
Neurological disorders in liver transplant candidates
14
Neurological disorders in liver transplant candidates: Pathophysiology and clinical assessment ☆ Paolo Feltracco a, ⁎, Annachiara Cagnin b , Cristiana Carollo a , Stefania Barbieri a , Carlo Ori a a Department of Medicine UO Anesthesia and Intensive Care, Padova University Hospital, Padova, Italy b Department of Neurosciences (DNS), University of Padova, Padova, Italy abstract Compromised liver function, as a consequence of acute liver insufficiency or severe chronic liver disease may be associated with various neurological syndromes, which involve both central and peripheral nervous system. Acute and severe hyperammoniemia inducing cellular metabolic alterations, prolonged state of “neuroinflamma- tion”, activation of brain microglia, accumulation of manganese and ammonia, and systemic inflammation are the main causative factors of brain damage in liver failure. The most widely recognized neurological complications of serious hepatocellular failure include hepatic encephalopathy, diffuse cerebral edema, Wilson disease, hepatic myelopathy, acquired hepatocerebral degeneration, cirrhosis-related Parkinsonism and osmotic demyelination syndrome. Neurological disorders affecting liver transplant candidates while in the waiting list may not only sig- nificantly influence preoperative morbidity and even mortality, but also represent important predictive factors for post-transplant neurological manifestations. Careful pre-transplant neurological evaluation is essential to de- fine severity and distribution of the neurological impairment, to identify the abnormalities still responsive to cur- rent treatment, and to potentially predict the inherent post-operative prognosis. The preferred specific indices of neurological pre-transplant assessment may vary among centers, however, even with the aid of the current bio- chemical, neurophysiological, neuropsychological and neuroimaging diagnostic tools, the correct diagnosis and differential diagnosis of various syndromes may be difficult. In this article the relevant pathophysiological and clinical aspects of the most frequent brain and peripheral nervous system diseases affecting liver transplant can- didates with acute or advanced chronic liver failure are briefly reported. The practical diagnostic findings useful for the preoperative assessment and treatment, as well as the expected neurological evolution after liver trans- plantation are also evaluated. © 2017 Elsevier Inc. All rights reserved. 1. Introduction Compromised liver function as a consequence of either acute hepatic failure or severe chronic liver disease and liver cirrhosis leads to insuffi- cient detoxification of some substances and catabolic products, which accumulate in the blood and are responsible for a broad range of neuro- logical and neuropsychiatric manifestations [1]. A strict relationship be- tween brain functioning and integrity of the liver is well known, and a pathological liver may be responsible for various neurological syn- dromes, which affect both the central nervous system (CNS) and the pe- ripheral nervous system [2,3]. Liver transplant candidates may experience a great variety of neurological disorders while on the waiting list, which may significantly influence preoperative morbidity and even mortality. It has been recog- nized that many neurological disorders associated with acute or chronic liver failure tend to improve or disappear after successful orthotopic liver transplantation (OLT); however, some minor “residual” clinical signs may persist postoperatively in a variable percentage of liver transplanted patients. Furthermore, pre-transplant subclinical neuro- logical symptoms may become apparent in the event of graft dysfunc- tion or severe postoperative metabolic disturbances [4,5]. Liver transplant recipients are affected by the highest rate of CNS complications among solid organ transplants (incidence between 10% and 85%), with focal and diffuse neurological deficits sometimes representing a major obstacle to the improvement of short- and long- term outcomes [6]. Relevant adverse post-OLT neurological events occur due to brain edema, increase of intracranial pressure, metabolic encephalopathy, cerebrovascular complications, osmotic demyelination syndrome, and opportunistic infections. Moreover, some pre-operative neurological alterations such as dysarthria or akinetic mutism, confu- sion and seizures, may worsen due to the neurotoxic effects of calcine- urin inhibitors drugs required to prevent graft rejection [4,7]. Full Transplantation Reviews 31 (2017) 193–206 ☆ Author contributions Carollo C and Barbieri S made literature search; Feltracco P and Cagnin AC acquired and analyzed the data, and drafted the article; all authors contributed to the manuscript preparation, data interpretation, revision for important intellectual con- tent, editing, and approved the final version. ⁎ Corresponding author at: Department of Medicine UO Anaesthesia and Intensive Care, Padua University Hospital, Via 8 febbraio 1848, 35128, Padua, Italy. Tel.: +39 498212222. E-mail address: [email protected] (P. Feltracco). http://dx.doi.org/10.1016/j.trre.2017.02.006 0955-470X/© 2017 Elsevier Inc. All rights reserved. Contents lists available at ScienceDirect Transplantation Reviews journal homepage: www.elsevier.com/locate/trre
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Neurological disorders in liver transplant candidates

Transplantation Reviews 31 (2017) 193–206
Contents lists available at ScienceDirect
Transplantation Reviews
j ourna l homepage: www.e lsev ie r .com/ locate / t r re
Neurological disorders in liver transplant candidates: Pathophysiology
and clinical assessment☆Paolo Feltracco a,⁎, Annachiara Cagnin b, Cristiana Carollo a, Stefania Barbieri a, Carlo Ori a
a Department of Medicine UO Anesthesia and Intensive Care, Padova University Hospital, Padova, Italyb Department of Neurosciences (DNS), University of Padova, Padova, Italy
a b s t r a c t
Compromised liver function, as a consequence of acute liver insufficiency or severe chronic liver disease may beassociated with various neurological syndromes, which involve both central and peripheral nervous system.Acute and severe hyperammoniemia inducing cellularmetabolic alterations, prolonged state of “neuroinflamma-tion”, activation of brainmicroglia, accumulation ofmanganese and ammonia, and systemic inflammation are themain causative factors of brain damage in liver failure. Themostwidely recognized neurological complications ofserious hepatocellular failure include hepatic encephalopathy, diffuse cerebral edema, Wilson disease, hepaticmyelopathy, acquired hepatocerebral degeneration, cirrhosis-related Parkinsonism and osmotic demyelinationsyndrome. Neurological disorders affecting liver transplant candidates while in thewaiting list may not only sig-nificantly influence preoperative morbidity and even mortality, but also represent important predictive factorsfor post-transplant neurological manifestations. Careful pre-transplant neurological evaluation is essential to de-fine severity and distribution of the neurological impairment, to identify the abnormalities still responsive to cur-rent treatment, and to potentially predict the inherent post-operative prognosis. The preferred specific indices ofneurological pre-transplant assessment may vary among centers, however, even with the aid of the current bio-chemical, neurophysiological, neuropsychological and neuroimaging diagnostic tools, the correct diagnosis anddifferential diagnosis of various syndromes may be difficult. In this article the relevant pathophysiological andclinical aspects of the most frequent brain and peripheral nervous system diseases affecting liver transplant can-didates with acute or advanced chronic liver failure are briefly reported. The practical diagnostic findings usefulfor the preoperative assessment and treatment, as well as the expected neurological evolution after liver trans-plantation are also evaluated.
© 2017 Elsevier Inc. All rights reserved.
1. Introduction
Compromised liver function as a consequence of either acute hepaticfailure or severe chronic liver disease and liver cirrhosis leads to insuffi-cient detoxification of some substances and catabolic products, whichaccumulate in the blood and are responsible for a broad range of neuro-logical and neuropsychiatric manifestations [1]. A strict relationship be-tween brain functioning and integrity of the liver is well known, and apathological liver may be responsible for various neurological syn-dromes, which affect both the central nervous system (CNS) and the pe-ripheral nervous system [2,3].
☆ Author contributions Carollo C and Barbieri S made literature search; Feltracco P andCagnin AC acquired and analyzed the data, and drafted the article; all authors contributedto themanuscript preparation, data interpretation, revision for important intellectual con-tent, editing, and approved the final version.⁎ Corresponding author at: Department ofMedicine UOAnaesthesia and Intensive Care,
Padua University Hospital, Via 8 febbraio 1848, 35128, Padua, Italy. Tel.: +39 498212222.E-mail address: [email protected] (P. Feltracco).
http://dx.doi.org/10.1016/j.trre.2017.02.0060955-470X/© 2017 Elsevier Inc. All rights reserved.
Liver transplant candidates may experience a great variety ofneurological disorderswhile on thewaiting list, whichmay significantlyinfluence preoperative morbidity and evenmortality. It has been recog-nized thatmany neurological disorders associatedwith acute or chronicliver failure tend to improve or disappear after successful orthotopicliver transplantation (OLT); however, some minor “residual” clinicalsigns may persist postoperatively in a variable percentage of livertransplanted patients. Furthermore, pre-transplant subclinical neuro-logical symptoms may become apparent in the event of graft dysfunc-tion or severe postoperative metabolic disturbances [4,5].
Liver transplant recipients are affected by the highest rate of CNScomplications among solid organ transplants (incidence between 10%and 85%), with focal and diffuse neurological deficits sometimesrepresenting a major obstacle to the improvement of short- and long-term outcomes [6]. Relevant adverse post-OLT neurological eventsoccur due to brain edema, increase of intracranial pressure, metabolicencephalopathy, cerebrovascular complications, osmotic demyelinationsyndrome, and opportunistic infections. Moreover, some pre-operativeneurological alterations such as dysarthria or akinetic mutism, confu-sion and seizures, may worsen due to the neurotoxic effects of calcine-urin inhibitors drugs required to prevent graft rejection [4,7]. Full

194 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
comprehension of the pathophysiology and proper management of theneurological manifestations of end stage liver failure has not yet beencompletely attained. In fact, multiple factors have been associatedwith brain damage, such as a prolonged state of brain “neuroinflamma-tion”, activation of brain microglia and inflammatory cells, accumula-tion of manganese and ammonia, altered permeability of the blood–brain barrier, altered neurotransmission, and inflammation of theperipheral nervous system [8]. Other negative direct or indirect neuro-logic effects are caused by chronicmalnutrition, gastrointestinal hemor-rhages, cerebral hypoperfusion and renal dysfunction [9–12]. The mostwidely recognized neurological complication of serious hepatocellularfailure is the complex syndrome of hepatic encephalopathy (HE), butmany other brain alterations associated with liver cirrhosis may occur,as listed in Table 1 [13].
Careful pre-transplant evaluation of the CNS and peripheral nervoussystem disorders is essential for identifying the abnormalities still re-sponsive to current medical treatment, and potentially predicting theinherent post-operative prognosis. An accurate assessment of baselineneurological features increases the understanding of how brain disor-ders can interfere with post-hospitalization quality of life in case of po-tential incomplete recovery after OLT. Patients with end-stage liverdisease are usually evaluated with indices that predict advanced dis-ease, such as the Child–Turcotte–Pugh score, or those that predict prog-nosis, such as the Model for End-stage Liver Disease score (MELD,MELD-Na). Preoperative neurological assessment is based on the specif-ic evaluation of both CNS and peripheral nervous system functions. Ex-amination of motor (pyramidal and extrapyramidal) and sensorysystem integrity, cranial nerves evaluation, as well as analysis of super-ficial and deep-tendon reflexes and cerebellar signs should always beperformed as first step neurological assessment before searching formore specific neurological features. Evaluation of the mental status,cognitive functions, speech characteristics, etc., is also extremely usefulin obtaining a detailed baseline neurological status andmonitoring pos-sible disease progression. Clinical and biochemical diagnostic tools, neu-rophysiological assessments (electroencephalography (EEG) and visual,auditory, and somatosensory-evoked potentials (EPs) and neuroimag-ing, have been adopted to correctly diagnose different stages of neuro-logical impairment. However, the choice of the preferred clinical orinstrumental parameters for neurological pre-transplant assessmentmay vary among centers, and the differential diagnosis of various syn-dromes may be difficult and critical, even with the use of “modern”technologies. This article mainly focuses on the most frequent CNSand peripheral nervous system diseases affecting liver transplant candi-dates with acute severe or advanced liver dysfunction. Patients withsevere liver dysfunction can have a great range of neurologicmanifesta-tions due to direct effects of hepatic disease on the central andperipheral nervous system (i.e. HE or acquired hepato-cerebral
Table 1Neurological manifestations associated with liver cirrhosis, from [13] with modifications.
Hepatic encephalopathy and minimal hepatic encephalopathy
Cirrhosis-related parkinsonismRaised intracranial pressure, cerebral edemaCNS infectious complicationsAcquired hepatocerebral degenerationCirrhotic or hepatic myelopathyCirrhosis related intracranial bleedingNeurologic complications related to specific aetiologies of liver diseaseNeurologic symptoms of Wilson diseaseHepatitis C infection related CNS complicationsOsmotic demyelination syndromeMarchiafava-Bignami diseaseWernicke encephalopathyNeurological disorders associated with malnutritionAlcoholic cerebellar degeneration, amblyopia, polyneuropathy,Wernicke–Korsakoff Disease
Alcohol related cerebral atrophy and cognitive decline
degeneration) or to diseaseswith concomitant hepatic and neurologicalinvolvement (i.e. Wilson disease). The neurological syndromes may re-quire a specific management, such in the case of acute liver failure, or inthe context of chronic liver cirrhosis or portosystemic shunting. The rel-evant pathophysiological and clinical aspects, the practical diagnosticfindings useful for the preoperative clinical assessment and treatment,as well as the expected neurological evolution after liver transplanta-tion, are briefly described.
