Eradicating Helicobacter pylori in non-ulcer dyspepsia may not be cost effective
10
Not again! See pp 501, 517, 562, 563 Designing safer medical devices requires financial and political support Editor—Berwick emphasises the need to redesign medical devices to help avoid errors. 1 In the European Union a task group from the European Standards Organisation (CEN) reported on ways to reduce the incidents of accidental misconnection of lines to patients. 2 It identified a need to differentiate between connectors used in lines and syringes for enteral feeding, vascu- lar access, and administering and sampling gases in the respiratory system, including a risk analysis of the results of misconnection. The report was not welcomed by EUCOMED, which represents several Euro- pean medical device manufacturers, because its proposals create more hazards for users and increase costs in a highly competitive sector of the medical device industry with high volume, low cost products. The Japanese government changed the design of connectors on syringes and enteral feed sys- tems in less than a year because of an associ- ated death, but none of the standards bodies in the European Union has so far volun- teered to develop new standards for connec- tor systems, as recommended by the task group. Central funding from the European Commission has been sought, but the work is effectively now on hold. Many non-interchangeable keyed con- nectors are manufactured, mostly for spe- cialised applications. Those that are not patented are freely available and could be fitted on to hypodermic syringes and lines, allowing differentiation of line or syringe by function—for example, respiratory, vascular, enteral, or neuraxial. A separate key for intrathecal needle and syringes is possible and would require the drugs to be supplied by the pharmacist in a specialised syringe. At least one connector system incorporates an anti-tamper lock, preventing unintended disconnection. Differentiation of connector is one prompt to increase safety, differentia- tion by size and shape of the drug container is another. Thus intravenous drug infusions should always be supplied with an intra- venous giving set pre-attached, and intrathe- cal drugs with a spinal needle. However, unless all access points are sealed off, drugs in an intravenous bag could be accessed by even a specialised intrathecal needle and syringe. Currently, medical hypodermic syringes have only one permitted type of connector in two types. 34 Since medical hypodermic syringes and lines are ubiquitous, the task of developing a global standard for a series of non-interchangeable connector systems for syringes and small bore tubing is daunting. Not having the correct type of syringe avail- able in an emergency would create its own hazards. Clearly, any new designs would need to be widely tested, a task meriting a multidisciplinary approach, with support from technical, psychological, and risk analysis experts. The Department of Health has promoted the reduction of accidents 5 and could take the lead here. Financial and political support, from both the medical profession and government, is urgently needed. Philip J Bickford Smith consultant anaesthetist Anaesthetic Department, Bradford Hospitals NHS Trust,West Yorkshire BD9 6RJ [email protected] PJBS is the clinical expert from the United Kingdom on the CEN Forum Task Group,“Luer Connectors.” 1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.) 2 CEN Forum Task Group,“Luer Fittings.” Luer connectors—a report to CEN. London: British Standards Institution, 2000. (PD CR13825:2000.) 3 British Standards Institution. Conical fittings with 6% (Luer) taper for syringes, needles and certain other medical equipment. Part 1. General requirements. London: BSI, 1994. (BS EN 20594-1:1994.) 4 British Standards Institution. Conical fittings with 6% (Luer) taper for syringes, needles and certain other medical equipment— lock fittings. London: BSI, 1997. (BS EN 1707:1997.) 5 Department of Health. An organisation with a memory; report of the expert group on learning from adverse events in the NHS chaired by the chief medical officer. London: Stationery Office, 2000. Erroneous intrathecal injection results from a problem with protocols Editor—The erroneous intrathecal admin- istration of vincristine to 13 patients (many of them children) in 15 years is not just a problem arising from inadequate time, training, and supervision of medical staff; neither can it be confidently prevented by modifying the equipment used. 1 Though I have not had access to the various investiga- tions, I am confident that most of the vincristine given had been labelled correctly and been prescribed for intravenous use in the patients who received it intrathecally. The accidents all occurred for the simple reason that the national protocols for treatment of childhood acute lymphoblastic leukaemia and the various derived regimens for adult leukaemia and lymphoma require that intrathecal methotrexate and intra- venous vincristine be given on the same day. This is particularly convenient for patients and their families and carers, but the result- ing 10 deaths and three cases of paralysis ought to prompt a review by the bodies issu- ing the protocols (the Medical Research Council and others). I know of no pharmacological reason why these two agents have to be given together, whether they are being given to induce remission or as maintenance treat- ment. The repeated disasters, despite the problem being well recognised by all those (senior and otherwise) involved in intrathe- cal treatment, surely point to the need to design the problem out of the system: give the intrathecal drugs on a separate visit to the intravenous ones. Local protocols speci- fying the use of the agents in separate rooms are not failsafe and not necessarily applica- ble or enforceable in every institution. J R C Seale consultant haematologist Ysbyty Gwynedd, Bangor LL57 2PW [email protected] 1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.) National guidelines are urgently needed Editor—Berwick rightly points out that mechanisms are needed to prevent trag- edies such as the erroneous intrathecal injection of vincristine from happening. 1 With the changes in cancer management after the Calman-Hine report, this issue Advice to authors We prefer to receive all responses electronically, sent either directly to our website or to the editorial office as email or on a disk. Processing your letter will be delayed unless it arrives in an electronic form. We are now posting all direct submissions to our website within 24 hours of receipt and our intention is to post all other electronic submissions there as well. All responses will be eligible for publication in the paper journal. Responses should be under 400 words and relate to articles published in the preceding month. They should include <5 references, in the Vancouver style,including one to the BMJ article to which they relate.We welcome illustrations. Please supply each author’s current appointment and full address, and a phone or fax number or email address for the corresponding author.We ask authors to declare any competing interest. Please send a stamped addressed envelope if you would like to know whether your letter has been accepted or rejected. Letters will be edited and may be shortened. bmj.com [email protected] Letters Website: bmj.com Email: [email protected] 548 BMJ VOLUME 322 3 MARCH 2001 bmj.com
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Eradicating Helicobacter pylori in non-ulcer dyspepsia may not be cost effective

Not again! See pp 501, 517, 562, 563
Designing safer medical devices requiresfinancial and political support
Editor—Berwick emphasises the need toredesign medical devices to help avoiderrors.1 In the European Union a task groupfrom the European Standards Organisation(CEN) reported on ways to reduce theincidents of accidental misconnection oflines to patients.2 It identified a need todifferentiate between connectors used inlines and syringes for enteral feeding, vascu-lar access, and administering and samplinggases in the respiratory system, including arisk analysis of the results of misconnection.
The report was not welcomed byEUCOMED, which represents several Euro-pean medical device manufacturers, becauseits proposals create more hazards for usersand increase costs in a highly competitivesector of the medical device industry withhigh volume, low cost products. TheJapanese government changed the design ofconnectors on syringes and enteral feed sys-tems in less than a year because of an associ-ated death, but none of the standards bodiesin the European Union has so far volun-teered to develop new standards for connec-tor systems, as recommended by the task
group. Central funding from the EuropeanCommission has been sought, but the workis effectively now on hold.
Many non-interchangeable keyed con-nectors are manufactured, mostly for spe-cialised applications. Those that are notpatented are freely available and could befitted on to hypodermic syringes and lines,allowing differentiation of line or syringe byfunction—for example, respiratory, vascular,enteral, or neuraxial. A separate key forintrathecal needle and syringes is possibleand would require the drugs to be suppliedby the pharmacist in a specialised syringe. Atleast one connector system incorporates ananti-tamper lock, preventing unintendeddisconnection. Differentiation of connectoris one prompt to increase safety, differentia-tion by size and shape of the drug containeris another. Thus intravenous drug infusionsshould always be supplied with an intra-venous giving set pre-attached, and intrathe-cal drugs with a spinal needle. However,unless all access points are sealed off, drugsin an intravenous bag could be accessed byeven a specialised intrathecal needle andsyringe.
Currently, medical hypodermic syringeshave only one permitted type of connectorin two types.3 4 Since medical hypodermicsyringes and lines are ubiquitous, the task ofdeveloping a global standard for a series ofnon-interchangeable connector systems forsyringes and small bore tubing is daunting.Not having the correct type of syringe avail-able in an emergency would create its ownhazards. Clearly, any new designs wouldneed to be widely tested, a task meriting amultidisciplinary approach, with supportfrom technical, psychological, and riskanalysis experts. The Department of Healthhas promoted the reduction of accidents5
and could take the lead here. Financial andpolitical support, from both the medicalprofession and government, is urgentlyneeded.Philip J Bickford Smith consultant anaesthetistAnaesthetic Department, Bradford Hospitals NHSTrust, West Yorkshire BD9 [email protected]
PJBS is the clinical expert from the United Kingdomon the CEN Forum Task Group, “Luer Connectors.”
1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.)2 CEN Forum Task Group, “Luer Fittings.” Luer connectors—a
report to CEN. London: British Standards Institution, 2000.(PD CR13825:2000.)
3 British Standards Institution. Conical fittings with 6% (Luer)taper for syringes, needles and certain other medical equipment.
Part 1. General requirements. London: BSI, 1994. (BS EN20594-1:1994.)
4 British Standards Institution. Conical fittings with 6% (Luer)taper for syringes, needles and certain other medical equipment—lock fittings. London: BSI, 1997. (BS EN 1707:1997.)
5 Department of Health. An organisation with a memory; reportof the expert group on learning from adverse events in the NHSchaired by the chief medical officer. London: Stationery Office,2000.
Erroneous intrathecal injection resultsfrom a problem with protocols
Editor—The erroneous intrathecal admin-istration of vincristine to 13 patients (manyof them children) in 15 years is not just aproblem arising from inadequate time,training, and supervision of medical staff;neither can it be confidently prevented bymodifying the equipment used.1 Though Ihave not had access to the various investiga-tions, I am confident that most of thevincristine given had been labelled correctlyand been prescribed for intravenous use inthe patients who received it intrathecally.
The accidents all occurred for the simplereason that the national protocols fortreatment of childhood acute lymphoblasticleukaemia and the various derived regimensfor adult leukaemia and lymphoma requirethat intrathecal methotrexate and intra-venous vincristine be given on the same day.This is particularly convenient for patientsand their families and carers, but the result-ing 10 deaths and three cases of paralysisought to prompt a review by the bodies issu-ing the protocols (the Medical ResearchCouncil and others).
