
Medical Consultation for Migraine: Results From the American Migraine Study
Upload
independentCategory
view
0download
0
ORIGINAL ARTICLE
Evidence for a Vascular Factor in Migraine
Mohammad S. Asghar, MD,1 Adam E. Hansen, PhD,2,3 Faisal M. Amin, MD,1
R. J. van der Geest, MS,4 Patrick van der Koning, MS,4 Henrik B. W. Larsson, MD, DMS,2,5
Jes Olesen, MD, DMS,1 and Messoud Ashina, MD, PhD, DMS1
Objective: It has been suggested that migraine is caused by neural dysfunction without involvement ofvasodilatation. Because dismissal of vascular mechanisms seemed premature, we examined diameter of extra- andintracranial vessels in migraine without aura patients.Methods: A novel high-resolution direct magnetic resonance angiography imaging technique was used to measurearterial circumference of the extracranial middle meningeal artery (MMA) and the intracranial middle cerebral artery(MCA). Data were obtained at baseline, during migraine attack, and after treatment with the migraine abortive drugsumatriptan (a 5-hydroxytryptamine agonist).Results: We found dilatation of both MMA and MCA during migraine attack (p ¼ 0.001). Sumatriptan administrationcaused amelioration of headache (p < 0.001) and contraction of MMA (p < 0.001), but MCA remained unchanged (p¼ 0.16). Exploratory analysis revealed that in migraine attacks with half-sided headache, there was only dilatation onthe headache side of MMA of 12.49% (95% confidence interval [CI], 4.16–20.83%) and of MCA of 12.88% (95% CI,3.49–22.27%) and no dilatation on the nonheadache side of MMA (95% CI, �4.27 to 11.53%) and MCA (95% CI,�6.7 to 14.28%). In double-sided headache we found bilateral vasodilatation of both MMA and MCA (p < 0.001).Interpretation: These data show that migraine without aura is associated with dilatation of extra- and intracerebralarteries and that the headache location is associated with the location of the vasodilatation. Furthermore,contraction of extracerebral and not intracerebral arteries is associated with amelioration of headache. Collectively,these data suggest that vasodilatation and perivascular release of vasoactive substances is an integral mechanism ofmigraine pathophysiology.
ANN NEUROL 2011;69:635–645
Migraine is the most prevalent neurological disorder,
with >80 million sufferers in Europe and the
United States.1 It is characterized by recurrent attacks of
severe headache that typically affect the patients in their
most productive years and thereby lead to absenteeism
from work, decreased working efficiency and causing a fi-
nancial loss of 27 billion per year in the European
Union.2 Despite recent advances, the mechanisms under-
lying migraine pain still remain elusive. For >100 years,
the role of vascular and neural mechanisms has been a
topic of intense debate.3 Supported by Wolff ’s long series
of impressive investigations,4 a vascular hypothesis of vas-
odilatation as causative for the migraine pain dominated
migraine research for most of the 20th century.5 More
recently, the neuronal hypothesis has, however, received
increasing support. Based on findings of brainstem acti-
vation,6,7 it was suggested that migraine pain is caused
by abnormal central interpretation of normal sensory
input in the trigeminal sensory system.8 Moreover, a cen-
tral locus of action of antimigraine drugs such as triptans
has been suggested.9 A recent study of nitroglycerin-
induced migraine using magnetic resonance angiography
(MRA) concluded that there was no evidence in the
study or in the literature for dilation of extra- or intrace-
rebral arteries during a migraine attack.10 The authors
requested more human studies to elucidate the issue.11
Convinced that vascular nociception is involved in mi-
graine, we applied a high-resolution 3T MRA to examine
View this article online at wileyonlinelibrary.com. DOI: 10.1002/ana.22292
Received Jul 20, 2010, and in revised form Aug 28, 2010. Accepted for publication Oct 1, 2010.
Address correspondence to Dr Ashina, Danish Headache Center and Department of Neurology, Glostrup Hospital, University of Copenhagen, Faculty
of Health Sciences, Nordre Ringvej 57, DK-2600 Glostrup, Copenhagen, Denmark. E-mail: [email protected]
From the 1Danish Headache Center and Department of Neurology, Glostrup Hospital, Faculty of Health Sciences, University of Copenhagen, Copenhagen,
Denmark; 2Functional Imaging Unit, Glostrup Hospital, Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark; 3Department of
Radiology, Glostrup Hospital, Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark; 4Division of Image Processing, Department of
Radiology, Leiden University Medical Center, Leiden, the Netherlands; and 5Department of Clinical Physiology and Nuclear Medicine, Glostrup Hospital,
Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark.
Additional supporting information can be found in the online version of this article.
VC 2011 American Neurological Association 635

whether dilatation of extra- and/or intracerebral arteries
occurs during migraine. We induced a migraine without
aura attack by infusion of calcitonin gene-related peptide
(CGRP). CGRP is a strong vasodilator12 present in peri-
vascular nerve fibers13 and known to induce migraine
attacks indistinguishable from spontaneous attacks in mi-
graine suffers.14 The latter is supported by the fact that
triggering of migraine is itself a fundamental feature of
the disorder, so that a so-called spontaneous attack, trig-
gered for example by missed sleep or food, is not differ-
entiated in clinical practice. Our hypothesis was that
both intra- and extracerebral arteries would be dilated
during a migraine attack, and in half-sided attacks we
expected to see dilatation on the headache side. In addi-
tion, we examined the effect of the selective antimigraine
drug sumatriptan, a 5-hydroxytryptamine (5-HT1B/D)
agonist, on arterial circumference during migraine
attacks. We hypothesized that sumatriptan would con-
strict arteries in association with pain relief.
Patients and Methods
Experimental DesignTwenty-four patients with migraine without aura received intra-
venous infusion of 1.5lg/min CGRP over 20 minutes (for
inclusion and exclusion criteria, see Supplementary Material).
CGRP infusion induces headache in healthy volunteers,15 and
delayed migraine attacks in patients with migraine without
aura.14 The patients were instructed that during the CGRP
infusion they might develop headache and several hours later a
delayed headache that could have migrainelike features. It was
emphasized that not all develop migraine headache after CGRP
infusion and that completion of the study did not depend on
the development of headache. If a subject developed migraine
she/he would be treated with a 6mg subcutaneous injection of
sumatriptan.
Before start of infusion, we recorded the circumference of
the middle meningeal artery (MMA) and middle cerebral artery
(MCA), blood pressure, pulse, and end tidal CO2. Headache
intensity was recorded on a 0 to 10 verbal rating scale (VRS).
Adverse events (AEs) such as nausea and other sensations relat-
ing to drug side effects were also recorded. After 40 minutes,
the subjects were removed from the magnet, and every 30
minutes headache score (VRS) and AEs were recorded. If sub-
jects developed delayed headache meeting the migraine criteria
(see Migraine Facts Box), they were placed in the magnet again
and new MRA recordings of MMA and MCA circumference
were preformed. The headache was subsequently treated with a
subcutaneous injection of 6mg sumatriptan. Fifteen minutes
later, when sumatriptan had reached its maximal serum concen-
tration, MRA recordings of MMA and MCA circumference
were repeated. If the subjects did not develop delayed headache
or migraine after 7 to 8 hours, MRA recordings of MMA and
MCA were repeated before discharge.
