
Etude de biomarqueurs de dysfonction atriale. - Theses.fr
115
THESE DE DOCTORAT DE L’ETABLISSEMENT UNIVERSITE BOURGOGNE FRANCHE-COMTE PREPAREE A L’UNITE DE RECHERCHE EA3920 ET L’UFR SCIENCES MEDICALES ET PHARMACEUTIQUES École doctorale Environnements-Santé (ED ES n°554) Doctorat de Sciences agronomiques et écologiques Biologie, médecine et santé Par Marc BADOZ Né le 01/06/1986 à Pontarlier Etude de biomarqueurs de dysfonction atriale. Thèse présentée et soutenue à Besançon, le 22/10/2021 Composition du Jury : Me Laurence JESEL-MOREL, professeur de cardiologie, Université de Strasbourg Rapporteur Mr Damien LOGEART, professeur de cardiologie, Université de Paris VII Rapporteur Me Marie-France SERONDE, professeur de cardiologie, Université de Franche-Comté Examinatrice Mr Christian DE CHILLOU, professeur de cardiologie, Université de Lorraine Examinateur Mr Gabriel LAURENT, professeur de cardiologie, Université de Bourgogne Examinateur Mr Nicolas MENEVEAU, professeur de cardiologie, Université de Franche-Comté Directeur de thèse
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Etude de biomarqueurs de dysfonction atriale. - Theses.fr
THESE DE DOCTORAT DE L’ETABLISSEMENT UNIVERSITE BOURGOGNE FRANCHE-COMTE
PREPAREE A L’UNITE DE RECHERCHE EA3920 ET L’UFR SCIENCES MEDICALES ET PHARMACEUTIQUES
École doctorale Environnements-Santé (ED ES n°554)
Doctorat de Sciences agronomiques et écologiques
Biologie, médecine et santé
Par
Marc BADOZ
Né le 01/06/1986 à Pontarlier
Etude de biomarqueurs de dysfonction atriale.
Thèse présentée et soutenue à Besançon, le 22/10/2021
Composition du Jury :
Me Laurence JESEL-MOREL, professeur de cardiologie, Université de Strasbourg Rapporteur Mr Damien LOGEART, professeur de cardiologie, Université de Paris VII Rapporteur Me Marie-France SERONDE, professeur de cardiologie, Université de Franche-Comté Examinatrice Mr Christian DE CHILLOU, professeur de cardiologie, Université de Lorraine Examinateur Mr Gabriel LAURENT, professeur de cardiologie, Université de Bourgogne Examinateur Mr Nicolas MENEVEAU, professeur de cardiologie, Université de Franche-Comté Directeur de thèse
THESE DE DOCTORAT DE L’ETABLISSEMENT UNIVERSITE BOURGOGNE FRANCHE-COMTE
PREPAREE A L’UNITE DE RECHERCHE EA3920 ET L’UFR SCIENCES MEDICALES ET PHARMACEUTIQUES
École doctorale Environnements-Santé (ED ES n°554)
Doctorat de Sciences agronomiques et écologiques
Biologie, médecine et santé
Par
Marc BADOZ
Né le 01/06/1986 à Pontarlier
Etude de biomarqueurs de dysfonction atriale.
Thèse présentée et soutenue à Besançon, le 22/10/2021
Composition du Jury :
Me Laurence JESEL-MOREL, professeur de cardiologie, Université de Strasbourg Rapporteur Mr Damien LOGEART, professeur de cardiologie, Université de Paris VII Rapporteur Me Marie-France SERONDE, professeur de cardiologie, Université de Franche-Comté Examinatrice Mr Christian DE CHILLOU, professeur de cardiologie, Université de Lorraine Examinateur Mr Gabriel LAURENT, professeur de cardiologie, Université de Bourgogne Examinateur Mr Nicolas MENEVEAU, professeur de cardiologie, Université de Franche-Comté Directeur de thèse
2
Remerciements
Madame le Professeur Laurence JESEL-MOREL
Vous me faites l’honneur de juger ce travail et d’en être rapporteur. Veuillez trouver l’expression de ma profonde gratitude.
Madame le Professeur Marie-France SERONDE
Votre intérêt pour les biomarqueurs en cardiologie et vos précédents travaux sur ce sujet ont été initiateurs de cette thèse. Soyez assurée de ma profonde reconnaissance.
Monsieur le Professeur Christian DE CHILLOU
Vous m’avez fait l’honneur de suivre l’évolution de mes travaux, d’y participer et de m’aider dans la finalisation de ceux-ci. C’est une grande fierté de vous compter dans les membres de ce jury.
Monsieur le Professeur Gabriel LAURENT
Vous avez accepté de participer à ce travail de thèse, votre aide et vos conseils ont été précieux. Je vous en suis profondément reconnaissant.
Monsieur le Professeur Damien LOGEART
Votre expertise dans le domaine des biomarqueurs est précieuse pour juger ce travail. Vous avez accepté d’en être rapporteur. Veuillez trouver l’expression de ma sincère reconnaissance.
Monsieur le Professeur Nicolas MENEVEAU
Vous m’avez apporté votre soutien pour chacun des travaux de cette thèse, votre œil expert et critique pour la méthodologie et la rédaction a permis d’aboutir aux différentes publications. Pour tout cela je vous remercie infiniment.
3
Publications en relation avec la thèse d’université :
Acutely decompensated heart failure with preserved and reduced ejection fraction present with
comparable haemodynamic congestion.
Lucas N.L. Van Aelst, Mattia Arrigo, Rui Placido, Eiichi Akiyama, Nicolas Girerd, Faiez Zannad,
Philippe Manivet, Patrick Rossignol, Marc Badoz, Malha Sadoune, Jean-Marie Launay, Etienne Gayat,
Carolyn S.P. Lam, Alain Cohen-Solal, Alexandre Mebazaa and Marie-France Seronde.
European Journal of Heart Failure (2018) 20, 738–747.
Role of cardiovascular biomarkers for the assessment of mitral stenosis and its complications.
Marc Badoz, Mattia Arrigo, Bernard Iung, Gullu Amioglu, Mehmet Birhan Yilmaz, Nicolas Meneveau,
Malha Sadoune, Agnes Brunette, Alexandre Mebazaa, Marie-France Seronde.
European Journal of Internal Medicine 34 (2016) 58–62.
Assessment of successful percutaneous mitral commissurotomy by MRproANP and sCD146.
Marc Badoz, Mattia Arrigo, Anne-Claire Mogenet, Malha Sadoune, Nicolas Meneveau, Alexandre
Mebazaa and Marie-France Seronde.
BMC Cardiovascular Disorders (2020) 20:157.
Impact of Midregional N-Terminal Pro–Atrial Natriuretic Peptide and Soluble Suppression of
Tumorigenicity 2 Levels on Heart Rhythm in Patients Treated With Catheter Ablation for Atrial
Fibrillation: The Biorhythm Study.
Marc Badoz, Guillaume Serzian, Baptiste Favoulet, Jean-Marc Sellal , Christian De Chillou, Néfissa
Hammache, Gabriel Laurent, Alexandre Mebazaa, Fiona Ecarnot, Karine Bardonnet, Marie-France
Seronde, François Schiele, Nicolas Meneveau.
Journal of the American Heart Association 2021;10:e020917. DOI: 10.1161/JAHA.121.020917.
4
Table des matières
Résumé
Abstract
I. Introduction
II. Rationnel
II.1. Biomarqueurs d’intérêt potentiel dans les pathologies atriales
II.1.1. Mid-Regional pro Atrial Natriuretic Peptide (MRproANP)
II.1.2. Soluble Cluster of Differentiation 146 (sCD146)
II.1.3. Soluble Suppression of Tumorigenicity 2 (sST2)
II.2. Situations cliniques pouvant justifier l’utilisation de ces biomarqueurs
II.2.1. Impact de l’insuffisance cardiaque au niveau atrial
II.2.2. Sténose mitrale et commissurotomie mitrale par voie percutanée
II.2.3. Fibrillation atriale et ablation endocavitaire
II.3. Synthèse
III. Corrélation entre Mid-Regional pro Atrial Natriuretic Peptide, Soluble Cluster of
Differentiation 146 et surfaces atriales droite et gauche
5
IV. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide et du Soluble Cluster of
Differentiation 146 dans l’évaluation de la sévérité et du traitement percutané de la sténose mitrale
IV.1. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide et du Soluble Cluster of
Differentiation 146 dans l’évaluation de la sévérité de la sténose mitrale
IV.2. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide et du Soluble Cluster of
Differentiation 146 dans l’évaluation du traitement percutané de la sténose mitrale
V. Evaluation du risque de récidive de fibrillation atriale à distance d’une procédure
d’ablation par le Mid-Regional pro Atrial Natriuretic Peptide et le Soluble Suppression of Tumorigenicity 2
VI. Synthèse et perspectives
VI.1. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide chez des patients atteints
de sténose mitrale
VI.2. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide chez des patients atteints
de fibrillation atriale
VI.3. Lien entre modifications structurelles de l’oreillette et Mid-Regional pro Atrial
Natriuretic Peptide
VI.4. Mid-Regional pro Atrial Natriuretic Peptide, synthèse et perspectives de recherche
VI.5. Intérêt du Soluble Cluster of Differentiation 146 chez des patients atteints de
sténose mitrale.
VI.6. Place du Soluble Cluster of Differentiation 146 dans l’insuffisance cardiaque
VI.7. Perspectives actuelles de recherche pour le Soluble Cluster of Differentiation 146
6
VI.8. Place du Soluble Suppression of Tumorigenicity 2 chez des patients traités par
ablation de fibrillation atriale
VI.9. Soluble Suppression of Tumorigenicity 2 et insuffisance cardiaque
VI.10. Synthèse et perspectives de recherche concernant le Soluble Suppression of
Tumorigenicity 2
VII. Conclusion
VIII. Références bibliographiques
7
Résumé
8
La pratique de la cardiologie fait appel de façon quotidienne à l’utilisation de biomarqueurs.
Cependant dans les pathologies à atteinte atriale prédominante, la performance diagnostique et
pronostique des biomarqueurs classiquement utilisés est peu démontrée. Nous nous sommes
donc intéressés à l’intérêt potentiel de trois biomarqueurs dans des pathologies affectant en
premier lieu l’oreillette : la fibrillation atriale (FA) et la sténose mitrale. Les biomarqueurs
concernés sont le MRproANP un peptide d’origine atriale, le sCD146 un marqueur d’origine
endothéliale et le sST2 un marqueur de fibrose. L’objectif de ce travail était l’évaluation de
leurs capacités diagnostiques et pronostiques chez des patients atteints de FA et de sténose
mitrale.
Dans la première publication (1) il était mis en évidence que le MRproANP, le sCD146
et le sST2 permettaient de discriminer une origine cardiaque congestive chez des patients
consultant pour dyspnée. Seuls les taux de MRproANP et sCD146 étaient liés à la dilatation
atriale, suggérant l’intérêt potentiel de ces biomarqueurs dans des pathologies avec atteinte
atriale.
Nous avons évalué dans une seconde publication (2) les concentrations plasmatiques de
MRproANP et de sCD146 chez des patients porteurs de sténoses mitrales serrées et
moyennement serrées. Les concentrations de ces deux biomarqueurs étaient toutes deux plus
élevées chez les patients porteurs de sténoses mitrales serrées en comparaison à ceux ayant des
sténoses moyennement serrées.
La troisième publication (3) fait suite à cette seconde étude. Elle a évalué les
concentrations de MRproANP, sCD146, BNP et NTproBNP, en pré et post commissurotomie
mitrale percutanée (CMP). Les taux initiaux de BNP, MRproANP, et sCD146 étaient
significativement abaissés en post CMP. Il n’existait pas de baisse significative de ces
biomarqueurs si les critères de succès de la CMP n’étaient pas remplis. Cette baisse semble
9
donc refléter l’amélioration hémodynamique induite par une procédure réalisée avec succès,
conférant au MRproANP et au sCD146 le rôle de marqueurs de succès d’une CMP.
L’ensemble de ces résultats concernant le sCD146 s’explique par sa libération au niveau
de l’endothélium de la circulation pulmonaire en réponse à la congestion induite par le
rétrécissement mitral. Les résultats concernant le MRproANP sont expliqués par une libération
conditionnée par la pression intra atriale gauche chez les patients porteurs de sténose mitrale.
A l’issu de ces 3 premières études, nous pouvons conclure que les taux de MRproANP
et de sCD146 sont des marqueurs de sévérité de la sténose mitrale et du résultat de son
traitement percutané.
Nous nous sommes enfin focalisés sur l’étude de ces biomarqueurs chez les patients en
FA (4). L’ablation de FA est au cœur de la prise en charge de cette pathologie. L’identification
des patients à risque de récidive post ablation est primordiale. Nous nous sommes ainsi
intéressés à l’impact des niveaux plasmatiques de MRproANP et de sST2 avant une ablation
sur le taux de récidive à un an. Le MRproANP était un prédicteur indépendant de récidive de
fibrillation atriale dans notre étude, le sST2 ne l’était pas. Un MRproANP au-delà d’un seuil de
107.9pmol/L était lié à un risque de récidive de FA multiplié par 25. Inversement en dessous
de ce seuil le risque de récidive à un an était de 4,2% avec une valeur prédictive négative très
élevée de 95.7%.
Dans cette même étude les concentrations pré-ablation de MRproANP étaient plus
élevées chez les patients en fibrillation qu’en rythme sinusal, et plus élevées dans les oreillettes
que dans le sang veineux périphérique. Ces données sont en faveur d’une sécrétion atriale du
MRproANP chez les patients en fibrillation.
10
Nous avons par ce travail pu montrer l’intérêt du MRproANP, du sCD146 et du sST2
pour le pronostic, le diagnostic de sévérité et le suivi des patients atteints de sténose mitrale ou
de FA.
11
Abstract
12
The assessment of biomarkers has become an integral part of the daily practice of
cardiology. However, in diseases affecting primarily the atria, the diagnostic and prognostic
role of widely used biomarkers is less well documented. Thus, we investigated the potential
utility of 3 biomarkers in diseases affecting primarily the atrium, namely atrial fibrillation (AF)
and mitral stenosis. The biomarkers investigated were MRproANP, a natriuretic peptide of
atrial origin; sCD146, a biomarker of endothelial origin; and sST2, a marker of fibrosis. The
aim of this work was to evaluate the diagnostic and prognostic capacities of these biomarkers
in patients with AF or mitral stenosis.
The first publication (1) investigated the performance of several biomarkers in patients
consulting for dyspnea. In this context, MRproANP, sCD146 and sST2 made it possible to
identify the cardiac origin of the dyspnea. In this study, only MRproANP and sCD146 levels
were found to be associated with right and left atrial dilation. This suggested the potential
interest of these biomarkers in pathologies affecting the atria.
In a second publication (2), we assessed plasma concentrations of MRproANP and
sCD146 in patients with moderate to severe mitral stenosis. Both biomarkers were significantly
higher in patients with severe mitral stenosis compared to those with moderate mitral stenosis.
The third publication (3) followed up on this theme by investigation the concentrations
of MRproANP, sCD146, BNP and NTproBNP before and after percutaneous mitral
commissurotomy (PMC). MR-proANP and plasma sCD146 were shown to decrease
significantly immediately after PMC. Of note, in this study, the significant changes in
biomarker levels were observed mainly in patients in whom the PMC procedure was judged
successful. The decrease in these biomarkers therefore seems to reflect the improvement in
hemodynamics induced by the successful procedure, making MRproANP and sCD146
adequate markers of procedural success after PMC.
13
Taken together, the results observed with sCD146 can be explained by the fact that it is
released by the endothelium in the pulmonary circulation in response to congestion caused by
mitral stenosis. A possible explanation for our findings regarding MRproANP is that its release
is conditioned by left intra-atrial pressure in patients with mitral stenosis.
After these three studies, we can conclude that MRproANP and sCD146 are markers of
the severity of mitral stenosis, and of the success of PMC.
Subsequently, we went on to investigate the utility of these biomarkers in patients with
AF (4). Catheter ablation is currently the cornerstone of AF therapy. The main limitation of
catheter ablation of AF is the success rate of the procedure, which ranges between 50 and 80%.
There is a strong need to identify patients at risk of recurrence after catheter ablation. To this
end, we investigated the impact of pre-procedural plasma levels of MRproANP and sST2 on
the rate of AF recurrence at 1 year after catheter ablation. We found that MRproANP was an
independent predictor of recurrence in our study, whereas sST2 was not. An MRproANP levels
above a threshold of 107.9pmol/L was found to be associated with a 25-fold increase in the risk
of AF recurrence. Conversely, patients with values below the threshold had a recurrence rate of
4.2%, with a high negative predictive value, at 95.7%.
In this study, we also observed that pre-procedural rates of MRproANP were highest in
patients in AF, compared to those in sinus rhythm. Concentrations did not significantly differ
between the right and left atria, but intra-atrial concentrations were significantly higher than
those observed in the peripheral blood. These data plead in favour of the atrial release of
MRproANP in patients in AF.
We demonstrated the utility of MRproANP, sCD146 and sST2for prognosis, diagnosis
of severity, and follow-up of patients with mitral stenosis or AF.
14
I. Introduction
15
La pratique de la cardiologie fait appel de façon quotidienne à l’utilisation de
biomarqueurs. Qu’il s’agisse des syndromes coronaires aigus, de la maladie thromboembolique
veineuse ou de l’insuffisance cardiaque, ils sont au cœur de la prise en charge par l’aide qu’ils
apportent dans le diagnostic, le pronostic et la stratification du risque, guidant ainsi le
traitement. La performance des biomarqueurs les plus utilisés, à savoir le BNP ou le NTproBNP
et la troponine, en termes de diagnostic et de pronostic dans ces pathologies est démontrée (5-
8). Cependant dans les pathologies à atteinte atriale prédominante, n’impliquant ni nécrose ni
atteinte ventriculaire, la performance diagnostique et pronostique de ces biomarqueurs
classiquement utilisés est moins bonne. C’est le cas par exemple de la sténose mitrale où la
survenue d’une HTAP et d’une dysfonction ventriculaire droite n’apparait qu’à un stade évolué
de la maladie alors que l’atteinte de l’oreillette gauche est au premier plan. Les données
échographiques permettent d’évaluer la sévérité de la sténose mitrale et ses complications mais
il n’existe que très peu de données concernant des biomarqueurs adaptés spécifiquement à cette
pathologie.
De manière plus générale il n’existe que peu de données concernant des biomarqueurs
plus spécifiquement atriaux qui puissent également s’appliquer aux pathologies rythmiques
atriales, en particulier à la fibrillation atriale. On s’appuie dans la fibrillation atriale sur des
données cliniques et échographiques permettant d’évaluer le niveau d’évolution et le pronostic
de cette pathologie. Il n’existe en revanche pas de biomarqueur fiable notamment pour prédire
l’évolution ou la récidive de la fibrillation atriale après une cardioversion électrique ou une
ablation endocavitaire. Pourtant leur utilisation en routine dans ces pathologies aurait une utilité
certaine dans le diagnostic de gravité de la pathologie, le suivi et également le pronostic à long
terme.
Le Mid-Regional pro Atrial Natriuretic Peptide (MRproANP) est la portion mid-
regional du NTproANP, il est un peptide plus spécifiquement atrial. Le Suppression of
16
Tumorigenicity 2 (sST est un marqueur de fibrose et le Soluble cluster of differentiation 146
(sCD146) est un marqueur d’origine endothéliale. Ces biomarqueurs ne sont pas utilisés dans
la pratique clinique actuelle.
Nous avons dans un premier travail collaboratif évalué le lien entre les concentrations
plasmatiques de ces trois biomarqueurs et la dilatation atriale ainsi que la capacité de ces
biomarqueurs à discriminer une origine cardiaque chez des patients dyspnéiques. Nous avons
ensuite choisi de nous intéresser au MRproANP et au sCD146 chez des patients porteurs de
sténoses mitrales, et notamment à leur capacité à évaluer la sévérité du rétrécissement et le
succès du traitement percutané de la sténose mitrale. Enfin chez des patients atteints de
fibrillation atriale, nous avons choisi d’évaluer la capacité du MRproANP et du sST2 à prédire
un succès ou une récidive de FA à distance d’une ablation endocavitaire.
17
II. Rationnel
18
II.1. Biomarqueurs d’intérêt potentiel dans les pathologies atriales
Trois biomarqueurs ont donc retenu notre attention pour être étudiés dans des
pathologies avec atteinte atriale : le MRproANP, un peptide natriurétique plus spécifiquement
atrial, portion mid-regional du NTproANP, le sCD146 un marqueur d’origine endothéliale et
enfin le sST2 un marqueur de fibrose notamment myocardique. Nous allons détailler dans ce
chapitre les données connues sur la sécrétion et la physiologie de ces biomarqueurs.
II.1.1. Mid-Regional pro Atrial Natriuretic Peptide (MRproANP)
L’ANP est un peptide natriurétique. Sa synthèse se fait sous la forme initiale d’une pro
hormone : le proANP. Chez l’homme, il existe une synthèse extracardiaque de ce peptide mais
le cardiomyocyte atrial est le principal site de synthèse. L’expression génique du proANP dans
les cardiomyocytes atriaux est en effet 30 à 50 fois plus élevée que dans les tissus extra atriaux
(9-11). Le proANP est libéré par les cardiomyocytes atriaux en réponse à la tension pariétale.
Il est clivé en ANP mature et en sa portion N Terminal le NTproANP. Il est plus stable et sa
demi-vie est beaucoup plus longue que l’ANP mature rendant son dosage plus intéressant (12,
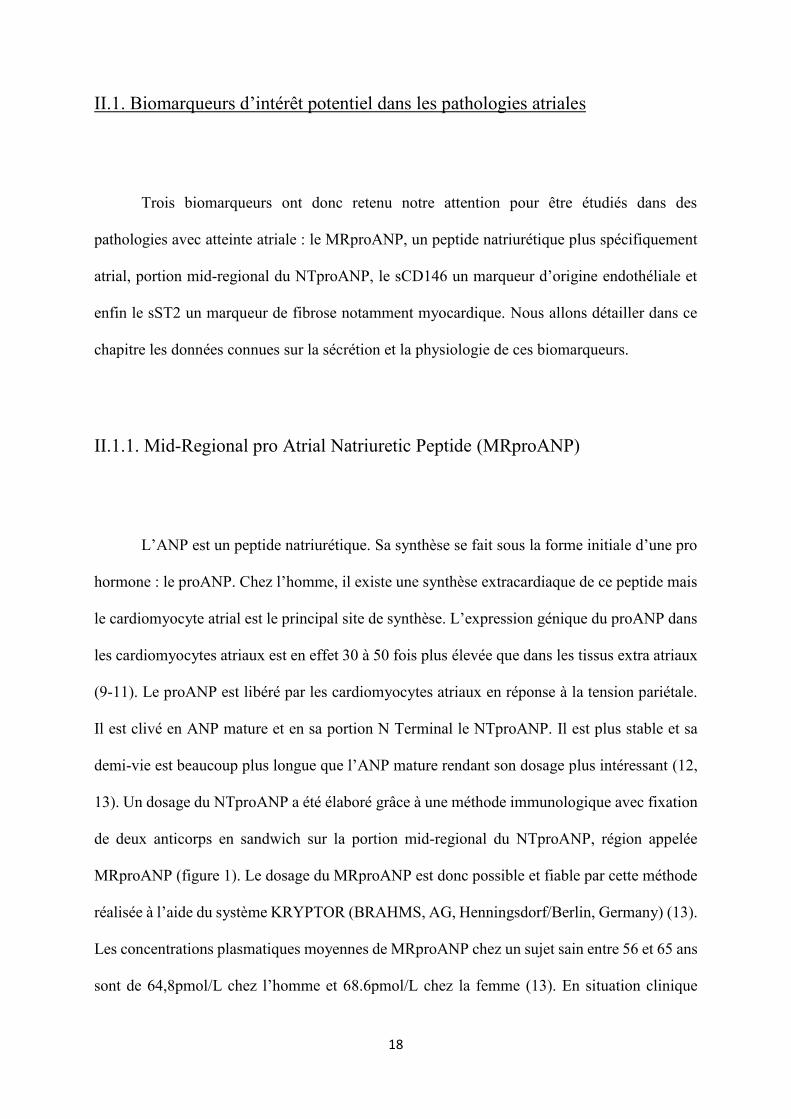
13). Un dosage du NTproANP a été élaboré grâce à une méthode immunologique avec fixation
de deux anticorps en sandwich sur la portion mid-regional du NTproANP, région appelée
MRproANP (figure 1). Le dosage du MRproANP est donc possible et fiable par cette méthode
réalisée à l’aide du système KRYPTOR (BRAHMS, AG, Henningsdorf/Berlin, Germany) (13).
Les concentrations plasmatiques moyennes de MRproANP chez un sujet sain entre 56 et 65 ans
sont de 64,8pmol/L chez l’homme et 68.6pmol/L chez la femme (13). En situation clinique
19
stable, sa variabilité est faible, elle ne varie pas significativement d’une année à l’autre chez un
même patient sans changement significatif de son poids (14). Son intérêt a été démontré dans
le diagnostic et le pronostic de l’insuffisance cardiaque (15-18). Il semble être un bon marqueur
de congestion et de rétention hydrosodée (19). Néanmoins il existe peu de données sur l’intérêt
de peptides plus spécifiquement atriaux dans des pathologies impliquant l’oreillette en premier
lieu.
Figure 1 : Fixation de 2 anticorps en sandwich sur la portion mid-regional du NTproANP pour
en permettre le dosage (MRproANP).
II.1.2. Soluble cluster of differentiation 146 (sCD146)
Le CD146 est une molécule d’adhésion exprimée par les cellules endothéliales
vasculaires. Elle est un composant de la jonction endothéliale (20, 21). Elle est impliquée dans
l’intégrité du vaisseau et dans la cohésion intercellulaire de l’endothélium (21, 22). Il a été
20
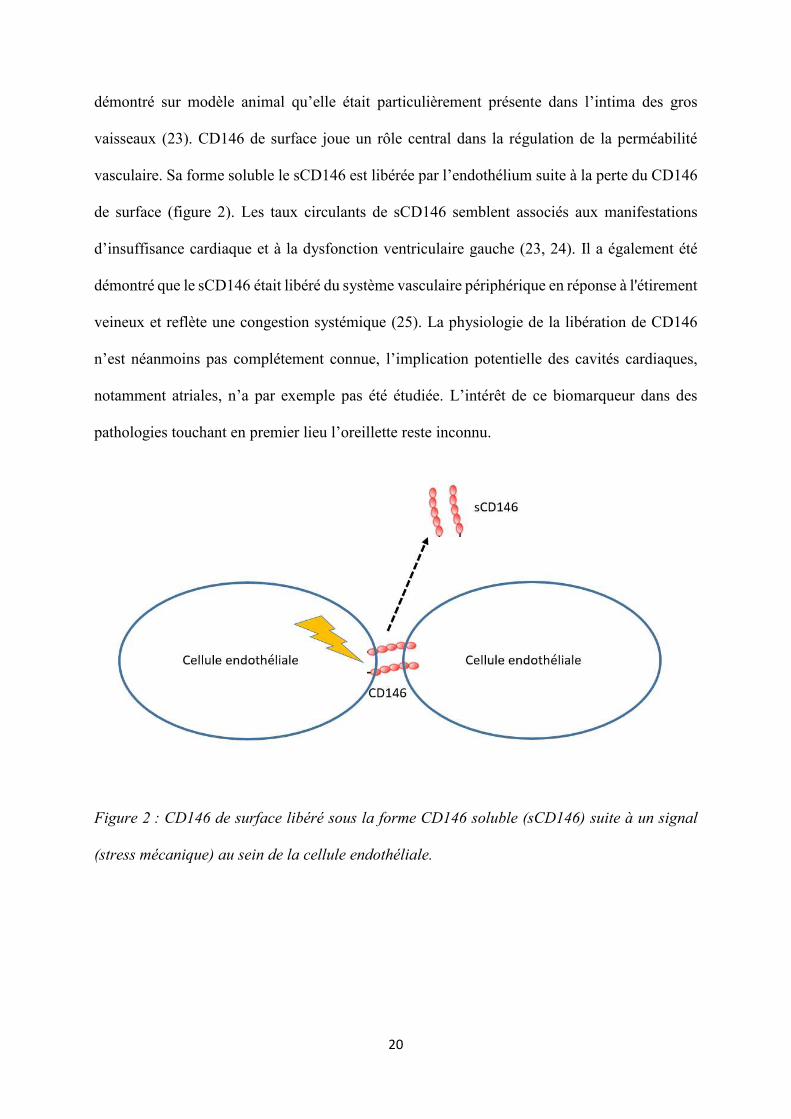
démontré sur modèle animal qu’elle était particulièrement présente dans l’intima des gros
vaisseaux (23). CD146 de surface joue un rôle central dans la régulation de la perméabilité
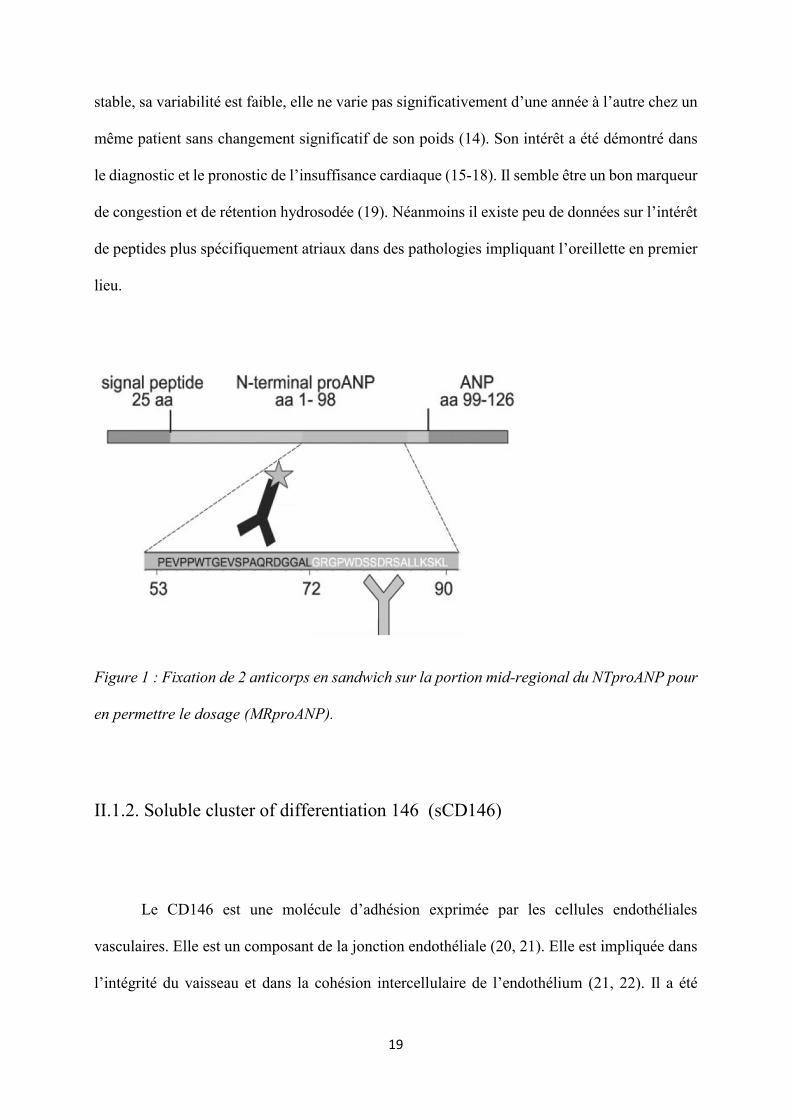
vasculaire. Sa forme soluble le sCD146 est libérée par l’endothélium suite à la perte du CD146
de surface (figure 2). Les taux circulants de sCD146 semblent associés aux manifestations
d’insuffisance cardiaque et à la dysfonction ventriculaire gauche (23, 24). Il a également été
démontré que le sCD146 était libéré du système vasculaire périphérique en réponse à l'étirement
veineux et reflète une congestion systémique (25). La physiologie de la libération de CD146
n’est néanmoins pas complétement connue, l’implication potentielle des cavités cardiaques,
notamment atriales, n’a par exemple pas été étudiée. L’intérêt de ce biomarqueur dans des
pathologies touchant en premier lieu l’oreillette reste inconnu.
Figure 2 : CD146 de surface libéré sous la forme CD146 soluble (sCD146) suite à un signal
(stress mécanique) au sein de la cellule endothéliale.
21
II.1.3. Soluble Suppression of Tumorigenicity 2 (sST2)
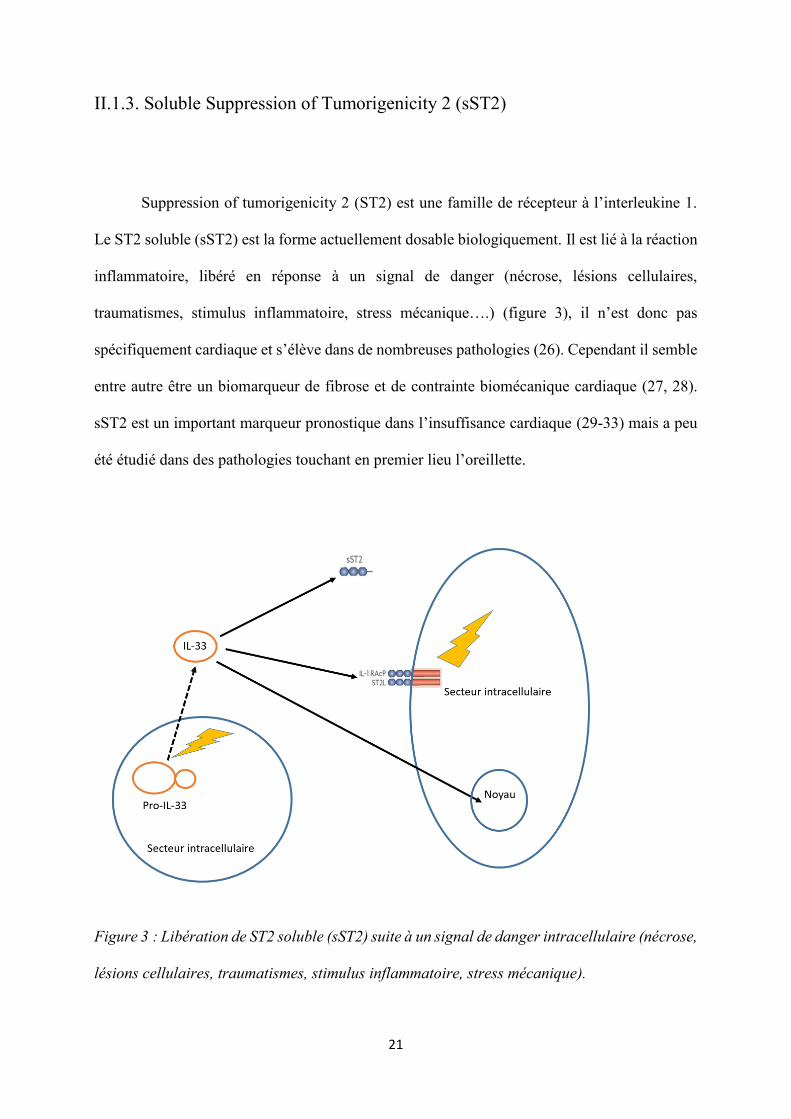
Suppression of tumorigenicity 2 (ST2) est une famille de récepteur à l’interleukine 1.
Le ST2 soluble (sST2) est la forme actuellement dosable biologiquement. Il est lié à la réaction
inflammatoire, libéré en réponse à un signal de danger (nécrose, lésions cellulaires,
traumatismes, stimulus inflammatoire, stress mécanique….) (figure 3), il n’est donc pas
spécifiquement cardiaque et s’élève dans de nombreuses pathologies (26). Cependant il semble
entre autre être un biomarqueur de fibrose et de contrainte biomécanique cardiaque (27, 28).
sST2 est un important marqueur pronostique dans l’insuffisance cardiaque (29-33) mais a peu
été étudié dans des pathologies touchant en premier lieu l’oreillette.
Figure 3 : Libération de ST2 soluble (sST2) suite à un signal de danger intracellulaire (nécrose,
lésions cellulaires, traumatismes, stimulus inflammatoire, stress mécanique).
22
II.2. Situations cliniques pouvant justifier l’utilisation de ces biomarqueurs
La sténose mitrale et la fibrillation atriale sont deux pathologies où l’atteinte est
prédominante sur l’oreillette gauche. Les trois biomarqueurs étudiés pourraient montrer un
intérêt pour le diagnostic et l’évaluation de la gravité de ces pathologies. Ils pourraient
également avoir un intérêt dans la prise en charge thérapeutique en tant que marqueur
pronostique ou de succès des interventions percutanées concernant l’oreillette gauche comme
la commissurotomie mitrale percutanée ou l’ablation de fibrillation atriale.
II.2.1. Impact de l’insuffisance cardiaque au niveau atrial
Dans l’insuffisance cardiaque, qu’elle soit à fraction d’éjection préservée ou altérée, la
pression télédiastolique ventriculaire ou précharge s'élève. Il s'en suit une élévation des
pressions en amont, notamment dans l’oreillette gauche puis dans les veines pulmonaires. Ce
phénomène est par la suite responsable de l’œdème pulmonaire. L’augmentation de pression
intra atriale entraine une dysfonction et une éventuelle dilatation atriale (34). L’insuffisance
cardiaque semble un modèle possible pour l’étude des biomarqueurs de dysfonction atriale.
II.2.2. Sténose mitrale et commissurotomie mitrale par voie percutanée
La sténose mitrale ou rétrécissement mitral s’observe préférentiellement chez les
femmes. Elle est secondaire à un rhumatisme articulaire aigu dans la grande majorité des cas.
23
Les autres causes possibles sont rares, qu’elles soient toxiques, congénitales ou post radiques.
Les lésions anatomiques caractéristiques du rétrécissement mitral associent :
- une fusion ou symphyse des commissures ;
- un épaississement des feuillets valvulaires qui peuvent, chez certains patients être calcifiés ;
- un remaniement de l’appareil sous-valvulaire associant, à des divers degrés, fusion des
cordages, raccourcissements et rétractions.
Le diagnostic et l’évaluation de la sévérité repose sur l’échographie cardiaque. La
surface mitrale et le gradient trans-mitral sont les paramètres pris en compte dans l’évaluation
de la sévérité. On parle de sténose mitrale pour un gradient dépassant 5 mmHg, la sténose
devient probablement serrée au-delà de 10 mmHg. Le gradient trans-mitral n’est pas le
paramètre de référence, celui-ci ne dépend en effet pas uniquement de la surface mitrale mais
également de la fréquence cardiaque, du débit cardiaque, du rythme cardiaque, des conditions
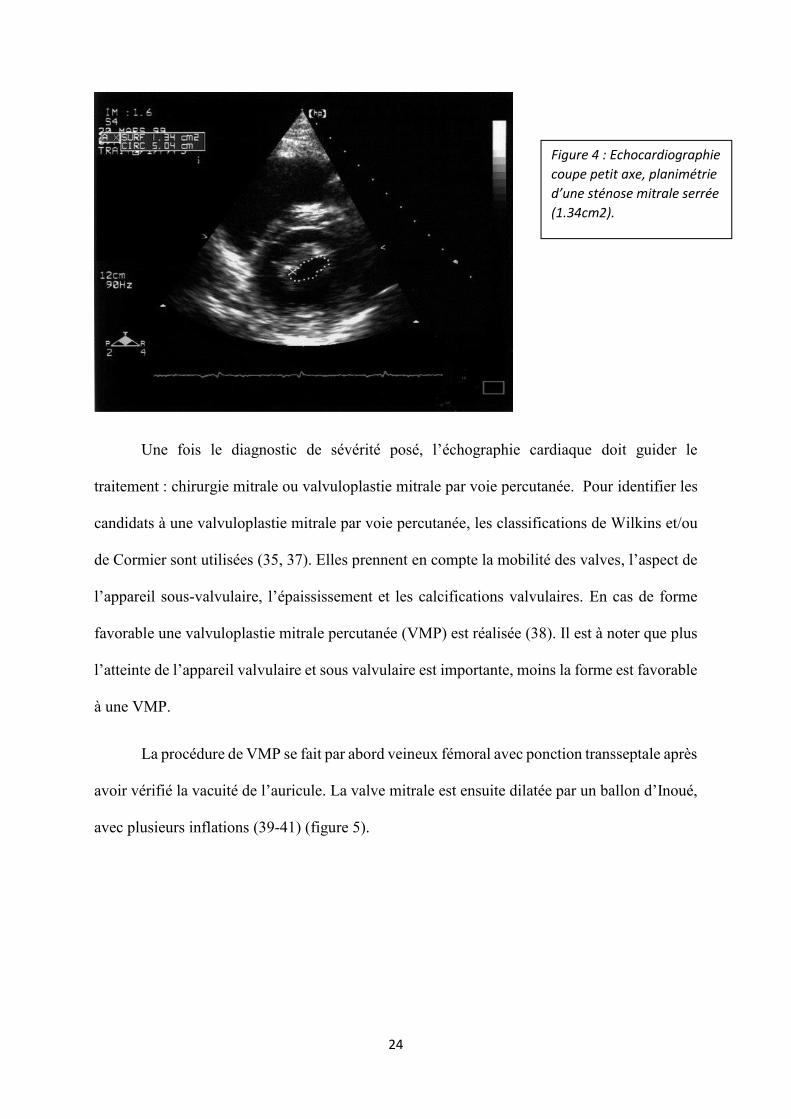
de charge et de l’existence d’une fuite associée. La surface mitrale mesurée en planimétrie est
la méthode de référence pour l’évaluation de la sévérité du rétrécissement mitral. La sténose
mitrale est considérée serrée pour une surface ≤ 1.5cm2 (35) ou 0.9-1cm2/m2. La mesure se
fait en coupe petit axe (figure 4). Les mesures réalisées ainsi sont les plus fiables, elles sont en
effet les mieux corrélées aux mesures directes per opératoires de l’orifice mitrale (36).
24
Une fois le diagnostic de sévérité posé, l’échographie cardiaque doit guider le
traitement : chirurgie mitrale ou valvuloplastie mitrale par voie percutanée. Pour identifier les
candidats à une valvuloplastie mitrale par voie percutanée, les classifications de Wilkins et/ou
de Cormier sont utilisées (35, 37). Elles prennent en compte la mobilité des valves, l’aspect de
l’appareil sous-valvulaire, l’épaississement et les calcifications valvulaires. En cas de forme
favorable une valvuloplastie mitrale percutanée (VMP) est réalisée (38). Il est à noter que plus
l’atteinte de l’appareil valvulaire et sous valvulaire est importante, moins la forme est favorable
à une VMP.
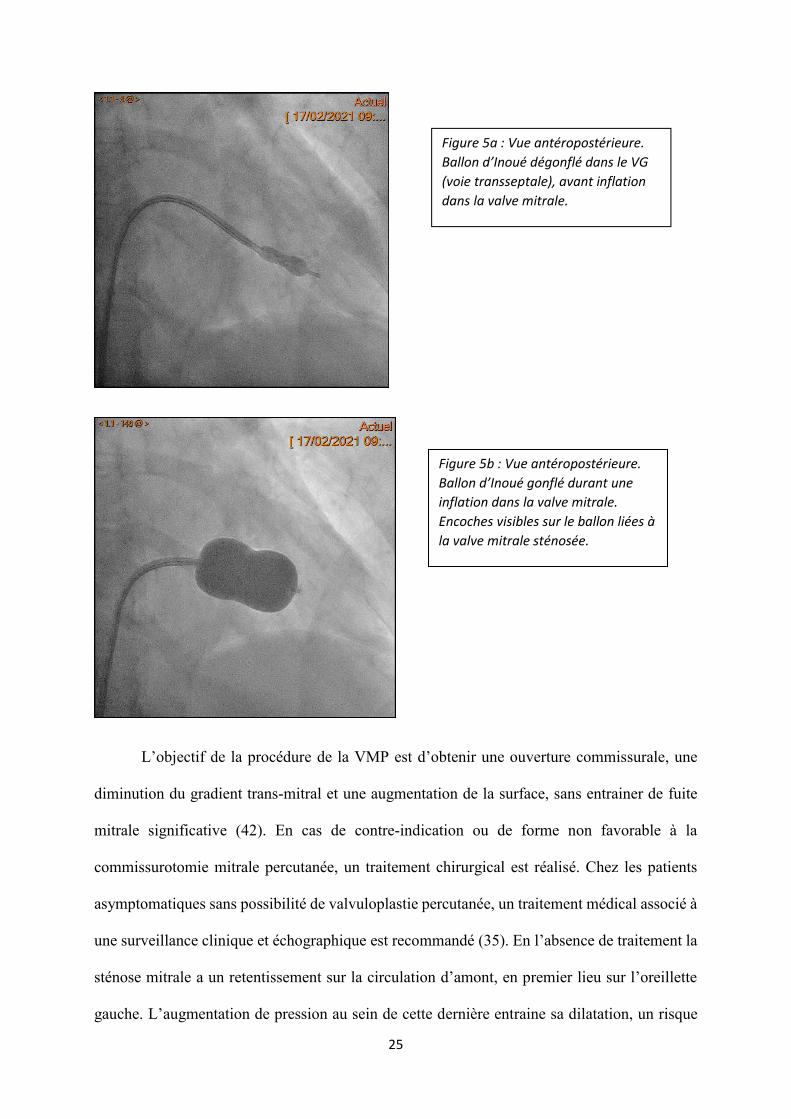
La procédure de VMP se fait par abord veineux fémoral avec ponction transseptale après
avoir vérifié la vacuité de l’auricule. La valve mitrale est ensuite dilatée par un ballon d’Inoué,
avec plusieurs inflations (39-41) (figure 5).
Figure 4 : Echocardiographie
coupe petit axe, planimétrie
d’une sténose mitrale serrée (1.34cm2).
25
L’objectif de la procédure de la VMP est d’obtenir une ouverture commissurale, une
diminution du gradient trans-mitral et une augmentation de la surface, sans entrainer de fuite
mitrale significative (42). En cas de contre-indication ou de forme non favorable à la
commissurotomie mitrale percutanée, un traitement chirurgical est réalisé. Chez les patients
asymptomatiques sans possibilité de valvuloplastie percutanée, un traitement médical associé à
une surveillance clinique et échographique est recommandé (35). En l’absence de traitement la
sténose mitrale a un retentissement sur la circulation d’amont, en premier lieu sur l’oreillette
gauche. L’augmentation de pression au sein de cette dernière entraine sa dilatation, un risque
Figure 5a : Vue antéropostérieure.
Ballon d’Inoué dégonflé dans le VG (voie transseptale), avant inflation
dans la valve mitrale.
Figure 5b : Vue antéropostérieure.
Ballon d’Inoué gonflé durant une inflation dans la valve mitrale.
Encoches visibles sur le ballon liées à
la valve mitrale sténosée.
26
accru de fibrillation atriale et de formation de thrombus intra-atrial gauche. Cette pathologie est
ainsi un bon modèle d’étude de biomarqueurs de dysfonction atriale gauche. Son évolution et
le succès ou l’échec de son traitement devraient en effet avoir un retentissement sur les niveaux
de ces biomarqueurs. Elle évolue ensuite vers une hypertension artérielle pulmonaire d’abord
post capillaire puis fixée. Le retentissement se fait par la suite naturellement sur les cavités
cardiaques droites avec une dilatation et une dysfonction ventriculaire droite. A un stade évolué
la sténose se manifeste essentiellement par des signes d’insuffisance cardiaque droite.
II.2.3. Fibrillation atriale et ablation endocavitaire
La fibrillation atriale (FA) est le trouble du rythme cardiaque de l’adulte le plus fréquent.
Il est particulièrement fréquent en Europe et en Amérique du Nord avec une prévalence au-delà
de 600 pour 100000 habitants. Sa prévalence est en augmentation constante. Les facteurs
connus favorisant la survenue de FA sont multiples, entre autres : la présence de cardiopathies
en particulier valvulaires ou ischémiques, l’insuffisance cardiaque, l’hypertension artérielle, le
diabète, l’obésité, le syndrome d’apnée du sommeil, la consommation excessive d’alcool,
l’excès ou le manque d’activité physique (43-47). La FA est identifiée sur un
électrocardiogramme par une absence d’activité atriale organisée, et une irrégularité des espaces
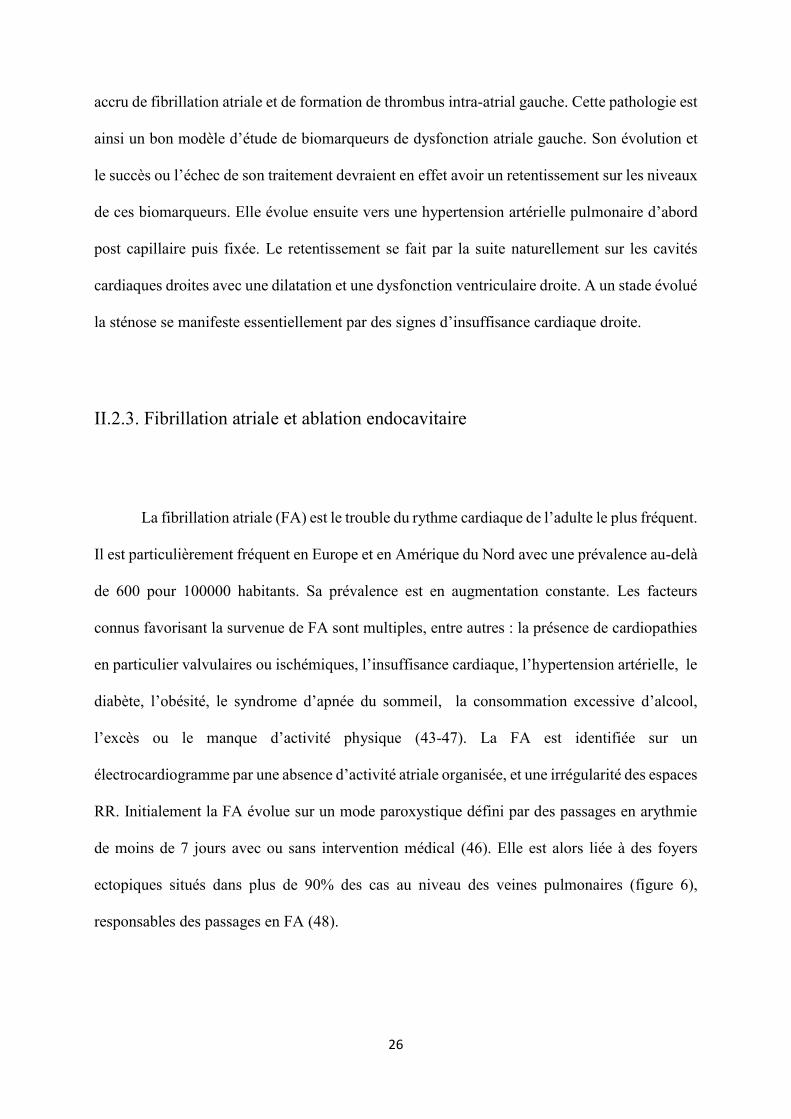
RR. Initialement la FA évolue sur un mode paroxystique défini par des passages en arythmie
de moins de 7 jours avec ou sans intervention médical (46). Elle est alors liée à des foyers
ectopiques situés dans plus de 90% des cas au niveau des veines pulmonaires (figure 6),
responsables des passages en FA (48).
27
Figure 6 : Situation de 69 foyers ectopiques focaux “triggers’’ des passages en FA chez 45
patients. Adapté de : Haïssaguerre M et al. Spontaneous initiation of atrial fibrillation by
ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659-66.
Sans traitement la FA devient ensuite persistante avec des passages de plus de 7 jours
puis “long-standing persistent’’ définie par plus d’un an de FA sans retour en rythme sinusal.
Enfin la FA est dite permanente lorsque médecin et patient s’accordent sur le fait de respecter
l’arythmie, de contrôler la fréquence cardiaque et les symptômes sans chercher à restaurer le
rythme sinusal (46). Cette évolution vers la FA persistante et éventuellement permanente est
liée à un remodelage électrique qui modifie l'expression et / ou la fonction des canaux ioniques
(49-54) (figure 7). Le remodelage électrique stabilise les réentrées et pérennise la fibrillation
atriale, il induit une récidive rapide après une cardioversion et également une résistance aux
anti-arythmiques (49). Le remodelage structurel, en particulier la fibrose (55-59), fait suite au
remodelage électrique (49, 50, 52, 53, 60, 61) (figure 7). La fibrose interstitielle sépare les
faisceaux musculaires, la fibrose réparatrice remplace quant à elle les cardiomyocytes. La
28
présence de fibroblastes ralenti ensuite localement la conduction. Il produit des zones de
conduction lente et des blocs de conduction. De cette manière le remodelage des oreillettes est
responsable d’activités électriques focales ou rotationnelles anormales de plus en plus
nombreuses (57). L’anatomie macroscopique de l’oreillette gauche se modifie alors également,
avec une dilatation de celle-ci (55, 56, 58).
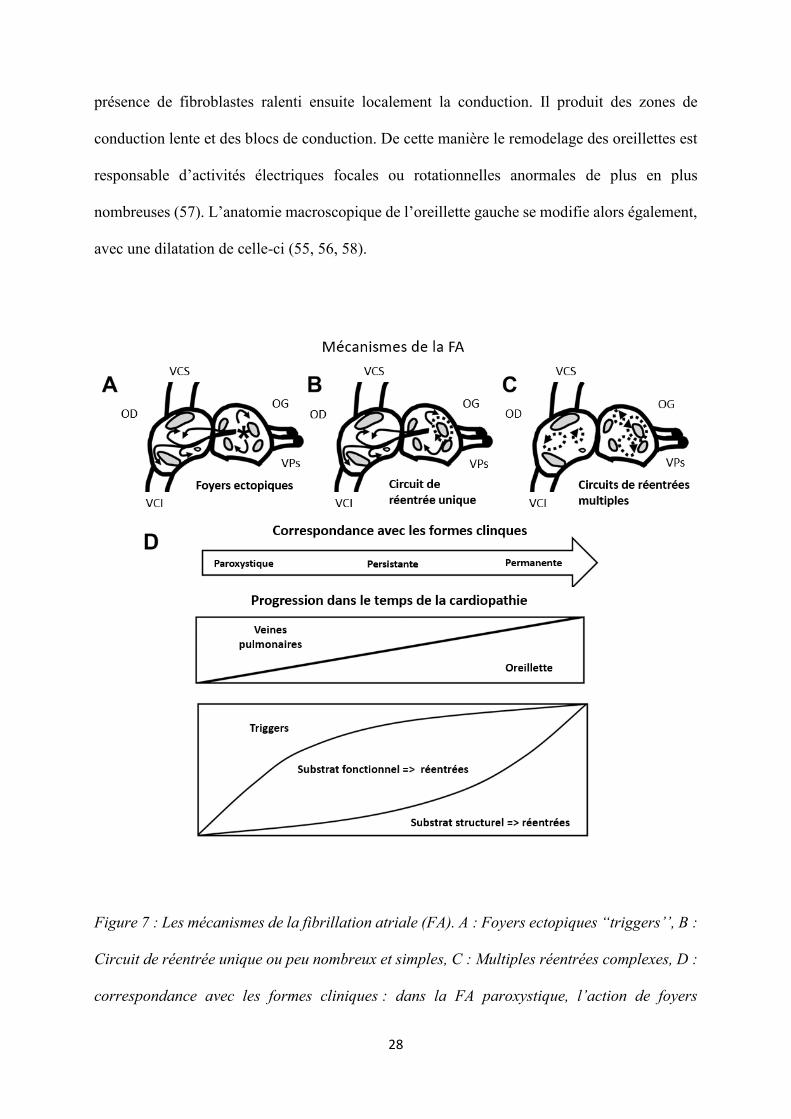
Figure 7 : Les mécanismes de la fibrillation atriale (FA). A : Foyers ectopiques “triggers’’, B :
Circuit de réentrée unique ou peu nombreux et simples, C : Multiples réentrées complexes, D :
correspondance avec les formes cliniques : dans la FA paroxystique, l’action de foyers
29
ectopiques “gâchettes’’ prédomine, particulièrement dans les veines pulmonaires, la FA
devient ensuite persistante et éventuellement permanente, il s’installe alors des circuits de
réentrées de plus en plus nombreux qui prédominent. Ces circuits ont d’abord un substrat
fonctionnel et secondairement un substrat structurel.
VCS : veine cave supérieure, VCI : veine cave inférieure, OD : oreillette droite, OG : oreillette
gauche, VPs : veines pulmonaires.
Adapté de Iwasaki YK, Nishida K, Kato T, Nattel S. Atrial fibrillation pathophysiology:
implications for management. Circulation. 2011.
Les principales manifestations cliniques de la fibrillation atriale sont les palpitations, la
dyspnée. Elle se complique essentiellement d’insuffisance cardiaque avec ou sans dysfonction
ventriculaire gauche ainsi que d’événements cardio-emboliques. La prévention des événements
cardio-emboliques repose sur la prescription d’anticoagulants oraux à doses curatives en cas de
score de risque embolique CHA2DS2 VASC ≥ 1 chez l’homme et ≥ 2 chez la femme (46, 62-
65).
En ce qui concerne la gestion rythmique il est décidé soit un contrôle de fréquence
cardiaque avec utilisation de traitements bradycardisants en cas de besoin, soit un contrôle de
rythme c’est-à-dire le maintien du rythme sinusal. Le maintien du rythme sinusal a fait la preuve
de sa supériorité dans la prise en charge de FA de découverte récente, sur la survenue
d’événements cardiovasculaires (66). L’ablation de fibrillation atriale est actuellement au centre
de la stratégie de contrôle du rythme cardiaque (46, 62, 67). Elle consiste en l’isolation des
veines pulmonaires où sont localisés les foyers ectopiques “triggers’’ de la FA (48). La
supériorité de l’ablation de fibrillation atriale, en comparaison au traitement anti-arythmique,
pour le maintien du rythme sinusal ainsi qu’en termes de morbi-mortalité chez les patients
30
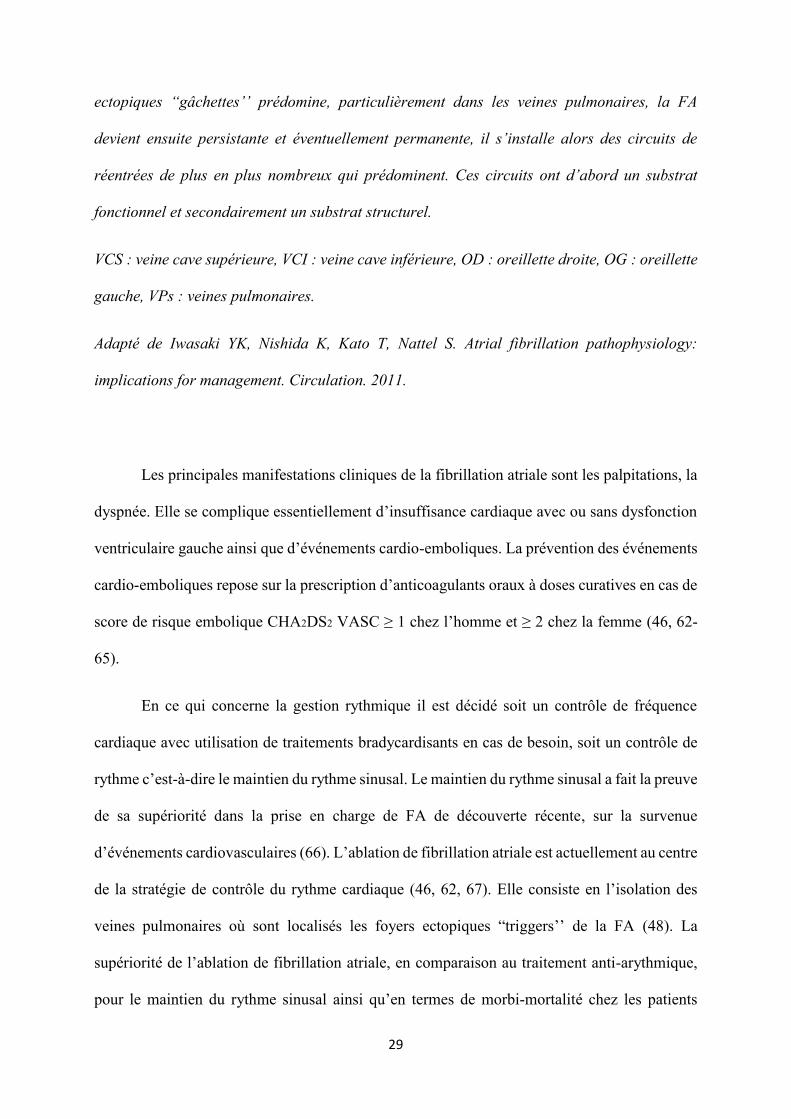
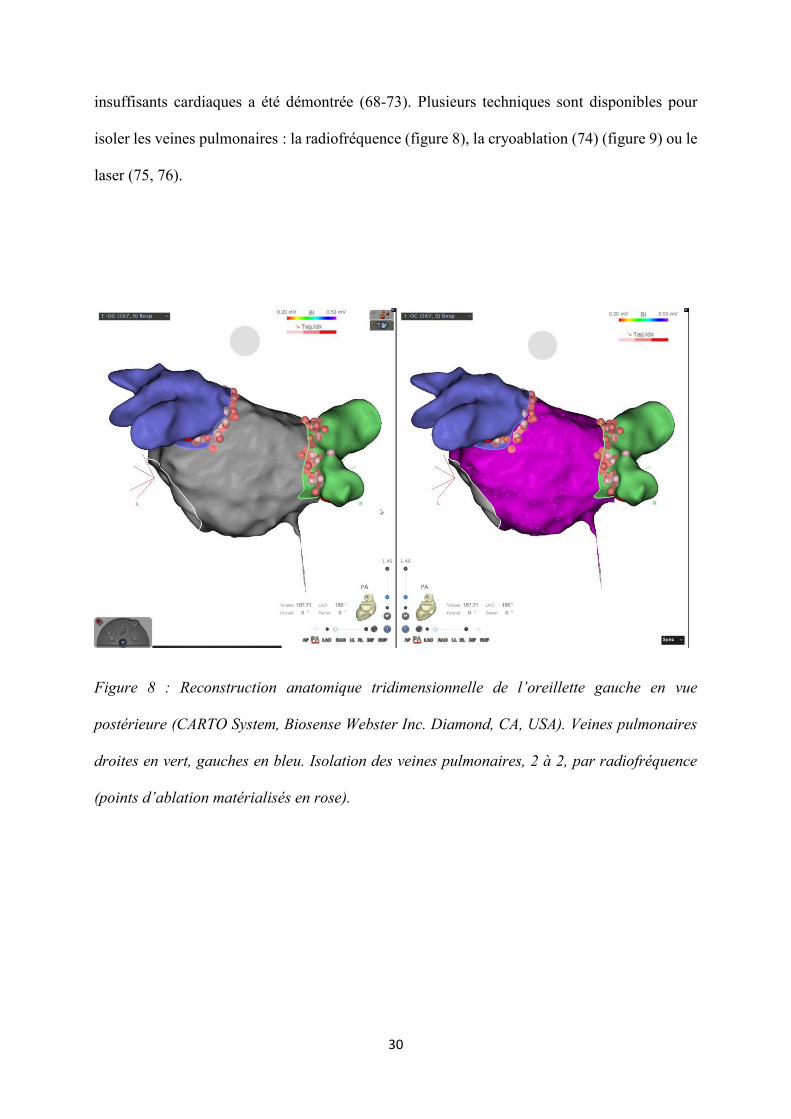
insuffisants cardiaques a été démontrée (68-73). Plusieurs techniques sont disponibles pour
isoler les veines pulmonaires : la radiofréquence (figure 8), la cryoablation (74) (figure 9) ou le
laser (75, 76).
Figure 8 : Reconstruction anatomique tridimensionnelle de l’oreillette gauche en vue
postérieure (CARTO System, Biosense Webster Inc. Diamond, CA, USA). Veines pulmonaires
droites en vert, gauches en bleu. Isolation des veines pulmonaires, 2 à 2, par radiofréquence
(points d’ablation matérialisés en rose).
31
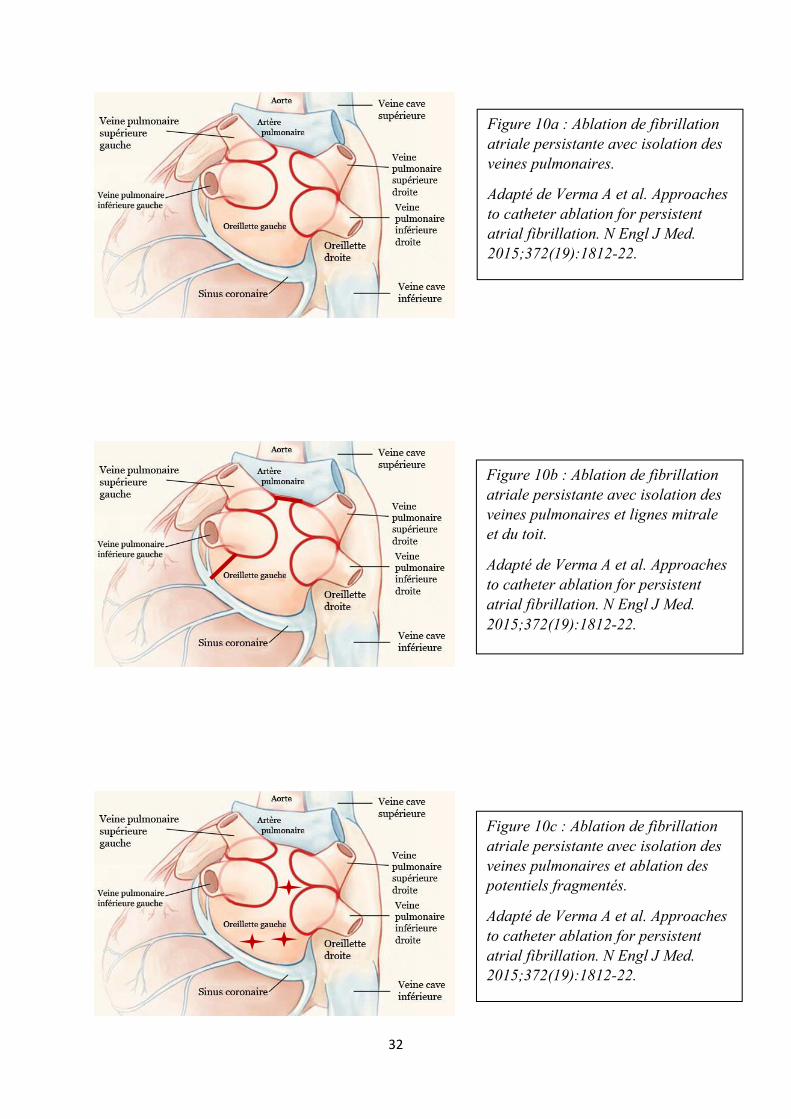
En cas de fibrillation persistante la radiofréquence est utilisée préférentiellement,
d’autres lésions peuvent alors être réalisées mais aucune n’a clairement démontré sa supériorité
(77) (figure 10).
Figure 9 : Ablation de fibrillation
atriale par cryothérapie. Vue
antéropostérieure. Opacification
d’une veine pulmonaire supérieure
gauche avec le cryoballon (Artic
Front Advance, Medtronic,
Minneapolis, MN, USA) en vue de
l’isolation.
32
Figure 10a : Ablation de fibrillation atriale persistante avec isolation des veines pulmonaires.
Adapté de Verma A et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812-22.
Figure 10b : Ablation de fibrillation atriale persistante avec isolation des veines pulmonaires et lignes mitrale et du toit.
Adapté de Verma A et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812-22.
Figure 10c : Ablation de fibrillation atriale persistante avec isolation des veines pulmonaires et ablation des potentiels fragmentés.
Adapté de Verma A et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812-22.
33
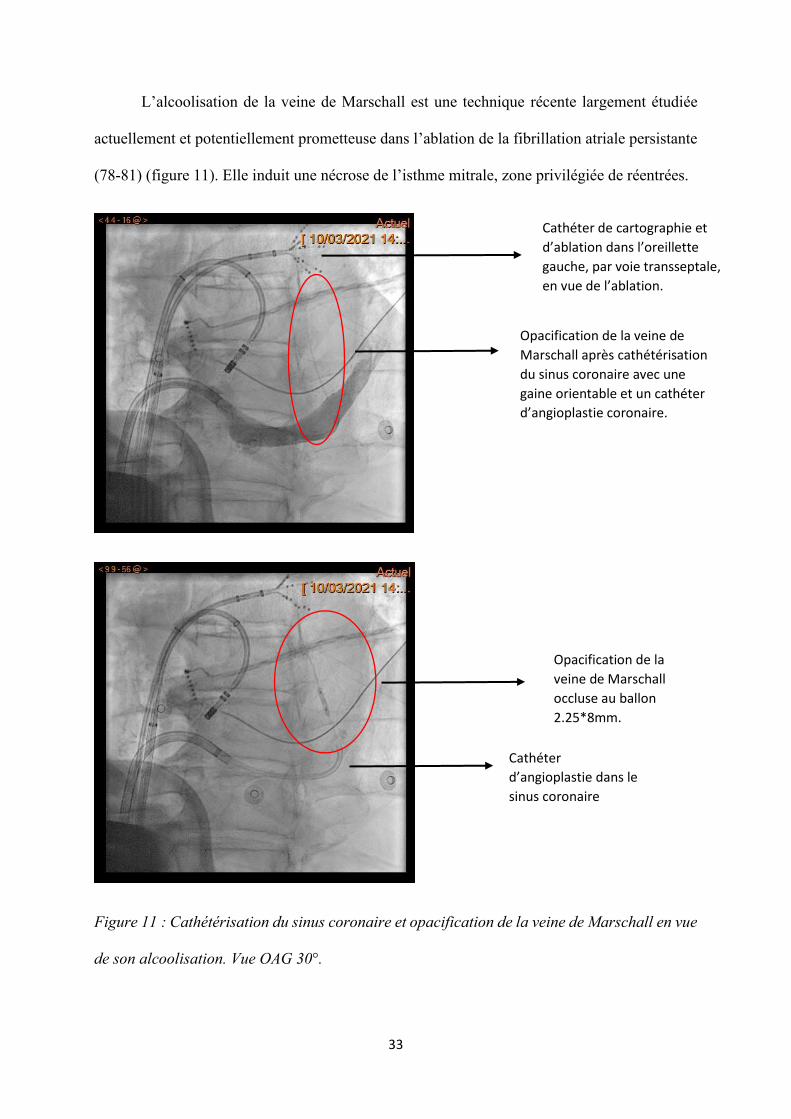
L’alcoolisation de la veine de Marschall est une technique récente largement étudiée
actuellement et potentiellement prometteuse dans l’ablation de la fibrillation atriale persistante
(78-81) (figure 11). Elle induit une nécrose de l’isthme mitrale, zone privilégiée de réentrées.
Figure 11 : Cathétérisation du sinus coronaire et opacification de la veine de Marschall en vue
de son alcoolisation. Vue OAG 30°.
Opacification de la
veine de Marschall
occluse au ballon
2.25*8mm.
Cathéter
d’angioplastie dans le sinus coronaire
Opacification de la veine de
Marschall après cathétérisation
du sinus coronaire avec une
gaine orientable et un cathéter
d’angioplastie coronaire.
Cathéter de cartographie et
d’ablation dans l’oreillette gauche, par voie transseptale,
en vue de l’ablation.
34
II.3. Synthèse
Dans un premier temps nous avons choisi d’évaluer ces 3 biomarqueurs en tant que
marqueurs de congestion chez des patients dyspnéiques et plus précisément, le lien entre
dilatation atriale et concentrations plasmatiques de MRproANP et sCD146 a été recherché.
Au vu de l’ensemble ces données, nous avons également décidé d’étudier le lien entre
les niveaux de MRproANP, sCD146 et la sévérité des sténoses mitrales, la présence de
complications de ces sténoses, ainsi que la capacité des biomarqueurs à identifier un succès de
commissurotomie mitrale percutanée.
Dans la fibrillation atriale nous avons choisi d’évaluer la capacité du MRproANP et du
sST2 à prédire un succès ou une récidive de FA à 1 an d’une ablation.
35
III. Corrélation entre Mid-Regional
pro Atrial Natriuretic Peptide,
Soluble Cluster of Differentiation 146
et surfaces atriales droite et gauche
36
Acutely decompensated heart failure with preserved and reduced ejection fraction
present with comparable haemodynamic congestion.
Lucas N.L. Van Aelst, Mattia Arrigo, Rui Placido, Eiichi Akiyama, Nicolas Girerd, Faiez
Zannad, Philippe Manivet, Patrick Rossignol, Marc Badoz, Malha Sadoune, Jean-Marie
Launay, Etienne Gayat, Carolyn S.P. Lam, Alain Cohen-Solal, Alexandre Mebazaa and
Marie-France Seronde.
European Journal of Heart Failure (2018) 20, 738–747.
AVANT PROPOS
L’insuffisance cardiaque gauche entraine une congestion veineuse pulmonaire liée à une
anomalie cardiaque structurelle ou fonctionnelle. Cette congestion est responsable de la
dyspnée ressentie par les patients insuffisants cardiaques, en particulier au moment des épisodes
de décompensation cardiaque. Chez un patient dyspnéique, le diagnostic étiologique vise à
discriminer une cause cardiaque liée à la congestion, d’une cause extra cardiaque.
La pathologie évolue naturellement vers l’hypertension pulmonaire et la dysfonction
ventriculaire droite (8, 82). L’insuffisance cardiaque, y compris à fraction d’éjection préservée,
est associé à une dysfonction et dilatation atriale (34).
L’article suivant s’intéresse à l’aide que pourraient apporter différents biomarqueurs,
notamment le MRproANP, le sCD146 et le sST2 dans l’évaluation de la congestion et dans le
bilan étiologique d’une dyspnée (cardiaque ou extra cardiaque). Il s’intéresse également au lien
entre dilatation atriale et niveau de sCD146 et de MRproANP.
European Journal of Heart Failure (2018) 20, 738–747 RESEARCH ARTICLEdoi:10.1002/ejhf.1050
Acutely decompensated heart failure with
preserved and reduced ejection fraction
present with comparable haemodynamic
congestionLucas N.L. Van Aelst1,2,3†, Mattia Arrigo3,4,5†, Rui Placido3,6†, Eiichi Akiyama3,7,
Nicolas Girerd8, Faiez Zannad8, Philippe Manivet3,9,10, Patrick Rossignol8,
Marc Badoz11, Malha Sadoune3, Jean-Marie Launay3,9,10, Etienne Gayat3,5,12,
Carolyn S.P. Lam13, Alain Cohen-Solal2,3,12, Alexandre Mebazaa3,5,12*†,
and Marie-France Seronde3,11†
1Department of Cardiovascular Sciences KU Leuven, Campus Gasthuisberg O&N1, Leuven, Belgium; 2Department of Cardiology, Hôpital Lariboisière, Paris, France; 3U942
INSERM, Assistance Publique – Hôpitaux de Paris, Paris, France; 4Division of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerland; 5Department
of Anesthesia and Critical Care, Hôpitaux Universitaires Saint Louis-Lariboisière, Paris, France; 6Hospital Santa Maria, Serv Cardiologia I, Lisbon Academic Medical Centre,
CCUL, Lisbon, Portugal; 7Division of Cardiology, Yokohama City University Medical Center, Minamiku, Yokohama, Japan; 8INSERM, Centre d’Investigations Cliniques
Plurithématique, CHRU de Nancy, Université de Lorraine, CHRU de Nancy, and F-CRIN INI-CRCT, Nancy, France; 9Department of Medical Biochemistry and Molecular Biology,
Hôpital Lariboisière, Paris, France; 10Biossip Analytical Platform, Center for Biological Resources, Lariboisière Hospital, Paris, France; 11Department of Cardiology, University
Hospital Jean Minjoz, Besançon, France; 12University Paris Diderot, Sorbonne Paris Cité, Paris, France; and 13National Heart Centre Singapore and Duke-National University of
Singapore, Singapore
Received 14 July 2017; revised 18 September 2017; accepted 26 September 2017 ; online publish-ahead-of-print 18 December 2017
Aims Congestion is a central feature of acute heart failure (HF) and its assessment is important for clinical decisions (e.g.
tailoring decongestive treatments). It remains uncertain whether patients with acute HF with preserved ejection
fraction (HFpEF) are comparably congested as in acute HF with reduced EF (HFrEF). This study assessed congestion,
right ventricular (RV) and renal dysfunction in acute HFpEF, HFrEF and non-cardiac dyspnoea.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Methods
and results
We compared echocardiographic and circulating biomarkers of congestion in 146 patients from the MEDIA-DHF
study: 101 with acute HF (38 HFpEF, 41 HFrEF, 22 HF with mid-range ejection fraction) and 45 with non-cardiac
dyspnoea. Compared with non-cardiac dyspnoea, patients with acute HF had larger left and right atria, higher E/e’,
pulmonary artery systolic pressure and inferior vena cava (IVC) diameter at rest, and lower IVC variability (all
P< 0.05). Mid-regional pro-atrial natriuretic peptide (MR-proANP) and soluble CD146 (sCD146), but not B-type
natriuretic peptide (BNP), correlated with echocardiographic markers of venous congestion. Despite a lower BNP
level, patients with HFpEF had similar evidence of venous congestion (enlarged IVC, left and right atria), RV dysfunction
(tricuspid annular plane systolic excursion), elevated MR-proANP and sCD146, and renal impairment (estimated
glomerular filtration rate; all P> 0.05) compared with HFrEF.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Conclusion In acute conditions, HFpEF and HFrEF presented in a comparable state of venous congestion, with similarly altered
RV and kidney function, despite higher BNP in HFrEF.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Keywords Heart failure • Biomarkers • Echocardiography • Diagnosis • Prognosis
*Corresponding author. Department of Anesthesia and Critical Care, Hôpitaux Universitaires Saint Louis-Lariboisière, 2 Rue Ambroise-Paré, 75010 Paris, France. Tel: +33 01
49958071, Fax: +33 01 49956954, Email: [email protected]†These authors contributed equally to this manuscript.
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology

