
Efficacy and safety of dopamine agonists in traumatic brain injury: a systematic review of...
18
Reviews Efficacy and Safety of Dopamine Agonists in Traumatic Brain Injury: A Systematic Review of Randomized Controlled Trials Anne Julie Frenette, 1 Salmaan Kanji, 2 Laura Rees, 3 David R. Williamson, 1 Marc M. Perreault, 4 Alexis F. Turgeon, 5 Francis Bernard, 6 and Dean A. Fergusson 2 Abstract In the intensive care unit, dopamine agonists (DA) have been used in traumatic brain injury (TBI) patients to augment or accelerate cognitive recovery and rehabilitation. However, the efficacy and safety of DA in this population is not well established. We conducted a systematic review of randomized controlled trials (RCTs) examining the clinical efficacy and safety of DA in patients with TBI. We searched MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials, comparing DA to either placebo, standard treatment, or another active comparator. There was no restriction for age, date, or language of publication. Sensitivity analyses were planned to evaluate the potential effect of timing of TBI, age, drugs, and year of publication on efficacy. Among the 790 citations identified, 20 RCTs evaluating methylphenidate, amantadine, and bromocriptine were eligible. Significant clinical heterogeneity was observed between and within studies, which precluded any pooling of data. Efficacy outcomes included mainly neuropsychological measures of cognitive functioning. A total of 76 different neuropsychological tests were used, but most of them (59%) only once. Only 5 studies systematically assessed safety. No trend could be drawn from the analysis of efficacy and safety. Important sources of bias in the studies were of major concern. Considering the absence of consensus regarding clinical outcome, the lack of safety assessment, and the high risk of bias in the included trials, more research is warranted before DA can be recommended in critically ill TBI patients. Key words: adult brain injury; dopamine agonists; traumatic brain injury Introduction T raumatic brain injury (TBI) is a leading cause of morbidity and mortality and is responsible for 50,000 deaths and 235,000 hospitalizations every year in the United States (Corrigan et al., 2010; Thurman and Guerrero, 1999). As many as 15–50% of patients surviving TBI will experience long-term disabilities, including neuropsychiatric sequelae such as sleep disturbances, arousal and attention disorders, cognitive impairment, depression, and aggressive behavior (Bales et al., 2009; Corrigan et al., 2010; Green et al., 2008; Fleminger, 2008; Ruttan et al., 2008). Neurotransmitters such as dopamine influence cognitive processes, movement control, and emotion (Bales et al., 2009; Thurman and Guerrero, 1999). Central dopaminergic path- way dysfunction may contribute to some of the neuropsy- chiatric sequelae in patients recovering from TBI (Bales et al., 2009). In the intensive care unit, step-down units, or on the ward, dopamine agonists (DA) are anecdotally used in pa- tients recovering from TBI in an attempt to augment vigilance or accelerate cognitive recovery and rehabilitation. However, the efficacy and safety of DA in this population is not clear (Francisco et al., 2007; Siddall, 2005; Tenovuo, 2006). The aim of the present systematic review was to determine the clinical efficacy and safety of DA in TBI patients compared to placebo, active control, or standard treatment (Moher et al., 2009). Methods Search strategy Randomized controlled trials (RCTs), were identified using both electronic and manual search strategies. In June 2010, we 1 Department of Pharmacy, Ho ˆ pital du Sacre ´-Coeur de Montre ´al, Faculty of Pharmacy 6 Department of Intensive Care, Ho ˆ pital du Sacre ´- Coeur de Montre ´al, University of Montre ´al, Montre ´al, Quebec, Canada. 2 Department of Pharmacy, Ottawa Hospital, Ottawa Hospital Research Institute, Ottawa, Ontario, Canada. 3 Rehabilitation Center, Ottawa Hospital, Ottawa, Ontario, Canada. 4 Department of Pharmacy, Montreal General Hospital, Faculty of Pharmacy Universite ´ de Montre ´al, Montre ´al, Quebec, Canada. 5 Department of Intensive Care, Ho ˆ pital de l’Enfant-Je ´sus de Que ´bec, Quebec, Canada. JOURNAL OF NEUROTRAUMA 29:1–18 (January 1, 2012) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2011.1812 1
Transcript of Efficacy and safety of dopamine agonists in traumatic brain injury: a systematic review of...

Reviews
Efficacy and Safety of Dopamine Agonistsin Traumatic Brain Injury: A Systematic Review
of Randomized Controlled Trials
Anne Julie Frenette,1 Salmaan Kanji,2 Laura Rees,3 David R. Williamson,1 Marc M. Perreault,4
Alexis F. Turgeon,5 Francis Bernard,6 and Dean A. Fergusson2
Abstract
In the intensive care unit, dopamine agonists (DA) have been used in traumatic brain injury (TBI) patients to augmentor accelerate cognitive recovery and rehabilitation. However, the efficacy and safety of DA in this population is notwell established. We conducted a systematic review of randomized controlled trials (RCTs) examining the clinicalefficacy and safety of DA in patients with TBI. We searchedMEDLINE, EMBASE, and the Cochrane Central Registerof Controlled Trials, comparingDA to either placebo, standard treatment, or another active comparator. Therewas norestriction for age, date, or language of publication. Sensitivity analyses were planned to evaluate the potential effectof timing of TBI, age, drugs, and year of publication on efficacy. Among the 790 citations identified, 20 RCTsevaluating methylphenidate, amantadine, and bromocriptine were eligible. Significant clinical heterogeneity wasobserved between and within studies, which precluded any pooling of data. Efficacy outcomes included mainlyneuropsychologicalmeasures of cognitive functioning. A total of 76 different neuropsychological tests were used, butmost of them (59%) only once. Only 5 studies systematically assessed safety. No trend could be drawn from theanalysis of efficacy and safety. Important sources of bias in the studieswere ofmajor concern. Considering the absenceof consensus regarding clinical outcome, the lack of safety assessment, and the high risk of bias in the included trials,more research is warranted before DA can be recommended in critically ill TBI patients.
Key words: adult brain injury; dopamine agonists; traumatic brain injury
Introduction
Traumatic brain injury (TBI) is a leading cause ofmorbidity and mortality and is responsible for 50,000
deaths and 235,000 hospitalizations every year in the UnitedStates (Corrigan et al., 2010; Thurman andGuerrero, 1999). Asmany as 15–50% of patients surviving TBI will experiencelong-term disabilities, including neuropsychiatric sequelaesuch as sleep disturbances, arousal and attention disorders,cognitive impairment, depression, and aggressive behavior(Bales et al., 2009; Corrigan et al., 2010; Green et al., 2008;Fleminger, 2008; Ruttan et al., 2008).
Neurotransmitters such as dopamine influence cognitiveprocesses, movement control, and emotion (Bales et al., 2009;Thurman and Guerrero, 1999). Central dopaminergic path-way dysfunction may contribute to some of the neuropsy-
chiatric sequelae in patients recovering from TBI (Bales et al.,2009). In the intensive care unit, step-down units, or on theward, dopamine agonists (DA) are anecdotally used in pa-tients recovering from TBI in an attempt to augment vigilanceor accelerate cognitive recovery and rehabilitation. However,the efficacy and safety of DA in this population is not clear(Francisco et al., 2007; Siddall, 2005; Tenovuo, 2006). The aimof the present systematic review was to determine the clinicalefficacy and safety of DA in TBI patients compared to placebo,active control, or standard treatment (Moher et al., 2009).
Methods
Search strategy
Randomized controlled trials (RCTs), were identified usingboth electronic andmanual search strategies. In June 2010, we
1Department of Pharmacy, Hopital du Sacre-Coeur de Montreal, Faculty of Pharmacy 6Department of Intensive Care, Hopital du Sacre-Coeur de Montreal, University of Montreal, Montreal, Quebec, Canada.
2Department of Pharmacy, Ottawa Hospital, Ottawa Hospital Research Institute, Ottawa, Ontario, Canada.3Rehabilitation Center, Ottawa Hospital, Ottawa, Ontario, Canada.4Department of Pharmacy, Montreal General Hospital, Faculty of Pharmacy Universite de Montreal, Montreal, Quebec, Canada.5Department of Intensive Care, Hopital de l’Enfant-Jesus de Quebec, Quebec, Canada.
JOURNAL OF NEUROTRAUMA 29:1–18 (January 1, 2012)ª Mary Ann Liebert, Inc.DOI: 10.1089/neu.2011.1812
1