2. Neurological aspects of hepatic encephalopathy
HE is a complex syndrome characterized by neuropsychiatric,neuropsychological and neurological disturbances caused by differentunderlying liver diseases or peri-hepatic vascular shunting, and influ-enced by a variety of precipitating factors. The development of HEmay manifest with a wide range of neurologic manifestations, whichare characterized by potential reversibility once the abnormality ofliver function is corrected. Sudden onset of confusion evolving rapidlyinto coma is a frequent presentation of acute HE episodes, often underthe trigger of some precipitating factors; in other circumstances, thesigns and symptoms may fluctuate slowly, with long periods withoutHE events [14]. Based on the clinical practice guidelines of theAmerican Association for the study of liver diseases (AASLD) and theEuropean Association for the study of the liver (EASL) [15], HE shouldbe classified according to four factors:
(1) the underlying disease; with type A HE resulting from acute liverfailure, type B resulting predominantly from portosystemic by-pass or shunting, and type C resulting from cirrhosis;
(2) the severity of manifestations; a summarized grading of severityof clinical manifestations of HE, according to both the WestHaven criteria (Old Classification) and International Society forHepatic Encephalopathies and Nitrogen Metabolism (ISHEN)classification, is reported in Table 2 [15],
(3) the time course; subdivided into episodic (spontaneous or pre-cipitated), recurrent (episodes occurring with a time interval of6 months or less), persistent (N2 weeks of mental statuschanges),
(4) the existence of precipitating factors; subdivided into spontane-ous non precipitated or precipitated (with specification of theprecipitating factors).
The so-called overt form of HE (OHE), definedwhen neurological andpsychiatric abnormalities are detected at the bedside, was divided intofour stages of severity based on the New Haven scale. However, giventhe largely subjective criteria for classifying a cirrhotic patient as stage1 HE, it was decided to abolish this stage of HE. Every cirrhotic patientwith disorientation to time has to be considered with definite OHE [16].
Minimal HE (MHE), once called covert HE, and defined when mini-mal or no symptoms are detected [17,18], occurs in nearly 70% of cir-rhotic patients; it has grown in importance over the recent years as itmay precede the development of OHE. MHE is defined as the presenceof test-dependent or clinical signs of brain dysfunction in patientswith chronic liver disease who are not disoriented or display asterixis.According to the ISHEN classification, covert HE (CHE) is essentiallythe amalgamation of stage 1 HE and MHE.
3. Neurological manifestations of acute liver failure (type HE)
Acute liver failure (ALF) is characterized by a rapid hepatocellularnecrosis that leads to the severe deterioration of liver function,alterations of coagulation and encephalopathy, which occurs withindays or weeks of the primary insult (less than 26 weeks) withoutevidence of pre-existing cirrhosis [19]. The most common aetiologies aredrug-induced liver injury (acetaminophen overdose being observed inb45%), food intoxication, viral hepatitis, autoimmune liver disease and is-chemic hepatitis. Neurologic manifestations are those of encephalopathy

Table 2Clinical grading of severity of HE and operative criteria; from [15] with modifications.
WCH including MHE ISHEN Description Suggested operative criteria
Unimpaired No encephalopathy, no history of HE Tested and proved to be normalMinimal Covert Psychometric or neuropsychological alterations of tests exploring
psychomotor speed/executive functions without clinical evidenceor mental change
Abnormal results of psychometric or neuropsychologicaltesting without clinical manifestations
Grade I Mild confusion, impaired attention, hypersomnia, insomnia orinversion of sleep patterns, depression or irritability, euphoriaor anxiety, intermittent disorientation
Despite oriented in time and space the patient appearsto have some cognitive/behavioral decay with respect tohis/her standard on clinical examination, or to the caregivers
Grade II Overt Apathy, drowsiness, lethargy, evident disorientation (usuallyfor time), obvious personality changes, inappropriate behavior,obvious asterixis, important deficits in the ability to performmental tasks
Disoriented for time (wrong day of the month, day of theweek, month, season or year) ± the other mentioned symptoms
Grade III Marked confusion, persistent disorientation and amnesia,somnolence to semi-stupor but responsive to intense verbalstimuli, unable to perform mental tasks, incoherent speech,gross disorientation for time and space, asterixis usually absent
Disoriented for space (wrong country state or region,city or place) ± the other mentioned symptoms
Grade IV Coma Patient without response to noxious stimuli
Table 3Basic principles of intensive care management of ALF patients.
Treatment of toxic injury,acetaminophen, mushroom poisoning
Antidotes; N–Acetylcysteine, activatedcharcoal penicillin
Sedation and mechanical ventilation(grade III HE, Glasgow Coma ScoreScale ≤8)
Normoventilation or short termhyperventilation if ↑ ICP
Optimal volume resuscitation andmaintenance of osmotic gradientacross BBB
Mixture of colloid and cristalloids,hypertonic saline or mannitol
Circulatory support and maintenanceof cerebral perfusion pressure
Inotropes, vasactive agents, steroids
Treatment of brain edema Sedatives, 30° head up, mannitol,dexamethasone, mild hypothermia,hyperventilation, ultrafiltration,indometacin (barbitures)
Treatment of subclinical seizures Phenitoin, levetiracetamRenal support Renal replacement therapies,
continuous hemofiltrationGlycemic control Glucose administration, careful
glycemic monitoringAntimicrobial treatment Broad spectrum antibiotics, antifungalsExtracorporeal liver assistanceand purification
Molecular Adsorbent RecirculatingSystem (MARS)Single Pass Albumin Dialysis (SPAD).Prometeus SystemPlasmapheresis
195P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
and brain edema. Encephalopathy is due to a rapid increase of bloodammonia level, which, in contrast to what happens in chronic liver fail-ure, determines an intense osmotic gradient for water, not responsiveto the cerebral compensatory osmotic mechanisms. Acute and severehyperammonemia induces cellularmetabolic alterations resulting in in-tracellular accumulation of hypertonic osmotic molecules (ions andamino acids), followed by an entry of water to re-establish the osmoticequilibrium. Accumulation of water in the brain causes astrocytic swell-ing and degeneration (cytotoxic edema); this phenomenon leads ini-tially to an increase in brain volume and then to an increase inintracranial pressure (ICP), with an exponential relationship at ad-vanced stages. Impaired cerebral vascular autoregulation with increasein cerebral blood flow is another mechanism involved in the develop-ment of brain edema. This is due to a physical breakdown of theblood–brain-barrier (BBB), which allows plasma macromolecules andother compounds to enter into the extracellular spacewith an addition-al increase in osmotic pressurewithin the brain (vasogenic edema). Thedegree ofwater accumulation in the brain in acute and chronic liver failureis different: higher quantities of water accumulate in ALF patients, whichare responsible for progressive elevation of ICP; patients with type B andtype C HE less frequently develop intracranial hypertension [1].
Early neurologic symptoms of ALF resembles a low grade HE, withattention deficits, somnolence, temporal and spatial disorientation, ap-athy or excitement, slow responses and reasoning; as cerebral edemaworsens stupor, psychomotor agitation or severe acute delirium mayrapidly evolve in a comatose state. Other associated symptoms may bemyoclonus or focal convulsive or non-convulsive seizures (generalizedseizures are uncommon), alteration of conjugate ocular gaze move-ments, and Babinski signs with increased muscle tone. Drowsinessand asterixis are frequently seen, however, they appear poorly correlat-ed with progression to more severe encephalopathy and intracranialhypertension [20]. Hyperreflexia and ankle clonus (involuntary andrhythmic contractions ofmuscleswhen stretched) have been correlatedwith an increased risk of progression from grade 3–4 coma and subse-quent development of severe brain edema [21]. When cerebral hyper-tension is severe, decerebrate or decorticate posturing is detectable, aswell as altered asymmetric pupillary responses suggestive of imminentdangerous elevation of ICP. Diffuse bilateral brain edema eventuallyleads to cerebral herniation andbrain death [22,23]. Repeated EEGmon-itoring should be considered in ALF patients for detecting non-convulsive seizures. Brain CT or MRI may detect indirect initial signs ofcellular edema, such as effacement of the cortical sulci, suprasellar andperimesencephalic cisterns; the neuroimaging features of advancedand irreversible forms may include complete disappearance of gray-white matter differentiation, transtentorial or cerebellar herniation orintracranial bleed. ALF is a critical condition requiring ICU admissionwhen the patient becomes agitated or has decreased levels of vigilance,
and a comprehensive intensive care as HEprogresses. Spontaneous liverregenerationmay occur approximately in 45% of patientswith ALF,withthe highest recovery and survival rate (55–65%) reported followingacetaminophen overdose or hepatitis A infection [19]. The general prin-ciples of ICU management of ALF patients are listed in Table 3.
Prioritization in organ allocation systems and a timely performedliver transplantation are fundamental in these patients since ALF is asso-ciated with high morbidity and mortality. The King's College Hospitalcriteria have been extensively used for patient selection, and were thefirst to differentiate between paracetamol-induced and other aetiol-ogies of ALF [24,25]. Patients fulfilling the criteria are very likely to dieif they do not receive transplants [25]. However, the King's Collegecriteria are acknowledged to have high degree of specificity but a lowlevel of sensitivity. In order to improve OLT candidate selection variousprognostic models have been proposed, such as SOFA score, APACHE II,MELD, and others based on composite scores of different clinicalmarkers on patient admission; however, all these models lack of signif-icant predictive value, specificity and validation in this setting [25]. Out-comes following OLT in ALF patients have improved in the recent years,with a better prognosis for ALF associated with paracetamol toxicity,and oneyear survival ranging between 74% and 84%. Although these re-sults are worse than those of patients grafted for other indications, they

196 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
compare very favorably or are even better than those seen in candidateswith end stage liver disease intensively treated or ventilated at the timeof organ allocation (oneyear survival of 64% and 54% respectively)[26,27].
Brain edema and intracranial hypertension resolve within 48 h fol-lowing liver transplantation when the graft function is good; however,various neurological symptoms such as tremor, seizures and speech dis-orders can persist in the early postoperative course. Livingdonor graftsfor ALF are frequently used in Asia (reported rates between 6% and15%); in Europe and USA living donation approximates only 1% of trans-plants for ALF. The emergency settings do not allow, in fact, sufficienttime to assess potential donor's spontaneous willingness to donate orto rule out important ethical and medical issues.
4. Neurological manifestations of type B and type C HE
The pathogenesis of OHE associated with portal-systemic shunting(type B) and cirrhosis (type C) remains still not completely clear; sub-stances such as ammonia that accumulate in the brain due to portal-systemic shunting, cerebral neuroinflammation and systemic inflam-mation, oxidative stress, and genetic difference in the conversion rateof glutamine to ammonia have been suggested to play major roles inthe development of OHE [28]. Ammonia stimulates the glutamine syn-thetase enzyme in the brain, which converts glutamate and ammoniainto glutamine. Increased diffusion of ammonia and other gut-derivedtoxins into the brain leads to glutamine accumulation, which induces ox-idative stress, energy failure, and morphologic changes in astrocytes (as-trocyte swelling). Ammonia alters the transfer of amino acids andelectrolytes across the astrocytes andneurons. Chronic hyperammonemiaper se induces neuroinflammation and a great variety of neurotransmitterand neurochemical modifications, such as alterations in the function ofthe glutamate-NOcGMP pathway in the cerebellum [29]. Systemic “pe-ripheral” inflammation, which mainly derives from bacterial infections,spontaneous peritonitis with damage to the intestinal barrier and bacteri-al translocation, may also maintain and potentiate the neuroinflamma-tion. Hyperammonemia and systemic inflammation play synergisticroles and cause well-known triggers for the development of OHE[30,31]. The contribution of neuroinflammation to the pathogenesis ofHE in patients with chronic liver diseases was studied using PET and li-gandswhich bind to the translocator protein (18 kDa) (TSPO), a surrogatemarker of microglial activation. In the study by Cagnin et al. [32]. in-creased binding of [11C](R)PK11195 to TSPO in the brains of cirrhotic pa-tients suggested that the presence of neuroinflammation in patients withHE was correlated with altered microglial function and hence with thegrade of cognitive impairment (Fig. 1b).
