
Preparation of Caco-2 cell sheets using plasma polymerised acrylic acid as a weak boundary layer
Upload
independentCategory
view
1download
0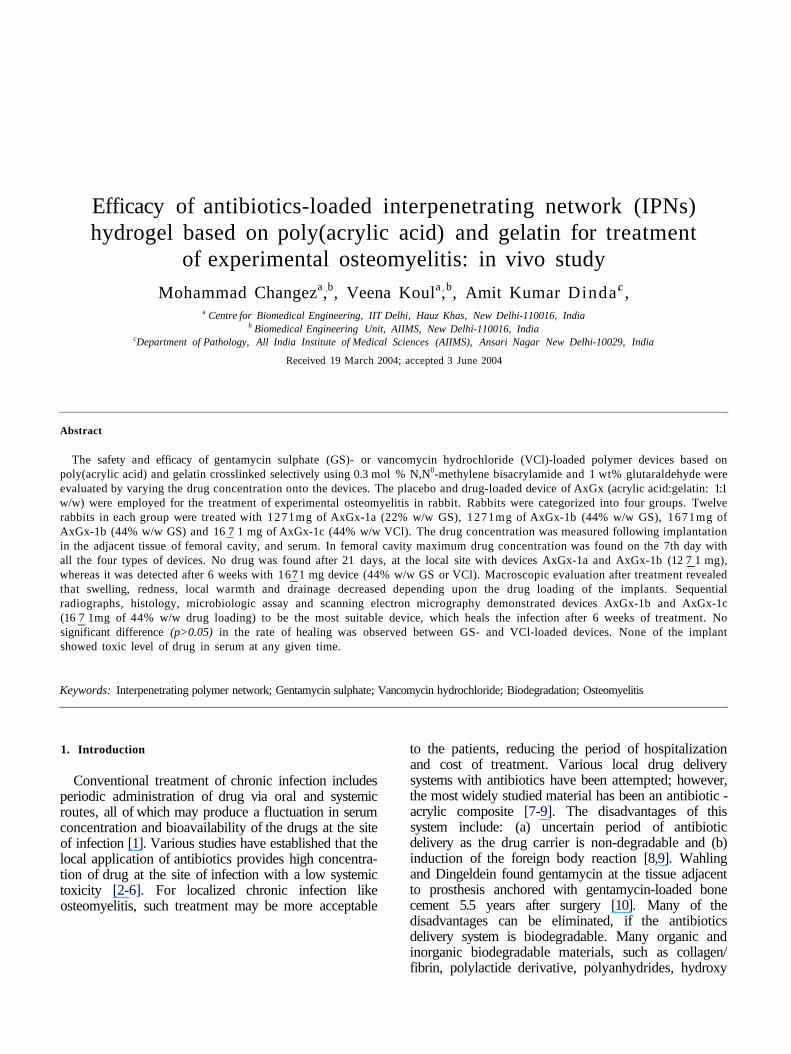
Efficacy of antibiotics-loaded interpenetrating network (IPNs)hydrogel based on poly(acrylic acid) and gelatin for treatment
of experimental osteomyelitis: in vivo study
Mohammad Changeza,b, Veena Koula,b, Amit Kumar Dinda c ,a Centre for Biomedical Engineering, IIT Delhi, Hauz Khas, New Delhi-110016, India
h Biomedical Engineering Unit, AIIMS, New Delhi-110016, IndiacDepartment of Pathology, All India Institute of Medical Sciences (AIIMS), Ansari Nagar New Delhi-10029, India
Received 19 March 2004; accepted 3 June 2004
Abstract
The safety and efficacy of gentamycin sulphate (GS)- or vancomycin hydrochloride (VCl)-loaded polymer devices based onpoly(acrylic acid) and gelatin crosslinked selectively using 0.3 mol % N,N0-methylene bisacrylamide and 1 wt% glutaraldehyde wereevaluated by varying the drug concentration onto the devices. The placebo and drug-loaded device of AxGx (acrylic acid:gelatin: 1:1w/w) were employed for the treatment of experimental osteomyelitis in rabbit. Rabbits were categorized into four groups. Twelverabbits in each group were treated with 1271mg of AxGx-1a (22% w/w GS), 1271mg of AxGx-1b (44% w/w GS), 1671mg ofAxGx-1b (44% w/w GS) and 16 7 1 mg of AxGx-1c (44% w/w VCl). The drug concentration was measured following implantationin the adjacent tissue of femoral cavity, and serum. In femoral cavity maximum drug concentration was found on the 7th day withall the four types of devices. No drug was found after 21 days, at the local site with devices AxGx-1a and AxGx-1b (12 7 1 mg),whereas it was detected after 6 weeks with 1671 mg device (44% w/w GS or VCl). Macroscopic evaluation after treatment revealedthat swelling, redness, local warmth and drainage decreased depending upon the drug loading of the implants. Sequentialradiographs, histology, microbiologic assay and scanning electron micrography demonstrated devices AxGx-1b and AxGx-1c(16 7 1mg of 44% w/w drug loading) to be the most suitable device, which heals the infection after 6 weeks of treatment. Nosignificant difference (p>0.05) in the rate of healing was observed between GS- and VCl-loaded devices. None of the implantshowed toxic level of drug in serum at any given time.
