
Emergency colectomy for cytomegalovirus ileocolitis in patients with the acquired immune deficiency...
7
Diseases of the COLON & RECTUM Vol. 31 October 1988 No. 10 Original Contributions Emergency Colectomy for Cytomegalovirus Ileocolitis in Patients with the Acquired Immune Deficiency Syndrome STEVEN D. WEXNER, M.D., WILLIAM B. SMITHY, M.D., CARLOS TRILLO, M.D., B. SMITH HOPKINS, M.D., THOMAS H. DAILEY, M.D. Wexner SD, Smithy WB, Trillo C, Hopkins BS, Dailey TH. Emer- gency colectomy for cytomegalovirus ileocolitis in patients with the acquired immune deficiency syndrome. Dis Colon Rectum 1988;31: 755-761. The charts of all patients with the acquired immune deficiency syn- drome (AIDS) who underwent emergency intra-abdominal surgery between January 1981 and July 1987 were reviewed. Eleven AIDS patients underwent 13 emergency laparotomies. Seven of these patients (64 percent) had cytomegalovirus (CMV) ileocolitis as the pathologic process requiring emergent surgical intervention. Four patients had hemorrhagic CMV proctocolitis and three had perforations of CMV ulcers of the ileum or rectosigmoid. The operations performed included three subtotal colectomies, two segmental resections, and two diverting stomas. The postoperative mortality rate in the CMV group was 28 percent at one day, 71 percent at one month, and 86 percent at six months. Furthermore, CMV ileocolonic pathology was directly respon- sible for 70 percent of the deaths in AIDS patients who underwent emergent exploratory laparotomy. [Key words: Acquired immune defi- ciency syndrome (AIDS); Cytomegalovirus (CMV); Ulcer; Colitis; Enteritis; Colectomy; Gastrointestinal bleeding] AS OF JANUARY 1988, over 53,000 cases of acquired immune deficiency syndrome (AIDS) had been reported in the United States.t Approximately 13,000 of these were in New York City. 2 In Manhattan, AIDS was the single largest cause of loss of productivity in men aged 25 to 44 Read at the meeting of the American Society of Colon and Rectal Surgeons, Anaheim, California, June 12 to 17, 1988. This paper received the Chicago Society of Colon and Rectal Surgeons Award. Address reprint requests to Dr. Wexner: Department of Colorectal Surgery, The Cleveland Clinic Florida, 3000West Cypress Creek Road, Fort Lauderdale, Florida 33309. From the Division of Colon and Rectal Surger% The Roosevelt Hospital, New York, New York years 3 and was the leading cause of death of men in that same age group. 4 Although New York City and San Francisco account for the majority of cases of AIDS, 5 the disease is frequently reported in all 50 of the United States, Puerto Rico, and nine territories. 6 A continued rising incidence is expected; over 250,000 cases are pro- jected by 1991. 7 Every surgeon will probably see AIDS patients, and therefore must understand the intra-abdominal manifes- tations of the disease. Furthermore, although consulta- tion in the elective setting may allow time for a search through the literature and an update on one's knowledge of AIDS, patients in extremis do not afford the surgeon the luxury of time. Consequently, all surgeons must be especially familiar with those AIDS-related diseases that are likely to present acutely. For example, intra-abdom- inal lymphoma and tuberculosis are seen in AIDS patients, but rarely require emergency surgery. 8 Sim- ilarly, splenectomy for control of hemorrhage secondary to idiopathic thrombocytopenia is required, but not usu- ally on an emergent basis. ~ 10 In addition, AIDS patients are subject to the same intra-abdominal pathologic pro- cesses as the control population: appendicitis, cholecysti- tis, and a variety of anorectal pathologies, n, ~ Two recent studies showed that 94 percent to 100 per- cent of healthy homosexual men were seropositive for 755
-
Upload
clevelandclinic -
Category
Documents
-
view
1 -
download
0
Transcript of Emergency colectomy for cytomegalovirus ileocolitis in patients with the acquired immune deficiency...
Diseases of the
C O L O N & R E C T U M
Vol. 31 October 1988 No. 10
Original Contributions
Emergency Colectomy for Cytomegalovirus Ileocolitis in Patients with the Acquired Immune Deficiency Syndrome
STEVEN D. WEXNER, M.D., WILLIAM B. SMITHY, M.D., CARLOS TRILLO, M.D., B. SMITH HOPKINS, M.D., THOMAS H. DAILEY, M.D.
Wexner SD, Smithy WB, Trillo C, Hopkins BS, Dailey TH. Emer- gency colectomy for cytomegalovirus ileocolitis in patients with the acquired immune deficiency syndrome. Dis Colon Rectum 1988;31: 755-761.