searched MEDLINE, EMBASE, and the Cochrane CentralRegister of Controlled Studies from the earliest accessibledate. We combined terms defining the study treatment (DA)and the study population (TBI). A specific filter was applied toMEDLINE and EMBASE search strategies to identify RCTs(Lefebvre et al., 2009; Scottish Intercollegiate GuidelinesNetwork, 2009). The bibliographies of all identified RCTs andthe reviews retrieved were manually searched for additionalstudies. The search strategy was reviewed by a qualifiedlibrarian. The full search strategy for MEDLINE is presentedin Appendix 1.
Eligibility criteria
We sought studies of TBI patients, without age restrictions,comparing the effect of the administration of a DA, includingmethylphenidate, bromocriptine, amantadine, levodopa, ro-pinirole, pramipexole, apo-morphine, cabergoline, and per-golide, to either placebo, standard treatment, or another activecomparator. We included studies addressing clinical efficacyusing any primary outcome measures and/or safety. Therewas no restriction for date or language of publication. Weexcluded unpublished studies, animal studies, and studiesassessing dopamine agonists in any other type of brain injury.Studies of mixed populations with TBI representing morethan 80% of patients, or for which data of TBI patients couldbe isolated, were included.
Study selection
Every study citation retrieved was evaluated by two in-dependent reviewers (A.J.F. and S.K.), according to the pre-viously described inclusion/exclusion criteria. Disagreementswere resolved by consensus.
Data extraction and validity assessment
Each study was evaluated independently and in duplicateby two reviewers (A.J.F. and S.K., M.M.P., D.R.W., F.B., orMarie-Soleil Delisle). Any disagreement was resolved by athird independent reviewer. Information was collected usinga standardized case report form that was revised after pilottesting on 5 studies by 5 different reviewers. Descriptivevariables for each trial were collected, including language ofpublication, country of randomization, source of funding,sample size, and objectives. Information on the study designincluded the type of RCT, blinding, method of randomization,number of participating centers, and screening and enrolmentof patients. Clinical variables including patient demographicdata, past medical history, concomitant drugs permitted,timing of DA administration since the injury, description ofthe TBI (i.e., mechanism of trauma, severity of TBI, severity ofglobal illness, and radiological findings), and evaluation ofthe pre-intervention level of functioning, cognitive function,and quality of life, were also collected if reported. Clinicaloutcomes included length of stay (intensive care unit [ICU]and hospital), mortality, side effects, functional scales, post-traumatic symptoms, and neuropsychological test outcomes.
Methodological quality was assessed using the rating in-strument developed by the Cochrane Handbook for Sys-tematic Reviews of Interventions (Higgins and Altman, 2008).In order to assess the carry-over effect in crossover studies, awashout period was considered appropriate when equal to at
least 5 half-lives of the study drug from the last dose, whenmore than one dose was administered in the study. Based onclinical considerations, an a priori washout period of 2 days ormore for a single-dose trial was considered suitable. In thesecrossover studies, we considered not reporting the results ofbaseline assessment after the washout period, and the inclu-sion of patients who dropped out after the first study period,as inappropriate (Higgins et al., 2008).
Data synthesis
Data related to study design, drug treatment, and patientdemographics, were described for each study. Pre-morbidconditions were described using three categories: functionalstatus, cognitive or psychological impairment, and quality oflife, when available. Severity of TBI and illness was assessedusing severity scales (Glasgow Coma Scale, Acute Physiologyand Chronic Health Evaluation II, and Injury Severity Score),and radiological findings (computed tomography [CT] scan),when available. Clinical outcomes measured by neuropsychi-atric questionnaires and scoring tools were categorized as ei-ther behavioral or cognitive outcomes. Cognitive outcomeswere further categorized into the following domains: attention,speed of processing and reaction time, memory, and executivefunctioning, according to the predominant domain measuredby the test (Patry and Mateer, 2006; Tsaousides, 2009). Sus-tained attention, focused attention, selective attention, alter-nating attention, and divided attention, were classified underattention. Clinical outcomes not falling into cognitive or be-havioral categories were classified as ‘‘other outcomes.’’
Sensitivity analyses were performed to evaluate the poten-tial effect of the following sub-groups on efficacy: early versuslate TBI, children versus adults (16 years of age or older), typeof drugs, and year of publication. Year of publication wasdichotomized into the following categories: before 1995, and1995 and after, based on the increased use of computer-based neuropsychological tests after 1994. Patients were con-sidered to have an early TBI if they were still in an acute carefacility (ICU or ward). Patients recruited in rehabilitationcenters or in the community were considered to have late TBI.
Safety was assessed by retrieving all adverse events re-ported. We specifically looked for information on pre-determined side effects that were clinically relevant in theevaluation of DA administration safety in TBI, in addition tothe reported findings. Information regarding how safety wasassessed in the individual studies was also collected. Eva-luation of side effects was considered appropriate, if (1) theauthors were using a prospectively validated side-effectchecklist or a pre-defined objectively measured endpoint; (2)if the method of assessing specific side effects was provided;and (3) if the timing for side-effect evaluation was providedand clinically relevant (Loke et al., 2008).
Results
Study selection
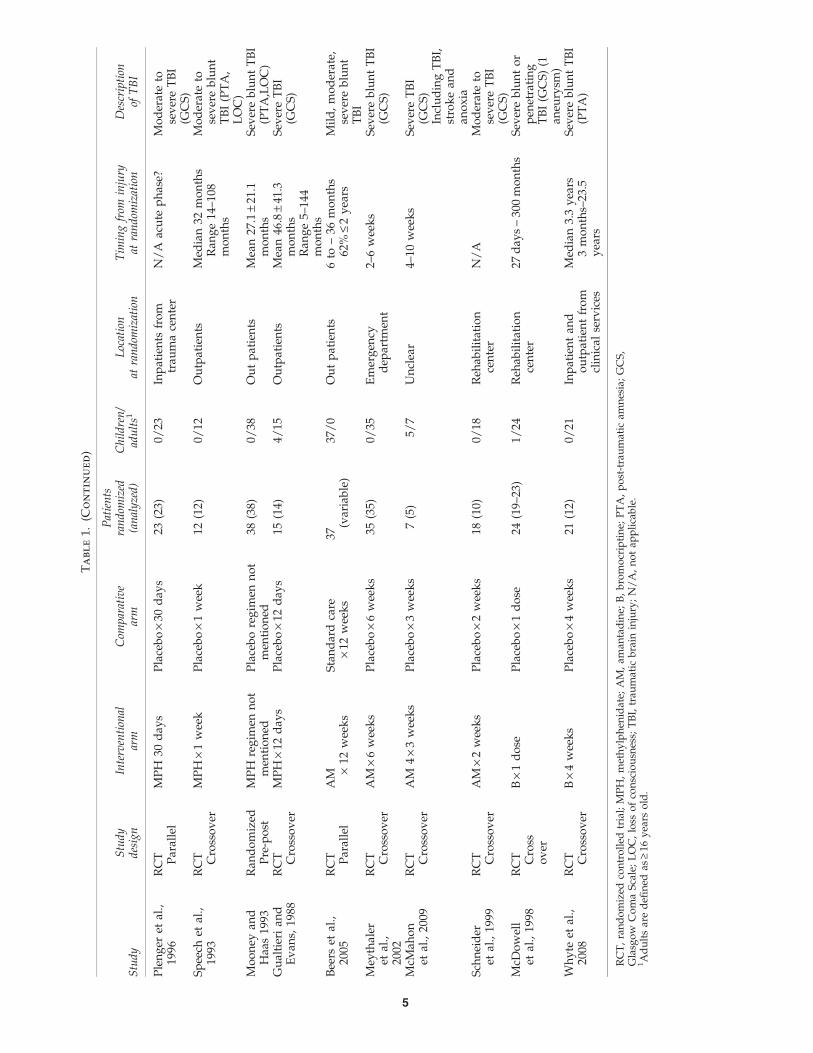
The search strategy identified 790 citations. Twenty studieswere included in the systematic review (Fig. 1). Demo-graphics of the study are listed in Table 1. One study pub-lished in Chinese only provided descriptive results that wereimpossible to analyze with regard to the objectives of thisstudy and was therefore rejected. Among those included, 14
2 FRENETTE ET AL.

evaluated methylphenidate, 4 evaluated amantadine, and 2evaluated bromocriptine. No study evaluating the use oflevodopa, apo-morphine, ropinirole, pramipexole, cabergo-line, or pergolide in TBI was identified.
Study characteristics
Twenty studies evaluated the administration of a DA in TBI,including a total of 480 patients (Alban et al., 2004; Beers et al.,2005; Gualtieri and Evans, 1988; Kim et al., 2006; Lee et al., 2005;Mahalick et al., 1998; McDowell et al., 1998; McMahon et al.,2009; Meythaler et al., 2002; Moein et al., 2006; Mooney andHaas, 1993; Plenger et al., 1996; Schneider et al., 1999; Speechet al., 1993; Whyte et al., 1997,2004,2008; Williams et al., 1998;Willmott and Ponsford, 2009; Willmott et al., 2009; Table 1).Dopamine agonists were compared to placebo in all but 2studies (Beers et al., 2005; Kim et al., 2006). One these studiesreported a comparison between amantadine and standard care(Beers et al., 2005). Sertraline was used as a comparator tomethylphenidate in the other study (Kim et al., 2006). Of the 20included studies, 14 (70%) used a crossover design, 5 (25%)useda parallel design, and 1 (5%) used a time series analysis. Themajority of studies (80%) were single-center studies. All studieswerepublished in English, and themajoritywas from theU.S.A.Other countries represented were Iran, Australia, and Korea.
Dosage regimen
Dosage did not vary much among the methylphenidatestudies (0.3–0.6mg/kg per day for adults). However, dura-
tion of treatment and follow-up period ranged from 1 day to 1month. A similar observation can be drawn regarding thedoses of amantadine that were used (200–300mg/kg/d inadults, and 4–6mg/kg/d in children). Duration of treatmentamong the studies using amantadine varied from 2 to 12weeks. A higher variation of dosing was seen among the 2studies using bromocriptine (2.5–10mg/d). One study used asingle dose (McDowell et al., 1998), and the other study fol-lowed patients for 4 weeks (Whyte et al., 2008).
Patient characteristics
Seven of the 20 studies included children (Beers et al., 2005;Gualtieri and Evans, 1988; Mahalick et al., 1998; McDowellet al., 1998; McMahon et al., 2009; Whyte et al., 1997; Williamset al., 1998), 3 of them exclusively (Beers et al., 2005; Mahalicket al., 1998; Williams et al., 1998). No study included patientsover 65 years old, although age was not always mentioned asan exclusion criterion. Some information on baseline level offunctioning and psychological and cognitive conditions wasavailable in 12 of 20 studies (Alban et al., 2004; Beers et al.,2005; Gualtieri and Evans, 1988; Kim et al., 2006; Lee et al.,2005; McMahon et al., 2009; Meythaler et al., 2002; Mooneyand Haas 1993; Whyte et al., 1997,2004,2008; Willmott andPonsford, 2009).
The level of functioning prior to randomization was as-sessed using different scales, including the Disability RatingScale (Alban et al., 2004; Whyte et al., 1997,2004,2008), theGlasgowOutcome Scale (Gualtieri, 1988; Gualtieri and Evans,1988; Mooney and Haas, 1993), and the Rancho Los Amigos
Records after duplicates removed (n = 790)
Records screened(n = 790)
Records excluded(n =754)
Full-text articles excluded (n = 16)
Reasons: 2 posters only
9 not RCT3 not TBI
1 duplicate1 impossible to analyse data
Full-text articles assessed for eligibility
(n = 36)
Studies included in qualitative synthesis
(n = 20)
Records identified through database searching
(n =925)
Additional records identified through other sources
(n = 0)
FIG. 1. Flow chart of the study (RCT, randomized controlled trial; TBI, traumatic brain injury).
DOPAMINE AGONISTS AND TRAUMATIC BRAIN INJURY 3

