
Epilepsy in ring 14 chromosome syndrome
8
Review Epilepsy in ring 14 chromosome syndrome Nicola Specchio a, ⁎, Marina Trivisano b , Domenico Serino a , Simona Cappelletti c , Antonio Carotenuto d , Dianela Claps a , Carlo Efisio Marras e , Lucia Fusco a , Maurizio Elia f , Federico Vigevano a a Neurology Unit, Bambino Gesù Children's Hospital IRCCS, Rome, Italy b Clinic for Nervous System Diseases, University of Foggia, Foggia, Italy c Unit of Clinical Psychology, Bambino Gesù Children's Hospital, IRCCS, Rome, Italy d Medical School, University of Naples, Naples, Italy e Neurosurgery Unit, Department of Neuroscience, Bambino Gesu' Children's Hospital, IRCCS, Rome, Italy f Unit of Neurology and Clinical Neurophysiopathology, Oasi Institute for Research on Mental Retardation and Brain Aging (IRCCS), Troina (EN), Italy abstract article info Article history: Received 27 June 2012 Revised 20 September 2012 Accepted 22 September 2012 Available online 14 November 2012 Keywords: Epilepsy Ring chromosome 14 Seizure semiology EEG finding Drug-resistant epilepsy Ring chromosome 14 [r(14)] is a rare disorder. The aim of this study was to describe two new cases of r(14) drug-resistant epilepsy, and, through an extensive review of literature, highlight those epileptological features which are more commonly found and which may help in early diagnosis, genetic counseling, and treatment. Epilepsy onset in r(14) syndrome takes place during the first year of life; seizures are generalized or focal and less frequently myoclonic. Seizures might be induced by fever. Focal seizures are characterized by staring, eye or head deviation, respiratory arrest, swallowing, and hypertonia/hypotonia or clonic movements. Ictal EEG might show both focal and diffuse discharges. Interictal EEG reveals mainly focal abnormalities. Mental retar- dation represents a constant feature. Neurological assessment yields a delay in motor skill acquisition and less frequently both pyramidal and cerebellar signs. Dysmorphic features are evident in the majority of cases. Epilepsy associated with r(14) has many features that entail a challenging diagnostic process. The reported cases of r(14)-related epilepsy seem to highlight a series of common elements which may be helpful in pointing the clinician towards a correct diagnosis. © 2012 Elsevier Inc. All rights reserved. 1. Introduction Ring chromosome 14 [r(14)] is a rare disorder described for the first time by Gilgenkrantz et al., in 1971 [1]. It is characterized by microcephaly, developmental delay, drug-resistant epilepsy, and ocular abnormalities, especially retinal dystrophy [2]. Dysmorphic features usually consist in epi-/telecanthi, broad/flat nasal bridge, high and prominent forehead, downward slanting eyes, large low- set ears, and blepharophimosis [3]. Epilepsy onset usually takes place during the first year of life with a high variety of seizure types. Seizures may be generalized tonic– clonic, complex partial, and minor motor [4]. The interictal EEG pattern can be normal or characterized by multifocal spikes and spike-and-wave complexes. Seizures are often drug-resistant and the outcome is severe [5]. Seizure semiology of r(14)-related epilepsy is extremely variable. The aim of this report is to describe two new cases of r(14) drug- resistant epilepsy, and, through an extensive review of literature, highlight those epileptological features which are more commonly found among such cases. In this way, we construct a hypothetical patient's profile, which may help in early diagnosis, genetic counseling, and treatment. 2. Methods We report in detail two new cases of r(14) including seizure semi- ology, interictal and ictal EEG findings, treatment, and cognitive and morphological assessment. Moreover we reviewed all published cases in which an association with epilepsy was reported. Since its first description, 59 cases have been published (for references see Table 1). We did not include the extensive series reported by Zollino et al. [2] because epilepsy features or EEG findings were not specified. 3. Case reports Table 1 summarizes the clinical findings in relation to the two new cases of r(14). All clinical data, EEG features, treatments, neurological conditions, the presence of associated features, and neuroimaging are reported. Moreover, a detailed description of seizure semiology is given. Epilepsy & Behavior 25 (2012) 585–592 ⁎ Corresponding author at: Division of Neurology, Bambino Gesù Children's Hospital- IRCCS, P.zza S. Onofrio 4, 00165, Rome, Italy. Fax: +39 0668592463. E-mail address: [email protected] (N. Specchio). 1525-5050/$ – see front matter © 2012 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.yebeh.2012.09.032 Contents lists available at SciVerse ScienceDirect Epilepsy & Behavior journal homepage: www.elsevier.com/locate/yebeh
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Epilepsy in ring 14 chromosome syndrome

Epilepsy & Behavior 25 (2012) 585–592
Contents lists available at SciVerse ScienceDirect
Epilepsy & Behavior
j ourna l homepage: www.e lsev ie r .com/ locate /yebeh
Review
Epilepsy in ring 14 chromosome syndrome
Nicola Specchio a,⁎, Marina Trivisano b, Domenico Serino a, Simona Cappelletti c, Antonio Carotenuto d,Dianela Claps a, Carlo Efisio Marras e, Lucia Fusco a, Maurizio Elia f, Federico Vigevano a
a Neurology Unit, Bambino Gesù Children's Hospital IRCCS, Rome, Italyb Clinic for Nervous System Diseases, University of Foggia, Foggia, Italyc Unit of Clinical Psychology, Bambino Gesù Children's Hospital, IRCCS, Rome, Italyd Medical School, University of Naples, Naples, Italye Neurosurgery Unit, Department of Neuroscience, Bambino Gesu' Children's Hospital, IRCCS, Rome, Italyf Unit of Neurology and Clinical Neurophysiopathology, Oasi Institute for Research on Mental Retardation and Brain Aging (IRCCS), Troina (EN), Italy
⁎ Corresponding author at: Division of Neurology, BamIRCCS, P.zza S. Onofrio 4, 00165, Rome, Italy. Fax: +39 0
E-mail address: [email protected] (N. Specch
1525-5050/$ – see front matter © 2012 Elsevier Inc. Allhttp://dx.doi.org/10.1016/j.yebeh.2012.09.032
a b s t r a c t
a r t i c l e i n f oArticle history:Received 27 June 2012Revised 20 September 2012Accepted 22 September 2012Available online 14 November 2012
Keywords:EpilepsyRing chromosome 14Seizure semiologyEEG findingDrug-resistant epilepsy
Ring chromosome 14 [r(14)] is a rare disorder. The aim of this study was to describe two new cases of r(14)drug-resistant epilepsy, and, through an extensive review of literature, highlight those epileptologicalfeatures which are more commonly found and which may help in early diagnosis, genetic counseling, andtreatment.Epilepsy onset in r(14) syndrome takes place during the first year of life; seizures are generalized or focal andless frequently myoclonic. Seizures might be induced by fever. Focal seizures are characterized by staring, eyeor head deviation, respiratory arrest, swallowing, and hypertonia/hypotonia or clonic movements. Ictal EEGmight show both focal and diffuse discharges. Interictal EEG reveals mainly focal abnormalities. Mental retar-dation represents a constant feature. Neurological assessment yields a delay in motor skill acquisition andless frequently both pyramidal and cerebellar signs. Dysmorphic features are evident in the majority ofcases. Epilepsy associated with r(14) has many features that entail a challenging diagnostic process. Thereported cases of r(14)-related epilepsy seem to highlight a series of common elements which may be helpfulin pointing the clinician towards a correct diagnosis.