Keywords: Interpenetrating polymer network; Gentamycin sulphate; Vancomycin hydrochloride; Biodegradation; Osteomyelitis
1. Introduction
Conventional treatment of chronic infection includesperiodic administration of drug via oral and systemicroutes, all of which may produce a fluctuation in serumconcentration and bioavailability of the drugs at the siteof infection [1]. Various studies have established that thelocal application of antibiotics provides high concentra-tion of drug at the site of infection with a low systemictoxicity [2-6]. For localized chronic infection likeosteomyelitis, such treatment may be more acceptable
to the patients, reducing the period of hospitalizationand cost of treatment. Various local drug deliverysystems with antibiotics have been attempted; however,the most widely studied material has been an antibiotic -acrylic composite [7-9]. The disadvantages of thissystem include: (a) uncertain period of antibioticdelivery as the drug carrier is non-degradable and (b)induction of the foreign body reaction [8,9]. Wahlingand Dingeldein found gentamycin at the tissue adjacentto prosthesis anchored with gentamycin-loaded bonecement 5.5 years after surgery [10]. Many of thedisadvantages can be eliminated, if the antibioticsdelivery system is biodegradable. Many organic andinorganic biodegradable materials, such as collagen/fibrin, polylactide derivative, polyanhydrides, hydroxy

TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
apatite, etc. were attempted. Collagen antibiotics spongeappears to be equally as popular as PMMA beads forthe treatment of bone infection and it has beencommercially available for the last 10 years [11]. But,in vitro antibiotics release from collagen sponges wasshort lived and completed within the first 4 days [12].Similarly, approximately 85% of loaded antibiotic wasreleased within 72 h from fibrin seal coats [13]. Hydroxyapatite due to similar chemical composition to naturalbone was considered an ideal candidate for long-termlocal antibiotics or drug delivery [14]. But the brittlenessand poor strength of hydroxy apatite limited its use.Ideal strategies for the management of osteomyelitis byimplant device should aim at the restoration of bonecongruity and maintenance of the high concentration ofantibiotics at the site of infection for prolonged periodof time [15]. Such a system also has to be biocompatible,biodegradable and cost effective.
The main aim of the present study was to optimize thedose of antibiotics (gentamycin sulphate (GS) andvancomycin hydrochloride (VCl)) -loaded interpenetrat-ing network hydrogel based on poly(acrylic acid (AA))and gelatin for at least 6 weeks in vivo release of drug atthe site of infection without systemic toxicity. Theperformance of the implant was evaluated by grossexamination, histological, microbiological evaluation,radiography and scanning electron microscopy (SEM).
2. Materials and methods
2.1. Chemicals
AA (G. S. Chemicals, Delhi, India) was purified bydistillation under reduced pressure. Gelatin (Ge) (TypeB), glutaraldehyde (25% AR), sodium metabisulphite (s.d. Fine Chem. Ltd., Delhi, India), N, N0-methylenebisacrylamide (BAm) and ammonium persulphate(SISCO research lab, Mumbai, India), Muellar HintonAgar and Muellar Hinton broth (Titan Biotech Limited,Bhiwandi, India), vancomycin hydrochloride (LillyPharma Fertigung, GmbH, Germany) and gentamycinsulphate (Kee pharma Ltd., New Delhi, India) wereused for the study.
2.2. Device synthesis
The devices were prepared following the methoddescribed previously [16]. Full interpenetrating polymernetwork (IPN) devices based on poly(AA) and gelatin,which are crosslinked selectively using 0.3 mol % ofN,N0-methylene bisacrylamide and 1 wt% of glutaralde-hyde, respectively. The IPNs were washed extensivelywith water to remove water-soluble moieties and driedin a vacuum oven to constant weight. The hydrogel lotwas designated as AxGx-1. According to in vitro/in vivoresults based on swelling, degradation, drug releaseproperties and toxicity, AA:Ge (1:1 w/w) was selectedfor the treatment of osteomyelitis (unpublished data).
2.3. Antibiotics loading in hydrogel
GS or VCl was loaded onto the devices by swellingphenomenon. Percentage increase in the weight of thehydrogels was considered as an amount of drug loading.For 44% and 22% w/w drug loading, 10 mg of polymersample was swollen in 10 ml of GS solution at aconcentration of 1.0 and 0.5mg/ml, respectively, inphosphate buffer (pH 7.4) at 37±0.1°C. For 44% VClloading in hydrogel, VCl concentration in solution was1.2mg/ml. To observe the leaching of polymer compo-nent from polymer network, the xerogel was immersedin phosphate buffer (pH 7.4) at 37°C. After immersingthe polymer sample for 48 h, it was taken out, dried andreweighed. The increase in the weight of the polymerwas taken as the amount of drug loaded, whereasnegligible change in weight was observed in neatpolymer. Furthermore, for the confirmation of percen-tage of drug loading in hydrogels, the amount of GS leftin the loading medium was determined by measuring theoptical density using method of Sampath et al. [17].Microbiological assay was also used to calculate the GSand VCl concentrations [18-19]. Table 1 shows thesample designation and composition of the devices.
2.4. Sterilization of devices
The devices were sterilized under UV light in alaminar flow bench for 24 h before implantation inrabbits [20].
Table 1Sample designation, feed composition of the full IPN at acrylic acid: gelatin ratio (AA:Ge) 1:1 w/w and gentamicin sulphate (GS) or vancomycinhydrochloride (VCl) loading
Network composition
AxGxAxGxAxGxAxGx
Sample designation
AxGx-1AxGx-1aAxGx-1bAxGx-1c
Concentration of BAm(mol %)
0.30.30.30.3
Concentration ofglutaraldehyde (w%)
1.01.01.01.0
Antibiotics loading(drug: %w/w)
—
22 (GS)44 (GS)44 (VCl)
TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
2.5. Development of osteomyelitis in rabbits andevaluation of the antibiotics-loaded implants for thetreatment of osteomyelitis
2.5.1. Induction of osteomyelitis and its treatmentExperiments were conducted on New Zealand white
rabbits, weighing between 1.5 and 2 kg. All animals wereprocured from the Central Animal House Facility of theAll India Institute of Medical Sciences (New Delhi,India) after due clearance from the Local EthicalCommittee. Haemolytic strain of Staphylococcus aureuswas obtained from a chronic osteomyelitis patientundergoing surgical treatment at the All India Instituteof Medical Sciences for induction of osteomyelitis.
