Evaluation of Normothermic Ischemia and Simple Cold Preservation Injury in Pig Kidney by Proton...
10
JOURNAL OF SURGICAL RESEARCH 68, 116–125 (1997) ARTICLE NO. JR964988 Evaluation of Normothermic Ischemia and Simple Cold Preservation Injury in Pig Kidney by Proton Nuclear Magnetic Resonance Spectroscopy 1 Thierry Hauet, M.D.,* , ² Denis Mothes, M.D.,* Jean Michel Goujon, M.D.,* Jean Claude Caritez, Ph.D.,* Laurence Le Moyec, Ph.D.,² Michel Carretier, M.D.,* and Michel Eugene, M.D., Ph.D.² *Laboratoire de Chirurgie Experimentale, Institut Nationale de Recherche Agronomique, Le Magneraud, 17000 Surgeres, France; and ²Laboratoire de RMN et Exploration Fonctionnelle, Hopital Saint Louis, 75010 Paris, France Submitted for publication July 9, 1996 INTRODUCTION The isolated perfused pig kidney (IPK) model was used to mimick the non-heart-beating donor situation. The current shortage of transplantable organs has This model was performed to assess initial renal func- caused a renewal of interest in kidneys obtained from tions after normothermic ischemia, cold flush, and 24 non-heart-beating (NHB) donors. A NHB donor is de- hr cold-storage preservation (CSP) with Euro-Collins fined as a donor whose cardiopulmonary function has and to determine normothermic ischemia and reperfu- totally ceased before arriving in the operating room. Kid- sion impairment by biochemical, histological, and pro- neys and other organs from these donors have suffered ton nuclear magnetic resonance (NMR) spectroscopy warm ischemia. Current preservation methods, how- analysis. Twenty-four pig kidneys were used. There ever, seem less appropriate to prevent damage during were three experimental groups: Group 1 (G1), control the storage of ischemic donor kidneys. The deleterious kidneys flushed with cold heparinized saline and im- effect of the combination of normothermic ischemia be- mediately perfused; Group 2 (G2), cold flush followed fore hypothermic storage is not yet satisfactorily re- by 24 hr CSP and reperfusion; and Group 3 (G3), 30 duced by preservation techniques [1]. The transplanta- min of normothermic ischemia followed by cold flush tion of kidneys from NHB donors has been reported by and 24 hr CSP and reperfusion. Kidneys were perfused few kidney transplant centers [2, 3], but overall graft for 2 hr at 37.57C for functional evaluation. Perfusate survival was not comparable to currently acceptable re- flow rate is significantly different for G3 (P õ 0.01). sults [4]. Moreover, all transplanted kidneys suffer some Glomerular filtration rate is less in G3 (P õ 0.05). Frac- unavoidable injury during procurement and transplant tional reabsorptions of sodium (FRNa / ) and glucose surgery. Allografts from cadaveric donors suffer addi- (Glc) excretion in urine are different in G3 (P õ 0.01 tional injury both from the hemodynamic instability as- and P õ 0.05, respectively). Amino acid excretion in sociated with the acute illness or trauma which caused NMR spectroscopy was higher in G3 (P õ 0.05). Ele- brain death of the donor and from the cold storage of vated levels of trimethylamine-N-oxide (TMAO) and the kidney while in transit to the recipient. Delayed lactate (Lac) were detected by proton NMR spectros- graft function (DGF) after renal transplantation re- copy in G2 and particularly G3. A peak is present in mains an important complication [5 – 7]. The mean risks G3 and related with poor glomerular and tubular func- affecting graft survival are acute tubular necrosis (ATN) tions and worse histological data. Malondialdehyde and rejection crisis. The incidence of ATN in cadaver tissue level was higher in G3. This study shows that the kidneys is 10 to 40% [7, 8] and may also influence the IPK with proton NMR spectroscopy may be a useful rejection crisis and graft survival [9, 10]. For these pa- method in the evaluation of kidneys after cold isch- tients, DGF entails a reinstitution of dialysis and reex- emia and transplantation. This model might be suit- posure to the associated morbidity and prolongation of able for a variety of experimental protocols, particu- hospital stay. DGF considerably increases the trans- larly to improve functional performance after isch- plantation cost to society and the social security system emia and reperfusion. q 1997 Academic Press [5, 6]. Currently, for the clinician, there are no clinically useful, practical, or noninvasive methods to assess the extent of kidney tubular degeneration of cold-stored kid- neys either before or at the time of removal, during their 1 This work was performed with research grants from the Ministry of Research 92C0746 and from Paris 7 University. storage, or after their transplantation. Recent studies 116 0022-4804/97 $25.00 Copyright q 1997 by Academic Press All rights of reproduction in any form reserved. AID JSR 4988 / 6n1c$$$$21 05-16-97 00:50:39 srgas
-
Upload
univ-poitiers -
Category
Documents
-
view
6 -
download
0
Transcript of Evaluation of Normothermic Ischemia and Simple Cold Preservation Injury in Pig Kidney by Proton...

