
Acute neuromuscular and fatigue responses to the rest-pause method
Available online at www.sciencedirect.com
ScienceDirect
Journal of Exercise Science & Fitness 11 (2013) 107e117www.elsevier.com/locate/jesf
Original article
Effects of antecedent flexibility conditioning on neuromuscular andsensorimotor performance during exercise-induced muscle damage
Nigel Gleeson a,*, Roger Eston b,c, Claire Minshull a, Andrea Bailey d, Abdul Hameed Al Kitani a,Haider Darain a, Christopher Yates a, David Rees d
a School of Health Sciences, Queen Margaret University, Edinburgh EH21 6UU, UKb School of Health Sciences, Sansom Institute for Health Research, University of South Australia, Adelaide, Australia
c Sport and Health Sciences, College of Life and Environmental Sciences, Exeter University, Exeter, UKdNational Centre for Sports Injury Surgery, Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry SY10 7AG, UK
Received 21 November 2013; accepted 22 November 2013
Available online 17 December 2013
Abstract
The aim of this study was to assess the effects of two modes of antecedent flexibility conditioning on neuromuscular and sensorimotorperformance during a subsequent episode of exercise-induced muscle damage (EIMD). Twenty-four males (age 20.9 � 2.3 years; height1.78 � 0.06 m; body mass 72.3 � 7.4 kg, mean � SD) were randomly assigned to interventions comprising 6 weeks of thrice-weekly flexibilityconditioning of the hip region and knee flexor musculature in the dominant limb involving proprioceptive neuromuscular facilitation (n ¼ 8),passive exercise (n ¼ 8), or no exercise as a control (n ¼ 8). Musculoskeletal, neuromuscular, and sensorimotor assessments were carried out atbaseline, after conditioning, and before and up to 168 hours after damaging exercise of the ipsilateral knee flexors. Flexibility conditioning andEIMD elicited transient performance decreases in volitional electromechanical delay (up to 40.1% compared to baseline; 67.5 � 12.3 milli-seconds vs. 47.9 � 9.7 milliseconds, mean � SD, 48-hour post- vs. pre-EIMD; p < 0.01), passive hip flexibility (up to 19.9%; 96.7� � 8.2� vs.120.7� � 11.0�, p < 0.001) and sensorimotor capability (manifold error increase to 10.8%; 10.8% � 6.9% vs. 0.3% � 3.7%, p < 0.05) andexceeded the effects of eccentric exercise alone. EIMD-related performance decreases were especially prominent when preceded by passiveflexibility conditioning, and were sufficiently potent following both modes of antecedent conditioning to raise concerns about compromisedcapability for rapid and dynamic stabilization of synovial joints.Copyright � 2013, The Society of Chinese Scholars on Exercise Physiology and Fitness. Published by Elsevier (Singapore) Pte Ltd. All rightsreserved.
Keywords: Flexibility; Muscle damage; Neuromuscular; Sensorimotor
Introduction
Skeletal muscle is susceptible to ultrastructural damagefollowing unaccustomed high-intensity eccentric exercise.1,2
Exercise-induced muscle damage (EIMD) may be attributedto excessive stressing of relatively small numbers of activemotor units and fibers,3 particularly type II fast-twitch fibers,4
whose recruitment also corresponds to the most rapid and
* Corresponding author. School of Health Sciences, Queen Margaret Uni-
versity, Edinburgh EH21 6UU, UK.
E-mail address: [email protected] (N. Gleeson).
1728-869X/$ - see front matter Copyright � 2013, The Society of Chinese Scholars on Exerci
http://dx.doi.org/10.1016/j.jesf.2013.11.003
forceful activation patterns and net joint moments.5 Thisprocess may be especially prominent in patterns of functionalactivity for which musculoskeletal systems such as the kneejoint have been operating at vulnerable positions near to fullextension6 and have been activating muscle eccentrically atrelatively long lengths, corresponding to the plateau ordescending limb of the muscle forceejoint angle curve. In thisscenario, an increased number of sarcomeres lengthen to thepoint of no myofilament overlap. Subsequent failure to re-interdigitate leads to disrupted sarcomeres and EIMD.7e11
Major functional consequences of EIMD are immediate andinvolve prolonged reductions in peakmuscle force ranging from
se Physiology and Fitness. Published by Elsevier (Singapore) Pte Ltd. All rights reserved.

108 N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
50% to 70%,12e15 reductions in peak power ranging from 15%to 20%, and decreases of approximately 25% in the rate of forcedevelopment.16e18 Corresponding changes in athletic perfor-mance can include a 2e3% reduction in sprint speed over10 m,19 a 10e15% increase in contact time during plyometricdrop jumping, a 9% decrease in jump height during squatjumping, a 5% decrease in counter-movement jump perfor-mance,20 and decrements in sensorimotor performance.21
Thus, the capability of the neuromuscular system to resistthreats of injury posed by external forces applied to synovialjoint systems may also be compromised under these circum-stances. Serious musculoskeletal injuries in pre-seasontraining22 may be associated with EIMD, since any decondi-tioning during the prior extended rest period23,24 could haveexacerbated susceptibility to EIMD and injury.25 Similarly,exercise challenges during rehabilitation programs inherentlyrepresent unaccustomed and strenuous tasks for a recentlyrestored musculoskeletal system possessing low physiologicalcapacity. This has given rise to clinical concerns that routineEIMD provocation during the rehabilitation process mayattenuate the recovery of the neuromuscular system to optimallevels of performance capacity and hinder dynamic stabiliza-tion of the musculoskeletal system.26
Flexibility and stiffness of muscle and connective tissuecould be important determinants of the extent of EIMDsymptoms. For example, increased passive hamstring musclestiffness is associated with reduced flexibility as assessed inthe straight-leg-raise range of motion (ROM) and with moresevere symptoms of damage.27 Evidence from cross-sectionalstudies suggests that the greater flexibility and compliance ofchildren’s muscles may explain why peak muscle force occursat longer muscle lengths in children than in adults and whyboys suffer less severe symptoms of EIMD than men do.28
Conditioning for flexibility offers potential amelioration ofthe apparent negative symptoms associated with EIMD. Priorconditioning might lead to a greater number of sarcomeres inseries within the muscle29 and decrease the length of indi-vidual sarcomeres as the muscle operates at any given lengthand joint position. Thus, less severe EIMD symptoms wouldbe expected because fewer sarcomeres would be operating inmechanically vulnerable positions. Passive stretching of themusculature involved and stretching following proprioceptiveneuromuscular facilitation (PNF) involving static activationsof the stretched muscle as an antecedent to optimizedmuscular relaxation have become popular modes of condi-tioning in contemporary practice owing to their efficacy.8,30
Mechanical loading of the knee joint can often exceed thetensile capacities of the passive structures31 during strenuousactivities. As a consequence, greater reliance may be placed onthe timely responses, functioning, and protective capabilities ofthe surrounding musculature to maintain joint integrity.32e38
Sensorimotor performance has been defined as the ability toscale volitional force and joint positioning precisely,35 and su-perior capability has been associated with protection frominjury.36e38 Electromechanical delay (EMD) is an importantaspect of motor performance and the reaction time between theonset of electrical activity and the onset of tension in skeletal
muscle.39 It is associated with propagation of action potentialsthrough muscles and, importantly, the rate of stretching of theseries elastic component (SEC).40 EMD performance may alsobe influenced by the loading of viscoelastic structures,which cancause creep within the affected tissue and modulation of theneuromuscular performance characteristics of the associatedmusculature.41e43 It has been shown that conditioning-relatedenhancement of flexibility and concomitant decreases in thestiffness of muscle and connective tissue negatively influenceEMD.44 By contrast, conditioning of sensorimotor performance,effective afferent and efferent signaling, and musculature acti-vation characteristics would be expected to favorably affect thecapability to scale and regulate motor responses precisely. Thismight be especially important at end-range joint positions, inwhich the majority of serious ligament injuries occur.6,38,44
A potentially interesting paradox is that while conditioning-related effects of increased compliance within joint- andmuscle-related connective tissue might usefully moderate theseverity of EIMD, they might also result in a hypercompliantsystem that would be less likely to be capable of restraining highjoint loads rapidly enough to prevent ligamentous injury.Furthermore, it is biologically plausible that conditioning- andEIMD-related changes in joint flexibility and the mechanicalcompliance characteristics within the joint system mightadversely affect sensorimotor performance and the capability toscale and regulate force, limb positioning, and other motor re-sponses precisely.45,46
While there has been evidence from two studies of a trendtowards an increase in flexibility of the hamstring musclegroup offering some protection from strength loss at longmuscle lengths following EIMD,47,48 no study to date hasinvestigated the interactive effects of conditioning for flexi-bility and EIMD on the capability for rapid neuromuscularactivation and sensorimotor performance.
