
Neuromuscular Blocking Agents - Elsevier
15
Drug Mechanism Class Metabolism/ Elimination Atracurium Nondepolarizing Benzylisoquinolinium plasma esterase/ Hofmann elimination Cisatracurium Nondepolarizing Benzylisoquinolinium plasma esterase/ Hofmann elimination* Mivacurium Nondepolarizing Benzylisoquinolinium plasma cholinesterase Pancuronium Nondepolarizing Aminosteroidal renal > hepatic Rocuronium Nondepolarizing Aminosteroidal renal < hepatic Summary Neuromuscular blocking agents (NMBAs) are used to facilitate endotracheal intubation and provide skeletal muscle relaxation during surgery or mechanical ventilation. NMBAs do not provide sedation, analgesia, or amnesia; administer only after unconsciousness has been induced and maintain adequate amnesia and analgesia throughout paralysis. NMBA selection depends on clinical application and patient factors; consider the onset and duration of action, adverse effects, and metabolism/excretion of each agent. Pharmacology Neuromuscular blocking agents (NMBAs) cause skeletal muscle relaxation by blocking acetylcholine, and therefore, the transmission of nerve impulses at the neuromuscular junction. Depolarizing NMBAs bind to and activate cholinergic receptor sites, making the muscle fiber refractory to the action of acetylcholine. Nondepolarizing NMBAs competitively antagonize cholinergic receptors. Nondepolarizing NMBAs are divided into 2 broad structural classes: aminosteroidal and benzylisoquinolinium agents. Differences in chemical structure reflect little but variance in drug elimination pathways.[52452][52486] [65358][65369][65389] Neuromuscular Blocking Agent General Pharmacology[65358][65369] Neuromuscular Blocking Agents
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Neuromuscular Blocking Agents - Elsevier

Drug Mechanism ClassMetabolism/
Elimination
Atracurium Nondepolarizing Benzylisoquinoliniumplasma esterase/
Hofmann elimination
Cisatracurium Nondepolarizing Benzylisoquinoliniumplasma esterase/
Hofmann elimination*
Mivacurium Nondepolarizing Benzylisoquinolinium plasma cholinesterase
Pancuronium Nondepolarizing Aminosteroidal renal > hepatic
Rocuronium Nondepolarizing Aminosteroidal renal < hepatic
Summary
Neuromuscular blocking agents (NMBAs) are used to facilitate endotracheal intubation and provideskeletal muscle relaxation during surgery or mechanical ventilation.
NMBAs do not provide sedation, analgesia, or amnesia; administer only after unconsciousness hasbeen induced and maintain adequate amnesia and analgesia throughout paralysis.
NMBA selection depends on clinical application and patient factors; consider the onset and durationof action, adverse effects, and metabolism/excretion of each agent.