Standard suspension (106/(colony-forming units)(cfu)/ml) was prepared in saline and kept in ice throughoutthe surgical procedure. For the development of osteo-myelitis, rabbits were anaesthetized with intravenousinjection of ketamine hydrochloride (40mg/kg). Themedullary cavity of rabbit femur was exposed through alateral approach and a small hole of 0.3 cm using dentaldrill was made at the middle of the femur. Bacterialsuspensions of 500 ml were directly delivered into themedullary cavity, the overlying fascia was repaired andwound was closed [21,22]. Using patient isolates,osteomyelitis was developed within 3 weeks of inocula-tion of organism in 60 rabbits out of a total 66 engagedfor the study. The treatment with the drug-loaded
(a)
• 1 week & 2 weeksS 3weeks E3 4weeksM 6weeks • 12weeks
Al Cl DB SI NB DB SI NB
o£oo</>
(c)
D 1 week Q2 weeksM 3weeks El 4weeks• 6weeks H 12weeks
Al Cl D B SI N B
ou
(d)
D 1 week S 2 weeksS3weeks E3 4weeksD 6weeks H 12weeks
Al Cl DB SI NB
"5.2
• 1 weekE 4weeks
S 2 weeks• Sweeks
13weeksI12weeks • 1 week
0 4weeks^ 2 weeksD 6weeks
13weeks112wecks
(e) Al Cl DB SI NB (f) A l Cl DB SI NB
Fig. 1. Histological finding of (a) group A, (b) group B, (c) group C, (d) group D, (e) group E and (f) group F animals.
TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
.I Fihrosis related tii
sham operation
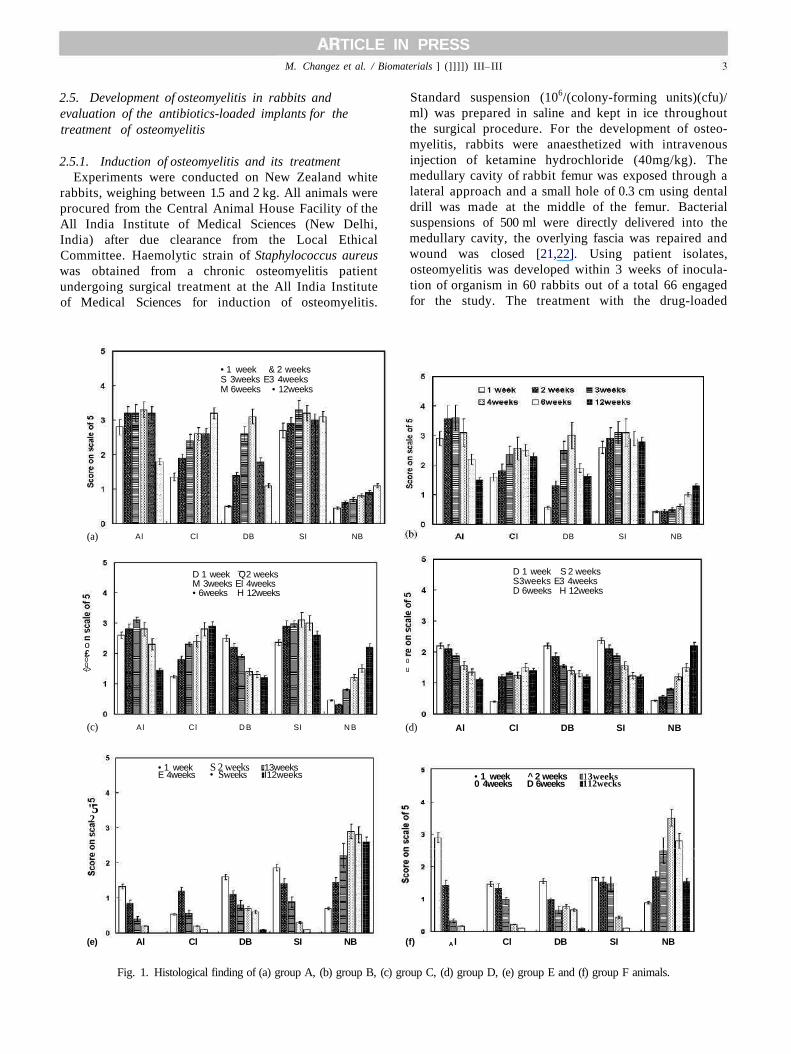
Fig. 2. Light micrograph of (a) sham-operated normal bone (groupG), (b) group A animals after 6 weeks osteomyelitis, (c) group Banimals after 6 weeks of implantation of AxGx-1 without drug (BC:bacterial colonies; NC: necrosis; DB: dead bone; AB: abscess; MS:marrow space) (H&E x 100).
implant was done after 1 week of gross, radiological andmicrobiologic confirmation of development of osteomye-litis in the animals. Cylindrical-shaped antibiotics-loaded
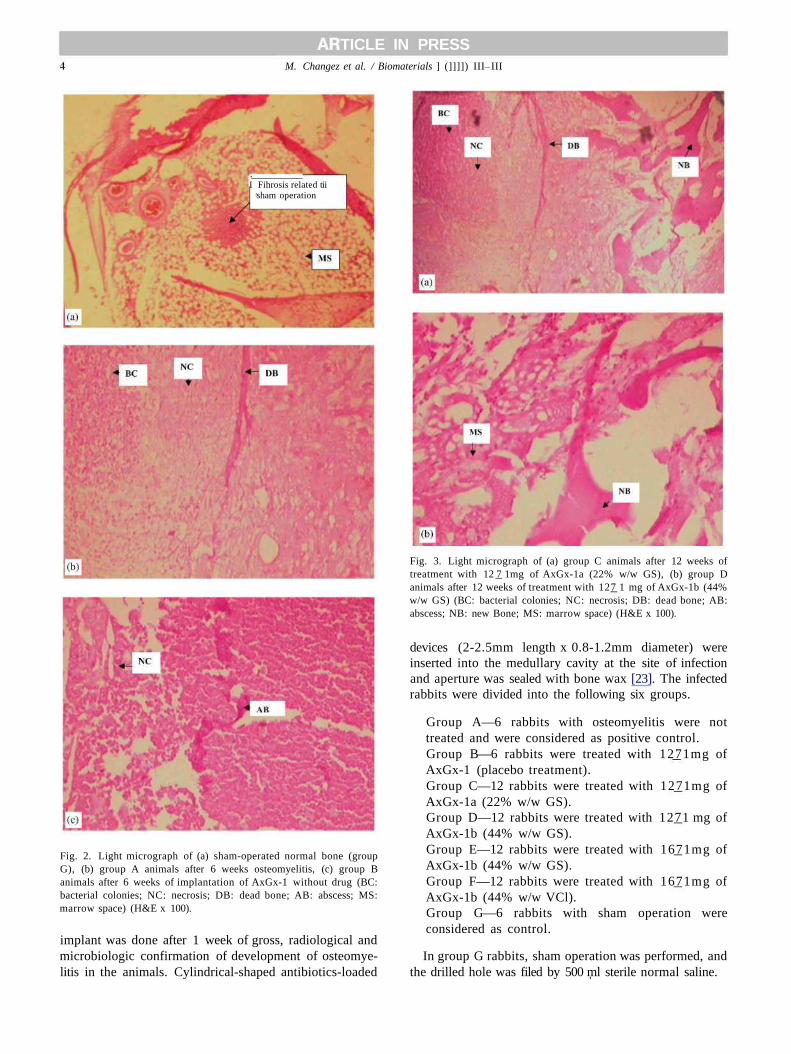
Fig. 3. Light micrograph of (a) group C animals after 12 weeks oftreatment with 12 7 1mg of AxGx-1a (22% w/w GS), (b) group Danimals after 12 weeks of treatment with 127 1 mg of AxGx-1b (44%w/w GS) (BC: bacterial colonies; NC: necrosis; DB: dead bone; AB:abscess; NB: new Bone; MS: marrow space) (H&E x 100).