The charts of all patients with the acquired immune deficiency syn- drome (AIDS) who underwent emergency intra-abdominal surgery between January 1981 and July 1987 were reviewed. Eleven AIDS patients underwent 13 emergency laparotomies. Seven of these patients (64 percent) had cytomegalovirus (CMV) ileocolitis as the pathologic process requiring emergent surgical intervention. Four patients had hemorrhagic CMV proctocolitis and three had perforations of CMV ulcers of the ileum or rectosigmoid. The operations performed included three subtotal colectomies, two segmental resections, and two diverting stomas. The postoperative mortality rate in the CMV group was 28 percent at one day, 71 percent at one month, and 86 percent at six months. Furthermore, CMV ileocolonic pathology was directly respon- sible for 70 percent of the deaths in AIDS patients who underwent emergent exploratory laparotomy. [Key words: Acquired immune defi- ciency syndrome (AIDS); Cytomegalovirus (CMV); Ulcer; Colitis; Enteritis; Colectomy; Gastrointestinal bleeding]
AS OF JANUARY 1988, over 53,000 cases of acquired i m m u n e deficiency syndrome (AIDS) had been reported in the Uni ted States.t Approximate ly 13,000 of these were in New York City. 2 In Manhat tan , AIDS was the single largest cause of loss of product ivi ty in men aged 25 to 44
Read at the meeting of the American Society of Colon and Rectal Surgeons, Anaheim, California, June 12 to 17, 1988. This paper received the Chicago Society of Colon and Rectal Surgeons Award.
Address reprint requests to Dr. Wexner: Department of Colorectal Surgery, The Cleveland Clinic Florida, 3000 West Cypress Creek Road, Fort Lauderdale, Florida 33309.
From the Division of Colon and Rectal Surger% The Roosevelt Hospital,
New York, New York
years 3 and was the leading cause of death of men in that same age group. 4 A l t h o u g h New York City and San Francisco account for the major i ty of cases of AIDS, 5 the disease is frequently reported in all 50 of the Uni ted States, Puer to Rico, and nine territories. 6 A cont inued rising incidence is expected; over 250,000 cases are pro- jected by 1991. 7
Every surgeon will probably see AIDS patients, and therefore mus t unders tand the in t ra-abdominal manifes- tations of the disease. Furthermore, a l though consulta- tion in the elective setting may allow time for a search th rough the literature and an update on one 's knowledge of AIDS, patients in extremis do not afford the surgeon the luxury of time. Consequent ly , all surgeons mus t be especially familiar with those AIDS-related diseases that are likely to present acutely. For example, in t ra-abdom- inal l y m p h o m a and tuberculosis are seen in AIDS patients, but rarely require emergency surgery. 8 Sim- ilarly, sp lenectomy for control of hemorrhage secondary to id iopathic th rombocytopenia is required, but not usu- ally on an emergent basis. ~ 10 In addit ion, AIDS patients are subject to the same int ra-abdominal pa thologic pro- cesses as the control popu la t ion : appendicit is , cholecysti- tis, and a variety of anorectal pathologies, n, ~
T w o recent studies showed that 94 percent to 100 per- cent of heal thy homosexua l men were seropositive for
755
Dis. Col, g: Rect. 756 WEXNER, ET AL. October 1988
cy tomega lov i rus (CMV). x3, ~4 Moreover, 14 percent of hea l thy h o m o s e x u a l men be tween the ages of 18 and 29 years were f o u n d to be actively infected, x4 Dissemina ted CMV has been ident i f ied at au topsy in 90 percent of al l AIDS patients.~5-~7 A l t h o u g h CMV can be p a t h o l o g i c a l l y iden t i f i ed in any o rgan in the body, its presence is no t associated u n i f o r m l y wi th c l in ica l changes. ~8 T h e com- m o n sequelae of CMV i leocol i t is are severe diarrhea, we igh t loss, fever, and occas iona l me lena and hematoche- zia. 19 Massive h e m o r r h a g e a n d pe r fo ra t ion can occur anywhere w i t h i n the gas t ro in tes t ina l tract; the t e rmina l i l e u m a n d c o l o n are the m o s t f r e q u e n t l y a f fec ted a r e a s . 18-20
T h e a ims of the present s tudy were: 1) to ident i fy the man i fe s t a t ions of CMV w i t h i n the t e rmina l p o r t i o n of the gas t ro in tes t ina l tract in AIDS patients; 2) to ascertain the relat ive inc idence of CMV i leoco lon ic p a t h o l o g y necess i ta t ing emergency surgery when c o m p a r e d wi th o the r i n t r a - a b d o m i n a l processes; 3) to analyze the types of therapy used; a n d 4) to reach conclus ions abou t app ro - pr ia te therapy.
Materials and Methods
T h e charts of a l l AIDS pa t ien t s w h o unde rwen t emer- gency exp lo ra to ry l a p a r o t o m y at the Roosevel t H o s p i t a l in New York Ci ty between J a n u a r y 1981 a n d Ju ly 1987
were reviewed retrospectively. Al l pa t ien ts d iagnosed as h a v i n g AIDS fulf i l led the cri teria def ined by the Centers for Disease Cont ro l . 2~ Each pa t i en t ' s char t was reviewed for the age, sex, r isk factors for AIDS, c l in ica l presenta- t ion, hosp i t a l course, opera t ive f indings , surgery per- formed, pos topera t ive course, in terval between d iagnos is of AIDS and surgery, and p o s t m o r t e m findings. In al l cases, t e lephone fo l low-up , office charts, and ou tpa t i en t c l inic records were used to ensure accuracy of the data.
Results
Eleven AIDS pa t ien ts unde rwen t 13 explora tory lapa- ro tomies on an emergency basis. Al l pa t ien ts were male homosexua l s ; six carr ied a d iagnos i s of AIDS before surgery and five were reclassif ied as hav ing AIDS in the pe r iopera t ive p e r i o d based on conf i rma to ry evidence. T h e mean age was 41 years, (range, 25 to 57).
