
Effects of a Monoclonal Antibody Raised Against Nerve Growth Factor on Skeletal Pain and Bone...
11
Effects of a Monoclonal Antibody Raised Against Nerve Growth Factor on Skeletal Pain and Bone Healing After Fracture of the C57BL/6J Mouse Femur Nathan J Koewler, 1,2 Katie T Freeman, 1,2 Ryan J Buus, 3 Monica B Herrera, 1 Juan M Jimenez-Andrade, 1 Joseph R Ghilardi, 3 Christopher M Peters, 1 Lucy J Sullivan, 1 Michael A Kuskowski, 4 Jack L Lewis, 5,6 and Patrick W Mantyh 1,3,7,8,9 ABSTRACT: A closed femur fracture pain model was developed in the C57BL/6J mouse. One day after fracture, a monoclonal antibody raised against nerve growth factor (anti-NGF) was delivered intraperitone- ally and resulted in a reduction in fracture pain-related behaviors of ∼50%. Anti-NGF therapy did not interfere with bone healing as assessed by mechanical testing and histomorphometric analysis. Introduction: Current therapies to treat skeletal fracture pain are limited. This is because of the side effect profile of available analgesics and the scarcity of animal models that can be used to understand the mecha- nisms that drive this pain. Whereas previous studies have shown that mineralized bone, marrow, and perios- teum are innervated by sensory and sympathetic fibers, it is not understood how skeletal pain is generated and maintained even in common conditions such as osteoarthritis, low back pain, or fracture. Materials and Methods: In this study, we characterized the pain-related behaviors after a closed femur fracture in the C57BL/6J mouse. Additionally, we assessed the effect of a monoclonal antibody that binds to and sequesters nerve growth factor (anti-NGF) on pain-related behaviors and bone healing (mechanical properties and histomorphometric analysis) after fracture. Results: Administration of anti-NGF therapy (10 mg/kg, days 1, 6, and 11 after fracture) resulted in a reduction of fracture pain-related behaviors of ∼50%. Attenuation of fracture pain was evident as early as 24 h after the initial dosing and remained efficacious throughout the course of fracture pain. Anti-NGF therapy did not modify biomechanical properties of the femur or histomorphometric indices of bone healing. Conclusions: These findings suggest that therapies that target NGF or its cognate receptor(s) may be effective in attenuating nonmalignant fracture pain without interfering with bone healing. J Bone Miner Res 2007;22:1732–1742. Published online on July 16, 2007; doi: 10.1359/JBMR.070711 Key words: rodent, bone, neural factors, bone histomorphometry, skeletal pain INTRODUCTION S KELETAL FRACTURE PAIN can have a significant impact on quality of life and functionality of the affected indi- vidual. (1) In the young population, fracture pain frequently results from sports injuries, car accidents, improvised ex- ploding devices, or landmines. (2,3) In this patient popula- tion, fracture pain can be difficult to control, interfere with effective rehabilitation, and may lead to the development of complex regional pain syndrome. (4,5) Skeletal fracture pain also impacts the elderly; painful osteoporotic fractures of the vertebrae, hip, or femur are common in both postmeno- pausal women and older men. (6–10) Pain caused by osteo- porotic fractures of the hip and femur greatly reduces mobility resulting in decreased bone and muscle mass, which leads to a marked increase in morbidity and mortal- ity. (11–13) The relative paucity of therapies to treat fracture pain is in large part caused by the scarcity of animal models that closely mirror the human condition, which would allow the development of mechanism-based therapies to treat this pain. Several studies have shown mineralized bone, mar- row, and periosteum receive a significant innervation by primary afferent sensory neurons (14) and postganglionic sympathetic neurons. (15–17) However, what remains un- known is how sensory neurons that innervate the skeleton are activated in common nonmalignant skeletal pain con- ditions such as osteoarthritis, low back pain, or fracture. The authors state that they have no conflicts of interest. 1 Neurosystems Center and Department of Diagnostic and Biological Sciences, University of Minnesota, Minneapolis, Minnesota, USA; 2These authors contributed equally to this study; 3 Research Service VA Medical Center, Minneapolis, Minnesota, USA; 4 GRECC, VA Medical Center, Minneapolis, Minnesota, USA; 5 Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, Minnesota, USA; 6 Department of Mechanical Engineering, University of Minnesota, Minneapolis, Minnesota, USA; 7 Department of Psychiatry, University of Minnesota, Minneapolis, Minnesota, USA; 8 Department of Neuroscience, University of Minnesota, Minneapolis, Minne- sota, USA; 9 Cancer Center, University of Minnesota, Minneapolis, Minnesota, USA. JOURNAL OF BONE AND MINERAL RESEARCH Volume 22, Number 11, 2007 Published online on July 16, 2007; doi: 10.1359/JBMR.070711 © 2007 American Society for Bone and Mineral Research 1732
Transcript of Effects of a Monoclonal Antibody Raised Against Nerve Growth Factor on Skeletal Pain and Bone...

Effects of a Monoclonal Antibody Raised Against Nerve GrowthFactor on Skeletal Pain and Bone Healing After Fracture of the
C57BL/6J Mouse Femur
Nathan J Koewler,1,2 Katie T Freeman,1,2 Ryan J Buus,3 Monica B Herrera,1 Juan M Jimenez-Andrade,1
Joseph R Ghilardi,3 Christopher M Peters,1 Lucy J Sullivan,1 Michael A Kuskowski,4 Jack L Lewis,5,6 andPatrick W Mantyh1,3,7,8,9
ABSTRACT: A closed femur fracture pain model was developed in the C57BL/6J mouse. One day afterfracture, a monoclonal antibody raised against nerve growth factor (anti-NGF) was delivered intraperitone-ally and resulted in a reduction in fracture pain-related behaviors of ∼50%. Anti-NGF therapy did notinterfere with bone healing as assessed by mechanical testing and histomorphometric analysis.
Introduction: Current therapies to treat skeletal fracture pain are limited. This is because of the side effectprofile of available analgesics and the scarcity of animal models that can be used to understand the mecha-nisms that drive this pain. Whereas previous studies have shown that mineralized bone, marrow, and perios-teum are innervated by sensory and sympathetic fibers, it is not understood how skeletal pain is generated andmaintained even in common conditions such as osteoarthritis, low back pain, or fracture.Materials and Methods: In this study, we characterized the pain-related behaviors after a closed femur fracturein the C57BL/6J mouse. Additionally, we assessed the effect of a monoclonal antibody that binds to andsequesters nerve growth factor (anti-NGF) on pain-related behaviors and bone healing (mechanical propertiesand histomorphometric analysis) after fracture.Results: Administration of anti-NGF therapy (10 mg/kg, days 1, 6, and 11 after fracture) resulted in a reductionof fracture pain-related behaviors of ∼50%. Attenuation of fracture pain was evident as early as 24 h after theinitial dosing and remained efficacious throughout the course of fracture pain. Anti-NGF therapy did notmodify biomechanical properties of the femur or histomorphometric indices of bone healing.Conclusions: These findings suggest that therapies that target NGF or its cognate receptor(s) may be effectivein attenuating nonmalignant fracture pain without interfering with bone healing.J Bone Miner Res 2007;22:1732–1742. Published online on July 16, 2007; doi: 10.1359/JBMR.070711
Key words: rodent, bone, neural factors, bone histomorphometry, skeletal pain
INTRODUCTION
SKELETAL FRACTURE PAIN can have a significant impact onquality of life and functionality of the affected indi-
vidual.(1) In the young population, fracture pain frequentlyresults from sports injuries, car accidents, improvised ex-ploding devices, or landmines.(2,3) In this patient popula-tion, fracture pain can be difficult to control, interfere witheffective rehabilitation, and may lead to the development ofcomplex regional pain syndrome.(4,5) Skeletal fracture painalso impacts the elderly; painful osteoporotic fractures ofthe vertebrae, hip, or femur are common in both postmeno-pausal women and older men.(6–10) Pain caused by osteo-
porotic fractures of the hip and femur greatly reducesmobility resulting in decreased bone and muscle mass,which leads to a marked increase in morbidity and mortal-ity.(11–13)
The relative paucity of therapies to treat fracture pain isin large part caused by the scarcity of animal models thatclosely mirror the human condition, which would allow thedevelopment of mechanism-based therapies to treat thispain. Several studies have shown mineralized bone, mar-row, and periosteum receive a significant innervation byprimary afferent sensory neurons(14) and postganglionicsympathetic neurons.(15–17) However, what remains un-known is how sensory neurons that innervate the skeletonare activated in common nonmalignant skeletal pain con-ditions such as osteoarthritis, low back pain, or fracture.The authors state that they have no conflicts of interest.
1Neurosystems Center and Department of Diagnostic and Biological Sciences, University of Minnesota, Minneapolis, Minnesota, USA;2These authors contributed equally to this study; 3Research Service VA Medical Center, Minneapolis, Minnesota, USA; 4GRECC, VAMedical Center, Minneapolis, Minnesota, USA; 5Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, Minnesota,USA; 6Department of Mechanical Engineering, University of Minnesota, Minneapolis, Minnesota, USA; 7Department of Psychiatry,University of Minnesota, Minneapolis, Minnesota, USA; 8Department of Neuroscience, University of Minnesota, Minneapolis, Minne-sota, USA; 9Cancer Center, University of Minnesota, Minneapolis, Minnesota, USA.