PharmacologyNeuromuscular blocking agents (NMBAs) cause skeletal muscle relaxation by blocking acetylcholine,and therefore, the transmission of nerve impulses at the neuromuscular junction. Depolarizing NMBAsbind to and activate cholinergic receptor sites, making the muscle fiber refractory to the action ofacetylcholine. Nondepolarizing NMBAs competitively antagonize cholinergic receptors. NondepolarizingNMBAs are divided into 2 broad structural classes: aminosteroidal and benzylisoquinolinium agents.Differences in chemical structure reflect little but variance in drug elimination pathways.[52452][52486]
[65358][65369][65389]
Neuromuscular Blocking Agent General Pharmacology[65358][65369]
Neuromuscular Blocking Agents

Succinylcholine Depolarizing Acetylcholine-like plasma cholinesterase
Vecuronium Nondepolarizing Aminosteroidal renal <= hepatic
*Less than 20% of elimination occurs via renal and hepatic pathways combined
Onset and Duration of Action of Neuromuscular Blocking Agents[52452][52486][65358][65369][65389]
Drug Onset (minutes) Duration (minutes)
Short-actingSuccinylcholine 0.5 to 1.5 5 to 10
Mivacurium 2 to 3 10 to 20
Intermediate-acting
Atracurium 3 to 5 20 to 35
Cisatracurium 2 to 5 20 to 60
Rocuronium 1 to 2 20 to 35
Vecuronium 3 to 5 20 to 45
Long-acting Pancuronium 2 to 5 60 to 100
Pharmacodynamics of Neuromuscular Blocking Agents[42613][52452][65345] [65358][65369]
Drug HistamineRelease Muscarinic Receptor Effect
Ganglionic/Vagal
BlockadeProlonged Blockade
Atracurium low to minimal none minimal to none rare
Cisatracurium minimal to none none none rare
Mivacurium low to minimal none none rare
Pancuronium minimal to none moderate blockade yes yes
Rocuronium minimal to none minimal blockade at high doses no
Succinylcholine minimal stimulation none with reduced plasma cholinesterase activity
Vecuronium none none at high doses yes
Therapeutic Use
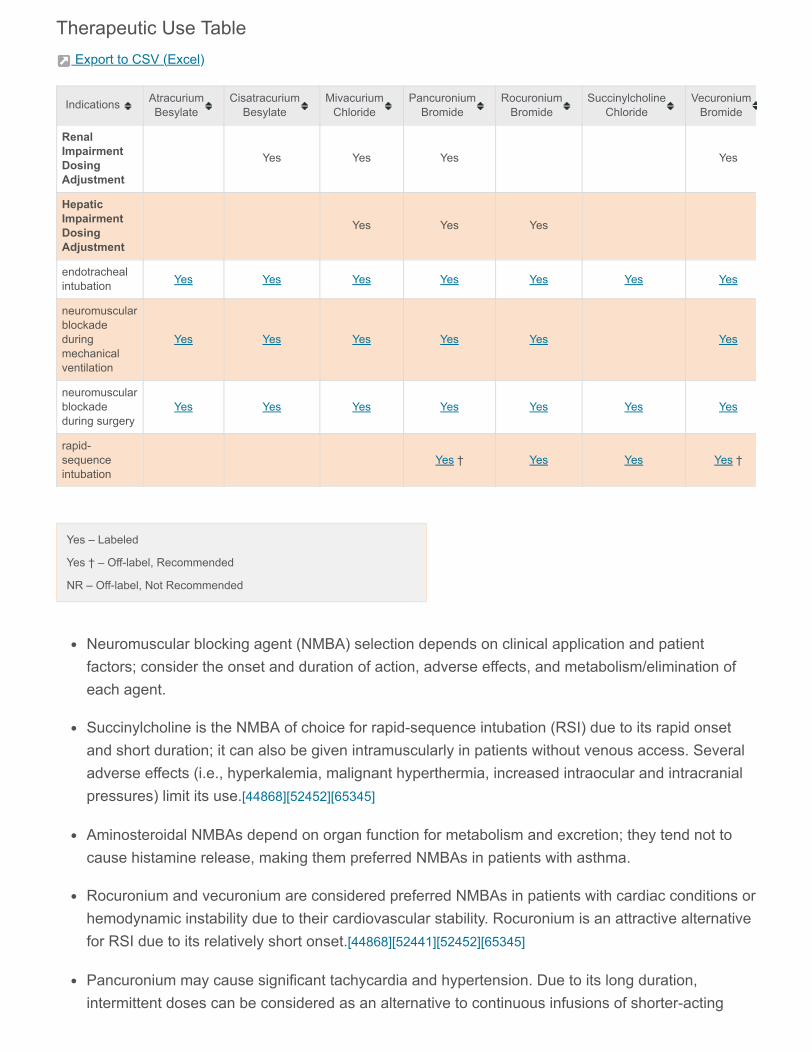
Therapeutic Use Table Export to CSV (Excel)
Yes – Labeled
Yes † – Off-label, Recommended
NR – Off-label, Not Recommended
Neuromuscular blocking agent (NMBA) selection depends on clinical application and patientfactors; consider the onset and duration of action, adverse effects, and metabolism/elimination ofeach agent.
Succinylcholine is the NMBA of choice for rapid-sequence intubation (RSI) due to its rapid onsetand short duration; it can also be given intramuscularly in patients without venous access. Severaladverse effects (i.e., hyperkalemia, malignant hyperthermia, increased intraocular and intracranialpressures) limit its use.[44868][52452][65345]
Aminosteroidal NMBAs depend on organ function for metabolism and excretion; they tend not tocause histamine release, making them preferred NMBAs in patients with asthma.
