Emergency Administration of Abciximab for Treatment of Patients With Acute Ischemic Stroke: Results...
14
Emergency Administration of Abciximab for Treatment of Patients With Acute Ischemic Stroke: Results of an International Phase III Trial Abciximab in Emergency Treatment of Stroke Trial (AbESTT-II) Harold P. Adams, Jr, MD; Mark B. Effron, MD; James Torner, PhD; Antoni Da ´valos, MD, PhD; Judith Frayne, MD; Philip Teal, MD; Jacques Leclerc, MD; Barry Oemar, MD; Lakshmi Padgett, PhD; Elliot S. Barnathan, MD; Werner Hacke, MD; for the AbESTT-II Investigators Background and Purpose—A previous randomized, placebo-controlled, double-blind study suggested that abciximab may be safe and effective in treatment of acute ischemic stroke. The current phase 3 study was planned to test the relative efficacy and safety of abciximab in patients with acute ischemic stroke with planned treatment within 5 hours since symptoms onset. Methods—An international, randomized, placebo-controlled, double-blind phase 3 trial tested intravenous administration of abciximab in 2 study cohorts using stratification variables of time since onset and stroke severity. The planned enrollment was 1800 patients. The primary cohort enrolled those patients who could be treated within 5 hours of onset of stroke. A companion cohort enrolled patients that were treated 5 to 6 hours after stroke as well as a smaller cohort of patients who could be treated within 3 hours of stroke present on awakening. The primary efficacy measure was the dichotomous modified Rankin Scale score at 3 months as adjusted to the baseline severity of stroke among subjects in the primary cohort. The primary safety outcome was the rate of symptomatic or fatal intracranial hemorrhage that occurred within 5 days of stroke. Results—The trial was terminated prematurely after 808 patients in all cohorts were enrolled by recommendation of an independent safety and efficacy monitoring board due to an unfavorable benefit-risk profile. At 3 months, approximately 33% of patients assigned placebo (72/218) and 32% of patients assigned abciximab (71/221; P0.944) in the primary cohort were judged to have a favorable response to treatment. The distributions of outcomes on the modified Rankin Scale were similar between the treated and control groups. Within 5 days of enrollment, 5.5% of abciximab-treated and 0.5% of placebo-treated patients in the primary cohort had symptomatic or fatal intracranial hemorrhage (P0.002). The trial also did not demonstrate an improvement in outcomes with abciximab among patients in the companion and wake-up cohorts. Although the number of patients was small, an increased rate of hemorrhage was noted within 5 days among patients in the wake-up population who received abciximab (13.6% versus 5% for placebo). Conclusions—This trial did not demonstrate either safety or efficacy of intravenous administration of abciximab for the treatment of patients with acute ischemic stroke regardless of end point or population studied. There was an increased rate of symptomatic or fatal intracranial hemorrhage in the primary and wake-up cohorts. (Stroke. 2008;39:87-99.) Key Words: abciximab acute stroke treatment hemorrhagic transformation ischemic stroke I nhibition of platelet aggregation is a major component of treatment strategies to prevent ischemic stroke. Platelet activation is a key step in thromboembolism and may be involved in the propagation of an arterial thrombus. Changes in platelet function and interactions with inflammatory cells or endothelial cells may affect perfusion, particularly in the microcirculation. 1–4 Abciximab, a chimeric mouse/human monoclonal antibody with high affinity for the platelet Received October 26, 2006; final revision received May 24, 2007; accepted June 14, 2007. From the Department of Neurology (H.P.A.), Carver College of Medicine, University of Iowa, Iowa City, USA; Eli Lilly and Company (M.B.E., J.L.), Indianapolis, Ind, USA; Department of Epidemiology (J.T.), College of Public Health, University of Iowa, Iowa City, USA; Department of Neurosciences (A.D.), Hospital Universitari Germans, Badalona, Spain; Stroke Research Unit (J.F.), Monash University, Melbourne, Victoria, Australia; Center for Stroke Research (P.T.), University of British Columbia, Vancouver, BC, Canada; Centocor Research and Development (B.O., L.P., E.S.B.), Malvern, Pa, USA; Department of Neurology (W.H.), University of Heidelberg, Heidelberg, Germany. Presented in part at the European Stroke Conference, Brussels, Belgium, May 19, 2006. Correspondence to Harold P. Adams, Jr, MD, Department of Neurology, University of Iowa, 200 Hawkins Drive, Iowa City, IA, 52242, USA. E-mail [email protected], or Werner Hacke, MD, Department of Neurology, University of Heidelberg, Im Neuenheimer Feld 400, D-69120, Heidelberg, Germany. E-mail [email protected] © 2007 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.106.476648 87 by guest on June 29, 2016 http://stroke.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Emergency Administration of Abciximab for Treatment of Patients With Acute Ischemic Stroke: Results...

Emergency Administration of Abciximab for Treatment ofPatients With Acute Ischemic Stroke: Results of an
International Phase III TrialAbciximab in Emergency Treatment of Stroke Trial (AbESTT-II)
Harold P. Adams, Jr, MD; Mark B. Effron, MD; James Torner, PhD; Antoni Davalos, MD, PhD;Judith Frayne, MD; Philip Teal, MD; Jacques Leclerc, MD; Barry Oemar, MD; Lakshmi Padgett, PhD;
Elliot S. Barnathan, MD; Werner Hacke, MD; for the AbESTT-II Investigators
Background and Purpose—A previous randomized, placebo-controlled, double-blind study suggested that abciximab maybe safe and effective in treatment of acute ischemic stroke. The current phase 3 study was planned to test the relativeefficacy and safety of abciximab in patients with acute ischemic stroke with planned treatment within 5 hours sincesymptoms onset.
Methods—An international, randomized, placebo-controlled, double-blind phase 3 trial tested intravenous administrationof abciximab in 2 study cohorts using stratification variables of time since onset and stroke severity. The plannedenrollment was 1800 patients. The primary cohort enrolled those patients who could be treated within 5 hours of onsetof stroke. A companion cohort enrolled patients that were treated 5 to 6 hours after stroke as well as a smaller cohortof patients who could be treated within 3 hours of stroke present on awakening. The primary efficacy measure was thedichotomous modified Rankin Scale score at 3 months as adjusted to the baseline severity of stroke among subjects inthe primary cohort. The primary safety outcome was the rate of symptomatic or fatal intracranial hemorrhage thatoccurred within 5 days of stroke.
Results—The trial was terminated prematurely after 808 patients in all cohorts were enrolled by recommendation of anindependent safety and efficacy monitoring board due to an unfavorable benefit-risk profile. At 3 months, approximately33% of patients assigned placebo (72/218) and 32% of patients assigned abciximab (71/221; P�0.944) in the primarycohort were judged to have a favorable response to treatment. The distributions of outcomes on the modified RankinScale were similar between the treated and control groups. Within 5 days of enrollment, �5.5% of abciximab-treatedand 0.5% of placebo-treated patients in the primary cohort had symptomatic or fatal intracranial hemorrhage (P�0.002).The trial also did not demonstrate an improvement in outcomes with abciximab among patients in the companion andwake-up cohorts. Although the number of patients was small, an increased rate of hemorrhage was noted within 5 daysamong patients in the wake-up population who received abciximab (13.6% versus 5% for placebo).
Conclusions—This trial did not demonstrate either safety or efficacy of intravenous administration of abciximab for thetreatment of patients with acute ischemic stroke regardless of end point or population studied. There was an increasedrate of symptomatic or fatal intracranial hemorrhage in the primary and wake-up cohorts. (Stroke. 2008;39:87-99.)
Key Words: abciximab � acute stroke treatment � hemorrhagic transformation � ischemic stroke
Inhibition of platelet aggregation is a major component oftreatment strategies to prevent ischemic stroke. Platelet
activation is a key step in thromboembolism and may beinvolved in the propagation of an arterial thrombus. Changes
in platelet function and interactions with inflammatory cellsor endothelial cells may affect perfusion, particularly in themicrocirculation.1–4 Abciximab, a chimeric mouse/humanmonoclonal antibody with high affinity for the platelet
Received October 26, 2006; final revision received May 24, 2007; accepted June 14, 2007.From the Department of Neurology (H.P.A.), Carver College of Medicine, University of Iowa, Iowa City, USA; Eli Lilly and Company (M.B.E., J.L.),
Indianapolis, Ind, USA; Department of Epidemiology (J.T.), College of Public Health, University of Iowa, Iowa City, USA; Department of Neurosciences(A.D.), Hospital Universitari Germans, Badalona, Spain; Stroke Research Unit (J.F.), Monash University, Melbourne, Victoria, Australia; Center forStroke Research (P.T.), University of British Columbia, Vancouver, BC, Canada; Centocor Research and Development (B.O., L.P., E.S.B.), Malvern, Pa,USA; Department of Neurology (W.H.), University of Heidelberg, Heidelberg, Germany.
