
Environmental and behavioural interventions to reduce activity limitation and improve quality of...
29
Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older people (Review) Skelton DA, Howe TE, Ballinger C, Neil F, Palmer S, Gray L This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2013, Issue 6 http://www.thecochranelibrary.com Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older people (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Transcript of Environmental and behavioural interventions to reduce activity limitation and improve quality of...
Environmental and behavioural interventions for reducingphysical activity limitation in community-dwelling visually
impaired older people (Review)
Skelton DA, Howe TE, Ballinger C, Neil F, Palmer S, Gray L
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2013, Issue 6
http://www.thecochranelibrary.com
Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .27NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iEnvironmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Environmental and behavioural interventions for reducingphysical activity limitation in community-dwelling visuallyimpaired older people
Dawn A Skelton1, Tracey E Howe2, Claire Ballinger3, Fiona Neil4, Shelagh Palmer5, Lyle Gray6
1School of Health & Life Sciences, Institute of Allied Health Research, Glasgow Caledonian University, Glasgow, UK. 2Glasgow City ofScience, Glasgow, UK. 3Research Design Service South Central, Faculty of Medicine, University of Southampton, Southampton, UK.4Community Falls Prevention Programme, Greater Glasgow and Clyde NHS, Glasgow, UK. 5Visibility, Glasgow, UK. 6Life Sceince,Glasgow Caledonian University, Glasgow, UK
Contact address: Dawn A Skelton, School of Health & Life Sciences, Institute of Allied Health Research, Glasgow Caledonian University,Cowcaddens Rd, Glasgow, G4 0BA, UK. [email protected].
Editorial group: Cochrane Eyes and Vision Group.Publication status and date: New, published in Issue 6, 2013.Review content assessed as up-to-date: 9 November 2012.
Citation: Skelton DA, Howe TE, Ballinger C, Neil F, Palmer S, Gray L. Environmental and behavioural interventions for reducingphysical activity limitation in community-dwelling visually impaired older people. Cochrane Database of Systematic Reviews 2013, Issue6. Art. No.: CD009233. DOI: 10.1002/14651858.CD009233.pub2.
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Impairment of vision is associated with a loss of function in activities of daily living. Avoidance of physical activity and consequentreduced functional capacity is common in older people with visual impairment and an important risk factor for falls. Indeed, the rateof falls and fractures is higher in older people with visual impairment than age-matched visually normal older people. Depression andanxiety is common in older people with vision impairment and leads to further restriction of activity, reduced social contact and reducedquality of life. Possible mechanisms to reduce activity restriction and therefore improve mobility and activity include environmentaland behavioural interventions delivered by a number of health professionals, including occupational therapists.
Objectives
The objective of this review was to assess the effectiveness of environmental and behavioural interventions in reducing activity limitationand improving quality of life amongst visually impaired older people.
Search methods
We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2012, Issue10), Ovid MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily, Ovid OLDMED-LINE, (January 1950 to November 2012), EMBASE (January 1980 to November 2012), Cumulative Index to Nursing and Al-lied Health Literature (CINAHL) (January 1937 to November 2012), Allied and Complementary Medicine Database (AMED)(January 1985 to November 2012), OT Seeker (inception to November 2012), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform(ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials. We lastsearched the electronic databases on 9 November 2012.
1Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Selection criteria
Randomised controlled trials (RCTs) and quasi-randomised controlled trials (Q-RCTs) that compared environmental interventions,behavioural interventions or both, versus control (placebo control or no intervention or usual care), and trials comparing differenttypes of environmental or behavioural interventions, in older people (aged 60 and over) with irreversible visual impairment livingindependently or in residential settings. To be eligible for inclusion the primary aim of studies must be reducing physical activitylimitation and must include a measure of physical activity. Secondary outcome measures included falls, fear of falling, quality of life.
Data collection and analysis
Two authors independently read abstracts retrieved by the search to identify eligibility and study quality. We contacted study authorsfor additional information.
Main results
Our searches found no RCTs or Q-RCTs that met the eligibility criteria for this review.
Authors’ conclusions
We are unable to reach any conclusion about the effectiveness of environmental or behavioural interventions for reducing physicalactivity limitation in community-dwelling visually impaired older people, as no eligible studies were found. However a number of studiesreviewed included only the secondary outcome measures of this review. Although behavioural interventions delivered by occupationaltherapists have been shown to reduce the rate of falls, we are unable to conclude if this is due to reduced activity restriction (increasedmobility) or reduced activity (lessening exposure to risk). There are inconclusive and conflicting results from trials evaluating theeffectiveness of behavioural and environmental interventions aimed at improving quality of life. Further research is necessary (such asongoing Dutch and UK trials considering the effectiveness of orientation and mobility training on activity restriction, physical activity,falls, fear of falling and quality of life in older adults with low vision, and the effect of an occupational therapist delivering home safetymodification, coping strategies and exercise with older people with low vision) before any conclusions can be reached.
P L A I N L A N G U A G E S U M M A R Y
Environmental and behavioural interventions to reduce activity limitation and improve quality of life in older people withvisual impairment
Visual impairment in older people is associated with avoidance of physical activity, anxiety and depression as well as an increased riskof falls and fractures. Standard ways to improve vision-related quality of life include provision of glasses, filters and other vision-relatedequipment - in other words, interventions which generally make reading or watching television or using a computer more achievable.The use of behavioural strategies to improve a person’s skill and confidence in activity or environmental changes in the home, work orleisure environment, such as improved lighting or highlighting stair edges, may help reduce activity restriction and improve quality oflife, both outside and inside the home. We searched for evidence from high quality trials on environmental or behavioural interventionsin older adults, living in the community or in residential settings, with irreversible vision impairment which aimed to reduce activityrestriction or increase general physical activity. We found no trials that met the inclusion criteria for the review. Further research intothis highly important issue needs to be done before any conclusions can be made.
B A C K G R O U N D
The prevalence of visual impairment is estimated by the WorldHealth Organization (WHO) to be 161 million worldwide(Resnikoff 2008). One in eight people in the UK over the age
of 75 and one in three over the age of 90 live with significantsight loss (Evans 2002). Older adults with visual impairment aremore likely to be physically dependent, have poorer quality of lifeand are more likely to move into residential settings than their
2Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

sighted peers (Ivers 1998; Klein 2003; Tinetti 1998). Impairmentof vision is associated with a loss of function in activities of dailyliving (Brouwer 2008; Salive 1994). A UK report by Visibility(Campbell 2005a) found that older people with visual impairmentare more likely to avoid activity due to their visual impairment.Anxiety and depression, leading to reduced activity, is commonin those with visual impairment (Evans 2007). There is an asso-ciation between vision and various health conditions and activitylimitations among older people. These include decreases in leisureactivities, Instrumental Activities of Daily Living (IADL) perfor-mance and social function, Activities of Daily Living (ADL) andcompromised mobility. The International Classification of Func-tioning (ICF) defines activity as “the nature and extent of perfor-mance of a function by a person” and activity limitations as “prob-lems of the performance of activities in nature, duration, and qual-ity” (WHO 2001). The daily problems in seeking leisure activitiesby older adults with low vision may have implications for otherhealth problems. Many older adults are not engaging in activitiesfor which they may have sufficient vision due to factors unrelatedto medical care. Inactivity and a lack of social connections shouldbe noted by ophthalmologists and others treating the older pop-ulation (Berger 2012). Challenging environments, struggling toobtain transportation, feelings of vulnerability, having decreasedenergy, and lacking assertiveness were all identified in interviewswith older visually impaired adults as reasons for not being phys-ically active and not feeling competent in such activities (Berger2012).
Visual impairment is also associated with increases in the inci-dence of hip fractures, depression and falls (Crews 2004). Avoid-ance of physical activity due to fear of falling is common amongolder people at risk of falling (Yardley 2002). Indeed, the rate offalls in older people with visual impairment is 1.7 times higher,and hip fractures are 1.3 to 1.9 times higher than in age-matchedvisually normal populations (Legood 2002). One study reportedthat activity restriction was present in 45% of those with visualimpairment, compared with only 24% in those without visual im-pairment who had experienced an injurious fall (Murphy 2002).Those with visual impairment were also more likely to admit tofear of falling (44%) even without a fall history. One study hasshown that perceived interference of vision loss on goal-directedbehaviour and expected activities has greater influence on distressand is subsequently predictive of disability in comparison with ob-jective symptoms (visual acuity) (Dreer 2008). It therefore seemslikely that the mechanism underpinning previous trials of main-taining mobility and physical activity, particularly with respect toenvironmental components, behavioural components or both, forpeople with visual impairment will be different from the generalpopulation.
Description of the condition
Visual impairment is defined as best-corrected visual acuity of thebetter eye less than 0.3 logMAR (Log of the Minimum Angleof Resolution) units or visual field defects within 30 degrees offixation. Blindness is defined as visual acuity less than 0.05 log-MAR units or visual field defects within 10 degrees of fixation(WHO 1992). A working definition of visual impairment is lowvision that cannot be corrected by standard glasses or by med-ical or surgical intervention. The top five conditions leading tovisual impairment and blindness in the UK are age-related macu-lar degeneration (AMD), glaucoma, diabetic retinopathy, myopicdegeneration and optic atrophy (Evans 2004). Age-related macu-lar degeneration and diabetic retinopathy are the most commoncauses of blindness in those over 65 years of age (Bamashmus 2004;Resnikoff 2004).
Description of the intervention
Environmental interventions include any targeted, intentional im-provement to the (usually indoor) physical environment, with theaim of reducing symptoms or improving wellbeing (Preedy 2009).In the case of visual impairment, this may incorporate adaptationsand modifications to an individual’s physical environment (usu-ally their home) as the result of a formal environmental assessmentthat identified potential hazards or restrictions. The aim of theenvironmental intervention is to enhance the individual’s abilityto perform daily living tasks safely and independently, facilitatingtheir safe mobility and improving confidence. Examples for anindividual with visual impairment include the removal of a rug,increased lighting in hallways and contrasting stripes on stairs.Behavioural interventions include the systematic implementationof procedures that result in lasting positive changes in an indi-vidual’s behaviour (Markowitz 2006a). ’Behavioural intervention’means the design, implementation, and evaluation of individual orgroup instructional and environmental modifications, includingprogrammes of behavioural instruction, to produce significant im-provement in human behaviour through skill acquisition and thereduction of problematic behaviour. These interventions, for peo-ple with visual impairment, might include, but are not restrictedto, the teaching of adaptive strategies to enhance changes in anindividual’s behaviour when negotiating and interacting with theirenvironment (Markowitz 2006b) and orientation and mobility(O&M) training (Virgili 2003). O&M training aims to teach thevisually impaired person how to ambulate and negotiate the envi-ronment safely and independently and may contribute to reducedactivity limitations and societal participation (Zijlstra 2009).Occupational therapists, as a profession, have the expertise to as-sess, devise and implement rehabilitation plans which incorpo-rate both types of interventions: an occupational therapy approachencompasses both environmental change and the interaction ofthe individual with their environment, their actions and theirbehavioural adaptations at home and in the community. Thisdynamic relationship between the person, their behaviour and
3Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

the environment has been described elsewhere (Clemson 2003;Markowitz 2006b). Many environmental risk assessments, andsome environmental modifications, are undertaken by other pro-fessionals but the relationship of the person, their behaviour andtheir environment may not be evaluated comprehensively.