devices (2-2.5mm length x 0.8-1.2mm diameter) wereinserted into the medullary cavity at the site of infectionand aperture was sealed with bone wax [23]. The infectedrabbits were divided into the following six groups.
Group A—6 rabbits with osteomyelitis were nottreated and were considered as positive control.Group B—6 rabbits were treated with 1271mg ofAxGx-1 (placebo treatment).Group C—12 rabbits were treated with 1271mg ofAxGx-1a (22% w/w GS).Group D—12 rabbits were treated with 1271 mg ofAxGx-1b (44% w/w GS).Group E—12 rabbits were treated with 1671mg ofAxGx-1b (44% w/w GS).Group F—12 rabbits were treated with 1671mg ofAxGx-1b (44% w/w VCl).Group G—6 rabbits with sham operation wereconsidered as control.
In group G rabbits, sham operation was performed, andthe drilled hole was filed by 500 ml sterile normal saline.
TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
2.5.2. Monitoring of the induction and treatment ofosteomyelitis
Induction and treatment of osteomyelitis in rabbitwas monitored by macroscopic, histopathological,microbiological and radiographical observation atdifferent time intervals. Gross observation was per-formed daily. Microbiological assay was carried out onalternate days till the stoppage of pus discharge, andradiography was done weekly. Blood samples werecollected at predetermined time intervals (1, 2, 3, 4, 5, 7,10, 14, 21, 28, 35 and 42 days) for the estimation ofantibiotics concentration as well as monitoring the renal(serum creatinine and blood urea nitrogen levels) andliver functions (serum transaminase levels). After treat-ment, one rabbit from groups A, B and G, two rabbitsfrom groups C, D, E and F were killed at 1, 2, 3, 4, 6 and12 weeks. Tissue fluid and implant collected wereevaluated for the local concentration of antibiotics.The femur along with its surrounding tissue and organslike liver, kidney, spleen, heart was fixed in 10%formalin for histopathological observations. Localwarmth, swelling and drainage from the site of infectionwere graded according to the method proposed byDahner and Funderburk [24]. The tissues were pro-cessed by an automatic tissue processor (Histo Kinette,Shandon, USA). Paraffin blocks were sectioned at 5 mmand stained with haematoxylin, eosin (H&E) formorphological evaluation, Grams stain was done forobservation of bacteria and Massons Trichrome stainsfor evaluation of fibrosis. The histological criteria usedto evaluate osteomyelitis were acute and chronicinflammation, adjacent soft tissue abscess formation,dead and new bone formation and presence of bacteria.These histological observations were graded in a scale of0-5 by two independent observers on coded slides. Thescale 0 signified the absence of feature and 5 showed themaximum presence of feature. Radiography of rabbitwas done using a Siemens-Multix-C, X-ray machine at asetting of 44 kV and 3.2mA/s. The distance between theX-ray source and the bone was 100 cm. The radio-graphic criteria used to evaluate osteomyelitis wereperiosteal elevation, architecture deformation, boneshaft widening, new bone formation and soft tissuedeformation [25]. These findings were correlated withthe culture report and histopathological results.
2.5.3. Estimation of drug in blood and at a local siteThe minimum inhibitory concentration of GS and
VCl in S. aureus (ATCC 259523) was established byusing an antibiotic tube dilution method in cationsupplemented Mueller-Hinton broth, containing5.0 x 105cfu/ml. After the minimum inhibitory concen-tration was determined, quantification of antibiotics inserum and bone cavity fluid was done by using anantibiotic disk diffusion method in the Mueller-Hintonagar [18,19].
2.6. Assessment of renal and liver function
Blood urea nitrogen, serum creatinine, SGOT andSGPT were measured by an auto analyzer (Dyna 5 Labsystem, USA).
2.7. Morphological studies of devices
The morphology of control after 1, 3 and 6 weeks ofimplantation of AxGx-1b (44% w/w GS) was studiedusing the Cambridge Stereoscan Model SGX1-10 SEM.
2.8. Statistical evaluation
All the data were statistically analysed by Student'st e s t for two-sample equal variance (homoscedastic)and statistical significance was accepted at po0.05.Experimental results were expressed as the mean 7 thestandard deviation of the mean.