I know of no pharmacological reasonwhy these two agents have to be giventogether, whether they are being given toinduce remission or as maintenance treat-ment. The repeated disasters, despite theproblem being well recognised by all those(senior and otherwise) involved in intrathe-cal treatment, surely point to the need todesign the problem out of the system: givethe intrathecal drugs on a separate visit tothe intravenous ones. Local protocols speci-fying the use of the agents in separate roomsare not failsafe and not necessarily applica-ble or enforceable in every institution.J R C Seale consultant haematologistYsbyty Gwynedd, Bangor LL57 [email protected]
1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.)
National guidelines are urgently needed
Editor—Berwick rightly points out thatmechanisms are needed to prevent trag-edies such as the erroneous intrathecalinjection of vincristine from happening.1
With the changes in cancer managementafter the Calman-Hine report, this issue
Advice to authorsWe prefer to receive all responses electronically,sent either directly to our website or to theeditorial office as email or on a disk. Processingyour letter will be delayed unless it arrives in anelectronic form.
We are now posting all direct submissions toour website within 24 hours of receipt and ourintention is to post all other electronicsubmissions there as well. All responses will beeligible for publication in the paper journal.
Responses should be under 400 words andrelate to articles published in the precedingmonth. They should include <5 references, in theVancouver style, including one to the BMJ articleto which they relate. We welcome illustrations.
Please supply each author’s currentappointment and full address, and a phone orfax number or email address for thecorresponding author. We ask authors to declareany competing interest. Please send a stampedaddressed envelope if you would like to knowwhether your letter has been accepted or rejected.
Letters will be edited and may be shortened.
Letters
Website: bmj.comEmail: [email protected]
548 BMJ VOLUME 322 3 MARCH 2001 bmj.com

needs to be urgently looked at andnationally agreed guidance issued.
At Sidcup we have been consciouslyaware of such errors and have for manyyears introduced practical steps to preventthis error from happening. The centralchemotherapy manufacturing unit labelsintrathecal treatments “for intrathecal useonly” and vincristine injections “fatal if givenintrathecally.” The drugs are delivered inseparate envelopes that are clearly markedfor intrathecal or intravenous use. Weseparate the intravenous from the intrathe-cal treatment in that specialist chemo-therapy nurses give the intravenous, andhaematology doctors the intrathecal treat-ments. Intrathecal follows intravenous treat-ment, so vincristine is given first. Mostimportantly, no junior doctor is allowed togive intrathecal treatment without one of thehaematology or oncology consultantssupervising the procedure. The drugs arecollected from the pharmacy by the special-ist chemotherapy nurses and handed to theconsultant or to juniors in the consultant’spresence. The consultant checks the injec-tions with the administering doctor and theelectronic prescription chart is signed byboth.
The problem arises not because of neg-ligence but from lack of experience and lackof seniority. By introducing such steps wenot only protect patients but raise awarenessand highlight to junior doctors the fatal riskthat comes from the simple switching ofsyringes.Saad M B Rassam consultant in haematology andoncologyQueen Mary’s Sidcup NHS Trust, Sidcup, KentDA14 6LT
1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.)
Only ocular treatments should bepackaged like eye drops . . .
Editor—Just as I was penning a letter abouthow medical errors are portrayed in themedia, Berwick has said it all.1 My letter wasnot about a case reported in the Daily Mail,however, but about a case reported in theBMJ.
I stared in disbelief at the picture in Min-erva on 20 January 2001.2 Why would amedical company be allowed to produce abottle of stoma deodorant that so closelymatched a bottle of eye drops? I expectedthe authors to point this out and perhapssuggest that the Medicines Control Agencyhave a system for controlling the packagingof products like these. The agency has, forexample, made strides in the packaging ofparacetamol to reduce suicide rates.1 3
Instead, the authors wrote (and the BMJpublished), “Great care must be taken whenpatients need ocular treatments in additionto other treatments contained in dropperbottles”—as if the staff on the ward somehowdid not try to take great care. Even Berwickreturns his videos to the wrong store: heshould take more care and be less human.
Once again healthcare workers arebeing exhorted to avoid an accident waitingto happen. Furthermore, such an accident is
likely to happen again—on wards, in homes(where patients with poor sight using eyedrops might have problems)—until someonesays that only ocular treatments should everbe put in packages that look like eyedroppers.Tim Wilson general practitionerMill Stream Surgery, Benson, OxfordshireOX10 [email protected]
1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.)2 Wheeler J, Shah P. Minerva picture. BMJ 2001;322:182. (20
January.)3 Robinson D, Smith AMJ, Johnston GD. Severity of
overdose after restriction of paracetamol availability: retro-spective study. BMJ 2000;321:926-7. (14 October.)
. . . and packaging of lignocaine must bechanged
Editor—Further to Berwick’s editorial onthe erroneous intrathecal injection ofvincristine1 and the picture in Minerva in thesame issue on the packaging of lignocaine,2
we report a pertinent incident.In 1994 our risk management depart-
ment was made aware that the containersand boxes containing 0.9% sodium chloride(normal saline) and 1% lignocaine werealmost identical and that these solutionswere being used side by side in the radiologydepartment. The potential for a serious inci-dent of mistakenly administering lignocaineas a flush was identified. No action was taken.
In 1999 a child was administeredlignocaine as a flush during an interven-tional procedure. The child required urgentmedical attention but did not develop longterm adverse effects. The incident was againreported to risk management, but no furtheraction was taken to reduce the risk of recur-rence. In April 2000 the danger of givinglignocaine for normal saline was again high-
lighted at a risk management meeting; noaction was taken.
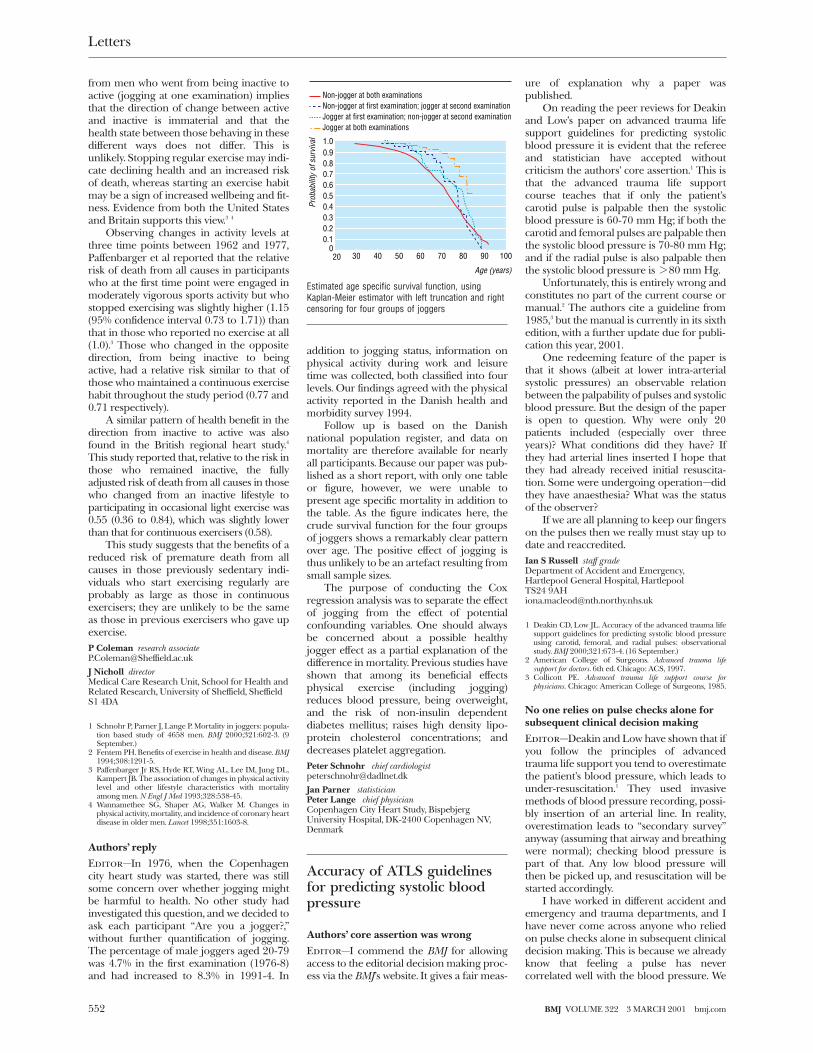
On 31 January 2001 four flushes weredrawn up before computed tomography(figure). Three of the four flushes were 1%lignocaine. This was noted before injectionand a near miss has been recorded andreported to risk management.
With the increasing cost of paymentsmade by the NHS for medical negligence itis time to change the packaging oflignocaine.Anmol Malhotra radiology registrarMathew Matson radiology consultantOtto Chan radiology consultantDepartment of Diagnostic Imaging (Radiology),Royal Hospitals NHS Trust, London E1 1BB
1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.)2 Dawes R, Vanner R. Minerva picture. BMJ 2001;322:308.
(3 February.)
*** Plus ça change. Dr R E Ferner of the WestMidlands Centre for Adverse Drug ReactionReporting, City Hospital NHS Trust, BirminghamB18 7QH, has reminded us that he highlighted theproblem of misleading drug packaging over fiveyears ago (BMJ 1995;311:514). He showed howlabels for lignocaine and normal saline were identi-cal apart from the lettering and suggested thatdiversity could mean the difference between life anddeath.
Patients must be properly informed toagree to or decline treatment
Editor—Obviously errors will always occurin health care.1 Unfortunately, the medicalprofession has traditionally kept quiet aboutthis sad fact of life—and death.
Doctors have considered it inappropri-ate to tell patients that mistakes, let alonetheir consequences, can all too easily occurduring the course of a procedure. Therefore,patients have not had the requisite infor-mation on which to make fully informeddecisions.
The motives for this secrecy have doubt-less been honourable. But the desire to sparepatients the additional trauma of beingreminded that we are all fallible can easilyslide into the suppression of crucial infor-mation about the risks associated with anintervention.