The aim of this study was to assess the effects of two modesof antecedent flexibility conditioning of the hip region andknee flexor musculature on musculoskeletal and sensorimotorperformance during a subsequent bout of EIMD in males.
Methodology
Participants
Twenty-four men (age 20.9 � 2.3 years; height1.78 � 0.06 m; body mass 72.3 � 7.4 kg, mean � SD) gaveinformed consent to participate in the study. All participantswere regularly involved in exercise (at least 3 times per week)and were asymptomatic at the time of assessment. Participantswere instructed to refrain from strenuous physical activity for the24 hours prior to testing. Assessment protocols were approvedby the Institutional Ethics Committee for Human Testing(University of Wales Bangor, UK).
Experimental procedures
Following habituation procedures, participants completed astandardized warm-up of 5 minutes of cycle ergometry (90 W)
109N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
and a further 5 minutes of static stretching of the musculatureinvolved.
The experimental design involved a mixed-model approachand comparison of the responses of three randomly allocatedindependent groups to: (1) a single-leg exercise interventionfor the preferred leg, with a contralateral limb and time-matched experimental control, to verify the extent ofconditioning-related changes in two types of flexibility; and(2) a subsequent treatment condition involving a single-legEIMD intervention with a contralateral limb experimentalcontrol.
Passive hip flexibility, peak force, volitional EMD (EMDV),magnetically evoked EMD (EMDE), and sensorimotor per-formance (force and position errors) capabilities were assessedin the knee flexor musculature in both the preferred andcontralateral control limb of participants before and immedi-ately after: (1) an intervention condition comprising 6 weeksof twice-weekly flexibility conditioning8,47 of the hip regionand knee flexor musculature in the preferred limb (defined asthe limb preferred for kicking of a ball with maximum ve-locity) involving PNF (n ¼ 8), passive exercise (n ¼ 8), or noconditioning as a control (n ¼ 8); and (2) a 6-week no-exercisecontrol undertaken prior to conditioning. The control periodallowed estimation of the extent of random biological varia-tions in outcomes and any intrusions from systematic effectssuch as learning. The duration used for flexibility conditioning
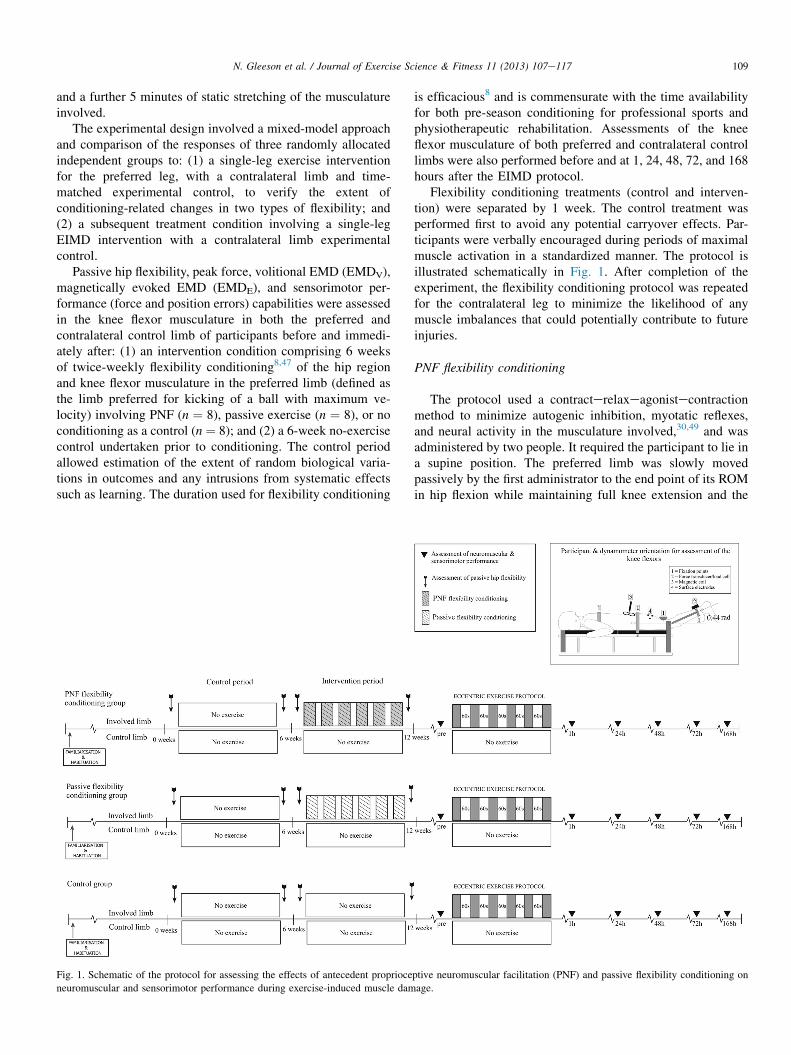
Fig. 1. Schematic of the protocol for assessing the effects of antecedent proprioce
neuromuscular and sensorimotor performance during exercise-induced muscle dam
is efficacious8 and is commensurate with the time availabilityfor both pre-season conditioning for professional sports andphysiotherapeutic rehabilitation. Assessments of the kneeflexor musculature of both preferred and contralateral controllimbs were also performed before and at 1, 24, 48, 72, and 168hours after the EIMD protocol.
Flexibility conditioning treatments (control and interven-tion) were separated by 1 week. The control treatment wasperformed first to avoid any potential carryover effects. Par-ticipants were verbally encouraged during periods of maximalmuscle activation in a standardized manner. The protocol isillustrated schematically in Fig. 1. After completion of theexperiment, the flexibility conditioning protocol was repeatedfor the contralateral leg to minimize the likelihood of anymuscle imbalances that could potentially contribute to futureinjuries.
PNF flexibility conditioning
The protocol used a contracterelaxeagonistecontractionmethod to minimize autogenic inhibition, myotatic reflexes,and neural activity in the musculature involved,30,49 and wasadministered by two people. It required the participant to lie ina supine position. The preferred limb was slowly movedpassively by the first administrator to the end point of its ROMin hip flexion while maintaining full knee extension and the
ptive neuromuscular facilitation (PNF) and passive flexibility conditioning on
age.

