
Safety of Chinese Herbal Medicine for Chronic Obstructive Pulmonary Disease
Upload
independentCategory
view
2download
0
edicine and Rehabilitation
Archives of Physical M journal homepage: www.archives-pmr.orgArchives of Physical Medicine and Rehabilitation 2013;-:-------
ORIGINAL ARTICLE
Effectiveness of Pulmonary Rehabilitation in Exercise Capacityand Quality of Life in Chronic Obstructive Pulmonary DiseasePatients With and Without Global Fat-Free Mass Depletion
Danilo C. Berton, MD, ScD,a Leonardo Silveira, PT,a Cassia C. Da Costa, PT, ScD,b
Rafael Machado De Souza, MSc,b Claudia D. Winter, MSc,b
Paulo Jose Zimermann Teixeira, MD, ScDb,c
From the aPost-Graduate Program in Sciences (Pulmonology), Federal University of Rio Grande do Sul, Porto Alegre; bHealth Science Institute,Feevale University, Novo Hamburgo; and cFederal University of Health Science of Porto Alegre, Pavilhao Pereira Filho, Santa Casa de PortoAlegre, Brazil.
Abstract
Objective: To investigate the effectiveness of pulmonary rehabilitation (PR) in exercise capacity and quality of life in patients with chronic
obstructive pulmonary disease (COPD) with and without global fat-free mass (FFM) depletion.
Design: Retrospective case-control.
Setting: Outpatient clinic, university center.
Participants: COPD patients (NZ102) that completed PR were initially evaluated.
Intervention: PR including whole-body and weight training for 12 weeks, 3 times per week.
Main Outcome Measures: St. George Respiratory Questionnaire (SGRQ), 6-minute walk distance (6MWD), and FFM evaluation applied before
and after PR.
Results: Patients were stratified according to their FFM status measured by bioelectric impedance. They were considered depleted if the FFM index
was �15kg/m2 in women and �16kg/m2 in men. From the initial sample, all depleted patients (nZ31) composed the FFM depleted group. It was
composed predominantly by women (68%) with a mean age� SD of 64.4�7.3 years and a forced expiratory volume in 1 second of 33.6%Z�13.2%
predicted. Paired for sex and age, 31 nondepleted patients were selected from the initial sample to compose the nondepleted group. Improvement in
the 6MWD was similar in these 2 groups after PR. Both groups improved SGRQ scores, although the observed power was small and did not allow
adequate comparison between depleted and nondepleted patients. Therewas no difference between groups in weight change, whereas FFM tended to
be greater in depleted patients. This increase had no correlation with the 6MWD or the SGRQ.
Conclusions: Benefits of PR to exercise capacity were similar comparing FFM depleted and nondepleted COPD patients. Although FFM change
tended to be greater in depleted patients, this increase had no definite relation with clinical outcomes.
Archives of Physical Medicine and Rehabilitation 2013;-:-------
ª 2013 by the American Congress of Rehabilitation Medicine
The cardinal symptoms in most patients with chronic obstructivepulmonary disease (COPD) are dyspnea and exercise intolerance,resulting in decreased health status.1 Extra-pulmonary manifes-tations often include profound peripheral muscle deconditioningand sarcopenia. Peripheral muscle weakness and an alteredmuscle energy metabolism have been recognized as contributing
Supported by Feevale University, Novo Hamburgo, Brazil.
No commercial party having a direct financial interest in the results of the research supporting
this article has or will confer a benefit on the authors or on any organization with which the authors
are associated.
0003-9993/13/$36 - see front matter ª 2013 by the American Congress of Re
http://dx.doi.org/10.1016/j.apmr.2013.02.005
factors to impaired exercise capacity,2,3 and these associationsare related to depletion of muscle mass.4 Loss of muscle masscauses significant impact on muscle function5 and on survival.6-9
No current treatment strategy could reverse the loss of lungfunction in these patients.1 Nonetheless, improvements in skel-etal muscle function after exercise training result in gains inexercise capacity despite the absence of changes in lungfunction.10
Improving peripheral skeletal muscle mass and function is,therefore, an important goal of pulmonary rehabilitation (PR)
habilitation Medicine

2 D.C. Berton et al
programs. PR is currently considered standard care for patientswith chronic lung diseases and is associated with improvement inimportant clinical outcomes, such as exercise capacity, health-related quality of life (HRQOL), and dyspnea.11 Unfortunately,poor adherence is common in daily practice of PR, because manyCOPD patients fail to attend programs and others drop out.12
Some studies have shown that low fat-free mass (FFM)13 andreduced quadriceps strength14 are major conditions associatedwith PR absenteeism and drop out, respectively.
Additionally, exercise can induce increased systemic inflam-matory and oxidative responses in muscle-wasted COPDpatients15 and can alter amino acid intermediary metabolism inpatients with COPD, regardless of muscle depletion.16 Increasingevidence associates systemic inflammation and oxidative stresswith muscle wasting and muscle dysfunction in COPD.17,18 FFMdepleted COPD patients may represent, therefore, a group lesslikely to improve in PR programs.