Giving patients all the informationnecessary to agree to or decline treatment,without generating numerous refusals, is thechallenge implicit in a meaningful doctor-patient partnership.Roger M Goss directorPatient Concern, PO Box 23732, London SW5 [email protected]
1 Berwick DM. Not again! BMJ 2001;322:247-8. (3 February.)
Data protection and patients’consent
Informed consent should be soughtbefore data are used by registries
Editor—The news story on the possibilitythat cancer registries might collapse as aresult of new guidance on patient confiden-tiality issued by the General Medical Council
Three of four flushes were 1% lignocaine instead ofnormal saline on 31 January 2001
Letters
549BMJ VOLUME 322 3 MARCH 2001 bmj.com

highlighted the difficulties faced by doctorswho must deal with increasing bureaucracy.1
In conjunction with a multidisciplinary teamfrom different parts of the United KingdomI was involved in establishing a prospectiveregister of pregnant women with epilepsy.Pregnancy in women with epilepsy is associ-ated with an increased risk of fetalmalformation.
As with cancer, there are variations inthe routine treatment of epilepsy in preg-nancy. It would be considered unethical tocarry out a clinical trial of treatment, butbecause many pregnancies occur in womenalready taking a variety of anti-epilepticdrugs (for many of which no reliable data onteratogenicity in humans exists) valuableinformation could become available if onlyit was collated. It was on this premise that theUK Epilepsy and Pregnancy Register wasestablished.
From the outset we identified the needfor confidentiality, and all patients includedin the register give informed consent. Fewpatients have refused or withdrawn consent,and indeed most are delighted that someresearch is being carried out on this subject.Although case ascertainment would prob-ably be higher if informed consent was notnecessary, this is an inevitable trade off madeto maintain patients’ trust.
A further difficulty faced by registries isthat of formal ethical approval. Approvalfor our register was obtained from amulticentre research ethics committee, butthis did not obviate the need to apply toover 200 local research ethics committees.Many of the local committees had idio-syncratic requirements and made idio-syncratic responses to our request. Dealingwith our share of the bureaucracy occupiedthe best part of 12 months and probablycaused the loss of a medium sizedAmazonian rainforest. Thus, we feel thatthis mechanism is an even greater hurdlethan that of confidentiality.
Along with other physicians andpatients, we believe that there is much infor-mation available on the way we managemany conditions if only this informationcould be more easily collated. The infor-mation provided by registries will increaseknowledge and ultimately benefit patients.However, the issue of informed consent andthe bureaucracy surrounding multicentreethical approval needs urgent review.James I Morrow consultant neurologistDepartment of Neurology, Royal Victoria Hospital,Belfast BT12 6BA
1 Brown P. Cancer registries fear imminent collapse. BMJ2000;321:849. (7 October.)
GMC is greater threat to research thanthe act
Editor—Like Strobl et al the NorthStaffordshire Local Research Ethics Com-mittee has been seriously considering dataprotection issues while not wishing toimpede research unnecessarily.1 We wereconcerned about the implications of theData Protection Act. We advised researchersto consider its implications, sought advice
from the data protection commissioner(emailed March 2000, response awaited),and as a last resort actually read the act.2
This is not a task to be undertaken lightly:the language is convoluted and arcane.None the less, section 33 of part IV of the actexempts research from most of the provi-sions of the act; further processing of datafor purposes for which it was not originallycollected (section 33 (2)) and publishing it isallowed provided the data has been anony-mised (section 33 (4)(b)). The transfer ofdata outside the European Union, however,is prohibited (data protection principle 8)unless adequate data protection has beenensured by the country outside the union.This could present difficulties for inter-national multicentre collaborations involv-ing countries outside the European Union.Section 30 (1) allows the secretary of state toorder that health information be exemptedfrom the provisions of the act.
The General Medical Council’s viewthat consent has to be obtained fromparticipants to allow data that is already on aregistry to be processed is a greater threatto epidemiological research than the DataProtection Act.3 We may end up in theridiculous situation in which non-medicalscientists are able to do epidemiologicalwork but registered doctors are not. Therehas to be a considered approach to the needfor explicit consent; this approach willdepend on the degree to which records havebeen anonymised and the degree to whichdata processing has separated data fromindividuals. If the GMC’s current position isfollowed to absurdity the Cochrane collabo-rators would have to get written consentfrom all participants before performing ameta-analysis.
In general, the provisions of the DataProtection Act are sensible, and researcherswould do well to comply with them or beable to justify any failure to do so. Althoughresearch is exempt from some importantprovisions, consent is the cornerstone ofethical research and the good intentionsof researchers and the inconvenience ofobtaining consent will not be sufficient toexplain to patients or research ethicscommittees the unauthorised processing ofpersonal data.Simon J Ellis chairmanNorth Staffordshire Local Research EthicsCommittee, North Staffordshire Health,Staffordshire ST4 4LX
1 Strobl J, Cave E, Walley T. Data protection legislation:interpretation and barriers to research. BMJ2000;321:890-2. (7 October.)
2 Data Protection Act 1998. www.hmso.gov.uk/acts/acts1998/19980029.htm (accessed 8 February 2000).
3 Brown P. Cancer registries fear imminent collapse. BMJ2000;321:849. (7 October.)
New Zealand model of consent offerssolution
Editor—Strobl et al raise important issuesabout interpreting data protection legisla-tion and its effects on research.1 These issuesare familiar to researchers in New Zealand.
We have used computerised patient datafor research since 1989 when the Royal New
Zealand College of General Practitioners’Dunedin Research Unit established its com-puter research network.2 Before the networkconducted any research, the proposal wasreviewed and approved by the local ethicscommittee. Subsequently, each proposedproject has been subjected to review by thecommittee. The data contained on thenetwork are anonymous: no names,addresses, or telephone numbers are everseen by researchers. Later in the network’sdevelopment, the unique alpha-numericcode used by the New Zealand public healthsystem was attached to many files. Through acomplicated process it was initially possibleto identify individual patients using thiscode. When this was recognised, a furtherstep was added to ensure that researchersreceived only encrypted identifiers. Thede-encryption program is held in a centralgovernment agency and the research dataare held in a university.
But where does this leave the patient’sconsent? Patients are informed by notices inthe offices of practices affiliated with theresearch network that information fromtheir consultation, investigation, or referralmay be used for research once it has beenstripped of identifying data. Patients areassumed to have given consent if theycontinue to be seen in practices affiliatedwith the network. So effective are theanonymisation processes that individualpatients cannot be identified, even towithdraw their data. Data from wholepractices can be excluded from researchprojects but data from individual patientscannot.
This is not a perfect system. It requirespatients to act in accordance with the socialresponsibility they incur when they use pub-lic health systems: that is, to accept responsi-bility to contribute to research that advancesmedical knowledge. It requires researchersto act responsibly in the public interestrather than promoting the commercialinterests of health related industries. Itrequires ethics committees to have a breadthof understanding of issues in medicalresearch that is difficult to achieve whenthere is short term committee membershipand high turnover. It requires everyone toquestion constantly what they are doing andwhy. But it has worked in New Zealand formore than a decade. This model may beeffective in other countries.Susan Dovey analystRobert Graham Center for Policy Studies in FamilyPractice and Primary Care, American Academy ofFamily Physicians, 2023 Massachusetts Ave NW,Washington, DC 20036, [email protected]
Murray Tilyard professor of general practiceDunedin School of Medicine, University of Otago,PO Box 913, Dunedin, New [email protected]
1 Strobl J, Cave E, Walley T. Data protection legislation:interpretation and barriers to research. BMJ2000;321:890-2. (7 October.)
2 Dovey SM, Tilyard MW. The computer research network ofthe Royal New Zealand College of General Practitioners:an approach to general practice research in New Zealand.Br J Gen Pract 1996; 46: 749-52.
Letters
550 BMJ VOLUME 322 3 MARCH 2001 bmj.com

Safeguards for research usinglarge scale DNA collections
Study will not be started before suitablearrangements are in place
Editor—As chairman of the expert plan-ning group set up by the Medical ResearchCouncil and Wellcome Trust, I can reassurereaders of the article by Kaye and Martinthat all the issues they raise about theproposed population study in the UnitedKingdom involving genetic informationhave been fully recognised.1 The study willnot and cannot be started until arrange-ments acceptable to all concerned are inplace. These arrangements are currentlybeing actively developed and entail consul-tation with lay and professional advisers.
The two main reasons behind the highdegree of public concern and debate aboutthe study in Iceland were the initialproposal for an “opt out” approach to con-sent for collection of some of the data andthe decision to license the databasesexclusively to a commercial company.Neither of these has ever been consideredas a possibility in the British study. Consentto take part will be on an “opt in” basis onlyafter full verbal and written explanationsand guarantees on confidentiality. Theavailability of fully anonymised material toothers in order to pursue the full scientificand therapeutic potential of the study willbe tightly controlled.
The study will be overseen and regulatedby a publicly accountable and independentbody responsible for reviewing all its pro-cedures and activities. In addition, full ethicalapproval will of course also have to beobtained. The United Kingdom has welldeveloped, high quality expertise in bothgenetics and population based research, andits diverse population and healthcare systemare additional advantages. Others haveemphasised the importance for futurehealth care of deriving the full benefit fromrecent and future developments in genetics.2
While the appropriate regulatory pro-cedures are being put in place we should notlose sight of the willingness of many peoplein this country to take part in research,including work likely to benefit othersperhaps more than themselves. We mustensure that they can express this readinessthrough their contribution to importantstudies such as the one the MedicalResearch Council and Wellcome Trust aresetting up.Tom Meade directorMedical Research Council Epidemiology andMedical Care Unit, Wolfson Institute of PreventiveMedicine, St Bartholomew’s and the Royal LondonSchool of Medicine and Dentistry, LondonEC1M [email protected]
1 Kaye J, Martin P. Safeguards for research using large scaleDNA collections. BMJ 2000;321:1146-8. (4 November.)
2 Fears R, Roberts D, Poste G. Rational or rationedmedicine? The promise of genetics for improved clinicalpractice. BMJ 2000;320:933-5.
Educational initiatives are essential forsuccess of population genetic studies
Editor—I was delighted to see the article byKaye and Martin on the proposed popula-tion health and diversity study of theMedical Research Council and the Well-come Trust.1 This proposal involves therecruitment of around 500 000 patientsthrough primary care for DNA isolation andgenotyping, to be linked to their medicalrecords and family histories. These will becorrelated with the prospective collection ofchanges in patients’ lifestyles and importanthealth events over several years.