110 N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
dorsiflexion of the foot to 90�. During the latter maneuver, theparticipant’s contralateral control limb was held by the secondadministrator in full knee extension, in contact with the sup-port surface and with the ipsilateral hip joint in a neutral po-sition. The participant verbally signaled unwillingness totolerate any further increases in ROM for the joint involved.
The participant then performed a maximal voluntarycontraction of the antagonist muscle group (knee flexors andhip extensors) of the preferred limb for 10 seconds while theleg was held in the standardized position at the end point of itsROM in hip flexion. The administrators gave strong verbalencouragement in a standardized manner to the participantduring each contraction. This procedure was followed by aperiod of relaxation of 5 seconds in duration. The participantwas then required to activate the agonist muscle groups (kneeextensors and hip flexors) maximally and, assisted by the firstadministrator, move the limb being conditioned to a new andimproved end-point position. This new position was held for10 seconds. This procedure was repeated twice more. Main-tenance of the end-point position for 10 seconds followedliterature recommendations on the experimental effect size forimprovements in flexibility.8
Passive flexibility conditioning
Following a similar protocol to that described for PNFflexibility conditioning, participants undertaking passive flex-ibility conditioning had the preferred limb taken slowly andpassively by the first administrator to the end point of its ROMin hip flexion. The end-point position was maintainedpassively by the administrator for a 10-second period and wasfollowed by 5 seconds of relaxation. This procedure wasrepeated twice more.
EIMD protocol
The EIMD protocol consisted of a warm-up (five sub-maximal and five maximal eccentric activations) of the kneeflexors of the preferred leg, followed by six sets (each sepa-rated by 1 minute) of 10 repetitions of maximal eccentricactivations (60�/second; movement range from 80� to 10� ofknee flexion, where 0� represents full extension) using anisokinetic dynamometer (Kin-Com, 500 H, Chattecx, Chatta-nooga, TN, USA) with the participant in a sitting position.Participants were requested to contract the knee flexorsmaximally to resist knee extension on each repetition and weregiven verbal encouragement and real-time visual feedback bymeans of a computerized visual display.
Assessment of passive hip flexibility
Participants lay supine on a padded mat with both legssplinted to prevent knee flexion. A Leighton flexometer(Spokane, WA, USA) was attached to the lateral epicondyle ofthe femur and the assessor flexed the hip through to themaximum ROM tolerated by the participant; the contralaterallimb was held straight and in contact with the ground. The
mean of three estimates of ROM (�0.5�) was used for sub-sequent analysis. The same protocol was used to assess thepassive hip flexibility of the contralateral limb; the order oflimb assessment was randomized.
Assessment of neuromuscular performance
Participants were secured in a prone position on a purpose-built dynamometer33 with the knee flexed to a functionallyrelevant angle of 25� (where 180� represents full extension),which is associated with the greatest mechanical strain on keyligaments.50 The bilateral lever arms of the dynamometer wereattached to the participant’s legs via padded ankle cuffs andadjustable strapping just proximal to the lateral malleolus.Further strapping was placed across the mid-thoracic spine,pelvis, and posterior thigh proximal to the knee. The axes ofrotation of the dynamometer and the knee joint were alignedas closely as possible. Following a series of submaximalwarm-up muscle activations, an auditory signal was givenrandomly within 1e4 seconds to instruct the participants toflex the knee joint as rapidly and forcefully as possible againstthe immovable restraint offered by the apparatus (load cell615, Tedea-Huntleigh, Cardiff, UK). Another auditory signalwas given to the participant after 2e3 seconds of maximalvoluntary muscle activation (MVMA) to cue neuromuscularrelaxation. Each MVMA was separated from the next by atleast 10 seconds.
Supra-maximal magnetic stimulation of the sciatic nerve(L4eL5) with associated activation of the knee flexors wasachieved by means of double-wound coil (120 mm) poweredby a Magstim 200 stimulator (Magstim, Whitland, UK). Theprotocol used to elicit and verify supra-maximal stimulationwas in accordance with methodology described previously.44
In brief, the magnetic coil was placed over the L4eL5 re-gion and small iterative changes in the coil position were madethat were commensurate with the increasing size of responsesduring a series of discrete stimulations. The optimum site forstimulation of the nerve was defined as the site that elicited thelargest twitch force and M-wave amplitude. Supra-maximalstimulation was verified by visual inspection of the data dur-ing a sequence of seven discrete stimulations of increasingintensity, starting at 40% of the maximal stimulator output andincreasing in 10% steps to 100%, and retrospective analyses ofM-wave and peak twitch-force data.44 This optimized coilposition was manually maintained throughout the remainder ofthe test. Three supra-maximal stimulations (100% of stimu-lator output), each separated by 10 seconds, were delivered toobtain three estimates of magnetically evoked neuromuscularperformance.
Indices of neuromuscular performance
Static peak force (PF) was recorded as the mean score ofthe highest force response achieved during three intra-trialreplicates. Compensation procedures for gravitational errorsin forces recorded in the vertical plane were undertakenimmediately prior to testing. EMDV and EMDE were

111N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
computed as the time delay between the onset of electricalactivity and the onset of force (mean of three intra-trial esti-mates). The onsets of force and electrical activity were definedas the first time point at which the recorded signal consistentlyexceeded the 95% confidence limits for the backgroundelectrical noise amplitude in quiescent muscle.44
Assessment of sensorimotor performance
All assessments were performed in the prone position, asdescribed above. Familiarization and learning (detailsdescribed below) for sensorimotor performance tasks tookplace the day before the control period. Brief refamiliarizationof each task was performed on each assessment occasion.Force error (FE) was evaluated during a series of five briefmuscular activations and relaxations (1 Hz) in which the aimwas precise and blind attainment of a target force (50% of PFat 25� of knee flexion) using the knee flexors. The FE extentdescribes the bias or constant error around a target force andlower scores reflect better sensorimotor performance. Duringlearning, participants received only standardized verbal feed-back during practice target matching (50% PF) and learned toself-perceive the performance outcomes on an arbitrary mea-surement scale without units. The task was deemed to havebeen learned once the participant was capable of consistentlyproducing 10 trials in which seven or more scores showederrors within � 2.0 N of the blind target force (approximatelyto the 99% confidence limits of the technical error associatedwith the load cell system). FE was computed asFE ¼ [(observed performance score � target performancescore) / target performance score] � 100%, and the mean errorfor five serial trials was used for subsequent data analysis.Positional error (PE) was assessed by five brief serial recip-rocal movements (1 Hz) aimed at precisely reproducingspecified knee angles. From a reference angle (90�), eachparticipant extended the knee to a specified target angle (25�)and then returned it to the reference angle without visualfeedback. Familiarization and learning procedures weresimilar to those described for FE. The target angle was learntin a blinded fashion and learning was verified to a prescribedlevel of precision (�2�). The dynamometer was equipped withdigital optical encoders for angle positioning and interfaced tothe computerized recording system. PE was described as meandiscrepancy from the target across five intra-trial replicatesand expressed as a percentage relative to the target kneeflexion angle as PE ¼ [(observed performance score � targetperformance score) / target performance score] � 100%.