Despite these findings, we believe that FFM depleted patientscan achieve the same clinical benefits after PR as nondepletedpatients. Previous studies evaluating depleted COPD inpatientsshowed an increase in FFM after rehabilitation, mainly whencombining rigorous nutritional supplementation with orwithout androgenic steroid administration.19,20 More recently,a community-based rehabilitation plus nutritional supportprogram demonstrated that wasted patients improved FFM andweight, a finding not observed in nonwasted patients.21
However, these studies did not primarily compare depleted andnondepleted COPD patients regarding improvement in exercisecapacity, HRQOL, and the relation of these clinical outcomeswith FFM changes after PR.
The aim of the current study is to evaluate the effects of anoutpatient PR program on improvements in exercise capacity,HRQOL, and FFM, contrasting FFM depleted and nondepletedpatients with moderate-to-severe COPD. The relations betweenchanges in FFM and clinical outcomes after PR were also eval-uated. We hypothesized that FFM depleted patients could achievesimilar clinical benefits as nondepleted COPD patients from anoutpatient PR program.
Methods
Participants
Pulmonary function, dyspnea, body composition, exercisecapacity, and disease-specific health status have been assessedprospectively in 129 consecutive pulmonary disease patientsbefore and after a specialized PR program. Subjects with clinical
List of abbreviations:
BMI body mass index
COPD chronic obstructive pulmonary disease
FEV1 forced expiratory volume in 1 second
FFM fat-free mass
FVC forced vital capacity
HRQOL health-related quality of life
MANOVA multiple analysis of variance
MRC Medical Research Council
PR pulmonary rehabilitation
RM repetition maximum
SGRQ St. George Respiratory Questionnaire
6MWD 6-minute walk distance
and functional diagnosis of COPD (nZ102) according to theglobal strategy for the diagnosis, management, and prevention ofCOPD guidelines1 (irreversible airflow limitation defined asforced expiratory volume in 1s [FEV1]/forced vital capacity[FVC] <.70) and FEV1 <80% of predicted normal values wereinitially selected. Thereafter, all FFM depleted patients withcomplete data for main outcome analysis (nZ31) and nondepletedpatients matched for age and sex to depleted patients (nZ31) wereincluded in the study analyses (fig 1). Patients also had diseasestability indicated by no change in medication dosage or exacer-bation of symptoms in the preceding 4 weeks.
The study was approved by the local ethics committee, and allsubjects gave written informed consent to participate in thePR program.
Design
This was a single-center, retrospective case-control study ofparticipants in a 12-week PR program. Exercise capacity (6-minutewalk distance), HRQOL using the St. George Respiratory Ques-tionnaire (SGRQ), and nutritional status were evaluated at baselineand after completion of PR (last day up to the following week).Effects of PR were analyzed according to patients’ FFM status, asmeasured by bioelectric impedance analysis. They were considereddepleted if FFM index was �15kg/m2 in women and �16kg/m2
in men.4
Pulmonary rehabilitation
Subjects participated in a standard comprehensive outpatient reha-bilitation program comprising endurance training and individuallyprescribed resistance training for 36 sessions over 12 weeks.
Aerobic exercise training was performed on a treadmill aimingto achieve the maximum tolerated exercise intensity for at least 20minutes. Speed was anchored to perceived effort ranked frommoderate to intense, according to the Borg scale.22 Thus, at thebeginning of each week, new increased speed was set in order tomaintain moderate to intense effort perception.
Resistance training involved gym equipmenta and free weights.Before being tested for 1 repetition maximum (RM), subjectsperformed 3 series of 15 light-weight repetitions for the musclegroup to be tested. Loads were initially set at 50% to 60% of 1RM during the first 2 weeks, and then they were graduallyincreased each week, as tolerated, toward 85% of 1 RM.23
Thereafter, the training workload was increased when more than12 repetitions per set could be performed. Resistance training wasperformed after aerobic training consisting of 2 sets per musclegroup, each of 8 to 12 repetitions.10 Exercises to strengthen theupper body included bench press (pectoralis), chest cross (hori-zontal flexion of the shoulder joint), shoulder press (trapezius),pull downs (latissimus dorsi), biceps flexion, triceps extens-ions, and exercises for abdominal muscles (sit-ups). Lower-body exercises included knee extension, knee flexion, andplantar flexion.
Dietary intake was advised based on 3-day food diaries,24-hour recall dietetic analysis, and nutritional status, as evalu-ated by body mass index (BMI). Subjects were managedaccording to their needs and nutritional status. Low-weightpatients (BMI <22kg/m2) or those considered to ingest insuffi-cient food received specific instruction to fulfill minimum dailyenergetic needs according to the total energetic value method,24
www.archives-pmr.org

Fig 1 Flowchart of study groups’ formation.
Rehabilitation in chronic obstructive pulmonary disease 3
aiming to consume 55% of carbohydrates, 30% lipids, and15% to 20% proteins. Total energetic value was estimatedthrough the basal metabolic rate multiplied by an activity factor(1.5) for light to moderately active subjects. After initial nutri-tional orientation, if caloric ingestion was judged inadequate,a daily polysaccharide supplementation (oral maltodextrinpowder) was recommended to make up to 15% of daily carbo-hydrate needs.