JOURNAL OF BONE AND MINERAL RESEARCHVolume 22, Number 11, 2007Published online on July 16, 2007; doi: 10.1359/JBMR.070711© 2007 American Society for Bone and Mineral Research
1732
JO704231 1732 1742 November

The closed femur fracture model was originally devel-oped in the rat(18) and subsequently in the mouse(19) toexplore the factors that contribute to bone healing.(20–22) Inthis study, we adapted this model in the C57BL/6J (C57)mouse strain and simultaneously examined indices of skel-etal pain and bone healing after fracture. One reason theC57 mouse was chosen is that many genetically modifiedmice have been developed in a C57 background,(23) andthese mice may be useful in understanding the factors thatgenerate and maintain skeletal pain. Additionally, C57mice have a greater reduction in BMD with age comparedwith many other strains of mice,(24) which suggests theymay be an effective strain for examining pain and bonehealing after osteoporotic fracture.(25,26) In this study, weshow a stereotypic progression of skeletal remodeling andpain-related behaviors after fracture of the femur in youngadult C57 mice. Administration of anti-nerve growth factor(NGF) therapy attenuated fracture-induced pain withoutnegatively influencing bone healing.
MATERIALS AND METHODS
Animals
Experiments were performed on a total of 6 adult maleC3H/HEJ (C3H) mice and 42 adult male C57BL/6J (C57)mice (Jackson Laboratories, Bar Harbor, ME, USA),weighing 20–25 g. Mice were housed in accordance with theNIH guidelines under specific pathogen-free conditions inpartial autoclaved cages maintained at 22°C with a 12-halternating light and dark cycle and were given food andwater ad libitum. All procedures were approved by the In-stitutional Animal Care and Use Committee at the Univer-sity of Minnesota.
Surgical and fracture procedure
Before femoral pin placement, mice received an intra-peritoneal injection of 100 mg/kg ketamine and 10 mg/kgxylazine to provide anesthesia. An incision of ∼6 mm wasmade in the skin and the proximal patellar ligament of theleft femur was severed, revealing the synovial space of theknee joint as previously described.(19,27) A 30-gauge needlewas used to core between the condyles into the medullarycanal of the left femur. Mice were immediately radio-graphed to ensure proper coring; any mice with needlesoutside of the medullary canal were killed. A 0.5-mm dentalburr was used to prime the opening of the hole, and a29-gauge needle was used as a pilot to widen the hole. Aprecut 0.011-in-diameter stainless steel wire (pin; SmallParts, Miami Lakes, FL, USA) was inserted into the med-ullary space for fracture stabilization, and dental amalgamwas used to secure the pin and close the hole. Wound clips(MikRon Precision, Gardena, CA, USA) were used toclose the incision and were removed 5 days after pin place-ment.
A closed mid-diaphyseal fracture of the left femur wasproduced 14 days after pin placement in mice under anes-thesia (100 mg/kg ketamine and 10 mg/kg xylazine, IP) us-ing a three-point bending device (BBC Specialty Automo-tive Center, Linden, NJ, USA) as previously described.(28)
The methodology used to induce a closed fracture of thefemur was originally described for the rat by Bonnarensand Einhorn(18) and later adapted for mice by Manigrassoand O’Connor.(19) Immediately after fracture, mice wereradiographed to ensure localization of fracture to mid-diaphysis of the femur. Mice that met any of the exclusioncriteria were immediately killed and were not used for thisstudy. Exclusion criteria were adapted from Gerstenfeld etal.(29) and included fractures located too far from the mid-diaphyseal region of the femur, dislodged pins, nonvisiblefracture after impact, and fragmentation of the bone. Afterrecovery from anesthesia after fracture, mice were allowedunrestricted movement and limb weight bearing.
Behavioral analysis
Mice were behaviorally analyzed before fracture (day 0)and at days 1, 2, 4, 7, 10, 14, 18, and 24 after fracture toassess ongoing (spontaneous) fracture pain-related behav-iors, as previously described.(32–42) Briefly, the number ofhind paw flinches and time spent guarding over a 2-minobservation period were recorded as measures of ongoingpain, because these endpoints are similar to observations inpatients who protect their fractured limb.(43) The numberof total vertical stands requiring the use of both hind limbs(used as a measure of loading on the fractured limb) wasrecorded during a 2-min observation period at each behav-ioral time-point. Total vertical stands were defined as thenumber of times the animal stands on both hind limbs sup-porting their entire body weight.(44,45) The experimentalprotocol consisted of three different groups: pin + vehicle(n � 7), fracture + vehicle (n � 2), and fracture + anti-NGF (n � 13). All C57 mice were behaviorally analyzed(guarding, flinching, and rearing) in all of the previouslystated time-points. To monitor the general health of themice, body weights were recorded throughout the experi-ment, and mice were observed for any potential side effectscaused by the therapy including ataxia, illness, or lethargy.
Treatment with anti-NGF therapy
The anti-NGF antibody, (mAb 911; Rinat Laboratories,PGRD, Palo Alto, CA, USA) is effective in sequesteringNGF. Thus, NGF is unable to bind to its receptors (trkAand p75) and exert its actions.(46) It binds to both humanand rodent NGF and does not appreciably bind to othermembers of the neurotrophin family.(46) Previous studieshave shown anti-NGF antibody possess a plasma half-life of∼5–6 days in the mouse and it does not appreciably cross theblood–brain barrier.(47)
Before behavioral and bone analysis, C57 mice were di-vided into three treatment groups, as previously stated, re-ceiving either vehicle (pin + vehicle and fracture + vehicle)or anti-NGF antibody (fracture + anti-NGF). Vehicle (ster-ile saline, IP) or anti-NGF antibody were administered tomice on days 1, 6, and 11 after fracture (10 mg/kg, IP, eachtime-point). Baseline behavioral analysis was conducted be-fore anti-NGF administration on day 1. Ten milligrams perkilogram was selected as this dose has been shown to beefficacious in bone cancer pain(27,37) and osteoarthritis(47)
rodent models.
NGF FRACTURE PAIN AND BONE HEALING IN C57 MICE 1733

Radiographical and µCT analysis
Radiograph (Specimen Radiography System Model MX-20; Faxitron X-ray Corp., Wheeling IL, USA; Kodak filmMin-R 2000; Kodak, Rochester, NY, USA) images of frac-tured femurs were obtained immediately after fracture andat all behavior time-points (days 1, 2, 4, 7, 10, 14, 18, and24), as well as day 30 and day 42. Fracture-induced callusformation was radiographically assessed at ×4 magnifica-tion.(48,49) The images were scanned (Scanjet XPA; HewlettPackard, Palo Alto, CA, USA) at 600-dpi resolution, andthe area of the callus was determined by a blinded investi-gator using Image ProPlus v 6.0 software (Media Cybernet-ics, Silver Spring, MD, USA). Additionally, the imageswere used to evaluate bone bridging of the fractured femursat all time-points. The mean bone bridging score was evalu-ated on a 0–4 scale based on Bergenstock et al.(28) Briefly,points were given for bridging across the two cortices of thefractured femur (one point each) and across the two pe-ripheral sides of the callus (one point each) by a blindedinvestigator.
�CT images of naïve femurs of C3H and C57 mice wereobtained with an eXplore Locus SP �CT (GE Healthcare,London, Ontario, Canada). The conebeam CT scannerused a 2300 × 2300 CCD detector with current and voltageset at 80 �A and 80 KVp, respectively. A 360° scan wasperformed with a 3000-ms integration time with images re-constructed at 16-�m3 resolution. 3D images were createdusing the MicroView analysis software (GE Healthcare)
Biomechanical analysis
The time-point to mechanically test the structuralstrength and stiffness of the fractured femurs was based onradiographic analysis that showed that day 42 was the firsttime that fractured femurs of our C57 mice treated withvehicle and anti-NGF had a score greater than 3 (where 0 isno bridging, and 4 is complete bridging across the callus).This bone bridging scoring system is based on that devisedby Bergenstock et al.(28) for assessing fracture healing out-comes. This time for healing agrees with the study by Tagu-chi et al.,(50) who also used a closed femur fracture in 8-wk-old male mice. In these mice, mature bone was evident at 5wk but not 3 wk after fracture. Additionally, Manigrassoand O’Connor(19) reported biomechanical properties of thehealing of mice femurs are not reached until 6 wk afterfracture. For these reasons, biomechanical testing was per-formed at day 42 (6 wk) in this study.
Briefly, mice were killed with compressed CO2 and per-fused intracardially with 12 ml of 0.1 M PBS. Pins wereremoved, and femurs were loaded to failure in four-pointbending at a displacement rate of 0.03 mm/s using a servo-hydraulic material test machine (Instron 5548 Microtester;Instron Corp., Norwood, MA, USA).(51) The femurs wereloaded at mid-diaphysis by two load points 5.4 mm apart onthe posterior surface and resting on two supports 9.0 mmapart on the anterior surface. Load and displacement datawere collected every 0.1 s using Bluehill 2 software (InstronCorp.) and exported to Microsoft Excel for analysis. Ipsi-lateral femurs were tested for all groups (n � 6 for eachgroup), pin + vehicle, fracture + vehicle, and fracture +
anti-NGF. Maximum load and stiffness were derived fromthe load-displacement curves.(51,52)
Histomorphometric analysis
Histomorphometric analysis of the fracture + vehicle andfracture + anti-NGF mice were performed as previouslydescribed.(53–55) Briefly, unfixed femurs were decalcified in10% EDTA for 1 wk at 4°C, paraffin-embedded, and seri-ally sectioned in the sagittal plane using a Leica Microsys-tems RM2135 microtome (Wetzlar, Germany) at 7 �mthickness. Five sections at least 150 �m apart spanning atleast 0.75 mm of the center of the fracture callus of eachanimal were stained with hematoxylin and eosin (H&E).(54)
Sections were photographed at ×20 using a SPOT II digitalcamera with SPOT image capture software (Diagnostic In-struments, Sterling Heights, MI, USA) attached to anOlympus BX51 microscope. Primary histomorphometricmeasurements included the area and perimeter of the totalcallus (T.Ar and T.Pm), void space (Vd.Ar and Vd.Pm),and trabeculae (Tb.Ar and Tb.Pm). The T.Ar and T.Pmwere obtained from the outer most boundary of the cal-lus.(53) The Vd.Ar and Vd.Pm contained all uncalcified ar-eas, including marrow cavity, within the callus.(57) Tb.Arand Tb.Pm were directly measured from the cancellousbone contained within the marrow.(58) All measurementswere performed by a blinded investigator using Image Pro-Plus v6.0.