Ope ra t i ons pe r fo rmed inc luded a p p e n d e c t o m y for per- forated append ic i t i s and subsequent r epa i r of the w o u n d dehiscence; l a p a r o t o m y for spon taneous bacterial per i to- nitis; subtota l gas t rec tomy and Bi l l ro th II anas tomos is for b l eed ing gastr ic l y m p h o m a ; and sp lenec tomy for acute i n t r a - a b d o m i n a l h e m o r r h a g e secondary to tubercu- lous in f i l t r a t ion of the spleen. T h e o the r cases al l re la ted to CMV ulcera t ions of the i leum, colon, and rectum, a n d are shown in T a b l e 1.
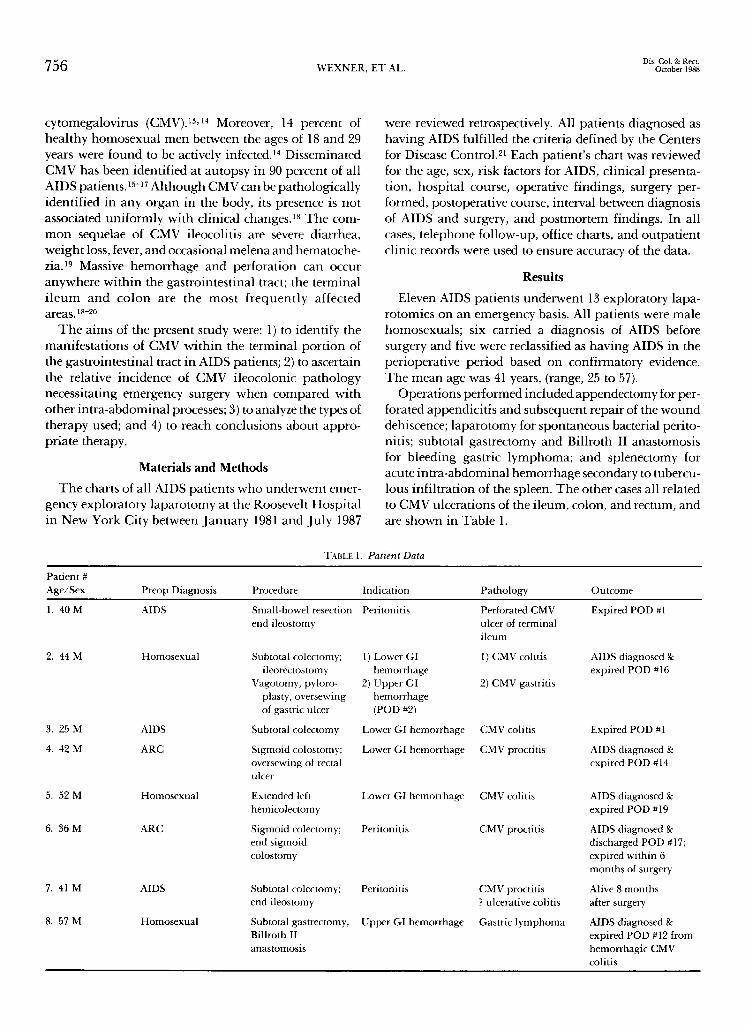
TABLE 1. Patient Data
Patient # Age/Sex Preop Diagnosis Procedure Indication Pathology Outcome
1. 40 M AIDS Small-bowel resection Peritonitis Perforated CMV Expired POD #1 end ileostomy ulcer of terminal
ileum
2. 44 M Homosexual Subtotal colectomy; 1) Lower GI 1) CMV colitis AIDS diagnosed gc ileorectostomy hemorrhage expired POD #16
Vagotomy, pyloro- 2) Upper GI 2) CMV gastritis plasty, oversewing hemorrhage of gastric ulcer (POD #2)
3. 25 M AIDS Subtotal colectomy Lower GI hemorrhage CMV colitis Expired POD #1
4. 42 M ARC Sigmoid colostomy; Lower GI hemorrhage CMV proctitis AIDS diagnosed ge oversewing of rectal expired POD #14 ulcer
5. 52 M Homosexual Extended left Lower GI hemorrhage CMV colitis AIDS diagnosed & hemicolectomy expired POD #19
6. 36 M ARC Sigmoid colectomy; Peritonitis CMV proctitis AIDS diagnosed gc end sigmoid discharged POD #17; colostomy expired within 6
months of surgery
Peritonitis CMV proctitis Alive 8 months ? ulcerative colitis after surgery
Upper GI hemorrhage Gastric lymphoma AIDS diagnosed g: expired POD #12 from hemorrhagic CMV colitis
7. 41 M AIDS Subtotal colectomy; end ileostomy
8. 57 M Homosexual Subtotal gastrectomy, Billroth II anastomosis
Volume 31 Number 10 EMERGENCY COLECTOMY IN AIDS PATIENTS 757
Hemorrhage and perforation of the CMV ulcerations occurred with similar frequencies. Four patients had hemorrhagic CMV colitis and three had perforations of the i leum or rectosigmoid. Cytomegalovirus is often a muhicentric disease, and expeditious curative resection of one involved area may not prevent subsequent complica- tions from other loci of CMV. Three cases will be outlined to illustrate this dilemma.