Migraine Facts
Migraine is the most common neurological disorder,
affecting 10% to 15% of the adult population in the
Western world. Prevalence is highest at age 25 to 55
years.1 After dementia and possibly stroke, migraine is
the most costly neurological disorder in the European
community, costing more than €27 billion a year in
direct and indirect costs.2
The diagnostic criteria for migraine without aura
according to the second edition of the International
Headache Classification41:
At least 5 attacks fulfilling the following criteria:
• Headache attacks lasting 4 to 72 hours (untreated or
successfully treated).
Headache has at least two of the following
characteristics:
• Unilateral location.
• Pulsating quality.
• Moderate or severe pain intensity.
• Aggravation by or causing avoidance of routine
physical activity (eg, walking or climbing stairs).
During headache at least 1 of the following:
• Nausea and/or vomiting.
• Photophobia and phonophobia.
• Symptoms not associated with another disorder.
Data Acquisition and Imaging ProtocolsAll subjects reported to the laboratory headache free for at least
5 days. Coffee, tea, cocoa, other methylxanthine-containing
foods or beverages, and tobacco were not allowed for at least
12 hours before start of the study. The subjects were placed in
the supine position in the scanner room, and a venous catheter
(Venflon) was inserted into the left antecubital vein for infu-
sion. Blood samples were collected to determine the baseline
hematocrit value and potassium and sodium levels. The subjects
were monitored for blood oxygen saturation, blood pressure,
and heart rate continuously during the study using a Veris
monitor (Medrad, Warrendale, PA). End-tidal CO2 was moni-
tored by a capnograph (Datex, Helsinki, Finland).
MRAMRA was performed on a 3.0T Philips Achieva Scanner (Phi-
lips Medical Systems, Best, the Netherlands) using an 8-element
phased-array receive head coil.
Using a high-resolution MRA technique, we obtained 2-
dimensional (2D) and 3D images of the extracranial MMA and
the intracranial MCA at baseline, during migraine attacks, and
ANNALS of Neurology
636 Volume 69, No. 4
after administration of sumatriptan. For vessel imaging, a 3D
inflow gradient echo sequence was used. First a scout MRA was
performed using field of view, 180 � 180 � 180mm3; acquired
matrix size (M � P), 180 � 180mm; acquired voxel resolution,
1.0 � 1.0 � 2.4mm3; reconstructed resolution, 0.34 � 0.34 �1.20mm3; repetition time, 23 milliseconds; echo time, 5.4
milliseconds; flip angle, 20�; SENSE factor, 2; 5 chunks, and
total scan duration, 3 minutes and 18 seconds. The scout MRA
was used to plan the subsequent MRA of MCA. MRA of
MCA was performed using field of view, 200 � 200 � 74mm;
acquired matrix size (M � P), 800 � 406; acquired voxel reso-
lution, 0.25 � 0.49 � 1.00mm3; reconstructed resolution, 0.20
� 0.20 � 0.5mm3; repetition time, 25 milliseconds; echo time,
3.5 milliseconds; flip angle, 20�; SENSE factor, 2; 4 chunks;
and total scan time, 9 minutes and 2 second. Angiography of
MMA was done using field of view, 200 � 200 � 16.1mm3;
acquired voxel resolution, 0.25 � 0.35 � 0.70mm3; reconstructed
resolution, 0.2 � 0.2 � 0.35mm3; repetition time, 25 milli-
seconds; echo time, 3.5 milliseconds; flip angle, 20�; SENSE factor,
2; 4 chunks; and total scan duration, 5 minutes and 28 seconds.
MRA Data AnalysisThe angiography data were transferred to a remote worksta-
tion in Dicom format. The MRA data where then analyzed
using the LKEB MRA Vessel wall analysis software from Lei-
den, the Netherlands.16 The reliability of measurements has
already been described and proven to be accurate with high
reproducibility by de Koning et al16 and applied in 2 previous
studies.10,17 The software provides automated contour detec-
tion and quantification of the luminal boundaries in vessel
segments with a minimal user interaction. In the 3D recon-
struction of the MRA data, the MCA was identified marking
the branch from the main trunk of the internal carotid artery.
In each scan, the exact same starting and ending point was
thus identified on MCA on both the right and the left side.
The software automatically calculated a path line and meas-
ured the circumference and mean diameter (mean value between
the measured maximum and minimum diameter) of the vessel.
The software did measurements every 0.2mm along the length
of the vessel perpendicular to the centerline. Analysis of MMA
was done in a similar manner, where MMA was identified on
both the right and left side marking the branch from the main
trunk of the maxillary artery. The data were then transferred to
Microsoft Excel and the mean of the measured variables (MCA
and MMA circumference) was calculated.
Statistical AnalysisAll absolute values are presented as mean 6 standard deviation.
Percent changes are reported as mean and 95% confidence
interval (CI) or mean 6 standard error of the mean. Headache
score is presented as median and quartiles. Baseline recordings
were obtained before administration of CGRP and included
MRA measurements, headache score, adverse events, and re-
cording of vascular variables.
We first tested for side-to-side differences in MMA and
MCA circumference at baseline using paired t tests. Because
there was no statistically significant difference, we first used the
mean of the right and left sides in the further testing. MMA
and MCA circumference, respectively, were tested: (1) during
the delayed headache phase against baseline using paired sample
t-test and (2) after treatment with sumatriptan against delayed
headache recordings using paired sample t test.
In patients who reported half sided headache, we exam-
ined changes in MMA and MCA circumference on the head-
ache side and the nonheadache side separately. The headache
and nonheadache sides were compared using baseline corrected
values. In case of bilateral headache, we compared changes in
right and left side MMA and MCA separately. We also tested
for differences between the right and left side using the baseline
corrected values. Five percent (p < 0.05) was accepted as the
level of significance. Statistical analysis was done using SPSS for
Mac 18.0 (SPSS Inc., Chicago, IL).