TV
1 Remodeling1 ut'honc
Bone marrw^* * * *
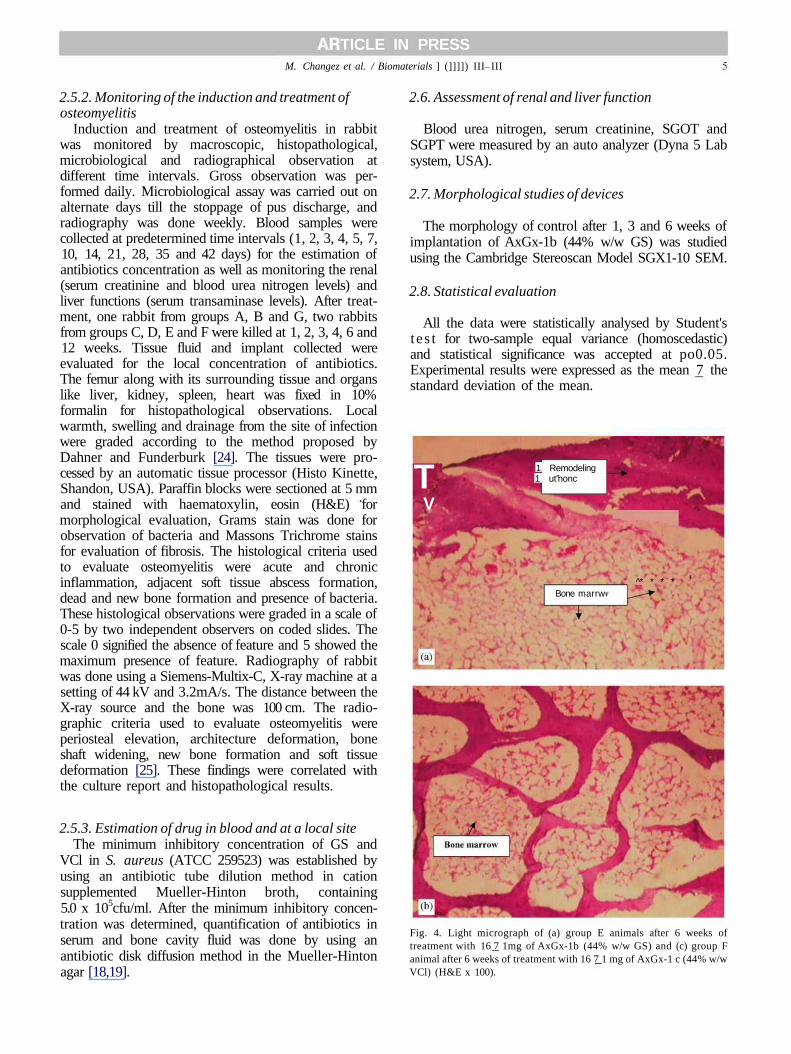
Fig. 4. Light micrograph of (a) group E animals after 6 weeks oftreatment with 16 7 1mg of AxGx-1b (44% w/w GS) and (c) group Fanimal after 6 weeks of treatment with 16 7 1 mg of AxGx-1 c (44% w/wVCl) (H&E x 100).
TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
3. Results
3.1. Macroscopic finding
The swelling (2.7 7 0.2) and redness (2.170.3) weremore in untreated animals of group A and B after 3weeks of confirmation of osteomyelitis and continuedtill 12 weeks of study period with drainage of pus. Incomparison, animals of groups C and D showedsignificantly reduced (po0.05) score of swelling(1.6 7 0.3) and local warmth (1.3 7 0.2) after the 3rdweek of treatment. Swelling subsided in group E and Fanimals, after the 2nd week of treatment (0.2 7 0.1) withdisappearance of local warmth and drainage of pus. As
expected with group G rabbits, swelling (1.170.10) andlocal warmth (0.95 7 0.15) were found only during the1st week, which may be due to the surgical procedure.
3.2. Histological observation
The histological scoring of group A-F rabbits withtime is depicted in Fig. 1a-f, respectively. The data ofgroup A and group B rabbits were similar withoutsignificant difference. Starting from the first week oftreatment, scores of group E and F animals weresignificantly lower (po0.01) than other group animals.Light micrograph pictures of sham-operated bone(group G), infected bone (group A) and placebo (12
• 1 weekC3 4weeks
9 2 weeks1 6 weeks
(b)
• 1 week E3 2 weeks^ 3weeks El 4weeksD6weeks M 12 weeks
PE A D W B ST N B
• 1 week El 2 weeksH3weeks El4weeksD 6weeks M 12weeks
• 1 weekEl 4weeks
^2 weeks• 6weeks
1 3weeks112weeks
(d)
D1 weekQ4weeks
BS 2 weeks • 3weeks• 6weeks H12weeks
(e) PE AD WB SI NB
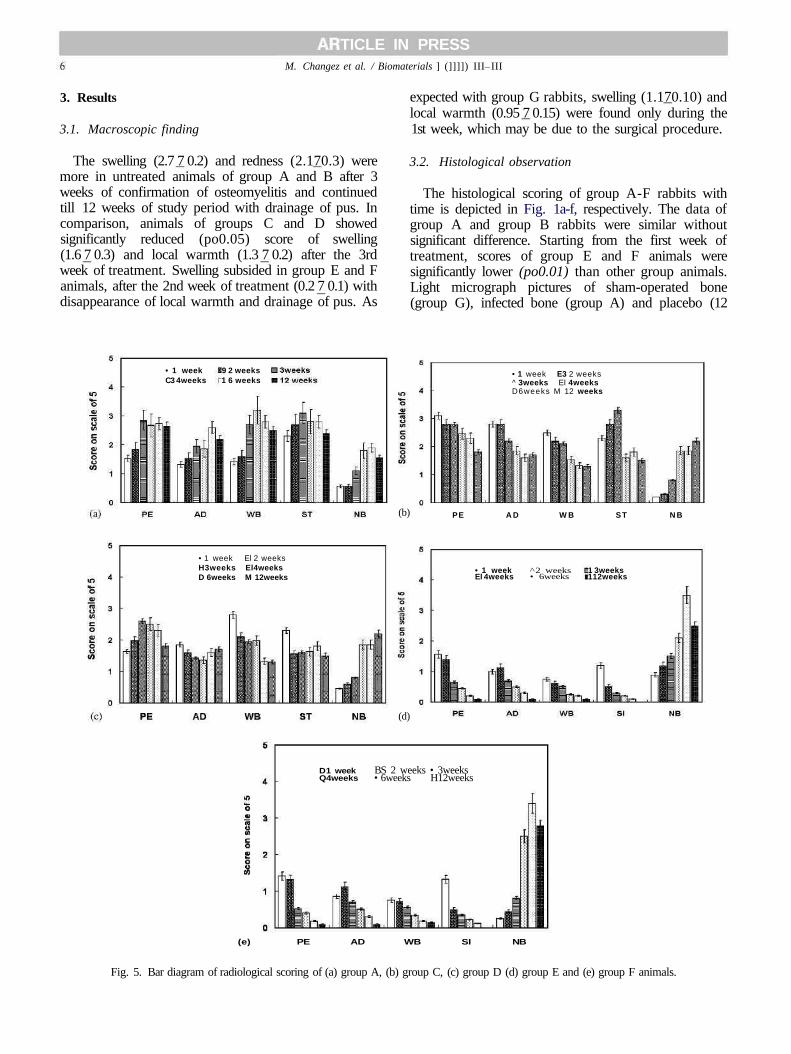
Fig. 5. Bar diagram of radiological scoring of (a) group A, (b) group C, (c) group D (d) group E and (e) group F animals.

TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
weeks) -treated bone (group B) are depicted in Fig. 2a-c,respectively. Comparing the inflammatory responses ofgroup A and group B animals, it appeared that placeboimplants did not change the type of inflammation orprogression of osteomyelitis. Fig. 3a and b depicts thelight micrograph of group C and D rabbits afterthe 12th week of treatment with 127 1mg of AxGx-1a(22% w/w GS) and AxGx-1b (44% w/w GS), respec-tively. The disease was not cured, but the severity ofinflammation was lesser in comparison to groups A andB. This is depicted in bar diagrams (Fig. 1), showing thepersistence of acute and chronic soft tissue inflammationup to the study time of 12 weeks. Fig. 4a and b showedthe complete healing of infection by 6 weeks followingtreatment with 167 1mg device, AxGx-1b (44% w/wGS) and 167 1mg device AxGx-1c (44% w/w VCl),respectively. The histological score for acute and chronicinflammation considerably decreased (po 0.001) at thefourth week of treatment for group E and group Fanimals, and it disappeared after 6 weeks. However,mild fibrosis, focal aggregates of lymphocytes, plasmacells and occasional multinucleated giant cells wereobserved at the implantation site. Adjacent bonemarrow and bony trabaeculae were histologicallyunremarkable after healing of infection and no granu-loma formation was seen (Fig. 4a and b). After the 12thweek, implant residue was no longer present at the localsite. This indicated that antibiotics carrier degraded andresorbed gradually during the course treatment withimplantation.
3.3. Radiological finding
The scores for radiological findings of groups A-F aredepicted in Fig. 5a-e, respectively. Fig. 6a and b,represents the normal and sham-operated morphologyof bone, respectively. Figs. 6c, d and 7a depict the X-rayimage of femur in untreated animals with progression of
osteomyelitis infection in the form of periosteal eleva-tion, architecture deformation, widening of the boneshaft, soft tissue deformity and swelling as well as newbone formation. Fig. 7b and c depicts the X-rays ofgroup C and D animals, respectively, after 12 weeks oftreatment without healing. Radiological evidence forhealing of infection treated with 167 1mg of deviceAxGx-1b (44% w/w GS) and AxGx-1c (44% w/w VCl)is shown in Fig. 7d and e, respectively. The effectivehealing was observed at 6 weeks of treatment. Therewere no differences in the overall findings of group Aand group B animals. According to scoring, group Cand D animals showed statistically significant (po0.05)improvement in comparison to the group A and Brabbits, but infection was not completely cured after12th weeks of treatment.
3.4. Local concentration of antibiotics
Table 2 depicts the mean concentration of GS in thebone cavity fluid. Concentration of drug in femur cavitywas not detected after 21 days of treatment with127 1mg of AxGx-1a (22% w/w GS) and AxGx-1b(44% w/w GS). However, local GS concentrations infemoral cavity were 26.33 7 4.2, 6.2172.21, 5.25 7 2.4,3.3 7 1.8, and 2.9271.3 on days 7, 14, 21, 28 and 42,respectively, after 167 1mg implantation of AxGx-1b.For group F animals, the mean local vancomycinhydrochloride concentration in femoral cavity was29.12 7 2.2, 8.2172.01, 4.2571.8, 3.571.2, and 2.95 70.8 on days 7, 14, 21, 28 and 42, respectively, after167 1 mg implantation of AxGx-1c (44% w/w VCl).
3.5. Serum concentration of antibiotics
Concentration of GS in serum for group C and Drabbits was in the range of 1.82 7 0.30, 1.23 70.20, 0.95 7 0.12, and 0.85 7 0.10 mg/ml, on days 1-4,
Fig. 6. X-rays of (a) normal bone, (b) sham-operated bone, (c) after 1 week of induction and (d) after 3 weeks of induction of infection.

TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
Fig. 7. X-rays of (a) group A rabbit after 6 weeks of treatment, (b) group C rabbit an after 12 weeks of treatment with 1271mg of AxGx-1a (22% w/wGS), (c) group D rabbit after 12 weeks of treatment with 1271mg of AxGx-1b (44% w/w GS), (d) 6 weeks of treatment with 16 7 1mg of AxGx-1b(44% w/w GS) and (e) 6 weeks of treatment with 16 7 1mg of AxGx-1c (44% w/w VCl).