Fig. 1. Brain MRI and PK11195-PET study of hepatic encephalopathy. T1 coronal brain MRI of aganglia (a), and the corresponding slice image obtained with 11C–PK11195-PET (b) showing d
Anothermechanism involved in the etiology of HE includes some al-terations in the permeability of the blood–brain barrier to water andother small molecules; these changes, secondary to the release ofTNFa and interleukins from microglial cells and astrocytes, not only in-crease the neuropsychological impairment due to hyperammonemia,but also promote the misdistribution of neurotransmitters [33–35]. Inpatients with HE, low grade brain edema, resulting as an osmotic re-sponse of the astrocytes to increased intracellular glutamine, andbrain white matter alterations on magnetic resonance-diffusion tensorimaging (MR-DTI) were demonstrated by Gomez-Anson et al. [35].The authors suggested that white matter alterations could be due tothe prolonged effects of neurotoxins and longstanding edema, whichare factors that are capable of inducing demyelination and irreversiblealterations. Persistent structural injuries to the white matter might notbe reversed with OLT [36]. Important factors that can precipitate HE in-clude gastrointestinal bleeding, hypokalemia, infections, dehydration,constipation, hypotension, oral protein load, deteriorating liver func-tion, anesthesia and surgery. However, sometimes no apparent precipi-tating factors are detectable. Many liver transplant candidates mayexperience one or more episodes of OHE at some time during their ill-ness, with the possible occurrence of a wide range of mental andmotor dysfunctions. Acute episodes of HE are characterized by the sud-den (or over hours to days) development of an acute confusional state,with impairedmental state, fetor hepaticus secondary to the exhalationof mercaptans, and neuromuscular disorders. Frank confusion, stuporand even deep comamay arise in case of delayed reversal or worseningof HE [16]. Neuropsychological deficits may initiate with apathy andlethargy and may involve multiple cognitive abilities, such as memory,language, visuospatial skills, attentional processes and executive func-tions. Aggression and hyperactivity progressing to dementia are otherpossible behavioral disturbances. Neuromuscular abnormalities arecommon, usually in the form of increased muscle tone, hyperreflexia,and asterixis. Signs of pyramidal tract dysfunction tend to disappear asHE progresses, and they are eventually replaced by hypotonia if comadevelops. Extrapyramidal symptoms, including tremor, rigidity, brady-kinesia, and shuffling gait, have also been described. Asterixis, althoughnot exclusive to HE, is a characteristic feature of this disease. It is causedby dysfunction of diencephalic motor centers that regulate the tone ofagonist and antagonist muscles [37]. Testing for eliciting asterixis in-cludes dorsiflexion of the patient's hands with the arms extended andthe fingers separated; under these conditions, involuntary flappingtremor and rapid, involuntary, flexion-extension movements of thewrist may arise. This tremor can also manifest in the tongue and lowerextremities, with difficulties in maintaining posture or position[28,35]. Asterixis tends to reverse as HE progresses to coma; at this
patient with hepatic encephalopathy showing hyperintense lesions in the bilateral basaliffuse microglial activation in the basal ganglia, midbrain and cerebral white matter.

Table 4Differential diagnoses of encephalopathy, from Refs. [48,50] with modifications.
CNS infectious diseases: meningitis, encephalitis, and intracranial abscess
Intracranial lesions: intracranial bleeding, cerebral edema, stroke, tumorMetabolic encephalopathy: hypoglycemia, vitamin B1 deficiency, electrolyteabnormalities, hypothyroidism, anoxia, hypercapnia, and uremia
Toxic encephalopathies including delirium tremensHyperammonemia from other causes: inherited urea cycle disordersToxic encephalopathy: acute alcohol intoxication, alcohol withdrawal,Wernicke encephalopathy
Encephalopathy from drugs: sedative-hypnotics, antidepressants,antipsychotic agents, and salicylates
Post-seizure encephalopathy
197P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
stage, other signs of predominant pyramidal involvement may becomeprevalent [16]. Focal neurological deficits, most often hemiparesis orhemiplegia, and visual disturbances, although rare, have also been re-ported in patients with OHE. Serious damage to various cortical struc-tures, also in the past medical history, and chronic injury to the retinalglia have been suggested to be causative factors [38–40]. Clinicalmanifestations of severe chronic HE may also occur in association withataxia, dysarthria, gait abnormalities, and tremor, which are typicalfindings with other coexisting diseases, such as myelopathy, acquiredhepatocerebral degeneration, and cirrhosis-related parkinsonism. Bra-dykinesia and other mild parkinsonian signs are common permanentneurological disorders between recurrent episodes of OHE. MHE refersto motor and cognitive deficits that are not noticeable on clinical exam-ination but are detected using specific neuropsychological or electro-physiological tests [41]. “Minimal” abnormalities of the neurocognitiveand motor functions primarily affect information processing, coordina-tion, the ability to perform complex tasks, such as driving, and the skillsto maintain spatial orientation, all with a subtle but negative impact ona patient's quality of life [14]. Early identification and treatment of MHEare important, not only to prevent deterioration of daily living but alsoto decrease the risk of the development of OHE, which is associatedwith increased mortality in patients with cirrhosis and, hence, reducedsurvival for candidates on the waiting list for liver transplant [42]. Dif-ferent psychometric tests, such as the Psychometric HE Score (PHES),the Number Connection Test A and B, the Line Tracing Test, the SerialDotting Test, the Digital Symbol Test, etc., can be applied to identify im-pairments in memory, attention, visuospatial abilities, and fine motorskills. They are particularly useful in detecting the subclinical symptomsofMHE and the severity of low-grade HE [43–45]. A detailed descriptionof these tests is beyond the scope of this article. The diagnosis of HE re-lies essentially on the clinical assessment, along with specific EEGchanges and neuroimaging findings, while the serum ammonia level isnot correlated with the presence or severity of HE. EEG may be usefulto diagnose and grade HE objectively. The classic EEG changes arehigh-amplitude low-frequency waves and triphasic waves. The degreeof alterations is related to disease severity, i.e., more severe OHE is relat-ed to slower EEG activity [43–45]. However, some findings are not spe-cific to HE, and triphasic waves are found in many other metabolicencephalopathies [46]. In patientswith cirrhosis and alteredmental sta-tus, EEG is also important in excluding non-convulsive seizure activity.
Recently, Schiff and coworkers [47] applied a low-cost, user-friendlyEEG system (the Emotiv EPOC 16 electrode cap), which also allows forEEG acquisition in settings with limited neurophysiological experience.This EEG recording tool is less expensive, wireless, non-invasive, porta-ble, and reusable, and it produces automated indices estimated to behighly comparable to those from standard EEG. Brain CT imaging haslow sensitivity for detecting early signs or MHE. In contrast, acute epi-sodes of OHE may display extensive cortical edema involving the deepgray matter. An MRI scan can offer more specific information. In fact,MRI with diffusion-weighted imaging (DWI) or fluid-attenuated inver-sion recovery (FLAIR) images may show alterations of the cingulategyrus and insular cortex, with sparing of the perirolandic and occipitalcortex. This pattern has been considered a characteristic feature of HE[48]. Cerebral edema, T1-weighted MRI hyperintensity of the globuspallidus and substantia nigra, white matter high signal intensities in-volving the hemispheric corticospinal tract, and diffuse cortical atrophyhave been commonly described in HE [49] (Fig. 1a). The clinical featuresof HE may be somewhat similar in several other clinical syndromes,which may enter the differential diagnosis. The most common diseasesin patients with liver disease leading to variable degrees of encephalop-athy and requiring diagnostic exclusion are reported in Table 4 [48,50].
A detailed description of type B, and type C HE management is be-yond the scope of this article; briefly, the basic principles of treatmentof these syndromes firstly include the assessment of severity of the dis-ease, with grade 1–2HE patients beingmanageable as outpatients if suf-ficient adherence to treatment is demonstrated and caregivers are
available, while hospitalization being instead required, sometimes inan intensive care setting, for grade 3–4HE individuals. Serious advancedHE may also require tracheal intubation to provide respiratoryassistance and to protect the patient from ab ingestis pneumonia, andsupportive cardio-circulatory measures to revert hemodynamic insta-bility. Correction of malnutrition e.g. avoidance of meals too rich in pro-teins, but at the same time avoidance of excessive protein restriction(ammonia-lowering strategies with recommended daily protein intakeof 1.2–1.5 g/kg in a daily energetic regimen of 35–40 kcal/kg), avoid-ance of sedatives, alcohol consumption, long fasting periods, preventionof renal hypoperfusion, hypovolemia, hypoglycemia, constipation, pre-vention of precipitating factors such as gastrointestinal bleeding, infec-tion, hyponatremia, thiamine deficiency, as well as reducing colonicammonia-producing gram-positive and gram-negative aerobic and an-aerobic bacteria, are the fundamental strategies of initial supportivecare [51–53]. Although no consensus has emerged concerning the ben-efits of branched chain aminoacid (BCAA) administration, avoiding aprevalent accumulation of aromatic amino acids and restoring the ap-propriate balance of BCCA levels might benefit HE patients [54]. Colonicand bowel cleansing with various laxatives, non-absorbable disaccha-rides, enemas administration, irrigation of the gut with mannitol via ap.o. tube, etc., may decrease colonic bacterial growth and potentiatethe elimination of nitrogenous compounds. Lactulose is the mainstayof treatment to lower blood ammonia concentration, even thoughcurrent standards of evidence-based medicine about its efficacy havenot met yet. Lactulose is catabolized by the bacterial flora to lactic acidand acetic acid, which reduce colonic pH and favor the transformationof NH3 in the non-absorbable NH4+. Other effects include ahyperosmolar load that improves gastrointestinal transit, an increasein stool volume which leads to increased fecal nitrogen excretion, andan increased incorporation of ammonia by bacteria. Probiotics are capa-ble to reduce plasma ammonia concentrations, but permanent clinicallyrelevant benefit and positive outcomes have not been demonstrated[55]. Antibiotic treatment with oral neomycin, metronidazole, vanco-mycin and rifaximin, has demonstrated to improve clinical and mentalstate and reduce the number of hospitalizations [56]. Other therapiessuch as dopaminergic agonists, benzodiazepine receptor antagonistflumazenil, L-ornithine-L-aspartate to lower serum ammonia levels,and levocarnitine have also been adopted, but with paucity of data onthe real benefit. Patients with nonresponsive HE should also be consid-ered for interventional radiological occlusion of large spontaneousportal-systemic splanchnic shunts. The development of OHE should beconsidered a “high priority” criterion for OLT because a successful trans-plant procedure can improve the clinical course; however, prioritizationof the candidate based exclusively on severe HE is not common amongvarious transplantation centers. Episodes of HE in liver transplant candi-dates usually recover without major neurological deficits, but severe oreven non-severe forms of HE may have a considerably negative impacton post-transplant outcomes. A history of HE while on the waiting listmay be a predictor of post-OLT neurologic disturbances, and some de-gree of persistent cognitive and/or motor deficit (permanent CNS dam-age) following the relapse of HE or MHE has been demonstrated [57].

198 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
Worse long-term psychometric testing results and global cognitivefunction in patients who had HE prior to transplantation have beenalso demonstrated by Sotil et al. [58].
Campagna et al. [59] reported that patients with a history of OHEshowed greater improvements in cognitive alterations after OLT thanpatients without a history; however, preoperative OHE was associatedwith both poorer global cognitive performance and worse EEG at the1-year follow-up evaluation. Other studies have demonstrated that per-manent deficits of memory, learning abilities, as well as minor motordeficits may be irreversible and may persist even after the liver trans-plant procedure [4,60]. However, in spite of potential and unpredictableresidual transient or permanent neurological deficits, and notwith-standing theMELD-based organ allocation systemdoes not assign prior-ity for severe HE, patients with severe HE can have a rapid reversal ofsymptoms and good outcome with timely performed liver transplanta-tion [15].
5. Neurological manifestations of Wilson disease
Wilson disease (WD, hepatolenticular degeneration), an autosomalrecessive disease caused by mutations in the ATP7B gene, is associatedwith an impairment of cellular copper transport and consequent toxicaccumulation of copper in the liver, brain and cornea. In the liver, bothmacrosteatotic and microsteatotic changes may occur, followed bylobular necrosis, periportal inflammation, swelling, and diffuse necrosis[61]. When the disease progresses, an initial picture resemblingautoimmune chronic hepatitis may lead to a mixed macronodular–micronodular histological pattern, eventually resulting in manifest cir-rhosis. In the setting of chronic “stable” liver disease, some patientsmay develop acute liver failure and rapid functional impairment.
Brain lesions in WD are mainly localized in the lenticular nuclei,where they present a brown color on gross pathology due to copper de-position [62]. Other lesions, such as gliosis, cystic changes, and necrosis,may be discovered in the cerebellum, cerebral cortex, thalamus andbrainstem. Characteristic ophthalmologic manifestations, known asKayser–Fleischer ring, are present in almost all patients with predomi-nant neurological WD and in approximately 50% of cases of hepaticWD. Kayser–Fleischer ring, typically brown to brownish-green in colorand more visible in the superior and inferior regions of the cornea, isalso due to copper deposits in the limbic region (Descemet membrane)of the cornea. Apart from presenting with the clinical findings ofvariable liver dysfunction, a large percentage of patients with WD areinitially diagnosed because of the occurrence of neurological distur-bances (neurologic WD) or psychiatric manifestations. Hepatic, neuro-logical and psychiatric presentations of WD occur in roughly equalproportions [63].
Relevant psychiatric symptoms of WD include personality changes,reckless, incongruous behavior, reactive depression or anxiety, irritabil-ity, impulsivity and disinhibition, emotionality, apathy, mania, and cat-atonia. Psychotic features are quite rare [64]. Subcortical dementia isassociated with slowness of thinking, decreased attention, memoryloss, poor planning and decision making and executive dysfunctionmay also be present.