Tabl
e1.
Dem
ograph
icsofth
eInclu
ded
Studies
Study
Study
design
Interventional
arm
Com
parative
arm
Patients
randomized
(analyzed)
Children/
adults1
Location
atrandomization
Tim
ingfrom
injury
atrandomization
Description
ofTBI
Willm
ottet
al.,
2009
RCT Crossover
MPH 1day
/2·6
day
s
Placeboonalternate
day
s·6day
s40
(40)
0/40
Reh
abilitation
center
Ran
ge12
–462
day
sMean68
.39–77
.09
day
s
SevereTBI(PTA,
GCS)
Willm
ottan
dPonsford,
2009
RCT Crossover
MPH 1day
/2·6
day
s
Placeboonalternate
day
s·6day
s40
(40)
0/40
Reh
abilitation
center
12–4
62day
sSevereTBI(PTA,
GCS)
Moeinet
al.,
2006
RCT Parallel
MPH
from
day
2untildisch
arge
Placebofrom
day
2untildisch
arge
80(80)
0/80
Intensivecare
unit
£48
hMildTBI(G
CS)
Kim
etal.,20
06RCT Parallel
MPH·1dose
Placebo·1dose
18(18)
0/18
Reh
abilitation
center
Mean1.6–0.5years
MPH:3.6–3.4
years
placebo
N/A
Lee
etal.,20
05RCT Parallel
MPH·4weeks
Sertraline·4weeks
OR
Placebo·4weeks
30(30)
0/30
Unclear
Meanyears
MPH
34.8–3.9;
sertraline
31.9–5.8;
placebo
30–6.5
MildTBI(PTA,
LOC)
Whyte
etal.,
2004
RCT Crossover
MPH
3weeks/
6Placeboon
alternated
weeks·3w
eeks/
6
39(34)
0/39
Reh
abilitation
centeran
doutpatients
Med
ian:3.2years
Ran
ge4months–
34.2
years
SeverebluntTBI
(PTA)
Alban
etal.,
2004
RCT Crossover
MPH
3weeks/
6Placeboon
alternated
weeks3
weeks/
6
35(33–35)
0/35
Reh
abilitation
centeran
doutpatients
Med
ian:3.2y
Ran
ge4months–
34.2
years
SeverebluntTBI
(PTA)
Mah
alicket
al.,
1998
RCT Crossover
MPH·14
day
sPlacebo·14
day
s14
(14)
14/0
Notmen
tioned
/unclear
Ran
ge1–
60months
Mean14
.4–14
.87
months
Mild,moderate
andsevereTBI
(GCS)
William
set
al.,
1998
RCT Crossover
MPH·4day
splacebo·4day
s10
(10)
10/0
Outpatients
Med
ian1.5year
Mean2.7–3.0
years
N/A
Whyte
etal.,
1997
RCT Crossover
MPH
1day
/2·6
day
sPlaceboonalternate
day
s·6day
s19
(9)
1/19
In-an
doutpatients
from
arehab
ilitation
center
Med
ian14
5day
sSeverebluntTBI
(GCS) (continued)
4
Tabl
e1.
(Continued
)
Study
Study
design
Interventional
arm
Com
parative
arm
Patients
randomized
(analyzed)
Children/
adults1
Location
atrandomization
Tim
ingfrom
injury
atrandomization
Description
ofTBI
Plenger
etal.,
1996
RCT Parallel
MPH
30day
sPlacebo·30
day
s23
(23)
0/23
Inpatients
from
trau
macenter
N/A
acute
phase?
Moderateto
severeTBI
(GCS)
Speech
etal.,
1993
RCT Crossover
MPH·1week
Placebo·1week
12(12)
0/12
Outpatients
Med
ian32
months
Ran
ge14
–108
months
Moderateto
severeblunt
TBI(PTA,
LOC)
Mooney
and
Haa
s19
93Ran
domized
Pre-post
MPH
regim
ennot
men
tioned
Placeboregim
ennot
men
tioned
38(38)
0/38
Outpatients
Mean27
.1–21
.1months
SeverebluntTBI
(PTA,LOC)
Gualtierian
dEvan
s,19
88RCT Crossover
MPH·12
day
sPlacebo·12
day
s15
(14)
4/15
Outpatients
Mean46
.8–41
.3months
Ran
ge5–
144
months
SevereTBI
(GCS)
Beers
etal.,
2005
RCT Parallel
AM ·
12weeks
Stan
dardcare
·12
weeks
37(variable)
37/0
Outpatients
6to
–36
months
62%
£2years
Mild,moderate,
severeblunt
TBI
Mey
thaler
etal.,
2002
RCT Crossover
AM
·6weeks
Placebo·6weeks
35(35)
0/35
Emergen
cydep
artm
ent
2–6weeks
SeverebluntTBI
(GCS)
McM
ahon
etal.,20
09RCT Crossover
AM
4·3weeks
Placebo·3weeks
7(5)
5/7
Unclear
4–10
weeks
SevereTBI
(GCS)
IncludingTBI,
strokean
dan
oxia
Schneider
etal.,19
99RCT Crossover
AM
·2weeks
Placebo·2weeks
18(10)
0/18
Reh
abilitation
center
N/A
Moderateto
severeTBI
(GCS)
McD
owell
etal.,19
98RCT Cross
over
B·1dose
Placebo·1dose
24(19–
23)
1/24
Reh
abilitation
center
27day
s–30
0months
Severebluntor
pen
etrating
TBI(G
CS)
(1an
eurysm
)W
hyte
etal.,
2008
RCT Crossover
B·4weeks
Placebo·4weeks
21(12)
0/21
Inpatientan
doutpatientfrom
clinical
services
Med
ian3.3years
3months–23
.5years
SeverebluntTBI
(PTA)
RCT,randomized
controlled
trial;MPH,methylphen
idate;
AM,am
antadine;
B,bromocriptine;
PTA,post-traumatic
amnesia;GCS,
Glasgow
ComaScale;
LOC,loss
ofconsciousness;TBI,trau
matic
brain
injury;N/A,notap
plicable.
1Adultsaredefi
ned
as‡16
years
old.
5

Scale (Gualtieri and Evans, 1988). Patients were described asseverely disabled in 2 studies (McMahon et al., 2009; Mey-thaler et al., 2002), moderately disabled in 3 studies (Albanet al., 2004; Whyte et al., 1997,2004), and mildly to moderatelydisabled in 2 studies (Gualtieri and Evans, 1988; Mooney andHaas, 1993).
Patients were described as having significant behavioral orcognitive deficits in 3 studies (Beers et al., 2005; Meythaleret al., 2002; McMahon et al., 2009), one of them including onlycomatose patients (McMahon et al., 2009). Other studies re-porting cognitive status included patients with intellectualquotient within normal range (Alban et al., 2004; Gualtieri andEvans, 1988; Speech et al., 1993; Whyte et al., 2004; Williamset al., 1998; Willmott and Ponsford 2009; Willmott et al., 2009),or with mild cognitive impairment (Kim et al., 2006; Lee et al.,2005). No study reported quality of life prior to randomization.
Severity of TBI
Location of patients at randomization can be found in Table1. Of note, only 3 studies included patients in a critical care
setting (intensive care unit, trauma unit, or emergency de-partment). Heterogeneity among andwithin studies arises forthe most part from the time elapsed from trauma to ran-domization, varying from less than 48 h to 34.2 years post-TBI.Information on global severity of illness at the time of injury(e.g., Abbreviated Injury Scale, Injury Severity Score, or AcutePhysiology and Chronic Health Evaluation II) was not avail-able in any of the studies. Only 7/20 (35%) studies reportedCT scan findings (Alban et al., 2004; Lee et al., 2005; Mahalicket al., 1998;McDowell et al., 1998;Moein et al., 2006; Schneideret al., 1999; Whyte et al., 2004), and it was not possible tocalculate aMarshall or Rotterdam score (Saatman et al., 2008).Severity of TBI was assessed using 3 different tools: loss ofconsciousness after injury, presence of post-traumatic amne-sia, and the GlasgowComa Scale. Nine studies (45%) includedexclusively patients suffering from severe TBI (Alban et al.,2004; Gualtieri and Evans, 1988; Meythaler et al., 2002;Mooney and Haas, 1993; Whyte et al., 1997,2004,2008; Will-mott and Ponsford, 2009; Willmott et al., 2009).
Studies describing the mechanism of trauma includedonly blunt TBI, except for 2 patients with penetrating TBI
Willmott and Ponsford 2009Moein 2006
Kim 2006
Lee 2005
Whyte 2004
Mahalick 1998
Williams 1998
Whyte 1997
Plenger 1996
Speech 1993
Mooney 1993Gualtieri and Evans 1988McMahon 2009
Beers 2005
Meythaler 2002
Schneider 1999
Whyte 2008
Mcdowell 1998
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Amantadine
Amantadine
Amantadine
Amantadine
Bromocriptine
Bromocriptine
Stu
dy
Dru
g
Sus
tain
ed A
rous
al a
nd/o
r Atte
ntio
n ta
sk (
50/5
0 &
20/
80)
Con
trol
led
Ora
l Wor
d A
ssoc
iatio
n te
st
Tow
er o
f Lon
don
Por
teus
Maz
e
Str
oop
Inte
rfer
ence
task
Wis
cons
in C
ardS
ortin
g te
st
FIG. 2. Tests assessing executive functioning.
6 FRENETTE ET AL.