Results
Twenty-four patients completed the study (20 women
and 4 men; mean age, 32 years [range, 21–54 years];
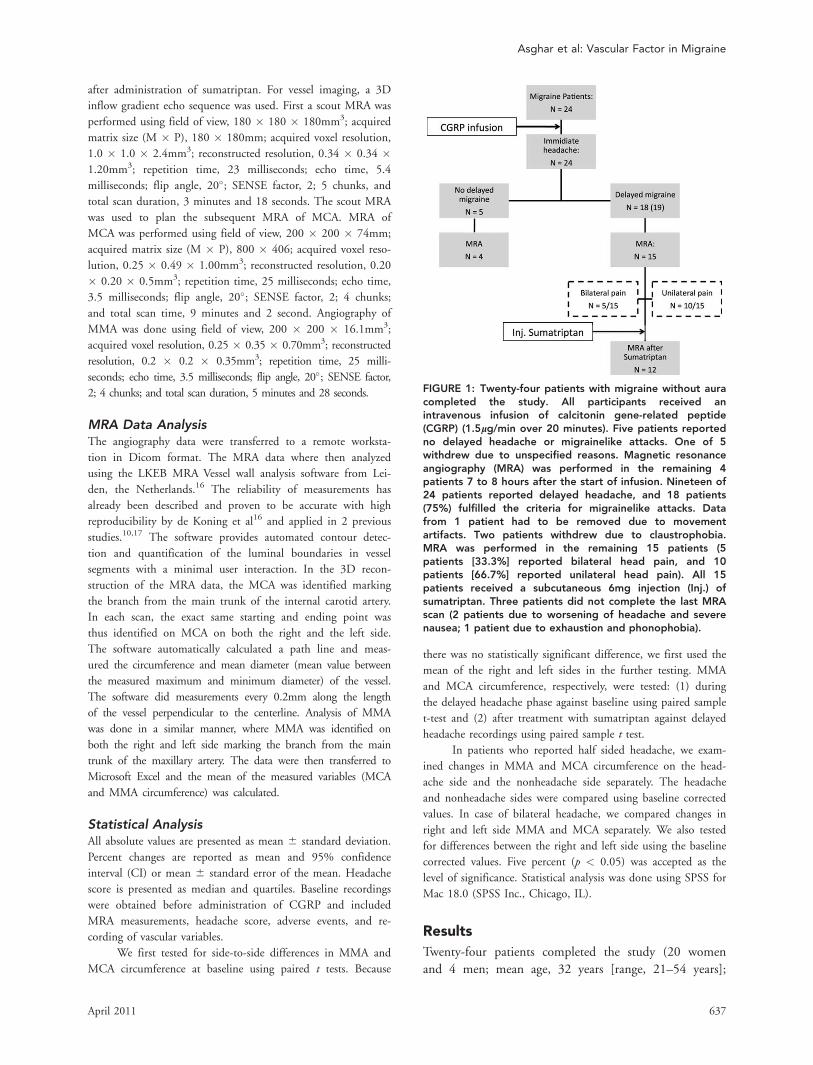
FIGURE 1: Twenty-four patients with migraine without auracompleted the study. All participants received anintravenous infusion of calcitonin gene-related peptide(CGRP) (1.5lg/min over 20 minutes). Five patients reportedno delayed headache or migrainelike attacks. One of 5withdrew due to unspecified reasons. Magnetic resonanceangiography (MRA) was performed in the remaining 4patients 7 to 8 hours after the start of infusion. Nineteen of24 patients reported delayed headache, and 18 patients(75%) fulfilled the criteria for migrainelike attacks. Datafrom 1 patient had to be removed due to movementartifacts. Two patients withdrew due to claustrophobia.MRA was performed in the remaining 15 patients (5patients [33.3%] reported bilateral head pain, and 10patients [66.7%] reported unilateral head pain). All 15patients received a subcutaneous 6mg injection (Inj.) ofsumatriptan. Three patients did not complete the last MRAscan (2 patients due to worsening of headache and severenausea; 1 patient due to exhaustion and phonophobia).
Asghar et al: Vascular Factor in Migraine
April 2011 637
mean weight, 66kg [range, 48–83kg]). The study profile
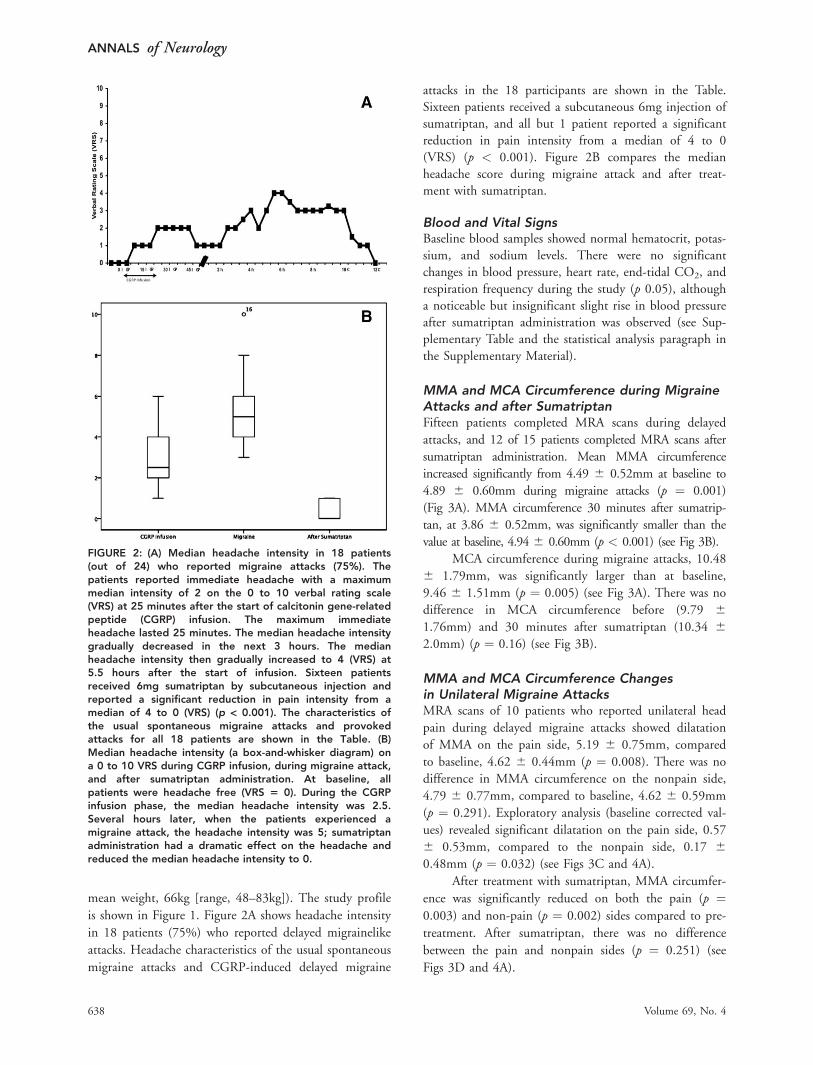
is shown in Figure 1. Figure 2A shows headache intensity
in 18 patients (75%) who reported delayed migrainelike
attacks. Headache characteristics of the usual spontaneous
migraine attacks and CGRP-induced delayed migraine
attacks in the 18 participants are shown in the Table.Sixteen patients received a subcutaneous 6mg injection ofsumatriptan, and all but 1 patient reported a significantreduction in pain intensity from a median of 4 to 0
(VRS) (p < 0.001). Figure 2B compares the medianheadache score during migraine attack and after treat-ment with sumatriptan.
Blood and Vital SignsBaseline blood samples showed normal hematocrit, potas-sium, and sodium levels. There were no significantchanges in blood pressure, heart rate, end-tidal CO2, and
respiration frequency during the study (p 0.05), althougha noticeable but insignificant slight rise in blood pressureafter sumatriptan administration was observed (see Sup-plementary Table and the statistical analysis paragraph in
the Supplementary Material).
MMA and MCA Circumference during MigraineAttacks and after SumatriptanFifteen patients completed MRA scans during delayed
attacks, and 12 of 15 patients completed MRA scans after
sumatriptan administration. Mean MMA circumference
increased significantly from 4.49 6 0.52mm at baseline to
4.89 6 0.60mm during migraine attacks (p ¼ 0.001)
(Fig 3A). MMA circumference 30 minutes after sumatrip-
tan, at 3.86 6 0.52mm, was significantly smaller than the
value at baseline, 4.94 6 0.60mm (p < 0.001) (see Fig 3B).
MCA circumference during migraine attacks, 10.48
6 1.79mm, was significantly larger than at baseline,
9.46 6 1.51mm (p ¼ 0.005) (see Fig 3A). There was no
difference in MCA circumference before (9.79 61.76mm) and 30 minutes after sumatriptan (10.34 62.0mm) (p ¼ 0.16) (see Fig 3B).
MMA and MCA Circumference Changesin Unilateral Migraine AttacksMRA scans of 10 patients who reported unilateral head
pain during delayed migraine attacks showed dilatation
of MMA on the pain side, 5.19 6 0.75mm, compared
to baseline, 4.62 6 0.44mm (p ¼ 0.008). There was no
difference in MMA circumference on the nonpain side,
4.79 6 0.77mm, compared to baseline, 4.62 6 0.59mm
(p ¼ 0.291). Exploratory analysis (baseline corrected val-
ues) revealed significant dilatation on the pain side, 0.57
6 0.53mm, compared to the nonpain side, 0.17 60.48mm (p ¼ 0.032) (see Figs 3C and 4A).