© 2012 Elsevier Inc. All rights reserved.
1. Introduction
Ring chromosome 14 [r(14)] is a rare disorder described for thefirst time by Gilgenkrantz et al., in 1971 [1]. It is characterized bymicrocephaly, developmental delay, drug-resistant epilepsy, andocular abnormalities, especially retinal dystrophy [2]. Dysmorphicfeatures usually consist in epi-/telecanthi, broad/flat nasal bridge,high and prominent forehead, downward slanting eyes, large low-set ears, and blepharophimosis [3].
Epilepsy onset usually takes place during the first year of life witha high variety of seizure types. Seizures may be generalized tonic–clonic, complex partial, and minor motor [4]. The interictal EEGpattern can be normal or characterized by multifocal spikes andspike-and-wave complexes. Seizures are often drug-resistant andthe outcome is severe [5].
Seizure semiology of r(14)-related epilepsy is extremely variable.The aim of this report is to describe two new cases of r(14) drug-resistant epilepsy, and, through an extensive review of literature,highlight those epileptological features which are more commonly
bino Gesù Children's Hospital-668592463.io).
rights reserved.
found among such cases. In this way, we construct a hypotheticalpatient's profile, which may help in early diagnosis, genetic counseling,and treatment.
2. Methods
We report in detail two new cases of r(14) including seizure semi-ology, interictal and ictal EEG findings, treatment, and cognitive andmorphological assessment. Moreover we reviewed all publishedcases in which an association with epilepsy was reported. Since itsfirst description, 59 cases have been published (for references seeTable 1). We did not include the extensive series reported by Zollinoet al. [2] because epilepsy features or EEG findings were not specified.
3. Case reports
Table 1 summarizes the clinical findings in relation to the two newcases of r(14). All clinical data, EEG features, treatments, neurologicalconditions, the presence of associated features, and neuroimaging arereported. Moreover, a detailed description of seizure semiology isgiven.

Fig. 1. Ictal EEG of case #1. The seizure starts with a diffuse flattening soon followed by synchronous bilateral and rhythmic slow waves of higher amplitude, bilaterally over the frontal regions. The seizure appears during sleep and ischaracterized by eye opening, fixed gaze, and upper limb hypertonia. It has a duration of 1 min.
586N.Specchio
etal./
Epilepsy&
Behavior25
(2012)585
–592

Fig. 2. A–E. Ictal EEG of case #2. (A) Theta activity is evident over the right temporo-parieto-occipital region. After 1 min, it tends to become rhythmic (B). After 3 min, the patient awakes (C), and more prominent high amplitude slow wavesare evident. The patient has left eye deviation, and mild upper limb hypertonia is evident over EMG traces; (D) after 5 min from the onset, EEG shows rhythmic spikes in the same region persisting until the end of the event (E) which takesplace 7 min after onset. F. Ictal EEG of tonic seizure during sleep. Diffuse decremental activity is evident, followed by low voltage fast activity and by rhythmic spikes over the frontal and central areas bilaterally. G. Interictal EEG during sleepshowing high amplitude slow waves over the frontal regions bilaterally.
587N.Specchio
etal./
Epilepsy&
Behavior25
(2012)585
–592

Table 1Clinical description of two new cases of ring 14 chromosome.