Indirect markers of muscle damage
Subjective scores for muscle soreness and blood sampleswere obtained before each assessment occasion. Participantsrated soreness on a 100-cm visual analog scale followingstretching and active knee flexion. Statements on the scaleincluded “my muscles do not feel sore at all” and “my musclesfeel so sore that I do not want to move them”, corresponding tonumerical ratings of 0 and 10, respectively.
Whole fresh blood (30 mL) was collected via fingertipcapillary puncture into heparinized tubes and pipetted onto teststrips for analysis of plasma creatine kinase (CK) activity bycolorimetry (Reflotron, Boehringer Mannheim, Mannheim,Germany). CK values were used as an indirect measure ofmuscle ultrastructural integrity and data were subjected tologarithmic transformations for statistical analysis.26
Statistical analysis
The effect of the two modes of flexibility conditioning onhip flexibility was assessed using separate two (condition:control or conditioning) by two (time: pre or post) by two(limb: involved or contralateral) by three (group: passive, PNF,or control) mixed-model analysis of variance (ANOVA) withrepeated measures for the first three factors. Assumptionsunderpinning the use of ANOVAwith repeated measures werechecked and violations were corrected using Green-houseeGeisser adjustment of the critical F-value, as indicatedby the subscript GG. Statistical analyses were performed usingSPSS version 19 (SPSS Inc., Chicago, IL, USA) and signifi-cance was set to p < 0.05.
Effects of EIMD on each measure of neuromuscular per-formance (PF, EMDV, EMDE, FE, PE, hip flexibility) wereevaluated using separate six (time: pre or 1, 24, 48, 72, or 168hours after) by two (limb: involved or contralateral) by three(group: passive, PNF, or control) mixed-model ANOVA withrepeated measures for the first two factors.
Perceived soreness and CK levels were assessed by separatesix (time: pre or 1, 24, 48, 72, or 168 hours after) by two (limb:involved or contralateral) by three (group: passive, PNF, orcontrol) mixed-model ANOVAwith repeated measures for thefirst two factors.
The experimental design offered an approximate power of0.80 for avoiding a type II error for a least detectable differ-ence of 16 N for PF, 5 milliseconds for EMDV, 2.5 millisec-onds for EMDE, 6% for FE, 8% for PE, and 1.5� for hipflexibility.
Results
Passive hip flexibility
A significant three-factor interaction showed that whilepassive hip flexibility was preserved during the control period,in the contralateral limb, and within the performance of thecontrol group, both flexibility conditioning programs elicited asimilarly significant improvement in hip flexibility comparedto baseline performance (passive: 99.6� � 5.0� vs.89.1� � 5.2�; PNF: 120.1� � 16.4� vs. 94.4� � 18.6�, groupmean score � SD; F[1,21] ¼ 14.0; p < 0.01). Prior to theantecedent conditioning interventions, passive hip flexibilitydid not differ between the groups (F[2, 21] ¼ 0.15; p > 0.5).
A significant leg � time interaction (F[5, 105] ¼ 2.8;p < 0.01) showed that while passive hip flexibility was pre-served in the contralateral leg, EIMD intervention elicitedsimilar levels of transient reductions in flexibility compared to
112 N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
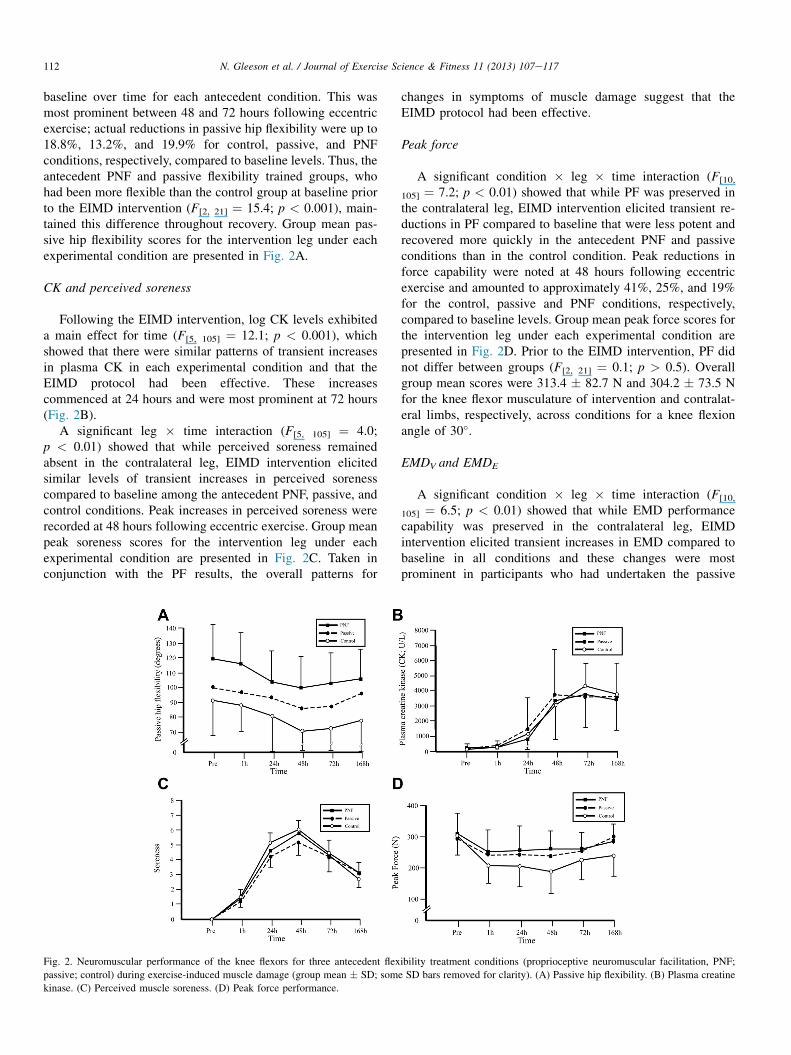
baseline over time for each antecedent condition. This wasmost prominent between 48 and 72 hours following eccentricexercise; actual reductions in passive hip flexibility were up to18.8%, 13.2%, and 19.9% for control, passive, and PNFconditions, respectively, compared to baseline levels. Thus, theantecedent PNF and passive flexibility trained groups, whohad been more flexible than the control group at baseline priorto the EIMD intervention (F[2, 21] ¼ 15.4; p < 0.001), main-tained this difference throughout recovery. Group mean pas-sive hip flexibility scores for the intervention leg under eachexperimental condition are presented in Fig. 2A.
CK and perceived soreness
Following the EIMD intervention, log CK levels exhibiteda main effect for time (F[5, 105] ¼ 12.1; p < 0.001), whichshowed that there were similar patterns of transient increasesin plasma CK in each experimental condition and that theEIMD protocol had been effective. These increasescommenced at 24 hours and were most prominent at 72 hours(Fig. 2B).
A significant leg � time interaction (F[5, 105] ¼ 4.0;p < 0.01) showed that while perceived soreness remainedabsent in the contralateral leg, EIMD intervention elicitedsimilar levels of transient increases in perceived sorenesscompared to baseline among the antecedent PNF, passive, andcontrol conditions. Peak increases in perceived soreness wererecorded at 48 hours following eccentric exercise. Group meanpeak soreness scores for the intervention leg under eachexperimental condition are presented in Fig. 2C. Taken inconjunction with the PF results, the overall patterns for
Fig. 2. Neuromuscular performance of the knee flexors for three antecedent flex
passive; control) during exercise-induced muscle damage (group mean � SD; som
kinase. (C) Perceived muscle soreness. (D) Peak force performance.
changes in symptoms of muscle damage suggest that theEIMD protocol had been effective.