(McDowell et al., 1998), 1 aneurysm (McDowell et al., 1998), 1stroke (McMahon et al., 2009), 1 cerebral anoxia (McMahonet al., 2009), and 1 suspected assault with unknown lesions(McDowell et al., 1998). These patients were included in theanalysis since it was not possible to exclude them from thedata provided.
Efficacy outcomes
Pooled estimates of outcome measures were planned, butwere not calculated due to the inconsistent outcomemeasuresused. Efficacy outcomes included mostly neuropsychologicaltests. Only one study used length of stay as a primary out-come, and showed both reduced hospital and intensive careunit stays with methylphenidate (Moein et al., 2006).
Neuropsychological assessment. A total of 76 differentneuropsychological tests were used to assess efficacy out-comes (see Figs. 2–7). Of these, 45 (59%) tests were only usedin one study. Of note, individual results of tests were not
provided in 31 out of 128 assessments (24%). The tests werecategorized into cognitive- and behavioral-predominant do-mains, except for 4 tests (Selective Attention Task, SymbolDigit Modalities Test, Sustained Arousal and/or AttentionTask 50/50 or 20/80, and Wisconsin Sorting Card Test), thatwere included in 2 domains.
Executive functioning. Executive functioning was as-sessed by a total of 6 tests in 8 studies. Three tests showedstatistically positive results in at least one study (Fig. 2). Only‘‘Sustained Arousal’’ and ‘‘Attention tasks,’’ an experimentaltest, showed positive results in two different studies (Whyteet al., 1997,2004). These two studies evaluated methylpheni-date in rehabilitating severe TBI.
Attention. A total of 21 tests were used to evaluate at-tention in 15 studies (Fig. 3). Of these, 10 tests (48%) yieldedstatistically positive results in at least one study. Two tests(Ruff 2&7 and Sustained arousal and attention tasks) hadstatistically significant positive results confirmed by two
Moein 2006
Kim 2006
Lee 2005
Whyte 2004
Mahalick 1998
Williams 1998
Whyte 1997
Plenger 1996
Speech 1993
Mooney 1993
McMahon 2009
Beers 2005
Meythaler 2002
Schneider 1999
Whyte 2008
Mcdowell 1998
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Amantadine
Amantadine
Amantadine
Amantadine
Bromocriptine
Bromocriptine
Stu
dy
Dru
g
Dis
trac
tion
task
Dua
l Tas
k
Sus
tain
ed A
ttent
ion
to R
espo
nse
task
Test
of e
very
day
atte
ntio
n
Ruf
f 2&
7 (a
ll su
bset
s)
Sym
bol D
igit
Mod
aliti
es te
st
Mod
ified
Pos
ner
Par
adig
m
Gor
don
Dia
gnos
tic S
yste
m
Con
tinuo
us P
erfo
rman
ce te
st
Dig
it sp
an (
WA
IS-R
)
Ser
ial D
igit
Lear
ning
(al
tern
ativ
e)
Lette
rCan
cella
tion
test
A&
B tr
ails
Sen
tens
e R
epet
ition
task
Spa
tial d
elay
ed-r
espo
nse
Sel
ectiv
e A
ttent
ion
task
Lette
r N
umbe
r S
eque
ncin
g ta
sk
Two-
back
wor
king
mem
ory
Sel
ectiv
e R
emin
ding
test
(or
alte
rnat
ive)
Rea
ding
spa
n
Sus
tain
ed a
rous
al a
nd a
ttent
ion
task
s (5
0/50
& 2
0/20
)
Willmott and Ponsford 2009
Gualtieri and Evans 1988
FIG. 3. Tests assessing attention (WAIS-R, revised Wechsler Adult Intelligence Scale).
DOPAMINE AGONISTS AND TRAUMATIC BRAIN INJURY 7

different studies (Mahalick et al., 1998; Whyte et al.,1997,2004; Willmott and Ponsford, 2009). All these studiesevaluated methylphenidate in a heterogeneous populationincluding mild to severe TBI. Out of the 21 tests, 9 (43%) wereexperimental measures.
Reaction time. Processing speed and reaction time wasevaluated in 8 studies, using a total of 8 different tests (Leeet al., 2005; Plenger et al., 1996; Speech et al., 1993; Whyteet al., 1997, 2004, 2008; Williams et al., 1998; Willmott andPonsford, 2009; Fig. 4). Five of them were experimental. Po-sitive results were shown by 3 tests. Choice reaction time task,a test used in all 8 studies, yielded positive results in 50% ofsubjects (Lee et al., 2005; Whyte et al., 1997; Willmott andPonsford, 2009). Studies showing positive results evaluatedmethylphenidate in mild and severe TBI, with duration oftreatment varying from 6 days to 4 weeks.
Memory. Memory was assessed by only 4 studies (Gual-tieri and Evans, 1988; Plenger et al., 1996; Schneider et al.,1999; Speech et al., 1993), using a total of 4 tests (Fig. 5). Alltests are published. Only 2 studies report individual test re-sults, both not showing any statistically significant difference.
Mood and behavior. A total of 21 tests were used toevaluate mood or behavior (Fig. 6). No trend can be drawn
from the analysis of the results. A total of 6 studies showedpositive results on a behavioralmeasure (Beers et al., 2005; Leeet al., 2005; McDowell et al., 1998; Mooney and Haas, 1993;Whyte et al., 1997,2004), but none of these positive resultswere replicated in another study.
Other measures. A total of 20 tests could not be classifiedas either a cognitive domain measure or a behavior measure,and are thus classified as other measures (Fig. 7). Of these, theWoodcock-Johnson battery, measuring general intellectualability, specific cognitive abilities, scholastic aptitude, orallanguage, and achievement, showed positive results in onestudy (Lee et al., 2005). The Disability Rating Scale, whichmeasures general functional changes over the course of re-covery from TBI, yielded positive results in one study (Plen-ger et al., 1996), which were not corroborated by a second(Meythaler et al., 2002).
In summary, no clear beneficial effect could be drawn inany of the predefined categories of outcome (see Figs. 2–7).Predetermined sensitivity analyses did not provide additionalinformation.
Safety outcomes
Twelve of 20 studies reported evaluation of adverse events(Alban et al., 2004; Beers et al., 2005; Lee et al., 2005;McMahon
Moein 2006
Kim 2006
Lee 2005
Whyte 2004
Mahalick 1998
Williams 1998
Whyte 1997
Plenger 1996
Speech 1993
Mooney 1993
McMahon 2009
Beers 2005
Meythaler 2002
Schneider 1999
Whyte 2008
Mcdowell 1998
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Amantadine
Amantadine
Amantadine
Amantadine
Bromocriptine
Bromocriptine
Stu
dy
Dru
g
Cho
ice
Rea
ctio
n Ti
me
task
Sel
ectiv
e A
ttent
ion
task
Sym
bol D
igit
Mod
aliti
es te
st
Men
tal A
rithm
etic
Tes
t
Ste
rnbe
rg M
emor
y S
cann
ing
test
Rap
id A
utom
atiz
ed N
amin
g te
st
Pha
sic
Aro
usal
task
Pac
ed A
udito
ry S
eria
l Add
ition
test
Willmott and Ponsford 2009
Gualtieri and Evans 1988
FIG. 4. Tests assessing processing speed and reaction time.
8 FRENETTE ET AL.

et al., 2009;Meythaler et al., 2002; Moein et al., 2006; Mooneyand Haas 1993; Plenger et al., 1996; Schneider et al., 1999;Whyte et al., 2008; Williams et al., 1998; Willmott et al.,2009). However, only 5 studies (Alban et al., 2004; McMa-hon et al., 2009; Plenger et al., 1996; Williams et al., 1998;Willmott et al., 2009) systematically assessed safety usingpre-defined objective measures or a tool for at least one sideeffect.
Two RCTs evaluating methylphenidate reported results ofside effects in a second publication as a primary outcome:Whyte and associates (2004) in Alban and associates (2004),and Willmott and Ponsford (2009) in Willmott and associates(2009). Although both studies mentioned a statistically sig-nificant increase in blood pressure and heart rate, their clinicalsignificance was not described. Among the 10 remainingstudies using methylphenidate, 5 reported the evaluation ofside effects (Table 2). No study reported systematic measuresof aggressive behavior, agitation, or delirium. All four studiesusing amantadine reported side effects. Most side effects were
reported as minor, and resolved spontaneously upon dis-continuation of the study drug.
Itching and tremors were the most common side effectsreported among patients on bromocriptine. However, theincidence did not differ significantly from placebo.
Five patients were withdrawn from the study because ofeither probable or possible side effects (Beers et al., 2005;Schneider et al., 1999; Whyte et al., 2008). These includedvomiting, dizziness, and elevated blood pressure, light-headedness and behavioral agitation, and rash and seizure.
Risk of bias
The analysis of risk of bias revealed that the majority ofstudies did not provide enough information on sequencegeneration and allocation concealment to assess their appro-priateness (Table 3). All but one study (Mooney and Haas,1993) were double-blinded, but the efficacy of randomizationwas rarely assessed. Of note, in 2 studies, the majority of
Moein 2006
Kim 2006
Lee 2005
Whyte 2004
Mahalick 1998
Williams 1998
Whyte 1997
Plenger 1996
Speech 1993
Mooney 1993
McMahon 2009
Beers 2005
Meythaler 2002
Schneider 1999
Whyte 2008
Mcdowell 1998
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Amantadine
Amantadine
Amantadine
Amantadine
Bromocriptine
Bromocriptine
Stu
dy
Dru
g
Ser
ial D
igit
Lear
ning
(al
tern
ativ
e)
Ben
ton
Vis
ual R
eten
tion
Test
Wec
hsle
r M
emor
y S
cale
Riv
erm
ead
Beh
avio
ural
mem
ory
test
Willmott and Ponsford 2009
Gualtieri and Evans 1988
FIG. 5. Tests assessing memory.
DOPAMINE AGONISTS AND TRAUMATIC BRAIN INJURY 9