Case report #1 Case report #2
Sex/age F/8.6 y M/5 yCytogenetic finding 46,XX,r(14)(p11;q32.33), FISH: del14q32.33-14qter 46,XY,r(14)(p11q32)[28]/45,XY,-14[4]Delivery and neonatal weight Spontaneous at term, 2650 gr Spontaneous at term, 2970 grFamilial history for seizures Not reported Mother: seizures induced by fever at the age of 2 and 6 mSeizure onset 8 m 9 mSeizure types at onset Generalized tonic seizures (10–30 secs), sometimes
followed by clonic jerks and perioral cyanosisCluster of focal seizures during a mild febrile episode
Fever Yes YesSeizures types during follow-up 1. Psychomotor arrest and eye deviation (alternatively
towards the left and the right side) both during awakeand sleep, with 5–6 day seizure clusters triggered byfever about every 30 days2. Focal seizures with secondary generalization3. Tonic seizures during sleep4. Myoclonic seizures during awake
1. Fixed gaze, perioral cyanosis, swallowing, and mildhypertonia of upper and lower limbs2. Episodes of upper limb jerks mainly during sleepand sometimes in clusters3. Tonic seizures during sleep
Status epilepticus Yes YesEEG ictal Rhythmic slow waves over bilateral frontal and
central areas preceded by a diffuse decrementalactivity (Fig. 1)
Posterior focal theta waves intermingled with spikesincreasing in amplitude and decreasing in frequency(Figs. 2A–E) or a diffuse decremental activity followedby low-voltage fast activity and bi-frontal spikes intonic seizures (Fig. 2F)
EEG interictal Slowing background activity associated with slowwaves and isolated spikes over bilateral frontal andtemporal regions
Slowing background activity associated with slowwaves and isolated spikes over bilateral frontal regions,which tended to increase during sleep (Fig. 2G)
Seizure-free period Max 6 m Max 2 mTreatment VPA, GVG, CBZ, TPM, CZP, LEV CBZ, CLB, LEV, VPA, PB, LTG, OXC, TPM, ketogenic dietBetter treatment association VPA, CLB, STP (significant reduction of seizure frequency,
in addition to a reduction of duration of clusters and norecurrence of SE)
VPA, TPM, ACTH (determined a 2-month seizure-free period)
Other genetic tests SCN1A, PCDH19 SCN1A, FISH Chromosome 15, Fra-X, UBE3A, MECP2, PCDH19Neurological features Walking at 18 m, mild ataxia was evident, language delay Severe ataxia, hypotonusNeuropsychological assessment Griffiths Developmental Scales: IQ 55 (4 y),
Stanford–Binet Scale: age-equivalent score of2y11m (5 y), Vineland Adaptive Behavior Scales:age of 2y5m (5 y)
BSID II Mental Scale at 18 m highlights an age-equivalentscore of 9 m
Associated features Hypertelorism, epicanthal folds, small palpebralfissures, low-set ears, and flat nasal bridge
Bilateral epicanthal folds, broad nasal bridge, high forehead,strabismus, short neck
Neuroimaging Mild dilatation of the left temporal horn (MR) Mild bilateral fronto-temporal-parietal atrophy (MR)
F = female, M = male, y = years, m = months, gr = grams, secs = seconds, max = maximum, VPA = valproate, GVG = Gamma-vinyl-GABA, CBZ = carbamazepine, TPM =topiramate, CZP = clonazepam, LEV = levetiracetam, CLB = clobazam, PB = phenobarbital, LTG = lamotrigine, OXC = oxcarbazepine, ACTH = adrenocorticotropic hormone,SE = status epilepticus, IQ = intelligent quotient, BSID II = Bayley Scale for Infant Development-Second Edition, MR = magnetic resonance.
588 N. Specchio et al. / Epilepsy & Behavior 25 (2012) 585–592
4. Review of previously reported cases
Table 2 shows all published cases [1,6–30].We are reporting 39 pre-viously published cases. Mean age at onset of epilepsy in all selectedcases was 9.4 months (range 0–30 months); seizures were reportedas generalized in 24 cases, focal in 19 cases, and myoclonic in 5, andless frequently, absences and atonic seizures were also reported. In 6cases (15%), seizures were induced by fever. Fifteen patients experi-enced two or more types of seizures. Clusters were reported in 5cases. Focal seizures, reported mainly as complex partial seizures,were characterized by staring, eye or head deviation, respiratory arrest,swallowing, and hypertonia/hypotonia or clonic movements. Ictal EEGwas reported in 9 cases: discharge was focal in 3 and diffuse in another6 cases. Interictal EEG was characterized mainly by the recurrence offocal abnormalities, spikes or slow waves in almost 50% of cases, andonly in 5 cases were they described as generalized. Data on cognitivedevelopment were available in 34 out of 39 cases. Mental retardationwas reported in all cases but 1: in 15 of them (38.4%), it was describedas severe; in 6 (15.3%), it was mild–moderate; and in 12 cases, thedegree of mental retardation was not specified. Microcephaly wasdescribed in 14 cases, motor delay in 24, hypotonus/hypertonia in8, and ataxia in 6 cases. Intentional tremor and nystagmus werealso reported. Neuroimaging was reported in 24 cases and showedmild to moderate atrophy in 13 (54%), and corpus callosum hypopla-sia in 1 (4%) case. It was reported as normal in the remaining cases.Dysmorphic features were reported in 30 cases.
5. Discussion
Ring 14 chromosome results from a breakage and rejoining of theshort and long arms of the chromosome, leading to deletion of a vari-able amount of chromosome [24]. A ring chromosome is unstable andgenerates different degrees ofmosaicism that could explain phenotypicvariability in r(14) patients. The size of deleted regions in patients withr(14) is the main characteristic of phenotypic variability.
Epilepsy associatedwith ring chromosome 14 hasmany features thatentail a challenging diagnostic process, inwhich heterogeneity in presen-tation of clinical characteristics is probably themost challenging factor ofall. In relation to seizure semiology and EEG findings, presentation of ep-ilepsy in our cases seems to be similar to that reported by Ville et al. [28].
Establishing key elements that may contribute to the developmentof a diagnostic flow chart is not an easy task but is fundamental forearly diagnosis and treatment.
We tried to analyze those features that seemed to be more con-stantly found in patients with ring chromosome 14 and which maybe used as landmarks in the diagnostic process itself.
The first important factor seems to be the age at onset: eventhough there is certain variability, age at onset is in most cases withinthe first year of life.