Presented in part at the European Stroke Conference, Brussels, Belgium, May 19, 2006.Correspondence to Harold P. Adams, Jr, MD, Department of Neurology, University of Iowa, 200 Hawkins Drive, Iowa City, IA, 52242, USA. E-mail
[email protected], or Werner Hacke, MD, Department of Neurology, University of Heidelberg, Im Neuenheimer Feld 400, D-69120, Heidelberg,Germany. E-mail [email protected]
© 2007 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.106.476648
87 by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

glycoprotein IIa/IIIb receptor, is indicated as an adjunct topercutaneous coronary intervention for the prevention ofcardiac ischemic complications. It also has been used as anadjunct to endovascular procedures or thrombolysis in ananimal model4 and for treatment of patients with ischemiccerebrovascular disease, including patients with acute ische-mic stroke.5–12
A dose-escalation study in 74 subjects suggested a low riskof symptomatic intracranial hemorrhage (ICH) when theagent was given up to 24 hours after onset of stroke.13 Theresults of the study suggested that abciximab given as a bolusdose (0.25 mg/kg) followed by a 12-hour infusion at a rate of0.125 �g/kg per minute was reasonably safe. In order toobtain additional information about safety and potentialefficacy, a larger randomized trial was performed.14 In thisstudy of 400 subjects treated with 6 hours of onset of stroke,symptomatic hemorrhages within 5 days were found in 7 of195 patients (3.6%) given abciximab and 2 of 199 patients(1.0%) in the control group. Treatment with abciximab wasassociated with a shift of favorable outcomes at 3 months asmeasured by the modified Rankin Scale (mRS). The trend ofpotential efficacy was most prominent among subjects treatedwithin 5 hours of onset of stroke.
In order to confirm the efficacy and safety of abciximab inthe early treatment of patients with acute ischemic stroke, theAbciximab in Emergency Stroke Treatment Trial–II(AbESTT-II) was performed. The primary objective was todetermine whether early administration (within 5 hours sincesymptom onset) of abciximab would be associated with asignificant increase in favorable outcomes at 3 months usingthe dichotomous scores obtained on mRS as influenced by thebaseline severity of the stroke.15 The secondary objective wasto compare the proportion of subjects with neurologicalrecovery at 3 months and all-cause mortality at 3 months inthe primary cohort. Another objective was to assess the safetyand potential efficacy in a group of subjects treated between5 and 6 hours after symptom onset. In addition, the studyenrolled a cohort of patients whose strokes were first detectedon awakening but who could be treated within the next 3hours to address the potential use of emergency therapy torestore perfusion. This aim was to obtain preliminary infor-mation about the potential efficacy of early treatment of thisgroup of patients, and it was stimulated by reports that manypatients with stroke present on awakening might respond in amanner similar to those patients who are treated within 3hours of stroke that occur during waking hours.16,17
Methods
Trial OrganizationAbESTT-II was an international randomized, double-blind, placebo-controlled phase 3 trial that tested the efficacy and safety ofintravenously administered abciximab given to patients with acuteischemic stroke. The trial was funded through research grants fromEli Lilly & Co and Centocor R&D Inc. Representatives of thesponsors participated in the design and conduct of the trial, includingas ex-officio members of the Executive Committee. An ExecutiveCommittee with coprincipal investigators (W.H. and H.P.A.) super-vised the trial (see Appendix for membership). Clinical coordinatingcenters were located in Heidelberg, Germany, and Iowa City, Iowa.
The members of the Executive Committee and the representatives ofthe sponsors were unaware of treatment assignment.
The participating sites, with the number of enrolled patients andprincipal investigators of the research teams, are listed in theAppendix. Assignment of treatments was performed via an interac-tive voice response system. Brain-imaging studies were collected onpatients and sent to a central CT core laboratory, and the studies wereinterpreted by independent neuroradiologists at the University ofIowa. A physician at Centocor served as the medical monitor for thetrial. All causes of death, suspected ICH, stroke progression, andstroke recurrent were reviewed and adjudicated by an independentClinical Endpoint Committee in a blinded fashion (see Appendix formembership). Their end points were used in the data analyses. Allindividual safety reports and interim analyses were shared with anindependent external safety and efficacy monitoring committee(SEMC); see Appendix). In order to maintain the blinding of theentire Executive Committee, one member of the Committee and onerepresentative of each of the sponsors not otherwise involved in thestudy interacted with the external SEMC at the time the decision wasmade to halt the trial prematurely. The other members of theExecutive Committee and the sponsors were not aware of treatmentallocation or specific information about the analyses at the time thetrial stopped.
The Executive committee (Appendix) is responsible for reportingthe scientific data and the writing of this article. The investigatorshad the opportunity to probe the database and to review the results ofthe analyses. The sponsors had the opportunity to review thispublication before its submission for the purpose of ensuring theaccuracy of the data and to determine whether documents needed tobe submitted to protect the intellectual property interests in thecompound or its uses. The trial was registered with the ClinicalTrials.gov with study number NCT 00073372.
ObjectivesThe primary efficacy objective was to compare outcomes, asmeasured by the proportion of mRS responders at 3 months in theprimary population in patients treated with abciximab versus pla-cebo. For patients with baseline National Institutes of Health StrokeScale (NIHSS) scores of 4 to 7, the goal was a mRS score of 0, forthose with a NIHSS score of 8 to 14, the measure of success was ascore of 0 or 1, and for patients with a NIHSS score of 15 to 22, thedesired mRS score was 0 to 2.15 Assuming the response rate to be26% to 31% in the placebo group as found in the AbESTT study, thesample size was chosen such that 1200 patients would have astatistical power of 80% to detect an effect size of 10% with a2-sided significance level of 0.05.14
Secondary efficacy analyses evaluated the proportion of patientswith neurological recovery (NIHSS score 0 to 1) or mortality at 3months; proportions of patients with minimal disability (mRS 0 to 1)at day 5/discharge, 10 days, 6 weeks and 3 months; Barthel Indexscores of 95 to 100 at 5 days/discharge, 10 days, 6 weeks and 3months; Barthel Index scores of 100 at 5 days/discharge, 10 days, 6weeks, and 3 months. Patients with stroke progression or neurolog-ical recovery (NIHSS 0 to 1) at 5 days/discharge and patients withstroke recurrence at 3 months were also analyzed. The distributionsof mRS, Barthel Index, and NIHSS scores at 3 months also wereassessed. Similar efficacy end points were analyzed among patientstreated 5 to 6 hours after stroke and among patients with stroke onawakening.
The primary safety end point was the rate of fatal or nonfatalsymptomatic ICH that was diagnosed within 5 days/discharge. Othersafety events included other ICH within 3 months, asymptomatichemorrhages found on CT within 5 days/discharge or at 3 months,true thrombocytopenia within 5 days/discharge and nonintracranialbleeding within 5 days/discharge. The safety analyses were per-formed independently in the primary and companion populations.
Study CohortsThe design of AbESTT-II included recruitment of patients into 2study cohorts, which were interlinked for baseline assessment,treatment regimen, and follow-up evaluations. However, for the
88 Stroke January 2008
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

statistical analyses for efficacy and safety, the 2 cohorts were treatedas 2 separate studies within the larger trial. This design was reviewedwith and approved by regulatory agencies.
The primary cohort included those persons who could be treatedwithin 5 hours of onset of stroke (randomization �4.5 hours). Thegoal was to recruit 1200 subjects into this cohort. The sample sizecalculations for the trial were based on the anticipated outcomes inthese subjects. The outcomes of the subjects enrolled in the primarycohort were used for the primary safety and efficacy analyses ofAbESTT-II, including any decision to prematurely halt the trial.
Because there was interest in testing the safety and efficacy ofabciximab among subjects treated at a slightly longer interval andamong those with stroke present on awakening, AbESTT-II plannedto evaluate safety and efficacy in another 600 subjects who could beenrolled in the companion cohort. The cohort included those patientswho could be treated 5 to 6 hours after stroke onset (randomization4.5 to 5.5 hours) or who could be treated within 3 hours ofawakening with signs of stroke (randomization �2.5 hours). Bothsafety and efficacy outcomes among the subjects in the companioncohort were analyzed independently from the primary cohort. Inaddition, responses among the subjects in the wake-up group wereevaluated independently from the other subjects in the companioncohort.
