. Kremer), Kiel, Germany; Klinikum der J.W.Goethe University (W.O. Bechstein), Frankfurt am Main,Germany; Klinishe Abteilung fur Transplantation (F. Muhl-bacher), Wien, Austria; Ludwig Maximilians Universitat (R.Schauer), Munchen, Germany; Medizinische Einrichtungender University zu Koln (A. Holscher), Koln, Germany;Medizinische Hochschule Hannover (J. Klempnauer), Han-nover,Germany; Ospedale Cisanello (F. Filipponi), Pisa,Italy; Ospedale Maggiore di Milano (L.R. Fassati), Milano,Italy; Ospedale Niguarda-Pizzamiglio II (D. Forti), Milano,Italy; Ospedale San Eugenio Tor Vergata (G. Casciani),Roma, Italy; Ospedali Riuniti di Bergamo (B. Gridelli), Ber-gamo, Italy; PET Centre (S. Keiding), Aarhus, Denmark;Pomeranian Medical Academy (R. Kostyrka), Szczecin,Poland; Regina Elena Cancer Hospital (G. Ettorre), Roma,Italy; Rigshospitalet (P. Kirkegaard), Copenhagen, Denmark;Rikshospitalet (I.B. Brekke), Oslo, Norway; Royal Free Hos-pital (K. Rolles), London, UK; Royal Infirmary of Edinburgh(J. Garden), Edinburgh, UK; Ruprecht-Karls-UniversityHeidelberg (E. Klar), Heidelberg, Germany; SahlgrenskaUniversity Hospital (S. Friman), Goteborg, Sweden; Sem-melweis Medical University (F. Perner), Budapest, Hungary;St Jame’s and Seacroft University Hospital (S. Pollard), Leeds,UK; St Vincent Hospital (O. Traynor), Dublin, Ireland; The
1242 Adam et al

Queen Elizabeth Hospital (P. McMaster), Birmingham, UK;U.C.J. Helsingfors (K. Hockerstedt), Helsinki, Finland;Unidad de Transplante Hepatico (C. Fernandez Sellez), LaCoruna, Spain; Universita Cattolico del Sacro Cuore (M.Castagneto), Roma, Italy; Universita Degli Studi di Roma(M. Rossi), Roma, Italy; Universita di Genova (U. Valente),Genova, Italy; Universitair Ziekenhuis (B. de Hemptinne),Ghent, Belgium; Universitair Ziekenhuizen Leuven (J.Pirenne), Leuven, Belgium; Universitat Erlangen-Nurnberg(T. Reck), Erlangen, Germany; Universitat Leipzig (J.Hauss), Leipzig, Germany; Universitat Regensburg (K.W.Jauch), Regensburg, Germany; Universitat Rostock (W.Schareck), Rostock, Germany; UniversitatskrankenhausEppendorf (X. Rogiers), Hamburg, Germany; Universitatspi-tal Zurich (P.A. Clavien), Zurich, Switzerland; Universi-tatspital Bern (D. Candinas), Bern, Switzerland; UniversityHospital (F. Bresadola), Udine, Italy; University HospitalGroningen (M.J.H. Slooff), Groningen, The Netherlands;University Hospital Leiden (O.T. Terpstra), Leiden, TheNetherlands; University of Medicine Carol Davila (I.Popescu), Bucharest, Romania; University of Modena e Reg-gio Emilia (A.D. Pinna), Modena, Italy; and University ofPadova (D.F. D’amico), Padova, Italy.
References
1. Select Committee of Experts on the Organisational Aspects ofCooperation in Organ and Tissue Transplantation. Internationalfigures on organ donation and transplantation activities, 1998.Organ Tissues 1999;1:73.
2. Adam R, Karam V, Delvart V, Hockerstedt K. Ten-year evolutionof liver transplantation in Europe—Report of the European LiverTransplant Registry (ELTR). In: Kockerling F, Schwartz SI (eds).Liver surgery. Operative techniques and avoidance of complica-tions. Heidelberg: Barth, 2001:195.
3. Adam R, Cailliez V, Majno P, Karam V, McMaster P, Calne YC,et al. Normalised intrinsic mortality risk in liver transplantation:European Liver Transplant Registry study. Lancet 2000;356:621.
4. Karam V, Gunson B, Roggen F, Grande L, Wannoff W, JanssenM, et al. Quality control of the European Liver Transplant Reg-istry: Results of audit visits to the contributing centres. Transplan-tation 2003;75:2167.
5. Morris P, Monaco A. Quality control of transplant registries.Transplantation 2003;75:2162.
6. Hanto D. Reliability of voluntary and compulsory databases andregistries in the United States. Transplantation 2003;75:2162.
7. Van Der Meulen J, Jacob M, Copley L. Assessing the quality of thedata in a transplant registry: The European Liver Transplant Reg-istry. Transplantation 2003;75:2164.
1243European Liver Transplant Registry Report




















