
Efficacy of a Unani formulation in Nazla Haar
168
Efficacy of a Unani formulation in Nazla Haar By A.H. AYSHAH FAZEENAH Dissertation submitted to t he Rajiv Gandhi University of Health Sciences, Karnataka, Bangal ore In partial fu lfillment of the requirements for the degree of MAHIRE TIB (MD Unani) i n MOALAJAT (Medicine) Under the guidance of Dr. Mohd. Aleemuddin Quamri Department of Moalajat National Institute of Unani Medicine Bangalore 2012
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Efficacy of a Unani formulation in Nazla Haar
Efficacy of a Unani formulation in Nazla Haar
By
A.H. AYSHAH FAZEENAH
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment
of the requirements for the degree of
MAHIRE TIB (MD Unani)
in
MOALAJAT (Medicine)
Under the guidance of
Dr. Mohd. Aleemuddin Quamri
Department of Moalajat National Institute of Unani Medicine
Bangalore 2012

ii
Rajiv Gandhi University of Health Sciences, Karnataka
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “Efficacy of a Unani formulation
in Nazla Haar” is a bonafide and genuine research work carried out by me under
the guidance of Dr. Mohd. Aleemuddin Quamri, Lecturer, Department of
Moalajat, National Institute of Unani Medicine, Bangalore.
Date:
Place: Bangalore A.H. Ayshah Fazeenah
iii
National Institute of Unani Medicine (Dept. of AYUSH, Ministry of Health & Family Welfare, Govt. of India)
Kottigepalya, Magadi Main Road, Bangalore-91 Telephone: 080-23584260, Ext: 262, Telefax: 080-23580725
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “Efficacy of a Unani formulation in
Nazla Haar” is a bonafide research work done by A.H. Ayshah Fazeenah in
partial fulfillment of the requirement for the degree of Mahire Tib (MD Unani) in
Moalajat under my supervision and guidance.
Dr. Mohd. Aleemuddin Quamri Lecturer
Department of Moalajat National Institute of Unani Medicine
Bangalore
Date:
Place: Bangalore
iv
National Institute of Unani Medicine (Dept. of AYUSH, Ministry of Health & Family Welfare, Govt. of India)
Kottigepalya, Magadi Main Road, Bangalore-91 Telephone: 080-23584260, Ext: 262, Telefax: 080-23580725
ENDORSEMENT BY THE HOD AND HEAD OF THE INSTITUTION
This is to certify that the dissertation entitled “Efficacy of a Unani formulation in
Nazla Haar” is a bonafide research work done by A . H . Ayshah Fazeenah under
the guidance of Dr. Mohd. Aleemuddin Quamri, Lecturer, Department of
Moalajat, National Institute of Unani Medicine, Bangalore.
Prof. Mansoor Ahmad Siddiqui Prof. M. A. Jafri Head of the Department Director Dept. of Moalajat National Institute of Unani Medicine National Institute of Unani Medicine Bangalore Bangalore
Date: Date:
Place: Bangalore Place: Bangalore

v
COPYRIGHT
Declaration by the Candidate I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the right to preserve, use and disseminate this dissertation /
thesis in print or electronic format for academic / research purpose.
Date: Place: Bangalore A.H. Ayshah Fazeenah
©Rajiv Gandhi University of Health Sciences, Karnataka

Dedicated to My Parents
and My Husband
for their
Never-ending Blessings, Love and
Encouragement

Acknowledgment
vi
ACKNOWLEDGEMENT
In the name of Allah, the most beneficent, merciful, omnipresent, omnipotent, anywhere and His
countless peace be upon His prophet and our prince of all living creature, head of Apostles, the
Load Muhammad, his family and his pious.
The completion of this dissertation is not only fulfillment of my dreams but also of my husband,
parents and mother-in-law who have sacrificed a lot for me in completion of this course. The
writing of a dissertation is obviously not possible without the support and company of
numerous people. It is a pleasant aspect that I have now the opportunity to express my gratitude
for all of them.
In the first place, I would like to express my gratitude to Indian High Commission and External
Resource Department, Sri Lanka for select me as a Government nominee for the AYUSH
Scholarship program. I oblige to thank Department of AYUSH, Ministry of Health and Family
Welfare, India and Indian Council for Cultural Relations (ICCR) New Delhi, for considered me as
a foreign nominee, providing me an opportunity for admission in MD course in NIUM, and
continuous financial support during the study.
It gives me immense pleasure to express my eternal and deep sense of gratitude and sincere
respect to my beloved teacher, guide and mentor Dr Mohd. Aleemuddin Quamri, Lecturer Dept.
of Moalajat, NIUM- Bangalore, without whose precious guidance, energetic suggestion,
constructive criticism, extra efforts, immense help, supervision and encouragement at each and
every point of this study, it would not have been possible for me to carry out this work. I
acknowledge his intelligent, diligent and serious help in transforming this would be fantastic
ideas into comprehensive and logical statements which are in front of you as a dissertation.
I wish to express my deep sense of gratitude to Prof. M. A. Jaffri, Director National Institute
of Unani Medicine (NIUM), Bangalore for moral encouragement and providing the necessary
facilities for research as and when sought for.
It is my duty to thanks to Prof. Kshanika Hirimburigama, Vice Chancellor, University of
Colombo and Dr. Jayasinghe, Director, Institute of Indigenous Medicine (IIM), Rajagiriya, Sri
Lanka giving me an opportunity to complete my PG study.
I express my sincere thanks to Prof. M A Siddiqui, HOD Moalajat NIUM Bangalore, for his
valuable suggestion, constant encouragement and cordial cooperation as and when sought for.
Acknowledgment
vii
I wish to express my cordial and humble thanks to beloved teachers o f IIM, University of
Colombo, Sri Lanka for their continuous encouragement, constant help and affectionate attitude
during the entire course of my study.
I take this opportunity to express my heartfelt reverence and highly obliged to my respected
teachers Prof. Dr. Mohd Anwar, HOD of Dept. of Ilaj Bil Tadbeer, Dr. Tanzil Ahmad, Reader,
Department of Moalajat, Dr. Abdul Nasir Ansari , Reader, Department of Ilaj Bil Tadbeer and
Dr. G. Sofi, lecturer, Dept. of Ilmul Advia, NIUM, for their kind support, guidance and
valuable suggestions.
I have much pleasure in expressing my grateful thanks to my colleagues Dr. Rumaiza, Dr.
Nasmeer, Dr. Musta Ali, Dr. Abdur Rasheed, Dr. Mohamed Ali, Dr. Razaur Rasheed, Dr.
Nadeem Ahmad, Dr. Abdal Ahamed, Dr. Qutubuddin, Dr. Sadique Ali, Dr. Nafees Iqbal, and
Dr. Aliya, whose advice has been great help to me. I sincerely appreciate their cooperation and
support.
I also express my thanks to my seniors Dr Raeesuddeen, Dr. Nusrat, and Dr. Azad as well as
juniors Dr. Humyra, Dr. Aslam, Dr. Sheeraz, Dr.Imtiyaz, Dr.Naseemul Hasan,
Dr.Sarfaraz, Dr. Yasir, Dr. Arshadwani, Dr. Ghuffran and Dr. Zahir who helped me to
complete this dissertation. I wish to thank from the core of my heart to all my batch mates from
the Depts. of Qabala, Hifzane Sehat, Ilmul Advia, and Ilmul Saidla.
I would like to express my sincere thanks to Dr. Renuka BN, Pathologist Hospital Laboratory,
NIUM for her kind support, advice and showing practical interest in my laboratory
work. I owe my sincere thanks to Mrs. Sanjeeda Tabassum (Biochemist), Mohd Haneef, Mohd
Zaki, Mrs. Kavitha , Rohit, and Govardan for helping me in my laboratory work. I
would like to thank Dr. Mahboob Pasha Consultant Radiologist and Mohd. Sameer for their
valuable co-operation during the trial. I also express my thanks to Dr. Nafees Khan, Chief
Pharmacist; Mr. Fazil and Mr. Kashif (NIUM pharmacy staff) for providing best quality drugs.
I express my intense sense of thanks to library staff (NIUM) Mr. Ehtisham. Mr. Danish and Mr.
Mudassir who never expressed signs of exhaustion in providing me literature. I am thankful to
Mr. Syed Tarique for his co-operation in my study.
It is my obligation to express my heartfelt gratitude to one of my paternal uncles M.S.M Razik,
design director at international capital trading for his moral, sound and stable support in each
and every step of my progress.

Acknowledgment
viii
This dissertation would never have been completed without love, moral support, patience,
devotion, compassion, generosity, encouragement, affection and sacrifice from my beloved
siblings and in-laws. I am greatly indebted to them.
Lastly I express my appreciation to all the patients, without whose co-operation, this
study would not be possible.
It is not possible to acknowledge individually all of my friends and colleagues who helped me
in various ways and in different aspects of the study, nevertheless, I am grateful to all of them
and at the same time I express my apology for all those whom I could not mention by their names.
I pray to Almighty Allah to show me the right path, the path of those whom He has
bestowed His Grace, those whose (portion) is not wrath, and who go not astray (Aameen).
Date: Fazeenah Hameed
Place: Bangalore
ix
LIST OF ABBREVIATIONS AND SYMBOLS USED
AD Anno Domain
AMP Adenine Mono Phosphate
AR Allergic Rhinitis
ARIA Allergic Rhinitis and its Impact on Asthma
AT After Treatment
Bal. Balghami
BC Before Christ
BT Before Treatment
β Beta
Chr. Christian
cm2 Centimeter squared
CRF Case Report Form
Dam. Damavi
DLC Differential Leukocyte Count
du. Dust
ed. Edition
e.g. Example
ESR Erythrocyte Sedimentation Rate
et al et alii or et alia (and other)
etc. etcetera (and the rest)
GCP Good Clinical Practice
gm Gram
GMP Good Manufacturing Practice
Hb Hemoglobin
HCl Hydrogen Chloride
x
hr. Hour
ICR International Consensus Report
i.e. “idest” (that is)
IgE Immunoglobulin E
IPD In Patient Department
L Liter
LFT liver Function test
ml milliliter
m meter
n total number
NARES Non Allergic Rhinitis with Eosinophilia Syndrome
NIUM National Institute of Unani Medicine
NSFE Nasal Smear For Eosinophils
OME Otitis Media with Effusion
OPD Out Patient Department
P Probability of error
PAR Perennial Allergic Rhinitis
PND Post Nasal Drip
PNS Para Nasal Sinuses
RAST Radioallergosorbent Test
RBS Random Blood Sugar
RFT Renal Function Test
S. Serum
SAR Seasonal Allergic Rhinitis
SEM Standard Error of Mean
SES Socio Economic Status
SGOT Serum Glutamic Oxaloacetic Transaminase

xi
SGPT Serum Glutamic Pyruvate Transaminase
T Lymph. Thymus Lymphocytes
TLC Total Leukocyte Count
TSSS Total Symptoms Severity Score
U.S. United State
Viz. Videlicet (namely)
Vol. Volume
WHO World Health organization
w .r. t. with respect to
Z Zizyphus
$ Dollar
≥ Greater than or equal
≤ Lesser than or equal
& ampersand = and
< Less than
> Greater than
% Percentage
0C Degree Centigrade

Abstract
xii
Abstract
Background: Nazla Haar is a multifactorial disease represents nasal and ocular symptoms that occur as a result of the development of an inflammatory hypersensitivity reaction in the nasal mucosa, with the common result being a sensation of excess mucous, sneezing and or nasal congestion, which is quite similar to that of rhinitis of absolute allergic origin. Its worldwide prevalence varies from 2% to 20%, nearly 80 million people experience 7 or more days of nasal or ocular symptoms in each year, as one of the commonest allergic disease, it affects more than 50% of atopies in India. Mostly disease onset is seen in 12- 16 years of age or 80% before the age of 20 with symptoms relatively uncommon over the age of 50 years. Despite the use of numerous newer therapeutic regimens it has remained confront because of relapse, recurrence and resistance. The holistic approach of Unani treatment will have a thriving management in diseases with temperamental affiliation and its evidences were found throughout the history that Unani medicine has proven efficacy in Nazla Haar, but lacking scientific data for validation. Therefore, a Unani formulation was selected to conduct a clinical study to evaluate safety and efficacy in Nazla Haar.
Method: A randomized single blind placebo controlled study was conducted over 40 patients after obtaining an informed consent by allocating them in to test (n=30) and placebo (n=10) groups. Test group was given decoction of Behidana, Unnab and Sapistan with Sharbate Banafsha, whereas, placebo group received caramel syrup, both groups were received drugs in a dosage of 25 ml twice a day for 15 days. The efficacy of the study was observed subjective and objectively in three follow ups, on four point scale Total Symptom Sever ity Score, the overall response was assessed by using statistical tests like Paired, Friedman, Fisher’s Exact and Kruskal- Wallis with Dunn’s Multiple Comparison.
Results: Test drug was found to be effective with P<0.01 in comparison with placebo.
Interpretation and conclusion: The study revealed that the test drug is effective in reducing the symptoms of Nazla Haar, without any adverse effects. Therefore, it is concluded that the test drugs can be used therapeutically.
Key words: Nazla Haar; rhinitis; Unani formulation; placebo; TSSS.
xiii
LIST OF CONTENTS
S. No. Topic Page No.
1. Introduction 1-6
2. Aims & Objectives 7
3. Review of literature 8- 58
4. Materials and Methods 59- 66
5. Results and Observations 67- 93
6. Discussion 94- 106
7. Conclusion 107- 108
8. Summary 109- 114
9. Bibliography 115- 126
10. Annexure 127-138

xiv
LIST OF TABLES
S. NO Titles Page No.
1. Distribution of patients according to Age 67
2. Distribution of patients according to Sex 68
3. Distribution of patients according to Marital status 69
4. Distribution of patients according to Religion 70
5. Distribution of patients according to Dietary habit 71
6. Distribution of patients according to Socio Economic Status 72
7. Distribution of patients according to Mizaj 73
8. Distribution of patients according to Family History 74
9. Distribution of patients according to Occupation 75
10. Distribution of patients according to Duration of illness 76
11. Distribution of patients according to Treatment history 77
12. Distribution of patients according to Seasonal variation 78
13. Distribution of patients according to Effect of Allergens 79
14. Effect of drugs on Rhinorrhoea 80
15. Effect of drugs on Sneezing 81
16. Effect of drugs on Nasal Congestion 82
17. Effect of drugs on Itchy Nose 83
18. Effect of drugs on Itchy Mouth or Throat 84
19. Effect of drugs on Lacrimation 85
20. Effect of drugs on PND 86
21. Effect of drugs on Headache 87
22. Effect of drugs on NSFE 88
23. Effect of Study on Objective cum Safety Parameters 89
24. Effect of drugs on TSSS 90
25. Overall Effect on the study based on TSSS and NSFE 91
26. Overall Effect on the study in terms of Response 92
27. Baseline characteristics of the research sample 93
xv
LIST OF GRAPHS
S. NO Titles Page No.
1. Distribution of patients according to Age 67
2. Distribution of patients according to Sex 68
3. Distribution of patients according to Marital status 69
4. Distribution of patients according to Religion 70
5. Distribution of patients according to Dietary habit 71
6. Distribution of patients according to Socio Economic Status 72
7. Distribution of patients according to Mizaj 73
8. Distribution of patients according to Family History 74
9. Distribution of patients according to Occupation 75
10. Distribution of patients according to Duration of illness 76
11. Distribution of patients according to Treatment history 77
12. Distribution of patients according to Seasonal variation 78
13. Distribution of patients according to Effect of Allergens 79
14. Effect of drugs on Rhinorrhoea 80
15. Effect of drugs on Sneezing 81
16. Effect of drugs on Nasal Congestion 82
17. Effect of drugs on Itchy Nose 83
18. Effect of drugs on Itchy Mouth or Throat 84
19. Effect of drugs on Lacrimation 85
20. Effect of drugs on PND 86
21. Effect of drugs on Headache 87
22. Effect of drugs on NSFE 88
23. Effect of drugs on TSSS 90
24. Overall effect on study in terms of Response 92

INTRODUCTION

Introduction
1
INTRODUCTION
Nazla is derived from the term Nuzool which means “to descend”, literally stands for
dripping down, and the same is being used synonymously for Zukam. In fact, it is the
falling of matter from the brain and its cavities either towards throat or nose, the
earlier is termed as Nazla and the later one is Zukam, both conditions exhibit similar
pathogenesis.
The nose is the superior part of the respiratory tract; its primary function is
humidification, filtration and olfaction, with a clean and refresh nasal mucous blanket
serving to trap particulate matter. Human beings normally produce about two liters of
mucus per day from their nasal lining. Its function and / dysfunction has been an issue
of concern to physicians throughout the ages. Moreover, upper respiratory diseases
are well known since Greco-Arabic period. Ibn Abbas Al Majoosi rightly described
Nazla under the heading of the disease of nose. Usually patients with nasal disorders
may present with a variety of chief complaints such as nasal symptoms rhinorrhea,
sneezing and congestion which may be due to allergic, infectious, inflammatory, or
structural causes. When normal nasal mucosal function is lost due to inflammation, it
leads to nasal crusting or obstruction, hypersecretion or postnasal drip, coughing,
facial pressure, and fatigue.
In Nazla the predominant symptoms are rhinorrhea, sneezing, nasal congestion and
itchy nose. Based on the nature of matter involved it is of two types i.e. Haar and
Barid. Nazla Haar is a state in which the matter descends from the brain towards
throat, which is very thin, watery like in consistency and irritative in nature, resulting
in the manifestation of rhinorrhea, nasal congestion, sneezing, redness of the face,
lacrimation, burning or itchy nose, eyes, heaviness of the head and malaise.
Introduction
2
Nazla Haar is a multifactorial disease manifested by nasal and ocular symptoms that
occur as a result of the development of an inflammatory hypersensitivity reaction to
either extrinsic or intrinsic or both factors. In fact it is a type of inflammatory process
of the nose, with the common result being a sensation of excess mucous and / or nasal
congestion. This state of disease is quite similar to that of rhinitis of absolute allergic
origin, in which the patient may perceive nasal drainage (fluid dripping from the nose)
either anteriorly or posteriorly, and the symptoms may last for a short duration and
sometimes persist despite treatment.
The most common ageing symptom of the disease onset is 12- 16 years or 80% before
the age of 20, with symptoms relatively uncommon over the age of 50 years. Usually
symptoms are often paroxysmal sneezing, rhinorrhea with clear watery irritative
secretions, nasal congestion and itching in the nares and palate. The effect of rhinitis
can be as severe as conditions such as asthma and diabetes. The patient may be able to
associate his or her symptoms with a particular season, location, activity or other
triggerers that gives insight into the type of offending factor. Epidemiological studies
have consistently shown that asthma and rhinitis often coexist in the same patients.
The prevalence of asthma varies from 10% to 40% in patients with rhinitis. One study
has shown that allergic rhinitis usually precedes asthma and can be considered as risk
factor for the development of asthma. Symptoms may improve with advancing age,
but the disease is chronic in nature and complete remission is uncommon,
emphasizing the importance of considering the disorder at all stages of life.
Nazla Haar is the most common and main reason that a patient seeks the advice of a
physician at primary care. Over 20 million visits by patients per year in US alone are
devoted to this complaint. Each year nearly 80 million people experience 7 or more
Introduction
3
days of nasal or ocular symptoms as the commonest allergic disease affecting more
than 50% of atopies in India. Its worldwide prevalence rate varies from 2% to 20%.
Recently, World Health Organization has estimated that 400 million people in the
world suffer from allergic rhinitis. Incidence rates in Asia-Pacific are estimated to be
as high as 48% and rising as societies become more urbanized and adopt western
lifestyles.
The prevalence of the disease as a result of respiratory allergy is constantly increasing
and is recognized as a major public health burden that causes major illness and
disability worldwide. Its disabling effect is found on all individuals irrespective of age
and ethnic background. Approximately 20 billion dollars are spent globally each year
in relation to its costs for medications, lost productivity and physician consultations,
under diagnosis, lack of treatment and non compliance are added in the economic
burden is significant and even heavier in societies with emerging incomes. High
consumption of health resources was observed in the ‘Allergies in Asia-Pacific’
survey, which revealed that children visited a physician on an average four times in a
year. When the cost of treating comorbidities such asthma is considered, the annual
per patient direct costs in Asian countries can be as high as $ 1,010 U.S. dollars per
person.
Though the disease is not a life threatening, but its impact as risk factors include a
combination of environmental and genetic interactions reflects the involvement of
nasal, ocular and constitutional symptoms with a variety of comorbid conditions,
including asthma, chronic sinusitis, nasal polyposis, secretory otitis media, and sleep
disorders which lead to open mouth breathing, sore throat and snoring. In addition to
daytime fatigue and somnolence, nocturnal sleep impairment is also associated with
Introduction
4
depression, irritability, memory defects, inability to concentrate and listless, decrease
alertness and overall reduced quality of life.
There is no standard set of criterion for the diagnosis of rhinitis based on nasal
symptoms alone. In most studies, the criteria for diagnosis are based on the subject’s
reporting or as a complex genetic disorder, in certain cases, patients give a positive
family history otherwise diagnosis is primarily based on the clinical symptoms and
exposure history. Physical examination reveals the changes in the nasal mucosa; in
children a transverse nasal crease, a high arched palate, mouth breathing and dental
malocclusion are often observed. Nasal smears (Hansel stains) of nasal secretions are
often required, which typically reveal eosinophils. The diagnosis is confirmed by
demonstration of specific IgE antibodies reactive to the relevant pollen through either
positive allergy skin tests or IgE immunoassays. Identification of specific triggering
allergens is essential for recommending appropriate environmental controls specific to
the causative allergen.
Medical management as offered by alternative or primary choice of treatment by the
people consists of the use of systemic antihistamines (Cetrizine HCl, Loratadine,
Diphenhydramine HCl, and Promethazine HCl etc.), decongestants (Ephedrine,
Phenylephrine, Oxymethazoline) and topical corticosteroids (Glucocorticosteroids,
Hydrocortisone) do not get cure for all patients, often necessitating immunotherapy
too. Due to the side effects associated with these drugs such as local nasal irritation
and burning, crusting, epistaxis, nasal septal perforation, pharyngeal candidiasis; and
high recurrence rates with limited success; moreover, first generation antihistamines
cross the blood brain barrier and have significant sedative and anticholinergic effects
that will interfere the activities of school, work, driving, or use of machinery,

Introduction
5
whereas, 10-15% of treated patients complained of sedation, virtually all subjects
demonstrate decreased motor skills, diminished driving ability and reduced cognition.
Despite the use of numerous newer therapeutic regimens, rhinitis has remained as
enigma because of relapse, recurrence and resistance. There is a dire need to develop
a safe and efficacious therapy from the treasures of Unani system of medicine which
offers a variety of effective and safe treatment modes for such disease. Because,
Unani system of medicine considered Nazla Haar is a disease with multiple
etiologies, accordingly it was treated with holistic approach by adopting the principles
of contrary to the disease state. In this context some common single drugs used such
as Banfsha, Behidana, Unnab, Sapistan, Asalussoos, Aalubukhara sheerin,
Turanjabeen, Tukhme khitmi muqashar, Kishneez khushk, Barg wa gule aazad, Gulab
sufaid, Anjeer siya, Maghze khiyar shamber, Sheere tukhme kahu muqashar, Sheere
maghze kaddu, and Maghze badam. Similarly certain compound drugs used are
Sharbate banfsha, Laooqe khashkhash, Luabe behidana, Sharbate unnab, Khameere
gauzaban, Triyaqe nazla and Sharbate fardyaris etc.
Based on the range of prescriptions comprises on single and compound formulations
mentioned by the Unani physicians for the management of Nazla Haar, a formulation
from Byaze Kabir is selected which consists of Behidana, Unnab and Sapistan in the
form of Joshanda along with Sharbate Banafsha may prove to be effective in the
management of Nazla Haar.
Therefore, the present study entitled “Efficacy of a Unani formulation in Nazla
Haar” was conducted at National Institute of Unani Medicine Hospital, Bangalore
over a period of 09 months from March 2011 to December 2011. A total of 55
patients were registered for screening out of which 15 patients did not fulfill the
Introduction
6
inclusion criteria, therefore, excluded, and remaining 40 patients were randomly
allocated to two groups viz, 30 in test and 10 in placebo. Test group was given
decoction of a Unani formulation along with Sharbate Banafsha 25ml orally twice a
day for 15 days and the placebo control group was treated by caramel syrup with the
same quantity and duration. The efficacy of the study was observed in both groups in
three follow ups i.e., 4th, 8th and 15th day, based on the severity of disease and the
effect of t he treatment on TSSS (Total Symptom Severity Score) a four point
arbitrary grading scale (0- absent; 1- mild; 2- moderate; 3- severe).
The pre and post treatment data from both groups were compared, test group has
shown very significant reduction (p<0.01) in the severity of subjective parameters like
rhinorrhoea, sneezing, nasal congestion, itchy nose, mouth or throat, lacrimation, post
nasal drip and headache, while placebo control group remained insignificant. The
objective parameters especially, NSFE was observed and analyzed in both groups the
test group after treatment effects exhibited highly significant (p<0.001) in
comparison of baseline before treatment, whereas, placebo control group has shown
no significant changes.
Moreover, this study has shown no clinically significant adverse effects, and overall
compliance to the treatment was commendable. On the basis of results and
observations, it can be concluded that the test drug is effective and safe as a treatment
for Nazla Haar.

OBJECTIVES

Objectives
7
OBJECTIVES OF THE STUDY
To evaluate safety and efficacy of a Unani formulation in Nazla Haar.
To validate the Unani concept of Nazla Haar with Rhinitis.
REVIEW
OF
LITERATURE

Review of Literature
8
HISTORICAL BACK GROUND OF NAZLA HAAR
‘Nazla Haar’ has been described as a disease in detail with signs and symptoms along
with treatment in various Unani texts under the chapter of ‘Nazla wa Zukam’.
According to Unani physicians, Nazla is a condition with watery irritating nasal
discharge dripping down towards the throat, if the same flow towards the nose, then it
is termed as Zukam.1
Nazla wa Zukam as disease with complex aetiology and difference of opinion in its
types was found throughout the period of ancient and medieval Unani practitioners,
but the predominant symptoms of Nazla resembling at par with the existing medical
condition rhinitis.
Probably, Hippocrates (460- 377 BC) was the first person who defined Nazla wa
Zukam along with its etiology, types and management.2
Galen (131-201 AD) defined different types of Nazla specifically Nazla Haar and its
complications with treatment.2
Rabban al Tabri (810- 895 AD) mentioned in detail about the types, causes and
treatment of Zukam besides considering Nazla as synonym.3
Mohamed Bin Zakaria al Razi (850-923 AD) described the aetiopathogenesis and
management of Nazla Haar.2
Hakeem Abul Mansoorul Hassan al Quamri (9th century AD) described Nazla as a
state in which fazil rutubate dimaghiya discharges from the ventricles of the brain
dribbled towards the palate, whereas, Zukam as a state where the same secretion
discharges through nostrils. He has also explained the differences between Nazla wa

Review of Literature
9
Zukam, as litting down of the fazil rutubate dimaghiya towards lungs and thoracic
region is Nazla. Furthermore, he classified Nazla wa Zukam into two types as Haar
and Barid.2
Ibn Abbas al Majoosi (930-999AD) has described in detail about the Nazla wa
Zukam as diseases under the heading of disease of nose, he has added that both
Warme Haar and Barid can affect the mucous membrane of the nose. 4
Ibn Sina (980-1037 A.D) in “Al Qanoon Fit Tibb” an encyclopedia of medicine,
served as a standard text book of medicine in Europe till 17th century A.D. described
extensively the etiopathogenesis, types, clinical presentation and treatment of Nazla
wa Zukam including Nazla Haar.5
Abul Hassan Ahmed Bin Mohd Tabri (10th century AD) applied the term Zukam to
all forms of Nazla wa Zukam.6
Ibn Zohar (11th century AD) an author of “Kitabul Taisir’ has quoted the term Nazla
and its treatment.7
Ibn Rushd (12th century AD) stated that Nazla is a condition in which rutubat falls
from the head and that can cause cough with bronchospasm.8
Abu al Hassan Ahmad Bin Jurjani (12th century AD) mentioned Nazla as a
condition where there is watery irritating nasal discharge (mad’dae raqeeqa) dripping
down towards the throat, if the same mad’da flows towards the nose with sense of
burning (sozish) is considered as Zukam.1
Allama Nafees Bin Auz Kirmani (15th century) associated certain terms with Nazla
wa Zukam, such as Coryza and Catarrh, where Nazla means ‘to descend’, Coryza for
‘nasal congestion’ and Catarrh for ‘running nose’.9

Review of Literature
10
Hakeem Mohd Akbar Arzani (17th century AD) explained the difference between
Nazla and Zukam similar to that of above mentioned Atibba.10
Azam Khan (1813 AD) and Allama Hakeem Mohd Kabeeruddin (1889- 1977 AD)
have considered Nazla wa Zukam as a common term, and described as the infiltration
of wastes from the brain, and origin of the causative substance (mad’da) is same in
both the conditions i.e. falling of mad’da from the brain.19, 11
The symptoms of Nazla Haar resembles with the symptoms of rhinitis, which occurs
mostly due to allergy. Allergic diseases such as asthma, urticaria and eczema
including rhinitis have been known for centuries, and their history dates back to
antiquity.13
In the modern medical literature nasal allergies were known as hay fever, and today
hay fever is the common name for allergic rhinitis, 14 especially for seasonal allergic
rhinitis.13, 15, 16
Seasonal allergic rhinitis was first described in the United States in 1872 (autumnal
catarrh or ragweed hay fever) and in England in 1873 (catarrhus aestivus). The
disease was well recognized in England and Germany by 1900 and in the United
States by 1920.17
Rhinitis is the inflammation of the nasal mucosa, usually due to allergic origin. The
term ‘allergy’ first appeared in the medical literature in 1906.13
In 1911, Sir Henry Dale identified the role of histamine in an allergic reaction, 13 and
the first paper on immunotherapy against pollen “toxin” was published in the same
period. At that time, hay fever was considered to be a disease of the affluent and was
rarely reported among working class people, especially farmers.17
Review of Literature
11
In 1929, the definition of allergic rhinitis was formulated by Hansel.18
In 1930s, allergic rhinitis became sufficiently common to allow the development of
the subspecialty of allergy.17
In 1935, the University of Virginia appointed a professor of Allergy as an established
area of concern in medicine.17
Review of Literature
12
DEFINITIONS
Nazla Haar is a condition with watery irritating nasal discharge dripping down
towards throat, 1 with sense of burning (sozish) in nose, face and eyes with
lacrimation, and also alters the sense of olfaction.5
Rhinitis is generally defined as an inflammatory process in the nose, which commonly
results being a sensation of excess mucous or nasal congestion. The patient may have
a sensation of fluid dripping from the nose, either coming from the nose anteriorly or
posteriorly.1, 10, 12, 19, 20, 21, 22, 24
Allergic rhinitis is an immunologic response of nasal mucosa to air born allergens18
and is characterized by watery nasal discharge, nasal obstruction, sneezing and itching
in the nose. This may also be associated with symptoms of itching in the eyes, palate
and pharynx.25
The International Consensus Report (ICR) defined rhinitis as, a patient with one or
more of the classical symptoms of nasal obstruction, rhinorrhea, sneezing, or itchy
nose. Further, its algorithm stated that the definition of rhinitis must include at least
any two of the nasal symptoms on most days.26
Review of Literature
13
ANATOMY AND PHYSIOLOGY OF NOSE
The nose is the superior part of the respiratory tract and contains the peripheral organ
of smell.27
The nose is divided into two as external nose and nasal cavity.28
The external nose has a skeletal framework particularly partly bony and partly
cartilaginous.
The nasal cavity extends from the external nares or nostrils to the posterior nasal
apertures, and is subdivided into right and left halves by the nasal septum. Each half
has a roof, a floor, and medial and lateral walls.28
The nasal mucosa lines the entire nasal cavities except for the vestibule of the nose. It
is firmly bound to the periosteum and perichondrium of the supporting structures of
the nose. The inferior 2/3 of the nasal mucosa is the respiratory
mucosa (Schneiderian membrane) 30 and air passing over this is warmed and
moistened before it passes into the lungs. The superior 1/3 is the olfactory mucosa.27
The total surface area available in the nasal mucosa is estimated to be about 180 cm2,
of which 10 cm2 is olfactory mucosa and 170 cm2 is the richly vascularized
respiratory mucosa.29
Nasal mucosa and respiratory epithelium:
The lining of the anterior part of the nasal cavity and vestibule is continuous with the
skin, and consists of keratinized stratified squamous epithelium overlying a
connective tissue lamina propria. Posteriorly, at the limen nasi, the mucosa lined at
first by nonkeratinizing stratified squamous epithelium, then by pseudostratified
ciliated (respiratory) epithelium with numerous goblet cells. Respiratory epithelium
Review of Literature
14
forms most of the surface of the nasal cavity, and so covers the conchae, meatuses,
floor and roof, except where the olfactory epithelium is present.31
The nasal mucosa has numerous underlying seromucous glands within its lamina
propria, which makes the surface sticky so that particles in the inspired air are
deposited on the surface. It is adherent to the periosteum or perichondrium of the
neighbouring skeletal structures. The mucosa is continuous with the nasopharyngeal
mucosa through the posterior nasal apertures, the conjunctiva through the naso-
lacrimal duct and the lacrimal canaliculi, and the mucosae of the sphenoidal,
ethmoidal, frontal and maxillary sinuses through their opening into the meatuses.31
Here mucous membrane shows variable thickness being thickest over nasal conchae
especially at their ends, quite thick over the nasal septum but very thin in the meatuses
and floor of the nose.25
Nerve supply:
Respiratory nasal mucosa is supplied chiefly by the trigeminal nerve.
The mucous membrane of the nasal septum is supplied chiefly by the nasopalatine
nerve, a branch of the maxillary nerve.
Anterior portion of the septum is supplied by the anterior ethmoidal nerve (a branch
of the nasociliary nerve) which is derived from the ophthalmic nerve.
The lateral walls of the nasal cavity are supplied by branches of the maxillary nerve;
the greater palatine nerve, and the anterior ethmoidal nerve.27