Seizure presentation shows great variability, but some recurrentfactors may be taken into account. As mentioned above, review of lit-erature highlights how epilepsy onset in ring chromosome 14 is typ-ically characterized by drug-resistant tonic-clonic seizures, complex
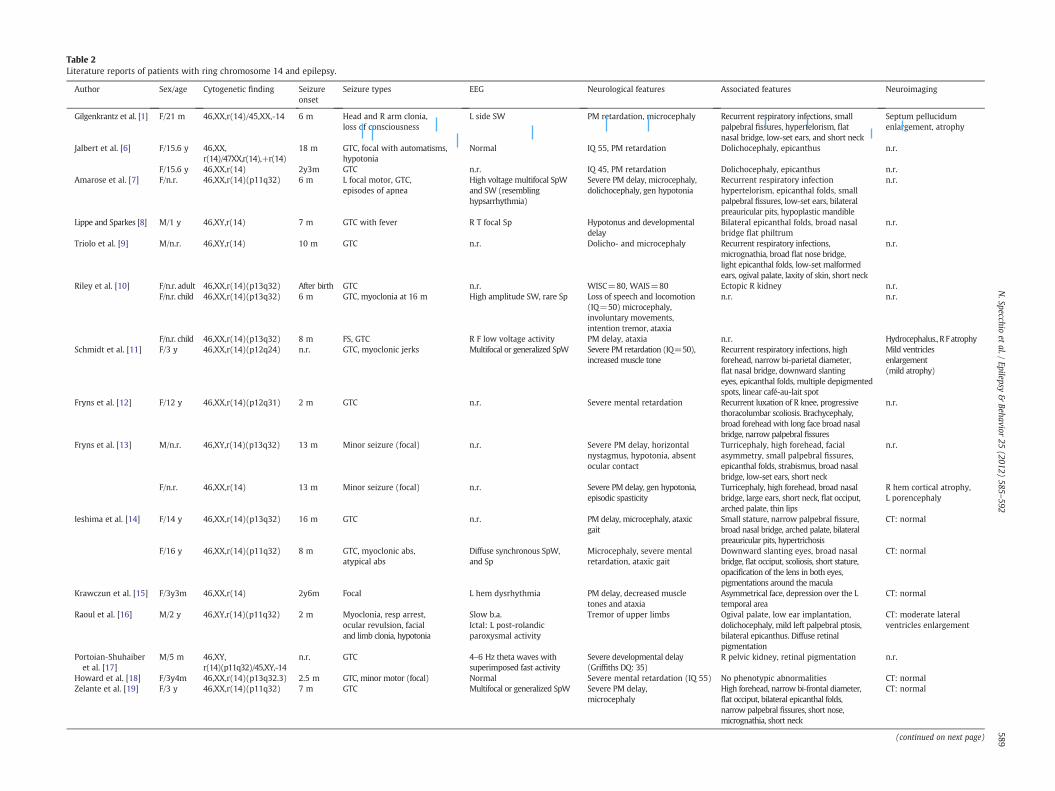
Table 2Literature reports of patients with ring chromosome 14 and epilepsy.
Author Sex/age Cytogenetic finding Seizureonset
Seizure types EEG Neurological features Associated features Neuroimaging
Gilgenkrantz et al. [1] F/21 m 46,XX,r(14)/45,XX,-14 6 m Head and R arm clonia,loss of consciousness
L side SW PM retardation, microcephaly Recurrent respiratory infections, smallpalpebral fissures, hypertelorism, flatnasal bridge, low-set ears, and short neck
Septum pellucidumenlargement, atrophy
Jalbert et al. [6] F/15.6 y 46,XX,r(14)/47XX,r(14),+r(14)
18 m GTC, focal with automatisms,hypotonia
Normal IQ 55, PM retardation Dolichocephaly, epicanthus n.r.
F/15.6 y 46,XX,r(14) 2y3m GTC n.r. IQ 45, PM retardation Dolichocephaly, epicanthus n.r.Amarose et al. [7] F/n.r. 46,XX,r(14)(p11q32) 6 m L focal motor, GTC,
episodes of apneaHigh voltage multifocal SpWand SW (resemblinghypsarrhythmia)
Severe PM delay, microcephaly,dolichocephaly, gen hypotonia
Recurrent respiratory infectionhypertelorism, epicanthal folds, smallpalpebral fissures, low-set ears, bilateralpreauricular pits, hypoplastic mandible
n.r.
Lippe and Sparkes [8] M/1 y 46,XY,r(14) 7 m GTC with fever R T focal Sp Hypotonus and developmentaldelay
Bilateral epicanthal folds, broad nasalbridge flat philtrum
n.r.
Triolo et al. [9] M/n.r. 46,XY,r(14) 10 m GTC n.r. Dolicho- and microcephaly Recurrent respiratory infections,micrognathia, broad flat nose bridge,light epicanthal folds, low-set malformedears, ogival palate, laxity of skin, short neck
n.r.
Riley et al. [10] F/n.r. adult 46,XX,r(14)(p13q32) After birth GTC n.r. WISC=80, WAIS=80 Ectopic R kidney n.r.F/n.r. child 46,XX,r(14)(p13q32) 6 m GTC, myoclonia at 16 m High amplitude SW, rare Sp Loss of speech and locomotion
(IQ=50) microcephaly,involuntary movements,intention tremor, ataxia
n.r. n.r.
F/n.r. child 46,XX,r(14)(p13q32) 8 m FS, GTC R F low voltage activity PM delay, ataxia n.r. Hydrocephalus., R F atrophySchmidt et al. [11] F/3 y 46,XX,r(14)(p12q24) n.r. GTC, myoclonic jerks Multifocal or generalized SpW Severe PM retardation (IQ=50),
increased muscle toneRecurrent respiratory infections, highforehead, narrow bi-parietal diameter,flat nasal bridge, downward slantingeyes, epicanthal folds, multiple depigmentedspots, linear café-au-lait spot
Mild ventriclesenlargement(mild atrophy)
Fryns et al. [12] F/12 y 46,XX,r(14)(p12q31) 2 m GTC n.r. Severe mental retardation Recurrent luxation of R knee, progressivethoracolumbar scoliosis. Brachycephaly,broad forehead with long face broad nasalbridge, narrow palpebral fissures
n.r.
Fryns et al. [13] M/n.r. 46,XY,r(14)(p13q32) 13 m Minor seizure (focal) n.r. Severe PM delay, horizontalnystagmus, hypotonia, absentocular contact
Turricephaly, high forehead, facialasymmetry, small palpebral fissures,epicanthal folds, strabismus, broad nasalbridge, low-set ears, short neck
n.r.