Table 2Local concentration
System
12 7 1mg AxGx-1a12 7 1mg AxGx-1b16 7 1mg AxGx-1b
of gentamicin sulphate in femoral
7 days
12.56 7 3.415.36 7 2.224.33 7 4.2
cavity (mg/ml)
1 days
3.26 7 1.213.95 7 1.127.2172.21
28 days
1.2370.301.5 7 0.75
5.35 7 2.4
2 days
3.271.8
s21 days
2.8271.3
respectively, after which it was not detectable. Forgroup E animals, serum drug concentrations were2.78 7 0.35, 2.13 7 0.27, 1.95 7 0.12, 1.170.10 and0.98 7 0.14 mg/ml on day 1, 2 3, 4 and 7 respectively.For group F animal, serum vancomycin hydrochlorideconcentrations were 3.28 7 0.31, 2.43 7 0.47, 1.35 7 0.12,and 1.170.10 mg/ml on days 1-4 respectively. After 7days, it was not detectable. The local concentration ofGS and VCl released from 1671mg of AxGx-1b andAxGx-1c (44% w/w drug) was higher than the minimuminhibitory concentration (MIC) and minimum bacter-icidal concentration (MBC) levels in this study evenafter 6 weeks of implantation. The high local antibioticsconcentration observed during the 1st week of treatmentwas mainly due to burst effect and then controlledrelease of drug was observed. As per the pharmacody-namics of antibiotics treatment for localized infectionlike osteomyelitis, initial high dose could be moreconvenient than a small dose for a longer period [26].The systemic blood concentration of antibiotics wasmuch below the toxic level in all these implants,supporting the advantage of this mode of treatment.
3.6. Blood urea nitrogen, serum creatinine and hepatictransaminases
Blood urea nitrogen, serum creatinine, SGOT andSGPT were within the normal limit, excluding thepossibility of renal or hepatocellular injury.
3.7. SEM observation of implants AxGx-1b
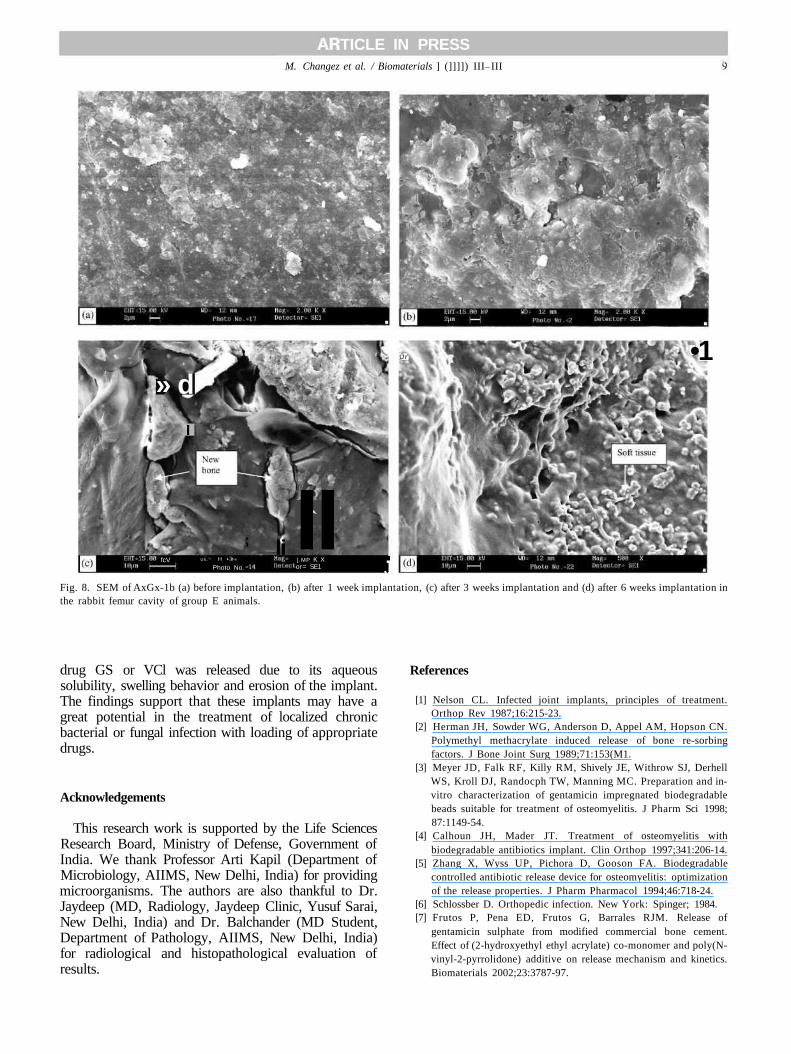
Fig. 8a-d depicted the GS-loaded AxGx-1b devicebefore implantation after 2, 3 and 6 weeks of implanta-tion on femoral cavity, respectively. Comparison to Fig.8a morphology of the implanted device was substan-tially changed with progress of time. In the 3rd week oftreatment, formation of new bone within the polymermatrix was seen (Fig. 8c), and after 6 weeks channelsdue to degradation were observed in polymer matrixalong with the formation of soft tissue. At 12 weeks oftreatment, polymer was not seen in the bone cavity.
4. Conclusion
The present multimodal study revealed that thetreatment of osteomyelitis by hydrogel implant wasdose dependent. The implants with 1271mg of drugAxGx-1a (22% w/w GS) and AxGx-1b (44% w/w GS)did not cure the infection till 12 weeks. However, with1671mg device (AxGx-1b or AxGx-1c) loaded with44% w/w antibiotic, the infection was healed within 6weeks. The implant material was well tolerated. Noresidual hydrogel was seen after the infection got cured.Kidney and liver function tests were within normallimits and no histological abnormality was detected invital organs. The serum levels of the drugs were verylow, excluding the possibility of systemic toxicity. The
TICLE IN PRESSM. Changez et al. / Biomaterials ] (]]]]) III III
:
» dI
fcV Ul i . H • r-
Photo No.
; li II] .MP K Xor= SE1 J
Ur •1
Fig. 8. SEM of AxGx-1b (a) before implantation, (b) after 1 week implantation, (c) after 3 weeks implantation and (d) after 6 weeks implantation inthe rabbit femur cavity of group E animals.
drug GS or VCl was released due to its aqueoussolubility, swelling behavior and erosion of the implant.The findings support that these implants may have agreat potential in the treatment of localized chronicbacterial or fungal infection with loading of appropriatedrugs.