This project may well represent the nextmajor advance in clinical medicine, but sev-eral matters arise from the proposal. Theactive participation of all the relevantprofessional groups and the patient popula-tion is a prerequisite for the success of theproject, both to enable the successfulrecruitment of patients and to maintain themomentum required to sustain such a long-term study. There are important educationalissues that should be addressed as a matterof urgency to enable professionals inprimary care to recruit patients, to obtaintheir informed consent, and to answer ques-tions that arise during the course of thestudy.
Current and emerging technologieswill allow rapid identification of mutationscausing well described single gene disorders,single nucleotide polymorphism profiling,and genomic sequencing. These powerfultechnologies may enable the identificationof predispositions to common, multifacto-rial disorders and predict individuals’responses to conventional therapeutic inter-ventions. On the basis of discussions withgeneral practitioners and practice nurses,and the findings of a recent informal surveyamong general practitioners in South Walesabout attitudes and knowledge of genetics(unpublished data), I think that few profes-sionals in primary care would be confidentin explaining the nature of these techniquesand the importance and implications of thedata that would be generated. This wouldseriously limit the ability of professionals inprimary care to obtain informed consentand answer questions that arise over theyears of the study. The long term nature ofthe proposals reinforces the view thateducation and training in genetics, and par-ticularly in the basic science that underpinsthe subject, are a priority for medical,nursing, and associated professions at thebasic, specialist, and continuing educationstages. The success of the proposed studyand future population genetic studies aredependent on this educational need beingimmediately and effectively addressed.Ian Hopkinson honorary consultant in primary caregenetic medicineClinical and Molecular Genetics Unit, Institute ofChild Health, London WC1N [email protected]
1 Kaye J, Martin P. Safeguards for research using large-scaleDNA collections. BMJ 2000;321:1146-8. (4 November.)
Mortality in joggers
Healthy jogger effect might explaindifferences in mortality
Editor—In their cohort study of mortalityin Danish men, Schnohr et al compared themortality in 96 men who reported that theywere joggers at two examinations in 1976-8and 1981-3 with that in 4562 men who werenon-joggers at both examinations.1 Theauthors followed up the cohort from 1976-8to 1998 and found that the joggers’ relativerisk of death was 0.39 (95% confidenceinterval 0.19 to 0.73).
The participants rather than the authorsdefined jogging. The paper does not includeinformation on how or how much the menexercised at the time of the examinations orin between and after the examinations. It isnot clear whether the men agreed on a com-mon definition of jogging.
At the time of the two examinations, in1976-8 and 1981-3, 217 (4.7%) and 202(4.3%) respectively of the 4658 men, aged20-79, reported that they were joggers.These numbers are surprisingly low. Accord-ing to a study carried out in 1994 by theDanish National Institute for Public Health,59.5% of men aged >16 exercised orconsidered themselves to be physicallyactive. Even among men aged >67, 55.4%exercised or considered themselves to bephysically active.2
No data on mortality are presented inthe paper. Because of the small number ofjoggers the relative risk of death ispresumably sensitive to small differences inmortality even though the difference issignificant.
The authors point out that their study isobservational and that it controls for age butnot for differences in lifestyle. A healthy jog-ger effect rather than jogging in itself mayexplain the difference in mortality.Hans Okkels Birk health [email protected]
Lars Onsberg Henriksen chief medical officerDepartment of Hospitals, Roskilde County,Postboks 170, DK-4000 Roskilde, Denmark
1 Schnohr P, Parner J, Lange P. Mortality in joggers: popula-tion based study of 4658 men. BMJ 2000;321:602-3. (9September.)
2 Danish Institute for Clinical Epidemiology. Danish healthand morbidity survey 1994. Copenhagen: DICE, 1998.(www.dike.dk/gammel/html/udgivel/engsusy/tabel/index.htm (table 8); accessed 16 Jan 2001.)
Benefits are seen in previously sedentaryindividuals who start exercising regularly
Editor—The Copenhagen city heart studyconfirms the association between regularexercise and a reduced risk of prematuredeath from certain illnesses.1 2 But theobserved reduction in the risk of death fromall causes only in those men who reportedjogging at both of two examinations carriedout five years apart conflicts with resultsreported elsewhere.3 4 We believe that thisarises from pooling the results of twopatterns of behaviour.
To combine the results from men whowent from being active to inactive with those
Letters
551BMJ VOLUME 322 3 MARCH 2001 bmj.com
from men who went from being inactive toactive (jogging at one examination) impliesthat the direction of change between activeand inactive is immaterial and that thehealth state between those behaving in thesedifferent ways does not differ. This isunlikely. Stopping regular exercise may indi-cate declining health and an increased riskof death, whereas starting an exercise habitmay be a sign of increased wellbeing and fit-ness. Evidence from both the United Statesand Britain supports this view.3 4
Observing changes in activity levels atthree time points between 1962 and 1977,Paffenbarger et al reported that the relativerisk of death from all causes in participantswho at the first time point were engaged inmoderately vigorous sports activity but whostopped exercising was slightly higher (1.15(95% confidence interval 0.73 to 1.71)) thanthat in those who reported no exercise at all(1.0).3 Those who changed in the oppositedirection, from being inactive to beingactive, had a relative risk similar to that ofthose who maintained a continuous exercisehabit throughout the study period (0.77 and0.71 respectively).
A similar pattern of health benefit in thedirection from inactive to active was alsofound in the British regional heart study.4
This study reported that, relative to the risk inthose who remained inactive, the fullyadjusted risk of death from all causes in thosewho changed from an inactive lifestyle toparticipating in occasional light exercise was0.55 (0.36 to 0.84), which was slightly lowerthan that for continuous exercisers (0.58).
This study suggests that the benefits of areduced risk of premature death from allcauses in those previously sedentary indi-viduals who start exercising regularly areprobably as large as those in continuousexercisers; they are unlikely to be the sameas those in previous exercisers who gave upexercise.P Coleman research [email protected]
J Nicholl directorMedical Care Research Unit, School for Health andRelated Research, University of Sheffield, SheffieldS1 4DA
1 Schnohr P, Parner J, Lange P. Mortality in joggers: popula-tion based study of 4658 men. BMJ 2000;321:602-3. (9September.)
2 Fentem PH. Benefits of exercise in health and disease. BMJ1994;308:1291-5.
3 Paffenbarger Jr RS, Hyde RT, Wing AL, Lee IM, Jung DL,Kampert JB. The association of changes in physical activitylevel and other lifestyle characteristics with mortalityamong men. N Engl J Med 1993;328:538-45.
4 Wannamethee SG, Shaper AG, Walker M. Changes inphysical activity, mortality, and incidence of coronary heartdisease in older men. Lancet 1998;351:1603-8.
Authors’ reply
Editor—In 1976, when the Copenhagencity heart study was started, there was stillsome concern over whether jogging mightbe harmful to health. No other study hadinvestigated this question, and we decided toask each participant “Are you a jogger?,”without further quantification of jogging.The percentage of male joggers aged 20-79was 4.7% in the first examination (1976-8)and had increased to 8.3% in 1991-4. In
addition to jogging status, information onphysical activity during work and leisuretime was collected, both classified into fourlevels. Our findings agreed with the physicalactivity reported in the Danish health andmorbidity survey 1994.
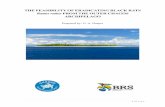
Follow up is based on the Danishnational population register, and data onmortality are therefore available for nearlyall participants. Because our paper was pub-lished as a short report, with only one tableor figure, however, we were unable topresent age specific mortality in addition tothe table. As the figure indicates here, thecrude survival function for the four groupsof joggers shows a remarkably clear patternover age. The positive effect of jogging isthus unlikely to be an artefact resulting fromsmall sample sizes.
The purpose of conducting the Coxregression analysis was to separate the effectof jogging from the effect of potentialconfounding variables. One should alwaysbe concerned about a possible healthyjogger effect as a partial explanation of thedifference in mortality. Previous studies haveshown that among its beneficial effectsphysical exercise (including jogging)reduces blood pressure, being overweight,and the risk of non-insulin dependentdiabetes mellitus; raises high density lipo-protein cholesterol concentrations; anddecreases platelet aggregation.Peter Schnohr chief [email protected]
Jan Parner statisticianPeter Lange chief physicianCopenhagen City Heart Study, BispebjergUniversity Hospital, DK-2400 Copenhagen NV,Denmark
Accuracy of ATLS guidelinesfor predicting systolic bloodpressure
Authors’ core assertion was wrong
Editor—I commend the BMJ for allowingaccess to the editorial decision making proc-ess via the BMJ’s website. It gives a fair meas-
ure of explanation why a paper waspublished.
On reading the peer reviews for Deakinand Low’s paper on advanced trauma lifesupport guidelines for predicting systolicblood pressure it is evident that the refereeand statistician have accepted withoutcriticism the authors’ core assertion.1 This isthat the advanced trauma life supportcourse teaches that if only the patient’scarotid pulse is palpable then the systolicblood pressure is 60-70 mm Hg; if both thecarotid and femoral pulses are palpable thenthe systolic blood pressure is 70-80 mm Hg;and if the radial pulse is also palpable thenthe systolic blood pressure is > 80 mm Hg.
Unfortunately, this is entirely wrong andconstitutes no part of the current course ormanual.2 The authors cite a guideline from1985,3 but the manual is currently in its sixthedition, with a further update due for publi-cation this year, 2001.
One redeeming feature of the paper isthat it shows (albeit at lower intra-arterialsystolic pressures) an observable relationbetween the palpability of pulses and systolicblood pressure. But the design of the paperis open to question. Why were only 20patients included (especially over threeyears)? What conditions did they have? Ifthey had arterial lines inserted I hope thatthey had already received initial resuscita-tion. Some were undergoing operation—didthey have anaesthesia? What was the statusof the observer?
If we are all planning to keep our fingerson the pulses then we really must stay up todate and reaccredited.Ian S Russell staff gradeDepartment of Accident and Emergency,Hartlepool General Hospital, HartlepoolTS24 [email protected]
1 Deakin CD, Low JL. Accuracy of the advanced trauma lifesupport guidelines for predicting systolic blood pressureusing carotid, femoral, and radial pulses: observationalstudy. BMJ 2000;321:673-4. (16 September.)