Patient 8, who had not yet been diagnosed as having AIDS, had a gastric hemorrhage secondary to a 2-cm l ymphoma of the lesser curvature. He underwent an emergency subtotal gastrectomy and Billroth II anasto- mosis. The initial postoperative course was complicated by cardiac arrest, pu lmonary edema, Pneumocystis cari- nii pneumonia , idiopathic thrombocytopenia, and sep- sis, all characteristic of AIDS. On the 12th postoperative day, he developed a massive lower gastrointestinal bleed. Multiple attempts at localization of the bleeding were unsuccessful. The patient suddenly went into shock and died. Autopsy revealed diffuse CMV of the heart, adrenal glands, spleen, pancreas, prostate, lymph nodes, and entire gastrointestinal tract. The cause of death was exsanguination from muhifocal ileocolonic CMV ulcers.
Patient 5, also not classified as having AIDS before
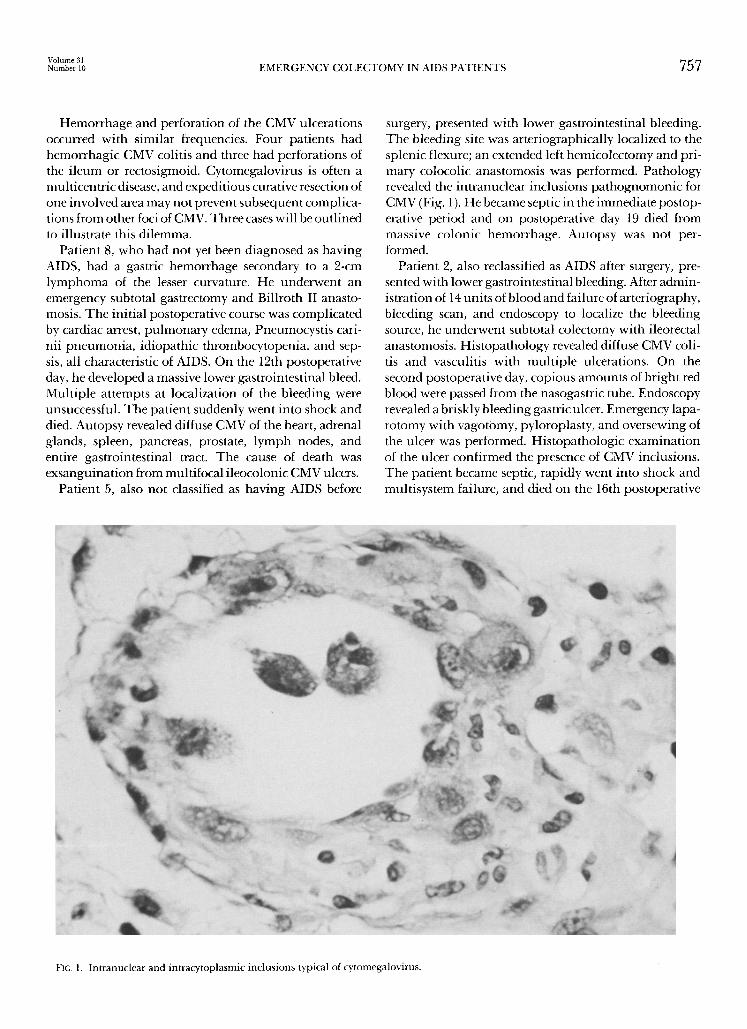
surgery, presented with lower gastrointestinal bleeding. The bleeding site was arteriographically localized to the splenic flexure; an extended left hemicolectomy and pri- mary colocolic anastomosis was performed. Pathology revealed the intranuclear inclusions pa thognomonic for CMV (Fig. 1). He became septic in the immediate postop- erative period and on postoperative day 19 died from massive colonic hemorrhage. Autopsy was not per- formed.
Patient 2, also reclassified as AIDS after surgery, pre- sented with lower gastrointestinal bleeding. After admin- istration of 14 units of blood and failure of arteriography, bleeding scan, and endoscopy to localize the bleeding source, he underwent subtotal colectomy with ileorectal anastomosis. His topathology revealed diffuse CMV coli- tis and vasculitis with mult iple ulcerations. On the second postoperative day, copious amounts of bright red blood were passed from the nasogastric tube. Endoscopy revealed a briskly bleeding gastric ulcer. Emergency lapa- rotomy with vagotomy, pyloroplasty, and oversewing of the ulcer was performed. Histopathologic examinat ion of the ulcer confirmed the presence of CMV inclusions. The patient became septic, rapidly went into shock and multisystem failure, and died on the 16th postoperative
FIG. 1. Intranuclear and intracytoplasmic inclusions typical of cytomegalovirus.

Dis. Col. & Rect. 758 W E X N E R , E T A L . October 1988
day. Autopsy revealed a clinically unsuspected dehisced ileorectal anastomosis with acute suppurative peritonitis and CMV ulcerations throughout the gastrointestinal tract.
Patients who were operated on for perforations of ileo- colonic CMV ulcerations did somewhat better than the hemorrhagic group. Patient 1, known preoperatively to have AIDS, presented in shock with diffuse peritonitis. Exploratory laparotomy revealed a perforated distal i leum and diffuse abdominal soilage. A localized resec- tion with an end ileostomy and mucous fistula of the right colon was performed. Histopathologic examina- tion revealed a perforated CMV ileal ulcer. The patient never recovered from the initial insult, and died within 24 hours of surgery. At the time of his death, bright red blood was emanat ing from both the ileostomy and the mucous fistula. The immediate cause of death was massive hemorrhage from mult iple CMV ulcerations of the small bowel and colon.