F/n.r. 46,XX,r(14) 13 m Minor seizure (focal) n.r. Severe PM delay, gen hypotonia,episodic spasticity
Turricephaly, high forehead, broad nasalbridge, large ears, short neck, flat occiput,arched palate, thin lips
R hem cortical atrophy,L porencephaly
Ieshima et al. [14] F/14 y 46,XX,r(14)(p13q32) 16 m GTC n.r. PM delay, microcephaly, ataxicgait
Small stature, narrow palpebral fissure,broad nasal bridge, arched palate, bilateralpreauricular pits, hypertrichosis
CT: normal
F/16 y 46,XX,r(14)(p11q32) 8 m GTC, myoclonic abs,atypical abs
Diffuse synchronous SpW,and Sp
Microcephaly, severe mentalretardation, ataxic gait
Downward slanting eyes, broad nasalbridge, flat occiput, scoliosis, short stature,opacification of the lens in both eyes,pigmentations around the macula
CT: normal
Krawczun et al. [15] F/3y3m 46,XX,r(14) 2y6m Focal L hem dysrhythmia PM delay, decreased muscletones and ataxia
Asymmetrical face, depression over the Ltemporal area
CT: normal
Raoul et al. [16] M/2 y 46,XY,r(14)(p11q32) 2 m Myoclonia, resp arrest,ocular revulsion, facialand limb clonia, hypotonia
Slow b.a.Ictal: L post-rolandicparoxysmal activity
Tremor of upper limbs Ogival palate, low ear implantation,dolichocephaly, mild left palpebral ptosis,bilateral epicanthus. Diffuse retinalpigmentation
CT: moderate lateralventricles enlargement
Portoian-Shuhaiberet al. [17]
M/5 m 46,XY,r(14)(p11q32)/45,XY,-14
n.r. GTC 4–6 Hz theta waves withsuperimposed fast activity
Severe developmental delay(Griffiths DQ: 35)
R pelvic kidney, retinal pigmentation n.r.
Howard et al. [18] F/3y4m 46,XX,r(14)(p13q32.3) 2.5 m GTC, minor motor (focal) Normal Severe mental retardation (IQ 55) No phenotypic abnormalities CT: normalZelante et al. [19] F/3 y 46,XX,r(14)(p11q32) 7 m GTC Multifocal or generalized SpW Severe PM delay,
microcephalyHigh forehead, narrow bi-frontal diameter,flat occiput, bilateral epicanthal folds,narrow palpebral fissures, short nose,micrognathia, short neck
CT: normal
(continued on next page)
589N.Specchio
etal./
Epilepsy&
Behavior25
(2012)585
–592
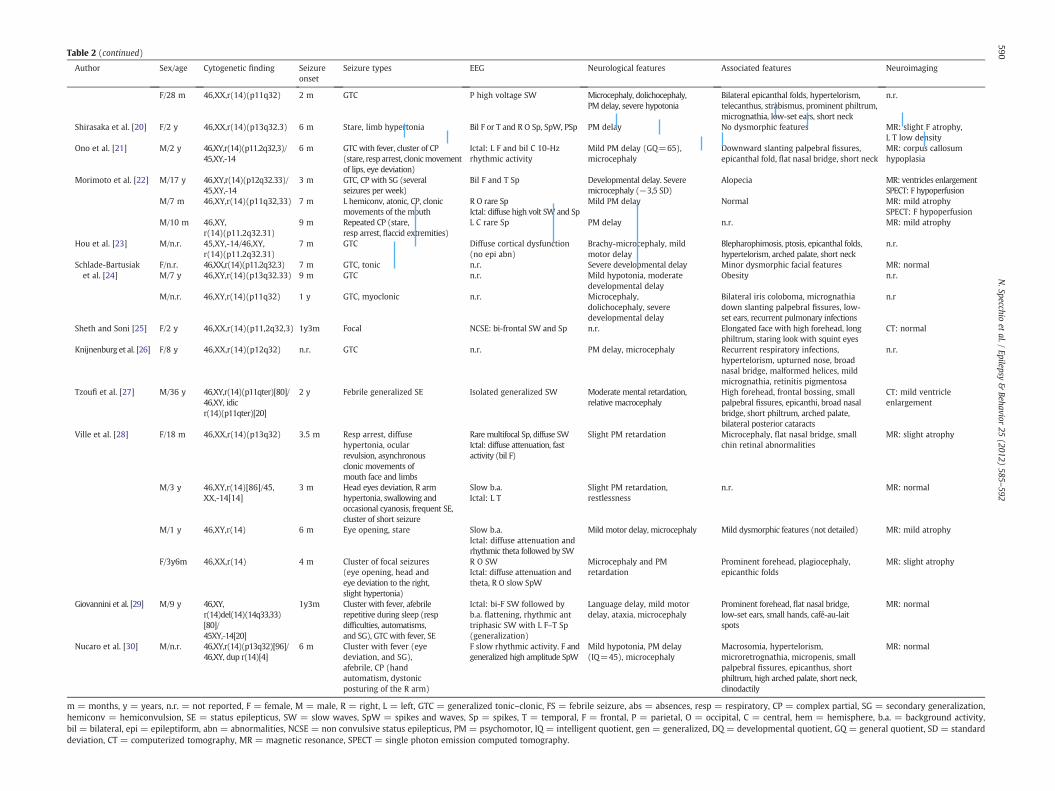
Table 2 (continued)
Author Sex/age Cytogenetic finding Seizureonset
Seizure types EEG Neurological features Associated features Neuroimaging
F/28 m 46,XX,r(14)(p11q32) 2 m GTC P high voltage SW Microcephaly, dolichocephaly,PM delay, severe hypotonia
Bilateral epicanthal folds, hypertelorism,telecanthus, strabismus, prominent philtrum,micrognathia, low-set ears, short neck
n.r.