Eligible patients were assigned to either abciximab or an identi-cally appearing placebo at a 1:1 randomization using minimizationprocedure with biased-coin assignment.18 The 4 balancing factorsused were: study population (primary or companion), site, baselineNIHSS score (4 to 7, 8 to 14, and 15 to 22—three groups) and timesince stroke onset.
Patients older than 18 years of age and with an acute ischemicstroke resulting in a baseline NIHSS score ranging from 4 to 22 wererecruited at 112 sites (see Appendix). Baseline evaluation included aclinical assessment, non–contrast-enhanced CT of the brain, andlaboratory tests. Baseline clinical assessments included a prestrokemRS and Barthel Index. Women of childbearing potential had apregnancy test and if the test was positive, the woman was excluded.Exclusion criteria for the trial were similar to other acute stroketreatment trials. Those patients that might be treated with intravenousrecombinant tissue plasminogen activator, including most seenwithin 3 hours of onset of stroke, were excluded. Patients with mild(NIHSS score �4) or severe (NIHSS score �22) were excluded. Therespective institutions’ human subject research boards had to ap-prove the protocol and consent. Before enrollment, the patient or asurrogate (where permitted) gave signed consent.
Treatment RegimenPharmacists at the sites were given identically appearing 5-mL vialsof abciximab or placebo. The study medication was administered asan initial bolus dose (0.25 mg/kg) followed by a 12-hour infusion(0.125 �g/kg per minute) up to a maximum infusion of 10 �g/min.
Ancillary Care and Follow-Up AssessmentsPatients were not to receive aspirin or other antithrombotic medica-tions until after a follow-up CT study that was performed 36 to 48hours after randomization. Thereafter, the selection of medicationswas at the discretion of the treating physician. Mechanical methodsfor prevention of deep vein thrombosis were allowed at any timeduring the study. Other interventions, including rehabilitation, wereencouraged. The protocol included recommendations for treatmentof potential complications including thrombocytopenia or seriousbleeding.
Close observation including frequent measurements of vital signswere done during the first 24 hours after completing the infusion ofstudy agent. Blood pressure parameters and recommendations fortreatment of hypertension were provided. Investigators performeddaily clinical assessments and scoring of the NIHSS through day 5 ordischarge, whichever was sooner. Follow-up assessments of the mRSand Barthel Index were done either by telephone or in person at 10days and 6 weeks. Investigators performed the NIHSS, mRS, andBarthel Index at �3 months. Intercurrent events and interventionswere recorded at the time of the follow-up studies.
Hematological studies, including platelet counts, were done atregular intervals until day 5 or discharge. A follow-up CT study wasdone at 36 to 48 hours after randomization. Additional brain-imagingtests during or after the acute treatment period could be ordered at thediscretion of the physician. Other diagnostic studies, includingvascular or cardiac imaging, were ordered by the treating physician.Copies of scheduled and unscheduled brain-imaging studies wereforwarded for central interpretation.
Adverse Experiences and OutcomesSerious adverse experiences were reported following regulatoryrequirements. Breaking of the study blind could be performed in theevent of an emergency that would require knowledge of thetreatment medication. Because of the effects of abciximab on plateletfunction, we included a time period of 5 days to monitor for acutetreatment period adverse experiences, including symptomatic intra-cranial hemorrhage.
Any deaths, including the presumed cause, which occurred within120 days of randomization, were recorded. However, all deathsoccurred before 90 days. Intracranial hemorrhages were diagnosedby the results of brain-imaging tests. The definitions of symptomaticor asymptomatic ICH used by this trial were described previously.14
Symptomatic intracranial hemorrhage was diagnosed if neurologicalworsening was detected and hemorrhage was found on brain imag-ing. A causal link was required. Both major and minor non-neurological bleeding and thrombocytopenia were recorded using thepreviously described definitions.14 In addition, other serious ornonserious adverse experiences were recorded through day 5 and 3months. Investigator-reported bleeding was reported through 3months. Major and minor bleeding events were reported through 5days. Adverse events were recorded through 3 months. Seriousadverse events were also reviewed through 5 days/discharge.
Outcomes were assessed at 5 days and 3 months (90 to 120 daysafter randomization) using the mRS score at 3 months as the primarymeasure of efficacy. Alternative methods to obtain follow-up infor-mation, such as house calls or assessment by a nonstudy physicianwere to be used if the patient could not return to the study site. Anyassessment performed �120 days after randomization was notincluded in the analysis. Other outcomes included neurologicalimprovement, neurological deterioration, stroke progression, or re-current stroke. The definitions of these outcomes have been de-scribed in a prior report.14
Statistical AnalysesThe trial examined safety and efficacy results independently in the 2study cohorts. In addition, results in the companion cohort wereevaluated separately for those patients treated 5 to 6 hours after onsetof stroke and those with stroke detected on awakening. All efficacyanalyses were performed on data from all randomized patients usingthe intention-to-treat principle. All safety analyses were performedon all patients who received at least some study treatment accordingto the actual treatment received. For the adjusted dichotomous mRSresponder analysis, data were inputed for patients with missingobservations on the 3-month mRS by carrying the last availablepostrandomization value. If no postbaseline values were available fora patient or if a patient died before the 3-month assessment, thepatient was considered to be a nonresponder for the 3-month mRSresponder end point. Wald test statistic from a logistic regressionmodel with baseline NIHSS groups as a covariate was used tocompare the 2 treatment groups.
Planned subgroup analyses in each of the cohorts were performedusing adjustments for age, sex, baseline NIHSS scores, time fromonset of symptoms, presence of diabetes, use of aspirin within 24hours or 7 days within randomization, or presence of new stroke onbaseline CT. In general, Mantel-Haenszel �2 statistics were used tocompare event rates or proportions between treatment groups fordichotomous secondary end points without a stratification variable.For rare events, Fisher exact test was performed. Mortality wascalculated using Kaplan–Meier estimates based on those deaths thatoccurred within 120 days of randomization. The log-rank test wasused to compare mortality between the treatment groups.
Adams et al Trial of Abciximab in Acute Ischemic Stroke 89
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

Periodic monitoring of safety data were performed by the SEMC.No formal statistical testing was done on this interim safety data.Two interim efficacy analyses were planned. These analyses were tobe performed when the first 400 and 700 subjects, respectively, in theprimary population had been randomized and 3-month end point datawere available. However, because this trial was terminated early, noplanned interim analyses were performed. Other unscheduled anal-yses, primarily for safety, could be performed at the discretion of the
SEMC or on alert of the trial’s safety monitor, who was unaware oftreatment allocation.
ResultsThe results of AbESTT-II are reported independently for theprimary and companion cohorts. In addition, the resultsamong subjects in the companion cohort are analyzed inde-pendently of the cohort of subjects with stroke present onawakening. The trial did not perform analyses aggregating thedata from the 3 cohorts.
Between December 2003 and September 2005, the trialrandomized a total of 808 patients in 112 sites. At anunscheduled interim analysis in the wake-up stroke patientsdue to a higher than anticipated overall intracranial hemor-rhage rate, the SEMC recommended that recruitment ofpatients into this part of the study be halted effective May 20,2005, because the rate of symptomatic ICH among patientsreceiving abciximab exceeded the anticipated safety margins.Subsequently, in September 2005, the SEMC recommendedsuspending enrollment in the entire trial. After a review of theefficacy data through 6 weeks of follow-up in �90% ofenrolled patients and through 3 months of 80% of all patientsenrolled, the SEMC recommended that the trial be haltedbecause of safety concerns and a less than acceptable benefit-risk ratio. This recommendation was accepted unanimouslyby the Executive Committee and the sponsors. Although thetrial halted recruitment, other study procedures, including
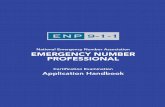
Figure 1. The distribution of patients in the AbESTT-II study is outlined. The primary cohort includes those patients who could beenrolled and randomized to study treatment within 4.5 hours after onset of stroke. The companion cohort includes those patients whocould be assigned study treatment in the period 4.5 to 5.5 hours after stroke or within 2.5 hours of awakening having been asleep forlonger than 5.5 (most commonly on arising in the morning).
Table 1. Primary Reasons for Nonenrollment
Reason Number
Neurological impairments �4 points on NIHSS orsigns rapidly resolving
2907
Neurological impairments �22 points on NIHSS 391
CT findings of hemorrhage 732
CT findings of infarction of �50% of MCA 137
Disabled before stroke (Barthel Index or Rankin Scale) 479
Received rtPA for stroke (�3 hours) 1104
Heparin treatment �48 hours 161
Other serious illness 571
Persistent hypertension that could not be controlled 130
Recent major hemorrhage 52
Need for contraindicated surgical therapy 28
Abnormal baseline coagulation tests 176
MCA indicates middle cerebral artery; rtPA, recombinant tissue plasminogenactivator.