How the intervention might work
Through changes in the home environment and behaviouralstrategies to negotiate the environment, the person with visual im-pairment may feel more confident that they can negotiate theirenvironment safely, thereby reducing concerns about their safetyand fear of falling. This should lead to greater mobility and habit-ual physical activity. This could be the mechanism behind previ-ous trials that have shown reductions in falls in those with visualimpairment following environmental and behavioural interven-tions (e.g. Campbell 2005b: La Grow 2006). Presentation of theinformation is also considered important and to be effective mustbe in collaboration with the person with visual impairment, in aproblem-solving rather than prescriptive manner, to allow themownership of the information and advice and to feel that it fitstheir abilities and preferences (Clemson 2008).
Why it is important to do this review
To date, no published literature review has been identified whichspecifically considers the effectiveness of environmental or be-havioural interventions in reducing physical activity limitationamong older people with visual impairment. The physiological,psychological, functional and societal benefits of regular physicalactivity amongst older people (WHO 2007) are irrefutable, andinterventions that improve habitual physical activity in visuallyimpaired older people are vital to promote public health. Trialswhich have adopted a holistic, participant-centred approach toenvironment modification (i.e. the consideration of the personwithin the context of the environment and their functional activi-ties/demands) have shown reductions in falls both within and out-side the home (Campbell 2005b; La Grow 2006), whereas trialsthat have considered removal of home hazards only (Stevens 2001)did not reduce the incidence of falls, even within the home. Onepotential mechanism for falls reduction could be that the visuallyimpaired person actually restricts their activity more as a resultof the intervention, which in the short term could reduce theirexposure to falls risk (La Grow 2006). There is therefore a need tofurther unpick the mechanism of reduction in falls in visually im-paired older people (La Grow 2006). Although interventions suchas those aimed at reducing falls may work by increasing mobilityand activity, they may also do the opposite. In one intervention,those allocated to exercise-only interventions, which had previ-ously been shown to reduce falls in older people, had no reductionin their risk of falls (La Grow 2006). A sub-analysis of those who
were compliant (performed the strength and balance exercises andwalking programme) did show a reduction in risk. The authorshypothesised that visually impaired older people who engage inmore activity reduce their risk, but those that avoid activity do not(La Grow 2006). Physical activity is known to have a U-shapedrelationship to falls with those least and those most active morelikely to fall (Gregg 2000). Trials rarely consider activity restrictionor physical activity alongside falls as an outcome measure, so themechanism remains unclear.Although there is a previous systematic review of the effect of in-terventions to reduce falls in older adults (Gillespie 2012), there isno specific review in those with visual impairment. The rate of fallsand injury is greater in older people with visual impairment thanvisually unimpaired older people (Legood 2002) and avoidanceof activity is not uncommon in those with poor vision (Campbell2005a). A previous systematic review on orientation interventionsto improve mobility in people with visual impairment (Virgili2003) considered performance in travel activities of daily life butnot more generalised physical activity or activity restriction. Al-though there is some potential overlap in terms of secondary out-comes (quality of life and people’s perceptions of the effects of ori-entation interventions on their lives), this review included partici-pants aged 16 and over, not older adults (aged 60 or over) with vi-sual impairment. An ongoing Cochrane review (Langelaan 2007)considers multidisciplinary and monodisciplinary rehabilitationon generic health-related and vision-related quality of life. Thisreview includes participants’ perception of the effect of rehabili-tation on activities in daily living and on participation in society,so again there is potential overlap. However, the review includesparticipants aged 18 and over, not specifically older adults (aged60 or over).
O B J E C T I V E S
The objective of this review was to assess the effectiveness of envi-ronmental and behavioural interventions in reducing activity lim-itation and improving quality of life amongst visually impairedolder people.
The following potential implications were also addressed in thisreview.
• Do the interventions reduce activity restriction and increasephysical activity and mobility in older people with visualimpairment? What quality of life effects are there?
• Do the interventions have the same effect in young-old andold-old, fallers and non-fallers, or those with different severity ofvisual impairment?
• Do the mix and intensity of the interventions affect theoutcome?
4Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

• Do the interventions have different effects in differentresidential settings?
• Does the training of the person delivering the interventionsaffect the outcome?
M E T H O D S
Criteria for considering studies for this review
Types of studies
We aimed to include randomised controlled trials (RCTs) andquasi-randomised controlled trials (Q-RCTs) that compared envi-ronmental interventions, behavioural interventions or both, ver-sus control (placebo control or no intervention or usual care), andtrials comparing different types of environmental or behaviouralinterventions. We did not include single studies that report onlyquality of life (as opposed to limitations in mobility and quality oflife) so as to avoid overlap with another ongoing Cochrane review(Langelaan 2007).
Types of participants
We aimed to include trials with the following participants:• Older people (aged 60 and over) with irreversible visual
impairment including, but not limited to, low visual acuity, poorcontrast sensitivity, poor depth perception and reduced visualfield.
• Older people with irreversible visual impairment and othermultiple disabilities, such as hearing loss, neurological ormusculoskeletal disease or cognitive impairments.
• Older people living independently and those living inresidential settings.
Types of interventions
Environmental interventions, behavioural interventions or both,including but not limited to visual rehabilitation (e.g. low visiondevices), removal of home hazards, home safety modifications,provision of adaptive or assistive equipment, advice on behaviouralchanges to improve safety in activities of daily living (IADL andADL), cognitive behavioural therapies, or other behavioural ther-apies aimed at changing behaviour.For any study included, we aimed to record the professional train-ing of the person delivering the interventions. The types of inter-ventions would also be rated on the intensity of the intervention,based on previously published criteria (evaluation of risk of personand environment; validated assessment tools; formal or observa-tional evaluation of functional capacity; and adequate follow-up)(Clemson 2008).
We did not include other vision-correction interventions (e.g.cataract surgery, corrective lenses or filters) in this review.
Types of outcome measures
Primary outcomes
To be eligible for inclusion the primary aim of the study was toreduce physical activity limitation and needed to include a measureof physical activity which might include the following:
• Continuous objective measures e.g. body fixed sensoractivity monitoring.
• Continuous subjective self report measures e.g. validatedquestionnaires such as Physical Activity Scale for the Elderly(PASE), Community Healthy Activities Model Program forSeniors (CHAMPS).
• Other self-reporting measures may be dichotomous e.g.single questions on physical activity.
Secondary outcomes
• Falls (rate (or number) of falls or number of fallers) and fall-related injuries. Prospective daily calendars returned monthly forat least one year is the preferred method for recording falls(Lamb 2005).
• Fear of falling (e.g. scales such as FES-I, ABC, FES, MFES,FHI, SAFFE and Single Item 1-4).
• Quality of life (e.g. Euroquol, SF12, SF36, WHOQoL orany other validated means of recording subjective QOL).
• Attitudes, beliefs and behaviours (e.g. AFRIS, OEE, SEE,FaB). The latter may also be ascertained via qualitative methodssuch as focus groups and interviews.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-als (CENTRAL) 2012, Issue 10, part of The Cochrane Library.www.thecochranelibrary.com (accessed 9 November 2012), OvidMEDLINE, Ovid MEDLINE In-Process and Other Non-In-dexed Citations, Ovid MEDLINE Daily, Ovid OLDMEDLINE,(January 1950 to November 2012), EMBASE (January 1980to November 2012), Cumulative Index to Nursing and AlliedHealth Literature (CINAHL) (January 1937 to November 2012),Allied and Complementary Medicine Database (AMED) (Jan-uary 1985 to November 2012), the metaRegister of ControlledTrials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical TrialsRegistry Platform (ICTRP) (www.who.int/ictrp/search/en). We
5Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

did not use any date or language restrictions in the electronicsearches for trials. We last searched the electronic databases on 9November 2012.We found that searches in PsycINFO, Applied Social SciencesIndex and Abstracts (ASSIA), Sociological Abstracts (SocioFILE),Science Citation Index, Social Sciences Citation Index, did notyield any additional papers and we were unable to choose specificcriteria to search for our inclusion criteria so it was decided thatthe databases searched above would give sufficient coverage. Therewere no date or language restrictions in the electronic searches fortrials.See: Appendices for details of search strategies for CENTRAL(Appendix 1), MEDLINE (Appendix 2), EMBASE (Appendix3), CINAHL (Appendix 4), AMED (Appendix 5), OTseeker (Appendix 6), mRCT (Appendix 7),ClinicalTrials.gov (Appendix8) and the ICTRP (Appendix 9).
Searching other resources
We contacted authors of any ongoing trials or abstracts found andsearched the reference lists of full papers reviewed, as identified inour electronic search.
Data collection and analysis
Selection of studies
Two review authors (DS and CB), working independently,screened all titles and abstracts generated by the searches for po-tentially relevant studies. We based the decision as to whether toinclude studies on the following criteria: the type of study; typeof participants; type of intervention and type of outcome mea-surements. Two review authors (DS and TH) assessed the full-textarticles of the selected titles and abstracts for eligibility accordingto the ’Criteria for considering studies for this review’ outlinedabove. We resolved disagreements by consensus. In one instance(where an abstract only was found) we sought additional informa-tion from the author; however, the full paper had not been pub-lished and the study did not meet the inclusion criteria.
Data extraction and management
We planned that when a study fulfilled the inclusion criteria, dataconcerning methodological issues, characteristics of participants,interventions and outcome measures would be independently ex-tracted using a standard extraction form and the review authorswould not be masked to the study’s authors, institutions or journalof publication. Where available and appropriate, we would havepresented quantitative data for the outcomes listed in the inclu-sion criteria in the analyses. Where studies report standard errorsof the means (SEMs), we would obtain standard deviations (SDs)
by multiplying SEMs by the square-root of the sample size. Wewould have attempted to contact authors of studies where therewas inadequate reporting of data to enable clarification and whereappropriate, to allow pooling.