patients or caregivers correctly guessed their attrition(Speech et al., 1993; Willmott and Ponsford, 2009). None ofthe studies had a published version of their protocol. There-fore, the selective reporting item could not be evaluated.Other sources of bias could be found in themajority of studies,and are described in Table 3. Based on the Cochrane Hand-book for Systematic Reviews, crossover design was consid-ered appropriate if the randomized population included onlystable patients (Higgins et al., 2008). Based on this criterion,crossover design was considered inappropriate in all stud-ies. The most common bias retrieved in parallel designstudies was selection bias. A lack of information did notallow comparison of groups to determine the efficacy ofrandomization.
Discussion
In this systematic review, we identified 20 RCTs evaluatingthe effect of DA on different functional outcome measures.However, considering the important clinical inconsistencies, a
meta-analysis of the included studies could not be performed.As an effect, we could not draw meaningful conclusionsregarding the efficacy of dopamine agonists in the patientrecovering from TBI. The main factors contributing toour inability to pool data were the lack of consistencyconcerning patient severity of trauma, timing from injury,pre-randomization psychological and cognitive condition,and most importantly, the wide range of clinical outcomemeasures used in the different studies. While other system-atic reviews of pharmacological therapies including dopa-mine agonists exist (Fleminger et al., 2006; Sivan et al., 2010;Writer and Schillerstrom, 2009), this is the first to focus on theuse of these drugs specifically in patients suffering from TBI,and to evaluate both cognitive and behavioral outcomes inaddition to other meaningful clinical outcomes from an acutecare point of view. Methodological limitations of other re-views include the use of a unique database, inclusion of non-randomized trials, an incomplete search strategy descrip-tion, language restriction, and lack of rigorous evaluation ofbias (Sivan et al., 2010; Writer and Schillerstrom, 2009).
Moein 2006
Kim 2006
Lee 2005
Whyte 2004
Mahalick 1998
Williams 1998
Whyte 1997
Plenger 1996
Speech 1993
Mooney 1993
McMahon 2009
Beers 2005
Meythaler 2002
Schneider 1999
Whyte 2008
Mcdowell 1998
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Amantadine
Amantadine
Amantadine
Amantadine
Bromocriptine
Bromocriptine
Stu
dy
Dru
g
Cla
ssro
om a
ttent
iven
ess
Sel
f rat
ing
Cog
nitiv
e F
ailu
res
Que
stio
nnai
re
Car
egiv
er C
ogni
tive
Fai
lure
Que
stio
nnai
re
Con
ners
Rat
ing
Sca
le
Wis
cons
in C
ardS
ortin
g te
st
Inat
tent
ive
Beh
avio
ur ta
sk
Rat
ing
Sca
le o
f Atte
ntio
nal B
ehav
iour
Kat
z A
djus
tmen
t Sca
le-B
ellig
eren
ce
Gen
eral
Psy
chop
atho
logy
clu
ster
sco
re K
atz
Pro
file
of M
ood
Sta
tes
- an
ger
host
ility
Adu
lt A
ctiv
ity s
cale
Exa
min
er's
Rat
ing
Sca
le
Beh
avio
ur R
atin
g In
vent
ory
of e
xecu
tive
func
tions
Neu
robe
havi
oura
l rat
ing
scal
e
Bec
k D
epre
ssio
n in
vent
ory
Ham
ilton
Rat
ing
scal
e fo
r D
epre
ssio
n
Riv
erm
ead
Pos
tcon
cuss
ion
Sym
ptom
s Q
uest
ionn
aire
Sm
ithK
line-
Bee
cham
Qua
lity
of L
ife S
cale
Leed
s S
leep
Eva
luat
ion
Que
stio
nnai
re
Cho
nnam
Epw
orth
Sle
epin
ess
Sca
le
Pos
tcon
cuss
iona
l sym
ptom
s in
terv
iew
Willmott and Ponsford 2009
Gualtieri and Evans 1988
FIG. 6. Tests assessing mood and behavior.
10 FRENETTE ET AL.

The impressive number of different tests used to assessneuropsychological outcomes in the included studies may bedue to different reasons, such as the lack of a gold standard, thebroad range of year of publication, the familiarity with a par-ticular battery of tests available, and the resources availableto researchers in different settings. Many studies used non-validated or experimental tools to assess outcomes. Moreover,clinical interpretation of statistically significant results was of-ten difficult due to a lack of effect size and reliable change indexreporting, the use of composite measures, and the lack ofreproducibility of the neuropsychological tests among thepatients. Choice of outcomemeasures and their analysis in TBIis still a matter of debate (Bagiella et al., 2010;Maas et al., 2010).Heterogeneity in outcomemeasures precludes any comparisonbetween studies, and consequently from drawing conclusionsregarding the efficacy of DA in TBI. Different groups haveproposed various validated outcome combinations, includingquality of life, neurobehavioral and neuropsychological status,
and global functional outcome, but none has reached the statusof a gold standard (Shukla et al., 2011). Future studies shouldaim at evaluating outcomes that are well described in the lit-erature, validated, appropriate for international use, have wellestablished normative data, are applicable to a broad spectrumof TBI, and are easy to administer (Wilde et al., 2010). Conse-quently, the Traumatic Brain Injury Outcome Workgroup hasproposed selected outcomes evaluating different domains ac-cording to those recommendations in both adults and pediatricpopulations (McCauley et al., 2011;Wilde et al., 2010). Perhapsthese recommendations should guide future studies regardingthe efficacy of DA in TBI.
The poor methodological quality of the included studieswas another concerning finding. The majority of studies useda crossover design, which may be appropriate when highinter-patient heterogeneity is likely, such as in a TBI popula-tion. However, patient condition should be stable in order toavoid the natural evolution of the condition to account for the
Moein 2006
Kim 2006
Lee 2005
Whyte 2004
Mahalick 1998
Williams 1998
Whyte 1997
Plenger 1996
Speech 1993
Mooney 1993
McMahon 2009
Beers 2005
Meythaler 2002
Schneider 1999
Whyte 2008
Mcdowell 1998
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Methylphenidate
Amantadine
Amantadine
Amantadine
Amantadine
Bromocriptine
Bromocriptine
Stu
dy
Dru
g
Wec
hsle
r Tes
t of A
dult
Rea
ding
Crit
ical
Flic
ker
Fus
ion
Thr
esho
ld
Com
pens
ator
y Tr
acki
ng te
st
MM
SE
Woo
dcoc
k-Jo
hnso
n ba
ttery
Per
due
Peg
boar
d
Dev
elop
men
tal T
est o
f Vis
ual-M
otor
Inte
grat
ion
Non
Ver
bal F
luen
cy te
st
Wec
hsle
r In
telli
genc
e S
cale
Gal
vest
on O
rient
atio
n an
d A
mne
sia
test
Bos
ton
Nam
ing
test
Pur
suit
Rot
or
FIM
-CO
G
Com
a/ne
ar c
oma
scal
e
Com
a re
cove
ry s
cale
-rev
ised
Wee
-FIM
Dis
abili
ty R
atin
g S
cale
Gla
sgow
out
com
e sc
ale
GC
S
Fin
gert
appi
ng
Willmott and Ponsford 2009
Gualtieri and Evans 1988
FIG. 7. Other tests (MMSE, Mini-Mental State Examination; FIM-COG, Functional Independence Measure trademark-cognitive; Wee-FIM, Functional Independence Measure for Children; GCS, Glasgow Coma Scale).
DOPAMINE AGONISTS AND TRAUMATIC BRAIN INJURY 11