Measurements
SpirometrySpirometric tests were performed using the spirometer,b accordingto published standard.25 Subjects completed at least 3 acceptablemaximal forced expiratory maneuvers before and 20 minutes after400mg inhaled salbutamol. The intraclass correlation coefficientwas described in a previous article26 as .99 and .95 for FVC andFEV1, respectively.
DyspneaDyspnea was evaluated by the modified Medical Research Council(MRC) scale, a 5-point scale that considers certain activities thatprovoke breathlessness.27 Patients had to grade their self-perceived dyspnea by using predefined statements (eg, 0: “I onlyget breathless with strenuous exercise”; 1: “I get short of breathwhen hurrying on the level or up a slight hill”; 2: “I walk slowerthan people of the same age on the level because of breathlessnessor have to stop for breath when walking at my own pace on the
www.archives-pmr.org
level”; 3: “I stop for breath after walking 90 to 100 meters (100yd)or after a few minutes on the level”; and 4: “I am too breathless toleave the house or breathless when dressing or undressing”).Patients were asked about their perceived breathlessness accordingto descriptive statements and classified into MRC dyspnea grades.Interobserver agreement in ratings of dyspnea using the MRCscale evaluated by weighted kappa was .92.28
Body compositionBody composition was measured noninvasively using whole-bodybioelectric impedance.c FFM was estimated using a specificregression equation described for patients with COPD.29 Duringthe measurement, patients lay in a supine position, clothed butwithout shoes or socks. Any metal object attached to the body wasremoved. Two electrodes were positioned on the dorsal surface ofthe right hand, and 2 additional electrodes were positioned on thedorsal surface of the right foot. The skin under the electrodes wascleaned with alcohol, and a thin layer of electrolyte gel wasapplied to each electrode before application. Measurements weremade after 6 hours of fasting and within 30 minutes after voiding.Patients were instructed to neither exercise nor ingest fatty foods24 hours beforehand. Alcoholic beverages were forbidden at least48 hours beforehand. Reliability of bioelectric impedance analysisindicates an intraclass correlation coefficient of .98 in patientswith COPD.30
Quality of life assessmentThe SGRQ measures disease-specific health status, and a locallanguage validated version was used.31 The answers to its 50 items
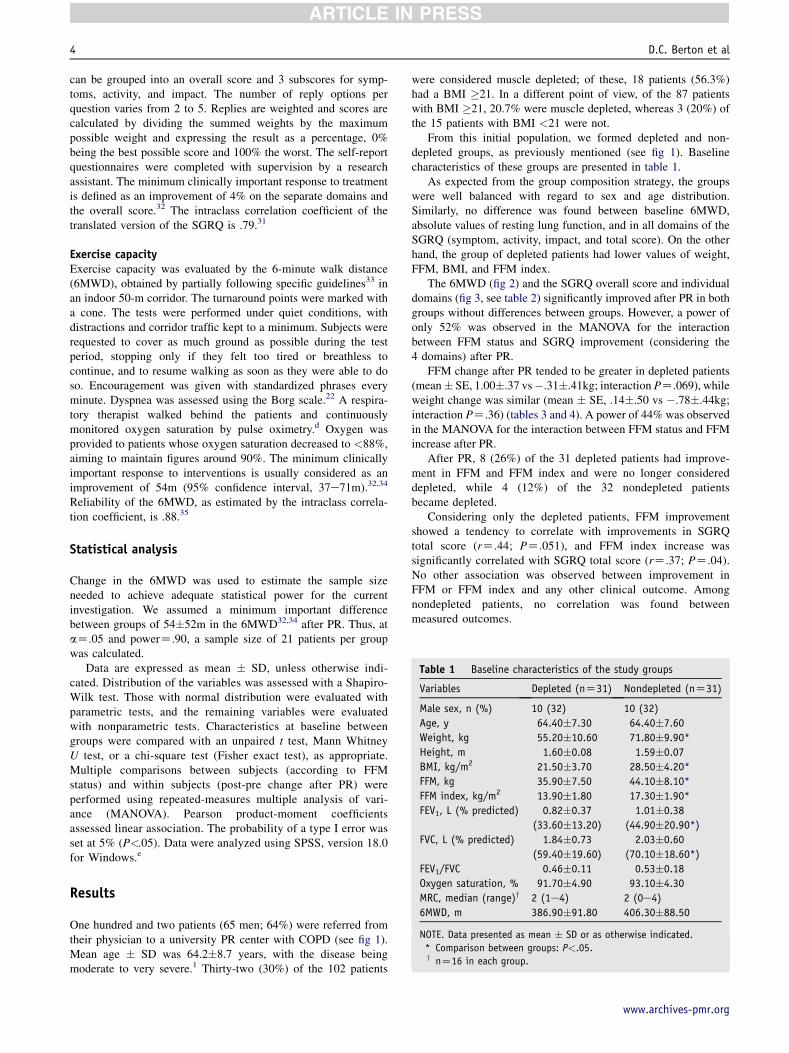
Table 1 Baseline characteristics of the study groups
Variables Depleted (nZ31) Nondepleted (nZ31)
Male sex, n (%) 10 (32) 10 (32)
Age, y 64.40�7.30 64.40�7.60
Weight, kg 55.20�10.60 71.80�9.90*
Height, m 1.60�0.08 1.59�0.07
BMI, kg/m2 21.50�3.70 28.50�4.20*
FFM, kg 35.90�7.50 44.10�8.10*
FFM index, kg/m2 13.90�1.80 17.30�1.90*
FEV1, L (% predicted) 0.82�0.37 1.01�0.38
(33.60�13.20) (44.90�20.90*)
FVC, L (% predicted) 1.84�0.73 2.03�0.60
(59.40�19.60) (70.10�18.60*)
FEV1/FVC 0.46�0.11 0.53�0.18
Oxygen saturation, % 91.70�4.90 93.10�4.30
MRC, median (range)y 2 (1e4) 2 (0e4)
6MWD, m 386.90�91.80 406.30�88.50
NOTE. Data presented as mean � SD or as otherwise indicated.