Acknowledgements
This research work is supported by the Life SciencesResearch Board, Ministry of Defense, Government ofIndia. We thank Professor Arti Kapil (Department ofMicrobiology, AIIMS, New Delhi, India) for providingmicroorganisms. The authors are also thankful to Dr.Jaydeep (MD, Radiology, Jaydeep Clinic, Yusuf Sarai,New Delhi, India) and Dr. Balchander (MD Student,Department of Pathology, AIIMS, New Delhi, India)for radiological and histopathological evaluation ofresults.
References
[1] Nelson CL. Infected joint implants, principles of treatment.Orthop Rev 1987;16:215-23.
[2] Herman JH, Sowder WG, Anderson D, Appel AM, Hopson CN.Polymethyl methacrylate induced release of bone re-sorbingfactors. J Bone Joint Surg 1989;71:153(M1.
[3] Meyer JD, Falk RF, Killy RM, Shively JE, Withrow SJ, DerhellWS, Kroll DJ, Randocph TW, Manning MC. Preparation and in-vitro characterization of gentamicin impregnated biodegradablebeads suitable for treatment of osteomyelitis. J Pharm Sci 1998;87:1149-54.
[4] Calhoun JH, Mader JT. Treatment of osteomyelitis withbiodegradable antibiotics implant. Clin Orthop 1997;341:206-14.
[5] Zhang X, Wyss UP, Pichora D, Gooson FA. Biodegradablecontrolled antibiotic release device for osteomyelitis: optimizationof the release properties. J Pharm Pharmacol 1994;46:718-24.
[6] Schlossber D. Orthopedic infection. New York: Spinger; 1984.[7] Frutos P, Pena ED, Frutos G, Barrales RJM. Release of
gentamicin sulphate from modified commercial bone cement.Effect of (2-hydroxyethyl ethyl acrylate) co-monomer and poly(N-vinyl-2-pyrrolidone) additive on release mechanism and kinetics.Biomaterials 2002;23:3787-97.
TICLE IN PRESS10 M. Changez et al. / Biomaterials ] (]]]]) III III
[8] Nelson CL, Evans RP, Blaha JD, Calhoun J, Henry SL, PatzakisMJ. A comparison of gentamicin-impregnated poly(methylmetha-crylate) bead implantation to conventional parenteral antibiotictherapy in infected total hip and kee arthoplasty. Clin Orthop1993;295:96-101.
[9] Majid SA, Lindberg LT, Gunterberg B, Siddiki MS. GentamicinPMMA beads in the treatment of chronic osteomyelitis. ActaOrthop Scand 1985;56:265-8.
[10] Wahlig H, Dingeldein E. Antibiotics and bone cement. Experi-mental and clinical long-term observations. Acta Orthop Scand1980;51:49-56.
[11] Kanellakopoulou KM, Bourboulis EJG. Carrier systems for thelocal delivery of antibiotics in bone infection. Drugs2000;59:1223-32.
[12] Wachol DZ, Pfeiffer M, Scholl E. Comparative investigationof drug delivery of collagen implants saturated in antibioticssolution and a sponge containing gentamicin. Biomaterial1996;17:1733-8.
[13] Redl H, Schlag G, Stanek G, Hirschi A, Seelich T. In vitroproperties of mixture of fibrin seal and antibiotics. Biomaterial1983;4:29-32.
[14] Sasaki S, Ishii Y. Apatite cement containing antibiotics: efficacyin treating experimental osteomyelitis. J Orthop Sci 1999;4:316-69.
[15] Sanchez E, Baro M, Soriano I, Perera A, Evora C. In vivo-in vitrostudy of biodegradable and osteointegrable gentamicin boneimplants. Eur J Pharmac Biopharm 2001;52:151-8.
[16] Burugapalli K, Bhatia D, Koul V, Choudhary V. Interpenetratingpolymer networks based on poly(acrylic acid) and gelatin I:swelling and thermal behavior. J Appl Polym Sci 2001;82:217-27.
[17] Sampath SS, Robinson DH. Comparison of new and existingspectrophotometer methods of analysis of tobramycin and otheramino glycosides. J Pharm Sci 1990;79:428-31.
[18] Prior S, Gamazo C, Irache JM, Merkle HP, Gander B.Gentamicin encapsulation in PLA/PLGA micro spheres in viewof treating Brucella infections. Int J Pharm 2000;196:115-25.
[19] Walker CA, Kopp B. Sensitive bioassay for vancomycin.Antimicrob Agents Chemother 1978;13:30-3.
[20] Shastri VP, Padera RF, Tarcha P, Langer R. A preliminary reporton the biocompatibility of photopolymerizable semi-interpene-trating anhydride networks. Biomaterials 2004;25:715-21.
[21] Nelson CL, Sandra GM, Robert AS, Mark SS, Thomas JR, KeithMO. The treatment of experimental osteomyelitis by surgicaldebribement and the implantation of calcium sulphate tobramy-cin pellets. J Orthop Res 2002;20:643-7.
[22] Norden CW, Keleti E. Experimental osteomyelitis caused byPseudomonas aeruginosa. J Infect Dis 1980;141:71—5.
[23] Ihsan G, Feza K, Fusun T, Alaeddinoglu GN, Vasif H. In vivoapplication of biodegradable controlled antibiotic release systemfor the treatment of implant related osteomyelitis. Biomaterial2001;22:73-80.
[24] Dahners LE, Funderburk CH. Gentamicin-loaded plaster of parisas a treatment of experimental osteomyelitis in rabbits. ClinOrthop 1987;219:278-82.
[25] Smeltzer MS, Thomas JR, Hickmon SG, Skinner RA, Nelson CL,Griffith D, Parr Jr TR, Evans RP. Characterization of rabbitsmodel of staphylococcal osteomyelitis. J Orthop Res 1997; 15:414-21.
[26] Henry SL, Galloway KP. Local antibacterial therapy for themanagement of orthopedic infection: pharmacokinetics consid-erations. Clin Pharmacokinet 1995:29:36^15.
Copyright © 2022 FDOKUMEN




