90 Stroke January 2008
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

scheduled follow-up assessments were completed on allpreviously enrolled subjects. The database was not lockedand the final analyses were not performed until these datawere received and verified.
Of 808 patients randomized, 7 patients were not includedin this analysis (5 withdrew consent, 2 have no informedconsent), for a total of 801 analyzable patients. During theperiod of enrollment, 9011 patients were screened. Theprimary reasons for not being enrolled in the trial are includedin Table 1. Many patients had multiple reasons for exclusion.
Four hundred thirty-nine, 319, and 43 patients were en-rolled in the primary, companion, and wake-up cohorts,respectively (Figure 1). Ten randomized patients did notreceive study agent, most commonly because of an elevatedblood pressure that met an exclusion criterion that developedafter entry (Figure 1). One patient assigned to receiveabciximab was administered placebo as a study agent. Threepatients in the companion cohort were not randomized but
received study drug and hence are included in the safetyanalyses. The study blind was broken in 8 instances (abcix-imab–6/placebo–2). The leading reason was a symptomaticICH that required a surgical intervention. Seventy-threepatients (abciximab–38/placebo–35) were treated with anti-thrombotic medication, most commonly aspirin, after ran-domization and before the follow-up CT scan.
Baseline CharacteristicsThe baseline characteristics of the study cohorts are describedin Tables 2 and 3. No differences were found in regard to riskfactors, prior use of antithrombotic medications, interval fromstroke, laboratory findings, results of baseline CT scan, orseverity of stroke. The stratification assured that numbers ofpatients in the 3 subgroups by NIHSS score (4 to 7, 8 to 14,and 15 to 22) were similar. The mean and median NIHSSscores in the abciximab and placebo-treated groups areincluded in the tables. Approximately 20% of the patients in
Table 2. Baseline Characteristics of the Study Cohorts
Primary Companion: 5–6 hours Companion: Wake-Up Stroke
Placebo Abciximab Placebo Abciximab Placebo Abciximab
No. of subjects 218 221 159 160 21 22
Mean age, y, mean�SD 70.2�13.1 68.0�14.1 67.9�13.9 69.4�12 70.5�11.6 68.6�12.4
Men/women 121/97 118/103 73/86 100/60 16/5 13/9
Race
White 207 (95.0) 204 (92.3) 146 (91.8) 149 (93.1) 19 (90.5) 21 (95.5)
Black 3 (1.4) 7 (3.2) 10 (6.3) 5 (3.1) 2 (9.5) 1 (4.5)
Other 8 (3.7) 10 (4.6) 3 (1.9) 6 (3.8) 0 (0) 0 (0)
Mean weight, kg, mean�SD 76.4�16.1 76.8�15.7 76.8�15.9 76.3�17.2 78.0�10.4 78.7�17.8
Location
Europe 134 (61.5) 142 (64.3) 97 (61.0) 89 (55.6) 16 (76.2) 15 (68.2)
North America 50 (22.9) 49 (22.2) 47 (29.6) 55 (34.4) 5 (23.8) 7 (31.8)
South Africa 11 (5.1) 10 (4.5) 4 (2.5) 6 (3.8) 0 (0) 0 (0)
South America 17 (7.8) 15 (6.8) 10 (6.3) 10 (6.3) 0 (0) 0 (0)
Australia 6 (2.8) 5 (2.3) 1 (0.6) 0 (0) 0 (0) 0 (0)
CT findings (217 subjects) (219 subjects) (156 patients) (158 patients) (21 patients) (22 patients)
New stroke* 62 (28.6) 59 (26.9) 42 (26.9) 50 (31.6) 8 (38.1) 9 (40.9)
Old stroke* 67 (30.9) 75 (34.2) 51 (32.7) 59 (37.3) 8 (38.1) 13 (59.1)
Previous TIA 17 (7.8) 21 (9.5) 15 (9.4) 17 (10.6) 0 (0) 3 (13.6)
Previous stroke 25 (11.5) 37 (16.7) 27 (17.0) 18 (11.3) 3 (14.3) 8 (36.4)
Aspirin �7 day 81 (37.2) 78 (35.3) 65 (40.9) 67 (41.9) 8 (38.1) 10 (45.5)
Aspirin �24 hours 69 (31.7) 67 (30.3) 54 (34.0) 49 (30.6) 6 (28.6) 9 (40.9)
Hypertension 149 (68.3) 151 (68.3) 122 (76.7) 106 (66.3) 12 (57.1) 15 (68.2)
Mean systolic BP, mm Hg, mean�SD 148.5�19.8 149.8�22.9 153.3�20.5 148.7�21.6 159.4�18.6 146.9�19.6
Mean diastolic BP, mm Hg, mean�SD 78.8�15.4 79.7�14.3 81.1�13.6 79.1�14.1 84.9�9.5 76.5�16.1
Diabetes 47 (21.6) 42 (19.0) 40 (25.2) 35 (21.9) 3 (14.3) 6 (27.3)
Mean serum glucose, mg/dL, mean�SD 134.9�53.1 132.6�47.2 140.3�55.9 137.2�57.5 128.5�40.7 138.8�44.4
Smoking 54 (24.8) 49 (22.2) 35 (22) 42 (26.3) 5 (23.8) 6 (27.3)
Prior MI 41 (18.8) 35 (15.8) 19 (11.9) 30 (18.8) 3 (14.3) 2 (9.1)
Atrial fibrillation 45 (20.6) 40 (18.1) 33 (20.8) 38 (23.8) 5 (23.8) 3 (13.6)
TIA indicates transient ischemic attack; BP, blood pressure; MI, myocardial infarction.Data presented as N (%) unless otherwise specified.*New stroke: changes on initial CT scan consistent with qualifying event. Old stroke: changes on initial CT scan consistent with event prior to qualifying event.
Adams et al Trial of Abciximab in Acute Ischemic Stroke 91
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

the primary population were enrolled within 3 hours of onsetof stroke.
Primary Cohort
Efficacy OutcomesFigure 2 shows the distribution of outcomes (mRS scores)and the rates of favorable outcomes as defined in theresponder analysis in the primary population at 3 months. Inaddition, the rates of favorable outcomes in subgroups di-vided by NIHSS scores of 4 to 7, 8 to 14, and 15 to 22 areshown. No treatment effect was noted in the primary cohortbetween the abciximab and placebo-treated patients at 3months. Adjustments for baseline NIHSS score, age, diabetesmellitus, prior aspirin use, or baseline CT findings did notaffect the results of the study. Other efficacy outcomes areincluded in Table 4. Stroke progression was diagnosed withinthe first 5 days in 17 abciximab-treated and 19 placebo-treated patients. Recurrent strokes were diagnosed during thefollow-up period in 7 abciximab-treated and 3 placebo-treated patients. No benefit from treatment could be detectedin these secondary analyses.
Symptomatic (Fatal or Nonfatal) ICHIn the primary cohort, symptomatic ICH was diagnosedwithin 5 days in 13 patients (abciximab–12 [5.5%]/placebo–1[0.5%]; P�0.002; Tables 5 and 6). These hemorrhages werefatal in 8 patients (abciximab–8 [3.7%]/placebo–0 [0%];P�0.004). Within 3 months, symptomatic or fatal ICH wasdiagnosed in 2 additional patients in the abciximab group,both of which were fatal (total abciximab–14; P��0.001;Table 4). Patients randomized within 3 hours of onset ofstroke did not have any difference in rates of bleeding orefficacy components compared with those patients treated atslightly longer periods. There was not a relationship of theseverity of neurological impairments, the baseline CT find-ings, or the prior use of medications and the development of
symptomatic hemorrhage in the entire primary cohort orthose enrolled within 3 hours.
MortalityOverall, 60 patients (abciximab–35, placebo–25) died duringthe follow-up period (Table 7). Figure 3 shows the Kaplan–Meier plot of the mortality through 3 months after random-ization of the primary population. The primary causes ofdeath were ICH in 11 patients (abciximab–11, placebo–0),initial stroke in 15 patients (abciximab–6, placebo–9), andrecurrent stroke in 3 (abciximab–3, placebo–0). Other causesof death were evenly distributed between the abciximab andplacebo patients.
Other Safety OutcomesThe rates of asymptomatic ICH, other serious bleeding andthrombocytopenia are listed in Table 7. Other serious adverseexperiences were diagnosed within 5 days in 30 abciximab-treated and 33 placebo-treated patients. Through the 3-monthtime period, serious adverse experiences were diagnosed in123 patients (abciximab–62, placebo–61). Most of theseother serious adverse events were neurological or neurovas-cular and related to the initial stroke as well as subsequentrespiratory disorders.