Tabl
e2.
Evalu
ation
ofSa
fety
andSideEffec
ts
Bromocriptine
Amantadine
Methylphenidate
Side
effects
Number
ofevents
Studies
Com
ments
Number
ofevents
Studies
Com
ments
Number
ofevents
Studies
Com
ments
Rash/itch
ing
3Whyte
etal.,
2008
3Schneider
etal.,1999;
Beers
etal.,2005
1patient
withdrawn
becau
seofrash
(Sch
neider
etal.,
1999)
5Alban
etal.,
2004
Seizures
N/A
None
1Mey
thaler
etal.,2002;
Beers
etal.,2005
2Moeinet
al.,
2006
Delirium/
confusion/
hallucinations
0Whyte
etal.,
2008
N/A
None
4Alban
etal.,
2004
Hem
odynam
icch
anges
2Whyte
etal.,
2008
1patientwithdrawn
becau
seof
decreased
blood
pressure
(Whyte
etal.,2008)
N/A
None
?Lee
etal.,2005;
Alban
etal.,
2004;Moein
etal.,2006
Number
ofev
ents
missing
(Lee
etal.,2005)
Statisticallymore
prevalen
tthan
with
placebo(p
<0.05)
(Moeinet
al.,2006;
Alban
etal.,2004)
Dizziness/
lightheaded
ness
2Whyte
etal.,
2008
1patientwithdrawn
becau
seof
lightheaded
ness
and1patient
withdrawnbecau
seofdizziness(W
hyte
etal.,2008)
N/A
None
4Alban
etal.,
2004
Diarrhea/
constipation
4Whyte
etal.,
2008
?Beers
etal.,2005
Number
ofev
ents
missing
2Alban
etal.,
2004
Number
ofev
ents
missing
(Lee
etal.,2005)
Nau
sea/
vomiting
2Whyte
etal.,
2008
1patientwithdrawn
becau
seofvomiting
(Whyte
etal.,2008)
1?Beers
etal.,2005;
McM
ahonet
al.,
2009
Number
ofev
ents
missing
2?
Alban
etal.,
2004;Lee
etal
2005
Number
ofev
ents
missing
(Lee
etal.,2005)
Headache
N/A
None
N/A
None
?Plenger
etal.,
1996
Number
ofev
ents
missing
Anxiety
1Whyte
etal.,
2008
N/A
None
7Alban
etal.,
2004
Tremors
2Whyte
etal.,
2008
N/A
None
4Alban
etal.,
2004
Sleepdisorder/
drowsiness
1Whyte
etal.,
2008
?Numbersofev
ents
missing(Beers
etal.,
2005)
Nodifference
found
onsleep
questionnaire
(McM
ahonet
al.,
2009)
12Alban
etal.,
2004
Statisticallymore
prevalen
tthan
withplacebo
(p<0.05)(A
lban
etal.,
2004)
Number
ofev
ents
missing(Plenger
etal.,
1996;Willm
ottet
al.,
2009)
Others
1sexu
aldisab
ility
Whyte
etal.,
2008
N/A
None
4Irritability;11
reduction
inap
petite;
2difficu
ltyin
urinating;
2blurred
vision;
6dry
mouth;
2weakness;
1sexu
aldisab
ility
Alban
etal.,
2004;
Willm
ott
etal.,2009
Number
ofev
ents
for
irritabilitymissing
(Willm
ottet
al.,2009)
Irritabilityan
dreductionin
appetite
statisticallymore
prevalen
tthan
with
placebo
?=totalnumber
ofev
ents
impossible
tocalculate
since
datawerenotprovided
byat
leastonestudy.
Allsideeffectswerepredetermined
exceptforsideeffectslisted
inthe‘‘o
thers’’section.
12

Tabl
e3.
RiskofBiasAssessm
ent
Riskof
bias
assessmentitem
s
Study
(drug)
Sequence
generation
Allocation
Blinding
Outcom
edata
Selective
reporting
Other
threats
tovalidity
Willm
ottet
al.,
2009
(MPH)
LL
H 75%
ofpatients
guessed
correctlytheir
attrition
LU
H Crossover
designless
suitab
leforpatients
inlower
range
oftimingpost
TBI
Carry-over
effect
possible
Moeinet
al.,
2006
(MPH)
H Based
onhosp
ital
record
number
H Based
onhosp
ital
record
number
LL
UH Im
possible
toassess
similarity
ofgroups
Possible
confusionbias
affectinglength
ofstay
Kim
etal.,20
06(M
PH)
LL
LL
UH Im
possible
toassess
ifgroups
aresimilar
Lee
etal.,20
05(M
PH)
UU
UH Missinginform
ationon
excluded
patients
UL Im
possible
toassess
similarity
ofgroups
Choiceoftoolan
dcomparator
(dep
ression)
Whyte
etal.,
2004
(MPH)
UU
LH Participan
tsthat
can’t
perform
atask
or
hav
esched
ule
conflicts
are
withdrawn
UH Crossover
designless
suitab
leforunstab
lepatients
Riskofcarry-over
Low
external
validity
Mah
alick
etal.,1
998
(MPH)
UU
LL
UH Crossover
less
suitab
lefor
unstab
lepatients
Riskofcarryover
William
set
al.,
1998
(MPH)
UU
LH Several
measu
resnot
completedbyall
subjects
UH Crossover
less
suitab
lefor
unstab
lepatients
Low
external
validity
Gualtierian
dEvan
s,19
88(M
PH)
UU
LL
H Rep
orting
resu
ltsfor
resp
onders
only
H Crossover
less
suitab
lefor
unstab
lepatients
Riskofcarry-over
Mooney
and
Haa
s,19
93(M
PH)
UU
H Simple
blind
LU
H Impossible
toassess
similarity
ofgroups
(continued)
13

Tabl
e3.
(Continued
)
Riskof
bias
assessmentitem
s
Study
(drug)
Sequence
generation
Allocation
Blinding
Outcom
edata
Selective
reporting
Other
threats
tovalidity
Speech
etal.,
1993
(MPH)
UU
H 12patients
and10
observerscorrectly
guessedattrition
UU
H Crossover
less
suitab
lefor
unstab
lepatients
Riskofcarryover
Whyte
etal.,
2008
(B)
UU
LH Patients
randomized
notan
alyzeddueto
seriousad
verse
even
tsPatients
consentedbut
dropped
or
withdrawn
UH 1/
3ofpatients
did
not
crossover
Low
external
validity
Crossover
less
suitab
lefor
unstab
lepatients
Riskofcarry-over
McD
owell
etal.,19
98(B)
UU
LH Number
ofpatients
varieswithtest
UH Crossover
less
suitab
lefor
unstab
lepatients
Riskofcarryover
McM
ahon
etal.,20
09(A
M)
UU
LH 2patients
withdrawn
from
analysis
UH Crossover
less
suitab
lefor
unstab
lepatients
Beers
etal.,
2005
(AM)
LU
H Paren
tsaw
areof
allocation
H Patients
lost
tofollow
upan
dtheir
allocationisunknown
Resultsonoutcome
provided
only
for13
patients
UH Stan
dardtreatm
entis
not
described
Impossible
toassess
ifgroups
aresimilar
Mey
thaler
etal.,20
02(A
M)
UU
UL
H Number
of
patients
screen
edin
unknown
H Crossover
designunsu
itab
leforacute
patients
Riskofcarry-over
Schneider
etal.,19
99(A
M)
UU
LH Missingdatafrom
8su
bjectswhodid
not
complete
thestudy
UH Tim
ingfrom
injury
unknown
U,uncertainrisk
ofbias;H,highrisk
ofbias;L,low
risk
ofbias;MPH,methylphen
idate;
B,bromocriptine;
AM,am
antadine.
14