JOURNAL OF SURGICAL RESEARCH 68, 116–125 (1997)ARTICLE NO. JR964988
Evaluation of Normothermic Ischemia and Simple Cold PreservationInjury in Pig Kidney by Proton Nuclear Magnetic
Resonance Spectroscopy1
Thierry Hauet, M.D.,*,† Denis Mothes, M.D.,* Jean Michel Goujon, M.D.,* Jean Claude Caritez, Ph.D.,*Laurence Le Moyec, Ph.D.,† Michel Carretier, M.D.,* and Michel Eugene, M.D., Ph.D.†
*Laboratoire de Chirurgie Experimentale, Institut Nationale de Recherche Agronomique, Le Magneraud, 17000 Surgeres, France; and†Laboratoire de RMN et Exploration Fonctionnelle, Hopital Saint Louis, 75010 Paris, France
Submitted for publication July 9, 1996
INTRODUCTIONThe isolated perfused pig kidney (IPK) model was
used to mimick the non-heart-beating donor situation. The current shortage of transplantable organs hasThis model was performed to assess initial renal func- caused a renewal of interest in kidneys obtained fromtions after normothermic ischemia, cold flush, and 24 non-heart-beating (NHB) donors. A NHB donor is de-hr cold-storage preservation (CSP) with Euro-Collins fined as a donor whose cardiopulmonary function hasand to determine normothermic ischemia and reperfu- totally ceased before arriving in the operating room. Kid-sion impairment by biochemical, histological, and pro- neys and other organs from these donors have sufferedton nuclear magnetic resonance (NMR) spectroscopy warm ischemia. Current preservation methods, how-analysis. Twenty-four pig kidneys were used. There ever, seem less appropriate to prevent damage duringwere three experimental groups: Group 1 (G1), control the storage of ischemic donor kidneys. The deleteriouskidneys flushed with cold heparinized saline and im- effect of the combination of normothermic ischemia be-mediately perfused; Group 2 (G2), cold flush followed fore hypothermic storage is not yet satisfactorily re-by 24 hr CSP and reperfusion; and Group 3 (G3), 30 duced by preservation techniques [1]. The transplanta-min of normothermic ischemia followed by cold flush tion of kidneys from NHB donors has been reported byand 24 hr CSP and reperfusion. Kidneys were perfused few kidney transplant centers [2, 3], but overall graftfor 2 hr at 37.57C for functional evaluation. Perfusate survival was not comparable to currently acceptable re-flow rate is significantly different for G3 (P õ 0.01). sults [4]. Moreover, all transplanted kidneys suffer someGlomerular filtration rate is less in G3 (Põ 0.05). Frac- unavoidable injury during procurement and transplanttional reabsorptions of sodium (FRNa/) and glucose
surgery. Allografts from cadaveric donors suffer addi-(Glc) excretion in urine are different in G3 (P õ 0.01tional injury both from the hemodynamic instability as-and P õ 0.05, respectively). Amino acid excretion insociated with the acute illness or trauma which causedNMR spectroscopy was higher in G3 (P õ 0.05). Ele-brain death of the donor and from the cold storage ofvated levels of trimethylamine-N-oxide (TMAO) andthe kidney while in transit to the recipient. Delayedlactate (Lac) were detected by proton NMR spectros-graft function (DGF) after renal transplantation re-copy in G2 and particularly G3. A peak is present inmains an important complication [5–7]. The mean risksG3 and related with poor glomerular and tubular func-affecting graft survival are acute tubular necrosis (ATN)tions and worse histological data. Malondialdehydeand rejection crisis. The incidence of ATN in cadavertissue level was higher in G3. This study shows that thekidneys is 10 to 40% [7, 8] and may also influence theIPK with proton NMR spectroscopy may be a usefulrejection crisis and graft survival [9, 10]. For these pa-method in the evaluation of kidneys after cold isch-tients, DGF entails a reinstitution of dialysis and reex-emia and transplantation. This model might be suit-posure to the associated morbidity and prolongation ofable for a variety of experimental protocols, particu-hospital stay. DGF considerably increases the trans-larly to improve functional performance after isch-plantation cost to society and the social security systememia and reperfusion. q 1997 Academic Press
[5, 6]. Currently, for the clinician, there are no clinicallyuseful, practical, or noninvasive methods to assess theextent of kidney tubular degeneration of cold-stored kid-neys either before or at the time of removal, during their1 This work was performed with research grants from the Ministry
of Research 92C0746 and from Paris 7 University. storage, or after their transplantation. Recent studies
1160022-4804/97 $25.00Copyright q 1997 by Academic PressAll rights of reproduction in any form reserved.
AID JSR 4988 / 6n1c$$$$21 05-16-97 00:50:39 srgas

117HAUET ET AL.: ASSESSMENT OF NORMOTHERMIC ISCHEMIA AND COLD STORAGE LESIONS
24 hr of cold-storage preservation (CSP). The pigs were randomizedhave demonstrated that the ischemic injury occurringinto three groups: (1) n Å 6, immediately reperfused after cold flushin the course of syngeneic renal transplant caused the(Group 1, control); (2) nÅ 9, cold flush followed by 24 hr of CSP (Groupincreased expression of adhesion molecules on the epi- 2); and (3) n Å 9, 30 min of normothermic ischemia then cold flush
thelium [11]. In addition, ischemia causes renal tubule followed by 24 hr of CSP (Group 3).cells to increase their expression of major histocompati- Isolated kidney perfusion system. After harvesting or at the end of
the hypothermic storage, the kidneys were weighed again and perfusedbility complex class II molecules [12].via renal artery with warmed (377C) and continuously gassed (95%High-resolution proton NMR spectroscopy can be usedO2–5% CO2) freshly prepared Kreb’s solution containing the followingfor the rapid multicomponent analysis of low molecular(in mmol/liter) adjusted at pH 7.40: 140 Na/, 25 HCO0
3 , 4.9 K/, 123compounds in small amounts (about 0.5 ml) of biological Cl0, 1.2 Mg2/, 2.2 Ca2/, 1.2 ionic Ca, 1.2 Mg2/, 1.2 inorganic phos-fluids [13, 14]. It is also a powerful technique to explore phates, 1.2 sulfates, 11 D-glucose, and 5.0 g/100 ml of bovine serum
albumin (fraction V, Sigma, St. Louis, MO) and 10 mg/liter creatininedynamic intermolecular interactions occurring within(Sigma) for determination of the glomerular filtration rate (GFR). Tothese fluids [15, 16]. An important analytical advantageimprove the stability of the tubular function and to assess proximalof NMR spectroscopy is that it provides a rapid, nonde-tubule cell function, a mixture of 22 L-amino acids in concentrationsstructive, and noninvasive analysis of metabolites pres- between 0.2 and 2.0 mM/liter was added using a commercial solution