Patient 7 was known to have both AIDS and CMV colitis. He presented with five synchronous sigmoid per- forations and underwent subtotal colectomy with over- sewing of the distal rectal s tump and creation of an end ileostomy. He did well for eight months after surgery. Pathologic study of the resected sigmoid colon suggested the possibility of ulcerative colitis as the immediate cause of perforation.
The postoperative mortality rate in the CMV group was 28 percent at one day, 71 percent at one month, and 86 percent at six months. In addition, one of the four patients who underwent emergent major abdominal surgery for a non-CMV cause died from CMV colitis (patient 8). Initially he underwent subtotal gastrectomy and Billroth II anastomosis for a hemorrhagic, ulcerated, gastric, lymphocytic lymphoma. He died on the 14th postoperative day from massive lower gastrointestinal bleeding. Autopsy identified hemorrhage from diffuse colonic CMV ulcerations as the immediate cause of death. Thus, CMV ileocolonic pathology was directly responsi- ble for 70 percent of all deaths in AIDS patients who underwent emergency major abdominal surgery. Mor- bidity was also formidable; every patient except one (patient 7) had at least one additional major postoperative complication. These included dehiscence of wounds and anastomoses, muhisystem failure, intractable sepsis, pneu- monia, and hemorrhage.
Discussion
Disseminated CMV has been found at autopsy in 90 percent of AIDS patients. 15-17 Organs involved include the lungs, central nervous system, eyes, skin, pancreas, adrenal glands, spleen, thyroid, and heart. Cytomegalovi- rus is known to cause ulceration and bleeding in the esophagus, stomach, small bowel, and colon.16,19, 20, 22, 23
In addition, perforations of CMV ulcers of the ileum and colon have been reported previously.l~ 18, 24, 25 Acalculous CMV cholecystitis and CMV papillit is causing papil lary stenosis have been reported previously.12,26, 27 In addition to CMV cholecystitis, CMV hepatitis has also been reported. 28 Even cytomegalovirus ulcers of a Kock pouch in a homosexual male have been described.29 Thus, it has been well documented that CMV can infect any port ion of the gastrointestinal tract, and can express itself by inflammation, hemorrhage, ulceration, or perforation.
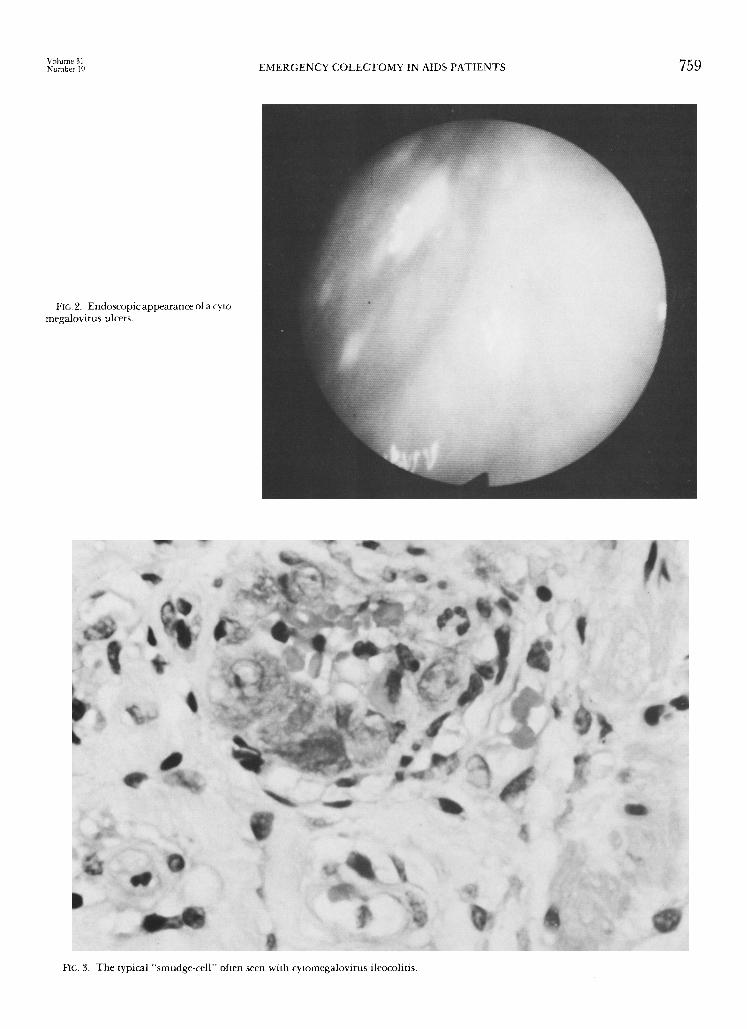
Endoscopic suspicion of CMV colitis should be con- firmed by biopsy. Biopsy of the ulcer is highly accurate in the diagnosis of CMV. Whereas viral culture of rectal swabs is only 30 percent sensitive, histopathologic exam- ination of biopsy specimens is 92 percent sensitive in the diagnosis of CMV colitis, s~ Grossly, the lesions range from erythematous patches, with or without shallow punctate ulcers, to mult iple wide, deep, coalescing ulcers; the latter often bleed easily. A confluent area of inf lamma- tion mimicking ulcerative colitis has been reported, s~ The ulcer edges are generally smooth and a whitish ulcer membrane may be present, as shown in Fig. 2.