* Comparison between groups: P<.05.y nZ16 in each group.
4 D.C. Berton et al
can be grouped into an overall score and 3 subscores for symp-toms, activity, and impact. The number of reply options perquestion varies from 2 to 5. Replies are weighted and scores arecalculated by dividing the summed weights by the maximumpossible weight and expressing the result as a percentage, 0%being the best possible score and 100% the worst. The self-reportquestionnaires were completed with supervision by a researchassistant. The minimum clinically important response to treatmentis defined as an improvement of 4% on the separate domains andthe overall score.32 The intraclass correlation coefficient of thetranslated version of the SGRQ is .79.31
Exercise capacityExercise capacity was evaluated by the 6-minute walk distance(6MWD), obtained by partially following specific guidelines33 inan indoor 50-m corridor. The turnaround points were marked witha cone. The tests were performed under quiet conditions, withdistractions and corridor traffic kept to a minimum. Subjects wererequested to cover as much ground as possible during the testperiod, stopping only if they felt too tired or breathless tocontinue, and to resume walking as soon as they were able to doso. Encouragement was given with standardized phrases everyminute. Dyspnea was assessed using the Borg scale.22 A respira-tory therapist walked behind the patients and continuouslymonitored oxygen saturation by pulse oximetry.d Oxygen wasprovided to patients whose oxygen saturation decreased to <88%,aiming to maintain figures around 90%. The minimum clinicallyimportant response to interventions is usually considered as animprovement of 54m (95% confidence interval, 37e71m).32,34
Reliability of the 6MWD, as estimated by the intraclass correla-tion coefficient, is .88.35
Statistical analysis
Change in the 6MWD was used to estimate the sample sizeneeded to achieve adequate statistical power for the currentinvestigation. We assumed a minimum important differencebetween groups of 54�52m in the 6MWD32,34 after PR. Thus, ataZ.05 and powerZ.90, a sample size of 21 patients per groupwas calculated.
Data are expressed as mean � SD, unless otherwise indi-cated. Distribution of the variables was assessed with a Shapiro-Wilk test. Those with normal distribution were evaluated withparametric tests, and the remaining variables were evaluatedwith nonparametric tests. Characteristics at baseline betweengroups were compared with an unpaired t test, Mann WhitneyU test, or a chi-square test (Fisher exact test), as appropriate.Multiple comparisons between subjects (according to FFMstatus) and within subjects (post-pre change after PR) wereperformed using repeated-measures multiple analysis of vari-ance (MANOVA). Pearson product-moment coefficientsassessed linear association. The probability of a type I error wasset at 5% (P<.05). Data were analyzed using SPSS, version 18.0for Windows.e
Results
One hundred and two patients (65 men; 64%) were referred fromtheir physician to a university PR center with COPD (see fig 1).Mean age � SD was 64.2�8.7 years, with the disease beingmoderate to very severe.1 Thirty-two (30%) of the 102 patients
were considered muscle depleted; of these, 18 patients (56.3%)had a BMI �21. In a different point of view, of the 87 patientswith BMI �21, 20.7% were muscle depleted, whereas 3 (20%) ofthe 15 patients with BMI <21 were not.
From this initial population, we formed depleted and non-depleted groups, as previously mentioned (see fig 1). Baselinecharacteristics of these groups are presented in table 1.
As expected from the group composition strategy, the groupswere well balanced with regard to sex and age distribution.Similarly, no difference was found between baseline 6MWD,absolute values of resting lung function, and in all domains of theSGRQ (symptom, activity, impact, and total score). On the otherhand, the group of depleted patients had lower values of weight,FFM, BMI, and FFM index.
The 6MWD (fig 2) and the SGRQ overall score and individualdomains (fig 3, see table 2) significantly improved after PR in bothgroups without differences between groups. However, a power ofonly 52% was observed in the MANOVA for the interactionbetween FFM status and SGRQ improvement (considering the4 domains) after PR.