ent at the millimolar level without preselection of instru- (Clintec Nutrition Clinique, Sevres, France). The solution was perfusedin a closed thermostatically controlled circuit. Perfusion flow ratemental conditions in small samples of untreated bioflu-(PFR) was adjusted to maintain renal arterial perfusion pressure (PP)ids [17]. When renal damage is present in humans orat 100 mm Hg. Perfusion was provided by a peristaltic pump (BSM 1,animals, the low-molecular-weight metabolite profile ofHospal, Lyon, France). PP was measured by a pressure transducerurine is significantly altered, and this is closely reflected (Statham P23 Dc, Grass, Quincy, MA). The outflow from the pump
in the proton NMR spectra [18–20]. passed through a hollow fiber-type oxygenator (0600 ECM, Sci-med,The aim of the present investigation was to evaluate Minneapolis, MN). Fifteen minutes after initiating perfusion, when a
steady state had been achieved, PFR, GFR, fractional reabsorption ofthe ability of proton NMR spectroscopy to study cold-sodium (FRNa/), release of lactic dehydrogenase (LDH, measured bystored kidney function after normothermic ischemiaNADH oxidation), pH in urine (APX70 pH-meter IFSET, Labo-mod-mimicking the clinical situation from NHB donors. The erne, Paris, France), and N-acetyl-b-D-glucosaminidase (NAG, mea-
study was conducted in a normothermic IPK model pre- sured by N-A-G Kit, Thames Genelink, Surrey, UK) in urine wereviously described [21], after cold storage. This model monitored at t15, t30, t45, t60, t90, and t120 during reperfusion. GFR
was evaluated from creatinine clearance using the formula GFR Åhas numerous advantages. Experiments are relativelyUrine flow rate 1 urine creatinine/perfusate creatinine. FRNa/ wassimple, rapid, and inexpensive. Evaluation methodscalculated using the formula FRNa/ Å 100 1 (1- urine Na//perfusateare reproducible and much more accurate than other Na/ 1 perfusate creatinine/urine creatinine. Citrate excretion in urine
models [22]. The IPK has become a useful method to and Lac excretion in perfusate were determined by biochemical meth-study the effects of the combination of hypothermic ods (Boerhinger Mabbheim Biochemicals, Germany). Amino acid uria
was determined by chromatographic technique. Urine and perfusatepreservation and normothermic reperfusion on renalsamples were also studied with proton NMR spectroscopy. After nor-function and metabolism [23].mothermic reperfusion, a slice from whole kidney was uniformlyminced with a razor blade and homogenized in 0.15% KCl solution.Fatty acid peroxidation was evaluated by renal tissue levels of malondi-MATERIALS AND METHODSaldehyde (MDA) and measured with thiobarbituric acid test [23, 24].An aliquot of renal tissue homogenate was heated with thiobarbituricAnimals. Large white male pigs weighing 30–35 kg were usedacid under acidic conditions and pink color formation measured at 530for the experiments (INRA Le Magneraud, Surgeres, France).nm. Results are presented as mmol of MDA per milligram of protein.
Cold-storage solutions. A standard Euro-Collins (EC) solution Protein contents was measured with Lowry’s technique (25).was studied. EC solution was manufactured by Pharmacie Centrale
NMR spectroscopy. The spectra were acquired at 400 MHz on ades Hopitaux (Paris, France) and supplied in 1-liter bottles. TheBruker AM400WB spectrometer. The experiments were performed incomposition of the solution used was as follows (mmol): 10 Na/, 1155-mm NMR tubes and samples were added with 10% D2O containingK/, 15 Cl0, 10 HCO0
3 , 15 HPO204 , 195 glucose. Osmolality was 355
0.75% TSP [sodium 3-(trimethyl-2,2,3,3)-1-propionate] to referencemosm and pH was 7.0.the chemical shifts (0 ppm). The water signal was suppressed by the
Experimental protocols. General anesthesia was induced with mi- presaturation technique (0.08 W for 2 sec). Spectra were acquireddazolam in a dose of 6 mg intravenously and with 2.0% halothane with 16K data points for a spectral width of 6024 Hz with a 5-msecand 6 liters/min oxygen via a mask prior to intubation and ventilation. pulse (607) and 128 scans were accumulated. The Fourier transformGeneral endotracheal anesthesia was maintained with halothane
was performed on 16K data points without filtering. Resonances were(1.0–1.5%), oxygene (6 liters/min), atropine sulfate (10 mg/kg iv), andidentified from the literature chemical shift data or by addition ofpancuronium bromide (0.1 mg/kg iv). Intraoperative monitoring wasstandard compounds when necessary. For urine spectra, the maincarried out by means of an electrocardiogram and a central venousresonances identified were creatinine (Ct), glucose (Glc), alanineline was placed into the internal jugular vein. During the surgical(Ala), valine (Val), leucine/isoleucine (leu/ileu), lactate (Lac), acetateprocedure animals received 1000 ml 0.9% saline intravenously. Both(Ace), hydroxybutyrate (OHB), citrate, and trimethylamine-N-oxidekidneys were exposed through a midline abdominal incision and care-(TMAO). Concentrations were related to Ct and expressed as mmol/fully freed from perirenal tissue and fat. Immediately after a kidneymol of Ct. Typical spectra of each experimental group are shown onwas harvested, the renal artery was canulated and the blood wasFigs. 1a and 1b. Amino acid excretion and renal glucose excretionflushed out. In one experimental group, the vessel pedicle of the kid-rates were also evaluated with the ratios of Glc, Ala, and Val to Ct.neys was cross-clamped for 30 min before removal to induce normo-
Histopathological examination. At the end of cold flush, after 24thermic renal ischemia. Control kidneys were flushed in situ with coldhr cold storage and reperfusion kidney samples were collected for(47C) heparinized saline. In the two experimental groups, kidneyslight and electron microscopy. Samples were fixed with Dubosq-Bra-were flushed in situ with 1000 ml of cold (47C) EC solution. The kid-zil and 10% formalin in 0.01 mmol/liter phosphate buffer (pH 7.42)neys were weighed and prepared for reperfusion or placed (in double
plastic bags on ice) in a further 500 ml of the flush solution at 47C for and embedded in paraffin. Conventional stains were applied (hema-
AID JSR 4988 / 6n1c$$$$21 05-16-97 00:50:39 srgas

118 JOURNAL OF SURGICAL RESEARCH: VOL. 68, NO. 2, MARCH 1997
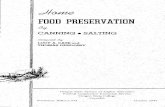
FIG. 1. (a, b) Proton NMR spectra from the urine of isolated perfused pig kidney after immediate reperfusion (G1) and a 24-hr cold-storage preservation without warm ischemia (G2) and with (G3) 1, glucose (Glc); 2, trimethylamine-N-oxide (TMAO); 3, creatinine (Ct); 4,citrate; 5, acetate (Ace); 6, alanine (Ala); 7, threonine and lactate (Thre / Lac); 8, hydroxybutirate (OHB); 9, valine and leucine/isoleucine(Val/Leu/Ileu); and peak X.