Rocuronium and vecuronium are considered preferred NMBAs in patients with cardiac conditions orhemodynamic instability due to their cardiovascular stability. Rocuronium is an attractive alternativefor RSI due to its relatively short onset.[44868][52441][52452][65345]
Pancuronium may cause significant tachycardia and hypertension. Due to its long duration,intermittent doses can be considered as an alternative to continuous infusions of shorter-acting
Indications AtracuriumBesylate
CisatracuriumBesylate
MivacuriumChloride
PancuroniumBromide
RocuroniumBromide
SuccinylcholineChloride
VecuroniumBromide
RenalImpairmentDosingAdjustment
Yes Yes Yes Yes
HepaticImpairmentDosingAdjustment
Yes Yes Yes
endotrachealintubation Yes Yes Yes Yes Yes Yes Yes
neuromuscularblockadeduringmechanicalventilation
Yes Yes Yes Yes Yes Yes
neuromuscularblockadeduring surgery
Yes Yes Yes Yes Yes Yes Yes
rapid-sequenceintubation
Yes † Yes Yes Yes †

NMBAs in patients requiring sustained paralysis.[52443]
Benzylisoquinolinium NMBAs undergo organ-independent degradation; they lack vagolytic activitybut are more likely to cause histamine release.[52452]
Atracurium and cisatracurium are attractive for continuous infusion use in critically ill patients, astheir metabolism is largely unrelated to hepatic or renal function.[65358]
A short course (48 hours or less) of NMBA by continuous infusion is recommended for patients withearly acute respiratory distress syndrome (ARDS) with a PaO2/FiO2 less than 150 mmHg.[61770]
[62859]
Comparative Efficacy
Succinylcholine is considered the neuromuscular blocking agent (NMBA) of choice for rapid-sequence intubation (RSI) due to its rapid onset and shorter duration; however, adverse effects limitits use. Rocuronium is an attractive alternative.[44868][52452][65345]
Both agents offer similar safety and efficacy for RSI when used in various patient populations.[65441][65442][65443] When dosed at 0.9 to 1.2 mg/kg, rocuronium's onset of action is similar tosuccinylcholine with a longer duration.[65442]
Neuromuscular Blocking Agent Comparative Efficacy Trials for Rapid-Sequence Intubation (RSI)
Citation Design/Regimen Results Conclusion
Marsch SC, etal. Crit Care2011;15:R199. [65441]
Randomized, controlled, single-blind trial comparingsuccinylcholine 1 mg/kg IV (n = 208) vs. rocuronium0.6 mg/kg IV (n = 208) for rapid-sequence intubationin critically ill adults. Patients were premedicated withfentanyl 1 mcg/kg IV, and etomidate 0.2 mg/kg IV orpropofol 1 mg/kg IV were used for induction.
Incidence ofoxygendesaturation,defined as adecrease inoxygensaturation of5% or more:
Succinylcholine:37%
Rocuronium:34%
(p = 0.67)
Incidence ofsevere oxygendesaturation,resulting in asaturationvalue of 80%or less:
Succinylcholine:10%
Incidence and severity of oxygendesaturations, quality of intubationconditions, and incidence of failed intubationattempts did not differ betweensuccinylcholine and rocuronium in critically illadults. The mean intubation sequence was14 seconds shorter after succinylcholinecompared to rocuronium. Hemodynamiceffects of intubation were similar in bothgroups.

Rocuronium:10%
(p = 1)
Duration ofintubationsequence:
Succinylcholine:
81 +/- 38seconds
Rocuronium:
95 +/- 48seconds
(p = 0.002)
Incidence offailed firstintubationattempt:
Succinylcholine:16%
Rocuronium:18%
(p = 0.4)
Intubationconditions(maximalscore = 9):
Succinylcholine:
8.3 +/- 0.8
Rocuronium:
8.2 +/- 0.9
(p = 0.7)
Magorian T, etal.Anesthesiology1993;79:913-918. [65442]
Randomized, controlled trial comparing rocuronium0.6, 0.9, or 1.2 mg/kg IV, vecuronium 0.1 mg/kg IV, orsuccinylcholine 1 mg/kg IV (total n = 50) for rapid-sequence induction of anesthesia in adult patientswho were ASA physical status 1 thru 3. Patients werepremedicated with midazolam 0.02 to 0.05 mg/kg IV,and incremental doses of thiopental 1 to 2 mg/kg IVwere given before neuromuscular blockade.