After treatment with sumatriptan, MMA circumfer-
ence was significantly reduced on both the pain (p ¼0.003) and non-pain (p ¼ 0.002) sides compared to pre-
treatment. After sumatriptan, there was no difference
between the pain and nonpain sides (p ¼ 0.251) (see
Figs 3D and 4A).
FIGURE 2: (A) Median headache intensity in 18 patients(out of 24) who reported migraine attacks (75%). Thepatients reported immediate headache with a maximummedian intensity of 2 on the 0 to 10 verbal rating scale(VRS) at 25 minutes after the start of calcitonin gene-relatedpeptide (CGRP) infusion. The maximum immediateheadache lasted 25 minutes. The median headache intensitygradually decreased in the next 3 hours. The medianheadache intensity then gradually increased to 4 (VRS) at5.5 hours after the start of infusion. Sixteen patientsreceived 6mg sumatriptan by subcutaneous injection andreported a significant reduction in pain intensity from amedian of 4 to 0 (VRS) (p < 0.001). The characteristics ofthe usual spontaneous migraine attacks and provokedattacks for all 18 patients are shown in the Table. (B)Median headache intensity (a box-and-whisker diagram) ona 0 to 10 VRS during CGRP infusion, during migraine attack,and after sumatriptan administration. At baseline, allpatients were headache free (VRS 5 0). During the CGRPinfusion phase, the median headache intensity was 2.5.Several hours later, when the patients experienced amigraine attack, the headache intensity was 5; sumatriptanadministration had a dramatic effect on the headache andreduced the median headache intensity to 0.
ANNALS of Neurology
638 Volume 69, No. 4
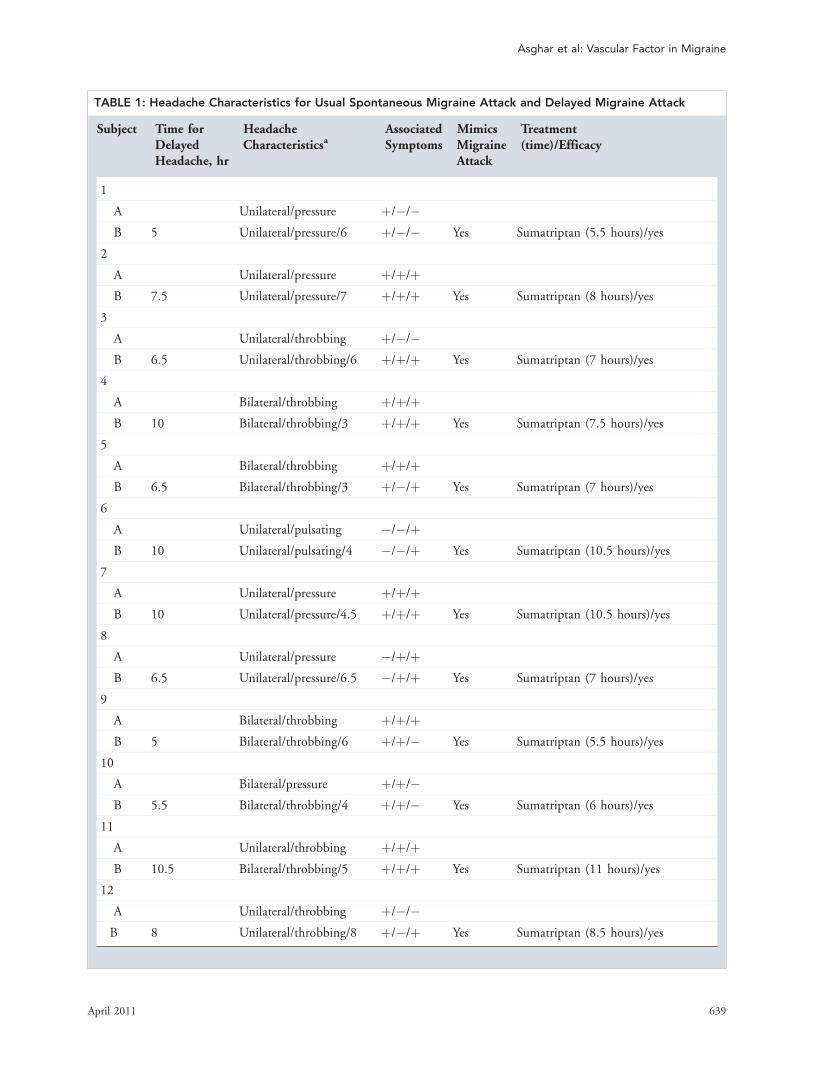
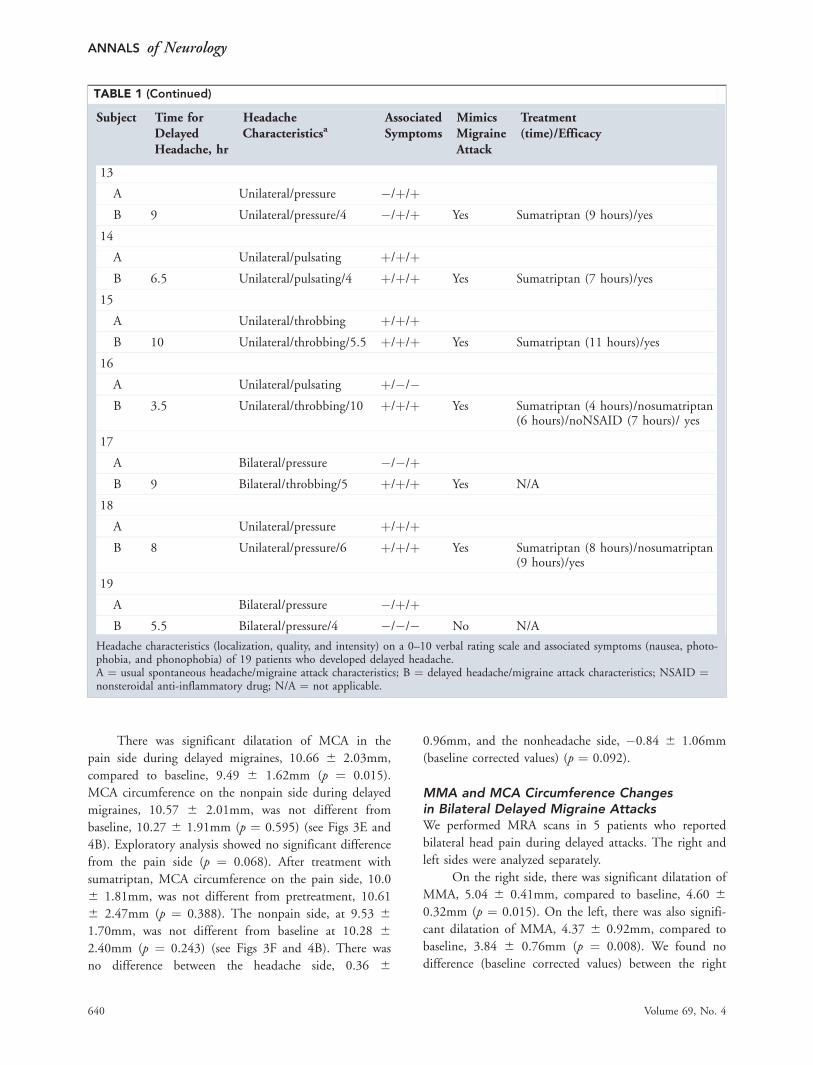
TABLE 1: Headache Characteristics for Usual Spontaneous Migraine Attack and Delayed Migraine Attack
Subject Time forDelayedHeadache, hr
HeadacheCharacteristicsa
AssociatedSymptoms
MimicsMigraineAttack
Treatment(time)/Efficacy
1
A Unilateral/pressure þ/�/�B 5 Unilateral/pressure/6 þ/�/� Yes Sumatriptan (5.5 hours)/yes
2
A Unilateral/pressure þ/þ/þB 7.5 Unilateral/pressure/7 þ/þ/þ Yes Sumatriptan (8 hours)/yes
3
A Unilateral/throbbing þ/�/�B 6.5 Unilateral/throbbing/6 þ/þ/þ Yes Sumatriptan (7 hours)/yes
4
A Bilateral/throbbing þ/þ/þB 10 Bilateral/throbbing/3 þ/þ/þ Yes Sumatriptan (7.5 hours)/yes
5
A Bilateral/throbbing þ/þ/þB 6.5 Bilateral/throbbing/3 þ/�/þ Yes Sumatriptan (7 hours)/yes
6
A Unilateral/pulsating �/�/þB 10 Unilateral/pulsating/4 �/�/þ Yes Sumatriptan (10.5 hours)/yes
7
A Unilateral/pressure þ/þ/þB 10 Unilateral/pressure/4.5 þ/þ/þ Yes Sumatriptan (10.5 hours)/yes
8
A Unilateral/pressure �/þ/þB 6.5 Unilateral/pressure/6.5 �/þ/þ Yes Sumatriptan (7 hours)/yes
9
A Bilateral/throbbing þ/þ/þB 5 Bilateral/throbbing/6 þ/þ/� Yes Sumatriptan (5.5 hours)/yes
10
A Bilateral/pressure þ/þ/�B 5.5 Bilateral/throbbing/4 þ/þ/� Yes Sumatriptan (6 hours)/yes