The histopathologic diagnosis is based on the finding of large, basophilic, intranuclear cytomegalic viral inclu- sions and granular cytoplasmic inclusions (Fig. 1). These entities are seen in endothelial cells, often in stromal histiocytes and macrophages in the setting of acute and chronic inf lammat ion and ulceration. The basophilic "smudge-cell" is considered highly suggestive of CMV infection (Fig. 3). Ideally, the findings of the intranuclear viral inclusions should be confirmed by viral culture of CMV.
Although CMV can be reliably diagnosed by these findings, its precise role in the cause of gastrointestinal ulceration is unknown. It is unclear whether CMV as the pr imary pathogen causes the ulcer by an ischemic vascu- litis, or whether it is simply an inhabitant of an already existing ulcer. 15, 26, 27 This is especially difficult to deter- mine because over 70 percent of male homosexual AIDS patients with CMV infection of the gastrointestinal tract have coexistent alimentary pathogens. 31 The more com- monly identified organisms include shigella, Salmonella, Candida, Mycobacteriurn avium and intracellularis and Cryptosporidium.2~ 31 Either the mucosal damage in- duced by these concurrent colitides facilitates enhanced viral replication, or CMV infection leads to greater sus- ceptibility to other gastrointestinal pathogens. Each may be a contributory mechanism.
Cytomegalovirus involvement of the bowel may cause bleeding by inducing a vasculitis in the involved segment. The vasculitis then results in ischemia, infarction, or both; the colon and terminal i leum appear to be the areas most frequently involved.25,3~ A similar mechanism prob- ably accounts for the bleeding associated with CMV infec-
Volume 3 l Number I0 E M E R G E N C Y C O L E C T O M Y IN AIDS P A T I E N T S 759
FIG. 2. Endoscopic appearance of a cyto- megalovirus ulcers.
FIG. 3, T h e typical "smudge-cel l" often seen wi th cytomegalovirus ileocolitis.

Dis. Col. & Rect. 760 W E X N E R , E T A L . October 1988
tion of the esophagus and stomach. 23 Hemorrhage from esophagogastric or ileocolic CMV erosions may result from either focal or diffuse areas of involvement. Both focal and diffuse types of ulceration may bleed either acutely or chronically. The similarity of the histopatho- logic picture of CMV colitis to that of mesenteric ische- mia has been noted. 2a The viral endothelial vasculitis may be limited to a very small unifocal area, and unless multi- ple sections are examined , the d iagnosis may be missed.ZZ, 34
The most common misdiagnoses are ulcerative colitis and granulomatous colitis.19, s0 Not only do the clinical and histopathologic findings of CMV colitis mimic those of other colitides, but so do bar ium enema findings. These findings include diffuse mucosal ulceration, aph- thous ulceration, granularity, skip areas, " thumbprint - ing," and linear ulceration. 19 Thus it is highly probable that patient 7 in this report sustained perforations of preoperatively proven CMV ulcers.
Patients with AIDS may require surgery for many rea- sons. T o better understand this challenging problem, it is important to divide the surgery into categories of major and minor, elective, urgent, and emergent. Several papers describe the reasons for and results of elective surgery in AIDS patients. Robinson and colleagues studied 21 AIDS patients who underwent 31 surgical procedures.l~ Twenty- four of these operations were performed on an elective basis, and 16 of these were minor procedures. Seven emer- gency operations were performed, but only two of these were laparotomies. Both of the emergency laparotomies were for perforations of CMV colitis: one at the splenic flexure and one in the transverse colon. The 30-day opera- tive mortality following emergency surgery was 57 per- cent, and both CMV colitis patients died within five months of surgery.
Nugent and O'Connel l reviewed 31 operations per- formed in 27 patients with either AIDS or AIDS-related complex (ARC). 35 Only five major abdominal procedures were in these data, and only three of these were performed on an emergent basis. T w o of the three emergent laparot- omies were for CMV colitis. One patient had a total colectomy performed for toxic megacolon due to CMV colitis, and the other had an unspecified type of colon resection with colostomy creation for a perforated CMV ulcer in the transverse colon. Both of these patients died within four months of surgery and the mortality for the entire series was 51 percent. The authors did not state the length of follow-up.
These mortali ty rates are not surprising when one con- siders that the six-month mortality rate following minor anorectal surgery in AIDS patients is 79 percent, n Fur- thermore, in the absence of complications such as hemor- rhage or perforation, the mean survival for AIDS patients with CMV infection of the distal gastrointestinal tract has
been reported as 6.7 months. 31 It is important to recognize the patient at risk for
AIDS. 21 A previous study by the authors ' group found that 15 percent of AIDS patients initially had an anorectal surgical problem before the diagnosis of AIDS. n Only three of the eight patients in this study were diagnosed as having AIDS before the time of emergent laparotomy; two additional patients were classified preoperatively as "ARC." These data agree with those presented by Hin- nant and colleagues, who found that CMV infection of the alimentary tract was the first manifestation of AIDS in 11 of the 19 patients in their series. ~ Furthermore, between 94 and 100 percent of homosexual men without overt immune deficiency display serologic positivity for CMV.13,14 This latter finding, however, may occur with- out diagnostic evidence of intranuclear cytomegalic inclu- sion bodies. It is possible that a cofactor, such as the h u m a n immune deficiency virus (HIV), is necessary for active intraepithelial viral replication of the CMV. Nel- son et al recently isolated HIV from bowel epithelial cells in AIDS patients, z6 It is hoped that further research will elucidate this dilemma.