Efficacy and Safety in the Companion CohortEnrolled 4.5 to 5.5 Hours After Onset of Stroke
Efficacy OutcomesFigure 4 shows the distribution of outcomes (mRS scores)and the rates of favorable outcomes as defined in theresponder analysis in the companion cohort treated 5 to 6hours after stroke at 3 months. In addition, the rates offavorable outcomes in subgroups divided by NIHSS scores of4 to 7, 8 to 14, and 15 to 22 are shown. No treatment effectwas noted. Adjustment for NIHSS score, age, diabetesmellitus, prior aspirin use, or baseline CT findings did notaffect the results of the study. Other efficacy outcomes are
Table 3. Severity and Timing of Stroke in the Study Cohorts
Primary Companion: 5–6 hours Companion: Wake-Up Stroke
Placebo Abciximab Placebo Abciximab Placebo Abciximab
No. of subjects 218 221 159 160 21 22
Time from stroketo randomization
�3 hours 49 (22.5) 45 (20.4)
3–4.5 hours 168 (77.1) 173 (78.3)
�4.5 hours 1 (0.5) 3 (1.4)
Mean interval 3.6 hours 3.6 hours 5.0 hours 5.0 hours 12.1 hours* 10.8 hours
Median interval 3.8 hours 3.7 hours 5.0 hours 5.1 hours 9.9 hours 9.7 hours
NIHSS score
Mean�SD 9.6�5.0 9.9�5.2 9.4�4.9 9.5�4.8 10.0�5.0 10.4�5.0
Median 8.0 8.0 8.0 8.0 9.0 10.0
4–7 101 (46.3) 102 (46.2) 74 (46.5) 73 (45.6) 9 (42.9) 7 (31.8)
8–14 74 (33.9) 70 (31.7) 56 (35.2) 56 (35.0) 8 (38.1) 11 (50.0)
15–22 43 (19.7) 49 (22.2) 29 (18.2) 31 (19.4) 4 (19.0) 4 (18.2)
Data presented as N (%) unless otherwise specified.*Interval from the patient was last known to be normal.
92 Stroke January 2008
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

included in Table 4. Stroke progression within 5 days wasdiagnosed in 37 patients (abciximab–16/placebo–21). Recur-rent strokes at 3 months occurred in 7 patients (abciximab–4/placebo–3). No benefit from treatment could be detected inthese secondary analyses.
Symptomatic (Fatal or Nonfatal) ICHIn this cohort, no significant difference in hemorrhages wasnoted between the 2 treatment groups, symptomatic or fatalICH was detected within 5 days in 4 patients (abciximab–3/placebo—1; Tables 5 and 6). These hemorrhages were fatal in3 patients (abciximab–2/placebo–1). Another 3 hemorrhageswere diagnosed during the follow-up period (abciximab–1/placebo–2), both being fatal in placebo.
MortalityOverall, 35 patients in the companion cohort died (abcix-imab–18, placebo–17; Table 7). The primary cause of deathwas initial stroke occurring in 11 of the 35 patients (abcix-imab–4/placebo–7). Other causes of death were evenly dis-tributed between the abciximab and placebo patients.
Other Safety OutcomesThe rates of asymptomatic ICH, other serious bleeding, andthrombocytopenia are described in Table 5. Other seriousadverse experiences were diagnosed within 5 days in 23
abciximab-treated and 33 placebo-treated patients. Through 3months, serious adverse experiences were diagnosed in 105patients (abciximab–48/placebo–57). Most of these otherserious adverse events were neurological or neurovascularand related to the initial stroke as well as subsequentrespiratory disorders and heart failure.
Efficacy and Safety in the Companion CohortWith Wake-Up Stroke
Efficacy OutcomesFigure 5 shows the distribution of outcomes (mRS scores)and the rates of favorable outcomes as defined in theresponder analysis in the companion cohort with wake-upstroke at 3 months. In addition, the rates of favorableoutcomes in subgroups divided by NIHSS scores of 4 to 7, 8to 14, and 15 to 22 are shown. No significant difference intreatment effect was noted. The numbers of patients in the 2treatment groups are relatively small; adjustment for NIHSSscore, age, diabetes mellitus, prior aspirin use, or baseline CTfindings did not affect the results of the study. Other efficacyoutcomes are included in Table 4. Stroke progression within5 days was diagnosed in 7 patients (abciximab–2/placebo–5).Recurrent strokes at 3 months occurred in 2 patients (abcix-imab–1/placebo–1). No benefit from treatment could bedetected.
Placebo
Abciximab
Percentage of patients
A
Placebo
Abciximab
Percentage of patients
A
33.0 34.7
44.6
9.3
32.1 33.337.1
22.4
0
20
40
60
% o
f Pat
ient
s
Placebo Abciximab
p=0.944 p=0.843 p=0.363 p=0.089
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
B
33.0 34.7
44.6
9.3
32.1 33.337.1
22.4
0
20
40
60
% o
f Pat
ient
s
Placebo Abciximab
p=0.944 p=0.843 p=0.363 p=0.089
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
33.0 34.7
44.6
9.3
32.1 33.337.1
22.4
0
20
40
60
% o
f Pat
ient
s
Placebo Abciximab
p=0.944 p=0.843 p=0.363 p=0.089
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
B
Figure 2. The distribution of scores on themRS (A) and the efficacy results at 3months using the adjusted dichotomousresponder analysis (B) in patients enrolledin the primary cohort is demonstrated forpatients treated either with abciximab orplacebo. In addition, the rates of favorableoutcomes for patients with a baselineNIHSS score of 4 to 7 (desired mRS score0), 8 to 14 (desired mRS score of 0 to 1),or 15 to 22 (desired mRS score 0 to 2) areshown (B).
Adams et al Trial of Abciximab in Acute Ischemic Stroke 93
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

Symptomatic (Fatal or Nonfatal) ICHSymptomatic ICH was diagnosed within 5 days in 4 patients(abciximab–3/placebo–1; Tables 4 and 5). These hemor-rhages were fatal in 3 patients (abciximab–2/placebo–1). Asubsequent fatal hemorrhage was diagnosed in the follow-upperiod in one patient treated with abciximab.
MortalityBesides having a high rate of bleeding complications, overallthis group of patients had a high rate of death, especiallyamong those treated with abciximab. Overall, 9 patients(abciximab–6/placebo–3) died during the follow-up period(Table 7). The primary causes of death in this group wereICH in 4 patients (abciximab–3/placebo–1) and cerebralinfarction in 1 patient (abciximab–1/placebo–0).
Other Safety OutcomesThe rates of asymptomatic ICH, other serious bleeding andthrombocytopenia are reported in Table 5. Other seriousadverse experiences were diagnosed within 5 days in 3abciximab-treated and 5 placebo-treated patients. Through 3months, serious adverse experiences were diagnosed in 13patients (abciximab–6/placebo–7). Most of these other seri-ous adverse events were due to atrial arrhythmias.
DiscussionThis large international trial planned to enroll 1800 patients(1200 in the primary cohort) to test the hypothesis thatabciximab would improve outcomes at 3 months after strokeusing a dichotomous end point on the mRS as influenced bythe baseline NIHSS score. The current trial, which was aphase 3 trial to test efficacy, was built on the success of thedose escalation pilot study and the confirmatory phase IIbtrial that were previously reported.13,14 The trial did not showbenefit from treatment with abciximab in any cohort exam-ined although the primary cohort had a significant increase in
symptomatic or fatal ICH. Based on the lack of a favorablebenefit:risk profile for the study at an interim analysis, andthat it was highly unlikely to demonstrate a favorable profileby enrolling more patients, the SEMC concluded and theinvestigators accepted to discontinue the study.
The previous study suggested that those patients treatedwithin 5 hours of onset of stroke likely would have thegreatest benefit from treatment with abciximab.14 This groupof patients became the primary cohort, for which the overalltrial’s primary safety and efficacy analyses were judged. Theconcept that early restoration of perfusion is associated withthe highest likelihood of improved outcomes is supported bythe meta-analyses of the trials of intravenous thrombolysis.19
This trial did not replicate the previous trial. No improvementin the rates of favorable outcomes with early treatment withabciximab was found. Approximately 20% of the patients inthis group were treated within 3 hours of onset of stroke.Even including this group of patients treated soon after onsetof stroke, an improvement in the rate of favorable outcomeswith treatment with abciximab could not be demonstrated.Analysis of the influence on results by baseline severity ofstroke showed heterogeneity in the results among the differ-ent populations and did not correlate with any evidence ofbenefit. Although the previous study found abciximab to bemost effective in moderate-to-severe stroke (NIHSS scores�15), severity of stroke at baseline did not affect response totreatment in this trial. Both the primary and secondaryoutcome measures of efficacy did not demonstrate atreatment-effect. Subgroups based on clinical and demo-graphic characteristics also demonstrated a lack of efficacy inthe primary outcomes. In summary, this trial did not find thatearly administration of abciximab was effective in improvingoutcomes at 3 months.