Total callus area (TOT.Ar; TOT.Ar � T.Ar − Vd.Ar +Tb.Ar), total callus perimeter (TOT.Pm; TOT.Pm � T.Pm+ Vd.Pm + Tb.Pm), and area of the cortical bone in thecallus (Ct.Ar; Ct.Ar � T.Ar − Vd.Ar) were derived asdescribed by Parfitt et al.(53,59) Standardized 3D histomor-phometric parameters of volumes and surfaces were ex-trapolated from 2D areas and perimeters. These includedtotal volume (TV), total bone volume (BV), bone surface(BS), cortical bone volume (CBV), and trabecular bonevolume (TBV; T.Ar � TV, TOT.Ar � BV, TOT.Pm �BS, Ct.Ar � CBV, Tb.Ar � TBV).(53) The parametersBV, CBV, and TBV were expressed as the percent of thetotal callus volume, BV (%), CBV (%), and TBV (%),respectively.(60–62) Microarchitecture analysis of the frac-ture callus was calculated from the aforementioned 3Dmeasures to assess trabecular thickness (Tb.Th; Tb.Th �2BV/BS), trabecular number [Tb.N; Tb.N � (BV/TV)/Tb.Th], and trabecular separation [Tb.Sp; Tb.Sp � Tb.Th ×TV/(BV-1)].(30,53,58,63,64)
Statistical analysis
The SPSS v. 11 statistics package (SPSS, Chicago, IL,USA) was used to perform statistical analyses. Group dif-ferences in spontaneous guarding, spontaneous flinching,and spontaneous vertical stands were assessed with anANOVA for the individual samples collected at each post-fracture time-point. Significant ANOVA results were fol-lowed by individual two-group comparisons using Fisher’sleast significant difference (LSD) pairwise multiple com-parison test. For bone healing data analysis, each depen-dent outcome variable was compared across groups using anonparametric ANOVA (Kruskal-Wallis) followed by non-
KOEWLER ET AL.1734

parametric posthoc comparisons between pairs of groupsusing the Mann-Whitney U-test. Results were consideredstatistically significant at p < 0.05. In all cases, the investi-gator was blind to the experimental status of each animal.
RESULTS
Comparison of femurs from C57 and C3H
Cortical bone thickness differences in two commonstrains of mice used in bone research, C57 and C3H, areshown in Fig. 1. C57 mice have thinner cortical walls com-pared with C3H mice as shown by multiple imaging tech-niques: cross-sectional �CT (Fig. 1A), cross-sectional H&E(Fig. 1B), longitudinal �CT (Fig. 1C), and radiographs(Fig. 1D).
Fracture production in C57 mice
The three-point fracture protocol resulted in reproduc-ible transverse or slightly oblique mid-diaphyseal femoralfractures (Fig. 2). In this study, 9 of 34 mice that werefractured met the exclusion criteria. Mice were killed im-mediately after fracture if any of the previously definedexclusion criteria were met,(29) which included fractures lo-cated too far from the mid-diaphyseal region of the femur,
dislodged pins, nonvisible fracture after impact, or fragmen-tation of the femur at the site of fracture.
Assessment of ongoing pain-related behaviors afrerfemoral fracture
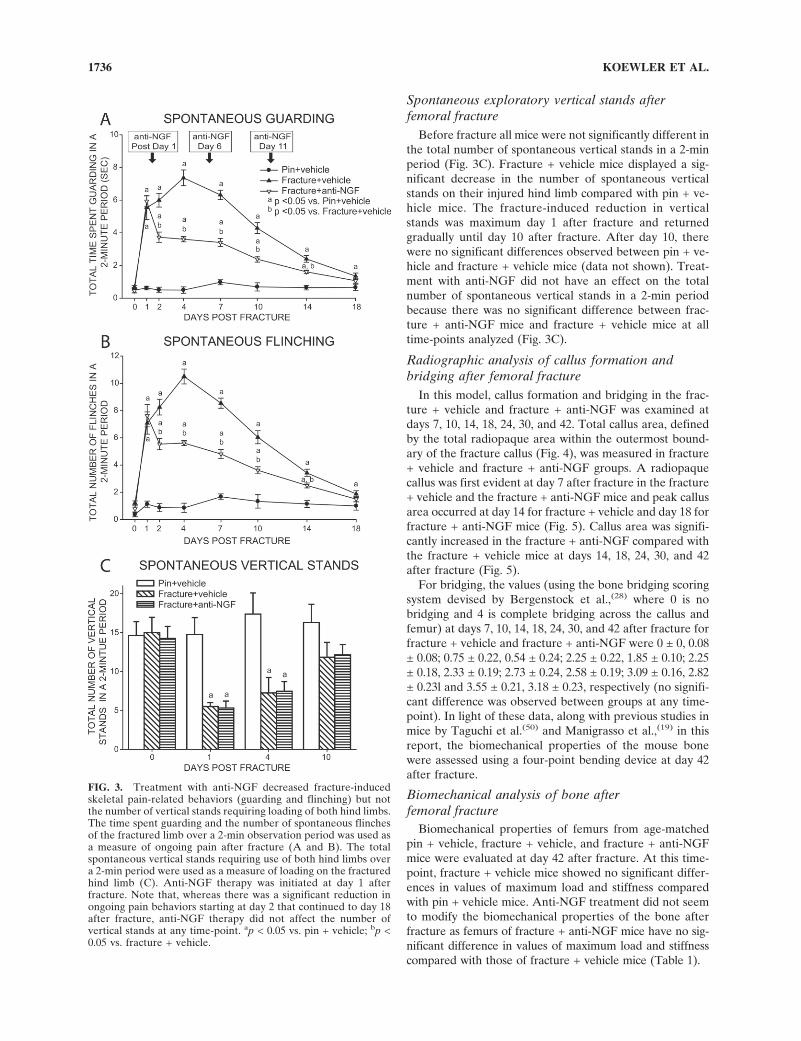
Ongoing (spontaneous guarding and flinching) pain-related behaviors were analyzed over a 2-min period in pin+ vehicle, fracture + vehicle, and fracture + anti-NGF mice.Fracture + vehicle mice exhibited a significantly greatertime spent guarding and a significantly increased number offlinches compared with pin + vehicle mice (Figs. 3A and3B) from day 1 through day 18 after fracture. These ongo-ing pain-related behaviors peaked at day 4 after fractureand decreased gradually through day 18 after fracture. Atday 24 after fracture pain-related behaviors in fracture +vehicle mice were not significantly different to those in pin+ vehicle mice (data not shown).
Treatment with anti-NGF (10 mg/kg, administered atdays 1, 6, and 11 after fracture) significantly reduced frac-ture-induced ongoing guarding and flinching pain-relatedbehaviors when compared with fracture + vehicle mice. Theanalgesic effect was evident at the first time-point examined(day 2), which was 24 h after initial administration of anti-NGF and this analgesic effect continued through day 18after fracture (Figs. 3A and 3B). There were no significantside effects, such as loss of weight, reduced luster of fur,ataxia, fever, or lethargy, observed in fracture + anti-NGFmice (data not shown).
FIG. 1. Different strains of inbred mice show differences in thethickness of the cortical bone of the femur. Cross-sectional �CTimages (A), hemotoxin and eosin (H&E)-stained sections (B),longitudinal �CT images (C), and longitudinal high-resolution ra-diolographical images (D) show differences in the thickness of thecortical bone in the mid-diaphysis of femur in C3H/HEJ vs.C57BL/6J mice. Note that the cortical wall of the femur of C3Hmice is thicker than age-matched C57 mice. Scale bar: (A) 1 mm;(B) � 50 �m; (C and D) � 1.5 mm.
FIG. 2. High-resolution images of C57BL/6J femurs obtainedfrom naïve (A), pin (B), and fracture (C) age-matched mice. Astainless steel pin was implanted into the intramedullary space at8 wk of age to provide the stability required for callus formationand bone healing of the femur. After 2 wk of recovery the femurswhere then fractured at 10 wk of age. The closed mid-diaphysealfracture of the left femur was produced using a three-point frac-ture device and the image shown in C is day 2 after fracture. Scalebar � 1.5 mm.
NGF FRACTURE PAIN AND BONE HEALING IN C57 MICE 1735
Fig 1 live 4/C
Spontaneous exploratory vertical stands afterfemoral fracture
Before fracture all mice were not significantly different inthe total number of spontaneous vertical stands in a 2-minperiod (Fig. 3C). Fracture + vehicle mice displayed a sig-nificant decrease in the number of spontaneous verticalstands on their injured hind limb compared with pin + ve-hicle mice. The fracture-induced reduction in verticalstands was maximum day 1 after fracture and returnedgradually until day 10 after fracture. After day 10, therewere no significant differences observed between pin + ve-hicle and fracture + vehicle mice (data not shown). Treat-ment with anti-NGF did not have an effect on the totalnumber of spontaneous vertical stands in a 2-min periodbecause there was no significant difference between frac-ture + anti-NGF mice and fracture + vehicle mice at alltime-points analyzed (Fig. 3C).