Acutely decompensated HFpEF and HFrEF 739
Introduction
Heart failure (HF) is a clinical syndrome resulting from an abnor-
mal cardiac structure or function which impairs the heart’s ability
to meet the oxygen and nutrient requirements of metabolizing
tissues, and leads to pulmonary venous congestion.1,2 ‘Backward’
failure may further lead to pulmonary venous hypertension, right
ventricular (RV) dysfunction, renal venous hypertension and renal
dysfunction. Bedside assessment of venous congestion is important
for the classification of acutely decompensated patients into ‘wet’
vs. ‘dry’ phenotypes, which then guides clinical management, e.g.
aggressive diuresis in ‘wet’ patients. Conversely, under-recognition
of the extent of venous congestion can lead to inadequate diure-
sis and higher rehospitalization rates. The assessment of venous
congestion is particularly challenging in patients with HF and pre-
served ejection fraction (HFpEF), who are frequently obese with
age-related non-cardiac co-morbidities.
We aimed to compare the extent of venous congestion, RV and
renal dysfunction at acute presentation in patients with HFpEF
vs. HF with reduced ejection fraction (HFrEF) and non-cardiac
dyspnoea using echocardiographic and circulating biomarkers.
Methods
Patient population
We analysed the data of patients included in MEDIA-DHF (The
Metabolic Road to Diastolic Heart Failure: Diastolic Heart Failure
study; NCT02446327). MEDIA-DHF enrolled patients with acute dys-
pnoea of non-cardiac origin, acutely decompensated heart failure
(ADHF) and chronic HF. For this specific substudy, a database was
constructed between February 2011 and April 2014, including eligible
patients admitted for acute dyspnoea of cardiac or non-cardiac ori-
gin as the main symptom at the emergency departments of Hôpital
Lariboisière (Paris) and Hôpital Universitaire Jean Minjoz (Besançon),
both in France. The aim of this study was to characterize acute HFpEF,
HFrEF and acute dyspnoea of non-cardiac origin, with special empha-
sis on congestion, RV and kidney dysfunction at admission. Inclusion
criteria were age>18 years and acute dyspnoea. Exclusion criteria
were acute coronary syndromes, inotropic support within the last 2 h
before inclusion, systolic blood pressure persistently below 90mmHg,
severe aortic or mitral valvulopathy, pneumothorax, recent surgery or
trauma (< 3months), severe or end-stage renal impairment (clearance
<30mL/min or dialysis), chronic liver disease, chronic infectious (bac-
terial of viral) disease, cerebrovascular disease or stroke in the last
3months, any malignant concomitant diseases or a malignant disease
in the last 5 years, systemic inflammatory diseases, such as autoim-
mune diseases, connective tissue diseases or collagenoses, pregnancy.
The adjudicated final diagnosis (ADHF or non-cardiac dyspnoea) was
performed independently by two cardiologists not in charge of the
patients, yet with unlimited access to clinical, biochemical and imaging
materials obtained in the emergency departments, intensive or cardiac
care units and during the remainder of the hospitalization. When the
two experts disagreed regarding the final diagnosis, a third physician
adjudicated the final diagnosis.3
The study protocol complied with the Declaration of Helsinki and
was approved by the ethics committee of the participating institutions
[Commission Nationale de l’Informatique et des Libertés (CNIL)
910198; Comité d’Evaluation de l’Ethique des projets de Recherche ........................................................................................................................................................................ Biomedicale (CEERB) 10–017]. All patients provided written informed
consent.
Echocardiography
Echocardiographic measurements of chamber and vessel dimensions
and cardiac systolic and diastolic functions were obtained according
to the guidelines by cardiologists experienced in echocardiographic
measurements (R.P. and M.F.S.) within 4 h of presentation for dysp-
noea in the emergency department, using standard acoustic windows
on a Philips CX50 or iE33 ultrasound system.4 We aimed for a com-
prehensive assessment of echocardiographic parameters of congestion,
systolic and diastolic ventricular function in every patient. When clin-
ical presentation interfered with appropriate cardiac imaging, assess-
ment of systolic function was prioritized over diastolic function and
left ventricular filling pressures, which were preferred over additional
echocardiographic parameters of congestion. Ventriculo–arterial cou-
pling was calculated as the quotient of end-systolic volume and stroke
volume.5 Investigators involved in image acquisition were blinded to
obtained natriuretic peptide levels and were not involved in further
statistical analysis of the data. ADHF patients were divided into three
subgroups based on their left ventricular ejection fraction (LVEF) on
admission: reduced LVEF <40% (HFrEF); mid-range LVEF between 40
and 49% (HFmrEF); preserved LVEF >50% (HFpEF).1
Biomarkers
During initial presentation in the emergency department and at dis-
charge, blood samples were collected in plastic tubes containing
ethylenediaminetetra-acetic acid. Aliquots of plasma samples were
stored at −80 ∘C for further analysis. Apart from routinely used mark-
ers of kidney and liver function, several plasma biomarkers reflect-
ing different pathophysiological pathways in HF were assessed: brain
natriuretic peptide (BNP; Abbott), mid-regional pro-atrial natriuretic
peptide (MR-proANP; BRAHMS AG - ThermoFisher), high sensitive
troponin I (hsTnI; Roche Diagnostics), cluster of differentiation 62E
and 146 (CD62E, soluble CD146 or sCD146; Biocytex), mid-regional
pro-adrenomedullin (MR-proADM; ThermoFisher Diagnostics), solu-
ble ST2 (Critical Diagnostics), galectin 3 (Abbott), C-reactive protein
(CRP; Siemens), procalcitonin (BRAHMS AG - ThermoFisher), inter-
cellular adhesion molecule 3 (ICAM3; Abcam), cystatine C (Abbott),
neutrophil gelatinase associated lipocalin (NGAL; Abbott).
Follow-up and outcome
After discharge, patient outcome was followed for 1 year, with struc-
tured telephone calls at 3, 6 and 12months after admission. An
adverse event was defined as death or cardiovascular rehospital-
ization, whichever came first. Death occurring on the first day of
(re)hospitalization was defined as death rather than (re)hospitalization.
Statistical analysis
Continuous variables are expressed as means with standard deviations
(SD) when normally distributed or as medians with interquar-
tile ranges (IQR) when not normally distributed. Normality was
assessed by the Shapiro–Wilk test. Categorical variables are pre-
sented as numbers and percentages. Groups were compared using
one-way analysis of variance (ANOVA) or non-parametric alter-
natives as appropriate. Subsequent pairwise comparisons were
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
740 L.N.L. Van Aelst et al.
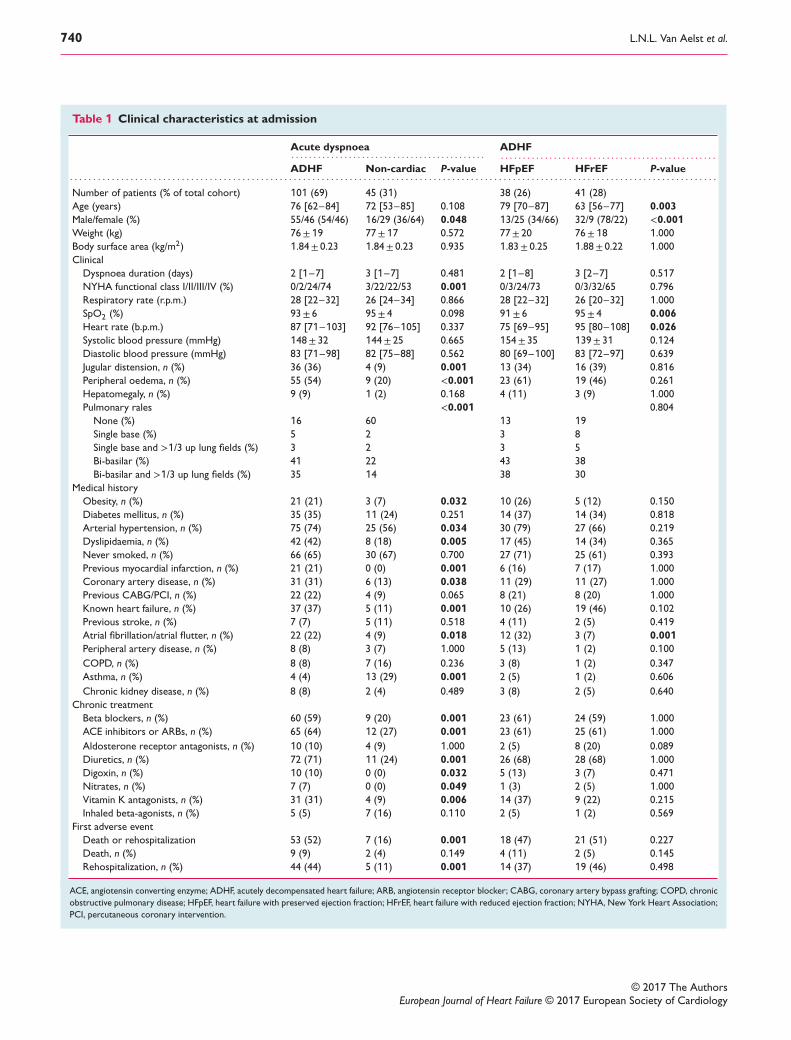
Table 1 Clinical characteristics at admission
Acute dyspnoea ADHF. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ADHF Non-cardiac P-value HFpEF HFrEF P-value. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Number of patients (% of total cohort) 101 (69) 45 (31) 38 (26) 41 (28)
Age (years) 76 [62–84] 72 [53–85] 0.108 79 [70–87] 63 [56–77] 0.003
Male/female (%) 55/46 (54/46) 16/29 (36/64) 0.048 13/25 (34/66) 32/9 (78/22) <0.001
Weight (kg) 76±19 77±17 0.572 77± 20 76±18 1.000
Body surface area (kg/m2) 1.84± 0.23 1.84± 0.23 0.935 1.83± 0.25 1.88± 0.22 1.000
Clinical
Dyspnoea duration (days) 2 [1–7] 3 [1–7] 0.481 2 [1–8] 3 [2–7] 0.517
NYHA functional class I/II/III/IV (%) 0/2/24/74 3/22/22/53 0.001 0/3/24/73 0/3/32/65 0.796
Respiratory rate (r.p.m.) 28 [22–32] 26 [24–34] 0.866 28 [22–32] 26 [20–32] 1.000
SpO2 (%) 93± 6 95± 4 0.098 91± 6 95± 4 0.006
Heart rate (b.p.m.) 87 [71–103] 92 [76–105] 0.337 75 [69–95] 95 [80–108] 0.026
Systolic blood pressure (mmHg) 148± 32 144± 25 0.665 154± 35 139± 31 0.124
Diastolic blood pressure (mmHg) 83 [71–98] 82 [75–88] 0.562 80 [69–100] 83 [72–97] 0.639
Jugular distension, n (%) 36 (36) 4 (9) 0.001 13 (34) 16 (39) 0.816
Peripheral oedema, n (%) 55 (54) 9 (20) <0.001 23 (61) 19 (46) 0.261
Hepatomegaly, n (%) 9 (9) 1 (2) 0.168 4 (11) 3 (9) 1.000
Pulmonary rales <0.001 0.804
None (%) 16 60 13 19
Single base (%) 5 2 3 8
Single base and >1/3 up lung fields (%) 3 2 3 5
Bi-basilar (%) 41 22 43 38
Bi-basilar and >1/3 up lung fields (%) 35 14 38 30
Medical history
Obesity, n (%) 21 (21) 3 (7) 0.032 10 (26) 5 (12) 0.150
Diabetes mellitus, n (%) 35 (35) 11 (24) 0.251 14 (37) 14 (34) 0.818
Arterial hypertension, n (%) 75 (74) 25 (56) 0.034 30 (79) 27 (66) 0.219
Dyslipidaemia, n (%) 42 (42) 8 (18) 0.005 17 (45) 14 (34) 0.365
Never smoked, n (%) 66 (65) 30 (67) 0.700 27 (71) 25 (61) 0.393
Previous myocardial infarction, n (%) 21 (21) 0 (0) 0.001 6 (16) 7 (17) 1.000
Coronary artery disease, n (%) 31 (31) 6 (13) 0.038 11 (29) 11 (27) 1.000
Previous CABG/PCI, n (%) 22 (22) 4 (9) 0.065 8 (21) 8 (20) 1.000
Known heart failure, n (%) 37 (37) 5 (11) 0.001 10 (26) 19 (46) 0.102
Previous stroke, n (%) 7 (7) 5 (11) 0.518 4 (11) 2 (5) 0.419
Atrial fibrillation/atrial flutter, n (%) 22 (22) 4 (9) 0.018 12 (32) 3 (7) 0.001
Peripheral artery disease, n (%)
COPD, n (%)
8 (8)
8 (8)
3 (7)
7 (16)
1.000
0.236
5 (13)
3 (8)
1 (2)
1 (2)
0.100
0.347
Asthma, n (%)
Chronic kidney disease, n (%)
4 (4)
8 (8)
13 (29)
2 (4)
0.001
0.489
2 (5)
3 (8)
1 (2)
2 (5)
0.606
0.640
Chronic treatment
Beta blockers, n (%) 60 (59) 9 (20) 0.001 23 (61) 24 (59) 1.000
ACE inhibitors or ARBs, n (%)
Aldosterone receptor antagonists, n (%)
65 (64)
10 (10)
12 (27)
4 (9)
0.001
1.000
23 (61)
2 (5)
25 (61)
8 (20)
1.000
0.089
Diuretics, n (%) 72 (71) 11 (24) 0.001 26 (68) 28 (68) 1.000
Digoxin, n (%) 10 (10) 0 (0) 0.032 5 (13) 3 (7) 0.471
Nitrates, n (%) 7 (7) 0 (0) 0.049 1 (3) 2 (5) 1.000
Vitamin K antagonists, n (%) 31 (31) 4 (9) 0.006 14 (37) 9 (22) 0.215
Inhaled beta-agonists, n (%) 5 (5) 7 (16) 0.110 2 (5) 1 (2) 0.569
First adverse event
Death or rehospitalization 53 (52) 7 (16) 0.001 18 (47) 21 (51) 0.227
Death, n (%) 9 (9) 2 (4) 0.149 4 (11) 2 (5) 0.145
Rehospitalization, n (%) 44 (44) 5 (11) 0.001 14 (37) 19 (46) 0.498
ACE, angiotensin converting enzyme; ADHF, acutely decompensated heart failure; ARB, angiotensin receptor blocker; CABG, coronary artery bypass grafting; COPD, chronic
obstructive pulmonary disease; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; NYHA, New York Heart Association;
PCI, percutaneous coronary intervention.
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
Acutely decompensated HFpEF and HFrEF 741
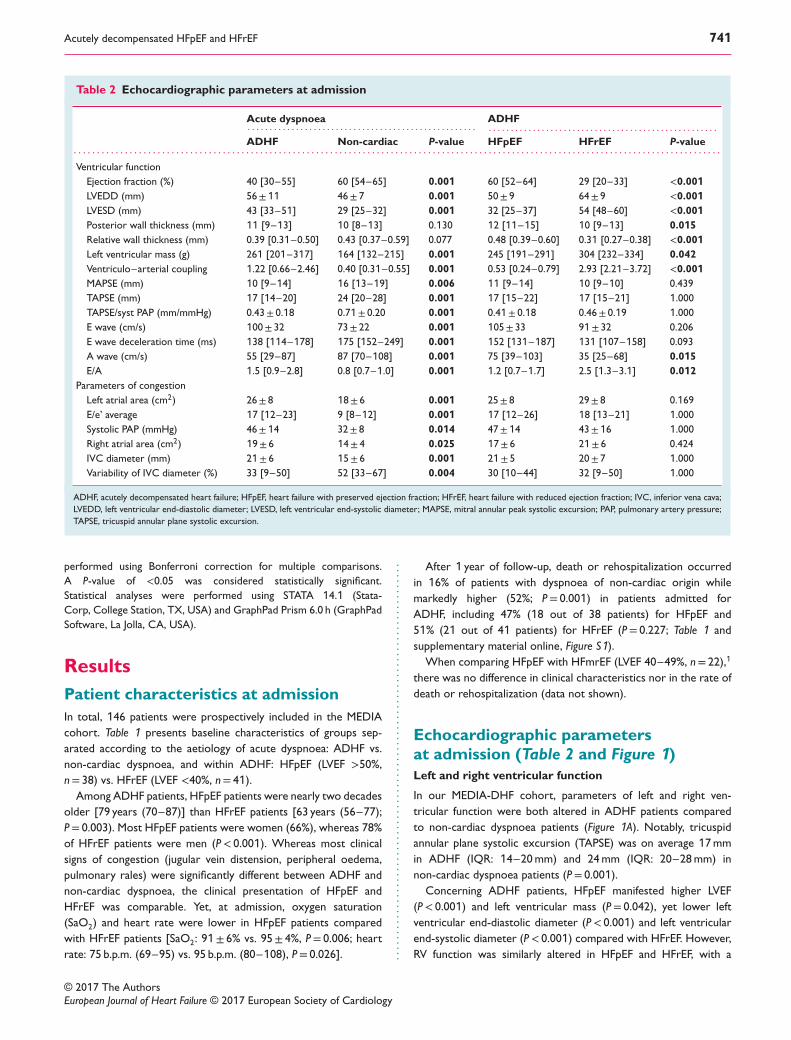
Table 2 Echocardiographic parameters at admission
Acute dyspnoea ADHF. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ADHF Non-cardiac P-value HFpEF HFrEF P-value. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Ventricular function
Ejection fraction (%) 40 [30–55] 60 [54–65] 0.001 60 [52–64] 29 [20–33] <0.001
LVEDD (mm) 56±11 46± 7 0.001 50± 9 64± 9 <0.001
LVESD (mm) 43 [33–51] 29 [25–32] 0.001 32 [25–37] 54 [48–60] <0.001
Posterior wall thickness (mm) 11 [9–13] 10 [8–13] 0.130 12 [11–15] 10 [9–13] 0.015
Relative wall thickness (mm) 0.39 [0.31–0.50] 0.43 [0.37–0.59] 0.077 0.48 [0.39–0.60] 0.31 [0.27–0.38] <0.001
Left ventricular mass (g) 261 [201–317] 164 [132–215] 0.001 245 [191–291] 304 [232–334] 0.042
Ventriculo–arterial coupling 1.22 [0.66–2.46] 0.40 [0.31–0.55] 0.001 0.53 [0.24–0.79] 2.93 [2.21–3.72] <0.001
MAPSE (mm) 10 [9–14] 16 [13–19] 0.006 11 [9–14] 10 [9–10] 0.439
TAPSE (mm) 17 [14–20] 24 [20–28] 0.001 17 [15–22] 17 [15–21] 1.000
TAPSE/syst PAP (mm/mmHg)
E wave (cm/s)
0.43± 0.18
100± 32
0.71± 0.20
73± 22
0.001
0.001
0.41± 0.18
105± 33
0.46± 0.19
91± 32
1.000
0.206
E wave deceleration time (ms) 138 [114–178] 175 [152–249] 0.001 152 [131–187] 131 [107–158] 0.093
A wave (cm/s) 55 [29–87] 87 [70–108] 0.001 75 [39–103] 35 [25–68] 0.015
E/A 1.5 [0.9–2.8] 0.8 [0.7–1.0] 0.001 1.2 [0.7–1.7] 2.5 [1.3–3.1] 0.012
Parameters of congestion
Left atrial area (cm2)
E/e’ average
26± 8
17 [12–23]
18± 6
9 [8–12]
0.001
0.001
25± 8
17 [12–26]
29± 8
18 [13–21]
0.169
1.000
Systolic PAP (mmHg) 46±14 32± 8 0.014 47±14 43±16 1.000
Right atrial area (cm2) 19± 6 14± 4 0.025 17± 6 21± 6 0.424
IVC diameter (mm) 21± 6 15± 6 0.001 21± 5 20± 7 1.000
Variability of IVC diameter (%) 33 [9–50] 52 [33–67] 0.004 30 [10–44] 32 [9–50] 1.000
ADHF, acutely decompensated heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IVC, inferior vena cava;
LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; MAPSE, mitral annular peak systolic excursion; PAP, pulmonary artery pressure;
TAPSE, tricuspid annular plane systolic excursion.
performed using Bonferroni correction for multiple comparisons.
A P-value of <0.05 was considered statistically significant.
Statistical analyses were performed using STATA 14.1 (Stata-
Corp, College Station, TX, USA) and GraphPad Prism 6.0 h (GraphPad
Software, La Jolla, CA, USA).
Results
Patient characteristics at admission
In total, 146 patients were prospectively included in the MEDIA
cohort. Table 1 presents baseline characteristics of groups sep-
arated according to the aetiology of acute dyspnoea: ADHF vs.
non-cardiac dyspnoea, and within ADHF: HFpEF (LVEF >50%,
n= 38) vs. HFrEF (LVEF <40%, n= 41).
Among ADHF patients, HFpEF patients were nearly two decades
older [79 years (70–87)] than HFrEF patients [63 years (56–77);
P= 0.003). Most HFpEF patients were women (66%), whereas 78%
of HFrEF patients were men (P< 0.001). Whereas most clinical
signs of congestion (jugular vein distension, peripheral oedema,
pulmonary rales) were significantly different between ADHF and
non-cardiac dyspnoea, the clinical presentation of HFpEF and
HFrEF was comparable. Yet, at admission, oxygen saturation
(SaO2) and heart rate were lower in HFpEF patients compared
with HFrEF patients [SaO2: 91± 6% vs. 95± 4%, P= 0.006; heart
rate: 75 b.p.m. (69–95) vs. 95 b.p.m. (80–108), P= 0.026]. ............................................................................ After 1 year of follow-up, death or rehospitalization occurred
in 16% of patients with dyspnoea of non-cardiac origin while
markedly higher (52%; P= 0.001) in patients admitted for
ADHF, including 47% (18 out of 38 patients) for HFpEF and
51% (21 out of 41 patients) for HFrEF (P= 0.227; Table 1 and
supplementary material online, Figure S1).
When comparing HFpEF with HFmrEF (LVEF 40–49%, n= 22),1
there was no difference in clinical characteristics nor in the rate of
death or rehospitalization (data not shown).
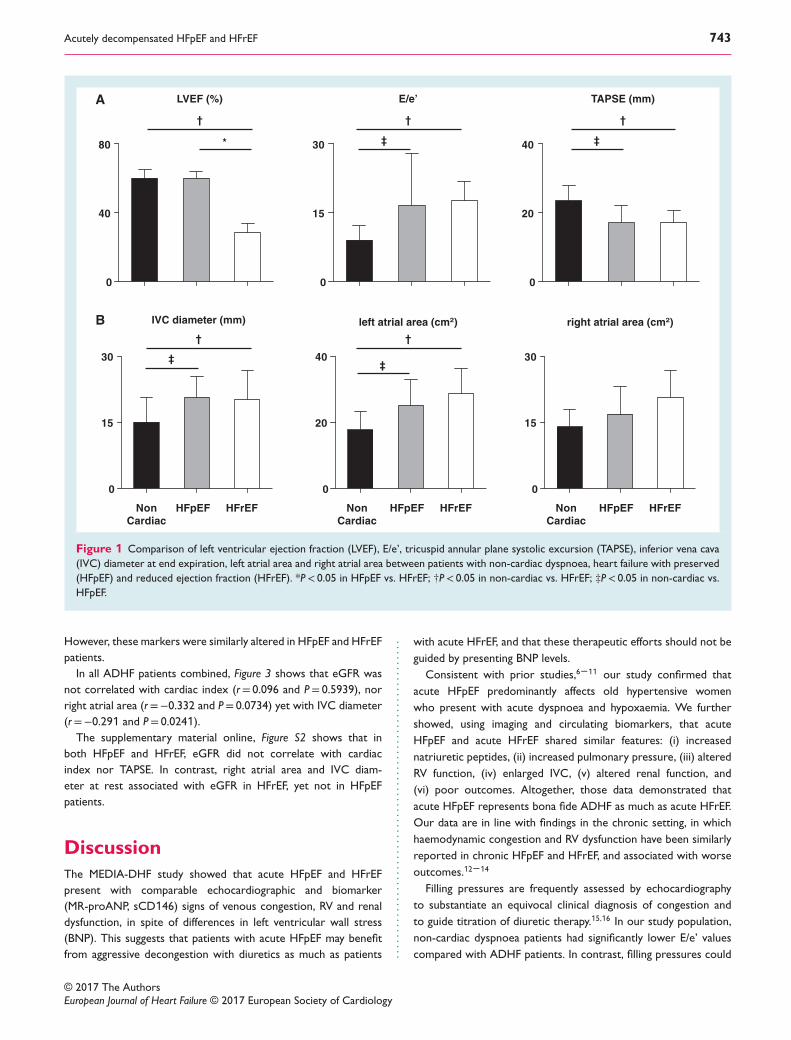
Echocardiographic parametersat admission (Table 2 and Figure 1)
Left and right ventricular function
In our MEDIA-DHF cohort, parameters of left and right ven-
tricular function were both altered in ADHF patients compared
to non-cardiac dyspnoea patients (Figure 1A). Notably, tricuspid
annular plane systolic excursion (TAPSE) was on average 17mm
in ADHF (IQR: 14–20mm) and 24mm (IQR: 20–28mm) in
non-cardiac dyspnoea patients (P= 0.001).
Concerning ADHF patients, HFpEF manifested higher LVEF
(P< 0.001) and left ventricular mass (P= 0.042), yet lower left
ventricular end-diastolic diameter (P< 0.001) and left ventricular
end-systolic diameter (P< 0.001) compared with HFrEF. However,
RV function was similarly altered in HFpEF and HFrEF, with a
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
742 L.N.L. Van Aelst et al.
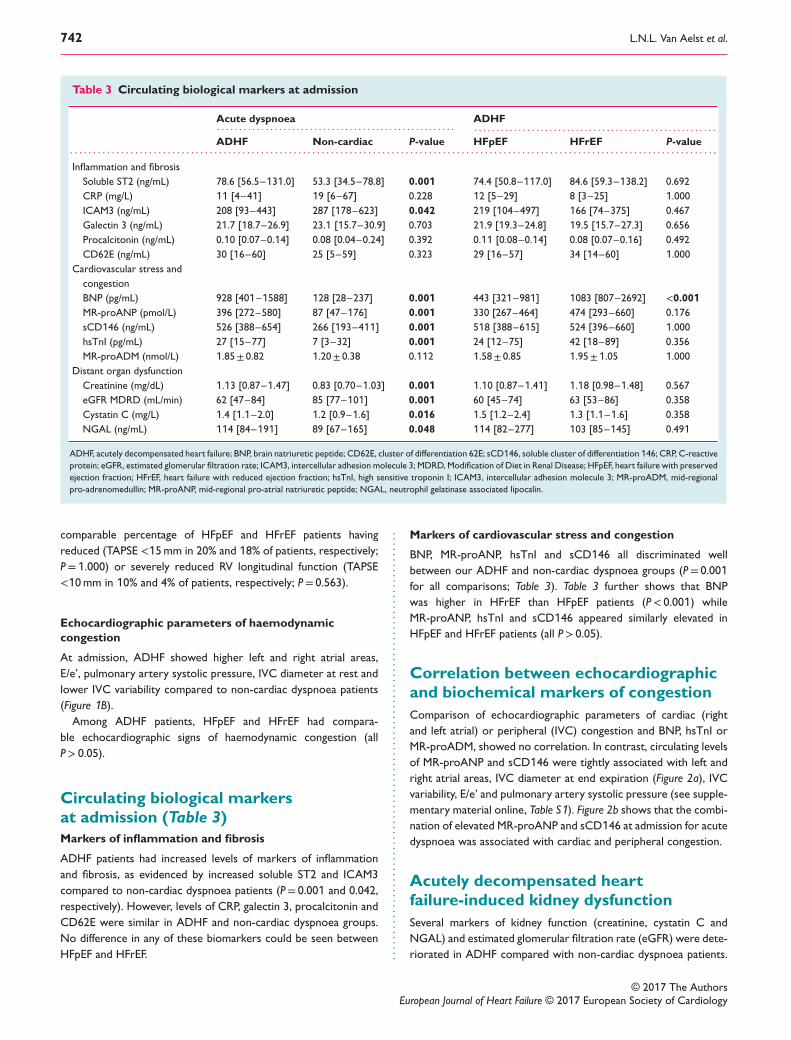
Table 3 Circulating biological markers at admission
Acute dyspnoea ADHF. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ADHF Non-cardiac P-value HFpEF HFrEF P-value. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Inflammation and fibrosis
Soluble ST2 (ng/mL) 78.6 [56.5–131.0] 53.3 [34.5–78.8] 0.001 74.4 [50.8–117.0] 84.6 [59.3–138.2] 0.692
CRP (mg/L) 11 [4–41] 19 [6–67] 0.228 12 [5–29] 8 [3–25] 1.000
ICAM3 (ng/mL) 208 [93–443] 287 [178–623] 0.042 219 [104–497] 166 [74–375] 0.467
Galectin 3 (ng/mL) 21.7 [18.7–26.9] 23.1 [15.7–30.9] 0.703 21.9 [19.3–24.8] 19.5 [15.7–27.3] 0.656
Procalcitonin (ng/mL) 0.10 [0.07–0.14] 0.08 [0.04–0.24] 0.392 0.11 [0.08–0.14] 0.08 [0.07–0.16] 0.492
CD62E (ng/mL) 30 [16–60] 25 [5–59] 0.323 29 [16–57] 34 [14–60] 1.000
Cardiovascular stress and
congestion
BNP (pg/mL) 928 [401–1588] 128 [28–237] 0.001 443 [321–981] 1083 [807–2692] <0.001
MR-proANP (pmol/L) 396 [272–580] 87 [47–176] 0.001 330 [267–464] 474 [293–660] 0.176
sCD146 (ng/mL) 526 [388–654] 266 [193–411] 0.001 518 [388–615] 524 [396–660] 1.000
hsTnI (pg/mL)
MR-proADM (nmol/L)
27 [15–77]
1.85± 0.82
7 [3–32]
1.20± 0.38
0.001
0.112
24 [12–75]
1.58± 0.85
42 [18–89]
1.95±1.05
0.356
1.000
Distant organ dysfunction
Creatinine (mg/dL) 1.13 [0.87–1.47] 0.83 [0.70–1.03] 0.001 1.10 [0.87–1.41] 1.18 [0.98–1.48] 0.567
eGFR MDRD (mL/min) 62 [47–84] 85 [77–101] 0.001 60 [45–74] 63 [53–86] 0.358
Cystatin C (mg/L) 1.4 [1.1–2.0] 1.2 [0.9–1.6] 0.016 1.5 [1.2–2.4] 1.3 [1.1–1.6] 0.358
NGAL (ng/mL) 114 [84–191] 89 [67–165] 0.048 114 [82–277] 103 [85–145] 0.491
ADHF, acutely decompensated heart failure; BNP, brain natriuretic peptide; CD62E, cluster of differentiation 62E; sCD146, soluble cluster of differentiation 146; CRP, C-reactive
protein; eGFR, estimated glomerular filtration rate; ICAM3, intercellular adhesion molecule 3; MDRD, Modification of Diet in Renal Disease; HFpEF, heart failure with preserved
ejection fraction; HFrEF, heart failure with reduced ejection fraction; hsTnI, high sensitive troponin I; ICAM3, intercellular adhesion molecule 3; MR-proADM, mid-regional
pro-adrenomedullin; MR-proANP, mid-regional pro-atrial natriuretic peptide; NGAL, neutrophil gelatinase associated lipocalin.
comparable percentage of HFpEF and HFrEF patients having
reduced (TAPSE <15mm in 20% and 18% of patients, respectively;
P=1.000) or severely reduced RV longitudinal function (TAPSE
<10mm in 10% and 4% of patients, respectively; P= 0.563).
Echocardiographic parameters of haemodynamic
congestion
At admission, ADHF showed higher left and right atrial areas,
E/e’, pulmonary artery systolic pressure, IVC diameter at rest and
lower IVC variability compared to non-cardiac dyspnoea patients
(Figure 1B).
Among ADHF patients, HFpEF and HFrEF had compara-
ble echocardiographic signs of haemodynamic congestion (all
P> 0.05).
Circulating biological markersat admission (Table 3)
Markers of inflammation and fibrosis
ADHF patients had increased levels of markers of inflammation
and fibrosis, as evidenced by increased soluble ST2 and ICAM3
compared to non-cardiac dyspnoea patients (P= 0.001 and 0.042,
respectively). However, levels of CRP, galectin 3, procalcitonin and
CD62E were similar in ADHF and non-cardiac dyspnoea groups.
No difference in any of these biomarkers could be seen between
HFpEF and HFrEF. .................................................................................. Markers of cardiovascular stress and congestion
BNP, MR-proANP, hsTnI and sCD146 all discriminated well
between our ADHF and non-cardiac dyspnoea groups (P= 0.001
for all comparisons; Table 3). Table 3 further shows that BNP
was higher in HFrEF than HFpEF patients (P< 0.001) while
MR-proANP, hsTnI and sCD146 appeared similarly elevated in
HFpEF and HFrEF patients (all P> 0.05).
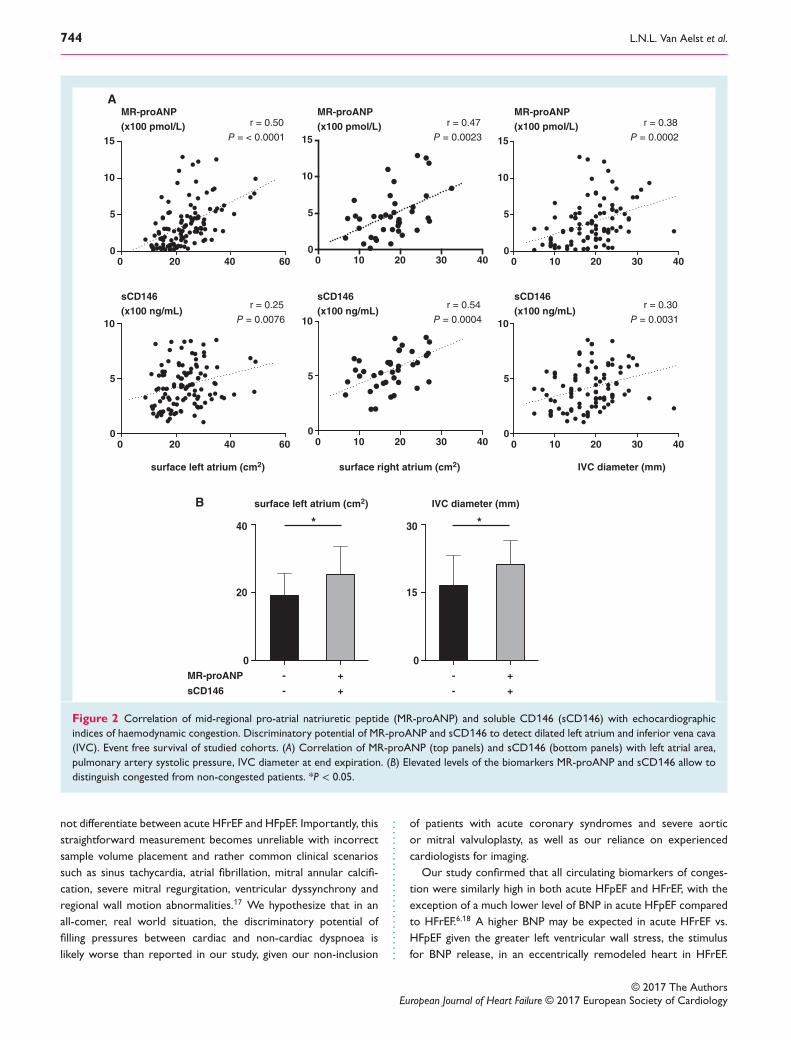
Correlation between echocardiographicand biochemical markers of congestion
Comparison of echocardiographic parameters of cardiac (right
and left atrial) or peripheral (IVC) congestion and BNP, hsTnI or
MR-proADM, showed no correlation. In contrast, circulating levels
of MR-proANP and sCD146 were tightly associated with left and
right atrial areas, IVC diameter at end expiration (Figure 2a), IVC
variability, E/e’ and pulmonary artery systolic pressure (see supple-
mentary material online, Table S1). Figure 2b shows that the combi-
nation of elevated MR-proANP and sCD146 at admission for acute
dyspnoea was associated with cardiac and peripheral congestion.
Acutely decompensated heartfailure-induced kidney dysfunction
Several markers of kidney function (creatinine, cystatin C and
NGAL) and estimated glomerular filtration rate (eGFR) were dete-
riorated in ADHF compared with non-cardiac dyspnoea patients.
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
Acutely decompensated HFpEF and HFrEF 743
HFpEF HFrEF
0
15
30
HFpEF HFrEF
0
20
40
Non
Cardiac
Non
Cardiac
Non
Cardiac
HFpEF HFrEF
0
15
30
right atrial area (cm2)
0
20
40
0
15
30
0
40
80
E/e’
left atrial area (cm2)IVC diameter (mm)
*
†
LVEF (%)
†
† †
TAPSE (mm)
†
‡
‡‡
A
B
‡
Figure 1 Comparison of left ventricular ejection fraction (LVEF), E/e’, tricuspid annular plane systolic excursion (TAPSE), inferior vena cava
(IVC) diameter at end expiration, left atrial area and right atrial area between patients with non-cardiac dyspnoea, heart failure with preserved
(HFpEF) and reduced ejection fraction (HFrEF). *P< 0.05 in HFpEF vs. HFrEF; †P< 0.05 in non-cardiac vs. HFrEF; ‡P< 0.05 in non-cardiac vs.
HFpEF.
However, these markers were similarly altered in HFpEF and HFrEF
patients.
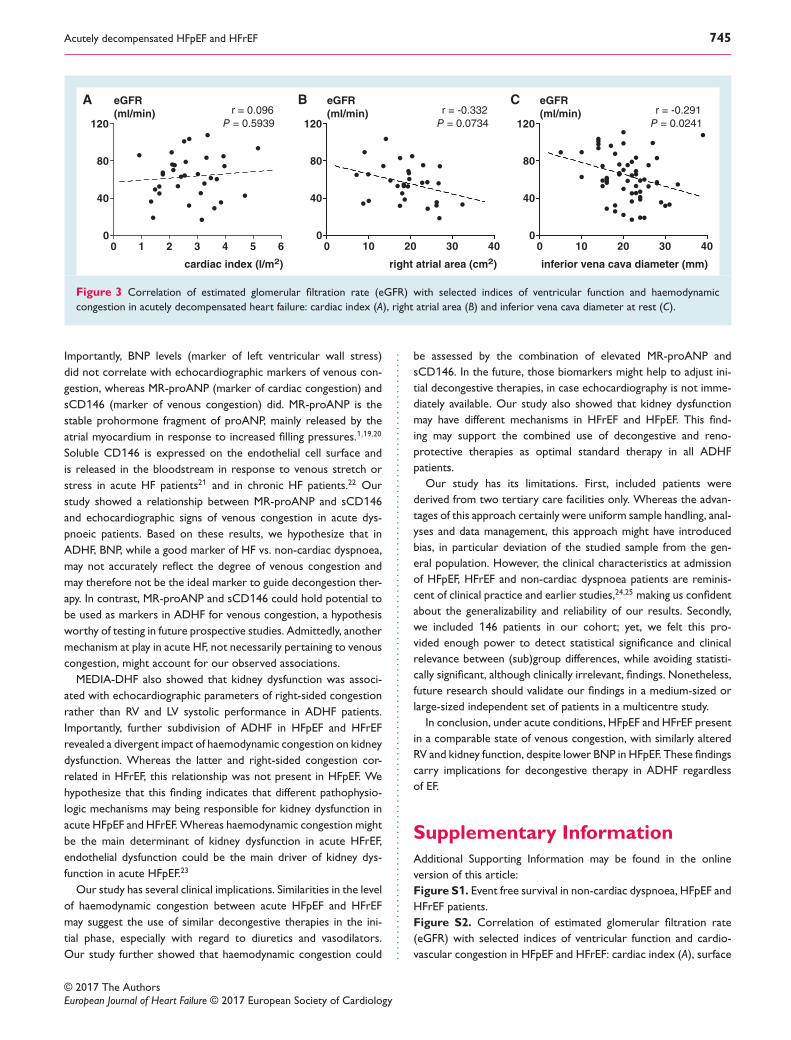
In all ADHF patients combined, Figure 3 shows that eGFR was
not correlated with cardiac index (r= 0.096 and P= 0.5939), nor
right atrial area (r=−0.332 and P= 0.0734) yet with IVC diameter
(r=−0.291 and P= 0.0241).
The supplementary material online, Figure S2 shows that in
both HFpEF and HFrEF, eGFR did not correlate with cardiac
index nor TAPSE. In contrast, right atrial area and IVC diam-
eter at rest associated with eGFR in HFrEF, yet not in HFpEF
patients.
Discussion
The MEDIA-DHF study showed that acute HFpEF and HFrEF
present with comparable echocardiographic and biomarker
(MR-proANP, sCD146) signs of venous congestion, RV and renal
dysfunction, in spite of differences in left ventricular wall stress
(BNP). This suggests that patients with acute HFpEF may benefit
from aggressive decongestion with diuretics as much as patients ............................................................. with acute HFrEF, and that these therapeutic efforts should not be
guided by presenting BNP levels.
Consistent with prior studies,6–11 our study confirmed that
acute HFpEF predominantly affects old hypertensive women
who present with acute dyspnoea and hypoxaemia. We further
showed, using imaging and circulating biomarkers, that acute
HFpEF and acute HFrEF shared similar features: (i) increased
natriuretic peptides, (ii) increased pulmonary pressure, (iii) altered
RV function, (iv) enlarged IVC, (v) altered renal function, and
(vi) poor outcomes. Altogether, those data demonstrated that
acute HFpEF represents bona fide ADHF as much as acute HFrEF.
Our data are in line with findings in the chronic setting, in which
haemodynamic congestion and RV dysfunction have been similarly
reported in chronic HFpEF and HFrEF, and associated with worse
outcomes.12–14
Filling pressures are frequently assessed by echocardiography
to substantiate an equivocal clinical diagnosis of congestion and
to guide titration of diuretic therapy.15,16 In our study population,
non-cardiac dyspnoea patients had significantly lower E/e’ values
compared with ADHF patients. In contrast, filling pressures could
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
744 L.N.L. Van Aelst et al.
0 10 20 30 400
5
10
0 10 20 30 400
5
10
15
0
15
30
20
40
0 10 20 30 400
5
10
0 20 40 600
5
10
0 10 20 30 400
5
10
15
0 20 40 600
5
10
15
MR-proANP
A
B
(x100 pmol/L)
MR-proANP
(x100 pmol/L)
MR-proANP
(x100 pmol/L)
sCD146
(x100 ng/mL)
sCD146
(x100 ng/mL)
sCD146
(x100 ng/mL)
surface left atrium (cm2) surface right atrium (cm2) IVC diameter (mm)
r = 0.25
P = 0.0076
r = 0.54
P = 0.0004
r = 0.30
P = 0.0031
r = 0.50
P = < 0.0001
r = 0.47
P = 0.0023
r = 0.38
P = 0.0002
-
-
0
MR-proANP
sCD146
+
+
-
-
+
+
*
surface left atrium (cm2) IVC diameter (mm)
*
Figure 2 Correlation of mid-regional pro-atrial natriuretic peptide (MR-proANP) and soluble CD146 (sCD146) with echocardiographic
indices of haemodynamic congestion. Discriminatory potential of MR-proANP and sCD146 to detect dilated left atrium and inferior vena cava
(IVC). Event free survival of studied cohorts. (A) Correlation of MR-proANP (top panels) and sCD146 (bottom panels) with left atrial area,
pulmonary artery systolic pressure, IVC diameter at end expiration. (B) Elevated levels of the biomarkers MR-proANP and sCD146 allow to
distinguish congested from non-congested patients. *P < 0.05.
not differentiate between acute HFrEF and HFpEF. Importantly, this
straightforward measurement becomes unreliable with incorrect
sample volume placement and rather common clinical scenarios
such as sinus tachycardia, atrial fibrillation, mitral annular calcifi-
cation, severe mitral regurgitation, ventricular dyssynchrony and
regional wall motion abnormalities.17 We hypothesize that in an
all-comer, real world situation, the discriminatory potential of
filling pressures between cardiac and non-cardiac dyspnoea is
likely worse than reported in our study, given our non-inclusion ........................... of patients with acute coronary syndromes and severe aortic
or mitral valvuloplasty, as well as our reliance on experienced
cardiologists for imaging.
Our study confirmed that all circulating biomarkers of conges-
tion were similarly high in both acute HFpEF and HFrEF, with the
exception of a much lower level of BNP in acute HFpEF compared
to HFrEF.6,18 A higher BNP may be expected in acute HFrEF vs.
HFpEF given the greater left ventricular wall stress, the stimulus
for BNP release, in an eccentrically remodeled heart in HFrEF.
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
Acutely decompensated HFpEF and HFrEF 745
0 10 20 30 400
40
80
120
0 10 20 30 400
40
80
120
0 1 2 3 4 5 60
40
80
120
eGFR
(ml/min)
eGFR A B C(ml/min)
eGFR
(ml/min)r = 0.096
P = 0.5939
r = -0.332
P = 0.0734
r = -0.291
P = 0.0241
right atrial area (cm2)cardiac index (l/m2) inferior vena cava diameter (mm)
Figure 3 Correlation of estimated glomerular filtration rate (eGFR) with selected indices of ventricular function and haemodynamic
congestion in acutely decompensated heart failure: cardiac index (A), right atrial area (B) and inferior vena cava diameter at rest (C).
Importantly, BNP levels (marker of left ventricular wall stress)
did not correlate with echocardiographic markers of venous con-
gestion, whereas MR-proANP (marker of cardiac congestion) and
sCD146 (marker of venous congestion) did. MR-proANP is the
stable prohormone fragment of proANP, mainly released by the
atrial myocardium in response to increased filling pressures.1,19,20
Soluble CD146 is expressed on the endothelial cell surface and
is released in the bloodstream in response to venous stretch or
stress in acute HF patients21 and in chronic HF patients.22 Our
study showed a relationship between MR-proANP and sCD146
and echocardiographic signs of venous congestion in acute dys-
pnoeic patients. Based on these results, we hypothesize that in
ADHF, BNP, while a good marker of HF vs. non-cardiac dyspnoea,
may not accurately reflect the degree of venous congestion and
may therefore not be the ideal marker to guide decongestion ther-
apy. In contrast, MR-proANP and sCD146 could hold potential to
be used as markers in ADHF for venous congestion, a hypothesis
worthy of testing in future prospective studies. Admittedly, another
mechanism at play in acute HF, not necessarily pertaining to venous
congestion, might account for our observed associations.
MEDIA-DHF also showed that kidney dysfunction was associ-
ated with echocardiographic parameters of right-sided congestion
rather than RV and LV systolic performance in ADHF patients.
Importantly, further subdivision of ADHF in HFpEF and HFrEF
revealed a divergent impact of haemodynamic congestion on kidney
dysfunction. Whereas the latter and right-sided congestion cor-
related in HFrEF, this relationship was not present in HFpEF. We
hypothesize that this finding indicates that different pathophysio-
logic mechanisms may being responsible for kidney dysfunction in
acute HFpEF and HFrEF.Whereas haemodynamic congestion might
be the main determinant of kidney dysfunction in acute HFrEF,
endothelial dysfunction could be the main driver of kidney dys-
function in acute HFpEF.23
Our study has several clinical implications. Similarities in the level
of haemodynamic congestion between acute HFpEF and HFrEF
may suggest the use of similar decongestive therapies in the ini-
tial phase, especially with regard to diuretics and vasodilators.
Our study further showed that haemodynamic congestion could .................................................................................................................... be assessed by the combination of elevated MR-proANP and
sCD146. In the future, those biomarkers might help to adjust ini-
tial decongestive therapies, in case echocardiography is not imme-
diately available. Our study also showed that kidney dysfunction
may have different mechanisms in HFrEF and HFpEF. This find-
ing may support the combined use of decongestive and reno-
protective therapies as optimal standard therapy in all ADHF
patients.
Our study has its limitations. First, included patients were
derived from two tertiary care facilities only. Whereas the advan-
tages of this approach certainly were uniform sample handling, anal-
yses and data management, this approach might have introduced
bias, in particular deviation of the studied sample from the gen-
eral population. However, the clinical characteristics at admission
of HFpEF, HFrEF and non-cardiac dyspnoea patients are reminis-
cent of clinical practice and earlier studies,24,25 making us confident
about the generalizability and reliability of our results. Secondly,
we included 146 patients in our cohort; yet, we felt this pro-
vided enough power to detect statistical significance and clinical
relevance between (sub)group differences, while avoiding statisti-
cally significant, although clinically irrelevant, findings. Nonetheless,
future research should validate our findings in a medium-sized or
large-sized independent set of patients in a multicentre study.
In conclusion, under acute conditions, HFpEF and HFrEF present
in a comparable state of venous congestion, with similarly altered
RV and kidney function, despite lower BNP in HFpEF. These findings
carry implications for decongestive therapy in ADHF regardless
of EF.
Supplementary Information
Additional Supporting Information may be found in the online
version of this article:
Figure S1. Event free survival in non-cardiac dyspnoea, HFpEF and
HFrEF patients.
Figure S2. Correlation of estimated glomerular filtration rate
(eGFR) with selected indices of ventricular function and cardio-
vascular congestion in HFpEF and HFrEF: cardiac index (A), surface
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology

746 L.N.L. Van Aelst et al.
of the right atrium (B) and inferior vena cava (IVC) diameter at
rest (C).
Table S1. Correlation of selected biomarkers with echocardio-
graphic parameters of haemodynamic congestion.
Funding
L.N.L.V.A. is supported by a training grant from the European Soci-
ety of Cardiology (2015; Sophia Antipolis, France) and a travelling
award from the International Society for Heart and Lung Trans-
plantation (August 2015 and 2016; Addison, TX, USA). L.N.L.V.A.
gratefully acknowledges the financial support from the Belgian Fund
for Cardiac Surgery through the Jacqueline Bernheim prize 2015
(Brussels, Belgium). M.A. is recipient of a fellowship of the Collège
de Médecine des Hôpitaux de Paris (Paris, France). M.F.S. received
a grant from the Ligue Française contre la Cardiomyopathie (Mont-
boissier, France). E.A. is supported by a research fellowship from
the Japan Heart Foundation (Tokyo, Japan). This study is supported
by a grant from the European Union (FP7-HEALTH-2010-MEDIA;
Luxembourg) to F.Z., P.R., A.M.
Conflict of interests: L.N.L.V.A., M.A., R.P., E.A., N.G., F.Z.,
P.M., M.B., M.S., J.M.L., E.G. and M.F.S. report no conflict of
interests. P.R. received lecture fees from CVRx and consult-
ing fees from Novartis, Relypsa, AstraZeneca, Stealth Peptides,
Fresenius, Vifor Fresenius Medical Care Renal Pharma, CTMA.
P.R. is cofounder of CardioRenal. A.C.S. received honoraria or
grants from Novartis, Servier, Roche Diagnostics, Alere, Bayer,
Vifor. A.M. received fees as member of advisory board and/or
Steering Committee from Cardiorentis, Adrenomed, MyCartis,
Neurotronik, ZS Pharma and Critical Diagnostics. C.S.P.L. has
received research support from Boston Scientific, Bayer, Ther-
moFisher, Medtronic and Vifor Pharma; and has consulted for
Bayer, Novartis, Takeda, Merck, Astra Zeneca, Janssen Research
& Development, LLC, Menarini, Boehringer Ingelheim and Abbott
Diagnostics.
References1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V,
Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoy-
annopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka
F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treat-
ment of acute and chronic heart failure: The Task Force for the diagnosis and
treatment of acute and chronic heart failure of the European Society of Cardiol-
ogy (ESC) developed with the special contribution of the Heart Failure Associa-
tion (HFA) of the ESC. Eur J Heart Fail 2016;18:891–975.
2. Braunwald E. Heart failure. JACC Heart Fail 2013;1:1–20.
3. Seronde MF, Laribi S, Collins SP, Deye N, Logeart D, Plaisance P, Cohen-Solal A,
Mebazaa A. Heart failure diagnosis in acute conditions has high agreement with
inpatient diagnosis. Eur J Emerg Med 2016;23:179–184.
4. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flach-
skampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D,
Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recom-
mendations for cardiac chamber quantification by echocardiography in adults:
an update from the American Society of Echocardiography and the European
Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2015;16:
233–270.
5. Chantler PD, Lakatta EG, Najjar SS. Arterial-ventricular coupling: mechanistic
insights into cardiovascular performance at rest and during exercise. J Appl Physiol
(1985) 2008;105:1342–1351.
6. Khalid U, Wruck LM, Quibrera PM, Bozkurt B, Nambi V, Virani SS, Jneid H,
Agarwal S, Chang PP, Loehr L, Basra SS, Rosamond W, Ballantyne CM, Deswal
A. BNP and obesity in acute decompensated heart failure with preserved vs. ........................................................................................................................................................................ reduced ejection fraction: The Atherosclerosis Risk in Communities Surveillance
Study. Int J Cardiol 2017;233:61–66.
7. Nakada Y, Kawakami R, Nakano T, Takitsume A, Nakagawa H, Ueda T, Nishida
T, Onoue K, Soeda T, Okayama S, Takeda Y, Watanabe M, Kawata H, Okura
H, Saito Y. Sex differences in clinical characteristics and long-term outcome in
acute decompensated heart failure patients with preserved and reduced ejection
fraction. Am J Physiol Heart Circ Physiol 2016;310:H813–H820.
8. Goyal P, Almarzooq ZI, Horn EM, Karas MG, Sobol I, Swaminathan RV, Feldman
DN, Minutello RM, Singh HS, Bergman GW, Wong SC, Kim LK. Characteristics
of hospitalizations for heart failure with preserved ejection fraction. Am J Med
2016;129:635.e15–26.
9. Bishu K, Deswal A, Chen HH, LeWinter MM, Lewis GD, Semigran MJ, Borlaug
BA, McNulty S, Hernandez AF, Braunwald E, Redfield MM. Biomarkers in acutely
decompensated heart failure with preserved or reduced ejection fraction. Am
Heart J 2012;164:763–770.e3.
10. Quiroz R, Doros G, Shaw P, Liang CS, Gauthier DF, Sam F. Comparison of
characteristics and outcomes of patients with heart failure preserved ejection
fraction versus reduced left ventricular ejection fraction in an urban cohort. Am
J Cardiol 2014;113:691–696.
11. Matsushita K, Minamishima T, Goda A, Ishiguro H, Kosho H, Sakata K, Satoh
T, Yoshino H. Comparison of the reliability of E/E’ to estimate pulmonary
capillary wedge pressure in heart failure patients with preserved ejection fraction
versus those with reduced ejection fraction. Int J Cardiovasc Imaging 2015;31:
1497–1502.
12. Aschauer S, Kammerlander AA, Zotter-Tufaro C, Ristl R, Pfaffenberger S,
Bachmann A, Duca F, Marzluf BA, Bonderman D, Mascherbauer J. The right
heart in heart failure with preserved ejection fraction: insights from cardiac
magnetic resonance imaging and invasive haemodynamics. Eur J Heart Fail 2016;18:
71–80.
13. Gulati A, Ismail TF, Jabbour A, Alpendurada F, Guha K, Ismail NA, Raza S, Khwaja
J, Brown TD, Morarji K, Liodakis E, Roughton M, Wage R, Pakrashi TC, Sharma
R, Carpenter JP, Cook SA, Cowie MR, Assomull RG, Pennell DJ, Prasad SK. The
prevalence and prognostic significance of right ventricular systolic dysfunction in
nonischemic dilated cardiomyopathy. Circulation 2013;128:1623–1633.
14. Melenovsky V, Andersen MJ, Andress K, Reddy YN, Borlaug BA. Lung congestion
in chronic heart failure: haemodynamic, clinical, and prognostic implications. Eur
J Heart Fail 2015;17:1161–1171.
15. Mitter SS, Shah SJ, Thomas JD. A Test in context: E/A and E/e’ to assess diastolic
dysfunction and LV filling pressure. J Am Coll Cardiol 2017;69:1451–1464.
16. Mullens W, Borowski AG, Curtin RJ, Thomas JD, Tang WH. Tissue Doppler
imaging in the estimation of intracardiac filling pressure in decompensated
patients with advanced systolic heart failure. Circulation 2009;119:62–70.
17. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA,
Waggoner AD, Flachskampf FA, Pellikka PA, Evangelisa A. Recommendations for
the evaluation of left ventricular diastolic function by echocardiography. Eur J
Echocardiogr 2009;10:165–193.
18. Maisel AS, McCord J, Nowak RM, Hollander JE, Wu AH, Duc P, Omland T,
Storrow AB, Krishnaswamy P, Abraham WT, Clopton P, Steg G, Aumont
MC, Westheim A, Knudsen CW, Perez A, Kamin R, Kazanegra R, Her-
rmann HC, McCullough PA; Breathing Not Properly Multinational Study
Investigators. Bedside B-Type natriuretic peptide in the emergency diagnosis
of heart failure with reduced or preserved ejection fraction. Results from
the Breathing Not Properly Multinational Study. J Am Coll Cardiol 2003;41:
2010–2017.
19. Maisel A, Mueller C, Nowak R, PeacockWF, Landsberg JW, Ponikowski P, Mockel
M, Hogan C, Wu AH, Richards M, Clopton P, Filippatos GS, Di Somma S, Anand
I, Ng L, Daniels LB, Neath SX, Christenson R, Potocki M, McCord J, Terracciano
G, Kremastinos D, Hartmann O, von Haehling S, Bergmann A, Morgenthaler NG,
Anker SD. Mid-region pro-hormone markers for diagnosis and prognosis in acute
dyspnea: results from the BACH (Biomarkers in Acute Heart Failure) trial. J Am
Coll Cardiol 2010;55:2062–2076.
20. Seronde MF, Gayat E, Logeart D, Lassus J, Laribi S, Boukef R, Sibellas F, Launay JM,
Manivet P, Sadoune M, Nouira S, Solal AC, Mebazaa A, Great N. Comparison of
the diagnostic and prognostic values of B-type and atrial-type natriuretic peptides
in acute heart failure. Int J Cardiol 2013;168:3404–3411.
21. Gayat E, Caillard A, Laribi S, Mueller C, Sadoune M, Seronde MF, Maisel
A, Bartunek J, Vanderheyden M, Desutter J, Dendale P, Thomas G,
Tavares M, Cohen-Solal A, Samuel JL, Mebazaa A. Soluble CD146, a new
endothelial biomarker of acutely decompensated heart failure. Int J Cardiol
2015;199:241–247.
22. Arrigo M, Truong QA, Onat D, Szymonifka J, Gayat E, Tolppanen H, Sadoune
M, Demmer RT, Wong KY, Launay JM, Samuel JL, Cohen-Solal A, Januzzi JL, Jr,
Singh JP, Colombo PC, Mebazaa A. Soluble CD146 is a novel marker of systemic
congestion in heart failure patients: an experimental mechanistic and transcardiac
clinical study. Clin Chem 2017;63:386–393.
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology

Acutely decompensated HFpEF and HFrEF 747
23. Ter Maaten JM, Damman K, Verhaar MC, Paulus WJ, Duncker DJ, Cheng
C, van Heerebeek L, Hillege HL, Lam CS, Navis G, Voors AA. Connecting
heart failure with preserved ejection fraction and renal dysfunction: the
role of endothelial dysfunction and inflammation. Eur J Heart Fail 2016;18:
588–598.
24. Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP,
Hochadel M, Komajda M, Lassus J, Lopez-Sendon JL, Ponikowski P, Tavazzi L;
EuroHeart Survey Investigators; Heart Failure Association, European Society ................. of Cardiology. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized
acute heart failure patients: description of population. Eur Heart J 2006;27:
2725–2736.
25. Eurlings LW, Sanders-van Wijk S, van Kimmenade R, Osinski A, van Helmond
L, Vallinga M, Crijns HJ, van Dieijen-Visser MP, Brunner-La Rocca HP, Pinto
YM. Multimarker strategy for short-term risk assessment in patients with
dyspnea in the emergency department: the MARKED (Multi mARKer Emergency
Dyspnea)-risk score. J Am Coll Cardiol 2012;60:1668–1677.
© 2017 The AuthorsEuropean Journal of Heart Failure © 2017 European Society of Cardiology
47
IV. Intérêt du Mid-Regional pro
Atrial Natriuretic Peptide et du
Soluble Cluster of Differentiation 146
dans l’évaluation de la sévérité et du
traitement percutané de la sténose
mitrale
48
IV.1. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide et du Soluble Cluster
of Differentiation 146 dans l’évaluation de la sévérité de la sténose mitrale
Role of cardiovascular biomarkers for the assessment of mitral stenosis and its
complications.
Marc Badoz, Mattia Arrigo, Bernard Iung, Gullu Amioglu, Mehmet Birhan Yilmaz,
Nicolas Meneveau, Malha Sadoune, Agnes Brunette, Alexandre Mebazaa, Marie-France
Seronde.
European Journal of Internal Medicine 34 (2016) 58–62.
AVANT PROPOS
La sténose mitrale est essentiellement d’origine rhumatismale. Même si la prévalence
du rhumatisme articulaire aigu a considérablement diminué, la sténose mitrale représente
encore 10% des valvulopathies (83). Les autres étiologies de sténose mitrale sont dégénératives,
et exceptionnellement post-radiques, congénitales ou toxiques.
La sténose mitrale provoque une augmentation de pression dans la circulation d’amont
à savoir dans l’oreillette gauche, la circulation pulmonaire et enfin les cavités droites. Elle
entraine donc : dilatation de l’oreillette gauche, fibrillation atriale, hypertension artérielle
pulmonaire post capillaire, et enfin à un stade évolué dilatation des cavités droites et
dysfonction ventriculaire droite.
49
L’utilisation de biomarqueurs liés à la sévérité de la sténose et donc au degré d’atteinte
de l’oreillette gauche aurait un intérêt majeur dans cette pathologie. En effet l’évaluation de la
sténose mitrale et de ses complications est classiquement réalisée en échographie cardiaque.
Cette évaluation est nécessaire pour le suivi et en cas d’apparition ou d’aggravation de la
dyspnée chez un porteur de sténose mitrale. L’échographie cardiaque peut poser problème en
termes notamment de disponibilité dans certains centres ou certaines zones peu médicalisées,
elle est opérateur dépendant, subjective et sa qualité dépend de l’échogénicité du patient. Les
formes très évoluées de sténoses mitrales, avec atteinte majeure de l’appareil sous valvulaire,
sont de plus en plus fréquentes, leur évaluation échographique est d’autant plus complexe. Dans
ces conditions l’utilisation d’un biomarqueur lié à la sévérité de la sténose et à ses complications
permettrait de s’affranchir des limites de l’échographie cardiaque. Nous nous sommes donc
intéressés aux performances d’un biomarqueur classique, le BNP, ainsi qu’au MRproANP et
au sCD146 dans ce cadre.