benefit or harm. Evolution and brain recuperation from a TBImay continue to occur up to several years after injury and isnot predictable (Lammi et al., 2005). A crossover design alsomandates a washout period between treatments, which has tobe long enough to avoid a carry-over effect. It has been shownthat dopamine receptors can downregulate during treatmentand upregulate following cessation of therapy in patientssuffering from Parkinson’s disease (Thobois et al., 2004). Inthe studies identified, the washout period was often not longenough to avoid a carry-over effect. The use of a parallel de-sign, which would overcome the carry-over problem, is lim-ited by the heterogeneity of the TBI population, which poses amethodological challenge. Similarity of the study groups seenin this population is often impossible to achieve unless largesample sizes are used, and pre-specified covariate adjust-ments are made (Maas et al., 2004,2010).
Assessment of safety was not consistent between studies,and a lack of rigor in the methodology of side-effect evalua-tion was considered a major limitation. Although somestudies did use a questionnaire or a standardized tool to as-sess side effects, they often relied on self-reporting of symp-toms. The studies also often failed to look prospectively forpotentially concerning side effects in a TBI population. Neu-rological and psychiatric adverse reactions such as seizures,delirium, hallucinations, and insomnia should be targeted askey safety outcomes, since they are clinically relevant in theTBI population, and are associated with the use of dopamineagonists in other human populations and animal models(Barone et al., 1992; Wood, 2010). A lack of information re-garding diagnosis of these side effects was also an issue.
Despite the results of our review, the dopaminergic systemis an obvious target for research of cognitive impairments inTBI. Dopamine receptors are known to be present in manyareas of the brain important to cognition, and are oftendamaged post-TBI (the hippocampus, striatum, and frontalcortex; Bales et al., 2009). The role of dopamine receptors incognitive domains such as attention, working memory, ex-ecutive functioning, and speed of processing is still a matter ofdebate (Nieoullon, 2002). However, some observations inhumans showing impairment in visuospatial, executive, andverbal fluency tests related to induced parkinsonism lead oneto think that dopamine participates in cognition (Burrusset al., 2000; Nieoullon, 2002; Stern et al., 1990). Radioimagingstudies in patients with Parkinson’s disease, schizophrenia,and attention-deficit/hyperactivity disorder provides sup-porting evidence (Bruck et al., 2001; Duchesne et al., 2002;Heilman et al., 1991; Tanaka, 2006).
The influence of dopaminergic drugs on neuronal plasticity,a concept of brain adaptation to injury over time, is also aconcerning feature (Ampuero et al., 2010; Larson and Zollman,2010). Dysfunction of the molecular processes influencingneuronal plasticity in the hippocampus may be a potentialcause for temporal and spatial memory impairment seen in TBI(Ampuero et al., 2010; Falo et al., 2006). The role for dopaminepathways in this process is unclear, but some data suggest thata modification of plasticity occurs with the exposure of variousneurotransmitter agonists and antagonists, including dopa-mine (Bales et al., 2009; Meintzschel and Ziemann, 2006). Forexample, benzodiazepines and haloperidol have been incrim-inated as possible causes of adverse effects on neuronal plas-ticity (Ampuero et al., 2010; Falo et al., 2006). Proper safetyevaluation of dopamine agonists in TBI is therefore warranted.
Conclusion
This systematic review is the first to evaluate the effect ofthe administration of dopamine agonists on different do-mains of cognition, behavior, and safety in TBI patients.Because of the significant clinical heterogeneity in the out-comemeasures used in the different studies, pooled analysescould not be performed, and consequently clear conclusionsabout the efficacy or safety of dopamine agonists in TBIpatients are difficult to draw. Despite the low incidence ofadverse events reported, most studies did not systematicallyscreen for them. In summary, our systematic review does notsupport the use of dopamine agonists as part of the treat-ment regimen for improving functional outcome measuresin either the acute or sub-acute phases of care in TBI patients.Future studies should first aim at standardizing and vali-dating a neuropsychological battery of tests in TBI. A clinicaltrial of dopamine agonists in TBI could then be designedusing standardized outcome measures with clear clinicalsignificance, including a validated neuropsychological bat-tery of tests. It should also use a parallel design in a largesample with predefined covariates, and should systemati-cally screen for potential side effects.
Acknowledgments
The authors would like to thank Ms. Marie-Soleil Delisle,Ms. Marie Frenette, andMs. Jodi Peters for their help with thisstudy.
Author Disclosure Statement
No competing financial interests exist.
References
Alban, J.P., Hopson, M.M., Ly, V., and Whyte, J. (2004). Effect ofmethylphenidate on vital signs and adverse effects in adultswith traumatic brain injury. Am. J. Phys. Med. Rehabil. 83,131–137.
Ampuero, E., Rubio, F.J., Falcon, R., Sandoval, M., Diaz-Veliz,G., Gonzalez, R.E., Earle, N., Dagnino-Subiabre, A., Aboitiz,F., Orrego, F., and Wyneken, U. (2010). Chronic fluoxetinetreatment induces structural plasticity and selective changes inglutamate receptor subunits in the rat cerebral cortex. Neu-roscience 169, 98–108.
Bagiella, E., Novack, T.A., Ansel, B., Diaz-Arrastia, R., Dikmen,S., Hart, T., and Temkin, N. (2010). Measuring outcome intraumatic brain injury treatment trials: recommendations fromthe traumatic brain injury clinical trials network. J. HeadTrauma Rehabil. 25, 375–382.
Bales, J.W., Wagner, A.K., Kline, A.E., and Dixon, C.E. (2009).Persistent cognitive dysfunction after traumatic brain injury:A dopamine hypothesis. Neurosci. Biobehav. Rev. 33, 981–1003.
Barone, P., Palma, V., de Bartolomeis, A., Cicarelli, G., andCampanella, G. (1992). Dopaminergic regulation of epilepticactivity. Neurochem. Int. 20 Suppl., 245S–249S.
Beers, S.R., Skold, A., Dixon, C.E., and Adelson, P.D. (2005).Neurobehavioral effects of amantadine after pediatric trau-matic brain injury: a preliminary report. J. Head Trauma Re-habil. 20, 450–463.
Bruck, A., Portin, R., Lindell, A., Laihinen, A., Bergman, J., Haa-paranta, M., Solin, O., and Rinne, J.O. (2001). Positron emissiontomography shows that impaired frontal lobe functioning in
DOPAMINE AGONISTS AND TRAUMATIC BRAIN INJURY 15

Parkinson’s disease is related to dopaminergic hypofunctionin the caudate nucleus. Neurosci. Lett. 311, 81–84.
Burruss, J.W., Hurley, R.A., Taber, K.H., Rauch, R.A., Norton,R.E., and Hayman, L.A. (2000). Functional neuroanatomy ofthe frontal lobe circuits. Radiology 214, 227–230.
Corrigan, J.D., Selassie, A.W., and Orman, J.A. (2010). The epi-demiology of traumatic brain injury. J. Head Trauma Rehabil.25, 72–80.
Duchesne, N., Soucy, J.P., Masson, H., Chouinard, S., and Be-dard, M.A. (2002). Cognitive deficits and striatal dopaminer-gic denervation in Parkinson’s disease: a single photonemission computed tomography study using 123iodine-beta-CIT in patients on and off levodopa. Clin. Neuropharmacol.25, 216–224.
Falo, M.C., Fillmore, H.L., Reeves, T.M., and Phillips, L.L. (2006).Matrix metalloproteinase-3 expression profile differentiatesadaptive and maladaptive synaptic plasticity induced bytraumatic brain injury. J. Neurosci. Res. 84, 768–781.
Fleminger, S., Greenwook, R.J., and Oliver, D.L. (2006). Phar-macological management for agitation and aggression inpeople with acquired brain injury. Cochrane Database Syst.Rev. 18, CD003299.
Fleminger, S. (2008). Long-term psychiatric disorders aftertraumatic brain injury. Eur. J. Anaesthesiol. Suppl. 42, 123–130.
Francisco, G.E., Walker, W.C., Zasler, N.D., and Bouffard, M.H.(2007). Pharmacological management of neurobehaviouralsequelae of traumatic brain injury: a survey of current phy-siatric practice. Brain Inj. 21, 1007–1014.
Green, R.E., Colella, B., Hebert, D.A., Bayley, M., Kang, H.S.,Till, C., and Monette, G. (2008). Prediction of return to pro-ductivity after severe traumatic brain injury: Investigations ofoptimal neuropsychological tests and timing of assessment.Arch. Phys. Med. Rehabil. 89, S51–S60.
Gualtieri, C.T., and Evans, R.W. (1988). Stimulant treatment forthe neurobehavioural sequelae of traumatic brain injury. BrainInj. 2, 273–290.
Gualtieri, C.T. (1988). Pharmacotherapy and the neurobeha-vioural sequelae of traumatic brain injury. Brain Inj. 2,101–129.
Heilman, K.M., Voeller, K.K., and Nadeau, S.E. (1991). A pos-sible pathophysiologic substrate of attention deficit hyperac-tivity disorder. J. Child Neurol. 6 Suppl. S76–S81.
Higgins, J., and Altman, D. (2008). Assessing risk of bias in in-cluded studies, in: Cochrane Handbook for Systematic Reviews ofInterventions. J.P.T. Higgins and S. Green (eds). The CochraneCollaboration, Version 5.0.1. Available from www.cochrane-handbook.org.
Higgins, J., Deeks, J., and Altman, D. (2008). Special topics instatistics, in: Cochrane Handbook for Systematic Reviews of In-terventions. J.P.T. Higgins and S. Green (eds). The CochraneCollaboration, Version 5.0.1. Available from www.cochrane-handbook.org.
Kim, Y.H., Ko, M.H., Na, S.Y., Park, S.H., and Kim, K.W. (2006).Effects of single-dose methylphenidate on cognitive perfor-mance in patients with traumatic brain injury: a double-blindplacebo-controlled study. Clin. Rehabil. 20, 24–30.
Lammi, M.H., Smith, V.H., Tate, R.L., and Taylor, C.M. (2005).The minimally conscious state and recovery potential: a fol-low-up study 2 to 5 years after traumatic brain injury. Arch.Phys. Med. Rehabil. 86, 746–754.
Larson, E.B., and Zollman, F.S. (2010). The effect of sleep med-ications on cognitive recovery from traumatic brain injury. J.Head Trauma Rehabil. 25, 61–67.
Lee, H., Kim, S.W., Kim, J.M., Shin, I.S., Yang, S.J., and Yoon, J.S.(2005). Comparing effects of methylphenidate, sertraline andplacebo on neuropsychiatric sequelae in patients with trau-matic brain injury. Hum. Psychopharmacol. 20, 97–104.
Lefebvre, C., Manheimer, E., and Glanville, J. (2009). Searchingfor studies, in: Cochrane Handbook for Systematic Reviews of In-terventions. J.P.T. Higgins and S. Green (eds). The CochraneCollaboration, Version 5.0.2. Available from www.cochrane-handbook.org.
Loke, Y., Price, D., and Herxheimer, A. (2008). Adverse effects,in: Cochrane Handbook for Systematic Review of Interventions.J.P.T. Higgins and S. Green (eds). The Cochrane Collabora-tion, Version 5.0.1. Available from www.cochrane-hand-book.org.
Maas, A.I., Marmarou, A., Murray, G.D., and Steyerberg, E.W.(2004). Clinical trials in traumatic brain injury: current prob-lems and future solutions. Acta Neurochir. Suppl. 89, 113–118.
Maas, A.I., Steyerberg, E.W., Marmarou, A., McHugh, G.S.,Lingsma, H.F., Butcher, I., Lu, J., Weir, J., Roozenbeek, B., andMurray, G.D. (2010). IMPACT recommendations for improv-ing the design and analysis of clinical trials in moderate tosevere traumatic brain injury. Neurotherapeutics 7, 127–134.
Mahalick, D.M., Carmel, P.W., Greenberg, J.P., Molofsky, W.,Brown, J.A., Heary, R.F., Marks, D., Zampella, E., Hodosh, R.,and von der Schmidt, E., 3rd. (1998). Psychopharmacologictreatment of acquired attention disorders in children withbrain injury. Pediatr. Neurosurg. 29, 121–126.
McCauley, S.R., Wilde, E.A., Anderson, V.A., Bedell, G., Beers,S.R., Campbell, T.F., Chapman, S.B., Ewing-Cobbs, L., Ger-ring, J., Gioia, G.A., Levin, H., Michaud, L., Prasad, M.R.,Swaine, B., Turkstra, L.A., Wade, S.L., and Yeates, K.O. (2011).Recommendations for the use of common outcome measuresin pediatric traumatic brain injury research. J. Neurotrauma[Epub ahead of print].
McDowell, S., Whyte, J., and D’Esposito, M. (1998). Differentialeffect of a dopaminergic agonist on prefrontal function intraumatic brain injury patients. Brain 121 (Pt. 6), 1155–1164.
McMahon, M.A., Vargus-Adams, J.N., Michaud, L.J., and Bean,J. (2009). Effects of amantadine in children with impairedconsciousness caused by acquired brain injury: a pilot study.Am. J. Phys. Med. Rehabil. 88, 525–532.
Meintzschel, F., and Ziemann, U. (2006). Modification of prac-tice-dependent plasticity in human motor cortex by neuro-modulators. Cereb. Cortex 16, 1106–1115.
Meythaler, J.M., Brunner, R.C., Johnson, A., and Novack, T.A.(2002). Amantadine to improve neurorecovery in traumaticbrain injury-associated diffuse axonal injury: a pilot double-blind randomized trial. J. Head Trauma Rehabil. 17, 300–313.
Moein, H., Khalili, H.A., and Keramatian, K. (2006). Effect ofmethylphenidate on ICU and hospital length of stay in pa-tients with severe and moderate traumatic brain injury. Clin.Neurol. Neurosurg. 108, 539–542.
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D.G. (2009).Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535.
Mooney, G.F., and Haas, L.J. (1993). Effect of methylphenidateon brain injury-related anger. Arch. Phys. Med. Rehabil. 74,153–160.
Nieoullon, A. (2002). Dopamine and the regulation of cognitionand attention. Prog. Neurobiol. 67, 53–83.
Patry, B.N., and Mateer, C.A. (2006). Neuropsychological as-sessment of moderate to severe traumatic brain injury, in:Psychological Knowledge in Court. G. Young, K. Nicholson, andA.W. Kane (eds). Springer: New York, pps. 352–377.
16 FRENETTE ET AL.