Radiographic analysis of callus formation andbridging after femoral fracture
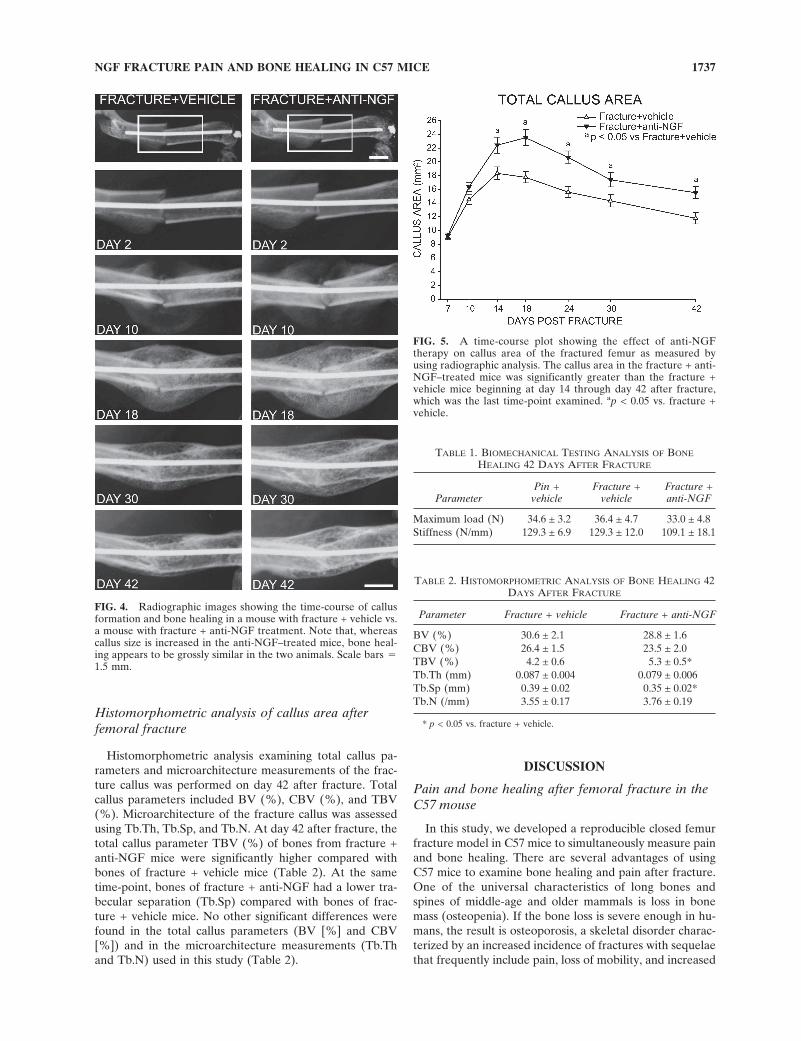
In this model, callus formation and bridging in the frac-ture + vehicle and fracture + anti-NGF was examined atdays 7, 10, 14, 18, 24, 30, and 42. Total callus area, definedby the total radiopaque area within the outermost bound-ary of the fracture callus (Fig. 4), was measured in fracture+ vehicle and fracture + anti-NGF groups. A radiopaquecallus was first evident at day 7 after fracture in the fracture+ vehicle and the fracture + anti-NGF mice and peak callusarea occurred at day 14 for fracture + vehicle and day 18 forfracture + anti-NGF mice (Fig. 5). Callus area was signifi-cantly increased in the fracture + anti-NGF compared withthe fracture + vehicle mice at days 14, 18, 24, 30, and 42after fracture (Fig. 5).
For bridging, the values (using the bone bridging scoringsystem devised by Bergenstock et al.,(28) where 0 is nobridging and 4 is complete bridging across the callus andfemur) at days 7, 10, 14, 18, 24, 30, and 42 after fracture forfracture + vehicle and fracture + anti-NGF were 0 ± 0, 0.08± 0.08; 0.75 ± 0.22, 0.54 ± 0.24; 2.25 ± 0.22, 1.85 ± 0.10; 2.25± 0.18, 2.33 ± 0.19; 2.73 ± 0.24, 2.58 ± 0.19; 3.09 ± 0.16, 2.82± 0.23l and 3.55 ± 0.21, 3.18 ± 0.23, respectively (no signifi-cant difference was observed between groups at any time-point). In light of these data, along with previous studies inmice by Taguchi et al.(50) and Manigrasso et al.,(19) in thisreport, the biomechanical properties of the mouse bonewere assessed using a four-point bending device at day 42after fracture.
Biomechanical analysis of bone afterfemoral fracture
Biomechanical properties of femurs from age-matchedpin + vehicle, fracture + vehicle, and fracture + anti-NGFmice were evaluated at day 42 after fracture. At this time-point, fracture + vehicle mice showed no significant differ-ences in values of maximum load and stiffness comparedwith pin + vehicle mice. Anti-NGF treatment did not seemto modify the biomechanical properties of the bone afterfracture as femurs of fracture + anti-NGF mice have no sig-nificant difference in values of maximum load and stiffnesscompared with those of fracture + vehicle mice (Table 1).
FIG. 3. Treatment with anti-NGF decreased fracture-inducedskeletal pain-related behaviors (guarding and flinching) but notthe number of vertical stands requiring loading of both hind limbs.The time spent guarding and the number of spontaneous flinchesof the fractured limb over a 2-min observation period was used asa measure of ongoing pain after fracture (A and B). The totalspontaneous vertical stands requiring use of both hind limbs overa 2-min period were used as a measure of loading on the fracturedhind limb (C). Anti-NGF therapy was initiated at day 1 afterfracture. Note that, whereas there was a significant reduction inongoing pain behaviors starting at day 2 that continued to day 18after fracture, anti-NGF therapy did not affect the number ofvertical stands at any time-point. ap < 0.05 vs. pin + vehicle; bp <0.05 vs. fracture + vehicle.
KOEWLER ET AL.1736
Histomorphometric analysis of callus area afterfemoral fracture
Histomorphometric analysis examining total callus pa-rameters and microarchitecture measurements of the frac-ture callus was performed on day 42 after fracture. Totalcallus parameters included BV (%), CBV (%), and TBV(%). Microarchitecture of the fracture callus was assessedusing Tb.Th, Tb.Sp, and Tb.N. At day 42 after fracture, thetotal callus parameter TBV (%) of bones from fracture +anti-NGF mice were significantly higher compared withbones of fracture + vehicle mice (Table 2). At the sametime-point, bones of fracture + anti-NGF had a lower tra-becular separation (Tb.Sp) compared with bones of frac-ture + vehicle mice. No other significant differences werefound in the total callus parameters (BV [%] and CBV[%]) and in the microarchitecture measurements (Tb.Thand Tb.N) used in this study (Table 2).
DISCUSSION
Pain and bone healing after femoral fracture in theC57 mouse
In this study, we developed a reproducible closed femurfracture model in C57 mice to simultaneously measure painand bone healing. There are several advantages of usingC57 mice to examine bone healing and pain after fracture.One of the universal characteristics of long bones andspines of middle-age and older mammals is loss in bonemass (osteopenia). If the bone loss is severe enough in hu-mans, the result is osteoporosis, a skeletal disorder charac-terized by an increased incidence of fractures with sequelaethat frequently include pain, loss of mobility, and increased
FIG. 4. Radiographic images showing the time-course of callusformation and bone healing in a mouse with fracture + vehicle vs.a mouse with fracture + anti-NGF treatment. Note that, whereascallus size is increased in the anti-NGF–treated mice, bone heal-ing appears to be grossly similar in the two animals. Scale bars �1.5 mm.
FIG. 5. A time-course plot showing the effect of anti-NGFtherapy on callus area of the fractured femur as measured byusing radiographic analysis. The callus area in the fracture + anti-NGF–treated mice was significantly greater than the fracture +vehicle mice beginning at day 14 through day 42 after fracture,which was the last time-point examined. ap < 0.05 vs. fracture +vehicle.
TABLE 1. BIOMECHANICAL TESTING ANALYSIS OF BONE
HEALING 42 DAYS AFTER FRACTURE
ParameterPin +
vehicleFracture +
vehicleFracture +anti-NGF
Maximum load (N) 34.6 ± 3.2 36.4 ± 4.7 33.0 ± 4.8Stiffness (N/mm) 129.3 ± 6.9 129.3 ± 12.0 109.1 ± 18.1
TABLE 2. HISTOMORPHOMETRIC ANALYSIS OF BONE HEALING 42DAYS AFTER FRACTURE
Parameter Fracture + vehicle Fracture + anti-NGF
BV (%) 30.6 ± 2.1 28.8 ± 1.6CBV (%) 26.4 ± 1.5 23.5 ± 2.0TBV (%) 4.2 ± 0.6 5.3 ± 0.5*Tb.Th (mm) 0.087 ± 0.004 0.079 ± 0.006Tb.Sp (mm) 0.39 ± 0.02 0.35 ± 0.02*Tb.N (/mm) 3.55 ± 0.17 3.76 ± 0.19
* p < 0.05 vs. fracture + vehicle.