Usually, neurologicmanifestations ofWDoccur between early child-hood and the fifth or sixth decade of life, and with a peak incidence be-fore the age of 20 [65]. Either when very subtle or when rapidlyprogressive, neurological disorders may manifest in patients who areasymptomatic from their liver disease [64]. Typical features of neurolog-ical WD include dysarthria, dystonia, tremor and parkinsonian signs. Inthe earlier stages, poor coordination, tremor and loss of finemotor con-trol are predominant, followed later by gait disturbance, rigidity, andpseudobulbar syndrome. Tremor can resemble essential tremor; thearms, head and legs are frequently involved,with absence of voice trem-or. In advanced WD, tremor may manifest with multiple position- andtask-dependent characteristics. Thewing beating tremor (amplitude in-creasingwith duration of posture holding), rest tremor, postural tremor,
and kinetic tremor may also be present in a mixed variety in severeforms of WD [66]. Dysarthria with other features, such as ataxia,hypokinesia, and dystonia, as well as speech impairment, is found in al-most all cases of neurological WD. Ataxic dysarthria, hypophonic orslurred dysarthria with variations in word spacing and volume is verycommon in patients with tremor [67]. Dystonia is also frequent, and itoftenworsenedwith disease progression.Mild initial focal or segmentaldystonia, blepharospasm, cervical dystonia (torticollis), and writer'scramp may evolve into multifocal, bilateral and generalized dystonia,with serious debilitating contractures in the most severe forms. A com-mon dystonic facial expression is known as risus sardonicus. Parkinso-nian features mainly include bradykinesia, imbalance, and cogwheelrigidity. Rigidity and tremor are typically asymmetric and are usually ac-companied by other neurologic deficits, such as hypophonic speech andmicrographia [65]. Choreoathetosis is more often observed in youngerpatients. The movements are involuntary with unpredictable contrac-tions, and they are variable in speed and direction; they usually affectthe distal limbs, but the face and trunk are also often involved. Slowwrithing movements with a sinuous quality can be associated. Violent,uncontrolledflailingmovements of the extremities,with proximalmus-cle involvement (ballism),may be observed in advancedWD. Cerebellarinvolvement is associated with overshoot dysmetria of the eyes andlimbs or ataxic dysarthria, limb incoordination, impaired accelerationand braking, and impaired tandem gait. Frank limb ataxia is uncommon[66]. Other manifestations include breakdown in the rhythm of repeti-tive, alternating single movements (dysrhythmia), breakdown of nor-mal coordination of joint rotations, hyperreflexia and myoclonus. Livertransplant candidates affected by WD, while on the waiting list, maymanifest great variability in different neurological disturbances, oftenin combination with the underlying hepatic manifestations. Amongthem, central pontine myelinolysis is often seen, and it may occur inthe absence of the commonly recognized etiological factors [68]. The di-agnosis of WD is based essentially on a high degree of suspicion in thepresence of abnormal liver function and movement disorders withatypical presentations. Kayser–Fleischer ring should be sought by an ac-curate ophthalmological inspection with a slit lamp, and liver biopsyshould be performed in a timely manner to evaluate liver copper con-tent and structural degeneration. An increased urinary copper concen-tration is highly suggestive of WD, as well as low serum levels ofceruloplasmin, which is a copper-carrying protein normally bound to90% of circulating copper. BrainMRI images show areas of high T2 signalin the lentiform and caudate nuclei, thalamus, and white matter. Theclassical signs of “face of the giant panda” in the midbrain, along withtectal plate hyperintensity, central pontinemyelinolysis-like abnormal-ities, and concurrent signal changes in basal ganglia, are common find-ings [69,70]. Medical treatment of WD is very effective and includespharmacologic agents capable of removing or detoxifying the tissuecopper that has accumulated, reducing the amount of toxic free copper,and preventing re-accumulation. Pharmacological treatment essentiallyincludes: a) chelators (D-penicillamine [DPA], not indicated in case ofkidney disease or in patients who are allergic to penicillin) or trientine,a second-line agent in case of intolerance to D-penicillamine; and b)zinc salts, whichmainly reduce copper absorption by increasing the en-dogenous chelator metallothionein in enteric cells [71]. Ammoniumtetrathiomolybdate, an agent which complexes copper in the intestinallumen and prevents its absorption, and in addition complexes copperwith albumin in the blood once it has been absorbed, has also been test-ed in patients with neurologicWD. However, its effects seem to be tran-sient and reverse with suspension of the drug [72]. Even thoughprospective, randomized studies directly comparing the safety and effi-cacy of these drugs in the treatment of WD are lacking, however, theyare included in the AASLD and EASL guidelines, which recommendzinc salts as a first line of treatment in patients with neurological symp-toms and in those who are presymptomatic, and chelators (DPA ortrientine) in non-neurological WD [73,74]. Zinc acetate therapy hasbeen proved successful as preventative therapy and maintenance

199P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
therapy for neurological WD [65]. However, various authors only con-sider zinc as an adjunctive therapy for the initial treatment of symptom-atic patients especially those with a high copper load [75,76]. Zinc isslow acting, it takesmonths to reverse copper toxicity, and carefulmon-itoring and follow-up for potential deterioration is recommended in thesymptomatic patients who better benefited from chelating agents [72].Improvement of symptoms in patients with neurologic WD is slow andmay be observed after 2–3 years. It has been shown that the neurologicstatus of WD patients may worsen with the initiation of D-penicillamine.The occurrence of newneurologic symptoms or any neurologic deteriora-tion after beginning of treatment, are likely due to themobilization of he-patic copper stores which may result in an increased brain copperexposure [77]. Hemodialysis, hemofiltration and plasma exchange withfresh frozen plasma replacement, have also been used as temporizingmeasures to remove copper.
A low copper diet and avoidance of copper-rich foods are also rec-ommended to prevent accumulation or re-accumulation of copper.
In untreated WD and in patients scarcely adherent to treatment,copper accumulation in the liver eventually leads to the developmentof cirrhosis, whereas the neurological disturbances progressively wors-en until serious dystonic, akinetic, and mutism complications occur.
It has been recognized that, although OLT represents the definitivetreatment for WD after drug treatment failure, prioritization on thetransplant waiting list usually occurs when liver dysfunction signifi-cantly worsens, an acute and severe impairment develops, or advancedliver failure (unresponsive to treatment) is already present at the timeof diagnosis. Deterioration of neurological symptoms, evenwhen signif-icant, is usually not considered for prioritization. The indication for OLTin patients with rather low-grade liver disease but disabling neurologicfeatures is still debated [78]. However, successful reversal of behavioraldisorders, psychosocial functions, brain MRI findings, and improve-ments of global neurological impairment with no recurrence of the dis-ease have been reported following OLT in many case reports, small caseseries, and largemulticentre studies [79–81]. In the recent literature andin clinical practice, although many patients with intractable neurologicmanifestations of WD have benefited from liver transplantation[82,83], evidence for both a positive final outcome after OLT and defin-itive reversal of neurological disturbances has not yet been demonstrat-ed. In fact, less favorable outcome when compared to transplantationsperformed for other etiologies, have been reported in patients with pro-gressive neurological deterioration not responsive to correct medicaltreatment [84]. On behalf of the Italian AISF 2000 OLT Study Group, ascoring systemwas introduced byMedici et al. [81] to assess objectivelytheneurological symptoms ofWD, not only retrospectively but also pro-spectively. According to this system, the impairment of neurologicalsigns (rigidity, bradykinesia, ataxia, tremor, dystonia, dyskinesia) andneurological function (walking, talking, eating and daily living activi-ties) is evaluated by the following score: 3 = no impairment; 2 =mild impairment; 1 = moderate impairment; and 0 = severe impair-ment. A higher score is suggestive of better preoperative neurologicalconditions and a reasonably better post-transplant outcome, while alower score is indicative of poor neurological status and a more difficultpostoperative recovery.
In accordancewith bothWang et al. [80]. andMedici et al. [81]., livertransplant may be the only life-saving treatment option for rapidlyevolving hepatic and neurological WD; however, patients with ad-vanced neuropsychiatric and neurological symptoms showed a signifi-cantly lower survival rate than other WD patients. Furthermore, in thestudy byMedici, the presence of neuropsychiatric symptomswas a neg-ative prognostic factor even when OLT led to complete resolution of theneurological symptoms. A France experience on long-term results ofOLT for WD [85] reported a 5-year and 10-year patient survival rate of87%. In their study “pure neurological” patients have a significantlyworse prognosis after LT when compared to hepatic WD patients. Con-sidering the current data, emergency liver transplantationmust be con-sidered when the initial manifestations of WD present with the
characteristics of fulminant liver failure; OLT may, in fact, potentiallycorrect the underlying hepatic metabolic defects. OLT may be also theonly option for patients with ALF and chronic liver disease or thosewith cirrhosis and portal hypertension who are unresponsive to orpoorly compliant with chelating medications. Finally, a timely andjustified OLT should be performed before neurological deficits becomeirreversible. In fact, patients with severe long-term neurological impair-ment are unlikely to recover after OLT. In the various evolving stages ofWD, frequent and accurate neurological evaluations by an experiencedneurologist, and preferentially by using standardized tools such as theUnified Wilson's Disease Rating Scale [86] are important. An accurateassessment is essential not only to characterize the severity of diseasecompletely but also to emphasize the potential importance ofperforming OLT before neurological impairment becomes irreversibleor even to contraindicate transplant in cases of definitive and perma-nent brain injury.
6. Acquired hepatocerebral degeneration (non-Wilsonianhepatolenticular degeneration)
Chronic acquired hepatocerebral degeneration (AHCD) is a rareclinico-pathological syndrome in the context of chronic hepatic failure,which occurs independently from the underlying liver disease and isnot related to acute encephalopathy. It is characterized by extrapyrami-dal, neuropsychiatric, and cerebellar disorders and almost always per-manent damage to brain tissue. This heterogeneous neurologicaldisorder has also been defined as non-Wilsonian hepatolenticular de-generation (NWHD) [87]. Patients affected by AHCD should not be ex-cluded from being listed for liver transplantation because OLT may bethe only effective therapy in some cases. The neuropsychiatric and cog-nitivemanifestations of AHCDmainly affect the attention and executivedomains, whereas chronic injury to the cerebellum may manifest withataxia anddysarthria, andbasal ganglia involvementmay induce abnormalmovements, such as dystonia, dyskinesia, athetosis and chorea. The devel-opment of a progressive hypokinetic-rigid syndrome in end stage liver fail-ure has been referred to as “cirrhosis-related parkinsonism”, whichappears to be unrelated to the etiology of liver disease. The incidence ofcirrhosis-related parkinsonism has been reported at 1 to 21% [88].
Alterations in the basal ganglia, dysfunction of the circuits and dis-ruptions in the networks connecting the prefrontal and frontal–parietalregions with the basal ganglia are considered the main pathogeneticmechanisms of parkinsonian motor features [89]. Histopathologicalbrain damage has been attributed to a possible role of manganese toxic-ity. In the presence of significant porto-systemic shunts, an excessiveamount of manganese, usually removed via the hepatobiliary route, ac-cumulates in the basal ganglia of patients with liver cirrhosis [90]. Theneurotoxic effects of increased brain manganese result in neuronalloss in the basal ganglia and cerebellum [91]. Other neuropathologicalfindings include patchy cortical necrosis, proliferation of Alzheimertype II glial cells, and diffuse reactive fibrillary gliosis [92]. The potential-ly broad range of clinical presentations of cirrhotic parkinsonism maysuggest a multifactorial pathophysiology. However, a constant findingis the presence of portal hypertension and of different degrees ofportosystemic shunts, which are not always observed with Doppler ul-trasonography [93]. Many studies have documented a significant nega-tive influence of manganese on the dopamine (DA) neurotransmittersystem, abnormality, which involves DAmetabolism, receptor integrity,displacement from its storage site, transport and release from dopami-nergic nerve endings [12,94]. An excessive amount of aromatic aminoacids, which may shift to the brain across the blood–brain barrier, hasbeen once advocated among the other causes by Fischer et al. [95],along with the presence of false dopaminergic neurotransmitters capa-ble of inducing structural brain damages such as octopamine. Diagnosisof AHCD is based on the assessment of cranial nerves, pyramidal andextra-pyramidal systems, cerebellar and sensory function, speech, cog-nitive abilities and mental status. The onset of parkinsonian signs may

200 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
be insidious, although the clinical picture can evolve rapidly into pro-gressive hypokinesia, hyperammonemia, tremor and rigidity, gait dis-turbances and postural instability. Cognitive dysfunction and/oralteration of consciousness are often significant. Although parkinsonismmay coexist with HE in some cirrhotic patients, it should not be con-fused with a manifestation of HE because AHCD-related parkinsonismpresents long-term, persistent extrapyramidal signs and relatively lesscognitive dysfunction [96]. The characteristics and severity of atypicalparkinsonism in potential candidates for liver transplantation can beassessed using the Unified Parkinson's Disease Rating Scale (UPDRS);the International Cooperative Ataxia Rating Scale (ICARS) can be usedto evaluate ataxia and cerebellar dysfunction [97,98].