Original Article
Role of cardiovascular biomarkers for the assessment of mitral stenosisand its complications
Marc Badoz a,1, Mattia Arrigo b,c,d,e,1, Bernard Iung f, Gullu Amioglu g, Mehmet Birhan Yilmaz g,Nicolas Meneveau a, Malha Sadoune b, Agnes Brunette a, Alexandre Mebazaa b,c,⁎,2, Marie-France Seronde a,2
a Besancon University Hospital, Besancon, Franceb INSERM UMR-S 942, Paris, Francec Department of Anesthesiology and Critical Care Medicine, AP-HP, Saint Louis Lariboisière University Hospitals, Paris, Franced Department of Cardiology, AP-HP, Saint Louis Lariboisière University Hospitals, Paris, Francee Department of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerlandf Department of Cardiology, AP-HP, Bichat University Hospitals, Paris, Franceg Sivas Numune Hospital, Sivas, Turkey
a b s t r a c ta r t i c l e i n f o
Article history:
Received 1 February 2016
Received in revised form 21 March 2016
Accepted 11 May 2016
Available online 25 May 2016
Background: Mitral stenosis (MS) may cause progressive dyspnea on exertion, pulmonary hypertension (PH),
atrial fibrillation and right ventricular (RV) failure. Patients with MS presenting with change in dyspnea severity
often require a complete cardiologic assessment, but the use of biomarkers may be an alternative for the initial
assessment of MS and its complications. The aim of this study was to evaluate the role of several cardiovascular
biomarkers for this purpose.
Methods: Clinically stable patientswithmoderate or severeMSwere included in this prospectivemulticenter ob-
servational study. ECG, transthoracic echocardiography and biomarker measurement (BNP, MR-proANP and
sCD146) were performed at inclusion. One cohort of patients with pre-capillary PH (PAH)was included for com-
parison of biomarker levels in different etiologies of PH.
Results: A total of 117 MS (70% severe, 30% moderate stenosis) were included. Plasma levels of all three bio-
markers were higher in severe MS compared to moderate MS. PH was associated with higher levels of BNP
and MR-proANP. The presence of atrial fibrillation increased plasma levels of BNP and sCD146, whereas MR-
proANPwas not affected by atrial fibrillation. PAH patients had higher levels of sCD146 compared toMS patients
with PH. RV dysfunction was associated with higher levels of sCD146.
Conclusion: MS and its complications affect plasma levels of cardiovascular biomarkers. The use of MR-proANP
may be helpful for the assessment of severe stenosis and the presence of PH in the early phase. sCD146 might
help identifying patients with more advanced PH and RV-dysfunction.
© 2016 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved.
Keywords:
Mitral stenosis
Pulmonary hypertension
Biomarker
BNP
MR-proANP
sCD146
1. Introduction
Mitral stenosis (MS) is often a sequel of rheumatic fever and,although rheumatic fever has greatly decreased in industrialized coun-tries, MS still causes significant morbidity and mortality worldwide.MS may not cause symptoms for years and then present with progres-sive dyspnea on exertion, pulmonary hypertension (PH), atrial fibrilla-tion, right ventricular (RV) failure.
Patients with MS presenting with change in dyspnea severity oftenrequire a complete cardiologic assessment including ECG and echocar-diography to exclude disease progression or complications. Indeed,echocardiography allows a comprehensive assessment of valve mor-phology, severity of stenosis and associated conditions. However, asdyspnea is a frequent cause of consultation of emergency departmentsand echocardiography is not always immediately available, especiallyin countries where MS is particularly frequent, the use of biomarkersmay be an interesting alternative for the initial assessment of MS andits complications.
The aims of this studywere to evaluate the role of several cardiovas-cular biomarkers (BNP, MR-proANP, sCD146) in the assessment of MSseverity and its complications, in particular atrialfibrillation, pulmonaryhypertension and RV dysfunction. Natriuretic peptides (e.g. BNP, NT-proBNP and MR-proANP) have been shown to accurately identify
European Journal of Internal Medicine 34 (2016) 58–62
⁎ Corresponding author at: Saint Louis LariboisièreUniversity Hospitals, 2, rueAmbroise
Paré, 75010 Paris, France. Tel.: +33 1 49 95 80 71.
E-mail address: [email protected] (A. Mebazaa).1 Equally contributing first authors.2 Equally contributing senior authors.
http://dx.doi.org/10.1016/j.ejim.2016.05.008
0953-6205/© 2016 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved.
Contents lists available at ScienceDirect
European Journal of Internal Medicine
j ourna l homepage: www.e lsev ie r .com/ locate /e j im

cardiac origin of dyspnea [1–3]. Very recently, the novel endothelial bio-marker sCD146, a marker of peripheral congestion, has been shown tohave similar diagnostic properties to detect cardiac origin of acutedyspnea [4].
Aim of the study was a more complete understanding of cardiovas-cular biomarker behavior in presence ofMS.We hypothesized that BNP,MR-proANP and sCD146 might be useful for the assessment of MSseverity and its complications, in particular pulmonary hypertension.
2. Methods
2.1. Study population
Consecutive, clinically stable patients withmoderate (valve area be-tween 1.5 and 2 cm2) or severe (valve area b 1.5 cm2)MSwere includedin the study between January 1st, 2011 andMarch 31st, 2015. This pro-spective multicenter observational study was performed at the Univer-sity Hospital of Besancon (France), Bichat University Hospital in Paris(France), and Cumhuriyet University Hospital of Sivas (Turkey). Exclu-sion criteria were: age b 18 years; left ventricular ejection fractionb40%; recent acute coronary syndrome or documented coronary dis-ease; combination of MS with severe aortic valve disease or more thanmild mitral regurgitation; recent (b1 month) cardiac decompensation.Patients with high heart rate (N110 beats perminute), uncontrolled hy-pertension (systolic blood pressure N 180 mm Hg), severe anemia(hemoglobin b 9 g/dL) or pregnancy were excluded as well.
One small cohort (n = 16) of patients with pre-capillary PH (PAH)examined at University Hospital of Besancon was included forcomparison of biomarker levels in different etiologies of pulmonaryhypertension.
2.2. Echocardiographic study
All patients underwent transthoracic echocardiography at inclusion,and measurements were made in accordance with the recommenda-tions of the European Association for Echocardiography [5]. Severity ofmitral valve stenosis (MS) was assessed by planimetric evaluation inthe parasternal short axis view. MS was considered severe if the valvearea was ≤1.5 cm2 and moderate if the valve area was between 1.5and 2 cm2. Extent of mitral regurgitation was estimated by color Dopp-ler according to an integrative approach [6] Left ventricular (LV) systolicfunction was evaluated by measurement of the LV ejection fraction bythe Simpson's biplane method. The left atrial size was assessed bymea-suring its area from the apical four chamber view or its volume in boththe four and two chamber views. The left atrium (LA)was considered tobedilated if areawas N20 cm2, or volume N 60mL, or diameter N 40mm.Pulmonary pressures were calculated from maximal tricuspid regurgi-tation velocity on continuous Doppler in the apical four chamberview, taking into account the size and compliance of the inferior venacava. A diagnosis of PH was retained for a tricuspid regurgitationvelocity N 2.8 m/s, corresponding to systolic pulmonary artery pressure(PAP) N30 mm Hg. Right ventricular (RV) function was assessed bymeasuring RV fractional area change (RV fac), tricuspid annular planesystolic excursion (TAPSE) and systolicmyocardial velocity at the lateraltricuspid annulus (TAPSE S′). RV dysfunction was defined as thealteration of any one of these three criteria (i.e. RV fac b 40%,TAPSE b 18 mm; TAPSE S′ b 12 cm/s).
2.3. Biomarker testing
Samples of venous bloodwere drawn on the same day as echocardi-ography was performed. Samples were centrifuged within 10 min in arefrigerated centrifuge, and stored at−80 °C.
BNP was measured using the ARCHITECT i2000 system (AbbottLaboratories, Chicago, IL, USA). MR-proANP was measured usingimmunoluminometric assay (B.R.A.H.M.S. AG, Hennigsdorf, Germany)
and sCD146 using the CY-QUANT ELISA sCD146 kit (Biocytex, Asnieres,France).
2.4. Statistical analysis
Continuous variables are expressed as median (interquartile range),nominal variables as frequency (percentages). Group characteristicswere compared with non-parametric tests: Fisher's exact test or theMann–Whitney U-test for two groups, as appropriate; Chi-square orthe Kruskal–Wallis H-test for three groups, as appropriate. For statisti-cally significant differences between the groups, subsequent pairwisecomparisons were performed using Dunn's procedure with Bonferronicorrection of the p-value for multiple comparisons. Corrected p-valuesare reported. Correlation analysis was performed using Spearman's cor-relation coefficient. The diagnostic performance of all three biomarkerswas assessed by receiver operating characteristic (ROC) analysis andexpressed as area under the curve (AUC). The null hypothesis wasrejected with an adjusted two-sided p-value b 0.05. All analyses wereperformed with the use of IBM SPSS Statistics, Version 21.0. (IBMCorp, Armonk NY, USA).
2.5. Ethical considerations
The study was conducted in accordance with the principles of theDeclaration of Helsinki and local national laws and was approved bythe local Ethical Committee. All patients provided written informedconsent. The study is registered with ClinicalTrials.gov under thenumber NCT01374880.
3. Results
3.1. Study population
A total of 117 patients, predominantly women (n = 96, 72%) withmitral stenosis were included (France n=51; Turkey n=66). In 82 pa-tients (70%) the stenosis was classified as severe and moderate in theother 35 patients (30%). The median planimetric area was 1.34 cm2
(IQR 1.1–1.58 cm2) and left atria were dilated in themajority of patients(n = 104, 89%) with a median diameter of 49 mm (42–54 mm) and avolume of 101 ml (75–135 ml). Pulmonary hypertension (n = 83,71%) and atrial fibrillation (n= 49, 42%) were common among MS pa-tients. Supplementary Fig. 1 illustrates the prevalence of severe stenosis,atrial fibrillation, pulmonary hypertension and their combinations inthe MS population. Table 1 summarizes the baseline characteristics ofthe MS patients. Baseline characteristics of patients with severe MS ac-cording to geographic region of enrollment are summarized in Supple-mentary Table 1.
3.2. Impact of severity ofMS, pulmonary hypertension and atrial fibrillation
on biomarkers.
Patients with severe MS were older (58 years (IQR 49–69 years) vs.47 years (IQR 40–59 years), p = 0.001) and reported more severesymptoms (NYHA classes III–IV: 39% vs. 3%, p b 0.001) compared to pa-tients withmoderateMS.Meanwhile, half of patients were in functionalclass NYHA II (39 patients (48%) with severe stenosis and 19 patients(54%) with moderate stenosis).
As shown in Fig. 1A, plasma levels of BNP (p = 0.029), MR-proANP(p = 0.027) and sCD146 (p = 0.011) were higher in patients with se-vere MS compared to moderate MS. The area under the curve (AUC)after ROC analysis to discriminate between severe and moderate MSwas between 0.63 and 0.65 for all three biomarkers (SupplementaryTable 2). Fig. 1B illustrates that MS patients with systolic pulmonarypressure above 30 mm Hg had higher levels of BNP (p = 0.025) andMR-proANP (p = 0.034) but no change of sCD146 levels compared topatients without PH. Systolic pulmonary artery pressure (sPAP)
59M. Badoz et al. / European Journal of Internal Medicine 34 (2016) 58–62
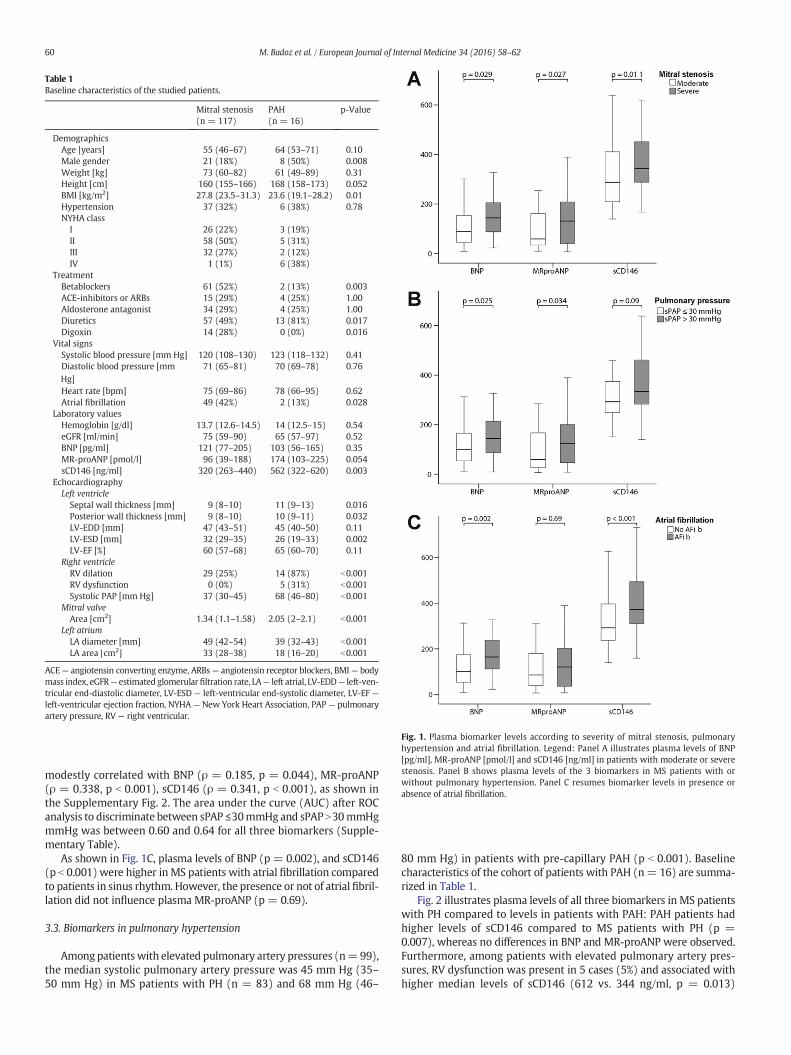
modestly correlated with BNP (ρ = 0.185, p = 0.044), MR-proANP(ρ = 0.338, p b 0.001), sCD146 (ρ = 0.341, p b 0.001), as shown inthe Supplementary Fig. 2. The area under the curve (AUC) after ROCanalysis to discriminate between sPAP ≤30mmHg and sPAP N30mmHgmmHg was between 0.60 and 0.64 for all three biomarkers (Supple-mentary Table).
As shown in Fig. 1C, plasma levels of BNP (p = 0.002), and sCD146(p b 0.001) were higher in MS patients with atrial fibrillation comparedto patients in sinus rhythm. However, the presence or not of atrial fibril-lation did not influence plasma MR-proANP (p = 0.69).
3.3. Biomarkers in pulmonary hypertension
Among patientswith elevated pulmonary artery pressures (n=99),the median systolic pulmonary artery pressure was 45 mm Hg (35–50 mm Hg) in MS patients with PH (n = 83) and 68 mm Hg (46–
80 mm Hg) in patients with pre-capillary PAH (p b 0.001). Baselinecharacteristics of the cohort of patients with PAH (n= 16) are summa-rized in Table 1.
Fig. 2 illustrates plasma levels of all three biomarkers in MS patientswith PH compared to levels in patients with PAH: PAH patients hadhigher levels of sCD146 compared to MS patients with PH (p =0.007), whereas no differences in BNP and MR-proANP were observed.Furthermore, among patients with elevated pulmonary artery pres-sures, RV dysfunction was present in 5 cases (5%) and associated withhigher median levels of sCD146 (612 vs. 344 ng/ml, p = 0.013)
Table 1
Baseline characteristics of the studied patients.
Mitral stenosis
(n = 117)
PAH
(n = 16)
p-Value
Demographics
Age |years] 55 (46–67) 64 (53–71) 0.10
Male gender 21 (18%) 8 (50%) 0.008
Weight [kg] 73 (60–82) 61 (49–89) 0.31
Height [cm] 160 (155–166) 168 (158–173) 0.052
BMI [kg/m2] 27.8 (23.5–31.3) 23.6 (19.1–28.2) 0.01
Hypertension 37 (32%) 6 (38%) 0.78
NYHA class
I 26 (22%) 3 (19%)
II 58 (50%) 5 (31%)
III 32 (27%) 2 (12%)
IV 1 (1%) 6 (38%)
Treatment
Betablockers 61 (52%) 2 (13%) 0.003
ACE-inhibitors or ARBs 15 (29%) 4 (25%) 1.00
Aldosterone antagonist 34 (29%) 4 (25%) 1.00
Diuretics 57 (49%) 13 (81%) 0.017
Digoxin 14 (28%) 0 (0%) 0.016
Vital signs
Systolic blood pressure [mm Hg] 120 (108–130) 123 (118–132) 0.41
Diastolic blood pressure [mm
Hg]
71 (65–81) 70 (69–78) 0.76
Heart rate [bpm] 75 (69–86) 78 (66–95) 0.62
Atrial fibrillation 49 (42%) 2 (13%) 0.028
Laboratory values
Hemoglobin [g/dl] 13.7 (12.6–14.5) 14 (12.5–15) 0.54
eGFR [ml/min] 75 (59–90) 65 (57–97) 0.52
BNP [pg/ml] 121 (77–205) 103 (56–165) 0.35
MR-proANP [pmol/l] 96 (39–188) 174 (103–225) 0.054
sCD146 [ng/ml] 320 (263–440) 562 (322–620) 0.003
Echocardiography
Left ventricle
Septal wall thickness [mm] 9 (8–10) 11 (9–13) 0.016
Posterior wall thickness [mm] 9 (8–10) 10 (9–11) 0.032
LV-EDD [mm] 47 (43–51) 45 (40–50) 0.11
LV-ESD [mm] 32 (29–35) 26 (19–33) 0.002
LV-EF [%] 60 (57–68) 65 (60–70) 0.11
Right ventricle
RV dilation 29 (25%) 14 (87%) b0.001
RV dysfunction 0 (0%) 5 (31%) b0.001
Systolic PAP [mm Hg] 37 (30–45) 68 (46–80) b0.001
Mitral valve
Area [cm2] 1.34 (1.1–1.58) 2.05 (2–2.1) b0.001
Left atrium
LA diameter [mm] 49 (42–54) 39 (32–43) b0.001
LA area |cm2] 33 (28–38) 18 (16–20) b0.001
ACE— angiotensin converting enzyme, ARBs— angiotensin receptor blockers, BMI— body
mass index, eGFR— estimated glomerularfiltration rate, LA— left atrial, LV-EDD— left-ven-
tricular end-diastolic diameter, LV-ESD — left-ventricular end-systolic diameter, LV-EF —
left-ventricular ejection fraction, NYHA— New York Heart Association, PAP— pulmonary
artery pressure, RV — right ventricular.
Fig. 1. Plasma biomarker levels according to severity of mitral stenosis, pulmonary
hypertension and atrial fibrillation. Legend: Panel A illustrates plasma levels of BNP
[pg/ml], MR-proANP [pmol/l] and sCD146 [ng/ml] in patients with moderate or severe
stenosis. Panel B shows plasma levels of the 3 biomarkers in MS patients with or
without pulmonary hypertension. Panel C resumes biomarker levels in presence or
absence of atrial fibrillation.
60 M. Badoz et al. / European Journal of Internal Medicine 34 (2016) 58–62

compared to patients with normal RV function, whereas no differencesin BNP and MR-proANP levels were observed.
4. Discussion
This study aimed at understanding the behavior of cardiovascularbiomarkers in presence of MS and testing their value in the assessmentof MS severity and its complications. This study, performed in a largeprospective cohort of MS patients, demonstrated that plasma levels ofBNP, MR-proANP and sCD146 were higher in patients with severe MScompared to patients with moderate MS. Atrial fibrillation affected allbiomarkers butMR-proANP, and pulmonary hypertensionwas associat-ed with higher levels of BNP and MR-proANP. Finally, PAH and RV dys-function were associated with elevated levels of sCD146.
The usefulness of measurement of natriuretic peptides, especiallyNT-proBNP to assess MS severity was previously described in severalanalyses of small cohorts [7–11]. Our study confirmed the associationbetween levels of BNP and severity of MS and extended the concept totwo other cardiovascular biomarkers, MR-proANP and sCD146. Further-more, atrial fibrillationwas shown to be associatedwith higher levels ofBNP and sCD146 in MS patients. Similar findings were previously de-scribed by Arat-Ozkan and coworkers [7], whereas subsequent studiescould not confirm an effect of atrial fibrillation on BNP or NT-proBNPlevels in MS [12,13]. As BNP and sCD146 levels are affected by the pres-ence of atrial fibrillation, intermittent arrhythmic episodes may impairthe ability of BNP or sCD146 in detecting changes in MS severity duringfollow-up. In contrast, our study showed that levels MR-proANP werenot affected by atrialfibrillation. This characteristicmakes this biomark-er particularly interesting for the evaluation of disease progression inMS patients, as changes in plasma levels might more accurately reflectchanges in MS severity, but needs to be confirmed in further studies.
Previous studies showed the association between pulmonary pres-sure and increased levels of BNP or NT-proBNP in MS [7,9,11,12]. Ourstudy confirmed that MS patients with PH, had higher levels BNP com-pared to MS patients without PH. Similar findings were shown for MR-proANP, whereas no difference in sCD146 levels was found.
On the other hand, among patients with pulmonary hypertension,higher levels of sCD146 were observed in patients with pre-capillaryPAH and in those with RV-dysfunction. The cause for this difference insCD146 levels is unknown.We hypothesize that elevated sCD146 levelsmight represent a more severe stage of pulmonary hypertension. In-deed, PAH patients had significantly higher levels of systolic pulmonarypressure compared toMS patients with PH. However, different underly-ing pathophysiologicalmechanisms between pre- and post-capillary PH(e.g. endothelial dysfunction) may also influence levels of sCD146 [14].
4.1. Limitations
This study also aimed at testing the behavior of cardiac biomarkersin more advanced PH with severe RV pressure overload and ventriculardysfunction. Severe PH and RV dysfunction are serious and, fortunately,rare complications of MS. In addition to including a quite large numberofMS patients through amulti-centric study design, a cohort of PAH pa-tients was included to explore biomarker behavior in advanced PH.However, since the number of patients with RV dysfunction remainedsmall and notable pathophysiological differences between PH second-ary to MS and PAH exist, our observations should be interpreted withcaution.
Given the observational design of the present study, the robustnessof these biomarkers for diagnostic and prognostic purposes and theircost-effectiveness in the follow-up evaluation of MS patients shouldbe prospectively validated in large multi-centric studies.
5. Conclusions
Mitral stenosis and its complications affect plasma levels ofcardiovascular biomarkers. The use of MR-proANP may be useful forthe assessment of severe stenosis and the presence of pulmonaryhypertension in the early phase,whereas sCD146might help identifyingpatients with more advanced pulmonary hypertension and RV-dysfunction.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ejim.2016.05.008.
Disclosures
This project was supported by the European Commission's SeventhFramework program under grant agreement N° 305507 (HOMAGE).MA is a recipient of a fellowship of the Collège de Médecine desHôpitaux de Paris. AM received speaker's honoraria from Abbott,Novartis, Orion, Roche et Servier. AM received fee as a member of advi-sory board and/or Steering Committee from Cardiorentis, Adrenomed,MyCartis, ZS Pharma and Critical Diagnostics.
References
[1] Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Rapidmeasurement of B-type natriuretic peptide in the emergency diagnosis of heart fail-ure. N Engl J Med 2002;347:161–7. http://dx.doi.org/10.1056/NEJMoa020233.
[2] Januzzi JL, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. TheN-terminal pro-BNP investigation of dyspnea in the emergency department(PRIDE) study. Am J Cardiol 2005;95:948–54. http://dx.doi.org/10.1016/j.amjcard.2004.12.032.
[3] Seronde M-F, Gayat E, Logeart D, Lassus J, Laribi S, Boukef R, et al. Comparison of thediagnostic and prognostic values of B-type and atrial-type natriuretic peptides inacute heart failure. Int J Cardiol 2013;168:3404–11. http://dx.doi.org/10.1016/j.ijcard.2013.04.164.
[4] Gayat E, Caillard A, Laribi S, Mueller C, SadouneM, SerondeM-F, et al. Soluble CD146,a new endothelial biomarker of acutely decompensated heart failure. Int J Cardiol2015;199:241–7. http://dx.doi.org/10.1016/j.ijcard.2015.07.039.
[5] Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echo-cardiographic assessment of valve stenosis: EAE/ASE recommendations for clinicalpractice. Eur J Echocardiogr 2009;10:1–25. http://dx.doi.org/10.1093/ejechocard/jen303.
[6] Lancellotti P, Tribouilloy C, Hagendorff A, Popescu BA, Edvardsen T, Pierard LA, et al.Recommendations for the echocardiographic assessment of native valvular regurgi-tation: an executive summary from the European Association of Cardiovascular Im-aging. Eur Heart J Cardiovasc Imaging 2013;14:611–44. http://dx.doi.org/10.1093/ehjci/jet105.
[7] Arat-Ozkan A, Kaya A, Yigit Z, Balci H, Okçün B, Yazicioglu N, et al. Serum N-terminalpro-BNP levels correlate with symptoms and echocardiographic findings in patientswith mitral stenosis. Echocardiography 2005;22:473–8. http://dx.doi.org/10.1111/j.1540-8175.2005.04085.x.
[8] Davutoglu V, Celik A, Aksoy M, Sezen Y, Soydinc S, Gunay N. Plasma NT-proBNP is apotential marker of disease severity and correlates with symptoms in patients withchronic rheumatic valve disease. Eur J Heart Fail 2005;7:532–6. http://dx.doi.org/10.1016/j.ejheart.2004.07.006.
[9] Iltumur K, Karabulut A, Yokus B, Yavuzkir M, Taskesen T, Toprak N. N-terminalproBNP plasma levels correlate with severity of mitral stenosis. J Heart Valve Dis2005;14:735–41.
Fig. 2. Plasma biomarker levels according to etiology of pulmonary hypertension. Legend:
The figure illustrates plasma levels of BNP [pg/ml], MR-proANP [pmol/l] and
sCD146 [ng/ml] in patients with pulmonary hypertension secondary to mitral stenosis
and pre-capillary pulmonary arterial hypertension.
61M. Badoz et al. / European Journal of Internal Medicine 34 (2016) 58–62
[10] Eryol NK, Dogan A, Ozdogru I, Inanc MT, Kaya MG, Kalay N. The relationship be-tween the level of plasma B-type natriuretic peptide and mitral stenosis. Int JCardiovasc Imaging 2007;23:569–74. http://dx.doi.org/10.1007/s10554-006-9174-8.
[11] Sharma V, Stewart RAH, Zeng I, Raffel C, Kerr AJ. Comparison of atrial and brain na-triuretic peptide for the assessment of mitral stenosis. Heart Lung Circ 2011;20:517–24. http://dx.doi.org/10.1016/j.hlc.2011.03.112.
[12] Shang YP, Lai L, Chen J, Zhang F, Wang X. Effects of percutaneous balloon mitralvalvuloplasty on plasma B-type natriuretic peptide in rheumatic mitral stenosiswith and without atrial fibrillation. J Heart Valve Dis 2005;14:453–9.
[13] Pourafkari L, Seyedhosseini S, Kazemi B, Esmaili H, Aslanabadi N. Changes in serumNT-pro BNP and left atrial BNP levels after percutaneous Transvenous mitralCommissurotomy in sinus rhythm versus atrial Firilation. J Cardiovasc Thorac Res2014;6:175–9. http://dx.doi.org/10.15171/jcvtr.2014.007.
[14] Smadja DM, Mauge L, Sanchez O, Silvestre JS, Guerin C, Godier A, et al. Distinct pat-terns of circulating endothelial cells in pulmonary hypertension. Eur Respir J 2010;36:1284–93. http://dx.doi.org/10.1183/09031936.00130809.
62 M. Badoz et al. / European Journal of Internal Medicine 34 (2016) 58–62
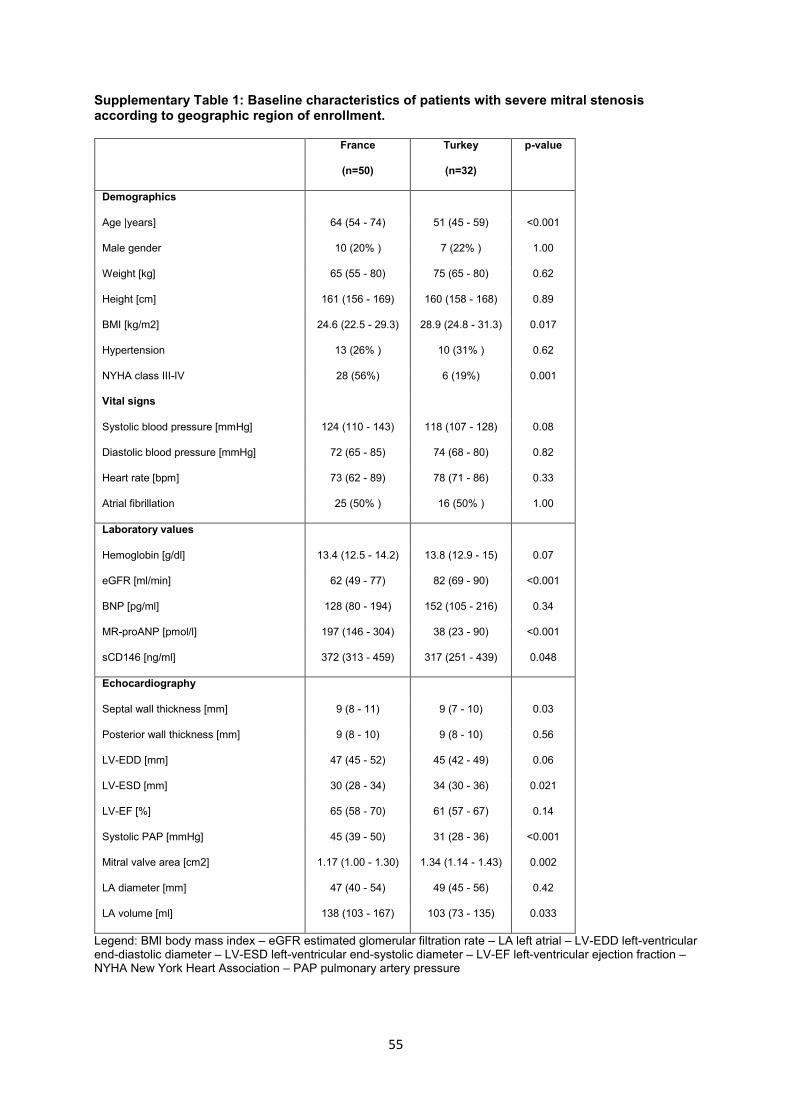
55
Supplementary Table 1: Baseline characteristics of patients with severe mitral stenosis according to geographic region of enrollment.
France
(n=50)
Turkey
(n=32)
p-value
Demographics
Age |years] 64 (54 - 74) 51 (45 - 59) <0.001
Male gender 10 (20% ) 7 (22% ) 1.00
Weight [kg] 65 (55 - 80) 75 (65 - 80) 0.62
Height [cm] 161 (156 - 169) 160 (158 - 168) 0.89
BMI [kg/m2] 24.6 (22.5 - 29.3) 28.9 (24.8 - 31.3) 0.017
Hypertension 13 (26% ) 10 (31% ) 0.62
NYHA class III-IV 28 (56%) 6 (19%) 0.001
Vital signs
Systolic blood pressure [mmHg] 124 (110 - 143) 118 (107 - 128) 0.08
Diastolic blood pressure [mmHg] 72 (65 - 85) 74 (68 - 80) 0.82
Heart rate [bpm] 73 (62 - 89) 78 (71 - 86) 0.33
Atrial fibrillation 25 (50% ) 16 (50% ) 1.00
Laboratory values
Hemoglobin [g/dl] 13.4 (12.5 - 14.2) 13.8 (12.9 - 15) 0.07
eGFR [ml/min] 62 (49 - 77) 82 (69 - 90) <0.001
BNP [pg/ml] 128 (80 - 194) 152 (105 - 216) 0.34
MR-proANP [pmol/l] 197 (146 - 304) 38 (23 - 90) <0.001
sCD146 [ng/ml] 372 (313 - 459) 317 (251 - 439) 0.048
Echocardiography
Septal wall thickness [mm] 9 (8 - 11) 9 (7 - 10) 0.03
Posterior wall thickness [mm] 9 (8 - 10) 9 (8 - 10) 0.56
LV-EDD [mm] 47 (45 - 52) 45 (42 - 49) 0.06
LV-ESD [mm] 30 (28 - 34) 34 (30 - 36) 0.021
LV-EF [%] 65 (58 - 70) 61 (57 - 67) 0.14
Systolic PAP [mmHg] 45 (39 - 50) 31 (28 - 36) <0.001
Mitral valve area [cm2] 1.17 (1.00 - 1.30) 1.34 (1.14 - 1.43) 0.002
LA diameter [mm] 47 (40 - 54) 49 (45 - 56) 0.42
LA volume [ml] 138 (103 - 167) 103 (73 - 135) 0.033
Legend: BMI body mass index – eGFR estimated glomerular filtration rate – LA left atrial – LV-EDD left-ventricular end-diastolic diameter – LV-ESD left-ventricular end-systolic diameter – LV-EF left-ventricular ejection fraction – NYHA New York Heart Association – PAP pulmonary artery pressure
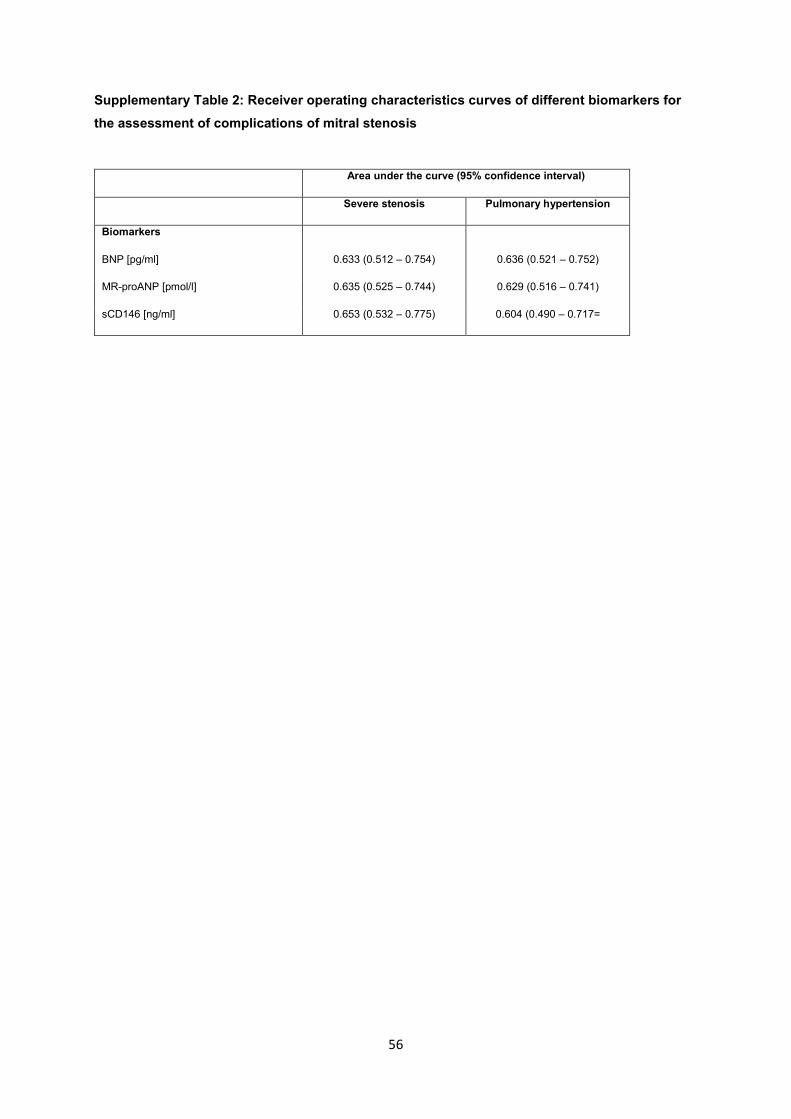
56
Supplementary Table 2: Receiver operating characteristics curves of different biomarkers for the assessment of complications of mitral stenosis
Area under the curve (95% confidence interval)
Severe stenosis Pulmonary hypertension
Biomarkers
BNP [pg/ml] 0.633 (0.512 – 0.754) 0.636 (0.521 – 0.752)
MR-proANP [pmol/l] 0.635 (0.525 – 0.744) 0.629 (0.516 – 0.741)
sCD146 [ng/ml] 0.653 (0.532 – 0.775) 0.604 (0.490 – 0.717=

57
Supplementary Fig. 1. Prevalence of severe stenosis, atrial fibrillation and pulmonary hypertension and their combination in MS patients.
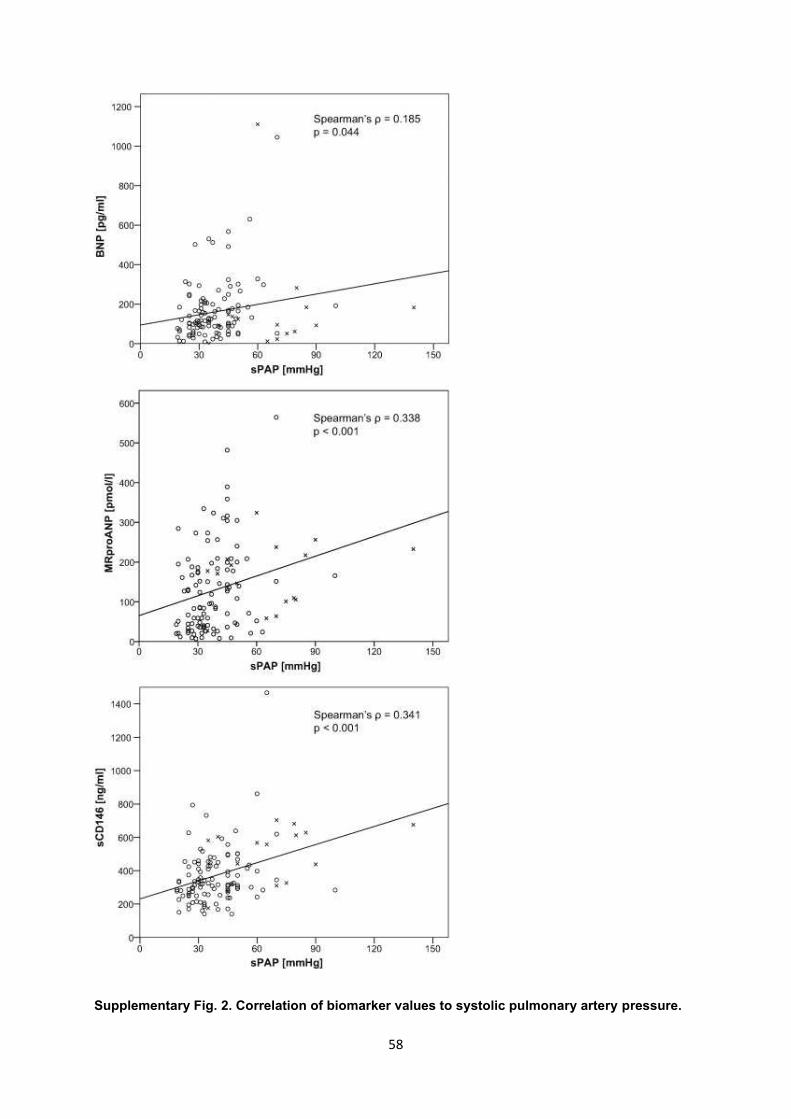
58
Supplementary Fig. 2. Correlation of biomarker values to systolic pulmonary artery pressure.
59
IV.2. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide et du Soluble Cluster
of Differentiation 146 dans l’évaluation du traitement percutané de la sténose
mitrale
Assessment of successful percutaneous mitral commissurotomy by MRproANP and
sCD146.
Marc Badoz, Mattia Arrigo, Anne-Claire Mogenet, Malha Sadoune, Nicolas Meneveau,
Alexandre Mebazaa and Marie-France Seronde.
BMC Cardiovascular Disorders (2020) 20:157.
AVANT PROPOS
La précédente publication a montré la pertinence du sCD146 pour évaluer la sévérité
d’une sténose mitrale ainsi que la présence de complications qu’elles soient rythmiques pour le
passage en FA, ou hémodynamiques avec la présence d’hypertension pulmonaire. Au vu des
connaissances actuelles (20-24) ceci pourrait s’expliquer par la répercussion quasi immédiate
qu’a la sténose mitrale sur la circulation pulmonaire. Nous pourrions émettre en effet
l’hypothèse que celui-ci est sécrété par l’endothélium pulmonaire en réponse à l’élévation de
pression.
Le MRproANP était lui aussi lié à la sévérité de la sténose mitrale, et à la présence de
complications en raison du retentissement directe qu’a la sténose mitrale sur le myocarde
60
atriale. L’élévation de sa concentration plasmatique n’était en revanche pas liée au passage en
FA dans cette pathologie.
Le traitement de la sténose mitrale serrée repose sur une levée de cet obstacle à la
vidange de l’oreillette gauche dans le ventricule. Si la forme anatomique le permet, une
valvuloplastie mitrale est réalisée par voie percutanée (VMP). Ce geste entraine une ouverture
de la valve mitrale, et de ce fait une baisse de pression intra atriale gauche. L’amélioration
hémodynamique et le succès de cette procédure pourraient être monitorés grâce au MRproANP
et au sCD146 étudiés dans la précédente publication. L’objectif étant de nouveau de s’affranchir
des limites de l’échographie cardiaque. Ce monitorage du succès procédural est possible si les
biomarqueurs en question sont liés au niveau de sévérité de la sténose, à la surface mitrale, et
aux modifications hémodynamiques qu’entraine la procédure en termes de baisse de gradient
OG/VG et de baisse des pressions artérielles pulmonaires. Le monitorage du succès immédiat
de la procédure est possible à condition également que la cinétique de libération des
biomarqueurs soit suffisamment réactive et soit telle qu’un succès procédural entraine une
diminution rapide des niveaux plasmatiques des biomarqueurs
La VMP se fait par abord veineux fémoral puis ponction transseptale. La valve mitrale
est alors dilatée grâce à un ballon d’Inoué, cette dilatation permet l’ouverture des commissures
mitrales particulièrement fusionnées dans les formes rhumatismales, la diminution du gradient
de pression entre oreillette gauche et ventricule et donc la limitation des répercussions
hémodynamiques d’amont.
Nous nous sommes donc intéressés aux niveaux de MRproANP et sCD146 avant et
après une procédure de VMP et leur capacité à évaluer le succès de la procédure.
RESEARCH ARTICLE Open Access
Assessment of successful percutaneousmitral commissurotomy by MRproANP andsCD146Marc Badoz1*, Mattia Arrigo2,3,4,5, Anne-Claire Mogenet1, Malha Sadoune2, Nicolas Meneveau1,
Alexandre Mebazaa2,3 and Marie-France Seronde1
Abstract
Background: We studied the course of plasma concentrations of 4 cardiovascular biomarkers: natriuretic peptides
(BNP, NT-proBNP; mid-regional (MR) pro-atrial NP); and soluble endothelial CD146 (sCD146), in patients with severe
mitral valve stenosis undergoing percutaneous mitral commissurotomy (PMC) to identify potential markers of
procedural success.
Methods: Biomarkers were tested in 40 patients the day before and the day after PMC. Success was defined as
mitral valve area ≥ 1.5 cm2; or an increase of ≥0.5 cm2 in mitral valve area associated with echocardiographic mitral
regurgitation <grade 3–4 post-PMC.
Results: Average age was 63.5 ± 12.7 years; 32(80%) were female. Before PMC, mean valve area was 1.1 ± 0.2 cm2,
mean gradient 9.1 ± 3.5 mmHg. PMC was successful in 30 (75%) and unsuccessful in 10 (25%). PMC yielded a significant
reduction in MR-proANP and sCD146, driven by a significant reduction in these biomarkers in patients with successful
procedure, whereas no reduction was observed in patients with unsuccessful procedure. A significant correlation was
found between changes in plasma sCD146 and the relative change in mitral valve area. Elevated pre-procedural sPAP
correlated with high sCD146, and accordingly, a significant correlation between the decrease in sPAP and sCD146 after
PMC was shown.
Conclusions: MR-proANP and plasma sCD146 decreased significantly immediately after successful PMC. They appear
to be markers of immediate success of PMC and of the hemodynamic improvement achieved by this procedure in
patients with MS.
Trial registration: This study is part of the cohorts registered with ClinicalTrials.gov on June 16, 2011 under the
number NCT01374880.
Keywords: Mitral stenosis, Biomarker, Brain natriuretic peptide, MRproANP
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] University Hospital, and EA3920, University of Burgundy
Franche-Comté, Besancon, France
Full list of author information is available at the end of the article
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157
https://doi.org/10.1186/s12872-020-01435-y