Peak force
A significant condition � leg � time interaction (F[10,
105] ¼ 7.2; p < 0.01) showed that while PF was preserved inthe contralateral leg, EIMD intervention elicited transient re-ductions in PF compared to baseline that were less potent andrecovered more quickly in the antecedent PNF and passiveconditions than in the control condition. Peak reductions inforce capability were noted at 48 hours following eccentricexercise and amounted to approximately 41%, 25%, and 19%for the control, passive and PNF conditions, respectively,compared to baseline levels. Group mean peak force scores forthe intervention leg under each experimental condition arepresented in Fig. 2D. Prior to the EIMD intervention, PF didnot differ between groups (F[2, 21] ¼ 0.1; p > 0.5). Overallgroup mean scores were 313.4 � 82.7 N and 304.2 � 73.5 Nfor the knee flexor musculature of intervention and contralat-eral limbs, respectively, across conditions for a knee flexionangle of 30�.
EMDV and EMDE
A significant condition � leg � time interaction (F[10,
105] ¼ 6.5; p < 0.01) showed that while EMD performancecapability was preserved in the contralateral leg, EIMDintervention elicited transient increases in EMD compared tobaseline in all conditions and these changes were mostprominent in participants who had undertaken the passive
ibility treatment conditions (proprioceptive neuromuscular facilitation, PNF;
e SD bars removed for clarity). (A) Passive hip flexibility. (B) Plasma creatine
113N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
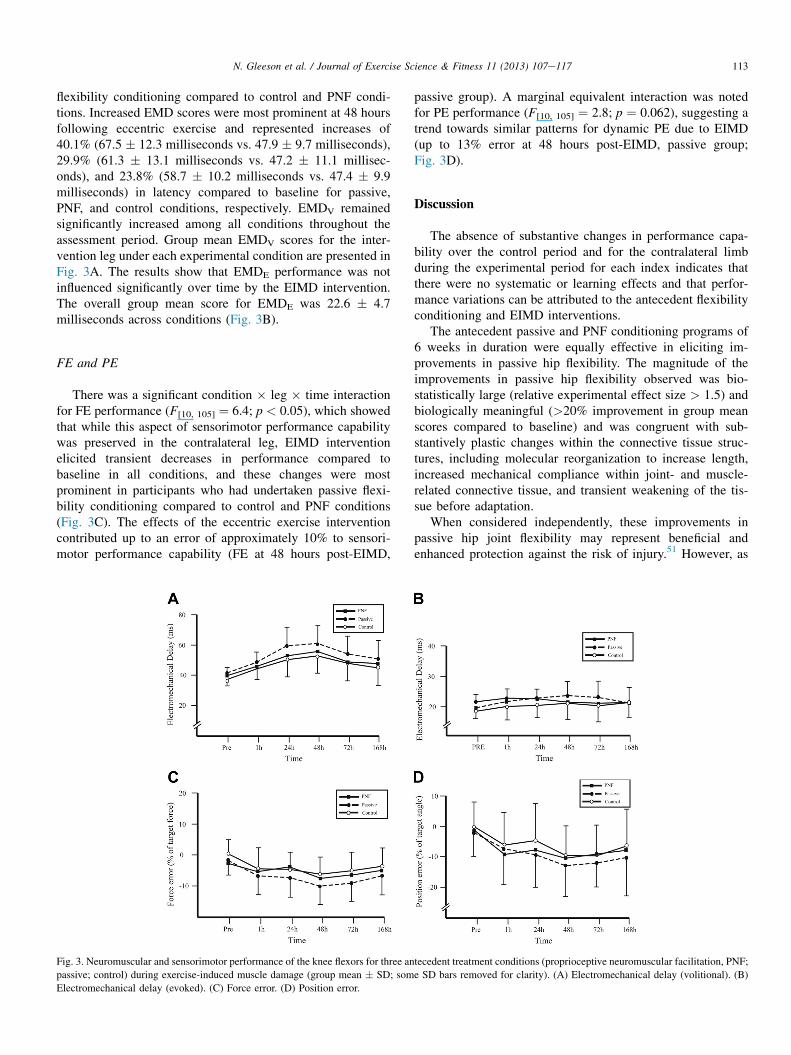
flexibility conditioning compared to control and PNF condi-tions. Increased EMD scores were most prominent at 48 hoursfollowing eccentric exercise and represented increases of40.1% (67.5 � 12.3 milliseconds vs. 47.9 � 9.7 milliseconds),29.9% (61.3 � 13.1 milliseconds vs. 47.2 � 11.1 millisec-onds), and 23.8% (58.7 � 10.2 milliseconds vs. 47.4 � 9.9milliseconds) in latency compared to baseline for passive,PNF, and control conditions, respectively. EMDV remainedsignificantly increased among all conditions throughout theassessment period. Group mean EMDV scores for the inter-vention leg under each experimental condition are presented inFig. 3A. The results show that EMDE performance was notinfluenced significantly over time by the EIMD intervention.The overall group mean score for EMDE was 22.6 � 4.7milliseconds across conditions (Fig. 3B).
FE and PE
There was a significant condition � leg � time interactionfor FE performance (F[10, 105] ¼ 6.4; p < 0.05), which showedthat while this aspect of sensorimotor performance capabilitywas preserved in the contralateral leg, EIMD interventionelicited transient decreases in performance compared tobaseline in all conditions, and these changes were mostprominent in participants who had undertaken passive flexi-bility conditioning compared to control and PNF conditions(Fig. 3C). The effects of the eccentric exercise interventioncontributed up to an error of approximately 10% to sensori-motor performance capability (FE at 48 hours post-EIMD,
Fig. 3. Neuromuscular and sensorimotor performance of the knee flexors for three an
passive; control) during exercise-induced muscle damage (group mean � SD; som
Electromechanical delay (evoked). (C) Force error. (D) Position error.
passive group). A marginal equivalent interaction was notedfor PE performance (F[10, 105] ¼ 2.8; p ¼ 0.062), suggesting atrend towards similar patterns for dynamic PE due to EIMD(up to 13% error at 48 hours post-EIMD, passive group;Fig. 3D).
Discussion
The absence of substantive changes in performance capa-bility over the control period and for the contralateral limbduring the experimental period for each index indicates thatthere were no systematic or learning effects and that perfor-mance variations can be attributed to the antecedent flexibilityconditioning and EIMD interventions.
The antecedent passive and PNF conditioning programs of6 weeks in duration were equally effective in eliciting im-provements in passive hip flexibility. The magnitude of theimprovements in passive hip flexibility observed was bio-statistically large (relative experimental effect size > 1.5) andbiologically meaningful (>20% improvement in group meanscores compared to baseline) and was congruent with sub-stantively plastic changes within the connective tissue struc-tures, including molecular reorganization to increase length,increased mechanical compliance within joint- and muscle-related connective tissue, and transient weakening of the tis-sue before adaptation.