2 American College of Surgeons. Advanced trauma lifesupport for doctors. 6th ed. Chicago: ACS, 1997.
3 Collicott PE. Advanced trauma life support course forphysicians. Chicago: American College of Surgeons, 1985.
No one relies on pulse checks alone forsubsequent clinical decision making
Editor—Deakin and Low have shown that ifyou follow the principles of advancedtrauma life support you tend to overestimatethe patient’s blood pressure, which leads tounder-resuscitation.1 They used invasivemethods of blood pressure recording, possi-bly insertion of an arterial line. In reality,overestimation leads to “secondary survey”anyway (assuming that airway and breathingwere normal); checking blood pressure ispart of that. Any low blood pressure willthen be picked up, and resuscitation will bestarted accordingly.
I have worked in different accident andemergency and trauma departments, and Ihave never come across anyone who reliedon pulse checks alone in subsequent clinicaldecision making. This is because we alreadyknow that feeling a pulse has nevercorrelated well with the blood pressure. We
Age (years)
Prob
abili
ty o
f sur
viva
l
20 30 40 50 60 70 80 90 1000
0.20.30.40.50.60.70.80.91.0
0.1
Non-jogger at both examinationsNon-jogger at first examination; jogger at second examinationJogger at first examination; non-jogger at second examinationJogger at both examinations
Estimated age specific survival function, usingKaplan-Meier estimator with left truncation and rightcensoring for four groups of joggers
Letters
552 BMJ VOLUME 322 3 MARCH 2001 bmj.com

also know that the advanced trauma lifesupport guidelines teach us very basic prin-ciples of resuscitation of trauma victims andthat often we have to use our brain to evalu-ate further, investigate, and treat a sickpatient.
I was disappointed that the authors didnot compare a standard method of checkingblood pressure (cuff and sphygmomanom-eter) with the invasive monitoring. I am surethat, if they had done, it would have given adifferent value. What do we do then? Wecannot put an arterial line in every patient tomonitor blood pressure.Zak Baig country general practitionerMinlaton Accident and Emergency Department,Minlaton, South Australia, [email protected]
1 Deakin CD, Low JL. Accuracy of the advanced trauma lifesupport guidelines for predicting systolic blood pressureusing carotid, femoral, and radial pulses: observationalstudy. BMJ 2000;321:673-4. (16 September.)
Earlier dogma seems to have beendropped now
Editor—Deakin and Low tested the relationbetween palpable pulses and systolic bloodpressure.1 We both remember being assuredof this relation as students (in the daysbefore evidence based medicine); theauthors’ paper questions this medical schooldogma.
Advanced trauma life support is oftenaccused of didacticism on many fronts, butwe do not think that it is guilty on this occa-sion. We are both instructors in advancedtrauma life support and have been involvedat provider level since 1991. We have no rec-ollection of this being taught as core courseknowledge. We note that the offendingguideline was published in 1985 and assumethat it has since been dropped.
Advanced trauma life support teachesthe need for rapid discovery and aggressivetreatment of initial, recurrent, or persistenthypovolaemia. The finding of an absentpulse at any site, other than for local reasons,should be presumed to signify appreciablehypovolaemia. The paper supports this.Gareth Quin consultant in accident and [email protected]
Gerard McCarthy consultant in accident andemergency medicineRoyal Gwent Hospital, Newport, Gwent NP9 2UB
1 Deakin CD, Low JL. Accuracy of the advanced trauma lifesupport guidelines for predicting systolic blood pressureusing carotid, femoral, and radial pulses: observationalstudy. BMJ 2000;321:673-4. (16 September.)
Author’s reply
Editor—The advanced trauma life supportcourse introduced the relation between pal-pable pulses and blood pressure in its firstedition in 1985. I agree that the papershould have clarified that the course hasnow stopped teaching this relation. In ashort report, however, there was not enoughspace to discuss the evolution of theguidelines.
The reference in our paper clearly refersto the 1985 guidelines. By quoting a
different reference, Russell is wrong instating that our core assertion is incorrect.The original advanced trauma life supportguidelines have been disseminated widelyand continue to be taught and cited.1–3 Theseunvalidated guidelines remain an often usedmethod of quickly assessing hypotensivepatients, and early advanced trauma lifesupport teaching (and instructors) must takeresponsibility for their international dis-semination and use.
Russell criticises the design of the paperin that only 20 patients were collected overthree years. I accept that this was a smallstudy, but it nevertheless generates data thatcast doubt on the relation between pulsesand blood pressure. Recruitment was lim-ited by the number of hypotensive traumapatients seen at this hospital each year. Rus-sell is correct in assuming that the patientsreceived initial resuscitation, and it is for thisreason that the number was limited. Are webeing criticised for adequate resuscitationthat has prevented hypotension in mostpatients? Collecting data over three years ishardly a cause for criticism.
Russell questions the 29 data pointsfrom 20 patients. We stated in the paper that“Not all pulses were palpable when areading was taken because of impairedpatient access.” The raw data were submittedto the BMJ, which declined to publish them.
Baig states he has never come acrossanyone who relied on pulse checks alone. Ihave worked in several trauma systems inthe United Kingdom, particularly in the pre-hospital arena, where quick assessment ofpalpable pulses is used as an initialassessment of blood pressure and manage-ment decisions are made on the basis ofpulses alone. Baig is also incorrect in statingthat “we already know that feeling a pulsehas never correlated well with the bloodpressure.” We do not.
Baig is disappointed that the study didnot compare invasive and non-invasive(cuff) measurements. This was not ouraim. As stated in the paper, non-invasiveblood pressure measurement in hypotensivepatients is inaccurate, and we deliberatelyavoided this measurement technique. Bloodpressure was changing rapidly in many ofthe patients, and non-invasive pressuremeasurement lags behind changes in actualblood pressure. It would be unethical to waitwhile non-invasive pressure was measuredbefore treating hypotension.Charles D Deakin consultant anaesthetistShackleton Department of Anaesthetics,Southampton General Hospital NHS Trust,Southampton SO16 [email protected]
1 Pre-Hospital Trauma Life Support Committee, Nationalassociation of Emergency Medical Technicians in coopera-tion with Committee on Trauma, American College ofSurgeons. Prehospital trauma life support—instructors’manual.3rd ed. St Louis, MO: Mosby, 1995.
2 Dalton AL, Limmer D, Mistovich JJ. Advanced medical lifesupport. New Jersey: Prentice Hall, 1999.
3 Eaton CJ. Essentials of immediate medical care. Edinburgh:Churchill Livingstone, 1999.
Severity of overdose afterrestriction of paracetamolavailability
Study’s results conflict with those of otherpapers
Editor—Robinson et al report a reductionin the amount of paracetamol ingested inoverdose since the introduction of reducedpack sizes and blister packing of over thecounter paracetamol in September 1998.1
They found no change, however, in the inci-dence of hepatotoxicity. Their results con-trast with those of other studies, which haveshown a 21% reduction in episodes of hepa-totoxicity and a 64% reduction in the devel-opment of severe hepatotoxicity.2 3
As they have stated, hepatic failure israre if < 12 g of paracetamol is ingested.4
But the median dose ingested in their studydid not reach this level. It is thus unsurpris-ing that the study included only five cases ofhepatotoxicity; given this low number, itseems imprudent to claim that no change inincidence has occurred.
In addition, the paracetamol concentra-tions quoted in the paper are low, consider-ing that concentrations > 200 mg/l fourhours after ingestion and > 130 mg/l sixhours after ingestion are used to guide theappropriate use of acetylcysteine treatment.Despite the low concentrations quoted,acetylcysteine was given to 25% and 31% ofpatients. This does not seem to accord withcurrent practice recommendations.
Robinson et al conclude that the changein pack size had no effect on the incidence ofsevere liver failure. In our view, a stricterdefinition of paracetamol overdose isrequired if we are to make sense of the con-flicting reports. Perhaps paracetamol over-dose should be confined to subjects whoclaim to have taken an overdose and have ameasurable serum concentration.
The burden of paracetamol poisoningon the NHS is high, with over 70 000episodes a year in Britain.5 It is worrying thatthe recent measures have not had a moredramatic effect on this serious problem. If, asTurvill et al say,3 only a 21% reduction hasbeen achieved then further measures suchas limiting paracetamol to prescription onlyshould be considered.C L Sheen clinical research [email protected]
T M MacDonald professor of pharmacology andpharmacoepidemiologyMedicines Monitoring Unit, University of Dundee,Ninewells Hospital and Medical School, DundeeDD1 9SY
Competing interests: CLS is funded by anunrestricted fellowship from Pfizer to study the tox-icity of over the counter non-steroidal anti-inflammatory drugs and other analgesics. TMM is amember of the subcommittee on pharmacovigi-lance of the Committee on Safety of Medicines.
1 Robinson D, Smith AMJ, Johnston GD. Severity ofoverdose after restriction of paracetamol availability: retro-spective study. BMJ 2000;321:926-7. (14 October.)
2 Prince MI, Thomas SHL, James OFW, Hudson M.Reduction in incidence of severe paracetamol poisoning.Lancet 2000;355:2047-8.
Letters
553BMJ VOLUME 322 3 MARCH 2001 bmj.com

3 Turvill JL, Burroughs AK, Moore KP. Change inoccurrence of paracetamol overdose in UK after introduc-tion of blister packs. Lancet 2000;355:2048-9.
4 Routledge P, Vale JA, Bateman DN, Johnston GD, Jones A,Judd A, et al. Paracetamol (acetaminophen) poisoning.BMJ 1998;317:1609-10.
5 Fagan E, Wannan G. Reducing paracetamol overdoses.BMJ 1996;313:1417-8.
Restriction has not reduced admissionswith self poisoning
Editor—The report by Robinson et al,1 andother reports,2 3 suggests that restriction ofsales of paracetamol has reduced thenumber and severity of paracetamol poison-ings. This is welcome, but the effect on allcases of self poisoning has not been consid-ered. Suspecting that selective restriction ofparacetamol would result in other drugsbeing substituted,4 we carried out a study tolook at this.
We surveyed all admissions for overdosebefore and after sales of paracetamol wererestricted: 116 patients (group A) wereadmitted in the six months before paraceta-mol was restricted (February-August 1998)and 112 patients (group B) duringFebruary-August 1999. Altogether 52 (45%)paracetamol poisonings occurred before therestrictions were put in place and 40 (36%)after. The number of paracetamol tabletstaken was known for 44 patients in group Aand 35 in group B. Thirty (68%) patientstook more than 16 tablets before rationingand 18 (51%) afterwards; this was reflectedin the need for treatment with acetyl-cysteine, which fell from 16 cases to nine.