Background
The use of natriuretic peptides has become widespread in
cardiology, with brain natriuretic peptide (BNP) and N-
terminal pro-B-type natriuretic peptide (NT-proBNP)
used daily as markers of heart failure [1–3]. However,
these two biomarkers remain imperfect for the diagnosis
of pulmonary and systemic congestion [4–6]. Therefore,
combining BNP/NT-proBNP with other biomarkers could
help to improve their diagnostic value. In this regard,
other natriuretic peptides such as mid-regional pro-atrial
natriuretic peptide (MR-proANP) are emerging as bio-
markers that are more strongly associated with venous
congestion of cardiac origin [7, 8].
Furthermore, the soluble form of CD146 (sCD146) - an
adhesion molecule expressed by vascular endothelial cells
and implicated in vessel integrity - is released by the endo-
thelium [9] and circulating sCD146 levels are related to pul-
monary congestion in heart failure [10, 11]. However, the
physiology of sCD146 release remains poorly described.
Some authors have shown that sCD146 is released from
the peripheral veins in response to stretch [12], but the in-
volvement of the heart cavities, notably the left ventricle,
and pulmonary circulation in the release of sCD146 during
congestion is unknown.
Mitral stenosis (MS) is a clinical condition that induces
left atrial and pulmonary congestion, with preservation of
the left ventricle. Successful percutaneous mitral commis-
surotomy (PMC) reduces left atrial and pulmonary pres-
sures. In this context, the objectives of the present study
were 1) to describe the behaviour of circulating natriuretic
peptides, namely BNP, NT-proBNP, MR-proANP, and
sCD146 before and after PMC for severe MS, and 2) to in-
vestigate a potential role of these cardiovascular bio-
markers to assess procedural success of PMC.
Methods
Prospective study performed in two university hospitals
(University Hospital Jean Minjoz, Besancon, and Univer-
sity Hospital Bichat, Paris, France). Biomarker measure-
ments were performed in the UMR-S942 Inserm, Paris,
France. The study was approved by the Institutional Re-
view Board of Paris North Hospitals, Paris 7 University,
AP-HP, Paris, France (Comité d’Evaluation de l’Ethique
des Projets de Recherche Biomédicale (CEERB) du GHU
Nord, IRB N°00006477) under the number 10–017. All
patients provided written informed consent.
Study population
Patients with symptomatic severe rheumatic MS with an
indication for PMC were included.
Echocardiographic evaluation
All patients underwent transthoracic (TTE) and trans-
oesophageal echocardiography (TOE) by trained operators
on the day before PMC. Echocardiographic control by
TTE was performed 24 h after the procedure to evaluate
procedural success.
Echocardiography was performed to assess left ven-
tricular ejection fraction (LVEF), measured using Simp-
son’s biplane method, severity of MS as assessed by the
mean transmitral gradient on continuous transmitral
Doppler, and mitral valve area as assessed by planimetry
in the parasternal short axis view in accordance with
current guidelines (14). MS was considered severe if the
valve area was ≤1.5 cm2 by planimetry. Further, the anat-
omy of the mitral valve was classified according to the
Wilkins score [13], which takes into account leaflet mo-
bility, leaflet thickening, subvalvular thickening, and cal-
cification. A Wilkins’ score > 8 is associated with
advanced leaflet deformity and unfavorable anatomy,
while a score ≤ 8 corresponds to a valve anatomy more
amenable to PMC. Mitral regurgitation grade was evalu-
ated semi-quantitatively by color flow Doppler imaging
[14]. Left atrial diameter was measured in the paraster-
nal long axis view; left atrial area and volume were eval-
uated in the 2-chamber and 4-chamber apical views.
The left atrium was considered to be dilated if diam-
eter > 40 mm or area > 20 cm2, or volume > 60 mL. Sys-
tolic pulmonary artery pressure was calculated according
to usual techniques and a diagnosis of pulmonary arter-
ial hypertension was retained if peak tricuspid regurgi-
tant velocity > 2.8 m/sec [15]. Significant (moderate or
severe) aortic stenosis was defined as a mean transaortic
gradient > 20mmHg by transthoracic echocardiography.
Definition of procedural success of PMC
Successful PMC was defined as a mitral valve area ≥ 1.5
cm2; or as an increase of ≥0.5 cm2 in mitral valve area
associated with mitral regurgitation less than grade 3–4
post-PMC as measured by echocardiography. Unsuc-
cessful procedural outcome was defined as a post-PMC
mitral valve area < 1.5 cm2; or an increase of < 0.5 cm2 in
mitral valve area or appearance of mitral regurgitation ≥
grade 3–4 [16].
PMC procedure
All procedures were performed in the cardiac
catheterization laboratory under local anesthetic by
trained, experienced operators using the femoral ap-
proach. The Inoue balloon (Toray Medical Co. Ltd.,
Tokyo, Japan) was used in all procedures. The balloon was
inflated gradually with echocardiographic guidance after
each inflation to check for appearance or aggravation of
mitral regurgitation and opening of the two commissures.
Commissural splitting was defined as either an increased
apparent opening angle of either commissure or increased
leaflet separation associated with an increased transverse
diameter of the orifice, or both [17, 18].
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 2 of 9
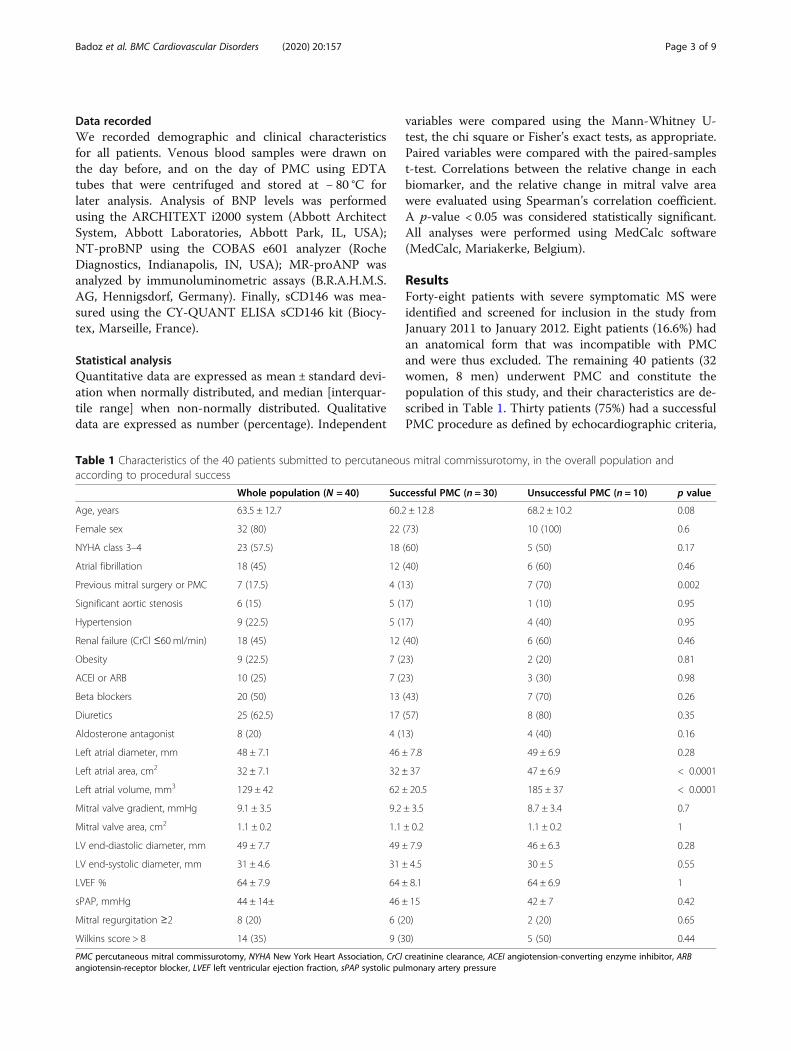
Data recorded
We recorded demographic and clinical characteristics
for all patients. Venous blood samples were drawn on
the day before, and on the day of PMC using EDTA
tubes that were centrifuged and stored at − 80 °C for
later analysis. Analysis of BNP levels was performed
using the ARCHITEXT i2000 system (Abbott Architect
System, Abbott Laboratories, Abbott Park, IL, USA);
NT-proBNP using the COBAS e601 analyzer (Roche
Diagnostics, Indianapolis, IN, USA); MR-proANP was
analyzed by immunoluminometric assays (B.R.A.H.M.S.
AG, Hennigsdorf, Germany). Finally, sCD146 was mea-
sured using the CY-QUANT ELISA sCD146 kit (Biocy-
tex, Marseille, France).
Statistical analysis
Quantitative data are expressed as mean ± standard devi-
ation when normally distributed, and median [interquar-
tile range] when non-normally distributed. Qualitative
data are expressed as number (percentage). Independent
variables were compared using the Mann-Whitney U-
test, the chi square or Fisher’s exact tests, as appropriate.
Paired variables were compared with the paired-samples
t-test. Correlations between the relative change in each
biomarker, and the relative change in mitral valve area
were evaluated using Spearman’s correlation coefficient.
A p-value < 0.05 was considered statistically significant.
All analyses were performed using MedCalc software
(MedCalc, Mariakerke, Belgium).
Results
Forty-eight patients with severe symptomatic MS were
identified and screened for inclusion in the study from
January 2011 to January 2012. Eight patients (16.6%) had
an anatomical form that was incompatible with PMC
and were thus excluded. The remaining 40 patients (32
women, 8 men) underwent PMC and constitute the
population of this study, and their characteristics are de-
scribed in Table 1. Thirty patients (75%) had a successful
PMC procedure as defined by echocardiographic criteria,
Table 1 Characteristics of the 40 patients submitted to percutaneous mitral commissurotomy, in the overall population and
according to procedural success
Whole population (N = 40) Successful PMC (n = 30) Unsuccessful PMC (n = 10) p value
Age, years 63.5 ± 12.7 60.2 ± 12.8 68.2 ± 10.2 0.08
Female sex 32 (80) 22 (73) 10 (100) 0.6
NYHA class 3–4 23 (57.5) 18 (60) 5 (50) 0.17
Atrial fibrillation 18 (45) 12 (40) 6 (60) 0.46
Previous mitral surgery or PMC 7 (17.5) 4 (13) 7 (70) 0.002
Significant aortic stenosis 6 (15) 5 (17) 1 (10) 0.95
Hypertension 9 (22.5) 5 (17) 4 (40) 0.95
Renal failure (CrCl ≤60 ml/min) 18 (45) 12 (40) 6 (60) 0.46
Obesity 9 (22.5) 7 (23) 2 (20) 0.81
ACEI or ARB 10 (25) 7 (23) 3 (30) 0.98
Beta blockers 20 (50) 13 (43) 7 (70) 0.26
Diuretics 25 (62.5) 17 (57) 8 (80) 0.35
Aldosterone antagonist 8 (20) 4 (13) 4 (40) 0.16
Left atrial diameter, mm 48 ± 7.1 46 ± 7.8 49 ± 6.9 0.28
Left atrial area, cm2 32 ± 7.1 32 ± 37 47 ± 6.9 < 0.0001
Left atrial volume, mm3 129 ± 42 62 ± 20.5 185 ± 37 < 0.0001
Mitral valve gradient, mmHg 9.1 ± 3.5 9.2 ± 3.5 8.7 ± 3.4 0.7
Mitral valve area, cm2 1.1 ± 0.2 1.1 ± 0.2 1.1 ± 0.2 1
LV end-diastolic diameter, mm 49 ± 7.7 49 ± 7.9 46 ± 6.3 0.28
LV end-systolic diameter, mm 31 ± 4.6 31 ± 4.5 30 ± 5 0.55
LVEF % 64 ± 7.9 64 ± 8.1 64 ± 6.9 1
sPAP, mmHg 44 ± 14± 46 ± 15 42 ± 7 0.42
Mitral regurgitation ≥2 8 (20) 6 (20) 2 (20) 0.65
Wilkins score > 8 14 (35) 9 (30) 5 (50) 0.44
PMC percutaneous mitral commissurotomy, NYHA New York Heart Association, CrCl creatinine clearance, ACEI angiotension-converting enzyme inhibitor, ARB
angiotensin-receptor blocker, LVEF left ventricular ejection fraction, sPAP systolic pulmonary artery pressure
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 3 of 9
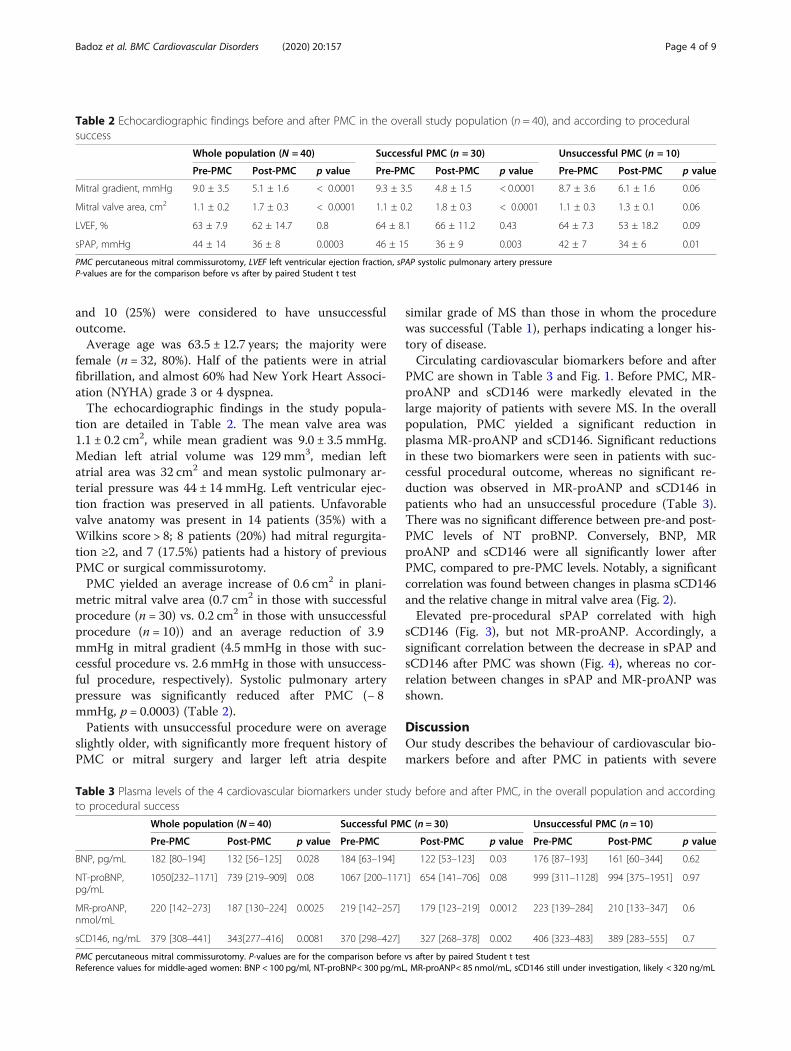
and 10 (25%) were considered to have unsuccessful
outcome.
Average age was 63.5 ± 12.7 years; the majority were
female (n = 32, 80%). Half of the patients were in atrial
fibrillation, and almost 60% had New York Heart Associ-
ation (NYHA) grade 3 or 4 dyspnea.
The echocardiographic findings in the study popula-
tion are detailed in Table 2. The mean valve area was
1.1 ± 0.2 cm2, while mean gradient was 9.0 ± 3.5 mmHg.
Median left atrial volume was 129 mm3, median left
atrial area was 32 cm2 and mean systolic pulmonary ar-
terial pressure was 44 ± 14 mmHg. Left ventricular ejec-
tion fraction was preserved in all patients. Unfavorable
valve anatomy was present in 14 patients (35%) with a
Wilkins score > 8; 8 patients (20%) had mitral regurgita-
tion ≥2, and 7 (17.5%) patients had a history of previous
PMC or surgical commissurotomy.
PMC yielded an average increase of 0.6 cm2 in plani-
metric mitral valve area (0.7 cm2 in those with successful
procedure (n = 30) vs. 0.2 cm2 in those with unsuccessful
procedure (n = 10)) and an average reduction of 3.9
mmHg in mitral gradient (4.5 mmHg in those with suc-
cessful procedure vs. 2.6 mmHg in those with unsuccess-
ful procedure, respectively). Systolic pulmonary artery
pressure was significantly reduced after PMC (− 8
mmHg, p = 0.0003) (Table 2).
Patients with unsuccessful procedure were on average
slightly older, with significantly more frequent history of
PMC or mitral surgery and larger left atria despite
similar grade of MS than those in whom the procedure
was successful (Table 1), perhaps indicating a longer his-
tory of disease.
Circulating cardiovascular biomarkers before and after
PMC are shown in Table 3 and Fig. 1. Before PMC, MR-
proANP and sCD146 were markedly elevated in the
large majority of patients with severe MS. In the overall
population, PMC yielded a significant reduction in
plasma MR-proANP and sCD146. Significant reductions
in these two biomarkers were seen in patients with suc-
cessful procedural outcome, whereas no significant re-
duction was observed in MR-proANP and sCD146 in
patients who had an unsuccessful procedure (Table 3).
There was no significant difference between pre-and post-
PMC levels of NT proBNP. Conversely, BNP, MR
proANP and sCD146 were all significantly lower after
PMC, compared to pre-PMC levels. Notably, a significant
correlation was found between changes in plasma sCD146
and the relative change in mitral valve area (Fig. 2).
Elevated pre-procedural sPAP correlated with high
sCD146 (Fig. 3), but not MR-proANP. Accordingly, a
significant correlation between the decrease in sPAP and
sCD146 after PMC was shown (Fig. 4), whereas no cor-
relation between changes in sPAP and MR-proANP was
shown.
Discussion
Our study describes the behaviour of cardiovascular bio-
markers before and after PMC in patients with severe
Table 2 Echocardiographic findings before and after PMC in the overall study population (n = 40), and according to procedural
success
Whole population (N = 40) Successful PMC (n = 30) Unsuccessful PMC (n = 10)
Pre-PMC Post-PMC p value Pre-PMC Post-PMC p value Pre-PMC Post-PMC p value
Mitral gradient, mmHg 9.0 ± 3.5 5.1 ± 1.6 < 0.0001 9.3 ± 3.5 4.8 ± 1.5 < 0.0001 8.7 ± 3.6 6.1 ± 1.6 0.06
Mitral valve area, cm2 1.1 ± 0.2 1.7 ± 0.3 < 0.0001 1.1 ± 0.2 1.8 ± 0.3 < 0.0001 1.1 ± 0.3 1.3 ± 0.1 0.06
LVEF, % 63 ± 7.9 62 ± 14.7 0.8 64 ± 8.1 66 ± 11.2 0.43 64 ± 7.3 53 ± 18.2 0.09
sPAP, mmHg 44 ± 14 36 ± 8 0.0003 46 ± 15 36 ± 9 0.003 42 ± 7 34 ± 6 0.01
PMC percutaneous mitral commissurotomy, LVEF left ventricular ejection fraction, sPAP systolic pulmonary artery pressure
P-values are for the comparison before vs after by paired Student t test
Table 3 Plasma levels of the 4 cardiovascular biomarkers under study before and after PMC, in the overall population and according
to procedural success
Whole population (N = 40) Successful PMC (n = 30) Unsuccessful PMC (n = 10)
Pre-PMC Post-PMC p value Pre-PMC Post-PMC p value Pre-PMC Post-PMC p value
BNP, pg/mL 182 [80–194] 132 [56–125] 0.028 184 [63–194] 122 [53–123] 0.03 176 [87–193] 161 [60–344] 0.62
NT-proBNP,pg/mL
1050[232–1171] 739 [219–909] 0.08 1067 [200–1171] 654 [141–706] 0.08 999 [311–1128] 994 [375–1951] 0.97
MR-proANP,nmol/mL
220 [142–273] 187 [130–224] 0.0025 219 [142–257] 179 [123–219] 0.0012 223 [139–284] 210 [133–347] 0.6
sCD146, ng/mL 379 [308–441] 343[277–416] 0.0081 370 [298–427] 327 [268–378] 0.002 406 [323–483] 389 [283–555] 0.7
PMC percutaneous mitral commissurotomy. P-values are for the comparison before vs after by paired Student t test
Reference values for middle-aged women: BNP < 100 pg/ml, NT-proBNP< 300 pg/mL, MR-proANP< 85 nmol/mL, sCD146 still under investigation, likely < 320 ng/mL
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 4 of 9
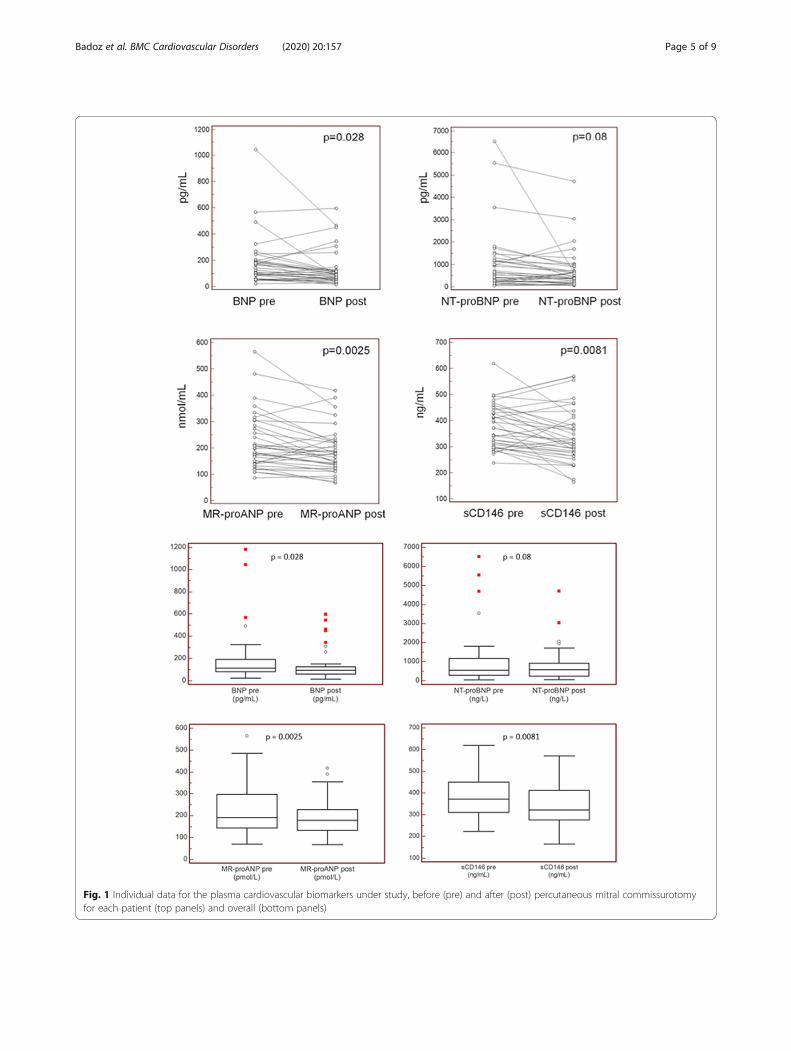
Fig. 1 Individual data for the plasma cardiovascular biomarkers under study, before (pre) and after (post) percutaneous mitral commissurotomy
for each patient (top panels) and overall (bottom panels)
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 5 of 9
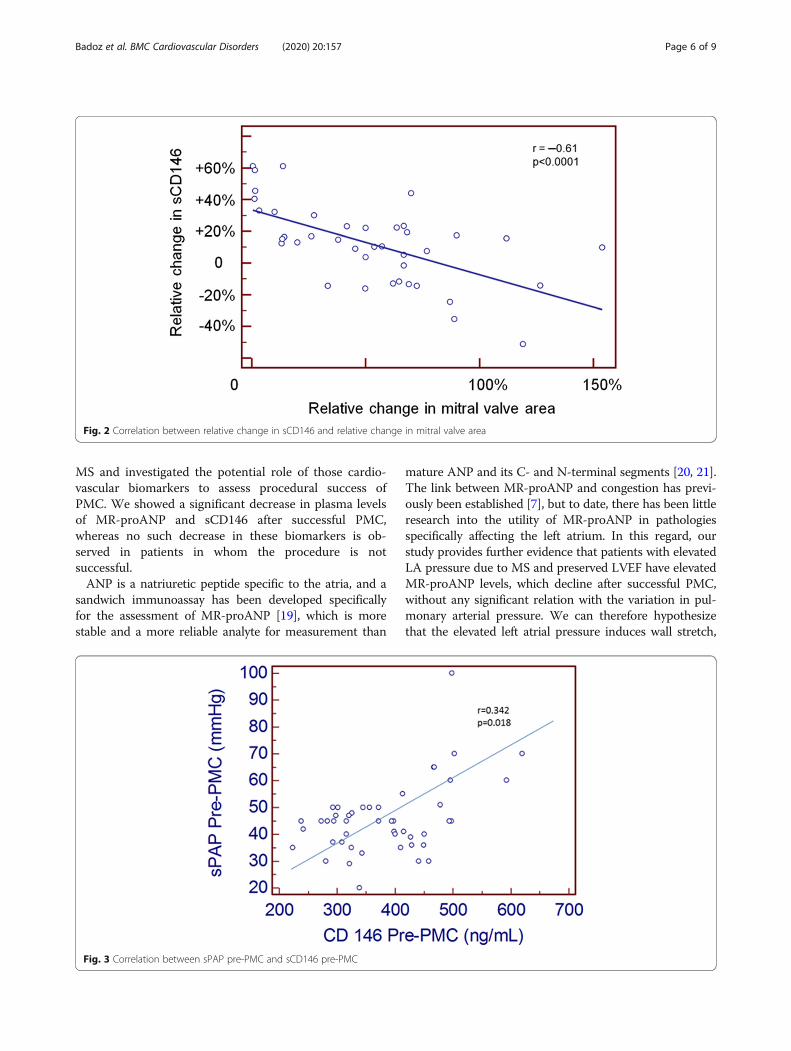
MS and investigated the potential role of those cardio-
vascular biomarkers to assess procedural success of
PMC. We showed a significant decrease in plasma levels
of MR-proANP and sCD146 after successful PMC,
whereas no such decrease in these biomarkers is ob-
served in patients in whom the procedure is not
successful.
ANP is a natriuretic peptide specific to the atria, and a
sandwich immunoassay has been developed specifically
for the assessment of MR-proANP [19], which is more
stable and a more reliable analyte for measurement than
mature ANP and its C- and N-terminal segments [20, 21].
The link between MR-proANP and congestion has previ-
ously been established [7], but to date, there has been little
research into the utility of MR-proANP in pathologies
specifically affecting the left atrium. In this regard, our
study provides further evidence that patients with elevated
LA pressure due to MS and preserved LVEF have elevated
MR-proANP levels, which decline after successful PMC,
without any significant relation with the variation in pul-
monary arterial pressure. We can therefore hypothesize
that the elevated left atrial pressure induces wall stretch,
Fig. 2 Correlation between relative change in sCD146 and relative change in mitral valve area
Fig. 3 Correlation between sPAP pre-PMC and sCD146 pre-PMC
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 6 of 9
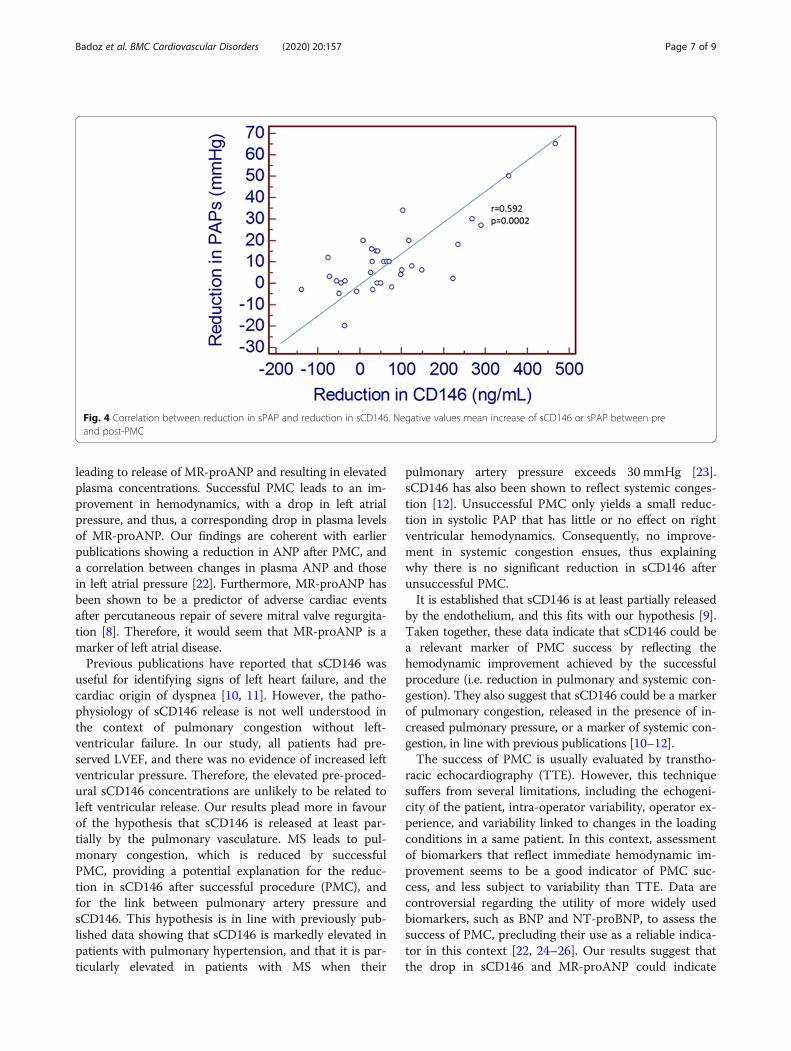
leading to release of MR-proANP and resulting in elevated
plasma concentrations. Successful PMC leads to an im-
provement in hemodynamics, with a drop in left atrial
pressure, and thus, a corresponding drop in plasma levels
of MR-proANP. Our findings are coherent with earlier
publications showing a reduction in ANP after PMC, and
a correlation between changes in plasma ANP and those
in left atrial pressure [22]. Furthermore, MR-proANP has
been shown to be a predictor of adverse cardiac events
after percutaneous repair of severe mitral valve regurgita-
tion [8]. Therefore, it would seem that MR-proANP is a
marker of left atrial disease.
Previous publications have reported that sCD146 was
useful for identifying signs of left heart failure, and the
cardiac origin of dyspnea [10, 11]. However, the patho-
physiology of sCD146 release is not well understood in
the context of pulmonary congestion without left-
ventricular failure. In our study, all patients had pre-
served LVEF, and there was no evidence of increased left
ventricular pressure. Therefore, the elevated pre-proced-
ural sCD146 concentrations are unlikely to be related to
left ventricular release. Our results plead more in favour
of the hypothesis that sCD146 is released at least par-
tially by the pulmonary vasculature. MS leads to pul-
monary congestion, which is reduced by successful
PMC, providing a potential explanation for the reduc-
tion in sCD146 after successful procedure (PMC), and
for the link between pulmonary artery pressure and
sCD146. This hypothesis is in line with previously pub-
lished data showing that sCD146 is markedly elevated in
patients with pulmonary hypertension, and that it is par-
ticularly elevated in patients with MS when their
pulmonary artery pressure exceeds 30 mmHg [23].
sCD146 has also been shown to reflect systemic conges-
tion [12]. Unsuccessful PMC only yields a small reduc-
tion in systolic PAP that has little or no effect on right
ventricular hemodynamics. Consequently, no improve-
ment in systemic congestion ensues, thus explaining
why there is no significant reduction in sCD146 after
unsuccessful PMC.
It is established that sCD146 is at least partially released
by the endothelium, and this fits with our hypothesis [9].
Taken together, these data indicate that sCD146 could be
a relevant marker of PMC success by reflecting the
hemodynamic improvement achieved by the successful
procedure (i.e. reduction in pulmonary and systemic con-
gestion). They also suggest that sCD146 could be a marker
of pulmonary congestion, released in the presence of in-
creased pulmonary pressure, or a marker of systemic con-
gestion, in line with previous publications [10–12].
The success of PMC is usually evaluated by transtho-
racic echocardiography (TTE). However, this technique
suffers from several limitations, including the echogeni-
city of the patient, intra-operator variability, operator ex-
perience, and variability linked to changes in the loading
conditions in a same patient. In this context, assessment
of biomarkers that reflect immediate hemodynamic im-
provement seems to be a good indicator of PMC suc-
cess, and less subject to variability than TTE. Data are
controversial regarding the utility of more widely used
biomarkers, such as BNP and NT-proBNP, to assess the
success of PMC, precluding their use as a reliable indica-
tor in this context [22, 24–26]. Our results suggest that
the drop in sCD146 and MR-proANP could indicate
Fig. 4 Correlation between reduction in sPAP and reduction in sCD146. Negative values mean increase of sCD146 or sPAP between pre
and post-PMC
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 7 of 9

immediate procedural success after PMC, reflecting the
hemodynamic improvement achieved by the proced-
ure, especially since the magnitude of the drop in
sCD146 is related to the benefit yielded by the PMC.
To the best of our knowledge, this is the first study
to report the utility of assessing sCD146 and MR-
proANP in the context of PMC.
Our study nonetheless has some limitations that deserve
to be underlined. Firstly, the sample size is relatively small,
although comparable to that of other studies in the field.
Clearly, the sample size is too small to allow identification
of a threshold for procedural success for these two bio-
markers, and consequently, also too low to allow calcula-
tion of their sensitivity and specificity. Furthermore, we
also lack additional hemodynamic parameters, notably in-
vasively measured left atrial pressure measurements. Fi-
nally, our data are from the immediate post-procedural
period, and no follow-up data regarding clinical, echo-
graphic or biological parameters were available in the
medium to long term. Therefore, further studies are war-
ranted to elucidate the pathophysiological mechanisms
underpinning the changes in these biomarkers and to
identify their exact relevance in this indication.
Conclusion
MR-proANP decreased significantly after PMC, likely
due to a reduction in atrial stretch achieved by the suc-
cessful procedure. Plasma sCD146 decreased signifi-
cantly immediately after successful PMC, likely due to
reduced endothelial release secondary to a reduction in
pulmonary pressure. MR-proANP and sCD146 appear
to be markers of immediate success of PMC and of the
hemodynamic improvement achieved by this procedure
in patients with MS.
Abbreviations
ANP: Atrial natriuretic peptide; BNP: Brain natriuretic peptide; LA: Left atrium/
atrial; LVEF: Left ventricular ejection fraction; MRproANP: Mid-regional pro-
atrial natriuretic peptide; MS: Mitral stenosis; NTproBNP: N-terminal pro-B-
type natriuretic peptide; PMC: Percutaneous mitral commissurotomy;
sCD146: Soluble CD146; sPAP: Systolic pulmonary artery pressure; TOE: Trans-
oesophageal echocardiography; TTE: Transthoracic echocardiography
Acknowledgements
None.
Authors’ contributions
NM, AM, MFS designed the study; MB, MA, ACM, MS, NM, AM, MFS acquired
the data; MA, MS, AM, MFS performed the assays and analysed the results;
MB, ACM, NM, AM, MFS interpreted the results; MB, ACM, NM, MFS drafted
the first version of the manuscript; MB, MA, ACM, MS, NM, AM, MFS read and
critically reviewed the final version of the manuscript; MB, MA, ACM, MS, NM,
AM, MFS approved the final version for publication.
Funding
This study received no extramural funding.
Availability of data and materials
The datasets used and/or analysed during the current study are available
from the corresponding author on reasonable request.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of Paris North
Hospitals, Paris 7 University, AP-HP, Paris, France (Comité d’Evaluation de
l’Ethique des Projets de Recherche Biomédicale (CEERB) du GHU Nord, IRB
N°00006477) under the number 10-017. All patients provided written in-
formed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Author details1Besancon University Hospital, and EA3920, University of Burgundy
Franche-Comté, Besancon, France. 2INSERM UMR-S 942, Paris, France.3Department of Anesthesiology and Critical Care Medicine, AP-HP, Saint
Louis Lariboisière University Hospitals, Paris, France. 4Department of
Cardiology, AP-HP, Saint Louis Lariboisière University Hospitals, Paris, France.5Department of Cardiology, University Heart Center, University Hospital
Zurich, Zurich, Switzerland.
Received: 25 November 2019 Accepted: 13 March 2020
References
1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V,
Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, et al. ESC guidelines for the
diagnosis and treatment of acute and chronic heart failure: the task force
for the diagnosis and treatment of acute and chronic heart failure of the
European Society of Cardiology (ESC). Developed with the special
contribution of the heart failure association (HFA) of the ESC. Eur J Heart
Fail. 2016;2016(18):891–975.
2. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow
GC, Geraci SA, Horwich T, Januzzi JL, et al. ACCF/AHA guideline for the
management of heart failure: a report of the American College of
Cardiology Foundation/American Heart Association task force on practice
guidelines. J Am Coll Cardiol. 2013;2013(62):e147–239.
3. Troughton R, Michael Felker G, Januzzi JL Jr. Natriuretic peptide-guided
heart failure management. Eur Heart J. 2014;35:16–24.
4. Harada E, Mizuno Y, Kugimiya F, Shono M, Maeda H, Yano N, Kuwahara K,
Yasue H. B-type natriuretic peptide in heart failure with preserved ejection
fraction- relevance to age-related left ventricular modeling in Japanese. Circ
J. 2017;81:1006–13.
5. Khalid U, Wruck LM, Quibrera PM, Bozkurt B, Nambi V, Virani SS, Jneid H,
Agarwal S, Chang PP, Loehr L, et al. BNP and obesity in acute
decompensated heart failure with preserved vs. reduced ejection fraction:
the atherosclerosis risk in communities surveillance study. Int J Cardiol.
2017;233:61–6.
6. Meijers WC, Hoekstra T, Jaarsma T, van Veldhuisen DJ, de Boer RA. Patients
with heart failure with preserved ejection fraction and low levels of
natriuretic peptides. Neth Heart J. 2016;24:287–95.
7. Van Aelst LNL, Arrigo M, Placido R, Akiyama E, Girerd N, Zannad F, Manivet
P, Rossignol P, Badoz M, Sadoune M, et al. Acutely decompensated heart
failure with preserved and reduced ejection fraction present with
comparable haemodynamic congestion. Eur J Heart Fail. 2018;20:738–47.
8. Wohrle J, Karakas M, Trepte U, Seeger J, Gonska B, Koenig W, Rottbauer W.
Midregional-proAtrial natriuretic peptide and high sensitive troponin T
strongly predict adverse outcome in patients undergoing percutaneous
repair of mitral valve regurgitation. PLoS One. 2015;10:e0137464.
9. Boneberg EM, Illges H, Legler DF, Furstenberger G. Soluble CD146 is
generated by ectodomain shedding of membrane CD146 in a calcium-
induced, matrix metalloprotease-dependent process. Microvasc Res. 2009;78:
325–31.
10. Gayat E, Caillard A, Laribi S, Mueller C, Sadoune M, Seronde MF, Maisel A,
Bartunek J, Vanderheyden M, Desutter J, et al. Soluble CD146, a new
endothelial biomarker of acutely decompensated heart failure. Int J Cardiol.
2015;199:241–7.
11. Kubena P, Arrigo M, Parenica J, Gayat E, Sadoune M, Ganovska E, Pavlusova
M, Littnerova S, Spinar J, Mebazaa A. Plasma levels of soluble CD146 reflect
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 8 of 9

the severity of pulmonary congestion better than brain natriuretic peptide
in acute coronary syndrome. Ann Lab Med. 2016;36:300–5.
12. Arrigo M, Truong QA, Onat D, Szymonifka J, Gayat E, Tolppanen H, Sadoune
M, Demmer RT, Wong KY, Launay JM, et al. Soluble CD146 is a novel marker
of systemic congestion in heart failure patients: an experimental
mechanistic and Transcardiac clinical study. Clin Chem. 2017;63:386–93.
13. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous
balloon dilatation of the mitral valve: an analysis of echocardiographic
variables related to outcome and the mechanism of dilatation. Br Heart J.
1988;60:299–308.
14. Helmcke F, Nanda NC, Hsiung MC, Soto B, Adey CK, Goyal RG, Gatewood RP
Jr. Color Doppler assessment of mitral regurgitation with orthogonal planes.
Circulation. 1987;75:175–83.
15. Frea S, Capriolo M, Marra WG, Cannillo M, Fusaro E, Libertucci D, Morello M,
Gaita F. Echo Doppler predictors of pulmonary artery hypertension in
patients with systemic sclerosis. Echocardiography. 2011;28:860–9.
16. Tuzcu EM, Block PC, Griffin BP, Newell JB, Palacios IF. Immediate and long-
term outcome of percutaneous mitral valvotomy in patients 65 years and
older. Circulation. 1992;85:963–71.
17. Fatkin D, Roy P, Morgan JJ, Feneley MP. Percutaneous balloon mitral
valvotomy with the Inoue single-balloon catheter: commissural morphology
as a determinant of outcome. J Am Coll Cardiol. 1993;21:390–7.
18. Reid CL, McKay CR, Chandraratna PA, Kawanishi DT, Rahimtoola SH.
Mechanisms of increase in mitral valve area and influence of anatomic
features in double-balloon, catheter balloon valvuloplasty in adults with
rheumatic mitral stenosis: a Doppler and two-dimensional
echocardiographic study. Circulation. 1987;76:628–36.
19. Morgenthaler NG, Struck J, Thomas B, Bergmann A. Immunoluminometric
assay for the midregion of pro-atrial natriuretic peptide in human plasma.
Clin Chem. 2004;50:234–6.
20. Ala-Kopsala M, Magga J, Peuhkurinen K, Leipala J, Ruskoaho H, Leppaluoto J,
Vuolteenaho O. Molecular heterogeneity has a major impact on the
measurement of circulating N-terminal fragments of A- and B-type
natriuretic peptides. Clin Chem. 2004;50:1576–88.
21. Seidler T, Pemberton C, Yandle T, Espiner E, Nicholls G, Richards M. The
amino terminal regions of proBNP and proANP oligomerise through leucine
zipper-like coiled-coil motifs. Biochem Biophys Res Commun. 1999;255:495–501.
22. Nakamura M, Kawata Y, Yoshida H, Arakawa N, Koeda T, Ichikawa T,
Funakoshi T, Hiramori K. Relationship between plasma atrial and brain
natriuretic peptide concentration and hemodynamic parameters during
percutaneous transvenous mitral valvulotomy in patients with mitral
stenosis. Am Heart J. 1992;124:1283–8.
23. Badoz M, Arrigo M, Iung B, Amioglu G, Yilmaz MB, Meneveau N, Sadoune M,
Brunette A, Mebazaa A, Seronde MF. Role of cardiovascular biomarkers for
the assessment of mitral stenosis and its complications. Eur J Intern Med.
2016;34:58–62.
24. Esteves WA, Lodi-Junqueira L, Neto CP, Tan TC, Nascimento BR, Mehrotra P,
Barbosa MM, Ribeiro AL, Nunes MC. The impact of right ventricular stroke
work on B-type natriuretic peptide levels in patients with mitral stenosis
undergoing percutaneous mitral valvuloplasty. J Interv Cardiol. 2013;26:501–8.
25. Pourafkari L, Seyedhosseini S, Kazemi B, Esmaili H, Aslanabadi N. Changes in
serum NT-pro BNP and left atrial BNP levels after percutaneous Transvenous
mitral Commissurotomy in sinus rhythm versus atrial Firilation. J Cardiovasc
Thorac Res. 2014;6:175–9.
26. Ramakrishnan S, Agarwal A, Singh S, Karthikeyan G, Seth S, Narang R,
Bhargava B. NT-pro-BNP levels as a marker of success of percutaneous
transvenous mitral commissurotomy. Indian Heart J. 2010;62:35–8.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in
published maps and institutional affiliations.
Badoz et al. BMC Cardiovascular Disorders (2020) 20:157 Page 9 of 9
70
V. Evaluation du risque de récidive
de fibrillation atriale à distance d’une
procédure d’ablation par le Mid-
Regional pro Atrial Natriuretic
Peptide et le Soluble Suppression of
Tumorigenicity 2.
71
Impact of Midregional N-Terminal Pro–Atrial Natriuretic Peptide and Soluble
Suppression of Tumorigenicity 2 Levels on Heart Rhythm in Patients Treated With
Catheter Ablation for Atrial Fibrillation: The Biorhythm Study.
Marc Badoz, Guillaume Serzian, Baptiste Favoulet, Jean-Marc Sellal , Christian De
Chillou, Néfissa Hammache, Gabriel Laurent, Alexandre Mebazaa, Fiona Ecarnot,
Karine Bardonnet, Marie-France Seronde, François Schiele, Nicolas Meneveau.
Journal of the American Heart Association 2021;10:e020917. DOI:
10.1161/JAHA.121.020917.
AVANT PROPOS
La fibrillation atriale est le trouble du rythme cardiaque le plus fréquent (46, 67). Elle
est initialement liée à des foyers ectopiques localisés au niveau de l’ostium des veines
pulmonaires initiateurs des passages en fibrillation atriale (48), elle se manifeste alors de
manière paroxystique. L’évolution naturelle de la pathologie se fait vers la persistance de celle-
ci, il s’y associe alors dilatation et fibrose de l’oreillette gauche (55, 56, 58, 59). L’ablation de
la fibrillation atriale est actuellement au centre de la prise en charge de cette pathologie, elle
consiste en l’isolation électrique des veines pulmonaires par abord transseptal (46, 48, 62, 67),
et en la réalisation éventuelle de lésions complémentaires (77). Les techniques les plus
couramment utilisées sont la radiofréquence et la cryoablation (74). La principale limite de la
technique est le pourcentage de récidive non négligeable (74, 76, 77, 84, 85), d’où l’importance
de stratifier le risque de récidive post procédure et d’identifier les potentiels bons répondeurs à
l’ablation. Cette évaluation du risque de récidive permet notamment de guider le suivi et le
traitement post procédure, par exemple en termes d’anti arythmiques.
72
Il n’existe pas de données solides concernant un biomarqueur prédicteur de récidives
dans les suites d’une ablation de fibrillation atriale. Le MRproANP est un peptide plus
spécifiquement atriale. Les deux publications précédentes (2, 3) ont montré son intérêt dans la
sténose mitrale, une pathologie affectant directement l’oreillette gauche. Il est marqueur de
sévérité du rétrécissement mitral et marqueur de succès d’une commissurotomie mitrale
percutanée. Il a peu été étudié dans l’ablation de fibrillation atriale.
Le sST2 est un marqueur de fibrose (27) et pronostique important dans l’insuffisance
cardiaque (29-33). Il n’existe que très peu de données sur le sST2 en tant que marqueur
pronostique dans l’ablation de fibrillation atriale.
L’article suivant s’intéresse donc à l’impact des niveaux de MRproANP et de sST2
plasmatiques pré procédure sur le taux de récidive à un an d’une ablation de fibrillation atriale.
Journal of the American Heart Association
J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 1
ORIGINAL RESEARCH
Impact of Midregional N- Terminal Pro– Atrial Natriuretic Peptide and Soluble Suppression of Tumorigenicity 2 Levels on Heart Rhythm in Patients Treated With Catheter Ablation for Atrial Fibrillation: The Biorhythm StudyMarc Badoz, MD; Guillaume Serzian, MD; Baptiste Favoulet, MD; Jean- Marc Sellal , MD;
Christian De Chillou , MD, PhD; Néfissa Hammache , MD; Gabriel Laurent, MD, PhD;
Alexandre Mebazaa, MD, PhD; Fiona Ecarnot, PhD; Karine Bardonnet, MD; Marie- France Seronde, MD, PhD;
François Schiele , MD, PhD; Nicolas Meneveau , MD, PhD
BACKGROUND: We assessed the impact of preprocedural plasma levels of MRproANP (midregional N- terminal pro– atrial natriu-
retic peptide) and sST2 (soluble suppression of tumorigenicity 2) on recurrence of atrial fibrillation (AF) at 1 year after catheter
ablation of AF.
METHODS AND RESULTS: This was a prospective, multicenter, observational study including patients undergoing catheter abla-
tion of AF. MRproANP and sST2 were measured in a peripheral venous blood preprocedure, and MRproANP was assessed
in the right and left atrial blood during ablation. The primary end point was recurrent AF between 3 and 12 months postab-
lation, defined as a documented (>30 seconds) episode of AF, flutter, or atrial tachycardia. We included 106 patients from
December 2017 to March 2019; 105 had complete follow- up, and the mean age was 63 years with 74.2% males. Overall, 34
patients (32.1%) had recurrent AF. In peripheral venous blood, MRproANP was significantly higher in patients with recurrent AF
(median, 192.2; [quartile 1– quartile 3, 155.9– 263.9] versus 97.1 [60.9– 150.7] pmol/L; P<0.0001), as was sST2 (median, 30.3
[quartile 1– quartile 3, 23.3– 39.3] versus 23.4 [95% CI, 17.4– 33.0] ng/mL; P=0.0033). In the atria, MRproANP was significantly
higher than in peripheral blood and was higher during AF than during sinus rhythm. Receiver operating characteristic curve
analysis identified a threshold of MRproANP>107.9 pmol/L to predict AF recurrence at 1 year and a threshold of >26.7 ng/mL
for sST2. By multivariate analysis, MRproANP>107.9 pmol/L was the only independent predictor of recurrent AF (OR, 24.27;
95% CI, 4.23– 139.18). MRproANP<107.9 pmol/L identified subjects at very low risk of recurrence (negative predictive value
>95%).
CONCLUSIONS: Elevated MRproANP level independently predicts recurrent AF, whereas sST2 levels do not appear to have any
prognostic value in assessing the risk of recurrence of AF up to 1 year after catheter ablation.
REGISTRATION: URL: https://www.clini caltr ials.gov; Unique identifier: NCT03351816.
Key Words: atrial fibrillation ■ biomarkers ■ catheter ablation ■ MRproANP ■ sST2
Correspondence to: Nicolas Meneveau, MD, PhD, Department of Cardiology, University Hospital Jean Minjoz, Boulevard Fleming, 25000 Besançon,
France.E- mail: [email protected]
Supplementary Material for this article is available at https://www.ahajo urnals.org/doi/suppl/ 10.1161/JAHA.121.020917.
For Sources of Funding and Disclosures, see page 10.
© 2021 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley. This is an open access article under the terms of the Creat ive
Commo ns Attri bution-NonCo mmercial License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited and
is not used for commercial purposes.
JAHA is available at: www.ahajournals.org/journal/jaha
Dow
nloaded from http://ahajournals.org by on June 30, 2021