When considered independently, these improvements inpassive hip joint flexibility may represent beneficial andenhanced protection against the risk of injury.51 However, as
tecedent treatment conditions (proprioceptive neuromuscular facilitation, PNF;
e SD bars removed for clarity). (A) Electromechanical delay (volitional). (B)

114 N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
alluded to earlier, conditioning-related increases in tissuelength and mechanical compliance may provoke hyper-compliance within the musculoskeletal system, involvingincreased muscle response times in the initiation of correctiveforces, which is less likely to be capable of restraining highjoint loads rapidly enough to prevent ligamentous injury.52
These effects may be especially important at knee flexionangles for which key ligamentous structures are already underthe greatest mechanical strain.50 Furthermore, when consid-ered in conjunction with the effects of cyclical loading ofviscoelastic tissue during sporting and work-related pursuits,the latter processes may contribute to extra injury risk becausecompliance characteristics and reflexive muscular activity maybe further adversely affected.43
The eccentric exercise protocol induced muscle damagecharacterized by increases in plasma CK and perceived sore-ness and a prolonged decrease in PF of the knee flexors. TheEIMD intervention elicited transient reductions in PFcompared to baseline that were less strong (peak 25% and19% reductions) and recovered more quickly in the PNF andpassive conditions, respectively, than in the control condition(peak 41% reduction compared to baseline). If, as hypothe-sized, PNF and passive flexibility conditioning resulted in anincrease in the number of sarcomeres in series, then it wouldbe reasonable to expect that this change would have affordedsome protection from EIMD and that this effect would be mostevident at long functional muscle length such as that used inthe current study (30� of knee flexion). The increase in thenumber of sarcomeres in series would tend to decrease thelength of individual sarcomeres and result in fewer operatingbeyond an optimal length, with associated increased vulnera-bility to damage.11
While there was a trend for better maintenance of strengthat long muscle length following EIMD in the flexibility-trained groups, there was no evidence that increased flexi-bility offered protection from soreness or overall musculo-skeletal stiffness. Similar levels and patterning of transientincreases in plasma CK, perceived soreness, and passive hipflexibility compared to baseline were noted among the PNF,passive, and control conditions.
It is interesting to note that most of the flexibilityconditioning-related gains in performance in the passive andPNF groups (w20% increase compared to baseline) weretransiently negated approximately 48 and 72 hours aftereccentric exercise by peak reductions in passive hip flexibility(13.2e19.9% reduction). When considered separately, thismight be interpreted as an indication of a transient loss inprotection from musculoskeletal injury associated withimproved flexibility characteristics of the joint system previ-ously elicited by conditioning.
However, the net effects of EIMD and antecedent condi-tioning for increased flexibility are likely to be complex,involving interactive responses to conditioning-relatedconformational changes to tissue and to more acute andtransient changes in the compliance characteristics of the tis-sue caused by EIMD. For example, the flexibility conditioningprograms we used focused on the inclusion of long-duration,
low-force stretches rather that short-duration, high-force bal-listic efforts to optimize the relative proportions of physio-logical stimuli within a stretch, producing plasticityadaptations rather than changes in tissue compliance. Plasticchanges within connective tissue structures include confor-mational changes in length due to molecular reorganizationand transient weakening of the tissue before adaptation.Conversely, compensatory adaptations involving shortening ofsome sarcomeres as compensation for those that have beenoverly-stretched and irreversibly damaged following eccentricexercise11 might stretch the elastic component in series withthe contractile component, and may elicit a greater residualSEC stretch. Furthermore, possible intra-muscular swellingobserved in several investigations following eccentric exer-cise53,54 may also induce stretching of the SEC by distensionof the musculature. These underlying mechanisms may alsoaffect the maximum muscular activation and the rate at whichdynamic stabilization of a joint system can occur.
EMD offers insight into the capability of the musculo-skeletal system to counteract potentially harmful dynamicforces in a timely manner by the most rapid response of theneuromuscular system. This capability may be more importantthan strength capability per se in protecting ligamentous tissueagainst injury.34,52,55 It is interesting to note that EMD per-formance capabilities were substantively decreased followingeccentric exercise in all conditions, but these changes wereaccentuated in participants who had undertaken passive flex-ibility conditioning (40.1% reduction).
Processes involved in the conversion of excitation intomuscle force can potentially contribute to conditioning- anddamage-related changes in the rate of muscle activation andforce-generating capability observed in the current study. It isbelieved that the majority of the EMD is determined by thetime taken to stretch the SEC,56 most of which is situated atconnective tissue attachments at the end of muscle fibers.
The differential changes in EMDV performance observedbetween PNF and passive flexibility conditioning suggestsubtle but important differences in the adaptation of connectivetissue to the two modes of antecedent flexibility conditioning,despite the similarity observed for the extent of improvementsin passive hip flexibility. For example, the passive conditioningintervention was likely to have elicited substantial focal in-creases in compliance. However, the net outcome of changes inmusculoskeletal stiffness and contractile tissue performanceassociated with PNF flexibility conditioning was less pro-nounced and had moderate performance effects on active as-sessments of EMD following EIMD that essentially matchedthose of the control group. It is conceivable that the staticmaximal voluntary activations of the agonist musculatureassociated with the PNF intervention were of sufficient dura-tion and volume to have elicited increased stiffness in the in-ternal structures of muscle tendon complex57 and ligamentousconnective tissue58 that might have counteracted much of theincreased compliance occurring solely as a result of passivestretching of the connective tissue.
Preservation of the capability to initiate muscle force maybe part of vital neuromuscular compensatory mechanisms to

115N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
protect the joint system in emergency scenarios. As alluded toearlier, the shift of optimal force production towards longermuscle length,11,53 in conjunction with the potential facilita-tory effects on EMD of SEC stretching, may also aid in theconservation of neuromuscular performance following eccen-tric exercise at joint angles for which key ligamentous struc-tures are under the greatest mechanical strain.
Irrespective of the mechanisms underpinning the deteriora-tion of performance, the extent of the impairment to EMDobserved, combined with decreased peak force capabilities,would be expected to substantially compromise the ability of theknee flexors to generate sufficient levels of force to counteractrapid, dynamic loading and thus to preserve joint integrity.
It is especially noteworthy that EMDE performance waspreserved following EIMD intervention, despite compromisedEMDV performance and an expectation of preferentialrecruitment5,22 and increased susceptibility of fast-twitch fi-bers to damage during eccentric exercise.4,16 While theexperimental design of this study may not have been sufficientto entirely exclude the possibility of a potential type II errorduring detection of subtle changes in EMDE performance,Strojnik and Komi59 also observed no impairment of electri-cally evoked EMD of the knee extensors after prolongedstretcheshortening in an inclined-sledge jumping protocol,suggesting that preservation of this aspect of performance mayhave biological underpinnings. Given that the stressful boutsof eccentric exercise within the EIMD protocol were regulatedby volitional efforts, it is possible that protective inhibitoryprocesses may have limited the recruitment of the total pool offast-twitch, high-threshold motor units.52 These high-thresholdunits may be preserved from damage and would thus besubsequently available to contribute to the maintenance ofevoked performance or to protective responses in a patient orsportsperson when a true emergency scenario is perceived.
