Evaluation of the Extent of Pulmonary Cysts and Their Association with Functional Variables and...
10
1 23 Lung ISSN 0341-2040 Volume 192 Number 6 Lung (2014) 192:967-974 DOI 10.1007/s00408-014-9641-2 Evaluation of the Extent of Pulmonary Cysts and Their Association with Functional Variables and Serum Markers in Lymphangioleiomyomatosis (LAM) Bruno Guedes Baldi, Mariana Sponholz Araujo, Carolina Salim Gonçalves Freitas, Gustavo Borges da Silva Teles, Ronaldo Adib Kairalla, et al.
Transcript of Evaluation of the Extent of Pulmonary Cysts and Their Association with Functional Variables and...
1 23
Lung ISSN 0341-2040Volume 192Number 6 Lung (2014) 192:967-974DOI 10.1007/s00408-014-9641-2
Evaluation of the Extent of PulmonaryCysts and Their Association withFunctional Variables and Serum Markersin Lymphangioleiomyomatosis (LAM)
Bruno Guedes Baldi, Mariana SponholzAraujo, Carolina Salim GonçalvesFreitas, Gustavo Borges da Silva Teles,Ronaldo Adib Kairalla, et al.

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Science
+Business Media New York. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.
INTERSTITIAL LUNG DISEASE
Evaluation of the Extent of Pulmonary Cysts and TheirAssociation with Functional Variables and Serum Markersin Lymphangioleiomyomatosis (LAM)
Bruno Guedes Baldi • Mariana Sponholz Araujo • Carolina Salim Goncalves Freitas •
Gustavo Borges da Silva Teles • Ronaldo Adib Kairalla • Olıvia Meira Dias •
Daniel Antunes Silva Pereira • Suzana Pinheiro Pimenta • Carlos Roberto Ribeiro Carvalho
Received: 2 June 2014 / Accepted: 1 September 2014 / Published online: 9 September 2014
� Springer Science+Business Media New York 2014
Abstract
Purpose Although computed tomography (CT) has been
used previously to assess disease severity in lymphangio-
leiomyomatosis (LAM), the associations between the extent
of pulmonary cysts on CT and six-minute walk test (6MWT),
matrix metalloproteinases (MMPs) and vascular endothelial
growth factor (VEGF-D) are not well established. We per-
formed a cross-sectional study to quantify the extent of
pulmonary cysts in CT and to establish their correlations
with pulmonary function tests (PFTs), 6MWT results,
including a composite index (desaturation–distance ratio,
DDR), and levels of VEGF-D and MMPs in LAM.
Methods Twenty-three LAM patients underwent CT
scanning to automatically quantify the extent of pulmonary
cysts and performed PFTs and 6MWT. Serum levels of
MMP-2, MMP-9, and VEGF-D were also measured.
Results The severity of pulmonary cystic involvement was
mild (the extent of cysts was 6.8 %) and correlated best with
FEV1/FVC (r = -0.84), residual volume (r = 0.66), DLCO
(r = -0.82), the DDR index (r = 0.77), and desaturation
during the 6MWT (r = -0.81). There was a weak
correlation with VEGF-D (r = 0.45), but no association was
found with MMP-2 and MMP-9.
Conclusions The severity of pulmonary cystic involve-
ment was mild in this sample of LAM patients and corre-
lated best with airway obstruction, air trapping, reduced
DLCO, the DDR index, and desaturation during the 6MWT.
Serum VEGF-D cannot be completely defined as a valu-
able marker of disease severity and there may be a mech-
anism independent of MMPs to explain the formation of
pulmonary cysts.
Keywords Computed tomography � Exercise �Lymphangioleiomyomatosis � Matrix metalloproteinase �Pulmonary function tests � Vascular endothelial growth
factor
Introduction
Lymphangioleiomyomatosis (LAM) is characterized by
atypical muscle cell proliferation, which can lead to vas-
cular and airway obstruction and formation of cysts. The
extent of pulmonary involvement in LAM varies from a
few scattered cysts to diffuse destruction of the lungs [1, 2].
An obstructive pattern, air trapping, and a reduced dif-
fusion capacity of the lungs for carbon monoxide (DLCO)
are the main findings in pulmonary function tests (PFTs) in
LAM [1–4]. Chest computed tomography (CT) shows
diffuse, thin-walled pulmonary cysts, together with pneu-
mothorax and pleural effusion [5–10].
PFTs are used most frequently to assess lung disease
severity, progression and response to treatment modalities;
forced expiratory volume in the first second (FEV1), and
DLCO are the main measurements recorded [1, 11–13].
However, there are some limitations to the use of PFTs,
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00408-014-9641-2) contains supplementarymaterial, which is available to authorized users.
B. G. Baldi (&) � M. S. Araujo � C. S. G. Freitas �R. A. Kairalla � O. M. Dias � D. A. S. Pereira �S. P. Pimenta � C. R. R. Carvalho
Pulmonary Division, Heart Institute (InCor), University of Sao
Paulo Medical School, Dr. Eneas de Carvalho Aguiar Avenue,
44, Fifth floor, Sao Paulo 05403-900, Brazil
e-mail: [email protected]
G. B. da Silva Teles
Department of Radiology, University of Sao Paulo Medical
School, Sao Paulo, Brazil
123
Lung (2014) 192:967–974
DOI 10.1007/s00408-014-9641-2
Author's personal copy

such as the need for patient cooperation and inter-test
variability. Other methods that may be used to assess the
severity of lung involvement in LAM include histological
scoring, exercise testing, and CT [3, 5–11, 14, 15]. The
walking distance and oxygen desaturation during the six-
minute walk test (6MWT) may also be used to evaluate the
severity of pulmonary involvement in LAM [3]. However,
a composite index that uses the continuous peripheral
oxygen saturation (SpO2) combined with the walking dis-
tance may be a more reliable tool than the isolated evalu-
ation of these variables for functional assessment of LAM
patients [16].