FFM change after PR tended to be greater in depleted patients(mean� SE, 1.00�.37 vs�.31�.41kg; interaction PZ.069), whileweight change was similar (mean � SE, .14�.50 vs �.78�.44kg;interaction PZ.36) (tables 3 and 4). A power of 44% was observedin the MANOVA for the interaction between FFM status and FFMincrease after PR.
After PR, 8 (26%) of the 31 depleted patients had improve-ment in FFM and FFM index and were no longer considereddepleted, while 4 (12%) of the 32 nondepleted patientsbecame depleted.
Considering only the depleted patients, FFM improvementshowed a tendency to correlate with improvements in SGRQtotal score (rZ.44; PZ.051), and FFM index increase wassignificantly correlated with SGRQ total score (rZ.37; PZ.04).No other association was observed between improvement inFFM or FFM index and any other clinical outcome. Amongnondepleted patients, no correlation was found betweenmeasured outcomes.
www.archives-pmr.org

Fig 2 Similar improvement in 6MWD changes after PR in patients
with (black) and without (white) FFM depletion. Data are shown as
mean � SE. *P<.05 comparing before and after PR within group.
Table 2 HRQOL before and after PR
Variables
Depleted (nZ31) Nondepleted (nZ31)
Before After Before After
SGRQ symptom 49.6�20.4 36.7�19.6* 49.9�19.5 29.1�13.4*
SGRQ activity 67.8�26.7 58.7�19.1* 72.0�18.7 45.5�23.4*
SGRQ impact 36.4�18.2 24.6�17.8* 32.8�15.0 17.8�15.0*
SGRQ total score 51.0�16.7 37.1�15.6* 47.3�13.3 29.1�15.3*
NOTE. Data presented as mean � SD.
* Comparison pre- and postrehabilitation within subjects; P<.05.
Rehabilitation in chronic obstructive pulmonary disease 5
Characteristics of the depleted patients that becamenondepleted after PR
Depleted patients that improved their nutritional status after PRhad greater weight (62.6�7.6 vs 52.6�14.4; PZ.02), BMI, andFFM index (15.1�1.3 vs 13.5�1.4; P<.03), as expected. Otherbaseline characteristics were similar. Compared with those thatremained depleted after PR, improvements in the 6MWD, SGRQscores, and weight were the same.
Discussion
This study demonstrated that clinical improvement in exercisecapacity and HRQOL after PR were achieved independently of thenutritional status by patients with COPD. However, the presentdata had a small observed power to detect significant differencesbetween groups in HRQOL changes. Nonetheless, both groupshad improvements in HRQOL greater than the minimum consid-ered clinically important. Also, FFM gain tended to be greater inpatients with FFM depletion (see tables 3 and 4). This change in
Fig 3 SGRQ changes after PR contrasting patients with (black) and
without (white) FFM mass depletion. Data are shown as mean � SE.
*P<.05 comparing before and after PR within group.
www.archives-pmr.org
body composition had marginal association with HRQOL (SGRQoverall score) improvement in depleted patients (rZ.44;PZ.051), while it was not associated with any other clinicalimprovements in any group.
Improvement in the 6MWD and HRQOL are known benefitsby PR in COPD patients.10,11 Our data corroborate that thesebenefits could be achieved in COPD patients independently ofFFM status. Improvement in exercise capacity was unequivocallysimilar in both groups. Although none of the groups exhibited thetraditional clinically meaningful mean improvement (>54m), bothachieved an updated value of minimum important difference forthe 6MWD of 25m.36 Despite the absence of statistical signifi-cance, final values of all domains (see table 2) and change after PRof symptom and activity scores (see fig 3) of the SGRQ seem to beworse in depleted patients.
The majority of previous studies that investigated improvementin the muscle mass of FFM depleted COPD patients in the contextof PR employed generous specific caloric19 or pharmacologicanabolic37,38 supplementation associated with exercise training anddid not directly compare them with nondepleted COPD patients.All these studies consistently demonstrated improvement in FFMwith different associated exercise training modalities (ie, strength38
or aerobic19,37). Furthermore, when analyzing only patients whoperformed exercise training and did not receive anabolic supple-mentation, like our data, the parameter of exercise capacityimproved, whereas the parameter of HRQOL showed conflictingresults.19,37 On the other hand, 1 study20 stratified depleted andnondepleted COPD patients, comparing aerobic training isolated orcombined with nutritional supplementation alone or associatedwith androgenic administration. Both supplemented arms showeda significant and similar improvement in FFM (around 1.9�2.5kg),while no significant increase was observed in the arm that used onlyexercise. In that study,20 the exercise training plus nutritional
Table 3 Anthropometrics characteristics before and after PR
contrasting depleted and nondepleted patients
Variables
Depleted (nZ31) Nondepleted (nZ31)
Before After Before After
Weight, kg 55.2�10.6 55.4�9.4 72.4�9.5* 71.6�9.4*
BMI, kg/m2 21.5�3.7 21.6�3.5 28.7�4.1* 28.3�4.1*
FFM, kg 35.8�7.5 36.8�7.3 44.2�8.2* 43.9�8.3*
FFM index, kg/m2 13.9�1.8 14.1�1.7 17.3�1.9* 17.2�2.2*
NOTE. Data presented as mean � SD. No difference was found in
comparison pre- and postrehabilitation within group.