NGF FRACTURE PAIN AND BONE HEALING IN C57 MICE 1737

loss of muscle and bone mass.(65) In general C57 mice havea relatively thin cortical wall, low BMD, and greater pro-pensity to develop osteoporosis as they age(25) comparedwith inbred strains of mice such as the C3H mice,(66) whichhave been used in our laboratory to examine malignantbone pain.(27,67)
A second advantage of using C57 mice is that a signifi-cant fraction of all genetically modified mice has been de-veloped in this strain.(23,68) Genetically modified mice in-cluding knockouts, knock-ins, and cell-specific expressionof fluorescent markers or proteins have revolutionized ourability to define the specific molecules and cells involved ingeneration of a variety of neurological diseases includingchronic pain.(23,68,69) Generating a pain fracture model inthe C57 background will allow investigators to use geneti-cally modified C57 mice without having to perform exten-sive backcrossing to simultaneously examine the role thatspecific molecules play in the pain and bone healing thatfollows fracture.(68) Additionally, the behavioral character-istics of C57 mice have been extensively studied in varietyof inflammatory and neuropathic pain models,(70,71) whichwill allow investigators to compare and contrast the anal-gesic efficacy of novel therapies in a commonly used strainof mice in different types of acute and chronic pain states.The reproducibility and robust endpoints for both fracture-induced pain behaviors and bone healing in the C57 modelshould thus allow investigators to examine the effects ofnovel, mechanism-based therapies on skeletal pain andbone healing in both young and aged mice.
Current analgesics used to treat fracture pain
A major reason fracture pain remains a significant healthproblem is the limited repertoire of analgesics available totreat this pain without negatively influencing fracture heal-ing and/or the ability of the patient to participate in effec-tive rehabilitation. For example, nonsteroidal anti-inflammatory drugs (NSAIDS), which are effective inreducing a variety of musculoskeletal pains,(72,73) have beenshown to inhibit fracture healing in both mice(74) andrats.(75) Thus, studies in rodents have shown that NSAIDSand selective cyclo-oxygenase-2 (COX-2) inhibitors hindercallus formation and effective bridging of the fracture sitethat results in delayed bone healing, increased incidence ofnonunion of bone, and decreased bone strength.(31,76,77)
These findings have been supported by similar studieswhere NSAIDS and COX-2 inhibitors appear to delay, butnot completely inhibit, bone healing and bridging after frac-ture.(4,78) These data, together with recent reports thatshow selective prostaglandin agonists of the EP2 receptoraccelerate bone healing after fracture(79,80) indeed suggestthat the use of NSAIDS and COX-2 inhibitors may delayfracture induced bone healing.
There are relatively few studies that have examined thedirect effect that opioids or their receptors may have onbone healing. However, opioids do have a variety of non-skeletal side effects that can inhibit bone healing. Opioidsas a class cause increased somnolence, agitation, constipa-tion, dizziness, and cognitive impairment that can reducemobility, resulting in loss of bone and muscle mass.(81) In
young individuals with severe fractures, long-term opiateuse can result in dependence and a reduced ability topromptly and fully participate in effective musculoskeletalrehabilitation that is necessary for early and effective bonehealing.(82,83) In elderly patients, opioid side effects tend tobe more pronounced.(84) After osteoporotic fractures in theelderly, minimum bed rest is desired to minimize inactivityinduced loss of bone and muscle mass.(85) However, admin-istration of strong opiates will, in general, reduce the abilityof these patients to effectively engage in the exercise andrehabilitation necessary for more rapid bone healing. To-gether, these data highlight the need for the development ofnovel, mechanism based therapies to treat skeletal pain thathave negligible or a positive effect on bone healing.
NGF, pain, and bone healing after fracture
Using this C57 model of fracture pain and bone healingwe show that, after femoral fracture, anti-NGF therapy re-duced pain related behaviors, while having either no effectin some measures or a positive effect in other measures ofbone healing. Concerning the timing of the administrationof anti-NGF therapy, it should be emphasized that anti-NGF was first administered 1 day after fracture, which is atime-point when a human would begin to receive long-termanalgesic therapy for fracture pain. The analgesic effect ofanti-NGF therapy in reducing skeletal pain was statisticallysignificant at the first time-point examined (which was day2 after fracture) and the analgesic efficacy of the therapyremained as long as pain-related behaviors were present.Importantly, the analgesic effect of anti-NGF did not resultin inappropriate loading of the fractured bones as assessedby the number of spontaneous vertical stands that requiremechanical loading of the two hind limbs. Additionally,anti-NGF therapy did not result in longer healing times thatmay occur when the fracture site is loaded or stressed in-appropriately as it does in both rodents and humans.(86,87)
In this study, we targeted anti-NGF for reducing nonma-lignant fracture pain because our previous results showedthat anti-NGF was efficacious in reducing malignant pain inmouse models of sarcoma- and prostate-induced bone can-cer pain.(27,37) These results showed that anti-NGF therapyresulted in a 50% reduction in fracture-induced pain be-haviors. We believe that anti-NGF is exerting its analgesiceffect by binding to and sequestering NGF, which preventsNGF binding to its cognate receptors trkA or p75.(88)
It has been reported that a variety of inflammatory, im-mune, and stromal cells upregulate the expression of NGFand NGF receptors after fracture(89) and tissue injury.(90) Inthe adult, NGF can directly activate and sensitize sensoryneurons involved in the conduction of pain originating fromthe skin(91–93) and visceral organs.(94,95) NGF is thought toexcite and sensitize sensory neurons by binding to its cog-nate receptors trkA and p75 that are expressed by a sub-population of mostly unmyelinated and thinly myelinatedsensory neurons.(88,96) NGF binding to trkA has beenshown to directly depolarize trkA expressing nociceptors invivo and in vitro and that binding of NGF to trkA directlylowers the threshold for depolarization in these neu-
KOEWLER ET AL.1738

rons.(88,97,98) Additionally, NGF has been shown to modu-late and/or sensitize a variety of neurotransmitters, recep-tors, ion channels, and structural molecules expressed bynociceptors including: neurotransmitters (substance P,brain derived neurotrophic factor, and CGRP), receptors(bradykinin, P2X3), channels (TRPV1, ASIC-3, and so-dium channels), transcription factors (ATF-3), and struc-tural molecules (neurofilaments and the sodium channelanchoring molecule p11).(88,96,99–101) It has also been shownthat NGF lowers the threshold and enhances the responseof nociceptors to mechanical stimuli,(102) suggesting thatNGF may play a role in activating/sensitizing mechano-transducers in sensory fibers that innervate bone. Together,the above results suggest that NGF may be an upstreamregulator of a variety of neurotransmitter/receptors that areexpressed by nociceptors that innervate the bone and thatare involved in sensing and transmitting pain after fractureof the skeleton.
One rather unique aspect of the sensory innervation ofbone, which may partially explain why anti-NGF therapy iseffective in relieving both malignant(27,37) and nonmalig-nant skeletal pain (this study), is that the majority of nervefibers innervating the bone seem to be CGRP-expressingfibers, nearly all of which co-express trkA.(103,104) Thus, inboth humans and rodents, the primary afferent sensory fi-bers that innervate the human(105) and rodent vertebraldiscs(106) and bone,(15,107–109) seem to be CGRP/trkA ex-pressing fibers with few unmyelinated nonpeptidergic IB4/RET+ nerve fibers being present in these tissues.(15) Thus,because bone seems to largely lack the redundancy of thenonpeptidergic IB4/RET+ nerve fibers that are present inskin,(110) anti-NGF may be particularly efficacious in reliev-ing bone pain where nociceptors that express CGRP/trkAare the primary nerve fiber population that is driving thepain.
We also examined whether anti-NGF therapy delaysfracture healing. As assessed radiographically and histo-morphometrically, chronic administration of anti-NGFtherapy increased the callus area around the fracture site inall time-points examined. Whereas callus size may not be areliable indicator of proper bone healing,(111,112) callus for-mation is required for the initial stabilization of the bonethat decreases fracture pain(113) and permits the proper de-struction and formation of mineralized bone at the fracturesite to begin to occur.(63,114,115) Based on this, it is possibleto suggest that the anti-NGF analgesic effect could be par-tially explained by an increase in the callus formation afterfracture. To examine bone healing, we performed biome-chanical and histomorphometric analysis of the bones 42days after fracture. When anti-NGF was administered at 1,6, and 11 days after fracture, anti-NGF therapy either hadno effect or a slightly positive effect on bone healing. Pre-vious results using topical application of NGF to the frac-ture site in the rat suggested that NGF could promote boneformation after fracture.(116) However, it is difficult to com-pare the penetration and pharmacokinetics of NGF whentopically applied to the rat bone(116) versus this study wherethe monoclonal antibody raised against NGF had a definedplasma half-life of 6 days(47) and was systemically availableto all sites outside the blood–brain barrier. Given the time
it takes to heal fractures of the femur in the mouse versushuman (weeks versus months) and the greater amount oftime the patient would be receiving anti-NGF therapy, fur-ther studies of the potential osteogenic effects of anti-NGFafter fracture are clearly warranted.
Current therapies to treat skeletal fracture pain are lim-ited. This is largely because of the side effects of currentlyavailable analgesics and the scarcity of animal models tostudy the mechanisms that generate and maintain this pain.In this study, we developed a fracture pain model in C57mice where pain and bone healing can be simultaneouslyassessed. One day after fracture, anti-NGF was deliveredsystemically and resulted in an ∼50% reduction in fracture-related pain behaviors. Anti-NGF therapy did not interferewith the mechanical strength of the newly formed bone andonly had a small but significant effect on bone healing asassessed by callus formation and histomorphometric analy-sis. Understanding the mechanisms that drive skeletal painto develop mechanism-based therapies will have significantpotential to improve rehabilitative outcomes in both youngand old patients with skeletal fractures.