Previous semiquantitative or quantitative studies have
used CT to evaluate lung disease severity in LAM and have
demonstrated correlations between the extent of pulmonary
cysts with PFTs [5–10]. CT is a non-invasive testing
method and requires minimal patient cooperation.
Serum levels of vascular endothelial growth factor
(VEGF-D), a lymphangiogenic growth factor, are increased
in most LAM patients. This marker seems to be associated
with disease severity and thus may potentially be useful for
assessing the course of the disease over the long term [17,
18]. Xu and co-authors have shown that VEGF-D levels are
correlated with a semiquantitative grade of cystic
involvement on CT [19]. Matrix metalloproteinases
(MMPs) are components of the extracellular matrix that
degrades some matrix substrates, including collagen and
elastin, in the pulmonary parenchyma. Previous studies
have shown that pulmonary lesions and serum from LAM
patients contain increased levels of MMPs, primarily
MMP-2 and MMP-9, which may play a role in the patho-
genesis of cystic lung destruction [13, 20–22]. Therefore, it
would be reasonable to correlate the extent of cysts on CT
with levels of MMPs in LAM patients.
The correlations between the extent of pulmonary cysts
and 6MWT parameters and levels of MMPs and VEGF-D are
not well characterized. Thus, the aims of this study were to
quantify the extent of pulmonary cysts using high-resolution
computed tomography (HRCT) images and to determine the
degree of correlations between the extent of cysts and
parameters of PFTs, the distance walked and oxygen desat-
uration during 6MWT, a composite index that uses the
desaturation during 6MWT combined with the walking
distance (desaturation–distance ratio, DDR), and serum
levels of VEGF-D, MMP-2, and MMP-9 in LAM patients.
Methods
Study Population
This cross-sectional study included 23 women with LAM
who were patients in our center between 2009 and 2011.
The diagnosis of LAM was confirmed by lung biopsy
(74 %), kidney biopsy (9 %), or by the combination of
typical HRCT findings with clinical features (17 %) [1].
No patients were evaluated during an exacerbation of dis-
ease or during an episode of pneumothorax or chylothorax.
This study was performed as part of an institutional
review board-approved protocol (0345/07), and all patients
gave written, informed consent.
Measurements
All measurements in each patient were performed within a
maximum period of 15 days.
Computed Tomography Scanning
All patients underwent CT scanning without intravenous
contrast injection. Ten-detector and 16-detector MDCT
scanners were used (MX8000 IDT10 or IDT16, Philips
Medical Systems, Cleveland, OH, USA). Scan data were
obtained in spiral mode with 10 9 0.75 mm or
16 9 0.75 mm collimation, with patients in prone position
and holding their breath at the end of inspirations. Expo-
sure settings were 150–280 mAs at 120 or 140 kVp,
depending on the participants weight. Axial images were
reconstructed with 1.0 mm thickness at 1.0 mm incre-
ments. All scans were reconstructed with a soft recon-
struction filter using a 512 9 512 matrix.
Quantitative Analysis
Quantification of cystic lesions was obtained by CT den-
sitovolumetry using a computer program (Advantage
Workstation Thoracic VCAR software; GE Medical Sys-
tems, Milwaukee, WS, USA) that allows for the automatic
segmentation of the lungs and airways. To obtain the
volume of pulmonary cysts, a threshold value of -950 HU
was applied to the segmented lungs to select pixels
between -1000 and -950 HU. The total lung volume, the
volume occupied by cysts and the ratio of the abnormal
cyst volume to the total lung volume were calculated
automatically. The image analysis and a manual correction
of the results to exclude bronchiectasis or residual pneu-
mothorax from cystic voxels were performed by a thoracic
radiologist (G.B.S.T) who was blind to the results from the
other exams. The method and the computer program used
to quantify the extent of cysts were very similar to those
performed by Avila and co-authors [7].
Pulmonary Function Tests
All measurements were obtained using standard methods
[23–25]. Spirometry was performed using a calibrated
968 Lung (2014) 192:967–974
123
Author's personal copy
pneumotachograph (Medical Graphics Corporation, MGC,
St. Paul, MN, USA, 2005), while lung volumes and DLCO
values were obtained with a body plethysmograph (Elite
Dx, Elite SeriesTM; MGC). The following variables were
obtained: forced vital capacity (FVC), FEV1, total lung
capacity (TLC), residual volume (RV), and DLCO. Pre-
dicted values were derived from the Brazilian population
[26–28].
Six-Minute Walk Test
Patients performed the 6MWT in accordance with standard
guidelines [29]. Oxygen saturation, as measured by pulse
oxymeter holter (Nonin WristOx� 3100Plymouth, MN,
USA), was obtained at rest and at the end of exercise.