Several features may differentiate cirrhosis-related parkinsonismfrom idiopathic Parkinson disease; the former syndrome presents a rel-ative absence of resting tremor (kinetic hand tremor is more commonthan resting tremor), early gait and balance dysfunction, mild cognitiveimpairment at the time of presentation, symmetric signs more oftenthan asymmetric, variable/transient signs and no levodopa responsive-ness [12,90]. These differences suggest that the cirrhotic-parkinsonismis different from idiopathic Parkinson disease, and various studieshave reported clinical improvement in extrapyramidal symptoms afterOLT [99,100]. However, due to substantial, irreversible neuronal cellloss in chronic advanced liver disease, parkinsonism in cirrhosis doesnot always reverse with OLT [101]. The routine diagnostic work-up in-cludes brain MRI and single photon emission tomography (SPECT) ofthe dopaminergic system (DaT-scan). In AHCD, T1-weighted MRI ischaracterized by signal hyperintensity in the internal pallidum, puta-men, caudate nucleus, capsula interna,mesencephalon, and cerebellum.These abnormalities are associated with manganese deposition in thebasal ganglia nuclei, but they may also be present in cirrhotic patientswithout extrapyramidal signs [102–104]. Burkhard and coworkersdemonstrated thatMRI hyperintensitiesmay also involve the substantianigra in patients with AHCD-associated parkinsonism symptoms [90].Neuroimaging is very helpful in differentiating AHCD from genetichepatolenticular degeneration (Wilson disease), as previously reported.SPECT studies of the striatal dopamine D2 receptors and measurementof dopamine transporter function have also been applied to diagnosethe severity of cirrhosis-related parkinsonism [105,106]. The beneficialeffects of L-DOPA in the treatment of cirrhosis-related parkinsonismhave not been fully demonstrated, although in some reports, improve-ments of hypokinesia and rigidity were noted following L-DOPA treat-ment [103]. It has been suggested that dopaminergic treatment canonly succeed if striatal dopamine D2 receptors are available, both atthe presynaptic and post-synaptic sites, and that the loss of DA trans-porter sites could contribute to the lack of response to L-DOPA [88].Treatmentwith bromocriptine (DA receptor agonist) has been associat-edwith significant improvements inmotor coordination, gait ataxia andtremor. Ammonia-lowering agents such as lactulose and antibiotics, andethylenediaminetetraacetic acid (EDTA), a chelator of manganese, havealso been administered, but with inconclusive results [95]. The adminis-tration of trientene, another drug with the capacity to chelate manga-nese, was found to decrease circulating manganese, attenuate MRIsignal hyperintensities, and improve parkinsonism [107].
Marked improvement of neurological signs and radiological abnor-malities with persistent reversibility, was observed in two patientsafter the administration of branched-chain amino acids (prolonged i.v.infusion of 350–500 ml/day of BAA, followed by 100–150 g/day oralBAA) [108], suggesting also a significant role of aromatic amino acidsin the AHCD pathogenesis.
The beneficial effect of liver transplantation, both in improving neu-rological disorders and in attenuating or even eliminating abnormalMRI signals [100], has been reported in various case reports and insmall case series. The association of parkinsonism, dementia and T1-MRI signal hyperintensity was considered by Fabiani et al. a determi-nant factor for indicating a liver transplant [109]. An improvement ofbradykinesia, gait difficulties, rigidity, tremor and normalization of
pallidalMRI hyperintensities, have been reported following a successfulOLT in N50% of patients with cirrhosis-related parkinsonism [110–112].However, no improvement after OLT, and only transient improvementfollowed by a gradual recurrence, has also been reported [110,113]. Acomprehensive neurological examination prior to transplant is manda-tory in order to assess the potential reversibility of the syndrome, and tofind out whether manganese deposition in the basal ganglia and nigralsubstance had already resulted in extensive cell lesions and irreversiblecerebral damage.
7. Hepatic myelopathy (cirrhotic or Porto-systemic myelopathy)
Hepatic myelopathy (HM) is a rare and severe neurological compli-cation of liver cirrhosis, characterized by chronic and progressive evolu-tion and permanent loss of myelin in the dorsal or lateral corticospinaltracts of the spinal cord. It affects approximately 2.5% of patients withchronic liver dysfunction [114]. The clinical features of HM havebeen reported in association with HE, post-shunt surgery or post-TIPSS (transjugular intrahepatic portal systemic shunting) proce-dures [115]. Increasing occurrence of HM has been documentedwith the diffusion of TIPSS as the standard procedure for refractoryvariceal bleeding [116].
Enhanced portosystemic shunting, leading to nitrogenous productsbypassing the liver, overproduction of fatty acids, indoles and mercap-tans, vitamin B deficiency, increased ammonia levels, hypoproteinemiaand malnutrition are among the most commonly recognized causes ofHM. Toxic metabolites and neurotoxins cause white matter demyelin-ation in the brain and the spinal cord, with a selective predispositionfor the motor system. Neuropathological studies have demonstratedsymmetrical demyelination, predominantly of the lateral corticospinalpyramidal tracts. Demyelination is a hallmark of the early stages ofHM, but with disease progression, a variable degree of irreversible axo-nal loss occurs that does not extend beyond the cervical cord level[115–117]. The typical features of HM include an insidious onset andthe progressive development of lower limb spastic paraplegia or quad-riplegia in the presence of symptoms of chronic liver disease, associatedwith extensive portosystemic collateral circulation. Difficulty inwalkingdue to stiffness andweakness of the lower limbs, limping gait, and drag-ging of the feet, along with loss of proprioception and vibratory sensesin the territory of the posterior column,may be observed. Asymmetricalsymptomsmay characterize the initial phases, but both legs are severelyaffected in the overt disease stage. Patients develop progressive puremotor spastic paraparesis without or with minimal involvement of theupper extremities and without sensory, bladder or bowel disturbances.Neurologic examination usually reveals normal sensory findings, hyper-active muscle stretch reflex of the lower extremities, muscle rigiditywith normal muscle power, no evident muscle atrophy, and extensorplantar responses. Although the symptoms of spinal cord injury do notparallel the mutable symptoms of HE, some similarities between HMand HE can be found, such as the coexistence of severe porto-systemicshunting, common cerebral and spinal MRI abnormalities, and variablemotor deficits at the lower extremities [118]. Sensorial involvement orsphincteric impairment is uncommon, as well as muscular atrophy.The disease mostly affects men, and in the severe forms it rapidly pro-gresses until confining them to awheelchair. Because axonal loss occursin the advanced stage of HM, an early diagnosis, at the time of initial de-myelination of the spinal cord, is mandatory to include the candidate onthe liver transplant list. Diagnosis of HM remains difficult and may bebased on the exclusion of other causes of spastic paraparesis. Problemsin diagnosis are associated with often coexisting HE, which may alsopresent with movement disorders. MRI spinal cord abnormalities andmotor-evoked potential (MEP) alterations may be suggestive of ad-vanced HM. An early assessment of the central motor conduction timewith MEP studies (more sensitive), while on the transplant waitinglist may be helpful for an early diagnosis.

201P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
Abnormal MRI signal alterations of the brain corticospinal tract withFLAIR images have also been reported in HM, emphasizing the possibleinvolvement of lesions beyond the spinal cord [118,119].
Various disorders must be considered in the differential diagnosis,including neurodegenerative amyotrophiclateral sclerosis, multiplesclerosis, hereditary spastic paraplegia, paraneoplastic syndromes,demyelination syndromes, such as neuromyelitis optica, toxicmyelopa-thy, radiation myelopathy, and spinal cord damage caused by compres-sion or vascular disease [110]. Treatment strategies commonly adoptedto reverse HE, such as reducing ammonia production and nitrogen ab-sorption, and administration of benzodiazepine receptor antagonists,have demonstrated little benefit in patients with HM [118]. Other mea-sures have included limitation of the intake of protein in the diet, largedoses of B group vitamins, neurotrophic drugs, oral neomycin, lactulose,xifaxan, gabapentin, and pentoxifylline, control of enteric bacteriagrowth, and colonic exclusion [120–122].
All these procedures have failed to produce significant improvementas spastic paraparesis seems to be refractory to medical treatment, andworsen even when encephalopathy is effectively averted. Occlusion oflarge splenorenal shunt using endovascular interventional procedureshas also been reported as an effective alternative therapeutic option,however, an impaired gait and a progressive worsened mobility wereobserved in the long term course [123]. OLT should be considered thefirst therapeutic option and the only approach to prevent disease pro-gression; therefore, an early diagnosis of HMand exclusion of other sim-ilar syndromes are fundamental for transplant list prioritization,because OLT may improve and reverse the neurological motor deficitand prognosis only when performed on a timely basis [118,124]. Theearly stage of the disease, in fact, only involves demyelination of the spi-nal cord,while at the advanced stage, the benefit fromOLT isminimal orabsent due to the occurrence of permanent axonal loss. Clinical and neu-roimaging improvements are the successful consequences of an expe-dited OLT. However, despite the awareness of positive neurologicaloutcomes achieved by early OLT, liver transplant candidates with evi-dent HMand lowMELD are not automatically prioritized on thewaitinglist. The first report on prioritization for transplantation with consider-ation of HM as an MELD exception was published by Caldwell et al. in2010 [118]. The authors were able to accomplish expedited OLT with agood neurological outcome after the granting of MELD exception pointsfor HM and upgrading MELD every three months. Waiting for a highMELDmay lead to possible worsening of HM, thus diminishing the like-lihood of both clinical and electrophysiological recovery following thetransplant procedure.
8. Osmotic demyelination syndrome
Patients with chronic liver failure are at increased risk of chronic se-vere hyponatremia because of pseudo-hyponatremia, hypovolemia,“beer” potomania syndrome in alcohol-addicted patients, malnutrition,prolonged diuretic use, and cerebral salt wasting syndrome [125]. Cere-bral edema and neurologic symptoms can arise due towatermovementinto the brain caused by hypotonic hyponatremia, but usually cerebraladaptation with lowering of the cerebral volume reduces the likelihoodof these complications. Central pontine and extrapontine myelinolysis,also called osmotic demyelination syndrome (ODS), is more commonin patients with alcohol-related chronic liver disease, and most of thecases are associated with overly rapid correction of chronichyponatremia. Rapid and large increases in serum sodium levels makethe pontine and extrapontine structures extremely vulnerable to injuryinduced by increased osmolarity. A similar mechanism, i.e. overtreat-ment of chronic hyponatremia in the presence of decreased organicosmolytes, is also involved in the development of central pontinemyelinolysis after liver transplantation [126]. The osmotic effects inthe setting of rapid correction of sodium levels particularly harm the ol-igodendrocytes, which constitute the myelin sheaths [127,128]. Sym-metrical myelin damage characterized by splitting, vacuolization, and
rupture of myelin sheaths, may affect all of the fiber tracts, with sub-stantial axonal damage. Moreover, concomitant significant deficits inorganic osmolytes, which are a common condition of alcoholic andmal-nourished patients, place oligodendrocytes at a high risk for cell shrink-age, permanent inflammatory infiltrates, and axonal demyelination[129]. Although demyelination prevalently occurs in the central pontinestructures (Fig. 2), it also affects some extrapontine regions, includingthe midbrain, thalamus, basal ganglia nuclei, and cerebellum, in atleast 10% of patients (Fig. 3). ODS, rather than central pontinemyelinolysis, more appropriately refers to demyelination in extrapontineregions after the correction of hyponatremia [127,130]. Clinical manifes-tations of central pontine myelinolysis include an enormous variety ofsymptoms, such as head andneckweakness, lethargy, confusion, seizures,dysarthria, dysphagia, vertical ophthalmoparesis, initialflaccidquadriparesis,rapidly evolving paraparesis or quadriparesis (usually symmetrical),delirium and coma. Neurological disorders may vary from minimalsymptoms to a full “locked in” syndrome, with paralysis of the lowercranial nerves and limb muscles, vertical eye movement reduction,and intact alertness and breathing ability [131]. Due to the sometimesnon-specific or minor signs, extrapontine myelinolysis may be under-recognized. The most common manifestations of extrapontinemyelinolysis may include tremor, abnormal movement disorders withchoreoathetosis, catatonia–dystonia, ataxia, myoclonic jerks, perma-nent parkinsonism and mutism [131]. Central pontine myelinolysis,which develops during postoperative recovery from liver transplanta-tion surgery, may initially manifest with confusion and/or weaknessor other symptoms similar to peripheral neuropathy, muscle diseaseor critical illness neuromyopathy [132]. Neurological examinationshould detect the severity of the ODS and the involvement of the ponsor adjacent brainstem areas or more distal supratentorial structures.Pseudobulbar palsy, spastic quadriplegia, and involvement of uppermotor neurons or the corticospinal tracts are characteristic findings,with variable limbweakness, increased limb tone, hyperactive reflexes,and the Babinski sign. Sensory function abnormalities are quite rare.