11
A Unilateral/throbbing þ/þ/þB 10.5 Bilateral/throbbing/5 þ/þ/þ Yes Sumatriptan (11 hours)/yes
12
A Unilateral/throbbing þ/�/�B 8 Unilateral/throbbing/8 þ/�/þ Yes Sumatriptan (8.5 hours)/yes
Asghar et al: Vascular Factor in Migraine
April 2011 639
There was significant dilatation of MCA in the
pain side during delayed migraines, 10.66 6 2.03mm,
compared to baseline, 9.49 6 1.62mm (p ¼ 0.015).
MCA circumference on the nonpain side during delayed
migraines, 10.57 6 2.01mm, was not different from
baseline, 10.27 6 1.91mm (p ¼ 0.595) (see Figs 3E and
4B). Exploratory analysis showed no significant difference
from the pain side (p ¼ 0.068). After treatment with
sumatriptan, MCA circumference on the pain side, 10.0
6 1.81mm, was not different from pretreatment, 10.61
6 2.47mm (p ¼ 0.388). The nonpain side, at 9.53 61.70mm, was not different from baseline at 10.28 6
2.40mm (p ¼ 0.243) (see Figs 3F and 4B). There was
no difference between the headache side, 0.36 6
0.96mm, and the nonheadache side, �0.84 6 1.06mm
(baseline corrected values) (p ¼ 0.092).
MMA and MCA Circumference Changesin Bilateral Delayed Migraine AttacksWe performed MRA scans in 5 patients who reported
bilateral head pain during delayed attacks. The right and
left sides were analyzed separately.
On the right side, there was significant dilatation of
MMA, 5.04 6 0.41mm, compared to baseline, 4.60 6
0.32mm (p ¼ 0.015). On the left, there was also signifi-
cant dilatation of MMA, 4.37 6 0.92mm, compared to
baseline, 3.84 6 0.76mm (p ¼ 0.008). We found no
difference (baseline corrected values) between the right
TABLE 1 (Continued)
Subject Time forDelayedHeadache, hr
HeadacheCharacteristicsa
AssociatedSymptoms
MimicsMigraineAttack
Treatment(time)/Efficacy
13
A Unilateral/pressure �/þ/þB 9 Unilateral/pressure/4 �/þ/þ Yes Sumatriptan (9 hours)/yes
14
A Unilateral/pulsating þ/þ/þB 6.5 Unilateral/pulsating/4 þ/þ/þ Yes Sumatriptan (7 hours)/yes
15
A Unilateral/throbbing þ/þ/þB 10 Unilateral/throbbing/5.5 þ/þ/þ Yes Sumatriptan (11 hours)/yes
16
A Unilateral/pulsating þ/�/�B 3.5 Unilateral/throbbing/10 þ/þ/þ Yes Sumatriptan (4 hours)/nosumatriptan
(6 hours)/noNSAID (7 hours)/ yes
17
A Bilateral/pressure �/�/þB 9 Bilateral/throbbing/5 þ/þ/þ Yes N/A
18
A Unilateral/pressure þ/þ/þB 8 Unilateral/pressure/6 þ/þ/þ Yes Sumatriptan (8 hours)/nosumatriptan
(9 hours)/yes
19
A Bilateral/pressure �/þ/þB 5.5 Bilateral/pressure/4 �/�/� No N/A
Headache characteristics (localization, quality, and intensity) on a 0–10 verbal rating scale and associated symptoms (nausea, photo-phobia, and phonophobia) of 19 patients who developed delayed headache.A ¼ usual spontaneous headache/migraine attack characteristics; B ¼ delayed headache/migraine attack characteristics; NSAID ¼nonsteroidal anti-inflammatory drug; N/A ¼ not applicable.