Mean onset ofaction:
Rocuronium 0.6mg/kg:
89 seconds
Rocuronium 0.9mg/kg:
75 seconds
Rocuronium 1.2mg/kg:
55 seconds
Vecuronium 0.1mg/kg:
Onset of action for rocuronium 0.9 and 1.2mg/kg was similar to succinylcholine.Rocuronium's duration of action wasprolonged compared to succinylcholine atthese doses; duration of action withrocuronium 1.2 mg/kg was significantlylonger compared to all other agents/doses.Recovery index was significantly shorter forsuccinylcholine but similar for all otheragents/doses.

144 seconds
Succinylcholine1 mg/kg: 50seconds
Mean durationof action:
Rocuronium 0.6mg/kg: 37minutes
Rocuronium 0.9mg/kg: 53minutes
Rocuronium 1.2mg/kg: 73minutes
Vecuronium 0.1mg/kg: 41minutes
Succinylcholine1 mg/kg: 9minutes
Mean recoveryindex:
Rocuronium 0.6mg/kg: 14minutes
Rocuronium 0.9mg/kg: 22minutes
Rocuronium 1.2mg/kg: 24minutes
Vecuronium 0.1mg/kg: 20minutes
Succinylcholine1 mg/kg: 2minutes

April MD, et al.Ann EmergMed2018;72:645-653. [65443]
International, multicenter, observational seriescomparing succinylcholine (n = 2,275; mean dose:1.8 mg/kg IV) and rocuronium (n = 1,800; meandose: 1.2 mg/kg IV) for rapid-sequence intubation inthe emergency department in patients older than 14years. Sedation agents included etomidate,ketamine, and propofol.
Incidence offirst-passintubationsuccess:
Succinylcholine87%
Rocuronium87.5%
(risk difference0.5%; 95% CI-1.6% to 2.6%)
Cormack-Lehane grade1 or 2 view:
Succinylcholine:88.5%
Rocuronium:89%
Incidence ofadverseevents:
Succinylcholine:14.7%
Rocuronium:14.8%
First-pass intubation success, glottic view,and incidence of adverse effects did notdiffer between succinylcholine androcuronium during emergency departmentintubation.
Adverse Reactions / Side EffectsTop 20 Adverse Reactions / Side Effects Table
Export to CSV (Excel)
AdverseReaction /Side Effect
AtracuriumBesylate
CisatracuriumBesylate
MivacuriumChloride
PancuroniumBromide
RocuroniumBromide
SuccinylcholineChloride
VecuroniumBromide
acutequadriplegicmyopathysyndrome
Reported Reported Reported Reported Reported Reported Reported
bronchospasm Reported 0.2 - 1.5% <1% Reported <1% Reported Reported
erythema 0.5 - 0.6% Reported <1% Reported Reported Reported Reported
flushing 1 - 29.2% 0.2% 16 - 25% Reported Reported Reported Reported
hypotension 0.6% 0.2% 0.3 - 4% Reported 0.1 - 2% Reported Reported
pruritus Reported Reported Reported Reported <1% Reported Reported
rash Reported 0.1% <1% Reported <1% Reported Reported

Anaphylactoid reactionsAlthough rare, severe anaphylactic or anaphylactoid reactions to neuromuscular blocking agents(NMBAs) have been reported; some cases have been fatal. Immediate availability of appropriateemergency treatment for anaphylaxis is advised because of the potential life-threatening severity of areaction.[42039] [48672] NMBAs are the most common cause of IgE-mediated anaphylaxis in anesthesia,with succinylcholine and rocuronium being the most frequent culprits.[65358] Cross-reactivity betweenNMBAs, both depolarizing and nondepolarizing, has been reported.[42039] [48672]
Histamine-related reactionsNeuromuscular blocking agents (NMBAs) with histamine-releasing properties (e.g., atracurium,mivacurium, succinylcholine) are more likely to cause bronchospasm, flushing, hypotension, and/ortachycardia. Histamine release may be related to dose or administration rate.[42613] [52452] [65358] [65389]
Cardiovascular reactionsPancuronium, atracurium, and succinylcholine have the greatest potential among neuromuscularblocking agents (NMBA) to cause adverse cardiovascular effects. Pancuronium causes tachycardia andincreased blood pressure as a result of vagal blockade and norepinephrine release from adrenergicnerve endings. Atracurium causes significant histamine release which may result in hypotension andtachycardia. Succinylcholine can cause vagal-mediated bradycardia, hypotension, and cardiac
AdverseReaction /Side Effect
AtracuriumBesylate
CisatracuriumBesylate
MivacuriumChloride
PancuroniumBromide
RocuroniumBromide
SuccinylcholineChloride
VecuroniumBromide
sinustachycardia Reported Reported <1% Reported <1.4% Reported Reported
urticaria Reported Reported <1% Reported Reported Reported Reported
wheezing 0.2 - 0.3% Reported <1% Reported <1% Reported Reported
bradycardia Reported 0.4% <1% Reported
hypertension Reported 0.1 - 2% Reported