ACKNOWLEDGMENTS
This work was supported by National Institutes of HealthGrants NS23970 and NS048021 and a Merit Review fromthe Veterans Administration. We thank ThereseSchachtele for excellent administrative assistance.
REFERENCES
1. Court-Brown CM, Koval KJ 2006 The epidemiology of frac-tures. In: Bucholz RW, Heckman JD, Court-Brown CM (eds.)Rockwood and Green’s Fractures in Adults, 6th ed., vol. 1.Lippincott Williams & Wilkins, Philadelphia, PA, USA, pp.95–143.
2. Hame SL, LaFemina JM, McAllister DR, Schaadt GW, Do-rey FJ 2004 Fractures in the collegiate athlete. Am J SportsMed 32:446–451.
3. Papadakis SA, Babourda EC, Mitsitskas TC, Markakidis S,Bachtis C, Koukouvis D, Tentes AA 2006 Anti-personnellandmine injuries during peace: Experience in a Europeancountry. Prehospital Disaster Med 21:237–240.
4. Koester MC, Spindler KP 2006 Pharmacologic agents in frac-ture healing. Clin Sports Med 25:63–73.
5. de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, StrickerBH, Sturkenboom MC 2006 The incidence of complex re-gional pain syndrome: A population-based study. Pain129:12–20.
6. Kasperk C, Hillmeier J, Noldge G, Grafe IA, Dafonseca K,Raupp D, Bardenheuer H, Libicher M, Liegibel UM, SommerU, Hilscher U, Pyerin W, Vetter M, Meinzer HP, Meeder PJ,Taylor RS, Nawroth P 2005 Treatment of painful vertebralfractures by kyphoplasty in patients with primary osteoporo-sis: A prospective nonrandomized controlled study. J BoneMiner Res 20:604–612.
7. Brenneman SK, Barrett-Connor E, Sajjan S, Markson LE,Siris ES 2006 Impact of recent fracture on health-related qual-ity of life in postmenopausal women. J Bone Miner Res21:809–816.
8. Melton LJ III 2003 Adverse outcomes of osteoporotic frac-tures in the general population. J Bone Miner Res 18:1139–1141.
9. Van der Klift M, De Laet CE, McCloskey EV, Hofman A,
NGF FRACTURE PAIN AND BONE HEALING IN C57 MICE 1739
Pols HA 2002 The incidence of vertebral fractures in men andwomen: The Rotterdam Study. J Bone Miner Res 17:1051–1056.
10. Kanis JA, Oden A, Johnell O, Jonsson B, de Laet C, DawsonA 2001 The burden of osteoporotic fractures: A method forsetting intervention thresholds. Osteoporos Int 12:417–427.
11. Center JR, Nguyen TV, Schneider D, Sambrook PN, EismanJA 1999 Mortality after all major types of osteoporotic frac-ture in men and women: An observational study. Lancet353:878–882.
12. Johnell O, Kanis J 2005 Epidemiology of osteoporotic frac-tures. Osteoporos Int 16(Suppl 2):S3–S7.
13. Johnell O, Kanis JA 2006 An estimate of the worldwideprevalence and disability associated with osteoporotic frac-tures. Osteoporos Int 17:1726–1733.
14. Iversen PO, Nicolaysen A, Hjeltnes N, Nja A, Benestad HB2004 Preserved granulocyte formation and function, as well asbone marrow innervation, in subjects with complete spinalcord injury. Br J Haematol 126:870–877.
15. Mach DB, Rogers SD, Sabino MC, Luger NM, Schwei MJ,Pomonis JD, Keyser CP, Clohisy DR, Adams DJ, O’Leary P,Mantyh PW 2002 Origins of skeletal pain: Sensory and sym-pathetic innervation of the mouse femur. Neuroscience113:155–166.
16. Hill EL, Elde R 1991 Distribution of CGRP-, VIP-, DßH-,SP-, and NPY-immunoreactive nerves in the periosteum ofthe rat. Cell Tissue Res 264:469–480.
17. Hukkanen M, Konttinen YT, Santavirta S, Paavolainen P, GuXH, Terenghi G, Polak JM 1993 Rapid proliferation of calci-tonin gene-related peptide-immunoreactive nerves duringhealing of rat tibial fracture suggests neural involvement inbone growth and remodelling. Neuroscience 54:969–979.
18. Bonnarens F, Einhorn TA 1984 Production of a standardclosed fracture in laboratory animal bone. J Orthop Res 2:97–101.
19. Manigrasso MB, O’Connor JP 2004 Characterization of aclosed femur fracture model in mice. J Orthop Trauma18:687–695.
20. Chhabra A, Zijerdi D, Zhang J, Kline A, Balian G, HurwitzS 2005 BMP-14 deficiency inhibits long bone fracture healing:A biochemical, histologic, and radiographic assessment. J Or-thop Trauma 19:629–634.
21. Fujii H, Kitazawa R, Maeda S, Mizuno K, Kitazawa S 1999Expression of platelet-derived growth factor proteins andtheir receptor alpha and beta mRNAs during fracture healingin the normal mouse. Histochem Cell Biol 112:131–138.
22. Yaoita H, Orimo H, Shirai Y, Shimada T 2000 Expression ofbone morphogenetic proteins and rat distal-less homologgenes following rat femoral fracture. J Bone Miner Metab18:63–70.
23. Wilson SG, Mogil JS 2001 Measuring pain in the (knockout)mouse: Big challenges in a small mammal. Behav Brain Res125:65–73.
24. Beamer WG, Donahue LR, Rosen CJ, Baylink DJ 1996 Ge-netic variability in adult bone density among inbred strains ofmice. Bone 18:397–403.
25. Ferguson VL, Ayers RA, Bateman TA, Simske SJ 2003 Bonedevelopment and age-related bone loss in male C57BL/6Jmice. Bone 33:387–398.
26. Wilhelmi G, Faust R 1976 Suitability of the C57 black mouseas an experimental animal for the study of skeletal changesdue to ageing, with special reference to osteo-arthrosis and itsresponse to tribenoside. Pharmacology 14:289–296.
27. Sevcik MA, Ghilardi JR, Peters CM, Lindsay TH, HalvorsonKG, Jonas BM, Kubota K, Kuskowski MA, Boustany L,Shelton DL, Mantyh PW 2005 Anti-NGF therapy profoundlyreduces bone cancer pain and the accompanying increase inmarkers of peripheral and central sensitization. Pain 115:128–141.
28. Bergenstock M, Min W, Simon AM, Sabatino C, O’ConnorJP 2005 A comparison between the effects of acetaminophenand celecoxib on bone fracture healing in rats. J OrthopTrauma 19:717–723.
29. Gerstenfeld LC, Al-Ghawas M, Alkhiary YM, Cullinane DM,Krall EA, Fitch JL, Webb EG, Thiede MA, Einhorn TA 2007Selective and nonselective cyclooxygenase-2 inhibitors andexperimental fracture-healing. Reversibility of effects aftershort-term treatment. J Bone Joint Surg Am 89:114–125.
30. Gerstenfeld LC, Alkhiary YM, Krall EA, Nicholls FH,Stapleton SN, Fitch JL, Bauer M, Kayal R, Graves DT, Jep-sen KJ, Einhorn TA 2006 Three-dimensional reconstructionof fracture callus morphogenesis. J Histochem Cytochem54:1215–1228.
31. Simon AM, Manigrasso MB, O’Connor JP 2002 Cyclo-oxygenase 2 function is essential for bone fracture healing. JBone Miner Res 17:963–976.
32. Blackburn-Munro G 2004 Pain-like behaviours in animals—how human are they? Trends Pharmacol Sci 25:299–305.
33. Goblirsch M, Zwolak P, Ramnaraine ML, Pan W, Lynch C,Alaei P, Clohisy DR 2006 Novel cytosine deaminase fusiongene enhances the effect of radiation on breast cancer in boneby reducing tumor burden, osteolysis, and skeletal fracture.Clin Cancer Res 12:3168–3176.
34. Vermeirsch H, Nuydens RM, Salmon PL, Meert TF 2004Bone cancer pain model in mice: Evaluation of pain behavior,bone destruction and morphine sensitivity. Pharmacol Bio-chem Behav 79:243–251.
35. Sabino MA, Ghilardi JR, Jongen JL, Keyser CP, Luger NM,Mach DB, Peters CM, Rogers SD, Schwei MJ, de Felipe C,Mantyh PW 2002 Simultaneous reduction in cancer pain,bone destruction, and tumor growth by selective inhibition ofcyclooxygenase-2. Cancer Res 62:7343–7349.
36. Honore P, Luger NM, Sabino MA, Schwei MJ, Rogers SD,Mach DB, O’Keefe PF, Ramnaraine ML, Clohisy DR, Man-tyh PW 2000 Osteoprotegerin blocks bone cancer-inducedskeletal destruction, skeletal pain and pain-related neuro-chemical reorganization of the spinal cord. Nat Med 6:521–528.
37. Halvorson KG, Kubota K, Sevcik MA, Lindsay TH, SotilloJE, Ghilardi JR, Rosol TJ, Boustany L, Shelton DL, MantyhPW 2005 A blocking antibody to nerve growth factor attenu-ates skeletal pain induced by prostate tumor cells growing inbone. Cancer Res 65:9426–9435.
38. Sevcik MA, Luger NM, Mach DB, Sabino MA, Peters CM,Ghilardi JR, Schwei MJ, Rohrich H, De Felipe C, KuskowskiMA, Mantyh PW 2004 Bone cancer pain: The effects of thebisphosphonate alendronate on pain, skeletal remodeling, tu-mor growth and tumor necrosis. Pain 111:169–180.