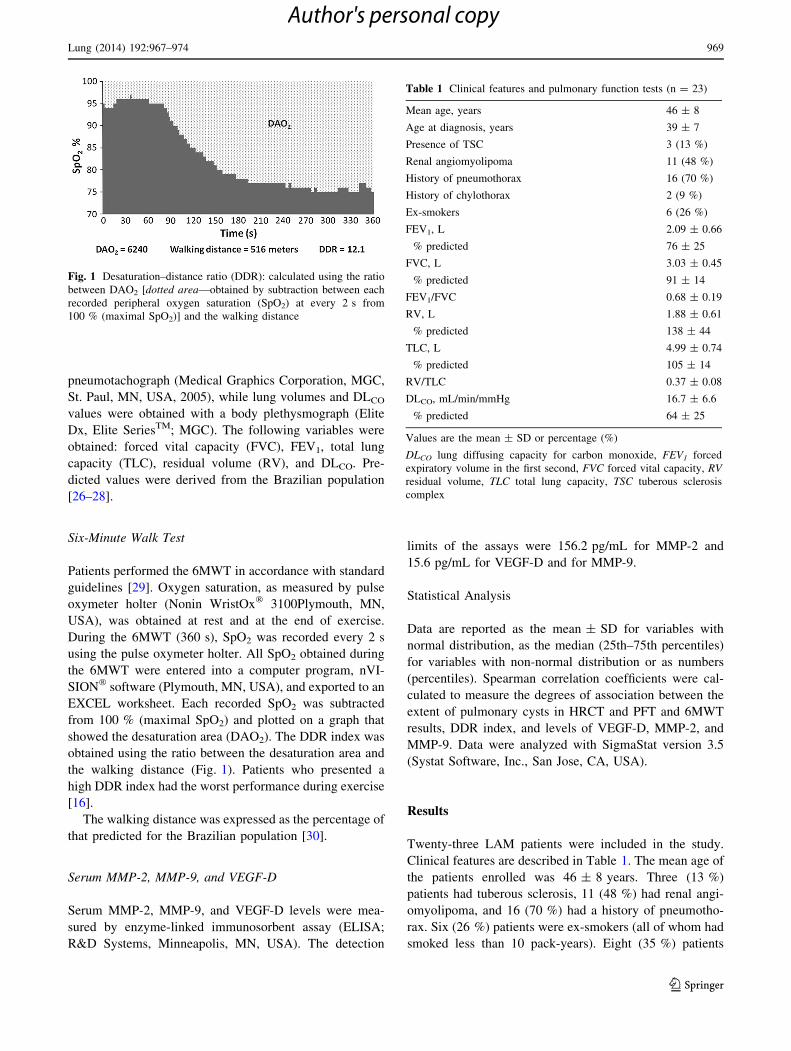
During the 6MWT (360 s), SpO2 was recorded every 2 s
using the pulse oxymeter holter. All SpO2 obtained during
the 6MWT were entered into a computer program, nVI-
SION� software (Plymouth, MN, USA), and exported to an
EXCEL worksheet. Each recorded SpO2 was subtracted
from 100 % (maximal SpO2) and plotted on a graph that
showed the desaturation area (DAO2). The DDR index was
obtained using the ratio between the desaturation area and
the walking distance (Fig. 1). Patients who presented a
high DDR index had the worst performance during exercise
[16].
The walking distance was expressed as the percentage of
that predicted for the Brazilian population [30].
Serum MMP-2, MMP-9, and VEGF-D
Serum MMP-2, MMP-9, and VEGF-D levels were mea-
sured by enzyme-linked immunosorbent assay (ELISA;
R&D Systems, Minneapolis, MN, USA). The detection
limits of the assays were 156.2 pg/mL for MMP-2 and
15.6 pg/mL for VEGF-D and for MMP-9.
Statistical Analysis
Data are reported as the mean ± SD for variables with
normal distribution, as the median (25th–75th percentiles)
for variables with non-normal distribution or as numbers
(percentiles). Spearman correlation coefficients were cal-
culated to measure the degrees of association between the
extent of pulmonary cysts in HRCT and PFT and 6MWT
results, DDR index, and levels of VEGF-D, MMP-2, and
MMP-9. Data were analyzed with SigmaStat version 3.5
(Systat Software, Inc., San Jose, CA, USA).
Results
Twenty-three LAM patients were included in the study.
Clinical features are described in Table 1. The mean age of
the patients enrolled was 46 ± 8 years. Three (13 %)
patients had tuberous sclerosis, 11 (48 %) had renal angi-
omyolipoma, and 16 (70 %) had a history of pneumotho-
rax. Six (26 %) patients were ex-smokers (all of whom had
smoked less than 10 pack-years). Eight (35 %) patients