J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 2
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
Catheter ablation is the cornerstone of therapy for
atrial fibrillation (AF).1,2 The main limitation of this
procedure is the success rate, which varies be-
tween 50% and 75%.3– 8 It may also lead to potentially
serious complications,3– 9 and therefore the careful se-
lection of patients is warranted to identify those likely to
yield the greatest benefit, in particular among patients
with preserved left ventricular function in whom no re-
duction in mortality has been reported after catheter
ablation of AF.10
Several clinical factors have previously been
identified as predictors of AF recurrence after cath-
eter ablation, including left atrium (LA) dilation,
type of AF (persistent versus paroxysmal), obe-
sity, diabetes mellitus, hypertension, sleep apnea,
or CHA2DS2VASC score.11– 23 Although biomarkers
are widely used in cardiac disease,24– 26 there is a
paucity of data concerning the prognostic impact
of biomarkers on the course of AF after catheter
ablation. Indeed, in a recent report from a National
Heart, Lung, and Blood Institute Virtual Workshop
describing research needs and priorities for cathe-
ter ablation of atrial fibrillation, Al- Khatib et al called
for the development of biomarkers “with the goal of
stratifying individuals for risks of complications and
benefit from AF ablation.”27
MRproANP (midregional N- terminal pro– atrial na-
triuretic peptide) is a stable peptide that results from
the cleavage of proANP (pro– atrial natriuretic pep-
tide) and is elevated in numerous pathologies spe-
cifically affecting the LA, such as mitral stenosis.28,29
Charitakis et al previously suggested that recurrent
AF postablation is more frequent in patients with ele-
vated MRproANP.30
Fibrosis is frequent in AF, and the degree of fibrosis
may be associated with AF recurrence after catheter
ablation.31 ST2 (suppression of tumorigenicity 2) from
the family of interleukin- 1 receptors, is a biomarker of
fibrosis and cardiac biomechanical constraint.32,33 Its
soluble form, sST2, can be detected using commer-
cially available assays. sST2 has been shown to be of
prognostic importance in heart failure,34– 38 but its utility
has not been widely investigated in the setting of AF.
In this context, the aim of the present study was to
assess the impact of plasma levels of MRproANP and
sST2 measured before catheter ablation for AF on the
rate of recurrence of AF at 1 year after ablation.
Secondary objectives were to (1) compare MRproANP
concentrations in the LA, right atrium (RA), and periph-
eral venous blood; (2) compare MRproANP concen-
trations in the LA and RA in sinus rhythm and during
AF; and (3) investigate the existence of a link between
plasma levels of MRproANP and sST2 and the LA area.
METHODS
The data that support the findings of this study are
available from the corresponding author upon reason-
able request.
We performed a prospective, multicenter, observa-
tional study in 3 university teaching hospitals in Eastern
France (Besançon, Nancy, and Dijon) from December
2017 to March 2019. The study protocol was approved
by the Ethics Committee Comité de Protection des
Personnes (CPP) Ile- de- France VI (CPP Ile- de- France
VI, No. 34– 17, approval number: 2017- A00731- 52, ap-
proved on June 9, 2017). The study was registered with
ClinicalTrials.gov under the number NCT03351816.
All patients provided written informed consent for
participation.
Study PopulationInclusion criteria were patients aged >18 years with
symptomatic paroxysmal or persistent AF2 with pre-
served left ventricular ejection fraction (≥45%) and in
whom a first catheter ablation of AF was to be per-
formed. The decision to perform catheter ablation was
made in accordance with the European Society of
Cardiology (ESC) guidelines.2,39
Exclusion criteria were patients aged <18 years
or >80 years; patients with significant valvular heart
CLINICAL PERSPECTIVE
What Is New?• We show for the first time that MRproANP
(midregional N- terminal pro– atrial natriuretic peptide) is an independent predictor of recurrent atrial fibrillation at 1 year after catheter ablation, whereby patients with preprocedural plasma MRproANP values exceeding 107.9 pmol/L have a 24- fold increase in risk.
What Are the Clinical Implications?• Patients with elevated MRproANP before cath-
eter ablation of atrial fibrillation warrant closer monitoring up to 1 year after the procedure and an adaptation of medical therapy, notably anti-arrhythmics, to take account of the increased risk of recurrence.
Nonstandard Abbreviations and Acronyms
MRproANP midregional N- terminal pro– atrial
natriuretic peptide
RA right atrium
sST2 soluble suppression of tumorigenicity 2
Dow
nloaded from http://ahajournals.org by on June 30, 2021

J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 3
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
disease, defined as symptomatic aortic regurgitation,
severe aortic or mitral stenosis, or mitral or tricuspid
insufficiency grade 3/4 or 4/4; presence of pulmonary
hypertension on echocardiography (>45 mm Hg);
chronic respiratory disease; chronic obstructive pul-
monary disease stages 2, 3, or 4; left ventricular ejec-
tion fraction <45%; recent (<1 month) decompensation
of heart failure; recent (<1 month) acute coronary syn-
drome; or anemia (hemoglobin <10 g/dL). We also ex-
cluded pregnant women, people under judicial or legal
protection, people with poor anticipated compliance,
people with no social security coverage, and individu-
als within the exclusion period of a prior clinical trial as
per the national register of research volunteers.
Ablation ProcedureTransthoracic and transoesophageal echocardiog-
raphy were performed by a trained operator before
the procedure to ensure the absence of intracardiac
thrombus and to record the following data as per cur-
rent guidelines40: left ventricular ejection fraction, LA
area in the 4- cavity view, and maximum thickness of
the interventricular septum. A maximum thickness
>13 mm was considered as left ventricular hypertro-
phy. Usual curative anticoagulant therapy was not
interrupted before the procedure. The aim of the pro-
cedure was pulmonary vein isolation. Additional lesions
were made at the discretion of the operator. A total of 2
types of procedures could be performed, namely, radi-
ofrequency ablation with an irrigated tip ablation cath-
eter with electrophysiological and anatomical mapping
of the LA or cryoablation.5 The choice of technique
(cryoablation or radiofrequency ablation) and the sys-
tem used for electroanatomical navigation in case of
radiofrequency ablation were at the discretion of the
operator. Procedures were performed by qualified and
experienced operators having a volume of activity of
at least 50 procedures each per year. Transthoracic
echocardiography was performed at the end of the
procedure to ensure an absence of pericardial effu-
sion. Treatment was administered after the procedure
in accordance with guidelines in force at the time of
the inclusions.1,39 Usual anticoagulant therapy was
then pursued for 8 weeks postprocedure in patients
with CHA2DS2VASC scores of 0 or indefinitely for pa-
tients with CHA2DS2VASC scores ≥1.1,2 Antiarrhythmic
agents could be continued at the operator’s discre-
tion. It was recommended that every effort be made to
maintain sinus rhythm.
MRproANP and sST2 MeasurementsMRproANP and sST2 were measured in peripheral
venous blood drawn within 24 hours before the cath-
eter ablation procedure. MRproANP was also meas-
ured in a sample of blood from the RA at the start of
the procedure and in a sample of blood from the LA
drawn immediately after transseptal puncture. Tubes
were centrifuged and stored at −20°C for later cen-
tralized analysis in the Biochemistry Department of
the University Hospital of Besancon. MRproANP was
measured using BRAHMS Kryptor Compact Plus
(Thermo Fisher Diagnostics SAS, Dardilly, France).
sST2 was also centrally analyzed in the Biochemistry
Department of the University Hospital of Besancon
using the Aspect Plus kit from Eurobio Ingen (Les Ulis,
France).
Study End PointsThe primary end point was recurrence of AF, defined as
occurrence between 3 and 12 months after the proce-
dure of a documented episode (documented by ECG,
Holter monitoring, ECG event recorder, or telemetry) of
AF, atrial tachycardia, or atrial flutter lasting >30 sec-
onds. All patients were followed up with 24- hour Holter
ECG monitoring and a clinical consultation at 3 months
(the end of a blanking period) and 12 months after the
procedure. Between the end of the blanking period
and the 12- month follow- up, patients were followed by
their treating cardiologist and/or general practitioner
who were informed of the patient’s participation in this
study and were requested to inform the coordinating
center of any intercurrent events. In case of symptoms
suggestive of recurrent arrhythmia, patients were seen
in consultation and had an ECG with the possibility of
additional Holter ECG monitoring, ECG event recorder,
or hospitalization with continuous ECG to identify
recurrence.
Statistical AnalysisQuantitative data are described as mean±SD or me-
dian (25th percentile [quartile 1]– 75th percentile [quar-
tile 3]) and were compared with the Student t test for
normally distributed variables or the Mann– Whitney
test for nonnormally distributed variables. Paired
tests were used as appropriate. Qualitative data are
expressed as number (percentage) and were com-
pared using the chi- square or Fisher exact test as
appropriate. Multivariate analysis was performed
using multivariable logistic regression. Variables with
a P value <0.20 by univariate analysis were included
in the model, and the results are expressed as odds
ratios (OR) and 95% CI. Receiver operating charac-
teristic (ROC) curves were constructed to identify the
threshold of sST2 and MRproANP that best predict
recurrence. Survival curves were generated using the
Kaplan– Meier method and compared with the log-
rank test. Correlations between quantitative variables
were examined using the Spearman correlation coef-
ficient. All tests were 2 sided, and a P value <0.05 was
considered statistically significant. All analyses were
Dow
nloaded from http://ahajournals.org by on June 30, 2021
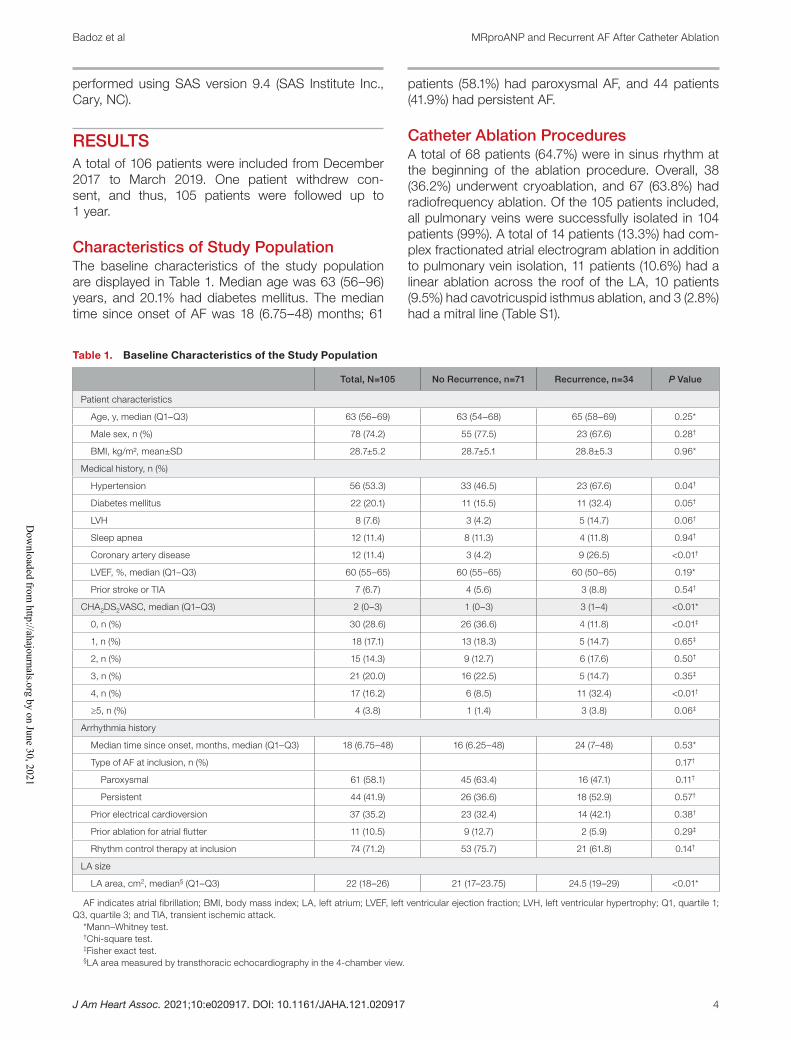
J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 4
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
performed using SAS version 9.4 (SAS Institute Inc.,
Cary, NC).
RESULTS
A total of 106 patients were included from December
2017 to March 2019. One patient withdrew con-
sent, and thus, 105 patients were followed up to
1 year.
Characteristics of Study PopulationThe baseline characteristics of the study population
are displayed in Table 1. Median age was 63 (56– 96)
years, and 20.1% had diabetes mellitus. The median
time since onset of AF was 18 (6.75– 48) months; 61
patients (58.1%) had paroxysmal AF, and 44 patients
(41.9%) had persistent AF.
Catheter Ablation ProceduresA total of 68 patients (64.7%) were in sinus rhythm at
the beginning of the ablation procedure. Overall, 38
(36.2%) underwent cryoablation, and 67 (63.8%) had
radiofrequency ablation. Of the 105 patients included,
all pulmonary veins were successfully isolated in 104
patients (99%). A total of 14 patients (13.3%) had com-
plex fractionated atrial electrogram ablation in addition
to pulmonary vein isolation, 11 patients (10.6%) had a
linear ablation across the roof of the LA, 10 patients
(9.5%) had cavotricuspid isthmus ablation, and 3 (2.8%)
had a mitral line (Table S1).
Table 1. Baseline Characteristics of the Study Population
Total, N=105 No Recurrence, n=71 Recurrence, n=34 P Value
Patient characteristics
Age, y, median (Q1– Q3) 63 (56– 69) 63 (54– 68) 65 (58– 69) 0.25*
Male sex, n (%) 78 (74.2) 55 (77.5) 23 (67.6) 0.28†
BMI, kg/m², mean±SD 28.7±5.2 28.7±5.1 28.8±5.3 0.96*
Medical history, n (%)
Hypertension 56 (53.3) 33 (46.5) 23 (67.6) 0.04†
Diabetes mellitus 22 (20.1) 11 (15.5) 11 (32.4) 0.05†
LVH 8 (7.6) 3 (4.2) 5 (14.7) 0.06†
Sleep apnea 12 (11.4) 8 (11.3) 4 (11.8) 0.94†
Coronary artery disease 12 (11.4) 3 (4.2) 9 (26.5) <0.01†
LVEF, %, median (Q1– Q3) 60 (55– 65) 60 (55– 65) 60 (50– 65) 0.19*
Prior stroke or TIA 7 (6.7) 4 (5.6) 3 (8.8) 0.54†
CHA2DS2VASC, median (Q1– Q3) 2 (0– 3) 1 (0– 3) 3 (1– 4) <0.01*
0, n (%) 30 (28.6) 26 (36.6) 4 (11.8) <0.01‡
1, n (%) 18 (17.1) 13 (18.3) 5 (14.7) 0.65‡
2, n (%) 15 (14.3) 9 (12.7) 6 (17.6) 0.50†
3, n (%) 21 (20.0) 16 (22.5) 5 (14.7) 0.35‡
4, n (%) 17 (16.2) 6 (8.5) 11 (32.4) <0.01†
≥5, n (%) 4 (3.8) 1 (1.4) 3 (3.8) 0.06‡
Arrhythmia history
Median time since onset, months, median (Q1– Q3) 18 (6.75– 48) 16 (6.25– 48) 24 (7– 48) 0.53*
Type of AF at inclusion, n (%) 0.17†
Paroxysmal 61 (58.1) 45 (63.4) 16 (47.1) 0.11†
Persistent 44 (41.9) 26 (36.6) 18 (52.9) 0.57†
Prior electrical cardioversion 37 (35.2) 23 (32.4) 14 (42.1) 0.38†
Prior ablation for atrial flutter 11 (10.5) 9 (12.7) 2 (5.9) 0.29‡
Rhythm control therapy at inclusion 74 (71.2) 53 (75.7) 21 (61.8) 0.14†
LA size
LA area, cm2, median§ (Q1– Q3) 22 (18– 26) 21 (17– 23.75) 24.5 (19– 29) <0.01*
AF indicates atrial fibrillation; BMI, body mass index; LA, left atrium; LVEF, left ventricular ejection fraction; LVH, left ventricular hypertrophy; Q1, quartile 1;
Q3, quartile 3; and TIA, transient ischemic attack.
*Mann– Whitney test.†Chi- square test.‡Fisher exact test.§LA area measured by transthoracic echocardiography in the 4- chamber view.
Dow
nloaded from http://ahajournals.org by on June 30, 2021

J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 5
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
Regarding complications, 2 patients had transient
ischemic attack or ischemic stroke, there was no car-
diac tamponade, one patient had persistent phrenic
paralysis at discharge after cryoablation; 1 patient had
an access point hematoma, 1 patient had postproce-
dural pulmonary edema, and 1 patient had perforation
of the mitral valve with significant mitral insufficiency
(Table S1).
In total, 62 patients (59.0%) received rhythm- control
therapy at discharge (Table S1).
Primary OutcomeOverall, 34 patients (32.3%) had recurrent AF at 1 year
(recurrence group). There were significantly more pa-
tients with hypertension (67.6% versus 46.5%; P=0.04)
and ischemic heart disease (26.5% versus 4.2%;
P<0.01) in the recurrence group. In this group, there
was also a higher CHA2DS2VASC score (median, 3
[quartile 1– quartile 3, 1– 4] versus 1 [0– 3]; P<0.01) and
more dilation of the LA in terms of the area measured
by transthoracic echocardiography (median, 21 [quar-
tile 1– quartile 3, 17– 23.75] versus 24.5 [19– 29] cm2;
P=0.02).
There was no difference in the rate of antiarrhyth-
mics use at 1 year after the procedure between groups
(47.1% versus 35.2%, recurrence versus no recurrence,
respectively; P=0.25; Table S1).
Biomarker Levels and AF RecurrenceMRproANP measured in peripheral venous blood
drawn preprocedure was significantly higher in pa-
tients with recurrence versus those without recurrence
(median, 192.2 [quartile 1– quartile 3, 155.9– 263.9] ver-
sus 97.1 [60.9– 150.7] pmol/L; P<0.01). MRproANP lev-
els measured in blood drawn from the LA and RA were
also significantly higher in patients in the recurrence
group (Table 2). Similarly, sST2 levels were significantly
higher in the recurrence group (median30.3 [quartile
1– quartile 3, 23.3– 39.3] versus 23.4 [17.4– 33.0] ng/mL;
P<0.01).
ROC curve analysis of plasma MRproANP mea-
sured in peripheral venous blood identified a threshold
value of >107.9 pmol/L as having the best predictive
value for recurrent AF at 1 year after ablation, with
a sensitivity of 94.1%, a specificity of 63.4%, and an
area under the ROC curve of 0.838 (P<0.01; Figure 1).
The associated positive predictive value and negative
predictive value (NPV) were, respectively, 55.2% and
95.7% (Table 3). For sST2, the threshold identified by
ROC curve analysis was >26.7 ng/mL, with a sensi-
tivity and a specificity of 73.5% and 64.8%, respec-
tively. The area under the ROC curve for sST2 was
0.678 and was significantly lower than the area under
the ROC curve for MRproANP (P<0.01; Figure 1). The
associated positive predictive value and NPV were,
respectively, 49.0% and 83.3% (Table 3). The propor-
tion of recurrence and nonrecurrence per quartiles of
MRproANP and sST2 are presented in Figure 2. There
was a significant difference in AF recurrence be-
tween groups when classified according to whether
MRproANP measured in peripheral venous blood
was above or below the threshold of 107.9 pmol/L
(Figure 3).
MRproANP levels were significantly higher in blood
drawn from the LA and RA than in peripheral venous
blood (median, 143.5 [quartile 1– quartile 3, 89.8–
208.3] versus 131.5 [73.5– 200.6] pmol/L [P<0.01]; and
median, 142.2 [quartile 1– quartile 3, 90.3– 210.3] ver-
sus 131.5 [73.5– 200.6] pmol/L [P<0.01]; respectively).
There was a significant correlation between MRproANP
levels in the atria (left and right) and peripheral venous
blood (P<0.01; Figure S1). There was no significant dif-
ference in MRproANP levels between the LA and RA
(Figure S2). MRproANP levels were higher in the LA
and RA when patients were in AF at the time of the
blood draw compared with blood samples performed
in sinus rhythm (median, 187.9 [quartile 1– quartile 3,
135.1– 288.4] versus 115.2 [81.9– 168.6] [P<0.01]; and
median, 191.0 [quartile 1– quartile 3, 127.0– 276.9] ver-
sus 109.4 [82.3– 169.8] pmol/L [P<0.01]; respectively;
Figure S3). The predictive value of MRproANP was the
same, regardless of the site of blood draw, as illus-
trated by the lack of difference between ROC curves
(Figure 4) and the sensitivity, specificity, positive pre-
dictive value, and NPV (using the best predictive value
Table 2. Results of MRproANP and sST2 Assessments
Total, N=105 No Recurrence, n=71 Recurrence, n=34 P Value*
MRproANP PV, pmol/L 131.3 (73.5– 200.6) 97.1 (60.9– 150.7) 192.2 (155.9– 263.9) <0.01
MRproANP LA, pmol/L 143.5 (89.8– 208.3) 110.7 (79.3– 172.1) 234.3 (163.4– 334.2) <0.01
MRproANP RA, pmol/L 142.2 (90.3– 210.3) 108.8 (81.8– 168.1) 207.8 (159.1– 347.2) <0.01
sST2 PV, ng/mL 26.4 (19.5– 36.4) 23.4 (17.4– 33.0) 30.3 (23.3– 39.8) <0.01
Values are provided as median (quartile 1– quartile 3). MRproANP indicates midregional N- terminal pro– atrial natriuretic peptide; MRproANP LA, level of
midregional N- terminal pro– atrial natriuretic peptide measured in blood drawn from the left atrium; MRproANP PV, midregional N- terminal pro– atrial natriuretic
peptide measured in peripheral venous blood; MRproANP RA, level of midregional N- terminal pro– atrial natriuretic peptide measured in blood drawn from the
right atrium; sST2, level of soluble suppression of tumorigenicity 2; and sST2 PV, soluble suppression of tumorigenicity 2 measured in peripheral venous blood.
*P values from Mann– Whitney tests.
Dow
nloaded from http://ahajournals.org by on June 30, 2021
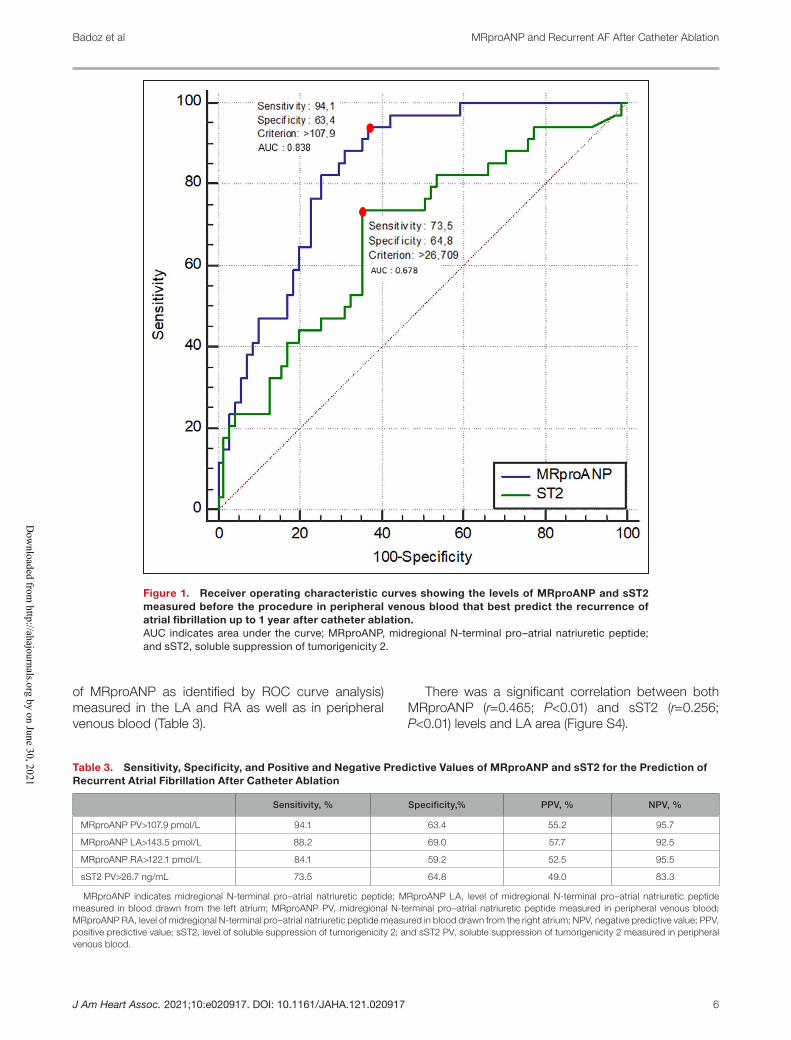
J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 6
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
of MRproANP as identified by ROC curve analysis)
measured in the LA and RA as well as in peripheral
venous blood (Table 3).
There was a significant correlation between both
MRproANP (r=0.465; P<0.01) and sST2 (r=0.256;
P<0.01) levels and LA area (Figure S4).
Figure 1. Receiver operating characteristic curves showing the levels of MRproANP and sST2
measured before the procedure in peripheral venous blood that best predict the recurrence of
atrial fibrillation up to 1 year after catheter ablation.
AUC indicates area under the curve; MRproANP, midregional N- terminal pro– atrial natriuretic peptide;
and sST2, soluble suppression of tumorigenicity 2.
Table 3. Sensitivity, Specificity, and Positive and Negative Predictive Values of MRproANP and sST2 for the Prediction of
Recurrent Atrial Fibrillation After Catheter Ablation
Sensitivity, % Specificity,% PPV, % NPV, %
MRproANP PV>107.9 pmol/L 94.1 63.4 55.2 95.7
MRproANP LA>143.5 pmol/L 88.2 69.0 57.7 92.5
MRproANP RA>122.1 pmol/L 84.1 59.2 52.5 95.5
sST2 PV>26.7 ng/mL 73.5 64.8 49.0 83.3
MRproANP indicates midregional N- terminal pro– atrial natriuretic peptide; MRproANP LA, level of midregional N- terminal pro– atrial natriuretic peptide
measured in blood drawn from the left atrium; MRproANP PV, midregional N- terminal pro– atrial natriuretic peptide measured in peripheral venous blood;
MRproANP RA, level of midregional N- terminal pro– atrial natriuretic peptide measured in blood drawn from the right atrium; NPV, negative predictive value; PPV,
positive predictive value; sST2, level of soluble suppression of tumorigenicity 2; and sST2 PV, soluble suppression of tumorigenicity 2 measured in peripheral
venous blood.
Dow
nloaded from http://ahajournals.org by on June 30, 2021
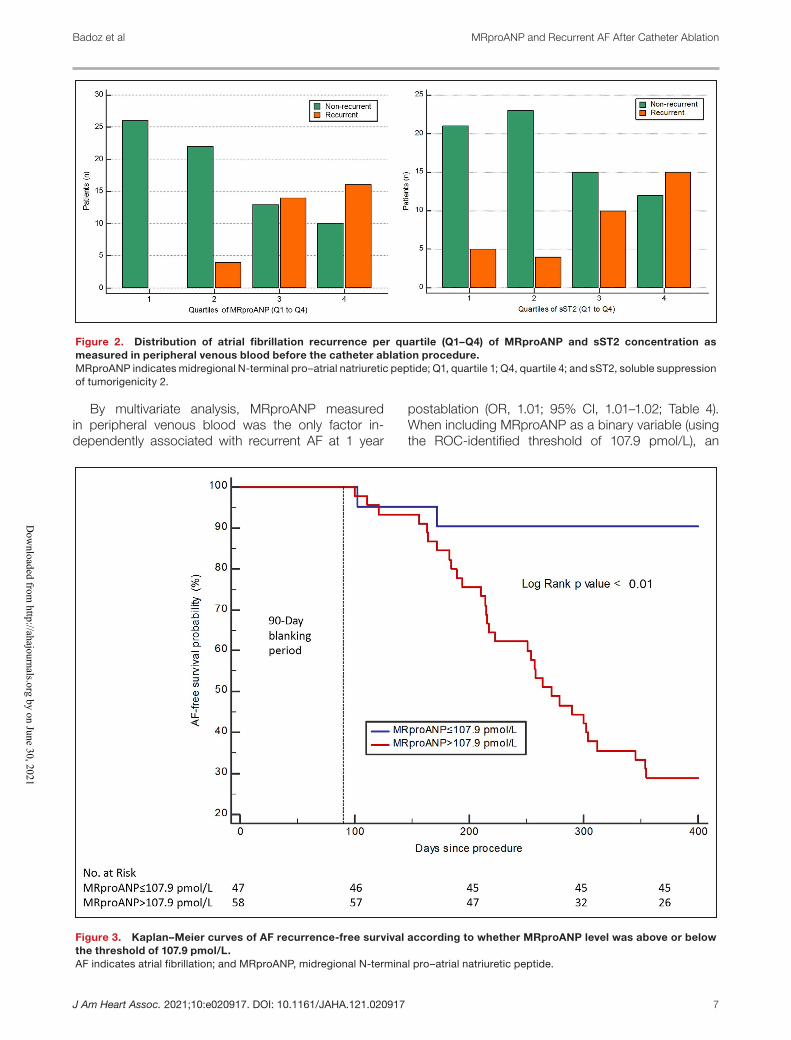
J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 7
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
By multivariate analysis, MRproANP measured
in peripheral venous blood was the only factor in-
dependently associated with recurrent AF at 1 year
postablation (OR, 1.01; 95% CI, 1.01– 1.02; Table 4).
When including MRproANP as a binary variable (using
the ROC- identified threshold of 107.9 pmol/L), an
Figure 2. Distribution of atrial fibrillation recurrence per quartile (Q1– Q4) of MRproANP and sST2 concentration as
measured in peripheral venous blood before the catheter ablation procedure.
MRproANP indicates midregional N- terminal pro– atrial natriuretic peptide; Q1, quartile 1; Q4, quartile 4; and sST2, soluble suppression
of tumorigenicity 2.
Figure 3. Kaplan– Meier curves of AF recurrence- free survival according to whether MRproANP level was above or below
the threshold of 107.9 pmol/L.
AF indicates atrial fibrillation; and MRproANP, midregional N- terminal pro– atrial natriuretic peptide.
Dow
nloaded from http://ahajournals.org by on June 30, 2021
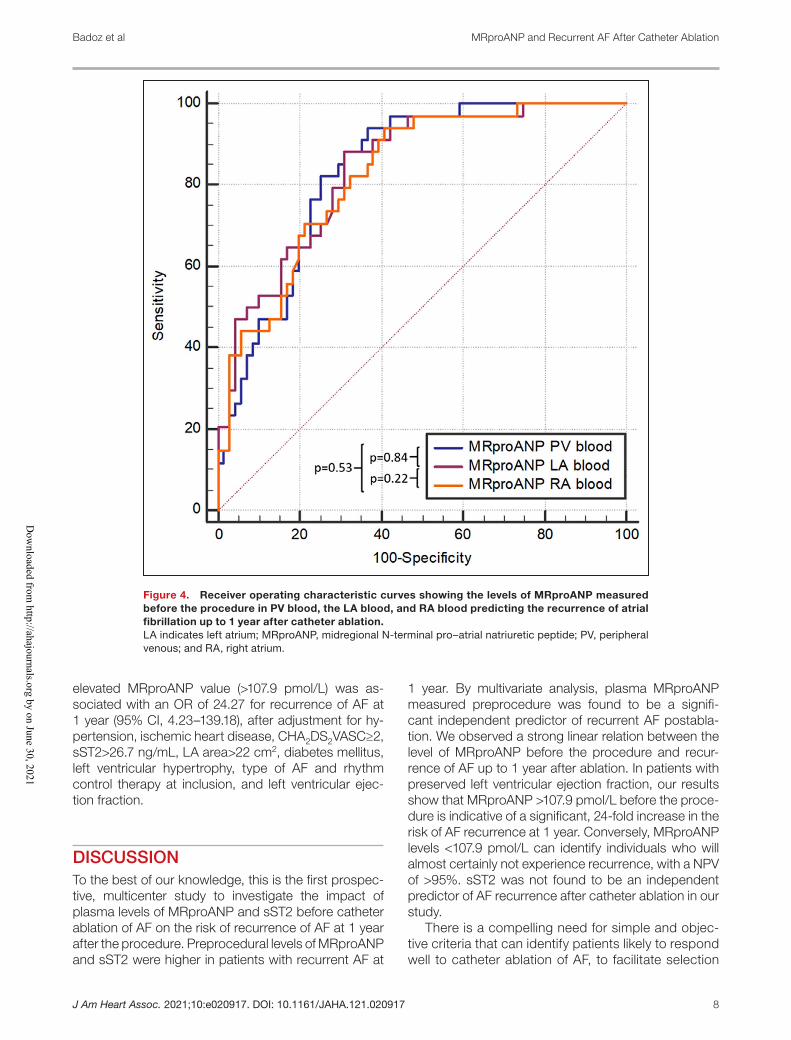
J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 8
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
elevated MRproANP value (>107.9 pmol/L) was as-
sociated with an OR of 24.27 for recurrence of AF at
1 year (95% CI, 4.23– 139.18), after adjustment for hy-
pertension, ischemic heart disease, CHA2DS2VASC≥2,
sST2>26.7 ng/mL, LA area>22 cm2, diabetes mellitus,
left ventricular hypertrophy, type of AF and rhythm
control therapy at inclusion, and left ventricular ejec-
tion fraction.
DISCUSSION
To the best of our knowledge, this is the first prospec-
tive, multicenter study to investigate the impact of
plasma levels of MRproANP and sST2 before catheter
ablation of AF on the risk of recurrence of AF at 1 year
after the procedure. Preprocedural levels of MRproANP
and sST2 were higher in patients with recurrent AF at
1 year. By multivariate analysis, plasma MRproANP
measured preprocedure was found to be a signifi-
cant independent predictor of recurrent AF postabla-
tion. We observed a strong linear relation between the
level of MRproANP before the procedure and recur-
rence of AF up to 1 year after ablation. In patients with
preserved left ventricular ejection fraction, our results
show that MRproANP >107.9 pmol/L before the proce-
dure is indicative of a significant, 24- fold increase in the
risk of AF recurrence at 1 year. Conversely, MRproANP
levels <107.9 pmol/L can identify individuals who will
almost certainly not experience recurrence, with a NPV
of >95%. sST2 was not found to be an independent
predictor of AF recurrence after catheter ablation in our
study.
There is a compelling need for simple and objec-
tive criteria that can identify patients likely to respond
well to catheter ablation of AF, to facilitate selection
Figure 4. Receiver operating characteristic curves showing the levels of MRproANP measured
before the procedure in PV blood, the LA blood, and RA blood predicting the recurrence of atrial
fibrillation up to 1 year after catheter ablation.
LA indicates left atrium; MRproANP, midregional N- terminal pro– atrial natriuretic peptide; PV, peripheral
venous; and RA, right atrium.
Dow
nloaded from http://ahajournals.org by on June 30, 2021
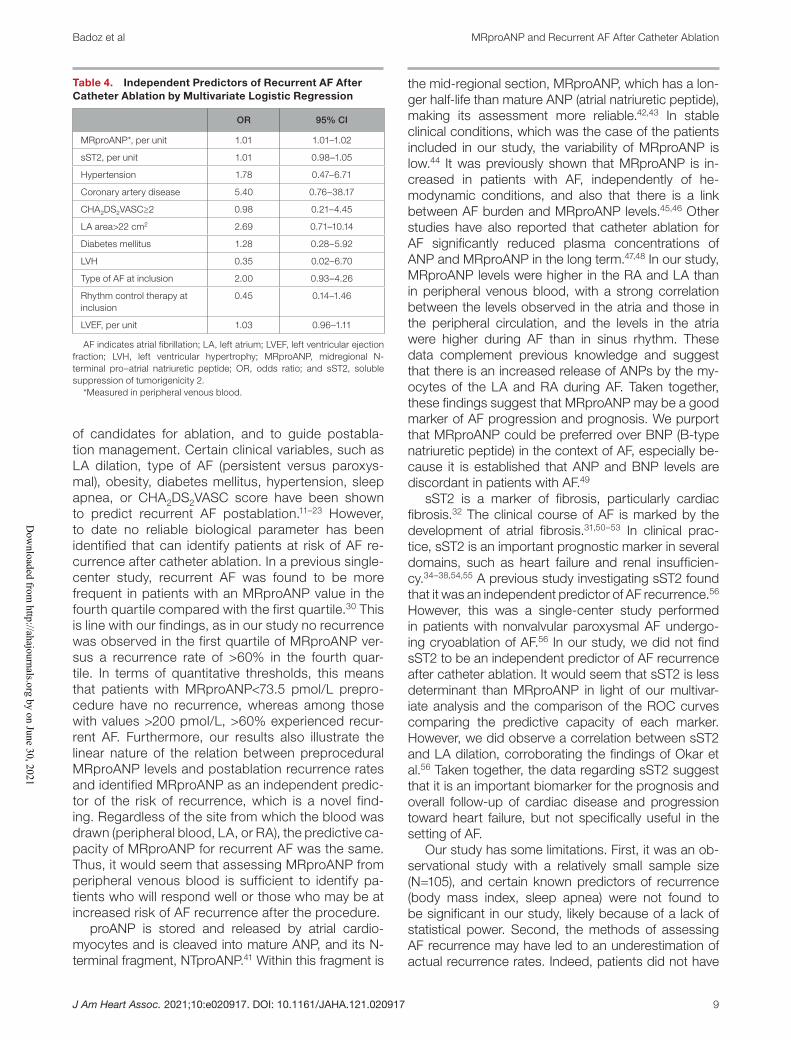
J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 9
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
of candidates for ablation, and to guide postabla-
tion management. Certain clinical variables, such as
LA dilation, type of AF (persistent versus paroxys-
mal), obesity, diabetes mellitus, hypertension, sleep
apnea, or CHA2DS2VASC score have been shown
to predict recurrent AF postablation.11– 23 However,
to date no reliable biological parameter has been
identified that can identify patients at risk of AF re-
currence after catheter ablation. In a previous single-
center study, recurrent AF was found to be more
frequent in patients with an MRproANP value in the
fourth quartile compared with the first quartile.30 This
is line with our findings, as in our study no recurrence
was observed in the first quartile of MRproANP ver-
sus a recurrence rate of >60% in the fourth quar-
tile. In terms of quantitative thresholds, this means
that patients with MRproANP<73.5 pmol/L prepro-
cedure have no recurrence, whereas among those
with values >200 pmol/L, >60% experienced recur-
rent AF. Furthermore, our results also illustrate the
linear nature of the relation between preprocedural
MRproANP levels and postablation recurrence rates
and identified MRproANP as an independent predic-
tor of the risk of recurrence, which is a novel find-
ing. Regardless of the site from which the blood was
drawn (peripheral blood, LA, or RA), the predictive ca-
pacity of MRproANP for recurrent AF was the same.
Thus, it would seem that assessing MRproANP from
peripheral venous blood is sufficient to identify pa-
tients who will respond well or those who may be at
increased risk of AF recurrence after the procedure.
proANP is stored and released by atrial cardio-
myocytes and is cleaved into mature ANP, and its N-
terminal fragment, NTproANP.41 Within this fragment is
the mid- regional section, MRproANP, which has a lon-
ger half- life than mature ANP (atrial natriuretic peptide),
making its assessment more reliable.42,43 In stable
clinical conditions, which was the case of the patients
included in our study, the variability of MRproANP is
low.44 It was previously shown that MRproANP is in-
creased in patients with AF, independently of he-
modynamic conditions, and also that there is a link
between AF burden and MRproANP levels.45,46 Other
studies have also reported that catheter ablation for
AF significantly reduced plasma concentrations of
ANP and MRproANP in the long term.47,48 In our study,
MRproANP levels were higher in the RA and LA than
in peripheral venous blood, with a strong correlation
between the levels observed in the atria and those in
the peripheral circulation, and the levels in the atria
were higher during AF than in sinus rhythm. These
data complement previous knowledge and suggest
that there is an increased release of ANPs by the my-
ocytes of the LA and RA during AF. Taken together,
these findings suggest that MRproANP may be a good
marker of AF progression and prognosis. We purport
that MRproANP could be preferred over BNP (B- type
natriuretic peptide) in the context of AF, especially be-
cause it is established that ANP and BNP levels are
discordant in patients with AF.49
sST2 is a marker of fibrosis, particularly cardiac
fibrosis.32 The clinical course of AF is marked by the
development of atrial fibrosis.31,50– 53 In clinical prac-
tice, sST2 is an important prognostic marker in several
domains, such as heart failure and renal insufficien-
cy.34– 38,54,55 A previous study investigating sST2 found
that it was an independent predictor of AF recurrence.56
However, this was a single- center study performed
in patients with nonvalvular paroxysmal AF undergo-
ing cryoablation of AF.56 In our study, we did not find
sST2 to be an independent predictor of AF recurrence
after catheter ablation. It would seem that sST2 is less
determinant than MRproANP in light of our multivar-
iate analysis and the comparison of the ROC curves
comparing the predictive capacity of each marker.
However, we did observe a correlation between sST2
and LA dilation, corroborating the findings of Okar et
al.56 Taken together, the data regarding sST2 suggest
that it is an important biomarker for the prognosis and
overall follow- up of cardiac disease and progression
toward heart failure, but not specifically useful in the
setting of AF.
Our study has some limitations. First, it was an ob-
servational study with a relatively small sample size
(N=105), and certain known predictors of recurrence
(body mass index, sleep apnea) were not found to
be significant in our study, likely because of a lack of
statistical power. Second, the methods of assessing
AF recurrence may have led to an underestimation of
actual recurrence rates. Indeed, patients did not have
Table 4. Independent Predictors of Recurrent AF After
Catheter Ablation by Multivariate Logistic Regression
OR 95% CI
MRproANP*, per unit 1.01 1.01– 1.02
sST2, per unit 1.01 0.98– 1.05
Hypertension 1.78 0.47– 6.71
Coronary artery disease 5.40 0.76– 38.17
CHA2DS2VASC≥2 0.98 0.21– 4.45
LA area>22 cm2 2.69 0.71– 10.14
Diabetes mellitus 1.28 0.28– 5.92
LVH 0.35 0.02– 6.70
Type of AF at inclusion 2.00 0.93– 4.26
Rhythm control therapy at
inclusion
0.45 0.14– 1.46
LVEF, per unit 1.03 0.96– 1.11
AF indicates atrial fibrillation; LA, left atrium; LVEF, left ventricular ejection
fraction; LVH, left ventricular hypertrophy; MRproANP, midregional N-
terminal pro– atrial natriuretic peptide; OR, odds ratio; and sST2, soluble
suppression of tumorigenicity 2.
*Measured in peripheral venous blood.
Dow
nloaded from http://ahajournals.org by on June 30, 2021