Although paracetamol overdosedeclined, non-paracetamol poisoningincreased (from 64 to 72 cases), predomi-nantly involving antidepressant, anti-psychotic, and sedative drugs. For bothsample periods the average time that eachpatient spent in hospital was the same (2.6days). One death occurred from a tricyclicoverdose. Although admissions with para-cetamol overdose fell, the numbers of casesand bed days needed for care did not alter.Drug selection in self poisoning is usuallydictated by what is immediately available,whether obtained over the counter or bymedical prescription.5
Our patients used over 50 different pre-scription only drugs for overdose, which hadbeen obtained previously for therapeuticpurposes. Our results suggest that patientsare now switching to alternative agents,often as part of a multidrug cocktail, withequivalent risk because of individual toxicityand interaction. There may be less demandon liver units,2 but the unwanted workloadfor general physicians is the same. Morerestraint in drug prescription may have agreater effect on the incidence and morbid-ity of, and mortality from, self poisoningthan this simplistic restriction of paraceta-mol has had.Mohan R Thomas staff grade physicianNigel I Jowett consultant [email protected] of Medicine, Withybush GeneralHospital, Pembrokeshire SA61 2PZ
Competing interests: None declared.
1 Robinson D, Smith AMJ, Johnston GD. Severity ofoverdose after restriction of paracetamol availability: retro-spective study. BMJ 2000;321:926-7. (14 October.)
2 Prince MI, Thomas SH, James OFW, Hudson M. Reductionin incidence of severe paracetamol poisoning. Lancet2000;355:2047-8.
3 Turvill JI, Burroughs AK, Moore KP. Change in occurrenceof paracetamol overdose in UK after introduction ofblister packs. Lancet 2000;355:2048-9.
4 Jowett NI. Limitation of over the counter sales of paraceta-mol. BMJ 1998;317:1657.
5 Hawton K, Ware C, Mistry H, Hewitt J, Kingsbury S,Roberts D, et al. Why patients choose paracetamol for selfpoisoning and their knowledge of its dangers. BMJ1995;310:164.
Why hasn’t strategy for minimisingparacetamol poisoning been enacted?
Editor—It has been well known for nearly20 years that adding methionine or acetyl-cysteine to each paracetamol (acetomi-nophen) tablet provides the liver withsufficient reserve of the sulphydryl group toconjugate the toxic paracetamol metabo-lites. So why haven’t our regulators man-dated such?
If paracetamol were a dietary supple-ment it would have been put into the “mosttoxic substance on earth” category andbanned long ago. Drug interactions with StJohn’s wort (most of which were hypotheti-cal) were acted on with great haste by regu-lators around the world, despite no deathsever having been associated with use of StJohn’s wort. Here we have a drug that isavailable from petrol stations and cornershops and has been killing thousands ofpeople around the world for years, and ourregulators turn a blind eye—even whenthere is a simple solution.
Why the double standards and thehypocrisy?Ron Law lecturer in managementFaculty of Business, Auckland University ofTechnology, Private Bag 92006, Auckland 1, [email protected]
Competing interests: RL is a member of the workinggroup advising the New Zealand Ministry of Healthon mandatory reporting of medical error policy. Heis also executive director of the National NutritionalFoods Association and is motivated by injustice.
Guidelines for prevention offalls in people aged over 65
Guidelines should state that assessmentof vision is important
Editor—A fall in an older person can havesevere personal as well as healthcareimplications. Feder et al have given impor-tant guidelines for the prevention of falls inpeople aged over 65.1 Their aim was totranslate trial evidence into recommenda-tions to reduce the rate of falls in peopleaged over 65.
The methods used to gather infor-mation did not seem to include anyreferences to the patients’ visual function.There have been several reports linkingpoor visual function with an increased riskof falls or fractures related to falls.2–4 A recentstudy by Ivers et al shows that decreasedvisual function is a risk factor for hipfractures.5
It would seem logical that people whodo not see well are more likely to fall thanthose who do see well. It is unfortunate, then,that the guidelines given do not contain anyreferences to improving visual function.Poor vision is quite common in elderly peo-ple. The causes are varied and include prob-lems related to spectacles (not wearingthem, incorrect prescription, scratchedlenses, inability to afford them, inappropri-ate lenses), cataracts, glaucoma, age relatedmacular degeneration, diabetic retinopathy,and other vascular abnormalities.
We believe that regular visual assess-ments should be included in the guidelinesaimed at the prevention of falls. An ophthal-mologist should assess patients with poten-tially treatable eye disease. Perhaps weshould more often consider the risk offalling when we assess our patients withcataracts and other eye disease. Certainly,patients with poor vision from untreatablecauses should be provided with low visionaids as appropriate. These patients may alsobe the ones most likely to benefit from otherinterventions, as set out by Feder et al.R R Seemongal-Dass specialist registrarT E James consultantC E Atherley specialist registrarDepartment of Ophthalmology, St James’sUniversity Hospital, Leeds LS9 [email protected]
Competing interests: None declared.
1 Feder G, Cryer C, Donovan S, Carter Y. Guidelines for theprevention of falls in people over 65. BMJ 2000;321:1007-11. (21 October.)
2 Klein BE, Klein R, Lee KE, Cruikshanks KJ. Performance-based and self-assessed measures of visual function asrelated to the history of falls, hip fractures, and measuredgait time. The Beaver Dam eye study. Ophthalmology1998;105:160-4.
3 Cummings SR. Treatable and untreatable risk factors forhip fracture. Bone 1996;18(suppl 3):165-7S.
4 Felson DT, Anderson JJ, Hannan MT, Wilson PW, Kiel DP.Impaired vision and hip fracture. The Framingham study.J Am Geriatr Soc 1989;37:495-500.
5 Ivers RQ, Norton R, Cumming RG, Butler M, CampbellAJ. Visual impairment and risk of hip fracture. Am J Epi-demiol 2000;152:633-9.
Health improvement plans mustincorporate falls and osteoporosisstrategies
Editor—Feder et al address the importantissue of minimising the injuries that resultfrom falls by elderly people.1 Falls are themost frequent cause of morbidity andmortality related to injury in elderly peopleand as such represent a major public healthproblem. Injuries related to falls will poseeven greater challenges to the health servicewith an ageing population.
Hip fracture is one of the most costlyand debilitating outcomes resulting from afall but occurs in only 1% of falls.2 It is wellknown, however, that over 90% of hipfractures are associated with a fall. Clearly,falling is only part of the problem. Fractureis determined not only by the propensity tofall but also by the underlying fragility of thebone. Experts estimate that in people agedover 75 over 90% of hip fractures are attrib-utable to fragile bones due to osteoporosis3;there is simply too little bone in the bone.
In the NHS at a local level, healthimprovement plans must integrate falls and
Letters
554 BMJ VOLUME 322 3 MARCH 2001 bmj.com
osteoporosis strategies. Without the integra-tion of these local initiatives elderly fallers willmost probably receive an assessment andintervention after falling but will not beassessed or treated to reduce the risk of frac-ture should a further fall occur. This wasshown recently in a study by Kamel et al,where only 5% of women admitted to a com-munity hospital in the United States over twoyears left with new drug treatment prescribedto prevent a further fracture.4 Furthermore,patients with osteoporosis may not have theirrisk of falling investigated and receive onlybone strengthening treatment.
Strategies to reduce fractures, especiallyof the hip, need to address both falling andbone strength. A review of more than 300publications related to falls, and interviewswith more than 50 healthcare professionals,led to the development of a simple fractureprevention model, which clearly highlightsthree intervention points for fracture (figure).5
Interventions that aim to prevent frac-tures should aim at reducing the risk of fall-ing, strengthening people’s bones, and reduc-ing the force of impact of a fall on people’sbones. It is to be hoped that the national serv-ice framework for older people’s services willpick up where Feder et al’s work leaves off, bymaking clear the need to address bothosteoporosis and falls in local strategies.Mark Chakravarty head of government affairsProcter and Gamble Pharmaceuticals, Staines,Middlesex TW18 [email protected]
Anna Sörman head of government and NHS policyAventis Pharmaceuticals, West Malling, KentME19 4AH
Competing interests: MC is employed by and hasshares in Procter and Gamble. AS is employed byand has shares in Aventis Pharma. Procter andGamble and Aventis Pharma form the Alliance forBetter Bone Health and manufacture and marketrisedronate sodium (Actonel) for postmenopausalosteoporosis.
1 Feder G, Cryer C, Donovan S, Carter Y. Guidelines for theprevention of falls in people over 65. BMJ 2000;321:1007-11. (21 October.)
2 Tinnetti ME, Speechley M, Ginter SF. Risk factors for fallsamong elderly persons living in the community. N Engl JMed 1988;319:1701-7.
3 Phillips S, Fox N, Jacobs J, Wright WE. The direct medicalcosts of osteoporosis for American women aged 45 andolder, 1986. Bone 1988;9:271-9.
4 Kamel HK, Hussain MS, Tariq S. Failure to diagnose andtreat osteoporosis in elderly patients hospitalized with hipfracture. Am J Med 2000;109:326-8.
5 National Institutes of Health Osteoporosis and RelatedBone Diseases National Resource Center. NIH ORBD-NRC news: falls and fracture prevention.. Vol 2, No 1.Washington, DC: NIH ORBD-NRC, 1999. Available atwww.osteo.org/newsvol2no1.html (accessed 22 Nov 2000).
Unicef is crucial in promotingand supporting breast feedingEditor—The report from the NHS Centrefor Reviews and Dissemination highlightsmany of the reasons why the work of theUnicef UK baby friendly initiative is a crucialcomponent of any strategy to promote andsupport breast feeding.1
Although breastfeeding rates in theUnited Kingdom have remained static since1980,2 a survey of 21 baby friendly hospitalshas found an increase of more than 10% inbreastfeeding initiation. The percentage ofbabies who are breast fed rose from 60% twoyears before the units received their babyfriendly award to 70.6% a year after theiraccreditation (table). Some of the largestincreases were in hospitals serving inner cityor deprived areas, which traditionally havelow rates. For example, breastfeeding initia-tion at the Ulster Hospital in Belfast hasincreased from 29% in 1995 to 55% now.Some hospitals in areas with traditionallystrong breastfeeding rates have also shownincreases with the Royal Surrey Hospital,Guildford, showing a rise from 74% in 1995to 86% today.