* Comparison between depleted and nondepleted subjects in a given
moment (before or after PR); P<.05.

Table 4 Significance (P) of main effects between and within
subjects as well as interactions (variable vs FFM depletion status)
of the global model and for each variable inside a determined
group (anthropometrics, SGRQ, and 6MWD)
Variables
Between
Subjects
Within
Subjects Interaction
Anthropometrics .000 .499 .034
Weight .000 .374 .200
BMI .000 .290 .095
FFM .000 .497 .069
FFM index .000 .577 .096
SGRQ .489 .000 .137
Symptom .313 .000 .194
Activity .330 .000 .009
Impact .150 .000 .480
Total .085 .000 .271
6MWD .305 .000 .805
6 D.C. Berton et al
supplementation arm had a greater FFM improvement in depletedcompared with nondepleted patients, and this finding had noinfluence on exercise capacity increase after PR. The main differ-ence with regard to our study is that the former study was con-ducted in an inpatient rehabilitation center allowing strict controlover daily caloric intake.
In contrast with our results, Franssen et al,39 studying onlynondepleted COPD patients, were able to induce FFM increasethrough an intensive inpatient exercise training program. In thatstudy,39 changes in FFM correlated weakly with changes inmaximal oxygen consumption (rZ.36; P<.05) but did not corre-late with changes in peak work rate or quadriceps strength. Again,these discrepant findings compared with our study could beattributed in part to the greater control in an inpatient program.
The strength exercise protocol used in the present study wasalmost the same as previously reported in another study toincrease FFM in COPD patients.40 What can be inferred from thepresent and all other previously cited studies19,20,37-39 is thatstrength training can increase FFM in COPD patients with orwithout depletion. The fundamental condition for this to occur isto provide an adequate nutritional support. Although dietaryintake was not rigidly controlled in the present study, onlydepleted patients received nutritional orientation and recommen-dations for caloric supplementation, as necessary (see Methodssection). Therefore, we speculate that nutritional counseling wasthe differential factor, which, associated with strength exercisetraining, could result in a tendency to greater FFM gains indepleted patients.
Increase in estimated muscle mass had no significant associ-ation with improvement in exercise capacity both in depleted20
and nondepleted patients.39 This suggests that effects on cellularenergy and intermediary metabolism should be considered toexplain the main benefits of exercise training independently ofmuscle mass. Bernard et al,40 aiming to investigate the effects ofadditional strength training on aerobic exercise in COPD patients,showed that strength training is effective in increasing musclemass. This change, however, did not translate into furtherimprovement in exercise tolerance or quality of life. Besides FFMgain, an increase in muscle function would also contribute to animprovement in HRQOL. Therefore, we believe that this is thereason why the association between increase in FFM and HRQOLwas only marginal.
The present study corroborates literature evidence that, despitemuscle depletion (and probably dysfunction) in some COPDpatients, a comprehensive rehabilitation program is able topromote important clinical improvements in muscle depleted41
and underweight COPD patients.42,43 Furthermore, depletedpatients tended to achieve significant gains in FFM. Therefore,exercise training is indicated for FFM depleted patientswith COPD.
Study limitations
Our study is underpowered to detect differences in HRQOLchange after PR between depleted and nondepleted patients.Nonetheless, FFM depleted patients could improve HRQOL ina clinically (4 units reduction) and statistically significant wayafter PR (see table 2 and fig 3).
FFM increase had practically no association with clinicalimprovements in depleted patients. Skeletal appendicular musclestrength, respiratory muscle pressures, and local measures ofmuscle mass were not evaluated. These measurements would beworth doing with the aim of assessing the whole benefit of PR whencomparing depleted and nondepleted COPD patients and mightprovide deeper insights regarding functional versus anatomicalimprovements in muscle performance. Such investigation couldcorroborate the inference that improved muscle function shouldoccur independently of muscle mass. Better muscles might result inincreased exercise capacity and reduced symptoms, which could betranslated into improved HRQOL. We did not assess exercisedyspnea and limitation with a cardiopulmonary exercise test;however, it could represent a valuable method for evaluatingmaximal exercise constraints before and after PR.
Finally, the possibility of bias introduced by the way the casesand controls were selected is a limitation inherent of thestudy design.
Conclusions
FFM depleted COPD patients participating in a comprehensiveoutpatient rehabilitation program obtained the same clinical gainsin exercise capacity as FFM nondepleted patients. Additionally,both groups achieved important clinical improvement in HRQOL.The increment in FFM tended to be greater in depleted patients,and this had no relation with clinical outcomes.