toxylin and eosin, periodic acid–Schiff). Analysis of cellular ultra- When a nonparametric test was needed, the Kruskall–Wallis analy-sis was used. Significant results were determined by P õ 0.05.structure using electron microscopy was also performed at the same
periods. Small pieces of renal tissue were fixed in 2.5% glutaralde-hyde, washed, and postfixed in 2% osmium tetroxide for 2 hr at 47C.
RESULTSAfter dehydration with ethanol, they were embedded in araldite.Ultrathin sections were stained with uranyl acetate and lead citrateand then examined under an electron microscope (JECL 100 CX, Perfusate flow rate and kidney weight. The PFR forTokyo, Japan). Histology was performed by a pathologist blind to each group at 15, 60, and 120 min is shown in Fig. 2.experimental conditions. Histological lesions were graded: 1, no ab- PFR for G1 and G2 was significantly different and alsonormality; 2, mild lesions affecting 10% of kidney samples; 3, lesions
for group G3 (P õ 0.01 at t15, t60, and t120). Theaffecting 25% of kidney samples; 4, lesions affecting 50% of kidneyweight variation before and after reperfusion was sig-samples; and 5, lesions affecting more than 75% of kidney samples.
The purpose of histopathological analysis was to evaluate morpholog- nificantly less important in G1 and G2 (Fig. 2).ical alterations after cold flush and 24 hr cold storage on proximal Tubular function and glomerular filtration rate. Re-tubular cells and particularly brush border.
sults are presented in Figs. 3a and 3b. Amino acid reab-Statistical analysis. Data are presented as means { standardsorption significantly decreased for G3 at t15, t60, anderror of the mean (SEM) and compared by using variance analysis
and the Student–Newman–Keuls test for multiple comparisons. t120 with NMR spectroscopy analysis. Cold-stored kid-
AID JSR 4988 / 6n1c$$$$22 05-16-97 00:50:39 srgas

119HAUET ET AL.: ASSESSMENT OF NORMOTHERMIC ISCHEMIA AND COLD STORAGE LESIONS
FIG. 1—Continued
neys after normothermic ischemia had significantly groups with normothermic ischemia and 24 hr CSP(Table 1).lower FRNa/. Glucose in urine showed a significantly
lower mean excretion in G2 and control and pH was Histological data. In optical microscopy, morpho-higher in G3. GFR after 15, 60, and 120 min was sig- logical studies showed that kidneys from the controlnificantly less for G3. group displayed normal renal architecture after cold
Tubular injury markers. Results are shown in flush. At the end of normothermic reperfusion, an ul-Figs. 4a and 4b. At t15, t60, and t120, LDH was sig- trastructural study of control kidneys exhibited onlynificantly greater for G3. NAG was significantly very localized edema and tubular dilatation. After 24greater in G3 after 15, 60, and 120 min of reperfusion. hr cold storage, the kidneys preserved with EC afterNMR spectroscopy exhibited that lactate release was normothermic ischemia presented with vacuolizationsignificantly less with G2 and control. In spectra, and a necrosis mean score higher than 75% of theTMAO was significantly more important with G2 and examined sample. In electron microscopy, we notedparticularly with G3 after normothermic ischemia. A 50% tubular desquamation and dilatation. The ultra-marker, imprecisely detected in our data bank, was structural study showed disruption of brush borderobserved in urine from kidneys after combination of and large interstitial edema. After cold preservationnormothermic ischemia and cold-storage preserva- and reperfusion, changes in the tubular structure,tion (peak X). sloughing of tubular cells, cast formation, and inter-
stitial edema were significantly lower with G2. WeRenal malondialdehyde production. After normo-thermic reperfusion, MDA tissue levels were higher in observed that mitochondrial depletion and disinte-
AID JSR 4988 / 6n1c$$$$23 05-16-97 00:50:39 srgas

120 JOURNAL OF SURGICAL RESEARCH: VOL. 68, NO. 2, MARCH 1997
transplantation. PP was 100 mm Hg because due tothe low viscosity of the perfusion fluid and the absenceof red blood cells, a high perfusate flow is necessary toensure physiological perfusion pressure. The deleteri-ous effect of the combination of normothermic ischemiaand cold storage on cell swelling, vascular resistance,glomerular filtration, tubular functions, and tubularinjuries has been clearly demonstrated in G3. Glomeru-lar filtration and PFR dramatically decreased after coldstorage (G2) and particularly after normothermic isch-emia (G3). Consequently in G2 and G3, vascular resis-tances during reperfusion are higher and related to amore important interstitial edema. Tubular functionsare also impaired after cold storage and normothermicischemia. FRNa/, pH in urine, and Glc excretion areconnected with lesions in the proximal tubule whichis the predominant site of renal sodium and glucosereabsorption. Urine Glc excretion rates are increasedin G3 and particularly in G2. FRNa/ reflecting Na/-K/-ATPase activity decreased in G3 and G2. These resultsdemonstrate that proximal tubule functions are lessefficient after cold ischemia and normothermic isch-emia. Urinary enzyme excretions which are related totubular injuries (bNAG and LDH) are more importantwith G3 and G2 according to functional parametersand histological studies. Moreover, EC solution offersa poor renal preservation ability, either after cold isch-emia or after combination of normothermic and coldischemia. This high K/-containing solution can induceFIG. 2. Weight variation after 24 hr cold storage and 2 hr reper-severe specific endothelial damage. EC may cause afusion (%). Perfusate flow rate after t15, t60, and t120 during reperfu-depolarization of the epithelial cell membrane and cansion (ml/min/g of tissue).lead to rapid cellular swelling. This phenomenon couldlead to impaired proximal tubular function. These re-sults using EC agree with those of recent studies using