ANNALS of Neurology
640 Volume 69, No. 4
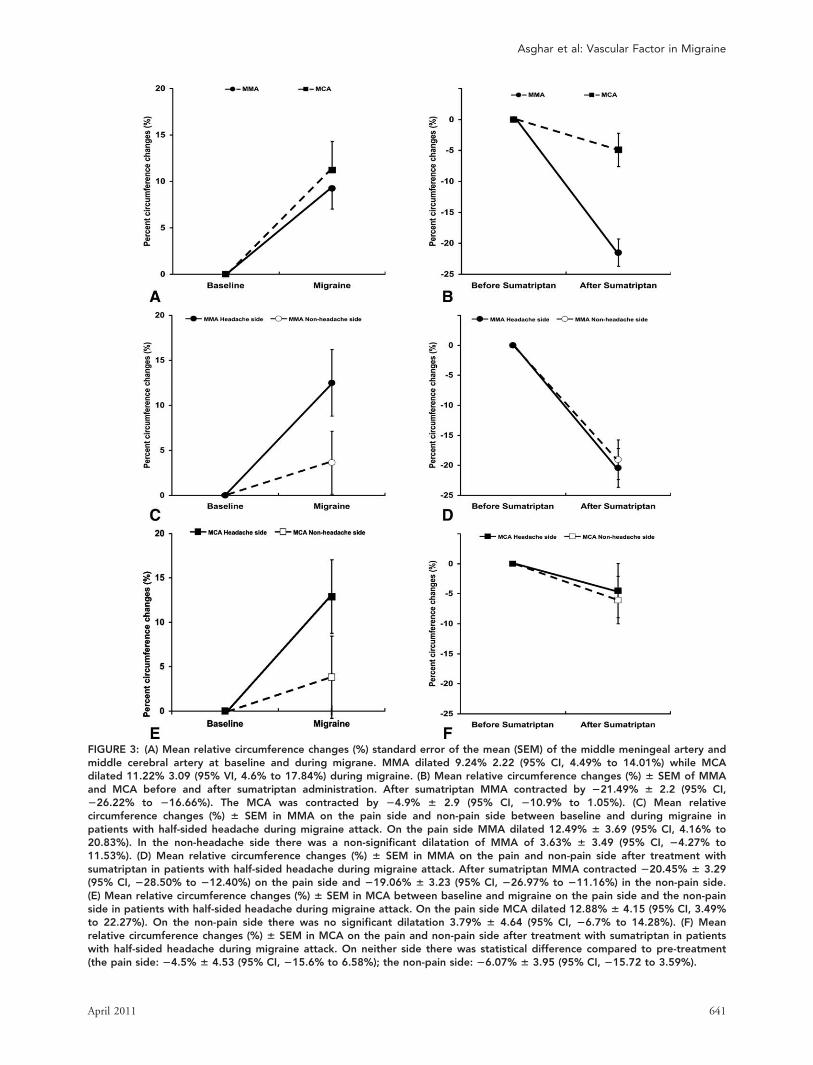
FIGURE 3: (A) Mean relative circumference changes (%) standard error of the mean (SEM) of the middle meningeal artery andmiddle cerebral artery at baseline and during migrane. MMA dilated 9.24% 2.22 (95% CI, 4.49% to 14.01%) while MCAdilated 11.22% 3.09 (95% VI, 4.6% to 17.84%) during migraine. (B) Mean relative circumference changes (%) 6 SEM of MMAand MCA before and after sumatriptan administration. After sumatriptan MMA contracted by 221.49% 6 2.2 (95% CI,226.22% to 216.66%). The MCA was contracted by 24.9% 6 2.9 (95% CI, 210.9% to 1.05%). (C) Mean relativecircumference changes (%) 6 SEM in MMA on the pain side and non-pain side between baseline and during migraine inpatients with half-sided headache during migraine attack. On the pain side MMA dilated 12.49% 6 3.69 (95% CI, 4.16% to20.83%). In the non-headache side there was a non-significant dilatation of MMA of 3.63% 6 3.49 (95% CI, 24.27% to11.53%). (D) Mean relative circumference changes (%) 6 SEM in MMA on the pain and non-pain side after treatment withsumatriptan in patients with half-sided headache during migraine attack. After sumatriptan MMA contracted 220.45% 6 3.29(95% CI, 228.50% to 212.40%) on the pain side and 219.06% 6 3.23 (95% CI, 226.97% to 211.16%) in the non-pain side.(E) Mean relative circumference changes (%) 6 SEM in MCA between baseline and migraine on the pain side and the non-painside in patients with half-sided headache during migraine attack. On the pain side MCA dilated 12.88% 6 4.15 (95% CI, 3.49%to 22.27%). On the non-pain side there was no significant dilatation 3.79% 6 4.64 (95% CI, 26.7% to 14.28%). (F) Meanrelative circumference changes (%) 6 SEM in MCA on the pain and non-pain side after treatment with sumatriptan in patientswith half-sided headache during migraine attack. On neither side there was statistical difference compared to pre-treatment(the pain side: 24.5% 6 4.53 (95% CI, 215.6% to 6.58%); the non-pain side: 26.07% 6 3.95 (95% CI, 215.72 to 3.59%).
Asghar et al: Vascular Factor in Migraine
April 2011 641

MMA, 0.43 6 0.23mm, and the left MMA, 0.52 6
0.24mm (p ¼ 0.392). After sumatriptan, there was sig-
nificant reduction of MMA circumference on both sides
(right side, p ¼ 0.004; left side, p ¼ 0.012). Exploratory
analysis revealed no difference between sides (p ¼0.119). (Supplementary Fig A).
There was significant dilatation of the right MCA
during delayed attacks, 9.99 6 2.02mm, compared to
baseline, 8.56 6 1.14mm (p ¼ 0.033). There was also
significant dilatation of the left MCA during attacks,
10.41 6 1.27mm, compared to baseline, 8.69 6 0.87mm
(p ¼ 0.021). There was no difference (baseline corrected
values) between the right MCA, 1.43 6 1.0mm, and the
left MCA, 1.73 6 1.05mm (p ¼ 0.671).
After sumatriptan, there was no reduction in MCA
circumference on either sides (right side, p ¼ 0.701; left
side, p ¼ 0.200) and no difference between the right and
left sides (p ¼ 0.057) (Supplementary Fig B).
MMA and MCA Circumference in PatientsReporting No Delayed AttacksMRA scans in 4 patients who did not report delayed head-
aches or migraine attacks were recorded 7 to 8 hours after
the start of CGRP infusion. MMA or MCA circumference
did not differ between postinfusion (MMA, 4.28 60.48mm; MCA, 10.76 6 1.57mm) and baseline (MMA,
4.3 6 0.41mm; MCA, 10.87 6 1.74mm) (p > 0.05).
Discussion
The major finding of the present study was that CGRP
induced delayed migraine attacks and that the migraine
attacks were associated with dilatation of both extra- and
intracranial vessels. Patients with unilateral migraine pain
had dilatation of the MMA and MCA on the pain side
but not on the pain-free side. In patients with bilateral mi-
graine pain, we recorded bilateral dilatation of both the
MMA and MCA. Moreover, sumatriptan reversed dilata-
tion of the MMA and aborted migraine attacks. We found
no effect of sumatriptan on the MCA circumference.
Scientists have long sought the origin of migraine
pain. In 1672, Thomas Willis proposed the first vascular
hypothesis of migraine. This was supported by Graham
and Wolff,18 who found extracranial arterial dilatation
during migraine attack. Blood vessel involvement in mi-
graine was further suggested by dilatation of pial arteries
and flow changes associated with experimental cortical
spreading depression19–21 and with migraine attacks with
aura.22–25 Ultrasonography studies during migraine
attacks without aura have shown a slight but significant
arterial dilatation.26,27 By itself, the dilatation was not
sufficient to physically cause head pain, but rather it was
thought to reflect leakage of dilator and pronociceptive
substances in the perivascular space or parasympathetic
efferent effects. These findings have been challenged by a
Doppler study28 and more recently in an MRA study.10
In contrast to the present data, the latter MRA study
reported that provoked migraine attacks are not associ-
ated with dilatation of the MMA and the MCA. In this
as well as in the present study the same magnetic reso-
nance imaging scanner (Philips 3T) and head coil were
used to obtain MRA images, and the same vessel-wall
software was used to analyze the arteries from the same
anatomical localizations (the extracranial part of the
MMA and the initial part of the MCA). Although differ-
ent migraine pharmacological triggers (glyceryl trinitrate
in the previous study) were used, patients in both studies
reported migraine attacks indistinguishable from sponta-
neous attacks. However, the major differences between
the 2 studies are that (1) we applied predefined pain in-
tensity criteria (VRS � 4) before a migraine attack
FIGURE 4: (A) Three-dimensional (3D) data of middlemeningeal artery (MMA) in 1 subject with half-sidedheadache during migraine attack. MMA dilates on theheadache side during migraine attack, whereas no dilatationis observed on the nonheadache side. After injection ofsumatriptan, MMA contracts on both sides. (B) 3D data ofmiddle cerebral artery (MCA) in 1 subject. MCA dilates onthe headache side during migraine attack, whereas nodilatation is observed on the nonheadache aside. Afterinjection of sumatriptan no contraction of MCA is observed.