Review of Literature
15
Olfactory epithelium:
The peripheral receptors for olfactory sensation are located bilaterally in areas of
sensory epithelium lining the posterodorsal parts of the nasal cavities. This covering
the posterior upper parts of the lateral nasal wall, including the back of the superior
concha, the sphenoethmoidal recess, the upper part of the perpendicular plate the
ethmoid and the roof of the nose arching between the septum and lateral wall,
including the underside of the cribriform plate. The olfactory epithelium is
considerably thicker than the respiratory epithelium.31
Arteries of the Nasal Mucosa
Mucosa of the nasal septum is derived from the maxillary artery (mainly) and greater
palatine artery.
Nasal mucosa supplied by the sphenopalatine artery which is a branch of the
maxillary artery, anterosuperior part of the mucosa of the lateral wall of the nasal
cavity and nasal septum supplied by anterior and posterior ethmoidal arteries,
branches of the ophthalmic artery.
Veins of the Nasal Mucosa
The veins of the nasal mucosa form a venous network of plexus in the connective
tissue of the nasal mucosa. Some of the veins open into the sphenopalatine vein and
drain to the pterygoid plexus. Others join the facial and infraorbital veins. Some
empty into the ophthalmic veins and drain into the cavernous sinus.31

Review of Literature
16
LITERATURE REVIEW
Nazla wa Zukam were used synonymously by most of the Unani physicians, but some
of them have difference of opinion, however, in both ailments, the mad’da drips from
the brain.1, 2, 5 The mawad of Nazla is sometimes temperamentally hot and thin in
consistency, or cold and viscous.1
Ibn Sina in “Al Qanoon Fit Tibb”, considered Nazla wa Zukam as two separate
disease entities. Nazla Haar is one of the types of Nazla, accordingly described
extensively about its etiopathogenesis, clinical presentation and treatment. 2, 5, 7, 19, 20
According to him both Nazla wa Zukam exhibit the complex state, i.e. falling of
mad’da from the brain.1, 5
Nazla wa Zukam have been considered as a common term to describe the ‘infiltration
of dimaghi fuzlat’ in the most of Unani texts, because in both conditions the mad’da
comes from the dimagh and move towards either nose or throat.5, 12, 19
Differentiating Nazla and Zukam by Buqrat, he defined Zukam is Nazla of nasal
mucosal lining, and the Nazla is a condition in which the nasal mucosa gets inflamed
and always associated with excessive nasal discharge.4, 32
According to Galen there are different types of Nazla, he has specifically defined
Nazla Haar and its complications with treatment. Further, he has clearly mentioned
the importance of hammam in Nazla Haar before the administration of munzij drugs.2
Mohamed Bin Zakaria al Razi has suggested and recommended treatment for various
types and origin of Nazla.2
According to Hakeem Abul Mansoorul Hassan al Quamri Nazla is a condition in
which fazil rutubate dimaghiya discharges from the ventricles of the brain towards the
Review of Literature
17
palate, whereas, in Zukam the same secretion dribbled towards the nostrils. He also
explained the marginal differences between Nazla wa Zukam; 5 as litting down of the
fazil rutubate dimaghiya towards lung and thoracic region as Nazla.11, 12 Furthermore,
he classified Nazla wa Zukam into two types as Haar and Barid.2, 5
According to Abul Hassan Ahmed Bin Mohd Tabri, the term Zukam as it is applicable
to all its types. According to him it is an accumulation (ihteqaq) of vapours
(bukharat) in the ventricles of the brain that started dissolving from the cavities of the
head. It supposes that the stagnant matter comes out after dissolutions of it in the form
of liquid, water or vapour through the nostrils, eyes and ears.6
Ibn Rushd has considered the Nazla is one of the causes for cough with
bronchospasm.8 According to Ahmad Hassan Jurjani Nazla is a condition where there
is watery irritating (mad’dae raqeeqa) nasal discharge dripping down towards the
throat, if the same mad’da flows towards the nose with sense of burning (sozish) is
considered as Zukam. Further, he has explained the quality and quantity of the
mawade Nazla, which involve in Nazla Haar.1, 10, 12, 19
Allama Nafees Bin Auz Kirmani has described literal meanings and definitions of the
terms; Zukam, Coryza and Catarrh. Nazla means to descend, Coryza for nasal
congestion and catarrh for running nose, all these conditions are manifested as a
results of inflammation of the nasal mucous membrane.9
According to Abul Hassan Ali Ibn Hubal Baghdadi, Nazla is a condition in which
falling of concentrated (teiz) substance from the dhimagh towards the throat and
chest.20

Review of Literature
18
It is well understood that the predominant symptoms of Nazla Haar (rhinitis) are
watery nasal discharge, irritative, nasal block (congestion), redness of the eyes,
cheeks and face, burning sensation of nose, lacrimation, postnasal drip and headache.
This state of disease is quite similar to that of rhinitis of absolute allergic origin. It is
also considered as a systemic illness may be associated with constitutional symptoms
such as fatigue, malaise and headache, 33 as well as it refers to the nasal and ocular
symptoms that occur as a result of an inflammatory hypersensitivity reaction to
aeroallergens deposited on the nasal mucosa and conjunctiva.24

Review of Literature
19
EPIDEMIOLOGY
Respiratory allergy (allergic rhinitis and asthma) is a high prevalence disease that
affects an average of 10-15% of the general population. Thus, allergic asthma and
rhinitis are probably the most common immune mediated disorders. The prevalence of
respiratory allergy, especially rhinitis is constantly increasing.34
Nazla Haar (rhinitis) is the most common and main reason that a patient seeks the
advice of a physician at primary care. Over 20 million visits by patients per year in
US alone are devoted to this complaint. Each year nearly 80 million people
experience 7 or more days of nasal or ocular symptoms as 24 the commonest allergic
disease affecting more than 50% of atopies in India.35 Its worldwide prevalence rate
varies from 2% to 20% and the maximum prevalence is observed in the second
decade of life.36 Recently, World Health Organization has estimated that 400 million
people in the world suffer from allergic rhinitis, which is a risk factor for asthma, and
is associated with other allergic diseases such as atopic dermatitis, conjunctivitis,
sinusitis, and nasal polyposis, which requires concomitant treatment 37. Incidence rates
in Asia-Pacific are estimated to be as high as 48% and rising as societies become
more urbanized and adopt western lifestyles.38
The prevalence of the disease as a result of respiratory allergy is constantly
increasing and is recognized as a major public health burden39 that causes major
illness and disability worldwide.41 Its disabling effect is found on all individuals
irrespective of age and ethnic background. Approximately 20 billion dollars are spent
globally each year in relation to its costs for medications, lost productivity and
physician consultations, under diagnosis, lack of treatment and non compliance are
added in the economic burden is significant and even heavier in societies with

Review of Literature
20
emerging incomes. High consumption of health resources was observed in the
‘Allergies in Asia-Pacific’ survey, which revealed that children visited a physician on
an average four times in a year. When the cost of treating comorbidities such as
asthma is considered the annual per patient direct costs in Asian countries can be as
high as $ 1,010 U.S. dollars per person.38
Epidemiological studies have consistently shown that asthma and rhinitis often
coexist in the same patients. The prevalence of asthma is less than 2% in subjects
without rhinitis while it varies from 10% to 40% in patients with rhinitis. 41 At the
same time one study has shown that allergic rhinitis usually precedes asthma and can
be considered as risk factor for the development of asthma 18, 41 Nazla Haar exists in
up to 80% of asthma patients and frequently exacerbates asthma and increases the risk
of asthma attacks.18 Chronic rhinitis occurring episodically or continuously is often as
a result of allergic hypersensitivity, though other causes may underlie this
syndrome.42
According to Allergies in Asia-Pacific survey, allergic rhinitis is one of the most
prevalent chronic diseases in children. A recent study has predicted that by the year
2020 as many as one out of two people up to 14 years of age may be affected. With
this projected prevalence, allergic rhinitis is becoming the most common chronic
disease in the pediatric population.38.
Review of Literature
21
AETIOLOGY
According to the doctrine of Unani medicine, any state that hampers the equilibrium
of humours (Akhlat) either qualitatively or quantitatively may cause disease.
Nazla Haar is a multi factorial disease 18 occurs as a result of the involvement of
various factors which affects the individual either intrinsically or extrinsically and
sometimes both.
Some of the aetilogies defined by various Unani practitioners are as:
1. According to Ibn Sina
Usually individuals with hot temperament (intrinsic factors) may likely to
develop Nazla Haar. 19
2. According to Samarqand
There are 8 causes for Nazla, viz, four are of Sue mizaj dimagh and other four
are Akhlate arba. 19
3. Extrinsic factors (Asbabe kharija)
Khariji hararat: hararat mizaj, hararate mizaj khaas, uncovered head,
exposure to sunlight, fire, garam hammam, working in hot environment,
applying pungent odour perfumes or smelling/ snuffing of hot drugs such as
mushk, jundbedastar, zafran, onion etc. massaging the head with hot oils or
usage of warm hair oils, sleeping immediately after food, consumption of hot
things like garlic, onion, mustard etc. , bathing after exercise followed by
improper wrapping, or strenuous psychic or physical activity; and also
exposure to allergen like pollen, cotton fur, feather, dust. 1, 3, 5, 6, 12, 19, 20, 21
4. Intrinsic factors (Asbabe dakhila): hammam, riyazat1, 3, 5, 6, 12, 19, 21
Review of Literature
22
5. Mostly both intrinsic and extrinsic factors together will produce Nazla wa
Zukam 1, 19
6. Sue mizaj haar 19
7. Sue mizaj of brain 20
8. Zoafe dimagh 21
9. Imtilae aam wa raas (plethora of body and head) 12, 19
10. Tukhma 19
11. Infealate nafsania 19, 21
12. Seasonal variation 21, 43
13. Predisposing factors: 42, 43
I. Age:
It occurs at all ages, 43 but the maximum prevalence is observed in the
second decade of life. 36
II. Heredity/ genetic predisposition play an important part:
If both parents are allergic, there is a high incidence of the disease
occurring in children. 25 But, one study results show that an adult with a
family history of asthma or rhinitis has a risk of three to four fold for
developing asthma and of two to six folds for developing rhinitis over
adults without a family history. 44
III. Hormonal:
Since the disease often begins at puberty. 43
IV. Occupational triggers 15

Review of Literature
23
PATHOPHYSIOLOGY
Allergic airway disease is characterized by local tissue damage and organ dysfunction
arising from an abnormal hypersensivity of nasal mucosa response to normally
harmless and ubiquitous environmental allergens.42
Generally, human beings normally produce about 2 L of mucus per day from their
nasal lining. The primary function of the nose is humidification, filtration and also an
olfaction, with a clean and refresh nasal mucous blanket serving to trap particulate
matter. The nasal and sinus lining consists of a ciliated respiratory epithelium; the
cilia function in a highly organized and orderly fashion under normal circumstances to
transport particulate matter trapped in the mucous blanket in a consistent fashion to
allow the mucus to be swallowed, thereby avoiding deposition. The parasympathetic
nervous system controls both vascular tone and mucus production in the nose.
Inflammatory conditions, such as common cold can cause the nasal and sinus lining to
swell. In a normal state, one side of the nose is relatively decongested and the other
side is relatively congested owing to vascular engorgement. This vascular dilatation
allows humidification and warming of inspired air and can also affect the ability to
discern odors in the process of olfaction.24
According to Unani system of medicine the genesis of Nazla is related with extrinsic
and intrinsic causative factors. One or the other of these causative factors causes sue
mizaj in the mucous membrane of the nose. Thus the mucous membrane gets inflamed
and produces secretions, which may be watery (raqeeq) or viscid (ghaleez), hot
(garam) and irritative (lazae) or cold (barid) and benign, distasteful or tasteless
depends upon the causative factors.45

Review of Literature
24
Usually it is believed that the effects of heat either externally or internally will causes
increase warmness in brain that leads to temperamental disturbance within the brain,
therefore, to bring back the normal temperament of the brain, the tabiat try to
neutralize the increased warmness of the brain by absorbing fluid from the body
towards the brain. As a result, an excessive amount of fluid accumulated inside the
brain and its cavities, which properly may not be able to metabolized as a
consequence of this, some amount of fluid still remain inside causing derangement of
the local temperament (sue mizaj dimagh) of the brain. Therefore, the brain tries to
expel the fluid which accumulated in the form of fuzlat by either through nostrils or
throat.
Based on the causes and quality of fluid which expels from the brain, it appears to be
an irritant, watery, salty, thin and viscid etc that may cause local tissue inflammation
of the nasal mucosa leading to dysfunction of nose, in modern sense it is considered
as immune response. The inflammatory response mediated by the immunological
factors generally bound to mast cells and basophils triggers the release of vasoactive,
enzymatic, and chemotactic mediators. 42 As a result, this reaction produces
degranulation of the mast cells with release of several chemical mediators, some of
which already exist in preformed state, while others are synthesized afresh. These
mediators are responsible for symptomatology of allergic disease. Depending on the
tissue involved, there may be vasodilation, mucosal oedema, and infiltration with
eosinophils, excessive secretion from nasal glands or smooth muscle contraction.25
This reaction is typically completed in 2 phases, an early phase and a late phase.46
The early phase occurs within minutes after an allergen exposure and is characterized
by sneezing, pruritus, rhinorrhoea and nasal congestion resulting largely from the

Review of Literature
25
interaction of histamine with target tissues of the upper airway by activation of tissue
mast cells sensitized by IgE antibodies. 46 Approximately half of all patients with
rhinitis experience the late phase response, which begins 2-4hours following initial
antigen exposure, reach maximal activity at 6-12 hours, and usually resolve within 12-
24 hours. This phase is typically characterized by congestion about 4 to 12 hours after
exposure that corresponds with the recruitment of many inflammatory cells.25, 46

Review of Literature
26
CLASSIFICATION OF NAZLA
Primarily two types of Nazla have been defined throughout the Unani literature based
on the involvement of temperament and matter. 2, 5, 19, 20, 22, 47
1. Nazla haar
2. Nazla barid
Apart from the above, some other types of Nazla are:
3. Aetiological types
3.1. Based on mad’da 22, 47
a. Nazla damavi
b. Nazla safravi
c. Nazla balghami
d. Nazla sawdavi
3.2. Based on factors 6
a. Nazla due to Asbabe kharija (extrinsic factors)
b. Nazla due to Asbabe dakhila (intrinsic factors)
4. Based on duration of illness
a. Nazla haad 5, 22 or acute rhinitis 16, , 25
b. Nazla muzmin 22 or chronic rhinitis 16, , 25

Review of Literature
27
5. WHO based ARIA classification 15, 39, 49
WHO’s former classification of rhinitis was:
i. Seasonal allergic rhinitis (SAR):
Symptoms appear in or around a particular season when the pollens of
particular plant, to which the patient is sensitive, are present in the
air.25
ii. Perennial allergic rhinitis (PAR):
Symptoms are present throughout the year.25
Later, this classification has been revised and adopted by the ARIA system, which is
based on the duration of symptoms and the severity of the disease.
5.1. Based on duration of symptoms
a) Intermittent rhinitis:
Symptoms that present four or less days per week or not more than
four consecutive weeks per year.
b) Persistence rhinitis:
Symptoms last for more than four days per week and for more than
four consecutive weeks per year.
5.2. Based on the severity
a) Mild
b) Moderate
c) Severe
6. Traditional classification 25, 33, 40
a. Allergic rhinitis
b. Nonallergic rhinitis
Review of Literature
28
CLINICAL FEATURES
Clinical features may vary from individual to individual in terms of severity,
frequency, duration and the nature of aetilogies involved. According to WHO, Nazla
Haar (Rhinitis) must include at least two of the nasal symptoms on most days.26 The
patient may be able to associate his or her symptoms with a particular season,
location, activity, or other trigger that gives insight into the type of offending factor.39
1. Nasal discharge (rhinorrhoea) 2, 5,10, 16, 19, 21, 24, 25, 26, 33, 36, 42, 43, 49, 50, 51, 52, 53
2. Paroxysmal sneezing 16, 21, 24, 26, 33, 36, 37, 42, 43, 49, 50, 51, 52, 53
3. Nasal congestion: 5, 16, 20, 21, 24, 25, 26, 33, 37, 42, 43, 49, 50, 51, 52, 53
4. Redness of face and eyes 1, 5, 19, 20, 21, 47
5. Hyper sensitivity 2
6. Burning, 2, 10, 16 irritation, 16, 43 and itching in the nose, eye and throat 1, 19, 20,
21, 24, 26, 33, 36, 37, 42, 43, 49, 50, 52
7. Lacrimation6, 24, 25, 33, 50
8. Post nasal drip (PND) 24, 25, 37
9. Mild headache 1, 6, 21, 25, 33, 43
10. Hot to touch (malmas) 5, 19
11. Hoarseness of voice 5
12. Excess thirsty 6, 21
13. Fatigue 4, 16, 24, 37, 43, 49
14. Lethargy 4
15. Nabz – Azeem, Saree’, wa Mutawatar 19, 47
16. Qarura- Yellowish 19, 47

Review of Literature
29
DIAGNOSIS
There is no standard set of criterion for the diagnosis of Nazla Haar based on nasal
symptoms alone.26, 41 In most of the studies, the criteria for diagnosis are based on the
subject’s reporting. 41 A detail history and physical examination is helpful, and also
gives clues to the possible factors. Nazla Haar is primarily a clinical diagnosis based
on symptoms and exposure history.24
DIFFERENTIAL DIAGNOSIS
The symptoms and signs of Nazla Haar frequently overlap with those of other forms
of Nazla wa Zukam and various anatomic abnormalities of the upper airway such as:
1. Nazla barid:
It occurs mainly due to excess Balgham, which is characterized by thick and
whitish nasal discharge (ghaleez, lesdaar mad’da) mild itching and irritation
in the nose, unilateral or bilateral nasal congestion 20 with facial pain. 21, 22
Also there is nasal speech, heaviness of forehead and nose, impaired sense of
smell and breathing difficulty.1, 5, 19, 20
2. Zukam:
It occurs due Infiltration of fuzlate dhimagh, which usually ghaleez and khaam
(thick and immature substance) 20 from the anterior part of the brain towards
the nose. The causative factors may be sue mizaj haar or barid, 4 and sudda
(obstruction).3 There is weakness or laziness, heaviness in the forehead, mild
headache, nasal congestion with dryness, sneezing, and irritating nasal
discharge on and off, 21 reddish nostrils with pain, lacrimation due to
inflammation (mutawarram), 54 nasal speech and impaired sense of smell.4

Review of Literature
30
3. Nonallergic rhinitis syndrome:
A. Vasomotor rhinitis:
It can be the primary cause of nasal congestion, rhinorrhea, 36or less
commonly, sneezing paroxysms 55 and pruritus.33 About one- fifth of patients
who seek medical attention at an allergy or immunology subspecialty clinic
complaining of chronic rhinitis will actually have non-allergic, vasomotor
rhinitis; one-third of patients in whom allergic rhinitis is diagnosed will have a
vasomotor component to the disease. Nonspecific nasal hyperreactivity leads
to symptoms triggered by cold temperature, inhaled irritants, strong odors,
spicy food, and other nonallergic environmental stimuli.55
B. Nonallergic rhinitis without eosinophilia:
It is characterized by perennial nasal symptoms of rhinorrhea and/or
congestion that are unrelated to allergen exposure. Nasal symptoms are often
provoked by sudden changes in the environment, airborne irritants or dietary
factors.56
C. Nonallergic rhinitis with eosinophilia syndrome (NARES):
It is characterized by perennial nasal symptoms (particularly nasal congestion)
with nasal and occasionally blood eosinophilia in the absence of documentable
allergen sensitivity.33, 56
D. Hormonal rhinitis:
It is most often characterized by nasal congestion and is usually secondary to
thyroid disease (hyperthyroid or hyperthyroid), pregnancy or oral
contraceptive use.24, 33, 56

Review of Literature
31
E. Drug induced rhinitis:
It is usually present with symptoms of chronic nasal congestion and occurs
following the use of both oral and topical medications. Responsible oral
medications include many antihypertensives (most common of which are bête-
blockers and methyldopa), and non steroidal anti-inflammatories. Use of
topical vasoconstrictors (e.g. oxymetazoline, phenylephrine) for longer than 3
days may result in a state of rebound nasal congestion termed ‘rhinitis
medicamentosa’. Repeated use of intra nasal cocaine and methamphetamines
may also cause rebound congestion and occasionally septal erosion and
perforation.33, 56
F. Food-related rhinitis:
It may occur because of IgE mediated reactions or vagally mediated
mechanism
(gustatory rhinitis).56
4. Infectious rhinosinusitis
a. Acute viral upper respiratory infection:
It presents with symptoms of rhinorrhea, congestion, sneezing, and
constitutional symptoms (fever, myalgia, malaise). Usually, no pruritus and
symptoms resolve within 7 to 10 days.56
b. Acute Bacterial rhinosinusitis:
It most often presents with symptoms of purulent anterior rhinorrhea or post
nasal drip, facial pain or pressure, and persistence or worsening of nasal
congestion. Chronic bacterial sinusitis usually presents with chronic (longer

Review of Literature
32
than 8 weeks) symptoms. However, no single symptom or sign is reliable for
distinguishing rhinitis from sinusitis.56
5. Anatomic abnormalities usually present with obstructive symptoms without other
symptoms of rhinitis, such as sneezing, rhinorrhea, or itching.56
a. Septal deviation:
It can be visualized with an otoscope. It is most often asymptomatic; severe
deviation may cause symptoms of unilateral congestion.
b. Adenoidal hypertrophy:
It is typically seen in young children, causes bilateral nasal obstruction, and is
often associated with nocturnal mouth breathing and snoring.
c. Nasal polyps:
These are benign, inflammatory growths that may result in unilateral or
bilateral nasal obstruction, rhinorrhoea, hyposmia and chronic sinusitis.24, 55, 56
d. Intranasal foreign bodies:
Usually occur in young children, often consists of a small plastic toy part.
Foreign bodies usually cause unilateral nasal obstruction with or without
rhinorrhoea.56
6. Systemic diseases involving the upper airway: 56
a. Wegener granulomatosis:
This is a systemic condition which affects the nose, upper respiratory tract,
lungs and kidneys. Rhinorrhoea starts with clear nasal discharge, which
becomes blood stained and purulent.43
Review of Literature
33
b. Sjogren syndrome:
It is an autoimmune disease that destroys exocrine glands and impairs mucous
gland function. Occasionally, the nose may be prominently involved, with
symptoms of congestion, dryness and crusting.43
c. Sarcoidosis:
This is a granulomatous systemic disease with nasal obstruction, purulent and
blood stained nasal discharge.43
Review of Literature
34
INVESTIGATIONS
The diagnostic tests for Nazla Haar are:
Complete blood picture with Haemogram
Total IgE levels
Nasal smear for eosinophils (NSFE) or Nasal cytology
Skin prick testing
Intradermal testing
Nasal provocation test
Radioallergosorbent test (RAST).35, 39, 57
Procedure of Nasal smears for eosinophils:
Sample of nasal secretion was obtained from either by blowing of the nose or by
gentle scraping of the lateral wall of the nasal cavity. The material was smeared on
glass slides, flooded them by diluted Giemsa stain (1ml Giemsa stain was diluted by 9
ml of distilled water), and kept them for dry. Then, the stained slides were observed
under the electronic microscopy in different powers for eosinophils.
Review of Literature
35
COMPLICATIONS ASSOCIATED WITH NAZLA HAAR
When Nazla Haar is untreated or inadequately treated, symptoms may become
chronic and contribute to conditions such as:
Bronchial Asthma (Ribu wa dama) Nazla Haar usually precedes asthma and
considered as a risk factor for the development of asthma. Nazla Haar exists in up to
80% of asthma patients and frequently exacerbates asthma and increases the risk of
asthma attacks.2, 15, 18, 20, 23, 24, 25, 41, 44, 51, 52, 58
Otitis media (Warme gosh): A study has shown that 40-50% of children older than 3
years with chronic otitis media have confirmed allergic rhinitis.19, 59, 65
Serous otitis media: Numerous studies have been performed to determine the
relation between allergy and otitis media with effusion (OME); the incidence of
allergic rhinitis in OME has been found to vary from 14% to 89%. 24, 25, 42, 59, 60
Nasal polyps, 15, 24, 25, 43 Rhinosinusitis, 59 Sinusitis, 15, 24, 25, 42, 65 Respiratory
infections and Orthodontic malformation, 15, 25 Dyspnoea, 20 Pneumonia
(Zaturriya), 1, 5 Pleurisy (Zatuljenb), Tuberculosis (Sil wa diq), 1, 2, 5, 20,
Stomachache (Darde medda), 1, 5, 19 Shosa, 20 Ishaal, 5,19, 20 Qulanj, 2, 5, 19 Falij,
Warme sadar, toothache, conjunctivitis, 19, 52 Migraine, Numbness (Khadar),
Deafness, 19 Fasade hazm, 2 and Khunnaq 1, 2
The day time tiredness experienced by the vast majority of the sufferers experience
disrupted sleep (Insomnia) at night due to nasal obstruction, which leads to open
mouth breathing, sore throat and snoring. 57 In addition to daytime fatigue and
somnolence, 63 nocturnal sleep impairment 14, 15, 18, 24, 57, 63, 65 is also associated with
depression, irritability, memory defects, inability to concentrate, 14, 34, 57, 61, 63 listless

Review of Literature
36
and irritable, 14, 61 decrease alertness and overall reduced quality of life. 18, 23, 52, 58, 63, 65
Further, Nazla Haar can alter the self perceived health status, pose limitations in
everyday activities and affect the working and school productivity, 34, 52, 65 and also
have detrimental effects on emotional and social wellbeing.65

Review of Literature
37
PREVENTIVE MEASURES
Avoid day time sleep and sleep on back 21 and / or sleep immediately
following meal.19
Devoid warmness of the body
Precaution from oily, Ghaleez lesdaar and delayed digestible foods, meat,
alcohol, onion, garlic, tea, akhrot, pista etc. sour things like milk, curd along
with Ghaleez and saqeel ghiza, 21 but if they feel weakness in the body, they
can use chicks with meats (ratab gosht), curd.19, 47
Reduce the quantity of food and drink 2, 19, 21
Try to avoid exposure to sunlight, hot or cold air and water. 2, 19, 21
Avoid strenuous exercise or physical activities.19
Samaghe suddab and Rai should be applied on the head immediately after
bath.2
The mainstay of treatment of Nazla Haar involves identification of avoidance of
provoking allergens where possible and the use of oral immunomodulatories.
Although the concept of allergen avoidance seems straightforward and obvious, in
practice it is often difficult to undertake. However, it is now possible to document
environmental allergen exposures with a great degree of precision. Allergen
avoidance measures such as: 56, 64.
No excessive use of seasonal fruits and khushboodar snuff (extreme flavors).21
Allergic rhinitis caused by exposure to plant pollens or seasonal molds,
avoidance of outdoor activity during peak pollen hours i.e. late morning to
early afternoon.
Review of Literature
38
Patients, who are allergic to grass pollen, may wear a surgical type mask while
moving in lawn or garden.
Use of an air conditioner to prevent air born pollen from entering the home
Patients who have perennial symptoms, down-filled comforters and wool
blankets may be kept away.
Washing of all sheets, mattress pads, pillowcases, and blankets every week in
hot water and detergent; this removes >95% of allergens.15
Wash bedding with hot wash (>550C) or eucalyptus oil to kill dust mites.15
Ensure rooms are well ventilated.15
Remove carpet and replace with washable, hard flooring.15
Remove extra soft furnishing and toys.15
According to Zakaria al Razi and Jalinoos, cupping over the nape of the neck is
advisable for itching in the nose and sneezing.2
Initial stage: adopting symptomatic measures:
Try to expel the mad’da 19, 47 by Inkibab with Banafsha, Nilofar, Nakhuna and
Babuna, 20 and apply fateela in the nose to divert the mad’da from throat or
chest.19, 47
Fasd is advisable if damavi khilt is involved 19, 20 followed by mushilat.20
Lateef ghiza like maushaeer 20
Munzijat 20
Hammam by luke warm water 20 is advisable before prescribing munzijat.2
Snuffing by luke warm shoneez and zeera.20
Should not use any medicines to arrest sneezing, this may interfere with the
nuzj of the mad’da, leading to collection of fuzlat in the brain.19
Review of Literature
39
USOOLE ILAJ
Effective treatment of Nazla Haar depends upon accurate clinical diagnosis and
assessment of the patient’s dominant symptoms. Although avoidance of interventions
can reduce extrinsic and intrinsic factors (allergen), they often fail to produce
clinically significant improvement as a result complete therapy is frequently
required.24
1. Izale sabab (Elimination of the cause)
Exposure to heat and / cold (intrinsic and extrinsic factors) should be
eliminated.
2. Correction of Sue mizaj:
I. Sue mizaj sada should be modulated with appropriate regimen and barid
makulat wa mashrubat, roghaniyat, nutulat, zimadat, quturat etc
II. Sue mizaj mad’di should be corrected through munzijat followed by Tanqia. 19
3. Ta’deele mizaj
4. Tadabeer:
Inkibab (steam inhalation), takmeed (fomentation), fasd (venesection) and use
of suitable oils for qutoor (nasal drops).
5. Ghiza:
Precaution from oily, ghaleez lesdaar and delayed digestible foods, meat,
alcohol, onion, garlic, mustard, tea, pista; sour things like milk, curd along
with ghaleez and saqeel ghiza
6. Muqawwiyate dimagh wa med’da 11

Review of Literature
40
Common single drugs used in Nazla are: 6, 20, 21
Banfsha, Behidana, Unnab, Sapistan, Asalussoos, Aalubukhara sheerin, Turanjabeen,
Tukhme khitmi muqashar, Kishneez khushk, Barg wa gule aazad, Gulab sufaid, Injeer
siya, Maghze khiyar shamber, Sheere tukhme kahu muqashar, Sheere maghze kaddu,
Maghze badam.
Compound drugs used in Nazla are: 6, 20, 21, 47
Sharbate banfsha, Sharbate khashkhash, Khameere khashkhash, Laooqe sapistan,
Laooqe khashkhash, Luabe behidana, Sharbate unnab, Habbe shifa, Khameere
gauzaban, Triyaqe nazla, Sharbate fardyaris.
Drugs used in modern medicine for rhinitis (Nazla): 24
Antihistamines: Antihistamines are the oldest drug used to treat allergic rhinitis and
are considered first- line therapy. Antihistamines compete with histamine for the H1-
receptor sites that contribute to sneezing, itching, rhinorrhea, and conjunctivitis. Oral
antihistamines ameliorate these symptoms of AR but generally do not improve nasal
congestion.
Decongestants: Decongestant such as pseudoephedrine treats nasal stuffiness but is
mild stimulants. These drugs are usually used in combination with antihistamines to
control the full spectrum of AR symptoms. Antihistamines and decongestant alone
generally do not provide satisfactory relief in patients with moderate to severe AR.
Leukotrienes Modifiers: leukotrienes modifiers (zafirlukast, montelukast, zileuton)
have conformed efficacy in AR comparable to that of antihistamines. This efficacy
reflects the presence and importance of these pro-inflammatory vasoactive mediators
in AR. Zafirlukast significantly reduces sneezing, rhinorrhea and in contrast to
antihistamines- nasal congestion in patients with SAR. Similarly, montelukast