Assessment of risk of bias in included studies
We planned, if there were included RCTs, for two review authorsto independently assess risk of bias in included studies using themethodology described in Chapter 8 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011). The stud-ies would have been assessed on the following criteria: randomsequence generation, allocation concealment, masking (blinding)of participants and personnel, masking of outcome assessment,incomplete outcome data, selective outcome reporting and othersources of bias. Due to the nature of this intervention it is not pos-sible to mask participants or staff providing the intervention. It ishowever possible to mask outcome assessors for objective measure-ments. Authors’ assessments were to be ’High risk of bias’, ’Lowrisk of bias’ or ’Unclear risk of bias’.
Measures of treatment effect
For each trial, we would have calculated a risk ratio (RR) and 95%confidence interval (CI) for dichotomous outcomes, and weightedmean differences (WMD) and 95% CI for continuous outcomes(reporting mean and SD or SEM). We would have calculated stan-dardised mean differences (SMDs) and 95% CIs when combiningresults from studies using different ways of measuring the sameconcept. We would have reported change scores separately as thesecannot be incorporated into meta-analyses of SMDs. Where ap-propriate, we would have pooled results of comparable groups oftrials using the fixed-effect model and would have calculated the95% CIs.
Unit of analysis issues
We planned to report the level at which randomisation occurredin the included studies as specified in Chapter 9 of the CochraneHandbook for Systematic Reviews of Interventions (Deeks 2011).Possible variations in study designs include cluster-randomised tri-als, cross-over trials, multiple treatments and multiple interven-tion groups. We would not have applied thresholds for eligibility(e.g. outcomes masked to allocation or minimum follow-up pe-riod) but would have reported details of the studies which mayhave affected interpretation of the data (e.g. short duration of in-tervention).
Dealing with missing data
If missing data were discovered during data extraction, we plannedto contact the original investigators of the study to request therequired information. It might also have been necessary to conduct
6Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

a sensitivity analysis if assumptions had been made (Deeks 2011).We planned to describe the potential effect of missing data uponconclusions drawn from this review.
Assessment of heterogeneity
We would have tested heterogeneity between comparable trialsafter due consideration of the value of I²; a value greater than 50%may indicate substantial heterogeneity (Higgins 2003). We wouldalso have considered methodological and clinical heterogeneity.In the presence of heterogeneity, depending on the number ofstudies and the direction of effect, we would have pooled the resultsof comparable groups of trials using the random-effects modeland would have calculated the 95% CIs or have considered thesubgroup analyses described later.
Assessment of reporting biases
We would have tested publication bias using funnel plots or othercorrective analytical methods, provided there was a sufficient num-ber of trials included in the systematic review. We would have re-viewed and discussed open and uncontrolled studies to identifyreporting bias.
Data synthesis
Where appropriate, we would have pooled results of comparablegroups of studies using the fixed-effect model and calculated 95%CIs. In the presence of heterogeneity, we would have pooled theresults of comparable groups of trials using the random-effectsmodel and calculated 95% CIs. In the case of methodological (in-cluding unit of analysis issues) or clinical heterogeneity, we wouldhave undertaken sensitivity analyses to examine the impact of thesestudies on the results.
Subgroup analysis and investigation of heterogeneity
The review authors planned to consider the following hypothesesusing subgroup analysis if sufficient data were available:
1. Behavioural interventions delivered in tandem withenvironmental interventions are more effective than eitherbehavioural or environmental interventions delivered on theirown.
2. Interventions are equally effective on differing severities ofvisual impairment.
3. Interventions are equally effective with fallers as they arewith the general older population (inclusion criteria at point ofrecruitment into the study).
Sensitivity analysis
We planned to undertake sensitivity analyses, where indicated, toinvestigate the effects of methodological quality. For example, ifappropriate, we would have looked at the effect of excluding quasi-randomised trials, as they will be at higher risk of bias. Many issuessuitable for sensitivity analysis are only identified during the re-view process where the individual peculiarities of the studies underinvestigation are identified. As no studies have been identified forinclusion in this review, we are unable to undertake such analyses.
Grading of evidence and summary of findings table
We planned to present major outcomes (including benefits andadverse events) in a ’Summary of findings’ table, which providesinformation on the quality of evidence and the magnitude of theintervention effect, as well as a summary of the main outcomedata as described in Chapter 11 of the Cochrane Handbook forSystematic Reviews of Interventions (Schünemann 2011). We wouldalso have presented an assessment of the overall quality of evidenceper outcome (high, moderate, low and very low) using the GRADEapproach (Schünemann 2011). We also planned to review the costof treatment in the included studies and other publications.
R E S U L T S
Description of studies
Results of the search
The electronic searches yielded a total of 6014 references from elec-tronic databases and two records from screening the citations frompotentially relevant references. One ongoing study was known tothe authors but not found in the searches of the included databases(UKCRN ID 10883). The Trials Search Co-ordinator scannedthe search results, removed duplicates and trial protocols, and re-moved 4330 references which were not relevant to the scope ofthe review. The authors screened the remaining 780 publishedreports to identify potentially relevant studies. We obtained full-text copies of 30 studies for further investigation. After readingthe full-text record we excluded all the studies. See Figure 1.
7Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Results from searching for studies for inclusion in the review.
8Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Three of the trials identified on the clinicaltrials.gov website maybe of interest to a future update of this review. The first aims todemonstrate how specified physical and emotional outcomes ofpersons with low vision change across time, with an RCT of a shamversus a problem-solving intervention. We await the publicationof this trial (recruitment due to end Oct 2011) (NCT00545220).The second trial has an intervention where a low vision occupa-tional therapist collaborates with a low vision optometrist to de-velop and implement a care plan based on a person’s vision sta-tus, rehabilitation potential, and personal rehabilitation goals - butoutcome measures only targeted vision function and vision-relatedquality of life. We await the publication of this trial (recruitmentdue to end July 2012) (NCT00769015), to see if there are anyoutcomes of interest within vision-related quality of life. Finally,a study in the Netherlands which has relevant outcome measures(Zijlstra 2009) is ongoing. See Characteristics of ongoing studies.Although removed at the screening stage, two other ongoingstudies were identified in the searches. One Australian study(published protocol) is considering the effects of a low vi-sion programme on ’positive and active engagement with life’(ACTRN12607000399493). The other study was identifiedthrough contacts of the authors. Based in the UK (UKCRN ID10883), this pilot (RCT) study, VIP2UK, aims to promote adher-ence to an occupational therapy and exercise intervention to reducefalls in older people with visual impairment. See Characteristicsof ongoing studies.
Included studies
No studies met the criteria for this review (see Figure 1).
Excluded studies
From the reports, we selected 30 studies for review in full text,but excluded all of them. Eight studies were not behavioural orenvironmental interventions aimed at increasing activity or re-ducing activity restriction; instead they were visual field training(Balliet 1985); residual vision training (Conrod 1986); featuresearch task (computerised vision training) (Kuyk 2010); percep-tual learning (paper-based) (Overbury 1996); use of microscopesto extend reading time (Scanlan 2004); eccentric viewing comput-erised intervention (Vukicevic 2009); educational programme toimprove self care, food preparation, home and financial manage-ment (Smith 2009). One study was aimed at improving skills at re-questing on-the-job accommodations from employers and there-fore had very few participants in the eligible age range (Rumrill1999).Of those interventions that were eligible (included an environ-mental or behavioural component), four were not RCTs (Gutman2002; Kuyk 2008; La Grow 2004; McCabe 2000) and had noactivity outcomes. One other was not an RCT but potentially
had a physical activity outcome of interest but this was a singlequestion on moderation of physical activity, questions on walkingin and out of the home and use of transport (Engel 2000). Thestudy was not controlled, did not report standard deviations (SDs)so as to assess effect size and had considerable drop out (Engel2000). One other was not an RCT, but rather an implementationpaper (how to implement the intervention) based on Campbell2005b (La Grow 2006). Two were abstracts which were actuallythe protocols for studies (Stelmack 2005; West 2004) and had noactivity outcomes. Fourteen did not have any outcome measuresof interest in this review (e.g. physical activity/activity restriction).Instead these studies had outcome measures such as falls and in-juries (Campbell 2005b; Cumming 2007; Day 2002); perceivedsecurity in the performance of daily occupations (Dahlin-Ivanoff2002); participation in daily activities (as opposed to physical ac-tivity) (Girdler 2010); reading skills (Stelmack 2008a; Stelmack2008b; Stelmack 2008c); improve quality of life (Reeves 2004) orwellbeing (Pankow 2004); improved physical function (Deremeik2007; Pankow 2004); associations between assistive devices andactivities of daily living (Eklund 2007); dependence in activitiesof daily living (Eklund 2008; Reeves 2004); and balance (Cheung2008). Although Cheung 2008 also had as an aim to increase con-fidence in safe ambulation, this was not assessed as an outcome.All trials which considered environmental or behavioural inter-ventions were with older people living in the community, exceptthe SEEING trial (Deremeik 2007) and West 2004, which werebased in nursing homes.
Risk of bias in included studies
There were no studies included in this review.
Effects of interventions
Our searches produced no RCTs or quasi-RCTs of behaviouralor environmental interventions to reduce activity restriction andimprove quality of life in older people with vision impairment thatmet our eligibility criteria.
D I S C U S S I O N
Although this could be considered an ‘empty review’, there is valuein publishing a review without includable studies, as it indicatesthe state of research evidence at a particular point in time andhighlights major research gaps (Lang 2007). There is value in suchreviews in informing clinicians, consumers, and other decisionmakers in health care when there is lack of robust evidence for oragainst a healthcare intervention (Green 2007).
9Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

It is important to note that, although we reviewed 14 RCTsof environmental and behavioural interventions in older peoplewith visually impairment, none of these had an outcome mea-sure that gauged their effectiveness on physical activity or physi-cal activity restriction. Some studies included outcome measuresof participation in daily activities (as opposed to physical activ-ity) (Girdler 2010); perceived security in performing occupations(Dahlin-Ivanoff 2002); associations between assistive devices andactivities of daily living (Eklund 2007); or dependence in activ-ities of daily living (Eklund 2008; Reeves 2004), which perhapsare markers or would be associated with activity restriction, butwere not listed in our a priori outcome measures. All of thesestudies included occupational therapists or vision rehabilitationofficers as the professionals delivering the intervention. Quality oflife (Girdler 2010; Reeves 2004), wellbeing (Pankow 2004) or im-provements in physical function (Deremeik 2007; Pankow 2004)were the other outcome measures of interest. One suite of studiesconcentrated on reading skills (Stelmack 2008a; Stelmack 2008b;Stelmack 2008c). Other studies assessed the interventions’ effec-tiveness on balance (Cheung 2008) or falls and injuries (Campbell2005b; Cumming 2007; Day 2002). However, it is not possible toknow if a reduction in falls risk is due to the participants’ reducedactivity (so reducing their exposure to risk) or their becoming bet-ter able to cope with their environment. It would have been usefulto have assessed whether falls per unit of activity (or exposure) werereduced in these studies as per the guidelines of ProFaNE (Lamb2005). Interestingly, Reeves 2004 showed no positive benefit oftheir intervention on quality of life and concluded that researchersshould be aware that, in people with macular degeneration at least,the determinants of quality of life may revolve more around lostsources of pleasure and relaxation (e.g. playing with grandchildrenor reading) than in their ability to perform essential activities ina constrained way. In other words, the value of reducing activityrestriction is important to patients.