ANNALS of Neurology
642 Volume 69, No. 4

qualified for MRA scans; (2) we calculated the artery cir-
cumference17 and not the average diameter, because
arteries do not always resemble a circle, and the intracra-
nial anatomy does not always permit uniform dilatation
of the arteries; and (3) to avoid possible partial volume
problems, and because the vessel wall analysis software
requires at least 3 voxels across the measured artery, we
used a high-resolution MRA with a very small voxel size
(MMA, 0.2 � 0.2 � 0.35mm and MCA, 0.2 � 0.2 �0.5mm), resulting in images with sufficient voxels across
the vessels (2.8 � 5 voxels across MMA and 2 � 5 vox-
els across MCA). In contrast, the previous study used an
image resolution with approximately double the voxel
size (MMA, 0.39 � 0.39 � 0.25mm and MCA, 0.43 �0.43 � 0.65mm), allowing only 2 � 2 voxels across
MMA and 1.5 � 2.3 voxels across MCA10 (for data ac-
quisition, imaging protocols, and MRA analysis methods,
see Supplementary Material). Thus, the previous study
might have been unable to detect the subvoxel size dilata-
tion of MMA and MCA observed in the present study.
At the present field strength (3T), the image resolution
we applied was the maximally practically feasible. Other-
wise, each scan would have been more time-consuming
and result in low compliance, because it is rather
unpleasant for patients to be in a scanner during a mi-
graine attack. For all these reasons, our finding of arterial
dilatation during a migraine attack is highly likely to be
correct.
These data thereby clearly demonstrate that extra-
and intracranial arteries are only dilated on the pain
side during half-sided migraine attacks, and that bilat-
eral dilatation is observed in double-sided headache
during migraine attacks. It is well known that CGRP
has a rather short half-life (�10 minutes),29 which
rules out the possibility that the dilatation observed can
be due to a carryover effect due to the initial CGRP
infusion. This is further supported by the present
study, in which the postinfusion control scan revealed
no dilatation in the patients who did not develop mi-
graine attacks.
The question arises whether the modest dilatation
by 9 to 12% reported here is sufficient to activate nor-
mal sensory afferents in the perivascular space or whether
it has an effect only on sensitized nociceptors. We suggest
the latter, because arterial diameters may dilate markedly,
for example, during blood pressure decreases, and pulsa-
tion may increase during physical exercise without
accompanying head pain. But what are the possible
mechanisms of sensitization and excitation of the nerve
terminals? If migraine attacks start in the brain30 and
cause nociception, this can only be caused by efferent ac-
tivity in perivascular nerves.31 Sensitization could be
caused by leakage of vasoactive/sensitizing substances
from trigeminal nerve terminals32,33 or by efferent activ-
ity in parasympathetic nerves34 and consequent release of
substances that may sensitize sensory afferents. We con-
clude that migraine attacks may be evoked in deep brain
structures, but these initiating mechanisms trigger peri-
vascular release of vasoactive substances causing sensitiza-
tion of trigeminal afferents, vasodilatation, and migraine
pain.
Is the Mode of Action of Sumatriptan Vascularor Neuronal?Sumatriptan (5-HT1B/1D receptor agonist) was originally
developed as a selective cranial vasoconstrictor.35 How-
ever, the mode of action of sumatriptan and other trip-
tans in migraine is far more complex than initially per-
ceived.36 A central site of action has received support in
recent years, and vascular mechanisms have been
doubted.37 In the present study, we found that subcuta-
neous sumatriptan reversed dilatation and even con-
tracted MMA but not MCA during migraine attacks.
Simultaneously, all patients reported amelioration of mi-
graine headache. In the absence of a placebo group, the
specificity of MMA response suggests that the reversal
response is attributable to sumatriptan. These data pro-
vide the strongest evidence to date that sumatriptan
blocks dilatation in the major artery supplying blood to
the dura mater during migraine attacks. Given that
sumatriptan significantly constricted the MMA and not
the MCA, the present data suggest that the vascular site
of action of sumatriptan is primarily extracranial. These
results are supported by a recent MRA study in healthy
subjects17 showing that sumatriptan induced vasocon-
striction of meningeal but not intracerebral artery and
reduced head pain intensity. Interestingly, previous stud-
ies have shown that sumatriptan also blocks plasma pro-
tein extravasation, vasodilatation, and activation of sen-
sory afferents in dura in the neurogenic inflammation
model of migraine.38 The neurogenic inflammation
model has been used as an assay to predict probable anti-
migraine efficacy without causing vasoconstriction. How-
ever, several highly effective compounds in animal mod-
els failed to relieve migraine in clinical trials (for review
see Williamson and Hargreaves39). In another animal
model of migraine, triptans exerted their antimigraine
action through presynaptic 5-HT1B/1D receptors in the
nucleus caudalis, thus blocking synaptic transmission
between axon terminals of the peripheral trigeminovascu-
lar neurons and cell bodies of their central counter-
parts.40 Collectively, the results from human and animal
studies suggest that sumatriptan exerts its antimigraine
Asghar et al: Vascular Factor in Migraine
April 2011 643

effect by a combined constriction of extracerebral arteries
and inhibition of nociceptive input from these arteries.
ConclusionsThe major outcome of the present study is that migraine
attacks are associated with extra- and intracerebral arterial
dilatation, in particular on the headache side. Further-
more, contraction of dural arteries by sumatriptan is
associated with headache relief, suggesting primarily an
extracerebral site of vascular action of sumatriptan. Cra-
nial blood vessels thus seem to be important players in
the pathophysiology of migraine.
Acknowledgment
The study was supported by grants from the University
of Copenhagen, the Danish Headache Society, the Lund-
beck Foundation through the Center for Neurovascular
Signaling, Danish Agency for Science, Technology, and
Innovation, and Danish Council for Independent
Research–Medical Sciences (grant 271-08-0446). The
study was also supported in part by a research grant
(33936) from the Investigator Initiated Studies Program
of Merck & Co., Inc. The opinions expressed in this pa-
per are those of the authors and do not necessarily repre-
sent those of Merck & Co., Inc.
The authors thank all participating subjects; Dr S. Pe-
dersen for his insights and advice during the study;
radiographers M. Lindhart, B. S. Møller, and H. Simon-
sen for their work during the experiments; and medical
students K. D. Berg, T. R. Kapijimpanga, V. Kristensen,
and C. Vorbeck for their assistance in the MRA scans
and for their work in analyzing the data.
Potential Conflicts of Interest
J.O. has received grants and/or research support from, has
been a consultant and/or scientific adviser for, and has been
in the speakers’ bureau of Allergan Inc, AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim, Eli Lilly,
GlaxoSmithKline, Janssen Pharmaceutical Products, Lund-
beck, Merck, and Pfizer. M.A. has received grant support
and honoraria for lecturing from Merck, and honoraria for
lecturing from Pfizer, GlaxoSmithKline, Norpharma, and
AstraZeneca, and is a consultant and/or scientific adviser
for Merck and BTG international. There are no conflicts of
interest for the remaining authors.
References1. Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, dis-
ease burden, and the need for preventive therapy. Neurology2007;68:343–349.
2. Andlin-Sobocki P, Jonsson B, Wittchen H, Olesen J. Cost of disor-ders of the brain in Europe. Eur J Neurol 2005;12(suppl 1):1–27.