Shirasaka et al. [20] F/2 y 46,XX,r(14)(p13q32.3) 6 m Stare, limb hypertonia Bil F or T and R O Sp, SpW, PSp PM delay No dysmorphic features MR: slight F atrophy,L T low density
Ono et al. [21] M/2 y 46,XY,r(14)(p11.2q32,3)/45,XY,-14
6 m GTC with fever, cluster of CP(stare, resp arrest, clonicmovementof lips, eye deviation)
Ictal: L F and bil C 10-Hzrhythmic activity
Mild PM delay (GQ=65),microcephaly
Downward slanting palpebral fissures,epicanthal fold, flat nasal bridge, short neck
MR: corpus callosumhypoplasia
Morimoto et al. [22] M/17 y 46,XY,r(14)(p12q32.33)/45,XY,-14
3 m GTC, CP with SG (severalseizures per week)
Bil F and T Sp Developmental delay. Severemicrocephaly (−3,5 SD)
Alopecia MR: ventricles enlargementSPECT: F hypoperfusion
M/7 m 46,XY,r(14)(p11q32,33) 7 m L hemiconv, atonic, CP, clonicmovements of the mouth
R O rare SpIctal: diffuse high volt SW and Sp
Mild PM delay Normal MR: mild atrophySPECT: F hypoperfusion
M/10 m 46,XY,r(14)(p11.2q32.31)
9 m Repeated CP (stare,resp arrest, flaccid extremities)
L C rare Sp PM delay n.r. MR: mild atrophy
Hou et al. [23] M/n.r. 45,XY,-14/46,XY,r(14)(p11.2q32.31)
7 m GTC Diffuse cortical dysfunction(no epi abn)
Brachy-microcephaly, mildmotor delay
Blepharophimosis, ptosis, epicanthal folds,hypertelorism, arched palate, short neck
n.r.
Schlade-Bartusiaket al. [24]
F/n.r. 46,XX,r(14)(p11.2q32.3) 7 m GTC, tonic n.r. Severe developmental delay Minor dysmorphic facial features MR: normalM/7 y 46,XY,r(14)(p13q32.33) 9 m GTC n.r. Mild hypotonia, moderate
developmental delayObesity n.r.
M/n.r. 46,XY,r(14)(p11q32) 1 y GTC, myoclonic n.r. Microcephaly,dolichocephaly, severedevelopmental delay
Bilateral iris coloboma, micrognathiadown slanting palpebral fissures, low-set ears, recurrent pulmonary infections
n.r
Sheth and Soni [25] F/2 y 46,XX,r(14)(p11,2q32,3) 1y3m Focal NCSE: bi-frontal SW and Sp n.r. Elongated face with high forehead, longphiltrum, staring look with squint eyes
CT: normal
Knijnenburg et al. [26] F/8 y 46,XX,r(14)(p12q32) n.r. GTC n.r. PM delay, microcephaly Recurrent respiratory infections,hypertelorism, upturned nose, broadnasal bridge, malformed helices, mildmicrognathia, retinitis pigmentosa
n.r.
Tzoufi et al. [27] M/36 y 46,XY,r(14)(p11qter)[80]/46,XY, idicr(14)(p11qter)[20]
2 y Febrile generalized SE Isolated generalized SW Moderate mental retardation,relative macrocephaly
High forehead, frontal bossing, smallpalpebral fissures, epicanthi, broad nasalbridge, short philtrum, arched palate,bilateral posterior cataracts
CT: mild ventricleenlargement
Ville et al. [28] F/18 m 46,XX,r(14)(p13q32) 3.5 m Resp arrest, diffusehypertonia, ocularrevulsion, asynchronousclonic movements ofmouth face and limbs
Rare multifocal Sp, diffuse SWIctal: diffuse attenuation, fastactivity (bil F)
Slight PM retardation Microcephaly, flat nasal bridge, smallchin retinal abnormalities
MR: slight atrophy
M/3 y 46,XY,r(14)[86]/45,XX,-14[14]
3 m Head eyes deviation, R armhypertonia, swallowing andoccasional cyanosis, frequent SE,cluster of short seizure
Slow b.a.Ictal: L T
Slight PM retardation,restlessness
n.r. MR: normal
M/1 y 46,XY,r(14) 6 m Eye opening, stare Slow b.a.Ictal: diffuse attenuation andrhythmic theta followed by SW
Mild motor delay, microcephaly Mild dysmorphic features (not detailed) MR: mild atrophy
F/3y6m 46,XX,r(14) 4 m Cluster of focal seizures(eye opening, head andeye deviation to the right,slight hypertonia)
R O SWIctal: diffuse attenuation andtheta, R O slow SpW
Microcephaly and PMretardation
Prominent forehead, plagiocephaly,epicanthic folds
MR: slight atrophy
Giovannini et al. [29] M/9 y 46,XY,r(14)del(14)(14q33,33)[80]/45XY,-14[20]
1y3m Cluster with fever, afebrilerepetitive during sleep (respdifficulties, automatisms,and SG), GTC with fever, SE
Ictal: bi-F SW followed byb.a. flattening, rhythmic anttriphasic SW with L F–T Sp(generalization)
Language delay, mild motordelay, ataxia, microcephaly
Prominent forehead, flat nasal bridge,low-set ears, small hands, café-au-laitspots
MR: normal
Nucaro et al. [30] M/n.r. 46,XY,r(14)(p13q32)[96]/46,XY, dup r(14)[4]
6 m Cluster with fever (eyedeviation, and SG),afebrile, CP (handautomatism, dystonicposturing of the R arm)
F slow rhythmic activity. F andgeneralized high amplitude SpW
Mild hypotonia, PM delay(IQ=45), microcephaly
Macrosomia, hypertelorism,microretrognathia, micropenis, smallpalpebral fissures, epicanthus, shortphiltrum, high arched palate, short neck,clinodactily
MR: normal
m = months, y = years, n.r. = not reported, F = female, M = male, R = right, L = left, GTC = generalized tonic–clonic, FS = febrile seizure, abs = absences, resp = respiratory, CP = complex partial, SG = secondary generalization,hemiconv = hemiconvulsion, SE = status epilepticus, SW = slow waves, SpW = spikes and waves, Sp = spikes, T = temporal, F = frontal, P = parietal, O = occipital, C = central, hem = hemisphere, b.a. = background activity,bil = bilateral, epi = epileptiform, abn = abnormalities, NCSE = non convulsive status epilepticus, PM = psychomotor, IQ = intelligent quotient, gen = generalized, DQ = developmental quotient, GQ = general quotient, SD = standarddeviation, CT = computerized tomography, MR = magnetic resonance, SPECT = single photon emission computed tomography.