A recent systematic review (Binns 2012) reminds researchers thatoutcome measures chosen to determine the effectiveness of low vi-sion services should reflect capacity within daily activities, withinthe home environment, rather than just on clinical outcomes.These reviewers, although including non-RCTs, only found seventrials, and whilst they felt able to confirm that rehabilitation ser-vices result in improved clinical and functional outcomes, theycommented that the number of studies meeting their inclusioncriteria was ‘pitifully small’. There is growing interest in physicalactivity in those living with low vision as reflected by a recentstudy considering the accuracy and validity of talking pedometersto measure activity in people with visual impairment (Holbrook2011). Trials which consider both subjective and objective physi-cal activity and activity restriction are necessary to see if interven-tions can make a difference to habitual physical activity.
However, we did find one ongoing RCT which is assessing orienta-tion and mobility (O&M) training in older people with low vision
and has activity restriction as an outcome measure (Zijlstra 2009).We also await an ongoing pilot RCT (UKCRN ID 10883) of in-creasing adherence to an occupational therapy-delivered home sa-fety and modification programme and an occupational therapist-delivered home exercise programme, with physical activity as acore outcome measure. We also await with interest the publicationof results from an Australian study which is considering the effectsof a low vision programme on ’positive and active engagementwith life’ (ACTRN12607000399493), and two American studieswhere it is unclear whether the outcome measures will meet ourcriteria (NCT00769015; NCT00545220). See ’Characteristics ofongoing studies’.
Of final note is the concern that interventions are rarely describedin detail, nor do they provide information on the most appropriateparticipant groups or types of visual impairment with which theyare most effective. It is important to customise interventions tosuit particular individuals and their needs and preferences. A ’blackbox’ of multiple interventions makes it difficult to pull out theeffectiveness of differing parts of the interventions (e.g. a mix ofenvironmental and behavioural interventions may make it difficultto disentangle which type of intervention is more appropriate forwhich participant group).
Summary of main results
Our searches produced no RCTs or quasi-RCTs of behaviouralor environmental interventions to reduce activity restriction andimprove quality of life in older people with vision impairment thatmet our eligibility criteria.
Potential biases in the review process
We attempted to minimise bias by two review authors indepen-dently reviewing the titles and abstracts. We did not restrict thearticles to English only so we should have minimised publicationbias. It is possible that our search terms were not broad enough, orwere restrictive. However all studies that the authors were aware ofwere picked up in the searches. The search for this review was com-pleted in November 2012. It is possible that relevant studies havebeen published in the interim period to publication but to counterthis, we will update the review bi-annually. We deliberately didnot narrow our population group and included both community-dwelling and care home/residential older adults so we do not feelthat we were too narrow in our approach to the population group.It is possible that we were too precise in our interventions by ex-cluding, for example, computerised visual field or eccentric viewtraining but the focus of this review was to consider modificationsto the home environment, and coping and enabling strategies tonegotiate safely in and out of the home. We excluded one studywhich considered perceived security in performing occupationalactivities and it could be countered that this would reflect activity
10Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

restriction, but this was not set a priori in the protocol. As nostudies met the selection criteria we can only comment that thereis so far no evidence of effect.
Agreements and disagreements with otherstudies or reviews
The Cochrane review Virgili 2003 considered the effectiveness ofO&M training in adults with low vision. The review included twosmall trials comparing O&M training to physical exercise, whichprovided weak evidence. O&M training had no effect in one studywhile it was found to be beneficial in the second. There is thereforelittle evidence on which type of O&M training is better for peoplewith low vision who have specific characteristics and needs.Work commissioned by the Thomas Pocklington Trust (Ballinger2009) aimed to carry out a qualitative evidence synthesis of quali-tative research exploring the views and experiences of older peoplewith visual impairment on participation in falls prevention initia-tives. Although no studies were found which explicitly sought toexplore the views of older visually impaired people per se, threestudies were included as all had relevant data which could be con-sidered, although the potential for synthesis was limited. The singletheme extending across all three studies was the capacity and desirefor autonomous decision-making around environmental modifi-cation by older people with visual impairment, informed by butnot dependent on the recommendations of others such as healthprofessionals. Other themes elicited from one or two studies in-cluded: the influence of function, ambiance, safety, cleanliness anduse of cues in decision-making about environmental modification.Although there is a previous systematic review of the effect of in-terventions to reduce falls in older adults (Gillespie 2012), thereis no specific review of those with visual impairment. However,Gillespie 2012 did show that home safety interventions were moreeffective in reducing rate of falls in the higher risk subgroup ofolder people. They also found that there was some evidence thatoccupational therapy-led interventions on home safety assessmentwere more effective than non-occupational therapy-led interven-tions for reducing rate of falls.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
We are unable to reach any conclusion as to the evidence behindthe effectiveness of environmental or behavioural interventionsfor reducing physical activity limitation in community-dwellingvisually impaired older people, as no eligible studies were found.However, the fact that we have been unable to show a lack ofevidence of effect does not mean there is no effect, merely thatthere are no eligible studies addressing this issue.
A number of studies reviewed included only the secondary out-come measures of this review. Although behavioural interventionsdelivered by occupational therapists have been shown to reducethe rate of falls, we are unable to conclude if this is due to re-duced activity restriction (increased mobility) or reduced activity(lessening exposure to risk). There are inconclusive and conflict-ing results arising from the evaluation of behavioural and envi-ronmental interventions aimed at improving quality of life. Thisis perhaps because many intervention studies have not focused oncoping strategies to engage with leisure activities and have insteadfocused on essential activities of daily living.
As restricted activity can lead to declining mobility, to distress andanxiety, and to an increased risk of falls, healthcare professionalsneed to consider ways to facilitate people to increase physical ac-tivity and help remove the barriers to activity in older people withvisual impairment.
Implications for research
There is a gap in knowledge concerning the effectiveness of be-havioural and environmental interventions in reducing activity re-striction and improving quality of life in older people with irre-versible vision loss. Further research, such as ongoing Dutch, Aus-tralian and UK trials, considering the effectiveness of orientationand mobility training on activity restriction, physical activity, falls,fear of falling and quality of life in older adults with low vision,are necessary before any conclusions can be reached.
A C K N O W L E D G E M E N T S
The review authors would like to acknowledge the Cochrane Eyesand Vision Group (CEVG), in particular, Anupa Shah for her pa-tience and detailed help, and Iris Gordon, Trials Search Co-ordina-tor, for compiling the search strategy and searches and to MarionKelt (Librarian, Glasgow Caledonian University) for her help inlocal searches. They would like to thank the Thomas PocklingtonTrust for part funding the review and Dr Senay Aydin for help inretrieving the papers for review by the authors. Finally, they wouldlike to thank Gianni Virgili (author of the Orientation and mo-bility training for adults with low vision Cochrane Review) andMaaike Langelaan (author of the Multidisciplinary rehabilitationand monodisciplinary rehabilitation for visually impaired adultsCochrane Review) for help in ensuring our review protocol wascomplementary to theirs, and Catey Bunce and Giovanni Sato fortheir comments on the protocol for this review, and Jennifer Evansand Giavanni Giacomelli for their comments on the full review.
Richard Wormald (Co-ordinating Editor for CEVG) acknowl-edges financial support for his CEVG research sessions from theDepartment of Health through the award made by the NationalInstitute for Health Research to Moorfields Eye Hospital NHS
11Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Foundation Trust and UCL Institute of Ophthalmology for a Spe-cialist Biomedical Research Centre for Ophthalmology.
The views expressed in this publication are those of the authorsand not necessarily those of the NIHR, NHS or the Departmentof Health.
R E F E R E N C E S
References to studies excluded from this review
Balliet 1985 {published data only}
Balliet R, Blood KM, Bach-Y-Rita P. Visual fieldrehabilitation in the cortically blind?. Journal of Neurology,Neurosurgery and Psychiatry 1985;48(11):1113–24.
Campbell 2005b {published data only}Campbell AJ, Robertson MC, La Grow SJ, Kerse NM,
Sanderson GF, Jacobs RJ, et al.Randomised controlled trialof prevention of falls in people aged ≥75 with severe visual
impairment: the VIP trial. BMJ 2005;331(7520):817.La Grow SJ, Robertson MC, Campbell AJ, Clarke GA,
Kerse NM. Reducing hazard related falls in people 75 yearsand older with significant visual impairment: how did a
successful program work?. Injury Prevention 2006;12(5):296–301.
Cheung 2008 {published data only}
Cheung KK, Au KY, Lam WW, Jones AY. Effects of astructured exercise programme on functional balance in
visually impaired elderly living in a residential setting. HongKong Physiotherapy Journal 2008;26(1):45–50.
Conrod 1986 {published data only}
Conrod BE, Bross M, White CW. Active and passiveperceptual learning in the visually impaired. Journal ofVisual Impairment and Blindness 1986;80(1):528–31.
Cumming 2007 {published data only}Cumming RG, Ivers R, Clemson L, Cullen J, Hayes MF,
Tanzer M, et al.Improving vision to prevent falls in frailolder people: a randomised trial. Journal of the AmericanGeriatrics Society 2007;55(2):175–81.
Dahlin-Ivanoff 2002 {published data only}
Dahlin Ivanoff S, Sonn U, Svensson E. A health educationprogram for elderly persons with visual impairments and
perceived security in the performance of daily occupations:a randomised study. American Journal of OccupationalTherapy 2002;56(3):322–30.
Day 2002 {published data only}Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S.
Randomised factorial trial of falls prevention among olderpeople living in their own homes. BMJ 2002;325(7356):
128.
Deremeik 2007 {published data only}Deremeik J, Broman AT, Freidman D, West SK, Massof
R, Park W, et al.Low vision rehabilitation in a nursinghome population: The SEEING study. Journal of VisualImpairment and Blindness 2007;101(11):701–14.
Eklund 2007 {published data only}
Eklund K, Dahlin-Ivanoff S. Low vision ADL and hearingassistive device use among older persons with visual
impairments. Disability and Rehabilitation. AssistiveTechnology 2007;2(6):326–34.
Eklund 2008 {published data only}Eklund K, Sjöstrand J, Dahlin-Ivanoff S. A randomised
controlled trial of a health-promotion programme andits effect on ADL dependence and self reported health
problems for the elderly visually impaired. ScandinavianJournal of Occupational Therapy 2008;15(2):68–74.