In order to determine whether patients could be success-fully treated at longer intervals (up to 6 hours after stroke),the companion population was included in this study. Thisgroup of patients was assigned treatment through anindependent randomization process. Because the intervalfrom stroke until treatment would be longer, it wasanticipated that the rates of favorable outcomes would be
Table 4. Secondary Measures of Efficacy Outcomes at 3Months in the Study Cohorts
Population Placebo, n (%) Abciximab, n (%) P Value
Neurologic recovery
Primary 92/218 (42.2) 96/221 (43.4) 0.794
Companion* 64/159 (40.3) 65/160 (40.6) 0.946
Wake-up 6/21 (28.6) 3/22 (13.6) 0.234
Neurological improvement
Primary 149/218 (68.3) 142/221 (64.3) 0.364
Companion* 103/159 (64.8) 107/160 (66.9) 0.693
Wake-up 14/21 (66.7) 10/22 (45.5) 0.161
Barthel Index score �95
Primary 124/218 (56.9) 126/221 (57.0) 0.978
Companion* 82/159 (51.6) 91/160 (56.9) 0.342
Wake-up 10/21 (47.6) 7/22 (31.8) 0.289
mRS score 0–1
Primary 97/218 (44.5) 94/221 (42.5) 0.679
Companion* 64/159 (40.3) 58/160 (36.3) 0.462
Wake-up 6/21 (28.6) 2/22 (9.1) 0.101
*Patients enrolled 4.5–5.5 hours after onset of stroke.
Table 5. Rates of Symptomatic and Fatal IntracranialHemorrhage Within 5 Days or 3 Months in the Study Cohorts
PopulationPlacebo,
n �n fatal� (%)Abciximab,
n �n fatal� (%) P Value
Symptomatic �fatal�intracranial hemorrhagewithin 5 days/discharge
Primary 1 �0�/217 (0.5) 12 �8�/217 (5.5) 0.002
Companion* 1 �1�/160 (0.6) 3 �2�/158 (1.9) 0.309
Wake-up 1 �1�/20 (5.0) 3 �2�/22 (13.6) 0.347
Symptomatic �fatal�intracranial hemorrhagewithin 3 months
Primary 1 �0�/217 (0.5) 14 �10�/217 (6.5) �0.001
Companion* 3 �3�/160 (1.9) 4 �2�/158 (2.5) 0.690
Wake-up 1 �1�/20 (5.0) 4 �3�/22 (18.2) 0.193
*Patients enrolled 4.5–5.5 hours after onset of stroke.
94 Stroke January 2008
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

less. Indeed, favorable outcomes dropped from 32.1%–33.0% to 23.3%–25.6%. Although the rate of favorableoutcomes was slightly higher with treatment with abcix-imab, these results were not significantly different. Thereis no obvious reason why intravenous administration ofabciximab would be effective at slightly longer treatmentperiod. This finding probably reflects the relatively smallnumber of patients in this treatment group and did not
justify continued recruitment of patients in this groupwhen the results among patients in the primary populationwere negative.
To date, patients who awaken after several hours of sleephave not been enrolled in clinical trials because the time ofonset of stroke has not been known. Serena et al16 observedthat some patients in this group might respond favorably toearly reperfusion therapy. Therefore, some patients were
Table 6. Cases of Symptomatic Hemorrhage
Primary Cohort
Subject Age/SexBaselineNIHSS Time of Event Location
Outcome(mRS score)
Abciximab
1 70/F 7 �12 hours IVH, SAH died
2 77/M 20 �5 days HT died
3 57/M� 6 �12 hours HT, IVH 2
4 59/F 16 �12 hours HT, IVH 4
5 74/M 12 �12 hours HT died
6 73/F 10 �12 hours HT, ICH, IVH died
7 80/F 15 48 hours–�day 5 HT 5
8 74/F 9 12–�48 hours HT, IVH died
9 84/M 17 �12 hours HT, IVH, SAH died
10 56/M 21 �5 days HT died
11 82/F 17 12–�48 hours HT 4
12 85/F 19 12–�48 hours IVH, SAH, SDH died
13 59/M 5 12–�48 hours HT, IVH died
14 80/F 13 12–�48 hours HT, IVH, SAH died
15 55/M 19 �12 hours HT died
Placebo
1 43/M 13 12–�48 hours HT 2
Companion Cohort: Treated 5–6 Hours
Abciximab
1 53/M 13 �12 hours HT 5
2 86/F 9 �5 days HT died
3 58/F 14 �12 hours HT, IVH died
4 29/F 11 �12 hours HT died
Placebo
1 67/M 7 �5 days HT died
2 73/F 13 �5 days HT, ICH died
3 78/M 11 12–�48 hours HT, IVH, SAH died
Companion Cohort (Wake-Up)
Abciximab
1 53/F 5 48 hours–�5 days ICH, IVH died
2 48/M 10 �12 hours HT, SAH died
3 79/M 21 �12 hours HT, IVH, SAH died
4 79/F# 17 12–�48 hours HT 5
Placebo
1 78/M 14 �12 hours HT, ICH, SAH, IVH, SDH died
HT indicates hemorrhagic transformation of qualifying infarction; ICH, intracerebral hemorrhage not instroke; IVH, intraventricular hemorrhage; SAH, subarachnoid hemorrhage; SDH, subdural hematoma.
�Did not receive study drug; #Not randomized but treated.
Adams et al Trial of Abciximab in Acute Ischemic Stroke 95
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

enrolled as a subgroup of the companion population. Basedon CT findings, Todo et al20 concluded that stroke atawakening in many patients may be secondary to events thathappen shortly before arousal. They concluded that thesepatients might be good candidates for acute stroke interven-
tions. Therefore, this trial included an exploratory arm toevaluate the potential efficacy of treatment among patientswith wake-up stroke. Although the mean NIHSS score wasslightly higher among the patients included in the wake-upstroke group, their outcomes in both treatment groups wereworse than those patients whose strokes occurred whileawake. The patients in the group receiving abciximab hadmore complications and overall outcomes were poorer. Be-cause of a concern about the potential safety of abciximabamong the patients in the wake-up stroke group, enrollmentwas suspended. Although the high rate of poor outcomes maybe unique to our study, our experience should cause otherinvestigators to approach this group of patients with caution.
Evaluation of the components of the design of the trial didnot identify any variable to explain the difference between theresults of this trial and our previous study. The treatmentregimen, entry criteria, ancillary care, and follow-up assess-ments were the same. Although the primary outcome measureof efficacy in this trial was changed to the adjusted dichoto-mous responder analysis for this trial, no benefit fromtreatment was seen in any other end point chosen. It isunlikely that the lack of benefit from abciximab shown in thistrial is the result of trial design but more likely the failure oftreatment. Other measures of favorable outcome, including amRS score of 0 to 1 at 3 months regardless of baselineseverity of stroke, neurological recovery, score of 95 to 100on the Barthel Index also showed no treatment effect. Otherstatistical methods, such as the shift in distribution analysis,have been used in clinical trials.21 Such an analysis would nothave provided different results for AbESTT-II.
Symptomatic ICH is a potential complication of any interven-tion used to restore or improve perfusion to the brain after acuteischemic stroke. In AbESTT, the risk of symptomatic ICH was�4% and none of the cases were fatal.14 In contrast, whereas theoverall risk of serious intracranial bleeding in this trial wasapproximately the same, many of the complications were fatal.In addition, the risk of symptomatic intracranial hemorrhagewith treatment with abciximab in AbESTT-II was less than thatreported with intravenous administration of thrombolytic
Table 7. Mortality, Serious Bleeding Complications orThrombocytopenia in the Study Cohorts
Population Placebo, n (%) Abciximab, n (%) P Value
Mortality at 3 months
Primary 25/218 (11.5) 35/221 (15.8) 0.167
Companion* 17/159 (10.7) 18/160 (11.3) 0.887
Wake-up 3/21 (14.3) 6/22 (27.3) 0.298
Asymptomatic intracranialhemorrhage at 5 days
Primary 15/217 (6.9) 21/217 (9.7) 0.297
Companion* 18/160 (11.3) 14/158 (8.9) 0.480
Wake-up 0/20 (0) 2/22 (9.1) 0.172
Asymptomatic intracranialhemorrhage within 3months
Primary 16/217 (7.4) 25/217 (11.5) 0.140
Companion* 19/160 (11.9) 15/158 (9.5) 0.493
Wake-up 0/20 (0) 2/22 (9.1%) 0.172
Major or minor bleedingat 5 days
Primary 7/215 (3.3) 15/214 (7.0) 0.080
Companion* 6/158 (3.8) 6/158 (3.8) 0.982
Wake-up 0/20 (0) 3/22 (13.6) 0.090
Thrombocytopenia† at 5days
Primary 0/217 (0) 6/217 (2.8) 0.014
Companion* 0/160 (0) 4/158 (2.5) 0.043
Wake-up 0/20 (0) 1/22 (4.5) 0.340
*Patients enrolled 4.5–5.5 hours after onset of stroke.†Platelet count �100 000/�L and at least 25% decrease from baseline
value.