590N.Specchio
etal./
Epilepsy&
Behavior25
(2012)585
–592

591N. Specchio et al. / Epilepsy & Behavior 25 (2012) 585–592
partial seizures (CPS), and minor motor seizures, as it was in ourpatients. Evolution of seizure pattern and semiology is extremelyvariable; however, a gradual progression and/or stabilization towardsCPS seems to be more common. Even if no specific pattern could beevidenced, focal seizures during the first year of life seem to be ahallmark of the disease; even though in some reports seizures wereclassified as generalized tonic–clonic, we cannot exclude a focalonset that preceded a secondary generalization due to the difficultyin establishing an accurate electro-clinical semiology during the firstyear of life.
Electroencephalogram pattern is even more variable than seizuresemiology. Ictal recordings have been reported [16,21,22,25,28,29]and findings are heterogeneous, as in our cases. The occurrence ofeither diffuse or focal discharges is not surprising in epilepsies relatedto chromosomal abnormalities. Interictal recordings are, however,more frequently reported, and focal slow waves, focal spikes, andmultifocal spike-and-waves seemed to be the most recurrent pat-terns, as in our cases. Delay in motor skill acquisition and mentalretardation are almost a constant feature in ring 14 chromosomepatients: this should be considered as part of the syndromic picture.No specific neuropsychological disabilities were found.
In relation to syndromic classification, it does not match any cur-rently classified conditions with onset during the first year of lifesuch as West Syndrome or Angelman Syndrome. We believe that itshould be considered as a separate entity with its own peculiar char-acteristics. We confirm that no characteristic seizure pattern andinterictal or ictal EEG findings are evident in r(14) patients as recentlypointed out [31]. However, regarding clinical evolution, the recur-rence of three successive stages has been proposed: during stage 1,seizures are frequently in clusters; during stage 2, seizures tend toremain stable and cognitive and motor delay become evident; andduring stage 3, epilepsy tends to be less severe [31].
In addition, while a febrile onset may almost be considered thehallmark of Dravet Syndrome [32], it may also be considered a fre-quent characteristic of r(14) patients, though taking into accountthe differences in epileptic syndrome evolution. In both of our cases,fever determined a worsening of seizures, as was also previouslyreported [8,21,27,29,30]. Seizure recurrence might be in clusters, asreported for other genetic epileptic conditions such as epilepsy dueto PCDH19 mutation [33], and a differential diagnosis should be con-sidered in those cases.
Ring chromosome 14-related epilepsy raises many issues re-garding possible successful treatment that still have not been an-swered. An interesting feature regarding our case #1 was thebeneficial, even if only partial, effect of stiripentol, which so farhas found a specific indication for Dravet Syndrome [34]. Althoughgiven the anecdotal nature of our finding, no evidence-based con-clusions might yet be drawn. Further research on the possible useof stiripentol in r(14)-related epilepsy may provide data on newtherapeutic strategies.
In this regard, it is interesting to note that the clinical picture asso-ciated with r(14) is characterized by early onset epilepsy, neurologi-cal deficits, and mental decline of variable degree. The reportedcases of r(14)-related epilepsy seem to also highlight a series of com-mon elements which may be helpful in pointing the clinician towardsa correct diagnosis. In our cases, numerous specific screening testshave been performed at the same time as karyotype analysis: wewould like to point out that a standard karyotype analysis should beconsidered as a first line of screening in case of early onset epilepsywithout a specific pattern suggestive of a particular etiology, moreso if associated with the recurrence of seizures in clusters and mentalretardation. We also suggest that in order to effectively exclude r(14),at least 100 cells should be examined.
Although an involvement of a region on chromosome 14 proximalto q32.2 in controlling pigmentation of the retinal/macular area of theeye [18] has been proposed, a constant reported finding was the
presence of a break point proximal to q32 also in cases without retinalpigmentation. On the other hand, abnormalities of genes proximallylocated on 14q11q13 may determine seizures, ocular anomalies, andalso microcephaly [31]. A constant finding in patients with r(14)chromosome is the loss of genetic material. According to Zollino[31], genes residing in the proximal 14q interval are dysregulatedthrough heterochromatinization spreading from the adjacent shortarm of the chromosome, and, therefore, molecular studies should beperformed in order to identify putative epilepsy genes.
Acknowledgments
We would like to thank the Neurophysiology Unit staff of theBambino Gesù Children's Hospital. We would also like to thank thepatients participating in this study and their families.
References
[1] Gilgenkrantz S, Cabrol C, Lausecker C, Hartleyb ME, Bohe B. The Dr syndrome.Study of a further case (46, XX, 14r). Ann Genet 1971;14:23-31.
[2] Zollino M, Seminara L, Orteschi D, et al. The ring 14 syndrome: clinical and molec-ular definition. Am J Med Genet A 2009;149:1116-24.
[3] van Karnebeek CD, Quick S, Sluijter S, Hulsbeek MM, Hoovers JM, Hennekam RC.Further delineation of the chromosome 14q terminal deletion syndrome. Am JMed Genet 2002;110:65-72.
[4] Battaglia A, Guerrini R. Chromosomal disorders associated with epilepsy. EpilepticDisord 2005;7:181-92.
[5] Bahi-Buisson N, Ville D, Eisermann M, Plouin P, Kaminsk A, Chrion C. Epilepsy inchromosome aberrations. Arch Pediatr 2005;12:449-58.