Engel 2000 {published data only}
Engel RJ, Welsh RL, Lewis LJ. Improving the well-beingof vision-impaired older adults through orientation and
mobility training and rehabilitation: an evaluation. Review2000;32(2):67–76.
Girdler 2010 {published data only}Girdler SJ, Boldy DP, Dhaliwal SS, Crowley M, Packer TL.
Vision self-management for older adults: a randomisedcontrolled trial. British Journal of Ophthalmology 2010;94
(2):223–8.
Gutman 2002 {published data only}Gutman C, Jaffe K. Group intervention for visually
impaired grandparents. Journal of Visual Impairment andBlindness 2002;96(10):741–3.
Kuyk 2008 {published data only}Kuyk T, Liu L, Elliott JL, Grubbs HE, Owsley C, McGwim
G Jr, et al.Health-related quality of life following blindrehabilitation. Quality of Life Research 2008;4(17):497–507.
Kuyk 2010 {published data only}
Kuyk T, Liu L, Elliott J, Fuhr B. Visual search trainingand obstacle avoidance in adults with visual impairments.
Journal of Visual Impairment and Blindness 2010;104(4):215–27.
La Grow 2004 {published data only}
La Grow SJ. The effectiveness of comprehensive low visionservices for older persons with visual impairments in New
Zealand. Journal of Visual Impairment and Blindness 2004;98(11):679–92.
McCabe 2000 {published data only}
McCabe P, Nason F, Demers Turco P, Friedman D, SeddonJM. Evaluating the effectiveness of a vision rehabilitation
intervention using an objective and subjective measure offunctional performance. Ophthalmic Epidemiology 2000;7
(4):259–70.
12Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Overbury 1996 {published data only}
Overbury O, Quillman RD. Perceptual learning inadventitious low vision: task specificity and practice.
Journal of Vision Rehabilitation 1996;10(1):7–14.
Pankow 2004 {published data only}Pankow L, Luchins D, Studebaker J, ChettleburghD. Evaluation of a vision rehabilitation program with
older adults with visual impairment. Topics in GeriatricRehabilitation 2004;20(3):223–32.
Reeves 2004 {published data only}
Reeves BC, Harper RA, Russell WB. Enhanced lowvision rehabilitation for people with age related macular
degeneration: a randomised controlled trial. British Journalof Opthalmology 2004;88(11):1443–49.
Rumrill 1999 {published data only}Rumrill PD. Effects of a social competence training program
on accomodation request activity, situational self efficacy,and Americans with disabilities act knowledge among
employed people with visual impairments and blindness.Journal of Vocational Rehabilitation 1999;12(1):25–31.
Scanlan 2004 {published data only}Scanlan JM, Cuddeford JE. Low vision rehabilitation: A
comparison of traditional and extended teaching programs.Journal of Visual Impairment and Blindness 2004;98(10):
601–10.
Smith 2009 {published data only}Smith TM, Thomas K, Dow K. The effect of an educational
program for persons with macular degeneration; A pilotstudy. Journal of Visual Impairment and Blindness 2009;103
(4):234–40.
Stelmack 2005 {published data only}
Stelmack J, Mancil R, Mancil G, Cummings R, Moran D,Rinne S, et al.Veterans Affairs Low Vision Intervention Trial
(LOVIT). Investigative Ophthalmology and Visual Science2005;46:E-Abstract 1920.
Stelmack J, Tang C, Reda D, Rinne S, Mancil R, CummingsRW, et al.The Veterans Affairs low vision intervention trial
follow up: twelve month outcomes. American Academy ofOptometry 2008;12:644–7.
Stelmack JA, Rinne S, Mancil RM, Dean D, Moran D,Tang XC, et al.Successful outcomes from a structured
curriculum used in the Veterans Affairs Low interventionTrial. Journal of Visual Impairment and Blindness 2008;102
(10):636–48.Stelmack JA, Tang XC, Reda DJ, Rinne S, Mancil
RM, Massof RW, et al.Outcomes of the Veteran AffairsLow Vision Intervention trial (LOVIT). Archives ofOphthalmology 2008;126(5):608–17.
Vukicevic 2009 {published data only}
Vukicevic M, Fitzmaurice K. Eccentric viewing trainingin the home environment: can it improve performance of
activities of daily living?. Journal of Visual Impairment andBlindness 2009;103(5):277–90.
West 2004 {published data only}West SK, Friedman DF, Broman AT, Munoz B, Bandeen-
Roche K, Deremeik J, et al.Effect of a vision restoration/
rehabilitation program on physical function in a population
of nursing home residents with visual loss. SEEINGClinical Trial. Investigative Ophthalmology and Visual Science2004;45:E-Abstract 1362.
References to ongoing studies
ACTRN12607000399493 {unpublished data only}
ACTRN12607000399493. A randomised controlled trialof a low vision self management program on quality of
life in people with low vision. apps.who.int/trialsearch/Trial.aspx?TrialID=ACTRN12607000399493 (accessed 13
December 2012).
NCT00545220 {unpublished data only}
NCT00545220. Problem solving training and low visionrehabilitation. clinicaltrials.gov/ct2/show/NCT00545220
(accessed 13 December 2012).
NCT00769015 {unpublished data only}NCT00769015. Low Vision Depression Prevention
Trial for Age Related Macular Degeneration (VITAL).clinicaltrials.gov/show/NCT00769015 (accessed 13
December 2012).
UKCRN ID 10883 {unpublished data only}
UKCRN ID 10883. Preventing falls in older peoplewith a visual impairment. public.ukcrn.org.uk/search/
StudyDetail.aspx?StudyID=10883.
Zijlstra 2009 {unpublished data only}
Zijlstra GA, van Rens GH, Scherder EJ, Brouwer DM, vander Velde J, Verstraten BF, et al.Effects and feasibility of a
standardised orientation and mobility training in using anidentification cane for older adults with low vision: design
of a randomised controlled trial. BMC Health ServicesResearch 2009;9:153.
Additional references
Ballinger 2009
Ballinger C, Neil F, Howe T, Skelton DA, Palmer S, Gray L.A qualitative evidence synthesis of the views and experiences
of older people with visual impairment about interventionsto reduce falls. Unpublished report submitted to the
Thomas Pocklington Trust. 2009.
Bamashmus 2004
Bamashmus MA, Matlhaga B, Dutton GN. Causes ofblindness and visual impairment in the west of Scotland.
Eye 2004;18(3):257–61.
Berger 2012Berger S. Is my world getting smaller? The challenges of
living with vision loss. Journal of Visual Impairment andBlindness 2012;106(1):5–16.
Binns 2012Binns A, Bunce C, Dickinson C, Harper R, Tudor-Edwards
R, Woodhouse M, et al.How effective is low vision serviceprovision? A systematic review. Survey of Opthalmology2012;57(1):34–65.
13Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Brouwer 2008
Brouwer D, Sadlo G. Limitations in mobility: experiencesof visually impaired older people. British Journal ofOccupational Therapy 2008;71(10):414–21.
Campbell 2005a
Campbell S. Deteriorating vision, falls and older people:the links. www.visibility.org.uk/what-we-do/research/#Falls
(accessed 7 August 2009).
Clemson 2003
Clemson L, Manor D, Fitzgerald MH. Behavioral factorscontributing to older adults falling in public places. OTJR:Occupation, Participation and Health 2003;23(3):107–17.
Clemson 2008
Clemson L, Mackenzie L, Ballinger C, Close JC, CummingRG. Environmental interventions to prevent falls in
community-dwelling older people: a meta-analysis ofrandomized trials. Journal of Aging Health 2008;20(8):
954–71.
Crews 2004Crews JE, Campbell VA. Vision impairment and hearing
loss among community-dwelling older Americans:implications for health and functioning. American Journalof Public Health 2004;94(5):823–9.
Deeks 2011
Deeks JJ, Higgins JPT, Altman DG. Chapter 9: Analysingdata and undertaking meta-analyses. In: Higgins JPT,
Green S (editors). Cochrane Handbook for SystematicReviews of Interventions Version 5.1.0 (updated March
2011). The Cochrane Collaboration, 2011. Available fromwww.handbook-cochrane.org.
Dreer 2008Dreer LE, Elliott TR, Berry J, Fletcher DC, Swanson M,
Christopher McNeal J. Cognitive appraisals, distress anddisability among persons in low vision rehabilitation. BritishJournal of Health Psychology 2008;13(Pt 3):449–61.
Evans 2002Evans JR, Fletcher AE, Wormald RP, Ng ES, Stirling S,
Smeeth L, et al.Prevalence of visual impairment in peopleaged 75 years and older in Britain: results from the MRC
trial of assessment and management of older people in thecommunity. British Journal of Opthalmology 2002;86(7):
795–800.
Evans 2004Evans JR, Fletcher AE, Wormald RP. Causes of visual
impairment in people aged 75 years and older in Britain:an add-on study to the MRC Trial of Assessment and
Management of Older People in the Community. BritishJournal of Ophthalmology 2004;88(3):365–70.
Evans 2007
Evans JR, Fletcher AE, Wormald RP. Depression andanxiety in visually impaired older people. Opthalmology2007;114(2):283–8.
Gillespie 2012
Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C,Gates S, Clemson LM, et al.Interventions for preventing
falls in older people living in the community. CochraneDatabase of Systematic Reviews 2012, Issue 9. [DOI:10.1002/14651858.CD007146.pub2]
Glanville 2006Glanville JM, Lefebvre C, Miles JN, Camosso-Stefinovic J.
How to identify randomized controlled trials in MEDLINE:ten years on. Journal of the Medical Library Association 2006;
94(2):130–6.
Green 2007
Green S, Higgins JPT, Schünemann HJ, Becker L. Responseto paper by Lang A, Edwards N, and Fleiszer A. Journal ofClinical Epidemiology 2007;60:598–99.
Gregg 2000Gregg EW, Pereira MA, Caspersen CJ. Physical activity,
falls, and fractures among older adults: a review of theepidemiologic evidence. Journal of the American GeriatricsSociety 2000;48(8):883–93.
Higgins 2003
Higgins JP, Thompson SG, Deeks JJ, Altman DG.Measuring inconsistency in meta-analysis. BMJ 2003;327
(7414):557–60.
Higgins 2011
Higgins JPT, Altman DG, Sterne JAC (editors). Chapter8: Assessing risk of bias in included studies. In: Higgins
JPT, Green S (editors). Cochrane Handbook for SystematicReviews of Interventions Version 5.1.0 (updated March
2011). The Cochrane Collaboration, 2011. Available fromwww.handbook-cochrane.org.
Holbrook 2011
Holbrook EA, Stevens SL, Kang M, Morgan DW. Validationof a talking pedometer for adults with visual impairment.