Abnormalities of brainstem-evoked potentials may be present, anddiffuse bihemispheric slowing may be observed on EEG. However, theclassical symmetric demyelination in the pons is only detected withbrain MRI, which can also demonstrate extrapontine myelinolysis(Figs. 2 and 3). On MRI, hyperintense lesions caused by relatively in-creased water content, without contrast enhancement, are visible onT2 images, while on T1 sequences they are detected as hypointense le-sions. Osmotic myelinolysis is often characterized by concomitant in-volvement of the basal ganglia and pons, the latter with a typicaltrident-shaped hyperintense signal in the central part with sparing ofthe ventrolateral pons and descending corticospinal tracts on T2-weighted or FLAIRM images [13]. However, a consistent drawback ofbrain MRI is that myelinolysis may become clearly positive only 25–30 days after disease onset (initially negative). DWI imaging has theability to detect lesions not yet detectable on T2, thus allowing for anearlier diagnosis [133]. Prevention of either the occurrence of severehyponatremia or the overly rapid rate of correction of the serum sodiumis fundamental for preventing ODS. Patients with signs and symptomsconsistent with ODS typically require ICU admission, with supportivetherapies aiming at potentially re-lowering their serum sodium andpreventing any deleterious neurological and systemic manifestationsof the disease. The approach to re-lowering serum sodium is the samein patients who have exceeded correction limits but who have not yetdeveloped manifestations of ODS. The optimal strategy to reversehypernatremia is still unclear, and the efficacy and safety unknown. Ad-ministration of hypotonic fluids, prevention of development of a waterdiuresis (i.e., urine osmolality less than 200 mosmol/kg), maintenanceof stimuli to increase antidiuretic hormone release, general supportivemeasures, and extracorporeal treatments are among the conventionallyrecognized measures for the hypernatremia-induced ODS. Quick re-lowering of sodium (within four hours of symptoms) has been associat-ed with better outcomes in animal models; in humans no conclusive
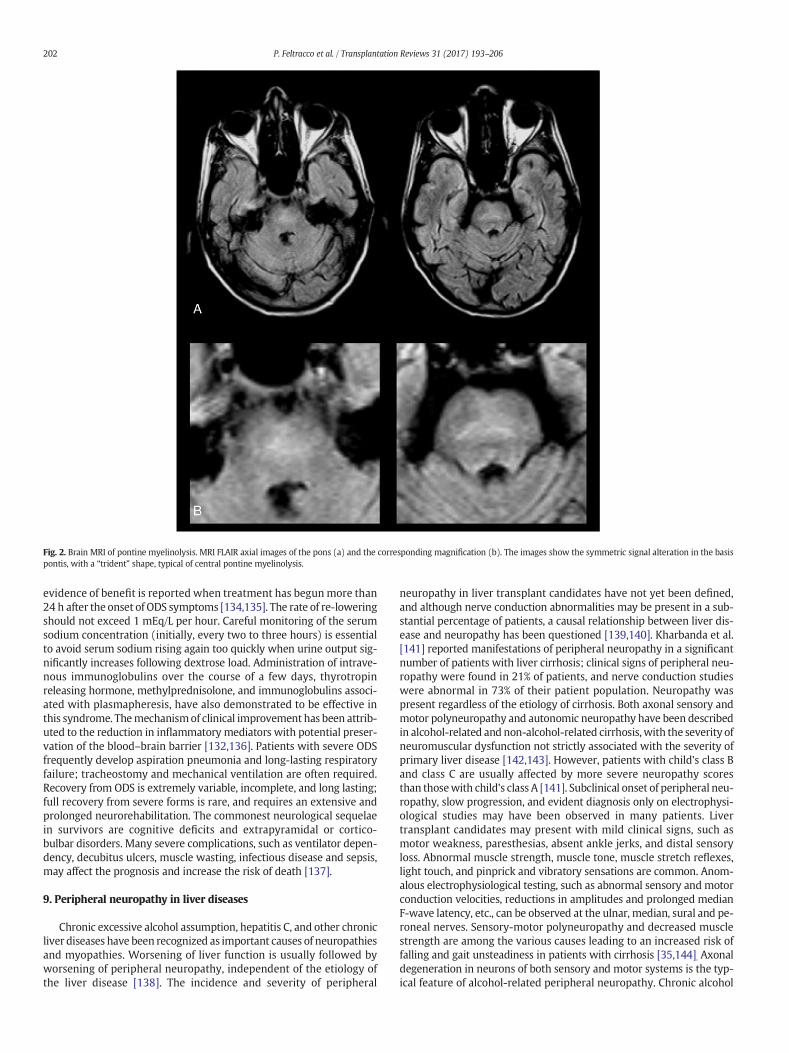
Fig. 2. Brain MRI of pontine myelinolysis. MRI FLAIR axial images of the pons (a) and the corresponding magnification (b). The images show the symmetric signal alteration in the basispontis, with a “trident” shape, typical of central pontine myelinolysis.
202 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
evidence of benefit is reported when treatment has begunmore than24 h after the onset of ODS symptoms [134,135]. The rate of re-loweringshould not exceed 1 mEq/L per hour. Careful monitoring of the serumsodium concentration (initially, every two to three hours) is essentialto avoid serum sodium rising again too quickly when urine output sig-nificantly increases following dextrose load. Administration of intrave-nous immunoglobulins over the course of a few days, thyrotropinreleasing hormone, methylprednisolone, and immunoglobulins associ-ated with plasmapheresis, have also demonstrated to be effective inthis syndrome. Themechanismof clinical improvement has been attrib-uted to the reduction in inflammatory mediators with potential preser-vation of the blood–brain barrier [132,136]. Patients with severe ODSfrequently develop aspiration pneumonia and long-lasting respiratoryfailure; tracheostomy and mechanical ventilation are often required.Recovery from ODS is extremely variable, incomplete, and long lasting;full recovery from severe forms is rare, and requires an extensive andprolonged neurorehabilitation. The commonest neurological sequelaein survivors are cognitive deficits and extrapyramidal or cortico-bulbar disorders. Many severe complications, such as ventilator depen-dency, decubitus ulcers, muscle wasting, infectious disease and sepsis,may affect the prognosis and increase the risk of death [137].
9. Peripheral neuropathy in liver diseases
Chronic excessive alcohol assumption, hepatitis C, and other chronicliver diseases have been recognized as important causes of neuropathiesand myopathies. Worsening of liver function is usually followed byworsening of peripheral neuropathy, independent of the etiology ofthe liver disease [138]. The incidence and severity of peripheral
neuropathy in liver transplant candidates have not yet been defined,and although nerve conduction abnormalities may be present in a sub-stantial percentage of patients, a causal relationship between liver dis-ease and neuropathy has been questioned [139,140]. Kharbanda et al.[141] reported manifestations of peripheral neuropathy in a significantnumber of patients with liver cirrhosis; clinical signs of peripheral neu-ropathy were found in 21% of patients, and nerve conduction studieswere abnormal in 73% of their patient population. Neuropathy waspresent regardless of the etiology of cirrhosis. Both axonal sensory andmotor polyneuropathy and autonomic neuropathy have been describedin alcohol-related and non-alcohol-related cirrhosis, with the severity ofneuromuscular dysfunction not strictly associated with the severity ofprimary liver disease [142,143]. However, patients with child's class Band class C are usually affected by more severe neuropathy scoresthan thosewith child's class A [141]. Subclinical onset of peripheral neu-ropathy, slow progression, and evident diagnosis only on electrophysi-ological studies may have been observed in many patients. Livertransplant candidates may present with mild clinical signs, such asmotor weakness, paresthesias, absent ankle jerks, and distal sensoryloss. Abnormal muscle strength, muscle tone, muscle stretch reflexes,light touch, and pinprick and vibratory sensations are common. Anom-alous electrophysiological testing, such as abnormal sensory and motorconduction velocities, reductions in amplitudes and prolonged medianF-wave latency, etc., can be observed at the ulnar, median, sural and pe-roneal nerves. Sensory-motor polyneuropathy and decreased musclestrength are among the various causes leading to an increased risk offalling and gait unsteadiness in patients with cirrhosis [35,144]. Axonaldegeneration in neurons of both sensory and motor systems is the typ-ical feature of alcohol-related peripheral neuropathy. Chronic alcohol

Fig. 3. Brain MRI of extrapontine myelinolysis. Brain MRI: coronal (a,b) and axial (c,d) T2-weighted images showing symmetric hyperintense lesions at the level of the cerebral peduncleand centrum midollare (open arrowheads) and at the level of the pallidum (gray arrow heads) and putamen (short arrows) consistent with extrapontine myelinolysis.
203P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
abuse, vitamin deficiencies, malnutrition, and “neurotoxins” are knownto contribute to alcoholic polyneuropathy [145]. Patients with alcohol-related polyneuropathy experience pain and motor weakness in thefeet, toes, and distal lower extremities and subsequently in other partsof the body; multiple peripheral nerves are damaged. Axonal degenera-tion often begins before clinical manifestations, which usually presentwith a gradual onset over months or even years [146]. Sensory symp-toms, such as paresthesias, dysesthesias, and weakness, generally ap-pear prior to motor symptoms, and over time, the symptoms progresstoward more proximal parts of the limbs. Symptoms develop symmet-rically; the legs are usually affected first, followed by the arms and thehands (stocking-and-glove pattern of sensory disturbances) [147].Mus-cle cramps, along with a burning sensation in the feet and calves, arevery common. Painful sensations in the arms and legsmay become con-stant (“pins and needles,”), sharp, or lancinating in some individuals.Motor deficits, such as weakness, muscle spasm, muscle atrophy, gaitataxia, erectile dysfunction, etc., may follow the sensory deficits, butthey are sometimes evident at initial presentation. At neurological ex-amination, the typical findings of alcohol-related polyneuropathy maybe detected in the presence of classical systemic manifestations ofchronic liver insufficiency; they include reduced sensation to vibrationin a “stocking-to-glove” distribution, muscle wasting in the lower ex-tremities, decrease in motor power, reduced deep tendon reflexes, ab-normalities of the gastrocnemius-soleus reflexes, reduced ankle/toedorsiflexion, thermic and proprioceptive disorders, and a variable de-gree of gait ataxia. Accurate medical workup, various laboratory tests,neuroimaging investigations, and nerve conduction studies may beneeded to exclude other causes of similar clinical syndromes, such as
diabetic neuropathy, lumbosacral plexopathy, amyotrophic lateral scle-rosis, peripheral and central nervous system diseases caused by vitamindeficits, and Guillain-Barre syndrome. Treatment options for peripheralneuropathy will depend on the type of symptoms that the individual isexperiencing. Avoidance of alcohol intake is the most important step intreating alcohol induced peripheral neuropathy. Correction of malnutri-tion, and in particular supplementation of B group vitamins and vitaminE are essential for the recovery of the glial and neuronal cells. Analgesics,antidepressants and antiepileptic drugs seem to help with dealing withthe discomfort and pain associated with peripheral neuropathy. The ef-ficacy of OLT on reversing peripheral and autonomic neuropathies asso-ciated with severe chronic liver disease has not been studiedextensively. Despite the paucity of literature clear benefits and signifi-cant improvement of muscle strength and other clinical signs havebeen reported following OLT in various case reports and small case se-ries. Abnormalities associated with the distal sensorimotor neuropathyand slowing of sensory nerve conduction velocities in the un-myelinated small axons resolved almost completely following success-ful transplant procedures [148–150]. Gane et al. [150] stated that pe-ripheral neuropathy in a patient with alcoholic cirrhosis is reversibleand should not constitute a contraindication toOLT, evenwhen the neu-ropathy is disabling.
10. Conclusion
People undergoing a liver transplant may often display abnormalneurologic examinations suggestive of HE or othermetabolic, toxic, vas-cular, or degenerative brain disorders associated with end stage liver

204 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
disease. A history of preoperative neurological complications has beenrecognized as an important factor predictive of post-transplant CNSand peripheral nerve dysfunction [4]. In addition, latent subclinical neu-rologic disturbances may postoperatively manifest or worsen as a con-sequence of various perioperative situations, such as hypotension,hypovolemia, surgical stress, hemorrhage, hypoxia, graft dysfunction,and the use of sedative or immunosuppressive drugs. A detailed neuro-logical assessment is among the various investigations that are usefulfor ensuring the feasibility of transplant, and all liver transplant candi-dates should undergo neurological examination before they are accept-ed on the waiting list for OLT. Preoperative consultation is essential toevaluate the extent of patient comorbidities, to recognize and differen-tiate subtle mental and motor abnormalities, to remove any potentiallyneurotoxic drugs, and to establish the best individualized option formedical management.
Conflict of interest statement
Each author has no financial interests or connections, direct or indi-rect, or other situations thatmight raise the question of bias in theworkreported or the conclusions.
References
[1] Ferro JM, Oliveira S. Neurologic manifestations of gastrointestinal and liver dis-eases. Curr Neurol Neurosci Rep 2014;14:487–93.
[2] Ardizzone G, Arrigo A, Schellino MM, et al. Neurological complications of liver cir-rhosis and orthotopic liver transplant. Transplant Proc 2006;38:789–92.
[3] Lewis M, Howdle PD. The neurology of liver failure. QJM 2003;96:623–33.[4] Dhar R, Young GB, Marotta P. Perioperative neurological complications after liver
transplantation are best predicted by pre-transplant hepatic encephalopathy.Neurocrit Care 2008;8:253–8.
[5] Zivković SA, Eidelman BH, Bond G, et al. The clinical spectrum of neurologic disor-ders after intestinal and multivisceral transplantation. Clin Transpl 2010;24:164–8.
[6] Wright AJ, Fishman JA. Central nervous system syndromes in solid organ transplantrecipients. Clin Infect Dis 2014;59:1001–11.
[7] Buis CI, Wiesner RH, Krom RA, Kremers WK, Wijdicks EF. Acute confusional statefollowing liver transplantation for alcoholic liver disease. Neurology 2002;59:601–5.
[8] Montoliu C, Llansola M, Vincente Felipo. Neuroinflammation and neurological al-terations in chronic liver disease. Neuroimmunol Neuroinflammation 2015;2:138–44.
[9] Heidelbaugh JJ, Bruderly M. Cirrhosis and chronic liver failure: part I. Diagnosis andevaluation. Am Fam Physician 2006;74:756–62.
[10] Koo JE, Lim YS, Myung SJ, et al. Hepatic myelopathy as a presenting neurologicalcomplication in patients with cirrhosis and spontaneous splenorenal shunt. KoreanJ Hepatol 2008;14:89–96.