[6] Jalbert P, Sele B, Jalbert H, Sirand L, Pison H, Couturier J. Ring chromosome 14 inmonozygotic twins. Ann Genet 1977;20:59-62.
[7] Amarose AP, Dorus E, Huttenlocher PR, Csaszar S. A ring 14 chromosome withdeleted short arm. Hum Genet 1980;54:145-7.
[8] Lippe BM, Sparkes RS. Ring 14 chromosome: association with seizures. Am J MedGenet 1981;9:301-5.
[9] Triolo O, Serra A, Bova R, Carlo Stella N, Caruso P. Infant male with ring chromo-some 14. Ann Genet 1981;24:236-8.
[10] Riley SB, Bucton KE, Ratcliffe SG, Syme J. Inheritance of a ring 14 chromosome.J Med Genet 1981;18:209-13.
[11] Schmidt R, Eviatar L, Nitowsky HM, Wong M, Miranda S. Ring 14 chromosome: adistinct clinical entity. J Med Genet 1981;18:304-7.
[12] Fryns JP, Petit P, Kleczkowska A, De Muelenaere A, ven den Berghe H. Ring chro-mosome 14 syndrome. Ann Genet 1982;25:179-80.
[13] Fryns JP, Kubien E, Kleczkowska A, Nawrocka-Kanska B, Van den Berghe H. Ringchromosome 14. A distinct clinical entity. J Genet Hum 1983;31:367-75.
[14] Ieshima A, Takeshita K, Yamamoto K. Ring 14 syndrome with decreased bonemineral content in two pubertal girls. Jinrui Idengaku Zasshi 1983;28:35-43.
[15] Krawczun M, Melink G, Cervenka J. Ring chromosome 14 and immunoglobulinlocus. Am J Med Genet 1984;17:465-9.
[16] Raoul O, Razavi F, Lescs MC, Bouhanna A. Ring chromosome 14. I. A case report onhomogeneous r(14). Ann Genet 1984;27:88-90.
[17] Portoian-Shuhaiber S, Al-Awadi S, Farag TI, Sundareshan TS, Jindal HR, Al-RashiedAA. Clinical findings in an Arab boy with ring (14)(mos 46, XY, r(14)/45, XY,-14).Ann Genet 1986;29:122-4.
[18] Howard PJ, Clark D, Dearlove J. Retinal/macular pigmentation in conjunction withring 14 chromosome. Hum Genet 1988;80:140-2.
[19] Zelante L, Torricelli F, Calvano S, Mingarelli R, Dallapiccola B. Ring chromosome 14syndrome. Report of two cases, including extended evaluation of a previouslyreported patient and review. Ann Genet 1991;34:93-7.
[20] Shirasaka Y, Ito M, Okuno T, Fujii T, Nozaki K, Mikawa H. Ring 14 chromosomewith complex partial seizures: a case report. Brain Dev 1992;14:257-60.
[21] Ono J, Nishiike K, Imai K, Otani K, Okada S. Ring chromosome 14 complicated withcomplex partial seizures and hypoplastic corpus callosum. Pediatr Neurol 1999;20:70-2.
[22] Morimoto M, Usuku T, Tanaka M, et al. Ring chromosome 14 with localization-related epilepsy: three cases. Epilepsia 2003;44:1245-9.
[23] Hou JW. Mosaic ring chromosome 14 and monosomy 14 presenting with growthretardation, epilepsy, and blepharophimosis. Chang Gung Med J 2004;27:373-8.
[24] Schlade-Bartusiak K, Costa T, Summers AM, Nowaczyk MJ, Cox DW. FISH-mappingof telomeric 14q32 deletions: search for the cause of seizures. Am J Med Genet A2005;138:218-24.
[25] Sheth FJ, Soni N. Ring chromosome 14 with epilepsy and development delay.Indian Pediatr 2006;43:744-5.
[26] Knijnenburg J, van Haeringen A, Hansson KB, et al. Ring chromosome formation asa novel escape mechanism in patients with inverted duplication and terminaldeletion. Eur J Hum Genet 2007;15:548-55.
[27] Tzoufi M, Kanioglou C, Dasoula A, et al. Mosaic trisomy r(14) associated withepilepsy and mental retardation. J Child Neurol 2007;22:869-73.
[28] Ville D, De Bellescize J, Nguyen MA, et al. Ring 14 chromosome presenting asearly-onset isolated partial epilepsy. Dev Med Child Neurol 2009;51:917-22.

592 N. Specchio et al. / Epilepsy & Behavior 25 (2012) 585–592
[29] Giovannini S, Frattini D, Scarano A, et al. Partial epilepsy complicated by convulsiveand nonconvulsive episodes of status epilepticus in a patient with ring 14 chromo-some syndrome. Epileptic Disord 2010;12:222-7.
[30] Nucaro AL, Falchi M, Pisano T, et al. Ring chromosome 14 mosaicism: an unusualcase associated with developmental delay and epilepsy, characterized by genomearray-CGH. Am J Med Genet A 2010;152:234-6.
[31] Zollino M, Ponzi E, Gobbi G, Neri G. The ring 14 syndrome. Eur J Med Genet2012;55:374-80.
[32] Dravet C, Bureau M, Oguni H, Fukuyama Y, Cokar O. Severe myoclonic epilepsy ininfancy (Dravet Syndrome). In: Roger J, Bureau M, Dravet C, Genton P, TassinariCA, Wolf P, editors. Epileptic syndromes in infancy, childhood and adolescence.4th edn. Montrouge: John Libbey Eurotext Ltd.; 2005. p. 77-89.
[33] Specchio N,Marini C, Terracciano A, et al. Spectrum of phenotypes in female patientswith epilepsy due to protocadherin 19 mutations. Epilepsia 2011;52:1251-7.
[34] Chiron C, Dulac O. The pharmacologic treatment of Dravet syndrome. Epilepsia2011;52(S2):72-5.




