gration were significantly higher with G3 (50%). In an isolated perfused organ technique [21–23, 28]. Inthe group with normothermic ischemia and CSP, tu- our model, renal malondialdehyde production, an indexbular morphometry revealed structural injury very of lipid peroxidation due to oxygen-free radicals, wassevere in proximal tubules and tubular cell brush bor- high in G3. The main source of oxygen-free radicals isder more impaired (Fig. 5). A high percentage (ú75%) endothelial cells but leukocytes play a major role inof proximal tubular cells exhibited necrosis, vacuoli- ischemic reperfusion injury by interaction with the en-zation, and interstitial edema. Results are presented dothelial cell. This model is cell free and there is noin Table 1. participation of leukocytes during reperfusion. Thus,
the ischemic reperfusion injury is only due to the endo-DISCUSSION thelial cell.
In situations where renal damage is present in hu-mans or animals, the metabolite profile of urine is sig-For this experimental model, we chose to use a pig
model of IPK for the following reasons. First, when nificantly altered and reflected in proton NMR spectraand can give information on the site and mechanism ofcompared with the classical canine or rat models, the
pig is more closely related to the human in terms of renal damage [15, 16]. In the present study, spectrafrom urine show many signals detected with a few min-functional renal physiology and anatomy [26]. Second,
the pig kidney is more susceptible to preservation in- utes of total scanning time. The high spectral informa-tion density from a wide range of chemical classes ofjury, and it is therefore a more sensitive model [27].
The IPK model is also interesting to limit in vivo exper- endogenous metabolites gives indications on the rela-tive activities of many cellular biochemical pathways.imental mammalian experiments. In this study, the
IPK model has been used to examine the functional, Proton NMR spectroscopy in biofluid biochemistry hasled to the discovery of new nephron damage markersmetabolic, and morphological effects of the normother-
mic ischemia before cold storage in a standard preser- such as TMAO associated with medullary injuries, lac-tate which proves that global ischemia and acetate pre-vation solution (EC). EC is used because it is one of
the two standard solutions, with UW, in use for renal cisely correlated with cortical lesions [15, 16, 20].
AID JSR 4988 / 6n1c$$$$23 05-16-97 00:50:39 srgas

121HAUET ET AL.: ASSESSMENT OF NORMOTHERMIC ISCHEMIA AND COLD STORAGE LESIONS
FIG. 3. (a, b) Tubular function and glomerular filtration. Functional results achieved 15, 60, and 120 min (t15, t60, t120) duringreperfusion with an isolated perfused pig kidney technique after a 24-hr cold storage with Eurocollins (G2 and G3) and no cold storage(G1). Results are mean values { SEM of Ala/Ct and Glc/Ct ratios (mmol/mol of creatinine), pH (unit), FRNa (%), and CCt (ml/min/g oftissue). *P õ 0.05, 7P õ 0.01.
TMAO is closely related to renal medullar osmolytes the renal medulla cells [15, 16]. In a clinical situation,elevated levels of TMAO were detected in plasma ofsynthesized in the medullar cells of the kidney to coun-
teract protein perturbation by a high urea concentra- patients with chronic renal failure or in the urine ofpatients with acute renal failure after exposure to phe-tion and to fill the osmotic gap between intracellular
and extracellular fluids [29, 30]. The high concentra- nol [16]. These preliminary results suggest that TMAOmay be important as a novel marker of renal medullarytion of methylamine (such as TMAO and betaine) in
the inner medulla is especially interesting since these damage.Regarding Lac, this acid is normally reabsorbed incompounds are known to offset the destabilizing effects
of urea on metabolic enzymes. The optimal ratio for the proximal tubule and abnormal excretion is due toeither a dysfunction of the proximal tubule or an in-this effect was determined to be one part methylamine
to two parts urea [31, 32]. A previous study has re- crease in plasma lactate or in lactate production byrenal cells. Lac reabsorption in proximal tubules is so-ported the presence of TMAO in the inner medulla of
the rat and rabbit kidney, but it could not detect TMAO dium dependent and driven by a sodium electrochemi-cal gradient coupled with the hydrolysis of ATP [15].in the urine or plasma, which implies that these me-
tabolites belong exclusively to the intracellular com- In this model, the increased Lac excretion could be re-lated to a decreased reabsorption related to tubularpartment [33]. The abnormal excretion of the renal
medullary osmolyte TMAO in G3 and G2 was associ- dysfunction but also to an increase in Lac productiondue to the increased anaerobic glycolysis which occursated with more intense medullar ischemia in this
group. In normal urine, this metabolite is not usually during cold-storage ischemia. Ace excretion is relatedalso with renal ischemia injury.found and its excretion may be related to leakage from
AID JSR 4988 / 6n1c$$$$23 05-16-97 00:50:39 srgas

122 JOURNAL OF SURGICAL RESEARCH: VOL. 68, NO. 2, MARCH 1997
FIG. 4. (a, b) Tubular injury markers. Results achieved 15, 60, and 120 min (t15, t60, t120) during reperfusion with an isolated perfusedpig kidney technique after 24 hr cold storage with Eurocollins (G2 and G3) and without cold storage (G1). Results are presented with meanvalues { SEM of TMAO/Ct (mmol/mol of creatinine) ratio, Lac (mmol/L), LDH (UI), and bNAG (UI). *P õ 0.001, 7Põ 0.01.