Reduced sensorimotor performance, including the ability toscale volitional force and joint positioning precisely, has beenassociated with increased risk of musculoskeletal injury viacompromised capabilities of the musculature to act synergis-tically and facilitate dynamic stabilization of a joint system.37
Increased flexibility has been linked to a greater number ofsarcomeres in series in muscle.47 A greater number of sarco-meres in series would decrease the length of individual sar-comeres at any given muscle length, leading to the optimalangle for force production at longer muscle lengths. Similarly,flexibility conditioning may potentially elicit decreased stiff-ness of the tendoneaponeurosis complex, which wouldenhance its capability to absorb strain imposed by activelengthening, thereby relieving strain on the muscle fibers.27
Such conformational changes in the structure of connectivetissue associated with improvements in flexibility may havebeen suspected of being capable of subtly disrupting the per-formance of proprioceptors such as tendon organs and re-ceptors within the structures of synovial joints. Alongsideexteroreceptors, the latter sensory machinery contributes to athe capability of a synovial joint to organize rapid forcefulresponses to disturbances, to determine its position, and todistinguish between self-generated and imposed movements.5
Importantly, EIMD elicited transient decreases in sensori-motor performance and the capability to scale volitional forceprecisely compared to baseline in all conditions. The latterchanges were most prominent in participants who had under-taken passive flexibility conditioning (w10%) compared tocontrol and PNF conditions. A similar trend for reduced pre-cision in the scaling of joint position was noted. This suggeststhat the functionally important capability of a joint system toscale and regulate motor responses precisely at vulnerableend-range joint positions was compromised by EIMD. Inconjunction with the effects of passive flexibility conditioningin particular, there may be a failure in the sensorimotor per-formance associated with a joint to compensate for substantiveconditioning-related changes to the length of its connectivetissue structures and likely changes to its compliance andneuromuscular activation characteristics.
The magnitude of the transient deterioration in EMD per-formance associated with EIMD and passive flexibility con-ditioning in particular was biostatistically large (relativeexperimental effect size > 1.5) and approached the lower limitof fatigue-related deterioration in EMD performance sus-pected of contributing to musculoskeletal injury.34 Thestrength of these changes considered alongside those for thedeterioration of sensorimotor performance, which has beencausally linked to injury36 and transient loss of strength andpassive hip flexibility, indicates a potential for increased riskof injury. This concern in relation to the use of antecedentpassive flexibility conditioning and eccentric exercise wouldalso apply to the use of PNF conditioning, but to a lesserextent.
Many athletes might be expected to experience aspects ofthese latter effects and a commensurate increased risk ofmusculoskeletal injury to a lesser or greater extent, dependingon specific needs and the manifold requirements for condi-tioning within contemporary sports practices. Contemporaryrehabilitation programs routinely feature the use of passivejoint movements as a means to enhance joint mobility andflexibility while managing the tensile loading of surgicallyreconstructed ligamentous tissue or shear and compressiveloading on joint surfaces to protect avascular autogenousgrafts.60 It may be an interesting paradox that while thisapproach to enhancing flexibility may protect joint health inthe acute phases of rehabilitation, the practice may ultimatelyexacerbate and carry over a vulnerability to injury in subse-quent phases of rehabilitation involving accelerated progresstowards the resumption of functionally relevant activities andEIMD. Our findings offer an important consideration that isrelevant for informed choice by clinicians and exercise sci-entists regarding optimized rehabilitation practice and inter-vention strategies.
In conclusion, our study has shown that conditioning-relatedincreases in the flexibility of the hamstring muscle group led tosome protection from strength loss following EIMD. Never-theless, the combined effects of flexibility conditioning andEIMD elicited significant transient decreases in neuromuscularactivation and in musculoskeletal and sensorimotor perfor-mance capabilities that exceeded the effects of eccentric

116 N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
exercise alone. The EIMD-related performance deteriorationwas most prominent in participants who completed passiveflexibility conditioning, but was sufficiently strong followingboth conditioning modes to raise concerns about commensuratelosses of capability for rapid and dynamic stabilization ofsynovial joints during episodes of threat from injury.
Conflicts of interest
There were no conflicts of interest associated with thisresearch.
References
1. Newham DJ, McPhail G, Mills KR, et al. Ultrastructural changes after
concentric and eccentric contractions of human muscle. J Neurol Sci.
1983;61:109e122.
2. Proske U, Morgan DL. Muscle damage from eccentric exercise: mecha-
nism, mechanical signs, adaptation and clinical applications. J Physiol.
2001;537:333e345.3. McHughM, Connolly DAJ, Eston RG, et al. Electromyographic analysis of
exercise resulting in symptoms of muscle damage. J Sports Sci. 2000;18:
163e172.4. Brockett CL, Morgan DL, Gregory JE, et al. Damage to different types of
motor units following repeated active lengthenings of the medial
gastrocnemius muscle of the cat. J Appl Physiol. 2002;92:1104e1110.
5. Enoka RM. Eccentric actions require unique activation strategies by the
nervous system. J Appl Physiol. 1996;81:2339e2346.
6. Rees D, Gleeson NP. The scientific assessment of the injured athlete. In:
Proceedings of the Football AssociationeRoyal College of Surgeons
Medical Conference. Lilleshall Hall National Sports Centre; 1999.
7. Byrne C, Eston RG, Edwards RHT. Characteristics of isometric and dy-
namic strength loss following eccentric exercise-induced muscle damage.
Scand J Med Sci Sports. 2001;11:134e140.
8. Rowlands AV, Marginson VF, Lee J. Chronic flexibility gains: effect of
isometric contraction duration during proprioceptive neuromuscular
facilitation stretching techniques. Res Q Exerc Sport. 2003;74:47e51.
9. Child RB, Saxton JM, Donnelly AE. Comparison of knee extensor muscle
actions on indices of damage and angle-specific force production in
humans. J Sports Sci. 1998;16:301e308.
10. Saxton JM, Donnelly AE. Length-specific impairment of skeletal muscle
contractile function after eccentric muscle actions in man. Clin Sci.
1996;90:119e125.
11. Morgan DL, Allen DG. Early events in stretch-induced muscle damage.
J Appl Physiol. 1999;87:2007e2015.
12. Clarkson PM, Kazunori N, Braun B. Muscle function after exercise-
induced muscle damage and rapid adaptation. Med Sci Sports Exerc.
1992;24:512e520.
13. Cleak MJ, Eston RG. Muscle soreness, swelling, stiffness and strength
loss after intense eccentric exercise. Br J Sports Med. 1992;26:267e272.
14. Rinard J, Clarkson PM, Smith L. Response of males and females to high-
force eccentric exercise. J Sports Sci. 2000;18:229e236.
15. Sayers SP, Clarkson PM. Force recovery after eccentric exercise in males
and females. Eur J Appl Physiol Occup Physiol. 2001;84:122e126.
16. Byrne C, Eston RG. Maximal intensity isometric and dynamic exercise
performance following eccentric muscle actions. J Sports Sci.
2002;20:951e959.17. Linnamo V, Bottas R, Komi PV. Force and EMG power spectrum during
and after eccentric and concentric fatigue. J Electromyogr Kinesiol.
2000;10:293e300.
18. Twist C, Eston RG. The effects of exercise-induced muscle damage on
maximal intensity, intermittent exercise. J Sports Sci. 2004;22:292e293.
19. Miles MP, Ives JC, Vincent KR. Neuromuscular control following
maximal eccentric exercise. Eur J Appl Physiol Occup Physiol.
1997;76:368e374.
20. Byrne C, Eston RG. The effect of exercise-induced muscle damage on
isometric and dynamic knee extensor strength and vertical jump perfor-
mance. J Sports Sci. 2002;20:417e425.
21. Twist C, Eston RG, Gleeson N. The effects of plyometric exercise on
unilateral balance performance. J Sports Sci. 2008;26:1073e1080.22. Hawkins R, Hulse M, Hodson A, et al. The Football Association medical
research programme: an audit of injuries in professional football. Br J
Sports Med. 2001;35:43e47.23. McHugh M, Connolly D, Eston RG, et al. Exercise-induced muscle
damage and potential mechanisms for the repeated bout effect. Sports
Med. 1999;27:157e170.