Fig. 1 Desaturation–distance ratio (DDR): calculated using the ratio
between DAO2 [dotted area—obtained by subtraction between each
recorded peripheral oxygen saturation (SpO2) at every 2 s from
100 % (maximal SpO2)] and the walking distance
Table 1 Clinical features and pulmonary function tests (n = 23)
Mean age, years 46 ± 8
Age at diagnosis, years 39 ± 7
Presence of TSC 3 (13 %)
Renal angiomyolipoma 11 (48 %)
History of pneumothorax 16 (70 %)
History of chylothorax 2 (9 %)
Ex-smokers 6 (26 %)
FEV1, L 2.09 ± 0.66
% predicted 76 ± 25
FVC, L 3.03 ± 0.45
% predicted 91 ± 14
FEV1/FVC 0.68 ± 0.19
RV, L 1.88 ± 0.61
% predicted 138 ± 44
TLC, L 4.99 ± 0.74
% predicted 105 ± 14
RV/TLC 0.37 ± 0.08
DLCO, mL/min/mmHg 16.7 ± 6.6
% predicted 64 ± 25
Values are the mean ± SD or percentage (%)
DLCO lung diffusing capacity for carbon monoxide, FEV1 forced
expiratory volume in the first second, FVC forced vital capacity, RV
residual volume, TLC total lung capacity, TSC tuberous sclerosis
complex
Lung (2014) 192:967–974 969
123
Author's personal copy
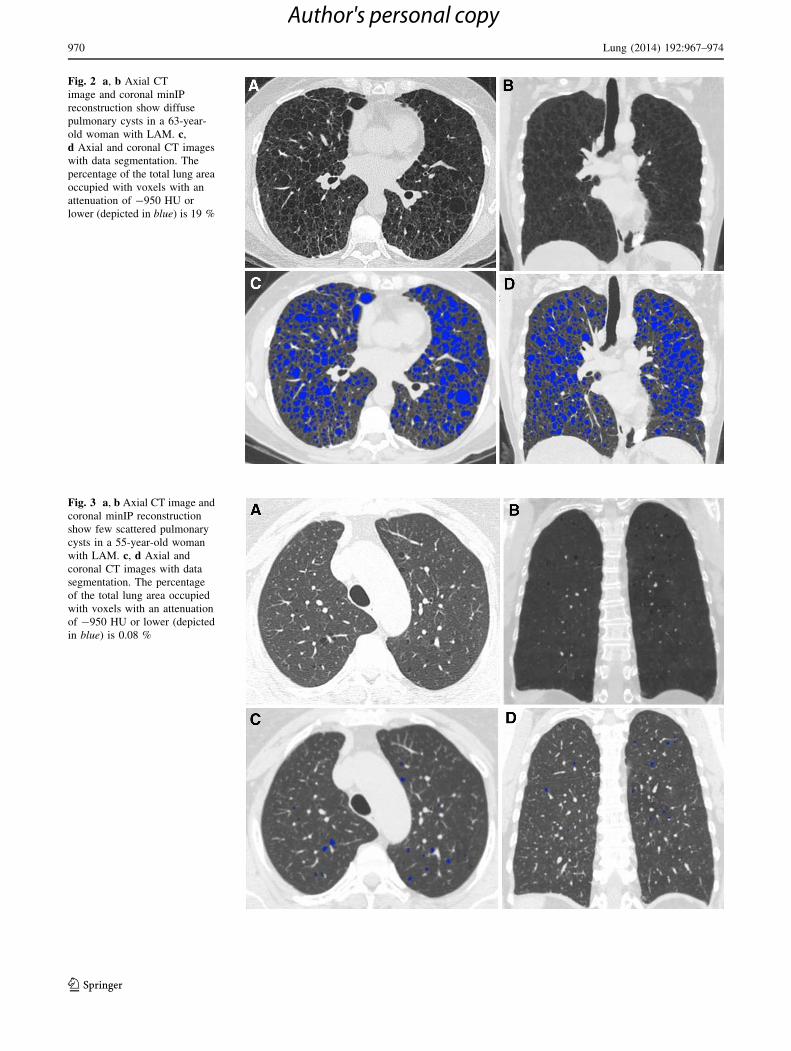
Fig. 2 a, b Axial CT
image and coronal minIP
reconstruction show diffuse
pulmonary cysts in a 63-year-
old woman with LAM. c,
d Axial and coronal CT images
with data segmentation. The
percentage of the total lung area
occupied with voxels with an
attenuation of -950 HU or
lower (depicted in blue) is 19 %
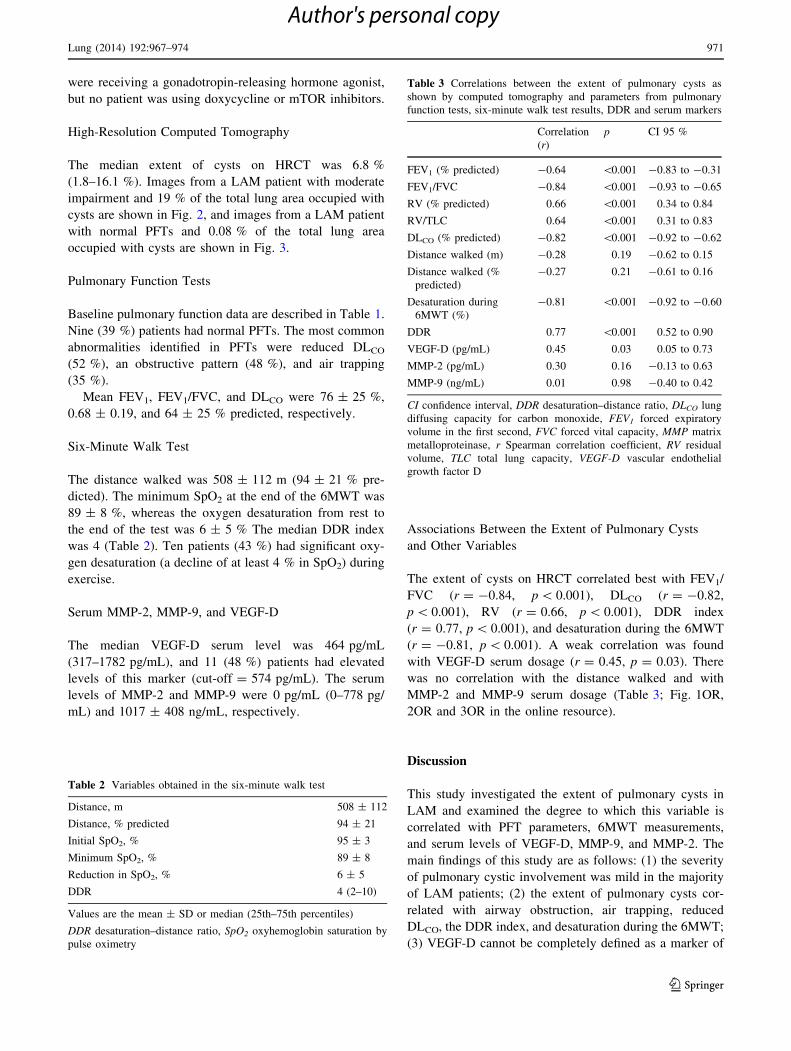
Fig. 3 a, b Axial CT image and
coronal minIP reconstruction
show few scattered pulmonary
cysts in a 55-year-old woman
with LAM. c, d Axial and
coronal CT images with data
segmentation. The percentage
of the total lung area occupied
with voxels with an attenuation
of -950 HU or lower (depicted
in blue) is 0.08 %
970 Lung (2014) 192:967–974
123
Author's personal copy
were receiving a gonadotropin-releasing hormone agonist,
but no patient was using doxycycline or mTOR inhibitors.