Review of Literature
41
significantly improves nasal and ocular symptoms as well as quality of life in patients
with SAR and PAR.
Nasal Cromolyn: Nasal Cromolyn stabilizes mast cells and mediates additional anti-
inflammatory activities towards macrophages and T lymphocytes. Although not as
effective as intranasal corticosteroids, Cromolyn provides relief in patients with mild
to moderate symptoms, and it may be effective in combination with corticosteroids in
the treatment of refractory symptoms.
Intranasal corticosteroids: Intranasal corticosteroids (fluticasone, triamcinolone,
flunisolide, budesonide, mometasone, and ciclesonide are the most effective AR
treatments and are considered the treatments of choice for patients with moderate to
severe SAR or PAR, due to the potential side effects of systemically administered
corticosteroids, topical nasal steroids. 66 Topical corticosteroid therapy does not
inhibit IgE synthesis or mast cell degranulation. Intranasal corticosteroids are not
universally effective and do not provide complete relief in all patients.
Immunotherapy: immunotherapy decreases the severity of AR, reduces the need for
pharmacotherapy, and significantly improves quality of life. In patients with severe
AR and conjunctivitis poorly controlled by antihistamines and intranasal
corticosteroids, immunotherapy can reduce allergen sensitivity by more than 10-folds,
as well as significantly decreasing total symptoms and reducing total antiallergic drug
usage.
Surgery: rhinitis is due to anatomical component to the disease such as nasal septal
deviation or nasal polyps, or even sinusitis surgery may be indicated. 15
Review of Literature
42
BEHIDANA
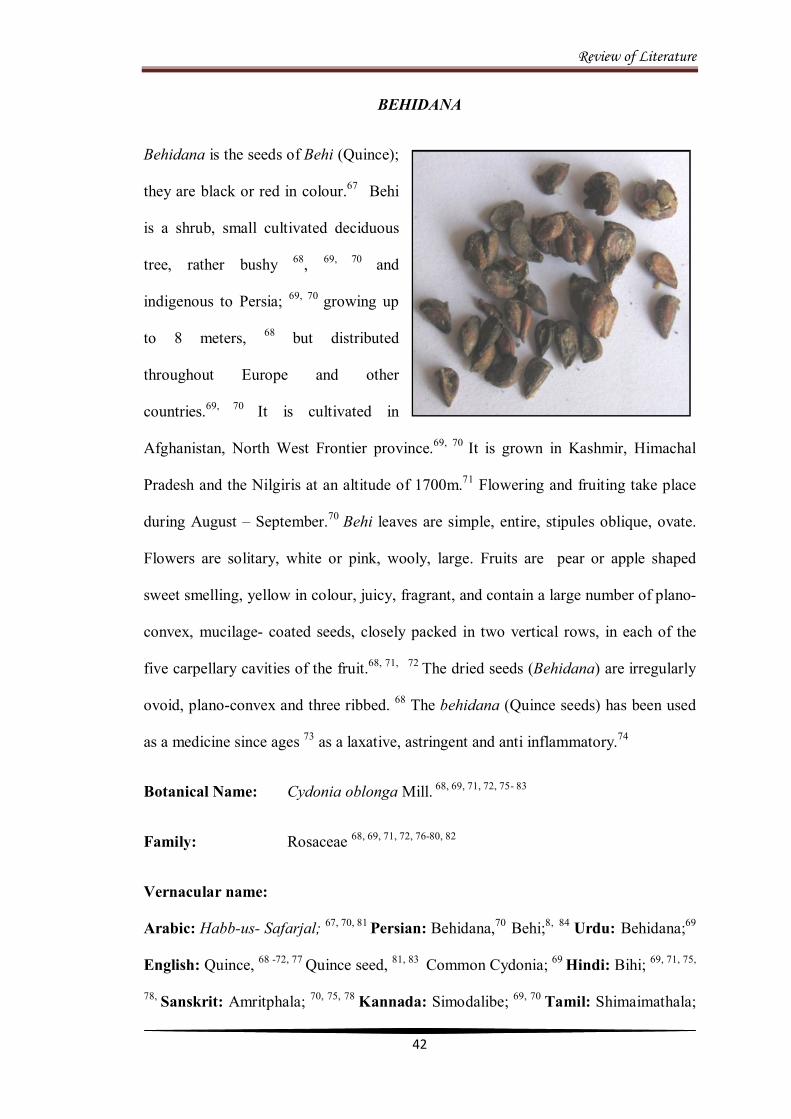
Behidana is the seeds of Behi (Quince);
they are black or red in colour.67 Behi
is a shrub, small cultivated deciduous
tree, rather bushy 68, 69, 70 and
indigenous to Persia; 69, 70 growing up
to 8 meters, 68 but distributed
throughout Europe and other
countries.69, 70 It is cultivated in
Afghanistan, North West Frontier province.69, 70 It is grown in Kashmir, Himachal
Pradesh and the Nilgiris at an altitude of 1700m.71 Flowering and fruiting take place
during August – September.70 Behi leaves are simple, entire, stipules oblique, ovate.
Flowers are solitary, white or pink, wooly, large. Fruits are pear or apple shaped
sweet smelling, yellow in colour, juicy, fragrant, and contain a large number of plano-
convex, mucilage- coated seeds, closely packed in two vertical rows, in each of the
five carpellary cavities of the fruit.68, 71, 72 The dried seeds (Behidana) are irregularly
ovoid, plano-convex and three ribbed. 68 The behidana (Quince seeds) has been used
as a medicine since ages 73 as a laxative, astringent and anti inflammatory.74
Botanical Name: Cydonia oblonga Mill. 68, 69, 71, 72, 75- 83
Family: Rosaceae 68, 69, 71, 72, 76-80, 82
Vernacular name:
Arabic: Habb-us- Safarjal; 67, 70, 81 Persian: Behidana,70 Behi;8, 84 Urdu: Behidana;69
English: Quince, 68 -72, 77 Quince seed, 81, 83 Common Cydonia; 69 Hindi: Bihi; 69, 71, 75,
78, Sanskrit: Amritphala; 70, 75, 78 Kannada: Simodalibe; 69, 70 Tamil: Shimaimathala;
Review of Literature
43
69, 71, 75, 76, 78, Telugu: Simadanimma; 69, 70, 75 Kashmiri: Bamsutu; 70, 75, 78 Unani: Bihi,
76 Bihidana, 72 Safarjal; 69 Bengali: Bihidana 71
Mizaj: Sard wa Tar 2o 67, 69, 70
Parts used: Seed, 68-72, 75-78 buds ,69, 78 bark, leaves, 69, 76, 78 fruits, 68, 69, 71, 75-
78, 82
Af’al (Actions):
Dafe nazla, Dafe sual haar, 69, 70 Dafe diq, 69 Muzliq, Mufarrih, 81 Mulattif , 69, 70, 72
Musakkine hararat, 67, 69, 70, 81 Qabiz, Mulayyan, Muqawwie bah, 67 Mushtahi,
Mufattih, Muqawwie med’da.85
Nafae Khas (Main Action):
Ishaal haar, 81 Mufarrih, Muqawwie dil wa dimagh 84
Iste’malat (Uses):
Nazla haar, 70, 81 Amraze khushunate halq, 69, 70, 81, 83 Sual yabis (dry cough),
Khushunate qasbaturriya, 67 Sil wa diq, 67, 81 Kasarate ataas, 85 Humma, 81 Zaheer,
Humuzate medda, 70 Qarhe ama, 69, 70 Amraze safravi, 67, 69 Qae balghami, Sozishe
baul, Nafsuddam, 67 Taskeene hararat, 84 Sozishe zaban, 67, 81 Peechish.69, 81
Miqdare khurak (Dosage):
Seeds 3- 5 Mashas (grams) 81, 85
Mazarrat (Adverse effects):
Mujaffif wa Murkhi med’da, 81, 84 Zoafe med’da wa kulliya 67
Muslih (Correctives):
For Garmi med’da – Kahnd; and Sardi med’da –Misri, 67 Qand sufaid, Badiyan,
Saunf 69; Shakkar and Badiyan.81
Review of Literature
44
Badal (Substitute): Isapghol 67, 69, 81
Murakkabat (Compound formulations):
Laooqe behidana, Banadiqe buzoor, Sharbate ejaz, 69, 70 Jawarishe safrjal, 69 Habbe
shaqeeqa, Habbe sil, Habbe surfa qavi, Qurse kaknaj, Laooqe nazli, Laooqe sapistan,
Laooqe shamoon.70
Ethanobotanical Description:
Actions:
Expectorant, 71, 82 soothing, 76 astringent, cardiac tonic, antispasmodic, 82 demulcent,
71, 72, 75, 76, 78, 82 laxative.68, 77
Therapeutic Uses:
Internally it is used in diarrhea, dysentery, 71, 72, 76, 78 constipation, 76 sore throat, 71-73, 78
fever, 71, 72, 78, gonorrhea, inflammation of the mucous membrane, 71 bronchitis. 68, 73, 77
Externally it applied in ulcers, burns and scalds.71, 73, 74, 76, 78
Chemical Composition:
Fixed oil, 68-70 cyanogenic glycosides, 68, 82 glycoside amygdalin, 72,76, 78 tannins, 68-70,
72 , 76mucilage, 68, 72, 76, 82 fatty oil, 76 ash, 72, 76 glucuronic acid residues, 80 volatile oil,
iron, calcium, phosphorus, magnesium, potassium, glycoside, steroid, protein, 69, 70
glucoside, amygdalin, ursolic acid, roseoside, mixture of n-paraffins, alcohol-
soluble extractive(s), β-sitosterol, saringosterol, palmitic, oleic, linoleic, and
marmelolactones A & B.70

Review of Literature
45
Scientific Reports:
1. An in vitro study has shown that Citrus and Cydonia compound can
potentially restore the disturbed immune state of rhinitis patients, which
essentially could be sufficient to make allergic symptoms disappear
permanently.86
2. A recent study has shown that a positive effects by Citrus and Cydonia
compound on allergic to grass pollen, suffering from hay fever, and the
necessity for the use of antihistamines with regard to the nature of the
complaints.86
3. A study has shown that Citrus and Cydonia compound is being prescribed
over eighty years as a subcutaneous injection or as a nasal spray for patients
who suffer from seasonal allergic rhinitis.86
4. The hot water extract of quince (Cydonia oblonga) has an inhibitory effect on
broad range of the late phase immune reactions of mast cells.87
5. The phenolic extract of quince leaf has properties of free-radical scavenging
and anti haemolytic activities.88
6. The phenolic extracts from leaves of Cydonia oblonga can be used as a better
and cheaper source of bioactive compounds and may have relevance in the
prevention of diseases in which free radicals are implicated.89
7. The leaves of Cydonia oblonga has been utilized in traditional medicine as
antitussive, antipyretic, sedative and antidiarrheic properties.89
8. The polyphenolic extracts of fruit from Cydonia oblonga has been proved that
it has antioxidant, antimicrobial (antibacterial and anti- influenza viral), and
anti ulcerative properties.89

Review of Literature
46
9. The methanolic extract of fruit of Cydonia oblonga has been proved that it has
antioxidant properties against oxidative haemolysis of human erythrocytes.90

Review of Literature
47
UNNAB
Unnab (Indian jujube) is a fruit of a well
known plant Zizyphus jujuba. The Indian
jujube is a spiny deciduous shrub or a
small tree commonly 6 to 10 meters high,
68, 91 usually armed; young branches and
flowers densely tomentose.71 Leaves are
alternate, elliptic ovate or sub orbicular to
ovoid- lanceolate, 68, 71 dark green and
glabrous above, slightly velvety beneath by pale-brown tomentum. 71 Flowers perfect
and axillary clusters or shortly peduncled cymes 71; 7-8 flowers in each cluster,
greenish yellow.68 The fruit has two varieties; the wild is small and round, while the
cultivated fruit is oval, fleshy, bigger in size and sweeter than the wild. 92 The
cultivated variety when ripe and dry is expectorant and mild laxative. Drupes 1.5-5cm
long, ovate to oblong, dark reddish- brown when ripe, containing a single stone
surrounded by 2 celled fleshy pulp, glabrous, edible. Seeds are plano- convex. 71 The
bark, wood and fruit come from Jurjan, China, and Nepal; the fruit is sweet and
moderately astringent about the size of a dried date with a small stone.93 Flowering
and fruiting take place during September to October.68
Unnab is indigenous and naturalized throughout India, 78 and in the outer Himalayas
altitude up to 1,350 meters; 76, 78 commonly cultivated in India, Japan, China, Africa,
Malaysia, Afghanistan and Australia.68
Botanical Name: Zizyphus jujube Mill. 68, 71, 75- 78, 80, 91, 93-95
Family: Rhamnaceae 68, 75-78, 94

Review of Literature
48
Vernacular name:
Arabic: Unnab; 96 Persian: Sailanah; 97 English: Indian jujube, 71, 76, 77 Common
jujube; 68, 76, 77 Hindi: Baer, 75, 91 Ber, 71, 75, 77, 91 Beri; 77, 91 Sanskrit: Ajapriya, 75
Badara, 71, 75, 77 Karkandhu, Kuvala, Maduraphala; 75 Urdu: Ber; 91 Unani: Ber, 76
Unab; 95 Sinhalese: Ilanda; 91 Malayalam: Elantha,75 Ilanta, Ilantappalam, 77
Badaram; 78, 91 Kannada: Yalachi, Elanji, 75, 77 Bore; 77, 78 Tamil: Ilandai, 77, 78, 91, 94
Ilantappalam, 77 Elladu; 71,75 Bengali: Ber, Boroi, 75 Kool; 71, 75 Marathi: Bor,75
Bera; 75, 91 Gujarathi: Bor, Bordi; 75 Telugu: Reegu, 75, 77, 91 Gangareegu, 75, 77, 78, 91
Karakandhavu. 75
Mizaj: Motadil – Haar Barid, 67, 81 Haar Ratab, 97 Barid Ratab 85
Parts used: Fruits, 67, 68, 71, 75-78, 81, 85, 91, 93, 94 seeds, 71, 75, 76 leaves 71, 75, 76, 78,
twigs, 71 barks 71, 76, 78 roots 71, 78
Af’al (Actions):
Musaffie khoon, 67 Mulattif, 85 Munzije akhlate ghaleeza, 81, 94 Mulayyane sadaro
ahasha, 94 Munaffise balgham, 81 Ta’deeluddam, 81, 84 Mulayyane taba’ 81 Mulayyane
akhlate raqeeqa, 84 Muallide khoon, Musakkin.84, 94
Nafae Khas (Main action):
Dafi’ khushunate halq, Musaffie khoon 81
Iste’malat (Uses):
Nazla wa zukam, 81 Sual yabis 84, 97 Ta’deeeluddam , 81, 85 Darde seena, jiger wa
gurda, 84, 85 Khushunate halq, 67, 97, Basoor wa kharash, Musakkine hararat, Taskeene
atash, Aatishak, 81 Khushunate seena.81, 97
Review of Literature
49
Miqdare khurak (Dosage):
5- 7 pieces 81, 85
Mazarrat (Adverse effects):
Med’da wa bah, 67, 81 Naf’fakh 67
Muslih (Correctives):
For Naf’fakh- Kahnd aur Maveez aur Gulab; 67Zoafe bah- Shahed 67
Shaker, Gulab aur Shahed 81
Badal (Substitute): Sapistan 67, 81
Murakkabat (Compound formulations):
Sharbate unnab, 67 Sharbate ejaz, Laooqe sapistan 81
Ethanobotanical Description:
Actions:
Anodyne, 71, 75-77, 80 cooling, tonic, 71, 75-77, 80, 91 astringent, stomachic, 71, 76 styptic, 71,
76-78, 91, 94 antidote to aconite poisoning, 80, expectorant, 71, 76, 93 mild laxative, 71, 76, 91
aphrodisiac, 77, 91 appetizer, 77 mucilaginous, 77, 78, 91, 94 nausea and vomiting, 80
digestive, 78, 91, 94 purgative, 77 nutrient, emollient, 76, 80 antitussive, anti allergic, 76
blood purifier. 78, 91, 93, 94
Therapeutic Uses:
Internally for skin diseases, 77, 91 purify blood, aid digestion, 78, 91, 94 useful in vitiated
condition of pitta, constipation, heamorrhages, flatulence, dyspepsia, 77 diarrhoea,
night sweats, hysteria, palpitational insomnia, general fatigue, 68, 77 vomiting, 77, 81, 91
hyperdipsia, 77, 91 removes biliousness, 91 nausea, 77, 80 abdominal pain in pregnancy. 80
Externally used in wounds, ulcers. 77, 80

Review of Literature
50
Chemical Composition:
Carbohydrates, protein 68, 98 amino acids, anthocyanins, fat, 68 linoleic acid, myristic
acid, palmitic acid, β-sitosterol, stigmasterol, 71 calcium, phosphorus, iron, carotene,
thiamine, riboflavin, niacin, vitamin C, ziziphic, 98 cyclic AMP and GMP, saponins,
jujuboside B, alphitolic acid, 76 mucilage, sugar, 93 tannin, 80, 98
Scientific Reports:
1. The anti-allergic activity of aqueous extracts of Z. jujuba was studied by
measuring its inhibitory effect on hyaluronidase (bovine testes) activation in
vitro. Z. jujuba was shown to have strong anti-allergic activity (Su et al.,
2000). 92
2. The study has proved that the essential oil from seeds of Z. jujuba has a useful
anti-inflammatory agent, and the anti-inflammatory effects of the major
pharmacological components present in the essential oil of Z. jujuba seeds
might accelerate the development of new drugs for various inflammatory
diseases. 99

Review of Literature
51
SAPISTAN
Sapistan is an edible 75 fruit of Cordia
dichotoma, which is a well known
drug used in Unani system of
medicine. This plant being perennial,
found throughout year.69 It is a
moderate 69 or medium 68 sized,
deciduous tree about 13- 14m high
with a short crooked trunk; 69, 71
leaves simple, 68 alternate, variable in form and size, 71 entire or slightly dentate,
elliptic-lanceolate to broad-ovate or oblong sub-3-nerved, 68, 69 with a rounded or
cordate base.68 Flowers white, 68 borne in many-flowered, 71 small in lax corymbs, 68,
69, 71 terminal or axillary cymes, 68 polygamous, hermaphrodite.71 Calyx glabrous or
minutely pubescent 68 without lobes; 69 fruits drupes, 68 berries, ovoid, subacute, 71
yellowish brown, pink or nearly black when ripe with a viscid sweetish; transparent
pulp surrounding a central stony part 68, 71 usually 1 seed.69, 71
The Cordia dichotoma grows throughout India in the warmer regions.68, 79 The fruits
are used extensively due to diverse pharmacological actions and therapeutic uses
attributed to it. Although, its leaves, bark and kernels are also having medicinal
importance but, fruits are mostly used for medicinal purposes as astringent,
anthelminitc, demulcent, diuretic, and expectorant hence used in diseases of chest and
urinary passage. 75 Flower appears in March- April the fruit ripens in May to July.69
Botanical Name: Cordia dichotoma Forst. f 68, 69, 71, 76-78, 97
Family: Boraginacae 68, 69, 71, 76-78
Review of Literature
52
Vernacular name:
Arabic: Dabaq;91 Persian: Sapistan; 79, 91 English: Sebestan plum, 91Sebestan fruit; 79
Hindi: Lasora, 75, 79, 91 Chota lasora; 75, 91 Sanskrit: Bahuvaraka; 75, 91 Urdu: Lasora;
91 Malayalam: Viri, 75 Cheruviri; 75, 91 Kannada: Chikkachalle; 75 Tamil:Naruvili 75,
91 Bengali: Bahubara, 75, 91 Bal-phal; 79 Gujarathi: Bargund, 75 Lepistan; 91 Telugu:
Chinna Nakkeru; 75, 91 Marati: Shelvant; 75
Mizaj: Motadil 67, 69
Motadil in Garam wa Sard 85, 98
Parts used: Fruit 67, 68, 71, 75, 76, 78, 79, 91, 93 bark, 68, 76-79, 91 leaves, 68, 76-78, 91
seeds 76, 91
Af’al (Actions):
Mulattif, Mudire baul, 69, Musakkin, 67, 69 Mulayyan, Munaffise balgham, Muzliq 81
Nafae Khas (Main actions):
Sual yabis 81
Iste’malat (Uses):
Nazla haar, 81 Khushunate halq, Zatul jenb, Shosa, Barsam, 67, 81 Varme halq, Sozishe
ama , Darde seena, Ishaale safra and sawda, Ta’deeluddam 67 wa safra, 67, 81
Taskeene atash, Sozishe baul, Sual yabis, 67, 81, 97 Khushunate seena, 81, 97 Aathsak,
Sozak, 69, Qatile kirme shikam, 67, 97 Hummiyat safravi wa damavi, Mulayyane taba, 81
Hummiyate harra. 97
Miqdare khurak (Dosage):
9- 15 pieces 81, 85
Review of Literature
53
Mazarrat (Adverse effects):
Zoafe med’da wa jigar 67, 81
Muslih (Correctives):
Unnab, Amla 67 wa barge gulab 81
Badal (Substitute):
Khitmi 67, 69, 81 or Unnab 67, 69
Murakkabat (Compound formulations):
Laooqe sapistan 69, 98
Ethanobotanical Description:
Actions:
Astringent, 71, 75, 76, 78, 91 expectorant, anthelminitc, diuretic, 68, 71, 75-78, 91 demulcent, 71,
75, 76, 78, 79 mucilaginous, 76, 79 cooling, purgative 68, 77, 91 aphrodisiac, emollient,
febrifuge.68, 77
Therapeutic Uses:
Internally; disease of chest, 71, 75, 76, 78, 79, 81 spleen 68, 71, 75, 77, 78, 91 and urinary passage,
71, 75, 76, 78 dyspepsia, 91 dry cough, chronic fevers, arthralgia, 68, 76, 91 diseases of
uterus, 79 scolding of urine, burning sensation of the throat, 91 vitiated conditions of
vata and pitta, leprosy, skin diseases, bronchitis, strangury, urethralgia, urethritis, 68,
77 disease of urethra.79, 91 External application - ringworm, ulcers 68, 77
Chemical Composition:
Carbohydrates, 69, 80 crude fibre, ash, protein, fat, 80 phenolics, tannins, potassium,
sodium, magnesium, steroids, 69 iron, calcium, 69, 76, 80 phytic acid, phytate
phosphorous, oxalic acid phosphorous, zinc, manganese, chromium, copper.76, 80
Review of Literature
54
Scientific Reports:
1. Methanolic extract of Cordia dichotoma seeds and leaves possess powerful
antioxidant activity. 101
2. The plant of Cordia dichotoma has been reported that it possesses analgesic,
anti-inflammatory and hepatoprotective activities. 102
3. Flavonoids contain fruit of Cordia dichotoma has the property of wound
healing.102
4. The seeds of the plant Cordia dichotoma forst f. have been reported that it has
anti-inflammatory property. 103
5. A study shown that the fruits of Cordia dichotoma are used as astringent,
expectorant, anthelminitc, purgative, diuretic, 101, 102, 103 cooling, aphrodisiac,
and emollient. 104
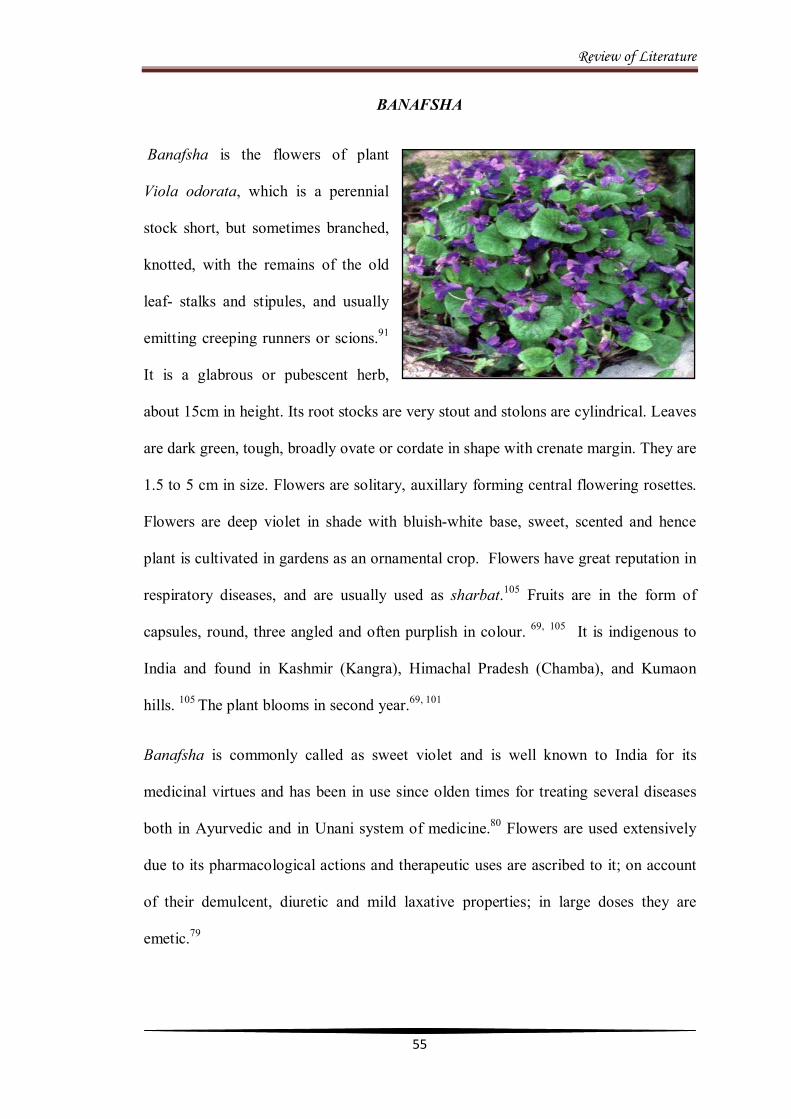
Review of Literature
55
BANAFSHA
Banafsha is the flowers of plant
Viola odorata, which is a perennial
stock short, but sometimes branched,
knotted, with the remains of the old
leaf- stalks and stipules, and usually
emitting creeping runners or scions.91
It is a glabrous or pubescent herb,
about 15cm in height. Its root stocks are very stout and stolons are cylindrical. Leaves
are dark green, tough, broadly ovate or cordate in shape with crenate margin. They are
1.5 to 5 cm in size. Flowers are solitary, auxillary forming central flowering rosettes.
Flowers are deep violet in shade with bluish-white base, sweet, scented and hence
plant is cultivated in gardens as an ornamental crop. Flowers have great reputation in
respiratory diseases, and are usually used as sharbat.105 Fruits are in the form of
capsules, round, three angled and often purplish in colour. 69, 105 It is indigenous to
India and found in Kashmir (Kangra), Himachal Pradesh (Chamba), and Kumaon
hills. 105 The plant blooms in second year.69, 101
Banafsha is commonly called as sweet violet and is well known to India for its
medicinal virtues and has been in use since olden times for treating several diseases
both in Ayurvedic and in Unani system of medicine.80 Flowers are used extensively
due to its pharmacological actions and therapeutic uses are ascribed to it; on account
of their demulcent, diuretic and mild laxative properties; in large doses they are
emetic.79
Review of Literature
56
The banafsha is available in commerce in three forms: (1) the dried aerial parts of the
herb, viz, the stems, leaves and flowers (Kashmiri banafsha); (2) only the dried
flowers (Gule banafsha); and (3) the aerial parts without flowers (Barge banafsha).80
Botanical Name: Viola odorata Linn. 68-70, 75-79, 83, 96
Family: Violaceae 68-70, 76-79
Vernacular name:
Arabic: Banafsaj, 69, 70, 81, 96 Firfeer; 69, 81, 91, 96 Persian: Gule Banafsha; 70 English:
Sweet violet, 68-70, 76, 77, 83, 105 Violet; 70 Hindi: Banafshah; 68-70, 77, 80 Sanskrit:
Banaphsha, 68, 77 Nilapushpa; 78 Urdu: Gule Banafsha; 69 Malayalam: Vayilettu; 78
Kannada: Violethoo; 68, 77, 80 Tamil: Vilaettu; 68-70, 77, 80 Bengali: Banafshah, 68-70, 77, 80
Banosa; 69, 80, 81 Marathi: Bagabanosa; 69, 70, 80 Gujarathi: Bahaphsa 69, 70, 80 Telugu:
Vialettu; 70 Kashmiri: Banafsha; 70 Unani: Banafshaa, Banafsaj 76
Mizaj: Sard wa Tar 1o 8, 67, 70, 100
Garam wa Khushk 1o 69
Parts used: Flowers, 68-70, 76, 80, 91, 96, 106 leaves, 76, 80, 83, 96 roots 78, 80, 91
Af’al (Actions):
Mulayyan, 8, 67, 69, 70, 81, 85 Mushil, Latafat, Lazoojat, Jazib, Muzliq, Islahe khoon, 67
Munaffise balgham Muhallile warm 69, 70, Muaddile safra, Musakkine khoon 81,
Murattib wa munavvim 8, 81
Nafae Khas (Main Action):
Mulayyane taba’81

Review of Literature
57
Iste’malat (Uses):
Zukam, 81 Nazla, Suaal 69, 70, 81, Mukharije safra, 85 Qabz, 67, 69, 70, 81 Ie’tidale safra, 67,
81 Tahleele lateef aur sakht warm, 67 Zatul jenb, Sudae haar, 81, 85 Saher,
Ta’deeluddam, Aashoobe cheshm, Humma, Taskeen atash, Zaturriya, Amraze haara
med’da wa jigar, 81 Darde kulliya 85
Miqdare khurak (Dosage):
Flowers 10gm or 20gm 67, 69
10-25gms70
Mazarrat (Adverse effects):
Mukarrab, 67, 81, 84 Matli 67
Muslih (Correctives):
Marzanjosh, 69, 81, 84 Nilofar 81, 84
Badal (Substitute):
Gule nilofar, 67, 69 Barge khubbazi, 67, 81 Asalussoos, 67, 69, 81 Rube soos, 67 Gauzaban 81
Murakkabat (Compound formulations):
Sharbate banafsha, 67, 70, 81, 95 Sharbate ustukhuddus, Sharbate arzani, 95 Khameere
banafsha, Roghane banafsha, 67, 70, 95 Habbe banafsha, 81 Itrifale zamani, 70, 95 Habbe
sil, Majoone antaki, Mufarre motadil, Mufarre yaqooti barid, Zimade warme
unsayain, Sharbate ejaz, Dayaqooza, Qairooti muhallil, Habbe ghariqoon, 70 Laooq
sapistan Khiyar shamberi.95

Review of Literature
58
Ethanobotanical Description:
Actions:
Expectorant, diuretic, 76, 93 anti-inflammatory, diaphoretic, antipyretic, 76 emollient,
demulcent, 78, 80, 91, 95 purgative, 93 febrifuge.78
Therapeutic Uses:
Biliousness, 78, 93 lung troubles, 78 catarrhal and pulmonary affections, diseases of liver
and intestine, 76 cough, hoarseness of voice, infantile ailments, 80, 91 sore-throat, 68, 77,
80, 91 fever, 68, 77 cancerous growth pain particularly in the mouth and throat.80
Chemical Composition:
Volatile oil, 80, 93, 95 violin, 68, 80, 93, 95 rutin, cyanin, 80, 95 emetine, violenic acid, 93
voilanin chloride, 76 anthocyanin, tocopherol, flavonoids, mucilage, ash, 76 methyl
salicylate, sugar, 80 salicylic acid, 93 saponins, glycosides, phenolic compounds,
tannins, resins, triterpines, potassium, magnesium, sodium, iron.69
Scientific Reports:
1. An aqueous extract of Viola odorata has been proved that it has anti
inflammatory property equal to corticosteroids in the treatment of
inflammatory conditions of the lung. 107
2. The extracts of phenolic compounds and flavonoids of Viola odorata Linn.
have been proved to possess antioxidant and free radical scavenging activities.
108
3. The herb Viola odorata shows antimycotic and antibacterial activity, and is
considered quite effective in the treatment of eczema.80
METHODOLOGY

Methodology
59
MATERIALS AND METHODS
The present clinical study entitled “Efficacy of a Unani formulation in Nazla Haar”
was conducted after enrolling the patients from outpatient department of National
Institute of Unani Medicine hospital, Bangalore, after the approval of the NIUM,
Institutional Ethical Committee for Biomedical research during March 2011 to
December 2011.
1. Criteria for selection Patients
Known case of Nazla Haar, and or patients having the symptoms like sneezing,
watery nasal discharge, sensation of nasal obstruction, itching sensation in the nose,
mouth or throat, tearing of the eyes, were carefully evaluated, based on the criterion
of inclusion and exclusion.
a. Inclusion criteria
Age between 12-50 years
Gender: males and females
Diagnosed patients of rhinitis
Patients with symptoms complex that consists of any combination
of the following: sneezing, rhinorrhea, nasal congestion, itching in
the nose, eyes, throat or mouth, postnasal drip and headache.
Patients who have agreed to sign the informed consent form and
follow the protocol.