injection sitereaction Reported <1% <1%
dizziness <1%
edema <1%
hiccups <1%
musclecramps <1%
nausea <1%
phlebitis <1%
vomiting <1%

arrhythmias; tachycardia and hypertension may occur due to sympathetic stimulation.[52452] [54407]
Pretreatment with atropine may prevent bradycardia associated with anticholinesterases.[42039] [65330] [65345]
SeizuresSeizures have been reported in intensive care unit patients after long-term infusion of atracurium tosupport mechanical ventilation. These patients usually had predisposing causes, such as head trauma,cerebral edema, hypoxic encephalopathy, viral encephalitis, or uremia. Laudanosine, a majorbiologically active metabolite of atracurium and cisatracurium without neuromuscular blocking activity,produces cerebral excitatory effects (i.e., generalized muscle twitching and seizures) at higher doseswhen administered to several species of animals; however, the relationship between CNS excitation andlaudanosine concentrations in humans has not been established.[42614] [48671]
TachyphylaxisPatients who receive neuromuscular blocking agents for a prolonged period may develop tachyphylaxis.Prolonged blockade leads to proliferation of acetylcholine receptors at the neuromuscular junctionresulting in increased drug requirements. Switch patients who develop tachyphylaxis to 1 agent and stillrequire paralysis to another agent. Continuous monitoring of neuromuscular transmission with aperipheral nerve stimulator is strongly recommended during continuous infusion or repeated dosing.[52441][52503]
Acute quadriplegic myopathy syndromeAcute quadriplegic myopathy syndrome (AQMS) has been associated with prolonged neuromuscularblocking agent (NMBA) exposure and presents as acute paresis, myonecrosis with increased creatinephosphokinase (CPK), and abnormal electromyography (EMG). Flaccid paralysis, decreased deeptendon reflexes, and respiratory insufficiency are present after drug discontinuation. Prolongedrehabilitation as well as chronic ventilatory support are often needed in patients with AQMS. Recoverymay take weeks to months. To reduce the risk of prolonged recovery and AQMS, periodic screening ofCPK during ongoing neuromuscular blockage may be helpful. Though periodic interruption of therapy isoften not feasible and there is no direct evidence showing that it reduces the incidence of AQMS, daily'drug holidays' may be considered for patients who will tolerate an interruption in therapy.[52503] [52486]
Immobility complicationsProlonged paralysis is associated with pooling and stasis of blood in the veins, which increases the riskof thrombosis. Skin breakdown, slowed gastrointestinal motility, peripheral muscle weakness, muscleatrophy are other complications of immobility.[65358] Prophylactic interventions, including frequentrepositioning, physical therapy, and sequential compression devices are warranted in intensive carepatients receiving prolonged neuromuscular blockade.[52482] [52503]
Corneal ulcersParalysis results in impaired eyelid closure and loss of corneal reflex, placing the cornea at risk fordrying, scarring, ulceration, and infection.[65358] Prophylactic eye care is essential; use artificial tears orophthalmic ointment at regular intervals in critically ill patients receiving prolonged neuromuscularblockade.[52482][52503]

Malignant hyperthermiaMalignant hyperthermia, an inherited disorder of muscle metabolism, often presents as prolongedmasseter spasm (jaw rigidity), which may progress to generalized rigidity, rhabdomyolysis, increasedoxygen demand, lactic acidosis, increased heart rate, profound fever, disseminated intravascularcoagulation (DIC), and cardiac arrhythmia. Malignant hyperthermia can be precipitated bysuccinylcholine; consider patients receiving nondepolarizing neuromuscular blocking agents (NMBAs)also to be at risk. If malignant hyperthermia is suspected, discontinue anesthesia immediately,implement supportive care, and administer dantrolene.[52486][54418][54419]