3. Isler H, Koehler PJ. History of the headache. In: Olesen J, Tfelt-Hansen P, Welch KM, et al. The headaches. 3rd ed. Philadelphia,PA: Lippincott Williams & Wilkins, 2005:1–7.
4. Ray BS, Wolff HG. Experimental studies on headache: pain-sensi-tive structures of the head and their significance in headache.Arch Surg 1940;41:813–856.
5. Brennan K, Charles A. An update on the blood vessel in migraine.Curr Opin Neurol 2010;23:266–274.
6. Weiller C, May A, Limmroth V, et al. Brain stem activation in spon-taneous human migraine attacks. Nat Med 1995;1:658–660.
7. Bahra A, Matharu MS, Buchel C, et al. Brainstem activation spe-cific to migraine headache. Lancet 2001;357:1016–1017.
8. May A, Goadsby PJ. The trigeminovascular system in humans:pathophysiologic implications for primary headache syndromes ofthe neural influences on the cerebral circulation. J Cereb BloodFlow Metab 1999;19:115–127.
9. Sakai Y, Dobson C, Diksic M, et al. Sumatriptan normalizes the mi-graine attack-related increase in brain serotonin synthesis. Neurol-ogy 2008;70:431–439.
10. Schoonman G, van der Grond J, Kortmann C, et al. Migraineheadache is not associated with cerebral or meningeal vasodilata-tion—a 3T magnetic resonance angiography study. Brain 2008;131(pt 8):2192–2200.
11. Schoonman GG, Ferrari MD. Reply to: Migraine headache is notassociated with cerebral or meningeal vasodilatation—a 3T mag-netic resonance angiography study. Brain 2008;132:e113.
12. Brain SD, Williams TJ, Tippins JR, et al. Calcitonin gene-relatedpeptide is a potent vasodilator. Nature 1985;313:54–56.
13. McCulloch J, Uddman R, Kingman TA, Edvinsson L. Calcitoningene-related peptide: functional role in cerebrovascular regula-tion. Proc Natl Acad Sci U S A 1986;83:5731–5735.
14. Lassen L, Haderslev P, Jacobsen V, et al. CGRP may play a causa-tive role in migraine. Cephalalgia 2002;22:54–61.
15. Petersen K, Lassen L, Birk S, et al. BIBNBS$6$7 antagonizes humanalpha-calcitonin gene related peptide-induced headache and extra-cerebral artery dilatation. Clin Pharmacol Ther 2005;77:202–213.
16. de Koning P, Schaap J, Janssen J, et al. Automated segmentationand analysis of vascular structures in magnetic resonance angio-graphic images. Magn Reson Med 2003;50:1189–1198.
17. Asghar MS, Hansen AE, Kapijimpanga TR, et al. Dilatation byCGRP of middle meningeal artery and reversal by sumatriptan innormal volunteers. Neurology 2010;75:1494–1495.
18. Graham JR, Wolff HG. Mechanism of migraine headache andaction or ergotamine tartrate. Arch Neurol Psychiatry 1938;39:737–763.
19. Wahl M, Schilling L, Parsons AA, Kaumann A. Involvement of calci-tonin gene-related peptide (CGRP) and nitric oxide (NO) in thepial artery dilatation elicited by cortical spreading depression.Brain Res 1994;637:204–210.
20. Lauritzen M, Fabricius M. Real time laser-Doppler perfusion imag-ing of cortical spreading depression in rat neocortex. Neuroreport1995;6:1271–1273.
21. Woods RP, Iacoboni M, Mazziotta JC. Brief report: bilateralspreading cerebral hypoperfusion during spontaneous migraineheadache. N Engl J Med 1994;331:1689–1692.
22. Olesen J, Larsen B, Lauritzen M. Focal hyperemia followed byspreading oligemia and impaired activation of rCBF in classic mi-graine. Ann Neurol 1981;9:344–352.
23. Lauritzen M, Olesen J. Regional cerebral blood flow during mi-graine attacks by xenon-133 inhalation and emission tomography.Brain 1984;107(pt 2):447–461.
ANNALS of Neurology
644 Volume 69, No. 4

24. Hadjikhani N, Sanchez Del Rio M, Wu O, et al. Mechanisms of mi-graine aura revealed by functional MRI in human visual cortex.Proc Natl Acad Sci U S A 2001;98:4687–4692.
25. Lauritzen M. Pathophysiology of the migraine aura: the spreadingdepression theory. Brain 1994;117:199–210.
26. Thomsen LL, Iversen HK, Olesen J. Cerebral blood flow velocitiesare reduced during attacks of unilateral migraine without aura.Cephalalgia 1995;15:109–116.
27. Iversen HK, Nielsen TH, Olesen J, Tfelt-Hansen P. Arterialresponses during migraine headache. Lancet 1990;336:837–839.
28. Zwetsloot CP, Caekebeke JF, Ferrari MD. Lack of asymmetry ofmiddle cerebral artery blood velocity in unilateral migraine. Stroke1993;24:1335–1338.
29. Brain S, Cambridge H. Calcitonin gene-related peptide: vasoactiveeffects and potential therapeutic role. Gen Pharmacol 1996;27:607–611.
30. Goadsby PJ, Charbit AR, Andreou AP, et al. Neurobiology of mi-graine. Neuroscience 2009;161:327–341.
31. Olesen J, Burstein R, Ashina M, Tfelt-Hansen P. Origin of pain inmigraine: evidence for peripheral sensitisation. Lancet Neurol2009;8:679–690.
32. Mayberg M, Langer RS, Zervas NT, Moskowitz MA. Perivascularmeningeal projections from cat trigeminal ganglia: possible path-way for vascular headaches in man. Science 1981;213:228–230.
33. Strassman AM, Raymond SA, Burstein R. Sensitization of menin-geal sensory neurons and the origin of headaches. Nature 1996;384:560–564.
34. Burstein R, Jakubowski M. Unitary hypothesis for multipletriggers of the pain and strain of migraine. J Comp Neurol 2005;493:9–14.
35. Humphrey PP, Goadsby PJ. The mode of action of sumatriptan isvascular? A debate. Cephalalgia 1994;14:401–410; discussion 393.
36. Ferrari MD, Goadsby PJ, Roon KI, Lipton RB. Triptans (serotonin,5-HT1B/1D agonists) in migraine: detailed results and methods ofa meta-analysis of 53 trials. Cephalalgia 2002;22:633–658.
37. Tfelt-Hansen PC. Does sumatriptan cross the blood-brain barrierin animals and man? J Headache Pain 2010;11:5–12.
38. Moskowitz MA. Neurogenic inflammation in the pathophysiology andtreatment of migraine. Neurology 1993;43(6 suppl 3):S16–S20.
39. Williamson DJ, Hargreaves RJ. Neurogenic inflammation in thecontext of migraine. Microsc Res Tech 2001;53:167–178.
40. Levy D, Jakubowski M, Burstein R. Disruption of communicationbetween peripheral and central trigeminovascular neurons medi-ates the antimigraine action of 5HT 1B/1D receptor agonists. ProcNatl Acad Sci U S A 2004;101:4274–4279.
41. Olesen J. The international classification of headache disorders.2nd edition (ICHD-II). Rev Neurol (Paris) 2005;161:689–691.
Asghar et al: Vascular Factor in Migraine
April 2011 645
Copyright © 2022 FDOKUMEN




