Compounding the problem of the lowuptake of breastfeeding is the rapid decline inprevalence. Each year, 75 000 mothers stopbreast feeding in the first postnatal week, butonly 1% say that this is how long they hadintended to breast feed for. The reasons mostgive for stopping relate to problems thatcould be avoided or solved if they were bettersupported.3 The principle behind the babyfriendly initiative is that best practice stand-ards should be adopted so that health profes-sionals are able to support mothers in theirchosen feeding method. Healthcare facilitieswhich implement best practice—the 10 stepsto successful breastfeeding for the maternityservices4 or the seven point plan for the pro-tection, promotion, and support of breastfeeding in community healthcare settings5—can be assessed and accredited as babyfriendly. The standards combine the founda-tions of good practice (policy, training,information) with changes to practice (skin toskin contact, rooming in, exclusive breastfeeding) and good cooperation between thedifferent parts of the health service and thevoluntary sector.
Thirty one maternity units in the UnitedKingdom have a full baby friendly award,and another 68 have a certificate of commit-ment, which rewards the development of adetailed action plan. We hope that the latest
report will accelerate progress among theremaining units.Andrew Radford programme directorUnicef UK Baby Friendly Initiative, London WC2H9TA
1 Kmietowicz Z. Breastfeeding programmes “should betargeted.” BMJ 2000;321:467. (19-26 August.)
2 Foster K, Lader D, Cheesbrough S. Infant feeding 1995.London: Stationery Office, 1997.
3 Unicef UK Baby Friendly Initiative. Baby friendly hospitalsshow strong increase in breastfeeding rates. Baby FriendlyNews No 6, July 2000
4 WHO/Unicef. Protecting, promoting and supporting breast-feeding: the special role of maternity services. A JointWHO/Unicef Statement. Geneva:WHO, 1989.
5 Unicef UK Baby Friendly Initiative. The baby friendly initia-tive in the community—an implementation guide. London:Unicef UK Baby Friendly Initiative, 1999.
Evidence and belief inattention deficit hyperactivitydisorder
Narrow focus of editorial wasdisappointing
Editor—The editorial by Zwi et al sug-gested that current practice in attentiondeficit hyperactivity disorder is largely basedon belief with little good evidence available.1
Its narrow focus on inadequate methods instudies was, however, disappointing, barelytouching the surface of the controversiessurrounding attention deficit hyperactivitydisorder and the prescription of stimulants.The disorder construct raises more ques-tions than it answers. For example, where isthe cut-off point between normal behaviourand attention deficit hyperactivity disorder?Who defines this, and why? (What does the> 30-fold variance in prevalence rates inepidemiology studies mean?) Why is thisdiagnosis predominantly given to boys? (IsWestern culture more concerned withexternalised behaviour seen in boys thaninternalised behaviour of girls?) Why thevery high rates of comorbidity with otherpsychiatric disorders? (Is attention deficithyperactivity disorder a research generatedidea that has little relation to the complexitycommonly found in clinical practice?) Is thedisorder being diagnosed more commonlybecause of a real increase or because of achange in the way certain behaviours areinterpreted? (If there is a real increase in thedisorder, what is the environmental cause?)
The wider questions about the prescrip-tion of stimulants were not considered inthis article. For example, does the prescrip-tion create a medical script for understand-ing life’s problems that could persist in adysfunctional way in later life (a pill to solveproblems)? Is it possible that, as well assometimes alleviating stigma, we as doctorsmay contribute to stigma and intolerance bylabelling and treating with drugs? Are webeing duped by a powerful multimillion dol-lar drug industry into miracle cures? It isalso incorrect, as Zwi et al stated, that there isno evidence of long term harmful conse-quences. Evidence (however poor the stud-ies) has been put forward that long termprescription of stimulants could result inpoor growth, cognitive deterioration, tics,
Fragility
Fracture
ForceFalls
Fracture prevention triangle
Birth rates and incidence of breast feeding in 21hospitals according to timing of accreditation byUnicef UK baby friendly initiative
Accreditation No of birthsNo (%) of babies
breast fed
Two years before 34538 20 719 (60.0)
One year before 34122 21 563 (63.2)
During 33861 22 365 (66.1)
One year after* 22552 15 930 (70.6)
*Includes figures for part of year for hospitals accreditedduring 1999.
Letters
555BMJ VOLUME 322 3 MARCH 2001 bmj.com

obsessionality, flat affect, moodiness, toler-ance, and dependence.
Parents making the difficult decisionwhether to accept stimulants for their childshould be given the full information aboutthe controversies to allow them to make aninformed decision. However, the medical lit-erature should also broaden the debate fromthe narrow tunnel vision of pure medicalmodels to develop a dialogue with other dis-ciplines and explore concepts such as atten-tion deficit hyperactivity disorder from adifferent perspective.Sami Timimi consultant child and adolescentpsychiatristLincoln District Healthcare NHS Trust, LincolnLN2 5RT
1 Zwi M, Ramchandani P, Joughin C. BMJ 2000;321:975-6.(21 October.)
Reintroduction of methylphenidate inItaly needs careful monitoring
Editor—In their editorial Zwi et al empha-sised that informed decision on the use ofstimulants for the treatment of attention defi-cit hyperactivity disorder must be based onstudies with good methods.1 Two weeks afterpublication of the editorial the BMJ reportedthat the National Institute for ClinicalExcellence (NICE) suggested that methyl-phenidate should be used as part of acomprehensive treatment programme forchildren with this disorder.2 In Italy methyl-phenidate was withdrawn from the market in1989 by the manufacturer, and since thenchildren with the disorder have receivedtreatment with tricyclic antidepressants, ben-zodiazepines, and questionable drugs that arenot evidence based. In October 2000 thissituation led a group of paediatricians in pri-mary care to lobby the national healthdepartment for the immediate reintroductionof methylphenidate. As a consequence, thedrug will once again be marketed in Italy.
This outcome has been reported as asuccess for primary care paediatricians, alsoappearing as such in the email responsesposted to the main Italian paediatric onlinediscussion group (www.pediatria.it). All cor-respondents were enthusiastic about theforthcoming availability of methylpheni-date, and none warned about the possibilityof overusing this stimulant or the need toeducate primary care paediatricians betteron the comprehensive management ofattention deficit hyperactivity disorder. Thisis worrying in Italy in view of the lack ofknowledge about the syndrome’s incidence,the lack of awareness in general practice ofdiagnostic criteria and therapeutic guide-lines, and the documented adverse reactionsthat necessitate systematic monitoring.3
We recently conducted a survey ofthe knowledge and attitudes towardsattention deficit hyperactivity disorderamong the 86 primary care paediatricians inTurin attending 77 378 children.4 Eighteenof the 56 respondents did not know aboutthe existence of this disorder, 34 did notknow the criteria needed for diagnosis, andonly six followed up suspected cases directly.The drug most used for the disorder was
niaprazine, an antihistamine commonlyprescribed in Italy and a few other countriesto treat children with sleep disorders.
We agree with the conclusion of Zwi et althat stimulants should be prescribed judi-ciously and monitored carefully. This is espe-cially true in Italy, where primary carepaediatricians so far have a limited experi-ence in the effective management of attentiondeficit hyperactivity disorder. Their role ininitiating prescribing for this condition alsoneeds to be thoroughly examined in specific,applied research initiatives.5
Maurizio Bonati headPiero Impicciatore senior research fellowChiara Pandolfini research fellowLaboratory for Mother and Child Health, Istituto diRicerche Farmacologiche Mario Negri, Via Eritrea62, 20157 Milano, [email protected]
1 Zwi M, Ramchandani P, Joughin C. Evidence and beliefs inADHD. BMJ 2000;321:975-6. (21 October.)
2 Dobson R. NICE issues new guidelines on Ritalin. BMJ2000;321:1100. (4 November.)
3 Barkley RA, McMurrey MB, Edelbrock CS, Robbins K.Side effects of methylphenidate in children with attentiondeficit hyperactivity disorder: a systemic, placebo-controlled evaluation. Pediatrics 1990;86:184-92.
4 Marchini L, Puzzo F, Pirella A, Pandolfini C, Campi R, Imp-icciatore P, et al. Se non sta fermo solo in USA scatta laricetta. Occhio Clinico Pediatria 2000;4:12-14.
5 Thomas P. The research needs of primary care. BMJ2000;321:2-3.
Twins and asthma
Difference in admission rates may be dueto other factors
Editor—Strachan et al found an interestingdifference between admissions to hospitalfor childhood asthma between twins andsingletons.1 They conclude that there isreduced risk of asthma among twins. Wefound no significant difference in question-naire based asthma diagnoses betweensingletons and twins aged 30-59 yearsamong the Finnish twin cohort, but we didnot give figures.2 The Finnish twin cohort isa population based sample of adult twinpairs of the same sex selected from the cen-tral population registry of Finland as pairsof individuals with the same birth date andsex, as well as the same surname and localcommunity of birth. These selection criteriaalso captured some unrelated individuals.The unpublished figures are based on12 024 twins and 2015 singletons. Agestandardised prevalences of asthma were 2.1(95% confidence interval 1.6 to 2.5) for maletwins and 2.1 (1.1 to 3.0) for male singletons.For women, prevalences were 2.1 (1.7 to 2.5)and 2.5 (1.4 to 3.5) respectively. Thesefindings are in accordance with studiesamong children and young adults from Fin-land and other Nordic countries.3–5 Thereported occurrences of asthma in thesetwin studies correspond to those found ingeneral populations. Although limitationsarise because of interstudy differences (suchas age range, definition of asthma, and studyperiod) these studies support our findingsamong older adults.
The reported differences in rates ofadmission to hospital may also be caused by
different use of medical care among twinsand singletons. Mothers of twins are on aver-age older than mothers of singletons, andthey usually also have other children. Theytherefore have more experience with chil-dren and their diseases. It is also probablethat, when one twin has been in hospital forasthma, parents do not seek help for his orher twin sibling so easily because the situationis already familiar and medication may evenbe available at home.Elisa Huovinen [email protected] of Public Health, University ofHelsinki, FIN-00014 Helsinki, Finland
Jaakko Kaprio professor of public [email protected] of Public Health and General Practice,University of Oulu, FIN-90014 Helsinki, Finland
1 Strachan DP, Moran SE, McInnery K, Smalls M. Reducedrisk of hospital admission for childhood asthma amongScottish twins: record linkage study. BMJ 2000;321:732-3.(23 September.)