[11] Geibprasert S, Gallucci M, Krings T. Alcohol-induced changes in the brain asassessed by MRI and CT. Eur Radiol 2010;20:1492–501.
[12] Butterworth RF. Parkinsonism in cirrhosis: pathogenesis and current therapeuticoptions. Metab Brain Dis 2013;28:261–7.
[13] Sureka B, Bansal K, Patidar Y, et al. Neurologic manifestations of chronic liver dis-ease and liver cirrhosis. Curr Probl Diagn Radiol 2015;44:449–61.
[14] Córdoba J. New assessment of hepatic encephalopathy. J Hepatol 2011;54:1030–40.
[15] Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease:2014 practice guideline by the American Association for the Study of Liver Diseasesand the European Association for the Study of the liver. Hepatology 2014;60:715–35.
[16] Allampati S, Mullen K. Nomenclature and definition of hepatic encephalopathy —an update. Clin Liver Dis 2015;5:68–70.
[17] McPhail MJ, Bajaj JS, Thomas HC, Taylor-Robinson SD. Pathogenesis and diagnosisof hepatic encephalopathy. Expert Rev Gastroenterol Hepatol 2010;4:365–78.
[18] Cordoba J. Hepatic encephalopathy: from the pathogenesis to the new treatments.ISRN Hepatol 2014;4:236–68.
[19] Lee WM. Acute liver failure. Semin Respir Crit Care Med 2012;33:36–45.[20] Bernal W, Wendon J. Acute liver failure. N Engl J Med 2013;369:2525–34.[21] Shawcross DL, Wendon JA. The neurological manifestations of acute liver failure.
Neurochem Int 2012;60:662–71. http://dx.doi.org/10.1016/j.neuint.2011.10.006[PMID: 22067133].
[22] Datar S, Wijdicks EF. Neurologic manifestations of acute liver failure. Handb ClinNeurol 2014;120:645–59.
[23] Scott TR, Kronsten VT, Hughes RD, Shawcross DL. Pathophysiology of cerebral oe-dema in acute liver failure. World J Gastroenterol 2013;19:9240–55.
[24] O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis infulminant hepatic failure. Gastroenterology 1989;97:439–45.
[25] Mendizabal M, Silva MO. Liver transplantation in acute liver failure: a challengingscenario. World J Gastroenterol 2016;22:1523–31.
[26] Freeman Jr RB, Steffick DE, Guidinger MK, et al. Liver and intestine transplantationin the United States, 1997-2006. Am J Transplant 2008;8:958–76.
[27] Germani G, Theocharidou E, Adam R, et al. Liver transplantation for acute liver fail-ure in Europe: outcomes over 20 years from the ELTR database. J Hepatol 2012;57:288–96.
[28] Romero-GómezM, Montagnese S, Jalan R. Hepatic encephalopathy in patients withacute decompensation of cirrhosis and acute-on-chronic liver failure. J Hepatol2015;62:437–47.
[29] Romero-GómezM. Role of phosphate-activated glutaminase in the pathogenesis ofhepatic encephalopathy. Metab Brain Dis 2005;20:319–25.
[30] Cauli O, Rodrigo R, Llansola M, et al. Glutamatergic and gabaergic neurotransmissionand neuronal circuits in hepatic encephalopathy. Metab Brain Dis 2009;24:69–80.
[31] Monfort P, Cauli O, Montoliu C, et al. Mechanisms of cognitive alterations inhyperammonemia and hepatic encephalopathy: therapeutical implications.Neurochem Int 2009;55:106–12.
[32] Cagnin A, Taylor-Robinson SD, Forton DM, Banati RB. In vivo imaging of cerebral"peripheral benzodiazepine binding sites" in patients with hepatic encephalopa-thy. Gut 2006;55:547–53.
[33] Rodrigo R, Cauli O, Gomez-Pinedo U, et al. Hyperammonemia induces neuroinflam-mation that contributes to cognitive impairment in rats with hepatic encephalop-athy. Gastroenterology 2010;139:675–84.
[34] Wright GA, Sharifi Y, Newman TA, et al. Characterisation of temporal microglia andastrocyte immune responses in bile duct-ligated rat models of cirrhosis. Liver Int2014;34:1184–91.
[35] Gómez-Ansón B, Román E, Fernández de Bobadilla R, et al. Alterations in cerebralwhite matter and neuropsychology in patients with cirrhosis and falls. PLoS One2015;10:e0118930.
[36] Guevara M, Baccaro ME, Gómez-Ansón B, et al. Cerebral magnetic resonance imag-ing reveals marked abnormalities of brain tissue density in patients with cirrhosiswithout overt hepatic encephalopathy. J Hepatol 2011;55:564–73.
[37] Timmermann L, Gross J, Butz M, et al. Mini-asterixis in hepatic encephalopathy in-duced by pathologic thalamo-motor-cortical coupling. Neurology 2003;61:689–92.
[38] Cadranel JF, Lebiez E, DiMartino V, et al. Focal neurological signs in hepatic enceph-alopathy in cirrhotic patients: an underestimated entity? Am J Gastroenterol 2001;96:515–8.
[39] Miyata Y, Motomura S, Tsuji Y, Koga S. Hepatic encephalopathy and reversible cor-tical blindness. Am J Gastroenterol 1988;83:780–2.
[40] Eckstein AK, Reichenbach A, Jacobi P, Weber P, Gregor M, Zrenner E. Hepaticretinopathia. Changes in retinal function. Vision Res 1997;37:1699–706.
[41] Ortiz M, Jacas C, Córdoba J. Minimal hepatic encephalopathy: diagnosis, clinical sig-nificance and recommendations. J Hepatol 2005;42(Suppl. 1):S45–53.
[42] Román E, Córdoba J, Torrens M, Guarner C, Soriano G. Falls and cognitive dysfunc-tion impair health-related quality of life in patients with cirrhosis. Eur JGastroenterol Hepatol 2013;25:77–84.
[43] Montagnese S, Merkel C, Amodio P. Encephalopathy or hepatic encephalopathy? JHepatol 2012;57:928–9.
[44] Van der Rijt CC, Schalm SW, De Groot GH, De Vlieger M. Objective measurement ofhepatic encephalopathy by means of automated EEG analysis. ElectroencephalogrClin Neurophysiol 1984;57:423–6.
[45] Montagnese S, Balistreri E, Schiff S, et al. Covert hepatic encephalopathy: agree-ment and predictive validity of different indices. World J Gastroenterol 2014;20:15756–62.
[46] Weissenborn K, Scholz M, Hinrichs H, et al. Neurophysiological assessment of earlyhepatic encephalopathy. Electroencephalogr Clin Neurophysiol 1990;75:289–95.
[47] Schiff S, Casa M, Di Caro V, et al. A low-cost, user-friendly electroencephalographicrecording system for the assessment of hepatic encephalopathy. Hepatology 2016;63:1651–9.
[48] Rovira A, Alonso J, Córdoba J. MR imaging findings in hepatic encephalopathy. AJNRAm J Neuroradiol 2008;29:1612–21.
[49] Alonso J, Córdoba J, Rovira A. Brain magnetic resonance in hepatic encephalopathy.Semin Ultrasound CT MR 2014;35:136–52.
[50] Dasarathy S, Mullen KD. Hepatic encephalopathy. Curr Treat Options Gastroenterol2001;4:517–26.
[51] Sheasgreen C, Lu L, Patel A. Pathophysiology, diagnosis, and management of hepat-ic encephalopathy. Inflammopharmacology 2014;22:319–26.
[52] Bajaj JS. Review article: the modern management of hepatic encephalopathy. Ali-ment Pharmacol Ther 2010;31:537–47.
[53] Amodio P, Bemeur C, Butterworth R, et al. The nutritional management of hepaticencephalopathy in patients with cirrhosis: International Society for Hepatic En-cephalopathy and Nitrogen Metabolism Consensus. Hepatology 2013;58:325–36.
[54] Chalasani N, Gitlin N. Severe recurrent hepatic encephalopathy that responded tooral branched chain amino acids. Am J Gastroenterol 1996;91:1266–8.
[55] Liu Q, Duan ZP, Ha DK, Bengmark S, Kurtovic J, Riordan SM. Synbiotic modulation ofgut flora: effect on minimal hepatic encephalopathy in patients with cirrhosis.Hepatology 2004;39:1441–9.
[56] Williams R, James OF,Warnes TW,MorganMY. Evaluation of the efficacy and safetyof rifaximin in the treatment of hepatic encephalopathy: a double-blind, random-ized, dose-finding multi-centre study. Eur J Gastroenterol Hepatol 2000;12:203–8.
[57] Rose C, Jalan R. Is minimal hepatic encephalopathy completely reversible followingliver transplantation? Liver Transpl 2004;10:84–7.
[58] Sotil EU, Gottstein J, Ayala E, Randolph C, Blei AT. Impact of preoperative overt he-patic encephalopathy on neurocognitive function after liver transplantation. LiverTranspl 2009;15:184–92.
[59] Campagna F, Montagnese S, Schiff S, et al. Cognitive impairment and electroen-cephalographic alterations before and after liver transplantation: what is revers-ible? Liver Transpl 2014;20:977–86.

205P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
[60] Bajaj JS, Schubert CM, Heuman DM, et al. Persistence of cognitive impairment afterresolution of overt hepatic encephalopathy. Gastroenterology 2010;138:2332–40.
[61] Dalvi A, Padmanaban M. Wilson's disease: etiology, diagnosis, and treatment. DisMon 2014;60:450–9.
[62] Das Shyamal K, Ray Kunal. Wilson's disease: an update. Nat Clin Pract Neurol 2006;2:482–93.
[63] Merle U, Schaefer M, Ferenci P, Stremmel W. Clinical presentation, diagnosis andlong-term outcome of Wilson's disease: a cohort study. Gut 2007;56:115–20.
[64] Akil M, Brewer GJ. Psychiatric and behavioral abnormalities in Wilson's disease.Adv Neurol 1995;65:171–8.
[65] Lorincz MT. Neurologic Wilson's disease. Ann N Y Acad Sci 2010;184:173–87.[66] Machado A, Chien HF, Deguti MM, et al. Neurological manifestations in Wilson's
disease: report of 119 cases. Mov Disord 2006;21:2192–6.[67] Starosta-Rubinstein S, Young AB, Kluin K, et al. Clinical assessment of 31 patients
with Wilson's disease. Correlations with structural changes on magnetic resonanceimaging. Arch Neurol 1987;44:365–70.
[68] Meenakshi-Sundaram S, Mahadevan A, Taly AB, Arunodaya GR, Swamy HS,Shankar SK. Wilson's disease: a clinico-neuropathological autopsy study. J ClinNeurosci 2008;15:409–17.
[69] Shivakumar R, Thomas SV. Teaching NeuroImages: face of the giant panda and hercub: MRI correlates of Wilson disease. Neurology 2009;72:e50–1.
[70] Soltanzadeh A, Soltanzadeh P, Nafissi S, et al. Wilson's disease: a great masquerad-er. Eur Neurol 2007;57:80–5.
[71] Członkowska A, Tomasz Litwin T. Treatment of Wilson's disease – another point ofview. Expert Opin Orphan Drugs 2015;3:239–43.
[72] Hui J, TangNL.Wilson's disease: a reviewof treatmentoptionswith a focus on zinc ther-apy. Orphan Drugs Res Rev 2012;2:35–45. http://dx.doi.org/10.2147/ODRR.S33896.
[73] Roberts EA, Schilsky ML, American Association for Study of Liver Diseases (AASLD).Diagnosis and treatment of Wilson disease: an update. Hepatology 2008;47:2089–111.
[74] European Association for Study of Liver. EASL clinical practice guidelines: Wilson'sdisease. J Hepatol 2012;56:671–85.
[75] Medici V, Trevisan CP, D'Inca R, et al. Diagnosis and management of Wilson's dis-ease: results of a single center experience. J Clin Gastroenterol 2006;40:936–41.
[76] Czlonkowska A, Gajda J, RodoM. Effects of long-term treatment inWilson's diseasewith D-penicillamine and zinc sulphate. J Neurol 1996;243:269–73.
[77] Pall HS, Williams AC, Blake DR. Deterioration ofWilson's disease following the startof penicillamine therapy. Arch Neurol 1989;46:359.
[78] Catana AM, Medici V. Liver transplantation for Wilson disease. World J Hepatol2012;27:5–10.
[79] Mocchegiani F, Gemini S, Vincenzi P, et al. Liver transplantation in neurologicalWilson's disease: is there indication? A case report. Transplant Proc 2014;46:2360–4.
[80] Wang XH, Zhang F, Li XC, et al. Eighteen living related liver transplants for Wilson'sdisease: a single-center. Transplant Proc 2004;36:2243–5.
[81] Medici V, Mirante VG, Fassati LR, et al. Monotematica AISF 2000 OLT study group.Liver transplantation forWilson's disease: the burden of neurological and psychiat-ric disorders. Liver Transpl 2005;11:1056–63.
[82] Sutcliffe RP,MaguireDD,Muiesan P, et al. Liver transplantation forWilson's disease:long-term results and quality-of-life assessment. Transplantation 2003;75:1003–6.
[83] Lui CC, Chen CL, Cheng YF, Lee TY. Recovery of neurological deficits in a case ofWilson's disease after liver transplantation. Transplant Proc 1998;30:3324–5.