Suppliersa. Aston; Sportmania, Avenida Victor Hugo Kunz, 2295, Novo
Hamburgo, Brazil.b. Microlab 3500; Cardinal Health UK,Tamussino, Rua Dr. Bar-
ros Cassal, 734, Porto Alegre, Brazil.c. Bodystat 1500; Nutricao Total Ltda. Rua Maestro Cardim,
1175. Sao Paulo, Brazil.d. Moriya 1001; J.G MORIYA, SP, Rua da Uniao 377, Sao Paulo,
Brazil.e. SPSS, 233 S Wacker Dr, 11th Fl, Chicago, IL 60606.
Keywords
Exercise; Muscles; Pulmonary disease, chronic obstructive;Rehabilitation
www.archives-pmr.org

Rehabilitation in chronic obstructive pulmonary disease 7
Corresponding author
Danilo C. Berton, MD, ScD, Dept of Pulmonology, ClinicalHospital of Porto Alegre, Federal University of Rio Grande doSul, Porto Alegre, Brazil, Rua Ramiro Barcelos, 2350 e Sala2050e CEP (Postal Code): 90035-003, Porto Alegre, RS, Brasil.E-mail address: [email protected].
References
1. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis,
management, and prevention of chronic obstructive pulmonary
disease: GOLD executive summary. Am J Respir Crit Care Med 2007;
176:532-55.
2. Gosselink R, Troosters T, Decramer M. Peripheral muscle weakness
contributes to exercise limitation in COPD. Am J Respir Crit Care
Med 1996;153:976-80.
3. Maltais F, Simard AA, Simard C, Jobin J, Desgagnes P, LeBlanc P.
Oxidative capacity of the skeletal muscle and lactic acid kinetics
during exercise in normal subjects and in patients with COPD. Am
J Respir Crit Care Med 1996;153:288-93.
4. Baarends EM, Schols AM, Mostert R, Wouters EF. Peak exercise
response in relation to tissue depletion in patients with chronic
obstructive pulmonary disease. Eur Respir J 1997;10:2807-13.
5. Engelen MP, Schols AM, Baken WC, Wesseling GJ, Wouters EF.
Nutritional depletion in relation to respiratory and peripheral skeletal
muscle function in out-patients with COPD. Eur Respir J 1994;7:
1793-7.
6. Schols AM, Broekhuizen R, Weling-Scheepers CA, Wouters EF. Body
composition and mortality in chronic obstructive pulmonary disease.
Am J Clin Nutr 2005;82:53-9.
7. Slinde F, Gronberg A, Engstrom CP, Rossander-Hulthen L, Larsson S.
Body composition by bioelectrical impedance predicts mortality in
chronic obstructive pulmonary disease patients. Respir Med 2005;99:
1004-9.
8. Marquis K, Debigare R, Lacasse Y, et al. Midthigh muscle cross-
sectional area is a better predictor of mortality than body mass
index in patients with chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 2002;166:809-13.
9. Vestbo J, Prescott E, Almdal T, et al. Body mass, fat-free body mass,
and prognosis in patients with chronic obstructive pulmonary disease
from a random population sample: findings from the Copenhagen City
Heart Study. Am J Respir Crit Care Med 2006;173:79-83.
10. Nici L, Donner C, Wouters E, et al. American Thoracic Soci-
ety/European Respiratory Society statement on pulmonary rehabili-
tation. Am J Respir Crit Care Med 2006;173:1390-413.
11. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary Rehabilitation:
Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines.
Chest 2007;131(5 Suppl):4S-42S.
12. Bjoernshave B, Korsgaard J, Nielsen CV. Does pulmonary rehabili-
tation work in clinical practice? A review on selection and dropout in
randomized controlled trials on pulmonary rehabilitation. Clin Epi-
demiol 2010;2:73-83.
13. Fischer MJ, Scharloo M, Abbink JJ, et al. Drop-out and attendance in
pulmonary rehabilitation: the role of clinical and psychosocial vari-
ables. Respir Med 2009;103:1564-71.
14. Garrod R, Marshall J, Barley E, Jones PW. Predictors of success and
failure in pulmonary rehabilitation. Eur Respir J 2006;27:788-94.
15. Van Helvoort HA, Heijdra YF, Thijs HM, Vina J, Wanten GJ,
Dekhuijzen PN. Exercise-induced systemic effects in muscle-wasted
patients with COPD. Med Sci Sports Exerc 2006;38:1543-52.
16. Engelen MP, Wouters EF, Deutz NE, Does JD, Schols AM. Effects of
exercise on amino acid metabolism in patients with chronic obstruc-
tive pulmonary disease. Am J Respir Crit Care Med 2001;163:859-64.
17. Reid MB. COPD as a muscle disease. Am J Respir Crit Care Med
2001;164:1101-2.
www.archives-pmr.org
18. CouillardA,MaltaisF,SaeyD,et al.Exercise-inducedquadricepsoxidative
stress and peripheral muscle dysfunction in patients with chronic obstruc-
tive pulmonary disease. Am J Respir Crit Care Med 2003;167:1664-9.
19. Creutzberg EC, Wouters EF, Mostert R, Weling-Scheepers CA,
Schols AM. Efficacy of nutritional supplementation therapy in depleted
patients with chronic obstructive pulmonary disease. Nutrition 2003;19:
120-7.