1299
0a
0
5
10
15
20
25
30
Sub
ject
s W
ho D
ied
(%)
Days
bamixicbAobecalP
0 30 60 90
p = 0.167
Figure 3. Efficacy Kaplan Meier plot of mortalitythrough 3 months for the primary cohort.
96 Stroke January 2008
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

agents.22,23 Still, comparisons about the hemorrhagic risks foundin AbESTT-II and the trials of thrombolysis should be madewith caution. The agents have different effects on thrombosis.Differences among the trials include the severity of baselinestrokes, interval from stroke onset until treatment, and the periodof observation for symptomatic hemorrhage (24 to 36 hoursversus 5 days). In addition, many patients screened forAbESTT-II were treated with thrombolysis and were excluded.
We have not identified factors, including ancillary care orprevious use of aspirin, that predicted an increased risk ofintracranial bleeding in this study. Although AbESTT-II usedthe same treatment regimen as the previous studies, therealways is a possibility that a lower dose or medication oranother treatment regimen could have lowered the risk ofintracranial bleeding. Because considerable interest remainsabout the possible role of abciximab in treating patients withacute cerebral ischemia in a variety of situations, futureresearchers may wish to look at a lower dose or differenttreatment regimen. At present, there seems little reason to testintravenous administration of abciximab in the dose andregimen that was evaluated in this study.
Although the number of patients enrolled in the wake-upgroup is small, randomization into this arm of the study was
halted earlier than the remainder of the trial because of thehigh rate (13.6% as compared with 5% for placebo) ofsymptomatic ICH among patients treated with abciximab.Given this experience, other investigators should use cautionwhen administering interventions to restore perfusion inpatients with wake-up strokes. Possibly, new criteria foreligibility based on clinical or imaging variables are neededbefore enrolling such patients in future trials.
Although the rates of symptomatic intracranial hemor-rhage among the patients enrolled in the primary popula-tion and those treated within 5 to 6 hours of stroke areimportant, these rates of bleeding might have been accept-able if there were improved outcomes from treatment.Thus, the lack of evidence of efficacy combined with theincreased potential risks from treatment resulted in thistrial’s premature discontinuation of enrollment. The trialsuggests that intravenous abciximab does not have a role inthe management of patients with acute ischemic stroke.The results of this trial should not be construed to reflectthe lack of efficacy or safety of abciximab in other formsof acute vascular disease, including acute myocardialischemia, or in other clinical settings, such as the use of theagent in conjunction with endovascular interventions.
Placebo
Abciximab
Percentage of patients
A
Placebo
Abciximab
Percentage of patients
A
23.3
14.9
33.9
24.125.6 27.4 25.0 22.6
0
20
40
60
% o
f Pat
ient
s
Placebo Abciximab
p=0.625 p=0.063 p=0.300 p=0.887
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
B
23.3
14.9
33.9
24.125.6 27.4 25.0 22.6
0
20
40
60
% o
f Pat
ient
s
Placebo Abciximab
p=0.625 p=0.063 p=0.300 p=0.887
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
23.3
14.9
33.9
24.125.6 27.4 25.0 22.6
0
20
40
60
% o
f Pat
ient
s
Placebo Abciximab
p=0.625 p=0.063 p=0.300 p=0.887
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
B
Figure 4. The distribution of scores on themRS (A) and the efficacy results at 3months using the adjusted dichotomousresponder analysis (B) in patients in thecompanion cohort enrolled between 4.5and 5.5 hours is demonstrated for patientstreated either with abciximab or placebo.In addition, the rates of favorable out-comes for patients with a baseline NIHSSscore of 4 to 7 (desired mRS score 0), 8to 14 (desired mRS score of 0 to 1), or 15to 22 (desired mRS score 0 to 2) areshown (B).
Adams et al Trial of Abciximab in Acute Ischemic Stroke 97
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

AppendixExecutive Committee Members
H.P. Adams, Jr, W. Hacke, A. Davalos, J. Torner, J.Frayne, P. Teal, J. Leclerc, B. Oemar, M.B. Effron.
Steering Committee MembersA. Demchuck, A. Massaro, R. Atkinson, P. Trouillas,
M.-H. Mahagne, M. Kaste, A. Grau, G. Ford, J. Frayne.
Coordinating CenterIowa: H.P. Adams, E. Leira, P. Davis, K. Grimsman;
Heidelberg: W. Hacke, P. Ringleb, P. Schnitzer.
SEMCD. Sherman, J. Easton, M. Eliasziw, G. Winslow, Dr
Wolf-Dieter Heiss, B. Thornton.
Investigators Who Recruited at Least on Patient(number of patients enrolled in each country includedin parenthesis)
Argentina (45): M. Pardal, A. Firstenfeld, B. Maskin, J.Furst. Australia (12): R. Markus, D. Crimmins. Austria (13):F. Fazekas, F. Aichner. Belgium (25): P. Cras, G. Vanhooren,V. Thijs, C. Willems. Brazil (22): F. Yamamoto, R. Gagliardi,A. Massaro. Canada (80): N. Bayer, A. Penn, P. Teal, V.Hachinski, L. Berger, A. Shuaib, A. Demchuk, D. Selchen.
Spain (139): E. Diez-Tejedor, R. Fernandes-Bolanos, F.Lopez, A. Chamorro, J. Roquer, J. Castillo, J. Alvarez-Sabin,A. Davalos, Y. Silva. Filand (19): J. Sivenius, M. Kaste.France (62): C. Magne, P. Trouillas, F. Woimant, M.Mahagne, P. Amarenco. Great Britain (2): G. Ford. Germany(108): R. Schneider, D. Nabavi, G. Seidel, R. Toepper, C.Kessler, P. Vogel, M. Jauss, G. Gahn, A. Grau, A. Mueller-Jensen, P. Berlit, W. Boessenecker, M. Schabet, A. Hetzel, H.Audebert, J. Glahn, R. Huber, P. Ringleb. Italy (17): P.Nichelli, I. Santilli, G. Comi. Netherlands (2): Dr van derWorp. Poland (79): J. Pniewski, A. Szczudlik, H.Hertmanowska, W. Nyka, Z. Stelmasiak, W. Drozdowski, W.Fryze, A. Kuczynska-Zardzewialy, A. Czlonkowska. Portugal(29): L. Cunha, G. Lopes, T. Pinho e Melo, A. Salgado. SouthAfrica (31): C. Guldenpfennig, J. Roos. Switzerland (11): J.Bogousslavsky, R. Baumgartner. United States (112) D.Kleindorfer, S. Starkman, J. Yasen, S. Braheny, J. Broderick,E. Jauch, S. Cruz-Flores, M. Schneck, E.M. Hekler, P.L.Kwen, C. Lewandowski, S. Rasmus, E. Leira, S. Kasner, R.Bernstein, L. Anderson, B. Demaerschalk, W. Felton, III,E.C. Haley, Jr, J. Hilburn, K. Ng, K. Levin, T. Devlin, M.Hammer.
Radiology CenterJ. Maley, M. White, J. Weigele.
Placebo
Abciximab
Percentage of patients
A
Placebo
Abciximab
Percentage of patients
A
14.311.1
25.0
4.5
14.3
0
20
40
% o
f Pat
ient
s
Placebo Abciximab
p=0.272 p=0.849 p=0.080 p=NA
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
0 0 0
B
14.311.1
25.0
4.5
14.3
0
20
40
% o
f Pat
ient
s
Placebo Abciximab
p=0.272 p=0.849 p=0.080 p=NA
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
0 0 0
14.311.1
25.0
4.5
14.3
0
20
40
% o
f Pat
ient
s
Placebo Abciximab
p=0.272 p=0.849 p=0.080 p=NA
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
14.311.1
25.0
4.5
14.3
0
20
40
% o
f Pat
ient
s
Placebo Abciximab
p=0.272 p=0.849 p=0.080 p=NA
Overall BaselineNIHSS 4-7
BaselineNIHSS 8-14
BaselineNIHSS 15-22
0 0 0
B
Figure 5. The distribution of scores on themRS (A) and the efficacy results at 3months using the adjusted dichotomousresponder analysis (B) in patients enrolledin the companion cohort with wake-upstroke is demonstrated for patients treatedeither with abciximab or placebo. In addi-tion, the rates of favorable outcomes forpatients with a baseline NIHSS score of 4to 7 (desired mRS score 0), 8 to 14(desired mRS score of 0 to 1), or 15 to 22(desired mRS score 0 to 2) are shown (B).