Glc/Ct, urinary amino acid excretion, and FRNa/ are sodium excretion are mainly affected by changes inGFR and proximal tubular reabsorption. Combinationmore important in G2 and particularly in G3; these
findings are consistent with the presence of major le- of glycosuria and amino acid uria with elevated levelsof the medullary osmolytes (TMAO), and also Lac andsions of the proximal tubule. For amino acids, elevation
in the excretion of alanine, valine, threonine, leucine, Ace suggested that both medullar and cortical damage.Regarding spectra, creatinine was also detected andand isoleucine is correlated with significant proximal
tubular dysfunction. Filtered amino acids are almost gave information on the GFR. Creatinine clearancecould be calculated from peak creatinine in urine andcompletely reabsorbed throughout the length of the
proximal tubule under normal conditions. Conse- plasma samples.Moreover, citrate excretion in urine is detected inquently, an interference with normal proximal tubular
functions is likely to be reflected in their reduced reab- G1 (control). Citrate is extensively reabsorbed in thenephron and previous studies have shown that thissorption, which is consistent with proximal tubular
damage produced by cold ischemia. Renal glucose and occurs predominantly in the proximal segments of thetubule [34]. Citrate excretion is closely related tochanges in acid–base balance. Tissue acidosis can dam-age cells and increases lactic acid production duringTABLE 1cold storage [35]. This could explain the presence of
Histological Evaluation and Malondialdehyde Tissue citrate excretion in G1 and not in G2 and G3. ThisLevels (MDA) (mmol of MDA per Milligram of Protein)result suggests that CSP and a combination of normo-in Kidneys That Underwent 24-hr CSPthermic ischemia and CSP cause a Kreb’s cycle impair-
Histology G1 G2 G3 ment and a proximal renal tubular acidosis stemmingVacuolization 1 2 5 either from an inhibition of renal carbonic anhydraseNecrosis 1 2 5 or from an increased use of anaerobic pathways second-Dilatation 1.5 2.5 4
ary to a mitochondrial insult or a combination of theseDetachment 1 3 5events. In the present study, citrate excretion is corre-Brush border 1 3 5
Edema 0.5 3 4.5 lated with a better regulation of intracellular pH in theScore 6 { 0.7 15.5 { 2.6* 28.5 { 4.9 control group. This marker allows a direct approach ofMDA 1.5 { 0.7 4.5 { 1.4** 8.9 { 1.2 energetic function recovery in this model.
The peak detected in G3 (Peak X) is related to theNote. Control group is not used in statistical analysis.* P õ 0.01. **P õ 0.001. most important tubular injury and very poor tubular
AID JSR 4988 / 6n1c$$$$23 05-16-97 00:50:39 srgas

123HAUET ET AL.: ASSESSMENT OF NORMOTHERMIC ISCHEMIA AND COLD STORAGE LESIONS
functions. An identical peak has been isolated in inten-sive care unit patients with sepsis syndrome and hypo-perfusion or after vascular surgery. This marker hasbeen isolated by gel filtration and according to its NMRcharacteristics, it is probably a peptide. In this study,the intensity of this peak could be a kidney injury indexrelated to ischemia or hypoperfusion damage. Thus,the peak value could predict kidney function after coldstorage and/or normothermic ischemia.
Recent studies have also identified with proton NMRspectroscopy a signal in urine associated with cyclo-sporine therapy. This resonance has been identified asthe vehicle of oral cyclosporine formulation. The inten-sity of this resonance in the 24-hr urine could be abetter index of the amount of cyclosporine absorbedduring this period [15, 16].
Other techniques can be combined with proton NMRspectroscopy, such as phosphorus-31 NMR spectros-copy. This technique also uses the magnetic propertiesof nuclei, such as phosphorus, to produce a chemicalshift spectrum. The signal gives a measure of the num-ber of mobile nuclei contributing to the peak, whichallows ratios of specific high energy phosphorus metab-olites to be calculated [36]. For renal transplantation,an important clinical advantage of this technique is tomeasure noninvasively intracellular phosphorus me-tabolites of the kidney in vivo and ex vivo, enablingthe study of specific metabolic parameters that may behelpful in establishing strong viability correlations.