High-Resolution Computed Tomography
The median extent of cysts on HRCT was 6.8 %
(1.8–16.1 %). Images from a LAM patient with moderate
impairment and 19 % of the total lung area occupied with
cysts are shown in Fig. 2, and images from a LAM patient
with normal PFTs and 0.08 % of the total lung area
occupied with cysts are shown in Fig. 3.
Pulmonary Function Tests
Baseline pulmonary function data are described in Table 1.
Nine (39 %) patients had normal PFTs. The most common
abnormalities identified in PFTs were reduced DLCO
(52 %), an obstructive pattern (48 %), and air trapping
(35 %).
Mean FEV1, FEV1/FVC, and DLCO were 76 ± 25 %,
0.68 ± 0.19, and 64 ± 25 % predicted, respectively.
Six-Minute Walk Test
The distance walked was 508 ± 112 m (94 ± 21 % pre-
dicted). The minimum SpO2 at the end of the 6MWT was
89 ± 8 %, whereas the oxygen desaturation from rest to
the end of the test was 6 ± 5 % The median DDR index
was 4 (Table 2). Ten patients (43 %) had significant oxy-
gen desaturation (a decline of at least 4 % in SpO2) during
exercise.
Serum MMP-2, MMP-9, and VEGF-D
The median VEGF-D serum level was 464 pg/mL
(317–1782 pg/mL), and 11 (48 %) patients had elevated
levels of this marker (cut-off = 574 pg/mL). The serum
levels of MMP-2 and MMP-9 were 0 pg/mL (0–778 pg/
mL) and 1017 ± 408 ng/mL, respectively.
Associations Between the Extent of Pulmonary Cysts
and Other Variables
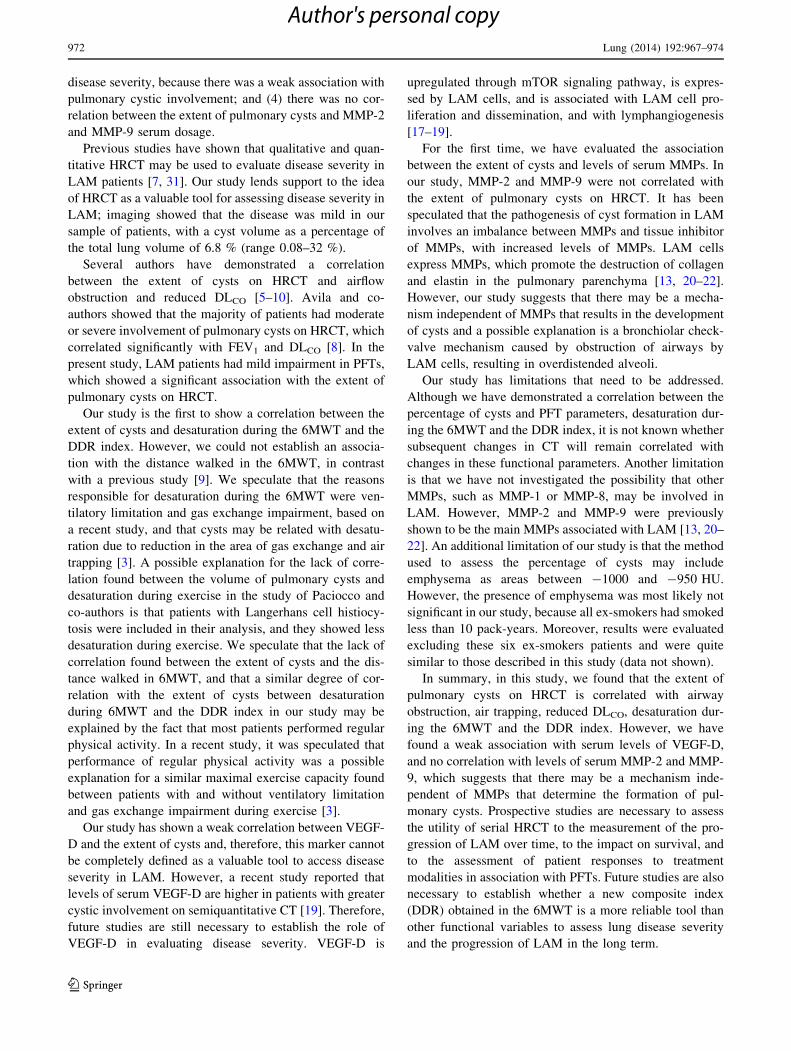
The extent of cysts on HRCT correlated best with FEV1/
FVC (r = -0.84, p \ 0.001), DLCO (r = -0.82,
p \ 0.001), RV (r = 0.66, p \ 0.001), DDR index
(r = 0.77, p \ 0.001), and desaturation during the 6MWT
(r = -0.81, p \ 0.001). A weak correlation was found
with VEGF-D serum dosage (r = 0.45, p = 0.03). There
was no correlation with the distance walked and with
MMP-2 and MMP-9 serum dosage (Table 3; Fig. 1OR,
2OR and 3OR in the online resource).