20. Schols AM, Soeters PB, Mostert R, Pluymers RJ, Wouters EF. Phys-
iologic effects of nutritional support and anabolic steroids in patients
with chronic obstructive pulmonary disease. A placebo-controlled
randomized trial. Am J Respir Crit Care Med 1995;152:1268-74.
21. van Wetering CR, Hoogendoorn M, Broekhuizen R, et al. Efficacy and
costs of nutritional rehabilitation in muscle-wasted patients with
chronic obstructive pulmonary disease in a community-based setting:
a prespecified subgroup analysis of the INTERCOM trial. J Am Med
Dir Assoc 2010;11:179-87.
22. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports
Exerc 1982;14:377-81.
23. Storer TW. Exercise in chronic pulmonary disease: resistance exercise
prescription. Med Sci Sports Exerc 2001;33(7 Suppl):S680-92.
24. World Health Organization. Physical status: the use and interpretation
of anthropometry. Geneva: World Health Organization; 1995.
25. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of
spirometry. Eur Respir J 2005;26:319-38.
26. Masa JF, Gonzalez MT, Pereira R, et al. Validity of spirometry per-
formed online. Eur Respir J 2011;37:911-8.
27. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA.
Usefulness of the Medical Research Council (MRC) dyspnoea scale as
a measure of disability in patients with chronic obstructive pulmonary
disease. Thorax 1999;54:581-6.
28. Mahler DA, Wells CK. Evaluation of clinical methods for rating
dyspnea. Chest 1988;93:580-6.
29. Schols AM, Wouters EF, Soeters PB, Westerterp KR. Body compo-
sition by bioelectrical-impedance analysis compared with deuterium
dilution and skinfold anthropometry in patients with chronic
obstructive pulmonary disease. Am J Clin Nutr 1991;53:421-4.
30. Steiner MC, Barton RL, Singh SJ, Morgan MD. Bedside methods
versus dual energy X-ray absorptiometry for body composition
measurement in COPD. Eur Respir J 2002;19:626-31.
31. Souza TC, Jardim JR, Jones P. Validacao do Questionario do Hospital
Saint George naDoenca Respiratoria (SGRQ) empacientes portadores de
doenca pulmonar obstrutiva cronica noBrasil. J Pneumol 2000;26:119-28.
32. Cazzola M, MacNee W, Martinez FJ, et al. Outcomes for COPD
pharmacological trials: from lung function to biomarkers. Eur Respir J
2008;31:416-69.
33. ATS Committee on Proficiency Standards for Clinical Pulmonary
Function Laboratories. ATS statement: guidelines for the six-minute
walk test. Am J Respir Crit Care Med 2002;166:111-7.
34. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting
small differences in functional status: the SixMinuteWalk test in chronic
lung disease patients. Am J Respir Crit Care Med 1997;155:1278-82.
35. Sciurba F, Criner GJ, Lee SM, et al. Six-minutewalk distance in chronic
obstructive pulmonary disease: reproducibility and effect of walking
course layout and length. Am J Respir Crit Care Med 2003;167:1522-7.
36. Holland AE, Hill CJ, Rasekaba T, Lee A, Naughton MT,
McDonald CF. Updating the minimal important difference for six-
minute walk distance in patients with chronic obstructive pulmonary
disease. Arch Phys Med Rehabil 2010;91:221-5.
37. Creutzberg EC, Wouters EF, Mostert R, Pluymers RJ, Schols AM. A role
for anabolic steroids in the rehabilitationof patientswithCOPD?Adouble-
blind, placebo-controlled, randomized trial. Chest 2003;124:1733-42.
38. Casaburi R, Bhasin S, Cosentino L, et al. Effects of testosterone and
resistance training in men with chronic obstructive pulmonary disease.
Am J Respir Crit Care Med 2004;170:870-8.
39. Franssen FM, Broekhuizen R, Janssen PP, Wouters EF, Schols AM.
Effects of whole-body exercise training on body composition and
functional capacity in normal-weight patients with COPD. Chest
2004;125:2021-8.

8 D.C. Berton et al
40. Bernard S, Whittom F, Leblanc P, et al. Aerobic and strength training
in patients with chronic obstructive pulmonary disease. Am J Respir
Crit Care Med 1999;159:896-901.
41. Vogiatzis I, Simoes DC, Stratakos G, et al. Effect of pulmonary
rehabilitation on muscle remodelling in cachectic patients with COPD.
Eur Respir J 2010;36:301-10.
42. Lan CC, Yang MC, Lee CH, et al. Pulmonary rehabilitation improves
exercise capacity and quality of life in underweight patients with
chronic obstructive pulmonary disease. Respirology 2011;16:276-83.
43. Sugawara K, Takahashi H, Kasai C, et al. Effects of nutritional
supplementation combined with low-intensity exercise in malnour-
ished patients with COPD. Respir Med 2010;104:1883-9.
www.archives-pmr.org
Copyright © 2022 FDOKUMEN




