24. Nosaka K, Sakamoto K, Newton M, et al. How long does the protective
effect of eccentric exercise-induced muscle damage last? Med Sci Sport
Exerc. 2001;33:1490e1495.
25. McHugh M, Connolly DAJ, Eston RG, et al. The role of passive muscle
stiffness in symptoms of exercise-induced muscle damage. Am J Sports
Med. 1999;27:594e599.
26. Gleeson NP, Eston R, Marginson V, et al. Effects of prior concentric
training on eccentric exercise-induced muscle damage. Br J Sports Med.
2003;37:119e125.
27. McHugh MP. Recent advances in the understanding of the repeated bout
effect: the protective effect against muscle damage from a single bout of
eccentric exercise. Scand J Med Sci Sports. 2003;13:88e97.28. Marginson V, Rowlands AR, Gleeson NP, et al. Comparison of the
symptoms of exercise-induced muscle damage after an initial and repeated
bout of plyometric exercise in men and boys. J Appl Physiol. 2005;99:
1174e1181.
29. Friden J. Changes in human skeletal muscle induced by long-term
eccentric exercise. Cell Tissue Res. 1984;236(2):365e372.
30. Burke DG, Culligan CJ, Holt LE. The theoretical basis of proprioceptive
neuromuscular facilitation. J Strength Cond Res. 2000;14:496e500.
31. Johansson H, Sjolander P, Sojka P. A sensory role for the cruciate liga-
ments. Clin Orthop Relat Res. 1991;16:161e178.
32. Minshull C, Gleeson N, Walters-Edwards M, et al. Effects of acute fatigue
on the volitional and magnetically-evoked electromechanical delay of the
knee flexors in males and females. Eur J Appl Physiol. 2007;
100:469e478.
33. Minshull C, Gleeson NP, Eston RG, et al. Single measurement reliability
and reproducibility of volitional and magnetically-evoked indices of
neuromuscular performance in adults. J Electromyogr Kinesiol. 2009;19:
1013e1023.
34. Gleeson NP, Reilly T, Mercer TH, et al. Influence of acute endurance
activity on leg neuromuscular and musculoskeletal performance. Med Sci
Sports Exerc. 1998;30:596e608.
35. Baltzopoulos V, Gleeson NP. Skeletal muscle function. In: Eston R,
Reilly T, eds. Physiology. 3rd ed. London: Routledge; 2008:3e40. Kin-
anthropometry and Exercise Physiology Laboratory Manual: Tests, Pro-
cedures and Data; vol. 2.
36. Hewett TE, Lindenfield TN, Riccobene JV, et al. The effect of neuro-
muscular training on the incidence of knee injury in female athletes. Am J
Sports Med. 1999;27:699e706.
37. Lattanzio JP, Petrella RJ, Sproule JR, et al. Effects of fatigue on knee
proprioception. Clin J Sports Med. 1997;7:22e27.38. Griffin E. Neuromuscular training and injury prevention in sports. Clin
Orthop Relat Res. 2003;409:53e60.
39. Zhou S, McKenna MJ, Lawson DL, et al. Effect of fatigue and sprint
training on electromechanical delay of the knee extensor muscles. Eur J
Appl Physiol. 1996;72:410e416.
40. Norman J, Komi PV. Electromechanical delay in skeletal muscle under
normal movement conditions. Acta Physiol Scand. 1979;106:241e248.41. Chu D, LeBlanc R, D’Ambrosia P, et al. Neuromuscular disorder in
response to anterior cruciate ligament creep. Clin Biomech. 2003;18:
222e230.
42. Sbriccoli P, Solomonow M, Zhou B-H, et al. Neuromuscular responses to
cyclic loading of the anterior cruciate ligament. Am J Sports Med.
2005;33:543e551.
43. Solomonow M. Ligaments: a source of work-related musculoskeletal
disorders. J Electromyogr Kinesiol. 2004;14:49e60.

117N. Gleeson et al. / Journal of Exercise Science & Fitness 11 (2013) 107e117
44. Minshull C, Rees D, Gleeson NP. Joint angle affects volitional and
magnetically evoked neuromuscular performance differentially. J Elec-
tromyogr Kinesiol. 2011;21:672e677.
45. Brockett C, Warren N, Gregory JE. A comparison of the effects of
concentric versus eccentric exercise on force and position sense at the
human elbow joint. Brain Res. 1997;771:251e258.
46. Saxton JM, Clarkson PM, James J. Neuromuscular dysfunction following
eccentric exercise. Med Sci Sports Exerc. 1995;27:1185e1193.47. Eston RG, Rowlands AV, Coulton D, et al. Effect of flexibility training on
symptoms of exercise-induced muscle damage: a preliminary study. J
Exerc Sci Fit. 2007;5:33e39.
48. Chen CH, Nosaka K, Chen HL, et al. Effects of flexibility training on
eccentric exercise-inducedmuscle damage.Med Sci Sports Exerc. 2011;43:
491e500.
49. Etnyre BR, Lee EJ. Chronic and acute flexibility of men and women
using three different stretching techniques. Res Q Exerc Sport. 1988;59:
222e228.
50. Beynnon BD, Johnson RJ. Anterior cruciate ligament injury rehabilitation
in athletes. Biomechanical considerations. Sports Med. 1996;22:54e64.
51. Hartig DE, Henderson JM. Increasing hamstring flexibility decreases
lower extremity overuse injuries in military basic trainees. Am J Sports
Med. 1999;27:173e176.
52. Mercer TH, Gleeson NP, Claridge S, et al. Prolonged intermittent high
intensity exercise impairs neuromuscular performance of the knee flexors.
Eur J Appl Physiol. 1998;77:560e562.
53. Brockett CL, Morgan DL, Proske U. Human hamstring muscles adapt to
eccentric exercise by changing optimum length. Med Sci Sports Exerc.
2001;33:783e790.
54. Foley JM, Jayraman RC, Prior BM. MR measurements of muscle damage
and adaptation after eccentric exercise. J Appl Physiol. 1999;87:
2311e2318.
55. Shultz SJ, Perrin DH, Adams MJ. Neuromuscular response characteristics
in men and women after knee perturbation in a single-leg, weight-bearing
stance. J Athl Train. 2001;36:37e43.
56. Cavanagh PR, Komi PV. Electromechanical delay in human skeletal
muscle under concentric and eccentric contractions. Eur J Appl Physiol
Occup Physiol. 1979;42:159e163.57. Kubo K, Kanehisa H, Ito M, et al. Effects of isometric training on the
elasticity of human tendon structures in vivo. J Appl Physiol. 2001;91:
26e32.
58. Woo SLY, Ritter MA, Amiel D, et al. The biomechanical and biochemical
properties of swine tendons long term effects of exercise on the digital
extensors. Connect Tissue Res. 1980;7:177e183.
59. Strojnik V, Komi PV. Neuromuscular fatigue after maximal stretcheshortening cycle exercise. J Appl Physiol. 1998;84:344e350.
60. Gleeson N, Parfitt G, Minshull C, et al. Influence of surgery and reha-
bilitation conditioning on psychophysiological fitness. J Exerc Sci Fit.
2008;6:71e86.
Copyright © 2022 FDOKUMEN




