J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 10
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
implanted Holter devices (implantable cardiac moni-
tors), and the duration of systematic ECG Holter mon-
itoring was only 24 hours, without the performance
of longer duration monitoring. Nevertheless, the like-
lihood of underestimation of AF recurrence is low given
than the recurrence rate at 1 year observed in our
study was similar to, if not higher than that reported in
other prospective studies.5,10,57 This may be explained
by the fact that all patients were symptomatic, mak-
ing the detection of recurrence easier. Indeed, patients
were instructed to consult the cardiologist or general
practitioner immediately in case of symptoms. In addi-
tion, if underestimation occurred, it likely affected both
groups equivalently. We therefore believe that the mon-
itoring modalities likely had little effect on the results.
In addition, multiple factors affect the success rate of
AF ablation and may confound the predictive role of
the markers. Nevertheless, MRproANP was found to
be an independent predictor even after adjustment
for potential confounders in multivariate analysis, thus
supporting the robustness of our findings. Finally, our
data deserve confirmation in a larger population to
confirm the prognostic value of MRproANP to identify
patients at high risk of AF recurrence up to 1 year after
catheter ablation of AF on top of previously identified
predictors.11– 13,18– 23
CONCLUSIONS
An elevated MRproANP level is an independent
predictor of recurrent AF at 1 year after catheter
ablation, whereas sST2 levels do not appear to
have any prognostic value in assessing the risk
of recurrence of AF up to 1 year. An MRproANP
level >107.9 pmol/L before the procedure is asso-
ciated with a 24- fold increase in the risk of recur-
rent AF within 1 year. Conversely, an MRproANP
value <107.9 pmol/L identif ies patients unlikely
to experience recurrent AF, with a high NPV.
Larger prospective studies are warranted to
confirm the utility of assessing MRproANP in this
setting.
ARTICLE INFORMATION
Received February 12, 2021; accepted May 13, 2021.
AffiliationsDepartment of Cardiology (M.B., G.S., B.F., F.E., M.S., F.S., N.M.); and
Department of Biochemistry (K.B.), University Hospital Besançon, Besançon,
France; EA3920, University of Burgundy Franche- Comté, Besançon, France
(M.B., F.E., M.S., F.S., N.M.); Department of Cardiology, Centre Hospitalier
Régional Universitaire de Nancy, Université de Lorraine, Nancy, France
(J.S., C.D.C., N.H.); IADI, INSERM U1254, Université de Lorraine, Nancy,
France (J.S., N.H.); Department of Cardiology, University Hospital François
Mitterand, Dijon, France (G.L.); INSERM UMR- S 942, Paris, France (A.M.);
and Department of Anesthesiology and Critical Care Medicine, Assistance
Publique - Hôpitaux de Paris, Saint Louis Lariboisière University Hospitals,
Paris, France (A.M.).
Sources of Funding
This study was partially funded by an unrestricted
grant from Abbott Medical France.
DisclosuresDr de Chillou reports personal fees from Biosense Webster, Medtronic,
Stereotaxis, and Mylan and nonfinancial support from Abbott and
Microport outside the submitted work. Dr Sellal reports personal fees
from Microport, Bayer, Mylan, Pfizer, and Boeringher outside the submit-
ted work. Dr Meneveau reports personal fees from Abbott, Bayer, Boston
Scientific, Bristol Myers Squibb, Edwards Lifesciences, and Terumo outside
the submitted work. Dr Seronde reports personal fees from Astra Zeneca,
Boehringer Ingelheim, Bayer, Bristol Myers Squibb, Novartis, and Servier
outside the submitted work. Dr Mebazaa reports personal fees from Orion,
Servier, Otsuka, Philips, Sanofi, Epygon, and Fire 1; grants and personal
fees from Roche, Adrenomed, and 4TEEN4; personal fees from grants from
Abbott; and grants and personal fees from Sphyngotec outside the submit-
ted work. Dr Schiele reports grants and personal fees from Bayer, Sanofi
Aventis, MSD, and Amgen; grants from St Jude Medical and Daiichi Sankyo;
and personal fees from Boehringer Ingelheim, Pfizer, Astra Zeneca, Mylan,
and Servier outside the submitted work. The remaining authors have no dis-
closures to report.
Supplementary MaterialTable S1
Figures S1- S4
REFERENCES
1. Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L,
Akar JG, Badhwar V, Brugada J, Camm J, et al. 2017 HRS/EHRA/
ECAS/APHRS/SOLAECE expert consensus statement on catheter and
surgical ablation of atrial fibrillation. Europace. 2018;20:e1– e160. DOI:
10.1093/europ ace/eux274.
2. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-
Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, et al. 2020
ESC Guidelines for the diagnosis and management of atrial fibrillation
developed in collaboration with the European Association of Cardio-
Thoracic Surgery (EACTS). Eur Heart J. 2021;42:373– 498. DOI:
10.1093/eurhe artj/ehaa612.
3. Dukkipati SR, Cuoco F, Kutinsky I, Aryana A, Bahnson TD, Lakkireddy
D, Woollett I, Issa ZF, Natale A, Reddy VY. Pulmonary vein isolation
using the visually guided laser balloon: a prospective, multicenter, and
randomized comparison to standard radiofrequency ablation. J Am Coll
Cardiol. 2015;66:1350– 1360. DOI: 10.1016/j.jacc.2015.07.036.
4. Hakalahti A, Biancari F, Nielsen JC, Raatikainen MJ. Radiofrequency
ablation vs. antiarrhythmic drug therapy as first line treatment of
symptomatic atrial fibrillation: systematic review and meta- analysis.
Europace. 2015;17:370– 378. DOI: 10.1093/europ ace/euu376.
5. Kuck K- H, Brugada J, Fürnkranz A, Metzner A, Ouyang F, Chun KRJ,
Elvan A, Arentz T, Bestehorn K, Pocock SJ, et al. Cryoballoon or ra-
diofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med.
2016;374:2235– 2245. DOI: 10.1056/NEJMo a1602014.
6. Morillo CA, Verma A, Connolly SJ, Kuck KH, Nair GM, Champagne J,
Sterns LD, Beresh H, Healey JS, Natale A. Radiofrequency ablation vs
antiarrhythmic drugs as first- line treatment of paroxysmal atrial fibril-
lation (RAAFT- 2): a randomized trial. JAMA. 2014;311:692– 700. DOI:
10.1001/jama.2014.467.
7. Verma A, Jiang C- Y, Betts TR, Chen J, Deisenhofer I, Mantovan R,
Macle L, Morillo CA, Haverkamp W, Weerasooriya R, et al. Approaches
to catheter ablation for persistent atrial fibrillation. N Engl J Med.
2015;372:1812– 1822. DOI: 10.1056/NEJMo a1408288.
8. Cosedis Nielsen J, Johannessen A, Raatikainen P, Hindricks G,
Walfridsson H, Kongstad O, Pehrson S, Englund A, Hartikainen J,
Mortensen LS, et al. Radiofrequency ablation as initial therapy in par-
oxysmal atrial fibrillation. N Engl J Med. 2012;367:1587– 1595. DOI:
10.1056/NEJMo a1113566.
9. Arbelo E, Brugada J, Hindricks G, Maggioni AP, Tavazzi L, Vardas P,
Laroche C, Anselme F, Inama G, Jais P, et al. The atrial fibrillation ab-
lation pilot study: a European Survey on Methodology and results of
catheter ablation for atrial fibrillation conducted by the European Heart
Dow
nloaded from http://ahajournals.org by on June 30, 2021

J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 11
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
Rhythm Association. Eur Heart J. 2014;35:1466– 1478. DOI: 10.1093/
eurhe artj/ehu001.
10. Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE,
Noseworthy PA, Rosenberg YD, Jeffries N, Mitchell LB, et al. Effect of
catheter ablation vs antiarrhythmic drug therapy on mortality, stroke,
bleeding, and cardiac arrest among patients with atrial fibrillation: the
CABANA randomized clinical trial. JAMA. 2019;321:1261– 1274. DOI:
10.1001/jama.2019.0693.
11. Balk EM, Garlitski AC, Alsheikh- Ali AA, Terasawa T, Chung M, Ip S.
Predictors of atrial fibrillation recurrence after radiofrequency cath-
eter ablation: a systematic review. J Cardiovasc Electrophysiol.
2010;21:1208– 1216. DOI: 10.1111/j.1540- 8167.2010.01798.x.
12. Chao T- F, Cheng C- C, Lin W- S, Tsao H- M, Lin Y- J, Chang S- L, Lo L- W,
Hu Y- F, Tuan T- C, Suenari K, et al. Associations among the CHADS(2)
score, atrial substrate properties, and outcome of catheter ablation in
patients with paroxysmal atrial fibrillation. Heart Rhythm. 2011;8:1155–
1159. DOI: 10.1016/j.hrthm.2011.03.016.
13. Winkle RA, Jarman JW, Mead RH, Engel G, Kong MH, Fleming W,
Patrawala RA. Predicting atrial fibrillation ablation outcome: the
CAAP- AF score. Heart Rhythm. 2016;13:2119– 2125. DOI: 10.1016/j.
hrthm.2016.07.018.
14. Kornej J, Hindricks G, Kosiuk J, Arya A, Sommer P, Husser D, Rolf
S, Richter S, Huo Y, Piorkowski C, et al. Comparison of CHADS2,
R2CHADS2, and CHA2DS2- VASc scores for the prediction of rhythm
outcomes after catheter ablation of atrial fibrillation: the Leipzig Heart
Center AF Ablation Registry. Circ Arrhythm Electrophysiol. 2014;7:281–
287. DOI: 10.1161/CIRCEP.113.001182.
15. Cai L, Yin Y, Ling Z, Su LI, Liu Z, Wu J, Du H, Lan X, Fan J, Chen W, et al.
Predictors of late recurrence of atrial fibrillation after catheter ablation.
Int J Cardiol. 2013;164:82– 87. DOI: 10.1016/j.ijcard.2011.06.094.
16. Ng CY, Liu T, Shehata M, Stevens S, Chugh SS, Wang X. Meta- analysis
of obstructive sleep apnea as predictor of atrial fibrillation recurrence
after catheter ablation. Am J Cardiol. 2011;108:47– 51. DOI: 10.1016/j.
amjca rd.2011.02.343.
17. Shukla A, Aizer A, Holmes D, Fowler S, Park DS, Bernstein S, Bernstein
N, Chinitz L. Effect of obstructive sleep apnea treatment on atrial fibril-
lation recurrence: a meta- analysis. JACC Clin Electrophysiol. 2015;1:41–
51. DOI: 10.1016/j.jacep.2015.02.014.
18. Abecasis J, Dourado R, Ferreira A, Saraiva C, Cavaco D, Santos KR,
Morgado FB, Adragão P, Silva A. Left atrial volume calculated by
multi- detector computed tomography may predict successful pulmo-
nary vein isolation in catheter ablation of atrial fibrillation. Europace.
2009;11:1289– 1294. DOI: 10.1093/europ ace/eup198.
19. Costa FM, Ferreira AM, Oliveira S, Santos PG, Durazzo A, Carmo P,
Santos KR, Cavaco D, Parreira L, Morgado F, et al. Left atrial volume is
more important than the type of atrial fibrillation in predicting the long-
term success of catheter ablation. Int J Cardiol. 2015;184:56– 61. DOI:
10.1016/j.ijcard.2015.01.060.
20. Nedios S, Kosiuk J, Koutalas E, Kornej J, Sommer P, Arya A, Richter
S, Rolf S, Husser D, Hindricks G, et al. Comparison of left atrial dimen-
sions in CT and echocardiography as predictors of long- term success
after catheter ablation of atrial fibrillation. J Interv Card Electrophysiol.
2015;43:237– 244. DOI: 10.1007/s1084 0- 015- 0010- 8.
21. Njoku A, Kannabhiran M, Arora R, Reddy P, Gopinathannair R,
Lakkireddy D, Dominic P. Left atrial volume predicts atrial fibrillation
recurrence after radiofrequency ablation: a meta- analysis. Europace.
2018;20:33– 42. DOI: 10.1093/europ ace/eux013.
22. Tang R- B, Yan X- L, Dong J- Z, Kalifa J, Long D- Y, Yu R- H, Bai R, Kang
J- P, Wu J- H, Sang C- H, et al. Predictors of recurrence after a repeat
ablation procedure for paroxysmal atrial fibrillation: role of left atrial
enlargement. Europace. 2014;16:1569– 1574. DOI: 10.1093/europ ace/
euu013.
23. Zhuang J, Wang Y, Tang K, Li X, Peng W, Liang C, Xu Y. Association
between left atrial size and atrial fibrillation recurrence after single cir-
cumferential pulmonary vein isolation: a systematic review and meta-
analysis of observational studies. Europace. 2012;14:638– 645. DOI:
10.1093/europ ace/eur364.
24. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS,
Falk V, González- Juanatey JR, Harjola V- P, Jankowska EA, et al. 2016
ESC Guidelines for the diagnosis and treatment of acute and chronic
heart failure: the Task Force for the diagnosis and treatment of acute
and chronic heart failure of the European Society of Cardiology (ESC)
Developed with the special contribution of the Heart Failure Association
(HFA) of the ESC. Eur Heart J. 2016;37:2129– 2200. DOI: 10.1093/eurhe
artj/ehw128.
25. Troughton R, Michael Felker G, Januzzi JL Jr. Natriuretic peptide-
guided heart failure management. Eur Heart J. 2014;35:16– 24. DOI:
10.1093/eurhe artj/eht463.
26. Writing Committee Members, Yancy CW, Jessup M, Bozkurt B, Butler
J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, et
al. 2013 ACCF/AHA guideline for the management of heart failure: a
report of the American College of Cardiology Foundation/American
Heart Association Task Force on practice guidelines. Circulation.
2013;128:e240– e327. DOI: 10.1161/CIR.0b013 e3182 9e8776.
27. Al- Khatib SM, Benjamin EJ, Buxton AE, Calkins H, Chung MK, Curtis
AB, Desvigne- Nickens P, Jais P, Packer DL, Piccini JP, et al. Research
needs and priorities for catheter ablation of atrial fibrillation: a report from
a national heart, lung, and blood institute virtual workshop. Circulation.
2020;141:482– 492. DOI: 10.1161/CIRCU LATIO NAHA.119.042706.
28. Badoz M, Arrigo M, Iung B, Amioglu G, Yilmaz MB, Meneveau N,
Sadoune M, Brunette A, Mebazaa A, Seronde MF. Role of cardio-
vascular biomarkers for the assessment of mitral stenosis and its
complications. Eur J Intern Med. 2016;34:58– 62. DOI: 10.1016/j.
ejim.2016.05.008.
29. Badoz M, Arrigo M, Mogenet AC, Sadoune M, Meneveau N, Mebazaa
A, Seronde MF. Assessment of successful percutaneous mitral com-
missurotomy by MRproANP and sCD146. BMC Cardiovasc Disord.
2020;20:157. DOI: 10.1186/s1287 2- 020- 01435 - y.
30. Charitakis E, Karlsson LO, Papageorgiou JM, Walfridsson U, Carlhäll
CJ. Echocardiographic and biochemical factors predicting arrhythmia
recurrence after catheter ablation of atrial fibrillation- an observational
study. Front Physiol. 2019;10:1215. DOI: 10.3389/fphys.2019.01215.
31. Ravassa S, Ballesteros G, Lopez B, Ramos P, Bragard J, Gonzalez A,
Moreno MU, Querejeta R, Vives E, Garcia- Bolao I, et al. Combination
of circulating type I collagen- related biomarkers is associated with
atrial fibrillation. J Am Coll Cardiol. 2019;73:1398– 1410. DOI: 10.1016/j.
jacc.2018.12.074.
32. Vianello E, Dozio E, Tacchini L, Frati L, Corsi Romanelli MM. ST2/IL- 33
signaling in cardiac fibrosis. Int J Biochem Cell Biol. 2019;116:105619.
DOI: 10.1016/j.biocel.2019.105619.
33. Weinberg EO, Shimpo M, Hurwitz S, Tominaga S, Rouleau JL, Lee RT.
Identification of serum soluble ST2 receptor as a novel heart failure
biomarker. Circulation. 2003;107:721– 726. DOI: 10.1161/01.CIR.00000
47274.66749.FE.
34. Aimo A, Vergaro G, Passino C, Ripoli A, Ky B, Miller WL, Bayes- Genis A,
Anand I, Januzzi JL, Emdin M. Prognostic value of soluble suppression
of tumorigenicity- 2 in chronic heart failure: a meta- analysis. JACC Heart
Fail. 2017;5:280– 286. DOI: 10.1016/j.jchf.2016.09.010.
35. Anand IS, Rector TS, Kuskowski M, Snider J, Cohn JN. Prognostic
value of soluble ST2 in the valsartan heart failure trial. Circ Heart Fail.
2014;7:418– 426. DOI: 10.1161/CIRCH EARTF AILURE.113.001036.
36. Gaggin HK, Szymonifka J, Bhardwaj A, Belcher A, De Berardinis B,
Motiwala S, Wang TJ, Januzzi JL Jr. Head- to- head comparison of serial
soluble ST2, growth differentiation factor- 15, and highly- sensitive tropo-
nin T measurements in patients with chronic heart failure. JACC Heart
Fail. 2014;2:65– 72. DOI: 10.1016/j.jchf.2013.10.005.
37. Ky B, French B, McCloskey K, Rame JE, McIntosh E, Shahi P, Dries
DL, Tang WHW, Wu AHB, Fang JC, et al. High- sensitivity ST2 for pre-
diction of adverse outcomes in chronic heart failure. Circ Heart Fail.
2011;4:180– 187. DOI: 10.1161/CIRCH EARTF AILURE.110.958223.
38. van Vark LC, Lesman- Leegte I, Baart SJ, Postmus D, Pinto YM, Orsel
JG, Westenbrink BD, Brunner- la Rocca HP, van Miltenburg AJM,
Boersma E, et al. Prognostic value of serial ST2 measurements in pa-
tients with acute heart failure. J Am Coll Cardiol. 2017;70:2378– 2388.
DOI: 10.1016/j.jacc.2017.09.026.
39. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B,
Castella M, Diener H- C, Heidbuchel H, Hendriks J, et al. 2016 ESC
Guidelines for the management of atrial fibrillation developed in collab-
oration with EACTS. Eur Heart J. 2016;37:2893– 2962. DOI: 10.1093/
eurhe artj/ehw210.
40. Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster
MC, Horton K, Ogunyankin KO, Palma RA, Velazquez EJ. Guidelines
for performing a comprehensive transthoracic echocardiographic ex-
amination in adults: recommendations from the American Society
of Echocardiography. J Am Soc Echocardiogr. 2019;32:1– 64. DOI:
10.1016/j.echo.2018.06.004.
Dow
nloaded from http://ahajournals.org by on June 30, 2021

J Am Heart Assoc. 2021;10:e020917. DOI: 10.1161/JAHA.121.020917 12
Badoz et al MRproANP and Recurrent AF After Catheter Ablation
41. Vesely DL. Atrial natriuretic peptide prohormone gene expression:
hormones and diseases that upregulate its expression. IUBMB Life.
2002;53:153– 159. DOI: 10.1080/15216 54021 2336.
42. Buckley MG, Marcus NJ, Yacoub MH. Cardiac peptide stability, aprotinin
and room temperature: importance for assessing cardiac function in clin-
ical practice. Clin Sci. 1999;97:689– 695. DOI: 10.1042/CS199 90194.
43. Morgenthaler NG, Struck J, Thomas B, Bergmann A.
Immunoluminometric assay for the midregion of pro- atrial natriuretic
peptide in human plasma. Clin Chem. 2004;50:234– 236. DOI: 10.1373/
clinc hem.2003.021204.
44. Kistorp C, Bliddal H, Goetze JP, Christensen R, Faber J. Cardiac natri-
uretic peptides in plasma increase after dietary induced weight loss in
obesity. BMC Obes. 2014;1:24. DOI: 10.1186/s4060 8- 014- 0024- 2.
45. Darkner S, Goetze JP, Chen X, Henningsen K, Pehrson S, Svendsen
JH. Natriuretic propeptides as markers of atrial fibrillation burden and
recurrence (from the AMIO- CAT trial). Am J Cardiol. 2017;120:1309–
1315. DOI: 10.1016/j.amjca rd.2017.07.018.
46. Sramko M, Wichterle D, Melenovsky V, Franekova J, Clemens M,
Fukunaga M, Kautzner J. Independent effect of atrial fibrillation on
natriuretic peptide release. Clin Res Cardiol. 2019;108:142– 149. DOI:
10.1007/s0039 2- 018- 1332- 1.
47. Jones DG, Haldar SK, Donovan J, McDonagh TA, Sharma R, Hussain
W, Markides V, Wong T. Biomarkers in persistent AF and heart failure:
impact of catheter ablation compared with rate control. Pacing Clin
Electrophysiol. 2016;39:926– 934. DOI: 10.1111/pace.12919.
48. Sacher F, Corcuff J- B, Schraub P, Le Bouffos V, Georges A, Jones SO,
Lafitte S, Bordachar P, Hocini M, Clementy J, et al. Chronic atrial fibril-
lation ablation impact on endocrine and mechanical cardiac functions.
Eur Heart J. 2008;29:1290– 1295. DOI: 10.1093/eurhe artj/ehm577.
49. Ellinor PT, Low AF, Patton KK, Shea MA, Macrae CA. Discordant
atrial natriuretic peptide and brain natriuretic peptide levels in lone
atrial fibrillation. J Am Coll Cardiol. 2005;45:82– 86. DOI: 10.1016/
j.jacc.2004.09.045.
50. Begg GA, Holden AV, Lip GY, Plein S, Tayebjee MH. Assessment of
atrial fibrosis for the rhythm control of atrial fibrillation. Int J Cardiol.
2016;220:155– 161. DOI: 10.1016/j.ijcard.2016.06.144.
51. Dzeshka MS, Lip GY, Snezhitskiy V, Shantsila E. Cardiac fibrosis in pa-
tients with atrial fibrillation: mechanisms and clinical implications. J Am
Coll Cardiol. 2015;66:943– 959. DOI: 10.1016/j.jacc.2015.06.1313.
52. Gal P, Marrouche NF. Magnetic resonance imaging of atrial fibrosis:
redefining atrial fibrillation to a syndrome. Eur Heart J. 2017;38:14– 19.
DOI: 10.1093/eurhe artj/ehv514.
53. Shinagawa K, Shi YF, Tardif JC, Leung TK, Nattel S. Dynamic nature
of atrial fibrillation substrate during development and reversal of heart
failure in dogs. Circulation. 2002;105:2672– 2678. DOI: 10.1161/01.
CIR.00000 16826.62813.F5.
54. O’Meara E, Prescott MF, Claggett B, Rouleau JL, Chiang LM, Solomon
SD, Packer M, McMurray JJV, Zile MR. Independent prognostic value
of serum soluble ST2 measurements in patients with heart failure and
a reduced ejection fraction in the PARADIGM- HF Trial (Prospective
Comparison of ARNI With ACEI to Determine Impact on Global Mortality
and Morbidity in Heart Failure). Circ Heart Fail. 2018;11:e004446. DOI:
10.1161/CIRCH EARTF AILURE.117.004446.
55. Tuegel C, Katz R, Alam M, Bhat Z, Bellovich K, de Boer I, Brosius F,
Gadegbeku C, Gipson D, Hawkins J, et al. GDF- 15, galectin 3, sol-
uble ST2, and risk of mortality and cardiovascular events in CKD.
Am J Kidney Dis. 2018;72:519– 528. DOI: 10.1053/j.ajkd.2018.
03.025.
56. Okar S, Kaypakli O, Şahin DY, Koç M. Fibrosis marker soluble ST2 pre-
dicts atrial fibrillation recurrence after cryoballoon catheter ablation of
nonvalvular paroxysmal atrial fibrillation. Korean Circ J. 2018;48:920–
929. DOI: 10.4070/kcj.2018.0047.
57. Marrouche NF, Brachmann J, Andresen D, Siebels J, Boersma
L, Jordaens L, Merkely B, Pokushalov E, Sanders P, Proff J, et al.
Catheter ablation for atrial fibrillation with heart failure. N Engl J Med.
2018;378:417– 427. DOI: 10.1056/NEJMo a1707855.
Dow
nloaded from http://ahajournals.org by on June 30, 2021

Supp
lem
enta
l Mat
eria
l
Downloaded from http://ahajournals.org by on June 30, 2021
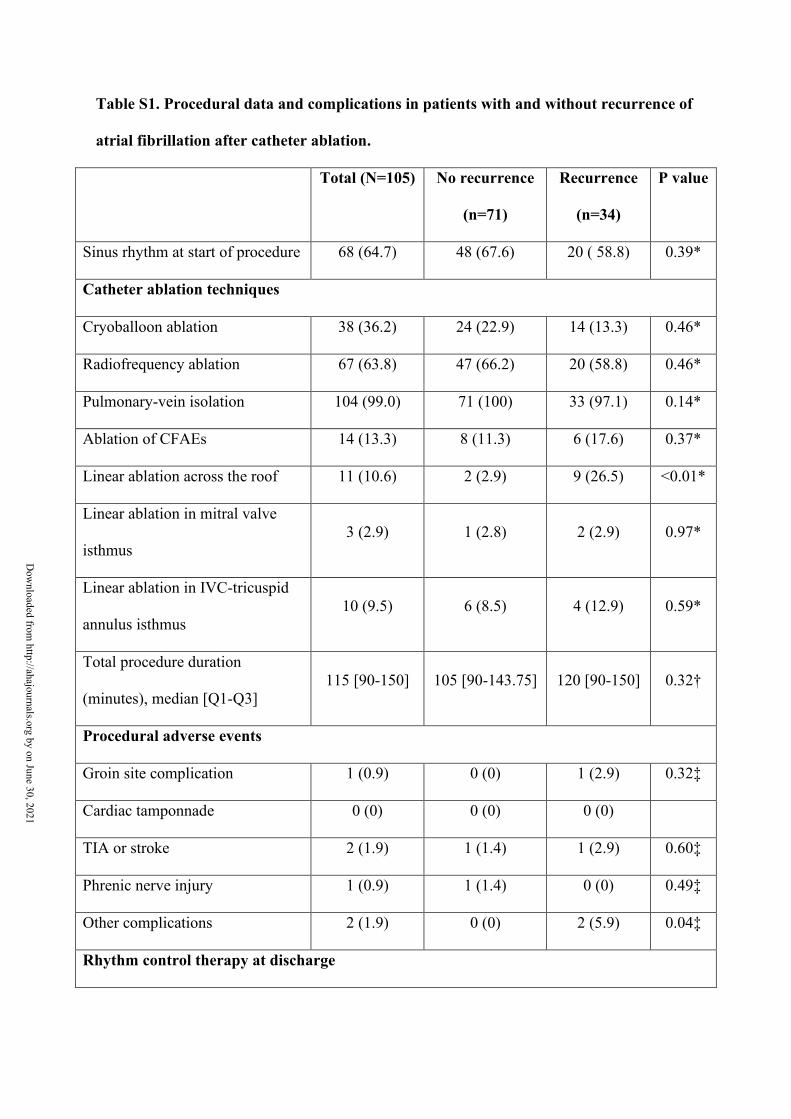
Table S1. Procedural data and complications in patients with and without recurrence of
atrial fibrillation after catheter ablation.
Total (N=105) No recurrence
(n=71)
Recurrence
(n=34)
P value
Sinus rhythm at start of procedure 68 (64.7) 48 (67.6) 20 ( 58.8) 0.39*
Catheter ablation techniques
Cryoballoon ablation 38 (36.2) 24 (22.9) 14 (13.3) 0.46*
Radiofrequency ablation 67 (63.8) 47 (66.2) 20 (58.8) 0.46*
Pulmonary-vein isolation 104 (99.0) 71 (100) 33 (97.1) 0.14*
Ablation of CFAEs 14 (13.3) 8 (11.3) 6 (17.6) 0.37*
Linear ablation across the roof 11 (10.6) 2 (2.9) 9 (26.5) <0.01*
Linear ablation in mitral valve
isthmus 3 (2.9) 1 (2.8) 2 (2.9) 0.97*
Linear ablation in IVC-tricuspid
annulus isthmus 10 (9.5) 6 (8.5) 4 (12.9) 0.59*
Total procedure duration
(minutes), median [Q1-Q3] 115 [90-150] 105 [90-143.75] 120 [90-150] 0.32†
Procedural adverse events
Groin site complication 1 (0.9) 0 (0) 1 (2.9) 0.32‡
Cardiac tamponnade 0 (0) 0 (0) 0 (0)
TIA or stroke 2 (1.9) 1 (1.4) 1 (2.9) 0.60‡
Phrenic nerve injury 1 (0.9) 1 (1.4) 0 (0) 0.49‡
Other complications 2 (1.9) 0 (0) 2 (5.9) 0.04‡
Rhythm control therapy at discharge
Dow
nloaded from http://ahajournals.org by on June 30, 2021
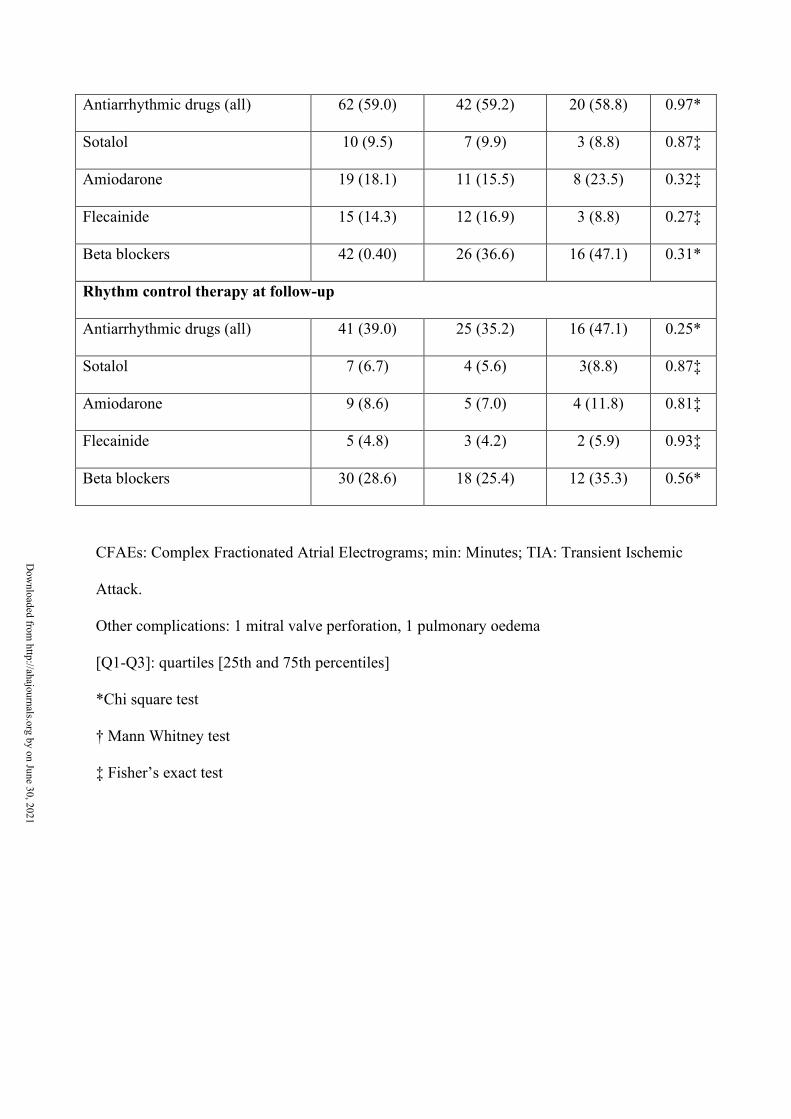
Antiarrhythmic drugs (all) 62 (59.0) 42 (59.2) 20 (58.8) 0.97*
Sotalol 10 (9.5) 7 (9.9) 3 (8.8) 0.87‡
Amiodarone 19 (18.1) 11 (15.5) 8 (23.5) 0.32‡
Flecainide 15 (14.3) 12 (16.9) 3 (8.8) 0.27‡
Beta blockers 42 (0.40) 26 (36.6) 16 (47.1) 0.31*
Rhythm control therapy at follow-up
Antiarrhythmic drugs (all) 41 (39.0) 25 (35.2) 16 (47.1) 0.25*
Sotalol 7 (6.7) 4 (5.6) 3(8.8) 0.87‡
Amiodarone 9 (8.6) 5 (7.0) 4 (11.8) 0.81‡
Flecainide 5 (4.8) 3 (4.2) 2 (5.9) 0.93‡
Beta blockers 30 (28.6) 18 (25.4) 12 (35.3) 0.56*
CFAEs: Complex Fractionated Atrial Electrograms; min: Minutes; TIA: Transient Ischemic
Attack.
Other complications: 1 mitral valve perforation, 1 pulmonary oedema
[Q1-Q3]: quartiles [25th and 75th percentiles]
*Chi square test
† Mann Whitney test
‡ Fisher’s exact test
Dow
nloaded from http://ahajournals.org by on June 30, 2021
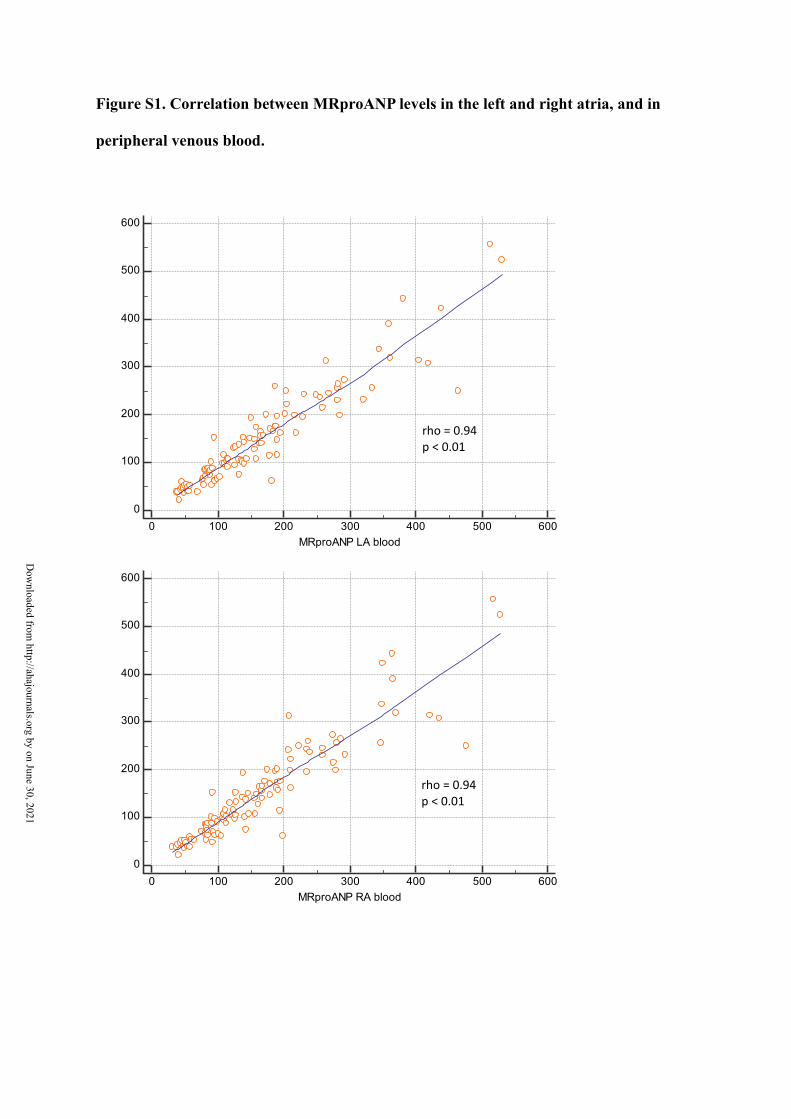
Figure S1. Correlation between MRproANP levels in the left and right atria, and in
peripheral venous blood.
0
100
200
300
400
500
600
0 100 200 300 400 500 600MRproANP LA blood
MR
proA
NP
PV b
lood
0
100
200
300
400
500
600
0 100 200 300 400 500 600MRproANP RA blood
MR
proA
NP
PV b
lood
rho = 0.94 p < 0.01
rho = 0.94 p < 0.01
Dow
nloaded from http://ahajournals.org by on June 30, 2021

Figure S2. Correlation between MRproANP (pmol/L) concentration in peripheral
venous blood, and in the left atrium (LA blood) and right atrium (RA blood) prior to
the catheter ablation procedure.
0
100
200
300
400
500
600
MR
proA
NP
(pm
ol/L
)
Peripheral_venous_blood LA_blood RA_blood
p<0.01 p=0.14
p<0.01
Dow
nloaded from http://ahajournals.org by on June 30, 2021
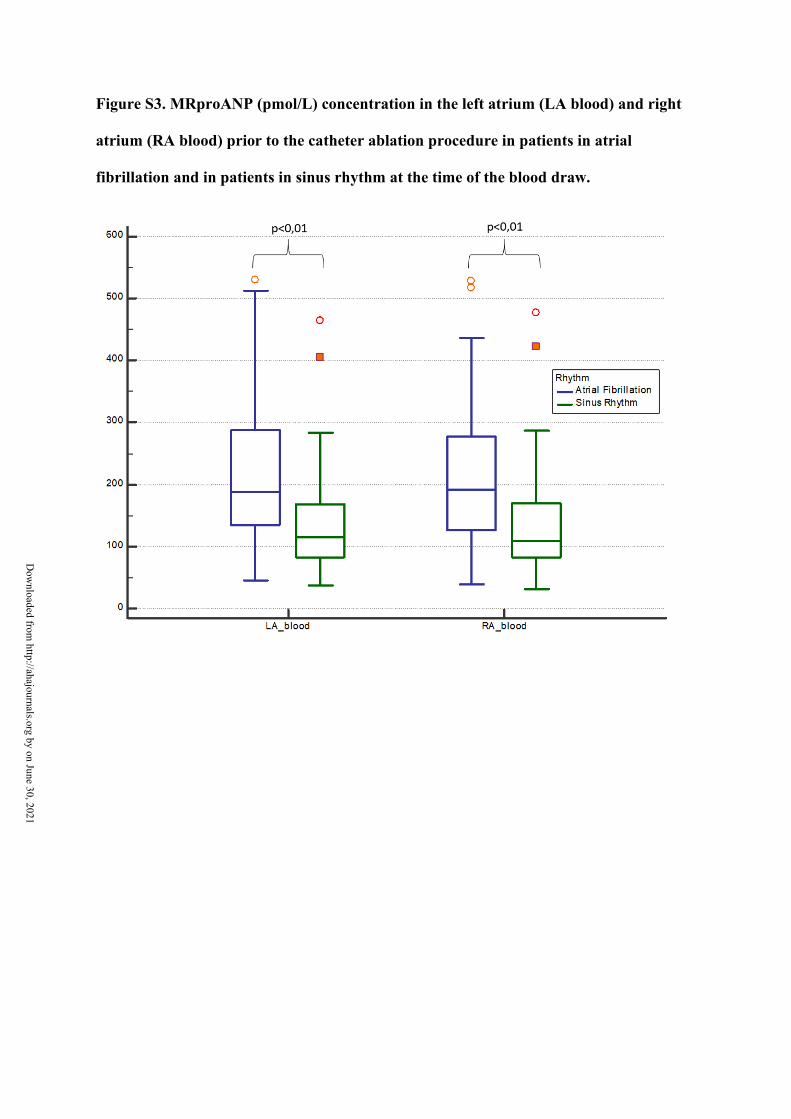
Figure S3. MRproANP (pmol/L) concentration in the left atrium (LA blood) and right
atrium (RA blood) prior to the catheter ablation procedure in patients in atrial
fibrillation and in patients in sinus rhythm at the time of the blood draw.
D
ownloaded from
http://ahajournals.org by on June 30, 2021
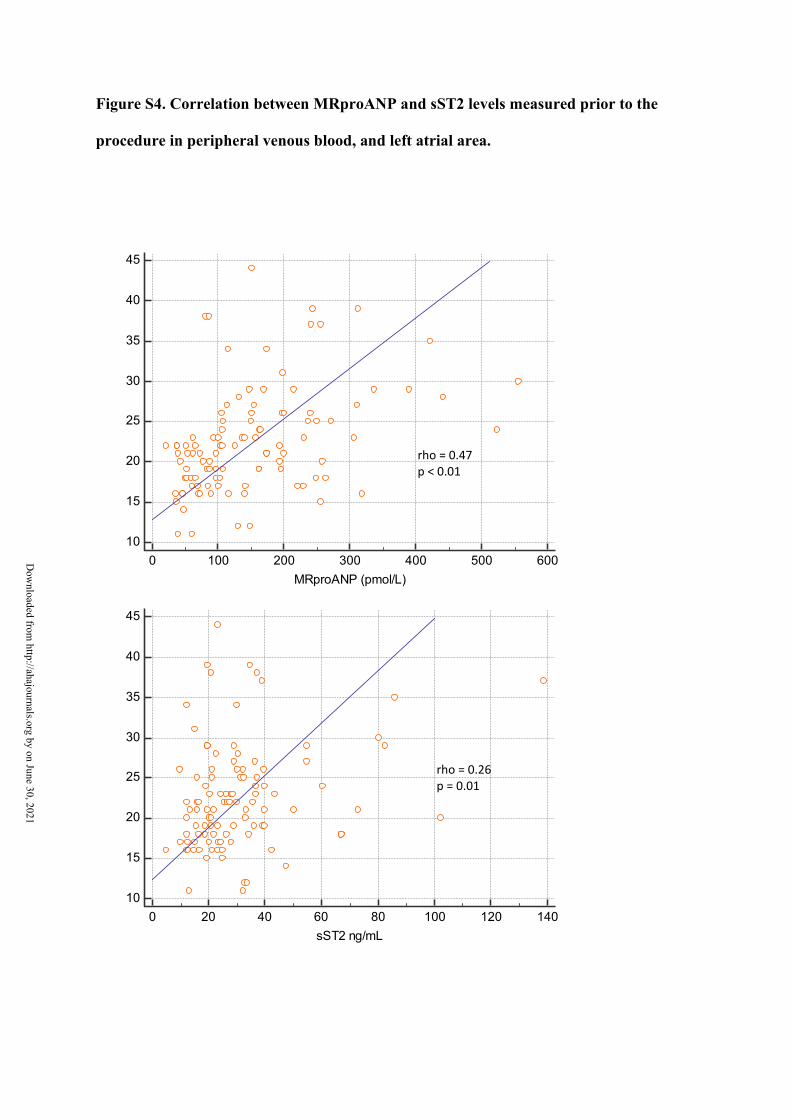
Figure S4. Correlation between MRproANP and sST2 levels measured prior to the
procedure in peripheral venous blood, and left atrial area.
10
15
20
25
30
35
40
45
0 20 40 60 80 100 120 140sST2 ng/mL
Left
atria
l sur
face
(cm
2)
10
15
20
25
30
35
40
45
0 100 200 300 400 500 600MRproANP (pmol/L)
Left
atria
l sur
face
(cm
2)
rho = 0.47 p < 0.01
rho = 0.26 p = 0.01
Dow
nloaded from http://ahajournals.org by on June 30, 2021
92
VI. Synthèse et
perspectives
93
Ce travail de thèse s’est intéressé, par la publication de 4 articles, à l’utilisation de
biomarqueurs potentiellement liés à la dysfonction atriale dans des pathologies affectant en
premier lieu l’oreillette.
Le MRproANP et le sCD146 étaient liés à la congestion et à la dilatation des oreillettes
droite et gauche chez des patients consultant pour dyspnée.
Dans la sténose mitrale le MRproANP et le sCD146 étaient liés à la fois à la sévérité de
la sténose, aux complications de la sténose et au succès d’une procédure de commissurotomie
percutanée.
Le MRproANP semblait avoir un intérêt pronostic important dans la fibrillation atriale,
alors que le sST2 n’était pas un prédicteur indépendant de récidive post ablation.
VI.1. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide chez des patients
atteints de sténose mitrale
Dans nos résultats nous avons montré que le MRproANP était significativement plus
élevé chez les patients lorsque la sténose mitrale était serrée en comparaison aux sténoses
mitrales moyennement serrées (2). Le MRproANP est secrété du fait de la contrainte pariétale
exercée sur les myocytes de l’oreillette gauche notamment. Ainsi plus la sténose mitrale devient
serrée, plus la pression atriale gauche augmente, plus la sécrétion s’élève.
Par ailleurs, chez les patients porteurs de sténose mitrale, le MRproANP était
significativement plus élevé en présence d’une hypertension artérielle pulmonaire (HTP)
compliquant la sténose mitrale. L’élévation du MRproANP était également présente chez des
patients atteints d’hypertension artérielle pulmonaire pré-capillaire, avec des niveaux proches
94
de ceux des patients porteurs de sténoses mitrales compliquées d’HTP (p=0.20). Par définition
l’oreillette gauche est épargnée dans l’hypertension artérielle pulmonaire pré-capillaire, la
répercussion de la pathologie se fait sur les cavités droites. Il existe probablement pour ces
patients une sécrétion de MRproANP provenant de l’oreillette droite. Cette hypothèse est
vraisemblable d’autant que les données de l’étude BIORHYTHM (4) plaidaient pour une
sécrétion du MRproANP par les oreillettes gauche et droite avec des concentrations de
MRproANP équivalentes entre oreillettes gauche et droite, plus élevées que dans le sang
veineux périphérique.
Lors d’une valvuloplastie mitrale percutanée (VMP), l’ouverture même partielle de
l’obstacle que constitue la sténose mitrale entraîne immédiatement une diminution de la
pression atriale gauche (86, 87), et ainsi une diminution significative du MRproANP que nous
avons mis en évidence (3). La diminution des pressions pulmonaires après VMP contribue
également à la diminution des concentrations de MRproANP par la diminution de la contrainte
pariétale exercée sur l’oreillette droite. La diminution significative du MRproANP dans les 24
heures en cas de succès d’une VMP est possible en raison d’une cinétique de sécrétion et de
décroissance adaptée et réactive, permettant à ce biomarqueur d’être un marqueur de succès
immédiat de la procédure. En cas d’échec de la VMP, la pression intra atriale gauche et les
pressions pulmonaires ne diminuent pas suffisamment pour entrainer une diminution
significative du MRproANP. Ces données confirment et actualisent, sur un plus grand nombre
de patients, de précédentes publications qui avaient mis en évidence une décroissance de l’ANP
après commissurotomie mitrale percutanée et un lien significatif entre diminution de la pression
atriale gauche et décroissance de l’ANP (86, 87).
Le MRproANP, d’après les articles publiés dans cette thèse, semble être un marqueur
fiable pour évaluer la sévérité d’une sténose mitrale et le succès de son traitement (2, 3). Il
n’existe pas de données plus récentes sur ce sujet.