98 Stroke January 2008
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

Adjudication CenterK. Sila, N. Pasca.
BITIS. Bhat, M. White, J. Maley, J. Weigele.
CentocorB. Oemar, G. Holtkamp, V. Valbert, M. Etzi, J. Kearl, T.
Henrick, J.D. Lu, L. Damaraju, E. Barnathan.
LillyJ. Croaning, R. Kovacs, J. Leclerc, V. Helm, S. Winings,
R. Lockhart, M.B. Effron.
Sources of FundingSupported by Eli Lilly and Company and Centocor Research andDevelopment (see text describing interactions between the sponsorsand the trial).
DisclosuresH.P.A. has a financially significant research grant that is sponsoredby Eli Lilly and Company and Centocor Research and Development.M.E. has a significant ownership interest in Eli Lilly and Company,and has been employed by Eli Lilly and Company. A.D., J.F., andP.T. have a financially significant research grant that is sponsored byEli Lilly and Company and Centocor Research and Development.J.L., L.P., E.B., and W.H. have significant ownership interests andhave been employed by Centocor Research and Development. B.O.and W.H. have ownership interests and have been employed by EliLilly and Company. J.C.T. has nothing to disclose.
References1. Zhang ZG, Chopp M, Goussev A, Lu D, Morris D, Tsang W, Powers C,
Ho KL. Cerebral microvascular obstruction by fibrin is associated withupregulation of PAI-1 acutely after onset of focal embolic ischemia inrats. J Neurosci. 1999;19:10898–10907.
2. Zhang ZG, Zhang L, Tsang W, Goussev A, Powers C, Ho KL, Morris D,Smyth SS, Coller BS, Chopp M. Dynamic platelet accumulation at thesite of the occluded middle cerebral artery and in downstreammicrovessels is associated with loss of microvascular integrity afterembolic middle cerebral artery occlusion. Brain Res. 2001;912:181–194.
3. Zhang L, Zhang Z, Zhang C, Zhang RL, Chopp M. Intravenous admin-istration of a GPIIb/IIIa receptor antagonist extends teh therapeuticwindow of intra-arterial tenecteplase-tissue-tissue plasminogen activatorin a rat stroke model. Stroke. 2004;35:2890–2895.
4. Zhang L, Zhang ZG, Zhang R, Morris D, Lu M, Coller BS, Chopp M.Adjuvant treatment with a glycoprotein IIb/IIIa receptor inhibitorincreases the therapeutic window for low-dose tissue plasminogen admin-istration in a rat model of embolic stroke. Circulation. 2003;107:2837–2843.
5. Morris DC, Silver B, Mitsias P, Lewandowski C, Patel S, Daley S, ZhangZG, Lu M. Treatment of acute stroke with recombinant tissue plasmin-ogen activator and abciximab. Acad Emerg Med. 2003;10:1396–1399.
6. Morris DC, Zhang L, Zhang ZG, Lu M, Berens KL, Brown PM, ChoppM. Extension of the therapeutic window for recombinant tissue plasmin-ogen activator with argatroban in a rat model of embolic stroke. Stroke.2001;32:2635–2640.
7. Qureshi AI, Suri FK, Khan J, Fessler RD, Guterman LR, Hopkins LN.Abciximab as an adjunct to high-risk carotid or vertebrobasilar angio-plasty: preliminary experience. Neurosurgery. 2000;46:1316–1325.
8. Qureshi AI, Suri MF, Ali Z, Kim SH, Lanzino G, Fessler RD. Carotidangioplasty and stent placement: a prospective analysis of perioperativecomplications and impact of intravenously administered abciximab.Neurosurgery. 2002;50:466–473.
9. lee KY, Heo JH, Lee SI, Yoon WB. Rescue treatment with abciximab inacute ischemic stroke. Neurology. 2001;56:1585–1587.
10. Ho DS, Wang Y, Chui M, Ho SL, Cheung RT. Intracarotid abciximabinjection to abort impending ischemic stroke during carotid angioplasty.Cerebrovasc Dis. 2001;11:300–304.
11. Mitsias PD, Lu M, Morris D, Silver B, Lewandowski C, Papamitsakis NI,Khaligi MM, Ebadian HB, Zhao Q, Soltanian-Zadeh H, Daley S,Hearshen D, Ewing JR, Patel SC, Chopp M. Treatment of acute supra-tentorial ischemic stroke with abciximab is safe and may result in earlyneurological improvement: A Preliminary Report. Cerebrovasc Dis.2004;18:249–250.
12. Mandava P, Lick SD, Rahman MA, Langsjoen H, Reddy KV, Nelson J,Kent TA. Initial saety experience of abciximab and heparin for acuteischemic stroke. Cerebrovasc Dis. 2005;19:276–278.
13. The Abciximab in Ischemic Stroke Investigators. Abciximab in acuteischemic stroke: a randomized, double-blind, placebo-controlled, dose-escalation study. Stroke. 2000;31:601–609.
14. Abciximab Emergent Stroke Treatment Trial (AbESTT) Investigators.Emergency administration of abciximab for treatment of patients withacute ischemic stroke. Results of a randomized phase 2 trial. Stroke.2005;36:880–890.
15. Adams HP Jr, Leclerc JR, Bluhmki E, Clarke W, Hansen MD, Hacke W.Measuring outcomes as a function of baseline severity of ischemic stroke.Cerebrovasc Dis. 2004;18:124–129.
16. Serena J, Davalos A, Segura T, MOstacero E, Castillo J. Stroke onawakening: looking for a more rational management. Cerebrovasc Dis.2003;16:128–133.
17. Fink JN, Kumar S, Horkan C, Linfante I, Selim MH, Caplan LR, SchlaugG. The stroke patient who woke up: clinical and radiological features,including diffusion and perfusion MRI. Stroke. 2002;33:988–993.
18. Pocock SJ, Simon R. Sequential treatment assignment with balancing forprognostic factors in the controlled clinical trial. Biometrics. 1975;31:103–115.
19. Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP,Brott T, Frankel M, Grotta JC, Haley EC Jr, Kwiatowski T, Levine SR,Lewandowski C, Lu M, Lyden P, Marler JR, Patel S, Tilley BC, AlbersG, Bluhmki E, Wilhelm M, Hamilton S; ATLANTIS Trials Investigators;ECASS Trials Investigators; NINDS rt-PA Study Group Investigators.Association of outcome with early stroke treatment: pooled analysis ofATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:768–774.
20. Todo K, Moriwaki H, Saito K, Tanaka M, Oe H, Naritomi H. Early CTfindings in unknown-onset and wake-up strokes. Cerebrovasc Dis. 2006;21:367–371.
21. Lees KR, Zivin JA, Ashwood T, Davalos A, Davis SM, Diener HC,Grotta J, Lyden P, Shuaib A, Hardemark HG, Wasiewski WW;Stroke-Acute Ischemic NXY Treatment (SAINT I) Trial Investigators.NXY-059 for Acute Ischemic Stroke. N Engl J Med. 2006;354:588–600.
22. The National Institute of Neurological Disorders and Stroke rt-PA StrokeStudy Group. Tissue plasminogen activator for acute ischemic stroke.N Engl J Med. 1995;333:1581–1587.
23. The NINDS t-PA Stroke Study Group. Intracerebral hemorrhage afterintravenous t-PA therapy for ischemic stroke. Stroke. 1997;28:2109–2118.
Adams et al Trial of Abciximab in Acute Ischemic Stroke 99
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from

for the AbESTT-II InvestigatorsJacques Leclerc, Barry Oemar, Lakshmi Padgett, Elliot S. Barnathan and Werner Hacke
Harold P. Adams, Jr, Mark B. Effron, James Torner, Antoni Dávalos, Judith Frayne, Philip Teal,Stroke Trial (AbESTT-II)
ofStroke: Results of an International Phase III Trial: Abciximab in Emergency Treatment Emergency Administration of Abciximab for Treatment of Patients With Acute Ischemic
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2007 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.106.476648
2008;39:87-99; originally published online November 21, 2007;Stroke.
http://stroke.ahajournals.org/content/39/1/87World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 29, 2016http://stroke.ahajournals.org/Downloaded from