Methodology
60
b. Exclusion criteria
A. Physiological status
Patients below 12 and above 50 years of age.
Pregnancy and lactating women
B. Pathological status
Atrophic rhinitis
Sinusitis
Deviated Nasal Septum
Nasal polyps/ Nasal growth/ Adenoids
Asthma
Patients with systemic diseases like diabetes mellitus,
cardiovascular, impaired renal and hepatic functions
C. Patients who refuse to give the written informed consent for the study.
2. Selection of patients
Patients fulfilling the inclusion criterion were subjected to haematological,
biochemical and radiological investigations for obligatory terms of inclusion criteria,
were enrolled in the study after obtaining a voluntary written informed consent.
a. History Taking
A detailed history was recorded based on their chief complaints with duration, age,
sex, religion, marital status, occupation, address, socio economic status on the basis of
Kuppuswamy’s socioeconomic scale.109 Personal history, treatment history, past
history of any disease, family history was also recorded in a predesigned and pretested
proforma.
Methodology
61
b. Examination:
Each patient was subjected to comprehensive general physical and systemic
examination with special emphasis on pulse, blood pressure, respiratory rate,
temperature, built, height, bodyweight, cyanosis, clubbing of fingers, mouth
breathing, lymphadenopathy and icterus etc. Likewise, careful systemic and local
examinations were also done to rule out for any findings and involvement of any other
serious illnesses. A thorough local examination of nasal cavity was performed for
colour of mucosa, swelling of turbinates, colour & consistency of nasal discharge and
nasal obstruction.
c. Investigations:
Investigations such as Hb%, TLC, DLC, ESR, RBS, RFT, LFT, X-ray PNS and Nasal
smear for eosinophils were carried out in all enrolled patients before and after
completion of the treatment, to exclude the patients other than Nazla Haar, to
establish the safety of the drugs (test and placebo), and as an objective parameters.
d. Assessment of Mizaj:
The Mizaj of the patients was determined on the basis of Ajnase ashra.
3. Informed consent
Patients fulfilling the inclusion criteria were asked to refer thoroughly the Informed
Consent sheet, which possess the details of study, including nature of drugs or
procedure administered, and its risk and benefits; moreover, the patients association
with the study is purely voluntary, they can ask any information / query with the
investigator. After the acceptance by the patients without any coercion asked to give
written informed consent duly signed with date.
Methodology
62
4. Method of Collection of Data:
Through clinical study of patients enrolled into the study from the OPD and IPD,
NIUM, Bangalore.
5. Study design:
Randomized, single blind, placebo controlled clinical study.
6. Sample size:
40 patients
7. Allocation of subjects into groups:
The 40 patients were randomly allocated into two groups comprising 30 patients in
test and 10 in placebo control group.
8. Duration of protocol:
15 days in both test and control groups.
9. Criteria for selection of drugs:
The Unani formulation consists of Behidana, Unnab and Sapistan in the form of
Joshanda along with Sharbate Banafsha 110 has been in use since a long time and
claimed its efficacy in Nazla Haar. Therefore, this formulation was selected from the
Bayaze Kabeer to validate its efficacy and safety.
The ingredients of Joshanda110 and Sharbate Banafsha 110, 111 along with their
dosage are given below:
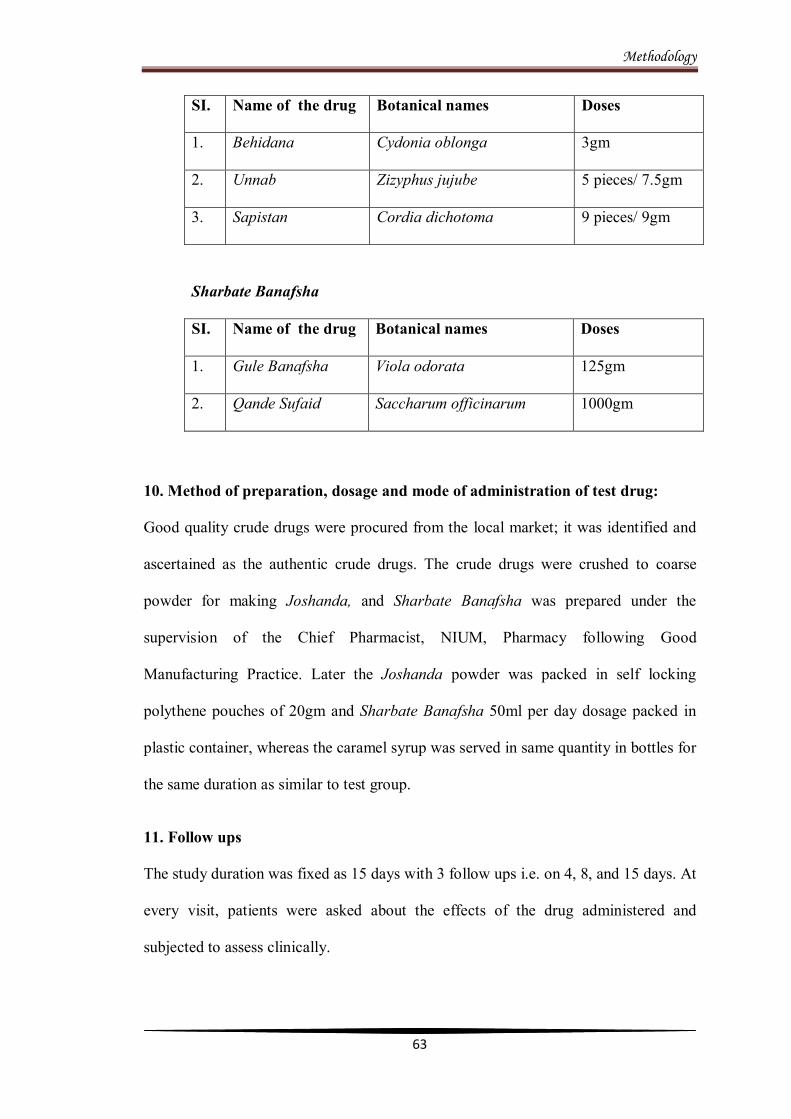
Methodology
63
SI. Name of the drug Botanical names Doses
1. Behidana Cydonia oblonga 3gm
2. Unnab Zizyphus jujube 5 pieces/ 7.5gm
3. Sapistan Cordia dichotoma 9 pieces/ 9gm
Sharbate Banafsha
SI. Name of the drug Botanical names Doses
1. Gule Banafsha Viola odorata 125gm
2. Qande Sufaid Saccharum officinarum 1000gm
10. Method of preparation, dosage and mode of administration of test drug:
Good quality crude drugs were procured from the local market; it was identified and
ascertained as the authentic crude drugs. The crude drugs were crushed to coarse
powder for making Joshanda, and Sharbate Banafsha was prepared under the
supervision of the Chief Pharmacist, NIUM, Pharmacy following Good
Manufacturing Practice. Later the Joshanda powder was packed in self locking
polythene pouches of 20gm and Sharbate Banafsha 50ml per day dosage packed in
plastic container, whereas the caramel syrup was served in same quantity in bottles for
the same duration as similar to test group.
11. Follow ups
The study duration was fixed as 15 days with 3 follow ups i.e. on 4, 8, and 15 days. At
every visit, patients were asked about the effects of the drug administered and
subjected to assess clinically.

Methodology
64
Concomitant treatment was not allowed during treatment in both groups. The patients
who were taking any other medicine as a treatment of Nazla Haar were advised to
observe abstinence for a week from consuming those drugs before commencing
treatment with the test or placebo.
12. Efficacy assessment:
Efficacy assessment was made subjective and objectively at each follow up with
reference to baseline symptoms up to 15th day of the treatment. Total Symptom
Severity Score (TSSS) is an objective method used in assessing the efficacy of the
study. The severity of 8 symptoms (rhinorrhoea, sneezing, nasal congestion,
itchy nose, itchy mouth or throat, lacrimation, post nasal drip and headache) was
rated on a 4 point scale (0-absent, 1- mild, 2- moderate, 3- severe). 112, 113, 114, 115
These scores were summed for each patient at each assessment point (based on the
involvement of the subjective parameters), to obtain a TSSS, with a maximum value
of 24 points. TSSS score of both, test and placebo control groups, was calculated
according to the method described by Rogkakou et al. 114
Therefore in each follow up, the patients were asked to rate the severity of their nasal
symptoms (sneezing, rhinorrhea, nasal obstruction and itching in the nose, mouth or
throat) and ocular symptoms (itchy eyes and watering of the eyes) on a four point scale
for each symptoms along with the side effects occurred during the treatment period.
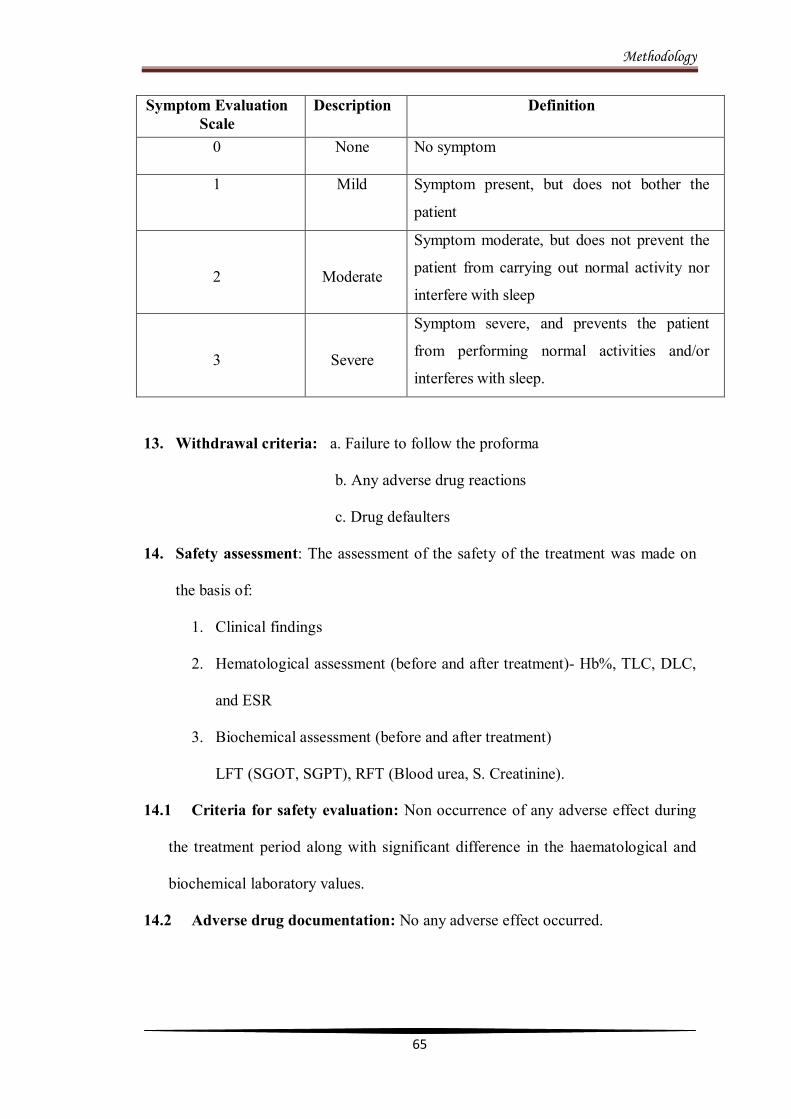
Methodology
65
Symptom Evaluation Scale
Description Definition
0 None No symptom
1 Mild Symptom present, but does not bother the
patient
2
Moderate
Symptom moderate, but does not prevent the
patient from carrying out normal activity nor
interfere with sleep
3
Severe
Symptom severe, and prevents the patient
from performing normal activities and/or
interferes with sleep.
13. Withdrawal criteria: a. Failure to follow the proforma
b. Any adverse drug reactions
c. Drug defaulters
14. Safety assessment: The assessment of the safety of the treatment was made on
the basis of:
1. Clinical findings
2. Hematological assessment (before and after treatment)- Hb%, TLC, DLC,
and ESR
3. Biochemical assessment (before and after treatment)
LFT (SGOT, SGPT), RFT (Blood urea, S. Creatinine).
14.1 Criteria for safety evaluation: Non occurrence of any adverse effect during
the treatment period along with significant difference in the haematological and
biochemical laboratory values.
14.2 Adverse drug documentation: No any adverse effect occurred.
Methodology
66
15. Methods: Adhered to the Good Clinical Practice (GCP).
16. Documentation: After completion of the study the case report form (CRF) along
with Informed consent forms will be submitted to the Department of Moalajat,
NIUM, Bangalore.
17. Statistics: The overall response was assessed by u s ing statistical tests like
Paired, Fisher’s exact test two tailed, Friedman, and Kruskal- Wallis with
Dunn’s Multiple Comparison.
RESULTS

Results and Observations
67
Table 1
Distribution of patients according to Age
n=40
Age
No. of Patients
Total No. of Patients
Percentage %
Test Group
Placebo control
Group
13-20
6
2
8
20
21-30
11 4
15
37.5
31-40
8
2
10
25
41-50
5
2
7
17.5
Total
30
10
40
100
02468
10121416
13-20 21-30 31-40 41-50
8
15
10
7
Graph-1: Distribution of patients according to Age
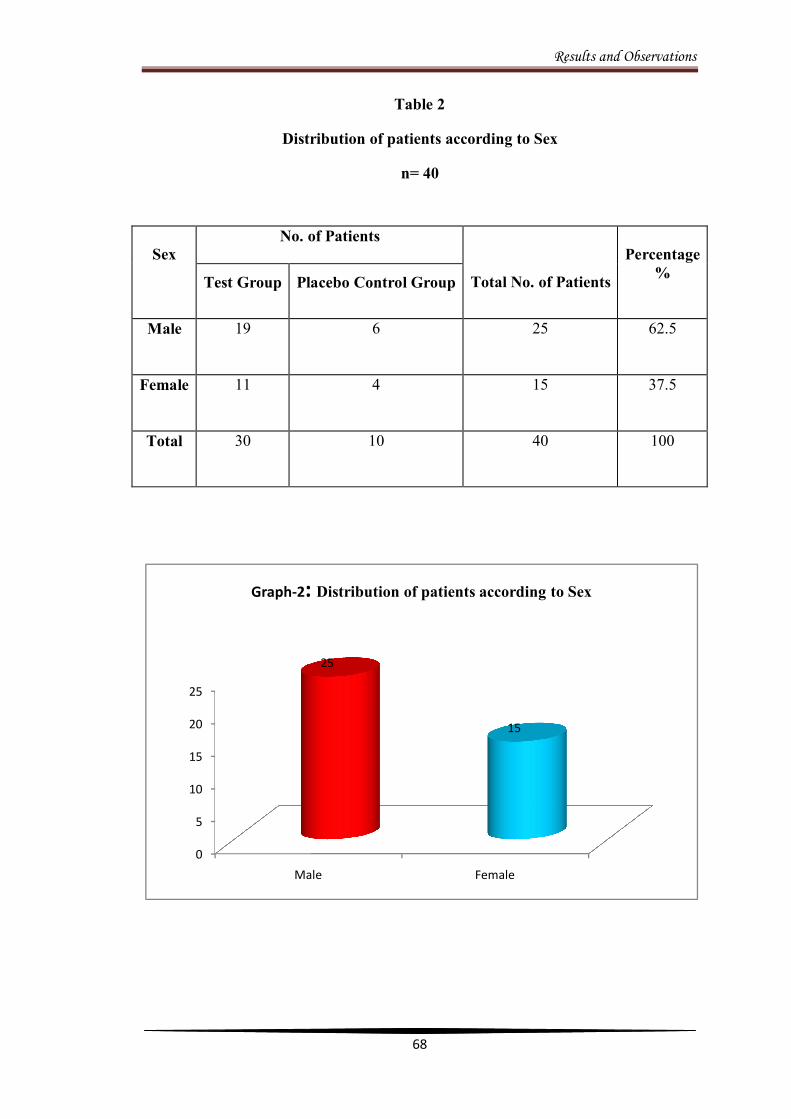
Results and Observations
68
Table 2
Distribution of patients according to Sex
n= 40
0
5
10
15
20
25
Male Female
25
15
Graph-2: Distribution of patients according to Sex
Sex
No. of Patients
Total No. of Patients
Percentage
%
Test Group
Placebo Control Group
Male
19
6
25
62.5
Female
11
4
15
37.5
Total
30
10
40
100

Results and Observations
69
Table 3
Distribution of patients according to Marital Status
n=40
Marital status
No. of Patients
Total No. of Patients
Percentage %
Test
Group
Placebo Control Group
Married
18
8
26
65
Unmarried
12
2
14
35
Total
30
10
40
100
0
5
10
15
20
25
30
Married Unmarried
26
14
Graph-3: Distribution of patients according to Marital Status

Results and Observations
70
Table 4
Distribution of patients according to Religion
n=40
Religion
No. of Patients
Total No. of
Patients
Percentage %
Test Group
Placebo Control Group
Hindu
16
06
22
55.0
Muslim
13
04
17
42.5
Christian
01
00
01
2.5
Total
30
10
40
100
0
5
10
15
20
25
Hindu Muslim Christian
22
17
1
Graph-4: Distribution of patients according to Religion

Results and Observations
71
Table 5
Distribution of patients according to Dietary Habit
n=40
Dietary habit
No. of Patients Total No. of
Patients
Percentage %
Test Group
Placebo Control Group
Vegetarian
1
3
4
10
Non vegetarian
29
7
36
90
Total
30
10
40
100
90%
10%
Graph-5: Distribution of patients according to Dietary Habit
Non Vegetarian
Vegetarain

Results and Observations
72
Table 6
Distribution of patients according to Socio Economic Status (SES)
n=40
SES
No. of Patients
Total No. of Patients
Percentage %
Test Group
Placebo Control Group
Upper
02
01
03
7.5
Middle
27
08
35
87.5
Lower
01
01
02
5.0
Total
30
10
40
100.0
7.5%
87.5%
5.0%
Figure-6: Distribution of patients according to SES
Upper
Middle
Lower
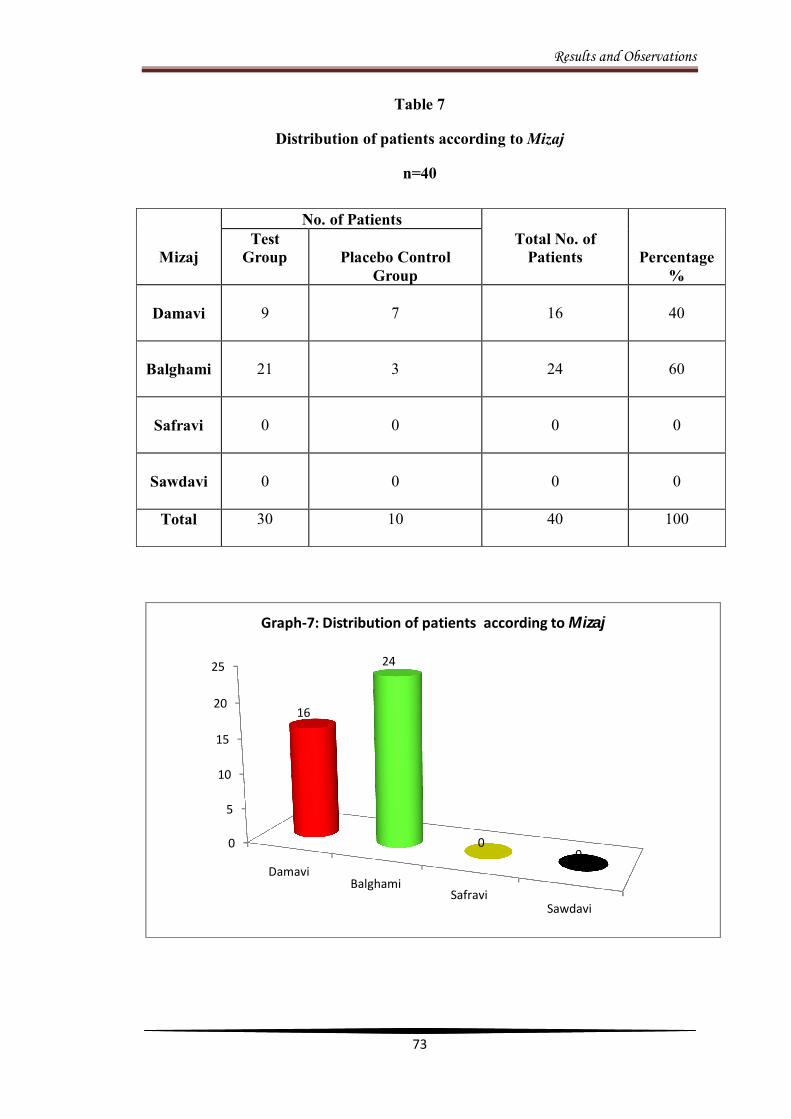
Results and Observations
73
Table 7
Distribution of patients according to Mizaj
n=40
0
5
10
15
20
25
DamaviBalghami
SafraviSawdavi
16
24
00
Graph-7: Distribution of patients according to Mizaj
Mizaj
No. of Patients Total No. of
Patients
Percentage %
Test Group
Placebo Control
Group
Damavi
9
7
16
40
Balghami
21
3
24
60
Safravi
0
0
0
0
Sawdavi
0
0
0
0
Total
30
10
40
100
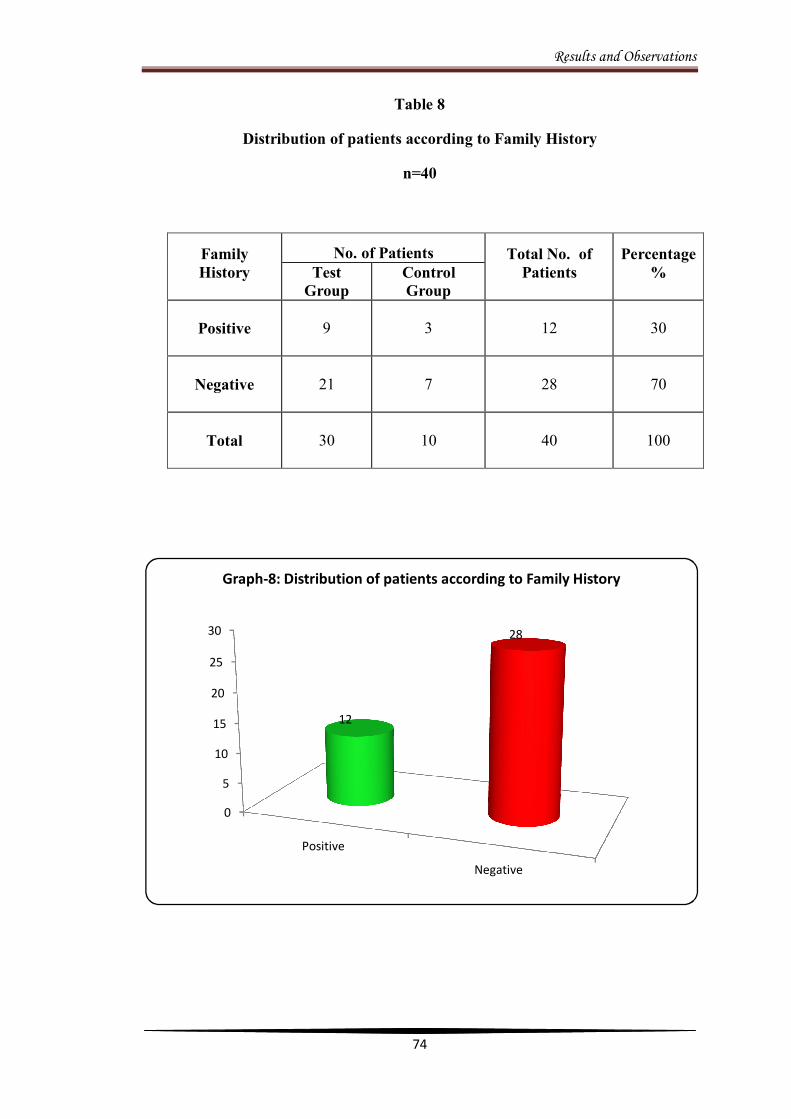
Results and Observations
74
Table 8
Distribution of patients according to Family History
n=40
Family History
No. of Patients Total No. of Patients
Percentage %
Test
Group Control Group
Positive
9
3
12
30
Negative
21
7
28
70
Total
30
10
40
100
0
5
10
15
20
25
30
Positive
Negative
12
28
Graph-8: Distribution of patients according to Family History

Results and Observations
75
Table 9
Distribution of patients according to Occupation
n=40
0123456789
1010
7
4
7
43
5
Figure-9: Distribution of patients according to Occupation
Occupation
N0. Of Patients Total No. of Patients
Percentage % Test Group Control Group
Students 9 1 10 25 Businessmen 3 4 7 17.5
Teachers 4 0 4 10 House wives 3 4 7 17.5
Tailors 4 0 4 10 Mechanics 2 1 3 7.5
Others 5 0 5 12.5 Total 30 10 40 100
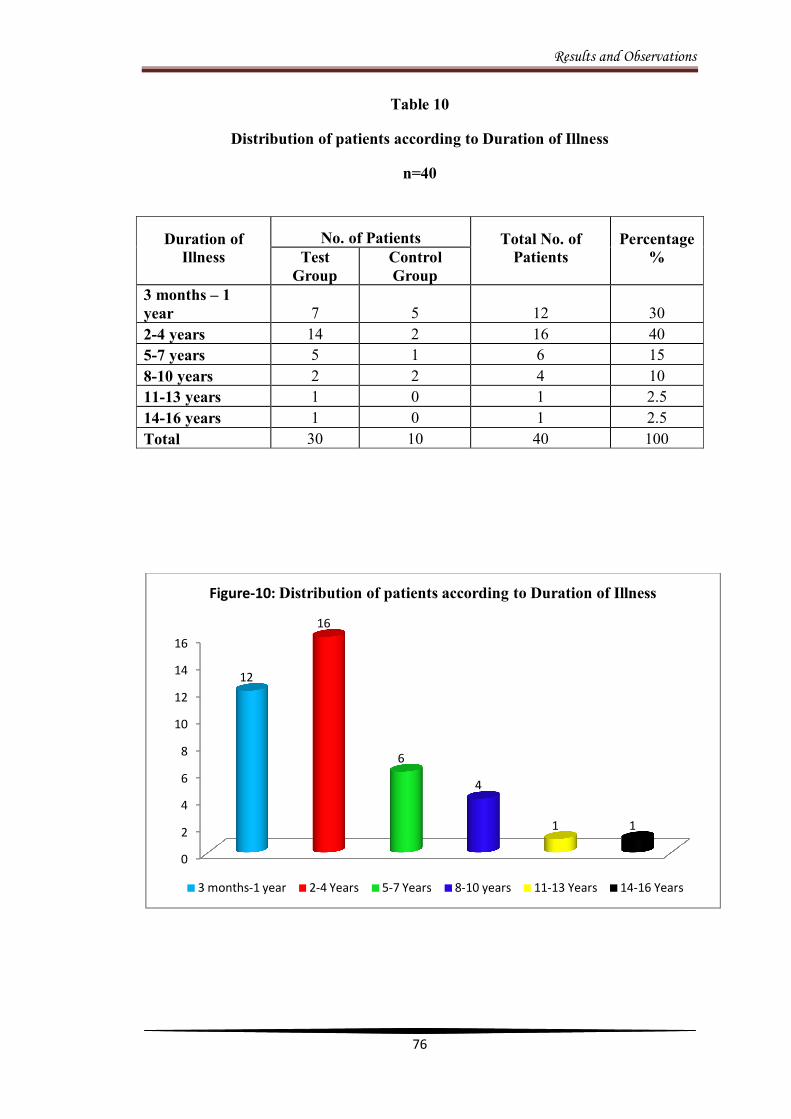
Results and Observations
76
Table 10
Distribution of patients according to Duration of Illness
n=40
0
2
4
6
8
10
12
14
16
12
16
6
4
1 1
Figure-10: Distribution of patients according to Duration of Illness
3 months-1 year 2-4 Years 5-7 Years 8-10 years 11-13 Years 14-16 Years
Duration of Illness
No. of Patients Total No. of Patients
Percentage %
Test
Group Control Group
3 months – 1 year 7 5 12 30 2-4 years 14 2 16 40 5-7 years 5 1 6 15 8-10 years 2 2 4 10 11-13 years 1 0 1 2.5 14-16 years 1 0 1 2.5 Total 30 10 40 100