2 Huovinen E, Kaprio J, Laitinen LA, Koskenvuo M.Incidence and prevalence of asthma among adult Finnishmen and women of the Finnish Twin Cohort from 1975 to1990, and their relation to hay fever and chronic bronchi-tis. Chest 1999;115:928-36.
3 Räsänen M, Laitinen T, Kaprio J, Koskenvuo M, LaitinenLA. Hay fever, asthma and number of older siblings—atwin study. Clin Exp Allergy 1997;27:515-8.
4 Skadhauge LR, Christensen K, Kyvik KO. Genetic andenvironmental influence on asthma: a population-basedstudy of 11,688 Danish twin pairs. Eur Respir J 1999;13:8-14.
5 Harris JR, Magnus P, Samuelsen SO, Tambs K. Noevidence for effects of family environment on asthma, aretrospective study of Norwegian twins. Am J Respir CritCare Med 1997;156:43-9.
Author’s reply
Editor—Huovinen and Kaprio present use-ful data suggesting that among adults there islittle difference in asthma prevalence betweentwins and singletons. There is growing recog-nition that wheezing illness in early child-hood (when most hospital admissions forasthma occur in the United Kingdom) maybe a different spectrum of disease to asthmain adulthood. This may explain the contrast-ing findings of our respective studies.
The three other studies cited byHuovinen and Kaprio did not compare twinsdirectly with singletons by using a standardmethod of identifying asthma, but simplycommented on the results from twin series inthe context of local prevalence studies, whichmay have used different case definitions. Thestrength of our study and that of Bråbäck et alis that identical methods of case ascertain-ment were used among twins and singletons,leading to less misleading comparisons.1
We alluded to the possibility thatpatterns of health service contact mighthave exaggerated the difference in admis-sion rates between twins and singletons.However, the cumulative risk of admissionfor asthma by age 10 years among Scottishsingletons born 1981-4 was only 2%, soit is unlikely that prior admission of theco-twin would influence asthma manage-ment in more than a small proportion oftwins.David Strachan professor of epidemiologyDepartment of Public Health Sciences, St George’sHospital Medical School, London SW17 0RE
1 Bråbäck L, Hedberg A. Perinatal risk factors for atopic dis-ease in conscripts. Clin Exp Allergy 1998;28:936-42.
Letters
556 BMJ VOLUME 322 3 MARCH 2001 bmj.com

Eradicating Helicobacter pyloriin non-ulcer dyspepsia may notbe cost effectiveEditor—Finding that patients with dyspep-sia gain modest benefits from eradication ofHelicobacter pylori, Moayyedi et al concludethat this intervention “may be cost effective.”1
This conclusion should be taken with quite abit of healthy scepticism. They say that onepatient benefiting out of 15 treated withantibiotics may represent good value formoney, depending on decision makers’ will-ingness to pay for relief of dyspepsia.However, the risks associated with theantibiotic treatment are not taken intoaccount in the economic model used.
The table summarises the results of twoof the included trials,2 3 showing an absoluteincrease in withdrawal from the trial due toadverse events. Number needed to harmvalues are very close to the number neededto treat found by Moayyedi et al, meaningthat of each 15 patients treated one couldbenefit but another one could experienceside effects leading to withdrawal from thetrial. Moreover, a message to test and eradi-cate H pylori in all patients with non-ulcerdyspepsia could lead to a long term risk ofantibiotic resistance.
Additionally, dyspepsia was “forced” intoa dichotomous outcome. There may bedifferent degrees of upper abdominal painor discomfort, so considering dyspepsia onlyas “present” or “absent” oversimplifies thepicture. In specifying a number needed totreat of 15, the authors cannot say whatimprovement is gained by patients whoresponded to treatment. If 15 patients aretreated and one of them benefits, how differ-ent is this one from the other 14? Data onquality of life included in the review seem toshow that there are no differences betweenthe eradication and control groups.
The studies included in this meta-analysis use quite different scales to measuredyspepsia. In the Glasgow scale, scores of0-1 out of 21 represent a favourableoutcome4; in some Likert scales, scores of0-1 out of 4 to 7 points represent the sameoutcome.2 3 The discriminative power ofthese scales is obviously very different, andcombining results derived from using suchscales may be problematic.
Eradicating H pylori does not seem todecrease the long term use of acid suppres-sive treatment. More than 50% of patientswith non-ulcer dyspepsia still take suchtreatment five years after the successfuleradication.5
Finally, most of the studies included inthis meta-analysis come from secondary
care. It may be difficult to generalise theseresults to primary care patients who maydiffer in terms of adherence to treatmentand severity of symptoms.Giulio Formoso [email protected]
Emilio Maestri consultantNicola Magrini head, Unit of Drug Evaluation andEvidence-Based Primary CareCentre for the Evaluation of Effectiveness of HealthCare, Viale Muratori 201, 41100 Modena, Italy
Maurizio Koch gastroenterologistLucio Capurso gastroenterologistDepartment of Gastroenterology, General HospitalS Filippo Neri, Rome, Italy
Alessandro Liberati professor of biostatisticsUniversity of Modena and Reggio Emilia, ViaUniversità 4, 41100 Modena
1 Moayyedi P, Soo S, Deeks J, Forman D, Mason J, Innes M, etal. Systematic review and economic evaluation ofHelicobacter pylori eradication treatment for non-ulcerdyspepsia. BMJ 2000;321:659-64. (16 September.)
2 Blum AL, Talley NJ, O’Morain C, van Zanten SV, Labenz J,Stolte M, et al. Lack of effect of treating Helicobacter pyloriin patients with nonulcer dyspepsia. Omeprazole plusClarithromycin and Amoxicillin Effect One Year afterTreatment (OCAY) Study Group. N Engl J Med1998;339:1875-81.
3 Talley NJ, Vakil N, Ballard ED 2nd, Fennerty MB. Absenceof benefit of eradicating Helicobacter pylori in patientswith nonulcer dyspepsia. N Engl J Med 1999;341:1106-11.
4 El-Omar EM, Banerjee S, Wirz A, McColl KE. The Glasgowdyspepsia severity score—a tool for the global measure-ment of dyspepsia. Eur J Gastroenterol Hepatol 1996;8:967-71.
5 Tan AC, Hartog GD, Mulder CJ. Eradication ofHelicobacter pylori does not decrease the long-term use ofacid-suppressive medication. Aliment Pharmacol Ther1999;13:1519-22.
Tobacco industry must notdump its high nitrosaminetobacco on poor countriesEditor—In the late 1970s Hoffmann’s groupdescribed the carcinogenic properties ofthe tobacco-specific nitrosamines including4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone and N’-nitrosonornicotine in aseries of experiments.1 These substances areformed during the curing process by achemical reaction between nicotine andnitrate. They are present in cigarettes,chewing tobacco, and snuff. One of thesubstances, 4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone, is of particular inter-est as it is a powerful lung adenocarcinogenin animals regardless of route of administra-tion. Adducts of N′-nitrosonornicotine and4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone are seen in the lungs of humansand animals and are closely correlated withcarcinogenicity.2
Hoffmann and Hoffmann later pub-lished analyses of a single regular cigarettebrand in the United States. In 1995 theyshowed an increase (of about half) in
4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone in the smoke during a timewhen the benz(a)pyrene level was stable.3
This was associated with an increase in thenitrate content of tobacco in the UnitedStates over that time and also with a fall inFederal Trade Commission measures of tarand nicotine.
The increase in 4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone (andother tobacco-specific nitrosamines) wasalso associated with the significant increasein the relative and absolute risk of adenocar-cinoma of the lung seen in the United Statesand other countries.3 It has been postulatedthat the increase in tobacco-specific nitro-samines (together with overinhalation dueto compensatory smoking behaviour) is atleast partly responsible for the increase inadenocarcinoma.3
Nitrosamine levels vary widely bothwithin brands and between countries.4 Thelevels of tobacco-specific nitrosamines insmoke have always been under the controlof the manufacturer. In 2000, new curingtechnology that leads to major reductions intobacco-specific nitrosamines was intro-duced in the United States.5 This develop-ment raises serious questions. Will surplushigh nitrosamine tobacco be exported? If sowill it go to countries, such as China, wherenitrosamines are already lower than they arein the United States? Will the global compa-nies use this technology worldwide? If not,why not?
Removing nitrosamines might wellreduce the incidence of adenocarcinomaover time. Only an experiment on continu-ing smokers will tell, and this should be setup. Removing nitrosamines will not affectthe epidemic of other cancers and diseasesassociated with tobacco, but there can be lit-tle excuse for not insisting that the tobaccoindustry uses this technology globally anddoes not dump its high nitrosamine tobaccoon poor countries. Every national govern-ment should take note.Nigel Gray senior research [email protected] Boyle directorDivision of Epidemiology and Biostatistics,European Institute of Oncology, 20141, Milan, Italy
1 Hecht SS, Chen CB, Hirota N, Ornaf RM, Tso TC,Hoffmann D. Tobacco-specific nitrosamines: formationfrom nicotine in vitro and during tobacco curing and car-cenogenicity in strain A mice. J Natl Cancer Inst1978;60:819-24.
2 Hecht SS. DNA adduct formation from tobacco-specificN-nitrosamines. Mutation Research 1999;424:127-42.
3 Hoffmann D, Hoffmann I. The changing cigarette,1950-1995. J Toxicol Environ Health 1997;50:307-64.
4 Gray N, Zaridse D, Robertson C, Krivosheeva L, SigachevaN, et al. Variation within global cigarette brands in tar,nicotine, and certain nitrosamines: analytic study. TobaccoControl 2000;9:351.
5 Fisher B. Curing the TSNA problem. Tobacco Reporter 2000Aug:53-6.
Withdrawals owing to side effects and numbers needed to harm in two trials of Helicobacter pylorieradication (follow up of one year)
Study
Withdrawal owing to side effects (%) Increase inabsolute risk No needed to harmEradication group Control group
Blum et al2 7 1 (omeprazole) 6.0 17
Talley et al3 4 0 (placebo) 4.0 25
There were 348 participants in the Blum et al study and 170 in the Talley et al study.Correspondence submitted electronicallyis available on our website
Letters
557BMJ VOLUME 322 3 MARCH 2001 bmj.com