Medicine Science Sports and Exercise 2011;43(6):1094–9.
Ivers 1998Ivers RQ, Cumming RG, Mitchell P, Attebo K. Visual
impairment and falls in older adults: The Blue MountainsEye Study. Journal of the American Geriatrics Society 1998;
46(1):58–64.
Klein 2003Klein B, Moss S, Klein R, Lee K, Cruickshanks K.
Associations of visual function with physical outcomes andlimitations 5 years later in an older population:The Beaver
Dam eye study. Ophthalmology 2003;110(4):644–50.
La Grow 2006
La Grow SJ, Robertson MC, Campbell AJ, Clarke GA,Kerse NM. Reducing hazard related falls in people 75 years
and older with significant visual impairment: how did asuccessful program work?. Injury Prevention 2006;12(5):
296–301.
Lamb 2005Lamb SE, Jorstad-Stein EC, Hauer K, Becker C.
Development of a common outcome data set for fall injuryprevention trials: The Prevention of Falls Network Europe
consensus. Journal of the American Geriatrics Society 2005;53(9):1618–22.
14Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lang 2007
Lang A, Edwards N, Fleiszera A. Empty systematic reviews:hidden perils and lessons learned. Journal of ClinicalEpidemiology 2007;60(6):595–7.
Langelaan 2007Langelaan M, van Nispen RMA, van Rens GHMB.
Multidisciplinary rehabilitation and monodisciplinaryrehabilitation for visually impaired adults. CochraneDatabase of Systematic Reviews 2007, Issue 2. [DOI:10.1002/14651858.CD006543]
Legood 2002Legood R, Scuffham P, Cryer C. Are we blind to injuries
in the visually impaired? A review of the literature. InjuryPrevention 2002;8(2):155–60.
Markowitz 2006a
Markowitz SN. Principles of modern low visionrehabilitation. Canadian Journal of Ophthalmology 2006;41
(3):289–312.
Markowitz 2006bMarkowitz M. Occupational therapy interventions in low
vision rehabilitation. Canadian Journal of Ophthalmology2006;41(3):340–7.
Murphy 2002
Murphy SL, Williams CS, Gill TM. Characteristicsassociated with fear of falling and activity restriction in
community-living older persons. Journal of the AmericanGeriatrics Society 2002;50(3):516–20.
Preedy 2009
Preedy VR, Watson RR. Handbook of disease burdens andquality of life measures. New York: Springer, 2009.
Resnikoff 2004
Resnikoff S, Pascolini D, Etya’ale D, Kocur I,Pararajasegaram R, Pokharel GP, et al.Global data on visual
impairment in the year 2002. Bulletin of the World HealthOrganization 2004;82(11):844–52.
Resnikoff 2008
Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Globalmagnitude of visual impairment caused by uncorrected
refractive errors in 2004. Bulletin of the World HealthOrganization 2008;86(1):63–70.
Salive 1994
Salive ME, Guralnik J, Glynn RJ, Christen W, WallaceRB, Ostfeld AM. Association of visual impairment with
mobility and physical function. Journal of the AmericanGeriatrics Society 1994;42(3):287–92.
Schünemann 2011Schünemann HJ, Oxman AD, Higgins JPT, Vist GE,
Glasziou P, Guyatt GH. Chapter 11: Presenting resultsand Summary of findings tables. In: Higgins JPT, Green
S (editors), Cochrane Handbook for Systematic Reviewsof Interventions Version 5.1.0 (updated March 2011).
The Cochrane Collaboration, 2011. Available from
www.handbook-cochrane.org.
Stelmack 2008a
Stelmack J, Tang C, Reda D, Rinne S, Mancil R, CummingsRW, et al.The Veterans Affairs low vision intervention trial
follow up: twelve month outcomes. American Academy ofOptometry 2008;12:644–7.
Stelmack 2008b
Stelmack JA, Rinne S, Mancil RM, Dean D, Moran D,Tang XC, et al.Successful outcomes from a structured
curriculum used in the Veterans Affairs Low interventionTrial. Journal of Visual Impairment and Blindness 2008;102
(10):636–48.
Stelmack 2008c
Stelmack JA, Tang XC, Reda DJ, Rinne S, MancilRM, Massof RW, et al.Outcomes of the Veteran Affairs
Low Vision Intervention trial (LOVIT). Archives ofOphthalmology 2008;126(5):608–17.
Stevens 2001Stevens M, Holman CD, Bennett N, De Klerk N.
Preventing falls in older people: outcome evaluation ofa randomized controlled trial. Journal of the AmericanGeriatrics Society 2001;49(11):1448–55.
Tinetti 1998Tinetti ME, Williams CS. The effect of falls and fall injuries
on functioning in community-dwelling older persons.Journals of Gerontology. Series A, Biological Sciences andMedical Sciences 1998;53(2):M112–9.
Virgili 2003
Virgili G, Rubin G. Orientation and mobility trainingfor adults with low vision. Cochrane Database ofSystematic Reviews 2003, Issue 1. [DOI: 10.1002/14651858.CD003925]
WHO 1992
World Health Organization. ICD-10:Internationalstatistical classification of diseases and related health
problems: tenth revision. Geneva:World HealthOrganization 1992.
WHO 2001
World Health Organization. ICIDH-2: InternationalClassification of Functioning, Disability and Health. 1st
Edition. Geneva: World Health Organization, 2001.
WHO 2007
World Health Organization. A guide for population-basedapproaches to increasing levels of physical activity. Geneva:
World Health Organization, 2007.
Yardley 2002Yardley L, Smith H. A prospective study of the relationship
between feared consequences of falling and avoidance ofactivity in community-living older people. Gerontologist2002;42(1):17–23.
∗ Indicates the major publication for the study
15Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Balliet 1985 Although an RCT, not a behavioural/environmental intervention (visual field training) and no physical activityoutcome measures
Campbell 2005b Although an RCT, aim of intervention was not to decrease physical activity limitation and no physical activityoutcome measures. Falls as secondary outcome measure. La Grow 2006 is an article about implementing thisRCT.
Cheung 2008 Although an RCT, aim of intervention was not to decrease physical activity limitation and no physical activityoutcome measures. Balance measures assessed. Although one aim was to increase confidence in safe ambulationthis was not assessed
Conrod 1986 Although an RCT, not a behavioural/environmental intervention (residual vision training) and no physicalactivity outcome measures
Cumming 2007 Although an RCT, aim of intervention was not to decrease physical activity limitation and no physical activityoutcome measures. Falls as secondary outcome measure. Most had change in glasses, with only a few havingan occupational therapy Intervention
Dahlin-Ivanoff 2002 Although an RCT, outcome measure was perceived security in the performance of daily occupations ratherthan a subjective or objective measure of physical activity or change in physical activity
Day 2002 Although an RCT, aim of intervention was not to decrease physical activity limitation and no physical activityoutcome measures. Falls as secondary outcome measure
Deremeik 2007 Although an RCT, aim of intervention was not to decrease physical activity limitation and no physical activityoutcome measures. Outcomes were rehabilitation goals and visual correction. Residents were based in anursing home
Eklund 2007 Although an RCT, aim of intervention was changing associations between assistive living devices and ADLdependence. No physical activity outcome measures
Eklund 2008 Although an RCT, aim of intervention was ADL dependence and self-reported health problems. No physicalactivity outcome measures
Engel 2000 Not an RCT or quasi-RCT. Physical activity outcomes not well reported and not validated
Girdler 2010 Although an RCT, aimed to increase participation in life situations but no physical activity outcome measures
Gutman 2002 Not an RCT or quasi-RCT and no physical activity outcome measures
Kuyk 2008 Not an RCT or quasi-RCT and no physical activity outcome measures
16Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
Kuyk 2010 Although an RCT, not a behavioural/environmental intervention (computerised vision training) and nophysical activity outcome measures
La Grow 2004 Not an RCT or quasi-RCT and no physical activity outcome measures
McCabe 2000 Not an RCT or quasi-RCT and no physical activity outcome measures
Overbury 1996 Although an RCT, not a behavioural/environmental intervention (perceptual learning training - paper-based)and no physical activity outcome measures
Pankow 2004 Although an RCT, aimed to improve wellbeing. No physical activity outcome measures
Reeves 2004 Although an RCT, aimed to improve quality of life. No physical activity outcome measures
Rumrill 1999 Although an RCT, not a behavioural/environmental intervention (skills at requesting accommodation fromemployers for employees so few older people) and no physical activity outcome measures
Scanlan 2004 Although an RCT, not a behavioural/environmental intervention (microscopes) to extend reading time) andno physical activity outcome measures
Smith 2009 Although an RCT, not a behavioural/environmental intervention (educational programme on self care, foodpreparation, home and financial management) and no physical activity outcome measures
Stelmack 2005 Abstract only. Protocol for an RCT study and no activity outcome measures. Relates to Stelmack 2008a;Stelmack 2008b and Stelmack 2008c.
Vukicevic 2009 Although an RCT, not a behavioural/environmental intervention (eccentric viewing computerised training)and no physical activity outcome measures
West 2004 Abstract only. Protocol for an RCT study and no activity outcome measures. Contacted author. Residents arebased in a nursing home
RCT: randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12607000399493
Trial name or title A randomised controlled trial of a low vision self management programme on quality of life in people withlow vision
Methods Randomised controlled trial Parallel
Participants Age 55 years and older, male and femaleInclusion criteria: Participants are clients of Vision Australia centres who have received a low vision assessment
17Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ACTRN12607000399493 (Continued)
within the last 12 months and meet the following inclusion criteria:i. visual acuity of < 6/12 and > 6/480 in the better eye with habitual correction;ii. age 55 years or older;iii. living independently (not in a nursing home);iv. English-speaking;v. no cognitive impairment as assessed by the six-item cognitive impairment test (Brooke & Bullock, 1999);vi. adequate hearing to respond to normal conversation.Exclusion criteria: Nil
Interventions Participants are randomised to receive either the new low vision self-management programme ’Living withLow Vision’ or continued access to usual low vision rehabilitation services.
The ’Living with Low Vision’ programme has been developed specifically for this study. It consists of eight 3-hour weekly facilitated group sessions. The programme is structured and a facilitator manual clearly outlinesthe content and delivery. As well as providing information, the topics in the programme are covered byexploring participants’ experiences, difficulties and solutions. Participants are encouraged to draw on theirextensive life experience and coping mechanisms and to develop new skills and strategies and apply thesenew techniques in their daily life. Participants are given the option to bring a relative, friend or carer to theprogramme with them
Outcomes Primary:The Impact of Vision Impairment Questionnaire (IVI) is used to assess the restriction of participation indaily activities in people with low vision (Lamoureux, Pallant, Pesudovs, Hassell, & Keeffe, 2006). The 28-item IVI has been extensively validated and has been shown to be sensitive to rehabilitation-induced changesin people with low vision.