Results and Observations
77
Table 11
Distribution of patients according to Treatment History
n=40
Treatment History
No. of Patients
Total No. of Patients
Percentage %
Test Group
Placebo Control Group
Positive
28
9
37
92.5
Negative
2
1
3
7.5
92.5%
7.5%
Graph-11: Distribution of patients according to Treatment History
Positive Negative
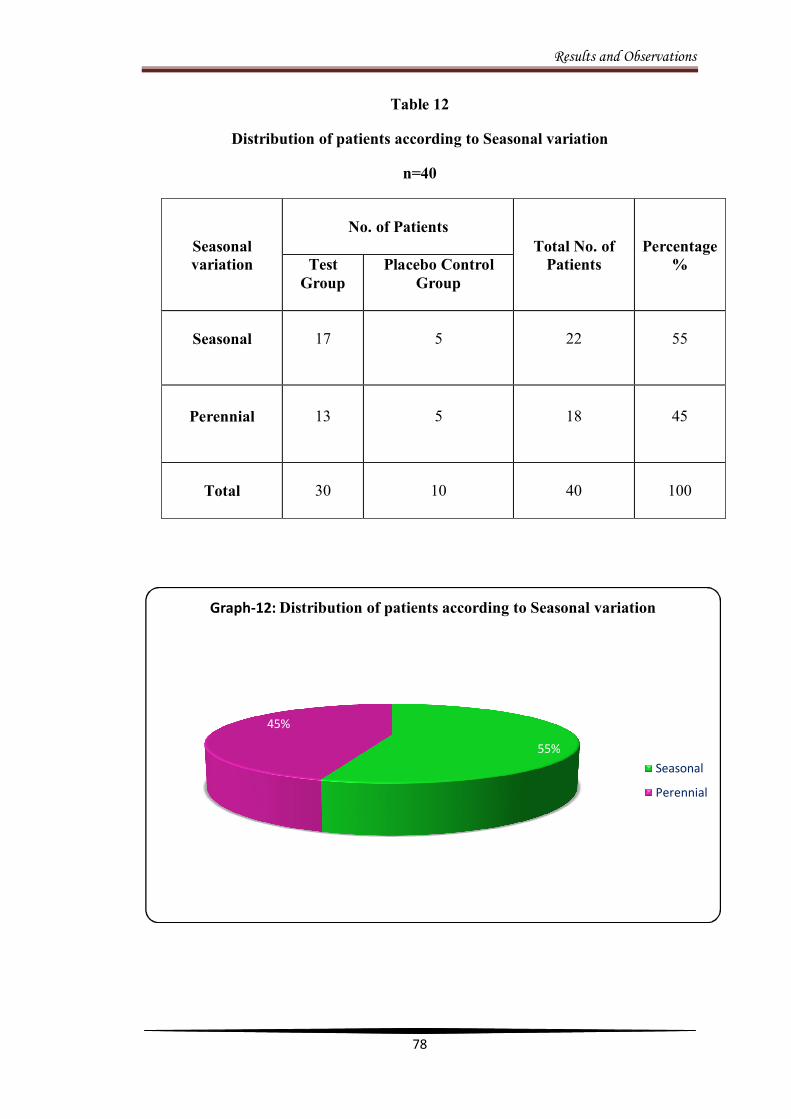
Results and Observations
78
Table 12
Distribution of patients according to Seasonal variation
n=40
Seasonal variation
No. of Patients
Total No. of Patients
Percentage %
Test Group
Placebo Control Group
Seasonal
17
5
22
55
Perennial
13
5
18
45
Total
30
10
40
100
55%
45%
Graph-12: Distribution of patients according to Seasonal variation
Seasonal
Perennial
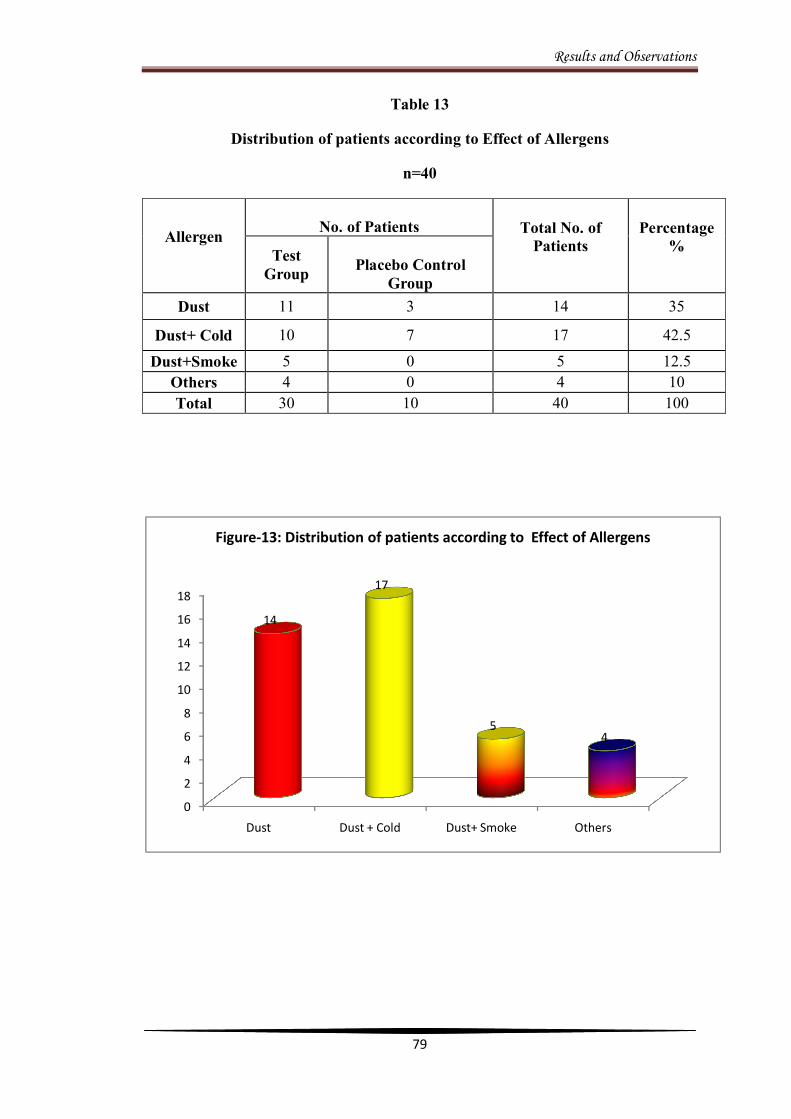
Results and Observations
79
Table 13
Distribution of patients according to Effect of Allergens
n=40
Allergen
No. of Patients Total No. of
Patients
Percentage %
Test Group
Placebo Control
Group Dust 11 3 14 35
Dust+ Cold 10 7 17 42.5
Dust+Smoke 5 0 5 12.5 Others 4 0 4 10 Total 30 10 40 100
0
2
4
6
8
10
12
14
16
18
Dust Dust + Cold Dust+ Smoke Others
14
17
54
Figure-13: Distribution of patients according to Effect of Allergens
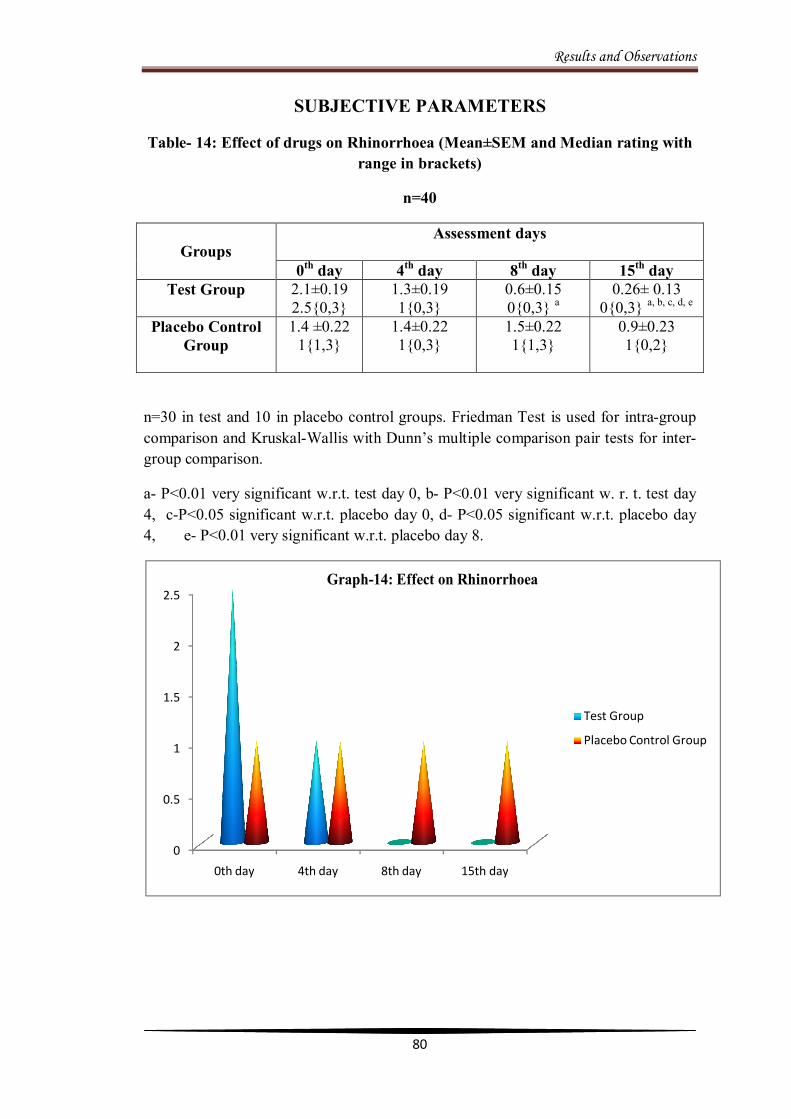
Results and Observations
80
SUBJECTIVE PARAMETERS
Table- 14: Effect of drugs on Rhinorrhoea (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day Test Group
2.1±0.19 2.5{0,3}
1.3±0.19 1{0,3}
0.6±0.15 0{0,3} a
0.26± 0.13 0{0,3} a, b, c, d, e
Placebo Control Group
1.4 ±0.22 1{1,3}
1.4±0.22 1{0,3}
1.5±0.22 1{1,3}
0.9±0.23 1{0,2}
n=30 in test and 10 in placebo control groups. Friedman Test is used for intra-group comparison and Kruskal-Wallis with Dunn’s multiple comparison pair tests for inter-group comparison.
a- P<0.01 very significant w.r.t. test day 0, b- P<0.01 very significant w. r. t. test day 4, c-P<0.05 significant w.r.t. placebo day 0, d- P<0.05 significant w.r.t. placebo day 4, e- P<0.01 very significant w.r.t. placebo day 8.
0
0.5
1
1.5
2
2.5
0th day 4th day 8th day 15th day
Test Group
Placebo Control Group
Graph-14: Effect on Rhinorrhoea
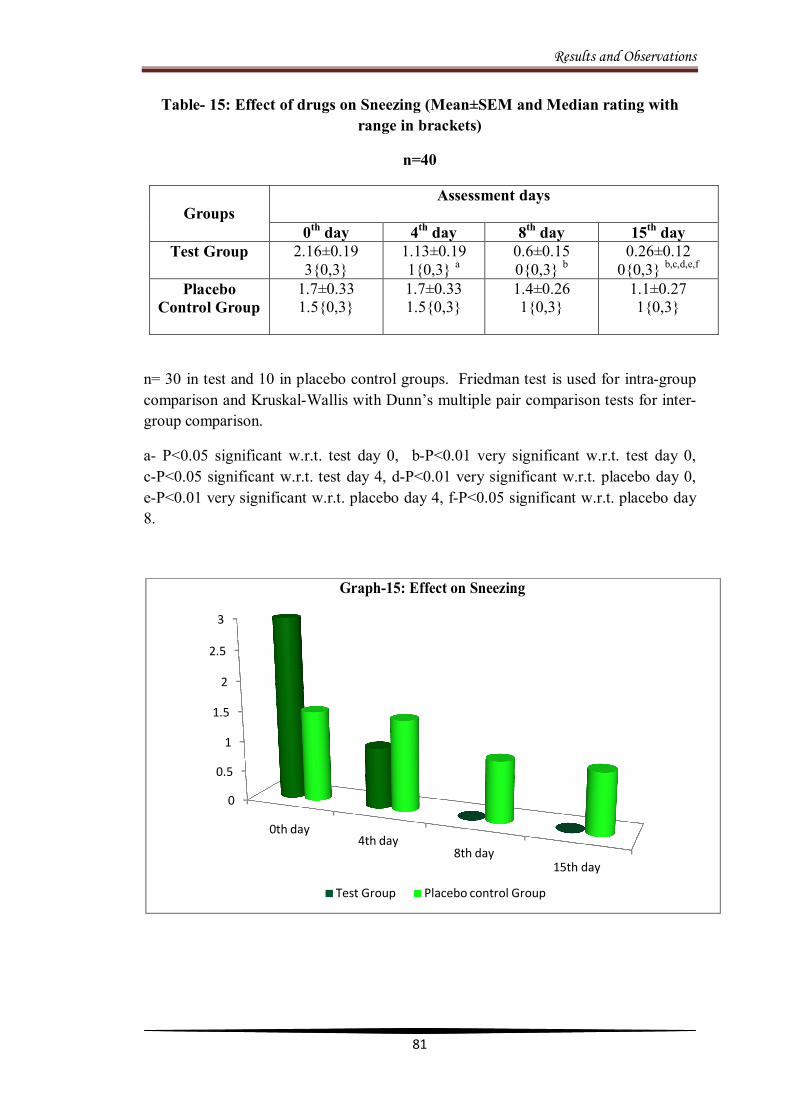
Results and Observations
81
Table- 15: Effect of drugs on Sneezing (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day Test Group
2.16±0.19
3{0,3} 1.13±0.19 1{0,3} a
0.6±0.15 0{0,3} b
0.26±0.12 0{0,3} b,c,d,e,f
Placebo Control Group
1.7±0.33 1.5{0,3}
1.7±0.33 1.5{0,3}
1.4±0.26 1{0,3}
1.1±0.27 1{0,3}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis with Dunn’s multiple pair comparison tests for inter-group comparison.
a- P<0.05 significant w.r.t. test day 0, b-P<0.01 very significant w.r.t. test day 0, c-P<0.05 significant w.r.t. test day 4, d-P<0.01 very significant w.r.t. placebo day 0, e-P<0.01 very significant w.r.t. placebo day 4, f-P<0.05 significant w.r.t. placebo day 8.
0
0.5
1
1.5
2
2.5
3
0th day4th day
8th day15th day
Test Group Placebo control Group
Graph-15: Effect on Sneezing
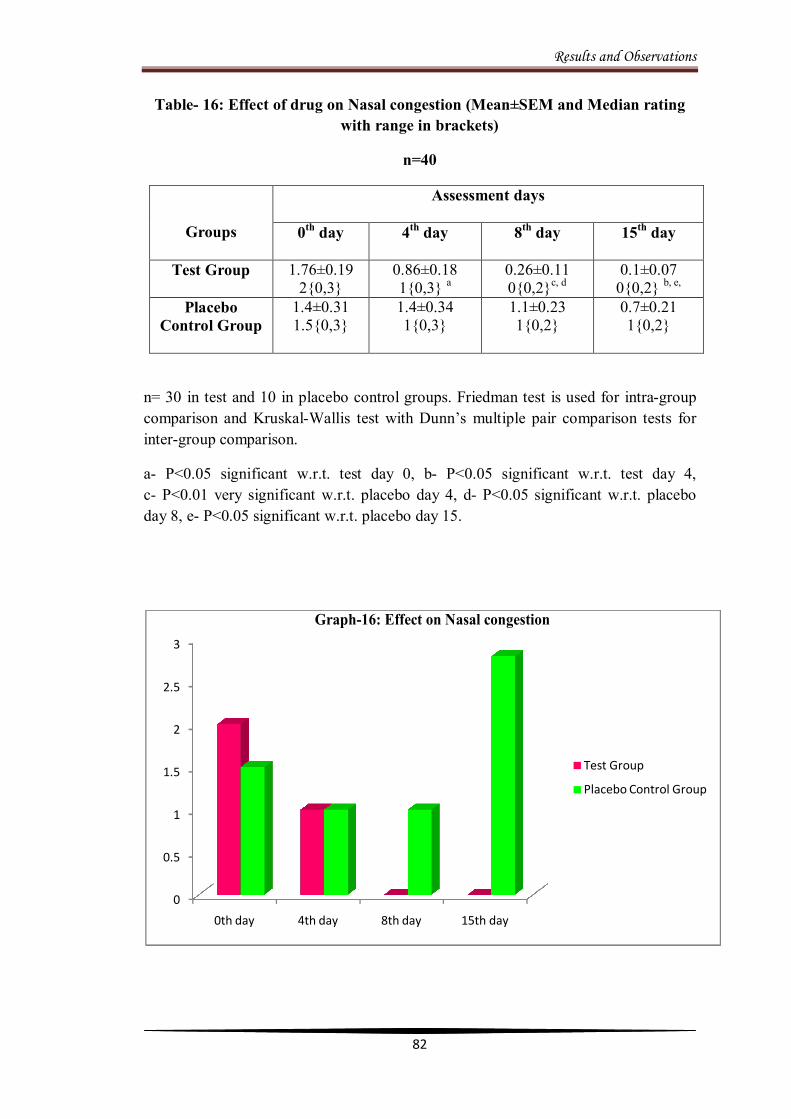
Results and Observations
82
Table- 16: Effect of drug on Nasal congestion (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day
Test Group
1.76±0.19 2{0,3}
0.86±0.18 1{0,3} a
0.26±0.11 0{0,2}c, d
0.1±0.07 0{0,2} b, e,
Placebo Control Group
1.4±0.31 1.5{0,3}
1.4±0.34 1{0,3}
1.1±0.23 1{0,2}
0.7±0.21 1{0,2}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis test with Dunn’s multiple pair comparison tests for inter-group comparison.
a- P<0.05 significant w.r.t. test day 0, b- P<0.05 significant w.r.t. test day 4, c- P<0.01 very significant w.r.t. placebo day 4, d- P<0.05 significant w.r.t. placebo day 8, e- P<0.05 significant w.r.t. placebo day 15.
0
0.5
1
1.5
2
2.5
3
0th day 4th day 8th day 15th day
Test Group
Placebo Control Group
Graph-16: Effect on Nasal congestion
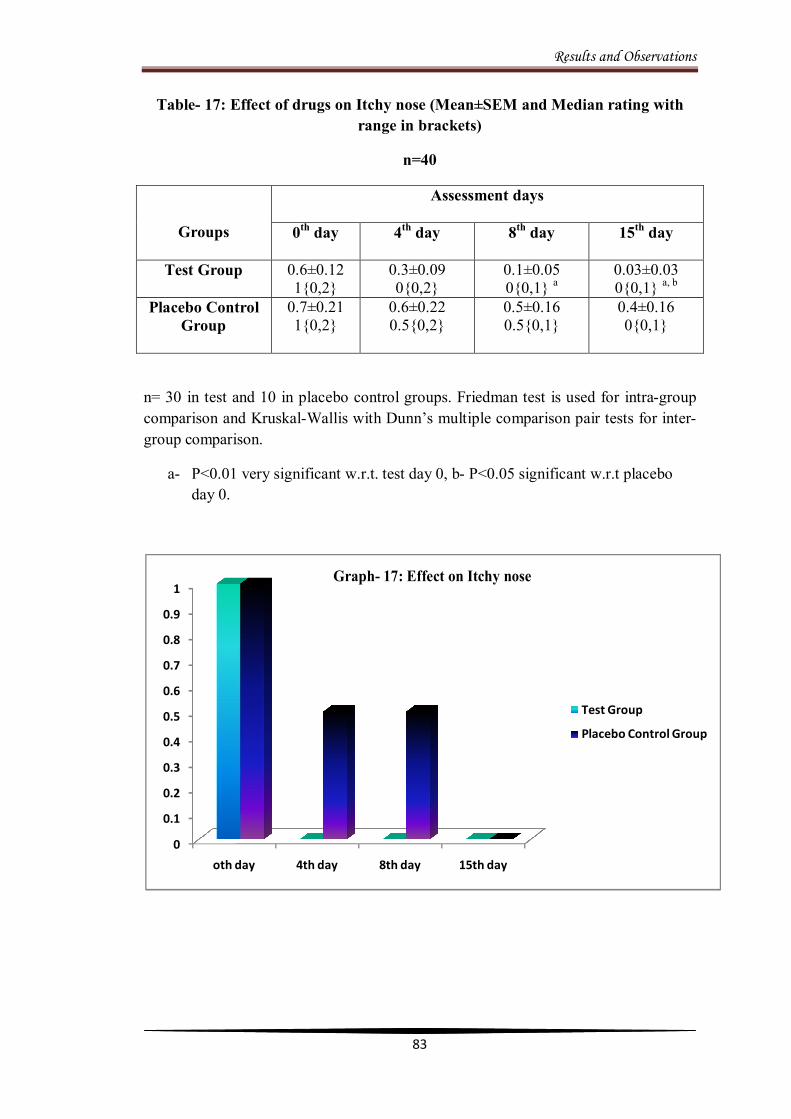
Results and Observations
83
Table- 17: Effect of drugs on Itchy nose (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day
Test Group
0.6±0.12 1{0,2}
0.3±0.09 0{0,2}
0.1±0.05 0{0,1} a
0.03±0.03 0{0,1} a, b
Placebo Control Group
0.7±0.21 1{0,2}
0.6±0.22 0.5{0,2}
0.5±0.16 0.5{0,1}
0.4±0.16 0{0,1}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis with Dunn’s multiple comparison pair tests for inter-group comparison.
a- P<0.01 very significant w.r.t. test day 0, b- P<0.05 significant w.r.t placebo day 0.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
oth day 4th day 8th day 15th day
Test Group
Placebo Control Group
Graph- 17: Effect on Itchy nose

Results and Observations
84
Table- 18: Effect of drugs on Itchy mouth or throat (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day
Test Group
0.6±0.11 1{0,2}
0.36±0.089 0{0,1}
0.2±0.07 0{0,1} a
0.03±0.03 0{0,1}
Placebo Control Group
0.4±0.16 0{0,1}
0.2±0.13 0{0,1}
0.3±0.15 0{0,1}
0.3±0.15 0{0,1}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis test with Dunn’s multiple comparison pair tests for inter-group comparison.
a- P<0.05 significant w.r.t. test day 0.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
oth day 4th day 8th day 15th day
Test Group
Placebo Control Group
Graph- 18: Effect on Itchy mouth or throat
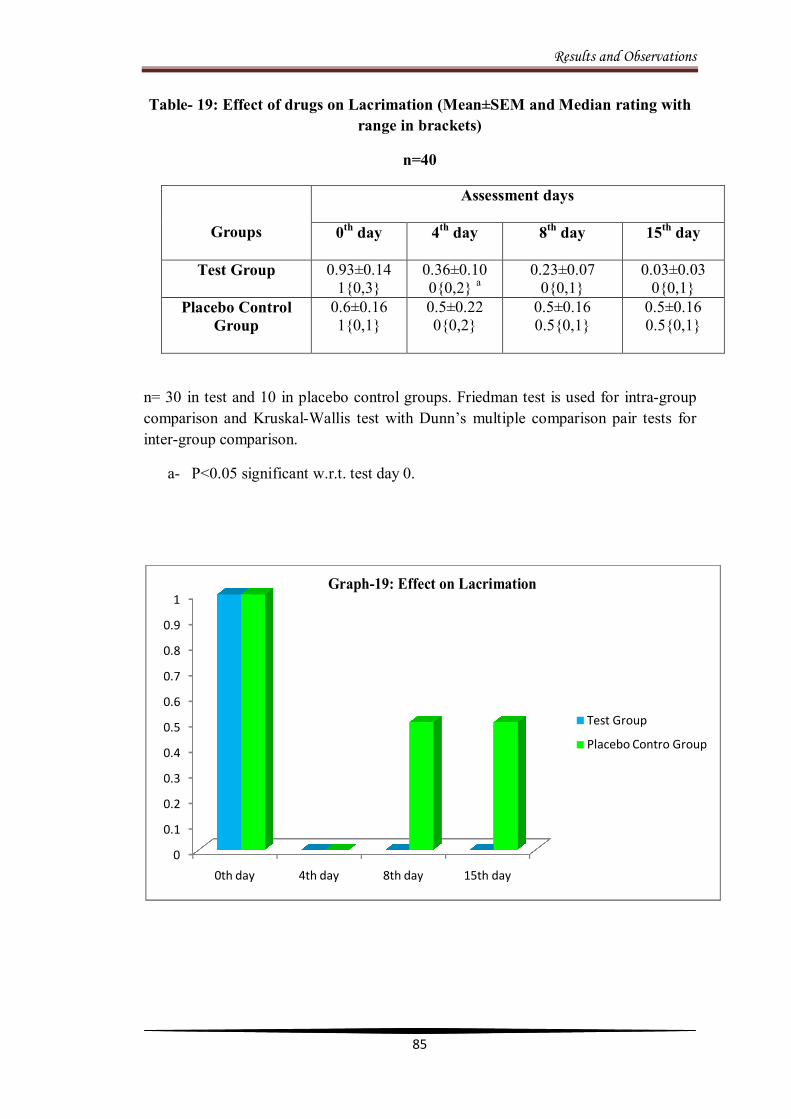
Results and Observations
85
Table- 19: Effect of drugs on Lacrimation (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day
Test Group
0.93±0.14 1{0,3}
0.36±0.10 0{0,2} a
0.23±0.07 0{0,1}
0.03±0.03 0{0,1}
Placebo Control Group
0.6±0.16 1{0,1}
0.5±0.22 0{0,2}
0.5±0.16 0.5{0,1}
0.5±0.16 0.5{0,1}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis test with Dunn’s multiple comparison pair tests for inter-group comparison.
a- P<0.05 significant w.r.t. test day 0.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0th day 4th day 8th day 15th day
Test Group
Placebo Contro Group
Graph-19: Effect on Lacrimation

Results and Observations
86
Table 20: Effect of drugs on Post nasal drip (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day
Test Group
0.66±0.15 0.5{0,3}
0.26±0.09 0{0,2}
0.10±0.05 0{0,1}
0±0.00 0{0,0} a, b, c
Placebo Control Group
1.00±0.36 1{0,3}
0.70±0.30 0.5{0,3}
0.80±0.29 1{0,3}
0.60±0.31 0{0,3}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis test with Dunn’s multiple comparison pair tests for inter-group comparison.
a- P<0.01 very significant w.r.t. test day 0, b- P<0.05 significant w.r.t. placebo day 0, c- P<0.05 significant w.r.t. placebo day 8.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0th day 4th day 8th day 15th day
Test Group
Placebo Control Group
Graph-20: Effect on Post nasal drip
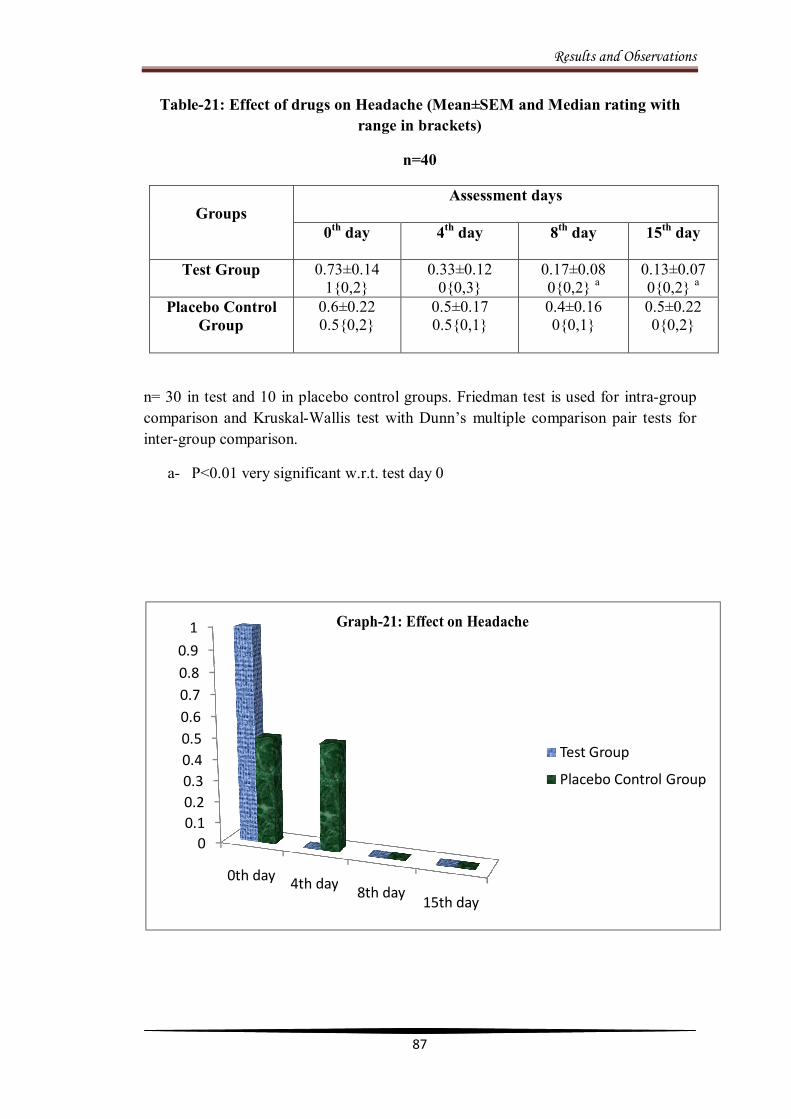
Results and Observations
87
Table-21: Effect of drugs on Headache (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Assessment days
0th day 4th day 8th day 15th day
Test Group
0.73±0.14 1{0,2}
0.33±0.12 0{0,3}
0.17±0.08 0{0,2} a
0.13±0.07 0{0,2} a
Placebo Control Group
0.6±0.22 0.5{0,2}
0.5±0.17 0.5{0,1}
0.4±0.16 0{0,1}
0.5±0.22 0{0,2}
n= 30 in test and 10 in placebo control groups. Friedman test is used for intra-group comparison and Kruskal-Wallis test with Dunn’s multiple comparison pair tests for inter-group comparison.
a- P<0.01 very significant w.r.t. test day 0
00.10.20.30.40.50.60.70.80.9
1
0th day 4th day 8th day15th day
Test Group
Placebo Control Group
Graph-21: Effect on Headache

Results and Observations
88
Table- 22: Effects of drugs on Nasal Smear for Eosinophils (NSFE) (Mean±SEM and Median rating with range in brackets)
n=40
Groups
Nasal Smear for Eosinophils Before treatment After treatment
Test Group
1.73±0.13 2{0,2}
0.03±0.09 a, 0{0,1}
Placebo Control Group
1.00±0.33 1{0,2}
0.8±0.33 0{0,2}
n= 30 in test and 10 in placebo control groups. Kruskal-Wallis test with Dunn’s multiple comparison pair tests are used for inter-group comparison.
a- P<0.001 extremely significant w.r.t. test before treatment,
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
BT AT
Test Group
Placebo Control Group
Graph-22: Effect on NSFE
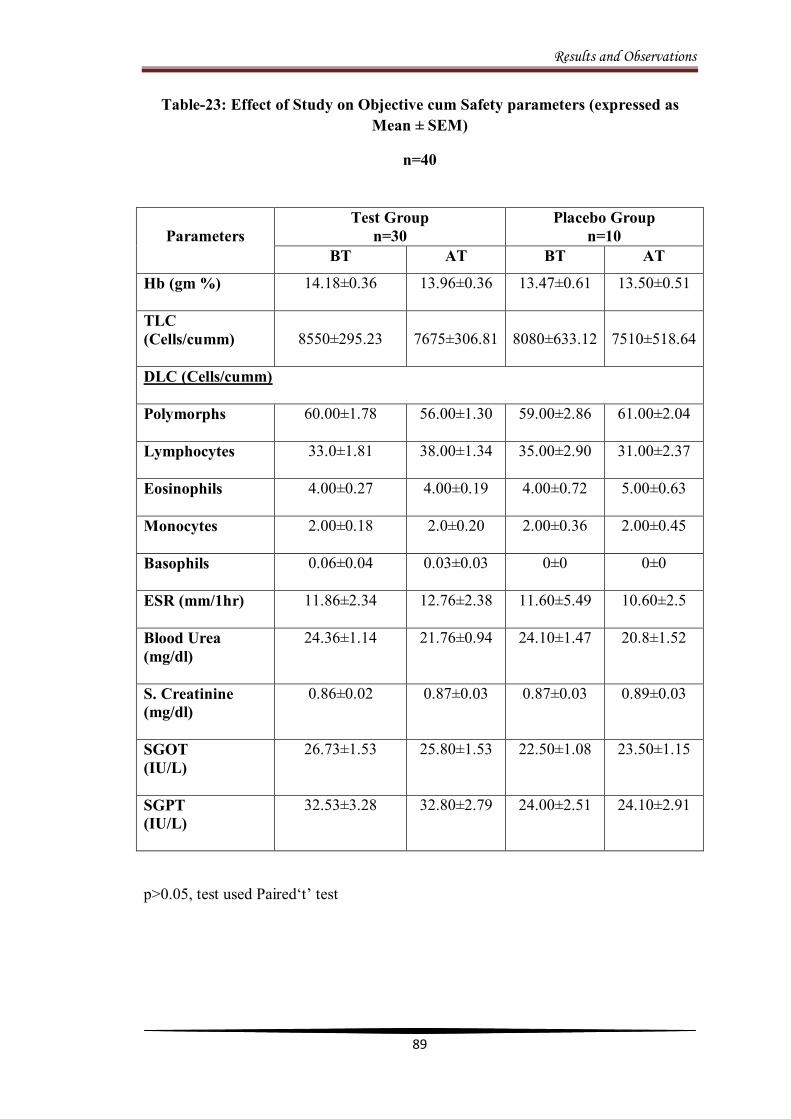
Results and Observations
89
Table-23: Effect of Study on Objective cum Safety parameters (expressed as Mean ± SEM)
n=40
p>0.05, test used Paired‘t’ test
Parameters
Test Group n=30
Placebo Group n=10
BT AT BT AT
Hb (gm %)
14.18±0.36 13.96±0.36 13.47±0.61 13.50±0.51
TLC (Cells/cumm)
8550±295.23
7675±306.81
8080±633.12
7510±518.64
DLC (Cells/cumm)
Polymorphs
60.00±1.78
56.00±1.30
59.00±2.86
61.00±2.04
Lymphocytes
33.0±1.81
38.00±1.34
35.00±2.90
31.00±2.37
Eosinophils
4.00±0.27
4.00±0.19
4.00±0.72
5.00±0.63
Monocytes
2.00±0.18
2.0±0.20
2.00±0.36
2.00±0.45
Basophils
0.06±0.04
0.03±0.03
0±0
0±0
ESR (mm/1hr)
11.86±2.34 12.76±2.38 11.60±5.49 10.60±2.5
Blood Urea (mg/dl)
24.36±1.14 21.76±0.94
24.10±1.47 20.8±1.52
S. Creatinine (mg/dl)
0.86±0.02 0.87±0.03 0.87±0.03 0.89±0.03
SGOT (IU/L)
26.73±1.53 25.80±1.53 22.50±1.08 23.50±1.15
SGPT (IU/L)
32.53±3.28 32.80±2.79 24.00±2.51 24.10±2.91

Results and Observations
90
Table-24: Effect of drugs on TSSS (Mean±SEM)
n=40
Group TSSS Before treatment After treatment
Test Group 9.6±0.64 0.90±0.32 a, b, c
Placebo Control
Group 7.80±1.03 5.00±0.94
n=30 in test and 10 in placebo control groups. Paired ‘t’ test is used for intra group comparison and Kruskal-Wallis test with Dunn’s multiple pair comparison tests for inter group comparison.
a- P<0.01 very significant w.r.t. test BT, b- P<0.01 very significant w.r.t. placebo BT, c- P<0.05 significant w.r.t. placebo AT.
0
1
2
3
4
5
6
7
8
9
10
BT AT
9.6
0.9
7.8
5Test Group
Placebo Control Group
Graph-24: Effect of drugs on TSSS

Results and Observations
91
Table-25
Overall Effect on the study Based on TSSS and NSFE
n=40
Groups
Sample
Size
Before Treatment After Treatment
NSFE
(+)
NSFE
(-)
TSSS
(Mean)
NSFE
(+)
NSFE
(-)
TSSS
(Mean)
Test Group
30
26
4
9.6
1*
4
0.9
Placebo
Control
Group
10
5
5
7.8
5
5
5.0
Total
40
31
9
17.4
5
9
5.9
* Significantly reduced in numbers.
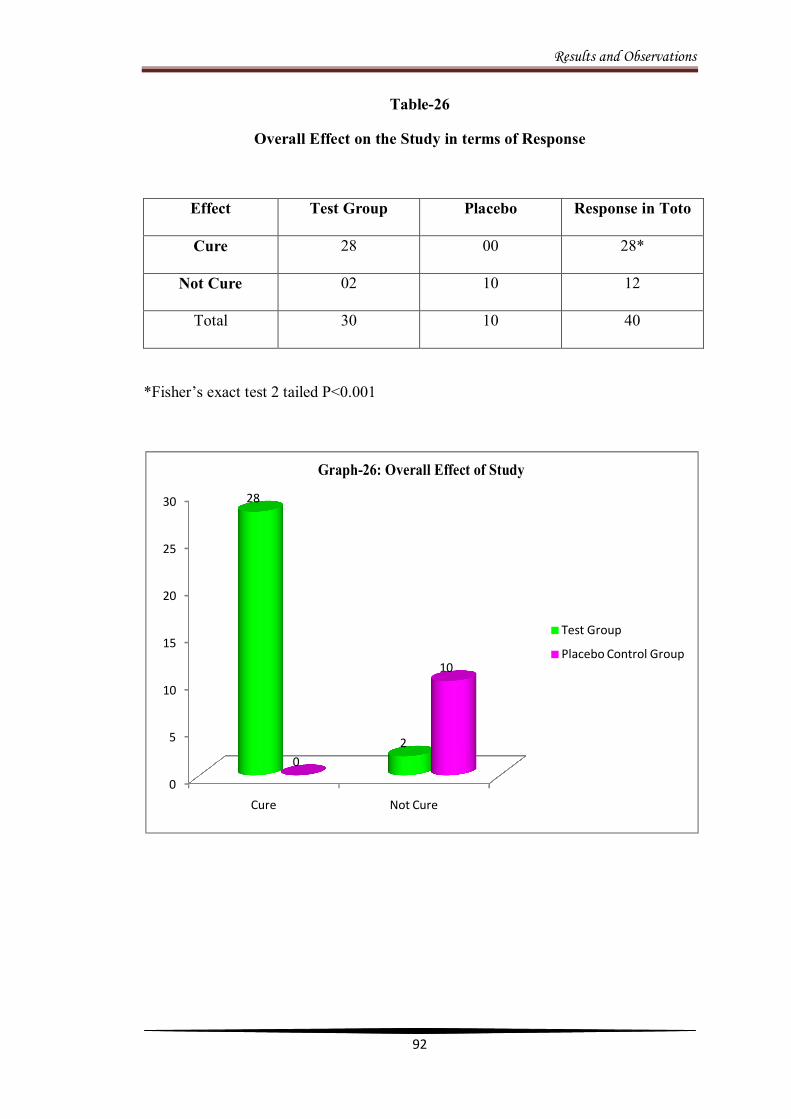
Results and Observations
92
Table-26
Overall Effect on the Study in terms of Response
Effect Test Group Placebo Response in Toto
Cure 28 00 28*
Not Cure 02 10 12
Total 30 10 40
*Fisher’s exact test 2 tailed P<0.001
0
5
10
15
20
25
30
Cure Not Cure
28
20
10
Test Group
Placebo Control Group
Graph-26: Overall Effect of Study

Results and Observations
93
Table- 27
Baseline characteristics of the research sample
n=40
Groups Characteristics
Test Group (n=30)
Placebo Control Group (n=10)
Age
29.60±3.39
29.86±1.83
Gender- Male Female
19
11
6
4
Haematological Value
Hb (gm %)
14.18±0.36 13.47±0.60
TLC (Cells/Cumm)
8550.00±295.23 8080.00±633.12
DLC (%): Polymorphs Lymphocytes Eosinophils Monocytes Basophils
60.00±1.784
33.00±1.81
4.00±0.27
2.00±0.18
0.0666±0.05
59.00±2.86
35.00±2.90
4.00±0.72
2.00±0.36
0.000±0.00
ESR (mm/1hr) 11.86±2.34 11.60±5.49 NSFE
1.73±0.13 1.00±0.33
Blood Urea (mg/dl)
24.36±1.14 24.10±1.47
S. Creatinine (mg/dl)
0.86±0.02 0.87±0.03
SGOT (IU/L)
26.73±1.53 22.50±1.08
SGPT (IU/L)
32.53±3.28 24.00±2.51
P>0.05, test used unpaired ‘t’ test for each parameter.