39. Peters CM, Ghilardi JR, Keyser CP, Kubota K, Lindsay TH,Luger NM, Mach DB, Schwei MJ, Sevcik MA, Mantyh PW2005 Tumor-induced injury of primary afferent sensory nervefibers in bone cancer pain. Exp Neurol 193:85–100.
40. Mouedden ME, Meert TF 2007 Pharmacological evaluationof opioid and non-opioid analgesics in a murine bone cancermodel of pain. Pharmacol Biochem Behav 86:458–467.
41. Luger NM, Sabino MA, Schwei MJ, Mach DB, Pomonis JD,Keyser CP, Rathbun M, Clohisy DR, Honore P, Yaksh TL,Mantyh PW 2002 Efficacy of systemic morphine suggests afundamental difference in the mechanisms that generate bonecancer vs inflammatory pain. Pain 99:397–406.
42. Sabino MA, Luger NM, Mach DB, Rogers SD, Schwei MJ,Mantyh PW 2003 Different tumors in bone each give rise to adistinct pattern of skeletal destruction, bone cancer-relatedpain behaviors and neurochemical changes in the central ner-vous system. Int J Cancer 104:550–558.
43. Santy J, Mackintosh C 2001 A phenomenological study ofpain following fractured shaft of femur. J Clin Nurs 10:521–527.
44. Hsieh YL 2006 Effects of ultrasound and diclofenac phono-phoresis on inflammatory pain relief: Suppression of induciblenitric oxide synthase in arthritic rats. Phys Ther 86:39–49.
45. Raghavendra V, Agrewala JN, Kulkarni SK 2000 Melatoninreversal of lipopolysacharides-induced thermal and behav-ioral hyperalgesia in mice. Eur J Pharmacol 395:15–21.
46. Hongo JS, Laramee GR, Urfer R, Shelton DL, Restivo T,Sadick M, Galloway A, Chu H, Winslow JW 2000 Antibody
KOEWLER ET AL.1740
binding regions on human nerve growth factor identified byhomolog- and alanine-scanning mutagenesis. Hybridoma19:215–227.
47. Shelton DL, Zeller J, Ho WH, Pons J, Rosenthal A 2005Nerve growth factor mediates hyperalgesia and cachexia inauto-immune arthritis. Pain 116:8–16.
48. Bergstrom J, Bostedor R, Masarachia P, Reszka A, Rodan G2000 Alendronate Is a Specific, Nanomolar Inhibitor of Far-nesyl Diphosphate Synthase. Arch Biochem Biophys373:231–241.
49. Koivukangas A, Tuukkanen J, Kippo K, Jamsa T, Hannuni-emi R, Pasanen I, Vaananen K, Jalovaara P 2003 Long-termadministration of clodronate does not prevent fracture heal-ing in rats. Clin Orthop 408:268–278.
50. Taguchi K, Ogawa R, Migita M, Hanawa H, Ito H, Orimo H2005 The role of bone marrow-derived cells in bone fracturerepair in a green fluorescent protein chimeric mouse model.Biochem Biophys Res Commun 331:31–36.
51. Ulrich-Vinther M, Schwarz EM, Pedersen FS, Soballe K, An-dreassen TT 2005 Gene therapy with human osteoprotegerindecreases callus remodeling with limited effects on biome-chanical properties. Bone 37:751–758.
52. Hiltunen A, Vuorio E, Aro HT 1993 A standardized experi-mental fracture in the mouse tibia. J Orthop Res 11:305–312.
53. Parfitt A, Drezner M, Glorieux F, Kanis J, Malluche H, Meu-nier P, Ott S, Recker R 1987 Bone histomorphometry: Stan-dardization of nomenclature, symbols, and units. J BoneMiner Res 2:595–610.
54. Gerstenfeld LC, Wronski TJ, Hollinger JO, Einhorn TA 2005Application of histomorphometric methods to the study ofbone repair. J Bone Miner Res 20:1715–1722.
55. Chappard D, Retailleau-Gaborit N, Legrand E, Basle MF,Audran M 2005 Comparison insight bone measurements byhistomorphometry and microCT. J Bone Miner Res 20:1177–1184.
56. Schmidmaier G, Wildemann B, Gabelein T, Heeger J, Kand-ziora F, Haas NP, Raschke M 2003 Synergistic effect of IGF-Iand TGF-beta1 on fracture healing in rats: Single versus com-bined application of IGF-I and TGF-beta1. Acta OrthopScand 74:604–610.
57. Alkhiary YM, Gerstenfeld LC, Krall E, Westmore M, Sato M,Mitlak BH, Einhorn TA 2005 Enhancement of experimentalfracture-healing by systemic administration of recombinanthuman parathyroid hormone (PTH 1-34). J Bone Joint SurgAm 87:731–741.
58. Yingling VR, Xiang Y, Raphan T, Schaffler MB, Koser K,Malique R 2007 The effect of a short-term delay of puberty ontrabecular bone mass and structure in female rats: A texture-based and histomorphometric analysis. Bone 40:419–424.
59. Akhter MP, Iwaniec UT, Covey MA, Cullen DM, KimmelDB, Recker RR 2000 Genetic variations in bone density, his-tomorphometry, and strength in mice. Calcif Tissue Int67:337–344.
60. Gabet Y, Muller R, Regev E, Sela J, Shteyer A, Salisbury K,Chorev M, Bab I 2004 Osteogenic growth peptide modulatesfracture callus structural and mechanical properties. Bone35:65–73.
61. Erdogan O, Esen E, Ustun Y, Kurkcu M, Akova T, GonlusenG, Uysal H, Cevlik F 2006 Effects of low-intensity pulsedultrasound on healing of mandibular fractures: An experi-mental study in rabbits. J Oral Maxillofac Surg 64:180–188.
62. Lu C, Miclau T, Hu D, Hansen E, Tsui K, Puttlitz C, MarcucioRS 2005 Cellular basis for age-related changes in fracturerepair. J Orthop Res 23:1300–1307.
63. Li M, Healy DR, Li Y, Simmons HA, Crawford DT, Ke HZ,Pan LC, Brown TA, Thompson DD 2005 Osteopenia andimpaired fracture healing in aged EP4 receptor knockoutmice. Bone 37:46–54.
64. Dalle Carbonare L, Valenti MT, Bertoldo F, Zanatta M, Ze-nari S, Realdi G, Lo Cascio V, Giannini S 2005 Bone micro-architecture evaluated by histomorphometry. Micron 36:609–616.
65. Gazit D, Zilberman Y, Ebner R, Kahn A 1998 Bone loss
(osteopenia) in old male mice results from diminished activityand availability of TGF-beta. J Cell Biochem 70:478–488.
66. Richman C, Kutilek S, Miyakoshi N, Srivastava AK, BeamerWG, Donahue LR, Rosen CJ, Wergedal JE, Baylink DJ, Mo-han S 2001 Postnatal and pubertal skeletal changes contributepredominantly to the differences in peak bone density be-tween C3H/HeJ and C57BL/6J mice. J Bone Miner Res16:386–397.
67. Luger NM, Honore P, Sabino MAC, Schwei MJ, Rogers SD,Mach DB, Clohisy DR, Mantyh PW 2001 Osteoprotegerindiminishes advanced bone cancer pain. Cancer Res 61:4038–4047.
68. Feng G, Lu J, Gross J 2004 Generation of transgenic mice. In:Luo DZ (ed.) Pain Research: Methods and Protocols. Hu-mana Press, Totowa, NJ, USA, pp. xi.
69. Feng G, Mellor RH, Bernstein M, Keller-Peck C, NguyenQT, Wallace M, Nerbonne JM, Lichtman JW, Sanes JR 2000Imaging neuronal subsets in transgenic mice expressing mul-tiple spectral variants of GFP. Neuron 28:41–51.
70. Caterina MJ, Leffler A, Malmberg AB, Martin WJ, Trafton J,Petersen-Zeitz KR, Koltzenburg M, Basbaum AI, Julius D2000 Impaired nociception and pain sensation in mice lackingthe capsaicin receptor. Science 288:306–313.
71. Amaya F, Wang H, Costigan M, Allchorne AJ, Hatcher JP,Egerton J, Stean T, Morisset V, Grose D, Gunthorpe MJ,Chessell IP, Tate S, Green PJ, Woolf CJ 2006 The voltage-gated sodium channel Na(v)1.9 is an effector of peripheralinflammatory pain hypersensitivity. J Neurosci 26:12852–12860.
72. Balano KB 1996 Anti-inflammatory drugs and myorelaxants.Pharmacology and clinical use in musculoskeletal disease.Prim Care 23:329–334.
73. Mason L, Moore RA, Edwards JE, Derry S, McQuay HJ 2004Topical NSAIDs for chronic musculoskeletal pain: Systematicreview and meta-analysis. BMC Musculoskelet Disord 19:5–28.
74. Murnaghan M, Li G, Marsh DR 2006 Nonsteroidal anti-inflammatory drug-induced fracture nonunion: An inhibitionof angiogenesis? J Bone Joint Surg Am 88(Suppl 3):140–147.
75. Simon AM, O’Connor JP 2007 Dose and time-dependent ef-fects of cyclooxygenase-2 inhibition on fracture-healing. JBone Joint Surg Am 89:500–511.
76. Leonelli SM, Goldberg BA, Safanda J, Bagwe MR, Sethurat-nam S, King SJ 2006 Effects of a cyclooxygenase-2 inhibitor(rofecoxib) on bone healing. Am J Orthop 35:79–84.