95
VI.2. Intérêt du Mid-Regional pro Atrial Natriuretic Peptide chez des patients
atteints de fibrillation atriale
Il n’a pas été mis en évidence de différence significative de MRproANP entre les
patients atteints de sténose mitrale avec fibrillation atriale et ceux sans fibrillation atriale (2).
Cette absence de différence significative (p=0.69) est possiblement lié à un manque de
puissance lié au faible effectif de notre étude. Nous avons en effet montré sur un plus grand
effectif que les concentrations veineuses périphériques et intra-atriales de MRproANP étaient
plus élevées en fibrillation atriale qu’en rythme sinusal (4).
Dans le domaine de l’ablation de fibrillation atriale, nous avons identifié un seuil de
107.9pmol/L au-delà duquel le risque de récidive de FA à 1 an de l’ablation est multiplié par
presque 25. Inversement, en dessous de ce seuil les patients sont très peu sujets à la récidive
(4.2%) avec une valeur prédictive négative très élevée de 95.7% (4). Il existait une relation
linéaire entre les niveaux de MRproANP pré procédure et le risque de récidive à un an de
l’ablation de fibrillation atriale.
Dans cette même étude les concentrations intra atriales de MRproANP étaient plus
élevées chez les patients en fibrillation qu’en rythme sinusal, que ce soit dans l’oreillette droite
ou gauche. Les concentrations intra atriales droite et gauche ne différaient pas significativement
entre elles, en revanche, elles étaient plus élevées que dans le sang veineux périphérique. Ces
résultats vont dans le sens d’une sécrétion du MRproANP par les oreillettes droite et gauche
chez les patients en fibrillation atriale.
96
A notre connaissance, il n’existe pas d’autre étude prospective s’intéressant au lien entre
MRproANP pré procédure et récidive de FA à long terme après une ablation. Sacher et al.
avaient démontré que le maintien du rythme sinusal après une ablation de fibrillation atriale
persistante entrainait une diminution importante du MRproANP à 3 mois (88). Charitakis et al.
suggéraient que le pourcentage de récidive de fibrillation atriale post ablation était plus élevé
pour des patients ayant des concentrations de MRproANP dans le quatrième quartile en
comparaison au premier quartile (89). Nos données confirment, de façon plus robuste, celles
publiées précédemment, en allant plus loin dans le lien récidive de FA et concentrations
plasmatiques de MRproANP.
VI.3. Lien entre modification structurelles de l’oreillette et Mid-Regional pro
Atrial Natriuretic Peptide
En ce qui concerne les modifications structurelles de l’oreillette liées à l’évolution des
différentes pathologies, il existait une corrélation significative entre la surface de l’oreillette
gauche mesurée en échographie cardiaque transthoracique et les concentrations plasmatiques
de MRproANP (4). Le lien entre dilatation des oreillettes droite et gauche et MRproANP a été
mis en évidence également dans une 2ème publication chez des patients présentant une dyspnée
aigue en lien ou non avec des manifestations d’insuffisance cardiaque (1). Des données
précédemment publiées avaient identifié ce lien dans d’autres populations, par exemple chez
des patients après un syndrome coronaire aigu (90). Le lien entre ces deux variables semble
donc réel.
Le MRproANP était un marqueur de congestion fiable dans les données que nous avons
publiées. Il était en effet significativement plus élevé chez des patients dont la dyspnée était liée
97
à des manifestations d’insuffisance cardiaque en comparaison à une dyspnée d’origine
extracardiaque. En revanche il ne permet pas de discriminer l’insuffisance cardiaque à fraction
d’éjection préservée de celle secondaire à une dysfonction ventriculaire gauche systolique (1).
VI.4. Mid-Regional pro Atrial Natriuretic Peptide, synthèse et perspectives de
recherche
Au vu de l’ensemble de ces données, nous pouvons conclure que le MRproANP est un
biomarqueur de dysfonction et d’atteinte atriale pouvant présenter un intérêt en pratique
clinique notamment pour l’évaluation de la sévérité des sténoses mitrales, du succès de leur
traitement et pour le pronostic des pathologies rythmiques atriales en premier lieu dans la
fibrillation atriale. Il ne semble pas être un bon marqueur de dysfonction systolique
ventriculaire.
En ce qui concerne la capacité pronostique du MRproANP dans le domaine de
fibrillation atriale, de récentes publications vont dans le même sens que nos données. Le
MRproANP prélevé en pré opératoire semble notamment prédicteur de survenue de fibrillation
atriale en post opératoire de chirurgie cardiaque (91). L’intérêt pronostique suscité par le
MRproANP touche d’autres domaines, y compris les plus récents. Il est prédicteur indépendant
de mortalité en cas de COVID-19 (92). Des données récentes confirment également le fait que
le MRproANP est un marqueur de dysfonction atriale gauche et de remodelage de l’oreillette
gauche (93).
Nous poursuivons nos travaux de recherche concernant ce biomarqueur. En particulier,
nous nous intéressons à l’impact pronostique du MRproANP en termes de récidives de
98
fibrillation atriale chez les patients de BIORHYTHM soumis à une cardioversion électrique.
L’objectif est bien sûr d’identifier si les taux plasmatiques de MRproANP peuvent prédire le
risque de récidive, mais aussi de savoir si les résultats publiés dans BIORHYTHM à partir des
patients ayant fait l’objet d’une ablation, peuvent être étendus à d’autres situations et à d’autres
types de populations, plus âgées dans ce cas, avec beaucoup plus de comorbidités.
Nous avons également débuté un travail prospectif cherchant à documenter à l’aide d’un
holter implantable, l’incidence de la fibrillation atriale chez des patients traités par fermeture
percutanée de foramen ovale perméable après un accident vasculaire cérébral ischémique :
l’étude PFO-AF (Prevalence of atrial Fibrillation in cryptogenic stroke with patent foramen
Ovale closure: PFO-AF study). Dans cette étude la concentration de MRproANP plasmatique
est dosée sur un prélèvement veineux périphérique pré procédural. Nous évaluerons le lien entre
la concentration de MRproANP et la survenue de fibrillation atriale à distance de la fermeture
de foramen ovale perméable.
VI.5. Intérêt du Soluble Cluster of Differentiation 146 chez des patients atteints
de sténose mitrale.
La seconde publication présentée (2) a montré que le sCD146 était plus élevé chez les
patients porteurs de sténoses mitrales serrées en comparaison à des sténoses mitrales non
serrées. Le sCD146 peut donc être utilisé comme marqueur de la sévérité de la sténose mitrale
comme le MRproANP. Il semble être également un marqueur de survenue de complications de
la sténose mitrale, telles que le passage en fibrillation atriale et l’apparition d’hypertension
artérielle pulmonaire. Il est à noter que les concentrations de sCD146 étaient plus élevées chez
les patients atteints d’hypertension artérielle pré-capillaire (HTAP) que chez ceux atteints de
99
sténose mitrale. Cette différence était toujours significative en comparant cette fois les sténoses
mitrales compliquées d’hypertension pulmonaire aux patients atteints d’HTAP, avec des
niveaux de sCD146 plus élevés chez les patients HTAP.
Le sCD146 est un marqueur d’origine endothéliale, avec notamment une sécrétion par
les gros vaisseaux de la circulation pulmonaire (20-22). Le sCD146 est de ce fait un marqueur
indirect de souffrance de l’oreillette gauche. En devenant serrée la sténose mitrale augmente les
pressions pulmonaires, avec apparition également d’autres complications telles que la FA. Cette
hypertension pulmonaire post capillaire provoque la libération du sCD146, expliquant nos
résultats. Nous expliquons ainsi également l’élévation majeure du sCD146 chez les patients
atteints d’hypertension artérielle pré-capillaire, les chiffres de pressions artérielles pulmonaires
étant plus élevés que ceux des patients avec rétrécissement mitral.
Après une valvuloplastie mitrale percutanée (VMP) réalisée avec succès, on notait une
décroissance du sCD146 alors que si la valvuloplastie est un échec il ne décroit pas
significativement (3). La concentration de sCD146 est corrélée à l’élévation des pressions
artérielles pulmonaires systoliques (PAPs) avant une VMP. La diminution de la concentration
plasmatique du sCD146 est corrélée à l’augmentation de la surface mitrale et à la réduction des
PAPs. Après un succès de valvuloplastie mitrale percutanée, la levée de l’obstacle mitral
entraîne une diminution de la congestion pulmonaire, des PAPs et ainsi une diminution des
niveaux de sCD146, ce qui en fait un marqueur fiable de succès procédural. Il est à noter
également que la diminution significative du sCD146 dans les 24 heures en cas de succès d’une
VMP est possible en raison d’une cinétique de sécrétion et de décroissance adaptée et réactive,
permettant à ce biomarqueur d’être un marqueur de succès immédiat de la procédure.
Nous expliquons ainsi le comportement du sCD146 chez les patients porteurs de sténose
mitrale. Il est un marqueur indirect de dysfonction atriale gauche dans ce contexte, en
représentant l’impact qu’a la cardiopathie sur la circulation pulmonaire en amont de l’oreillette
100
gauche. Il est dans ce cadre un marqueur fiable de sévérité, de complications et de succès du
traitement du rétrécissement mitral.
VI.6. Place du Soluble Cluster of Differentiation 146 dans l’insuffisance
cardiaque
En ce qui concerne l’insuffisance cardiaque, le sCD146 est un marqueur de congestion
pulmonaire et périphérique. Il était en effet significativement plus élevé lorsque la dyspnée
présentée par un patient était liée à des manifestations d’insuffisance cardiaque (1). Il était,
dans la même publication, lié à la dilatation des oreillettes droite et gauche. En revanche il est
à noter que le sCD146 ne permettait pas de discriminer insuffisance cardiaque à fraction
d’éjection préservée ou altérée (1), il est donc purement dans ce cadre un marqueur de
congestion libéré par les gros vaisseaux pulmonaires et périphériques sans lien avec la fonction
ventriculaire gauche.
VI.7. Perspectives actuelles de recherche pour le Soluble Cluster of
Differentiation 146
Le sCD146 a essentiellement été étudié dans le domaine de l’insuffisance cardiaque (1,
23-25), il a montré son intérêt en tant que marqueur de congestion pulmonaire et périphérique.
A notre connaissance il n’existe pas d’autres publications s’intéressant au sCD146 dans le cadre
du rétrécissement mitral.
101
La recherche concernant le sCD146 se poursuit dans divers domaines extra
cardiologiques. Il semblerait par exemple que le sCD146 soit un marqueur d’inflammation au
niveau neurologique central et marqueur de dysfonctionnement de la barrière hémato-
encéphalique (94). Il aurait également une utilité en cancérologie (95) et un intérêt pronostique
dans les néphropathies diabétiques (96).
VI.8. Place du Soluble Suppression of Tumorigenicity 2 chez des patients traités
par ablation de fibrillation atriale
Le sST2 est un marqueur de fibrose (27, 28). L’évolution de la fibrillation atriale est
marquée au niveau structurel par une fibrose atriale (55, 58). Nous nous sommes donc intéressés
à la capacité qu’a ce biomarqueur à prédire les récidives de fibrillation atriale à un an d’une
procédure d’ablation (4). Le sST2 est en effet plus élevé chez patients présentant une récidive
de fibrillation atriale. Une valeur de seuil de 26.7ng/mL prédit une récidive de FA avec valeur
prédictive négative de 83.3% et valeur prédictive positive de 49%. Cependant le sST2 n’était
pas un prédicteur indépendant de récidive de fibrillation atriale dans nos résultats. Deux travaux
publiés récemment semblent aller à l’encontre de nos conclusions (97, 98). En effet dans ces
deux publications le sST2 était un prédicteur de récidive de FA chez des patients traités par
ablation avec des seuils identiques ou très proches de celui que nous avons identifié sur notre
courbe ROC : 26.7ng/mL (4) vs 26,9ng/mL (97) et 26,65ng/mL (98). Ce phénomène est lié à
notre modèle multivarié qui a inclu, à la différence des deux autres publications, une variable
particulièrement robuste dans la prédiction de la récidive : le niveau de MRproANP
plasmatique pré-procédural. Il s’agissait du seul prédicteur de récidive de FA dans notre
modèle. En utilisant, avec nos données, un autre modèle multivarié excluant cette variable, le
102
niveau de sST2 avant ablation est également prédicteur indépendant de récidive. Nos données
sont donc au final en accord avec les publications précédentes (97, 98). Nos résultats montrent
cependant que, même si le sST2 semble être un prédicteur de récidive de fibrillation atriale post
ablation, le MRproANP est plus performant dans ce cadre.
Le sST2 était par ailleurs lié à la dilatation de l’oreillette gauche dans nos données (4)
ainsi que dans différentes publications (97-99). Celui-ci semble également être lié à la présence
ou à l’apparition de zones atriales gauches pathologiques électriquement (zones de bas voltage)
chez des patients traités par ablation de FA (97, 98). Le sST2 est donc un marqueur de
modifications structurelles de l’oreillette gauche, que ce soit par la dilatation, la fibrose, ou la
présence de zones de bas de voltages identifiées en électrophysiologie.
VI.9. Soluble Suppression of Tumorigenicity 2 et insuffisance cardiaque
Dans nos données, sST2 était significativement plus élevé lorsqu’un patient présentait
une dyspnée d’origine cardiaque que lorsque la cause était extracardiaque (1). Il semble être lui
aussi un bon marqueur de congestion. Et, tout comme le MRproANP et le sCD146, il ne semble
pas être un marqueur de dysfonction systolique ventriculaire gauche puisque qu’il n’existait pas
de différence significative de sST2 entre les patients présentant une insuffisance cardiaque à
fraction d’éjection préservée et ceux en insuffisance cardiaque secondaire à une altération de la
fraction d’éjection ventriculaire gauche.
103
VI.10. Synthèse et perspectives de recherche concernant le Soluble Suppression
of Tumorigenicity 2
Le sST2 est connu comme marqueur pronostic dans l’insuffisance cardiaque (29-33,
100). Dans nos résultats il semble donc lié aux manifestations congestives et aux modifications
structurelles de l’oreillette gauche. Il semble lié à la récidive de FA post ablation mais
l’utilisation du MRproANP doit être préférée dans cette indication.
Dans la seconde partie de l’étude BIORHYTHM, nous nous intéresserons une nouvelle
fois à la capacité qu’a le sST2 (et le MRproANP) à prédire la récidive de fibrillation atriale à 1
an, mais cette fois après cardioversion électrique. Le sST2 ne semblait en effet pas le meilleur
biomarqueur pour prédire la récidive de FA dans une population traitée par ablation. La
population traitée par cardioversion électrique est différente, plus âgée, avec plus de
comorbidités et peut-être davantage de fibrose et de dilatation atriale. Nous évaluerons donc de
nouveau le sST2 dans une population différente.
Le sST2 suscite de l’intérêt actuellement dans le domaine de la fibrillation atriale, il est
lié à la présence de zones de bas voltages chez des patients traités par ablation (97-99), il est
associé chez les insuffisants rénaux au risque de survenue de FA (101). Le sST2 est étudié dans
d’autres domaines également, il semble par exemple être un bon marqueur de réponse
inflammatoire et de sévérité du COVID-19 (102).
104
VII. Conclusion
105
Les biomarqueurs étudiés (MRproANP, sCD146, sST2) sont encore peu ou pas utilisés
en pratique clinique quotidienne. Ils pourraient trouver leur place en complément des
biomarqueurs communément utilisés comme le BNP, le NTproBNP et la troponine dans des
pathologies affectant principalement l’oreillette. Nous avons, par ce travail, mis en évidence
leur capacité à identifier les répercussions hémodynamiques et structurelles, au niveau atrial,
de certaines pathologies cardiaques. Nous avons pu montrer leur intérêt pour le pronostic, le
diagnostic de sévérité et le suivi des patients atteints de sténose mitrale ou de fibrillation atriale.
Le MRproANP est un peptide natriurétique plus spécifiquement atrial. D’après les
articles publiés dans cette thèse, il semble être un marqueur fiable pour évaluer la sévérité d’une
sténose mitrale et le succès immédiat de son traitement par voie percutanée. Il est par ailleurs
un excellent prédicteur de récidive de fibrillation atriale à 1 an d’une ablation avec un seuil
identifié de 107.9pmol/L en pré procédure au-delà duquel le risque de récidive est multiplié par
presque 25. En dessous de ce seuil les patients sont très peu sujets à la récidive avec une valeur
prédictive négative très élevée de 95.7%
Le sCD146 est un marqueur indirect de dysfonction et de souffrance atriale gauche chez
les patients porteurs de sténose mitrale en représentant l’impact qu’a la cardiopathie sur la
circulation pulmonaire en amont de l’oreillette gauche. Il est dans ce cadre un marqueur fiable
de sévérité, de complication du rétrécissement mitral. Il s’élève en effet significativement
lorsque le rétrécissement devient serré ou qu’apparaissent fibrillation atriale ou hypertension
pulmonaire. Il est enfin un marqueur de succès immédiat du traitement du rétrécissement mitral
par commissurotomie percutanée, il décroit significativement en cas de succès procédural.
Le sST2 est lié à la récidive de fibrillation atriale post ablation, mais le MRproANP plus
performant dans cette indication doit lui être préféré.
Ces trois biomarqueurs sont liés significativement à la dilatation de l’oreillette gauche.

106
L’utilisation de ces trois biomarqueurs demande à être validée sur de plus grandes
populations notamment dans la fibrillation atriale, la sténose mitrale ou d’autres pathologies
affectant en premier lieu l’oreillette.
107
VIII. Références bibliographiques
108
1. Van Aelst LNL, Arrigo M, Placido R, Akiyama E, Girerd N, Zannad F, et al. Acutely
decompensated heart failure with preserved and reduced ejection fraction present with comparable
haemodynamic congestion. Eur J Heart Fail. 2018;20(4):738-47.
2. Badoz M, Arrigo M, Iung B, Amioglu G, Yilmaz MB, Meneveau N, et al. Role of cardiovascular
biomarkers for the assessment of mitral stenosis and its complications. Eur J Intern Med. 2016;34:58-
62.
3. Badoz M, Arrigo M, Mogenet AC, Sadoune M, Meneveau N, Mebazaa A, et al. Assessment of
successful percutaneous mitral commissurotomy by MRproANP and sCD146. BMC Cardiovasc Disord.
2020;20(1):157.
4. Badoz M, Serzian G, Favoulet B, Sellal JM, De Chillou C, Hammache N, et al. Impact of
Midregional N-Terminal Pro-Atrial Natriuretic Peptide and Soluble Suppression of Tumorigenicity 2
Levels on Heart Rhythm in Patients Treated With Catheter Ablation for Atrial Fibrillation: The
Biorhythm Study. J Am Heart Assoc. 2021:e020917.
5. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC
Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation. Eur Heart J. 2020.
6. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC
Guidelines for the management of acute myocardial infarction in patients presenting with ST-
segment elevation: The Task Force for the management of acute myocardial infarction in patients
presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J.
2018;39(2):119-77.
7. Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. 2019 ESC
Guidelines for the diagnosis and management of acute pulmonary embolism developed in
collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603.
8. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC
Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the
diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology
(ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur
Heart J. 2016;37(27):2129-200.
9. Vesely DL. Atrial natriuretic peptide prohormone gene expression: hormones and diseases
that upregulate its expression. IUBMB Life. 2002;53(3):153-9.
10. Gardner DG, Deschepper CF, Ganong WF, Hane S, Fiddes J, Baxter JD, et al. Extra-atrial
expression of the gene for atrial natriuretic factor. Proc Natl Acad Sci U S A. 1986;83(18):6697-701.
11. Poulos JE, Gower WR, Jr., Sullebarger JT, Fontanet HL, Vesely DL. Congestive heart failure:
increased cardiac and extracardiac atrial natriuretic peptide gene expression. Cardiovasc Res.
1996;32(5):909-19.
12. Buckley MG, Marcus NJ, Yacoub MH. Cardiac peptide stability, aprotinin and room
temperature: importance for assessing cardiac function in clinical practice. Clin Sci (Lond).
1999;97(6):689-95.
13. Morgenthaler NG, Struck J, Thomas B, Bergmann A. Immunoluminometric assay for the
midregion of pro-atrial natriuretic peptide in human plasma. Clin Chem. 2004;50(1):234-6.
14. Kistorp C, Bliddal H, Goetze JP, Christensen R, Faber J. Cardiac natriuretic peptides in plasma
increase after dietary induced weight loss in obesity. BMC Obes. 2014;1:24.
15. Maisel A, Mueller C, Nowak R, Peacock WF, Landsberg JW, Ponikowski P, et al. Mid-region
pro-hormone markers for diagnosis and prognosis in acute dyspnea: results from the BACH
(Biomarkers in Acute Heart Failure) trial. J Am Coll Cardiol. 2010;55(19):2062-76.
16. Seronde MF, Gayat E, Logeart D, Lassus J, Laribi S, Boukef R, et al. Comparison of the
diagnostic and prognostic values of B-type and atrial-type natriuretic peptides in acute heart failure.
Int J Cardiol. 2013;168(4):3404-11.
17. Cinar O, Cevik E, Acar A, Kaya C, Ardic S, Comert B, et al. Evaluation of mid-regional pro-atrial
natriuretic peptide, procalcitonin, and mid-regional pro-adrenomedullin for the diagnosis and risk
stratification of dyspneic ED patients. Am J Emerg Med. 2012;30(9):1915-20.
109
18. Gohar A, Rutten FH, den Ruijter H, Kelder JC, von Haehling S, Anker SD, et al. Mid-regional
pro-atrial natriuretic peptide for the early detection of non-acute heart failure. Eur J Heart Fail.
2019;21(10):1219-27.
19. Nigro N, Winzeler B, Suter-Widmer I, Schuetz P, Arici B, Bally M, et al. Mid-regional pro-atrial
natriuretic peptide and the assessment of volaemic status and differential diagnosis of profound
hyponatraemia. J Intern Med. 2015;278(1):29-37.
20. Bardin N, Anfosso F, Massé JM, Cramer E, Sabatier F, Le Bivic A, et al. Identification of CD146
as a component of the endothelial junction involved in the control of cell-cell cohesion. Blood.
2001;98(13):3677-84.
21. Anfosso F, Bardin N, Vivier E, Sabatier F, Sampol J, Dignat-George F. Outside-in signaling
pathway linked to CD146 engagement in human endothelial cells. J Biol Chem. 2001;276(2):1564-9.
22. Boneberg EM, Illges H, Legler DF, Fürstenberger G. Soluble CD146 is generated by
ectodomain shedding of membrane CD146 in a calcium-induced, matrix metalloprotease-dependent
process. Microvasc Res. 2009;78(3):325-31.
23. Gayat E, Caillard A, Laribi S, Mueller C, Sadoune M, Seronde MF, et al. Soluble CD146, a new
endothelial biomarker of acutely decompensated heart failure. Int J Cardiol. 2015;199:241-7.
24. Kubena P, Arrigo M, Parenica J, Gayat E, Sadoune M, Ganovska E, et al. Plasma Levels of
Soluble CD146 Reflect the Severity of Pulmonary Congestion Better Than Brain Natriuretic Peptide in
Acute Coronary Syndrome. Ann Lab Med. 2016;36(4):300-5.
25. Arrigo M, Truong QA, Onat D, Szymonifka J, Gayat E, Tolppanen H, et al. Soluble CD146 Is a
Novel Marker of Systemic Congestion in Heart Failure Patients: An Experimental Mechanistic and
Transcardiac Clinical Study. Clin Chem. 2017;63(1):386-93.
26. Pusceddu I, Dieplinger B, Mueller T. ST2 and the ST2/IL-33 signalling pathway-biochemistry
and pathophysiology in animal models and humans. Clin Chim Acta. 2019;495:493-500.
27. Vianello E, Dozio E, Tacchini L, Frati L, Corsi Romanelli MM. ST2/IL-33 signaling in cardiac
fibrosis. Int J Biochem Cell Biol. 2019;116:105619.
28. Weinberg EO, Shimpo M, Hurwitz S, Tominaga S, Rouleau JL, Lee RT. Identification of serum
soluble ST2 receptor as a novel heart failure biomarker. Circulation. 2003;107(5):721-6.
29. van Vark LC, Lesman-Leegte I, Baart SJ, Postmus D, Pinto YM, Orsel JG, et al. Prognostic Value
of Serial ST2 Measurements in Patients With Acute Heart Failure. J Am Coll Cardiol.
2017;70(19):2378-88.
30. Aimo A, Vergaro G, Passino C, Ripoli A, Ky B, Miller WL, et al. Prognostic Value of Soluble
Suppression of Tumorigenicity-2 in Chronic Heart Failure: A Meta-Analysis. JACC Heart Fail.
2017;5(4):280-6.
31. Ky B, French B, McCloskey K, Rame JE, McIntosh E, Shahi P, et al. High-sensitivity ST2 for
prediction of adverse outcomes in chronic heart failure. Circ Heart Fail. 2011;4(2):180-7.
32. Gaggin HK, Szymonifka J, Bhardwaj A, Belcher A, De Berardinis B, Motiwala S, et al. Head-to-
head comparison of serial soluble ST2, growth differentiation factor-15, and highly-sensitive troponin
T measurements in patients with chronic heart failure. JACC Heart Fail. 2014;2(1):65-72.
33. Anand IS, Rector TS, Kuskowski M, Snider J, Cohn JN. Prognostic value of soluble ST2 in the
Valsartan Heart Failure Trial. Circ Heart Fail. 2014;7(3):418-26.
34. Rossi A, Gheorghiade M, Triposkiadis F, Solomon SD, Pieske B, Butler J. Left atrium in heart
failure with preserved ejection fraction: structure, function, and significance. Circ Heart Fail.
2014;7(6):1042-9.
35. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS
Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-91.
36. Faletra F, Pezzano A, Jr., Fusco R, Mantero A, Corno R, Crivellaro W, et al. Measurement of
mitral valve area in mitral stenosis: four echocardiographic methods compared with direct
measurement of anatomic orifices. J Am Coll Cardiol. 1996;28(5):1190-7.
37. Nunes MC, Tan TC, Elmariah S, do Lago R, Margey R, Cruz-Gonzalez I, et al. The echo score
revisited: Impact of incorporating commissural morphology and leaflet displacement to the
110
prediction of outcome for patients undergoing percutaneous mitral valvuloplasty. Circulation.
2014;129(8):886-95.
38. Chandrashekhar Y, Westaby S, Narula J. Mitral stenosis. Lancet. 2009;374(9697):1271-83.
39. Herrmann HC, Feldman T, Isner JM, Bashore T, Holmes DR, Jr., Rothbaum DA, et al.
Comparison of results of percutaneous balloon valvuloplasty in patients with mild and moderate
mitral stenosis to those with severe mitral stenosis. The North American Inoue Balloon Investigators.
Am J Cardiol. 1993;71(15):1300-3.
40. Inoue K. Percutaneous transvenous mitral commissurotomy using the Inoue balloon. Eur
Heart J. 1991;12 Suppl B:99-108.
41. Inoue K, Feldman T. Percutaneous transvenous mitral commissurotomy using the Inoue
balloon catheter. Cathet Cardiovasc Diagn. 1993;28(2):119-25.
42. Tuzcu EM, Block PC, Griffin BP, Newell JB, Palacios IF. Immediate and long-term outcome of
percutaneous mitral valvotomy in patients 65 years and older. Circulation. 1992;85(3):963-71.
43. Allan V, Honarbakhsh S, Casas JP, Wallace J, Hunter R, Schilling R, et al. Are cardiovascular risk
factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis
of 23 factors in 32 population-based cohorts of 20 million participants. Thromb Haemost.
2017;117(5):837-50.
44. Aune D, Feng T, Schlesinger S, Janszky I, Norat T, Riboli E. Diabetes mellitus, blood glucose
and the risk of atrial fibrillation: A systematic review and meta-analysis of cohort studies. J Diabetes
Complications. 2018;32(5):501-11.
45. Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. Heart
Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association.
Circulation. 2019;139(10):e56-e528.
46. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC
Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the
European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42(5):373-498.
47. Zöller B, Ohlsson H, Sundquist J, Sundquist K. High familial risk of atrial fibrillation/atrial
flutter in multiplex families: a nationwide family study in Sweden. J Am Heart Assoc.
2012;2(1):e003384.
48. Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous
initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med.
1998;339(10):659-66.
49. Iwasaki YK, Nishida K, Kato T, Nattel S. Atrial fibrillation pathophysiology: implications for
management. Circulation. 2011;124(20):2264-74.
50. Wakili R, Voigt N, Kääb S, Dobrev D, Nattel S. Recent advances in the molecular
pathophysiology of atrial fibrillation. J Clin Invest. 2011;121(8):2955-68.
51. Allessie MA, Boyden PA, Camm AJ, Kléber AG, Lab MJ, Legato MJ, et al. Pathophysiology and
prevention of atrial fibrillation. Circulation. 2001;103(5):769-77.
52. Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial
fibrillation: a translational appraisal. Physiol Rev. 2011;91(1):265-325.
53. Nattel S, Burstein B, Dobrev D. Atrial remodeling and atrial fibrillation: mechanisms and
implications. Circ Arrhythm Electrophysiol. 2008;1(1):62-73.
54. Shiroshita-Takeshita A, Mitamura H, Ogawa S, Nattel S. Rate-dependence of atrial
tachycardia effects on atrial refractoriness and atrial fibrillation maintenance. Cardiovasc Res.
2009;81(1):90-7.
55. Begg GA, Holden AV, Lip GY, Plein S, Tayebjee MH. Assessment of atrial fibrosis for the
rhythm control of atrial fibrillation. Int J Cardiol. 2016;220:155-61.
56. Gal P, Marrouche NF. Magnetic resonance imaging of atrial fibrosis: redefining atrial
fibrillation to a syndrome. Eur Heart J. 2017;38(1):14-9.
57. Lau DH, Linz D, Schotten U, Mahajan R, Sanders P, Kalman JM. Pathophysiology of
Paroxysmal and Persistent Atrial Fibrillation: Rotors, Foci and Fibrosis. Heart Lung Circ.
2017;26(9):887-93.
111
58. Dzeshka MS, Lip GY, Snezhitskiy V, Shantsila E. Cardiac Fibrosis in Patients With Atrial
Fibrillation: Mechanisms and Clinical Implications. J Am Coll Cardiol. 2015;66(8):943-59.
59. Shinagawa K, Shi YF, Tardif JC, Leung TK, Nattel S. Dynamic nature of atrial fibrillation
substrate during development and reversal of heart failure in dogs. Circulation. 2002;105(22):2672-8.
60. Yue L, Xie J, Nattel S. Molecular determinants of cardiac fibroblast electrical function and
therapeutic implications for atrial fibrillation. Cardiovasc Res. 2011;89(4):744-53.
61. Burstein B, Comtois P, Michael G, Nishida K, Villeneuve L, Yeh YH, et al. Changes in connexin
expression and the atrial fibrillation substrate in congestive heart failure. Circ Res.
2009;105(12):1213-22.
62. Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, et al. 2017
HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of
atrial fibrillation. Europace. 2018;20(1):e1-e160.
63. Coppens M, Eikelboom JW, Hart RG, Yusuf S, Lip GY, Dorian P, et al. The CHA2DS2-VASc score
identifies those patients with atrial fibrillation and a CHADS2 score of 1 who are unlikely to benefit
from oral anticoagulant therapy. Eur Heart J. 2013;34(3):170-6.
64. Lip GY, Frison L, Halperin JL, Lane DA. Identifying patients at high risk for stroke despite
anticoagulation: a comparison of contemporary stroke risk stratification schemes in an
anticoagulated atrial fibrillation cohort. Stroke. 2010;41(12):2731-8.
65. Melgaard L, Gorst-Rasmussen A, Lane DA, Rasmussen LH, Larsen TB, Lip GY. Assessment of
the CHA2DS2-VASc Score in Predicting Ischemic Stroke, Thromboembolism, and Death in Patients
With Heart Failure With and Without Atrial Fibrillation. Jama. 2015;314(10):1030-8.
66. Kirchhof P, Camm AJ, Goette A, Brandes A, Eckardt L, Elvan A, et al. Early Rhythm-Control
Therapy in Patients with Atrial Fibrillation. N Engl J Med. 2020;383(14):1305-16.
67. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for
the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J.
2016;37(38):2893-962.
68. Cosedis Nielsen J, Johannessen A, Raatikainen P, Hindricks G, Walfridsson H, Kongstad O, et
al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med.
2012;367(17):1587-95.
69. Marrouche NF, Brachmann J, Andresen D, Siebels J, Boersma L, Jordaens L, et al. Catheter
Ablation for Atrial Fibrillation with Heart Failure. N Engl J Med. 2018;378(5):417-27.
70. Di Biase L, Mohanty P, Mohanty S, Santangeli P, Trivedi C, Lakkireddy D, et al. Ablation Versus
Amiodarone for Treatment of Persistent Atrial Fibrillation in Patients With Congestive Heart Failure
and an Implanted Device: Results From the AATAC Multicenter Randomized Trial. Circulation.
2016;133(17):1637-44.
71. Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE, et al. Effect of Catheter
Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among
Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. Jama. 2019;321(13):1261-74.
72. Jaïs P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, et al. Catheter ablation versus
antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation. 2008;118(24):2498-505.
73. Asad ZUA, Yousif A, Khan MS, Al-Khatib SM, Stavrakis S. Catheter Ablation Versus Medical
Therapy for Atrial Fibrillation: A Systematic Review and Meta-Analysis of Randomized Controlled
Trials. Circ Arrhythm Electrophysiol. 2019;12(9):e007414.
74. Kuck KH, Brugada J, Fürnkranz A, Metzner A, Ouyang F, Chun KR, et al. Cryoballoon or
Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N Engl J Med. 2016;374(23):2235-45.
75. Dukkipati SR, Neuzil P, Kautzner J, Petru J, Wichterle D, Skoda J, et al. The durability of
pulmonary vein isolation using the visually guided laser balloon catheter: multicenter results of
pulmonary vein remapping studies. Heart Rhythm. 2012;9(6):919-25.
76. Dukkipati SR, Cuoco F, Kutinsky I, Aryana A, Bahnson TD, Lakkireddy D, et al. Pulmonary Vein
Isolation Using the Visually Guided Laser Balloon: A Prospective, Multicenter, and Randomized
Comparison to Standard Radiofrequency Ablation. J Am Coll Cardiol. 2015;66(12):1350-60.
112
77. Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter
ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812-22.
78. Valderrábano M, Peterson LE, Swarup V, Schurmann PA, Makkar A, Doshi RN, et al. Effect of
Catheter Ablation With Vein of Marshall Ethanol Infusion vs Catheter Ablation Alone on Persistent
Atrial Fibrillation: The VENUS Randomized Clinical Trial. Jama. 2020;324(16):1620-8.
79. Lam A, Denis A, Pambrun T, Duchateau J, Jais P, Derval N. How we met the vein of Marshall in
the mirror. Europace. 2019;21(12):1842.
80. Derval N, Duchateau J, Denis A, Ramirez FD, Mahida S, André C, et al. Marshall bundle
elimination, Pulmonary vein isolation, and Line completion for ANatomical ablation of persistent
atrial fibrillation (Marshall-PLAN): Prospective, single-center study. Heart Rhythm. 2020.
81. Pambrun T, Denis A, Duchateau J, Sacher F, Hocini M, Jaïs P, et al. MARSHALL bundles
elimination, Pulmonary veins isolation and Lines completion for ANatomical ablation of persistent
atrial fibrillation: MARSHALL-PLAN case series. J Cardiovasc Electrophysiol. 2019;30(1):7-15.
82. Braunwald E. Heart failure. JACC Heart Fail. 2013;1(1):1-20.
83. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, et al. A prospective
survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart
Disease. Eur Heart J. 2003;24(13):1231-43.
84. Morillo CA, Verma A, Connolly SJ, Kuck KH, Nair GM, Champagne J, et al. Radiofrequency
ablation vs antiarrhythmic drugs as first-line treatment of paroxysmal atrial fibrillation (RAAFT-2): a
randomized trial. Jama. 2014;311(7):692-700.
85. Hakalahti A, Biancari F, Nielsen JC, Raatikainen MJ. Radiofrequency ablation vs.
antiarrhythmic drug therapy as first line treatment of symptomatic atrial fibrillation: systematic
review and meta-analysis. Europace. 2015;17(3):370-8.
86. Ishikura F, Nagata S, Hirata Y, Kimura K, Nakatani S, Tamai J, et al. Rapid reduction of plasma
atrial natriuretic peptide levels during percutaneous transvenous mitral commissurotomy in patients
with mitral stenosis. Circulation. 1989;79(1):47-50.
87. Nakamura M, Kawata Y, Yoshida H, Arakawa N, Koeda T, Ichikawa T, et al. Relationship
between plasma atrial and brain natriuretic peptide concentration and hemodynamic parameters
during percutaneous transvenous mitral valvulotomy in patients with mitral stenosis. Am Heart J.
1992;124(5):1283-8.
88. Sacher F, Corcuff JB, Schraub P, Le Bouffos V, Georges A, Jones SO, et al. Chronic atrial
fibrillation ablation impact on endocrine and mechanical cardiac functions. Eur Heart J.
2008;29(10):1290-5.
89. Charitakis E, Karlsson LO, Papageorgiou JM, Walfridsson U, Carlhäll CJ. Echocardiographic and
Biochemical Factors Predicting Arrhythmia Recurrence After Catheter Ablation of Atrial Fibrillation-
An Observational Study. Front Physiol. 2019;10:1215.
90. Bakkestrøm R, Andersen MJ, Ersbøll M, Bro-Jeppesen J, Gustafsson F, Køber L, et al. Early
changes in left atrial volume after acute myocardial infarction. Relation to invasive hemodynamics at
rest and during exercise. Int J Cardiol. 2016;223:717-22.
91. Hofer F, Hammer A, Steininger M, Kazem N, Koller L, Steinlechner B, et al. The Prognostic
Potential of Atrial Natriuretic Peptide on the Development of Post-Operative Atrial Fibrillation after
Cardiac Surgery. Thromb Haemost. 2021.
92. Kaufmann CC, Ahmed A, Kassem M, Freynhofer MK, Jäger B, Aicher G, et al. Mid-regional
pro-atrial natriuretic peptide independently predicts short-term mortality in COVID-19. Eur J Clin
Invest. 2021:e13531.
93. Putko BN, Savu A, Kaul P, Ezekowitz J, Dyck JR, Anderson TJ, et al. Left atrial remodelling, mid-
regional pro-atrial natriuretic peptide, and prognosis across a range of ejection fractions in heart
failure. Eur Heart J Cardiovasc Imaging. 2021;22(2):220-8.
94. Wang D, Duan H, Feng J, Xiang J, Feng L, Liu D, et al. Soluble CD146, a cerebrospinal fluid
marker for neuroinflammation, promotes blood-brain barrier dysfunction. Theranostics.
2020;10(1):231-46.
113
95. Stalin J, Traboulsi W, Vivancos-Stalin L, Nollet M, Joshkon A, Bachelier R, et al. Therapeutic
targeting of soluble CD146/MCAM with the M2J-1 monoclonal antibody prevents metastasis
development and procoagulant activity in CD146-positive invasive tumors. Int J Cancer.
2020;147(6):1666-79.
96. Li X, Wen J, Dong Y, Zhang Q, Guan J, Liu F, et al. Wnt5a promotes renal tubular inflammation
in diabetic nephropathy by binding to CD146 through noncanonical Wnt signaling. Cell Death Dis.
2021;12(1):92.
97. Liu H, Wang K, Lin Y, Liang X, Zhao S, Li M, et al. Role of sST2 in predicting recurrence of atrial
fibrillation after radiofrequency catheter ablation. Pacing Clin Electrophysiol. 2020;43(11):1235-41.
98. Wang Z, Cheng L, Zhang J, Liang Z, Dong R, Hang F, et al. Serum-Soluble ST2 Is a Novel
Biomarker for Evaluating Left Atrial Low-Voltage Zone in Paroxysmal Atrial Fibrillation. Med Sci
Monit. 2020;26:e926221.
99. Okar S, Kaypakli O, Şahin DY, Koç M. Fibrosis Marker Soluble ST2 Predicts Atrial Fibrillation Recurrence after Cryoballoon Catheter Ablation of Nonvalvular Paroxysmal Atrial Fibrillation. Korean
Circ J. 2018;48(10):920-9.
100. Chen C, Qu X, Gao Z, Zheng G, Wang Y, Chen X, et al. Soluble ST2 in Patients with Nonvalvular
Atrial Fibrillation and Prediction of Heart Failure. Int Heart J. 2018;59(1):58-63.
101. Lamprea-Montealegre JA, Zelnick LR, Shlipak MG, Floyd JS, Anderson AH, He J, et al. Cardiac
Biomarkers and Risk of Atrial Fibrillation in Chronic Kidney Disease: The CRIC Study. J Am Heart Assoc.
2019;8(15):e012200.
102. Zeng Z, Hong XY, Li Y, Chen W, Ye G, Li Y, et al. Serum-soluble ST2 as a novel biomarker
reflecting inflammatory status and illness severity in patients with COVID-19. Biomark Med.
2020;14(17):1619-29.

Titre : Etude de biomarqueurs de dysfonction atriale.
Mots clés : biomarqueurs, dysfonction atriale, fibrillation atriale, sténose mitrale, MRproANP, sCD146
Résumé : La pratique de la cardiologie fait appel de façon quotidienne à l’utilisation de biomarqueurs. Cependant dans les pathologies à atteinte atriale prédominante, la performance diagnostique et pronostique des biomarqueurs classiquement utilisés est peu démontrée. Nous nous sommes donc intéressés à l’intérêt potentiel de trois biomarqueurs dans des pathologies affectant en premier lieu l’oreillette : la fibrillation atriale (FA) et la sténose mitrale. Les biomarqueurs concernés sont le MRproANP un peptide d’origine atriale, le sCD146 un marqueur d’origine endothéliale et le sST2 un marqueur de fibrose. L’objectif de ce travail était l’évaluation de leurs capacités diagnostiques et pronostiques chez des patients atteints de FA et de sténose mitrale. Dans la première publication (1) il était mis en évidence que le MRproANP, le sCD146 et le sST2 permettaient de discriminer une origine cardiaque congestive chez des patients consultant pour dyspnée. Seuls les taux de MRproANP et sCD146 étaient liés à la dilatation atriale, suggérant l’intérêt potentiel de ces biomarqueurs dans des pathologies avec atteinte atriale. Nous avons évalué dans une seconde publication (2) les concentrations plasmatiques de MRproANP et de sCD146 chez des patients porteurs de sténoses mitrales serrées et moyennement serrées. Les concentrations de ces deux biomarqueurs étaient toutes deux plus élevées chez les patients porteurs de sténoses mitrales serrées en comparaison à ceux ayant des sténoses moyennement serrées. La troisième publication (3) fait suite à cette seconde étude. Elle a évalué les concentrations de MRproANP, sCD146, BNP et NTproBNP, en pré et post commissurotomie mitrale percutanée (CMP). Les taux initiaux de BNP, MRproANP, et sCD146 étaient significativement abaissés en post CMP. Il n’existait pas de baisse significative de ces biomarqueurs si les critères de succès de la CMP n’étaient pas remplis. Cette baisse semble donc refléter l’amélioration hémodynamique induite par une procédure réalisée
avec succès, conférant au MRproANP et au sCD146 le rôle de marqueurs de succès d’une CMP. L’ensemble de ces résultats concernant le sCD146 s’explique par sa libération au niveau de l’endothélium de la circulation pulmonaire en réponse à la congestion induite par le rétrécissement mitral. Les résultats concernant le MRproANP sont expliqués par une libération conditionnée par la pression intra atriale gauche chez les patients porteurs de sténose mitrale. A l’issu de ces 3 premières études, nous pouvons conclure que les taux de MRproANP et de sCD146 sont des marqueurs de sévérité de la sténose mitrale et du résultat de son traitement percutané. Nous nous sommes enfin focalisés sur l’étude de ces biomarqueurs chez les patients en FA (4). L’ablation de FA est au cœur de la prise en charge de cette pathologie. L’identification des patients à risque de récidive post ablation est primordiale. Nous nous sommes ainsi intéressés à l’impact des niveaux plasmatiques de MRproANP et de sST2 avant une ablation sur le taux de récidive à un an. Le MRproANP était un prédicteur indépendant de récidive de fibrillation atriale dans notre étude, le sST2 ne l’était pas. Un MRproANP au-delà d’un seuil de 107.9pmol/L était lié à un risque de récidive de FA multiplié par 25. Inversement en dessous de ce seuil le risque de récidive à un an était de 4,2% avec une valeur prédictive négative très élevée de 95.7%. Dans cette même étude les concentrations pré-ablation de MRproANP étaient plus élevées chez les patients en fibrillation qu’en rythme sinusal, et plus élevées dans les oreillettes que dans le sang veineux périphérique. Ces données sont en faveur d’une sécrétion atriale du MRproANP chez les patients en fibrillation. Nous avons par ce travail pu montrer l’intérêt du MRproANP, du sCD146 et du sST2 pour le pronostic, le diagnostic de sévérité et le suivi des patients atteints de sténose mitrale ou de FA.
Title : Atrial dysfunction biomarkers.
Keywords : biomarkers, atrial dysfonction, atrial fibrillation, mitral stenosis, MRproANP, sCD146
Abstract : The assessment of biomarkers has become an integral part of the daily practice of cardiology. However, in diseases affecting primarily the atria, the diagnostic and prognostic role of widely used biomarkers is less well documented. Thus, we investigated the potential utility of 3 biomarkers in diseases affecting primarily the atrium, namely atrial fibrillation (AF) and mitral stenosis. The biomarkers investigated were MRproANP, a natriuretic peptide of atrial origin; sCD146, a biomarker of endothelial origin; and sST2, a marker of fibrosis. The aim of this work was to evaluate the diagnostic and prognostic capacities of these biomarkers in patients with AF or mitral stenosis. The first publication (1) investigated the performance of several biomarkers in patients consulting for dyspnea. In this context, MRproANP, sCD146 and sST2 made it possible to identify the cardiac origin of the dyspnea. In this study, only MRproANP and sCD146 levels were found to be associated with right and left atrial dilation. This suggested the potential interest of these biomarkers in pathologies affecting the atria. In a second publication (2), we assessed plasma concentrations of MRproANP and sCD146 in patients with moderate to severe mitral stenosis. Both biomarkers were significantly higher in patients with severe mitral stenosis compared to those with moderate mitral stenosis. The third publication (3) followed up on this theme by investigation the concentrations of MRproANP, sCD146, BNP and NTproBNP before and after percutaneous mitral commissurotomy (PMC). MR-proANP and plasma sCD146 were shown to decrease significantly immediately after PMC. Of note, in this study, the significant changes in biomarker levels were observed mainly in patients in whom the PMC procedure was judged successful. The decrease in these biomarkers therefore seems to reflect the improvement in hemodynamics induced by the successful procedure, making MRproANP and sCD146 adequate markers of procedural success after PMC.
Taken together, the results observed with sCD146 can be explained by the fact that it is released by the endothelium in the pulmonary circulation in response to congestion caused by mitral stenosis. A possible explanation for our findings regarding MRproANP is that its release is conditioned by left intra-atrial pressure in patients with mitral stenosis. After these three studies, we can conclude that MRproANP and sCD146 are markers of the severity of mitral stenosis, and of the success of PMC. Subsequently, we went on to investigate the utility of these biomarkers in patients with AF (4). Catheter ablation is currently the cornerstone of AF therapy. The main limitation of catheter ablation of AF is the success rate of the procedure, which ranges between 50 and 80%. There is a strong need to identify patients at risk of recurrence after catheter ablation. To this end, we investigated the impact of pre-procedural plasma levels of MRproANP and sST2 on the rate of AF recurrence at 1 year after catheter ablation. We found that MRproANP was an independent predictor of recurrence in our study, whereas sST2 was not. An MRproANP levels above a threshold of 107.9pmol/L was found to be associated with a 25-fold increase in the risk of AF recurrence. Conversely, patients with values below the threshold had a recurrence rate of 4.2%, with a high negative predictive value, at 95.7%. In this study, we also observed that pre-procedural rates of MRproANP were highest in patients in AF, compared to those in sinus rhythm. Concentrations did not significantly differ between the right and left atria, but intra-atrial concentrations were significantly higher than those observed in the peripheral blood. These data plead in favour of the atrial release of MRproANP in patients in AF. We demonstrated the utility of MRproANP, sCD146 and sST2for prognosis, diagnosis of severity, and follow-up of patients with mitral stenosis or AF.
Université Bourgogne Franche-Comté
32, avenue de l’Observatoire
25000 Besançon




