DISCUSSION

Discussion
94
DISCUSSION
The present study was a randomized single blind placebo control clinical trial,
designed to evaluate the safety and efficacy of a Unani formulation in the treatment of
Nazla Haar on scientific basis and modern parameters. This study was conducted at
National Institute of Unani Medicine Hospital, Bangalore over a period of 9 months
from March 2011 to December 2011. A total of 55 patients were registered for
screening, out of which 15 patients did not fulfill the inclusion criteria hence excluded
from the study, and remaining 40 patients completed the course of treatment, out of
which 30 allocated to test and 10 to placebo control groups.
Test group patients were given Unani formulation, which consists of Behidana,
Unnab, and Sapistan in the form of Joshanda along with Sharbate Banafsha 25ml
orally twice a day for 15 days while, placebo control group was treated by caramel
syrup with the same quantity and duration. The severity of subjective parameters
rhinorrhoea, sneezing, nasal congestion, itchy nose, itchy mouth or throat,
lacrimation, post nasal drip and headache were rated on 4 point scale (0-absent, 1-
mild, 2-moderate and 3- severe). These scores were summed in each patient at
assessment point on 0th, 4th, 8th and 15th day to obtain a Total Symptom Severity Score
(TSSS), and the objective parameter NSFE was assessed before and after treatment.
The observations recorded from the trial have been depicted in tables and graphs. The
discussion on the data showing efficacy of the treatment on various subjective and
objective parameters along with demographic data is being presented below in order
to draw inference and to arrive at a conclusion.
In this study a maximum of 37.5% patients were observed in age group of 21-30 years
followed by 25% in age group 31-40 years, 20% patients were observed in 13-20
Discussion
95
years of age and 17.5% in 41-50 years (Table-1 and Graph 1). This study shows a
high incidence of disease in patients between the age of 3rd, 4th and 2nd decade of life.
This study partly exhibit the prevalence of rhinitis is observed in 2nd decade according
to Kumar & Clerk. The mean age of subjects enrolled in the study was found with
29.8 years, which corresponds with the incidence of mean age (29.6 years) from the
study reported by Maiti R et al 112 (2010).
Out of 40 patients enrolled into the study 62.5% i.e., 25 were males and 37.5% i.e., 15
were in females (Table-2 and Graph- 2). Sex wise incidence of the disease as per the
studies of Kurowski M et al 115 (2004) males 79.2%, females 20.8% and Aubier M et
al 116 (2001) 83.0% males and 16.7% females respectively reveal similar evidence.
No credible data is available to demonstrate the existence of this disease among a
particular community in the society. However, this study represents predominance
among Hindu patients with 55% followed by Muslims 42.5% and Christian 2.5%
(Table- 4 and Graph- 4).
Dietary habit was considered on the basis of consuming regularly vegetarian and
non-vegetarian type of diet. Out of 40 patients, 90% were recorded to be of non-
vegetarian and 10% vegetarian (Table- 5 and Graph- 5). This finding is in accordance
with the study by Jan RH and Wen SH 117 (2007) that allergic diseases were less
commonly reported among children consuming a moderate vegetarian diet. As per the
description available in Unani literature, people fond of eating non-vegetarian diet
found to suffer more likely with Nazla Haar. 21
In this study the highest prevalence was observed in middle income group 87.5%,
followed by upper 7.5% and only 5% lower group (Table-6 and Graph-6). These
findings reveal that the middle income group was mostly affected, with least number

Discussion
96
of patients in lower income group; it is evident that this is a disease of affluent with
the reference to Jan RH and Wen SH 117 (2007) and http://www.update.com.
Moreover, this study reflects that more number of patients attending the OPD is from
middle income group.
This study revealed that 60% patients were found to be Balghami and 40% were
Damavi Mizaj (Table 7 and Graph- 7). It is contrary to the description of the cause of
the disease according to Unani system of medicine, although it was defined that
certain factors such as extrinsic and intrinsic will play a role in the cause of the
disease, irrespective of individuals own temperament.
Though this study represents only 30% of positive family history and 70% with
negative (Table- 8 and Graph-8). This observation correspond with the study of
Lundback B 44 (1998) two to six fold for developing rhinitis over adults without a
family history. But according to Dhingra, the chances of children developing allergy
are 20% and 47% respectively, if one or both parents suffer from allergic diathesis. 25
This study revealed occupation of the patients as 25% students, 17.5% each in house
wives and businessmen, 12.5% others, 10% each in teachers and tailors, and 7.5%
mechanics. This study finding is in accordance with the study of Gelis N et al 118
(2007) house wives, public services employees and private employees appear to be
allergic in significantly higher percentage than others (Table- 9 and Graph-9).
This study reported a maximum of 40% patients had 2- 4 years of duration of illness,
followed by 30% with 3 months to 1 year, 15% with 5-7years, 10% with 8-10 years
and 2.5% with 11-16 years of duration (Table 10 and Graph-10). This indicates that
the disease is chronic and resilient in nature and progress slowly. This observation is
in accordance with the findings observed by Kurowski M et al 115 (2004) rhinitis
Discussion
97
symptoms for 2 or more years , Majani G et al 119 (2001) more than 2 years of disease
and Aubier M et al 116 (2001) 2 years or more of duration of symptoms.
Out of 40 patients studied, 55% were found suffering from seasonal allergic rhinitis
and 45% from perennial allergic rhinitis (Table 12 and Graph- 12). This finding is in
consonance with the observation of the study conducted by Alyasin S and Amin R 120
(2007) i.e., 52% seasonal, and 48% perennial along with other mixed types.
Among 40 patients, 42.5% were found allergic to dust and cold, 35% allergic to dust
alone, 12.5% were allergic to dust and smoke, and 10% allergic to others (Table 13
and Graph-13).
Effect of study on subjective parameters
The effect of study on various subjective parameters such as Rhinorrhoea,
Sneezing, Nasal congestion, Itchy nose, Itchy mouth or throat, Lacrimation,
Post nasal drip and Headache were assessed on 0th , 4th , 8 t h and 15th day, and
evaluated on the basis of TSSS an arbitrary grading score scale for severity ranges
from 0 to 3.
Effect on rhinorrhoea:
In test group the median score with range were observed as 2.5 [0, 3], 1[0, 3], 0[0,3],
and 0[0,3] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of rhinorrhoea, very significantly with p<0.01,
this reduction was found on 8th day when compared with median score of 0th day. In
placebo control group the median score with range were observed as 1 [1, 3], 1[0, 3],
1[1,3], and 1 [0, 2] respectively. Intra group comparison revealed that there was no
significant reduction in rhinorrhoea severity till 15th day when compared with 0th
day.
Discussion
98
When median score of the both groups test and placebo were compared with each
other, it was found that there was significant (p<0.05) and very significant (p<0.001)
reduction in severity of rhinorrhoea on 15th day of test with respect to 0th day and 8th
day placebo respectively (Table 14 and Graph-14). This result indicated that the test
drug is effective in reducing rhinorrhoea. This improvement might be due to the
Qabiz action of Behidana and Lazoojat of Banafsha. These results were claimed and
documented by Najmul Ghani. 67
Effect on sneezing:
In test group the median score with range were observed as 3 [0, 3], 1[0, 3], 0[0,3],
and 0[0,3] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of sneezing, significantly with p<0.05, this
reduction was found on 4th day when compared with median score of 0th day. In
placebo control group the median score with range were observed as 1.5 [0, 3], 1.5[0,
3], 1[0, 3], and 1 [0, 3] respectively. Intra group comparison revealed that there was
no significant reduction in sneezing severity till 15th day when compared with 0th
day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was very significant (p<0.01) reduction in severity of
sneezing on 15th day with respect to 4th day placebo (Table 15 and Graph- 15). The
results showed that the test drug is effective in controlling sneezing. This effect may
be due to anti-allergic property of Behidana and Unnab, which is in conformity with
the properties of the drugs described by Khare CP, Baar EW et al and Su et al.76, 86, 92
Discussion
99
Effect on nasal congestion
In test group the median score with range were observed as 2[0, 3], 1[0, 3], 0[0,2],
and 0[0,2] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of nasal congestion, significantly with p<0.05, this
reduction was found on 4th day when compared with median score of 0th day. In
placebo control group the median score with range were observed as 1.5 [0, 3], 1[0,
3], 1[0, 2], and 1 [0, 2] respectively. Intra group comparison revealed that there was
no significant reduction in nasal congestion severity till 15th day when compared
with 0th day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was very significant (p<0.01) reduction in severity of
nasal congestion on 8th day with respect to 4th day placebo (Table 16 and Graph-16).
The present study revealed that the test drug is effective in relieving nasal
congestion. The improvement might be due to Mulattif action of Behidana, Unnab,
Sapistan and Banafsha; muhallil of Banafsha. These functions are in accordance
with the description given by Najmul Ghani, Kabeeruddin and Anonymous. 67, 69, 70,
72, 85
Effect on itchy nose
In test group the median score with range were observed as 1 [0, 2], 0[0, 2], 0[0,1],
and 0[0,1] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of itchy nose, very significantly with p<0.01, this
reduction was found on 8th day when compared with median score of 0th day. In
placebo control group the median score with range were observed as 1 [0, 2], 0.5 [0,
2], 0.5 [0, 1], and 0 [0, 1] respectively. Intra group comparison revealed that there
Discussion
100
was no significant reduction in itchy nose severity till 15th day when compared with
0th day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was significant (p<0.05) reduction in severity of itchy
nose on 15th day with respect to 0th day placebo (Table 17 and Figure 17). This
study exposed that the test drug is useful in reducing itchy nose. The effect may be
due to Musakkine hararat and Mufarrih properties of Behidana; Musaffie khoon and
Ta’deeluddam actions of Unnab; Muaddile safra and Murattib of Banafsha. The
above mentioned drugs are in accordance with the description given by Ibn Rushd,
Najmul Ghani, Kabeeruddin, Hakeem MAH and Anonymous. 8, 67, 69, 70, 81, 84
Effect on itchy mouth or throat
In test group the median score with range were observed as 1 [0, 2], 0 [0, 1], 0[0, 1],
and 0[0, 1] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of itchy mouth or throat, significantly with
p<0.05, this reduction was found on 8th day when compared with median score of 0th
day. In placebo control group the median score with range were observed as 0 [0,1],
0[0, 1], 0[0, 1], and 0 [0, 1] respectively. Intra group comparison revealed that there
was no significant reduction in itchy mouth or throat severity till 15th day when
compared with 0th day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was no significant reduction in severity of itchy mouth
or throat with respect to placebo (Table 18 and Graph-18). It was observed that the
test drug has the property to control itchy mouth or throat, which may be due to
Musakkine hararat and Mufarrih actions of Behidana; ta’deeluddam prosperity of

Discussion
101
Unnab; Muaddile safra and Murattib actions of Banafsha. These findings of above
mentioned drugs are in accordance with the description given by Ibn Rushd, Najmul
Ghani, Kabeeruddin, Hakeem MAH and Anonymous. 8, 69, 67, 70, 81, 84
Effect on lacrimation
In test group the median score with range were observed as 1 [0, 3], 0[0, 2], 0[0,1],
and 0[0,1] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of lacrimation, significantly with p<0.05, this
reduction was found on 4th day when compared with median score of 0th day. In
placebo control group the median score with range were observed as 1 [0, 1], 0[0, 2],
0.5 [0, 1], and 0.5 [0, 1] respectively. Intra group comparison revealed that there
was no significant reduction in lacrimation severity till 15th day when compared with
0th day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was no significant reduction in severity of lacrimation
with respect to placebo control (Table 19 and Graph-19). The result revealed that
the test drug was effective in alleviating the symptom lacrimation, which may be due
to the properties of Musakkine hararat, Qabiz and Mufarrih of Behidana; Lazoojat
of Banafsha. These results coincide with the findings documented by Najmul Ghani,
Kabeeruddin and Anonymous. 67, 69, 70, 81
Effect on post nasal drip
In test group the median score with range were observed as 0.5 [0, 3], 0[0, 2], 0[0,1]
and 0[0,0] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of post nasal drip, very significantly with p<0.01,
this reduction was found on 15th day when compared with median score of 0th day.
Discussion
102
In placebo control group the median score with range were observed as 1 [0, 3], 0.5
[0, 3], 1[0,3], and 0 [0, 3] respectively. Intra group comparison revealed that there
was no significant reduction in post nasal drip severity till 15th day when compared
with 0th day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was significant (p<0.05) reduction in severity of post
nasal drip on 15th day with respect to 0th day of placebo (Table 20 and Graph-20).
The result evidence that the test drug was effective in reducing the symptom post
nasal drip, which might be due to Dafe nazla property of Behidana. This result is in
accordance with the properties of the drugs suggested by Anonymous. 69, 70
Effect on headache
In test group the median score with range were observed as 1 [0, 2], 0[0, 3], 0[0, 2]
and 0[0, 2] respectively. When intra group comparison was made, it was found that
the test drug reduced the severity of headache, very significantly with p<0.01, this
reduction was found on 8th day when compared with median score of 0th day. In
placebo control group the median score with range were observed as 0.5 [0, 2], 0.5 [0,
1], 0[0, 1] and 0 [0, 2] respectively. Intra group comparison revealed that there was
no significant reduction in headache severity till 15th day when compared with 0th
day.
When median score of the both groups test and placebo were compared with each
other, it was found that there was no significant reduction in severity of headache
with respect to placebo (Table 21 and Graph-21). It was observed that the test drug
was more effective in alleviating the symptom headache. This improvement might
be due to Musakkin action of Unnab and Sapistan; Mulayyane akhlate raqeeqa of
Discussion
103
Unnab; Muhallile warm and Munawwim of Banafsha. These findings of above
mentioned drugs are in accordance with the description given by Ibn Rushd, Najmul
Ghani, Kabeeruddin, Hakeem MAH and Anonymous. 8, 67, 69, 70, 81, 84, 94
The overall improvement in the disease reflected in the form of regression of
various symptoms may be due to the t emperament and different pharmacological
effects of the drugs like Dafe nazla, Muzliq, Mufarrih, Mulattif, Musakkine hararat,
Qabiz, Mufattih, Munzije akhlate ghaleeza, Mulayyane akhlate raqeeqa, Munaffise
balgham, Muhallile warm, Muaddile safra, Ta’deeluddam, Lazoojat, and Murattib
wa munawwim of various ingredients of test formulation which contain Behidana,
Unnab, Sapistan and Banafsha. The beneficial effect of test formulation is
corroborated by the use of these drugs in a variety of respiratory diseases by Unani
scholars is in consonance with the pharmacological actions of drugs described in
Unani literature. Certain experimental studies have shown that Behidana (Cydonia
oblonga) has an inhibitory effect on broad range of the late phase immune reactions
of mast cells, 87 Unnab (Zizyphus jujuba) possesses anti allergic and anti-
inflammatory properties, 92, 99 Sapistan (Cordia dichotoma) has analgesic, anti-
inflammatory, expectorant and hepatoprotective properties, 101-103 similarly the
aqueous extract of Banafsha (Viola odorata) has anti-inflammatory property equal to
corticosteroids in the treatment of inflammatory conditions of the lung. 107
Effect on NSFE
Out of 30 only 26 patients in test and 5 out of 10 in placebo control groups were
positive with nasal smear for eosinophils (NSFE) on baseline day of before
treatment. After the completion of treatment i.e., day 15th, in test group, 1 patient’s
NSFE was found still positive with reduction in number in comparison to baseline,
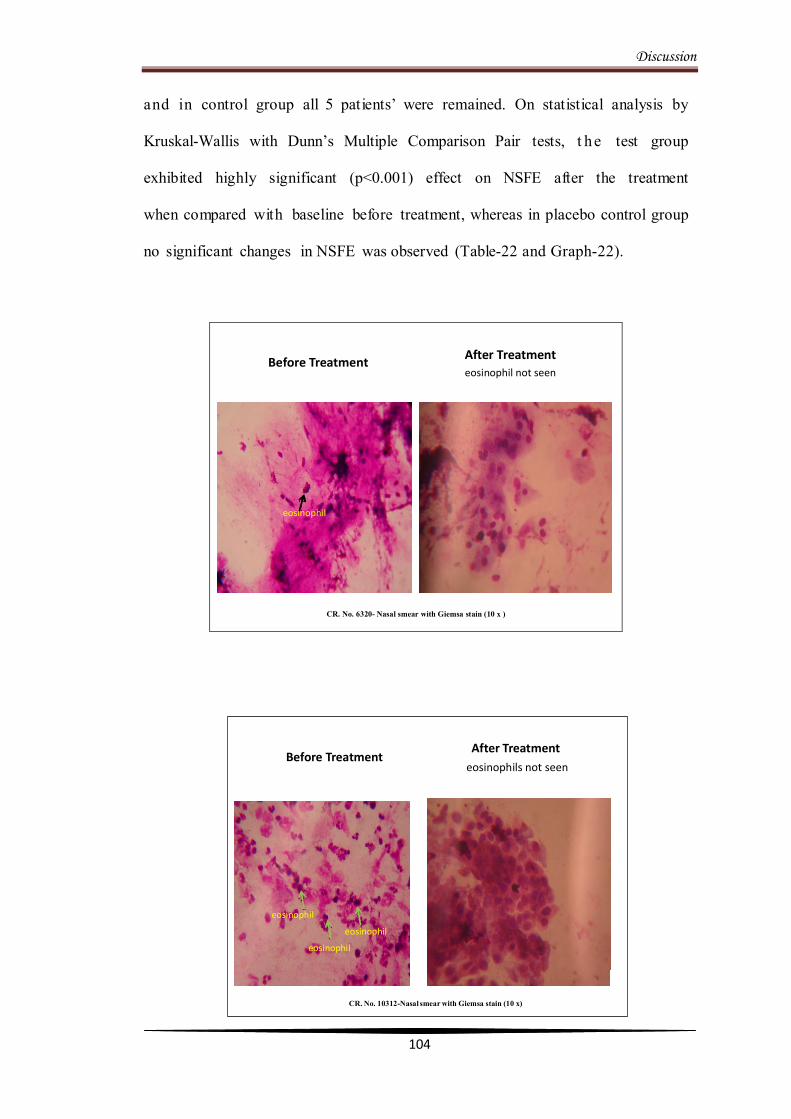
Discussion
104
and in control group all 5 patients’ were remained. On statistical analysis by
Kruskal-Wallis with Dunn’s Multiple Comparison Pair tests, t he test group
exhibited highly significant (p<0.001) effect on NSFE after the treatment
when compared with baseline before treatment, whereas in placebo control group
no significant changes in NSFE was observed (Table-22 and Graph-22).
Before Treatment After Treatment eosinophil not seen
eosinophil
CR. No. 6320- Nasal smear with Giemsa stain (10 x )
Before TreatmentAfter Treatment
eosinophils not seen
eosinophil
eosinophil
eosinophil
CR. No. 10312-Nasal smear with Giemsa stain (10 x)
Discussion
105
Overall effect on Study
The overall effect of the study is determined based on the TSSS of Mean ± SEM of
subjective parameters. The TSSS in test group before treatment was 9.60 ±0.64 and
0.90±0.32 after treatment, whilst it was 7.80±1.03 and 5.00±0.94 respectively in
placebo control group. When the Mean ± SEM of TSSS in both groups were
compared statistically by using Paired‘t’ test for intra group, and Kruskal–Wallis
with post Dunn’s Multiple Comparison tests for intergroup. It was observed that the
test group was found very significant with p value <0.01 after the treatment when
compared with placebo control and test before treatment (Table-24 and Graph-24).
Moreover, the effect of the study determined in terms of CURE and NOT CURE is
based on the difference of TSSS individual subjective symptoms score along with the
effect on NSFE before treatment was compared with after treatment (Table-25), those
found to be between 0 - ≤ 2 with negative or significant reduction in the number of
NSFE is considered as “cure” , whereas, any change of TSSS with > 2 or remain
unchanged along with no significant reduction or presence of eosinophils is
considered as “not cure”.
In test group out of 30 patients 28 (93.33%) were found < 2 TSSS along with negative
eosinophils, whilst, the placebo group patients were remained positive eosinophils
along with marginal reduction in TSSS without significant change in eosinophils
(Table-25). When the efficacy of both groups in terms of Cure and Not cure was
compared statistically employing Fisher’s Exact test-2 tailed, it was observed that test
drug was highly significant (p<0.001) in comparison to placebo group (Table-26 and
Graph-26).
Discussion
106
Safety evaluation of the Drugs
In order to determine safety of the test drug, parameters like Haemogram, ESR, LFT
and RFT were carried out at base line and at the end of the treatment. The data were
analyzed by using Paired‘t’ test. There was no significant difference observed
(p>0.05) between pre and post treatment for each safety parameters (Table-23).
Hence, it is suggested that the formulation can be used safely at the prescribed
therapeutic dose.

CONCLUSION
Conclusion
107
CONCLUSION
Nazla Haar is a common disease distributed worldwide with prevalence rate that
varies from 2% to 20%. Recently WHO has estimated that 400 million people in the
world suffer from allergic rhinitis. Incidence rates in Asia-Pacific are estimated to be
as high as 48% and rising as societies become more urbanized and adopt western
lifestyles. The symptoms of the disease may improve with advancing age, but the
disease is chronic in nature and complete remission is uncommon, emphasizing the
importance of considering the disorder at all stages of life. It is a major airway
disease, which causes morbidity and significantly impairs patients’ quality of life. It is
also associated with conditions like asthma, sinusitis, nasal polyps, and lower airway
infection.
The present study entitled “Efficacy of a Unani formulation in Nazla Haar” was
conducted at National Institute of Unani Medicine Hospital, Bangalore, in 40
patients with two groups; test and placebo control. Test group was given a Joshanda
of Unani formulation (Behidana, Unnab and Sapistan) along with Sharbate Banafsha
and the placebo control group caramel syrup 25 ml twice a day for 15 days.
The pre and post treatment data from both groups were compared, test group has
shown statistically significant reduction with p<0.01 in the severity of subjective
parameters, while in placebo control group, remained insignificant till 15th day of
treatment. The objective parameter NSFE was found extremely significant (p<0.001)
in test group in comparison to placebo group.
This study reveals that the disease is more common among the younger age group of
people with phlegmatic humour, and socioeconomically middle income category.
Conclusion
108
Majority of the subjects were suffered from seasonal state of Nazla Haar was due to
exposure to either dust, or dust and smoke. Moreover, this study has shown no
clinically significant adverse effects, and overall compliance to the treatment was
commendable. On the basis of results and observation, it can be concluded that the
test drug is effective and safe as a treatment for Nazla Haar.
However, due to the available resources and constrains this study was conducted with
limited parameters, to make the study more comprehensive it could be conducted in
large sample size on various parameters.

SUMMARY
Summary
109
SUMMARY
A randomized single blind placebo controlled clinical study entitled “Efficacy of a
Unani Formulation in Nazla Haar” was conducted after enrolling the patients from
OPD of National Institute of Unani Medicine hospital, Bangalore, after the approval
of the NIUM, Institutional Ethical Committee for Biomedical research during March
2011 to December 2011.
Patients fulfilling the inclusion criterion were subjected to haematological,
biochemical and radiological investigations for obligatory terms of inclusion criteria,
and then enrolled in the study after obtaining a voluntary written informed consent,
then randomized in to two groups test (n=30) and placebo control (n=10); test group
was given a decoction of Behidana, Unnab and Sapistan with Sharbate Banafsha,
placebo group was served caramel syrup 25ml twice a day for 15 days in both groups
respectively. The efficacy of the study was assessed in both groups in terms of
subjective and objective parameters in three follow ups i.e., 4th, 8th and 15th day, based
on the severity of disease and the effect of the treatment on four point scale (0-
absent; 1- mild; 2- moderate; 3- severe). Overall response of study in both groups
was evaluated o n Total Symptom Severity Score (TSSS). The clinical improvement
was recorded on the CRF specifically designed for the study.
After the completion of study, the pre and post treatment data from both groups were
compared, test group has shown significant reduction (P<0.01) in the severity of
subjective parameters like rhinorrhoea, sneezing, nasal congestion, itchy nose, mouth
or throat, lacrimation, post nasal drip and headache, whereas in placebo control group
there was no significant reduction till 15th day of treatment. The objective parameters
especially, NSFE was observed and analyzed in both groups before and after
Summary
110
treatment, by using Kruskal-Wallis with Dunn’s Multiple Comparison Pair tests, the
test group after treatment effects exhibited highly significant (P<0.001) in
comparison of baseline before treatment, whereas, placebo control group has shown
no significant changes.
Moreover, this study has shown no significant adverse effects were observed during
the course of treatment in the test group, and overall compliance to the treatment was
commendable.
Age:
The mean age of the subjects was 29.8 years. The maximum of 35 (62.5%)
patients were found between 21-40 years. This data suggests that the disease is
more prevalent in young adulthood.
Sex:
Male constituted 62.5% and female 37.5%.
Marital status:
65% patients were married and 35% were unmarried in both test and control groups.
Religion:
55% patients were Hindu followed by 42.5% Muslims and 2.5% was Christian.
Dietary habit:
90% patients were non-vegetarian and only 10% were vegetarian.
Socioeconomic status:
Majority of the subjects 87.5% were belonged to middle income category,
followed by upper 7.5% and lower 5%.
Summary
111
Mizaj:
The highest number of subjects was found with Balghami 60% followed by 40%
Damavi temperament.
Family history:
Positive family history was present only in 30% patients and 70% were negative.
Occupation:
The highest incidence of 25% was observed in students followed by 17.5% each in
house wives and businessmen, and 10% each in teachers and tailors.
Duration of illness:
The maximum numbers of patients 40% were found with 2-4 years of duration of
illness followed by 30% with 3 months to 1 year.
Effect of Study on Subjective Parameters
Effect on rhinorrhoea:
Statistically ve r y significant reduction (P<0.01) was observed on 8th day of the
treatment when compared with median score of 0th day in test group. When median
score of the both groups was compared with each other, it was found that there was
significant (P<0.05) and extremely significant (P<0.001) reductions in severity of
rhinorrhoea on 15th day of test, with respect to 0th day and 8th day placebo
respectively.

Summary
112
Effect on sneezing:
Statistically significant reduct ion (P<0.05) was found on 4th day of the treatment
when compared with median score of 0th day in test group. When median score of
the both groups was compared with each other, it was found that there was a very
significant (P<0.01) reduction in severity of sneezing on 15th day of test with respect
to 4th day placebo.
Effect on nasal congestion:
Statistically significant reduction (P<0.05) was found on 4th day of the treatment
when compared with median score of 0th day test group. When median score of the
both groups placebo and test drug were compared with each other, it was found that
there was significant (P<0.05) reduction in severity of nasal congestion on 8th day
with respect to 4th day placebo.
Effect on itchy nose:
Statistically very significant reduction (P<0.01) was found on 8th day of the
treatment when compared with median score of 0th day in test group. When median
score of the both groups was compared with each other, it was found that there was
significant (P<0.05) reduction in severity of itchy nose on 15th day with respect to 0th
day placebo.
Effect on itchy mouth or throat:
Statistically significant reduction (p<0.05) was found on 8th day of the treatment
when compared with median score of 0th day in test group. When median score of
the both groups was compared with each other, it was found that there was no
significant (P>0.05) reduction in severity of itchy mouth or throat with respect to
placebo.

Summary
113
Effect on lacrimation:
Statistically significant reduction (p<0.05) was found on 4th the day of the
treatment when compared with median score of 0th day in test group. When median
score of the both groups was compared with each other, it was found that there was
no significant (P>0.05) reduction in severity of lacrimation with respect to placebo.
Effect on post nasal drip:
Statistically very significant reduction (p<0.01) was found on 15th day of the
treatment when compared with median score of 0th day in test group. When median
score of the both groups was compared with each other, it was found that there was
significant (P<0.05) reduction in severity of post nasal drip on 15th day with respect
to 0th day placebo.
Effect on headache:
Statistically very significant reduction (p<0.01) was found on 8th day of the
treatment when compared with median score of 0th day in test group. When median
score of the both groups was compared with each other, it was found that there was
no significant (P>0.05) reduction in severity of headache with respect to placebo.
Effect on NSFE
26 patients in test and 5 patients in placebo control groups were positive for NSFE
before treatment on baseline. After the completion of treatment, 1 patient in test
(though reveals positive NSFE, but significant reduction in number of eosinophils)
and all 5 patients in control groups were found positive on. On statistical analysis
t h e test group exhibited highly significant (p<0.001) effect on NSFE after
the treatment when compared with baseline before treatment, whereas in placebo
control group has shown no significant changes in NSFE.
Summary
114
Effect on TSSS:
When the Mean ± SEM of TSSS o f subjective parameters in both groups was
compared statistically and observed that the Mean ± SEM scores of TSSS of
test group was found significantly lowered (P <0.01) after the treatment when
compared with Mean ± SEM scores of TSSS of placebo control and test before
treatment. The inference of the results indicates that the test formulation is effective
in reducing TSSS scores of Nazla Haar.
Overall Effect on the study:
The overall effect of the study reveals that the test group was found very significant
with p value <0.01 after the treatment when compared with placebo control and test
before treatment. In test group out of 30 patients 28 were found < 2 TSSS along with
negative eosinophils, while the placebo group revealed marginal reduction in TSSS
without significant change in eosinophils. The total response of the study in terms of
cure and not cure is observed as out of 30 patients in test group 28 (93.33%) were
cured, and 2 (6.67%) were not cured, whereas, placebo group reveals nil result as
denoted not cured.
BIBLIOGRAPHY

Bibliography
115
BIBLIOGRAPHY
1. Ismail Jurjani. Zakheere Khwarizam Shahi. (Urdu translation by Khan HH).
Vol. 2. Part- 6. New Delhi: Idara Kitabush Shifa; 2010: 201-203.
2. Quamri AMH. Ghina Mana Ma Tarjuma Minhajul Ilaj. (Urdu translation by
CCRUM).1st ed. New Delhi: Ministry of Health and Family Welfare; 2008:
121- 127.
3. Tabri R. Firdausul Hikmat. (Urdu translation by Hakeem MA Shah). Faisal
publication; 2002: 178, 179.
4. Majusi A. Kamilus Sana’a. (Urdu translation by Kantoori GH) Vol. 2.
Lucknow: Munshi Naval Kishore; 2010: 357, 483, 484.
5. Ibn Sina. Al Qanoon fit Tibb. (Urdu translation by Kantoori GH). Vol. 1,
Part 4. New Delhi: Idara Kitabul Shifa; 2010: 660, 661.
6. Tabri AM. Al Moalajat Al Buqratia. (Urdu translation by CCRUM). Vol.1.
New Delhi: Ministry of Health and Family Welfare; 1997: 313-317.
7. Ibn Zohar AMAM. Kitab al Taisir Fil Mudawat wat Tadbir. (Urdu
translation by CCRUM). 1st ed. New Delhi: Ministry of Health and Family
Welfare; 1986: 31.
8. Ibne Rushid AWM. Kitab Al Kulliyat. (Urdu translation by CCRUM). 2nd
ed. New Delhi: Ministry of Health and Family Welfare; 1987: 118, 253, 280.
9. Nafeesi. Moalejat Nafeesi (Arabic). Lucknow: Matba Munshi Naval
Kishore; 1324 Hijri: 210-211.
10. Arzani A. Mizanut Tib. New Delhi: Idara kitabush Shifa; 2002: 59
11. Khan MA. Al Akseer. (Urdu Translation by Kabeeruddin M).Vol. 1. New
Delhi: Eijaz Publishing House; 2003:362-373.
12. Arzani A. Tibe Akbar. (Urdu translation by Hussain M). New Delhi: Idara

Bibliography
116
Kitabush Shifa; 2010: 99-102.
13. Azizi MH. Rhazes and the first clinically exact description of hay fever
(seasonal allergic rhinitis). Iran J Med Sci. Vol. 35; 2010 Sep 262, 263.
14. www.allergy.org.au (Cited 2012 February 02)
15. Rimmer SJ. Allergic rhinitis spring into action. Medicine today. 2007 Nov
47-59.
16. Maqbool M. Text book of Ear, Nose and Throat Diseases. 10th ed. P 145,
147, 148, 152-154.
17. http://www.uptodate.com/contents/clinical-manifestations-and-
epidemiology-of -allergic-rhinitis-rhinosinusitis. (Cited 2012 January 18)
18. http://www.biomedcentral.com/1472-6815/11/3 (Cited 2011 October 11)
19. Khan MA. Akseer Azam; Vol. 1. New Delhi: Idara Kitabush Shifa; 2011:
210- 213.
20. Ibn Hubal. Kitabul Mukhtarat Fil Tibb. (Urdu translation by CCRUM). Vol.
III. New Delhi: Ministry of Health & Family Welfare, Govt. of India; 2004:
130-132.
21. Khan A. Haziq. Karachi: Madina Publishing Company; 1983: 73-78.
22. Qarshi MH. Jamiul Hikmat. New Delhi: Idara Kitabush Shifa. 2011: 521-
523.
23. Ulrik CS, Linstow ML, Backer V. Prevalence and Predictors of Rhinitis in
Danish Children and Adolescents. Allergy. Vol. 55. 2000: 1019-1026.
24. Goldman L, Schafer AI. Cecil medicine. 24th ed. New Delhi: Elsevier India
Private Ltd; 2012: 1622- 1628, 2455-57.
25. PL Dhingra, S Dhingra. Diseases of Ear, Nose and Throat. 5th ed. 2010: 153,
155, 168, 169, 180-185.