HyperkalemiaSuccinylcholine-induced depolarization may cause sufficient potassium efflux to produce hyperkalemia.[65369] In predisposed patients, a sudden, large increase in serum potassium may cause cardiacdysrhythmias and cardiac arrest.[52452] There have been rare reports of acute rhabdomyolysis withhyperkalemia followed by ventricular dysrhythmias, cardiac arrest, and death after the administration ofsuccinylcholine to apparently healthy pediatric patients who were subsequently found to haveundiagnosed skeletal muscle myopathy, most frequently Duchenne's muscular dystrophy. Thissyndrome often presents as peaked T-waves and sudden cardiac arrest within minutes after theadministration of succinylcholine in healthy appearing pediatric patients (usually, but not exclusively,males, and most frequently 8 years or younger). There have also been reports in adolescents.Therefore, when a healthy appearing infant or child develops cardiac arrest soon after administration ofsuccinylcholine, not felt to be due to inadequate ventilation, oxygenation, or anesthetic overdose,institute immediate treatment for hyperkalemia, including intravenous calcium, bicarbonate, glucose withinsulin, and hyperventilation. Due to the abrupt onset of this syndrome, routine resuscitative measuresare likely to be unsuccessful. However, extraordinary and prolonged resuscitative efforts have resultedin successful resuscitation in some reported cases.[42039]
Increased intracranial pressureSuccinylcholine may cause transient increased intracranial pressure immediately after administrationand during the fasciculation phase. Slight increases in pressure may persist after the onset of paralysis.Induction of adequate anesthesia before succinylcholine administration may minimize the drug's effecton intracranial pressure.[42039] [52486]
Drug Interactions
AntibioticsSystemic administration of certain antibiotics, such as aminoglycosides, clindamycin, vancomycin,tetracyclines, bacitracin, polymyxins, colistin, and sodium colistimethate, may enhance or prolong theneuromuscular blocking action of neuromuscular blocking agents (NMBAs). If these or other newlyintroduced antibiotics are used in conjunction with NMBAs, consider unexpected prolongation ofneuromuscular block a possibility. The use of peripheral nerve stimulator is strongly recommended to
evaluate the level of neuromuscular blockade, to assess the need for additional doses of the NMBA,and to determine whether adjustments need to be made to the dose with subsequent administration.[42031] [42614] [48672]
AnticonvulsantsConcomitant use of a nondepolarizing neuromuscular blocking agent (NMBA) in patients receivinganticonvulsants, such as carbamazepine or phenytoin, may increase resistance to the neuromuscularblockade action of nondepolarizing NMBAs, resulting in shorter durations of neuromuscular blockadeand higher infusion rate requirements. The use of peripheral nerve stimulator is strongly recommendedto evaluate the level of neuromuscular blockade, to assess the need for additional doses of NMBA, andto determine whether adjustments need to be made to the dose with subsequent administration. Whilethe mechanism for development of resistance is not known, receptor up-regulation may be acontributing factor.[42031] [42614]
CorticosteroidsAn acute myopathy has been observed with the use of high doses of corticosteroids in patientsreceiving concomitant long-term therapy with neuromuscular blockers. Limit the period of use ofneuromuscular blockers and corticosteroids and only use when the specific advantages of the drugsoutweigh the risks for acute myopathy. Clinical improvement or recovery after stopping therapy mayrequire weeks to years.[41961] [42031] [54278] [61750]
Inhalational anestheticsUse of volatile inhalational anesthetics with neuromuscular blocking agents (NMBAs) will enhanceneuromuscular blockade. Potentiation is most prominent with use of enflurane and isoflurane. Reductionof the initial dose or infusion rate of the NMBA may need to be considered.[41961] [42031] [42613] [42614] [48671] [48672]
Local anestheticsLocal anesthetics have been shown to increase the duration of neuromuscular block and decreaseinfusion requirements of neuromuscular blocking agents (NMBAs). The use of peripheral nervestimulator is strongly recommended to evaluate the level of neuromuscular blockade, to assess theneed for additional doses of NMBA, and to determine whether adjustments need to be made to the dosewith subsequent administration.[42031][42039][42614]