The Depression Anxiety Stress Scale (DASS) is used to assess psychological wellbeing (Henry & Crawford,2005; Lovibond & Lovibond, 2004). This is a 21-item self-report measure that provides three 7-item subscalesof negative affect: depression, anxiety and stressSecondary:Adaptation to Age-related Vision Loss Scale (AVL-12) is used to assess psychosocial adaptation to vision loss,including acceptance of limitations, attitudes towards rehabilitation and appropriate help from family andfriends (Horowitz & Reinhardt, 2006)The General Self-Efficacy Scale (GSES) is used to assess general self-efficacy (Jerusalem & Schwarzer, 1992)The Health Education Impact Questionnaire (HEIQ) scales: ’Skill and technique acquisition’ (five items) and’Positive and active engagement in life’ (five items) are used to determine the direct impact of the programmeon strategies to manage low vision and engagement in life (Nolte, Elsworth, Sinclair, & Osborne, 2006)The Positive and Negative Affect Schedule (PANAS) is used to assess the both positive and negative mood(Watson, Clark, & Tellegen, 1988)
Starting date 1/03/2007
Contact information Jill Keefe
Notes
18Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

NCT00545220
Trial name or title Problem Solving Training and Low Vision Rehabilitation
Methods Randomised controlled trial Parallel
Participants Aged 19 and over (including older people), male and female.Inclusion Criteria:
• +19 yrs of age;• Underwent a low vision rehabilitation initial eye exam;• No more than 2 errors on cognitive on cognitive screening measure (SPBS);• Must have access to telephone;• No significant hearing problems;• No significant communication problems;• Speaks fluent English.
Exclusion Criteria: Nil
Interventions Participants are randomised to:Experimental Group - Behavioural: problem-solving trainingSham Comparator - Behavioural: Sham
Outcomes No information
Starting date October 2007
Contact information Laura Dreer
Notes
NCT00769015
Trial name or title Low Vision Depression Prevention Trial for Age Related Macular Degeneration (VITAL)
Methods Randomised,controlled clinical trial
Participants Aged 65 years and older, male and femaleInclusion Criteria: bilateral AMD and subthreshold depressive symptoms. At least 1 vision goal that isimportant yet difficult to carry outExclusion Criteria: healthy older people;
• Uncontrolled glaucoma, diabetic retinopathy, corneal dystrophy, or cataracts for which surgery withinsix months is likely will be exclusionary conditions;
• Current diagnosis of depression;• Cognitive impairment;• Life-threatening illness or any other health conditions that interfere with study activities;• Patients who have received low vision rehabilitation or home-based occupational therapy (OT) in the
preceding 12 months will be excluded.
Interventions Collaborative Low Vision Rehabilitation (LVR) (optometrist and home-based occupational therapist (OT))or enhanced LVR (optometrist and home-based Supportive Therapy (ST)). In this study, usual care LVR isenhanced with ST, which is a standardised placebo psychological treatment that controls for attentionIn BA-LVR, a low vision OT will deliver Behavior Activation (BA), a psychological treatment to prevent
19Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

NCT00769015 (Continued)
depression. This will be administered in the context of the standard of low vision care for OTs as defined by theAmerican Occupational Therapy Association (AOTA). The OTs will collaborate with low vision optometrists,who will deliver the standard of low vision care as defined by the American Optometric Association. Theoptometrists will evaluate remaining vision and magnification needs, prescribe optical devices, and providethe OTs with initial care plans. The OTs will subsequently meet with participants in their homes six timesover 12 weeks to enhance device use, home modifications, and compensatory strategies
Outcomes Primary Outcome Measures: DepressionSecondary Outcome Measures: Vision Function and Quality of Life
Starting date June 2009
Contact information Robin Casten
Notes
UKCRN ID 10883
Trial name or title VIP2UK: Preventing falls in older people with a visual impairment
Methods Pilot randomised controlled trial
Participants Aged 75 years and over• Independent community-dwelling;• Able to walk around their own residence;• Cognitively able to participate in the programme;• Able to understand the study requirements.
Vision-related inclusion criteria:• Binocular visual acuity less than 0.6 LogMAR (Snellen equivalent 6/24), stratified into (i) 0.61.0
LogMAR (1.0 LogMar = Snellens 6/60), (ii) less than 1.0 LogMAR, and/or• Moderate visual field loss, defined as affecting more than 20% of the test location used in a binocular
Estermann test, stratified into (i) those missing < 50% of the test locations, (ii) those missing > 50% of thetest location.
Interventions Occupational therapist delivering home safety assessment and modifications with the approval of visually-impaired older people. Occupational therapist delivering the Otago home exercise programme, with supportof peer mentors (buddies) that provide additional home visits and telephone calls throughout the intervention
Outcomes PhoneFITT physical activity questionnaire, quality of life.
Starting date May 2011
Contact information H. Waterman
Notes
20Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Zijlstra 2009
Trial name or title Evaluation of a standardised orientation and mobility training in older adults with low vision
Methods Randomised controlled trial
Participants Older adults (55 yrs and older) with low vision living in the community
Interventions Standardised Orientation and Mobility (O&M) Training versus Regular O&M Training (comparator)
Outcomes Primary Outcomes: Activities of daily life (subscale of the Groningen Activity Restriction Scale (GARS)),Distance activities and mobility (subscales of the Visual Functioning Questionnaire (VFQ))Secondary Outcomes: activities index (Frenchay Activities Index (FAI)), social support interactions (SocialSupport List (SSL 12-I)), health-related quality of life (EuroQol 5D (EQ5D)), feelings of anxiety (anxietysubscale of the Hospital Anxiety and Depression Scale (HADS-A)), concerns about falling (falls efficacy scaleinternational (FES-I))
Starting date Nov 2007
Contact information G.I.J.M. Kempen
Notes Information on the training delivered - http://www.ncbi.nlm.nih.gov/pubmed/22734105
21Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
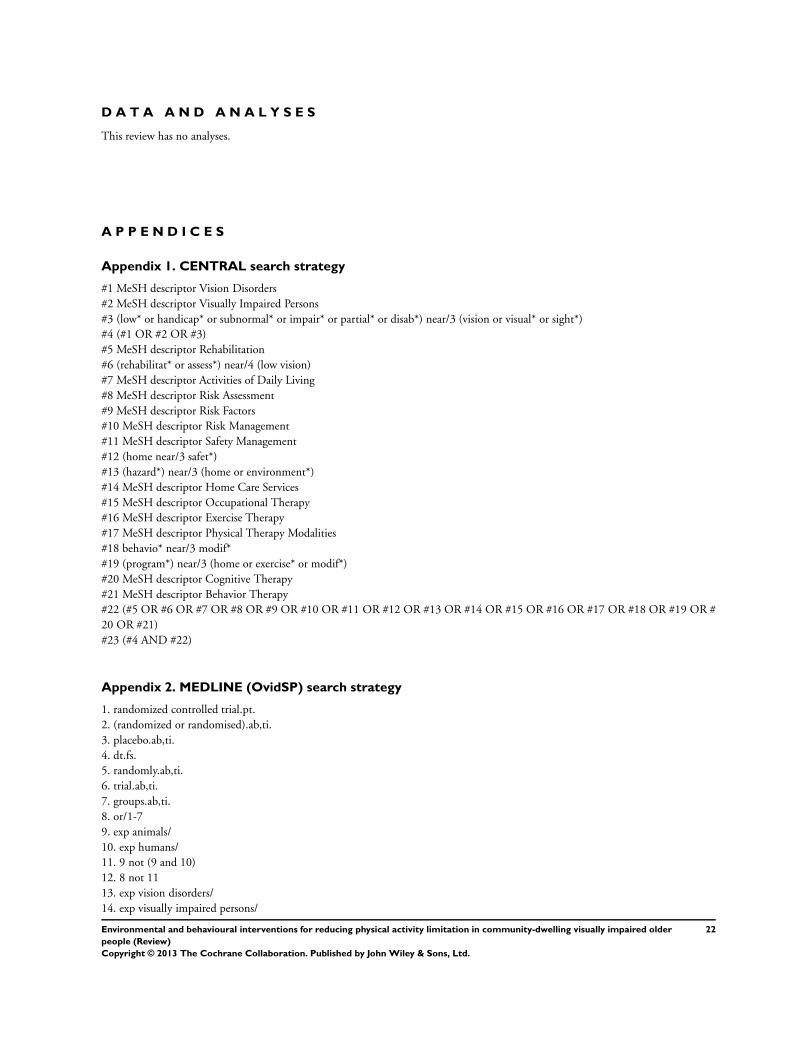
D A T A A N D A N A L Y S E S
This review has no analyses.