Discussion
This study investigated the extent of pulmonary cysts in
LAM and examined the degree to which this variable is
correlated with PFT parameters, 6MWT measurements,
and serum levels of VEGF-D, MMP-9, and MMP-2. The
main findings of this study are as follows: (1) the severity
of pulmonary cystic involvement was mild in the majority
of LAM patients; (2) the extent of pulmonary cysts cor-
related with airway obstruction, air trapping, reduced
DLCO, the DDR index, and desaturation during the 6MWT;
(3) VEGF-D cannot be completely defined as a marker of
Table 2 Variables obtained in the six-minute walk test
Distance, m 508 ± 112
Distance, % predicted 94 ± 21
Initial SpO2, % 95 ± 3
Minimum SpO2, % 89 ± 8
Reduction in SpO2, % 6 ± 5
DDR 4 (2–10)
Values are the mean ± SD or median (25th–75th percentiles)
DDR desaturation–distance ratio, SpO2 oxyhemoglobin saturation by
pulse oximetry
Table 3 Correlations between the extent of pulmonary cysts as
shown by computed tomography and parameters from pulmonary
function tests, six-minute walk test results, DDR and serum markers
Correlation
(r)
p CI 95 %
FEV1 (% predicted) -0.64 \0.001 -0.83 to -0.31
FEV1/FVC -0.84 \0.001 -0.93 to -0.65
RV (% predicted) 0.66 \0.001 0.34 to 0.84
RV/TLC 0.64 \0.001 0.31 to 0.83
DLCO (% predicted) -0.82 \0.001 -0.92 to -0.62
Distance walked (m) -0.28 0.19 -0.62 to 0.15
Distance walked (%
predicted)
-0.27 0.21 -0.61 to 0.16
Desaturation during
6MWT (%)
-0.81 \0.001 -0.92 to -0.60
DDR 0.77 \0.001 0.52 to 0.90
VEGF-D (pg/mL) 0.45 0.03 0.05 to 0.73
MMP-2 (pg/mL) 0.30 0.16 -0.13 to 0.63
MMP-9 (ng/mL) 0.01 0.98 -0.40 to 0.42
CI confidence interval, DDR desaturation–distance ratio, DLCO lung
diffusing capacity for carbon monoxide, FEV1 forced expiratory
volume in the first second, FVC forced vital capacity, MMP matrix
metalloproteinase, r Spearman correlation coefficient, RV residual
volume, TLC total lung capacity, VEGF-D vascular endothelial
growth factor D
Lung (2014) 192:967–974 971
123
Author's personal copy
disease severity, because there was a weak association with
pulmonary cystic involvement; and (4) there was no cor-
relation between the extent of pulmonary cysts and MMP-2
and MMP-9 serum dosage.
Previous studies have shown that qualitative and quan-
titative HRCT may be used to evaluate disease severity in
LAM patients [7, 31]. Our study lends support to the idea
of HRCT as a valuable tool for assessing disease severity in
LAM; imaging showed that the disease was mild in our
sample of patients, with a cyst volume as a percentage of
the total lung volume of 6.8 % (range 0.08–32 %).
Several authors have demonstrated a correlation
between the extent of cysts on HRCT and airflow
obstruction and reduced DLCO [5–10]. Avila and co-
authors showed that the majority of patients had moderate
or severe involvement of pulmonary cysts on HRCT, which
correlated significantly with FEV1 and DLCO [8]. In the
present study, LAM patients had mild impairment in PFTs,
which showed a significant association with the extent of
pulmonary cysts on HRCT.
Our study is the first to show a correlation between the
extent of cysts and desaturation during the 6MWT and the
DDR index. However, we could not establish an associa-
tion with the distance walked in the 6MWT, in contrast
with a previous study [9]. We speculate that the reasons
responsible for desaturation during the 6MWT were ven-
tilatory limitation and gas exchange impairment, based on
a recent study, and that cysts may be related with desatu-
ration due to reduction in the area of gas exchange and air
trapping [3]. A possible explanation for the lack of corre-
lation found between the volume of pulmonary cysts and
desaturation during exercise in the study of Paciocco and
co-authors is that patients with Langerhans cell histiocy-
tosis were included in their analysis, and they showed less
desaturation during exercise. We speculate that the lack of
correlation found between the extent of cysts and the dis-
tance walked in 6MWT, and that a similar degree of cor-
relation with the extent of cysts between desaturation
during 6MWT and the DDR index in our study may be
explained by the fact that most patients performed regular
physical activity. In a recent study, it was speculated that
performance of regular physical activity was a possible
explanation for a similar maximal exercise capacity found
between patients with and without ventilatory limitation
and gas exchange impairment during exercise [3].
Our study has shown a weak correlation between VEGF-
D and the extent of cysts and, therefore, this marker cannot
be completely defined as a valuable tool to access disease
severity in LAM. However, a recent study reported that
levels of serum VEGF-D are higher in patients with greater
cystic involvement on semiquantitative CT [19]. Therefore,
future studies are still necessary to establish the role of
VEGF-D in evaluating disease severity. VEGF-D is
upregulated through mTOR signaling pathway, is expres-
sed by LAM cells, and is associated with LAM cell pro-
liferation and dissemination, and with lymphangiogenesis
[17–19].
For the first time, we have evaluated the association
between the extent of cysts and levels of serum MMPs. In
our study, MMP-2 and MMP-9 were not correlated with
the extent of pulmonary cysts on HRCT. It has been
speculated that the pathogenesis of cyst formation in LAM
involves an imbalance between MMPs and tissue inhibitor
of MMPs, with increased levels of MMPs. LAM cells
express MMPs, which promote the destruction of collagen
and elastin in the pulmonary parenchyma [13, 20–22].
However, our study suggests that there may be a mecha-
nism independent of MMPs that results in the development
of cysts and a possible explanation is a bronchiolar check-
valve mechanism caused by obstruction of airways by
LAM cells, resulting in overdistended alveoli.
Our study has limitations that need to be addressed.
Although we have demonstrated a correlation between the
percentage of cysts and PFT parameters, desaturation dur-
ing the 6MWT and the DDR index, it is not known whether
subsequent changes in CT will remain correlated with
changes in these functional parameters. Another limitation
is that we have not investigated the possibility that other
MMPs, such as MMP-1 or MMP-8, may be involved in
LAM. However, MMP-2 and MMP-9 were previously
shown to be the main MMPs associated with LAM [13, 20–
22]. An additional limitation of our study is that the method
used to assess the percentage of cysts may include
emphysema as areas between -1000 and -950 HU.