Conclusions
As the incidence and prevalence of AIDS increase, the colon and rectal surgeon will be called on with increasing frequency to evaluate and treat AIDS patients. It is, there- fore, imperative that every surgeon recognize the patient at risk for AIDS and be able to determine which patients may benefit from operative intervention. All too often the diagnosis is unsuspected preoperatively and becomes obvious after surgery, when the multiple manifestations of AIDS rapidly develop.
Cytomegalovirus ileocolitis was responsible for 64 per- cent of emergency laparotomies in this series. This fre- quency is similar to the 100 and 67 percent frequencies reported by others. 1~ Overall, CMV ileocolitis was directly responsible for the deaths of 70 percent of all AIDS patients who underwent emergent laparotomy at the Roosevelt Hospital. The postoperative mortality rate in this series was 28 percent at one day, 71 percent at one month, and 86 percent at six months.
For treatment purposes, it is helpful to divide CMV ileocolonic ulcers into those that have bled and those that have perforated. The first step in both cases is to have a frank discussion with the patient, the family, and with all of the other physicians involved in the patient 's care. If the decision to proceed with aggressive intervention is made, then laparotomy is required for perforations. Because of the multifocal nature of CMV, colonic perfo- rations should be treated by total abdominal colectomy and end ileostomy with closure of the rectal stump. Distal small-bowel perforations should probably be treated by segmental resection with an end-stoma and mucous fis-
Volume 31 Number 10 EMERGENCY COLECTOMY IN AIDS PATIENTS 761
tu la . A l t h o u g h it is h e l p f u l to loca l ize the site of ga s t ro in -
tes t ina l b leed ing , i t s h o u l d n o t c h a n g e the t he rapy
e m p l o y e d . If the b l e e d i n g c a n n o t be c o n t r o l l e d by conser -
va t ive m e a n s such as t r ans fus ion , colonoscopic f u l g u r a -
t ion , o r a n g i o g r a p h i c e m b o l i z a t i o n , to ta l a b d o m i n a l
c o l e c t o m y a n d e n d i l e o s t o m y s h o u l d be pe r fo rmed . If
s m a l l - b o w e l b l e e d i n g is ev ident , the si te m a y be loca l ized
by i n t r a o p e r a t i v e e n t e r o e n d o s c o p y ; s e g m e n t a l resec t ion
w i t h o u t a n a s t o m o s i s s h o u l d be done .
F o u r i m p o r t a n t c o n c l u s i o n s are: 1) r e c o g n i z e the cri te-
r ia of A I D S a n d the g r o u p of p a t i e n t s at risk, as C M V
i l eoco l i t i s m a y be the i n i t i a l m a n i f e s t a t i o n of A I D S ; 2)
c y t o m e g a l o v i r u s is a m u l t i f o c a l disease; its exc i s ion f r o m
o n e p o r t i o n of the g a s t r o i n t e s t i n a l t ract m a y be f o l l o w e d
by a C M V c o m p l i c a t i o n e l sewhere ; 3) m o r b i d i t y a n d m o r -
ta l i ty assoc ia ted w i t h m a j o r e m e r g e n t i l e o c o l o n i c resec-
t i on for C M V in A I D S pa t i en t s are h i g h a n d the life
e x p e c t a n c y in these p a t i e n t s is shor t ; a n d 4) a n a s t o m o t i c
c o m p l i c a t i o n s are p o o r l y to le ra ted in A I D S pa t ien ts ,
t he re fo re , a n a s t o m o s e s s h o u l d be a v o i d e d w h e n e v e r
poss ib le .
References
1. Centers for Disease Control. AIDS weekly surveillance report. Atlanta, February 15, 1988.
2. New York City Department of Health. AIDS Surveillance Unit. AIDS update. New York, January 15, 1988.
3. Kristal AR. The impact of the acquired immune deficiency syn- drome on patterns of premature death in New York City. JAMA 1986; 255:2306-10.
4. New York City Department of Health. Bureau of Vital Statistics. 1986 Annual Report. New York, July 31, 1987.
5. Centers for Disease Control. Update: AIDS in the U.S. MMWR 1986;35:17-21.
6. Centers for Disease Control. AIDS surveillance data. Atlanta, Feb- ruary 2, 1987.
7. Coolfont Report: a Public Health Service plan for prevention and control of AIDS and the AIDS virus. Public Health Service Report 1986;101:341-8.
8. DeVita VT, Hellman S, Rosenberg SA, eds. AIDS: etiology, diag- nosis, treatment, and prevention. Philadelphia: JB Lippincott, 1985.
9. Walsh C, Krigel R, Lennette E, Karpatkin S. Thrombocytopenia in homosexual patients. Ann Intern Med 1985; 103:542-5.
10. Robinson G, Wilson SE, Williams RA. Surgery in patients with acquired immunodeficiency syndrome. Arch Surg 1987;122: 1117-20.