The great parts of the markers detected by protonand phosphorus NMR spectroscopy are intracellular.With the recent availability of a large-bore NMR spec-troscopy system, cadaveric kidneys could be studiedduring cold storage within their sterile containers.Spectra would be obtained preoperatively without re-moval from or disruption of the sterile storage con-tainer or interruption of hypothermia [37]. This tech-nique would enable osmolytes, metabolic level, andphosphorus and intracellular pH to be directly moni-tored in whole kidneys noninvasively. These prelimi-nary results suggest that NMR spectroscopy is a nonde-structive technique of assessing the functional level ofkidneys. This method is also able to assess viabilityduring preservation or after normothermic ischemia.NMR spectroscopy can be applied to the evaluation ofdonors before retrieval. In addition, the ability to quan-titate damage in kidneys may help monitoring of ther-apy, such as cyclosporine, in the posttransplantationperiod. Cyclosporine is a nephrotoxic drug and its pre-mature use may lead to an increase in kidney injury.
CONCLUSION
Proton NMR spectroscopy can be used to assess andpredict kidney function after cold storage with a combi-
FIG. 5. Brush border of proximal tubular cell after cold storage nation of different markers. From a technical point of(original magnification { 3300). (A) Kidney sample from control view, the method enables biological screening withgroup. (B) Kidney sample after 24 hr cold storage without warm
minimal sample preparation and with a single pulseischemia. (C) Kidney sample after warm ischemia and 24 hr cold-storage preservation. bb, brush border; L, tubular lumen. experiment: no other method can detect, in the course
AID JSR 4988 / 6n1c$$$$23 05-16-97 00:50:39 srgas

124 JOURNAL OF SURGICAL RESEARCH: VOL. 68, NO. 2, MARCH 1997
and expression of major histocompatibility and adhesion mole-of the same experiment, the presence of TMAO, aminocules on renal tubule cells and capillary endothelium. J. Am.acids, ketone bodies, or glucose and simultaneously un-Soc. Nephrol. 5: 983, 1994.cover new biochemical markers. Work is in progress to
12. Shackleton, C. R., Ettinger, S. L., McLoughlin, M. G., Scuda-analyze precisely this new peak and its presence with more, C. H., Miller, R. R., and Keown, P. A. Effect of recoverydifferent normothermic ischemia periods. Future de- from ischemic injury on class I and class II MHC antigen expres-velopments in cold-storage solutions can be expected sion. Transplantation 49: 641, 1990.and the IPK model associated with NMR spectroscopy 13. Nicholson, J. K., and Wilson, I. D. High resolution proton mag-
netic resonance spectroscopy of biological fluids. Prog. NMRmight be useful as a screening method to test new solu-Spectrosc. 21: 449, 1989.tions or new preservation methods and as a novel ap-
14. Brown, J. C. C., Mills, G. A., Sadler, P. J., and Walker, V. H-1proach to the monitoring of renal transplant functionNMR studies of urine from premature and sick babies. Magn.in a more scientific and rational manner. Study is inReson. Med. 11: 193, 1989.
progress to assess other preservation solutions in an15. Le Moyec, L., Pruna, A., Eugene, M., Bedrossian, J., Idatte,identical situation with IPK and with an autotrans- J. M., Huneau, J. F., and Tome, D. Proton nuclear magnetic
plantation model which is probably closely related to resonance spectroscopy of urine and plasma in renal trans-the clinical situation. This technique can also be very plantation follow-up. Nephron. 65: 433, 1993.interesting for evaluation of kidney from cadaveric do- 16. Foxall, P. J. D., Mellote, G. J., Bending, M. R., Lindon, J. C.,
and Nicholson, J. K. NMR spectroscopy as a novel approach tonors particularly with hemodynamic instability andthe monitoring of renal transplant function. Kidney Int. 43: 234,during cold storage prior to transplant.1993.
17. Bales, J. R., Higham, D. P., Howe, I., Nicholson, J. K., andREFERENCES Sadler, P. J. Use of high resolution proton nuclear magneticresonance spectroscopy for rapid multi-component analysis of
1. Booster, M. H., Wijnen, R. M. H., Vroemen, J. P. A. M., van urine. Clin. Chem. 30: 426, 1984.Hoof, J. P., and Koostra, G. In situ preservation of kidneys from
18. Nicholson, J. K., Timbrell, J. A., and Sadler, P. J. Proton NMRnon-heart-beating donors: Proposal for a standardized protocol.spectra as indicator of renal damage. Mol. Pharmacol. 27: 644,Transplantation 3: 613, 1993.1984.2. Didlake, R. H., Raju, S., and Smith, G. V. Utilization and func-
19. Gartland, K. P. R., Lindon, J. C., Beddell, C. R., and Nicholson,tion of kidneys obtained from non-heart beating donors. Trans-J. K. Application of pattern recognition methods to the analysisplantation 38: 90, 1984.of toxicological data generated by NMR spectroscopy. Mol.3. Castelao, A. M., Grino, J. M., Gonzalez, C., Gilvernet, S., An-Pharmacol. 39: 629, 1991.dres, E., Seron, D., Torras, J., Galceran, J. M., Bover, J., Serral-
20. Gartland, K. P. R., Bonner, F. W., Timbrell, J. A., and Nichol-lach, N., and Alsina, J. Long-term renal function of kidneysson, J. K. Biochemical characterisation of para-aminophenol-transplanted from non-heart beating cadaver donors. Trans-induced nephrotoxic lesions in the F344 rat. Arch. Toxicol. 63:plant. Proc. 23: 2584, 1991.97, 1989.4. Paprocki, S., Kruk, R., Ertrurk, E., and Cerilli, J. A technique
for successful transplantation of organs from non-heart beating 21. Badia, P., Hauet, T., Mothes, D., Goujon, J. M., Tallineau, C.,cadaver donors. Transplantation 54: 381, 1992. Poncharreau, R., Carretier, M., Caritez, J. C., Robert, R., Eu-
gene, M., and Piriou, A. Functional activity of isolated perfused5. Troppmann, C., Gillingham, K. J., Benedetti, E., Almond, P. S.,kidney transplant after flush and 48-hour cold storage. Trans-Gruessner, R. W. G., Najarian, J. S., and Matas, A. J. Delayedplant. Proc. 28: 308, 1996.graft function, acute rejection, and outcome after cadaver renal
transplantation. A multivariate analysis. Transplantation 59: 22. Ramella, S. G., Hadj-Aissa, A., Barbieux, A., Steghens, J. P.,962, 1995. Colpart, J. J., Zech, P., and Pozet, N. Evaluation of a high so-
dium–low potassium cold-storage solution by the isolated per-6. Koning, O. H. J., van Bockel, J. H., van der Woude, F. J., Per-fused rat kidney technique. Nephrol. Dial. Transplant. 75: 842,sijn, G. G., Hermans, J., and Ploeg, R. J. for the European1995.Multicenter Study Group on Organ Preservation: Risk factors
for delayed graft function in University of Wisconsin solution 23. Herrero, I., Torras, J., Carrera, M., Castells, A., Pasto, L., Gil-preserved kidneys from multiorgan donors. Transplant. Proc. Vernet, S., Alsina, J., and Grinyo, J. M. Evaluation of a preser-27: 752, 1995. vation solution containing fructose-1,6-diphosphate and manni-
7. Anderson, C. B., Sicard, G. A., and Etheredge, E. E. Delayed tol using the isolated perfused rat kidney. Comparison withprimary renal function and cadaver renal allograft results. Euro-Collins and University of Wisconsin solutions. Nephrol.Surg. Gynecol. Obstet. 149: 697, 1979. Dial. Transplant. 10: 519, 1995.