Magnesium saltsMagnesium may enhance or prolong the neuromuscular blocking action of neuromuscular blockingagents. The use of peripheral nerve stimulator is strongly recommended to evaluate the level ofneuromuscular blockade, to assess the need for additional doses of NMBA, and to determine whetheradjustments need to be made to the dose with subsequent administration.[42031][42039][42614][48672]
Drugs that reduce plasma cholinesterase activityConsider the possibility of prolonged neuromuscular block after administration of mivacurium orsuccinylcholine in patients with reduced plasma cholinesterase activity. Plasma cholinesterase activitymay be diminished by chronic administration of oral contraceptives, corticosteroid therapy, certain

monoamine oxidase inhibitors, or by drugs that irreversibly inhibit plasma cholinesterase, such asorganophosphate insecticides and certain antineoplastic drugs.[42039] [42613]
Safety IssuesSafety Issues Table
Export to CSV (Excel)
X – Contraindicated
X-BBW – Contraindicated and Black Box Warning
BBW – Black Box Warning, Not Contraindicated
Yes – REMS or MedGuide is available
Requires specialized care setting
Safety Issue AtracuriumBesylate
CisatracuriumBesylate
MivacuriumChloride
PancuroniumBromide
RocuroniumBromide
SuccinylcholineChloride
VecuroniumBromide
REMS
MedGuide
benzyl alcoholhypersensitivity X
bromidehypersensitivity X X X
burns X
children BBW
hyperkalemia BBW
infants BBW
malignanthyperthermia X
myopathy X
neonates X BBW
neuromuscularblocking agenthypersensitivity
X
prematureneonates X
requires anexperiencedclinician
BBW BBW
rhabdomyolysis BBW
trauma X

Neuromuscular blocking agent administration requires an experienced clinician who is familiar with itsactions and the possible complications that may occur after its use as well as requires a specializedcare setting where facilities for intubation, artificial respiration, oxygen therapy, and reversal agents areimmediately available.[42031] [42614] [48672]
AwarenessNeuromuscular blocking agents (NMBAs) do not provide sedation or analgesia and, in general, shouldbe administered only after unconsciousness has been induced. Maintain adequate amnesia andanalgesia throughout paralysis to avoid patient distress. Use of a peripheral nerve stimulator will permitthe most advantageous use of NMBAs, minimize the possibility of overdosage or underdosage, andassist in the evaluation of recovery. Monitor visual and tactile stimulation on muscle movement as wellas heart rate, blood pressure, and mechanical ventilator status during administration.[52441]
BurnsSuccinylcholine is contraindicated in patients after the acute phase of major burn injury due to the risk ofhyperkalemia. In addition, patients with burns have a decreased sensitivity to nondepolarizing agents'ability to produce neuromuscular blockade. Resistance to blockade usually develops in patients withburns more than 10% total body surface area approximately 1 week after thermal injury. Increaseddoses may be required in burn patients; alteration in drug effect may be seen for up to 1 year.[52478] [52482]
Electrolyte and acid-base imbalanceElectrolyte imbalance can alter a patient's sensitivity to neuromuscular blocking agents (NMBAs).Hypercalcemia can decrease sensitivity to NMBAs, while most other electrolyte disturbances increasesensitivity (e.g., hypokalemia, hypocalcemia, hypermagnesemia). Use NMBAs cautiously in patientswith conditions that may lead to electrolyte imbalances, such as adrenal insufficiency. Severe acid/baseimbalance may alter a patient's sensitivity to NMBAs: metabolic alkalosis, metabolic acidosis, andrespiratory acidosis may enhance neuromuscular blockade and/or prolong recovery time, whilerespiratory alkalosis reduces the potency of the drug.[42031] [48672] [52846] Use succinylcholine withcaution in patients with electrolyte abnormalities because of the potential for developing severehyperkalemia.[42039] [52486] Do not use succinylcholine in any patient with a serum potassium of morethan 5.5 mEq/L.[54427]
Neuromuscular diseaseUse neuromuscular blocking agents with caution in patients with neuromuscular disease (e.g.,myasthenia gravis, myasthenic syndrome [Eaton Lambert syndrome]); prolonged or exaggeratedneuromuscular blockade may occur after neuromuscular blocking agent use.[48672] [52486] [53645]