Bibliography
117
26. Wang DY, Niti M, Smith JD, Yeoh KH, Ng TP. Rhinitis: do diagnostic
criteria affect the prevalence and treatment. Allergy. Vol. 2002 Feb; 57: 150-
154.
27. http://download.videohelp.com/vitualis/med/nasal cavity.htm (Cited 2012
February 28)
28. BD Chaurasia’s. Human Anatomy Regional and Applied Dissection and
Clinical. Head and Neck and Brain. Vo. 3. 4th ed. 2004: 227-231
29. http://intranasal.net/anatomyphysiology/default.htm #Nasal Cavity Function.
(Cited 2012 February 28)
30. http://pathologyoutlines.com/nasal.html # normal histology. (Cited 2012
February 28)
31. Standring S. Gray’s Anatomy. The Anatomical Basis of Clinical Practice. 39th
ed. Churchill Livingston; 2005: 567-574.
32. Ibn Sina. Al Qanoon Fit Tibb (Arabic version). Vol.3. New Delhi: Jamia
Hamdard; 1418 Hijri 243, 244.
33. Quillen DM, Feller DB. Diagnosing rhinitis: Allergic vs Non allergic.
American Family Physician. 2006 May Vol. 73: 1583-1590.
34. Passalacqua G, Canonica GW, Baiardini I. Rhinitis, rhinosinusitis and quality
of life in children. Pediatr Allergy Immunol. 2007: 18 (18): 40-45.
35. Chowdary VS, Vinay kumar EC, Rao JJ, Rao R, Babu KR, Rangamani V. A
study on Serum IgE and Eosinophils in Respiratory Allergy Patients. Indian J
Allergy Asthma Immunol 2003; 17(1): 21-24.
36. Kumar & Clark. Clinical medicine. 6th ed. Elsevier; 2006: 895-899
37. http://www.pollinex.com/professionals/news-events/2011/09/23/allergic-
rhinitis-affects-40-of-children-worldwide-and-prevalence-is-increasing.
Bibliography
118
(Cited 2012 January 18)
38. Allergiesinasiapacific.com/pdfs/ar_backgrounder.pdf. (Cited 2012 March 07)
39. Deem K, Sherris D and Ponikau JU. Management of allergic rhinitis-
implementation of evidence-based guidelines. TOUCH BRIEFINGS 2008:
100-104.
40. Rondon C, Fernandez J, Canto G, Blanca M. Local Allergic Rhinitis: Concept,
Clinical Manifestations and Diagnostic Approach. J Investig Allergol Clin
Immunol 2010. Vol. 20(5): 364-371.
41. Ozdoganoglu T, Songu M. The burden of Allergic Rhinitis and asthma.
Therapeutic Advances in Respiratory Disease. 2012, 6(1): 11-23.
42. McPhee SJ, Lingappa VR, Ganong WF, Lange JD. Pathophysiology of
Disease an Introduction to Clinical medicine. 2nd ed. Chapter 3. 1997: 36, 37.
43. Bhargava KB, Bhargava SK, Shah TM. A Short Textbook of E.N.T. Diseases
for students and Practitioners. 6th ed. Mumbai Usha Publications. 2002: 143,
150, 154, 155.
44. Lundback B. Epidemiology of rhinitis and asthma. Clinical and Experimental
Allergy: Journal of the British Society for Allergy and Clinical Immunology
1998: 3-10.
45. Kausar Chandpuri. Moajizul Qanoon. New Delhi: National Council for
Promotion of Urdu Language; 1998: 283, 284.
46. Tinana AM, Bloebaum RM, Grant JA. Managing Allergic Rhinitis: The Role
of Pharmacotherapy. Drug Benefit Trends. 2009 Nov 9; Vol. 21 PNM.
47. Jilani G. Makhzanul Ilaj; Vol-1; New Delhi: Idara Kitabush Shifa; 2005: 167,
168.
Bibliography
119
48. Jaffri SAH, Siddique MH. Daqaiqul Ilaj (Urdu Translation). Deoband: Vol. 1.
Mukhtar Press; YNM: 245-248.
49. Deraz TE. Immunopathogenesis of allergic rhinitis. Egypt J Pediatr Allergy
Immunol 2010: 8(1): 3-7.
50. Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL et
a l. Harrison’s Principles of Internal Medicine.17thed. Vol-2. New Delhi:
Mc Graw Hill; 2008: 2069-2070.
51. Angier E, Willington J, Scadding G, Holmes S, Walker S. Management of
Allergic and non-allergic rhinitis: a primary care summary of the BSACI
guideline. Primary Care Respiratory Journal. 2010; 19 (3): 217-222.
52. Navarro A, Colas C, Anton E, Conde J, Davila I, Dordal MT et al.
Epidemiology of Allergic Rhinitis in Allergy Consultations in Spain:
Allerglogica-2005. J Investig Allergol Clin Immunol. 2009; vol.19: 7-13.
53. Boon NA, Cumming AD, John G. Davidson’s Principles & Practice of
Medicine. Part 1. 20th ed. 2007: 729.
54. Jilani G. Makhzanul Hikmat. Vol-2; New Delhi: Eijaz Publishing House;
1996: 338.
55. McPhee SJ, Papadakis MA, Tierney LM. Current medical diagnosis and
treatment. 2008: PNM (Soft Copy).
56. Daniel C, Thomas B, Jonathan C. Manual of allergy and immunology:
Diagnosis and Therapy. 4th ed. Lippincott Williams & Wilkins Publishers.
2002: 28-31.
57. Conner SJ. Evaluation and treatment of the patient with allergic rhinitis. The
Journal of Family Practice. 2002 Oct Vol. 51: 883-890.
Bibliography
120
58. Koga T, Matsuse H, Kohrogi H, Kohno S, Aizawa H. Impact of nasal
condition on self-assessed Disease Control and Treatment Satisfaction in
Patients with Asthma Complicated by Allergic Rhinitis. Allergology
International. 2007; 56: 427-431.
59. Eapen RJ, Ebert CS, Pillsbury HC. Allergic Rhinitis - History and
Presentation. Otolaryngology Clin N Am. 2008: 325-330.
60. Al Anazy FH. The Role of Nasal Allergy in Otitis Media with Effusion.
Bahrain Medical Bulletin. 2011 March Vol.33. PNM.
61. Jauregui I, Mullol J, Davila I, Ferrer M, Bartra J, Cuvillo AD et al. Allergic
Rhinitis and school performance. J Investig Allergol Clin Immunol. Vol. 19;
2009: 32-39.
62. http://www.emedicine.medscape.com/article/134825-overview. (Cited 2012
January 02)
63. Storms W. Allergic Rhinitis- induced nasal congestion: its impact on sleep
quality. Primary Care Respiratory Journal 2008; 17 (1): 7-18.
64. http://www.thirdage.com/hc/c/allergic-rhinitis-prevention. (Cited 2012
January 28)
65. Weiner JM, Abramson MJ, Puy RM. Intranasal corticosteroids versus oral H1
receptor antagonists in allergic rhinitis: systematic review of randomized
controlled trials. BMJ. 1998 December 12; 317(7173): 1624-1629.
66. Kyrmizakis DE, Papadakis CE, Lohuis PJFM, Manolarakis G, Karakostas E,
Amanakis Z. Acute candidiasis of the oro-and hypopharynx as the result of
topical intranasal steroids administration. Rhinology.1999 October 28; 38: 87-
89.
Bibliography
121
67. Ghani N. Khazainul Advia. New Delhi: Idara Kitabul Shifa; 2010: 397, 398,
419, 420, 787, 788, 950, 951.
68. Prajapathi ND, Purohit SS, Sharma AK, Kumar T. A Handbook of Medicinal
Plants. 1st ed. Jodhpur: Agrobios (India); 2009: 167, 184, 185, 540, 541, 553.
69. Anonymous. Standardization of Single Drugs of Unani Medicine. Part II, III.
New Delhi: Central Council for Research in Unani Medicine (CCRUM).
Ministry of Health & Family Welfare, Govt. of India; 1992: 46, 48, 50, 149,
152, 254, 260.
70. Anonymous. The Unani Pharmacopeia of India. Part 1, Vol. II. New Delhi:
Ministry of Health and Family Welfare, Govt. of India. 2007: 27- 28, 41-42.
71. Chatterjee A, Pakrashi SC. The treatise on Indian Medicinal plants. Vol. 2, 3,
4. New Delhi: National Institute of Science Communication and Information
Resources (CSIR); 2010: 10, 11, 163, 164, 212, 213.
72. Anonymous. Medicinal plants in Folklores of Kashmir Himalayas. New Delhi:
CCRUM, Ministry of Health & Family Welfare, Govt. of India. 2001: 96
73. http://www.motherherbs.com/cydonia-oblonga.html. (Cited 2011 November
28)
74. http://www.naturalmedicinalherbs.net/herbs/c/cydonia-oblonga=quince.php.
(Cited 2011 November 28)
75. Anonymous. The useful plants of India. New Delhi: National Institute of
Science Communication and Information Resources (CSIR); 2006: 140, 141,
154, 679, 680, 702.
76. Khare CP. Indian Medicinal plants an illustrated dictionary with 215 pictures
of crude herbs. New Delhi: 2007; 173, 190, 191, 706, 735, 736.
Bibliography
122
77. Prajapathi ND, Kumar U. Agro’s Dictionary of Medicinal Plants. Jodhpur,
Agrobios (India); 2003: 92, 100, 370, 371, 383.
78. Chopra RN, Nayar SL, Chopra IC. Glossary of Indian Medicinal plants. 1sted.
New Delhi: National Institute of Science Communication and Information
Resources (CSIR); 2002:77, 86, 255, 261.
79. Nadkarni KM. Indian Plants and Drugs with their Medical Properties and
Uses. New Delhi: Srishti Book Distributers; 2005: 379, 1038, 1274- 1275,
1316- 1317.
80. Anonymous. The Wealth of India. Vol. II, X, XI. New Delhi: Council of
Scientific and Industrial Research; 2003: 514, 515, 111, 112, 201, 319, 320.
81. Kabiruddin M. Makhzanul Mufradat. New Delhi: Idara Kitabul Shifa; 2007:
116, 117, 118, 251, 295.
82. Evans WC. Treas and Evans Pharmacognosy. 15th ed. London: Saunders
Publishers; 2008: 29, 211, 456, 481.
83. Ibn Sina. Al Qanoon fit Tibb (English Translation) Vol-2. New Delhi:
Jamia Hamdard; 1998: 111, 254, 261, 327, 328.
84. Hakeem Mohd Abdul Hakeeem. Bustanul Mufradat. New Delhi: Idarul
Kitabul Shifa; 2002: 138, 139, 149, 396.
85. Kabeeruddin M. Ilmul Advia Nafeesi. New Delhi: Aijaz Publishing House;
2007: 79, 162, 163, 164, 167, 168.
86. Baars EW and Savelkoul HFJ. Citrus/ Cydonia comp. can restore the
immunological balance in seasonal allergic rhinitis- related immunological
parameters In Vitro. Hindawi Publishing Corporation Mediators of
Inflammation. Vol. 2008, Article ID 496467. 5 PNM.
Bibliography
123
87. Kawahara T and Zuka T. Inhibitory effect of hot-water extract of quince
(Cydonia oblonga) on immunoglobulin E- dependent late-phase immune
reactions of mast cells. Chemistry and Material Science, Cytotechnology. Vol.
63: 143-152.
88. Costa RM, Magalhães AS, Pereira JA, Andrade PB, Valentão P, Carvalho M
et al. Evaluation of free radical-scavenging and anti haemolytic activities of
quince (Cydonia oblonga) leaf: A comparative study with green tea (Camellia
sinensis). Food and Chemical Toxicology 47 (2009) 860-865.
89. Oliveira AP, Pereira JA, Andrade PB, Valentao P, Seabra RM and Silva BM.
Phenolic profile of Cydonia oblonga Miller leaves. J. Agric. Food Chem.
2007, 55, 7926- 7930.
90. Magalhães AS, Silva BM, Pereira JA, Andrade PB, Valentão P, Carvalho M.
Protective effect of quince (Cydonia oblonga Miller) fruit against oxidative
haemolysis of human erythrocytes. Food and Chemical Toxicology 47 (2009)
1372-1377.
91. Kirtikar KR, Basu BD, An ICS. Indian Medicinal Plants with Illustration. Vol.
I, III, VII. 2nd ed. Uttaranchal: Oriental enterprises; 2003: 281, 282, 819, 821,
822, 2310, 2313, 2314.
92. Su, X., Chen, Z., Jiao, B., Huang, Q., Li, W. (2000) Studies on anti-allergic
activity of common food stuffs in China and their constituents. [Chinese]. In,
Vol. 21. Journal of Southwest Agricultural University, 15. PNM.
93. Dymock W, Warden CJH, Hooper D. Pharmacographia Indica- A History of
the Principal Drugs. Vol. I, II. New Delhi: Srishti Book Distributors; 2005:
140-141, 350, 351, 518- 520.
Bibliography
124
94. Anonymous. Contribution of the Unani Medicinal Plants from North Arcot
District-Tamil Nadu, CCRUM. New Delhi: Ministry of Health & Family
Welfare. 1992: 125.
95. Syed HM. Hamdard pharmacopoeia of Eastern Medicine. Delhi: Sri Satguru
Publications; 1997: 12, 19, 30, 31, 36, 45, 66, 171, 176, 248.
96. Ibn Al Baitar. Al Jamiul Mufradatul Advia val Aghzia. (Urdu translation
CCRUM). New Delhi: Ministry of Health & Family Welfare, Govt. of India;
Vol.III. 1999: 23-24, 314, 315.
97. Ibn Al Baitar. Al Jamiul Mufradatul Advia val Aghzia. (Urdu translation
CCRUM). New Delhi: Ministry of Health & Family Welfare, Govt. of India;
Vol. I. 1986: 287-289.
98. http://www.ayurnepal.com/medicinal plants/219-zizyphus jujuba.html. (Cited
2011 June 12)
99. Al-Reza SM, Yoon JI, Kim HJ, Kim JS, Kang SC. Anti-inflammatory activity
of seed essential oil from Zizyphus jujuba. Food and Chemical Toxicology 48
(2010): 639-643.
100. Haleem MA. Mufarradate Azeezia. New Delhi: CCRUM, Dept. of AYUSH,
Ministry of Health & Family Welfare, Govt. of India. 2009: 35, 103.
101. Singh R, Lawania RD, Mishra A, Gupta R. Role of Cordia dichotoma seeds
and leaves extract in degenerative disorders. International journal of
Pharmaceutical Sciences Review and Research. Vol. 2, 2010 May-June: 21-
24.
102. Kuppast IJ and Nayak PV. Wound healing activity of Cordia dichotoma Forst.
F. fruits. Research Article. Vol. 5(2), 2006 March-April: 99-102.

Bibliography
125
103. Sharma US, Sharma UK, Sutar N. Singh A and Shukla DK. Anti-
inflammatory activity of Cordia dichotoma forst f. seeds extracts. International
Journal of Pharmaceuticals Analysis, Vol. 2, 2010: 01-04.
104. Maisale AB, Attimarad SL, Haradagatti DS, Karigar A. Anthelmintic activity
of fruit pulp of Cordia dichotoma. International Journal of Research in
Ayurveda & Pharmacy, 1 (2), 2010 Nov-Dec: 597-600.
105. Kokate Ck, Purohit AP, Gokhale SB. Pharmacognosy. 43rd ed. 2009: 11.54,
11.55
106. Bentley R and Trimen H. Medicinal Plants. Vol. I, III, 1st ed. Delhi: Asiatic
Publishing House; 2002: 133-135, 569- 571.
107. Koochek MH, Pipelzadeh MH, Mardani H. The Effectiveness of Viola
odorata in the Prevention and Treatment of Formalin-Induced Lung Damage
in the Rat. Journal of Herbs, Spices and medical Plants. Vol. 10, 2003: 95-103.
108. Ebrahimzadeh MA, Nabavi SM, Nabavi SF, Bahramian F and Bekhradnia AR.
Antioxidant and free Radical Scavanging Activity of H. Officinalis L. Var.
Angustifolius, V. Odorata, B. Hyrcana and C. Speciosum. Pak. J. Pharm. Sci.,
Vol. 23, NO. 1, 2010 Jan: 29-34.
109. http://medcosmospsm.blogspot.in/. (Cited 2010 January 10)
110. Kabeeruddin A. Bayaze Kabeer. Delhi: Idara Kitabush Shifa; 2010: 13.
111. Anonymous. National Formulary of Unani Medicine. Part I Urdu Edition.
New Delhi: Govt. of India, Ministry of Health & Family Welfare. 1993:334.
112. Maiti R, Rahman J, Jaida J, Allala U, and Palani A. Rupatadine and
Levocetrizine for Seasonal Allergic Rhinitis a Comparative Study of Efficacy
and Safety. Archotolaryngol Head Neck Surg. Vol. 136 (8), 2010 Aug: 796-
800.
Bibliography
126
113. http://www.ncbi.nlm.nih.gov/pubmed/11859651. (Cited 2012 March 09)
114. Rogkakou, Anthi, Villa, Elisa, Garelli, Valentina et al. Persistent Allergic
Rhinitis and the XPERT Study. World Allergy Organization Journal. Vol. 4,
2011 March: 32-36.
115. Kurowski M, Kuna P, and Gorski P. Montelukast plus Cetrizine in the
prophylactic treatment of seasonal allergic rhinitis: influence on clinical
symptoms and nasal allergic inflammation. European Journal of Allergy and
Clinical immunology. Vol. 59, 2004 March: 280-288.
116. Aubier M, Neukirch C, Peiffer C, and Melac M. Effect of Cetrizine on
bronchial hyperresponsiveness in patients with seasonal allergic rhinitis and
asthma. European Journal of Allergy and Clinical immunology. Vol. 56, 2001
Jan: 35-42.
117. Jan RH, and Wen SH. The relationship between vegetarian diets and the
prevalence of Asthma, allergic rhinitis and atopic eczema in Taiwanese school
children. Tzu Chi Med J 2007, 19: 60- 65.
118. Gelis N, Prokopakis E, Helidonis E, and Velegrakis G. Investigation of the
relationship between allergic rhinitis and personality traits using semeiometry.
Hippokratika Quarterly Medical Journal. 2007 Jul-Sep; 11(3): 138-141.
119. Majani G, Biardin I, Giardin A, Senna GE, Minale P, D’ulisee S et al. Health
related quality of life assessment in young adults with seasonal allergic
rhinitis. European Journal of Allergy and Clinical immunology. Vol. 56, 2001
April: 313-317.
120. Alyasin S and Amin R. The Evaluation of New Classification of Allergic
Rhinitis in Patients Referred to a Clinic in the City of Shiraz. Iran J Allergy
Asthma Immunol. 2007 March; 6(1): 27-31.
ANNEXURES

Annexure
127
Annexure-I
“Efficacy of a Unani formulation in Nazla Haar” National Institute of Unani medicine
Case Record Form
S. NO: ……………….. OPD/ IPD NO: …………..……CR NO:..………………. Name:…………….…….................................. Age/Sex: ……………………… Father / Husband’s / Guardian name:………….….……………………………….. Religion: ……………………………… Marital status: ………………… Occupation:................................................................. Present Address with telephone number:…………………………………………. ……………………………………………………………………………………….. ………………………………………………………………………………………. ……………………………………………………………………………………… Group Allocated: Test:……………………….. Control:…………………………………… Date of starting of treatment: ……........................ ……………………………….. Date of completion of treatment: ……………………... …………………………. Chief Complaints with duration:
No Features 0 1 2 3 Since 1 Running nose 2 Sneezing 3 Nasal congestion 4 Itchy nose, 5 Itchy mouth or throat 6 Itchy eyes/ lacrimation 7 PND 8 Headache
H/O Present illness: ………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………..……………………………..…………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………....

Annexure
128
Family history: Father.................................................. Mother………………………… Brother................................................ Sister………………………….. Son/s…………………………….. Daughter/s……………………. Personal history: 1. Appetite: Good / Fair/Poor. 2. Thirst: excess/moderate 3. Diet:Veg. /Non Veg /Mixed 4. Bowel habit: regular/constipated/loose stool 5. Bladder: normal/abnormal 6. Sleep: sound/disturbed/normal 7. Swimming: occasional 8. Psychological status: ………. 9. Learning ability: 10. Productivity at work or school: Habits: Snuffs: occasional/moderate/heavy/nil Tobacco/betel chewing: occasional/moderate/heavy/nil Alcohol: occasional/moderate/heavy/nil Smoking: occasional/moderate/heavy/nil Allergy: Dust/Cold/Smoke/Perfumes/Offensive odors/ Others- if any specify:………………… Socio-economic history:
1. Independent 2. Dependent
Upper class/Upper Middle class/Lower Middle Class…………………………………. Upper Lower class/Lower class……………………………………………………… Education…………………………………….…Income…………………………. Occupational history: Name of work ……………………... Nature of work …………………………… Treatment history: Allopathic / Unani / Ayurvedic / Homeopathic……………………………………………

Annexure
129
GENERAL PHYSICAL EXAMINATION 1. Built ……………… …………. 2. Body weight…………………………. 3. Height ............................... 4. Pallor.................................................... 5. Cyanosis Y/N 6. Clubbing of finger Y/N 7. Icterus Y/N 8. Edema Y/N 9. Lymphadenopathy Y/N 10. Mouth breathing Y/N 10. Vital signs: Pulse: …………beats/min. Blood pressure: ……………mmHg Temperature: …………… Respiratory rate:…………breath/min. SYSTEMIC EXAMINATION: 1. Nervous system:
Higher mental functions: …………………………………………………………. Motor functions: …………………………………………………………………. Sensory functions: ……………………………………………………………….. Reflexes: ………………………………………………………………………….
2. Cardiovascular System:
Inspection………………………………………………………………………… Palpation………………………………………………………………………… Percussion………………………………………………………………………… Auscultation………………………………………………………………………
3. Respiratory system:
Inspection………………………………………………………………………… Palpation………………………………………………………………………… Percussion………………………………………………………………................. Auscultation………………………………………………………………………
4. Digestive system:
Inspection………………………………………………………………………… Palpation………………………………………………………………………… Percussion………………………………………………………………................. Auscultation ……………………………………………………………………….
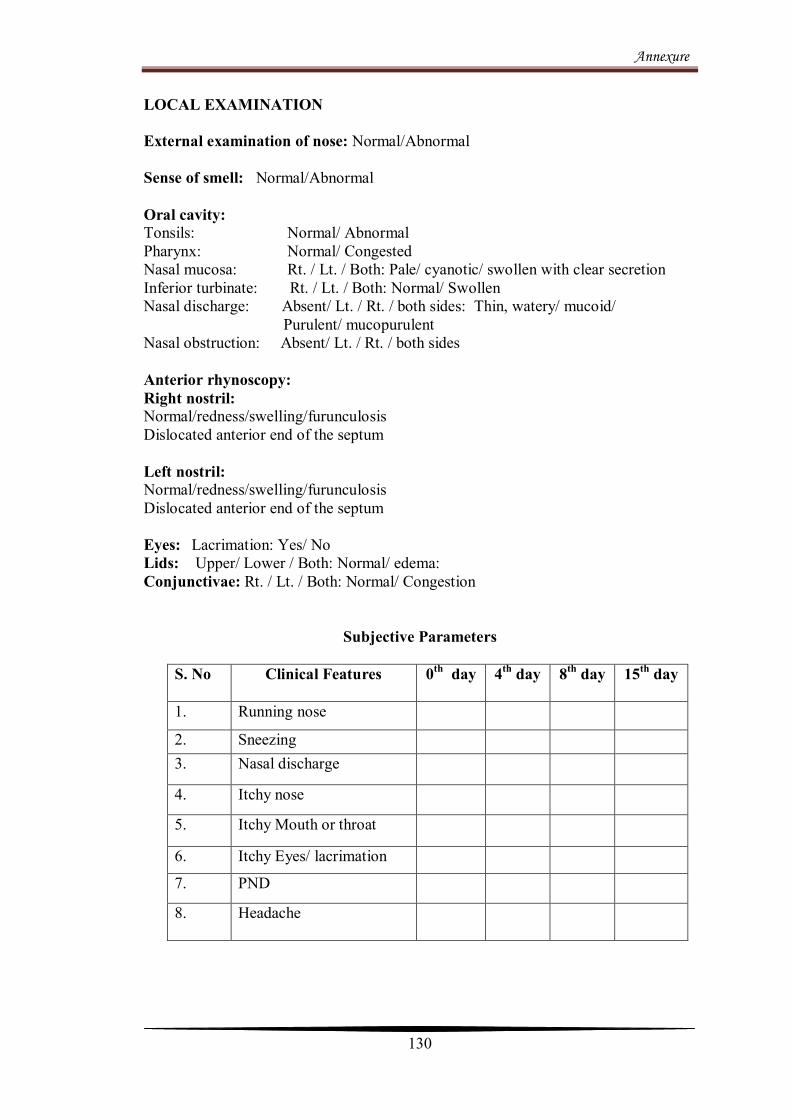
Annexure
130
LOCAL EXAMINATION External examination of nose: Normal/Abnormal Sense of smell: Normal/Abnormal Oral cavity: Tonsils: Normal/ Abnormal Pharynx: Normal/ Congested Nasal mucosa: Rt. / Lt. / Both: Pale/ cyanotic/ swollen with clear secretion Inferior turbinate: Rt. / Lt. / Both: Normal/ Swollen Nasal discharge: Absent/ Lt. / Rt. / both sides: Thin, watery/ mucoid/ Purulent/ mucopurulent Nasal obstruction: Absent/ Lt. / Rt. / both sides Anterior rhynoscopy: Right nostril: Normal/redness/swelling/furunculosis Dislocated anterior end of the septum Left nostril: Normal/redness/swelling/furunculosis Dislocated anterior end of the septum Eyes: Lacrimation: Yes/ No Lids: Upper/ Lower / Both: Normal/ edema: Conjunctivae: Rt. / Lt. / Both: Normal/ Congestion
Subjective Parameters
S. No Clinical Features
0th day 4th day 8th day 15th day
1. Running nose
2. Sneezing 3. Nasal discharge
4. Itchy nose
5. Itchy Mouth or throat
6. Itchy Eyes/ lacrimation
7. PND
8. Headache
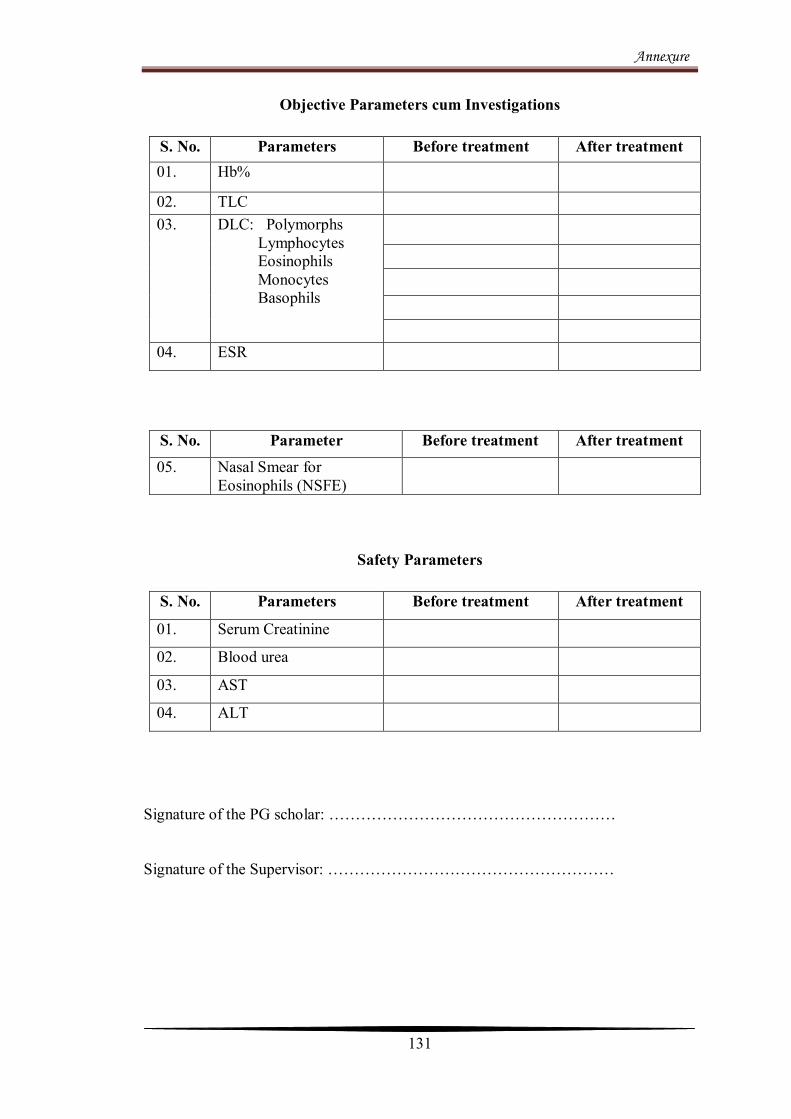
Annexure
131
Objective Parameters cum Investigations
Safety Parameters
Signature of the PG scholar: ……………………………………………… Signature of the Supervisor: ………………………………………………
S. No. Parameters Before treatment After treatment 01. Hb%
02. TLC 03. DLC: Polymorphs
Lymphocytes Eosinophils Monocytes Basophils
04. ESR
S. No. Parameter Before treatment After treatment 05. Nasal Smear for
Eosinophils (NSFE)
S. No. Parameters Before treatment After treatment
01. Serum Creatinine
02. Blood urea
03. AST
04. ALT

Annexure
132
Annexure-II
Proforma for Assessing Mizaj
Name of the patient with Age & Sex:……………………………..………………. Parameter Damavi Balghami Safravi Sawdavi
Complexion Reddish/wheat brown
1 Chalky/whitish 0.75 Pale/ yellowish
0.5 Blackish 0.25
Body built Muscular & broad
1 Fatty & broad 0.75 Moderate in muscular & thin
0.5 Skeletal 0.25
Touch Hot & soft 1 Cold & soft 0.75 Hot & dry 0.5 Cold & dry
0.25
Hair Blackish 1 Brownish 0.75 Yellowish 0.5 Black & white
0.25
Movement Active 1 Dull 0.75 Hyperactive 0.5 Less active
0.25
Diet most liked
Cold & dry 1 Hot & dry 0.75 Cold & moist
0.5 Hot & moist
0.25
Weather most suitable
Spring 1 Summer 0.75 Winter 0.5 Autumn 0.25
Sleep Normal 1 Excess 0.75 Inadequate 0.5 Insomnia 0.25 Pulse Normal rate
70-80/min 1
Slow 60-70/min normal volume
0.75
Rapid 80-100/min normal volume
0.5
Slow 60-70/min low volume
0.25
Emotions Normal 1 Calm & quiet 0.75 angry 0.5 Nervous 0.25 Total points
Range of Temperament in numbers:
Damavi= 7.51- 10.00
Balghami= 5.10- 7.50
Safravi= 2.51-5.00
Sawdavi= 0.00-2.50
Damvi
Balghami Safravi Sawdavi

Annexure
133
Annexure-III
KUPPUSWAMI'S CLASSIFICATION (Modified for 2008/’09)
Score cord A Education Score
1. Professional Degree , PG and Above 7 2. Graduate 6 3. Intermediate or Past High School Diploma 5 4. High School Certificate 4
5. Middle School Completion 3 6. Primary School or Literate 2 7. Illiterate/ Uneducated 1 B
Occupation Score
1. Profession 10 2. Semi Profession 6 3. Clerk, Shop Owner, Farm Owner 5 4. Skilled Worker/ House wife 4 5. Semi Skilled Worker 3 6. Unskilled 2 7. Unemployed 1 C. PER CAPITA INCOME ( Rs. Per Month )
1. 1500 or above 12 2. 750-1499 10 3. 565-749 6 4. 375-564 4 5. 225-374 3 6. 75-224 2 7. Below 75 1
The Total Score is Graded as follows: Upper 26-29 Upper Middle 16-25 Lower Middle 11-15 Upper Lower 5-10 Lower < 5

Annexure
134
Annexure-IV
Informed Consent Form “Efficacy of a Unani formulation in Nazla Haar” Information to the participants
The main aim of the present study is to evaluate the efficacy of a pharmacopeial
compound formulation, in comparison of placebo, to provide safe, effective and
economic drug for the management of Nazla Haar. Various forms of medicinal
preparations such as sharbat, laooq, qurs, haboob and joshanda are used in the
treatment of Nazla Haar. The test formulation is a combination of drugs possessing
anti-inflammatory and soothing properties used in the form of Joshanda (decoction)
along with Sharbat (Syrup), and an inert substance (placebo). The total duration of the
study is 15 days. There are no reasonably foreseeable risks or discomforts to you
during the research. The confidentiality of records identifying you will be strictly
maintained and only the research scholar or the guide will have access to your
medical records. All your blood/any sample will be utilized only for research purpose.
You may contact me for trial related queries, and you have rights to clear all your
doubts regarding the treatment or any possible adverse reactions of the treatment. No
anticipated prorated payment shall be made to you for participating in the trial. You
are responsible for all consequences of the treatment, either benefit or harm on
participation in the trial. You have to answer all the pertinent questions asked by the
research scholar regarding your illness.
Undertaking by the Investigator
Your consent to participate in the above mentioned study by A. H. Ayshah Fazeenah,
P.G. Scholar, Dept. of Moalajat, NIUM, Bangalore is sought. You have the right to
refuse consent or withdraw the same during any part of the study without giving any
reason. In such an event, you will continue to receive the treatment as usual. If you
have any doubts about the study, please feel free to clarify the same. Even during the
study, you are free to contact the investigators for clarification if you desire. All the
information / data collected from you will be kept in strict confidence.