Plenger, P.M., Dixon, C.E., Castillo, R.M., Frankowski, R.F.,Yablon, S.A., and Levin, H.S. (1996). Subacute methylpheni-date treatment for moderate to moderately severe traumaticbrain injury: a preliminary double-blind placebo-controlledstudy. Arch. Phys. Med. Rehabil. 77, 536–540.
Ruttan, L., Martin, K., Liu, A., Colella, B., and Green, R.E. (2008).Long-term cognitive outcome in moderate to severe traumaticbrain injury: A meta-analysis examining timed and untimedtests at 1 and 4.5 or more years after injury. Arch. Phys. Med.Rehabil. 89, S69–S76.
Saatman, K.E., Duhaime, A.C., Bullock, R., Maas, A.I., Valadka,A., and Manley, G.T. (2008). Classification of traumatic braininjury for targeted therapies. J. Neurotrauma 25, 719–738.
Schneider, W.N., Drew-Cates, J., Wong, T.M., and Dombovy,M.L. (1999). Cognitive and behavioural efficacy of amantadinein acute traumatic brain injury: an initial double-blind place-bo-controlled study. Brain Inj. 13, 863–872.
Scottish Intercollegiate Guidelines Network. Search filters, in:Scottish Intercollegiate Guidelines Network. Retrieved No-vember 2009 from http://www.sign.ac.uk/methodology/fil-ters.html#random.
Shukla, D., Devi, B.I., and Agrawal, A. (2011). Outcome mea-sures for traumatic brain injury. Clin. Neurol. Neurosurg. 113,435–441.
Siddall, O.M. (2005). Use of methylphenidate in traumatic braininjury. Ann. Pharmacother. 39, 1309–1313.
Sivan, M., Neumann, V., Kent, R., Stroud, A., and Bhakta, B.B.(2010). Pharmacotherapy for treatment of attention deficitsafter non-progressive acquired brain injury. A systematic re-view. Clin. Rehabil. 24, 110–121.
Speech, T.J., Rao, S.M., Osmon, D.C., and Sperry, L.T. (1993). Adouble-blind controlled study of methylphenidate treatmentin closed head injury. Brain Inj. 7, 333–338.
Stern, Y., Tetrud, J.W., Martin, W.R., Kutner, S.J., and Langston,J.W. (1990). Cognitive change following MPTP exposure.Neurology 40, 261–264.
Tanaka, S. (2006). Dopaminergic control of working memoryand its relevance to schizophrenia: a circuit dynamics per-spective. Neuroscience 139, 153–171.
Tenovuo, O. (2006). Pharmacological enhancement of cognitiveand behavioral deficits after traumatic brain injury. Curr.Opin. Neurol. 19, 528–533.
Thobois, S., Vingerhoets, F., Fraix, V., Xie-Brustolin, J., Mollion,H., Costes, N., Mertens, P., Benabid, A.L., Pollak, P., andBroussolle, E. (2004). Role of dopaminergic treatment in do-pamine receptor down-regulation in advanced Parkinsondisease: a positron emission tomographic study. Arch. Neurol.61, 1705–1709.
Thurman, D., and Guerrero, J. (1999). Trends in hospitalizationassociated with traumatic brain injury. JAMA 282, 954–957.
Tsaousides, T., and Gordon, W.A. (2009). Cognitive rehabilita-tion following traumatic brain injury: Assessment to treat-ment. Mt. Sinai J. Med. 76, 173–181.
Whyte, J., Hart, T., Schuster, K., Fleming, M., Polansky, M., andCoslett, H.B. (1997). Effects of methylphenidate on attentionalfunction after traumatic brain injury. A randomized, placebo-controlled trial. Am. J. Phys. Med. Rehabil. 76, 440–450.
Whyte, J., Hart, T., Vaccaro, M., Grieb-Neff, P., Risser, A., Po-lansky, M., and Coslett, H.B. (2004). Effects of methylpheni-date on attention deficits after traumatic brain injury: amultidimensional, randomized, controlled trial. Am. J. Phys.Med. Rehabil. 83, 401–420.
Whyte, J., Vaccaro, M., Grieb-Neff, P., Hart, T., Polansky, M.,and Coslett, H.B. (2008). The effects of bromocriptine on at-tention deficits after traumatic brain injury: a placebo-con-trolled pilot study. Am. J. Phys. Med. Rehabil. 87, 85–99.
Wilde, E.A., Whiteneck, G.G., Bogner, J., Bushnik, T., Cifu, D.X.,Dikmen, S., French, L., Giacino, J.T., Hart, T., Malec, J.F., Millis,S.R., Novack, T.A., Sherer, M., Tulsky, D.S., Vanderploeg, R.D.,and von Steinbuechel. N. (2010). Recommendations for the useof common outcome measures in traumatic brain injury re-search. Arch. Phys. Med. Rehabil. 91, 1650–1660.
Williams, S.E., Ris, M.D., Ayyangar, R., Schefft, B.K., and Berch,D. (1998). Recovery in pediatric brain injury: is psychostimu-lant medication beneficial? J. Head Trauma Rehabil. 13, 73–81.
Willmott, C., and Ponsford, J. (2009). Efficacy of methylphenidatein the rehabilitation of attention following traumatic brain in-jury: a randomised, crossover, double blind, placebo controlledinpatient trial. J. Neurol. Neurosurg. Psychiatry 80, 552–557.
Willmott, C., Ponsford, J., Olver, J., and Ponsford, M. (2009).Safety of methylphenidate following traumatic brain injury:impact on vital signs and side-effects during inpatient reha-bilitation. J. Rehabil. Med. 41, 585–587.
Wood, L.D. (2010). Clinical review and treatment of select ad-verse effects of dopamine receptor agonists in Parkinson’sdisease. Drugs Aging 27, 295–310.
Writer, B.W., and Schillerstrom, J.E. (2009). Psychopharmacolo-gical treatment for cognitive impairment in survivors oftraumatic brain injury: a critical review. J. NeuropsychiatryClin. Neurosci. 21, 362–370.
Address correspondence to:Anne Julie Frenette, BPharm, M.Sc.Hopital du Sacre-Coeur de Montreal
Faculty of PharmacyUniversity of Montreal
5400 Gouin OuestMontreal, Quebec, Canada, H4J 1C5
E-mail: [email protected]
(Appendix follows/)
DOPAMINE AGONISTS AND TRAUMATIC BRAIN INJURY 17

Appendix 1. Search Strategy for MEDLINE
1 head trauma.mp. 99192 head injury.mp. 366813 head injuries.mp. 111774 brain trauma.mp. 24215 ‘‘brain injuries’’.mp. or expBrain Injuries/ 1053836 cerebral trauma.mp. 9987 cerebral injury.mp. 25928 cerebral injuries.mp. 6669 ‘‘craniocerebral trauma’’.mp. or exp Craniocerebral Trauma/ 21137310 craniocerebral injury.mp. 92011 craniocerebral injuries.mp. 100812 brain injury.mp. 8193713 Traumatic brain injury.mp. 2421514 Traumatic brain injuries.mp. 127515 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 23495316 exp Dopamine Agonists/ 13445117 dopamine agonist$.tw. 1128518 bromocriptine.tw. 1222719 amantadine.tw. 530020 levodopa.tw. 1413421 methylphenidate.tw. 829222 apomorphine.tw. 1588723 ropinirole.tw. 105824 pramipexole.tw. 136725 pergolide.tw. 202526 cabergoline.tw. 159127 exp Dopamine Agents/ 29840028 or/16-27 31259329 15 and 28 363030 Randomized controlled trial.pt. 57270931 Controlled clinical trial.pt. 16080832 randomized.ab. 54810033 placebo.ab. 33807734 Drug therapy.fs. 139336235 randomly.ab. 35954036 group.ab. 258074537 trial.ab. 50674938 37 or 36 or 35 or 34 or 33 or 32 or 31 or 30 462654639 38 and 29 92540 remove duplicates from 39 790
18 FRENETTE ET AL.




