A P P E N D I C E S
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor Vision Disorders#2 MeSH descriptor Visually Impaired Persons#3 (low* or handicap* or subnormal* or impair* or partial* or disab*) near/3 (vision or visual* or sight*)#4 (#1 OR #2 OR #3)#5 MeSH descriptor Rehabilitation#6 (rehabilitat* or assess*) near/4 (low vision)#7 MeSH descriptor Activities of Daily Living#8 MeSH descriptor Risk Assessment#9 MeSH descriptor Risk Factors#10 MeSH descriptor Risk Management#11 MeSH descriptor Safety Management#12 (home near/3 safet*)#13 (hazard*) near/3 (home or environment*)#14 MeSH descriptor Home Care Services#15 MeSH descriptor Occupational Therapy#16 MeSH descriptor Exercise Therapy#17 MeSH descriptor Physical Therapy Modalities#18 behavio* near/3 modif*#19 (program*) near/3 (home or exercise* or modif*)#20 MeSH descriptor Cognitive Therapy#21 MeSH descriptor Behavior Therapy#22 (#5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21)#23 (#4 AND #22)
Appendix 2. MEDLINE (OvidSP) search strategy
1. randomized controlled trial.pt.2. (randomized or randomised).ab,ti.3. placebo.ab,ti.4. dt.fs.5. randomly.ab,ti.6. trial.ab,ti.7. groups.ab,ti.8. or/1-79. exp animals/10. exp humans/11. 9 not (9 and 10)12. 8 not 1113. exp vision disorders/14. exp visually impaired persons/
22Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
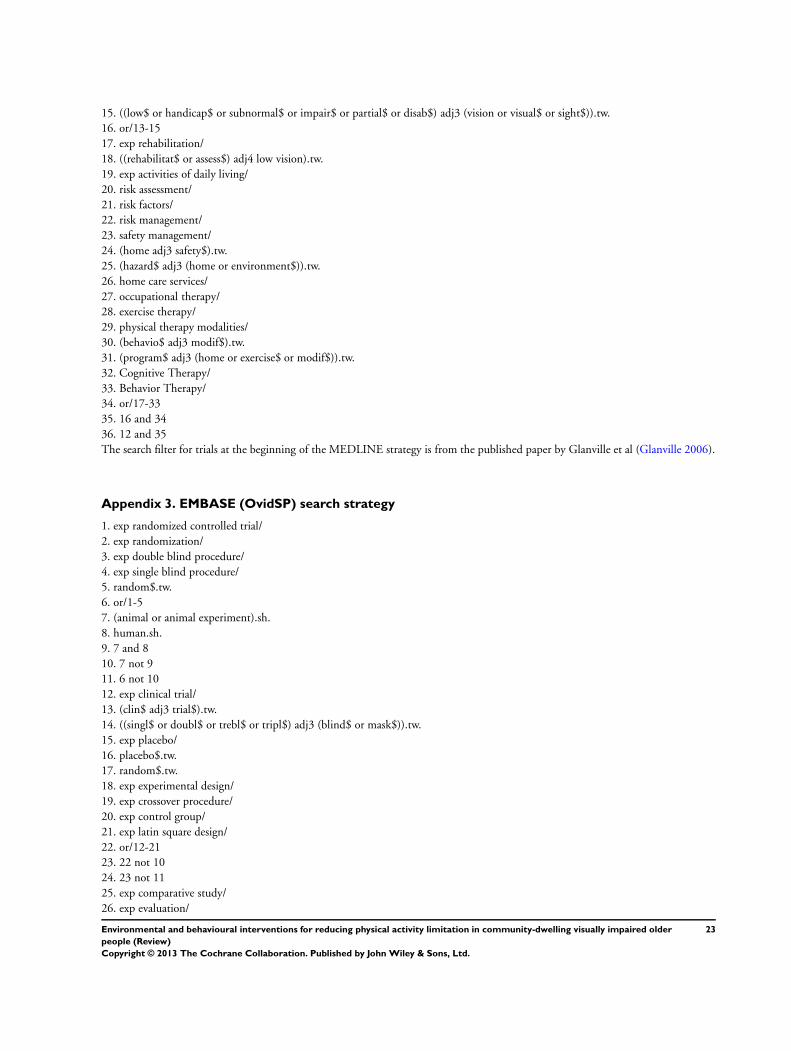
15. ((low$ or handicap$ or subnormal$ or impair$ or partial$ or disab$) adj3 (vision or visual$ or sight$)).tw.16. or/13-1517. exp rehabilitation/18. ((rehabilitat$ or assess$) adj4 low vision).tw.19. exp activities of daily living/20. risk assessment/21. risk factors/22. risk management/23. safety management/24. (home adj3 safety$).tw.25. (hazard$ adj3 (home or environment$)).tw.26. home care services/27. occupational therapy/28. exercise therapy/29. physical therapy modalities/30. (behavio$ adj3 modif$).tw.31. (program$ adj3 (home or exercise$ or modif$)).tw.32. Cognitive Therapy/33. Behavior Therapy/34. or/17-3335. 16 and 3436. 12 and 35The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville et al (Glanville 2006).
Appendix 3. EMBASE (OvidSP) search strategy
1. exp randomized controlled trial/2. exp randomization/3. exp double blind procedure/4. exp single blind procedure/5. random$.tw.6. or/1-57. (animal or animal experiment).sh.8. human.sh.9. 7 and 810. 7 not 911. 6 not 1012. exp clinical trial/13. (clin$ adj3 trial$).tw.14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw.15. exp placebo/16. placebo$.tw.17. random$.tw.18. exp experimental design/19. exp crossover procedure/20. exp control group/21. exp latin square design/22. or/12-2123. 22 not 1024. 23 not 1125. exp comparative study/26. exp evaluation/
23Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

27. exp prospective study/28. (control$ or prospectiv$ or volunteer$).tw.29. or/25-2830. 29 not 1031. 30 not (11 or 23)32. 11 or 24 or 3133. exp vision disorder/34. exp visual impairment/35. ((low$ or handicap$ or subnormal$ or impair$ or partial$ or disab$) adj3 (vision or visual$ or sight$)).tw.36. or/33-3537. exp rehabilitation/38. ((rehabilitat$ or assess$) adj4 low vision).tw.39. exp daily life activities/40. risk assessment/41. risk factor/42. exp home safety/43. (home adj3 safety$).tw.44. exp falling/45. (hazard$ adj3 (home or environment$)).tw.46. home care/47. occupational therapy/48. kinesiotherapy/49. exp physiotherapy/50. (behavio$ adj3 modif$).tw.51. (program$ adj3 (home or exercise$ or modif$)).tw.52. Cognitive Therapy/53. Behavior Therapy/54. or/37-5355. 36 and 5456. 32 and 55
Appendix 4. CINAHL (EBSCO) search strategy
S42 S40 and S41S41 (MH “Aged+”) OR (MH “Aged, 80 and Over”) OR (MH “Frail Elderly”)S40 S12 and S39S39 S20 and S38S38 S21 or S22 or S23 or S24 or S25 or S26 or S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37S37 (MH “Behavior Therapy+”) OR (MH “Behavior Therapy (Iowa NIC) (Non-Cinahl)”)S36 (MH “Cognitive Therapy”) OR (MH “Cognitive Therapy (Iowa NIC) (Non-Cinahl)”)S35 TX ((program* n3 home) or (program* n3 exercise) or (program* n3 modif*))S34 TX behavio* n3 modif*S33 (MH “Physical Therapy”)S32 (MH “Exercise Therapy: Ambulation (Iowa NIC)”) OR (MH “Exercise Therapy: Balance (Iowa NIC)”)S31 (MH “Occupational Therapy+”)S30 (MH “Home Health Care”)S29 TX ((hazard* n3 home) or (hazard* n3 environment*))S28 TX home n3 safety*S27 (MH “Risk Management”) OR (MH “Risk Management (Iowa NIC) (Non-Cinahl)”)S26 (MH “Risk Factors”)S25 (MH “Risk Assessment”) OR (MH “Fall Risk Assessment Tool”)
24Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S24 (MH “Activities of Daily Living+”) OR (MH “Activities of Daily Living (Saba CCC)”) OR (MH “Activities of Daily LivingAlteration (Saba CCC)”) OR (MH “Instrumental Activities of Daily Living (Saba CCC)”) OR (MH “Instrumental Activities of DailyLiving Alteration (Saba CCC)”) OR (MH “Altered Activities of Daily Living (NANDA) (Non-Cinahl)”) OR (MH “Self Care: Activitiesof Daily Living (Iowa NOC)”) OR (MH “Self-Care: Instrumental Activities of Daily Living (Iowa NOC)”)S23 TX assess* n4 vision*S22 TX rehabilitat* n4 vision*S21 (MH “Rehabilitation of Vision Impaired+”)S20 S13 or S14 or S15 or S16 or S17 or S18 or S19S19 TX ((disab* n3 vision) or (disab* n3 visual*) or (disab* n3 sight))S18 TX ((partial* n3 vision) or (partial* n3 visual*) or (partial* n3 sight))S17 TX ((impair* n3 vision) or (impair* n3 visual*) or (impair* n3 sight))S16 TX ((subnormal* n3 vision) or (subnormal* n3 visual*) or (subnormal* n3 sight))S15 TX ((handicap* n3 vision) or (handicap* n3 visual*) or (handicap* n3 sight))S14 TX ((low* n3 vision) or (low* n3 visual*) or (low* n3 sight))S13 (MH “Vision Disorders+”)S12 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11S11 TX allocat* random*S10 (MM “Quantitative Studies”)S9 (MM “Placebos”)S8 TX placebo*S7 TX random* allocat*S6 (MM “Random Assignment”)S5 TX randomi* control* trial*S4 TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl*n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) )S3 TX clinic* n1 trial*S2 PT Clinical trialS1 (MH “Clinical Trials+”)
Appendix 5. AMED (OvidSP) search strategy
1. vision disorders/2. ((low$ or handicap$ or subnormal$ or impair$ or partial$ or disab$) adj3 (vision or visual$ or sight$)).tw.3. or/1-24. Rehabilitation/5. ((rehabilitat$ or assess$) adj4 low vision).tw.6. “Activities of daily living”/7. Risk/8. Safety/9. (home adj3 safety$).tw.10. (hazard$ adj3 (home or environment$)).tw.11. Home care services/12. Occupational therapy/13. Exercise therapy/14. physical therapy modalities/15. (behavio$ adj3 modif$).tw.16. (program$ adj3 (home or exercise$ or modif$)).tw.17. Cognitive therapy/18. Behavior therapy/19. or/4-1820. 3 and 1921. “Randomized controlled trials”/
25Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

22. prospective studies/23. single blind method/24. random$.tw.25. placebo$.tw.26. trial$.tw.27. groups.tw.28. ((singl$ or doubl$) adj3 (blind$ or mask$)).tw.29. or/21-2830. 20 and 29
Appendix 6. OTseeker search strategy
low vision AND rehabilitation AND random
Appendix 7. metaRegister of Controlled Trials search strategy
low vision and rehabilitation
Appendix 8. ClinicalTrials.gov search strategy
Low Vision AND Rehabilitation
Appendix 9. ICTRP search strategy
Low Vision AND Rehabilitation
C O N T R I B U T I O N S O F A U T H O R S
Skelton, Ballinger, Neil and Howe conceived and developed the protocol. Gray and Palmer commented on drafts of the protocol andsearch strategies. Skelton and Howe reviewed all selected publications, with Gray as adjudicator. Ballinger, Howe, Palmer and Graycommented on drafts of the review.
D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R T
26Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Internal sources
• Visibility, UK.Salary SP
• Southampton University, UK.Salary CB
• Glasgow Caledonian University, UK.Salary DS, TH, LG
• NHS Greater Glasgow & Clyde, UK.Salary FN
External sources
• Thomas Pocklington Trust, UK.Partial financial support (CB) for review
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
Our search strategy changed slightly - see ’Electronic searches’ section earlier.
N O T E S
The protocol and review has had slight amendment to the a priori subgroup analyses. The review authors planned to consider thefollowing hypotheses for subgroup analysis if sufficient data were available:
1. Behavioural interventions delivered in tandem with environmental interventions are more effective than either behavioural orenvironmental interventions delivered on their own.
2. Interventions are equally effective on differing severities of visual impairment.
3. Interventions are equally effective with fallers as they are with the general older population (inclusion criteria at point ofrecruitment into the study).
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Independent Living; ∗Motor Activity; Visually Impaired Persons [∗rehabilitation]
MeSH check words
Aged; Humans
27Environmental and behavioural interventions for reducing physical activity limitation in community-dwelling visually impaired older
people (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.




