Annexure
135
Efficacy of a Unani formulation in
Nazla Haar
Patient Consent Form
OPD/IPD No:……………………. Date:……………………
I ………………………………………………….exercising my free power of choice,
hereby give my consent to be included as a subject in the clinical trial for the
treatment of Nazla Haar. I understand that I may be treated with these drugs for the
disease; I am suffering from Nazla Haar. I have been informed to my satisfaction, by
attending physician the purpose of the clinical trial and the nature of drug treatment
and follow up including the laboratory investigations to monitor and safeguard my
body function.
I am also aware of my right to opt out of the trial at any time during the course of the
trial without having to give the reason for doing so.
………………………… …………………….
Signature of PG Scholar: Signature of the patient
……………………..
Name of Supervisor

Annexure
136
KEY TO MASTER CHART
AT After Treatment
Bal. Balghami
Baso. Basophils
BT Before Treatment
Bus . Business
Chr Christian
CK Cook
Clk Clerk
cm centimeter
co. Cold
C.Op Computer operator
Cpt Carpenter
CR N0. Clinical Record Number
cumm Cubic millimeter
Dam. Damvi
Dl Decileter
DLC Differential Leukocyte Count
Dvr. Driver
du dust
Eosin. Eosinophils
ESR Erythrocyte Sedimentation Rate
F Female
gm gram
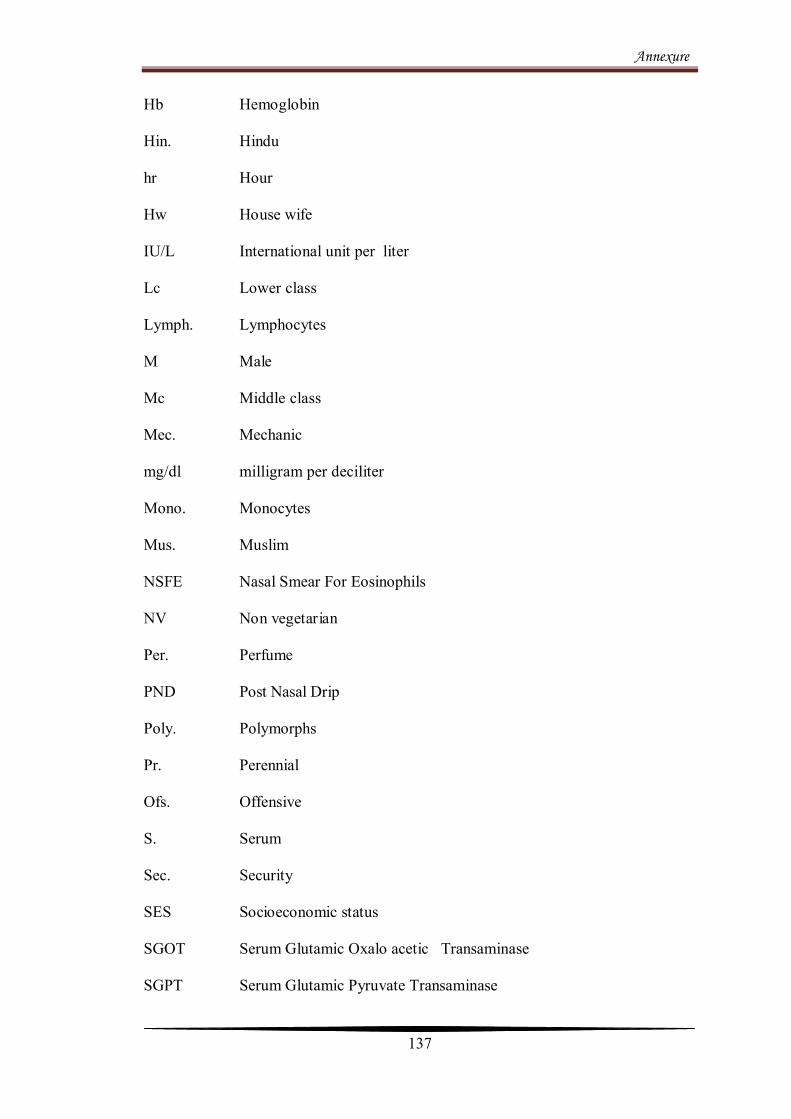
Annexure
137
Hb Hemoglobin
Hin. Hindu
hr Hour
Hw House wife
IU/L International unit per liter
Lc Lower class
Lymph. Lymphocytes
M Male
Mc Middle class
Mec. Mechanic
mg/dl milligram per deciliter
Mono. Monocytes
Mus. Muslim
NSFE Nasal Smear For Eosinophils
NV Non vegetarian
Per. Perfume
PND Post Nasal Drip
Poly. Polymorphs
Pr. Perennial
Ofs. Offensive
S. Serum
Sec. Security
SES Socioeconomic status
SGOT Serum Glutamic Oxalo acetic Transaminase
SGPT Serum Glutamic Pyruvate Transaminase
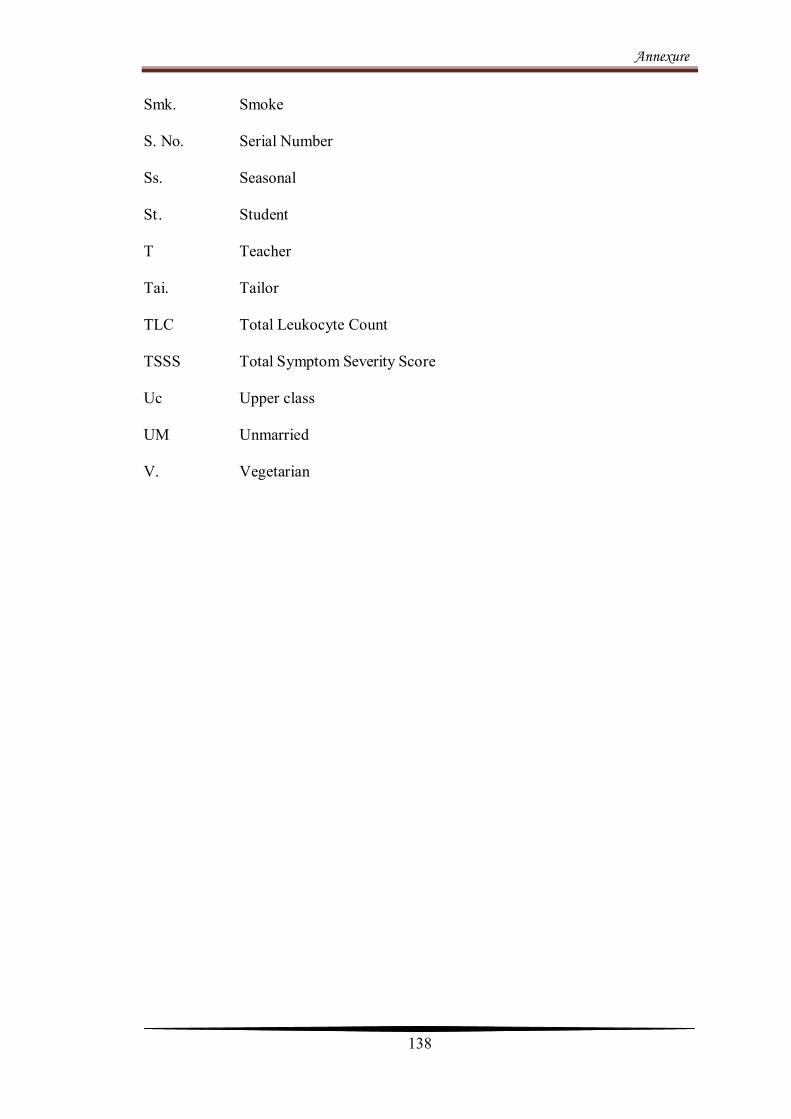
Annexure
138
Smk. Smoke
S. No. Serial Number
Ss. Seasonal
St . Student
T Teacher
Tai. Tailor
TLC Total Leukocyte Count
TSSS Total Symptom Severity Score
Uc Upper class
UM Unmarried
V. Vegetarian
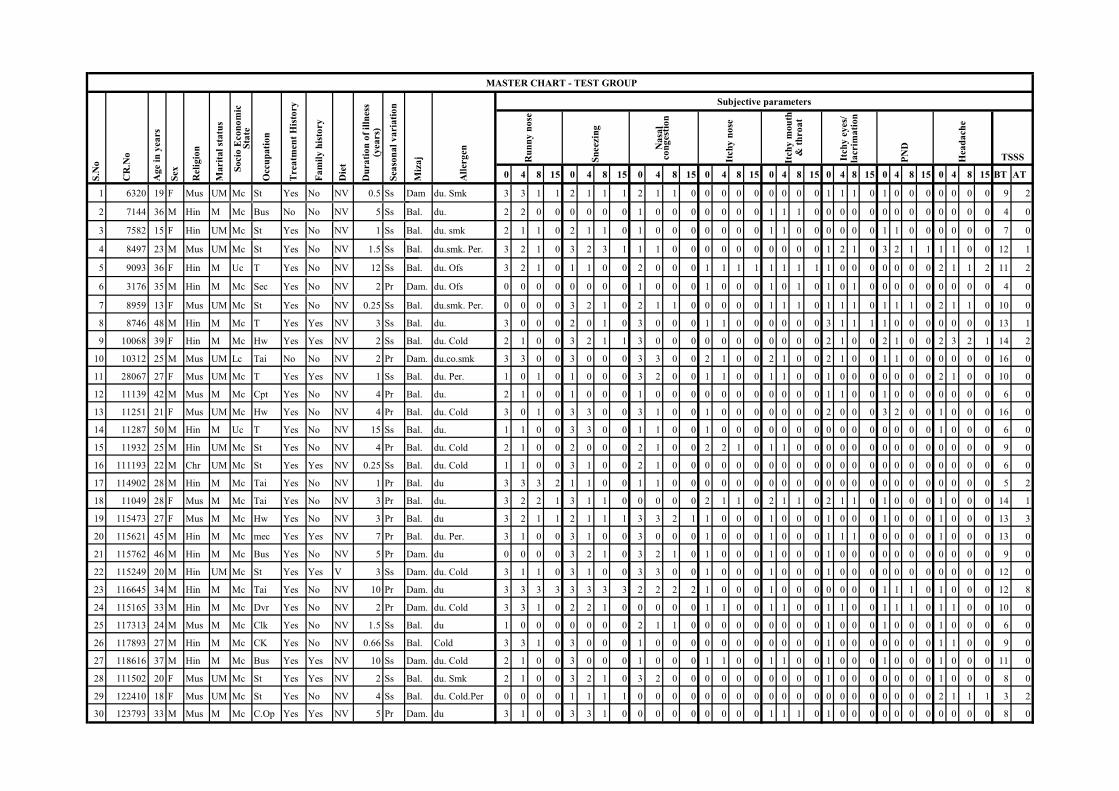
0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 BT AT
1 6320 19 F Mus UM Mc St Yes No NV 0.5 Ss Dam du. Smk 3 3 1 1 2 1 1 1 2 1 1 0 0 0 0 0 0 0 0 0 1 1 1 0 1 0 0 0 0 0 0 0 9 2
2 7144 36 M Hin M Mc Bus No No NV 5 Ss Bal. du. 2 2 0 0 0 0 0 0 1 0 0 0 0 0 0 0 1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 4 0
3 7582 15 F Hin UM Mc St Yes No NV 1 Ss Bal. du. smk 2 1 1 0 2 1 1 0 1 0 0 0 0 0 0 0 1 1 0 0 0 0 0 0 1 1 0 0 0 0 0 0 7 0
4 8497 23 M Mus UM Mc St Yes No NV 1.5 Ss Bal. du.smk. Per. 3 2 1 0 3 2 3 1 1 1 0 0 0 0 0 0 0 0 0 0 1 2 1 0 3 2 1 1 1 1 0 0 12 1
5 9093 36 F Hin M Uc T Yes No NV 12 Ss Bal. du. Ofs 3 2 1 0 1 1 0 0 2 0 0 0 1 1 1 1 1 1 1 1 1 0 0 0 0 0 0 0 2 1 1 2 11 2
6 3176 35 M Hin M Mc Sec Yes No NV 2 Pr Dam. du. Ofs 0 0 0 0 0 0 0 0 1 0 0 0 1 0 0 0 1 0 1 0 1 0 1 0 0 0 0 0 0 0 0 0 4 0
7 8959 13 F Mus UM Mc St Yes No NV 0.25 Ss Bal. du.smk. Per. 0 0 0 0 3 2 1 0 2 1 1 0 0 0 0 0 1 1 1 0 1 1 1 0 1 1 1 0 2 1 1 0 10 0
8 8746 48 M Hin M Mc T Yes Yes NV 3 Ss Bal. du. 3 0 0 0 2 0 1 0 3 0 0 0 1 1 0 0 0 0 0 0 3 1 1 1 1 0 0 0 0 0 0 0 13 1
9 10068 39 F Hin M Mc Hw Yes Yes NV 2 Ss Bal. du. Cold 2 1 0 0 3 2 1 1 3 0 0 0 0 0 0 0 0 0 0 0 2 1 0 0 2 1 0 0 2 3 2 1 14 2
10 10312 25 M Mus UM Lc Tai No No NV 2 Pr Dam. du.co.smk 3 3 0 0 3 0 0 0 3 3 0 0 2 1 0 0 2 1 0 0 2 1 0 0 1 1 0 0 0 0 0 0 16 0
11 28067 27 F Mus UM Mc T Yes Yes NV 1 Ss Bal. du. Per. 1 0 1 0 1 0 0 0 3 2 0 0 1 1 0 0 1 1 0 0 1 0 0 0 0 0 0 0 2 1 0 0 10 0
12 11139 42 M Mus M Mc Cpt Yes No NV 4 Pr Bal. du. 2 1 0 0 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 1 1 0 0 1 0 0 0 0 0 0 0 6 0
13 11251 21 F Mus UM Mc Hw Yes No NV 4 Pr Bal. du. Cold 3 0 1 0 3 3 0 0 3 1 0 0 1 0 0 0 0 0 0 0 2 0 0 0 3 2 0 0 1 0 0 0 16 0
14 11287 50 M Hin M Uc T Yes No NV 15 Ss Bal. du. 1 1 0 0 3 3 0 0 1 1 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 6 0
15 11932 25 M Hin UM Mc St Yes No NV 4 Pr Bal. du. Cold 2 1 0 0 2 0 0 0 2 1 0 0 2 2 1 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 9 0
16 111193 22 M Chr UM Mc St Yes Yes NV 0.25 Ss Bal. du. Cold 1 1 0 0 3 1 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 6 0
17 114902 28 M Hin M Mc Tai Yes No NV 1 Pr Bal. du 3 3 3 2 1 1 0 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 5 2
18 11049 28 F Mus M Mc Tai Yes No NV 3 Pr Bal. du. 3 2 2 1 3 1 1 0 0 0 0 0 2 1 1 0 2 1 1 0 2 1 1 0 1 0 0 0 1 0 0 0 14 1
19 115473 27 F Mus M Mc Hw Yes No NV 3 Pr Bal. du 3 2 1 1 2 1 1 1 3 3 2 1 1 0 0 0 1 0 0 0 1 0 0 0 1 0 0 0 1 0 0 0 13 3
20 115621 45 M Hin M Mc mec Yes Yes NV 7 Pr Bal. du. Per. 3 1 0 0 3 1 0 0 3 0 0 0 1 0 0 0 1 0 0 0 1 1 1 0 0 0 0 0 1 0 0 0 13 0
21 115762 46 M Hin M Mc Bus Yes No NV 5 Pr Dam. du 0 0 0 0 3 2 1 0 3 2 1 0 1 0 0 0 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 9 0
22 115249 20 M Hin UM Mc St Yes Yes V 3 Ss Dam. du. Cold 3 1 1 0 3 1 0 0 3 3 0 0 1 0 0 0 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 12 0
23 116645 34 M Hin M Mc Tai Yes No NV 10 Pr Dam. du 3 3 3 3 3 3 3 3 2 2 2 2 1 0 0 0 1 0 0 0 0 0 0 0 1 1 1 0 1 0 0 0 12 8
24 115165 33 M Hin M Mc Dvr Yes No NV 2 Pr Dam. du. Cold 3 3 1 0 2 2 1 0 0 0 0 0 1 1 0 0 1 1 0 0 1 1 0 0 1 1 1 0 1 1 0 0 10 0
25 117313 24 M Mus M Mc Clk Yes No NV 1.5 Ss Bal. du 1 0 0 0 0 0 0 0 2 1 1 0 0 0 0 0 0 0 0 0 1 0 0 0 1 0 0 0 1 0 0 0 6 0
26 117893 27 M Hin M Mc CK Yes No NV 0.66 Ss Bal. Cold 3 3 1 0 3 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 1 1 0 0 9 0
27 118616 37 M Hin M Mc Bus Yes Yes NV 10 Ss Dam. du. Cold 2 1 0 0 3 0 0 0 1 0 0 0 1 1 0 0 1 1 0 0 1 0 0 0 1 0 0 0 1 0 0 0 11 0
28 111502 20 F Mus UM Mc St Yes Yes NV 2 Ss Bal. du. Smk 2 1 0 0 3 2 1 0 3 2 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 1 0 0 0 8 0
29 122410 18 F Mus UM Mc St Yes No NV 4 Ss Bal. du. Cold.Per 0 0 0 0 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 1 1 1 3 2
30 123793 33 M Mus M Mc C.Op Yes Yes NV 5 Pr Dam. du 3 1 0 0 3 3 1 0 0 0 0 0 0 0 0 0 1 1 1 0 1 0 0 0 0 0 0 0 0 0 0 0 8 0
MASTER CHART - TEST GROUP
Itch
y m
ou
th
& t
hro
at
Itch
y e
yes
/ la
crim
ati
on
PN
D
Hea
da
che
Du
rati
on
of
illn
ess
(yea
rs)
Sea
son
al
va
riati
on
Miz
aj
All
erg
en
Tre
atm
ent
His
tory
Fa
mil
y h
isto
ry
Die
t Sn
eezi
ng
Na
sal
con
ges
tio
n
Itch
y n
ose
S.N
o
CR
.No
Age
in y
ears
Sex
Rel
igio
n
Ru
nn
y n
ose
Mari
tal
statu
s
Soci
o E
con
om
ic
Sta
te
Occ
up
ati
on
Subjective parameters
TSSS

0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 0 4 8 15 BT AT
1 8809 28 F Hin M Mc Hw Yes No NV 10 Ss Dam. du. 1 1 1 1 0 0 0 0 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 1 1 1 1 1 1 1 1 4 4
2 10691 23 F Mus M Mc Hw Yes No NV 1 Pr Dam. du, Cold 1 1 1 0 1 1 1 0 2 1 1 0 1 1 1 0 1 0 0 0 1 0 0 0 0 0 0 0 1 1 0 0 8 1
3 11850 20 F Mus M Lc Hw Yes No NV 1 Pr Bal. du. 1 1 1 1 1 1 1 1 1 1 1 1 0 0 0 0 0 0 0 0 1 1 1 1 3 3 3 3 0 0 0 0 7 7
4 114732 23 M Mus UM Mc mec Yes No NV 0.5 Pr Dam. du. Cold 3 3 3 2 3 3 2 2 2 3 2 1 1 0 1 1 1 0 1 1 1 0 1 1 3 0 1 1 0 0 0 0 14 10
5 115477 33 M Hin M Mc Sl.mn No Yes NV 6 Pr Dam. du.cold 1 1 1 1 3 3 3 3 3 3 2 2 0 0 0 0 0 0 0 0 1 2 1 1 0 0 0 0 0 0 0 0 8 7
6 112444 45 M Mus M Mc Owr Yes No NV 3 Ss Dam. du. 1 1 1 0 2 2 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1 1 0 1 1 1 1 6 3
7 115433 33 F Hin M Mc Hw Yes No NV 3 Pr Bal. du.cold 2 2 2 0 3 3 2 1 2 2 1 0 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 0 0 0 12 6
8 116088 50 M Hin M Uc Bus Yes Yes V 10 Ss Dam. du. Cold 1 1 2 1 1 1 1 1 2 2 2 1 1 1 0 0 0 0 0 0 0 0 0 0 1 1 1 1 1 1 1 1 7 6
9 116087 18 M Hin UM Mc St Yes Yes V 0.25 Ss Dam. du. Cold 1 1 1 1 2 2 2 1 0 0 0 0 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 5 3
10 119065 23 M Hin M Mc Sl.mn Yes No V 1 Ss Bal. du. Cold 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 0 0 2 1 1 2 9 9
MASTER CHART- PLACEBO CONTROL GROUP
S.N
o
CR
No
Age
in y
ears
Sex
Rel
igio
n
Mar
ital s
tatu
s
Soci
o E
cono
mic
Sta
te
Itch
y ey
es/ l
acri
mat
ion
Occ
upat
ion
Tre
atm
ent H
isto
ry
Fam
ily h
isto
ry
Die
t
Dur
atio
n of
illn
ess i
n ye
ars
Seas
onal
var
iatio
n
PND
Hea
dach
e
Miz
aj
Alle
rgen
Run
ny n
ose
Snee
zing
Nas
al c
onge
stio
n
Itch
y no
se
Itch
y m
outh
& th
roat
Subjective parameters
TSSS
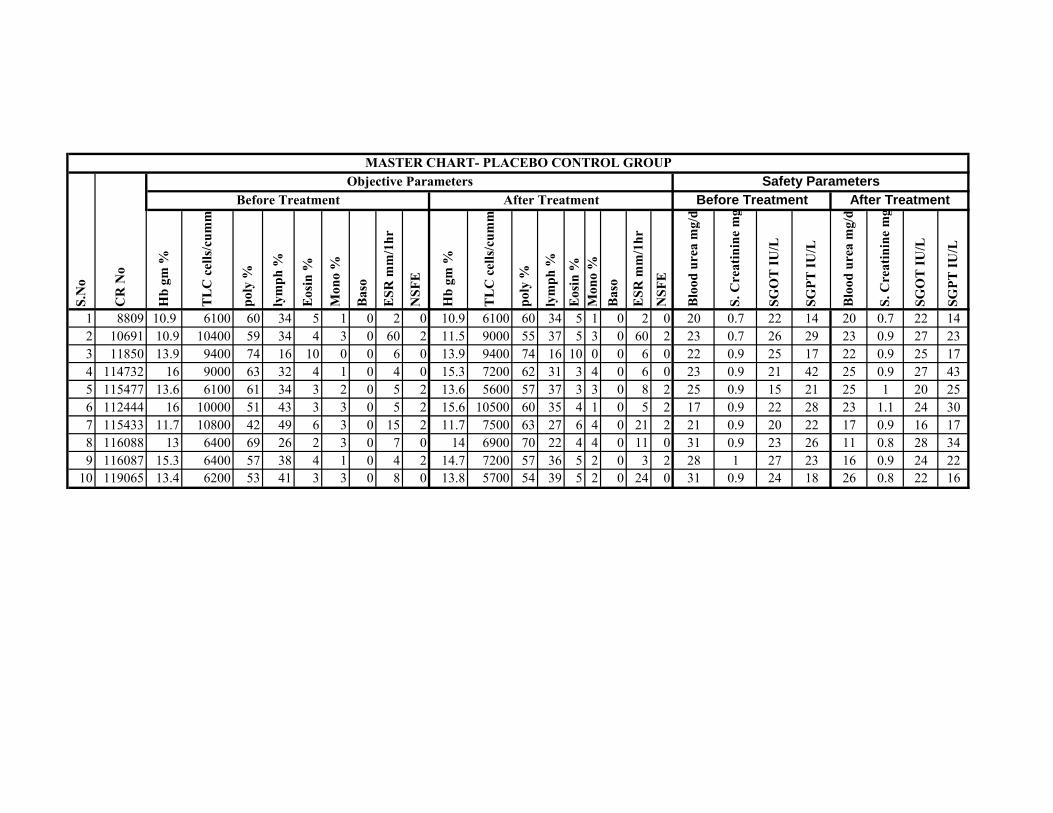
1 8809 10.9 6100 60 34 5 1 0 2 0 10.9 6100 60 34 5 1 0 2 0 20 0.7 22 14 20 0.7 22 142 10691 10.9 10400 59 34 4 3 0 60 2 11.5 9000 55 37 5 3 0 60 2 23 0.7 26 29 23 0.9 27 233 11850 13.9 9400 74 16 10 0 0 6 0 13.9 9400 74 16 10 0 0 6 0 22 0.9 25 17 22 0.9 25 174 114732 16 9000 63 32 4 1 0 4 0 15.3 7200 62 31 3 4 0 6 0 23 0.9 21 42 25 0.9 27 435 115477 13.6 6100 61 34 3 2 0 5 2 13.6 5600 57 37 3 3 0 8 2 25 0.9 15 21 25 1 20 256 112444 16 10000 51 43 3 3 0 5 2 15.6 10500 60 35 4 1 0 5 2 17 0.9 22 28 23 1.1 24 307 115433 11.7 10800 42 49 6 3 0 15 2 11.7 7500 63 27 6 4 0 21 2 21 0.9 20 22 17 0.9 16 178 116088 13 6400 69 26 2 3 0 7 0 14 6900 70 22 4 4 0 11 0 31 0.9 23 26 11 0.8 28 349 116087 15.3 6400 57 38 4 1 0 4 2 14.7 7200 57 36 5 2 0 3 2 28 1 27 23 16 0.9 24 22
10 119065 13.4 6200 53 41 3 3 0 8 0 13.8 5700 54 39 5 2 0 24 0 31 0.9 24 18 26 0.8 22 16
Objective Parameters
S.N
o
CR
No
Before Treatment After Treatment
poly
%
lym
ph %
Eosi
n %
Mon
o %
Mon
o %
Safety Parameters MASTER CHART- PLACEBO CONTROL GROUP
ESR
mm
/1hr
Hb
gm %
TLC
cel
ls/c
umm
Baso
NSF
E
Baso
NSF
E
ESR
mm
/1hr
Hb
gm %
TLC
cel
ls/c
umm
poly
%
lym
ph %
Eosi
n %
Bloo
d ur
ea m
g/dl
Bloo
d ur
ea m
g/dl
S. C
reat
inin
e m
g/dl
SGO
T IU
/L
SGPT
IU/L
Before Treatment After Treatment
S. C
reat
inin
e m
g/dl
SGO
T IU
/L
SGPT
IU/L
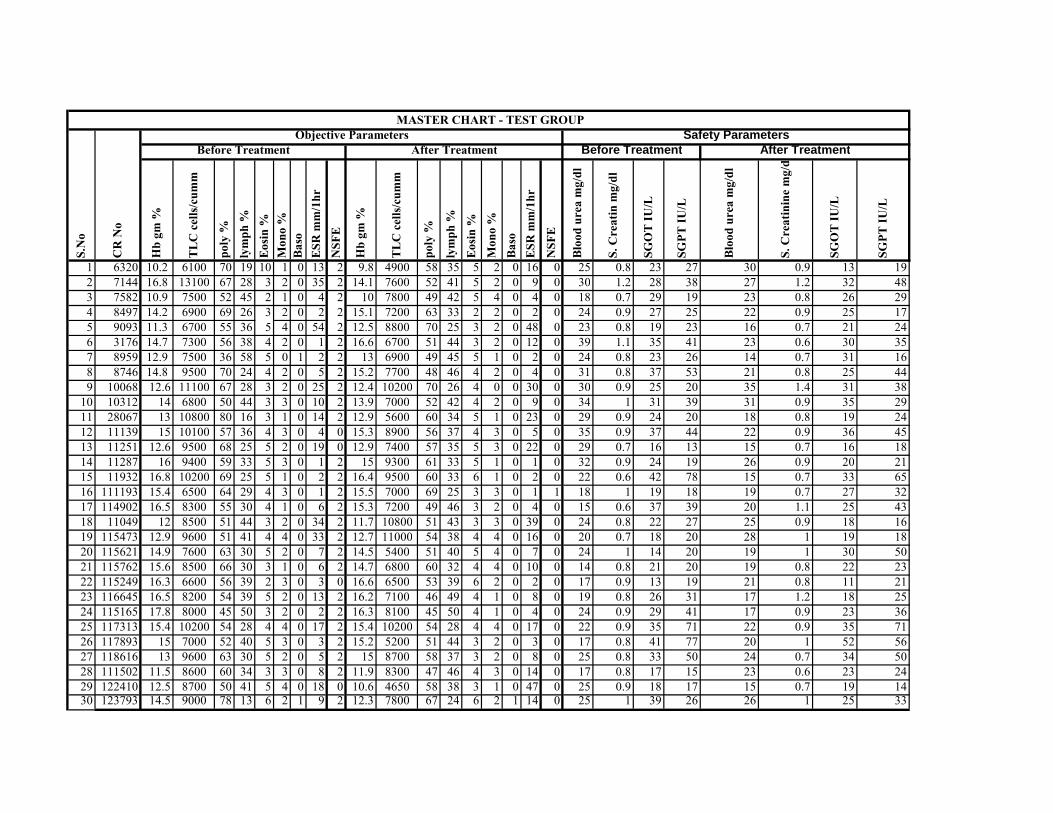
1 6320 10.2 6100 70 19 10 1 0 13 2 9.8 4900 58 35 5 2 0 16 0 25 0.8 23 27 30 0.9 13 192 7144 16.8 13100 67 28 3 2 0 35 2 14.1 7600 52 41 5 2 0 9 0 30 1.2 28 38 27 1.2 32 483 7582 10.9 7500 52 45 2 1 0 4 2 10 7800 49 42 5 4 0 4 0 18 0.7 29 19 23 0.8 26 294 8497 14.2 6900 69 26 3 2 0 2 2 15.1 7200 63 33 2 2 0 2 0 24 0.9 27 25 22 0.9 25 175 9093 11.3 6700 55 36 5 4 0 54 2 12.5 8800 70 25 3 2 0 48 0 23 0.8 19 23 16 0.7 21 246 3176 14.7 7300 56 38 4 2 0 1 2 16.6 6700 51 44 3 2 0 12 0 39 1.1 35 41 23 0.6 30 357 8959 12.9 7500 36 58 5 0 1 2 2 13 6900 49 45 5 1 0 2 0 24 0.8 23 26 14 0.7 31 168 8746 14.8 9500 70 24 4 2 0 5 2 15.2 7700 48 46 4 2 0 4 0 31 0.8 37 53 21 0.8 25 449 10068 12.6 11100 67 28 3 2 0 25 2 12.4 10200 70 26 4 0 0 30 0 30 0.9 25 20 35 1.4 31 38
10 10312 14 6800 50 44 3 3 0 10 2 13.9 7000 52 42 4 2 0 9 0 34 1 31 39 31 0.9 35 2911 28067 13 10800 80 16 3 1 0 14 2 12.9 5600 60 34 5 1 0 23 0 29 0.9 24 20 18 0.8 19 2412 11139 15 10100 57 36 4 3 0 4 0 15.3 8900 56 37 4 3 0 5 0 35 0.9 37 44 22 0.9 36 4513 11251 12.6 9500 68 25 5 2 0 19 0 12.9 7400 57 35 5 3 0 22 0 29 0.7 16 13 15 0.7 16 1814 11287 16 9400 59 33 5 3 0 1 2 15 9300 61 33 5 1 0 1 0 32 0.9 24 19 26 0.9 20 2115 11932 16.8 10200 69 25 5 1 0 2 2 16.4 9500 60 33 6 1 0 2 0 22 0.6 42 78 15 0.7 33 6516 111193 15.4 6500 64 29 4 3 0 1 2 15.5 7000 69 25 3 3 0 1 1 18 1 19 18 19 0.7 27 3217 114902 16.5 8300 55 30 4 1 0 6 2 15.3 7200 49 46 3 2 0 4 0 15 0.6 37 39 20 1.1 25 4318 11049 12 8500 51 44 3 2 0 34 2 11.7 10800 51 43 3 3 0 39 0 24 0.8 22 27 25 0.9 18 1619 115473 12.9 9600 51 41 4 4 0 33 2 12.7 11000 54 38 4 4 0 16 0 20 0.7 18 20 28 1 19 1820 115621 14.9 7600 63 30 5 2 0 7 2 14.5 5400 51 40 5 4 0 7 0 24 1 14 20 19 1 30 5021 115762 15.6 8500 66 30 3 1 0 6 2 14.7 6800 60 32 4 4 0 10 0 14 0.8 21 20 19 0.8 22 2322 115249 16.3 6600 56 39 2 3 0 3 0 16.6 6500 53 39 6 2 0 2 0 17 0.9 13 19 21 0.8 11 2123 116645 16.5 8200 54 39 5 2 0 13 2 16.2 7100 46 49 4 1 0 8 0 19 0.8 26 31 17 1.2 18 2524 115165 17.8 8000 45 50 3 2 0 2 2 16.3 8100 45 50 4 1 0 4 0 24 0.9 29 41 17 0.9 23 3625 117313 15.4 10200 54 28 4 4 0 17 2 15.4 10200 54 28 4 4 0 17 0 22 0.9 35 71 22 0.9 35 7126 117893 15 7000 52 40 5 3 0 3 2 15.2 5200 51 44 3 2 0 3 0 17 0.8 41 77 20 1 52 5627 118616 13 9600 63 30 5 2 0 5 2 15 8700 58 37 3 2 0 8 0 25 0.8 33 50 24 0.7 34 5028 111502 11.5 8600 60 34 3 3 0 8 2 11.9 8300 47 46 4 3 0 14 0 17 0.8 17 15 23 0.6 23 2429 122410 12.5 8700 50 41 5 4 0 18 0 10.6 4650 58 38 3 1 0 47 0 25 0.9 18 17 15 0.7 19 1430 123793 14.5 9000 78 13 6 2 1 9 2 12.3 7800 67 24 6 2 1 14 0 25 1 39 26 26 1 25 33
Safety Parameters MASTER CHART - TEST GROUP
CR
No
S.N
o
Before Treatment
TLC
cel
ls/cu
mm
Mon
o %
poly
%
lym
ph %
After Treatment
Mon
o %
Objective Parameters
Eosin
%
Before Treatment After Treatment
poly
%ly
mph
%Eo
sin %
NSF
E
NSF
E
Hb
gm %
TLC
cel
ls/cu
mm
Baso
Baso
ESR
mm
/1hr
ESR
mm
/1hr
Hb
gm %
S. C
reat
inin
e m
g/dl
SGO
T IU
/L
SGPT
IU/L
Bloo
d ur
ea m
g/dl
S. C
reat
in m
g/dl
SGO
T IU
/L
SGPT
IU/L
Bloo
d ur
ea m
g/dl




