Because myasthenia gravis involves destruction of acetylcholine receptors instead of receptorupregulation, as seen in other neuromuscular diseases, these patients tend to be less sensitive to theeffects of succinylcholine compared to nondepolarizing agents (e.g., rocuronium, vecuronium).[53645] [54397] Additionally, patients with weak muscle tone are at an increased risk for airway and ventilationcomplications. Monitor patients carefully until recovery is fully complete.[48672]
Obesity

Obese patients are at an increased risk for airway and ventilation complications. [48672] Use ideal bodyweight or adjusted body weight for dosing in obese and morbidly obese adult patients (body mass index
30 kg/m2 or more).[62859] Guidelines for sustained neuromuscular blockade in critically ill childrenrecommend calculating the dose according to IBW.[52443]
Pseudocholinesterase deficiencyConsider the possibility of prolonged neuromuscular block after administration of mivacurium orsuccinylcholine in patients with reduced plasma cholinesterase activity (pseudocholinesterasedeficiency). Plasma cholinesterase activity may be diminished in the presence of genetic abnormalitiesof plasma cholinesterase (e.g., patients heterozygous or homozygous for atypical plasmacholinesterase gene), liver or kidney disease, malignant tumors, infection, burns, anemia,decompensated heart disease, peptic ulcer disease, or myxedema. Plasma cholinesterase activity mayalso be diminished by chronic administration of oral contraceptives, corticosteroid therapy, or certainmonoamine oxidase inhibitors and by cholinesterase inhibitor toxicity due to irreversible inhibitors ofplasma cholinesterase (e.g., organophosphate insecticides, echothiophate, and certain antineoplasticdrugs). Use mivacurium with caution, if at all, in patients known or suspected of being homozygous forthe atypical plasma cholinesterase gene; initial doses more than 0.03 mg/kg are not recommended inhomozygous patients. Mivacurium infusions are not recommended in homozygous patients. Mivacuriumhas been used safely in patients heterozygous for the atypical plasma cholinesterase gene and ingenotypically normal patients with reduced plasma cholinesterase activity. After an initial dose ofmivacurium 0.15 mg/kg, the clinically effective duration of block in heterozygous patients may beapproximately 10 minutes longer than in patients with normal genotype and normal plasmacholinesterase activity. Lower infusion rates of mivacurium are recommended in these patients.[42039] [42613]
Pediatric patientsBased on physiologic differences, neonates and infants tend to be more sensitive to paralysis withneuromuscular blocking agents, while children tend to require larger doses than those of infants oradults.[52501] [52452] Acute rhabdomyolysis, hyperkalemia, cardiac dysrhythmia, and fatal cardiac arresthas been associated with succinylcholine use in pediatric patients with undiagnosed myopathies.Because it is difficult to assess which patients are at risk, limit the use of succinylcholine in pediatricpatients for emergency intubation or when immediate securing of the airway is necessary (e.g.,laryngospasm, difficult airway, full stomach) or for intramuscular use when a suitable vein isinaccessible.[42039]
Hepatic impairmentHepatic impairment may enhance or prolong neuromuscular blockade associated with aminosteroidalneuromuscular blocking agents due to prolonged half-life and reduced clearance.[42031] [48672] [65345]
Although organ-independent elimination is the primary pathway for cisatracurium elimination, the liverplays a minor role in metabolite elimination. Metabolite (e.g., laudanosine) half-life is prolonged andconcentrations may be higher after long-term cisatracurium administration in patients with hepaticdysfunction.[42614]
Renal impairment

Substantial variability can be seen in the duration of neuromuscular blockade associated withaminosteroidal neuromuscular blocking agents in patients with renal impairment.[42031] [48672] [65345]
Although organ-independent elimination is the primary pathway for cisatracurium elimination, thekidneys play a minor role in metabolite elimination. Metabolite (e.g., laudanosine) half-life is prolongedand concentrations may be higher after long-term cisatracurium administration in patients with renaldysfunction.[42614]
Copyright © 2021 Elsevier Inc. All rights reserved.



