11. Wexner SD, Smithy WB, Milsom JW, Dailey TH. The surgical management of anorectal diseases in AIDS and pre-AIDS patients. Dis Colon Rectum 1986;29:719-23.
12. Wexner SD. Major abdominal surgery in AIDS patients. In: Gold- berg SW, ed. Principles of Colon and Rectal Surgery. Minneapo- lis: University of Minnesota Press, 1988:40-54.
13. Lange M, Klein EB, Kornfield H, Cooper LZ, Grieco MH. Cytomegalovirus isolation from healthy homosexual men. JAMA 1984;252:1908-10.
14. Drew WL, Mintz L, Miner RC, Sands M, Ketterer B. Prevalence of cytomegalovirus infection in homosexual men. J Infect Dis 1981;143:188-92.
15. Quinn TC. Gastrointestinal manifestations of AIDS. Pract Gas- troenterol 1985;9:23-4.
16. Knapp AB, Horst DA, Eliopoulos G, et al. Widespread cytomega- lovirus gastroenterocolitis in a patient with acquired immu- nodeficiency syndrome. Gastroenterology 1983;85:1399-402.
17. Gertler SL, Pressman J, Price P, Brozinsky S, Miyai K. Gastrointes- tinal cytomegalovirus infection in a homosexual man with severe acquired immunodeficiency syndrome. Gastroenterology 1983 ;85:1403-6.
18. Frank D, Raicht RF. Intestinal perforation associated with cyto- megalovirus infection in patients with acquired immune defi- ciency syndrome. Am J Gastroenterol 1984;79:201-5.
19. Frager DH, Frager JD, Wolf EL, et al. Cytomegalovirus colitis in acquired immune deficiency syndrome: radiologic spectrum. Gastrointest Radiol 1986; 11:241-6.
20. Wexner SD. Sexually transmitted diseases of the colon, rectum, and anus. In: Goldberg SM, Gordon PH, Nivatvongs S, eds. Princi- ples and practices of surgery of the colon, rectum, and anus (in press).
21. Leads from the MMWR. Revision of the CDC surveillance case definition for acquired immunodeficiency syndrome. JAMA 1987;258:1143 -54.
22. Houin HP, Gruenberg JC, Fisher E J, Metzger E. Multiple small bowel perforations secondary to cytomegalovirus in a patient with acquired immunodeficiency syndrome. Henry Ford Hosp Med J 1987;35:17-9.
23. Balthazar E J, Meigbow AJ, Hulnick DH. Cytomegalovirus eso- phagitis and gastritis in AIDS. AJR 1985;144:1201-4.
24. Kram HB, Hino ST, Cohen RE, DeSantis SA, Schoemaker WC. Spontaneous colonic perforation secondary to cytomegalovirus infection in a patient with acquired immune deficiency sydrome. Crit Care Med 1984;12:469-71.
25. Foucar E, Mukai K, Foucar K, et al. Colon ulceration in lethal cytomegalovirus infection. Am J Clin Pathol 1981;76:788-801.
26. Kevin H, Jonas RB, Chowdhury O, Robbins S. Acalculous chole- cystitis and cytomegalovirus infection in the acquired immu- nodeficiency syndrome. Ann Intern Med 1986;104:53-4.
27. Schneiderman D J, Cello JP, Laing FC. Papillary stenosis and sclerosing cholangitis in the acquired immunodeficiency syn- drome. Ann Intern Med 1987;106:546-9.
28. Kahn DG, Garfinkle JM, Klonoff DC, Pembrook L J, Morrow DJ. Cryptosporidial and cytomegaloviral hepatitis and cholecystitis. Arch Pathol Lab Med 1987; 111:879-81.
29. Blackman E, Vimadel S, Nash G. Significance of gastrointestinal cytomegalovirus in homosexual males. Am J Gastroenterol 1984; 79:935-40.
30. Culpepper-Morgan JA, Kotler DP, Scholes JV, Tierney AR. Eval- uation of diagnostic criteria for mucosal cytomegalic inclusion disease in the acquired immune deficiency syndrome. Am J Gastroenterol 1987;82:1264-70.
31. Hinnant KL, Rotterdam HZ, Bell ET, Tapper ML. Cytomegalovi- rus infection of the alimentary tract: a clinicopathological corre- lation. Am J Gastroentereol 1986;81:944-50.
32. Meiselman MS, Cello JP, Margaretten W. Cytomegalovirus colitis. Report of the clinical, endoscopic and pathologic findings in two patients with acquired immune deficiency syndrome. Gas- troenterology 1985;88:171-5.
33. Underwood JCE, Corbett CL. Persistent diarrhea and hypoalbu- minemia associated with cytomegalovirus enteritis. Br Med J 1978;1:1029-30.
34. Campbell DS, Piercey JR, Shnitka JK, et al. Cytomegalovirus- associated gastric ulcer. Gastroenterology 1977;72:533-5.
35. Nugent P, O'Connell TX. The surgeon's role in treating acquired immunodeficiency syndrome. Arch Surg 1986; 121:1117-20.
36. Nelson JA, Wiley CA, Reynolds-Kohler C, Reese CE, Margaretten W, Levy JA. Human immunodeficiency virus detected in bowel epithelium from patients with gastrointestinal symptoms. Lan- cet 1988; 1:259-62.




