77. Gerstenfeld LC, Thiede M, Seibert K, Mielke C, Phippard D,Svagr B, Cullinane D, Einhorn TA 2003 Differential inhibi-tion of fracture healing by non-selective and cyclooxygenase-2selective non-steroidal anti-inflammatory drugs. J Orthop Res21:670–675.
78. Bhattacharyya T, Levin R, Vrahas MS, Solomon DH 2005Nonsteroidal antiinflammatory drugs and nonunion of hu-meral shaft fractures. Arthritis Rheum 53:364–367.
79. Li M, Ke HZ, Qi H, Healy DR, Li Y, Crawford DT, ParalkarVM, Owen TA, Cameron KO, Lefker BA, Brown TA,Thompson DD 2003 A novel, non-prostanoid EP2 receptor-selective prostaglandin E2 agonist stimulates local bone for-mation and enhances fracture healing. J Bone Miner Res18:2033–2042.
80. Paralkar VM, Borovecki F, Ke HZ, Cameron KO, Lefker B,Grasser WA, Owen TA, Li M, DaSilva-Jardine P, Zhou M,Dunn RL, Dumont F, Korsmeyer R, Krasney P, Brown TA,Plowchalk D, Vukicevic S, Thompson DD 2003 An EP2 re-ceptor-selective prostaglandin E2 agonist induces bone heal-ing. Proc Natl Acad Sci USA 100:6736–6740.
81. Ensrud KE, Blackwell T, Mangione CM, Bowman PJ, BauerDC, Schwartz A, Hanlon JT, Nevitt MC, Whooley MA 2003Central nervous system active medications and risk for frac-tures in older women. Arch Intern Med 163:949–957.
82. Mahowald ML, Singh JA, Majeski P 2005 Opioid use by pa-tients in an orthopedics spine clinic. Arthritis Rheum 52:312–321.
83. Massey GM, Dodds HN, Roberts CS, Servoss TJ, Blondell
NGF FRACTURE PAIN AND BONE HEALING IN C57 MICE 1741
RD 2005 Toxicology screening in orthopedic trauma patientspredicting duration of prescription opioid use. J Addict Dis24:31–41.
84. Feinberg SD 2000 Prescribing analgesics. How to improvefunction and avoid toxicity when treating chronic pain. Geri-atrics 55:44,49–50,53.
85. Zuckerman JD 1996 Hip fracture. N Engl J Med 334:1519–1525.
86. Gardner MJ, van der Meulen MC, Demetrakopoulos D,Wright TM, Myers ER, Bostrom MP 2006 In vivo cyclic axialcompression affects bone healing in the mouse tibia. J OrthopRes 24:1679–1686.
87. Kenwright J, Gardner T 1998 Mechanical influences on tibialfracture healing. Clin Orthop 355(Suppl):S179–S190.
88. Hefti FF, Rosenthal A, Walicke PA, Wyatt S, Vergara G,Shelton DL, Davies AM 2006 Novel class of pain drugs basedon antagonism of NGF. Trends Pharmacol Sci 27:85–91.
89. Grills BL, Schuijers JA 1998 Immunohistochemical localiza-tion of nerve growth factor in fractured and unfractured ratbone. Acta Orthop Scand 69:415–419.
90. McMahon SB, Bennett DLH, Bevan S 2006 Inflammatory me-diators and modulators of pain. In: McMahon SB, Koltzen-burg M (eds.) Wall and Melzack’s Textbook of Pain, 5th ed.Elsevier/Churchill Livingstone, Philadelphia, PA, USA, pp.xviii.
91. Bennett DL, Koltzenburg M, Priestley JV, Shelton DL, Mc-Mahon SB 1998 Endogenous nerve growth factor regulatesthe sensitivity of nociceptors in the adult rat. Eur J Neurosci10:1282–1291.
92. Lewin GR, Rueff A, Mendell LM 1994 Peripheral and centralmechanisms of NGF-induced hyperalgesia. Eur J Neurosci6:1903–1912.
93. Lewin GR, Ritter AM, Mendell LM 1993 Nerve growth fac-tor-induced hyperalgesia in the neonatal and adult rat. J Neu-rosci 13:2136–2148.
94. Dmitrieva N, McMahon SB 1996 Sensitisation of visceral af-ferents by nerve growth factor in the adult rat. Pain 66:87–97.
95. Delafoy L, Raymond F, Doherty AM, Eschalier A, Diop L2003 Role of nerve growth factor in the trinitrobenzene sul-fonic acid-induced colonic hypersensitivity. Pain 105:489–497.
96. Pezet S, McMahon SB 2006 Neurotrophins: Mediators andmodulators of pain. Annu Rev Neurosci 29:507–538.
97. Shu X, Mendell LM 2001 Acute sensitization by NGF of theresponse of small-diameter sensory neurons to capsaicin. JNeurophysiol 86:2931–2938.
98. Kerr BJ, Souslova V, McMahon SB, Wood JN 2001 A role forthe TTX-resistant sodium channel Nav 1.8 in NGF-inducedhyperalgesia, but not neuropathic pain. Neuroreport 12:3077–3080.
99. Bielefeldt K, Ozaki N, Gebhart GF 2003 Role of nervegrowth factor in modulation of gastric afferent neurons in therat. Am J Physiol Gastrointest Liver Physiol 284:G499–G507.
100. Gould HJ III, Gould TN, England JD, Paul D, Liu ZP, Levin-son SR 2000 A possible role for nerve growth factor in theaugmentation of sodium channels in models of chronic pain.Brain Res 854:19–29.
101. Ji RR, Samad TA, Jin SX, Schmoll R, Woolf CJ 2002 p38MAPK activation by NGF in primary sensory neurons afterinflammation increases TRPV1 levels and maintains heat hy-peralgesia. Neuron 36:57–68.
102. Malik-Hall M, Dina OA, Levine JD 2005 Primary afferentnociceptor mechanisms mediating NGF-induced mechanicalhyperalgesia. Eur J Neurosci 21:3387–3394.
103. Averill S, McMahon SB, Clary DO, Reichardt LF, Priestley
JV 1995 Immunocytochemical localization of trkA receptorsin chemically identified subgroups of adult rat sensory neu-rons. Eur J Neurosci 7:1484–1494.
104. Walsh GS, Krol KM, Kawaja MD 1999 Absence of the p75neurotrophin receptor alters the pattern of sympathosensorysprouting in the trigeminal ganglia of mice overexpressingnerve growth factor. J Neurosci 19:258–273.
105. Ozawa T, Ohtori S, Inoue G, Aoki Y, Moriya H, Takahashi K2006 The degenerated lumbar intervertebral disc is innervatedprimarily by peptide-containing sensory nerve fibers in hu-mans. Spine 31:2418–2422.
106. Ozawa T, Aoki Y, Ohtori S, Takahashi K, Chiba T, Ino H,Moriya H 2003 The dorsal portion of the lumbar interverte-bral disc is innervated primarily by small peptide-containingdorsal root ganglion neurons in rats. Neurosci Lett 344:65–67.
107. Bjurholm A, Kreicbergs A, Brodin E, Schultzberg M 1988Substance P- and CGRP-immunoreactive nerves in bone.Peptides 9:165–171.
108. Hill EL, Elde R 1988 Calcitonin gene-related peptide-immunoreactive nerve fibers in mandibular periosteum of rat:Evidence for primary afferent origin. Neurosci Lett 85:172–178.
109. Artico M, Bosco S, Cavallotti C, Agostinelli E, Giuliani-Piccari G, Sciorio S, Cocco L, Vitale M 2002 Noradrenergicand cholinergic innervation of the bone marrow. Int J MolMed 10:77–80.
110. Zylka MJ, Rice FL, Anderson DJ 2005 Topographically dis-tinct epidermal nociceptive circuits revealed by axonal tracerstargeted to Mrgprd. Neuron 45:17–25.
111. Panjabi MM, Walter SD, Karuda M, White AA, Lawson JP1985 Correlations of radiographic analysis of healing fractureswith strength: A statistical analysis of experimental osteoto-mies. J Orthop Res 3:212–218.
112. Blokhuis TJ, de Bruine JH, Bramer JA, den Boer FC, BakkerFC, Patka P, Haarman HJ, Manoliu RA 2001 The reliabilityof plain radiography in experimental fracture healing. Skel-etal Radiol 30:151–156.
113. Bonica JJ, Bonica JJ 1990 The Management of Pain, 2nd ed.Lea & Febiger, Philadelphia, PA, USA.
114. Holzer G, Majeska RJ, Lundy MW, Hartke JR, Einhorn TA1999 Parathyroid hormone enhances fracture healing. A pre-liminary report. Clin Orthop 366:258–263.
115. Manabe T, Mori S, Mashiba T, Kaji Y, Iwata K, KomatsubaraS, Seki A, Sun YX, Yamamoto T 2007 Human parathyroidhormone (1-34) accelerates natural fracture healing process inthe femoral osteotomy model of cynomolgus monkeys. Bone34:346–351.
116. Grills BL, Schuijers JA, Ward AR 1997 Topical application ofnerve growth factor improves fracture healing in rats. J Or-thop Res 15:235–242.
Address reprint requests to:Patrick W Mantyh, PhD
Neurosystems Center18-208 Moos Tower
University of Minnesota515 Delaware Street SE
Minneapolis, MN 55455, USAE-mail: [email protected]
Received in original form April 18, 2007; revised form June 15,2007; accepted July 9, 2007.
KOEWLER ET AL.1742




