However, the presence of emphysema was most likely not
significant in our study, because all ex-smokers had smoked
less than 10 pack-years. Moreover, results were evaluated
excluding these six ex-smokers patients and were quite
similar to those described in this study (data not shown).
In summary, in this study, we found that the extent of
pulmonary cysts on HRCT is correlated with airway
obstruction, air trapping, reduced DLCO, desaturation dur-
ing the 6MWT and the DDR index. However, we have
found a weak association with serum levels of VEGF-D,
and no correlation with levels of serum MMP-2 and MMP-
9, which suggests that there may be a mechanism inde-
pendent of MMPs that determine the formation of pul-
monary cysts. Prospective studies are necessary to assess
the utility of serial HRCT to the measurement of the pro-
gression of LAM over time, to the impact on survival, and
to the assessment of patient responses to treatment
modalities in association with PFTs. Future studies are also
necessary to establish whether a new composite index
(DDR) obtained in the 6MWT is a more reliable tool than
other functional variables to assess lung disease severity
and the progression of LAM in the long term.
972 Lung (2014) 192:967–974
123
Author's personal copy

Conflict of interest Bruno Guedes Baldi, Mariana Sponholz Ara-
ujo, Carolina Salim Goncalves Freitas, Gustavo Borges da Silva
Teles, Ronaldo Adib Kairalla, Olıvia Meira Dias, Daniel Antunes
Silva Pereira, Suzana Pinheiro Pimenta, and Carlos Roberto Ribeiro
Carvalho have no conflict of interest to declare.
References
1. Johnson SR, Cordier JF, Lazor R, Cottin V, Costabel U, Harari S,
Reynaud-Gaubert M, Boehler A, Brauner M, Popper H, Bonetti
F, Kingswood C, Review Panel of the ERS LAM Task Force
(2010) European Respiratory Society guidelines for the diagnosis
and management of lymphangioleiomyomatosis. Eur Respir J
35:14–26
2. Ryu JH, Moss J, Beck GJ, Lee JC, Brown KK, Chapman JT,
Finlay GA, Olson EJ, Ruoss SJ, Maurer JR, Raffin TA, Peavy
HH, McCarthy K, Taveira-Dasilva A, McCormack FX, Avila
NA, Decastro RM, Jacobs SS, Stylianou M, Fanburg BL, NHLBI
LAM Registry Group (2006) The NHLBI lymphangioleiomy-
omatosis registry: characteristics of 230 patients at enrollment.
Am J Respir Crit Care Med 173:105–111
3. Baldi BG, Albuquerque AL, Pimenta SP, Salge JM, Kairalla RA,
Carvalho CR (2012) Exercise performance and dynamic hyper-
inflation in lymphangioleiomyomatosis. Am J Respir Crit Care
Med 186:341–348
4. Taveira-DaSilva AM, Hedin C, Stylianou MP, Travis WD,
Matsui K, Ferrans VJ, Moss J (2001) Reversible airflow
obstruction, proliferation of abnormal smooth muscle cells, and
impairment of gas exchange as predictors of outcome in lym-
phangioleiomyomatosis. Am J Respir Crit Care Med
164:1072–1076
5. Yao J, Taveira-DaSilva AM, Colby TV, Moss J (2012) CT
grading of lung disease in lymphangioleiomyomatosis. AJR Am J
Roentgenol 199:787–793
6. Schmithorst VJ, Altes TA, Young LR, Franz DN, Bissler JJ,
McCormack FX, Dardzinski BJ, Brody AS (2009) Automated
algorithm for quantifying the extent of cystic change on volu-
metric chest CT: initial results in lymphangioleiomyomatosis.
AJR Am J Roentgenol 192:1037–1044
7. Avila NA, Kelly JA, Dwyer AJ, Johnson DL, Jones EC, Moss J
(2002) Lymphangioleiomyomatosis: correlation of qualitative
and quantitative thin-section CT with pulmonary function tests
and assessment of dependence on pleurodesis. Radiology
223:189–197
8. Avila NA, Chen CC, Chu SC, Wu M, Jones EC, Neumann RD,
Moss J (2000) Pulmonary lymphangioleiomyomatosis: correla-
tion of ventilation-perfusion scintigraphy, chest radiography, and
CT with pulmonary function tests. Radiology 214:441–446
9. Paciocco G, Uslenghi E, Bianchi A, Mazzarella G, Roviaro GC,
Vecchi G, Harari S (2004) Diffuse cystic lung diseases: corre-
lation between radiologic and functional status. Chest
125:135–142
10. Crausman RS, Lynch DA, Mortenson RL, King TE Jr, Irvin CG,
Hale VA, Newell JD Jr (1996) Quantitative CT predicts the
severity of physiologic dysfunction in patients with lymphan-
gioleiomyomatosis. Chest 109:131–137
11. Taveira-DaSilva AM, Pacheco-Rodriguez G, Moss J (2010) The
natural history of lymphangioleiomyomatosis: markers of sever-
ity, rate of progression and prognosis. Lymphat Res Biol 8:9–19
12. McCormack FX, Inoue Y, Moss J, Singer LG, Strange C, Nakata
K, Barker AF, Chapman JT, Brantly ML, Stocks JM, Brown KK,
Lynch JP 3rd, Goldberg HJ, Young LR, Kinder BW, Downey GP,
Sullivan EJ, Colby TV, McKay RT, Cohen MM, Korbee L,
Taveira-DaSilva AM, Lee HS, Krischer JP, Trapnell BC,
National Institutes of Health Rare Lung Diseases Consortium,
MILES Trial Group (2011) Efficacy and safety of sirolimus in