[84] Cheng F, Li GQ, Zhang F, et al. Outcomes of living-related liver transplantation forWilson's disease: a single-center experience in China. Transplantation 2009;87:751–7. http://dx.doi.org/10.1097/TP.0b013e318198a46e.
[85] Guillaud O, Dumortier J, Sobesky R, et al. Long term results of liver transplantationfor Wilson's disease: experience in France. J Hepatol 2014;60:579–89. http://dx.doi.org/10.1016/j.jhep.2013.10.025.
[86] Członkowska A, Tarnacka B, Möller JC, et al. UnifiedWilson's disease rating scale - aproposal for the neurological scoring ofWilson's disease patients. Neurol NeurochirPol 2007;41:1–12.
[87] Nagappa M, Sinha S, Saini JS, et al. Non-Wilsonian hepatolenticular degeneration:clinical and MRI observations in four families from South India. J Clin Neurosci2016;27:91–4.
[88] Tryc AB, Goldbecker A, Berding G, et al. Cirrhosis-related parkinsonism: prevalence,mechanisms and response to treatments. J Hepatol 2013;58:698–705.
[89] Nagano-Saito A, Kato T, Arahata Y, et al. Cognitive- and motor-related regions inParkinson's disease: FDOPA and FDG PET studies. Neuroimage 2004;22:553–61.
[90] Burkhard PR, Delavelle J, Du Pasquier R, Spahr L. Chronic parkinsonism associatedwith cirrhosis: a distinct subset of acquired hepatocerebral degeneration. ArchNeurol 2003;60:521–8.
[91] Rose C, Butterworth RF, Zayed J, et al. Manganese deposition in basal ganglia struc-tures results from both portal-systemic shunting and liver dysfunction. Gastroen-terology 1999;117:640–4.
[92] Lee J, Lacomis D, Comu S, et al. Acquired hepatocerebral degeneration: MR andpathologic findings. AJNR Am J Neuroradiol 1998;19:485–7.
[93] Romeiro FG, Américo MF, Yamashiro FS, et al. Acquired hepatocerebral degenera-tion and hepatic encephalopathy: correlations and variety of clinical presentationsin overt and subclinical liver disease. Arq Neuropsiquiatr 2011;69:496–501.
[94] Butterworth RF, Spahr L, Fontaine S, Layrargues GP. Manganese toxicity, dopami-nergic dysfunction and hepatic encephalopathy. Metab Brain Dis 1995;10:259–67.
[95] Fischer JE, Baldessarini RJ. False neurotransmitters and hepatic failure. Lancet 1971;2:75–80.
[96] Inoue E, Hori S, Narumi Y, et al. Portal-systemic encephalopathy: presence of basalganglia lesions with high signal intensity on MR images. Radiology 1991;179:551–5.
[97] Stebbins GT, Goetz CG. Factor structure of the unified Parkinson's disease ratingscale: motor examination section. Mov Disord 1998;13:633–6.
[98] Trouillas P, Takayanagi T, Hallett M, et al. International cooperative ataxia ratingscale for pharmacological assessment of the cerebellar syndrome. The ataxia neu-ropharmacology Committee of the World Federation of neurology. J Neurol Sci1997;145:205–11.
[99] Shulman LM, Minagar A, Weiner WJ. Reversal of parkinsonism following livertransplantation. Neurology 2003;60:519.
[100] Stracciari A, Baldin E, Cretella L, et al. Chronic acquired hepatocerebral degenera-tion: effects of liver transplantation on neurological manifestations. Neurol Sci2011;32:411–5.
[101] Lazeyras F, Spahr L, DuPasquier R, et al. Persistence of mild parkinsonism 4monthsafter liver transplantation in patients with preoperative minimal hepatic encepha-lopathy: a study on neuroradiological and blood manganese changes. Transpl Int2002;15:188–95.
[102] Spahr L, Vingerhoets F, Lazeyras F, et al. Magnetic resonance imaging and protonspectroscopic alterations correlate with parkinsonian signs in patients with cirrho-sis. Gastroenterology 2000;119:774–81.
[103] Klos KJ, Ahlskog JE, Josephs KA, et al. Neurologic spectrum of chronic liver failureand basal ganglia T1 hyperintensity on magnetic resonance imaging: probablemanganese neurotoxicity. Arch Neurol 2005;62:1385–90.
[104] Maffeo E, Montuschi A, Stura G, Giordana MT. Chronic acquired hepatocerebral de-generation, pallidal T1 MRI hyperintensity and manganese in a series of cirrhoticpatients. Neurol Sci 2014;35:523–30.
[105] Van Laere K, Varrone A, Booij J, et al. EANM procedure guidelines for brain neuro-transmission SPECT/PET using dopamine D2 receptor ligands, version 2. Eur J NuclMed Mol Imaging 2010;37:434–42.
[106] Berding G, Brücke T, Odin P, et al. [123I]beta-CIT SPECT imaging of dopamine andserotonin transporters in Parkinson's disease and multiple system atrophy.Nuklearmedizin 2003;42:31–8.
[107] Park HK, Kim SM, Choi CG, et al. Effect of trientine on manganese intoxication in apatient with acquired hepatocerebral degeneration. Mov Disord 2008;23:768–70.
[108] Ueki Y, Isozaki E, Miyazaki Y, et al. Clinical and neuroradiological improvement inchronic acquired hepatocerebral degeneration after branched-chain amino acidtherapy. Acta Neurol Scand 2002;106:113–6.
[109] Fabiani G, Rogacheski E, Wiederkehr JC, et al. Liver transplantation in a patient withrapid onset parkinsonism-dementia complex induced by manganism secondary toliver failure. Arq Neuropsiquiatr 2007;65:685–8.
[110] Pinarbasi B, Kaymakoglu S, Matur Z, et al. Are acquired hepatocerebral degenera-tion and hepatic myelopathy reversible? J Clin Gastroenterol 2009;43:176–81.
[111] Powell EE, Pender MP, Chalk JB, et al. Improvement in chronic hepatocerebral de-generation following liver transplantation. Gastroenterology 1990;98:1079–82.
[112] Roger F. Butterworth parkinsonism in cirrhosis: pathogenesis and current thera-peutic options. Metab Brain Dis 2013;28:261–7.
[113] Servin-Abad L, Tzaki SA, Schiff ER, Regev A. Acquired hepatocerebral degenerationin a patient with HCV cirrhosis: complete resolution with subsequent recurrenceafter liver transplantation. Liver Transpl 2006;12:1161–5.
[114] Cui M, Zhang X,Mu F. Hepatic myelopathy associatedwith advanced liver cirrhosis.Saudi Med J 2012;33:1352–4.
[115] Panicker J, Sinha S, Taly AB, Ravishankar S, Arunodaya GR. Hepatic myelopathy: arare complication following extrahepatic portal vein occlusion and lienorenalshunt. Neurol India 2006;54:298–300.
[116] Conn HO, Rossle M, Levy L, Glocker FX. Portosystemic myelopathy: spasticparaparesis after portosystemic shunting. Scand J Gastroenterol 2006;41:619–25.
[117] Mendoza G, Marti-Fàbregas J, Kulisevsky J, Escartín A. Hepatic myelopathy: a rarecomplication of portacaval shunt. Eur Neurol 1994;34:209–12.
[118] Caldwell C, Werdiger N, Jakab S, et al. Use of model for end-stage liver disease ex-ception points for early liver transplantation and successful reversal of hepatic my-elopathy with a review of the literature. Liver Transpl 2010;16:818–26.
[119] Nardone R, Buratti T, Oliviero A, et al. Corticospinal involvement in patients with aportosystemic shunt due to liver cirrhosis: a MEP study. J Neurol 2006;253:81–5.
[120] Campellone JV, Lacomis D, Giuliani MJ, et al. Hepatic myelopathy. Case report withreview of the literature. Clin Neurol Neurosurg 1996;98:242–6.
[121] QuB, Liu C, Guo L, et al. The role of liver transplantation in the treatment of hepaticmy-elopathy: case report with review of the literature. Transplant Proc 2009;41:1987–9.
[122] Liao H, Yan Z, PengW, Hong H. Hepatic myelopathy: case report and review of theliterature. Liver Res Open J 2015;1:45–55.
[123] Wang MQ, Liu FY, Duan F. Management of surgical splenorenal shunt-related he-patic myelopathy with endovascular interventional techniques. World JGastroenterol 2012;18:7104–8.
[124] Nardone R, Höller Y, Storti M, et al. Spinal cord involvement in patients with cirrho-sis. World J Gastroenterol 2014;20:2578–85.
[125] Liamis GL, Milionis HJ, Rizos EC, et al. Mechanisms of hyponatraemia in alcohol pa-tients. Alcohol Alcohol 2000;35:612–6.
[126] Crivellin C, Cagnin A, Manara R, et al. Risk factors for central pontine andextrapontinemyelinolysis after liver transplantation: a single-center study. Trans-plantation 2015;99:1257–64.
[127] Lien YH, Shapiro JI, Chan L. Study of brain electrolytes and organic osmolytes dur-ing correction of chronic hyponatremia. Implications for the pathogenesis of cen-tral pontinemyelinolysis. J Clin Invest 1991;88:303–9.
[128] Singh TD, Fugate JE, Rabinstein AA. Central pontine and extrapontinemyelinolysis:a systematic review. Eur J Neurol 2014;21:1443–50.
[129] Abbott R, Silber E, Felber J, Ekpo E. Osmotic demyelination syndrome. BMJ 2005;331:829–30.
[130] Brown WD. Osmotic demyelination disorders: central pontine and extrapontinemyelinolysis. Curr Opin Neurol 2000;13:691–7.
[131] Martin RJ. Central pontine and extrapontine myelinolysis: the osmotic demyelin-ation syndromes. J Neurol Neurosurg Psychiatry 2004;75(Suppl. 3):iii22–8.

206 P. Feltracco et al. / Transplantation Reviews 31 (2017) 193–206
[132] Saner FH, KoeppenS,MeyerM, et al. Treatment of central pontinemyelinolysiswith plas-mapheresis and immunoglobulins in liver transplant patient. Transpl Int 2008;21:390–1.
[133] Ruzek KA, Campeau NG, Miller GM. Early diagnosis of central pontinemyelinolysiswith diffusion-weighted imaging. AJNR Am J Neuroradiol 2004;25:210–3.
[134] Oya S, Tsutsumi K, Ueki K, Kirino T. Reinduction of hyponatremia to treat centralpontinemyelinolysis. Neurology 2001;57:1931.
[135] King JD, Rosner MH. Osmotic demyelination syndrome. Am J Med Sci 2010;339:561–7.
[136] Grimaldi D, Cavalleri F, Vallone S, et al. Plasmapheresis improves the outcome ofcentral pontine myelinolysis. J Neurol 2005;252:734–5.
[137] Louis G, Megarbane B, Lavoué S, et al. Long-term outcome of patients hospitalizedin intensive care units with central or extrapontine myelinolysis. Crit Care Med2012;40:970e2.
[138] Chaudhry V, Corse AM, O'Brian R, et al. Autonomic and peripheral (sensorimotor)neuropathy in chronic liver disease: a clinical and electrophysiologic study.Hepatology 1999;29:1698–703.
[139] Asbury A. Hepatic neuropathy. In: Dyck Pj, Thomas Pk, Lambert Eh, editors. Periph-eral neuropathy. 2nd ed. Philadelphia: Saunders; 1984. p. 1826–32.
[140] Asbury A, Dyck PJ, Thomas PH, Lambert EH. Neuropathies with renal failure, hepat-ic disorders chronic renal insufficiency and critical illness. Peripheral neuropathy.3rd ed. Philadelphia: Saunders; 1993. p. 1251–65.
[141] Kharbanda PS, Prabhakar S, Chawla YK, et al. Peripheral neuropathy in liver cirrho-sis. J Gastroenterol Hepatol 2003;18:922–6.
[142] Hendrickse MT, Triger DR. Peripheral and cardiovascular autonomic impairment inchronic liver disease: prevalence and relation to hepatic function. J Hepatol 1992;16:177.
[143] Kempler P, Váradi A, Szalay F. Autonomic neuropathy in liver disease. Lancet 1989;2:1332.
[144] Butterworth RF. Liver: risk of falls in cirrhosis predicted by psychometric testing.Nat Rev Gastroenterol Hepatol 2012;9:197–8.
[145] Mellion M, Gilchrist JM, de la Monte S. Alcohol-related peripheral neuropathy: nu-tritional, toxic, or both? Muscle Nerve 2011;43:309–16.
[146] Koike H, Sobue G. Alcoholic neuropathy. Curr Opin Neurol 2006;19:481–6.[147] Bhidayasiri R, Lisak R. International neurology. Wiley-Blackwell 2016:413–4.[148] McDougall Alan John, Davies Leo, McCaughan Geoffrey William. Rapid improve-
ment of autonomic and peripheral neuropathy after liver transplantation: a singlecase report. Liver Transpl 2002;8:164–6.
[149] Hockerstedt K, Kajaste S, Muuronen A, et al. Encephalopathy and neuropathy inend-stage liver disease before and after liver transplantation. J Hepatol 1992;16:31–7.
[150] Gane E, Bergman R, Hutchinson D. Resolution of alcoholic neuropathy followingliver transplantation. Liver Transpl 2004;10:1545–8.




