8. Barry, J. M., Norman, D., Fuchs, E. F., Fisher, S., and Bennet, 24. Yagui, K. Lipid peroxides and human diseases. Chem. Phys.W. M. Influence of acute tubular necrosis on first cadaver kid- Lipids 45: 337, 1987.ney transplant function. J. Urol. 132: 234, 1984. 25. Lowry, O. H., Rosebrough, N. J., Farr, A. L., and Randall, R. J.
9. Halloran, P., Aprile, M. A., and Farewell, V. Early function as Protein measurement with the Folin phenol reagent. J. Biol.the principal correlate of graft survival. A multivariable analy- Chem. 193: 265, 1951.sis of 200 cadaveric renal transplants treated with a protocol 26. Craddock, G. N. Species differences in response to renal isch-incorporating antilymphocyte globulin and cyclosporine. Trans- emia. Arch. Surg. 111: 582, 1976.plantation 46: 223, 1988.
27. Kreiss, H., Lacombe, M., Cianconni, C., and Marinov, V. 48-10. Kumar, M. S., Stephan, R., Chui, J., Brezin, J., Lyons, P., Katz,Hour kidney preservation: Initial perfusion with potassium-rickS. M., and Abouna, G. M. Comparative study of cadaver donorsolution. Rev. Eur. Etudes Clin. Biol. 17: 192, 1972.kidneys preserved in University of Wisconsin solution for less
28. Masaki, Y., Kumano, K., Endo, T., and Koshiba, K. Effects ofthan or longer than 30 hours. Transplant. Proc. 25: 3053, 1993.a new solution for cold kidney preservation studied on isolated11. Lu, C. Y., Ar’Rajab, A., Dawidson, I., Sicher, S. C., and Wright,perfused rat kidney. Transplant. Proc. 26: 2045, 1994.W. J. Ischemic injury during syngeneic rat kidney transplanta-
tion results in trafficking of inflammatory cells into the kidney 29. Gartland, K. P. R., Bonner, F. W., and Nicholson, J. K. Investi-
AID JSR 4988 / 6n1c$$$$24 05-16-97 00:50:39 srgas

125HAUET ET AL.: ASSESSMENT OF NORMOTHERMIC ISCHEMIA AND COLD STORAGE LESIONS
gations into the biochemical effects of region-specific nephrotox- 34. Hamm, L. L. Renal handling of citrate. Kidney Int. 38: 728,1990.ins. Mol. Pharmacol. 35: 242, 1989.
35. Kallerhoff, M., Holscher, M., Kehrer, G., Klab, G., and Bret-30. Bell, J. D., Lee, J. A., Lee, H. A., Sadler, P. J., Wilkie, D. R., andschneider, H. J. Effects of preservation conditions and tempera-Woodman, R. H. Nuclear magnetic resonance studies of bloodture on tissue acidification in canine kidneys. Transplantationplasma and urine from subjects with chronic renal failure: Iden- 39: 485, 1985.
tification of trimethylamine-N-oxide. Biochem. Biophys. Acta36. Lietzenmayer, R., Henze, E., Knorpp, R., Schwamborn, C.,1096: 101, 1991. Clausen, M., Schnur, G., and Adam, W. E. Application of P-31
31. Somero, G. N. From dogfish to dog: Trimethyl-amine protects nuclear magnetic resonance spectroscopy to a new experimentalkidney perfusion model using cadaveric porcine kidneys fromproteins from urea. News Physiol. Sci. 1: 9, 1986.slaughterhouse. Nephron 57: 340, 1991.32. Balaban, R. S., and Burg, M. B. Osmotically active organic sol-
37. Bretan, P. N., Baldwin, N., Novick, A. C., Majors, A., Easley,utes in the renal inner medulla. Kidney Int. 31: 562, 1987.K., Ng, T., Stowe, N., Rehm, P., Sreem, S. B., and Steinmuller,
33. Balaban, R. S., and Knepper, M. A. Nitrogen 14 nuclear mag- D. R. Pretransplant assessment of renal viability by phospho-netic resonance spectroscopy of mammalian tissues. Am. J. rus-31 magnetic resonance spectroscopy. Transplantation 48:
48, 1989.Physiol. 245: C439–C444, 1983.
AID JSR 4988 / 6n1c$$$$24 05-16-97 00:50:39 srgas