lymphangioleiomyomatosis. N Engl J Med 364:1595–1606
13. Pimenta SP, Baldi BG, Kairalla RA, Carvalho CR (2013)
Doxycycline use in patients with lymphangioleiomyomatosis:
biomarkers and pulmonary function response. J Bras Pneumol
39:5–15
14. Matsui K, Beasley MB, Nelson WK, Barnes PM, Bechtle J, Falk
R, Ferrans VJ, Moss J, Travis WD (2001) Prognostic significance
of pulmonary lymphangioleiomyomatosis histologic score. Am J
Surg Pathol 25:479–484
15. Taveira-DaSilva AM, Stylianou MP, Hedin CJ, Kristof AS, Avila
NA, Rabel A, Travis WD, Moss J (2003) Maximal oxygen uptake
and severity of disease in lymphangioleiomyomatosis. Am J
Respir Crit Care Med 168:1427–1431
16. Pimenta SP, Rocha RB, Baldi BG, Kawassaki AM, Kairalla RA,
Carvalho CR (2010) Desaturation–distance ratio: a new concept
for a functional assessment of interstitial lung diseases. Clinics
65:841–846
17. Young LR, Vandyke R, Gulleman PM, Inoue Y, Brown KK,
Schmidt LS, Linehan WM, Hajjar F, Kinder BW, Trapnell BC,
Bissler JJ, Franz DN, McCormack FX (2010) Serum vascular
endothelial growth factor-D prospectively distinguishes lym-
phangioleiomyomatosis from other diseases. Chest 138:674–681
18. Young L, Lee HS, Inoue Y, Moss J, Singer LG, Strange C,
Nakata K, Barker AF, Chapman JT, Brantly ML, Stocks JM,
Brown KK, Lynch JP 3rd, Goldberg HJ, Downey GP, Swigris JJ,
Taveira-DaSilva AM, Krischer JP, Trapnell BC, McCormack FX,
MILES Trial Group (2013) Serum VEGF-D a concentration as a
biomarker of lymphangioleiomyomatosis severity and treatment
response: a prospective analysis of the Multicenter International
Lymphangioleiomyomatosis Efficacy of Sirolimus (MILES) trial.
Lancet Respir Med 1:445–452
19. Xu KF, Zhang P, Tian X, Ma A, Li X, Zhou J, Zeng N, Gui YS,
Guo Z, Feng R, Zhang W, Sun W, Cai B (2013) The role of
vascular endothelial growth factor-D in diagnosis of lymphan-
gioleiomyomatosis (LAM). Respir Med 107:263–268
20. Odajima N, Betsuyaku T, Nasuhara Y, Inoue H, Seyama K, Ni-
shimura M (2009) Matrix metalloproteinases in blood from
patients with LAM. Respir Med 103:124–129
21. Hayashi T, Fleming MV, Stetler-Stevenson WG, Liotta LA, Moss
J, Ferrans VJ, Travis WD (1997) Immunohistochemical study of
matrix metalloproteinases (MMPs) and their tissue inhibitors
(TIMPs) in pulmonary lymphangioleiomyomatosis (LAM). Hum
Pathol 28:1071–1078
22. Pimenta SP, Baldi BG, Acencio MM, Kairalla RA, Carvalho CR
(2011) Doxycycline use in patients with lymphangioleiomy-
omatosis: safety and efficacy in metalloproteinase blockade.
J Bras Pneumol 37:424–430
23. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R,
Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P,
Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D,
Pedersen OF, Pellegrino R, Viegi G, Wanger J, ATS/ERS Task
Force (2005) Standardisation of spirometry. Eur Respir J
26:319–338
24. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V,
Burgos F, Casaburi R, Crapo R, Enright P, van der Grinten CP,
Gustafsson P, Hankinson J, Jensen R, Johnson D, Macintyre N,
McKay R, Miller MR, Navajas D, Pellegrino R, Viegi G, ATS/
ERS Task Force (2005) Standardisation of the measurement of
lung volumes. Eur Respir J 26:511–522
25. Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten
CP, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P,
Gustafsson P, Hankinson J, Jensen R, McKay R, Miller MR,
Navajas D, Pedersen OF, Pellegrino R, Wanger J, ATS/ERS Task
Lung (2014) 192:967–974 973
123
Author's personal copy

Force (2005) Standardisation of the single-breath determination
of carbon monoxide uptake in the lung. Eur Respir J 26:720–735
26. Pereira CA, Sato T, Rodrigues SC (2007) New reference values
for forced spirometry in white adults in Brazil. J Bras Pneumol
33:397–406
27. Neder JA, Andreoni S, Castelo-Filho A, Nery LE (1999) Refer-
ence values for lung function tests. I. Static volumes. Braz J Med
Biol Res 32:703–717
28. Neder JA, Andreoni S, Peres C, Nery LE (1999) Reference values
for lung function tests. III. Carbon monoxide diffusing capacity
(transfer factor). Braz J Med Biol Res 32:729–737
29. Ats A (2002) ATS statement: guidelines for the six-minute walk
test. Am J Respir Crit Care Med 166:111–117
30. Soares MR, Pereira CAC (2011) Six-minute walk test: reference
values for healthy adults in Brazil. J Bras Pneumol 37:576–583
31. Tobino K, Hirai T, Johkoh T, Kurihara M, Fujimoto K, Tomiyama
N, Mishima M, Takahashi K, Seyama K (2012) Differentiation
between Birt–Hogg–Dube syndrome and lymphangioleiomy-
omatosis: quantitative analysis of pulmonary cysts on computed
tomography of the chest in 66 females. Eur J Radiol
81:1340–1346
974 Lung (2014) 192:967–974
123
Author's personal copy